Embed Size (px)
Citation preview
Unawareness of de®cits after righthemisphere stroke: double-dissociationsof anosognosias
Jehkonen M, Ahonen J-P, Dastidar P, Laippala P, Vilkki J.Unawareness of de®cits after right hemisphere stroke: double-dissociations of anosognosias.Acta Neurol Scand 2000: 102: 378±384. # Munksgaard 2000.
Objectives ± The aim was to study whether anosognosia for hemiparesis,anosognosia for neglect and general unawareness of illness double-dissociate, indicating that anosognosias are speci®c and independentimpairments of awareness. On the other hand, anosognosias may beassociated with one another and with general cognitive dysfunction,which decreases awareness of de®cits. The persistence and predictivevalue of anosognosias was examined during a 1-year follow-up. Patientsand methods ± Fifty-seven consecutive patients with acute righthemisphere infarction underwent neurological and neuroradiologicalexaminations, neuropsychological testing and an interview 10 days, 3months and 1 year after onset. Results ± Anosognosia for neglect andanosognosia for hemiparesis double-dissociated, as did unawareness ofillness and anosognosia for neglect. Patients showing unawareness ofillness or anosognosia for neglect and anosognosia for hemiparesis hadpoorer orientation and verbal memory than patients who were aware ofthese defects. Unawareness of illness and anosognosia for hemiparesisdisappeared during 3-month follow-up. Conclusion ± Double-dissocia-tions demonstrate that anosognosias for different defects are indepen-dent and speci®c impairments of awareness, although general cognitivedisorder may also reduce awareness of defects. Unawareness of illnessand anosognosia for hemiparesis disappear rapidly and can hardly bedirect causes of poor long-term recovery. However, transient anosog-nosia may be associated with persistent disorders which result in pooroutcome.
M. Jehkonen1,2, J-P. Ahonen2,P. Dastidar3, P. Laippala4, J. Vilkki5
1University of Tampere, Department of Psychology,
and 2Tampere University Hospital, Department of
Neurology and Rehabilitation, Tampere, Finland;3Tampere University Hospital, Department of
Diagnostic Radiology, Tampere, Finland; 4Tampere
School of Public Health, University of Tampere and
Tampere University Hospital, Tampere, Finland;5University of Helsinki, Department of Psychology, and
Helsinki University Central Hospital, Department of
Neurosurgery, Helsinki, Finland
Key words: stroke; neglect; anosognosia; recovery
Dr Mervi Jehkonen, Tampere University Hospital, P.O.
Box 2000, FIN-33521 Tampere, Finland
Tel.: +358 3 247 6498
Fax: +358 3 247 5314
email: klmeje@uta.®
Accepted for publication August 30, 2000
Anosognosia (for motor impairment or visual ®elddefect) is associated with disorientation, confusionand severe generalized cognitive disorder (1, 2). Onthe other hand, anosognosias for speci®c de®citsmay occur in patients with intact orientation (3, 4).The view that anosognosias are speci®c andindependent disorders which may occur withoutgeneralized cognitive dysfunction is based onobservations that anosognosias for various de®citsdissociate (3±8). However, we have not foundprevious reports of clear double-dissociations ofanosognosias in a prospective series of patients.
Cutting (1) suggested that neglect or agnosia mayplay an important role in the pathogenesis of
anosognosia for limb weakness, and that severeneglect could be conceived as a kind of unawarenessof space contralateral to the lesion. Bisiach et al. (5)demonstrated that anosognosia for motor impair-ment after right hemisphere lesion is associated withpersonal and extrapersonal neglect, but they alsoreported a double-dissociation of these de®cits,indicating that neglect is not a necessary conditionfor anosognosia for hemiparesis or for anosognosiafor visual ®eld defect. Anosognosias for these defectshave been studied, but there are only few studies onunawareness of neglect (8), even though neglect isusually considered in relation to anosognosias forother defects.
