Embed Size (px)
Citation preview

Jordan Surgical Clinical Congress
Optimal Surgical Education for Better Care
Smoking Free Congress
In Collaboration with
American College of Surgeons Jordan Chapter1st Annual Clinical Congress
5th-8th May, 2016Le Royal Hotel
Amman - Jordan
• The Jordanian Society of Obstetricians & Gynecologists• Jordan Vascular Society• Cardiac Surgery Association• Thoracic Surgery Society• The Jordanian Orthopedic Association• The Jordanian Association of Pediatric Surgeons• Brain & Neurosurgery Society• Jordan ENT, Head & Neck Surgeons• Jordanian Society for Plastic & Reconstructive Surgery• Jordanian Association of Urological Surgeons
Under The Patronage of H.E Minister of Health


His Majesty KingAbdulla Ibn Al-Hussein II


His Royal Highness Crown PrinceHussein Bin Abdullah II


1
American College of SurgeonsJordan Chapter
• WElC
OM
E •
• Dear Colleagues,
On behalf of the Jordan Surgical Societies and the Jordan chapter of the American College of Surgeons (ACS) I’d like to welcome each of you to our Jordan Surgical Clinical Congress and its parallel scientific activities which will be held on5th-8th May, 2016 in Amman Jordan.Our Vision with the Jordan Surgical Clinical Congress is to help the surgical community in Jordan to improve the surgical education and to raise the standards of surgical care.
The theme of our congress (Optimal Surgical Education for Better Care) will reflect our main concern in addition to the scientific efforts in all other surgical fields. We would greatly urge your support and encourage your participation and attendance to our congress.We wish our guests an enjoyable time in beautiful Amman.
Professor Dr. Abdalla Bashir M.D., FRCSEd. ,FACS.President of the CongressGovernor, Jordan ACS Chapter

2
American College of SurgeonsJordan Chapter
Date Activities
3rd- 5th May, 2016 ATLS Course
5th May, 2016 Opening Ceremony
5th May - 7th May, 2016 Scientific program
6th May, 2016The American College of Surgeons Surgical Competition“Surgical Jeopardy”
7th -8th May, 2016 ACS General Surgery Review Course
7th -8th May, 2016Trauma Evaluation &Management Course TEAM for Medical Students
• IMPO
RTAN
T DATES •
3
American College of SurgeonsJordan Chapter
• CO
MM
ITTEES •
• Organizing Committee• Khaled Ajarmeh (Chair) • Abdul Naser Shunaigat• Ahmad Uriqat• Ahmad Bashir• Ala’a Alzu’bi• Amer Amireh• Firas Obeidat• Hazim Al Ajarmeh• Islam Al Awamleh• Mohammad Zitawi• Osama Hamed• Rami Yaghan• Said Al Natour
• Scientific Committee• Zaki Qulaghassi (Chair)• Abdullah Al-Qudah• Amer Shurbaji• Ali Al Ebous• Ehab Massad• Fayez Dawood• Hanan RIhani• Hashem Al Momani• Khaldoun Haddadin• Khaled Ajarmeh• Maha Qubain• Mohammed Abu Ein• Mohannad Alquda• Maher Maaita • Mahmoud Al Masri• Mahmoud Odat• Mahmoud Qatarneh• Mahmoud Wreikat• Ma’moun Al Qaryouti• Mazen El Zibdeh• Nasser Qassed Ahmad• Nayef Freiwan• Osama Hamed• Said Natour• Salah Trabsheh• Samir Smadi• Wael Na’asan• Walid Masoud• Waseem Al Mefleh

4
American College of SurgeonsJordan Chapter
• Social Committee• Mohammad Alshobaki (Chair)• Abeer Eunab• Ahmad Uriqat• Fadi Falah• Maher Maaita• Majdi Soudi• Muhannad Qulaghassi
• Financial & Exhibition Committee• Abdul Naser Shunaigat (Chair)• Ahmad Bashir
• Asharaf Faouri
• Media & Communications Committee• Osama Hamed (Chair)• Mohammad Zitawi
• CO
MM
ITTEES •

5
• ADVISO
Ry PAN
El •
• Dr. Abdelhadi Breizat, MOH• Dr. Abdelkareem Al-Omari, KAUH• Dr. Abdul-Aziz Ziadat, JUH• Dr. Abdul Naser Shunaigat, Private Sector• Dr. Abdalla Bashir, JH• Dr. Abdullah Al Qudah, Private Sector• Dr. Abdullatif Okla, Private Sector• Dr. Adel Al-Shuraideh, Private Sector• Dr. Adnan Abu-Qamer, KHMC• Dr. Ahmad Al Raymoony, KHMC• Dr. Amer Amireh, KHMC• Dr. Amer Shurbaji, KHMC• Dr. Ali Al-Sarayrah, Hashemite University• Dr. Ali Al Ebous, KHCC• Dr. Basem Hamdan, KHCC• Dr. Basheer Al-Jarrah, Private Sector• Dr. Basheer Bani Mustafa, Private Sector• Dr. Daoud Hanania, Private Sector• Dr. Emad Habaybeh, Private Sector• Dr. Eyad Gargaz, Hashemite University• Dr. Fahmi Al-Mohammad, Private Sector• Dr. Faisal Mousa, Private Sector• Dr. Fayez Hmood, MOH• Dr. Ghaith Shubilat, Private Sector• Dr. Hashem Al Momani , JUH• Dr. Hayel Ejeilat , Privte Sector• Dr. Hisham Bani Hamad, Private Sector• Dr. Issa Sawaqed, KHMC• Dr. Jamal Haddad, Private Sector• Dr. Jamal Massad, JUH• Dr. Jihad Al Masri, Private Sector• Dr. Kamal Bani-Hani, Hashemite University• Dr. Khalaf Al-Jader, Private Sector• Dr. Khaldoun Haddadin, RMS• Dr. Maher Maaita, KHMC • Dr. Mahmoud Al Qatarneh, Privte Sector • Dr. Mahmood Abukhalaf, Private Sector
• Dr. Mahmoud Wreikat, Private Sector• Dr. Mazen El Zibdeh, Private Sector• Dr. Moath Al-Smadi, JUH• Dr. Mohammad Abu Ein, Private Sector• Dr. Mohammad Abusamen, KHMC• Dr. Mohammad Dweiri, KHMC• Dr. Mohammad Fteha, Private sector• Dr. Mustafa Steitieh, Private Sector• Dr. Nabeel Batarseh, Private Sector• Dr. Nabeel Hamati, Private Sector• Dr. Nader Al-Bsool, JUH• Dr. Naif Fraiwan , Privte Sector• Dr. Najeh Al-Omari, KHMC• Dr. Naser Al-Hammori, H.U• Dr. Nemr Al Khtum, KHMC• Dr. Nidal younis, H.U• Dr. Omar Al Zoubi, KHMC• Dr. Rami yaghan, KAUH• Dr. Saeed Al-Natour, Private Sector• Dr. Saeed Fayoumi , Privte Sector• Dr. Saeed Jarbou, Private Sector• Dr. Saad Jaber, KHMC• Dr. Salam Daradkeh, Private Sector• Dr. Salah Halaseh, Private Sector• Dr. Sameer Al-Smadi, KHMC• Dr. Tahseen Mohajer, Private Sector• Dr. Tariq Al-Jaberi, JUST• Dr. Wa’el AlNa’ssan, KHMC• Dr. Wael Fatayer, Private Sector• Dr. Walid Masoud , Privte Sector• Dr. yousef Uraiqat, Private Sector• Dr. yousef Zreiqat, KHMC• Dr. Zaki Qulaghassi, Private Sector• Dr. Zahran Bdeir, Private Sector

6
American College of SurgeonsJordan Chapter
• GUEST SPEA
KERS •
Dr. Abdallah FayyadDr. Ali HallalDr. Alper TokerDr. Ayman Agha Dr. Bishara AtiyehDr. Courtney TownsendDr. Eman SbeityDr. Essam Al Halaby Dr. Gabriel Planas RibóDr. George Abi SaadDr. Goro HondaDr. Haitham Al Salahat Dr. Hamad BahiliDr. Hisham El-Minawi Dr. Hossam FodaDr. Jamal J. HoballahDr. Munier NazzalDr. Saud al turki Dr. yahia BalbaaDr. yaser Jamaal
UKLebanonTurkeyGermany LebanonUSALebanonEgyptSpainLebanonJapanUAEKSAEgyptEgyptLebanonUSAKSAEgyptKSA

7
American College of SurgeonsJordan Chapter
• lOC
Al SPEA
KERS •
Dr. Abdelhadi Braizat Dr. Adnan Abo Gamar Dr. Ahmad Al-RaymoonyDr. Ahmad Bashir Dr. Ahmad Uraiqat Dr. Ahmad Zarour Dr. Akram Al-IbraheemDr. Ali Abu Seini Dr. Ali Dabous Dr. Amjad Bani HaniDr. Ashraf Faouri Dr. Aiman Obaid Dr. Castro SiffariniDr. Emad HijaziDr. Enas younis Dr. Firas Hammouri Dr. Firas Ibrahim Dr. Ghada NimriDr. Ghassan KhayyatDr. Haitham AltaaniDr. Hani Hadidi Dr. Hashem Momani Dr. Hashim Qudah Dr. Hazem Ajarma Dr. Hiba Abbadi Dr. Ibrahim Daradka Dr. Isam latayfeh Dr. Jamal Al-Aidi Dr. Kamil Fram Dr. Khaldoun Gharaibeh Dr. Khaldoun Haddadin
Dr. Khalid Ajarmeh Dr. Khalid Safi Dr. Khalil Ghandour Dr. lamees ArabiyatDr. lara Abu Ghazaleh Dr. layal AsirDr. Mahmoud Al-Masri Dr. Mahmoud Odat Dr. Mais Alkarmi Dr. Mamoun Al-QaryoutiDr. Maymona AttiyatDr. Mazen El-Zibdeh Dr. Mohammad Abu Ein Dr. Mohammad Al Qudah Dr. Mohannad Al-Qudah Dr. Nagham Alkaragholli Dr. Najeh Alomari Dr. Osama HamedDr. Rami Azab Dr. Sameer Smadi Dr. Samer Geizawi Dr. Sanaa HammouryDr. Salah TarabshehDr. Shadi Hamouri Dr. Suzan BakhietDr. Wa’el AlNa’ssan Dr. Wasim Al-Mefleh Dr. yanal AlnaserDr. Zaid Qarem Dr. Zeid Abu Ghosh

8
American College of SurgeonsJordan Chapter
• GUEST SPEA
KERS BIO •
Prof. Courtney M. Townsend, USAPresident-Elect of the American College of Surgeons (ACS) Courtney M. Townsend, Jr., MD, FACSRobertson-Poth Distinguished Chair in General Surgery, department of surgery, University of Texas Medical Branch (UTMB), GalvestonPresident-Elect of the American College of Surgeons (ACS).Dr. Townsend is a highly esteemed surgical educator, and fellow of ACS since 1981. He has held many leadership roles in the organization, including Secretary (2006-2013), Chair of the ACS Board of Governors (2004-2005), and a member of the Board’s Executive Committee (1999-2003). Dr. Townsend is professor of surgery and professor of physician’s assistant studies at the University of Texas Graduate School of Biomedical Sciences, UTMB. He earned his medical degree and completed his internship and general surgery training at UTMB. He completed a surgical oncology fellowship at the University of California-Los Angeles (UCLA).Dr. Townsend has been editor-in-chief of the Sabiston Textbook for Surgery: The Biological Basis of Modern Surgical Practice since 2000 and was the editor of Surgical Oncology (1992-1999). He has served on the editorial board of the Journal of the American College of Surgeons (JACS), Surgery, and The American Journal of Surgery. He has authored or co-authored 416 articles in peer-reviewed publications, 123 articles in other publications, and 364 scientific research abstracts.Dr. Townsend has also served in leadership roles in several other medical organizations. He is past-director and chairman of the American Board of Surgery (2000-2006); served on the Accreditation Council for Graduate Medical Education Residency Review Committee for Surgery (1994-1999); American Surgical Association president (2007-2008) He is an honorary member of the Society of Black Academic Surgeons and the Association of Women Surgeons (AWS) and is a recipient of the John P. McGovern Lifetime Achievement Award in Oslerian Medicine.
9
American College of SurgeonsJordan Chapter
• GUEST SPEA
KERS BIO •
Dr. Jamal Hoballah, lebanonchair of the International Governors workgroup of the American College of Surgeons.Dr. Jamal Hoballah received his MD from the American University of Beirut in 1981. He joined New York University (NYU) in 1982 where he completed his general surgery residency in 1987 and a trauma/critical care fellowship in 1988. He remained on the faculty at NYU for two years before moving to the University of Iowa where he completed his vascular fellowship in 1991. Dr. Hoballah then joined the Department of Surgery at the University of Iowa where he became a tenured professor of surgery, director of the Vascular Surgery Fellowship program, and chairman of the Vascular Surgery Division in 2002. In 2007, Dr. Hoballah was appointed the surgical director of the University of Iowa Heart and Vascular Center. In 2008, Dr. Hoballah returned to AUBMC where he serves as the Chairman of the Department of Surgery, as well as the Head of the Division of Vascular Surgery since 2011.Dr. Hoballah is Board certified in general surgery, vascular surgery, and surgical critical care. He has obtained an executive MBA from the Tippie School of Business at the University of Iowa in 2001 and completed a program on Leadership Development for Physicians in Academic Health Centers at Harvard School of Public Health in 2004.Dr. Hoballah’s areas of clinical and research interest include endovascular surgery, infrainguinal revascularization, acute limb ischemia, and surgical education. He has authored and co-authored over 90 papers in peer reviewed journals and over 40 book chapters. In addition, he has been the sole author of a vascular surgery book and co-editor of seven other surgical books. He also serves as a reviewer for several surgical journals.Dr. Hoballah is a member of numerous prestigious surgical societies and has served as president of the Johnson County Medical Society and president of the Iowa Vascular Society. He served as an examiner for the American Board of Surgery and the American Board of Vascular Surgery. He has received several awards including the Attending of the Year award at NYU in 1989 and the Teacher of the Year award at the University of Iowa in 1996. He has been selected to the Best Doctors in American list for several years. Dr. Hoballah is the past chair of the International

10
American College of SurgeonsJordan Chapter
• GUEST SPEA
KERS BIO •
Relations Committee of the American College of Surgeons. He is the Governor of the ACS Lebanon Chapter, and the chair of the International Governors workgroup of the American College of Surgeons.
Abdallah M Fayyad, UKI started my training as an SHO in the North East of England. I joined Queen Mary University of London (Barts and the London) as a clinical lecturer in Obstetrics and Gynaecology, and completed my MD thesis in 2006.I am RCOG accredited subspecialist in Urogynaecology. I have received my subspecialty training at St Mary’s Hospital, Manchester, a regional and national referral centre for tertiary and laparoscopic Urogynaecology. I completed training in advanced laparoscopic Urogynaecology and complex pelvic floor surgery by a leading Urogynaecologist and minimal access surgeon (CCT obtained September 2009). I am currently a Consultant Gynaecologist and Subspecialist in Urogynaecology and Pelvic Reconstructive Surgery at Luton and Dunstable University Hospital NHS Foundation Trust. My particular research interests are laparoscopic urogynaecology, uterine preserving prolapse surgery, new surgical techniques for managing pelvic organ prolapse and urinary incontinence, laparoscopic hysterectomy and the management of lower urinary tract symptoms in women with medical conditions. I have published widely in Obstetrics and Gynaecology and in Urogynaecology. I sit on the International Urogynecology Association (IUGA) Education Committee. I sat on the British Society of Urogynaecology Meeting Committee and RCOG assessor for subspecialty training in Urogynaecology. I have developed guidelines for service provision in Urogynaecology that has been adopted nationally. I am a member of the International Urogynecology Association (IUGA) Education Committee and the Exchange program sub committee. I am a member of the British Society of Gynaecologic Endoscopy (BSGE) and the International Continence Society (ICS). I am also a member of the Society of Gynecological Surgeons (SGS), the leading American Society for vaginal and reconstructive surgeons (invitation only membership).

11
American College of SurgeonsJordan Chapter
• GUEST SPEA
KERS BIO •
Dr. Ali Hallal, lebanon is currently a an assistant professor of clinical surgery at the American University of Beirut Medical Center (AUBMC) where he works as Trauma , Upper GI surgeon and Intensivist. He is the program director for the trauma and surgical intensive care fellowship at the AUBMC. He had his Trauma and Critical Care fellowship training at Jackson Memorial Hospital Miami USA, and Upper GI training at ST Thomas’ Hospital London. He works as a consultant surgeon at King’s College Hospital London where he developed the acute care service before joining the AUBMC in 2011. His main research interest is in trauma system, sepsis and esophageal cancer.
Dr. Alper Toker, TurkeyAlper Toker received MD degree after completion of Marmara University, School of Medicine (1992 ).He started the residency program at Istanbul University, Istanbul Medical Faculty, Department of Thoracic and Cardiovascular Surgery (1992),He worked 2 more years in the same department after completion of residency program (1997) until 1999. He did his military service at the Military Academy at Thoracic Surgery Dept, GATA (1999-2000)He engaged in organization Department of General Thoracic Surgery at Istanbul University, Istanbul Medical Faculty, (2001-on ward ). He is the Professor of Thoracic Surgery and Director from 2009 on.He observed in Germany, Austria and United States during his thoracic surgery education.He is a council member of ESTS from 2009 on and the president of the ESTS on 2015, now, the past president.His academic interests include lung cancer extended surgery, Videothoracoscopic surgery (lung cancer and myasthenia gravis), mediastinal surgery and robotic lung cancer operations.

12
American College of SurgeonsJordan Chapter
• GUEST SPEA
KERS BIO •
Dr. Ayman Agha, GermanyProf. Dr. med. Ayman AghaHead of Surgery1993 – 2013 University Hospital of RegensburgFranz-Josef-Strauß-Allee 93053 RegensburgSubspeciality: Minimal invasive colorectal surgerySince 03/2014 Chief of Department of SurgeryKlinikum Munich-BogenhausenEnglschalkinger Str. 7781925 MunichSurgical expertise:Minimal invasive surgery in following fields:- Laparoscopic esophagectomy- Laparoscopic hepatobiliary surgery- Laparoscopic colorectal surgery- Laparoscopic endocrine surgery
Dr. Bishara Atiyeh, lebanonis a prof of Plastic and reconstructive surgery at the American university of Beirut , he has been guest speaker in numerous meeting and is the author of more than 200 scientific papers and two books on body contouring and breast cancer surgery and the principle of oncoplastic surgery.

