Embed Size (px)
Citation preview
Undergraduate and Graduate Student Coping with
Stressful Experiences: A New Look at the Continuum of Distress,
Suicidal Experiences and Campus Intervention Opportunities
Elizabeth Wilson, Ashley Boynton, Stuart Irvin, & Andrea Saathoff
The University of Texas at Austin
Introduction
Founded in 1991 at the University of Texas at Austin
6 completed studies to date
Membership in Consortium is determined study-by-study, and all are encouraged and welcome to participate
Research is an essential ingredient for defining a specialty of college mental health Penn State’s CSCMH, NCHA, Director’s Surveys, etc.
National Suicide Statistics 2nd leading cause of death on college campuses
National suicide rates for college students range from 6.5 to 7.5 per 100,000 Compared to 16 per 100,000 in age-matched peers
Roughly 25% of campus suicides are counseling center clients, nationally Suicides in CC clients are 3.3 times greater than non-clients When taking into consideration the 4 most significant risk
factors (previous attempts, psychiatric illness, gender, and firearms), you would expect clients of CCs to commit suicide 20 times more than non-clients.
(Schwartz, 2006, 2011)
Overview of Presentation Goals
Broaden the current clinical intervention treatment model to include a preventive, population-focused intervention approach
Explore college student self-report data on suicidal experiences and coping during recent stressors
Sections of presentation Expansion: Intervention approaches and distress/suicidality continuum
Overview of 2011 data Demographics
Nature of stressful period
Suicidal ideation and behavior
Qualities of self: Connectedness /belongingness and sense of coherence
Implications for population-focused prevention
Discussion
“The present era of epidemiology is coming to a close. The focus on risk factors at the individual level- the hallmark of this era- will no longer serve. We need to be concerned equally with causal pathways at the societal level and with pathogenesis and causality at the molecular level.” (Susser & Susser, 1996)
Prevention Campaigns At their core, population prevention programs are
organizational change efforts that often involve legislation and policy adjustments, environmental re-engineering and management, modification of processes/procedures, programmatic interventions, advocacy, and, at times, clinical interventions.
They require two types and waves of linked interventions: Ecological interventions
Psychoeducational proactive interventions
Prevention Campaigns Goal to shift the well-being of the population
Frolich and Potvin (1999) state that when many people lower their risk, even a little, the total benefit for the population is larger than if a few people at high risk experience a large reduction. This is consistent with the notion that groups of individuals function collectively, and as such, are affected by the average functioning of individuals around them.
0
5000
10000
15000
20000
25000
30000
Entire sample This is all just too much
I wish this would all end
I have to escape
I wish I was dead
I want to kill myself
I might kill myself
I will kill myself
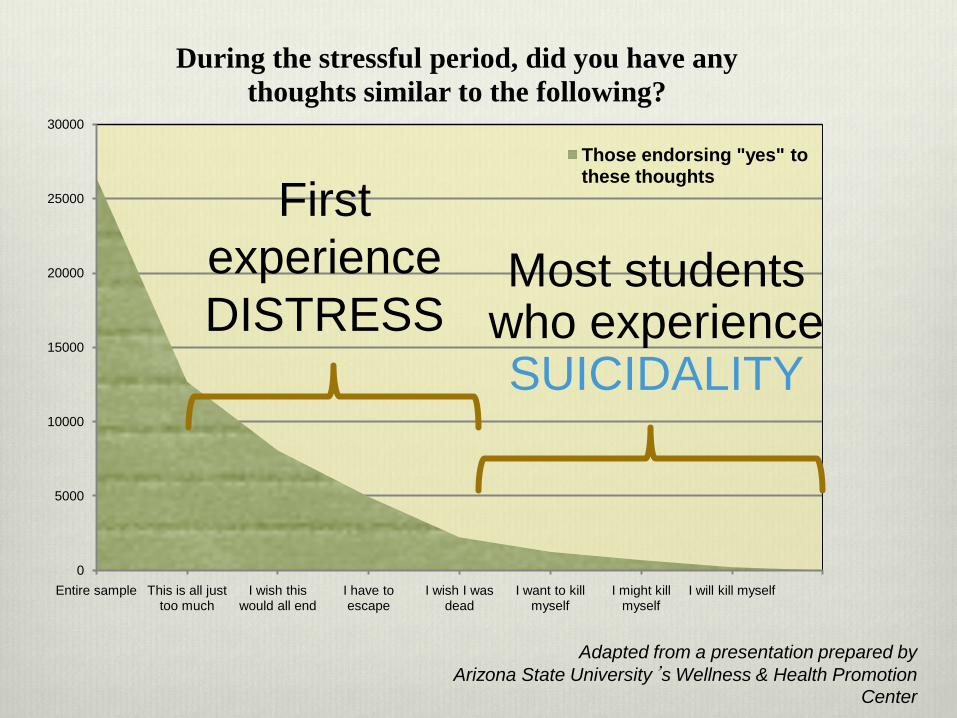
During the stressful period, did you have any thoughts similar to the following?
Those endorsing "yes" to these thoughts
Most students who experience SUICIDALITY
First experience DISTRESS
Adapted from a presentation prepared by Arizona State University’s Wellness & Health Promotion
Center
0
5000
10000
15000
20000
25000
30000
Entire sample This is all just too much
I wish this would all end
I have to escape
I wish I was dead
I want to kill myself
I might kill myself
I will kill myself
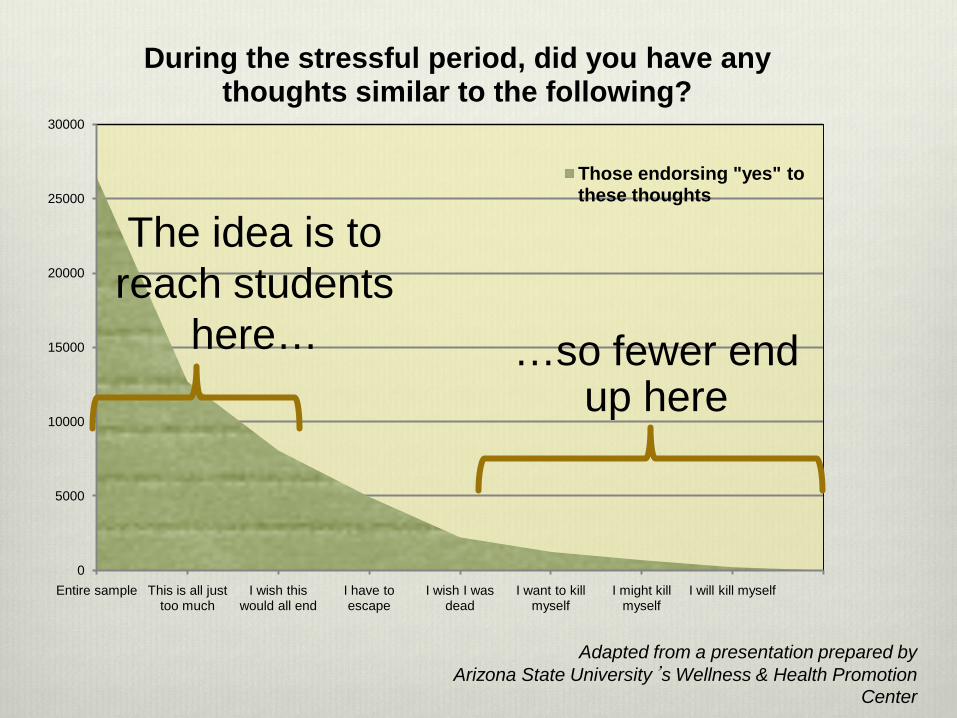
During the stressful period, did you have any thoughts similar to the following?