Acta Neurol Scand 2000: 102: 378±384Printed in UK. All rights reserved
Copyright # Munksgaard 2000
ACTA NEUROLOGICASCANDINAVICA
ISSN 0001-6314
378

Pedersen et al. (2, 9) found in their largecommunity-based series of stroke patients thatanosognosia (for hemiparesis and/or hemianopia)is a strong predictor of poor recovery during the acuteand early stage. Gialanella & Mattioli (10) reportedthat anosognosia (for hemiplegia) is a negativeprognostic factor for motor and functional recovery.It would certainly be important to clarify the unity ordiversity and persistence of unawareness of de®cits,because anosognosias for different defects do notnecessarily have similar prognostic implications.
Our aim was to study whether anosognosia forhemiparesis, anosognosia for neglect and generalunawareness of illness tend to co-occur, or whetherthey dissociate and even double-dissociate, indicat-ing that anosognosias are independent from oneanother and cannot be explained by reference to acommon underlying disorder. We were primarilyinterested in anosognosia for neglect and anosog-nosia for hemiparesis, because neglect and hemi-paresis clearly restrict independent and productiveactivity. Moreover, we examined whether patientswith anosognosia are more disoriented and haveworse verbal memory than patients who are aware oftheir illness or de®cits. Poor awareness of defectsmay complicate rehabilitation and compensation ofthese defects and adjustment to living independentlyin the community. If anosognosias cause poorlong-term functional outcome, then these disordersshould persist after the acute period of stroke.Therefore we studied the persistence of anosogno-sias during a 1-year follow-up period.
Patients and methods
We examined 57 consecutive patients who accordingto neurological examination had acute right hemi-sphere brain infarct. The patients were admitted toTampere University Hospital as emergency casesbetween February, 1994 and March, 1998. Allpatients underwent computerized tomography, 53of them also had an MRI examination. Thosepatients were excluded who had a history of neuro-logical disorders, who showed insuf®cient coopera-tion because of a lowered level of consciousness,severe primary visual impairment, who were left-handed and aged over 75 years. Neuropsychologicaland neurological examinations were carried outwithin 10 days of onset (mean=6.1; SD=1.97;range=2±10). Follow-up studies were conducted 3and 12 months after onset. None of the patients hadrecurrent stroke events during the follow-up. Allpatients volunteered to take part and gave theirinformed consent. The study was approved by theEthical Committee of Tampere University Hospital.
No infarction was visualized in 2 patients. Both ofthem had mild sensory and motor disorders in theacute phase. Five patients had infarction in the ponsand 8 patients had 2 right hemisphere infarcts. Onepatient had developmental dyslexia that clearlydisturbed his performance in the BehaviouralInattention subtests (11±13) requiring reading, buthe did not show signs of neglect. He was excludedfrom the further analyses. We had 56 patients in theacute examination, 53 patients in the 3-monthexamination and 49 in the 12-month examination.Three patients were lost at the 3-month follow-up: 1patient refused to participate and 2 patients couldnot be fully examined because of fatigue. In additionto these 3 patients, 4 further patients failed tocomplete the 12-month examination: 1 patient waspoorly motivated and completed only part of theneuropsychological tests, 2 patients refused toparticipate, and 1 patient died.
Neuropsychological examination
The patients were ®rst examined with neuropsycho-logical tests and then interviewed using a ques-tionnaire. The presence of neglect was determinedwith the 6 conventional subtests of the BehaviouralInattention Test (BIT) (11±13): line crossing, lettercancellation, star cancellation, ®gure and shapecopying, line bisection and representational draw-ing. Patients who did not reach the original cut-offscore (11) in at least 2 of the 6 conventional BITsubtests, were considered as neglect patients. Thenumber of the tests in which the cut-off score was notreached indicated the severity of neglect: 0=noneglect; 1=mild inattention; 2±4=moderateneglect; and 5±6=severe neglect.
Unawareness of neglect was assessed by askingthe patient directly: ``Do you have any dif®cultiesobserving any part of the space?'' If necessary, thepatient was given the following alternatives: left side,right side, none or both sides. Fourteen patientsreported this dif®culty in the ®rst examination andall of them speci®ed that it was on the left side.
General unawareness of illness and unawarenessof hemiparesis were assessed using Cutting's (1)questions. Patients were considered to be unaware ofillness if they gave inadequate answers to either ofthe 2 questions: ``Why are you here?'' and ``What isthe matter with you?''.