13
American College of SurgeonsJordan Chapter
• GUEST SPEA
KERS BIO •
Dr. Eman Sbaity, lebanonReceived medical degree from “Beirut Arab University” in 2005Surgery Residency at AUBMC 2005-2010.Followed by Breast Surgical Oncology training at Johns Hopkins,USA for 1 year 2010-2011Then 1 year of clinical research at Hopkins Sidney-Kimmel breast cancer center 2011-2012Surgical Oncology fellowship at MSKCC for 1 year 2012-2013, during which training was focused on colorectal cancer , gastric cancer, and retroperitoneal and soft tissue sarcomas.“Fellow of the European Board of General Surgery”: Certified by the European board of general surgery in June 2014.Joined the department of surgery at AUBMC in june 2014.Currently pursuing a masters in SHARP (Scholars in Health Research Program) at AUB.Member of many committees at AUBMC:- Cancer Prevention taskforce- Research Funding Committee- Scientific Committee- Medical Record CommitteeCo-leader of the “Private Clinics Committee”ACGMEI core faculty member and member of the Clinical Competency Evaluation committee.Clinical interest in: breast cancer with special interest in the new “Nipple Sparing Mastectomy”, retroperitoneal and soft tissue sarcomas sarcoma , and gastric cancers. Special research interest in translational research and outcome research.Member of national and international surgical oncology societies.

14
American College of SurgeonsJordan Chapter
Dr. Essam Al Halaby, EgyptProfessor of Pediatric Surgery, Faculty of Medicine, Tanta University, Egypt,International Certified trainer/HRD ConsultantPresident of Pan African Pediatric Surgical Association (PAPSA)Vice President of the Egyptian Society of Pediatric Surgery (EPSA)Editor in-Chief Annals of Pediatric SurgeryBiography:Essam A. Elhalaby is the chief of pediatric surgery in Faculty of Medicine, Tanta University, He was graduated from Tnata University at 1981. He completed his general surgery residency program at 1986. He got his postgraduate Master and MD degrees in surgery from Tanta University at 1986 and 1996. He spent two years (1991-1993) as a research fellow at division of pediatric surgery, university of Michigan, Ann Arbor USA.He is an international board certified trainer and human resources and development consultant since 2008. Dr. Elhalaby was appointed as a lecturer, then associate professor, then professor in pediatric surgery in faculty of medicine taint university.in addition to his very busy academic and clinical commitments, he has established the quality assurance unit at the medical school on 2004, and he was the director of that unit until 2014.Prof. Elhalaby has many national, regional and international contributions.He has been an invited guest lecturer or scientific presenter at 187 major national & international conferences. he conducted workshops ignominy arab, european and african countries.he is the editor in chief of annals of pediatric surgery, and has been serving as an editorial board member in order journals. he has published more than 85 papers in reputed journals.Prof Elhalaby has a great interest in africa, he is currently the president of Pan African pediatric surgical association (PAPSA), in addition of serving as the senior board member of egyptian fellowship in pediatric surgery, and egyptian pediatric surgical association (EPSA)
• GUEST SPEA
KERS BIO •

15
American College of SurgeonsJordan Chapter
Dr. Gabriel Planas Ribó, SpainEDUCATIONMember number of Colegio Oficial de Médicos: 32901Place and date of birth: Barcelona, November 27, 1964Bachelor of Medicine and Surgery. University of Córdoba. Spain. February 1998 Specialty in Plastic Surgery. University Tor Vergata. Rome, Italy. 2004 PhD Cum Laude 50/50 e Lode with the title “L´Effetto Piezoeléttrico e il rimodellamento Craniofacciale: Uno Studio Sperimentale” Ph.D in Medicine and Surgery by the Universidad Autónoma de Barcelona “ Cum Laude” 2011PUBLICATIONS- Virtual Changes of the Shape of the Lips Aesthetic Plastic Surgery 23:32-35, 1999. - The Retraction of the Oral Opening in Burned PatientsPlast. Recons. Surg.1999 Mar, 103(3):1082-6. - Prótesis Glúteas. Cir. Plast. Iberolatinamer. Vol. 27 n 3, 2001.- Supervivencia a largo plazo de los injertos grasos. Cirugía Plastica Iberolatinoamericana- March 2006.- Chapter: Cirugia Plástica de La parálisis: Paralisis Facial Periferica complicaciones y secuelas (2010-11-18)- Open Case en la Revista European Aesthetic Plastic Surgery Journal, Num 2, July 2014
• GUEST SPEA
KERS BIO •

16
American College of SurgeonsJordan Chapter
Dr. George S. Abi Saad, lebanonProfessor of Clinical Surgery Head, Trauma Services and Surgical Critical CareChairman, ATLS MENA Chairman, ATLS Lebanon Director, PHTLS LebanonDirector, ATCN LebanonDirector, Continuing Medical Education officeAttending in the Department of Emergency medicine American University of Beirut Medical centerEx-president of the Lebanese Society of Critical Care Medicine - LSCCM EX-Middle East Representative in the Council of European Society of Intensive Care Medicine (ESICM) Vice president of Pan Arab Society of Critical Care Medicine (IPACCMS)Have many publications in the field of Trauma, surgical critical care and general surgery Member of many hospital committees including Hospital Mortality and Morbidity, Nutrition Committee, Blood and Blood products Committee and Critical care Committee
Dr. Goro Honda, JapanGoro Honda, MD, PhD, FACSChief SurgeonDepartment of Hepato-Biliary-Pancreatic SurgeryTokyo Metropolitan Cancer and Infectious Diseases Center, Komagome Hospital1992 MD, Kumamoto University School of Medicine, Kumamoto, Japan2009 Ph.D., Kyoto University Graduate School of Medicine, Kyoto, JapanBoard Certified Surgeon of Japan Surgical Society, the Japan Society of Gastroenterological Surgery, Japan Society for Endoscopic Surgery, Japanese Society of HBP Surgery, and Japanese Biliary Association
• GUEST SPEA
KERS BIO •
17
American College of SurgeonsJordan Chapter
Dr. Haytham El Salhat, UAEHaytham. N. El-Salhat, MD, MBA, FACS, FRCS (Glasgow) is a consultant surgeon. He currently serves as Chair of Surgical Oncology and Chief of all Surgical Departments in Alnoor Airport Road as well as Medical Director of the Oncology Service Line in Al Noor Hospital Group. In addition to his interest in soft tissue Sarcoma, GI, Pancreatic surgery, he is also skilled in breast Onco-plastic surgery.
Dr. Hamad Mohammad Hamad, KSAAl- Bahili is a multi- organ transplant surgeon with an expertise in living donor liver and kidney transplant for pediatric and adult. He is the Director of a newly established multi-organ transplant at Prince Sultan Military Medical City, Riyadh KSA, he worked at King Faisal Specialist Hospital & Research Center, Riyadh KSA as Section head and consultant for liver & small bowel transplant and Hepatobiliary and Pancreatic surgery.Dr. Bahili completed his residency training program at King Faisal Specialist Hospital & Research Center, Riyadh KSA. In 2010 he successfully obtained is fellowship for Multi – Organ Transplantation & Hepatobiliary Surgery in Toronto, Canada. He is an actively member in Pan Arab Liver Transplant Society (PALTS), Middle East, North Africa (MENAI) chapter of Hepatobiliary Surgery of EHPBA, International liver transplant society (ILTS) and American Transplant society.
Dr. Hisham El-Minawi, EgyptDr Hisham El Minawi Professor of Plastic SurgeryKasr el Aini School of MedicineCairo UniversityDirector of Zamalek Medical Center
• GUEST SPEA
KERS BIO •

18
American College of SurgeonsJordan Chapter
Dr. Hossam M.T. Foda, EgyptProfessor & Head of Facial Plastic Surgery Otolaryngology Dept. Alexandria Medical School, Egypt Dr. Hossam Foda completed his Otolaryngology residency at Alexandria University in Egypt then moved to the United States to join the University of Texas (UTHSC) in Houston where he completed a two-year clinical fellowship in facial plastic and reconstructive surgery. At completion of his fellowship Dr. Foda published a Doctorate-degree thesis on Rhinoplasty techniques and was awarded his Doctorate degree in 1994. Dr. Foda then returned to Alexandria University where he founded a division of facial plastic surgery in the Otolaryngology department. As a Professor and Director of that division, Dr. Foda started training the Otolaryngology residents on all facial plastic procedures, he also supervised Masters and Doctorate degree theses on a variety of topics in the field of facial plastic surgery. Dr. Foda’s practice have been focused exclusively on rhinoplasty for the last 20 years during which he made valuable contributions to the literature of Rhinoplasty by publishing numerous scientific articles and book chapters mostly on nasal tip modifying techniques, management of nasal deviations, and correction of cosmetic and functional problems resulting from failed previous rhinoplasties. In 2012, Dr. Foda was selected to serve on the board of directors of the Rhinoplasty Society of Europe. Dr. Foda has been invited to lecture at most of the leading Rhinoplasty courses around the globe and has been invited to give Rhinoplasty live surgical demonstrations in Hamburg, Dubai, Munich, Bergamo, Madrid, London, Tehran, Stuttgart, Odessa, Riyadh, Palma de Mallorca, Karlsruhe, Kuwait, Asturias.
• GUEST SPEA
KERS BIO •

19
American College of SurgeonsJordan Chapter
Munier Nazzal, USAA graduate of the University of Kuwait medical school. Obtained his a training and Kuwait and not getting them and the United States. His is a fellow of the Royal College of surgeons and Glasgow, ddle of the and medical College of surgery. As well as I ddle all the American College of clinical wound specialist. Board certi ed in general, vascular and the wound surgery. Obtained his vascular training from the University of Iowa in the United States. Dr. Nazzal is a member of many national and international organizations. Loading and American College of surgery, American venous forum, member of the peripheral vascular Society, member of the Society VASCULAR surgery council member of the American College of surgery of Ohio chapter. A member of the and American program director Society. Has multiple publications including more than 60 articles in per review journals, more than 200 abstracts, more than 200 national and international presentations. Member all day dictatorial board of vascular surgery, ad hoc reviewer for a number of journals including vascular surgery, Journal of vascular surgery, annals of vascular surgery, and others Dr. Nazzal is the chief of vascular and endovascular surgery at the University of Toledo Medical Center, Gen. surgery program director, associated chair of surgery, medical Director of the vascular laboratory, and establishing and director the wound and hyperbaric Center at the University of Toledo, Medical Director of the Waseon Wound/Hyperbaric Center.
• GUEST SPEA
KERS BIO •

20
American College of SurgeonsJordan Chapter
Dr. Saudi Al-Turki, KSASaud Al Turki, MD, ODTS, FACS Consultant, Vascular Surgery Department of Surgery – King Abdulaziz Medical City Director, Trauma Courses Office, Deanship of Postgraduate Education King Saud Bin Abdulaziz University for Health Sciences Regional Director, ATOM Course, Saudi Arabian Chapter ATCN & PHTLS Courses, Medical Director, Saudi Arabian Chapter Director, Trauma Research Section King Abdullah International Medical Research Center Chief, American College of Surgeons Committee On Trauma - Region XVII Clinical Appointment: Consultant of Vascular Surgery, Department of Surgery at King Abdulaziz Medical City. Obtained his MBBS in 1985, became a fellow of the American College of Surgeons in 1990, an Assistant Professor of Vascular Surgery at King Saud bin Abdulaziz University for Health Sciences. Completed all his training from the residency to senior level at Ysbyty, United Kingdom and became a prominent consultant in the field of Vascular Surgery since 1994 at King Abdulaziz Medical City. Administrative & Academic Appointments: He is the 1st ever appointed Chief for the Region XVII (MENA) by the American College of Surgeons, Committee On Trauma. In his role as Chief, he is in-charged for monitoring and overseeing all MENA region trauma activities and would be responsible for the countries promulgation of such courses endorse by the American College of Surgeons (i.e. ATLS, ATCN, PHTLS, ATOM, DMEP) As the Director, Trauma Courses Office, Deanship of Postgraduate Education at King Saud bin Abdulaziz University for Health Sciences Chairman, Trauma Programs, he is in charge of Saudi Arabian Chapter trauma activities propagations (ATLS, ATOM, ATCN, PHTLS), which are now offered in more than 30 centers within the Kingdom of Saudi Arabia and in partnership with the Gulf States (Bahrain and Kuwait). As Director, Trauma Research Section, King Abdullah International Medical Research Center. He has served
• GUEST SPEA
KERS BIO •

21
American College of SurgeonsJordan Chapter
in the capacity of Executive Director of Academic Affairs at the King Abdulaziz Medical City for several years. During his tenure as Executive Director, he had been actively involved in chairing several committees in the institution. Because of his vast and tremendous experience, he had been invited as lecturer and speaker in many different Symposia, Conferences, Workshops and Courses. He had been authored and co-authored in many different publications, abstracts and presentations. His remarkable contributions made him distinguished and notorious that resulted for his recognition and receiving several plaques and awards of appreciations for his tremendous work.
Dr. yahia Balbaa, EgyptDr. Balbaa is an Egyptian cardiothoracic surgeon, who was trained in general surgery as well as cardiothoracic surgery in Cairo. He had further training in Milano-Italy. His main interest is total arterial revascularization as well as minimally invasive approaches in mitral valve repairDr. Yahia is now a professor of cardiothoracic surgery in the university of Cairo and working as the head of cardiothoracic surgery division in Dar El Fouad hospital, Cairo
Dr. yaser Jamaal, KSAProfessor of Pediatrics and Plastic SurgeryKing Abdulaziz University Hospital
• GUEST SPEA
KERS BIO •



PROXIMATE® Linear CuttersConsistent staple formation for more confidence
Product Overview
• PROXIMATE® Linear Cutters designed for consistent staple formation and hemostasis
• Longest available cut line with 100mm device to transect more tissue in one firing
• One-hand placement frees the surgeon’s other hand to manage tissue
Applicable Specialities
• Bariatric
• Colorectal
• Thoracic
Features Benefits
Safety lockout feature Prevents firing of used reload
Unique CAM mechanism Helps ensure consistent staple formation
Intermediate locking position Tissue can be manipulated without separating the instrument
One-handed placement Frees the surgeon’s other hand to manage tissue
Tissue retaining button Helps secure tisssue in the proper position
Four di� erent reloads available Accommodates a variety of tissue thicknesses

25
American College of SurgeonsJordan Chapter
• OPEN
ING
CEREM
ON
Ey •
09:00- 09:02 Royal Anthem
09:03-09:08 Recitation from the Holy Quran
09:10-09:15 President of the Conference Speech Dr. Abdullah Al-Bashir (Jordan)
09:15-09:20 American College of Surgeons (ACS) President ELECT Prof. Courtney Townsend (USA)
09:20-09:25 President of the Jordan Medical Association Speech
09:25-09:30 H. E Minister of Health
09:30-10:00 Opening Conference Exhibition
10:00-10:30 Coffee Break
Thursday May 5th 08:00-09:00: Registration09:00-10:00: Opening Ceremony

26
American College of SurgeonsJordan Chapter
• SCIEN
TIFIC PRO
GRA
M SUM
MERy •
TIME ROOM1 ROOM2 ROOM3
THURSDAy MAy 5TH8:00-9:00 Registration
9:00-10:00 Opening Ceremony10:00-10:30 Break10:30-12:30 Surgical Education Session12:30-1:30 Lunch
1:30-3:30 Surgical Oncology Session
Thoracic Surgery Session
Orthopedic; Management
of Bone Defects Session
3:30-4:00 Break
4:00-6:00 Trauma Surgery Session
Urology Surgery Session
Pediatric Surgery Session
FRIDAy MAy 6TH8:00-10:00 Surgical Jeopardy10:00-10:30 Break
10:30-12:30 Women In Surgery Cardiac Surgery Session
ENT Surgery Session
12:30-2:00 Lunch and Prayer
2:00-4:00
Transplant: Cadaveric Liver Transplantation
Session
Vascular Surgery Session
4:00-4:30 Break
4:30-6:30Minimal Invasive
Surgery/HPB Session
Obstetricians & Gynecology Surgery Session
Plastic Surgery Session
8:00 Gala Dinner

27
American College of SurgeonsJordan Chapter
• SCIEN
TIFIC PRO
GRA
M SUM
MERy •
TIME ROOM1 ROOM2
SATURDAy MAy 7TH
8:00-10:00 ACS General Surgery Review Course: Abdominal TEAM
10:00-10:30 Break
10:30-12-30 ACS General Surgery Review Course: Alimentary TEAM
12:30-1:30 Lunch
1:30-3:00 ACS General Surgery Review Course: Breast TEAM
3:30-4:00 Break
4:00-4:45 ACS General Surgery Review Course: Endocrine
5:00-6:00 ACS General Surgery Review Course: Vascular
SUNDAy MAy 8TH
8:00-10:00 ACS General Surgery Review Course: Trauma TEAM
10:00-10:30 Break
10:30-12-40ACS General Surgery
Review Course: Critical Care
TEAM
12:40-2:00 Lunch
2:00-3:30ACS General Surgery
Review Course: Perioperative Care 1
TEAM
3:30-4:00 Break
4:00-5:30ACS General Surgery
Review Course: Perioperative Care 2
XXXXXXXX
5:30-6:30 Certificates and Feedback
28
American College of SurgeonsJordan Chapter
• SCIENTIFIC PROGRAM •

29
American College of SurgeonsJordan Chapter
• THURSDAy M
Ay 5TH •
THURSDAy MAy 5TH-All ROOMSSurgical Education Session (10:30-12:30)Moderator: Dr. Mahmoud Abu KhalafPanelists: Dr. Courtney Townsend, Dr. Jamal Hoballah, Dr. Abdullah AL-Bashir
TIME All ROOMS
10:30-10:50 Establishing Surgical Residency Curriculums: Where to Start and How to Do?, Dr. Courtney Townsend (USA)
10:50-11:10 Transforming US Surgical Education System into the Middle East: the AUB Experience, Dr. Jamal Hoballah (Lebanon)
11:10-11:20 Can we Improve Things in Jordan?, Dr. Nidal Younes (Jordan)
11:20-11:30 Results of Jordan Surgery Residents Survey
11:30-11:40 Proposal for Improving Surgical Education at RMS,Dr. Khaldoun Haddadin (Jordan)
11:40-12:00 Assessment of Surgery Residents: Where, When and How?, Dr. Courtney Townsend (USA)
12:00-12:30 Discussion12:30-1:30 Lunch