Those endorsing "yes" to these thoughts
…so fewer end up here
The idea is to reach students
here…
Adapted from a presentation prepared by Arizona State University’s Wellness & Health Promotion
Center
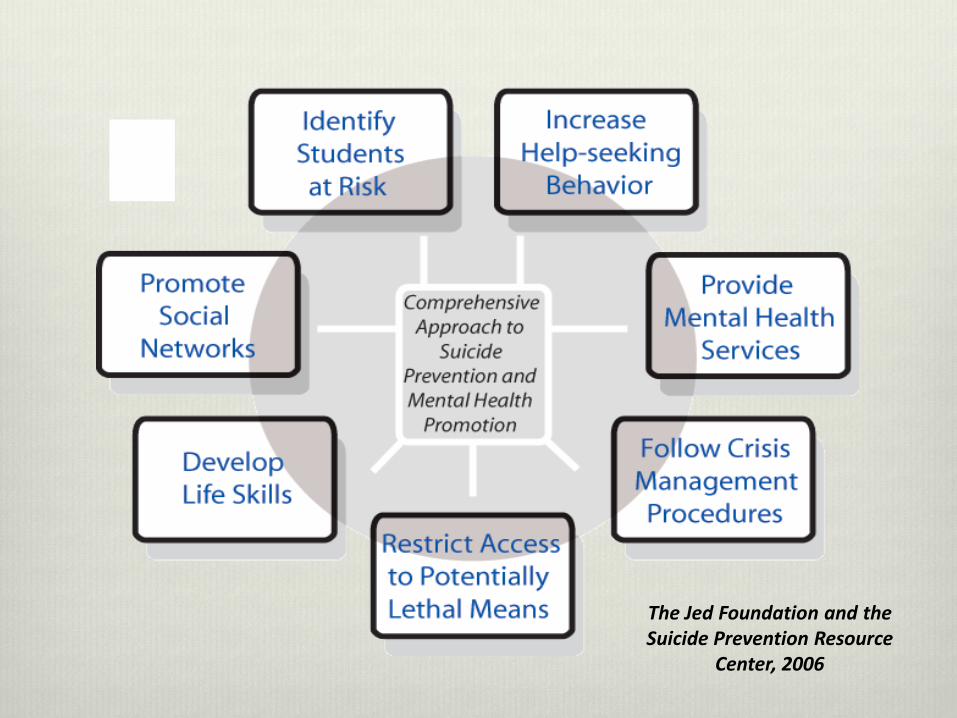
The Jed Foundation and the Suicide Prevention Resource
Center, 2006
Voice of the student…What could your college or university have provided you or
done differently to better help you manage during this stressful time?”
“To be able to talk to a professional for more than an hour or more than once a week.”
“Weekend and/or evening opportunities for counseling on campus.”
Overview of Presentation Sections of presentation
Expansion: Intervention approaches and distress/suicidality continuum
Overview of 2011 data
Demographics
Nature of stressful period
Suicidal ideation and behavior
Qualities of self: Connectedness/belongingness and sense of coherence
Implications for Population-focused prevention
Discussion
Overview of 2011 Data“Undergraduate and Graduate Student Coping
with Stressful Experiences”
“Undergraduate and Graduate Student Coping with Stressful Experiences” (2011)
Brief overview of current study characteristics: Over 26,000 undergraduate and graduate student
responses (~101,000 surveys sent)
74 colleges and universities participated
Random sample at each school
Web-based survey, anonymous, intervention
26% response rate
Demographics fairly comparable to NCHA
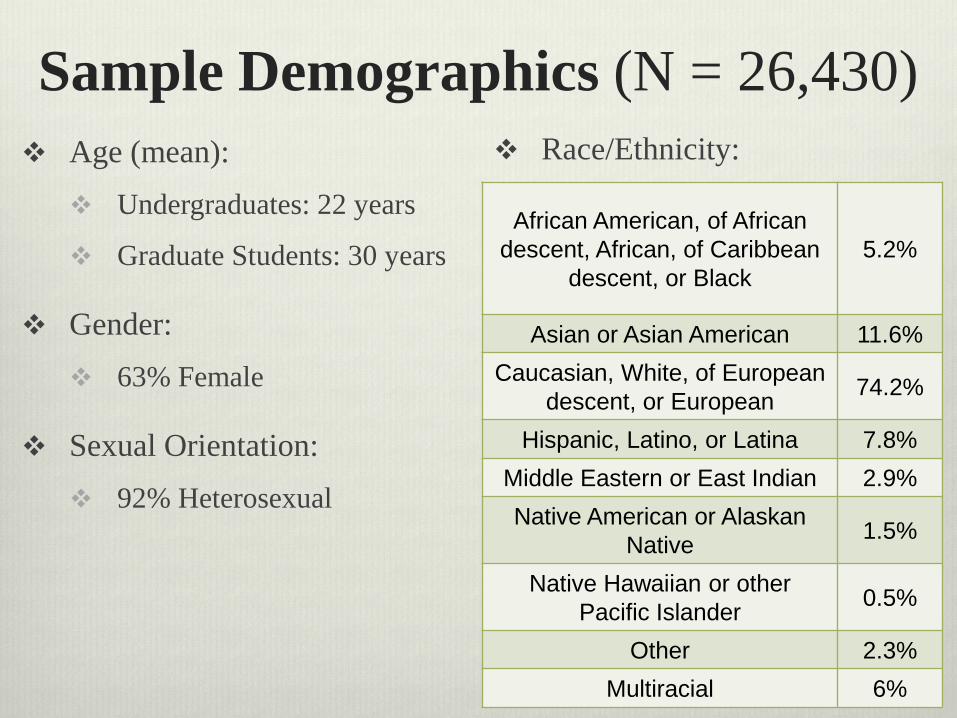
Sample Demographics (N = 26,430) Age (mean):
Undergraduates: 22 years
Graduate Students: 30 years
Gender: 63% Female
Sexual Orientation: 92% Heterosexual
African American, of African descent, African, of Caribbean
descent, or Black5.2%
Asian or Asian American 11.6%Caucasian, White, of European
descent, or European 74.2%
Hispanic, Latino, or Latina 7.8%Middle Eastern or East Indian 2.9%Native American or Alaskan
Native 1.5%
Native Hawaiian or other Pacific Islander 0.5%
Other 2.3%Multiracial 6%
Race/Ethnicity:
Organization of Survey Demographics
Preexisting vulnerabilities
Baseline for Sense of Coherence and Belongingness (Qualities of Self) & Social Connectedness Mindfulness
Stressful period “Please reflect on the most stressful period of time that you have experienced
in the past 12 months…
“Now please focus on the "worst point….”