If the patients gave inadequate answers to any ofthe following 7 questions, they were considered to beunaware of hemiparesis: ``Is there anything wrongwith your arm or leg?''; ``Is it weak, paralyzed ornumb?''; ``How does it feel?''; (arm picked up)``What is this?''; ``Can you lift it?''; ``You clearlyhave some problem with this?''; (asked to lift arms)
Unawareness of de®cits after right hemisphere stroke
379

``Can't you see that the two arms are not at the samelevel?''.
Orientation and memory were studied with theOrientation (range: 0±5 points) and LogicalMemory (range: 0±46 points) subtests of theWechsler Memory Scale (WMS) (14). Version I ofthe Logical Memory subtest was presented at the10-day examination and version II was presented atthe 3-month and at the 12-month examinations.
Neurological and neuroradiological examinations
A complete neurological examination, includingconfrontational assessment of visual ®elds, wasperformed on the same day as the neuropsycholo-gical assessment, or not more than 1 day before orafter it. The degree of motor defect and hemianopiawas evaluated using the NIH Stroke Scale (15) 2±10days, 3 months and 12 months after the infarct.Hemiparesis was scored using a scale from 0(=normal) to 4 (=severe hemiparesis) for leg andarm separately, and these scores were summed togive a range from 0 to 8: 0=no motor defect;1±2=mild hemiparesis; 3±5=moderate hemipar-esis; and 6±8=severe hemiparesis. Visual ®eld defectwas scored as absent (=0) or present (=1).
All patients were examined with computerizedtomography (CT), 53 with magnetic resonanceimaging (MRI) of the brain. On average theneuroradiological studies were carried out 6 daysafter onset (SD=2.6; range=0±12). The sizes of theinfarctions were determined on the basis of the T2
weighted MRI images by manual tracing or, whendigital images were not available (n=10), on thebasis of the CT images by a method described byBroderick et al. (16).
Statistical analyses
The statistical analyses are based on 2-way analysisof variance for repeated measures and t-tests forindependent samples. In the latter we tested theequality of the variance using Levene's test; ifindicated, a separate variance t-test was applied.Computation was carried out using SPSS/Win(version 9.0) (17).
Results
Table 1 describes the patients' demographic andclinical characteristics at each examination. Fourpatients had a variable neglect diagnosis: they hadneglect at the 10-day examination and at the12-month examination, but not at the 3-monthexamination.
Double-dissociations of anosognosias
A double-dissociation of anosognosia for neglectand unawareness of illness is shown in Table 2. Tenpatients were unaware of neglect but aware ofillness, while 2 patients were unaware of illness butrecognized their severe neglect. Both of the latter 2patients also had severe hemiparesis and wereanosognosic for hemiparesis. Their Orientationwas normal (score=5), but 1 of them did notreach the median (score=20) of the LogicalMemory. Of the 10 patients who were unaware ofneglect and aware of illness, 1 patient had severeneglect with normal performance in the Orientationand Logical Memory tests. Thus there were 2patients who showed double-dissociation of ano-sognosia for severe neglect and unawareness ofillness and whose normal verbal memory perfor-mance indicated that their anosognosia was notsecondary to general cognitive disorder or dementia.
Unawareness of illness and anosognosia forhemiparesis dissociated, but did not double-dissoci-ate. Table 3 shows that 4 patients were aware ofillness, but unaware of hemiparesis. None wasunaware of illness and aware of hemiparesis.
A double-dissociation of anosognosia for neglectand anosognosia for hemiparesis is shown inTable 4. Three patients were unaware of neglectand aware of hemiparesis. Two of them had severe
Table 1. Patients' demographical and clinical characteristics at each examination
Follow-up times
Variables 10 days 3 months 12 months
Number of patients 56 53 49
Sex (F/M) 20/36 18/35 18/31
Hemianopia 13 (23%) 7 (13%) 7 (14%)
Hemiparesis 19 (34%) 12 (23%) 12 (25%)
Neglect (BITC) 21 (38%) 9 (17%) 9 (18%)
Age: (meantSD) 63.23 (10.21) 62.67 (10.21) 62.41 (10.41)
Orientation: (meantSD) 4.61 (0.71) 4.87 (0.38) 4.76 (0.52)
Logical memory: (meantSD) 19.77 (6.35) 18.70 (6.66) 19.71 (5.97)
Abbreviations: BITC=the conventional subtests of the Behavioural Inattention Test.Neglect patients did not reach the original cut-off score in at least 2 of the 6 BITCsubtests.
