Embed Size (px)
Citation preview
Uncertain but Determined Let’s talk about WHO, WHI and WHY
Peter van de Weijer MD PHD
The Netherlands
1
March
2005
Hongkong

CliniciansWome
n
© PHMvdW 2005
Health care for Women
Researchers
Not an issue for just one group
Policy makers
Healthcare industry
Health EducatorsEpidemiologists
Healthcare administrators
Nurses

Clinician Women
© PHMvdW 2005
Provide
Medical Practice
relationship
ongoing personal
Experience
Health care for Women
health care
Medical Knowledge , based on the best available evidence
• to understand and evaluate research findings• to apply “true” research evidence to clinical practice
The need to be taken care of
• tto communicate about evidence, risks and benefits

1960 Symptom relief – preservation of “youth”
© PHMvdW 2005
History
1970
1980
Unopposed estrogen - endometrial cancer
Prevention of osteoporosis ; coronary heart disease ; Alzheimer’s disease
Progestins eliminate risk endometrial cancer
1993 Women’s Health Initiative to evaluate putative protective effects of HT on chronic diseases of aging
National Institutes of Health 700 million dollar – public
funding

Women’s Health Initiative (WHI) Study Outline
Examination of long-term strategies for the prevention of morbidity and mortality in postmenopausal women.
The WHI program includes 4 clinical studiesmore than 100.000 women participating
1) Effects of PremPro® (0.625mg CEE/2.5mg MPA) on CHD
2) Effects of Premarin® (0.625 mg CEE) on CHD
3) Effects of a low-fat and high-fiber diet
4) Effects of vitamin D + calcium
To Understand and Evaluate Research Findings
CHD: Coronary Heart Disease
12-year duration
Women’s Health Initiative (WHI) Study Outline
To Understand and Evaluate Research Findings
Two large, randomized, placebo-controlled clinical trials planned duration 8.5 years.
Prempro® (0.625 mg CEE, 2.5 mg MPA) vs. placebo– 16,608 women– 50-79 years of age (mean age 63.2 years)
Premarin® (0.625 mg CEE) vs. placebo– 10,739 women with prior hysterectomy,– 50-79 years of age (mean age 63.6 years)
Outcomes
Primary outcome Coronary heart diseases (CHD)
non-fatal myocardial infarction and CHD death
Secondary outcome Stroke, Venous Thromboembolism, Colorectal Cancer,
Osteoporosis-related fractures, all-cause Mortality
Primary adverse outcome Invasive breast cancer

Fisher WA et al. Maturitas 2000 ; 37 : 1-14
© PHMvdW 2005
I. Study design and level of evidence
II. Results ; Absolute risks
IV. Population studied similar to your practice population
III. Time of initiation of therapy and duration
V. Decision analysis based on all health outcomes
To Understand and Evaluate Research Findings

Observation
Estimation
Hypothesis
TestRandomised double blind
placebo controlled
Test does not support hypothesis
Test does support hypothesis
revise
Observational studies
RCT
MWS
WHI
© PHMvdW 2005
Clinical research
HERS
NHS

Types of Studies Used in Investigating HT
Observational studies
Studies in defined groups of the population.
They observe factors determining and influencing the
frequency (incidence) and distribution of health-related
events.
Observed factors are instrumental in defining endpoints
for further randomised clinical studies.
Only RR > 3 are probably causational; RR: 1-2 attributable to bias
Nurses’ Health Study (NHS); Million Women Study
Types of Studies Used in Investigating HT
Randomised controlled trials
Studies on individuals
to evaluate the efficacy of HT in comparison with a control group (e.g. vs. placebo).
Women’s Health Initiative (WHI)
Heart and Estrogen/Progestogen Replacement Study (HERS)