Coping during stressful period Experiences during the stressful period
What resources were helpful or could have been helpful

Contributors to Stressful PeriodSelect all the apply
N = 26,430
Contributed to stressful time
Academics 73%
Financial problems 31%
Friendship problems 18%
Life transition 27%
Family problems 20%
Death of close family/friend 9%
Emotional health problems 15%
Physical health problems 13%
Problems experienced by others 9%
Problems at work 13%
Other 7.6%
Drugs or alcohol 3.6%
Other traumatic experience 2.4%
Discrimination 2.7%
Sexual orientation concerns 1.5%
Relationship violence 1%
Suicide of close family member/friend 1%
Sexual assault 1%
Gender identity concerns 1%
15% Academic only
27% Non-academic only
58% Combined
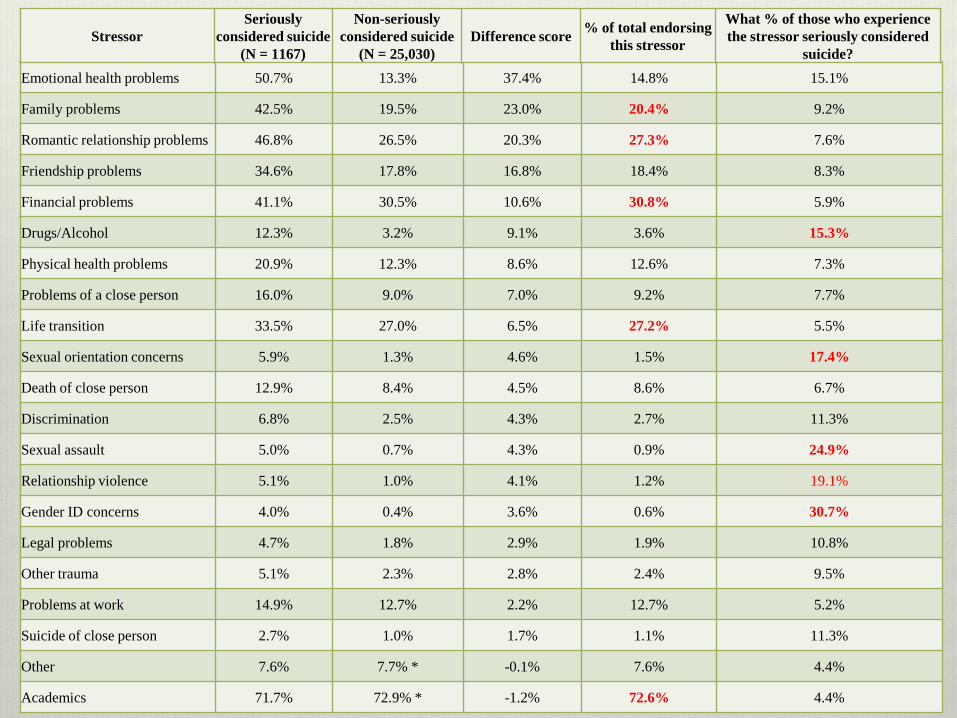
Emotional health problems 50.7% 13.3% 37.4% 14.8% 15.1%
Family problems 42.5% 19.5% 23.0% 20.4% 9.2%
Romantic relationship problems 46.8% 26.5% 20.3% 27.3% 7.6%
Friendship problems 34.6% 17.8% 16.8% 18.4% 8.3%
Financial problems 41.1% 30.5% 10.6% 30.8% 5.9%
Drugs/Alcohol 12.3% 3.2% 9.1% 3.6% 15.3%
Physical health problems 20.9% 12.3% 8.6% 12.6% 7.3%
Problems of a close person 16.0% 9.0% 7.0% 9.2% 7.7%
Life transition 33.5% 27.0% 6.5% 27.2% 5.5%
Sexual orientation concerns 5.9% 1.3% 4.6% 1.5% 17.4%
Death of close person 12.9% 8.4% 4.5% 8.6% 6.7%
Discrimination 6.8% 2.5% 4.3% 2.7% 11.3%
Sexual assault 5.0% 0.7% 4.3% 0.9% 24.9%
Relationship violence 5.1% 1.0% 4.1% 1.2% 19.1%
Gender ID concerns 4.0% 0.4% 3.6% 0.6% 30.7%
Legal problems 4.7% 1.8% 2.9% 1.9% 10.8%
Other trauma 5.1% 2.3% 2.8% 2.4% 9.5%
Problems at work 14.9% 12.7% 2.2% 12.7% 5.2%
Suicide of close person 2.7% 1.0% 1.7% 1.1% 11.3%
Other 7.6% 7.7% * -0.1% 7.6% 4.4%
Academics 71.7% 72.9% * -1.2% 72.6% 4.4%
StressorSeriously
considered suicide (N = 1167)
Non-seriously considered suicide
(N = 25,030)Difference score % of total endorsing
this stressor
What % of those who experience the stressor seriously considered
suicide?
Discussion Are these the contributors to stress that you expected?
How can these be addressed at the population level?
How can these be addressed at the clinical level? More on this to come...
Voice of the student…“Let me know it existed! Let me know it was available – in
all 3 years as a student I did not know there was counseling services available.”
“I wish I knew of counselors on campus sooner. Maybe letting it be known during orientation.”
Overview of Presentation Sections of presentation
Expansion: Intervention approaches and distress/suicidality continuum
Overview of 2011 data
Demographics
Nature of stressful period
Suicidal ideation and behavior
Qualities of self: Connectedness/belongingness and sense of coherence
Implications for Population-focused prevention
Discussion

Suicidal Ideation and BehaviorA look at 2011 student self reports

Self-Reports of LifetimeSuicidal Ideation and Attempts
Suicidal Ideation
Have you ever seriously consideredattempting suicide at some point in
your life?
N = 26,430
20%
Suicide Attempts
How many times in your life have you attempted suicide?
(% indicating 1 or more times)
N = 26,430
6%

When First Considered Suicide
N = 5,319
When did you first seriously consider
attempting suicide?
