Embed Size (px)
Citation preview

Unbound (Free) Bilirubin:Improving the Paradigm for Evaluating Neonatal Jaundice
Charles E. Ahlfors,1* Richard P. Wennberg,2 J. Donald Ostrow,3 and Claudio Tiribelli4
BACKGROUND: The serum or plasma total bilirubin con-centration (BT) has long been the standard clinical lab-oratory test for evaluating neonatal jaundice, despitestudies showing that BT correlates poorly with acutebilirubin encephalopathy (ABE) and its sequelae in-cluding death, classical kernicterus, or bilirubin-induced neurological dysfunction (BIND). The poorcorrelation between BT and ABE is commonly attrib-uted to the confounding effects of comorbidities suchas hemolytic diseases, prematurity, asphyxia, or infec-tion. Mounting evidence suggests, however, that BT
inherently performs poorly because it is the plasmanon–protein-bound (unbound or free) bilirubin con-centration (Bf), rather than BT, that is more closely as-sociated with central nervous system bilirubin concen-trations and therefore ABE and its sequelae.
CONTENT: This article reviews (a) the complex relation-ship between serum or plasma bilirubin measurementsand ABE, (b) the history underlying the limited use ofBf in the clinical setting, (c) the peroxidase method formeasuring Bf and technical and other issues involved inadapting the measurement to routine clinical use, (d)clinical experience using Bf in the management of new-born jaundice, and (e) the value of Bf measurements inresearch investigating bilirubin pathochemistry.
SUMMARY: Increasing evidence from clinical studies,clinical experience, and basic research investigating bil-irubin neurotoxicity supports efforts to incorporate Bf
expeditiously into the routine evaluation of newbornjaundice.© 2009 American Association for Clinical Chemistry
Clinical Chemistry recently published a Citation Classicentitled “Unbound Bilirubin: A Better Predictor of
Kernicterus?” (1 ). The article noted that preventingacute bilirubin encephalopathy (ABE)5 and its seriousneurological sequelae in jaundiced newborns remains aserious and unresolved concern for clinicians. It wenton to suggest that the serum or plasma non–protein-bound bilirubin concentration (free or unbound bili-rubin, Bf) as measured by the much-cited peroxidasemethod (1, 2 ) may provide better guidance for therapythan the conventionally used total bilirubin concentra-tion (BT). The issue of BT vs Bf was also raised in arecent prospective National Institute of Child Healthand Human Development (NICHD) phototherapystudy that found considerable overlap in BT values invery low birth weight infants with and withoutbilirubin-associated deafness, and those authors sug-gested that Bf might have better differentiated the 2groups (3 ).
Although evidence suggesting that Bf would be su-perior to BT in the clinical management of jaundicednewborns first appeared in the 1950s (4 ), Bf has lan-guished for decades on the periphery of clinical prac-tice as well as basic research investigating the patho-chemistry of bilirubin neurotoxicity. Many clinicians,clinical chemists, and even researchers working in thefield of bilirubin neurotoxicity are unfamiliar with Bf
measurement or its clinical application. Recent eventshave renewed interest in Bf (5 ), and the intent of thisreview is to provide a framework for understandinghow Bf measurements might augment both the care ofjaundiced newborns and our understanding of thepathochemistry of ABE.
Neonatal jaundice is caused by the retention ofunconjugated bilirubin (UCB) during the normal,transient postnatal imbalance between UCB produc-tion and elimination. Although the condition is gener-ally inconsequential except for the noticeable jaundice,
1 Division of Neonatology, Department of Pediatrics, Stanford University School ofMedicine, Palo Alto, CA; 2 Division of Neonatology, Department of Pediatrics,and 3 Gastroenterology/Hepatology Division, Department of Medicine, Univer-sity of Washington School of Medicine, Seattle, WA; 4 Centro Studi Fegato andDepartment of Life Sciences, University of Trieste, Trieste, Italy.
* Address correspondence to this author at: PO Box 2904, Vashon, WA 98070.E-mail [email protected].
Received December 2, 2008; accepted February 27, 2009.Previously published online at DOI: 10.1373/clinchem.2008.121269
5 Nonstandard abbreviations: ABE, acute bilirubin encephalopathy; Bf, unbound(free) bilirubin; BT, total bilirubin; NICHD, National Institute of Child Health andHuman Development; UCB, unconjugated bilirubin; BIND, bilirubin-inducedneurological dysfunction; CNS, central nervous system; P, concentration ofplasma bilirubin-binding proteins; Kf, UCB–protein equilibrium association con-stant; ABR, auditory brainstem response; HRP, horseradish peroxidase; Kp,first-order rate constant for the HRP-catalyzed oxidation of bilirubin by peroxide;FDA, US Food and Drug Administration; Bfss, steady-state Bf; kd, bilirubin–protein dissociation rate constant; ka, bilirubin–protein association rate con-stant; CSF, cerebrospinal fluid.
Clinical Chemistry 55:71288–1299 (2009) Review
1288
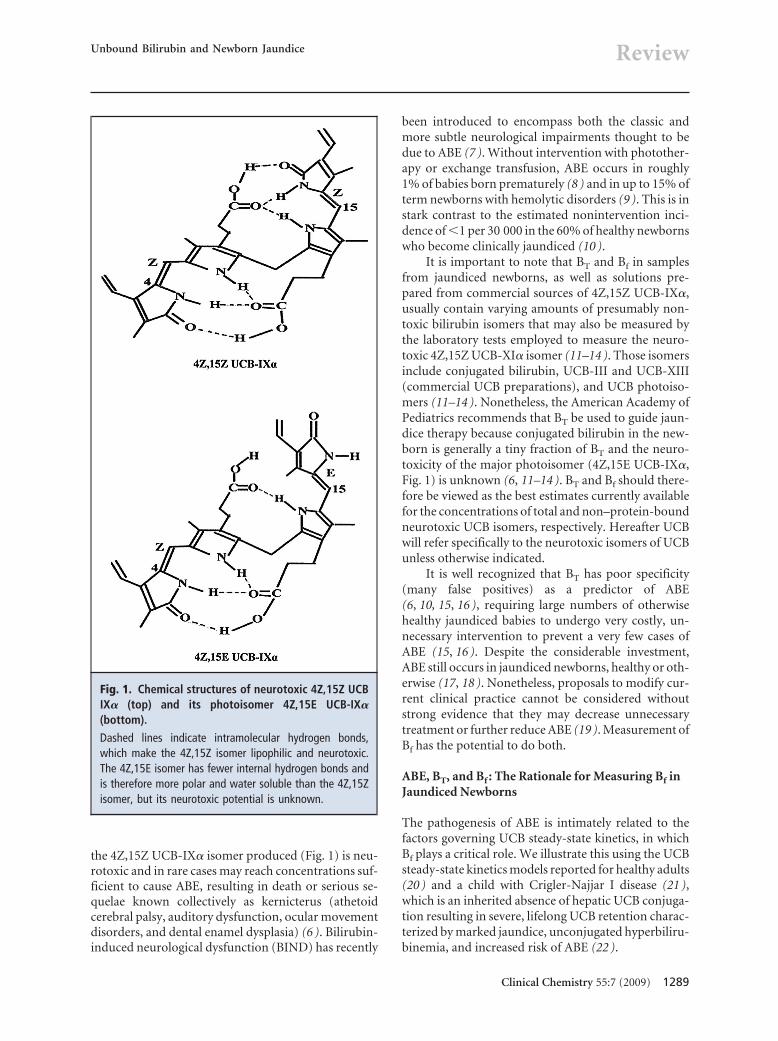
the 4Z,15Z UCB-IX� isomer produced (Fig. 1) is neu-rotoxic and in rare cases may reach concentrations suf-ficient to cause ABE, resulting in death or serious se-quelae known collectively as kernicterus (athetoidcerebral palsy, auditory dysfunction, ocular movementdisorders, and dental enamel dysplasia) (6 ). Bilirubin-induced neurological dysfunction (BIND) has recently
been introduced to encompass both the classic andmore subtle neurological impairments thought to bedue to ABE (7 ). Without intervention with photother-apy or exchange transfusion, ABE occurs in roughly1% of babies born prematurely (8 ) and in up to 15% ofterm newborns with hemolytic disorders (9 ). This is instark contrast to the estimated nonintervention inci-dence of �1 per 30 000 in the 60% of healthy newbornswho become clinically jaundiced (10 ).