30
American College of SurgeonsJordan Chapter
THURSDAy MAy 5TH-ROOM 1Surgical Oncology Session (1:30-3:30)Moderators: Dr. Jamal Masaad, Dr. Rami Yaghan, Dr.Fayez Daoud
TIME lECTURES ON ROOM 11:30-1:45 Nipple Sparing Mastectomy, Dr. Eman Sbeity (Lebanon)
1:45-2:00 Contralateral Prophylactic Mastectomy , Is there a Surgical Benefit? Dr. Ali Abu Seini (Jordan)
2:00-2:15 Breast Cancer Surgery Research in the Arab World and the Region., Dr. Mahmoud Al-Masri (Jordan)
2:15- 2:30 Role of PET-CT in Breast Cancer Management, Dr. AkramAl-Ibraheem (Jordan)
2:30-2:45 Laparoscopic Rectal Cancer Surgery, is the Pendulum swinging back?, Dr. Ayman Agha (Germany)
2:45-3:00“Watch and Waite” Strategy in Rectal Cancer with Clinical Complete Response After Neoadjuvant Chemotherapy, Dr. Haytham El Salhat (UAE)
3:00-3:15 Update in Differentiated Thyroid Cancer Management, Dr. Enas Younis (Jordan)
3:15-3:30 Discussion3:30-4:00 Break
• THURSDAy M
Ay 5TH - RO
OM
1 •

31
American College of SurgeonsJordan Chapter
THURSDAy MAy 5TH-ROOM 2Thoracic Surgery Session (1:30-3:30)Moderators: Dr. Saeed Al Fayoomi, Dr. Nayef Fraywan
TIME lECTURES ON ROOM 21:30-1:50 Extended Resection for Lung Cancer, Dr. Alper Toker (Turkey)
1:50-2:05 Forthcoming (Eighth Edition) of the TNM Staging for Non-Small Cell Lung Cancer, Dr. Shadi Hamouri (Jordan)
2:05- 2:25 Robotic Surgery for Lung Cancer, Dr. Alper Toker (Turkey)
2:25-2:40 VATS Thymectomy Right or Left Approach Experience at KHMC, Dr. Hani Hadidi (Jordan)
2:40-3:00 Tracheal Resection for Malignant and Benign Conditions, Dr. Alper Toker (Turkey)
3:00-3:15 Esophageal Perforation Review of High Volume Center Experience, Dr. Jamal Al-Aidi (Jordan)
3:15-3:30 Discussion3:30-4:00 Break
• THURSDAy M
Ay 5TH - RO
OM
2 •

32
American College of SurgeonsJordan Chapter
THURSDAy MAy 5TH-ROOM 3Orthopedic; Management of Bone Defects Session (1:30-3:30)Moderators: Dr. Mahmoud Odat, Dr. Jamal Qunash
TIME lECTURES ON ROOM 3
1:30-1:45 Bone Graft and Bone Substitutes, Dr. Mahmoud Odat (Jordan)
1:45-2:00 Managements of Bone Defect, Dr. Ghassan Khayyat (Jordan)
2:00-2:15 Bone Transport Using Ring Fixator, Dr. Mohammad Abu Ein (Jordan)
2:15- 2:30 Bone Defects Treated by Ilizarov, Dr. Castro Siffarini (Jordan)
2:30-2:45 Bone Defect Treated by Allograft, Dr. Hashim Qudah (Jordan)
2:45-3:00 Bone Defect Treated By Induced Membrane Technique, Dr. Firas Ibrahim (Jordan)
3:00-3:15 Managements of Bone Defect in Chronic Shoulder Dislocation, Dr. Zaid Qarem (Jordan)
3:15-3:30 Discussion3:30-4:00 Break
• THURSDAy M
Ay 5TH - RO
OM
3 •

33
American College of SurgeonsJordan Chapter
THURSDAy MAy 5TH-ROOM 1Trauma Surgery Session (4:00-6:00) Moderators: Dr. Ahmad Zarour, Dr. Mahmoud Odat
TIME lECTURES ON ROOM 1
4:00-4:15 Trauma Care in Jordan. Where we Stand?, Dr. Mahmoud Odat (Jordan)
4:15-4:30 Challenges to Develop Trauma System in KSA, Dr. Saudi Al-Turki (KSA)
4:30-4:45 Influence of ATLS in KSA, Dr. Saudi Al-Turki (KSA)
4:45-5:00 Pre-Hospital Care: The Future in Jordan, Dr. Hazem Ajarma (Jordan)
5:00- 5:15 The Role of Trauma System in Mass Causality, The Military Experience, Dr. Ahmad Uraiqat (Jordan)
5:15- 5:30 Establishing a Trauma System in Jordan, Dr. Ahmad Zarour (Jordan)
5:30- 5:45 Damage Control Surgery: Indications and How to Do it?,Dr. George Abi Saad (Lebanon )
5:45-6:00 Discussion and Feedback
• THURSDAy M
Ay 5TH - RO
OM
1 •

34
American College of SurgeonsJordan Chapter
THURSDAy MAy 5TH-ROOM 2Urology Surgery Session (4:00-6:00)Moderators: Dr. Said Ajlouni, Dr. Muhannad Nasser, Dr. Jabr Zaben
TIME lECTURES ON ROOM 2
4:00-4:20 Surgery for Locally Advanced and Olio Metastatic Prostate Cancer, Dr. Rami Azab (Jordan)
4:20-4:40 Guidelines and Update on Muscle Invasive Bladder Cancer, Dr. Firas Hammouri (Jordan)
4:40-5:00 Updates on Testicular Tumor Management, Dr. Khaldoun Gharaibeh (Jordan)
5:00-5:20 Nephron Sparing Surgery: Expanded Indications and Refined Techniques, Dr. Adnan Abo Gamar (Jordan)
5:20-5:40 Updates in the Management of Upper Urothelial Tumors, Dr. Samer Geizawi (Jordan)
5:40- 5:50Over the Counter Antibiotics? Effects on Escherichia Coli Incidence and Resistance in Uncomplicated Urinary Tract Infections in Jordan, Dr. Zeid Abu Ghosh (Jordan)
5:50-6:00Does Low Case Volume at Private Practice Predict Outcome of Advanced Laparoscopic Renal Surgery?, Dr. Khalid Safi (Jordan)
• THURSDAy M
Ay 5TH - RO
OM
2 •

35
American College of SurgeonsJordan Chapter
THURSDAy MAy 5TH-ROOM 3Pediatric Surgery Session (4:00-6:00)Moderators: Dr. Hayel Eajelat, Dr. Hashem Momani, Dr. Hassan Aljaded
TIME lECTURES ON ROOM 34:00-4:30 Intersex Anomalies, Dr. Yaser Jamaal (KSA)
4:30-4:40 Neuroblastoma: Successful Escalation Through Multi Disciplinary Team, Dr. Khalil Ghandour (Jordan)
4:40-4:55 Familial Malrotation of the Intestine, Dr. Hashem Momani (Jordan)
4:55-5:10 Augmentation Cystoplasty for Congenital Neurogenic Bladder in Children, Dr. Ibrahim Daradka (Jordan)
5:10-5:25Laparoscopic and Laparoscopic Assisted Pyeloplasty for Repair of Pelvi-Ureteric Junction Obstruction in Children, Dr. Najeh Alomari (Jordan)
5:25-5:40 Re Do surgery in Hirschsprung Disease, Dr. Essam Al Halaby (Egypt)
5:40-5:50 Experience with Minimal Invasive Surgery in Children and Infancies, Dr. Ahmad Al-Raymoony (Jordan)
5:50-6:00Pneumatic Reduction of Pediatric Intussusception (Our Experience at Queen Rania Al-Abdullah Hospital for Children), Dr. Wasim Al-Mefleh (Jordan)
• THURSDAy M
Ay 5TH - RO
OM
3 •

36
American College of SurgeonsJordan Chapter
• FRIDAy M
Ay 6TH •
FRIDAy MAy 6TH-All ROOMSSurgical Jeopardy (8:00-10:00)Moderator: Osama H Hamed, MD, FACSCo-Moderators: Mohannad Qulaghassi, MD, Tawfiq Shobaki, MD Judges: Saed Natour, MD, FACS , Ashraf Haddad, MD
Team 1: Jordan University Hospital: Tayseer Al Tarawneh, Hiba HawashinTeam 2: Jordan University of Science and Technology: Asem Qandah, Saqer AbdullatTeam 3: Royal Medical Services: Mutaz Naffa, Hiba Al AbbadiTeam 4: Jordan Hospital: Majd Haddadin, Laith RabadiTeam 5: Specialty Hospital: Rami Owais, Abdullah RamadanTeam 6: Islamic Hospital: Ibrahim Numan, Ibrahim Rajab
10:00-10:30 - Break

37
American College of SurgeonsJordan Chapter
FRIDAy MAy 6TH-ROOM 1Women In Surgery (10:30-12-30)Moderators: Dr. Hanan Rihan, Dr. Bareqa Salah, Dr. Sanaa Hammoury, Dr. Ghada Nimri
TIME lECTURES ON ROOM 1
10:30-10:50 The History of Women in Surgery, Dr. Lara Abu Ghazaleh (Jordan)
10:50-12:00
My Experience:Dr. Sanaa Hammoury Dr. Ghada Nimri Dr. Lamees ArabiyatDr. Layal AsirDr. Suzan BakhietDr. Maymona AttiyatDr. Nagham Alkaragholli (Challenges Facing Women Surgeons)Dr. Hiba Abbadi (Surgery&Feminity: True&False concepts)Dr. Mais Alkarmi
12:00-12:15 Dr. Eiman Sbaity (Lebanon)
12:15-12:30 Advocating for Minorities in Surgery : The American College of Surgeons Experience by Dr. Courtney Townsend (USA)
12:30-2:00 Lunch and Prayer
• FRIDAy M
Ay 6TH - RO
OM
1 •

38
American College of SurgeonsJordan Chapter
FRIDAy MAy 6TH-ROOM 2Cardiac Surgery Session (10:30-12-30)Moderators; Dr. Abdullah Al-Qudah, Dr. Ali Abu Rumman, Dr. Moath Smadi
TIME lECTURES ON ROOM 2
10:30-10:50 Multiple Arterial Revascularization in CABG, Benefits, and How to Plan it?, Yahia Balbaa, MD, (Egypt)
10:50-11:05 Stroke After Cardiac Surgery,Dr. Emad Hijazi, MD (Jordan)
11:05-11:20 Arterial Conduits in Coronary Artery Revascularization, Dr. Haitham Altaani (Jordan)
11:20-11:35 Minimally Invasive Mitral Valve Surgery, Dr.Amjad Bani Hani, (Jordan)
11:35-11:50 Papillary Fibro-Elastoma, An Unusual Presentation of a Cardiac Tumor, Dr. Yanal AlNaser (Jordan)
11:50-12:05Surgical Aspects in the Treatment of Hypertrophic Obstructive Cardiomyopathy, Salah Eldien Altarabsheh (Jordan)
12:05-12:25 When to Postpone Cardiac Surgical Procedure in our Daily Practice? By Dr. Yahia Balbaa, (Egypt)
12:25-12:40 Discussion12:40-2:00 Lunch and Prayer
• FRIDAy M
Ay 6TH - RO
OM
2 •

39
American College of SurgeonsJordan Chapter
FRIDAy MAy 6TH-ROOM 3ENT Surgery Session (10:30-12-30)Modrators: Dr. Nemer Al-Khtoum, Dr. Abdel-Sattar Wreikat
TIME lECTURES ON ROOM 310:30-10:50 Open Rhinoplasty Approach, Dr. Hossam Foda (Egypt)10:50-11:10 Tip Suturing Techniques, Dr. Hossam Foda (Egypt)11:10-11:30 The Deviated Nose, Dr. Hossam Foda (Egypt)11:30-11:50 Revision Rhinoplasty, Dr. Hossam Foda (Egypt)
11:50-12:10 Endoscopic SPG Block: A New None-Invasive Technique,Dr. Mohannad Al-Qudah (Jordan)
12:10-12:30 Discussion12:30-2:00 Lunch and Prayer • FRIDA
y MA
y 6TH - ROO
M 3 •

40
American College of SurgeonsJordan Chapter
FRIDAy MAy 6TH-ROOM 1Transplant: Cadaveric liver Transplantation Session (2:00-4:10)Moderators: Dr. Abdel Aziz Ziadat, Dr. Ali Obaidat, Dr. Saeb Hammoudi
TIME lECTURES ON ROOM 1
2:00-2:10 Jordan Experience in Cadaveric Liver Transplantation, Limited but Optimistic, Dr. Khalid Ajarmeh (Jordan)
2:10-2:30 Saudi Arabia Experience in Cadaveric Liver Transplantation,Dr. Hamad Bahili (KSA)
2:30-2:50 Comparison Between Cadaveric and Living Donor Liver Transplantation, Dr. Ayman Obaid (Jordan)
2:50- 3:10 Obstacles Facing Cadaveric Liver Transplantation Program in Jordan, Dr. Sameer Smadi (Jordan)
3:10- 3:30 Saudi Arabia Efforts in Encouraging Cadaveric Liver Transplantation, Dr. Hamad Bahili (KSA)
3:30-3:50 Jordan Efforts in Encouraging Cadaveric Liver Transplantation, Dr. Abdelhadi Braizat (Jordan)
3:50-4:00 Islet Cell Transplantation, Dr. Ali Dabous (Jordan)
4:00-4:10 Discussion and Questions4:10-4:30 Break
• FRIDAy M
Ay 6TH - RO
OM
1 •

41
American College of SurgeonsJordan Chapter
FRIDAy MAy 6TH-ROOM 3Vascular Surgery Session (2:00-4:00)Moderators: Dr. Walid Masoud, Dr. Saber Rawashdeh, Dr. Ziad Quran
TIME lECTURES ON ROOM 3
2:00-2:20 Endovascular Treatment of Ruptured Aortic Aneurysms:Where is the Evidence?, Dr. Jamal Hoballah (Lebanon)
2:20-2:40 Carotid Arterial Disease and Coronary Artery Disease: What is the Best Approach, Dr. Munier Nazzal ( USA)
2:40-3:00Fluoroscopic Guided Thrombo-Embolectomy for Acute Limb Ischemia: a Valuable Technique, Dr. Jamal Hoballah (Lebanon)
3:00-3:20 Vascular Shunts for Portal Decompression, Dr. Mamoun AlBasheer (Jordan)
3:20-3:40 Fenestrated and Branched Grafts, Dr Munier Nazzal (USA)3:40-4:00 Difficult Case Presentations, Dr. Osama Hirzallah (Jordan)4:00-4:30 Break
• FRIDAy M
Ay 6TH - RO
OM
3 •

42
American College of SurgeonsJordan Chapter
FRIDAy MAy 6TH-ROOM 1Minimal Invasive Surgery/HPB Session (4:30-6:30)Moderators : Dr. Khalil Zayadeen, Dr. Samir Smadi, Dr. Salam DaradkehDr. Firas Obeidat
TIME lECTURES ON ROOM 1
4:30-4:45
Laparoscopic Cholecystectomy Exposing the Inner Layer of the Subserosal (SS-Inner) Layer of the Gallbladder Can Fill the Gap of the Shortness of the Critical View of Safety,Dr. Goro Honda (Japan)
4:45-5:00Laparoscopic Complete Mesocolic Excision (CME) for Right Colon Cancer: Evidence and Technique, Dr. Ayman Agha (Germany)
5:00-5:15Laparoscopic Transabdominal Lateral Adrenalectomy;6 years Experience at King Hussein Medical CenterWa’el AlNa’ssan
5:15-5:30 Algorithm for Management of Leak After Sleeve Gastrectomy, Dr. Ahmad Bashir (Jordan)
5:30-5:40 Laparoscopic Splenectomy for Massive Splenomegally: Technical Details, Dr. Osama Hamed (Jordan)
5:40-5:55 Laparoscopic Adrenalectomy for Large Tumors: Trans-or Retroperitoneal?, Dr. Ayman Agha (Germany)
5:55-6:25 Application of Minimally Invasive Surgery for Benign and Malignant Pancreatic Diseases, Goro Honda (Japan)
6:25-6:40 Cystic Neoplasms of the Pancreas, the RMS Experience,Dr. Ashraf Faouri (Jordan)
6:40-6:55 Questions and Discussion
8:00 Gala Dinner
• FRIDAy M
Ay 6TH - RO
OM
1 •

43
American College of SurgeonsJordan Chapter
FRIDAy MAy 6TH-ROOM 2Obstetricians & Gynecology Surgery Session(4:30-6:30)Moderators: Dr. Falah Khalifa, Dr. Mazen Fraij, Dr. Maha Quba’en
TIME lECTURES ON ROOM 2
4:30-4:55 Fertility Preservation in Gynecological Malignancy Patients,Dr. Kamil Fram (Jordan)
4:55-5:20 Rupture Uterus in Pregnancy and Labor, Dr. Mazen El-Zibdeh (Jordan)
5:20-5:50 New Approach in Surgical Management of Pelvic Organ Prolapse, Dr. Abdallah Fayyad (UK)
5:50-6:15 Hysteroscopy Update, Dr. Mohammad Al Qudah (Jordan)
6:15-6:30 Hysterectomy in the 21st Century, Different Approach and Different Challenges, Dr. Isam Latayfeh (Jordan)
8:00 Gala Dinner
• FRIDAy M
Ay 6TH - RO
OM
2 •

44
American College of SurgeonsJordan Chapter
FRIDAy MAy 6TH-ROOM 3Plastic Surgery Session (4:30-6:30)Moderators: Dr. Mutaz AL-Karmi, Dr. Mahmoud WreikatDr. Mohammad Abu Al-Samen
TIME lECTURES ON ROOM 3
4:30-4:50 Planas Mammary Reduction Technique, Dr. Gabriel Planas (Spain)
4:50-5:10 Tips and Tricks in Inferior Pedicle Breast Reduction, Dr. Hisham El-Minawi (Egypt)
5:10-5:30 Immediate Single Stage Breast Reconstruction Using Dermal Barrier Flap, Dr. Bishara Atiyeh (Lebanon)
5:30-5:50 Augmentation Mastopexy With Implants, Dr. Gabriel Planas (Spain)
5:50-6:10 Fat Injection in Breast Remodeling, Dr. Hisham El-Minawi (Egypt)
6:10-6:30 Therapeutic Reduction Mammoplasty (TRM), Dr. Bishara Atiyeh (Lebanon)
8:00 Gala Dinner
• FRIDAy M
Ay 6TH - RO
OM
3 •
45
American College of SurgeonsJordan Chapter
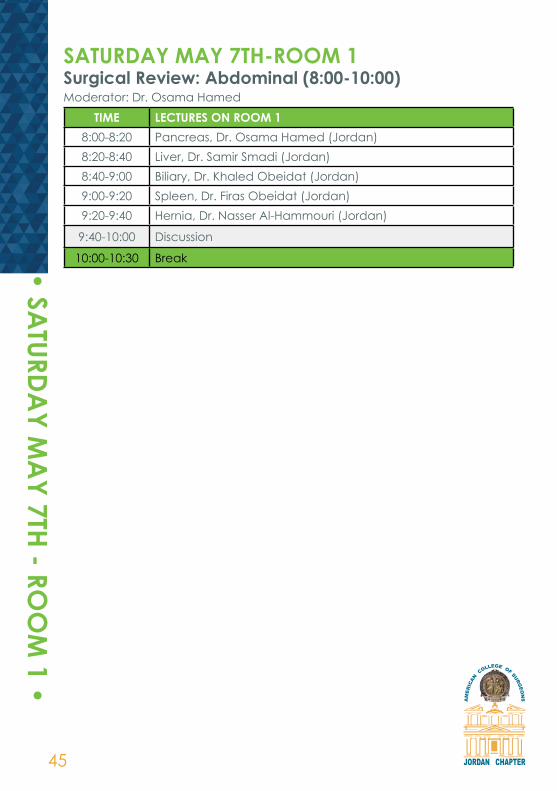
SATURDAy MAy 7TH-ROOM 1Surgical Review: Abdominal (8:00-10:00)Moderator: Dr. Osama Hamed
TIME lECTURES ON ROOM 18:00-8:20 Pancreas, Dr. Osama Hamed (Jordan)8:20-8:40 Liver, Dr. Samir Smadi (Jordan)8:40-9:00 Biliary, Dr. Khaled Obeidat (Jordan)9:00-9:20 Spleen, Dr. Firas Obeidat (Jordan)9:20-9:40 Hernia, Dr. Nasser Al-Hammouri (Jordan)
9:40-10:00 Discussion
10:00-10:30 Break• SATURDA
y MA
y 7TH - ROO
M 1 •