Before or while in middle school 27%
While in high school 41%
After high school but before college 4%
While in college 19%
After college and before graduate school 4%
While in graduate school 3%
Other 3%
* Of those who considered suicide at some point in their life
72%
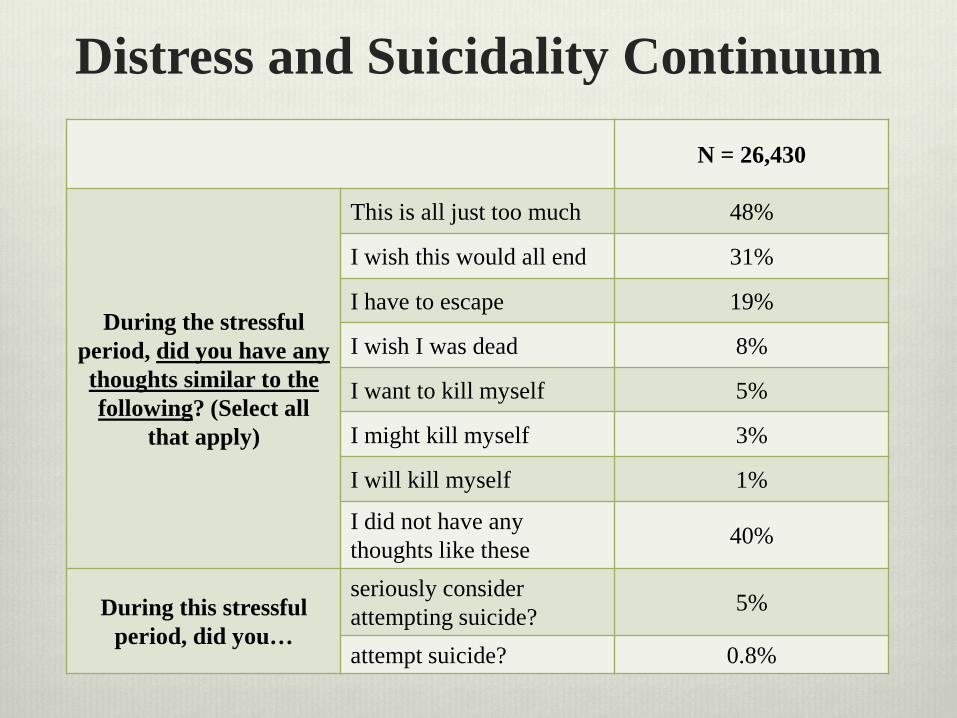
Distress and Suicidality Continuum
N = 26,430
During the stressful period, did you have any thoughts similar to the following? (Select all
that apply)
This is all just too much 48%
I wish this would all end 31%
I have to escape 19%
I wish I was dead 8%
I want to kill myself 5%
I might kill myself 3%
I will kill myself 1%
I did not have any thoughts like these 40%
During this stressful period, did you…
seriously consider attempting suicide? 5%
attempt suicide? 0.8%
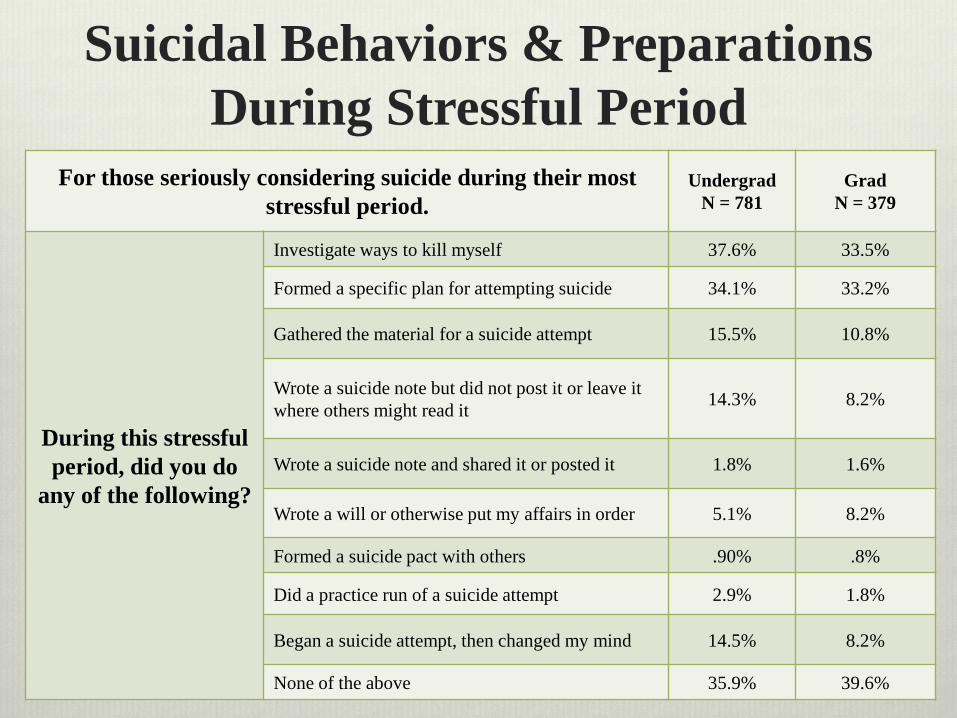
Suicidal Behaviors & Preparations During Stressful Period
For those seriously considering suicide during their most stressful period.
UndergradN = 781
GradN = 379
During this stressful period, did you do
any of the following?