Table 2. The presence or absence of neglect and the awareness (A) or unawareness
(UA) of neglect and/or illness at the 10-day examination
Awareness of illness
Neglect A UA Total
Nx 28 ± 28
NxA 7 ± 7
N+A 5 2 7
N+UA 10 4 14
Total 50 6 56
Abbreviations: Nx=no neglect; N+=neglect.Bold ®gures indicate double-dissociations.
Jehkonen et al.
380

neglect with poor results in the Orientation orLogical Memory tests, and 1 had moderate neglectwith normal results in the Orientation and LogicalMemory tests. Four patients were unaware ofhemiparesis and aware of neglect. All 4 patientshad severe hemiparesis and severe neglect, and 2 ofthem showed normal performance on theOrientation and Logical Memory tests. There wasat least 1 patient with normal performance in theOrientation and Logical Memory tests in eachsubgroup involved in the double dissociations,demonstrating that generalized cognitive dysfunc-tion was not a necessary condition for anosognosiasor for their double-dissociation.
Hemianopia was observed in 6 (17%) of the 35patients without neglect and in 7 (33%) of the 21neglect patients. Seven patients without neglectreported dif®culties in observing things on the leftside (Tables 2 and 4). Five of them had hemianopia.Two patients who did not have hemiparesis accord-ing to the neurological examination reportedabnormal feelings in their left limbs (Tables 3 and4). Both were unaware of illness.
Orientation and Logical Memory in patients with and without
anosognosia
Table 5 shows that the patients who were unawareof illness performed less well in the Logical Memorytest and had more severe neglect than those whowere aware of illness. A t-test for independentsamples indicated that the differences between thegroups were signi®cant (t(54)=2.460, P=0.017 andt(5.42)=2.711, P=0.039, respectively). Patientswho were unaware of neglect had worseOrientation than the patients who were aware ofthe de®cit (t(18.116)=2.308, P=0.033). On averagethe patients with anosognosia for hemiparesis hadmore severe neglect (t(17)=3.616, P=0.002) andlarger infarction (t(17)=x2.318, P=0.033) thanthose who were aware of hemiparesis, but thesegroups did not differ signi®cantly on theOrientation or Logical Memory tests.
Three- and 12-month follow-up examinations
At the 3-month follow-up examination, 1 patientrefused to participate and 2 patients were unable tocomplete the examination because of fatigue. At theacute stage 1 of them was unaware of illness andhemiparesis. Two patients had neglect and wereaware of it, while 1 patient was hemiparetic.
None of the remaining 53 patients were unawareof illness or anosognosic for hemiparesis at the3-month examination. Five out of the 9 neglectpatients were unaware of neglect. Four of them alsohad hemiparesis. Some patients showed variation intheir anosognosia for neglect: 3 patients were awareof their neglect at the 10-day examination butunaware of it at the 3-month follow-up.
If anosognosias are manifestations of generalcognitive disorder or confusional state indicated bypoor verbal memory, then improvement in verbalmemory after the acute period should be morepronounced in patients whose awareness of de®citsimproves compared to those whose awareness doesnot change or declines. We compared the patientswho were unaware of illness but became aware of itduring the 3-month follow-up to the rest of thepatients who were aware of illness in both examina-tions with a 2-way analysis of variance for repeatedmeasures, using the Logical Memory scores at the10-day and 3-month examinations as dependentvariables. The patients who were unaware of illnessin the acute stage showed an improvement in theirmean Logical Memory performance from 14.8 to19.6 (n=5) during the 3-month follow-up. Thecorresponding means among the patients who wereaware of illness in both examinations were 20.5 and18.6 (n=49). This interaction was signi®cant (F(1,52)=9.113, P=0.004).
