Embed Size (px)
Citation preview

Umbilical artery flow velocity waveforms and placentalresistance: The effects of embolization of theumbilical circulation
BrianJ.Trudinger, M.D., Denise Stevens, B.Se., Anita Connelly, B.Se.,J. Robert S. HaIes, Ph.D., George Alexander, D.Se., Laurenee Bradley, B.Se.,AIan Faweett, B.Se., and Rosemary S. Thompson, Ph.D.
Westmead and Prospect, New South Wales, Australia
Embolization of the umbilicaf placental circulation in fetal lambs was carried out to occlude the smaU
vessels of the placental vascular bed and to observe the effect on the umbilical artery flow and flowvelocity waveforms. Thirteen singleton fetuses were studied from day 120 of pregnancy. Embolization wasachieved by injecting approximately 9 x 106 microspheres of 15 p.m diameter into the fetal pfacentaI
cotyledons along the umbilical arteries over 9 days. Umbilical and uterine flows were measured by
radioactive microsphere counting. The umbilical placental resistance was increased (0.25 to 0.35 mmHg' ml . mirr ') by embolization, and there was an increase in the umbilical artery systolic/diastolic ratio.
Embolizalion produced a significant fall in umbilical flow expressed either as totaillow (312 to 237ml· min ") or when normalized by reference against splanchnic f10w (3.36 to 1.53). We conclude that the
umbilical artery flow velocity waveform systolic/diastolic ratio measures the reflection coefficient at theperipheral vascular bed (the "resistance vessels") of the placenta. (AMJ OBSTET GVNECOL 1987;157;1443-8.)
Key words: Umbilical blood flow, flow velocity waveforms, embolization, Doppler uItrasound
Studies of umbilical artery flow velocity waveformsin normal human pregnancy' indicate a pattern of highdiastolic flow velocity (point B) relative to the systolicpeak velocity (point A) (low AlB or peak systolic to leastdiastolic ratio). With advancing gestational age the ratioof peak systolic to least diastolic velocity (AlB) decreases. This pattern has been assumed to be due tothe low resistance of this vascular bed. Umbilical circulation resistance has been clirectly measured in ovinepregnancy'" and founel to decrease with increasing gesrational age.
The umbilical artery velocity waveform pattern isquite different in situations of antenatal fetal compromise, as indicated by subsequent birth of a small forgestational age infant. The diastolic flow velocity (B) islow relative to the systolic peak velocity (A), so that thesystolic/diastolic (AlB) ratio is high. 1.1.3 A placental rni-
From the Fetal Welfare Laboratory, Department or Obstetncs andGynaecology, University of Sydney at Westmead Hospital, and theIan Clunies Ross Animal Research Laborator», CommonwealthScientific and Industrial Research Organization.
This work was supported by the joint University of Sydney-Commonwealth Scientific and Industrial Research Organization ResearchFund and National Health and Medical Research Council ofAustralia.
Presented at the Thirty-third Annual Meeting of the Society for Gynecologic Investigation, Toronto, Ontario, Canada, March 19-22,1986.
Reprint requests: Brian j. Trudinger, Department of Obstetrics andGynaecology, The University of Sydney at Westmead Hospital,Westmead, New South Wales 2145, Australia.
crovascular cerrelative study has elemonstrated a lossof small arteries in the tertiary villi of the placentae ofhuman patients exhibiting a high systolic/diastolic(AlB) velocity ratio." The loss of these vessels would beexpected to increase resistance, because they are theresistance vessels of the fetal placental circulation.
Our purpose was to examine the relationship between umbilical artery flow velocity waveforms anelboth volume blood flow and resistance in the umbilicalcirculation of sheep. Experimental alteration in resistance was produced by a technique of microsphere ern
bolization of the fetal umbilical cotyleelonary circulation. Embolization of the ovine maternal uteroplacentalcirculation with microspheres has been used to alterresistance and decrease fiOW7. , O to provide an experimental model offetal growth retardation. Embolizationof the umbilical placental circulation has not been previously reported.