It is important to note that BT and Bf in samplesfrom jaundiced newborns, as well as solutions pre-pared from commercial sources of 4Z,15Z UCB-IX�,usually contain varying amounts of presumably non-toxic bilirubin isomers that may also be measured bythe laboratory tests employed to measure the neuro-toxic 4Z,15Z UCB-XI� isomer (11–14 ). Those isomersinclude conjugated bilirubin, UCB-III and UCB-XIII(commercial UCB preparations), and UCB photoiso-mers (11–14 ). Nonetheless, the American Academy ofPediatrics recommends that BT be used to guide jaun-dice therapy because conjugated bilirubin in the new-born is generally a tiny fraction of BT and the neuro-toxicity of the major photoisomer (4Z,15E UCB-IX�,Fig. 1) is unknown (6, 11–14 ). BT and Bf should there-fore be viewed as the best estimates currently availablefor the concentrations of total and non–protein-boundneurotoxic UCB isomers, respectively. Hereafter UCBwill refer specifically to the neurotoxic isomers of UCBunless otherwise indicated.
It is well recognized that BT has poor specificity(many false positives) as a predictor of ABE(6, 10, 15, 16 ), requiring large numbers of otherwisehealthy jaundiced babies to undergo very costly, un-necessary intervention to prevent a very few cases ofABE (15, 16 ). Despite the considerable investment,ABE still occurs in jaundiced newborns, healthy or oth-erwise (17, 18 ). Nonetheless, proposals to modify cur-rent clinical practice cannot be considered withoutstrong evidence that they may decrease unnecessarytreatment or further reduce ABE (19 ). Measurement ofBf has the potential to do both.
ABE, BT, and Bf : The Rationale for Measuring Bf inJaundiced Newborns
The pathogenesis of ABE is intimately related to thefactors governing UCB steady-state kinetics, in whichBf plays a critical role. We illustrate this using the UCBsteady-state kinetics models reported for healthy adults(20 ) and a child with Crigler-Najjar I disease (21 ),which is an inherited absence of hepatic UCB conjuga-tion resulting in severe, lifelong UCB retention charac-terized by marked jaundice, unconjugated hyperbiliru-binemia, and increased risk of ABE (22 ).
Fig. 1. Chemical structures of neurotoxic 4Z,15Z UCBIX� (top) and its photoisomer 4Z,15E UCB-IX�(bottom).
Dashed lines indicate intramolecular hydrogen bonds,which make the 4Z,15Z isomer lipophilic and neurotoxic.The 4Z,15E isomer has fewer internal hydrogen bonds andis therefore more polar and water soluble than the 4Z,15Zisomer, but its neurotoxic potential is unknown.
Unbound Bilirubin and Newborn Jaundice Review
Clinical Chemistry 55:7 (2009) 1289
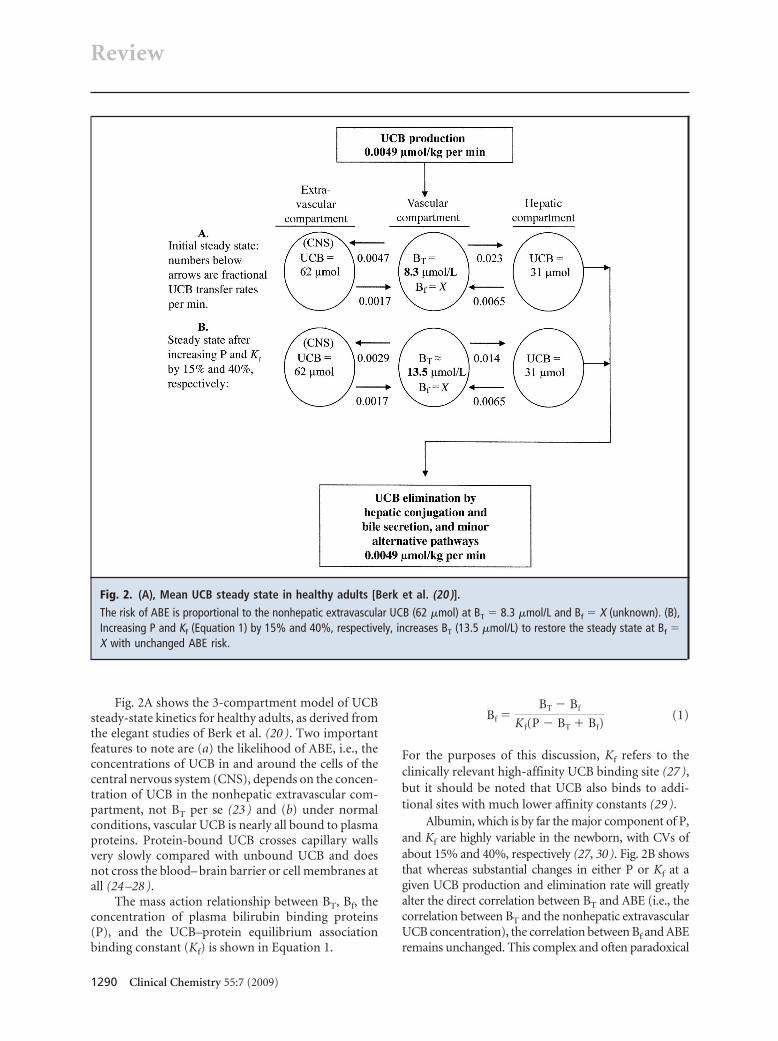
Fig. 2A shows the 3-compartment model of UCBsteady-state kinetics for healthy adults, as derived fromthe elegant studies of Berk et al. (20 ). Two importantfeatures to note are (a) the likelihood of ABE, i.e., theconcentrations of UCB in and around the cells of thecentral nervous system (CNS), depends on the concen-tration of UCB in the nonhepatic extravascular com-partment, not BT per se (23 ) and (b) under normalconditions, vascular UCB is nearly all bound to plasmaproteins. Protein-bound UCB crosses capillary wallsvery slowly compared with unbound UCB and doesnot cross the blood– brain barrier or cell membranes atall (24 –28 ).
The mass action relationship between BT, Bf, theconcentration of plasma bilirubin binding proteins(P), and the UCB–protein equilibrium associationbinding constant (Kf) is shown in Equation 1.
Bf �BT � Bf
Kf(P � BT � Bf)(1)
For the purposes of this discussion, Kf refers to theclinically relevant high-affinity UCB binding site (27 ),but it should be noted that UCB also binds to addi-tional sites with much lower affinity constants (29 ).
Albumin, which is by far the major component of P,and Kf are highly variable in the newborn, with CVs ofabout 15% and 40%, respectively (27, 30). Fig. 2B showsthat whereas substantial changes in either P or Kf at agiven UCB production and elimination rate will greatlyalter the direct correlation between BT and ABE (i.e., thecorrelation between BT and the nonhepatic extravascularUCB concentration), the correlation between Bf and ABEremains unchanged. This complex and often paradoxical
Fig. 2. (A), Mean UCB steady state in healthy adults [Berk et al. (20 )].The risk of ABE is proportional to the nonhepatic extravascular UCB (62 �mol) at BT � 8.3 �mol/L and Bf � X (unknown). (B),Increasing P and Kf (Equation 1) by 15% and 40%, respectively, increases BT (13.5 �mol/L) to restore the steady state at Bf �X with unchanged ABE risk.
Review
1290 Clinical Chemistry 55:7 (2009)
interplay between the UCB binding variables in Equation1 and ABE is not accounted for when a single BT interven-tion threshold is applied across a diverse population ofnewborns (6, 30).
Extrapolating the concepts illustrated in Fig. 2 toneonatal jaundice, the rate of vascular UCB increaseand peak BT will be directly correlated with (a) themagnitude of the imbalance between UCB productionand elimination and (b) the magnitudes of P and Kf.
Increases in the UCB production/elimination imbal-ance at constant P and Kf will increase BT, Bf, and therisk of ABE. However, increases in P and Kf at constantUCB production/elimination imbalance will increaseBT but not Bf or the risk of ABE (Fig. 2B). Variations inP and Kf in the newborn undermine the ability of BT
but not that of Bf to predict ABE, and Bf should inher-ently correlate better than BT with ABE in jaundicednewborns.