The patients who were anosognosic for hemipar-esis at the acute stage became aware of the defectwithin 3 months. They were compared to thepatients who were aware of their hemiparesis atboth examinations with a similar 2-way analysis ofvariance for repeated measures. The mean LogicalMemory score improved from 15.0 to 17.6 (n=7) inthe anosognosic group. In the group with intact
Table 3. The presence or absence of hemiparesis and the awareness (A) or
unawareness (UA) of hemiparesis and/or illness at the 10-day examination
Awareness of illness
Hemiparesis A UA Total
Hx 35 ± 35
HxA ± 2 2
H+A 11 ± 11
H+UA 4 4 8
Total 50 6 56
Abbreviations: Hx=no hemiparesis; H+=hemiparesis.
Table 4. The presence or absence of neglect and hemiparesis with awareness (A) or
unawareness (UA) of the defect at the 10-day examination
Neglect Hx HxA H+A H+UA Total
Nx 23 ± 5 ± 28
NxA 6 ± 1 ± 7
N+A 1 ± 2 4 7
N+UA 5 2 3 4 14
Total 35 2 11 8 56
Abbreviations: Nx=no neglect; N+=neglect. Hx=no hemiparesis;H+=hemiparesis.
Unawareness of de®cits after right hemisphere stroke
381
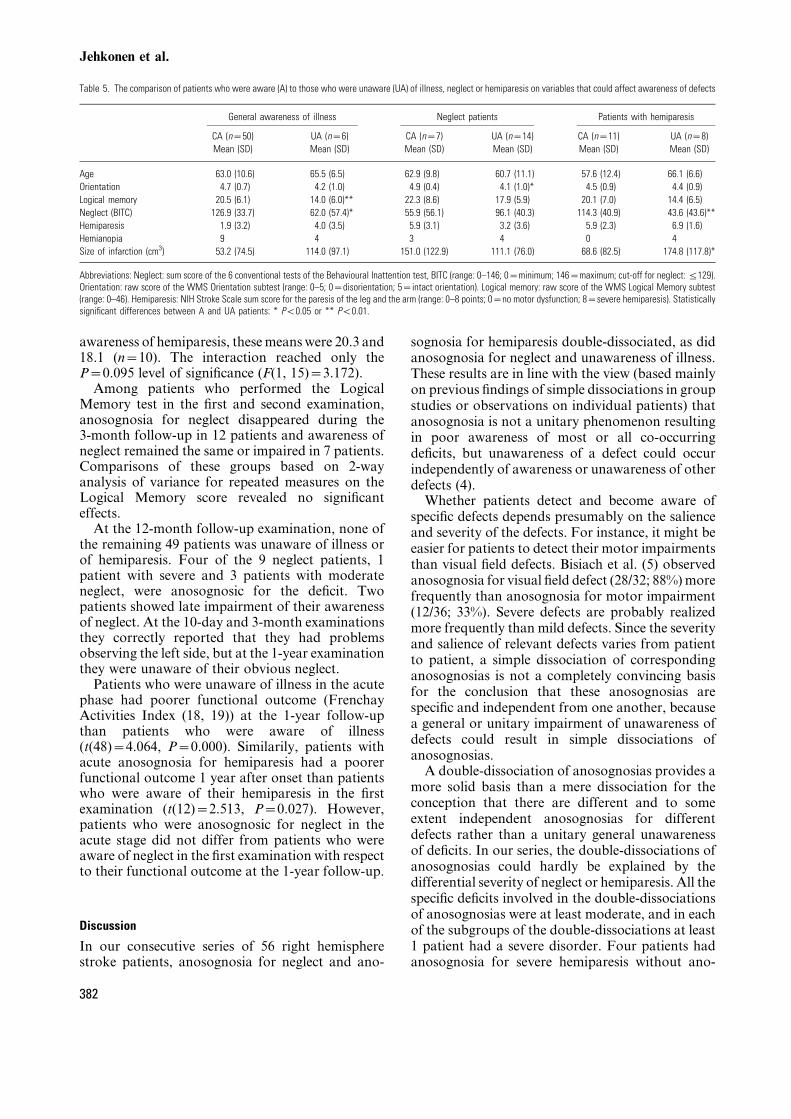
awareness of hemiparesis, these means were 20.3 and18.1 (n=10). The interaction reached only theP=0.095 level of signi®cance (F(1, 15)=3.172).