Material and methods
Proparation of animals, Thirteen ewes of knownmating date were surgically prepared between days 115anel 120 of gestation. The ewes were fasted for 24 hoursbefore the operation. Anesthesia was induced withI gm of thiopenral, the ewe was intubateel, and anesthesia was maintained by inhalation of a nitrousoxiele/oxygen with fluothane mixture. All surgery wasdone by use of an aseptic technique. The uterus wasfirst exposed by a mielline incision, the fetal Iamb waspalpated, and a small incision was made in the uterus
1443
1444 Trudinger et al. December 1987Am J Obstet Gynecol
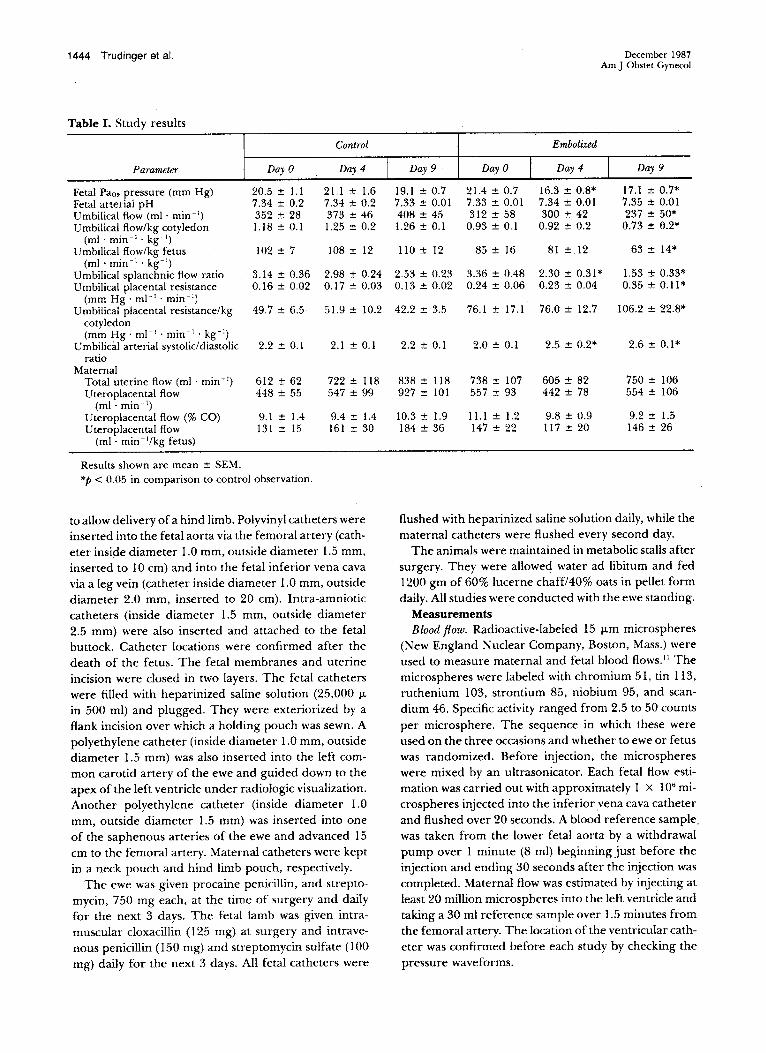
Table I. Study results
Control Embolited
Parameter Day 0 I Day 4 I Day 9 DayO I Day 4 I Day 9
Fetal Pa". pressure (mm Hg) 20.5 :!: l.l 21.1 :!: 1.6 19 .1 :!: 0 .7 21.4 :!: 0 .7 16.3 :!: 0 .8* 17.1 :!: 0 .7*Fetal arterial pH 7.34 :!: 0 .2 7.34:!: 0.2 7.33 :!: 0 .01 7.33 :!: 0 .01 7.34 :!: 0 .01 7.35 :!: 0 .01Umbilical ftow (rnl : min") 352 :!: 28 373 :!: 46 408 :!: 45 312 :!: 58 300 :!: 42 237 :!: 50*Umbilical ftow/kg cotyledon 1.18 :!: 0.1 1.25 :!: 0.2 1.26 :!: 0.1 0.93 :!: 0.1 0.92 :!: 0.2 0.73:!: 0.2*
(rnl : min" . kg- I)Umbilical ftow/kg fetus 102 :!: 7 108:!: 12 110 :!: 12 8 5 :!: 16 81 :!: 12 63 :!: 14*
(rnl : rnin " . kg- I)Umbilical splanchnic ftow ratio 3.14 :!: 0 .36 2.98 :!: 0 .24 2.53 :!: 0 .23 3.36 :!: 0.48 2.30 :!: 0 .31* 1.53 :!: 0 .33*Umbilical placental resistance 0.16 :!: 0 .02 0.17 :!: 0.03 0.13:!: 0.02 0.24 :!: 0 .06 0.23 :!: 0 .04 0.35 :!: 0 .11*
(mm Hg ' mi-I. min")Umbilical placental resistance/kg 49.7 :!: 6 .5 51.9 :!: 10 .2 42.2 :!: 3.5 76.1 :!: 17.1 76.0 :!: 12.7 106 .2 :!: 22.8*
cotyledon(mm Hg ' mI-I. rnin " . kg-')
Umbilical arteria l systolic/diastolic 2.2 :!: 0 .1 2.1 :!: 0 .1 2.2 :!: 0 .1 2.0 :!: 0 .1 2.5 :!: 0 .2* 2.6:!: 0.1*ratio
MaternalTotal uterine ftow (rnl : min- I) 612 :!: 62 722:!: 118 838 :!: 118 738:!: 107 605 :!: 82 750 :!: 106Uteroplacental ftow 448 :!: 5 5 547 :!: 99 927 :!: 101 5 57 :!: 93 442 :!: 7 8 554 :!: 106