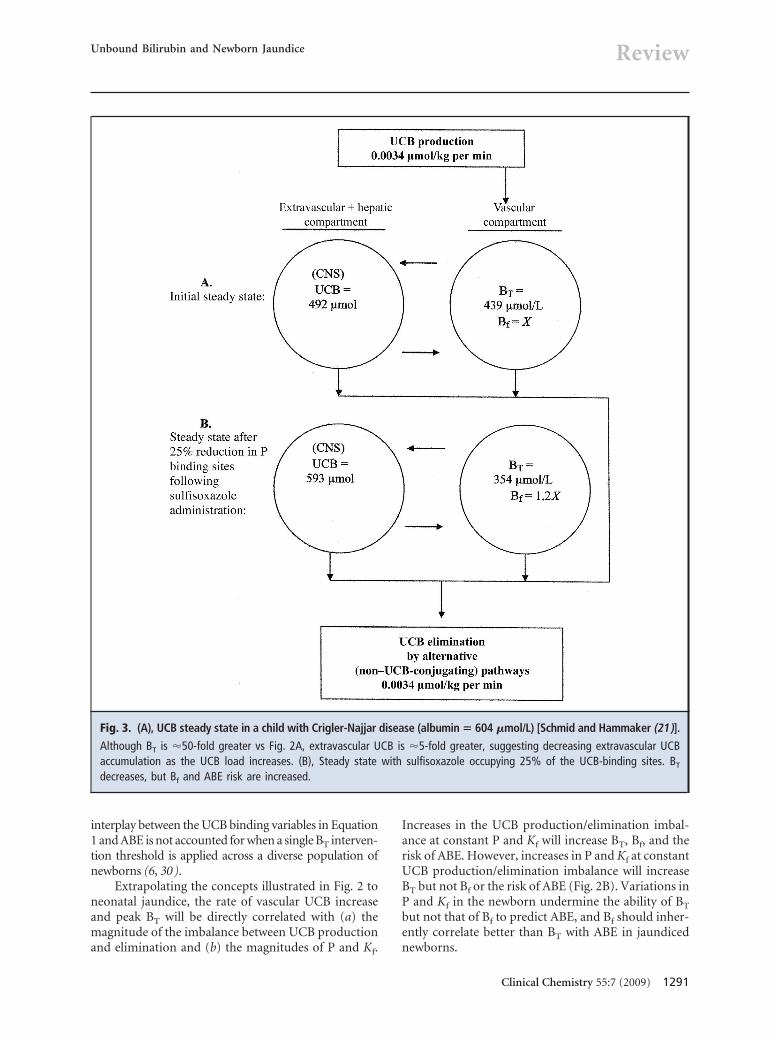
Fig. 3. (A), UCB steady state in a child with Crigler-Najjar disease (albumin � 604 �mol/L) [Schmid and Hammaker (21)].Although BT is �50-fold greater vs Fig. 2A, extravascular UCB is �5-fold greater, suggesting decreasing extravascular UCBaccumulation as the UCB load increases. (B), Steady state with sulfisoxazole occupying 25% of the UCB-binding sites. BT
decreases, but Bf and ABE risk are increased.
Unbound Bilirubin and Newborn Jaundice Review
Clinical Chemistry 55:7 (2009) 1291

Fig. 3A uses the UCB steady-state kinetics in anotherwise healthy child with Crigler-Najjar I disease(21 ) to illustrate that the relationships between BT, Bf,and ABE change as UCB accumulates. Compared withFig. 2A, BT in Fig. 3A is about 50 times greater (439 vs8.3 �mol/L), but the nonvascular UCB is only about 5times higher (492 vs 93 �mol of extravascular and he-patic UCB). This difference suggests that as UCB accu-mulates, an increasingly smaller fraction of the UCBload resides extravascularly. This phenomenon may re-sult from increased activity of facilitated and activetransport mechanisms for extravascular efflux of UCB(28 ), nonconjugating pathways for UCB catabolism(31, 32 ), and increasing saturation of non-CNS ex-travascular UCB reservoirs such as fatty tissue (�1% ofthe extravascular UCB resides in the CNS in animalmodels) (33 ).
Fig. 4 illustrates the clinical interplay of BT, Bf, andABE as the UCB load increases. Paradoxically, as P be-comes saturated with UCB, the incremental increase inBT per incremental increase in the UCB load decreaseswhile the incremental increase in Bf, which is still a tinyfraction of BT (29 ), accelerates. This in turn acceleratesthe extravascular accumulation of UCB and the risk ofABE. Therefore, without a confirming Bf measure-ment, an increased but stable BT in the clinical settingshould not be (but often is) taken as reassurance thatthe risk of ABE is not increasing.
Despite the rationale and arguments presentedabove, the poor correlation between BT and ABE is cus-tomarily attributed to comorbidities that may make theCNS more susceptible to UCB neurotoxicity (e.g., he-molysis, prematurity, asphyxia, infection) or extenuat-
ing clinical circumstances (15, 19, 34 ). Even the well-documented association between illness and impairedplasma protein binding of ligands, including UCB, israrely considered (35, 36 ). On closer examination,however, this tendency to marginalize the role of UCBbinding in ABE results more from historical circum-stances than a failure to appreciate the relationship be-tween UCB binding and ABE (6, 15 ). Invoking UCBbinding to explain the poor correlation between BT
and ABE without a substantial amount of supportingclinical data is merely speculation, and there has been aremarkable paucity of UCB-binding data in the clinicalliterature.
Where’s the Bf? A Brief Clinical History of ABE, BT,and Bf
In retrospect, BT remains entrenched at the cores ofclinical algorithms designed to prevent ABE (6 ) pri-marily because Bf measurements were not available un-til 20 years after UCB was clearly established as thecause of ABE. By then, other advances in newborncare had significantly altered the clinical outcomes ofnewborn jaundice and the perceived need for Bf
measurements.In the early 1950s, ABE was a serious problem
mainly for babies who had Rh or ABO hemolytic dis-ease or who were born prematurely (8, 9 ). Treatmentwith the newly described exchange transfusion wasrisky but significantly lowered the incidence of ABE inboth of these high-risk groups. The suggestion that theprocedure be used at BT �20 mg/dL (342 �mol/L) forbabies with hemolytic disease (9 ) was quickly appliedto all jaundiced newborns.
The complex interplay between BT, Bf, and ABEsoon became apparent when premature babies givensulfisoxazole for infection prophylaxis developed ABEand died despite a “low” BT (23 ). It was soon discov-ered that sulfisoxazole competes with UCB for proteinbinding sites, producing a new UCB steady state with alower BT but higher Bf and extravascular UCB, as illus-trated in Fig. 3B. The increased extravascular UCB of-ten reached levels sufficient to cause ABE despite thelow BT (23 ), a phenomenon that still haunts clinicalpractice (37, 38 ).
The sulfisoxazole experience alerted clinicians tothe role of UCB binding in the pathogenesis of ABE,and methods for measuring UCB binding were pur-sued in hopes of better identifying babies truly needinga potentially lifesaving but also very risky exchangetransfusion (4 ). Measuring Bf directly proved elusive,however, and the early tests measuring plasma “satura-tion” with UCB (i.e., plasma UCB-binding capacity)ultimately proved unsuitable for routine clinical labo-ratory use (39, 40 ).
Fig. 4. As the BT/P molar ratio approaches 1 in ajaundiced newborn, the high-affinity binding site(Equation 1) is nearly saturated, and Bf and the risk ofABE will accelerate dramatically with further in-creases in the UCB load [Jacobsen (29 )].BT, however, will increase more slowly because less of theUCB produced is retained in the vascular space.
Review
1292 Clinical Chemistry 55:7 (2009)

Ironically, by the time the peroxidase method formeasuring Bf finally arrived on the scene in 1974 (2 ),ABE had become a rare event in the newborn popula-tions at greatest risk. Rhogam prophylaxis had nearlyeliminated Rh hemolytic disease, and phototherapy toenhance UCB elimination substantially reduced thenumbers of exchange transfusions needed to preventABE in premature babies. Furthermore, a prospectivestudy of ill, premature newborns found neither BT or Bf
to be predictive of kernicterus at autopsy (41 ). Al-though this study was later shown to have serious tech-nical shortcomings (42 ), the now-rare incidence ofABE made prospective determination of the Bf thresh-old for ABE problematic in any case. Phototherapyseemed a safe and effective method for maintaining BT
below the concentrations at which exchange transfu-sion would be needed in most babies, and it becameincreasingly difficult to see how measuring Bf wouldsubstantially alter clinical care (43 ).