Among patients who performed the LogicalMemory test in the ®rst and second examination,anosognosia for neglect disappeared during the3-month follow-up in 12 patients and awareness ofneglect remained the same or impaired in 7 patients.Comparisons of these groups based on 2-wayanalysis of variance for repeated measures on theLogical Memory score revealed no signi®canteffects.
At the 12-month follow-up examination, none ofthe remaining 49 patients was unaware of illness orof hemiparesis. Four of the 9 neglect patients, 1patient with severe and 3 patients with moderateneglect, were anosognosic for the de®cit. Twopatients showed late impairment of their awarenessof neglect. At the 10-day and 3-month examinationsthey correctly reported that they had problemsobserving the left side, but at the 1-year examinationthey were unaware of their obvious neglect.
Patients who were unaware of illness in the acutephase had poorer functional outcome (FrenchayActivities Index (18, 19)) at the 1-year follow-upthan patients who were aware of illness(t(48)=4.064, P=0.000). Similarily, patients withacute anosognosia for hemiparesis had a poorerfunctional outcome 1 year after onset than patientswho were aware of their hemiparesis in the ®rstexamination (t(12)=2.513, P=0.027). However,patients who were anosognosic for neglect in theacute stage did not differ from patients who wereaware of neglect in the ®rst examination with respectto their functional outcome at the 1-year follow-up.
Discussion
In our consecutive series of 56 right hemispherestroke patients, anosognosia for neglect and ano-
sognosia for hemiparesis double-dissociated, as didanosognosia for neglect and unawareness of illness.These results are in line with the view (based mainlyon previous ®ndings of simple dissociations in groupstudies or observations on individual patients) thatanosognosia is not a unitary phenomenon resultingin poor awareness of most or all co-occurringde®cits, but unawareness of a defect could occurindependently of awareness or unawareness of otherdefects (4).
Whether patients detect and become aware ofspeci®c defects depends presumably on the salienceand severity of the defects. For instance, it might beeasier for patients to detect their motor impairmentsthan visual ®eld defects. Bisiach et al. (5) observedanosognosia for visual ®eld defect (28/32; 88%) morefrequently than anosognosia for motor impairment(12/36; 33%). Severe defects are probably realizedmore frequently than mild defects. Since the severityand salience of relevant defects varies from patientto patient, a simple dissociation of correspondinganosognosias is not a completely convincing basisfor the conclusion that these anosognosias arespeci®c and independent from one another, becausea general or unitary impairment of unawareness ofdefects could result in simple dissociations ofanosognosias.
A double-dissociation of anosognosias provides amore solid basis than a mere dissociation for theconception that there are different and to someextent independent anosognosias for differentdefects rather than a unitary general unawarenessof de®cits. In our series, the double-dissociations ofanosognosias could hardly be explained by thedifferential severity of neglect or hemiparesis. All thespeci®c de®cits involved in the double-dissociationsof anosognosias were at least moderate, and in eachof the subgroups of the double-dissociations at least1 patient had a severe disorder. Four patients hadanosognosia for severe hemiparesis without ano-
Table 5. The comparison of patients who were aware (A) to those who were unaware (UA) of illness, neglect or hemiparesis on variables that could affect awareness of defects
General awareness of illness Neglect patients Patients with hemiparesis
CA (n=50) UA (n=6) CA (n=7) UA (n=14) CA (n=11) UA (n=8)
Mean (SD) Mean (SD) Mean (SD) Mean (SD) Mean (SD) Mean (SD)
Age 63.0 (10.6) 65.5 (6.5) 62.9 (9.8) 60.7 (11.1) 57.6 (12.4) 66.1 (6.6)
Orientation 4.7 (0.7) 4.2 (1.0) 4.9 (0.4) 4.1 (1.0)* 4.5 (0.9) 4.4 (0.9)
Logical memory 20.5 (6.1) 14.0 (6.0)** 22.3 (8.6) 17.9 (5.9) 20.1 (7.0) 14.4 (6.5)
Neglect (BITC) 126.9 (33.7) 62.0 (57.4)* 55.9 (56.1) 96.1 (40.3) 114.3 (40.9) 43.6 (43.6)**
Hemiparesis 1.9 (3.2) 4.0 (3.5) 5.9 (3.1) 3.2 (3.6) 5.9 (2.3) 6.9 (1.6)
Hemianopia 9 4 3 4 0 4
Size of infarction (cm3) 53.2 (74.5) 114.0 (97.1) 151.0 (122.9) 111.1 (76.0) 68.6 (82.5) 174.8 (117.8)*
Abbreviations: Neglect: sum score of the 6 conventional tests of the Behavioural Inattention test, BITC (range: 0±146; 0=minimum; 146=maximum; cut-off for neglect: j129).Orientation: raw score of the WMS Orientation subtest (range: 0±5; 0=disorientation; 5=intact orientation). Logical memory: raw score of the WMS Logical Memory subtest(range: 0±46). Hemiparesis: NIH Stroke Scale sum score for the paresis of the leg and the arm (range: 0±8 points; 0=no motor dysfunction; 8=severe hemiparesis). Statisticallysigni®cant differences between A and UA patients: * P<0.05 or ** P<0.01.