(mi · min- ')Uteroplacental ftow (% CO) 9.1 :!: 1.4 9.4 :!: 1.4 1O.3:!: 1.9 11.1 ::!: 1.2 9.8 :!: 0 .9 9.2 ::!: 1.5Uteroplacental ftow 131 ::!: 15 161 ::!: 30 184 :!: 36 147::!: 22 117 ::!: 20 146 :!: 26
(ml - min-' /kg fetus)
Results shown are mean ::!: SEM.*p < 0.05 in comparison 10 control observation.
to allow delivery of a hind limb. Polyvinyl catheters wereinse rted into the feta l aorta via the femoral artery (catheter inside diarneter 1.0 rnm, outside diameter 1.5 mrn ,inserted to 10 cm ) and into the fetal inferior vena cavavia a leg vein (cathete r inside diameter 1.0 mm, outsidediameter 2.0 mrn, inserted to 20 cm) . lntra-amnioticcatheters (inside diameter 1.5 mrn , outside diameter2.5 mm) were also inserted and attached to the fetalbu ttock. Cathete r locations were confirmed after thedeath of the fetus. The fetal me mbranes an d ute rineincision were closed in two layers. The fetal catheterswere filled with heparinized saline solution (25,000 11in 500 ml) and plugged. They were exteriorized by aflank incision over which a holding pouch was sewn . Apolyethylene catheter (inside diameter 1.0 mrn , outsidediameter 1.5 mm) was also inserted int o the left cornmon carotid artery of the ewe and guided down to theapex of the left ventricle under radiologie visualization.Another polyethylene catheter (inside diameter 1.0mm, outside d iameter 1.5 mm) was inserted into oneof the saphenous arteries of the ewe and advanced 15cm to the femoral artery. Maternal catheters were keptin a neck pouch and hind limb pouch, respectively.
The cwe was given procaine penicillin , and streptomycin, 750 mg each, at the time of surge ry and d ailyfor the next 3 days. The fetal lamb was given intramuscular cloxacillin (125 mg) at surgery and intravenous pcnicillin (150 mg ) and streptomycin sulfate (100mg) daily for the next 3 days. All fet al catheters were
flushed with heparinized saline solution daily, while thematernal catheters were flushed every second day.
The animals were rnaintained in metabolic stalls aftersurgery. T hey were allowed water ad libitum and fed1200 gm of 60 % lucerne chaff/40% oats in pellet formdaily. All studies were conducted with the ewe standing.