Investigate ways to kill myself 37.6% 33.5%
Formed a specific plan for attempting suicide 34.1% 33.2%
Gathered the material for a suicide attempt 15.5% 10.8%
Wrote a suicide note but did not post it or leave it where others might read it 14.3% 8.2%
Wrote a suicide note and shared it or posted it 1.8% 1.6%
Wrote a will or otherwise put my affairs in order 5.1% 8.2%
Formed a suicide pact with others .90% .8%
Did a practice run of a suicide attempt 2.9% 1.8%
Began a suicide attempt, then changed my mind 14.5% 8.2%
None of the above 35.9% 39.6%
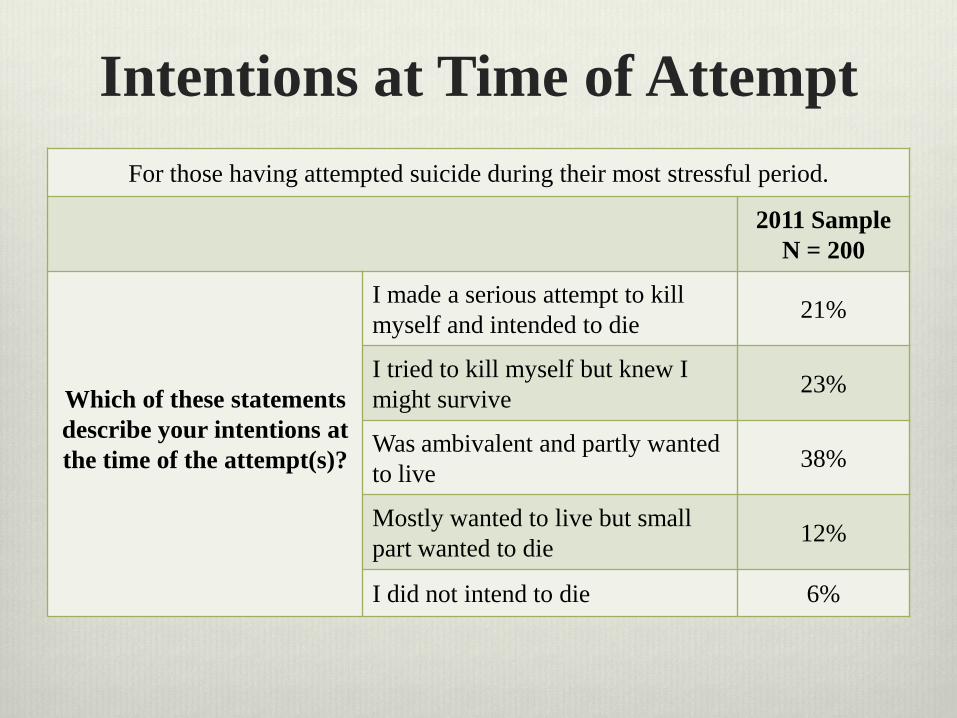
Intentions at Time of AttemptFor those having attempted suicide during their most stressful period.
2011 SampleN = 200
Which of these statementsdescribe your intentions at the time of the attempt(s)?
I made a serious attempt to kill myself and intended to die 21%
I tried to kill myself but knew I might survive 23%
Was ambivalent and partly wanted to live 38%
Mostly wanted to live but small part wanted to die 12%
I did not intend to die 6%
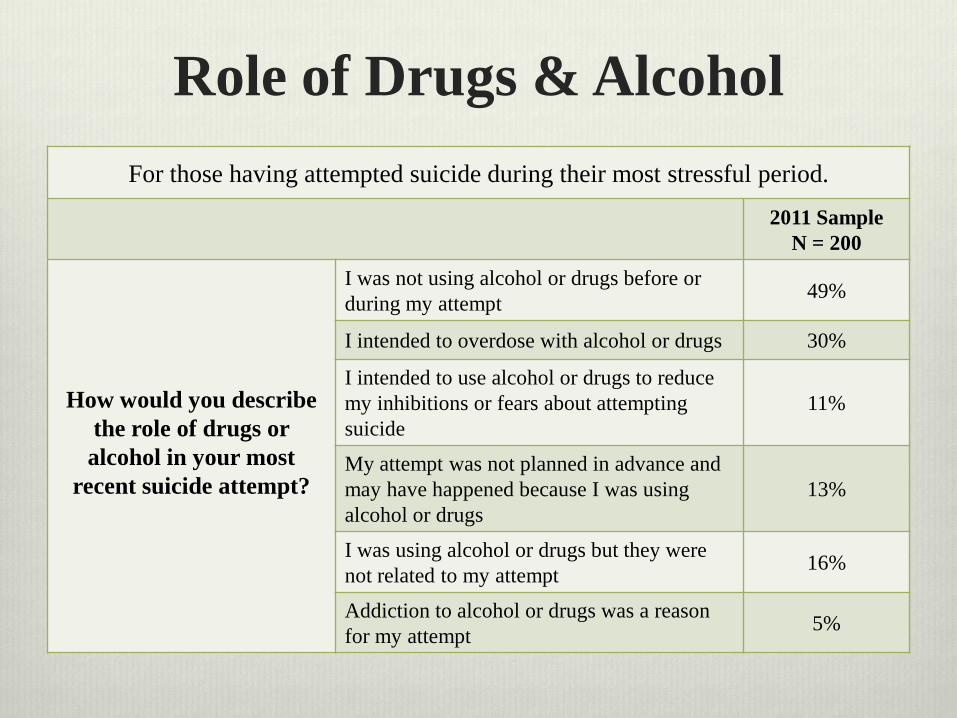
Role of Drugs & AlcoholFor those having attempted suicide during their most stressful period.
2011 SampleN = 200
How would you describe the role of drugs or alcohol in your most
recent suicide attempt?
I was not using alcohol or drugs before or during my attempt 49%
I intended to overdose with alcohol or drugs 30%
I intended to use alcohol or drugs to reduce my inhibitions or fears about attempting suicide
11%
My attempt was not planned in advance and may have happened because I was using alcohol or drugs
13%
I was using alcohol or drugs but they were not related to my attempt 16%
Addiction to alcohol or drugs was a reason for my attempt 5%
Voice of the student…“So many students live off campus and participate in on-line
learning. I think the university counseling service should have on-line services to students.”
“Being able to have a counseling session over the phone, maybe.”
Overview of Presentation Sections of presentation
Expansion: Intervention approaches and distress/suicidality continuum
Overview of 2011 data
Demographics
Nature of stressful period
Suicidal ideation and behavior
Qualities of self: Connectedness/belongingness and sense of coherence
Implications for Population-focused prevention
Discussion
Qualities of SelfConnectedness/Belongingness
and Sense of Coherence
Sense of Coherence Model focusing, not on factors explaining disease, but on factors
that promote health, conceptualizing maintenance or improvement of health on a continuum. ‘Salutogenesis’ coined.