Jehkonen et al.
382

sognosia for severe neglect, and 3 patients hadanosognosia for neglect (1 severe and 2 moderate)without anosognosia for hemiparesis (2 severe and 1moderate).
The double-dissociation of anosognosia forneglect and unawareness of illness is a somewhatparadoxical ®nding, as one might assume thatgeneral unawareness of illness implies or includesanosognosias for speci®c de®cits. Only 6 patientsanswered inadequately one or both of the interviewquestions concerning awareness of illness (``Why areyou here?'' and ``What is wrong with you?''). All ofthem were neglect patients, and 2 of them wereaware of their neglect. These 2 patients answeredadequately that they had dif®culties observing theleft side of the space, but failed to realize that itmeant something was wrong with them and that thiswas why they were at the clinic. In this sense theywere unaware of illness, but aware of neglect.
Ten patients were anosognosic for their neglectbut aware of their illness. This is not surprising,because awareness of illness does not imply aware-ness of each of the de®cits associated with an illness.These observations suggest that anosognosias forspeci®c defects and general unawareness of illnesscould be independent impairments of awareness.Another possible explanation is that patients whowere confused or had general attentional orcognitive impairment were inclined to give unrea-listic, inconsistent and unreliable answers in theanosognosia interview. These two explanations arenot necessarily contradictory, but they may in factbe complementary.
Patients who showed unawareness of illness hadpoorer verbal memory than other patients. A similarpattern was observed when patients with anosog-nosia for neglect or anosognosia for hemiparesiswere compared to patients who were aware of theirneglect or hemiparesis, respectively. The groupscompared were small and the differences were notstatistically convincing. Nevertheless, the differ-ences were in line with the view that generalcognitive dysfunction decreases awareness of de®-cits. Those patients whose awareness of illness orawareness of hemiparesis improved during thefollow-up showed more improvement in verbalmemory than patients whose awareness did notimprove. This lends further support to the view thatan improvement of general cognitive functioningincreases general awareness of de®cits.
On the other hand, each of the 4 subgroups ofpatients which showed the 2 double-dissociations inour study included at least 1 patient whoseperformances in the Orientation and LogicalMemory subtests were normal. Therefore thedouble-dissociations cannot be explained simply
by reference to demented or confused patients'unreliable answers to the anosognosia interview.Consequently, general cognitive dysfunction couldnot be the sole explanation for unawareness ofde®cits. These ®ndings demonstrate that anosogno-sias could be independent and speci®c impairmentsof awareness. Although general cognitive disorderimpairs awareness of de®cits, patients with appar-ently normal cognitive capacity could also beunaware of considerable defects.
Pedersen et al. (2) found that anosognosia (forhemiparesis and/or visual ®eld defect) predicts poorshort-term outcome after stroke. Our results lendpartial support to this ®nding: unawareness of illnessand anosognosia for hemiparesis predicted poorfunctional outcome after a 12-month follow-up.However, anosognosia for neglect did not have clearprognostic value. Our previous result (19) indicatedthat acute neglect is a strong predictor of poorfunctional outcome, but the present ®ndings suggestthat anosognosia for neglect does not improve theprediction among patients with acute neglect.