With the issue of ABE in high-risk neonatal pop-ulations apparently resolved without Bf measurement,attention turned to a major problem with jaundice inthe large group of healthy newborns. The a priori BT
�20 mg/dL exchange transfusion guideline, nowwhimsically christened vigintiphobia (fear of 20) (44 ),had morphed over the years into the clinical (and legal)cornerstone for jaundice intervention in healthy new-borns. However, a BT �20 mg/dL, unlike ABE, was afairly common occurrence in healthy newborns despitethe availability of phototherapy (34 ), and exchangetransfusion with its considerable morbidity and mor-tality (45 ) was frequently called for to prevent a rareillness (10 ). It is not surprising that clinicians arbi-trarily began treating most of these babies with photo-therapy alone. Historical evidence seemed supportiveof this untested practice and even suggested that jaun-dice in healthy babies was benign and being managedfar too aggressively (46 ). Unfortunately, ABE suddenlyappeared in previously healthy newborns in the mid1980s when the increasingly laissez-faire approach tojaundice collided with early postnatal hospital dis-charge (47 ). A worldwide reexamination of the man-agement of newborn jaundice ensued that largely fo-cused on systematic issues such as patient monitoringand follow-up, and Bf was considered only in passing(6, 19, 34 ).
Evidence also emerged questioning the adequacyof the varied and experientially based BT exchangetransfusion guidelines used for premature newborns(30 ). In a prospective NICHD study done in the 1970scomparing phototherapy with exchange transfusion,there were 3 cases of autopsy proven kernicterus in the216 babies with birth weights �1250 g, but only 1 had aBT above the study exchange transfusion threshold of10 mg/dL (171 �mol/L) (48 ). There were also reports
of hearing deficits associated with peak BT below ac-cepted exchange transfusion guidelines (49 ), but moreimportantly, 2 observational studies now documenteda significant association of ABE with Bf but not BT insick, premature newborns (50, 51 ). It was the intro-duction of the auditory brainstem response (ABR) forassessing newborn hearing in the early 1980s, however,that resurrected the issue of Bf in the management ofnewborn jaundice in earnest.
The ABR provided for the first time a noninvasiveand quantifiable outcome measure for assessing UCBneurotoxicity. UCB was quickly shown to induce ABRchanges that could progress to permanent signal loss orbe reversed by exchange transfusion (52, 53 ). There isnow unequivocal evidence that UCB-induced ABRchanges are predicted by Bf but not BT in both prema-ture and term newborns (54 –57 ). In addition, UCBinjury in susceptible areas of the CNS can now be doc-umented using newer imaging techniques in vivo suchas MRI (37, 58 ), providing yet another new outcomemeasure for documenting UCB injury.
It once again seems warranted and feasible to testthe hypothesis that Bf measurements will improve theclinical management of newborn jaundice by betteridentifying babies needing treatment and minimizingunnecessary intervention (5 ). The peroxidase test formeasuring Bf is well suited for this purpose.
The Peroxidase Test for Measuring Bf
The horseradish peroxidase (HRP) methodology of Ja-cobsen and Wennberg (1, 2 ) is based on the observa-tion that HRP catalyzes UCB oxidation by peroxide(typically hydrogen peroxide or ethyl hydrogen perox-ide), but protein-bound UCB is protected and only Bf
reacts (2, 31 ). The first-order rate constant for the re-action (Kp) is determined from the reaction velocity(rate of decrease in UCB peak light absorbance at 440nm) in the absence of UCB-binding proteins (i.e.,[UCB] � Bf, Equation 2a) and then used to calculate Bf
from the reaction velocity (rate of decrease in UCBlight absorbance peak at 460 nm) when binding pro-teins are present (Equation 2b) (2 ).
d�UCB�
dt� Kp�HRP��UCB� (2a)
dBT
dt� Kp�HRP�Bf (2b)
Integrated forms of the equations can also be used toobtain Kp and Bf (59 ), and BT is calculated from theinitial absorbance of the sample corrected for any he-moglobin interference (2 ). The test has been auto-mated (60, 61 ), requires small sample volumes (�100�L of serum or plasma), and is quantitative, rapid (2–3
Unbound Bilirubin and Newborn Jaundice Review
Clinical Chemistry 55:7 (2009) 1293

min), and inexpensive. Because the method directly as-says Bf, the lower-affinity UCB-binding sites will notobscure test endpoints as they do with the binding teststhat attempt to measure serum or plasma UCB bindingcapacity (29, 39, 40 ).
A US Food and Drug Administration (FDA)-approved commercial spectrophotometer (UB-A1 An-alyzer, Arrows Co Ltd) (62 ) provides automated read-outs of BT (mg/dL) and Bf (�g/dL). BT is obtained aftermanually diluting the sample 41-fold with phosphatebuffer, and a HRP reagent is added to obtain Bf. Thereagents are stable at 8 °C for a month after reconstitu-tion, and controls for BT and Bf are provided. The CVsfor BT and Bf are about 2% and 5%, respectively. Al-though many clinical studies have been done with thisdevice (11–14, 27, 51, 54 –57, 61, 63, 64 ), it is not cur-rently marketed in the US.
Several things interfere with the Bf measurementby the peroxidase test: (a) Hemoglobin is a weak per-oxidase and has considerable absorbance at 460 nm.Moderate hemolysis (hemoglobin �5 g/dL in the un-diluted sample (62 )) adds peroxidase activity that canfalsely increase Bf, and severe hemolysis overwhelmsUCB light absorbance at 460 nm, falsely lowering Bf
while falsely increasing BT (2, 62 ). (b) Conjugated bil-irubin is more readily oxidized than UCB and, at levelshigher than about 1 mg/dL, will falsely increase Bf
(13, 65 ). The test can be modified to avoid this prob-lem (65 ). (c) Paraben preservatives falsely increase Bf
by generating free radicals that rapidly oxidize UCB(66 ). (d) Bilirubin photoisomers appear to have littleeffect on Kf (Equation 1) in clinical studies (11, 12 ),although a recent in vitro study using nonneonatalsamples suggests that photoisomers may interfere un-predictably with the peroxidase test (14 ). The peroxi-dase method reacts far more readily with 4Z,15Z UCB-IX� than with UCB photoisomers, and the 4Z,15ZUCB-IX� oxidation products have far less light absor-bance than those of the photoisomers (11 ). (e) The pHand ionic composition (particularly chloride and phos-phate ion) of the reaction medium may alter bindingand the measured Bf (59, 63 ). (f) As with all enzyme-catalyzed reactions, Bf will vary with reaction temper-ature (62 ). (g) Substantial non–HRP-catalyzed UCBoxidation may occur depending on the type of perox-ide used (2, 62 ) and will falsely increase Bf unless acorrection is applied (2 ). (h) The large sample dilution(typically 40-fold) can attenuate the effect of weak UCBbinding competitors such as sulfisoxazole (Fig. 3B),causing underestimation of Bf (42 ).
Perhaps the most serious error made when usingthe peroxidase test is the failure to appreciate that the Bf
determined by the peroxidase test is a steady-state Bf
(Bfss) (27 ), where
Bfss �kd(BT � Bfss)
�ka�P � BT � Bfss�� � �Kp�HRP��(3)
and kd and ka are the UCB–protein dissociation andassociation rate constants, respectively (ka/kd � Kf inEquation 1). Bfss is nearly equal to the equilibrium Bf
only when ka(P BT Bfss) �� Kp[HRP] andEquation 3 and Equation 1 are nearly identical. Whenthis is not the case, Bfss underestimates the equilibriumBf, and the error worsens as the equilibrium Bf in-creases (27, 63 ). This error is easily avoided by measur-ing Bf at 2 or more HRP concentrations. When Bfss isindependent of the HRP concentration (Equation 3 �Equation 1), Bfss is a reliable estimate of the equilib-rium Bf at each HRP concentration. When Bfss de-creases with increasing HRP, however, the equilibriumBf is equal to the inverse of the intercept of the plot of1/Bfss vs [HRP], as explained in detail elsewhere(27, 59, 61 ).