46
American College of SurgeonsJordan Chapter
SATURDAy MAy 7TH-ROOM 2TEAM (Treatment Evaluation And Management) (8:00-10:00)Moderators: Dr. Ahmad Zarour, Dr. Mahmoud Odat
TIME lECTURES ON ROOM 28:00-8:15 Welcome and Introduction, Dr. Mahmoud Odat (Jordan)
8:15-8:30 “Bad” Initial Assessment Demonstration and Discussion,Dr. Ahmad Zarour (Jordan)
8:30-9:15 Slide Lectures I, Dr. Mahmoud Odat (Jordan)9:15-10:00 Slide Lectures II, Dr. Ahmad Zarour (Jordan)10:00-10:30 Break• SA
TURDAy M
Ay 7TH - RO
OM
2 •

47
American College of SurgeonsJordan Chapter
SATURDAy MAy 7TH-ROOM 1Surgical Review: Alimentary (10:30-12:30)Moderator: Dr. Zaki Qulaghassi (Jordan)
TIME lECTURES ON ROOM 1
10:30-10:50 GERD/ Hiatal Hernia/Achalasiam Dr. Saed Al-Natour (Jordan)
10:50-11:10 Esophageal/Gastric Malignancy, Dr. Salah Halaseh (Jordan)11:10-11:30 Colorectal Cancer, Dr. Amer Amireh (Jordan)11:30-11:50 Benign Colorectal Disease, Dr. Tareq Al-Jabery (Jordan)
11:50-12:10 Bowel Obstruction/GI Bleeding/Peptic Ulcer DiseaseDr. Fayez Daoud (Jordan)
12:10-12:30 Discussion
12:30-1:30 Lunch
• SATURDA
y MA
y 7TH - ROO
M 1 •

48
American College of SurgeonsJordan Chapter
SATURDAy MAy 7TH-ROOM 2TEAM (Treatment Evaluation And Management) (10:30-12:30)Moderators: Dr. Ahmad Zarour, Dr. Mahmoud Odat
TIME lECTURES ON ROOM 2
10:30-10:55 “Good” Initial Assessment Demonstration and Discussion,Dr. Ahmad Zarour (Jordan)
10:55-11:00 Move to Scenario Sessions
11:00-11:40
Group Sessions:(a) Focused Discussion (40 min, Groups I+II)by Dr. Mamoun Qaryouti, Dr. Ruba Al-Hamad(b) Simulated Patient 1 (20 min, Groups III)Switch Between Groups III, IVby Dr. Odai Al-Sayegh (c) Simulated Patient 2 (20 min, Groups IV)by Dr. Abdulla Khwaldeh
11:40-11:50 Switch
11:50-12:30
Group Sessions:(a) Focused Discussion (40 min, Groups III+IV)By Dr. Mamoun Qaryouti, Dr. Ruba Al-Hamad(b) Simulated Patient 1 (20 min, Group I)Switch Between Group I, IIby Odai Al-Sayegh(c) Simulated Patient 2 (20 min, Group II)by Dr. Abdulla Khwaldeh, Dr. Maymona Atteyat
12:30-1:30 Lunch
• SATURDA
y MA
y 7TH - ROO
M 2 •

49
American College of SurgeonsJordan Chapter
SATURDAy MAy 7TH-ROOM 1Surgical Review: Breast (1:30-3:00)Moderator: Dr. Mahmoud Al Masri (Jordan)
TIME lECTURES ON ROOM 11:30-1:57 Benign Breast Disease, Dr. Eman Sbeity (Lebanon)1:57-2:24 Breast Cancer, Dr. Mahmoud Al-Masri (Jordan)
2:24-2:51 Breast Cancer in Special Situations and Adjuvant Therapies,Dr. Eman Sbeity (Lebanon)
2:51-3:00 Discussion
3:30-4:00 Break
• SATURDA
y MA
y 7TH - ROO
M 1 •

50
American College of SurgeonsJordan Chapter
SATURDAy MAy 7TH-ROOM 2TEAM (Treatment Evaluation And Management)(1:30-3:00)Moderators: Dr. Ahmad Zarour, Dr. Mahmoud Odat
TIME lECTURES ON ROOM 21:30-2:00 Exam, Dr. Ahmad Zarour (Jordan)2:00-2:30 Summary/Adjourn, Dr. Ahmad Zarour, Dr. Mahmoud Odat3:30-4:00 Break
• SATURDA
y MA
y 7TH - ROO
M 2 •

51
American College of SurgeonsJordan Chapter
SATURDAy MAy 7TH-ROOM 1Surgical Review: Endocrine (4:00-4:45)Moderator: Dr. Nidal Younes (Jordan)
TIME lECTURES ON ROOM 14:00-4:30 Endocrine, Dr. Nidal Younes (Jordan)
4:30-4:45 Discussion
Surgical Review: Vascular (5:00-6:00)Moderator: Mamoun Al-Qaryouti
TIME lECTURES ON ROOM 1
5:00-5:10 Peripheral Vascular/ Critical Limb Ischemia, Dr. Jamal Hoballah (Lebanon)
5:10-5:20 Discussion 5:20-5:30 Vascular Diseasse, Dr. Munir Nazzal (USA)5:30-5:40 Discussion
5:40-5:50 Vascular Disease: Management and Diagnosis, Dr. Jamal Hoballah (Lebanon)
5:50-6:00 Discussion
• SATURDA
y MA
y 7TH - ROO
M 1 •

52
American College of SurgeonsJordan Chapter
SUNDAy MAy 8TH-ROOM 1Surgical Review: Trauma (8:00-10:00)Moderator: Dr. Khaled Ajarma
TIME lECTURES ON ROOM 1
8:00-8:37 Trauma, Resuscitation, Head and Neck Injuries, Dr. Ahmad Zaarour (Jordan)
8:37-9:14 Chest and Abdominal Trauma, Dr. Maymona Atteyat (Jordan)
9:14-9:51 Pelvic, Vascular and Extremity, Dr. Mahmoud Odat (Jordan)
9:51-10:00 Discussion
10:00-10:30 Break
• SUNDA
y MA
y 8TH - ROO
M 1 •

53
American College of SurgeonsJordan Chapter
SUNDAy MAy 8TH-ROOM 2TEAM (Treatment Evaluation And Management) (8:00-10:00)Moderators: Dr. Ahmad Uraiqat, Dr. Mahmoud Odat
TIME lECTURES ON ROOM 28:00-8:15 Welcome and Introduction, Dr. Mahmoud Odat (Jordan)
8:15-8:30 “Bad” Initial Assessment Demonstration and Discussion,Dr. Ahmad Uraiqat (Jordan)
8:30-9:15 Slide Lectures I, Dr. Mahmoud Odat (Jordan)9:15-10:00 Slide Lectures II, Dr. Ahmad Uraiqat (Jordan)10:00-10:30 Break
• SUNDA
y MA
y 8TH - ROO
M 2 •

54
American College of SurgeonsJordan Chapter
SUNDAy MAy 8TH-ROOM 1Surgical Review: Critical Care (10:30-12:40)Moderator: Dr. Saed Natour (Jordan)
TIME lECTURES ON ROOM 110:30-11:01 Perioperative Cardiac Evaluation, Dr. Ali Hallal (Lebanon)11:01-11:32 DVT/ PE Prophylaxis and Treatment, Dr. Ali Hallal (Lebanon)11:32-12:03 Critical Care: Respiratory, Dr. George Abi Saad (Lebanon)12:03-12:34 Critical Care: Cardiac, Dr. George Abi Saad (Lebanon)
12:34-12:40 Discussion
12:40-2:00 Lunch
• SUNDA
y MA
y 8TH - ROO
M 1 •

55
American College of SurgeonsJordan Chapter
SUNDAy MAy 8TH-ROOM 2TEAM (Treatment Evaluation And Management) (10:30-12:30)
TIME lECTURES ON ROOM 2
10:30-10:55 “Good” Initial Assessment Demonstration and Discussion,Dr. Ahmad Uraiqat (Jordan)
10:55-11:00 Move to Scenario Sessions
11:00-11:40
Group Sessions:(a) Focused Discussion (40 min, Groups I+II)by Dr. Jehad Al Ajlouni, Dr. Ahmad jabr,(b) Simulated Patient 1 (20 min, Groups III)switch between Groups III, IVby Dr. Fadi Al Rousan(c) Simulated Patient 2 (20 min, Groups IV)by Dr. Abdelhamid Al Abadi
11:40-11:50 Switch
11:50-12:30
Group Sessions:(a) Focused Discussion (40 min, Groups III+IV)by Dr. Jehad Al Ajlouni, Dr. A Jabr(b) Simulated patient 1 (20 min, Group I)Switch between Group I, IIby Dr. Fadi Al RousanSimulated Patient 2 (20 min, Group II)by Dr. Abdelhamid Al Abadi
12:30-2:00 Lunch
• SUNDA
y MA
y 8TH - ROO
M 2 •
56
American College of SurgeonsJordan Chapter
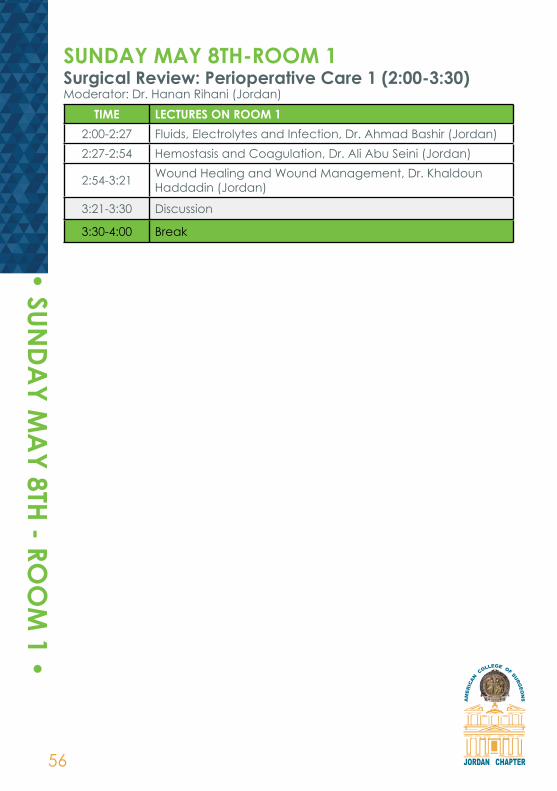
SUNDAy MAy 8TH-ROOM 1Surgical Review: Perioperative Care 1 (2:00-3:30)Moderator: Dr. Hanan Rihani (Jordan)
TIME lECTURES ON ROOM 12:00-2:27 Fluids, Electrolytes and Infection, Dr. Ahmad Bashir (Jordan)2:27-2:54 Hemostasis and Coagulation, Dr. Ali Abu Seini (Jordan)
2:54-3:21 Wound Healing and Wound Management, Dr. Khaldoun Haddadin (Jordan)
3:21-3:30 Discussion
3:30-4:00 Break
• SUNDA
y MA
y 8TH - ROO
M 1 •

57
American College of SurgeonsJordan Chapter
SUNDAy MAy 8TH-ROOM 2TEAM (Treatment Evaluation And Management) (2:00-3:00)
TIME lECTURES ON ROOM 22:00-2:30 EXAM, Dr. Ahmad Uraiqat (Jordan)2:30-3:00 Summary/Adjourn, Dr. Ahmad Uraiqat, Dr. Mahmoud Odat3:30-4:00 Break
• SUNDA
y MA
y 8TH - ROO
M 2 •

58
American College of SurgeonsJordan Chapter
SUNDAy MAy 8TH-ROOM 1Surgical Review: Perioperative Care 2 (4:00-5:30)Moderator: Dr. Hanan Rihani (Jordan)
TIME lECTURES ON ROOM 14:00-4:27 Nutrition, Dr. Osama Hamed (Jordan)4:27-4:54 Renal Function, Dr. Almothanna Shanaah (Jordan)4:54-5:21 Pharmacology, Dr. Hanan Rihani (Jordan)
5:21-5:30 Discussion
CERTIFICATES AND FEEDBACK
• SUNDA
y MA
y 8TH - ROO
M 1 •


60
American College of SurgeonsJordan Chapter
• ABSTRACTS •

61
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Establishing Surgical Residency Curriculums: Where to Start and How to Do? Dr. Courtney Townsend (USA)
Essentials include graduate certified medical school, a progressively graded course study and clinical experience under guidance and supervision with certified surgeons. There must be productive increases in responsibility based upon verified increased ability up to complete management of with patients.
Transforming US Surgical Education System Into the Middle East: the AUB Experience Dr. Jamal Joballah, (Jordan)
The Department of Surgery at the American University of Beirut (AUB) was established and chaired in 1867 by Dr George E. Post. It is currently composed of seven divisions: General Surgery, Orthopedic Surgery, Plastic Surgery, Urology, Neurosurgery, Vascular Surgery and Cardiothoracic Surgery. The Surgical Residency Training program at AUB is the first residency training program in the Middle East. It was established in 1946 by Dr Joseph J. McDonald and became accredited by the American Board of Surgery during his chairmanship. Up till the Lebanese civil war back in 1978 the surgical residency program at the American University was the only program outside the United States whose graduates were allowed to sit for the American Board of Surgery without having to repeat any of their surgical training in the US. This privilege was lost during the civil war. With the establishment of new rules by the Accreditation Council of Graduate Medical Education (ACGME), such status could not be regained. During the past 8 years, major efforts have been carried by the faculty and residents of the Department of Surgery to realign and comply with the ACGME requirements. Currently the Department of Surgery is applying for accreditation by the ACGME International. The challenges of this journey, its benefits and the AUB experience will be presented
Can We Improve Things in Jordan ?Dr. Nidal Younes (Jordan)

62
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Proposal for Improving Surgical Education at RMSBrig. Dr. Khaldoun Haddadin, BSc, MB ChB, FRCS (Eng)Consultant Plastic Reconstructive SurgeonChairman Department of Surgery, King Hussein Medical Center - Jordan
The Royal Medical Services prides itself in its Dedication to Continuous Medical EducationWe have a duty to enable surgeons to achieve and maintain the highest standards of Post-Graduate Training and ultimately of patient care. The apprenticeship model of training lacks structure, focus and accountability. Modern structures of training have adopted a competency based model which moves emphasis away from set examinations towards structured supervised learning and assessment in the workplace with definable endpoints where the resident takes responsibility for his or her own learning.Over the last few months we have started to develop the infrastructure for such a system at RMS including: – Development of website to include each Resident’s Portfolio and eLogbook – Introduction of syllabus during each rotation with work-based assessments of clinical cases and procedures, to be included in the resident’s portfolio– Appointment of Educational and Clinical Supervisors for each resident to mentor, advise and continually supervise training– Introduction of Smart Card for automatically calculating the attendance of scientific activities– Changes in regulations to include discussion of portfolio and logbook within the yearly OSCE exam at RMS– Mandate the residents attend predefined established courses such as BSS, ACLS, ATLS etc, during the Residency Program–Progression to 4th year in residency program dependent on passing part 1 of the Jordanian Board of General SurgeryIt is hoped this pilot scheme will develop and progress to keep in line with the regulations of The Jordanian Medical Council
Assessment of Surgery Residents: Where, When and How? Dr. Courtney Townsend (USA)
Surgical residency has moved from preceptor based to competency based model. This requires periodic examinations both didactic and skills-based application and verification for step-wise increase in responsibility.
Nipple Sparing MastectomyDr. Eman Sbeity (Lebanon)

63
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Contralateral Prophylactic Mastectomy is there Survival Benefit?Dr. Ali Abu Seini (Jordan)
Breast Cancer Surgery Research in the Arab World and the Region. Dr. Mahmoud Al-Masri (Jordan)
Breast Cancer is one of the most common type of breast cancer among women in the Arab world. Research in breast cancer in general and in breast cancer surgery in practical is important for each country or region inorder to understand trend at presentation, Management and cultural differences. In addition , no doubt that high research activates in breast cancer surgery can reflected positively in clinical practice.Despite surgery being one of the main modalities for treatment breast cancer, investment in breast cancer surgical research in all Arab countries is very low.In this presentation, the contribution and Trends, the Arab countries to Breast cancer surgery research will be presented and compared in non-Arabs Middle Eastern Countries. The result of questionnaire to explore the knowledge . Attitude and Practice (KAP) toward clinical research among King Hussein Cancer Center physician and general public to identify barriers toward research involvement will be discussed.