Description of the levels of evidence
Level I properly randomized, controlled trial
Level II-1 well-designed controlled trial, no randomization
Level II-2 well-designed cohort or case-control analytic studypreferably from more than one centre or group
Level II-3 Multiple time series with or without the intervention (cross-sectional, uncontrolled investigational )
Level III Opinions of respected authorities that are based on clinical experience, reports from expert
committees
Report of the US Preventive Services Task Force. Guide to Cinician Preventive Services2nd edition Baltimore Williams & Wilkins 1996
Research findings
© PHMvdW 2005
FDA
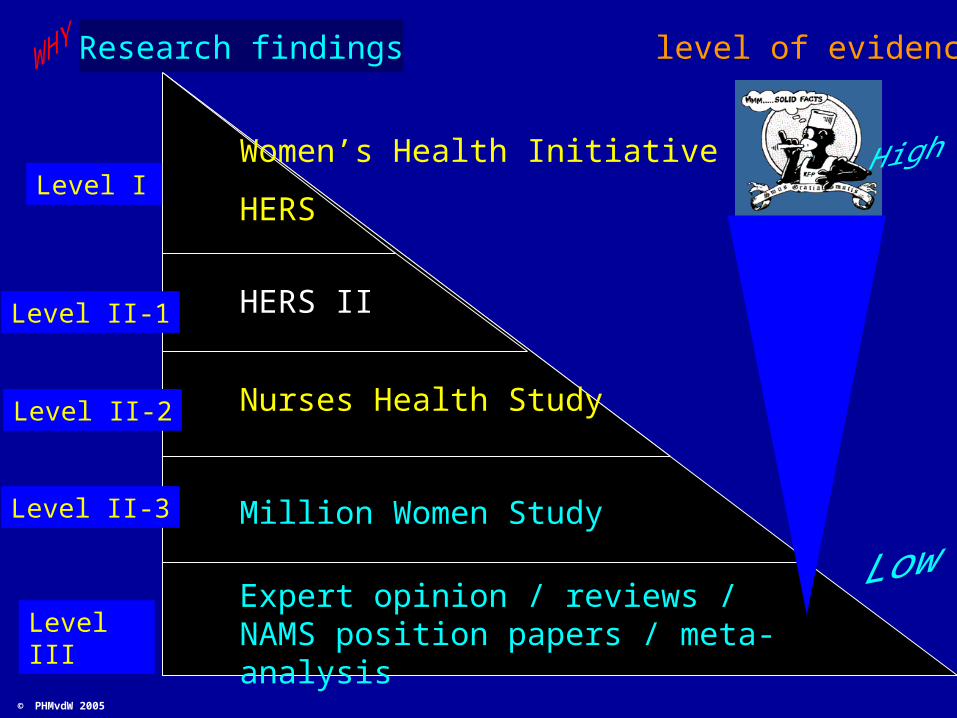
Level III
Women’s Health Initiative
HERS
Level II-2
Level II-3
Level II-1
Level I
Nurses Health Study
Million Women Study
Expert opinion / reviews / NAMS position papers / meta-analysis
HERS II
Research findings level of evidence
© PHMvdW 2005

Women’s Health Initiative (WHI) Results
To Understand and Evaluate Research Findings Level I
© PHMvdW 2005
Placebo CEE MPA RR 95% CI
Breastcancer 33 41 1.26 1.00-1.59 4 Chlebowski JAMA 2003;289:3243-53
CHD 33 39 1.24 1.00-1.54 3 Manson N Engl J Med 2003;349:523-9
Stroke 24 31 1.44 1.09-1.90 4 Rossouw JAMA 2002;288:321-333
Deep Ven Thr 13 26 2.11 1.58-2.82 9 Rossouw JAMA 2002
Coloncancer 16 10 0.63 0.43-0.92 -3 Rossouw JAMA 2002
Endom. Cancer 6.9 5.6 0.81 0.48-1.36 -0,7 Anderson JAMA 2003;290:1739-48
Ovarian Cancer 2.7 4.2 1.58 0.77-3.24 0,8 Anderson JAMA 2003
Hipfracture 16 11 0.67 0.47-0.96 -2,5 Cauley JAMA 2003;290:1729-38
Tot fractures 199 152 0.76 0.69-0.83 -23,5 Cauley JAMA 2003
Tot Mortality 53 52 0.98 0.82-1.18 -0,5 Rossouw JAMA 2002
Absolute riskN / 10000 /yr
Relative risk ReferenceCEE /MPA
extra 5 yrs risk
per 1000 women