(Antonovsky, 1993)
3 components of SOC: Comprehensibility, manageability, meaningfulness
(Antonovsky, 1993)
Strongly related to perceived health, especially mental health
(Eriksson & Lindstrom, 2006)
Seemingly a health-promoting resource that bolsters resilience
(Eriksson & Lindstrom, 2006)
Social Connectedness & Belongingness
Linked to health and well-being (Armstrong & Oomen-Early, 2009; Baumeister & Leary, 1995;
Joiner et al, 2009)
Theorized to play important role in preventing desire for death (Joiner, 2005)
Increasing social connectedness on college campuses is a key strategy for suicide prevention (SPRC, 2004; CDC 2008)
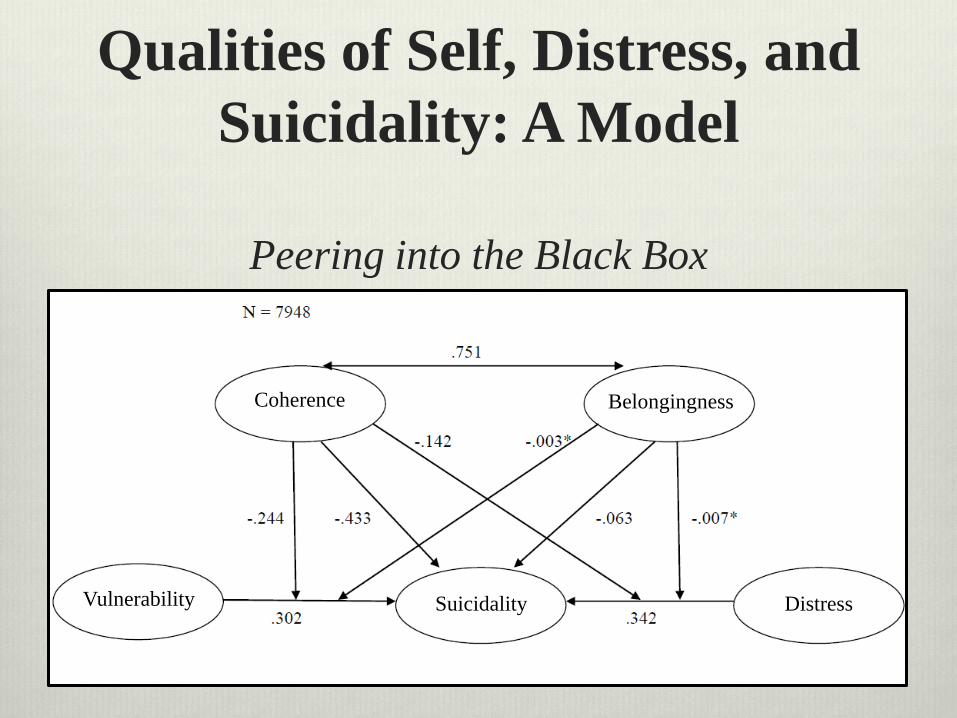
Qualities of Self, Distress, and Suicidality: A Model
Peering into the Black Box
Coherence Belongingness
Suicidality DistressVulnerability
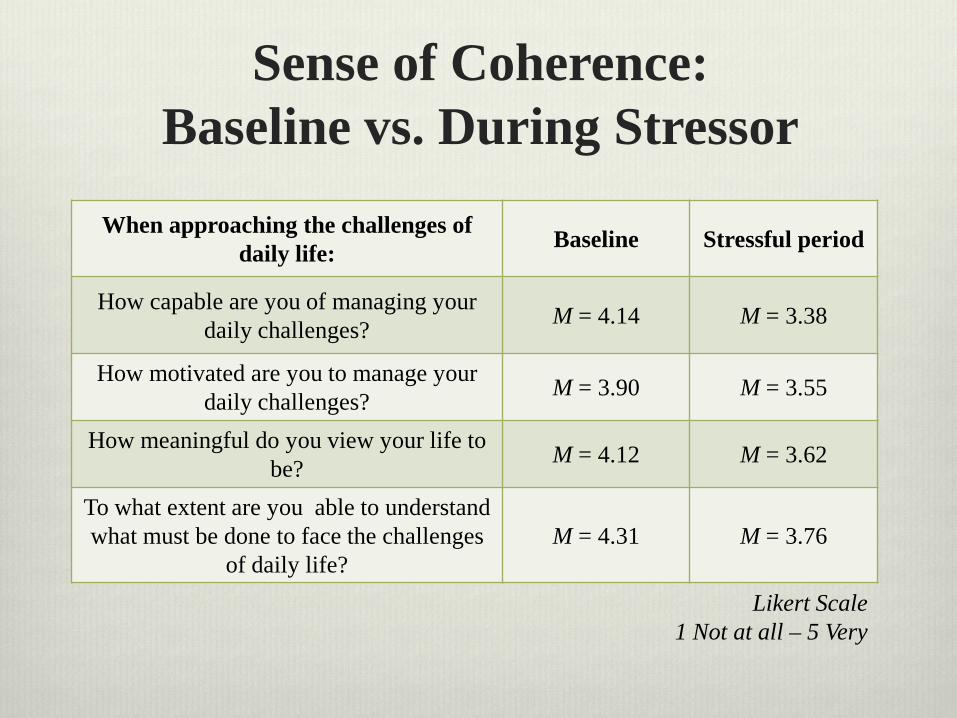
Sense of Coherence:Baseline vs. During Stressor
When approaching the challenges of daily life: Baseline Stressful period
How capable are you of managing your daily challenges? M = 4.14 M = 3.38
How motivated are you to manage your daily challenges? M = 3.90 M = 3.55
How meaningful do you view your life to be? M = 4.12 M = 3.62
To what extent are you able to understand what must be done to face the challenges
of daily life?M = 4.31 M = 3.76
Likert Scale1 Not at all – 5 Very
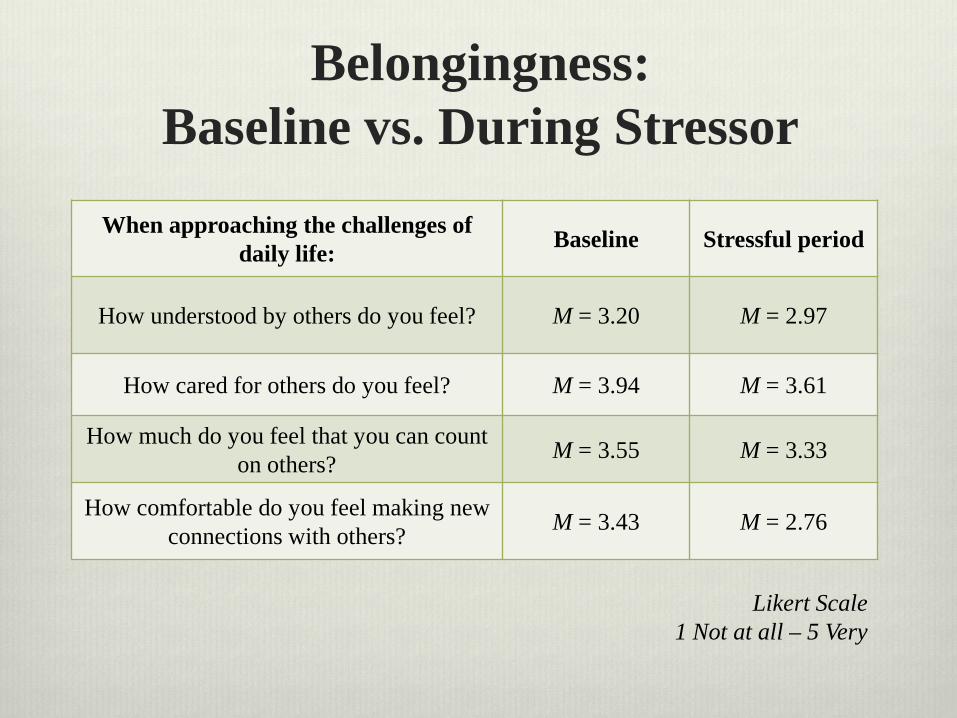
Belongingness:Baseline vs. During Stressor
When approaching the challenges of daily life: Baseline Stressful period
How understood by others do you feel? M = 3.20 M = 2.97
How cared for others do you feel? M = 3.94 M = 3.61
How much do you feel that you can count on others? M = 3.55 M = 3.33
How comfortable do you feel making new connections with others? M = 3.43 M = 2.76