64
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
The Role of PET/CT in Management of Breast CancerDr. Akram Al-Ibraheem
Positron emission tomography combined with computed tomography (PET/CT) has been receiving increasing attention during last two decades as an effective hybrid modality in modern oncology practice. Although FDG PET has been introduced as a powerful imaging modality in different cancers, still its role is not well comprehended for management of breast cancer. The utilization of imaging to stage patients with breast cancer has evolved from a reliance on conventional techniques, such as the bone scan and computed tomography (CT), to more advanced hybrid molecular imaging, such as PET/CT in certain situations. Taking into account the considerable cost of this modality, appropriate usage is critical to optimize healthcare delivery. There is no strong evidence to support the role of FDG PET/CT in characterization of breast masses or screening for breast cancer or for the detection of axillary nodal involvement. However, FDG PET/CT is appropriate in higher-risk populations for definitive whole-body initial staging and for the differentiation of recurrent tumor from post-therapy changes. Literature has shown also value in the restaging of patients with recurrent breast tumors. Tumor biologic features represent an evolving area of interest in defining treatment. In this context, an emergent potential indication for FDG PET is a tool in prognostic stratification and for assessing early response to therapy. In routine surveillance, FDG PET/CT is strongly discouraged for patients with asymptomatic breast cancer who have achieved a complete response. This presentation will discuss the evolving co-relation between molecular imaging and anatomic in breast cancer with focusing on FDG PET/CT.
laparoscopic Rectal Cancer Surgery, Is the Pendulum Swinging Back? Dr. Ayman Agha (Germany)
Laparoscopic Complete Mesocolic Excision (CME) for Right Colon Cancer: Evidence and TechniqueAlthough the impact of complete mesocolic excision (CME) on overall as well as disease-free survival in patients with adenocarcinoma of the right hemicolon is still a matter of debate, CME becomes more and more standard procedure for oncologic right hemicolectomy due to the higher lymph node resection rate. This procedure can be performed safely by the laparoscopic approach. Nevertheless, there are some technical specialities and difficulties that have to be taken into account. Knowing the technical tricks and ‘classical’ pitfalls plays a pivotal role for save and proper surgery. A consistent training program with experienced laparoscopic surgeons may help to avoid or minimize intraoperative as well as postoperative complications during the learning curve.

65
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
“Watch and Waite” Strategy in Rectal Cancer with Clinical Complete Response After Neoadjuvant C Cheomradiotherapy Dr. Haytham El Salhat (UAE)
Update in Differentiated Thyroid Cancer Management Dr. Enas Younis (Jordan)
Update in differentiated thyroid cancer management. Epidemiologic studies have shown the prevalence of palpable thyroid nodules to be approximately 5% in women and 1% in men living in iodine-sufficient parts of the world . In contrast, high-resolution ultrasound (US) can detect thyroid nodules in 19–68% of randomly selected individuals with higher frequencies in women and the elderly . The clinical importance of thyroid nodules rests with the need to exclude thyroid cancer, which occurs in 7–15% depending on age, sex, radiation exposure history, family history, and other factors. Differentiated thyroid cancer (DTC), which includes papillary and follicular cancer, comprises the vast majority (>90%) of all thyroid cancers.The contemporary management of differentiated thyroid cancer equires a multidisciplinary approach involving primary care physicians, endocrinologists, surgeons, pathologists, nuclear medicine specialists, and sometimes radiologists and oncologists for diagnosis, treatment, and long-term surveillance. Despite the fact that most cases of well-differentiated thyroid carcinoma have an excellent prognosis, optimal treatment of the disease remains controversial. Perhaps because of the slow growth of the tumors and the infrequency with which patients die of the disease, The optimal extent of surgical resection continues to be debated, Many have questioned whether a lymph node dissection is beneficial to patients, and if so, how extensive such a dissection should be, as does the question of which patients should receive radioactive iodine. Over the last 15–20 years, there have been many advances in the diagnosis and therapy of both thyroid nodules and DTC, but clinicalcontroversy exists in many areas.

66
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Extended Resection for lung Cancer Dr. Alper Toker (Turkey)
Group Florence Nightingale, Department of Thoracic Surgery, Istanbul Locally advanced lung cancer (T3 or T4) has worse prognosis than lower T stage disease. The diagnosis is usually made radiologically. Where there is no evidence of N2 disease, distant metastasis, and the invasion of definitely unresectable structures , the patients’ radiology should be consulted to an experienced surgeon in the field of T4 tumor resection. Patients with limited invasion of the carina, left atrium, superior vena cava, or pulmonary artery may be able to be completely resected. Palliative incomplete resections of T4 disease is not an option in the treatment and are associated with very high morbidity and mortality. Surgical resection remains an important part of the therapy for patients with locally advanced lung cancer. Modern vascular reconstruction techniques and bronchoplastic procedures may allow complete resection of locally advanced tumors with favorable 5-year survival rates and low morbidity and mortality.
Forthcoming (Eighth Edition) of the TNM Staging for Non-Small Cell Lung Cancer Dr. Shadi Hamouri (Jordan)
Robotic Surgery for Lung Cancer Dr. Alper Toker (Turkey)Tracheal resections: Indications, techniques and resultsGroup Florence Nightingale, Department of Thoracic Surgery, Istanbul
Postintubation lesions are the most common indication for tracheal resection and reconstruction. Tracheal resection and reconstructions for tracheal tumors and stenosis is a well-described procedure. However, there are some certain situations which carry high risks, such as subglottic resections. Other indications include secondary tracheal tumors, tracheal trauma tracheoesophageal and tracheal innominate fisutlas. In this presentation patient selection, surgical technique, complications and results will be presented.

67
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
VATS Thymectomy Right or left Approach Experience at KHMC Dr. Hani Hadidi (Jordan)VATS Thymectomy Approaches.Our experience at KHMCHani Al Hadidi MD, Jamal Al Aydi MD, Mazen Al Omary MD, Fwaz Khmash MD, Amany mashagbeh SN
Objective: In this study we reviewed our experience in the transition of unilateral thoracoscopic thymectomy from left approach to right approach with high light on technical aspects for improving learning curve in our division.Methods:A retrospective study healed at (King Hussein Medical City) during a period from jan.2007 to april.2016. Data were collected from a computerized system of the thoracic division. Radiological data were retrieved from PACX system and pathological analysis was taken from pathological Laboratory department. All patients were analyzed, in terms of age, gender and modality of surgical approach, post operative outcome, and histopathology results.Results: 70 cases of nonthymomatous myasthenia gravis underwent thoracoscopic thymectomy; 26cases were males and 44 females. The right approach was performed in 60 cases and 10 cases through left approach. Mean age was (30.5) as it ranged from 14 to 62 years. No mortality in our study was noted. Most common post operative complication was site operation pain (intercostal neuralgia).Time of the procedure varied from 45 mints to 180 minutes (90.52 minutes mean) hospital stay was variable from 3 to 7 days (mean 3.7)Conclusions: Thoracoscopic thymectomy known to be feasible and safe procedure for myasthenia gravis disease with sooner recovery and shorter hospital stay .The right approach has been more popular with better learning curve in our study.Key words: Video-assisted thoracoscopic surgery, Thymectomy, myasthenia gravis.

68
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Tracheal Resection for Malignant and Benign ConditionsDr. Alper Toker (Turkey)
Group Florence Nightingale, Department of Thoracic Surgery, Istanbul Surgical use of robots has evolved during the last decade. However, the academic experience with robotic lung segmentectomy remains limited.Prospectively recorded clinical data of 205 patients who underwent robotic lung anatomic resections with robot-assisted thoracoscopic surgery were retrospectively reviewed. All cases were done using the da Vinci System. A three incision portal technique with a 3 cm utility incision in the posterior 10th to 11th intercostal space or anterior 5th intercostal space was performed. Individual dissection, ligation and division of the hilar structures were performed. Systematic mediastinal lymph node dissection or sampling was performed in patients either with primary or secondary metastatic cancers. Robot-assisted thoracoscopic anatomic resections for malignant and benign lesions appears to be practical, safe, and associated with few complications and short postoperative hospitalization. Lymph node removal also appears oncologically acceptable for early lung cancer patients. Benefits in terms of postoperative pain, respiratory function, and quality of life needs a comparative, prospective series particularly with video-assisted thoracoscopic surgery.
Esophageal Perforation Review of High Volume Center Experience Dr. Jamal Al-Aidi (Jordan)
Bone Graft and Bone SubstitutesDr. Mahmoud Odat (Jordan)
Managements of Bone DefectDr. Ghassan Khayyat (Jordan)
Bone Transport Using Ring Fixator Dr. Mohammad Abu Ein (Jordan)

69
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Bone Defects Treated by IlizarovDr. Castro Siffarini (Jordan)
We have treated 67 cases in Jordan of bone defects for long bones by internal bone transport using the Ilizarov method by bone transportation with deformity correction or without, with using multifunctional systems or bifocal regimes. The causes of the bone defects were open fractures in 24 segments and infected non-unions in 37, in 6 cases the fractures where non infected non-unions. The average length of the defects was 7.1 cm. There were one-level transports, two-level transports, one-level transport with fibular or ulna transport, and fibular transports. Docking site where registered in 31 cases. Problems segments underwent bone grafting. Acute shortening or docking was performed in 10 cases. Bone union was achieved in all cases. The average time of external fixation was 8 months and the average time to union was 7.1 months. Bone grafting at the docking site was used in 29 cases.

70
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Bone Defects Treated by AllograftDr. Hashem AlQdhah
Segmental long-bone defects are rare injuries, making study of their treatment and outcomes difficult. Long-bone defects are one of the most challenging problems associated with limb reconstruction following high-energy extremity trauma. Without reconstitution of structural integrity, amputation is the likely result.The management of bone defects caused by trauma and nonunion continues to represent a substantial clinical challenge in the management of orthopaedic trauma patients. The current orthopaedic literature on segmental bone loss is limited to case reports, case series, and observational studies, making it difficult to establish sound conclusions on the basis of the levels of evidence provided. A variety of treatment options have been described and reported in the literature. The relative rarity of these injuries means that high level, comparative evidence to guide their management is sparse. As such, treatment decisions must be based on knowledge of the available evidence, contemporary fracture management principles, and consideration of patient and surgeon factors. The treatment of delayed unions, malunions, and nonunions requires restoration of alignment, stable fixation. The treatment of large segmental diaphyseal bone deficiencies presents a formidable challenge. The standard treatment modalities such as cancellous bone grafting, cortical allografts, vascularized bone transfer, or distraction osteogenesis .Bone-graft materials usually have one or more components: an osteoconductive matrix, which supports the ingrowth of new bone; osteoinductive proteins, which support mitogenesis of undifferentiated cells; and osteogenic cells (osteoblasts or osteoblast precursors), which are capable of forming bone in the proper environment.Autologous bone graft, usually harvested from the iliac crest, is an excellent graft material, but its availability may be limited and the procedure to harvest the material is associated with complications. Bone-graft substitutes can either replace autologous bone graft or expand an existing amount of autologous bone graft. Various forms of bone-graft substitutes are available and include allograft bone preparations such as demineralized bone matrix and calcium-based materialsBone allografts in the reconstruction of skeletal defects have a long and somewhat controversial history in orthopedic surgery. Until relatively recently, they were viewed with little enthusiasm, chiefly because of the unpredictability of the end result of the surgical treatment.Extensive preoperative planning, meticulous operative technique, and an extended period of postoperative rehabilitation are required for optimal results.

71
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Bone Defect Treated by Induced Membrane TechniqueDr. Firas Suleiman Al-IbrahimRoyal Medical Services
Treatment of bone defects after trauma or after osteomyelitis in long bones was a challenge to most orthopedic surgeons. many techniques like bone transport by external frames, vascularized bone graft and allogarfts were used but not without complications. Induced membrane technique or what is know as Masquelet technique is a relatively new technique, it is done in two stages the first stage start by aggressive and extensive debridment to all infected bone and tissue or dead bone in cases of trauma and filling the bone defect by Bone Cement for 6-8 weeks, followed by a second stage of replacing the bone cement with bone graft taking care to preserve the membrane induced by the bone cement. here i will describe the technique and discuss few cases done in Royal Medical Services.
Managements of Bone Defect in Chronic Shoulder DislocationDr. Zaid Qarem (Jordan)
Shoulders with recurrent anterior instability often have combined bony defects of the humeral head and glenoid.Combined bony defects will lead to increased instability compared with an isolated defect, and the “critical” size of humeral head and glenoid defects that need to be addressed to restore stability will be smaller when combined rather than isolated.The glenoid track uses both glenoid and humeral head bone loss to predict subsequent risk of humeral head engagement and possible dislocation. The glenoid track shows us that restoring the track to its natural width should be among the surgeon’s first priority in restoring shoulder stability
Trauma Care in Jordan. Where We Stand? Dr. Mahmoud Odat (Jordan)

72
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Challenges to Develop Trauma System in KSA Dr. Saudi Al-Turki (KSA)Challenges in Developing the Trauma System in Saudi Arabia
Trauma is the leading cause of death for persons aged 1 through 44 years. In Saudi Arabia RTA is a major cause of morbidity and mortality at a rate exceeding heart diseases and cancer combined. Planning and implementing a Trauma system in Saudi Arabia is very challenging due to several factors including the lack of accurate and valid injury statistics, the involvement of different sectors concerned with trauma care and many Health services providers including Ministry of Health, Military Hospitals, University Hospitals, National Guard Hospitals, Security Hospitals, and the Private Sector Hospitals. Introducing trauma system to this country will face administrative, political and technical obstacles and it’s a major challenge, however because of the impact on reducing mortality and morbidity at a national level, it makes those challenges worthwhile. Due to the magnitude of trauma, the development and implementation of a National Trauma System have been deemed necessary in order to improve trauma care and outcome. Studies have shown that the in hospital morbidity and mortality can be reduced by 20%-25% for patients treated in Trauma centers. KAMC together with KAIMRC have taken the lead in developing the National Trauma Research Project, part of this project is the development of Trauma Registry, which is mainly an essential tool for trauma research. Research is the core of trauma care system; it provides the foundation for system development and performance improvement. Our goal is to provide the necessary information for Trauma program to direct all resources, conduct quality assurance, engage in injury surveillance, and develop injury prevention and control strategies in Saudi Arabia
45 Influence of ATlS in KSA Dr. Saudi Al-Turki (KSA)
Pre-Hospital Care: the Future in Jordan Dr. Hazem Ajarma (Jordan)
73
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
The Role of Trauma System in Mass Causality, The Military ExperienceAhmad Uraiqat MD FRCS FACS
A trauma system is a chain of arrangements and preparedness to provide quality response to injured from the site of injury to the appropriate hospital for the full range of care. An effective trauma system may potentially manage mass casualty incidence better. Mass casualty management strategy is closely linked to the existing trauma system.Medical lessons learned from military conflicts led to the development of civilian trauma systems.The aim of a trauma system is to save maximum lives through preparedness to achieve speed and efficiency in providing quality response in traumatic events. It ensures that all injured patients gain access to the appropriate level of care in a timely, coordinated and cost effective manner. Manpower training at every level or cadre of health worker, besides doctors, is needed to develop an efficient trauma system so that every person managing the trauma victim becomes a knowledge worker and can speak in the “same language” and wavelength.
Damage Control Surgery: Indications and How to Do it? Dr. George Abi Saad (Lebanon)
Damage control surgery is one of the major advances in surgical technique in the past 20 years. The principles of damage control contravene most standard surgical teaching practices - that the best operation for a patient is one, definitive procedure.However it is now well recognized, that multiple trauma patients are more likely to die from their intra-operative metabolic failure that from a failure to complete operative repairs. Patients who have Hypothermia T<35, Acidosis pH<7.2 and Coagulopathy PTT>60 with prolonged OR exposure, shock and massive transfusion will need a staged operative strategy. The operating team must undergo a paradigm shift in their ‘mindset’ if the patient is to survive such devastating injuries.Scheme: O Phase IO Rapid termination of operative procedureO Phase IIO Correction of physiologic abnormalities in the ICU O Phase IIIO Definitive surgery

74
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Surgery for locally Advanced and Oligo Metastatic Prostate CancerDr. Rami Azab (Jordan)
Guidelines, and Update on Muscle Invasive Bladder Cancer Firas Al-Hammouri MD, Urology ConsultantPrince Hussein Urology Center, King Hussein Medical Center
Bladder cancer (BC) is the eleventh most commonly diagnosed cancer worldwide. The incidence and Mortality rate vary across countries. The majority of patients with muscle-invasive disease have invasion at first presentation. 20% will progress to muscle-invasive disease after an initial diagnosis of non–muscle-invasive bladder cancer. Muscle-invasive bladder cancer is a highly lethal entity and if left untreated will result in mortality within 2 years of diagnosis in 85% of cases. According to the EAU non muscle invasive urinary bladder cancer guidelines, it is reasonable to propose immediate radical cystectomy to those patients who are at highest risk of progression and in the case of intravesical therapy failure. For patients with clinical T2-T4a, N0, M0 disease, radical cystectomy and bilateral pelvic lymph node dissection remains the gold standard therapy by which all other treatment modalities should be compared. The extent of lymph node dissection level has not been established to date. Complication of radical cystectomy is directly related to pre-existing co-morbidity, surgical procedure, bowel anastomosis, urinary diversion and the biological age.There are many advantages and disadvantages for administration Neo-adjuvant chemotherapy (Cisplatin- based combination) for operable disease and N0M0.Multimodality bladder – preserving treatment could be offered as an alternative in selected, well-informed and compliant patients, especially for whom cystectomy is not an option to preserve the bladder and QoL, without compromising outcome.In my presentation I will summarize the updates in muscle invasive bladder cancer.
Updates on Testicular Tumor Management Dr. Khaldoun Gharaibeh (Jordan)
Nephron Sparing Surgery: Expanded Indications and Refined Techniques Dr. Adnan Abo Gamar (Jordan)
Updates in the Management of Upper Urothelial TumorsDr. Samer Geizawi (Jordan)

75
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Intersex Anomalies Dr. Yasir S . Jamal (KSA)Staged Genital Reconstructive &Aesthetic surgery
Disorders of sex differentiation includes wide spectrum of intersex abnormalities Which needs prompt action and extensive chromosomal ,laboratory, radiological and endoscopic workup to solve the problem and to reach correct decision For the appropriate sex assignment .over the last 30 years 800 patients were managed at the center of sex determination and correction at king Abdul Aziz university hospital , Jeddah , Saudi Arabia In this presentation the staged reconstructive and aesthetic surgical management of wide spectrum of the intersex patients will be presented

76
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Neuroblastoma: Successful Escalation Through Multi Disciplinary Team Dr. Khalil Ghandour (Jordan)Neuroblastoma : Successful treatment de-escalation through Multidisciplinary careHadeel Halalsheh, MD; Taleb Ismael, MD; Khalil Ghandour, MD; Mohammad Albohaisi, RN; Iyad Sultan, MD
Background: Treatment of neuroblastoma is decided on the basis of risk stratification. Treatment of low and intermediate risk (L/IR) neuroblastoma needs judicious use of different modalities. These patients are typically over treated when their care is scattered. We report our experience with emphasis on the role of multidisciplinary care. We also propose an algorithm for management in countries with limited resources.Methods: We conducted a retrospective analysis of children with L/IR NB who presented to KHCC between Jan2003 and Dec2009. Patients’ characteristics, treatment modalities and outcome were analyzed. All cases were discussed in multidisciplinary clinic where a pediatric oncologist, radiologist, pediatric surgeon and a radiation oncologist were present. Results: We identified 40 patients (21 males) with L/IR NB (25 LR). The median age at diagnosis was 9 months (range, 2 to 48). Stage distribution was as follows: stage I, 8; stage II, 14; stage III, 7 and stage IVs, 10 patients. MYCN was amplified in 3 patients with stage I. 26 patients had operative intervention and gross total resection was achieved in 21. Chemotherapy was given to 20 patients (50%) with most (15 patients) receiving < 4 cycles. The 5-year EFS was 92±4.4% and the 5-yaer OS was 98±2.5%. Three patients died; two relapsed 15 and 39 months after diagnosis and died of disease; the third patient died of hemorrhage and renal shut down after surgery. Another patient developed progression of the residual mass 47 months after diagnosis and was lost for follow up. Conclusion: For children with non-high risk neuroblastoma there is a real possibility for further treatment reduction while maintaining the same good outcome as with more intensive and prolonged protocol dictated treatment. Such treatment can be modified only through multidisciplinary team discussion. This pioneering approach has been well received and appreciated. It is expected to form the basis of a formal treatment protocol under the auspices of the Global Neuroblastoma Network group this coming April 2016, to be formally accepted and implemented as the standard of care in countries with limited medical and financial resources.