Women’s Health Initiative (WHI) Results
To Understand and Evaluate Research Findings Level I
© PHMvdW 2005
Placebo CEE MPA
Breastcancer 33 41 4
CHD 33 39 3
Stroke 24 31 4
Deep Ven Thr 13 26 9
Coloncancer 16 10 -3
Endom. Cancer 6.9 5.6 -0,7Ovarian
Cancer 2.7 4.2 0,8
Hipfracture 16 11 -2,5
Tot fractures 199 152 -23,5
Tot Mortality 53 52 -0,5
Absolute riskN / 10000 /yr
CEE /MPAextra 5 yrs risk
per 1000 women
HT should not be started or continued for
Primary prevention of CHD
Secundary prevention of CHD
HT for the treatment of osteoporosis
will require balancing risks and benefits including
Risks and benefits of alternatives to HT

Women’s Health Initiative (WHI) Results
To Understand and Evaluate Research Findings Level I
© PHMvdW 2005
Placebo CEE MPA RR 95% CI
Breastcancer 33 26 0.77 0.59-1.01 -3.5 WHI Steering JAMA 2004;291:1701-12
CHD 54 49 0.91 0.75-1.12 -2,5 WHI Steering JAMA 2004
Stroke 32 44 1.39 1.10-1.77 6 WHI Steering JAMA 2004
Deep Ven Thr 21 28 1.33 0.99-1.79 3,5 WHI Steering JAMA 2004
Coloncancer 16 17 1.08 0.75-1.55 0.5 WHI Steering JAMA 2004
Endom. Cancer
Ovarian Cancer
Hipfracture 17 11 0.61 0.41-0.91 -3 WHI Steering JAMA 2004
Tot fractures 195 139 0.70 0.63-0.79 -28 WHI Steering JAMA 2004
Tot Mortality 78 81 1.04 0.88-1.22 1,5 WHI Steering JAMA 2004
Absolute riskN / 10000 /yr
Relative risk ReferenceCEE extra 5 yrs risk
per 1000 women

Women’s Health Initiative (WHI) Results
To Understand and Evaluate Research Findings Level I
© PHMvdW 2005
Placebo CEE MPA RR 95% CI
Breastcancer 33 26 0.77 0.59-1.01 -3.5 WHI Steering JAMA 2004;291:1701-12
CHD 54 49 0.91 0.75-1.12 -2,5 WHI Steering JAMA 2004
Stroke 32 44 1.39 1.10-1.77 6 WHI Steering JAMA 2004
Deep Ven Thr 21 28 1.33 0.99-1.79 3,5 WHI Steering JAMA 2004
Coloncancer 16 17 1.08 0.75-1.55 0.5 WHI Steering JAMA 2004
Endom. Cancer
Ovarian Cancer
Hipfracture 17 11 0.61 0.41-0.91 -3 WHI Steering JAMA 2004
Tot fractures 195 139 0.70 0.63-0.79 -28 WHI Steering JAMA 2004
Tot Mortality 78 81 1.04 0.88-1.22 1,5 WHI Steering JAMA 2004
Absolute riskN / 10000 /yr
Relative risk ReferenceCEE extra 5 yrs risk
per 1000 women
HT should not be started or continued for
Primary prevention of CHD
Secundary prevention of CHD
HT for the treatment of osteoporosis
will require balancing risks and benefits including
Risks and benefits of alternatives to HT
Low dose therapy less risk
for stroke and DVT

Fisher WA et al. Maturitas 2000 ; 37 : 1-14
© PHMvdW 2005
I. Study design and level of evidence
II. Results ; Absolute risks
To Understand and Evaluate Research Findings
Absolute risks are relevant for general practice

Risk factor Accounts for …percent
of breastcancer
ModifiableRisk factor ?
Age (increasing) 70% -80% No
Familial (multiple genetic/environmental factors)
15%-20% Possible
Herediatary Predisposition (single gene mutation)
5% - 10% No
BREAST CANCER
ACOG Bulletin Breastcancer Obstet Gynecol 2004: 104; 11-16
© PHMvdW 2005
Most of the recognized risk factors for breastcancer
are not modifiable