The most important result of this study was thatunawareness of illness and anosognosia for hemi-paresis disappeared completely within 3 months ofstroke. Three months after onset, these transientanosognosias could not be direct causes of poorfunctional recovery. However, it is likely that acuteanosognosias and especially unawareness of illnessare associated with other, more persistent de®citsand general cognitive disorders which hinderrecovery. Therefore acute and transient anosogno-sias could predict poor outcome 1 year after stroke.
Acknowledgements
This study was supported by grants from the Medical ResearchFund of Tampere University Hospital, the Finnish CulturalFoundation, the Scienti®c Research Fund of the City of Tampereand the Finnish Graduate School of Psychology.
References
1. CUTTING J. Study of anosognosia. J Neurol NeurosurgPsychiatry 1978;41:548±55.
2. PEDERSEN PM, JOÈ RGENSEN HS, NAKAYAMA H, RAASCHOU HO,OLSEN TS. Frequency, determinants, and consequencesof anosognosia in acute stroke. J Neuro Rehab 1996;10:243±50.
3. BISIACH E, GEMINIANI G. Anosognosia related to hemiplegiaand hemianopia. In: PRIGATANO GP, SCHACTER DL, eds.Awareness of de®cit after brain injury. Clinical and theoret-ical issues. New York: Oxford University Press, 1991:17±39.
4. MCGLYNN SM, SCHACTER DL. Unawareness of de®cits inneuropsychological syndromes. J Clin Exp Neuropsychol1989;11:143±205.
5. BISIACH E, VALLAR G, PERANI D, PAPAGNO C, BERTI A. Un-awareness of disease following lesions of the right hemi-sphere: anosognosia for hemiplegia and anosognosia forhemianopia. Neuropsychologia 1986;24:471±82.
Unawareness of de®cits after right hemisphere stroke
383

6. BISIACH E, VALLAR G. Hemineglect in humans. In: BOLLER F,GRAFMAN J, eds. Handbook of Neuropsychology. Amster-dam: Elsevier Science Publishers, 1988:195±222.
7. ROBERTSON IH, HALLIGAN PW. Spatial neglect: A clinicalhandbook for diagnosis and treatment. Hove: PsychologyPress Ltd, 1999:19±40.
8. AZOUVI P, MARCHAL F, SAMUEL C et al. Functional conse-quences and awareness of unilateral neglect: a study of anevaluation scale. Neuropsychological Rehabilitation 1996;6:133±50.
9. PEDERSEN PM, JOÈ RGENSEN HS, NAKAYAMA H, RAASCHOU HO,OLSEN TS. Hemineglect in acute stroke ± incidence andprognostic implications. The Copenhagen Stroke Study. AmJ Phys Med Rehabil 1997;76:122±7.
10. GIALANELLA B, MATTIOLI F. Anosognosia and extrapersonalneglect as predictors of functional recovery following righthemisphere stroke. Neuropsychological Rehabilitation 1992;2:169±78.
11. WILSON B, COCKBURN J, HALLIGAN P. Behavioural InattentionTest. Titch®eld, UK: Thames Valley Test Company, 1987.
12. WILSON B, COCKBURN J, HALLIGAN P. Development of abehavioural test of visuo-spatial neglect. Arch Phys Med1987;68:98±102.
13. HALLIGAN P, COCKBURN J, WILSON B. The behavioural assess-ment of visual neglect. Neuropsychological Rehabilitation1991;1:5±32.
14. WECHSLER D. A standardised memory scale for clinical use. JPsychology 1945;19:87±95.
15. GOLDSTEIN LB, BERTELS C, DAVIS JN. Interrater reliability ofthe NIH Stroke Scale. Arch Neurol 1989;46:660±2.
16. BRODERICK JP, BROTT TG, DULDNER JE, TOMSICK T,HUSTER G. Volume of intracerebral hemorrhage. A power-ful and easy-to-use predictor of 30-day mortality. Stroke1993;24:987±93.
17. SPSS for Windows 9. 0. Chicago: SPSS Inc, 1999.18. HOLBROOK M, SKILBECK CE. An activities index for use with
stroke patients. Age Ageing 1983;12:166±70.19. JEHKONEN M, AHONEN J-P, DASTIDAR P et al. Visual neglect as a
predictor of functional outcome 1 year after stroke. ActaNeurol Scand 2000;101:195±201.
Jehkonen et al.
384