A pseudo-error in the method occurs when di-luted samples are used because the apparent Kf for thealbumin binding of UCB as well as many other ligandsincreases with sample dilution (61, 63, 67, 68 ). Kf in-creases steeply below albumin concentrations of about100 �mol/L, most likely due to the dissociation of al-bumin oligomers that bind UCB less avidly than thealbumin monomer (68 ). Bf measured at the standard40-fold sample dilution traditionally used for the per-oxidase test (2 ) is lower than but correlates directly andsignificantly with Bf measured at minimal sample dilu-tion (61, 63 ). Furthermore, Bf measured in dilutedsamples has been superior to BT in predicting ABE- orUCB-induced ABR changes (50, 51, 54 –57 ). Nonethe-less, because dilution alters both intrinsic albuminbinding and may also attenuate the effects of weak UCBbinding competitors, it would seem prudent to mea-sure Bf at minimal sample dilution if possible.
The only clinical laboratory control for Bf is sup-plied with the commercial instrument described above.Kp may be determined directly using solutions of UCB(Equation 2A), but the instability of UCB solutionsmake this approach problematic for clinical laborato-ries. UCB surrogates such as purpurogallin or the morestable biliverdin (69 ) could be employed to verify HRPactivity, but specific Bf controls with a human albuminmatrix to stabilize UCB are more desirable. Current BT
clinical laboratory controls may also prove useful inthis regard (61 ), and it may be feasible to develop newBf controls composed of UCB and human albumin so-lutions that are cross-referenced to Bf measured byother binding methods (68 ).
Intervention (reference) Bf thresholds for usingphototherapy or exchange transfusion can only beapproximated from available data at this time (50, 51, 54–57, 64, 70). P and Kf will need to be determined in larger
Review
1294 Clinical Chemistry 55:7 (2009)

populations of newborns to determine the range of Bf
values occurring at the specific BT currently used to guidetherapy (6, 30, 34). UCB-binding isotherms can readilybe constructed for this purpose by titrating individualsamples and umbilical cord blood with UCB and measur-ing Bf over the range of BT observed clinically (2, 60).Because both BT and the BT/albumin ratio guidelines forexchange transfusion decrease with gestation and birthweight (30), Bf intervention thresholds should encom-pass these parameters as well.
Can Bf Alter Clinical Practice? A Brief Summary of aClinical Experience with the Peroxidase Test
The first author of this review (C.E. Ahlfors) has usedthe peroxidase test in the clinical management of new-born jaundice. BT and Bf were measured at 2 HRP con-centrations using a UB-A1 Analyzer in a CLIA-certifiedlaboratory. The reference exchange transfusion Bf
threshold, extrapolated from existing literature and ad-justed for birth weight, was 1.3 �g/dL per kg of birthweight (22 nmol/L per kg), with a maximum allowableBf of 4 �g/dL (66 nmol/L) (41, 50, 51, 64, 70 ). Giventhe limited clinical experience with the reference Bf,however, we restricted its use such that exchange trans-fusions were never administered or withheld on thebasis of Bf alone. Exchange transfusions were per-formed when the BT or the BT/albumin ratio reachedexchange transfusion criteria (6, 30 ) or symptoms sug-gestive of ABE were present (6 ).
Bf was measured 294 times in 257 babies over 4years (Table 1). Several publications resulted from thislimited data set, including the first measurement of Bf
in a case of lethal kernicterus in the US (64 ) and repu-diation of a published model for brain UCB uptakebased on BT (27 ). Most importantly, we reported thatBf but not BT was significantly associated with abnor-mal automated ABR hearing screens in term babies(56 ), and that Bf and especially the Bf/BT ratio (a mea-sure of binding affinity that is proportional to 1/Kf),but not BT, predicted abnormal automated ABR hear-ing screens, regardless of clinical circumstances (57 ).
The American Academy of Pediatrics guidelinesrecommend exchange transfusion at BT �30 mg/dL(6 ), and above this concentration about half of the ba-bies with Rh hemolytic disease develop ABE (9 ). Weencountered 4 babies with BT �30 mg/dL. One hadlethal kernicterus (Bf 7.63 �g/dL, 130 nmol/L) and diedbefore exchange transfusion could be performed (64 ),and the other 3 received exchange transfusions. Onlyone of the 3 had a Bf above the exchange transfusionthreshold (Bf 4.41 �g/dL, 75 nmol/L), and that babywas lethargic and failed an automated ABR hearingscreen before exchange transfusion but then passed theABR screen (64 ). The other 2 babies (Bf 2.87 �g/dL and
2.80 �g/dL) had no obvious symptoms and passed theautomated ABR before receiving exchange transfu-sions. One also had a normal MRI examination. Add-ing Bf, automated ABR, and MRI to our evaluation ofthese babies enhanced our assessments of the likeli-hood of ABE and the urgency with which treatmentwas needed in these babies.
The American Academy of Pediatrics guidelinesconsider BT between 25 and 30 mg/dL a gray zonewhere phototherapy should be provided but exchangetransfusion is left to the discretion of the clinician (6 ).We readmitted 64 babies for jaundice, 13 of whom hadBT between 25 and 30 mg/dL. All the Bf values, whichranged from 1.23 to 2.99 �g/dL (21–51 nmol/L), werebelow the reference Bf concentrations, and all 13 babiespassed an automated ABR hearing screen on admis-sion. This provided us considerable reassurance thatphototherapy alone was sufficient for these babies.
An important but underappreciated tactic we oftenused was to measure Bf early in the clinical course whenbabies were at increased risk of ABE (e.g., had hemolysisor were born prematurely). This allowed us to estimatethe BT and BT/albumin ratio at the reference Bf for com-parison with the recommended exchange transfusion BT
and BT/albumin ratio for babies with that condition (30).Kf was calculated from the albumin concentration, BT,and Bf using Equation 1, and then reinserted into theequation along with the albumin and reference Bf (22nmol/L � birth weight in kg up to 66 nmol/L) to calculatethe BT and the BT/albumin ratio at the reference Bf. Com-paring these with the recommended intervention BT andthe BT/albumin ratio allowed us to individualize our in-tervention strategies for each patient. The importance ofapplying this tactic as well as the general concepts outlinedin this review to clinical practice and research are illus-trated by comparing our clinical experience with prema-ture newborns of�1 kg birth weight (Table 1) with that ofthe recent NICHD phototherapy study (3).