Risk factor Accounts for …percent
of breastcancer
ModifiableRisk factor ?
Age (increasing) 70% -80% No
Familial (multiple genetic/environmental factors)
15%-20% Possible
Herediatary Predisposition (single gene mutation)
5% - 10% No
BREAST CANCER
ACOG Bulletin Breastcancer Obstet Gynecol 2004: 104; 11-16© PHMvdW 2005
Risk factor Relative risk Modifiable ?
Age at menarche 14 yrs vs 11 yrs 1 : 1.3 No
Parity multiparous : nulliparous
1 : 1.3 possible
Age at first birth 20 yrs vs 30 yrs 1 : 1.5 possible
Age at menopause 42 yrs vs 52 yrs 1 : 2.0 possible
Body weight normal weight : obesity
1 : 1.5 yes
Serum lipids normal vs raised 1 : 1.6 yes
Antibiotic use never vs 1-50 days/life
1 : 1.5 yes
Alcohol consumption none vs ≥20 g daily 1 : 1.3 yes
Hormone Therapy none vs CEE/MPA/5yrs
1 : 1.3 yes
Physical Activity active vs non-active 1 : 1.2 yes
Fisher WA et al. Maturitas 2000 ; 37 : 1-14
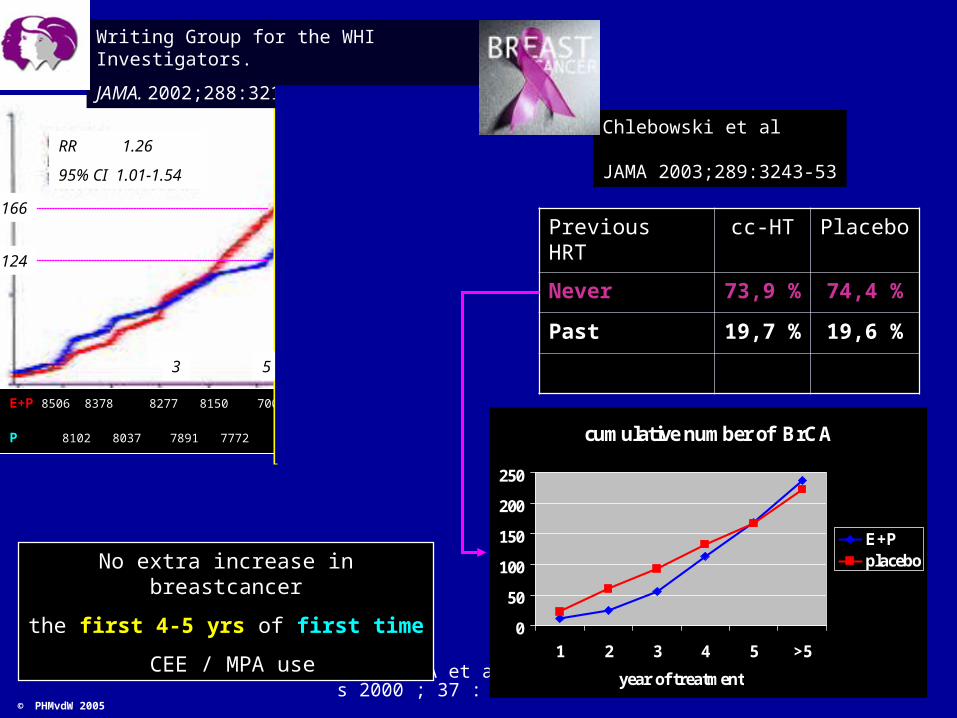
E+P 8506 8378 8277 8150 7000 4234 2064 801
P 8102 8037 7891 7772 6819 3922 1740 523
Writing Group for the WHI Investigators.
JAMA. 2002;288:321-33
Previous HRT cc-HT Placebo
Never 73,9 % 74,4 %
Past 19,7 % 19,6 %
RR 1.26
95% CI 1.01-1.54
53 yr
124
166
Chlebowski et al
JAMA 2003;289:3243-53
cumulative number of BrCA
0
50
100
150
200
250
1 2 3 4 5 >5
year of treatment
E+Pplacebo
No extra increase in breastcancer
the first 4-5 yrs of first time
CEE / MPA use
© PHMvdW 2005
Fisher WA et al. Maturitas 2000 ; 37 : 1-14
© PHMvdW 2005
Lesson
No extra increase in breastcancer
the first 4-5 yrs of first CEE / MPA use
started after the age of 50 years
Level I
Evidence
Time of initiation of treatmentDuration of therapy