Likert Scale1 Not at all – 5 Very
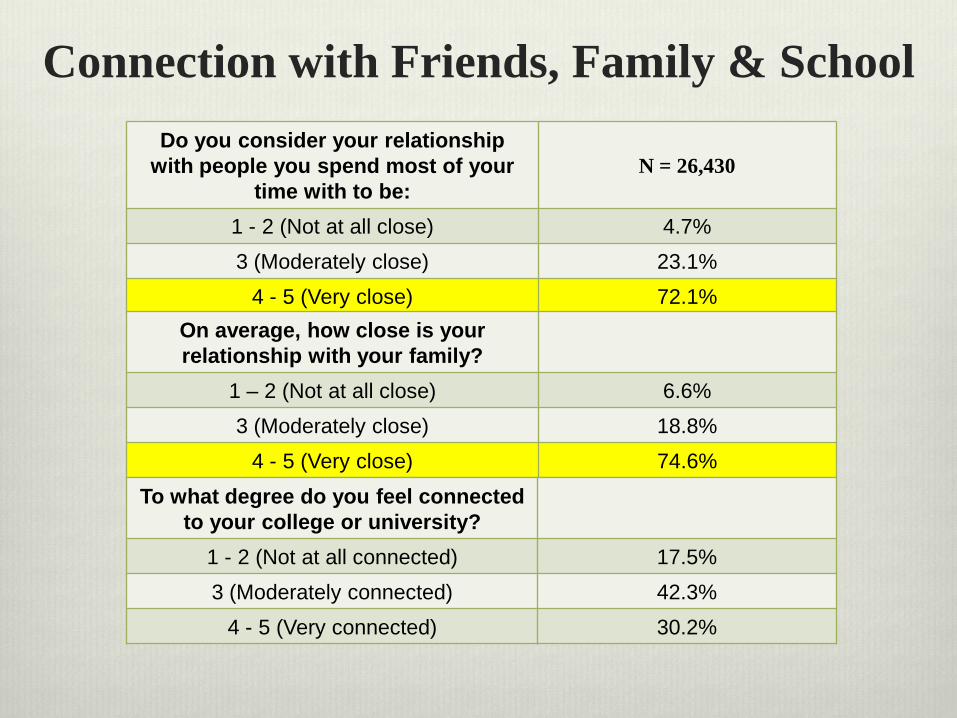
Connection with Friends, Family & School Do you consider your relationship
with people you spend most of your time with to be:
N = 26,430
1 - 2 (Not at all close) 4.7%3 (Moderately close) 23.1%
4 - 5 (Very close) 72.1%On average, how close is your relationship with your family?
1 – 2 (Not at all close) 6.6%3 (Moderately close) 18.8%
4 - 5 (Very close) 74.6%To what degree do you feel connected
to your college or university?1 - 2 (Not at all connected) 17.5%3 (Moderately connected) 42.3%
4 - 5 (Very connected) 30.2%
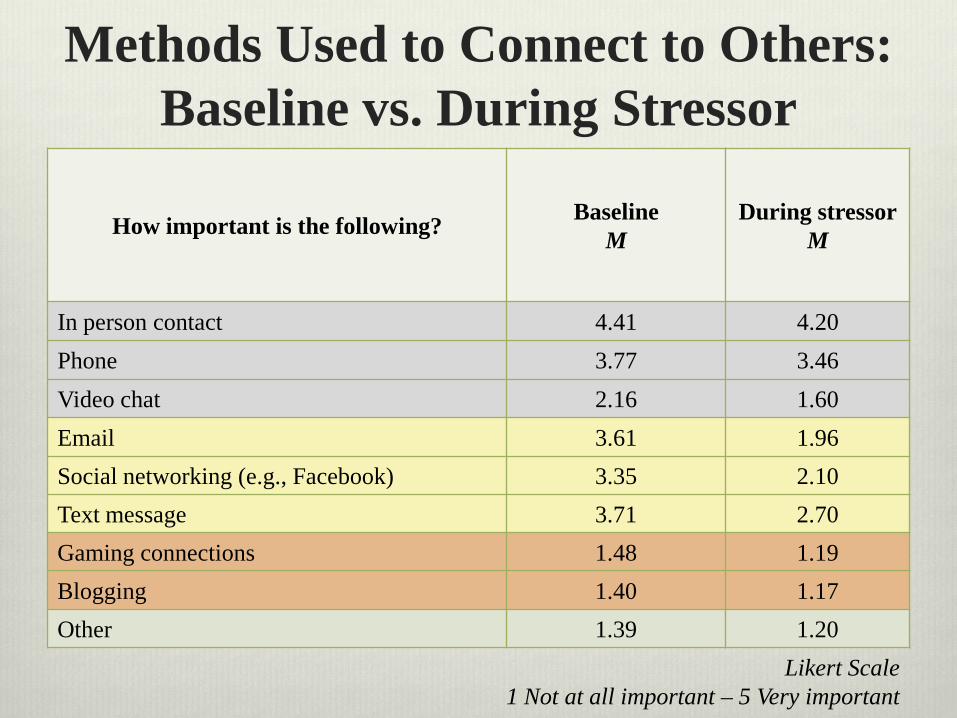
Methods Used to Connect to Others: Baseline vs. During Stressor
How important is the following? BaselineM
During stressorM
In person contact 4.41 4.20Phone 3.77 3.46Video chat 2.16 1.60Email 3.61 1.96Social networking (e.g., Facebook) 3.35 2.10Text message 3.71 2.70Gaming connections 1.48 1.19Blogging 1.40 1.17Other 1.39 1.20
Likert Scale1 Not at all important – 5 Very important

Help Seeking For Suicidal Thoughts(2006 Study)
Asked of those who had seriously considered attempting suicide (n=1321)
54% Told One or More People Romantic Partner: 34%
Peer: 33%
Family: 16%
Professional: 14%
Other (Clergy, Professor, RA): 3%
Discussion How might qualities of self be addressed at the
population/clinical level to affect one’s likelihood of experiencing stress/distress/suicidality?
How can clinicians account for help-seeking patterns to prevent distress/suicidality on campus?
Voice of the student… “I dropped a class when my father died. When I called to get
grief counseling they said I was ineligible because I wasn’t full time. I explained the situation and they refused.”
“If they had offered more than 6 sessions with a counselor.”