The NICHD phototherapy study admitted 984 ba-bies into its conservative phototherapy group in whichphototherapy and exchange transfusion were consid-ered at BT thresholds of 8 and 10 mg/dL and 13 and 15mg/dL for birth weights �0.750 kg and �0.751 kg, re-spectively. Peak BT averaged 9.8 mg/dL, and 13 babiesreached BT exchange transfusion thresholds, with 3 re-ceiving the procedure (0.3%) and 10 receiving aug-mented phototherapy according to study guidelines.Twenty-eight babies (3%) had severe hearing loss de-fined as requiring bilateral hearing aids, about 10 timesthe rate of congenital deafness in the newborn popula-tion (71 ). We measured UCB binding in 59 similarbabies (Table 1), half of whom had binding measuredbefore 48 h of age. Phototherapy was applied at thediscretion of the attending physician and using our ex-
Unbound Bilirubin and Newborn Jaundice Review
Clinical Chemistry 55:7 (2009) 1295
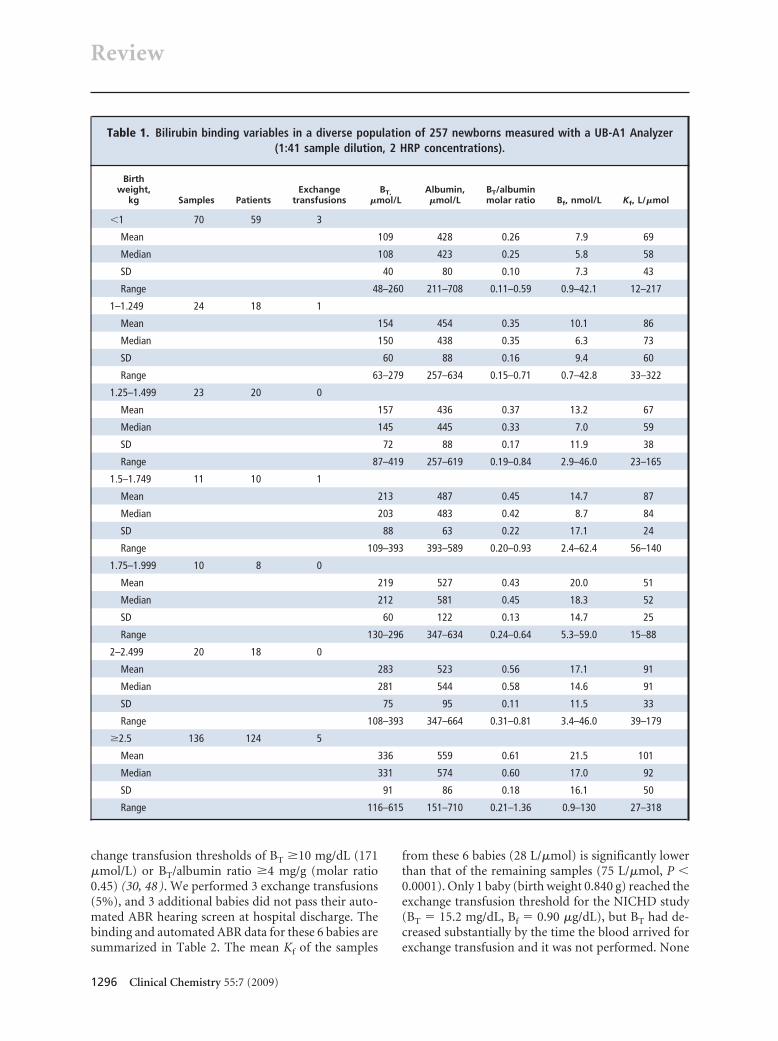
change transfusion thresholds of BT �10 mg/dL (171�mol/L) or BT/albumin ratio �4 mg/g (molar ratio0.45) (30, 48 ). We performed 3 exchange transfusions(5%), and 3 additional babies did not pass their auto-mated ABR hearing screen at hospital discharge. Thebinding and automated ABR data for these 6 babies aresummarized in Table 2. The mean Kf of the samples
from these 6 babies (28 L/�mol) is significantly lowerthan that of the remaining samples (75 L/�mol, P �0.0001). Only 1 baby (birth weight 0.840 g) reached theexchange transfusion threshold for the NICHD study(BT � 15.2 mg/dL, Bf � 0.90 �g/dL), but BT had de-creased substantially by the time the blood arrived forexchange transfusion and it was not performed. None
Table 1. Bilirubin binding variables in a diverse population of 257 newborns measured with a UB-A1 Analyzer(1:41 sample dilution, 2 HRP concentrations).
Birthweight,
kg Samples PatientsExchange
transfusionsBT,
�mol/LAlbumin,�mol/L
BT/albuminmolar ratio Bf, nmol/L Kf, L/�mol
�1 70 59 3
Mean 109 428 0.26 7.9 69
Median 108 423 0.25 5.8 58
SD 40 80 0.10 7.3 43
Range 48–260 211–708 0.11–0.59 0.9–42.1 12–217
1–1.249 24 18 1
Mean 154 454 0.35 10.1 86
Median 150 438 0.35 6.3 73
SD 60 88 0.16 9.4 60
Range 63–279 257–634 0.15–0.71 0.7–42.8 33–322
1.25–1.499 23 20 0
Mean 157 436 0.37 13.2 67
Median 145 445 0.33 7.0 59
SD 72 88 0.17 11.9 38
Range 87–419 257–619 0.19–0.84 2.9–46.0 23–165
1.5–1.749 11 10 1
Mean 213 487 0.45 14.7 87
Median 203 483 0.42 8.7 84
SD 88 63 0.22 17.1 24
Range 109–393 393–589 0.20–0.93 2.4–62.4 56–140
1.75–1.999 10 8 0
Mean 219 527 0.43 20.0 51
Median 212 581 0.45 18.3 52
SD 60 122 0.13 14.7 25
Range 130–296 347–634 0.24–0.64 5.3–59.0 15–88
2–2.499 20 18 0
Mean 283 523 0.56 17.1 91
Median 281 544 0.58 14.6 91
SD 75 95 0.11 11.5 33
Range 108–393 347–664 0.31–0.81 3.4–46.0 39–179
�2.5 136 124 5
Mean 336 559 0.61 21.5 101
Median 331 574 0.60 17.0 92
SD 91 86 0.18 16.1 50
Range 116–615 151–710 0.21–1.36 0.9–130 27–318
Review
1296 Clinical Chemistry 55:7 (2009)

of our 50 surviving babies have required bilateral hear-ing aids.
As we have pointed out in this review, the increasein the UCB load required to increase the BT from 8 to10 mg/dL (the NICHD study phototherapy thresholdsfor 0.750 and 0.751 kg babies, respectively) can be sub-stantial. Even worse, ABE may occur before reaching 10mg/dL if P is approaching saturation at 8 mg/dL, asillustrated in Fig. 4. Measuring UCB binding early inthe clinical course in the NICHD study could havehelped identify patients for whom the study interven-tion criteria might have been inappropriate. In addi-tion, UCB-binding measurements would have alsobeen very informative in all 16 NICHD study babiesthat reached the BT exchange transfusion criteria, only5 of whom received the procedure.
Comparing our clinical experience with conven-tional approaches to jaundice management clearly in-dicates that Bf measurements, especially when coupledwith ABR and MRI imaging, can substantially improveclinical practice. Babies with very poor UCB bindingcan be identified who might otherwise undergo unde-tected and unsuspected ABE at BT considered too lowfor ABE to occur. Screening for jaundice at newborndischarge is now being considered, and screening withUCB binding to obtain Kf would be valuable. A higherKf at increased hour-specific discharge BT arguesagainst excessive UCB production, whereas a lower Kf
at nondescript discharge BT identifies an increased riskfor ABE at unexpectedly low BT (6 ). The ultimate ad-vantage of measuring UCB binding is individualizationof jaundice management, where one BT interventioncriterion clearly can never fit all.
Research Applications of Bf Measurements
Measuring Bf in the media of cell culture models ofbilirubin toxicity has been addressed only recently(59, 72 ). It has been now been demonstrated directlythat in vitro cytotoxicity is accurately predicted by Bf
but not BT, irrespective of whether human or bovineserum albumin or fetal calf serum is used in the me-dium (59 ). Such measurements with cultured neuronsand astrocytes may provide considerable insight intothe concentrations of Bf in the cerebrospinal fluid(CSF) and extracellular fluid of the CNS that are likelyto produce bilirubin neurotoxicity in vivo (73 ). In ad-dition, Bf measurements may help evaluate the consid-erable variation in susceptibility of cell lines to biliru-bin toxicity and the specific anatomical patterns ofkernicterus that occur in vivo (74 ).
In vitro aspects of UCB binding may also be rele-vant in vivo. The enhanced effect of albumin dilutionon UCB–albumin binding noted above may play animportant role in the movement of UCB from blood toCSF across the choroid plexus. The albumin concen-tration in the CSF is about 2% that of the blood, and,consistent with the enhancement of albumin bindingaffinity with dilution noted above (67– 69 ), the re-ported BT/albumin ratios in CSF are higher than thecorresponding ratios in the blood (75 ). The higher af-finity of the less concentrated albumin in the CSFwould create a gradient favoring net diffusion of un-bound UCB from plasma into the CSF.
Summary and Conclusions
There is now strong evidence that Bf measurementscould significantly improve the clinical management ofnewborn jaundice by better detecting those babiesneeding treatment and by reducing unnecessary inter-vention. Bf measurements in basic and clinical researchmay provide further insight into the pathochemistryof ABE. We must continually remind ourselves thatour goal in measuring vascular bilirubin levels is not toprevent hyperbilirubinemia per se, but to preventbilirubin-induced brain injury. The emerging clinicalevidence strongly supports the theoretical consider-ations indicating that measurement of Bf may contrib-ute substantially to achieving this goal.
Table 2. Bilirubin binding variables (UB-A1 Analyzer, 1:41 sample dilution, 2 HRP concentrations) in babies bornat <1 kg who received exchange transfusions or had an abnormal automated ABR hearing screening
at hospital discharge.