MeasurementsBlood ft ow. Radioactive-labeled 15 11m microspheres
(New England Nuclear Company, Boston, Mass.) wereused to measure maternal and fe tal blood flOWS. ' 1Themicrospheres were labeled with chromium 51, tin 113,ruthenium 103, strontium 85, niobium 95, and scandium 46 . Specific activity ranged from 2.5 to 50 countsper microsphere. The sequence in which these wereused on the three occasions and whether to ewe or fetuswas randomized. Before injection, the microsphereswere mixed by an ultrasonicator. Each fetal How estirnation was carried out with approximately 1 x 106 microspheres injec ted into the inferior vena cava catheteran d flushed ove r 20 seconds. A blood reference sam plewas taken from the lower fetal aorta by a withdrawalpump over 1 rninute (8 ml) beginning just before theinjection and ending 30 seconds after the injection wascompleted. Maternal flow was estimated by injecting atleast 20 million microspheres into th e left ventricle andtaking a 30 ml reference sam ple over 1.5 minutes fromthe femoral artery. The location of the ventricular catheter was confirmed before each study by checking thepressure waveforms.
Volume 157Num ber 6
Embolization of umbilical circulalion 1445
1.5
t
,EllaoUIATlON
t t ti i• •
t tl ~
lTUDY DAY
,s
tttj
o
• ........ ~ .
r------------------,------------------------1..
.. • -------------------1..,. . . .,.• _lKltY
DAY 111-tlO
J •
.2
Fig. 1. Mean ( :!:SEM) results of the fetal stud ies in the controlgroup and in those in whom the umbilical arte ries were ernboIized dai ly. Significant d ifferences (p< 0.05) between thecontroI and embolized groups are shown (*).
e= CONTROL (n ~7)
•• DAILY UMS. A.EMBOL'N (n ~ e)
were recorded by a pressure transducer (Bell and Howeil , Pasa dena, Ca lif.) and a record er (Model M19, Devices, Ca mb ridge, Eng land). Mate rnal and fetal heartra tes were de te rmined from the arterial pressu rewaves. Blood gases and pH were measured by a bloodgas analyzer (Rad iometer, Co penhagen, Denmark ).
Experimental protocol. The stud y began 4 to 7 daysafter su rgery, with seven contro! and six animals to beembolized. Blood flow with radioactive microsphereswas measured at the sta rt of the study and repeated ondays 4 and 9 of the ex per imental period . B100d sam pieswere ta ken from the ewe an d fetus for blood gas analysis just before these measu rements. Umbilical arteryflow velocity waveforrns were recorded daily.
I n the umbilical ar tery embolization group, approx-
At the end of the experiment th e ewes were killedwith an overd ose of pentobarbitaI sodi um (600 mg),and tissues of interest were dissected, weighed , homogenized, and placed in preweighed count in g vials.T he uterus (myometrium and endometriurn), fetalmernbran es, and fe tal organs were treated in a similarmanner. The cotyledons were counted indi vid ua lly toconfirm uniform distri bution of microspheres to thecotyledons and th e results were totaled .
Reference blood an d tissue sam pIe vials were countedin conjunction with sta ndard and bac kground vials inan au to ma ted ga mma co unter, and nu clid e separationwas performed by computer. Flow was calculated as:(Number of microspheres per gram times referencesam pie flow rate) d ivided by Number of microspheresin reference sampie. Umbi lical Row in the two grou pswas also normalized by expression as a ra tio to the totalsplanchnic Row. Splanchnic flow was calcu lated as thetotal of liver, spleen, pancr eas, kidney, sto rnach, andintestine flows. Becau se the referen ce sam pie fo r micros phere determination of blood flow was taken fromthe lower aorta, flow to these organs was accuratelyrneasured .
Tot al absolute resistance in the umbil ical bed wascalcu lated as th e quotient of mean arterial pressureminu s central (inferior vena cava) venous pressure an dto tal flow. Resistan ce was also calculated per kilog ra mcotyledonary ma ss.