Fisher WA et al. Maturitas 2000 ; 37 : 1-14
© PHMvdW 2005
I. Study design and level of evidence
II. Results ; Absolute risks
To Understand and Evaluate Research Findings
Absolute risks are relevant for general practice
Time of initiation of therapy and duration

Fisher WA et al. Maturitas 2000 ; 37 : 1-14
© PHMvdW 2005
I. Study design and level of evidence
II. Results , Absolute risks
III. Time of initiation of therapy and duration
“Study findings indicate that combined HT is associated with an increased
risk of breast cancer. Women considering HT should be counseled that
the absolute risk of breastcancer for any individual remains relatively low“
ACOG Breastcancer Obstet Gynecol 2004;104: 11-16
To Understand and Evaluate Research Findings

Fisher WA et al. Maturitas 2000 ; 37 : 1-14
© PHMvdW 2005
Applicability to general practice
I. Study design and level of evidence
II. Results; Absolute risks
IV. Population studied similar to your practice population
III. Time of initiation of therapy and duration
To Understand and Evaluate Research Findings

Women’s Health Initiative (WHI)Study Population
Mean age at recruitment: 63 years
Past or current smokers: 50%
Women treated for hypertension: 36-48%
Women on lipid lowering medications: 13-15%
BMI > 25: 70-79%
Women treated for diabetes: 4-8%

Fisher WA et al. Maturitas 2000 ; 37 : 1-14
© PHMvdW 2005
I. Study design and level of evidence
II. Results; Absolute risks
IV. Population studied similar to your practice population
III. Time of initiation of therapy and duration
V. Decision analysis based on all health outcomes
To Understand and Evaluate Research Findings
Fisher WA et al. Maturitas 2000 ; 37 : 1-14
© PHMvdW 2005
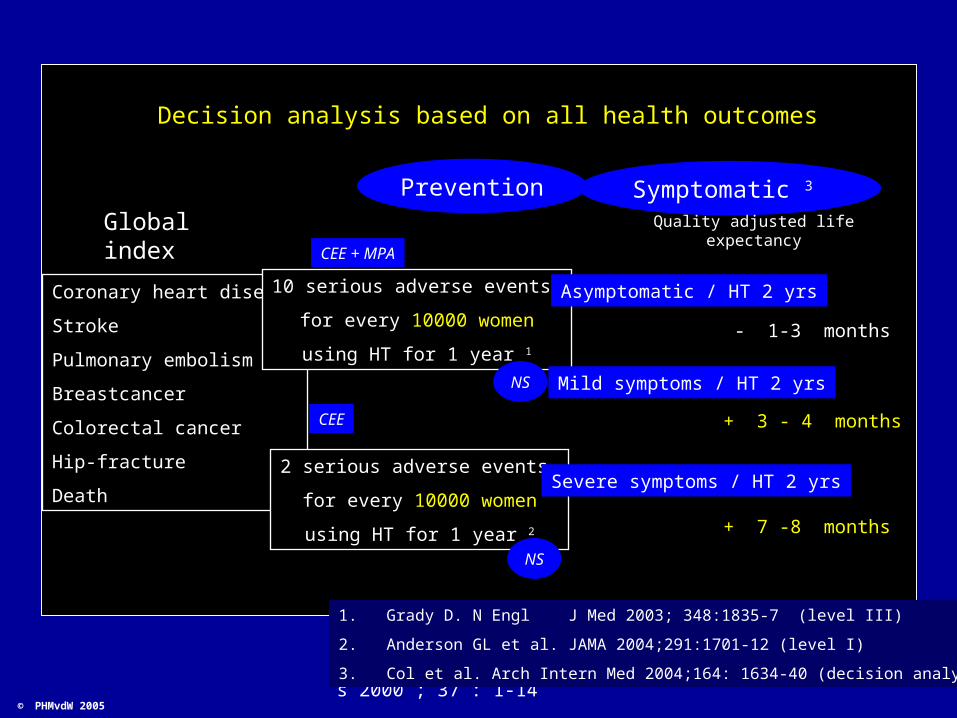
Decision analysis based on all health outcomes
Global index
Coronary heart disease
Stroke
Pulmonary embolism
Breastcancer
Colorectal cancer
Hip-fracture
Death
Prevention
CEE + MPA
CEE
10 serious adverse events
for every 10000 women
using HT for 1 year 1
2 serious adverse events
for every 10000 women
using HT for 1 year 2
NS
NS
1. Grady D. N Engl J Med 2003; 348:1835-7 (level III)
2. Anderson GL et al. JAMA 2004;291:1701-12 (level I)
3. Col et al. Arch Intern Med 2004;164: 1634-40 (decision analysis)
Symptomatic 3
Asymptomatic / HT 2 yrs
Quality adjusted life expectancy
Mild symptoms / HT 2 yrs
Severe symptoms / HT 2 yrs
- 1-3 months
+ 3 - 4 months
+ 7 -8 months
Clinician Women
© PHMvdW 2005
Health care for Women
Provide
Medical Practice
The need to be taken care of
relationship
ongoing personal
health care