Birth weight,kg
Exchangetransfusion
Automated ABRat discharge
BT, �mol/L(mg/dL)
Bf, nmol/L(�g/dL)
Albumin, �mol/L(g/dL) Kf, L/�mol
0.823 Yes Normal 111 (6.5) 21 (1.22) 211 (1.4) 53
0.580 Yes Not done 166 (9.7) 42 (2.46) 498 (3.3) 12
0.622 Yes Died 173 (10.1) 34 (1.99) 513 (3.5) 15
0.777 No Abnormal 54.7 (3.2) 5.2 (0.31) 423 (2.8) 28
0.583 No Abnormal 66.7 (3.9) 8.2 (0.48) 544 (3.6) 17
0.619 No Abnormal 94.0 (5.5) 5.3 (0.34) 483 (3.2) 42
Unbound Bilirubin and Newborn Jaundice Review
Clinical Chemistry 55:7 (2009) 1297

Author Contributions: All authors confirmed they have contributed tothe intellectual content of this paper and have met the following 3 re-quirements: (a) significant contributions to the conception and design,acquisition of data, or analysis and interpretation of data; (b) draftingor revising the article for intellectual content; and (c) final approval ofthe published article.
Authors’ Disclosures of Potential Conflicts of Interest: Uponmanuscript submission, all authors completed the Disclosures of Poten-tial Conflict of Interest form. Potential conflicts of interest:
Employment or Leadership: None declared.
Consultant or Advisory Role: None declared.Stock Ownership: None declared.Honoraria: None declared.Research Funding: C. Tiribelli, Telethon-Italy (grant no. GGP05062)and Regione Autonoma Friuli Venezia.Expert Testimony: None declared.Other remuneration: J.D. Ostrow, Centro Studi Fegato, payment oflocal travel expenses.
Role of Sponsor: The funding organizations played no role in thedesign of study, choice of enrolled patients, review and interpretationof data, or preparation or approval of manuscript.
References
1. Wennberg RP. Unbound bilirubin: a better predic-tor of kernicterus? Clin Chem 2008;54:207–8.
2. Jacobsen J, Wennberg RP. Determination of un-bound bilirubin in the serum of newborns. ClinChem 1974;20:783–9.
3. Morris BH, Oh W, Tyson JE, Stevenson DK, PhelpsDL, O’Shea TM, et al. Aggressive vs. conservativephototherapy for infants with extremely low birthweight. N Engl J Med 2008;359:1885–96.
4. Odell GB. Studies in kernicterus. I. The proteinbinding of bilirubin. J Clin Invest 1959;38:823–33.
5. Wennberg RP, Ahlfors CE, Bhutani VK, JohnsonLH, Shapiro SM. Toward understandingkernicterus: a challenge to improve the man-agement of jaundiced newborns. Pediatrics2006;117:474 – 85.
6. American Academy of Pediatrics, Subcommit-tee on Hyperbilirubinemia. Management of hy-perbilirubinemia in the newborn infant 35 ormore weeks of gestation. Pediatrics 2004;114:297–316.
7. Shapiro SM. Definition of the clinical spectrum ofkernicterus and bilirubin induced neurologicaldysfunction (BIND). J Perinatol 2005;25:54–9.
8. Wishingrad L, Cornblath M, Takakuwa T, Rozen-feld IM, Elegant LD, Kaufman A, et al. Studies ofnon-hemolytic hyperbilirubinemia in prematureinfants: I. Prospective randomized selection forexchange transfusion with observations on thelevels of serum bilirubin with and without ex-change transfusion and neurologic evaluationsone year after birth. Pediatrics 1965;36:162–72.
9. Hsia DY, Allen FH, Gellis SS, Diamond LK. Eryth-roblastosis fetalis VIII. Studies of serum bilirubinin relation to kernicterus. N Engl J Med 1952;247:668–71.
10. Trolle D. Discussion on the advisability of per-forming exchange transfusion in neonatal jaun-dice of unknown aetiology. Acta Paediatr 1961;50:392–8.
11. Itoh S, Yamakawa T, Onishi S, Isobe K, ManageM, Sasaki K. The effect of bilirubin photoisomerson unbound-bilirubin concentration estimated bythe peroxidase method. Biochem J 1986;239:417–21.
12. Myara A, Sender A, Valette V, Rostoker C,Paumier D, Capoulade C, et al. Early changes incutaneous bilirubin and serum bilirubin isomersduring intensive phototherapy of jaundiced neo-nates with green and blue light. Biol Neonate1997;71:75–82.
13. Itoh S, Kawada K, Kusaka T, Yasuda S, Okada H,
Imai T, Isobe K. Influence of glucuronosyl bilirubinand (EZ)-cyclobilirubin on determination of serumunbound bilirubin by UB-analyser. Ann Clin Bio-chem 2002;39:583–8.
14. McDonagh AF, Vreman HJ, Wong RJ, StevensonDK. Photoisomers: Obfuscating factors in the per-oxidase measurement of unbound bilirubin? Pe-diatrics 2009;123:67–76.
15. Ip S, Chung M, Kulig J, O’Brien R, Sege R, GlickenS, et al. An evidence-based review of importantissues concerning neonatal hyperbilirubinemia.Pediatrics 2004;114:e130–53.
16. Suresh G. Cost-effectiveness of strategies in-tended to prevent kernicterus in newborn infants.Pediatrics 2004;114:917–27.
17. Sheridan SE. Parents of infants and children withkernicterus. J Perinatol 2005;25:227–8.
18. Oh W, Tyson JE, Fanaroff AA, Vohr BR, Perrit R,Stoll BJ, et al. Association between peak serumbilirubin and neurodevelopmental outcomes inextremely low birth weight infants. Pediatrics2003;112:773–9.
19. Blackmon LR, Fanaroff AA, Raju TNK. Researchon prevention of bilirubin-induced brain injuryand kernicterus: National Institute of Child Healthand Human Development Conference ExecutiveSummary. Pediatrics 2004;114:229–43.
20. Berk PD, Howe RB, Bloomer JR, Berlin NI. Studiesof bilirubin kinetics in normal adults. J Clin Invest1969;48:2176–90.
21. Schmid R, Hammaker L. Metabolism and dispo-sition of C14-bilirubin in congenital nonhemolyticjaundice. J Clin Invest 1963;42:1720–34.
22. Strauss KA, Robinson DL, Vreman HJ, Puffen-berger EG, Hart G, Morton DH. Management ofhyperbilirubinemia and prevention of kernicterusin 20 patients with Crigler-Najjar disease. EurJ Pediatr 2006;165:306–19.
23. Harris RC, Lucey JF, MacClean JR. Kernicterus inpremature infants associated with low concentra-tions of bilirubin in the plasma. Pediatrics 1958;21:875–84.
24. Bloomer JR, Berk PD, Vergalla J, Berlin NI.Influence of albumin on the hepatic uptake ofunconjugated bilirubin. Clin Sci Mol Med 1973;45:503–16.
25. Bloomer JR, Berk PD, Vergalla J, Berlin NI. Influ-ence of albumin on the extravascular distributionof unconjugated bilirubin. Clin Sci Mol Med 1973;45:5–526.
26. Stollman YR, Gartner U, Theilmann L, Ohmi N.Hepatic bilirubin uptake is not facilitated by al-bumin binding. J Clin Invest 1983;72:718–23.
27. Ahlfors CE, Parker AE. Evaluation of a model forbrain bilirubin uptake in jaundiced newborns.Pediatr Res 2005;58:1175–9.
28. Ostrow JD, Pascolo L, Brites D, Tiribelli C. Molec-ular basis of bilirubin-induced neurotoxicity.Trends Mol Med 2004;10:65–70.
29. Jacobsen J. Binding of bilirubin to albumin—determination of the dissociation constants. FEBSLett 1969;6:112–4.
30. Ahlfors CE. Criteria for exchange transfusion injaundiced newborns. Pediatrics 1994;93:488–94.
31. Brodersen R, Bartels P. Enzymatic oxidation ofbilirubin. Eur J Biochem 1969;10:468–73.
32. Kapitulnik J, Hardwick JP, Ostrow JD, WebsterCC, Park SS, Gelboin HV. Increase in a specificcytochrome P-450 isoenzyme in the liver of con-genitally jaundiced Gunn rats. Biochem J 1987;242:297–300.
33. Davis DR, Yeary RA. Effect of sulfadimethoxine ontissue distribution of 14C bilirubin in the newbornand adult hyperbilirubinemic Gunn rat. PediatrRes 1975;9:846–50.
34. Bhutani VK, Johnson LH, Maisels MJ, NewmanTB, Phibbs C, Stark AR, Yeargin-Allsopp M. Ker-nicterus. Epidemiological strategies for its pre-vention through systems-based approaches. JPerinatol 2004;24:650–62.