Umbilical artery flow velocity waveforrn recording. A4 MH z continuous wave Doppler tra nsducer and direction al Doppler blood velocimeter was used (ModelD 10, Med asonics, Mou ntain View, Calif.). With the ewesta nding, contact jelly was spread over the lower ab domen and the tran sducer searched until the characteristic fetal umb ilical artery waveform sound washe ard . Fetal and maternal signa ls were d istingu ishedby checking the hear t rate . The umbilical artery signalcould be d isplayed along with the umbil ical vein signa lwith flow in the opposite direction, I t could be dis tingu ished au di bly and visually from signa ls of the fe talao rta . T his fea ture was used in recogn ition. Unlike Rowin intra-abdominal great veins , Row in the umbilicalvein does not show cardiac pulsations . Umbilical arterywaveforms were recorded fro m at leas t foul' sites foreach study, The data were rec orded and sto red on audiota pe to permit lat er measurement after spee rrumanalysis (Medasonics SP25) display. Reco rd ings of seleered study pe riods were transferred to ultraviolet paper (Mod el FO R 1002 fibe ro ptic recorder, Medelec,Woking, England) 01' Polaroid film for measu rement.T he peak systo lic and least diastolic flow velocities weremeasured and their ratio calcu lated by averaging theratio from each site du ring the study period .