77
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Familial Malrotation of the Intestine Dr. Hashem Momani ( Jordan)Hashem M. Al-Momania*, Mahmoud Abu-Khalafa, Ayman Musmara, Khaled Al-Zabenb,Azmi Al-Hadidic a. Department of general Surgery, The University of Jordan, Faculty of Medicine, Amman, Jordan b. Department of anesthesia, The University of Jordan, Faculty of Medicine, Amman, Jordan c. department of radiology, The University of Jordan, Faculty of Medicine, Amman, Jordan Background: To determine the inheritance pattern and outcome in familial intestinal malrotation Methodology: In the present study a total of eleven patients in three different families with surgically proved malrotation of the intestine are described in relation to presentation, management and their outcome Results: The total number of cases of malrotation in the three families was 11; Sex incidence: 6 females and 5 males. All patients underwent operative treatment except one patient who was asymptomatic. The outcome: all died except three giving a mortality of 82% Conclusion: The present study showed a strong evidence of autosomal dominant pattern of inheritance in familial intestinal malrotation . As the outcome the familial type of intestinal malrotation is poor we suggest screening the close relatives of the affected individual if they have minor symptoms .

78
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Augmentation Cystoplasty for Congenital Neurogenic Bladder in ChildrenIbrahim Daradka MD (Jordan)Augmentation Cystoplasty for Congenital Neurogenic Bladder in children: Our experience At King Hussein Medical Center. Amman-Jordan
Aim: Preservation of renal function in children with neurogenic bladder is the goal of treatment. This study analyzed the evolution of renal function in patients with Congenital Neurogenic bladder after bladder argumentation.Material / Methods: we retrospectively reviewed medical records Of 22 patients males (n=21) and female (n= 1) with neurogenic bladder between (1998 – 2014) at King Hussein Medical Center /Queen Rania hospital for children.10/22 patients underwent urinary bladder augmentation with mitroffanof, using ileal segment for augmentation and using an appendix as a conduit. Data were collected in order to the: age, gender, etiology, associated congenital abnormalities, complications, and post medical and surgical treatment outcome.Results: The mean age of patients at presentation for bladder augmentation was 6.1 years. Bladder augmentation with mitrofanoff was performed in: Patients with posterior urethral valve (59%), myelomeningocele (18%), ectopia Vesica (4.5%).High grade vesicoureteric reflux (VUR) was most frequent seen in patients with PUV. Improvement of renal function and good outcome was seen in 80% of patients who underwent augmentation cystoplasty.Conclusion: Augmentation cystoplasty is widely used in the surgical management of neurogenic bladder. A significant reduction of social and physical impaction of the disease on patients and families and satisfactory improvement of renal function can be achieved with surgical intervention.

79
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
laparoscopic and laparoscopic Assisted Pyeloplasty for Repair of Pelvi-Ureteric Junction Abstruction in Children Dr. Najeh Alomari (Jordan)Laparoscopic & Laparoscopic Assisted Pyeloplasty for Repair of Pelvi-ureteric Junction Obstruction in ChildrenNajeh yousef Alomari, MD, FACS, IMRCS/FRACS.FEBPS, JBPS, JBGSHala Falahat RN. Afnan Rasalan RN.Queen Rania
Objectives: Over the past 7 years, the treatment of choice for pelvi-ureteric junction obstruction in our team is by laparoscopy & laparoscopic assisted technique. The aim of this study is to evaluate our experience in transperitoneal laparoscopic & laparoscopic assisted pyeloplasty in children with pelvi-ureteric junction obstruction. We review the safety, efficacy, outcome parameters of operative time, analgesic requirement, and hospital stay. We present the follow up protocol and complications. Methods: With Institutional Review Board approval, the data of all patients undergoing laparoscopic & laparoscopic assisted pyeloplasty at Queen Rania Hospital for Children / King Hussein Medical Center were retrospectively reviewed of prospectively collected data over 7 years (June 2008-2015). Medical records of 180 patients underwent transperitoneal laparoscopic and laparoscopic assisted Anderson Hynes dismembered pyeloplasty in children were reviewed. The indication for pyeloplasty was kidney obstruction with deterioration of renal function on diuretic dynamic renogram (MAG3) scan and ultrasound. Laparoscopic assisted pyeloplasty done in 155 patients, 25 patients underwent totally laparoscopic pyeloplasty, reduction of the renal pelvis performed in 140 patients. JJ stent was inserted by laparoscopy and laparoscopic assisted maneuver in 170 patients. Perianastomotic drain was placed for 2 days in 15 patients. Bladder catheter was inserted in all patients for 24-48 hours. Follow-up included clinical assessment, functional assessment by ultrasound and (MAG3) scan after removing the JJ stent at 2 and 6 months.Results: The patients included 80 females and 100 males; the mean age was 6,4 years (range 2 months -12 years). Right sided pyeloplasty N=77, left sided pyeloplasty N=103. An aberrant crossing vessel N=18, bilateral pyeloplasty N=8, bilateral pyeloplasty for crossing vessels N=4. Re-do pyeloplasty by laparoscopy N=6. Mean operating time for the totally laparoscopic pyeloplasty was 200 min (range 120-400 minutes), while for the laparoscopic assisted pyeloplasty was 70 minutes (range 50-95 minutes), P value (<0.05). 30 patients had other laparoscopic surgery with the pyeloplasty simultaneously. Mean hospital stay range from 2 to 5 days. There were no peri-operative complications, no conversion to open pyeloplasty. No blood transfusion required no anastomotic leak and no mortalities. 165 patients showed improvement of renal function after removal of JJ stent by ultrasound and isotope scan, 6 patients underwent once balloon dilation for anastomotic stenosis 3 months post-operatively.

80
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Conclusion: Transperitoneal laparoscopic and laparoscopic assisted pyeloplasty in children are feasible, effective and safe techniques with minimal complications and gives excellent long-term cosmetic and functional results. The hospital stay and convalescence are short and hence rapid return to normal activity is expected with less analgesia requirements however, the laparoscopic pyeloplasty is more difficult and the operative time remains longer than open pyeloplasty, while the laparoscopic assisted pyeloplasty operative time is even less than the open procedure. These procedures should be standardized and practiced in pediatric surgical units under the supervision of expert pediatric laparoscopic surgeons with high experience in pediatric urology to achieve the best outcome and learning curve. Keywords: laparoscopy, laparoscopic assisted ,pyeloplasty, children
Re Do Surgery in Hirschsprung DiseaseEssam A Elhalaby, MD
Department of pediatric surgery, faculty of medicine, Tanta universityDespite the remarkable progress in the management of Hirschsprung’s disease (HD), a significant percentage of patients may not do well after their initial definitive operations, and some may even require redo surgery. The decision of redo surgery depends on clinical assessment, anatomical evaluation using contrast enema and other imaging studies, redo tissue diagnosis and sometimes anorectal motility studies.This presentation will highlight the frequent causes for failure of initial surgery, and describe our current protocol for management and outcome after implementing this protocol to this group of patients.Based on our cumulative experience during the past three decades, we believe that:1- in many cases, redo surgery can relieve the long suffering of many of patients with unfavorable functional results after initial surgery2- The outcome of redo surgery for HD in terms of continence and stooling frequency depends on the magnitude of sphincteric injury, which might have occurred during initial surgery.3- Redo endorectal pull-through is both feasible and safe whenever an adequate rectal cuff exits.4- Repeated myectomy should be condemned to avoid repeated injury to sphincteric complex with high risk of developing anorectal incontinence.

81
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Experience with Minimal Invasive Surgery in Children and Infancies Dr. Ahmad Al-Raymoony (Jordan) Author: Dr. Ahmad Ibrahim AL-Raymoony M.D., MBCHB, JBGS, JBPS, FRACS.Dr. Waseem AL- Meflh M.D,JBGS.JBPS.Job Details: Division Of Pediatric Surgery - Queen Rania ALAbdullah Hospital For Children. Consultant and Chief of Pediatric Surgery Department . Queen Rania ALAbdullah Hospital For Children. -king Hussein Medical Center.Royal Medical Services
Objectives:To evaluate our experience with minimally invasive surgery in children and infants at Queen Rania AL Abdullah Hospital For Children. Methods: a retrospective study included all those patients undergoing a minimally invasive surgical procedure between January 2008 and june 2014,the total number of the patients were 448 children . demographics, type of operation, complications, and length of hospital stay were recorded.Results: A 448 minimally invasive procedures were performed: Soave-Georgesonendorectal colon pull-through for Hirschsprung’s disease (N.=32); laparoscopic pullthrough for imperforated anus (N.=28); laparoscopic cholecystectomy (N.=21); laparoscopic Nissen fundoplication for gastroesophageal reflux disease (N.=12); laparoscopic assisted gastrostomy (N.=25);laparoscopic appendectomy (N. =23); laparoscopic varicocelectomy (N.=34) laparoscopic nephrectomy (N.=18); laparoscopic repair of morgagnic hernia(N.=19); laparoscopic herniotomy (N.=88); laparoscopic exploration testis and orchidopexies (N.=97);laparoscopic or thoracoscopic tumor resection or biopsy (N.=26); laparoscopic assisted mickeles diverticulum resection(N.=11); thoracoscopic repair of diaphragmatic eventration and pleural decortication(N.=14). The median age was 5 years;there weight range between( 3 to 25) kg; the median length of hospital stay was 3 days;Ninety-nine percent of procedures were completed successfully endoscopically. the complications rate was 0.9% (N.=4) and no mortalityConclusion: According to our experience, minimally invasive surgery is a safe and efficacious alternative to conventional surgery in children. It was associated with shorter Length of hospital stay and improved quality of life, with less pain and better aesthetic results. It has become the preferred surgical treatment option by parents.Keywords: minimal invasive , surgery, Children, infants

82
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Pneumatic Reduction of Pediatric Rania Al-Abdullah Hospital for Children) Dr. Wasim Al-Mefleh (Jordan)Pneumatic reduction of pediatric intussusception (Our experience at Queen Rania Al-Abdullah Hospital for Children)Waseem Al-Meflh, MD; Ahmad Abu Quraa, MD; Gaith Khaswneh, MD; Amir Al-Ibrahim, MD; Baha Abdullah, MD; Najeh Al-Omary, MD.Department of Pediatric surgery, Queen Rania Al- Abdulla Hospital for Children, K.H.M.C, Amman, Jordan.
Objective: The purpose of our study was to report our experience in the management of pediatric intussusception using Pneumatic reduction regarding the outcome, complications, success and failure rate.Method: A retrospective study was done at Queen Rania Al-Abdullah Hospital for Children in the period from September 2012 to December 2014, total number of cases were forty five, thirty two were males (71.1%) and thirteen were females (28.9%), male to female ratio was 2.5:1, The ages of patients ranged from two months to three years with a mean age of 9 months.Results: Pneumatic reduction under fluoroscopic guidance was done for forty five patients who presented with intussusception for the first time and for four recurrent intussusceptions that had occurred in four patients, in forty cases (88.9%) Pneumatic reduction was successful while unfortunately it failed in five cases (11.1%). No intestinal perforations occurredwhile using this technique.Conclusion: Pneumatic reduction under fluoroscopic guidance is a safe, simple, cost effectivetechnique with a high success rate; it is a quick procedure, easy to perform with a low radiation exposure.
The History of Women in Surgery Dr. Lara Abu Ghazaleh (Jordan)

83
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
My Experience :Dr. Sanaa Hammoury Dr. Ghada Nimri Dr. Lamees ArabiyatDr. Layal AsirDr. Suzan BakhietDr. Maymona AttiyatDr. Nagham Alkaragholli (Challenges Facing Women Surgeons)Dr. Mais Alkarmi
Surgery and Femininity.. True and False ConceptsDr. Heba G. Al-Abbadi
Despite the great social revolution that has opened most of the closed communities to the rest of world, Middle East societies remain of the most conservative and closed communities. A complex network of religious believes, customs, traditions, impact of wars, poverty, lack of awareness despite education, and a low national self-esteem, has contributed to suffering of women on a daily basis by the name of conservativeness. From early childhood girls are being brought up as being inferior to their male counterparts. For most of families, at a certain period of time, education was exclusive to boys. Recently, a gross change has been noticed by having the number of girls joining universities exceeding that of boys. Being hard workers, women have managed to prove themselves as leaders in many academic and scientific branches. However; women still suffer in every time they choose to go into a branch of life that is used to be exclusive for men.Surgery is a branch of medicine that is hard to both sexes. Only those with a unique combination of high intelligence, tolerance, sharp decision making and excellent communication skills can become successful surgeons and withstand the stress of daily surgical life. Though expanding slowly, the number of female surgeons in Jordan is still low. Continuous discouragement and a big halo of misconceptions surrounding the issue are the main two reasons. As a neighbor country still believes that women are unable to drive a car, Jordanians still see women unable to handle surgery!Femininity is the most precious value every woman is afraid to lose when joining surgery, an idea implanted by the disappointing community of men and women, to add to the obstacles female surgeon are already encountering. After five hard years in the surgical career, I have concluded that surgery has added to my personality much of strength, empathy, wisdom and tolerance. It has never detracted of my dignity, internal beauty or femininity.In this brief presentation I will review some of the critical stations in my career as a female surgeon and go through some of the common wrong concepts trying to visualize the true face of reality.
84
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Advocating for Minorities in Surgery: The American College of Surgeons Experience Dr. Courtney Townsend (USA)
The American College of Surgeons is dedicated to a Fellowship that mentors our population. There are multiple efforts to support women and other underrepresented minorities in all activities of the College and leadership positions.
Multiple Arterial Revascularization in CABG, Benefits, and how to Plan It?Dr. Yahia Balbaa, (Egypt)
Stroke After Cardiac Surgery Dr. Emad Hijazi, (Jordan)
Arterial Conduits in Coronary Artery RevascularizationDr. Haitham Altaani, (Jordan)
Minimally Invasive Mitral Valve Surgery Dr.Amjad Bani Hani, (Jordan)
Papillary Fibro-Elastoma, An Unusual Presentation of a Cardiac Tumor Yanal Alnaser, (Jordan)
A 41 year old male patient, with no previous medical illnesses, presented to hospital with a history of left sided weakness and mouth deviation. The event lasted for a couple of hours and was followed by complete recovery. He reported a similar episode six months prior to his hospitalisation that was brief and “ managed at home” .He was in normal sinus rhythm and had a normal carotid scan.Brain CT showed a small old infarct in his right temporal area.Cardiac echo showed a mass on the aortic cusps highly suggestive of papillary Fibroelastoma. Intraoperative findings, showed a small mass, later on proven by histopathology to be a Fibroelastoma, on the ventricular side of the non-coronary aortic cusp . The presentation is very unusual for a Fibroelastoma to be on the ventricular side of the non-coronary aortic cusp, causing recurrent TIA’s .Research showed a similar case to be reported in the UK, but associated with left sided chest pains)

85
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Surgical Aspects in the Treatment of Hypertrophic Obstructive Cardiomyopathy Dr. Salah Eldien Altarabsheh, (Jordan)
Hypertrophic obstructive cardiomyopathy is as an inherited autosomal dominant disorder and an important cause for heart failure. Symptomatology ranges from totally asymptomatic status to sudden cardiac death. Mechanisms proposed are obstruction at the left ventricular outflow tract, functional mitral valve regurgitation, diastolic ventricular dysfunction, and recurrent ventricular arrhythmias. Left ventricular basal septal myectomy is considered by many to be the gold standard therapy for symptomatic patients. There are many surgical considerations that should be considered during surgery such as: preserving the aortic and mitral valves, avoiding the conduction bundle and adequacy of relieving the left ventricular outflow obstructionProper pre-operative and intra-operative echocardiographic assessment is highly crucial for the surgeon in particular.
When to Postpone Cardiac Surgical Procedure in our Daily Practice? Dr. Yahia Balbaa, (Egypt)
Open Rhinoplasty Approach Dr. Hossam Foda (Egypt)Author: Hossam M.T. Foda, M.DProfessor, Head of Facial Plastic SurgeryDepartment of Otolaryngology, Alexandria Medical School, Egypt.
The Middle Eastern nose presents a unique challenge for the rhinoplastic surgeon. Most of the surgeons refrain of using external approach out of the fear of the unpredictable healing of the thick heavy nasal skin. In over 5000 external rhinoplasties, done by the author, no cases of wound dehiscence, infection, or keloid formation were encountered. Subjectively, only 1.5% found the scar unacceptable, while objectively 6.5% showed some degrees of scar widening, depression, hyperpigmentation. The two-layered closure of the incision significantly reduced the incidence of wide depressed columellar scars. Additionally, the thick heavy skin envelop requires increasing the strength and support of the cartilaginous framework to avoid the common postoperative complications of pollybeak deformity and loss of tip projection, rotation, and definition.References:

86
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
-Foda HMT: Revision Rhinoplasty: The lost tip support. In Hathiram BT, Khattar VS (eds.), Atlas of Operative Otolaryngology Head & Neck Surgery, Jaypee Brothers Medical Publishers, New Delhi, pp. 988-992, 2013-Foda HMT: External rhinoplasty for the Arabian nose: A columellar scar analysis. Aesth Plast Surg. 28(5):312-316, 2004.-Foda HMT: Rhinoplasty for the multiply revised nose. Am J Otolaryngol. 26(1):28-34, 2005.-Foda HMT: Mersiline Mesh in Premaxillary Augmentation. Aesthetic Plastic Surgery; 29: 169-173, 2005-Foda HMT: The Caudal Septum Replacement Graft. Archives of Facial Plastic Surgery Journal; 10(3):152-157, 2008
Tip Suturing Techniques Dr. Hossam Foda (Egypt)
The droopy tip is a common nasal deformity in which the tip is inferiorly rotated.500 consecutive rhinoplasty cases were studied to assess the incidence and causes of the droopy tip deformity, and to evaluate the role of three alar cartilage modifying techniques, lateral crural steal (LCS), lateral crural overlay (LCO), and tongue-in-groove (TIG), in correcting such deformity. The external rhinoplasty approach was used in all cases. Only one of the three alar cartilage modifying techniques was used in each case and the degree of tip rotation and projection were measured both pre- and postoperatively. The incidence of droopy tip was 72% and the use of an alar cartilage modifying technique was required in 85% of these cases in order to achieve the desired degree of rotation. The main causes for the droopy tip included; inferiorly oriented alar cartilages (85%), overdeveloped scrolls of upper lateral cartilages (73%), high anterior septal angle (65%), and thick skin of the nasal lobule (56%). The LCS increased nasal tip rotation and projection, the LCO increased tip rotation and decreased tip projection, and TIG increased tip rotation without significantly changing the amount of projection. The