45 yrs 50 55 yrs
Fertility
Menstrual cycle problems
Flushes / night sweats
Urogenital atrophy
OsteoporosisDiabetes CVD
Contraception
PMS
Pre
Arthritis
CarcinomaBreast Colon
Ovarian Cervical
Perimenopause Post
EyesightHearing
?
?
Climacteric Medicine
UterineBleeding
© PHMvdW 2004
Cognitivefunction
» Strength
Menopause
45 yrs 50 55 yrs
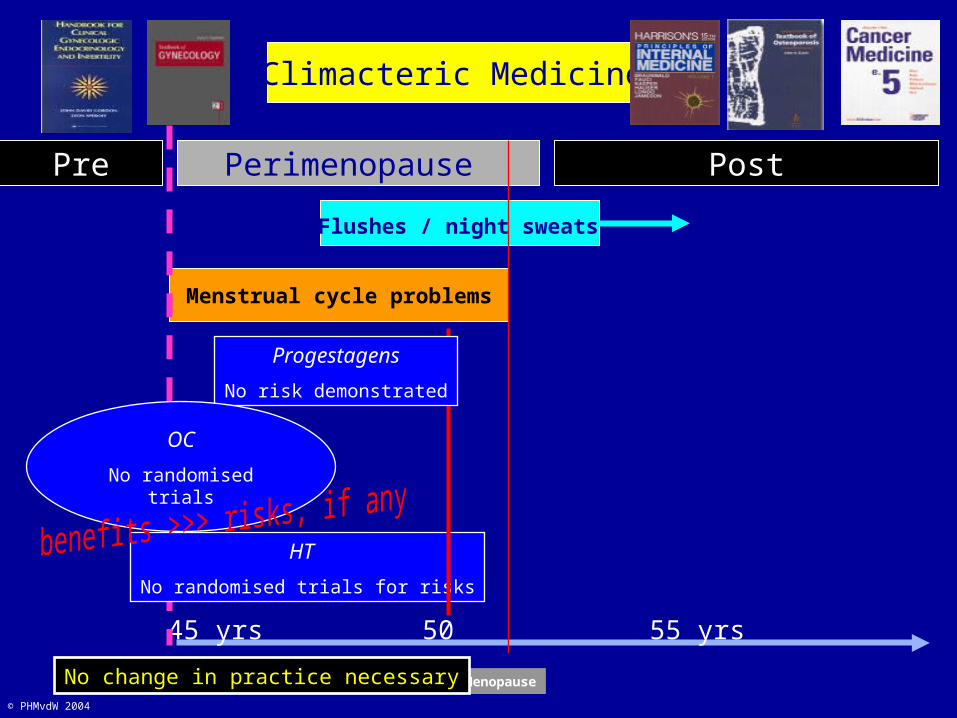
Menstrual cycle problems
Flushes / night sweats
Pre Perimenopause Post
Climacteric Medicine
© PHMvdW 2004
Menopause
HT
No randomised trials for risks
Progestagens
No risk demonstrated
OC
No randomised trials
No change in practice necessary