Miscellaneous. Arterial venous and arnniotic pressures
1446 Trudinger et al.
SHEEP No. 556
3
•0
fi •• CI: • • •I- ~ • •~~2~< •<-(.)1--Ul:<m-::E~~I- EMBOLISATION~ 1Ul t t t t t t t t t
T i2 3 4 5 6 7 6 9
STUDY DAY
Decemb er 1987Am J Obs tet GynecoI
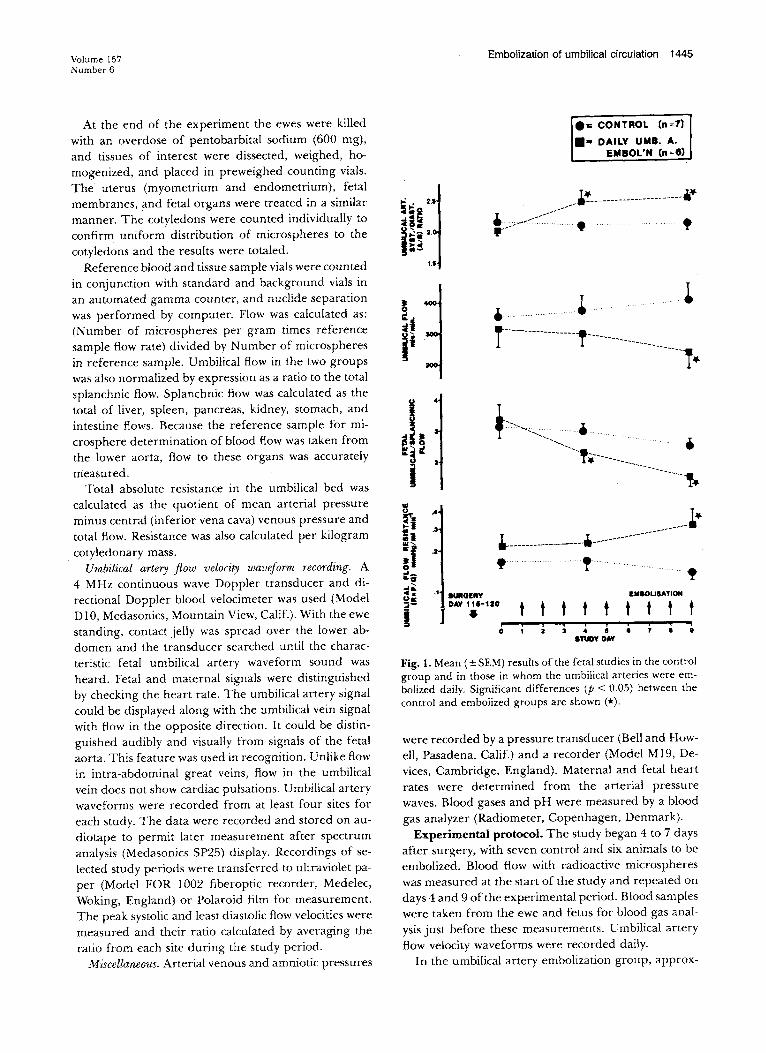
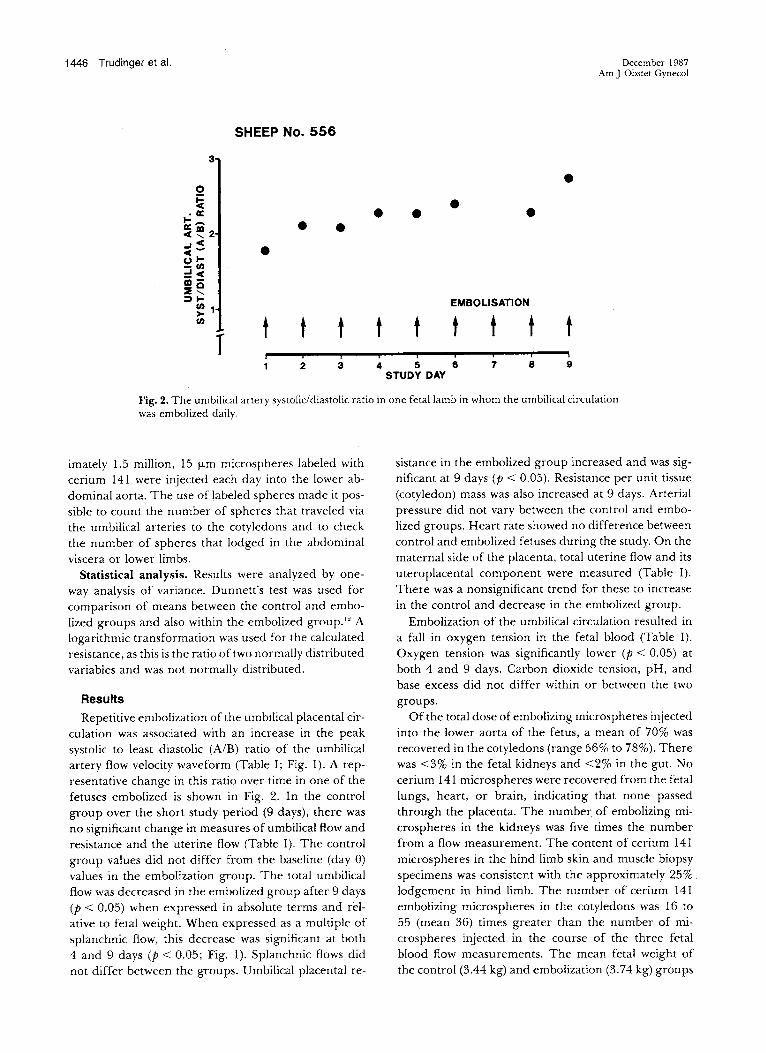
Fig. 2. The umbil ical artery systolic!diastolic rati o in one fetallamb in whom the umbilical circulationwas embolized da ily.
imately 1.5 million , 15 J.Lm microspheres labeied withcerium 141 were injected each day into the lower abdominal aorta. The use of labeied spheres made it possible to count the number of spheres tha t traveled viathe um bilical arteries to the cotyledo ns and to checkthe number of spheres that lodged in the abdominalviscera or lower limbs.
Statistical analysis. Results wer e ana lyzed by oneway an alysis of va riance . Dunnett's test was used forcompa rison of means between the control and ernbolized groups and also with in the embolized group. " Alogarithmic transformation was used for the caiculatedresistance, as this is the ratio oftwo normally distributedvariables and was no t normally distributed .