87
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
LCO resulted in the highest degrees of rotation, followed by the LCS, and finally the TIG technique. According to our results; the LCS is best indicated in cases with droopy underprojected nasal tip, the LCO in cases of droopy overprojected nasal tip, and the TIG in cases where the droopy nasal tip is associated with an adequate amount of projection.References:-Foda HMT: External Rhinoplasty: A critical analysis of 500 cases. Journal of Laryngology & Otology; 117:473-77, 2003.-Foda HMT: External rhinoplasty for the Arabian nose: A columellar scar analysis. Aesth Plast Surg. 28(5):312-316, 2004.-Foda HMT: Management of the droopy tip: A comparison of three alar cartilage modifying techniques. Journal of Plastic Reconstructive Surgery; 112(5): 1408-1418, 2003.-Foda, H.M.T. Alar setback technique: A controlled method of nasal tip deprojection. Arch Otolaryngol Head Neck Surg. 127: 1341, 2001.-Foda, H.M.T., Kridel, R.W.H. Lateral crural steal and lateral crural overlay: An objective evaluation. Arch Otolaryngol Head Neck Surg. 125: 1365, 1999.-Kridel, R.W.H., Scott, B.A., Foda, H.M.T. The tongue-in-groove technique in septorhinoplasty: A ten year experience. Arch Facial Plast Surg. 1(4): 246, 1999.-Foda HMT: Mersiline Mesh in Premaxillary Augmentation. Aesthetic Plastic Surgery; 29: 169-173, 2005
The Deviated NoseDr. Hossam Foda (Egypt)
The deviated nose presents an esthetic as well as a functional problem that can be difficult to treat. The deviated nasal septum is a major contributing factor in the crooked nose deformity; accordingly, a successful correction of the deviated nose usually requires a combined septorhinoplastic procedure. The external approach, beside giving a panoramic view of the external bonycartilaginous framework of the nose, it also allows direct visualization of the dorsal and caudal septum. This direct exposure allows for accurate assessment of the often complex pathologic condition thus greatly enhancing the possibility of a successful outcome. This study was conducted on 800 patients seeking rhinoplasty to correct external nasal deviations; 71 percent of them suffered of variable degrees of nasal obstruction. Septal surgery was necessary in 736 (92%) patients, not only to improve breathing but to achieve a straight symmetric external nose as well. A graduated surgical approach was adopted to allow correction of the dorsal and caudal deviations of the nasal septum without weakening its structural support to the nasal dorsum or nasal tip. The approach depended on full mobilization of deviated cartilage, followed by straightening of the cartilage and its fixation in the corrected position by using

88
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
bony splinting grafts through an external rhinoplasty approach. References:-Foda HMT: External Rhinoplasty: A critical analysis of 500 cases. Journal of Laryngology & Otology 117:473-77, 2003-Foda HMT, Bassyouni K: Rhinoplasty in the unilateral cleft lip nasal deformity. Journal of Laryngology & Otology 114: 345-350, 2000.-Foda HMT: The role of septal surgery in management of the deviated nose. Plast Reconstr Surg. 115(2):406-15, 2005-Foda HMT: The crooked nose: Correction of the dorsal and caudal septum deviations. HNO Journal, 58:889-906, 2010
Revision RhinoplastyDr. Hossam Foda (Egypt)
Operating on a patient who had multiple previous rhinoplasties represents the ultimate challenge for any rhinoplastic surgeon. The aim of this study was to evaluate the functional and aesthetic problems involving the tip lobule in revision rhinoplasty.The study included a retrospective review of 1000 cases presenting for revision rhinoplasty. On analysis of patients’ problems; Functionally; 68% suffered of nasal obstruction which was mainly due to septal deviations and nasal valve problems. Aesthetically; commonest deformities of the upper two-thirds of the nose included; pollybeak (64%), dorsal irregularities (54%), dorsal saddle (44%), and open roof deformity (42%), while the deformities of lower third included; depressed tip (68%), tip contour irregularities (60%), and overrotated tip (42%). Nasal grafting was necessary in all cases; usually more than one type of graft was used in each case. Postoperatively; 79% of the patients, with preoperative nasal obstruction, reported improved breathing, 82% were satisfied with their aesthetic result, and only 18% requested further revision to correct minor deformities.Methods of prevention and treatment of such deformities will be thoroughly discussedRefrences:-Foda HMT: The Caudal Septum Replacement Graft. Archives of Facial Plastic Surgery Journal; 10(3):152-157, 2008-Foda HMT: Mersiline Mesh in Premaxillary Augmentation. Aesthetic Plastic Surgery; 29: 169-173, 2005-Foda HMT: Rhinoplasty for the multiply revised nose. Am J Otolaryngol. 26(1):28-34, 2005-Foda HMT: External Rhinoplasty: A critical analysis of 500 cases. Journal of

89
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Laryngology & Otology 117:473-77, 2003-Foda HMT: The role of septal surgery in management of the deviated nose. Plast Reconstr Surg. 115(2):406-15, 2005-Foda HMT: The crooked nose: Correction of the dorsal and caudal septum deviations. HNO Journal, 58:889-906, 2010 -Foda HMT. The one-stage rhinoplasty septal perforation repair. J Laryngol Otol. 1999; 113: 728-733-Foda HMT, Magdy EA: “Combining Rhinoplasty with Septal Perforation Repair” Facial Plastic Surgery Journal; 24(4):281-8, 2006
Endoscopic SPG Block: A New None- Invasive Technique Dr. Mohannad Al-Qudah (Jordan)
Jordan Experience in Cadaveric liver Transplantation, limited But Optimistic Dr. Khalid Ajarmeh (Jordan)
Jordan experience in cadaveric liver transplantation, limited but optimisticCadaverous liver donation is an excellent medical option offered by transplant centers to treat end stage liver disease (ESLD) patients.Although it is well adapted and widely used procedure worldwide but still limited in Arabic countriesIn Jordan, in contrary to living liver donation, it is very limited in number (five cases) since 2009 and this mainly due to psycho-social and cultural background.In this talk I will analyze these performed 5 cases regarding the indications, surgical technique, difficulties, complications and mortality trying to conclude the main reasons beyond this shortage of cadaverous liver donation and how to improve it in the future
Saudi Arabia Experience in Cadaveric liver Transplantation

90
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Dr. Hamad Bahili (KSA)
Comparison Between Cadaveric and living Donor liver Transplantation Dr. Aiman Obaid (Jordan)
Living donor liver transplantation (LDLT) has appeared as an excellent alternative to deceased donor liver transplantation (DDLT), since the number of patients waiting for liver transplantation (LT) has been markedly increased. On the other hand, whether it can realize operative outcomes similar to those achieved with DDLT for adult patients still detabale Literature Review was performed to compare the operative outcomes of LDLT and DDLT recipients In comparison with DDLT, LDLT was associated with a significantly longer DRO and a shorter CIT, biliary complications, vascular complications and retransplantation occurs more often for LDLT recipients living donation is not necessarily superior over deceased donation in LT
Obstacles Facing Cadaveric liver Transplantation Program in Jordan Dr. Sameer Smadi (Jordan)Obstacles facing cadaveric liver transplantation program in JordanS. Smadi, K. Ajarmeh T. mnaizel, R. Jarrah, A. Abadi, H. Shnikat, L. Shobaki, S. Al-Qusous, A. Edwan, M. Ghatashah S. Egzzawie, , A.Faori, A. Obeidat, H. Gharaybeh, G. Dhayat, A. Ziadin,A. Zoubi
� Organ transplantation is one of the greatest achievements of modern surgery, it is no longer experimental. Around 21,000 transplants /year (UNOS) and around 96,000 waitingJordan was the first country in Arab world to establish transplantation lawalso it was the first country in the region to start renal transplantation on 1972 by Royal medical services. The total number of patients with renal failure increase annually by 15-20%. The mortality rate from renal failure is about 5-10% Every patient cost about 11 thousands JD every year (without counting the drugs cost, shunt procedures and admission to hospital). Renal Transplantation cost about 17 thousand JD in the first year, this cost drop to 6 thousand JD in the second year then it become about three to five thousands yearly after that. The immediate success rate of renal transplantation is 90% from live donors and 80% from cadavers.Cadaveric organ transplantation was performed only in 6 donors during the last 10 years in Jordan comparing to 210 living donor liver transplantation

91
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Why cadaver organ transplantation is still immature and retarded in Jordan?What obstacles the program face? And how can we overcome those problems?
Saudi Arabia Efforts in Encouraging Cadaveric liver TransplantationDr. Hamad Bahili (KSA)
Jordan Efforts in Encouraging Cadaveric liver Transplantation Dr. Abdelhadi Braizat (Jordan)Building up a Deceased Donor Organ Transplant Program:Challenges & Solutions Abdel-Hadi Breizat MD; Ph.DDirector of Jordanian Center for Organ Transplantation Directorate; Amman, Jordan
In Jordan law for cornea donation issuedin the year 1956. Human organ transplantation started in the year 1972. Legislationfor organ donation and transplantation from both living and deceased donor established in the year 1977. Country has good infrastructures and well trained human recourses wherefirst in the region heart transplant performed in 1985, there is also a fair governmental financial support to the transplantation services. Nevertheless transplantation activity depending mainly on the living donation (99%) and the available organs cover only about (5%) of the needs, so activation and build up a deceased donor transplantation program became a national task.In year 2010thegovernment established a new institution which had been activated in 2012 to take over all the transplantation activity in the country. The initial few people and the leader (champions) who agreed to start working on transplantation program experienced much excitement, airiness, frustration, absolute depression and continuous rejection. Resistance came from many quarters and was prevalent in large organizations and it was

92
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
obvious among individual physicians. The champions did not gave up and demonstrated leadingship roll which supported by high rank officials and they continue creating favorable social, legal, cultural environments for the success of a transplant program, building national, regional and international relationships to help in acquiring and training all the personal who are responsible for providing crucial support to the program, involving and using the mass media continuously.Finally the outline of the program was drawn and the instructions, general rules and guidelines were issued and put together in a Directory (Manual) for official use in April 2015.After that there was a report of eight cases of potential brain death donors, with conformation of the diagnosis in six of them, and in one case there was an organs retrieval and allocation according to the adopted rules of priorityin the national waiting list and this was the first case in the country where a donated organ transferred from donating hospital to anotherone. In addition the numberof transplant operations increased by 26% in 2015 of that in 2014. A major challenge was also the acceptance of the new regulations by major institutions and the pressure they put to impose themselves as a leading forces with the attempt of alienation theothers.But with education, practice and leadership the barriers could be overcome.
Islet Cell Transplantation Dr. Ali Dabous (Jordan)
Despite modern medical breakthroughs, diabetes mellitus is a worldwide leading cause of morbidity and mortality. Definitive surgical treatment of diabetes mellitus was established with the advent and refinement of clinical pancreas transplantation in the 1960s. During the following decades, critical discoveries involving islet isolation and engraftment took place.Islet transplantation is a well-established therapeutic treatment for a subset of patients with complicated type I diabetes mellitus. Prior to the Edmonton Protocol, only 9% of the 267 islet transplant recipients since 1999 were insulin independent for 1 year. In 2000, the Edmonton group reported the achievement of insulin independence in seven consecutive patients, which in a collaborative team effort propagated expansion of clinical islet transplan¬tation centers worldwide in an effort to ameliorate the consequences of this disease. To date, clinical islet transplantation

93
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
has established improved success with insulin independence rates up to 5 years post-transplant with minimal complications. In spite of marked clinical success, donor availability and selection, engraftment, and side effects of immunosuppression remain as existing obstacles to be addressed to further improve this therapy. With ongoing experimental and clini¬cal studies, islet transplantation continues to be an exciting and attractive therapy to treat type I diabetes mellitus with the prospect of shifting from a treatment for some to a cure for all.In the other hand. Chronic pancreatitis is a progressive inflammatory disease causing irreversible structural damage to the pancreatic parenchyma. In severe cases, the endocrine function is also impaired. Surgical resection of the pancreas is considered the final option in the treatment of chronic pancreatitis. Extensive pancreatic resection of >70% of the pancreas may cause diabetes. The addition of an islet autotransplant offers the possibility of postoperative glucose control.In this presentation I will review the recent advances and future challenges of Islet cells transplantation.
Endovascular Treatment of Ruptured Aortic Aneurysms: Where is the Evidence? Dr. Jamal Hoballah (Lebanon)
Ruptured abdominal aortic aneurysms RAAA continue to be among the most challenging surgical emergencies. During the last three decades, the perioperative mortality of open elective AAA replacement has dropped to 3-5%. However, the mortality rates of emergency open repair of RAAA remained very high ranging from 40-50%, despite the advances in modern vascular surgery. With the introduction of endovascular AAA repair (EVAR) and its utilization in treating RAAA, lower mortality rates are being reported. It is unclear however whether the lower mortality rates are due to a selection bias or the new technology. The available evidence will be presented.
Carotid Arterial Disease and Coronary Artery Disease: What is the Best Approach Dr. Munier Nazzal ( USA)
Fluoroscopic Guided Thrombo-Embolectomy for Acute limb Ischemia: a Valuable Technique Dr. Jamal Hoballah (Lebanon)
Acute limb ischemia is a complex pathology that requires prompt intervention to prevent limb loss and decrease morbidity and mortality. Thromboembolectomy continues to be a main part of the treatment of acute limb ischemia. Traditionally,

94
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
thromboembolectomy is performed using a blind technique. The introduction of endovascular technology into the armamentarium of the vascular surgeon, has allowed the incorporation of fluoroscopy and endovascular skills to guide embolectomy and achieve better and safer thrombus removal. The value and technical aspect of fluoroscopic guided embolectomy will be described.
Vascular Shunts for Portal Decompression Dr. Mamoun AlBasheer (Jordan)
Fenestrated and Branched GraftsDr Munier Nazzal (USA)
Difficult Case PresentationsDr. Osama Hirzallah (Jordan)
laparoscopic Cholecystectomy Exposing the Inner layer of the Subserosal (SS-Inner) layer of the Gallbladder Can Fill the Gap of the Shortness of the Critical View of Safety. Dr. Goro Honda (Japan)Goro Honda, MD, PhD, FACSDept. of Surgery, Tokyo Metropolitan Cancer and Infectious Diseases Center Komagome Hospital, Tokyo, Japan
During laparoscopic cholecystectomy (LC), misidentification of the cystic duct, which causes major bile duct injuries, can result from wrong or incomplete dissection of Calot’s triangle. Therefore, the critical view of

95
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
safety (CVS) has been accepted as a safe method for gaining a sufficient view of Calot’s triangle before transecting the cystic duct. However, bile duct injury can occur by a wrong approach to a CVS, even in cases without aberrant anatomy of the bile duct. Additionally, in cases of badly inflamed gallbladders, it is often hard to achieve a CVS, because Calot’s triangle is often solid and cannot be expanded. As for landmarks to initiate LC safely, only superficial structures, for example, Rouviére’s sulcus, the base of segment 4, and the sentinel node, have been proposed in previous reports. However, likening LC to mountain climbing, with only these proposals including CVS, it is a kind of guidebook that describes only mountain views from the base (i.e. superficial structures) and near the top (i.e. CVS), but does not describe any route of the climb.We have proposed a standardized procedure which proceed identifying a particular layer of the gallbladder wall as a landmark. Histologically, the subserosal (SS) layer of the gallbladder wall can be divided into an inner (SS-Inner) layer, which consists of vasculature and abundant fibrous tissue, and an outer (SS-Outer) layer, which consists of fat tissue and fibrous tissue. By cutting the serosa and then ablating most of the fat tissue, namely, the SS-Outer layer, around the gallbladder, the SS-Inner layer, the surface of which is shiny and through which a reticulated vascular structure can be seen, is exposed. By this approach, other structures around the gallbladder is not exposed, so that it can be avoided injuring them.Furthermore, because we noticed most of aberrant hepatic ducts is a right posterior hepatic duct that ran from the right posterior section linearly toward the common hepatic ducts, common bile duct, cystic duct or cystic body, passing on the caudal side of the right portal vein in Rouviére’s sulcus, we have investigated whether such hepatic duct existed or not in preoperative images in every cases.We have safely performed LC, using our standardized preoperative evaluation and operative procedure, for many cases with cholecystitis with highly inflamed gallbladders. The standardized procedure, in which gallbladder dissection proceeds exposing the SS-Inner layer in the

96
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
gallbladder wall as a route of the climb, should become the universal standard of LC.
laparoscopic Complete Mesocolic Excision (CME) for Right Colon Cancer: Evidence and TechniqueDr. Ayman Agha (Germany)
Although the impact of complete mesocolic excision (CME) on overall as well as disease-free survival in patients with adenocarcinoma of the right hemicolon is still a matter of debate, CME becomes more and more standard procedure for oncologic right hemicolectomy due to the higher lymph node resection rate. This procedure can be performed safely by the laparoscopic approach. Nevertheless, there are some technical specialities and difficulties that have to be taken into account. Knowing the technical tricks and ‘classical’ pitfalls plays a pivotal role for save and proper surgery. A consistent training program with experienced laparoscopic surgeons may help to avoid or minimize intraoperative as well as postoperative complications during the learning curve.
laparoscopic Transabdominal lateral Adrenalectomy;Wa’el AlNa’ssan, MD, FACS. Consultant General, Laparoscopic and Bariatric Surgeon Head of Laparoscopic and Bariatric Unit.King Hussein Medical Center
Objective: To evaluate our experience in laparoscopic transabdominal lateral Adrenalectomy for functioning and nonfunctioning tumors regarding, tumor size, operative time, blood loss, conversion rate, hospital stay, and complications.Methods: This is a retrospective study conducted at King Hussein Medical Center between Jan 2010 and Jan 2016. Transabdominal lateral Adrenalectomy was done for 103 patients by the same team. Time of the procedure from starting the first incision tell closure of the last incision was recorded. The blood loss was measured. Average hospital stay was recorded. Complications during surgery and during hospitalization were identified and managed.Results: Patients were 40 males and 63 females, average size of the tumors were (4.5 cm) between (1.5-6 cm), average operative time was (65 min) between (40 – 100 min), conversion rate was zero, estimated blood loss was (40 ml), between ( 10-100 ml), average hospital stay was (1.7days) between ( 1-2 days), and the main complications during surgery were bleeding, and postoperatively were atelectasis and pain mainly shoulder pain. Conclusion: Laparoscopic transabdominal lateral Adrenalectomy