Overview of Presentation Sections of presentation
Expansion: Intervention approaches and distress/suicidality continuum
Overview of 2011 data
Demographics
Nature of stressful period
Suicidal ideation and behavior
Qualities of self: Connectedness/belongingness and sense of coherence
Implications for Population-focused prevention
Discussion
2006 Data: Studies completed and in progress Wong, J. & Brownson, C. (in process). A mediation model of professional psychological help
seeking for suicide ideation among Asian American and White American college students.
Brownson, C., Becker, M. S., & Jaggars, S. (in press). Suicidal behavior and help seeking among diverse college students. Journal of College Counseling.
Drum, D. J., & Burton Denmark, A. (2012). Campus suicide prevention: Bridging paradigms and forging partnerships. Harvard Review of Psychiatry, 20, 209-21.
Brownson, C., Drum, D., Smith, S., & Denmark, A. (2011). Differences in suicidal experiences of male and female undergraduate and graduate students. Journal of College Student Psychotherapy, 25, 277-94.
Drum D.J., & Burton Denmark A. (2011). College suicide prevention programs and interventions. In: Lamis DA, Lester D, eds. Understanding and Preventing College Student Suicide.
Wong, Y. J., Brownson, C., & Schwing, A. E. (2011). Risk and protective factors associated with Asian American students’ suicidal ideation: A multi-campus, national study. Journal of College Student Development, 52, 396-408.
Drum, D., Brownson, C., Denmark, A., & Smith, S. (2009). New data on the nature of suicidal crises in college students: Shifting the paradigm. Professional Psychology: Research and Practice, 40, 213-22.
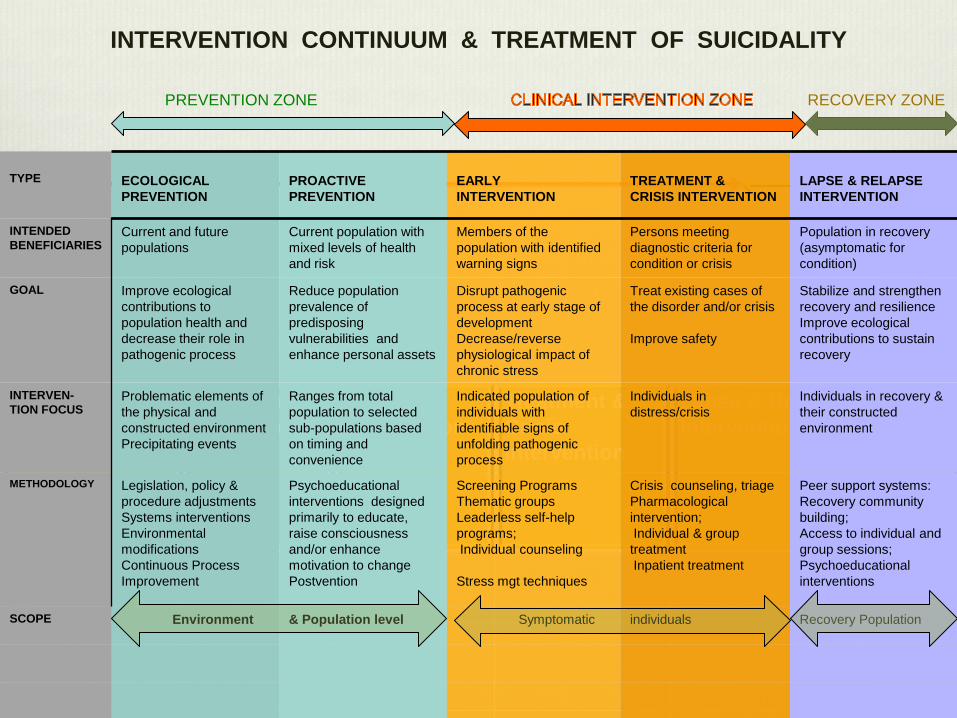
Ecological prevention
Proactive Prevention
Early Intervention
Treatment & CrisisIntervention
Lapse & Relapse Intervention
TYPE ECOLOGICAL PREVENTION
PROACTIVE PREVENTION
EARLYINTERVENTION
TREATMENT &CRISIS INTERVENTION
LAPSE & RELAPSE INTERVENTION
INTENDED BENEFICIARIES
Current and future populations
Current population with mixed levels of health and risk
Members of the population with identified warning signs
Persons meeting diagnostic criteria for condition or crisis
Population in recovery (asymptomatic for condition)
GOAL Improve ecological contributions to population health and decrease their role in pathogenic process
Reduce population prevalence of predisposing vulnerabilities and enhance personal assets
Disrupt pathogenic process at early stage of development Decrease/reverse physiological impact of chronic stress
Treat existing cases of the disorder and/or crisis
Improve safety
Stabilize and strengthen recovery and resilienceImprove ecological contributions to sustain recovery
INTERVEN-TION FOCUS
Problematic elements of the physical and constructed environment Precipitating events
Ranges from total population to selected sub-populations based on timing and convenience
Indicated population of individuals with identifiable signs of unfolding pathogenic process
Individuals in distress/crisis
Individuals in recovery & their constructed environment
METHODOLOGY Legislation, policy & procedure adjustmentsSystems interventionsEnvironmental modificationsContinuous Process Improvement
Psychoeducational interventions designed primarily to educate, raise consciousness and/or enhance motivation to changePostvention
Screening Programs Thematic groups Leaderless self-help programs;Individual counseling
Stress mgt techniques
Crisis counseling, triage Pharmacological intervention;Individual & group treatmentInpatient treatment
Peer support systems: Recovery community building;Access to individual and group sessions;Psychoeducational interventions
SCOPE Environment & Population level Symptomatic individuals Recovery Population
INTERVENTION CONTINUUM & TREATMENT OF SUICIDALITY
PREVENTION ZONE RECOVERY ZONE
What can we do? Effectively target our limited resources
Utilize clinical resources to address needs of those who are highly distressed or at high risk
Expand population-based approaches to fit nature of population
Enhance capacity of existing support networks
Bolster students’ ability to preserve self during stressful times
Develop a climate that reduces barriers to help
Your ideas?
College Student Suicide Prevention Listserve
To participate in an ongoing conversation – Join a listserve about suicide in higher education by
contacting Marian Trattner, Suicide Prevention Coordinator at UT Austin, at [email protected]
Sections of presentation
Expansion: Intervention approaches and distress/suicidality continuum
Overview of 2011 data
Demographics
Nature of stressful period
Suicidal ideation and behavior
Qualities of self: Connectedness/belongingness and sense of coherence
Implications for Population-focused prevention
Discussion
Overview of Presentation
Questions?
Special Thanks To The 26,000 Student Research Participants
The 74 Research Consortium Participating Institutions and Counseling Center Directors
The Research Consortium team
http://cmhc.utexas.edu/researchconsortium.htmlConsortium Director: Chris Brownson, PhD
Email: [email protected]