35. Reynolds RC, Cluff LE. Interaction of serum andsodium salicylate: changes during acute infectionand its influence on pharmacological activity. BullJohns Hopkins Hosp 1960;107:278–90.
36. Ebbesen F, Knudsen A. The possible risk of bili-rubin encephalopathy as predicted by plasmaparameters in neonates with previous severe as-phyxia. Eur J Pediatr 1992;151:910–2.
37. Govaert P, Lequin M, Swarte R, Robben S, De CooR, Weisglas-Kuperus N, et al. Changes in globuspallidus with (pre)term kernicterus. Pediatrics2003;112:1256–63.
38. Merhar SL, Gilbert DL. Clinical (video) findingsand cerebrospinal fluid neurotransmitters in 2children with severe chronic bilirubin encephalop-athy, including a former preterm infant withoutmarked hyperbilirubinemia. Pediatrics 2005;116:1226–30.
39. Waters WJ, Porter, E. Indications for exchangetransfusion based upon the role of albumin in thetreatment of hemolytic disease of the newborn.Pediatrics 1964;33:749–57.
40. Tyall RG, Peake MJ. Theoretical constraints in themeasurement of serum bilirubin binding capacity.Clin Biochem 1982;15:146–51.
41. Ritter DA, Kenny JD, Norton HJ, Rudolph AJ. A
Review
1298 Clinical Chemistry 55:7 (2009)

prospective study of free bilirubin and other riskfactors in the development of kernicterus in pre-mature infants. Pediatrics 1982;69:260–6.
42. Ahlfors CE. Benzyl alcohol, kernicterus, and un-bound bilirubin. J Pediatr 2001;139:317–9.
43. Cashore W, Gartner L, Oh W, Stern L. Clinicalapplication of bilirubin-binding determinations:current status. J Pediatr 1978;93:827–33.
44. Watchko JF, Oski FA. Bilirubin 20 mg/dL � vig-intiphobia. Pediatrics 1983;71:660–3.
45. Keenan WJ, Novak KK, Sutherland JM, Bryla DA,Fetterly KL. Morbidity and mortality associatedwith exchange transfusion. Pediatrics 1985;75s:417–21.
46. Newman TB, Maisels MJ. Evaluation and treat-ment of jaundice in the term newborn: a kinder,gentler approach. Pediatrics 1992;89:809–18.
47. Brown AK, Johnson LL. Loss of concern aboutjaundice and the re-emergence of kernicterus infull-term infants in the era of managed care. In:Fanaroff AA, Klaus MH, editors. The Yearbook ofNeonatal and Perinatal Medicine. St. Louis, MO:Mosby, 1996;17–28.
48. Gartner LM, Lee KS, Keenan WJ, White NB, BrylaDA. Effect of phototherapy on albumin binding ofbilirubin. Pediatrics 1985;75s:401–6.
49. Bergman I, Hirsch RP, Fria TJ, Shapiro SM, Holz-man I, Painter MJ. Cause of hearing loss in thehigh-risk premature infant. J Pediatr 1985;106:95–101.
50. Cashore WJ, Oh W. Unbound bilirubin and ker-nicterus in low-birth-weight infants. Pediatrics1982;69:481–5.
51. Nakamura H, Yonetani M, Uetani Y, Funato M,Lee Y. Determination of serum unbound bilirubinfor prediction of kernicterus in low birth weightinfants. Acta Paediatr Jpn 1992;34:642–7.
52. Kaga K, Kitazumi E, Kodama K. Auditory brainstem responses of kernicterus infants. Int J Pedi-atr Otorhinolaryngol 1979;1:255–64.
53. Wennberg RP, Ahlfors CE, Bickers R, McMurtryCA, Shetter JL. Abnormal auditory brainstemresponse in a newborn infant withhyperbilirubinemia: improvement with ex-
change transfusion. J Pediatr 1982;100:624 – 6.54. Funato M, Tamai H, Shimada S, Nakamura H.
Vigintiphobia, unbound bilirubin, and auditorybrainstem responses. Pediatrics 1994;93:50–3.
55. Amin SB, Ahlfors C, Orlando MS, Dalzell LE, MerleKS, Guillet R. Bilirubin and serial auditory brain-stem responses in premature infants. Pediatrics2001;107:664–70.
56. Ahlfors CE, Parker AE. Unbound bilirubin is asso-ciated with abnormal automated auditory brain-stem responses in jaundiced newborns. Pediatrics2008;121:976–8.
57. Ahlfors CE, Amin SB, Parker AE. Unbound biliru-bin predicts abnormal automated auditory brain-stem response in a diverse newborn population. JPerinatol 2009;29:305–9.
58. Penn AA, Enzmann DR, Hahn JS, Stevenson DK.Kernicterus in a full term infant. Pediatrics 1994;93:1003–6.
59. Burgos LR, Calligaris S, Wennberg RP, Ahlfors CE,Malik SG, Ostrow JD, Tiribelli C. Factors affectingthe binding of bilirubin to serum albumins: vali-dation and application of the peroxidase method.Pediatr Res 2006;60:724–8.
60. Wennberg RP, Rasmussen L, Ahlfors CE, Valaes T.Mechanized determination of apparent unboundbilirubin concentration in serum. Clin Chem 1979;24:1444–7.
61. Ahlfors CE, Marshall GD, Wolcott DK, Olson DC,Van Overmeire B. Measurement of unbound bil-irubin by the peroxidase test using Zone Fluidics.Clin Chim Acta 2006;365:78–85.
62. Shimabuku R, Nakamura H. Total and unboundbilirubin determined using an automated per-oxidase micromethod. Kobe J Med Sci 1982;28:91–104.
63. Ahlfors CE, Vreman HJ, Wong RJ, Bender GS, OHW, Morris BH, Stevenson DK. Effects of sampledilution, peroxidase concentration, and chlorideion on the measurement of unbound bilirubin inpremature newborns. Clin Biochem 2007;40:261–7.
64. Ahlfors CE, Herbsman O. Unbound bilirubin in aterm newborn with kernicterus. Pediatrics 2003;
111:1110–2.65. Ahlfors CE. Measurement of plasma unbound
unconjugated bilirubin. Anal Biochem 2000;279:130–5.
66. Rasmussen LF, Ahlfors CE, Wennberg RP. Theeffect of paraben preservatives on the albuminbinding of bilirubin. J Pediatr 1976;89:475–8.
67. Boobis SW, Chignell CF. Effect of protein concen-tration on the binding of drugs to human serumalbumin–I. Sulfadiazine, salicylate and phenylbu-tazone. Biochem Pharmacol 1979;28:751–6.
68. Weisiger RA, Ostrow JD, Koehler RK, Webster CC,Mukerjee P, Pascolo L, Tiribelli C. Affinity ofhuman serum albumin for bilirubin varies withalbumin concentration and buffer composition:results of a novel ultrafiltration method. J BiolChem 2001;276:29953–6.
69. Ahlfors CE. Competitive interaction of biliverdinand bilirubin only at the primary bilirubin bindingsite on human albumin. Anal Biochem 1981;110:295–307.
70. Ahlfors CE. Unbound bilirubin associated withkernicterus: a historical approach. J Pediatr 2000;137:540–4.
71. Mehl AL, Thomas V. The Colorado newborn hear-ing screening project, 1992–1999: on the thresh-old of effective population-based universal new-born hearing screening. Pediatrics 2002;109:e7.
72. Ostrow JD, Pascolo L, Tiribelli C. Reassessment ofthe unbound concentrations of unconjugated bil-irubin in relation to neurotoxicity in vitro. PediatrRes 2003;54:98–104.
73. Calligaris S, Bellarosa C, Giraudi P, WennbergRW, Ostrow JD, Tiribelli C. Cytotoxicity is pre-dicted by unbound and not total bilirubin con-centration. Ped Res 2007;62:576–80.
74. Silva RF, Rodrigues CM, Brites D. Rat culturedneuronal and glial cells respond differently totoxicity of unconjugated bilirubin. Pediatr Res2002;51:535–41.
75. Kulkarni SV, Merchant RH, Gupte SC, DivekarRM. Clinical significance of serum and cerebro-spinal fluid bilirubin indices in neonatal jaundice.Indian Pediatr 1989;26:1202–8.
Unbound Bilirubin and Newborn Jaundice Review
Clinical Chemistry 55:7 (2009) 1299