97
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
is optimal and safe operating technique associated with few complications and very law conversion rate, with best patient outcome.This procedure now is the gold standard technique for Adrenalectomy in the world and at our institute.
Algorithm of Management of leak after Sleeve GastrectomyAhmad Bashir, MD, FACS, FASMBS
Laparoscopic Sleeve Gastrectomy (LSG) is the most frequent bariatric procedure performed worldwide. Leak after LSG is one of the most feared complications by surgeons performing this procedure. This talk presents a literature review of the different methods of managing such a complication. It will also include a combined algorithm of best methods according to nature of leak.
laparoscopic Splenectomy for Massive Splenomegally: Technical DetailsDr. Osama Hamed(Jordan)Video Laparoscopic Splenectomy for Massive Splenomegaly in Hematology/Oncology Patients: Technical DetailsOsama H. Hamed, MD, FACSDepartment of Surgery, Arab Medical Center
Background: Laparoscopic Splenectomy was introduced in early 1990’s, it has been associated with lower morbidity and mortality compared to open splenectomy. Despite the wide acceptance for this approach for normal size spleen, laparoscopic splenectomy for massive splenomegaly represents a real challenge for the surgical team. In this video we describe our experience with laparoscopic splenectomy for massive splenomegaly (>20cm in craniocudal measurement) and provide some technical details of the procedure. Methods: 9 patients with massive splenomegaly Secondary to Hematology/Oncology disorders underwent Laparoscopic splenectomy at King Hussein Cancer Center over the last 3 years.Results: 4 patient had splenic marginal zone lymphoma, 2 patients had hairy cell leukemia and 3 patients had lymphoma with hypersplenism.. We had conversion in 1 patient due to sever adhesions in the left Upper quadrant from previous radiation and splenic artery embolization. Three patients had post op complications ( one left portal vein thrombosis, one CNC hemorrhage due to sever thrombocytopenia and one patient had post op heart attack and pneumonia).Conclusions: Laparoscopic splenectomy for massive splenomegaly in hematology/oncology patients is technically challenging, and carries a significant morbidity due to late referral. In this video we

98
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
provide our experience and some technical details of the procedure.
laparoscopic Adrenalectomy for large Tumors: Trans-or Retroperitoneal? Dr. Ayman Agha (Germany)Technical Aspects of Laparoscopic Total Mesocolic Excision for Rectal Cancer
Total mesorectal excision (TME) has shown to reduce the risk of local recurrence in patients with rectal cancer. Although the overall survival rate is not altered the surgical quality of TME defined by the MERCURY score plays a pivotal role regarding the local recurrence rate and therefore quality of life. Several studies could show that laparoscopic rectal resection is not inferior to the open approach regarding the quality of surgery and the clinical and oncological outcome. Thus, laparoscopic rectal resection may become the new standard of care. Nervertheless, there is a significant learning curve to obtain a high quality of surgical outcome and especially of TME. The technical differences and specialities in comparison to the open approach have to be considered for the nerve sparing laparoscopic TME with proper resection margins and intact mesorectal plane.
Application of Minimally Invasive Surgery for Benign and Malignant Pancreatic Diseases Dr. Goro Honda (Japan)Application of Minimally invasive surgery for benign and malignant pancreatic diseasesGoro Honda, MD, PhD, FACSDept. of Surgery, Tokyo Metropolitan Cancer and Infectious Diseases Center Komagome Hospital, Tokyo, Japan
In Japan, laparoscopic pancreatic surgeries have been performed at limited high-volume center. In this April, application of laparoscopic pancreatic surgeries covered by national insurance was extended by the government. Pancreaticoduodenectomy without extended lymphadenectomy

99
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
applied to borderline malignant lesion (IPMN, MCN, PNTE, etc.) and non-invasive ampulla or lower bile duct carcinoma became laparoscopically available under national insurance, as well as distal pancreatectomy for pancreatic ductal carcinoma, so called Radical antegrade modular pancreatosplenectomy (RAMPS). These applications of national insurance are reasonable, because laparoscopic pancreaticoduodenectomy takes long time even without extended lymphadenectomy, while laparoscopic RAMPS does not take so long time and makes meticulous surgery available in laparoscopic magnified view. Our standardized procedures for laparoscopic pancreaticoduodenectomy and laparoscopic distal pancreatectomy for pancreatic cancer are presented.
Cystic Neoplasms of the Pancreas, the RMS Experience Dr. Ashraf Faouri (Jordan)Pancreatic cystic lesions: Pitfalls in diagnosis and management.Ashraf F. Al-Faouri, MD, MRCS, FACSSenior Specialist in General & Hepatobiliopancreatic surgery and Liver Transplantation, King Hussein Medical Center, Amman, Jordan
Background: Pancreatic cystic lesions are commonly found on cross-sectional imaging with an estimated incidence of 1-2.4/100 individuals/ year. While most of these lesions are asymptomatic, benign or non-neoplastic pseudocysts, the minority which represents true neoplastic cysts impose diagnostic and management challenge.Aim: to present the clinical, radiological and pathological data of 31 patients with pancreatic cystic lesions managed at King Hussein Medical Center over 15 years period. We will also emphasize pitfalls in diagnosis and management. Material & Method: Our pathology department database was searched for pancreatic cystic lesion, pancreatic neoplasm, pancreatic pseudocyst, mucinous cystadenoma, serous cystadenoma, pseudopapillary tumor and IPMN. The medical files and the PACS (picture archiving and communication system) were reviewed. 31 patients with definite diagnosis of pancreatic cystic neoplasms and pseudocysts were identified for analysis. Results: 31 patients were included in the final analysis with 18 males. The mean age was 45.6±17.7 (range 15-78). Pancreatic pseudocysts were the most common pathology occurring in 15 patients (48.4%). Five patients (16.1%) had mucinous cystic neoplasms, 3 of them were malignant. Three patients had IPMN (9.7%) with invasive carcinoma found in 2 of them. Two patients had serous cystadenoma and two had solid pseudopapillary tumors (6.5% each). The remaining 4 patients (12.9%) had benign simple epithelial cyst. We have found major pitfalls in management of some of these patients that will be presented in the conference.

100
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Conclusion: the rarity of cystic pancreatic neoplasms and the wide differential diagnosis impose difficulty in diagnosis and management. These patients should be referred to experienced pancreatic surgeons with special interest in their management.
Fertility Preservation in Gynecological Malignancy Patients Dr. Kamil Fram (Jordan)
Rupture Uterus in Pregnancy and labor Dr. Mazen El-Zibdeh (Jordan)Senior consultant Ob.Gyn Gardens Hospital Amman
Rupture uterus in pregnancy is rare and often with high catastrophic complications and high fetal and maternal morbidity. Several factors are well recognized to increase the risk of rupture. Initial significant symptoms are non specific and sometimes delay the definitive therapy. Risk factors are well recognized and in modern obstetric practice the incidence of uterine rupture is low .Normal un scared uterus is least susceptible to rupture but grand multiparity , neglected labor malpresentation , instrumental delivery and the uterotonics over stimulation are among the predisposing factors.As primary cesarean section rates are increasing world wide the risk of uterine rupture in subsequent pregnancies is increasing. Women undergoing trial of labor have two to three times risk of uterine rupture than in women who have elective cesarean section. The effect of previous c .section on the rate of subsequent pregnancy related rupture will be discussed. In modern practice rupture uterus should be prevented by minimizing the risk factors; mainly uterine scar and increasing inter delivery interval, and improving labor facilities .Delivery after previous c section or the scared uterus should be in a tertiary centers where prompt initiation of management can be done successfully.
New Approach in Surgical Management of Pelvic Organ Prolapse Dr. Abdallah Fayyad (UK)
Hysteroscopy Update Dr. Mohammad Al Qudah (Jordan)
Hysterectomy in the 21st Century, Different Approach and Different Challenges Dr. Isam Latayfeh (Jordan)

101
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Planas Mammary Reduction Technique Dr. Gabriel Planas (Spain)
PLANAS REDUCTION MAMMOPLASTYAesthetic Plastic Surgery Nº 4, 1988.This technique is a modification of Strömbeck’s technique, based in a superior pedicle to transport the nipple-areola complex to its new position, and an inferior glandular-fat one to fill the breast.The marking of the patient, should be always measured in a standing up position, where the length of the submammary fold incision is the key for the rest of the measurements.We first deepitelize the area around the areola, with the Schwartzman’s maneuver, keel incision as recommended by Dr. Pitanguy; then, the upper flap is widely undermined to the level of the second rib, deepitelization of the inferior pedicle, the nipple-areola complex is mobilized, the inferior pedicle is reduced to obtain the desired volume and fixed to the fascia of major pectoral muscle, at the level of the second rib.No drains are used, and a light compression is placed overnight.
Tips and Tricks in Inferior Pedicle Breast Reduction Dr. Hisham El-Minawi (Egypt)
Immediate Single Stage Breast Reconstruction Using Dermal Barrier Flap Dr. Bishara Atiyeh (Lebanon)
Augmentation Mastopexy with Implants Dr. Gabriel Planas (Spain)AUGMENTATION MASTOPEXY WITH IMPLANTS
In this presentation we evaluate our different ways to approach mastopexy with implants, depending on the type of ptosis the patient has.Grade I or pseudoptosis, where the NAC is over the submammary fold.Grade II, where the NAC is at the level of the submammary fold.Grade III, where NAC is below the submammary fold, between 23 and 28 cm of the sternal notch.Grade IV, where the NAC is lower than 28 cm of the sternal notch. In Grade I, we will use only implants, in grade II, a periareolar pexy plus implants, in grade III a vertical pexy and implants are needed; and in cases of grade IV we will need an inverted T elevation with implants.

102
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •
Fat injection in Breast Remodeling Dr. Hisham El-Minawi (Egypt)Therapeutic Reduction Mammoplasty (TRM)Dr. Bishara Atiyeh (Lebanon)

103
American College of SurgeonsJordan Chapter
• ABSTRA
CTS •



106
• SESSION
S •
• Parallel session:
I- ACS General Surgery Review CourseFirst time in Jordan
Date: Saturday and Sunday May 7-8, 2016Location: Le Royal Hotel Amman JordanSpeakers: Highly Qualified International, Regional & National Expert SpeakersFees: 70 JD *Spots are limited & will be filled on first come basisTargeted Audience: Senior Surgery Residents, New Surgeons Preparing for the Surgery Board, and Experienced Surgeons for CME.Topics : Abdominal, Alimentary, Breast, Endocrine, Vascular, Trauma,Critical Care, Perioperative Care, Pharmacology.
The most comprehensive General Surgery Review Course
For Registration or Questions please contact Conference Secretariat [email protected]

107
• Parallel sessions:
II- Advanced Trauma life Support Course ATlS
Date: Monday, Tuesday and Wednesday May 3-5, 2016Location: National Emergency Medical Services Education Centre (NEMSEC)Course Chair & Director: Mahmoud Odat, MD, FACSFees: This course will be sponsored by the Jordan Chapter of the American College of Surgeons
Instructors:Dr. Ahmad Uraiqat, Dr. Ahmad Zarour, Dr. Oday Al Sayegh, Maimonah Atiat, Dr. Omar Abu Zytoon.Standby Dr. Ahmad Shalaldah
Nomination will be accepted from Residency Program Directors and Chairman of the Department of Surgery made directly to:Osama Hamed, MD, FACS, Secretary of ACS Jordan Chapter [email protected] or Conference Secretariat [email protected].
• SESSION
S •

108
American College of SurgeonsJordan Chapter
• Parallel sessions:
III- The American College of Surgeons Surgical Competition “Surgical Jeopardy”
First time in Jordan & first time outside the US
Date: Friday May 6th, 2016Location: Le Royal Hotel Amman Jordan
Jordanian Residency Programs are invited to nominate teams from 2 residents to participate in the American College of Surgeons Surgical Competition “ Surgical Jeopardy”, Surgical Jeopardy allows teams of residents to showcase their surgical knowledge. There will be valuable prizes for the winning teamNomination will be accepted from General Surgery Residency Programs and Chairman of Departments of surgery made directly to:Osama H. Hamed, MD, FACS, Secretary of ACS Jordan Chapter [email protected] Conference Secretariat [email protected].
• SESSION
S •

109
American College of SurgeonsJordan Chapter
• Parallel sessions:
IV- Trauma Evaluation & Management Course TEAM for Medical Students
First time in Jordan
Date: Saturday and Sunday May 7-8, 2016Location: Le Royal Hotel Amman JordanSpeakers: Highly Qualified International, Regional & National Experts ATLS Faculty
TEAM 1st day Chairs: Dr. Ahmad Zarour, Mahmoud OdatInstructors: Dr. Mamoun Gariouti, Dr. Oday Al Sayegh,Dr. Rubaa, Maimonah Atiat, Dr. Abdallah Khwaldah
TEAM 2nd day Chairs: Dr. Ahmad Uraiqat, Mahmoud OdatInstructors: Dr. Jehad Al Ajlouni, Dr. Ahmad Jabr,Dr. Fadi Al Rousan, Dr. Abdelhamid Al Abadi
*Spots are limited & will be filled on first come basisTrauma Evaluation and Management® (TEAM®) introduces the concepts of trauma assessment and management to medical students during their clinical years.The core content is adapted from the American College of Surgeons (ACS) Advanced Trauma Life Support® (ATLS®) course. Developed by the ATLS Committee of the ACS Committee on Trauma, TEAM is an expanded version of the ATLS “Initial Assessment and Management” lecture.For Registration or Questions please contact Conference Secretariat [email protected]
• SESSION
S •


111
American College of SurgeonsJordan Chapter
• FlOO
R MA
P •
Booth 1: Edifice Medical Solutions
Booth 2: Sadaf Medical
Booth 3: Convatec (Kawar Drugstore)
Booth 4,5: AstraZeneca
Booth 6: Pfizer
Booth 7: SADCO
Booths 8,9: SANOFI
Booths 10,11,12: Petra Drug Store (Ethicon)
Booth 13: Promedz
Booth 14: Fakhouri Medical Supplies
Booth 15: Arab Medical & Scientific Alliance (AMSA)
Booth 16: Jordan Medicare
Booths 17,18,19: Hikma Pharmaceuticals
Booths 20,21,22: Medtronic
Booth 23: Al-Wafi Group For Marketing & Int’l Trade Co. Ltd.
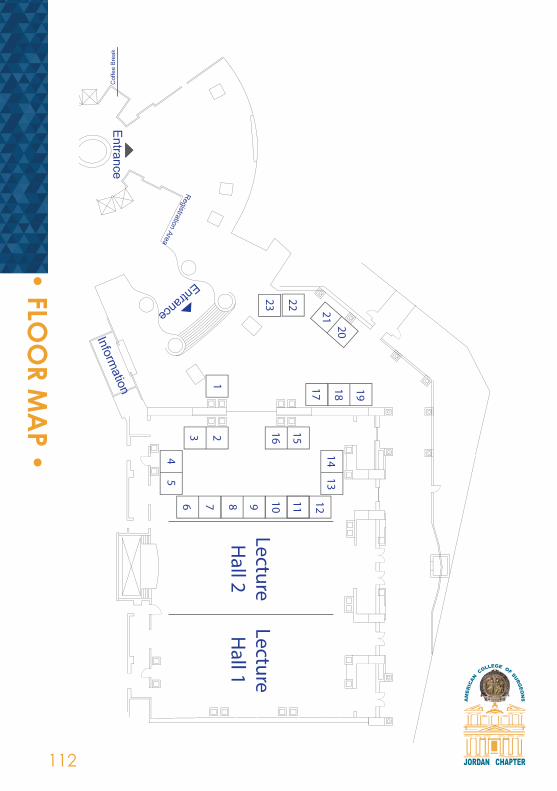
112
American College of SurgeonsJordan Chapter
• FlOO
R MA
P •
LectureH
all 1LectureH
all 21 17 18 19
1413
151623
12
2021
2223
111098764
5

113
American College of SurgeonsJordan Chapter
• SPON
SORS •
• DIAMOND/MAIN SPONSOR •
• PlATINUM SPONSOR •

114
American College of SurgeonsJordan Chapter
• SPON
SORS •
• GOlD SPONSOR •
• SIlVER SPONSOR •

115
American College of SurgeonsJordan Chapter
• SPON
SORS •
صـــــــــــــروحنصمم الحلول الطبيةلألجهزة والمستلزمات الطبية

116
American College of SurgeonsJordan Chapter
• SPON
SORS •
AL-WAFI DRUG STORE

117
• INFO JORDAN
Jordan is a land steeped in history. It has been home to some of mankind’s earliest settlements and villages, and relics of many of the world’s great civilizations can still be seen today. As the crossroads of the Middle East, the
lands of Jordan and Palestine have served as a strategic nexus connecting Asia, Africa and Europe. Thus, since the dawn of civilization, Jordan’s geography has given it an important role to play as a conduit for trade and communications, connecting east and west, north and south. Jordan continues to play this role today. Take an interactive tour through Jordan’s history starting from the Paleolithic Era, right up to modern day with our Interactive Historical Timeline.Jordan is located in the Middle East and borders Syria, Saudi Arabia, the Red Sea, Palestine, and Iraq. Covering some 89,342 sq.km, it is located at 31 00 N, 36 00 E.
• ABO
UT JORDA
N •

118
Mobile phonesDelegates are kindly requested to switch off their mobile phones during the sessions.
WeatherWeather avarage temperature in May
CurrencyOne Jordanian Dinar is equivalent to 1.4 USD.
Wifi available free on site
Hours of Sun Humidlty (%) Max. Temp (c) Min. Temp (c)
10 43 26 12
• GEN
ERAl IN
FORM
ATIO
N •
Conference venueLe Royal Hotel Amman
Registration Fees Registration Fees 70 JD, (Medical Students and Residents free registration).
RegistrationRegistration starts on 5th May,from 8:00 am to 17:00 pmand from 8:30 am to 16:00 pm daily thereafter.
Registration Fees Include• Congress bag.• Programme book• Opening ceremony and reception• Admission to the exhibition.• Meals.• Coffee breaks
Badges• The participants name badges serve as an admission pass to all scientific sessions, theexhibition and the congress area.
• Participants are kindly requested to keep their name badges displayed at all times during the congress.




Conference Secretariat:Tel.: +962 6 582 0738Fax: +962 6 582 0873Mobile: +962 799 193 733Email: [email protected] www.gec-jo.com
• CO
NTA
CT US •





