45 yrs 50 55 yrs
Flushes / night sweats
Pre Perimenopause Post
Climacteric Medicine
© PHMvdW 2004
Menopause
First 5 yrs HT use
No increase for Br Ca
QALY > Symptomatic
No change in practice necessary No change in practice necessary
45 yrs 50 55 yrs
Pre Perimenopause Post
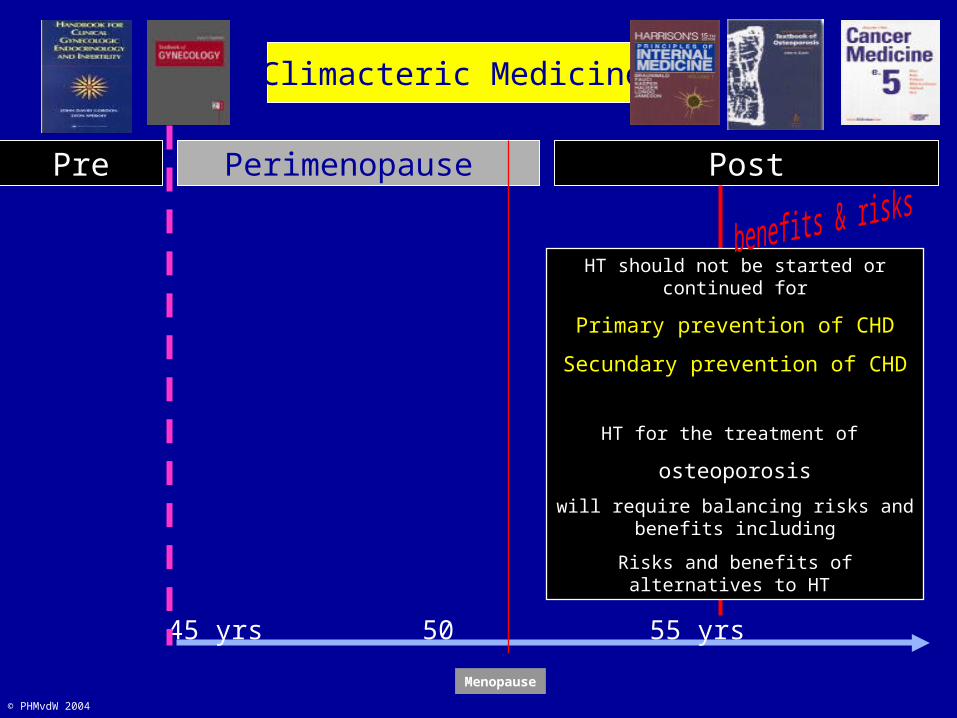
Climacteric Medicine
© PHMvdW 2004
Menopause
HT should not be started or continued for
Primary prevention of CHD
Secundary prevention of CHD
HT for the treatment of
osteoporosis
will require balancing risks and benefits including
Risks and benefits of alternatives to HT

Menopause
45 yrs 50 yrs 55 yrs
Menstrual cycle problemsBleeding problems
Flushes Night sweats
Urogenital atrophy
DUPHASTON ® 10 / 20
FEMOSTON ® 1 / 10
FEMOSTON ® 1 / 5
Low dose
for
estrogens
Proper dose
for
progestagens
Clinician Women
© PHMvdW 2004
Health care for Women
Medical Practice
relationship
ongoing personal
The Art of Medicine the unique combination of
ExperienceMedical Knowledge Intuition
Judgment Communication
Curiosity Compassion
EpidemiologistsHealth care industry PolicymakersAdministrators Researchers