Results
Repetitive embolization of the umbilical placental cir culation was assoc iated with an increase in the peaksystolic to least diastolic (A l B) ratio of the umbilicalartery Aow velocity waveform (T able 1; Fig. I). A representative change in thi s ratio over time in one of thefetuses embolized is sho wn in Fig. 2. In the controlgroup over the short study period (9 days), there wasno signifi cant change in measures of umbilical Aowandresistance and the ut erine Aow (T able I). The controlgroup values did not d iffer frorn the baseline (da y 0)values in th e embolization gro up. T he tot al umbilicalAow was d ecreased in the embolized grou p afte r 9 days(p < 0.05) when expressed in absolu te te rms and relative to fet al weight. Wh cn expressed as a multiple ofsplanchnic Aow, this decrease was significant at bot h4 and 9 days (p < 0.05; Fig. 1). Spl an chnic flows didnot differ between the gro ups. Um bilical placental re-
sistance in the embolized gr oup increased and was significant at 9 days (p < 0.05). Resistance per unir tissue(cotyledon ) mass was also increased at 9 days. Arterialpressure d id not vary between the cont ro l and ernbo
lized gr oups. Heart rate showed no difference betweencontrol and embolized fetuses during the study. On thematernal sid e of the placenta , tot al uterine Aow and itsuteroplacental compo nen t were measured (Table I).There was a nonsignificant trend for these to increasein the contro l and decrease in the embolized group.
Embolizarion of the umbilical circulat ion resulted ina fall in oxygen ten sion in the fetal blood (Table I).Oxygen tension was significantly lower (P < 0.05) atboth 4 and 9 days. Carbon dioxide ten sion, pH, andbase excess did not d iffer wirhin or bet ween the twogroups.
Of the total dose ofembolizing microspheres injectedint o the lower aorta of the fetus , a mean of 70% wasrecovered in the cot yledon s (range 56% to 78%). Therewas < 3% in the fetal kidneys and < 2% in the gut. Nocerium 14 I micro spheres were recovered from the fetallungs, heart, or brain , indicating that none passedthrough the placenta. The number of embolizing microspheres in the kidneys was five time s the numberfrom a flow measurement. The content of cerium 141microspheres in th e hind limb skin and muscle biopsyspecimen s was con sistent with the approxim ately 25 % .lodgemcnt in hind limb. The number of cerium 141embolizing microspheres in the cotyled ons was 16 to55 (mean 36) tim es grcatcr th an th c nu rnbe r of microspheres inj ected in th e course of the thrcc fetalblood flow measurernents. The mcan fetal weight ofthe con trol (3.44 kg) and cmbolization (3.74 kg) groups

Volurne 157Num ber 6
did not differ significantly, and the fetal /cotyled onweight ratio was similar in the two groups.
Comment
Embolizarion of the umbilical circulation was carriedout to obliterate the peripheral arterial tree in the fetalcotyledon s and to observe the effect on umbilical placental flow velocity waveforms. These have been proposed as a simple ari d sensitive index of umbilical cir culation and rel ated to feta l weifare. I. U Umbilical placental resistance was increased by ernbolizati on .Embolization resulted in a change in the pattern of theumbilical flow velocity waveform, with an increase inthe systolicldiastolic ratio. There was a reduction in thevolurne flow in the umbilical circulation relative to thecontrol group in both absolute terms and when expressed as a multiple of the splanchnic circulation.There was no change in art erial pressure. This mayhave occur red had we continued furtherembolization .The d ata on visceral blood flow does not suggest ashutdown of vascular beds to improve urnbili cal flow.
The change in flow velocity waveform observed afterembolization corresponds to the change theoreticallypredicted as a result of increased peripheral or downstream resistance. With each cardiac irnpulse, pressureand flow waves travel out along the art erial tree. Waverefle ction occurs downstrearn at the site of a rte ria lbranches an d especially a t the Ievel of the "resistance"vessels." The extent of reflection (reflection coefficient)is increased by narrowing of these cha nnels" (red ucedcross-section area of res istance vessels of the vascularbed ). The waveform obse rved is the sum of the incidentand refle cted (negative) waves so that a reduced dia stolic component would be predicted if reflection isincreased. The systolicldiastolic (A lB ) ratio was suggested to quantitate thi s effect. Other indices used forthis purpose include the pulsatilit y index and the resistan ce index. We have compared these and sho wnthern to be very highly correlated in the umbilical circulation. "
The cha nge in the systolic/diastolic ra tio was significant at 4 da ys, but um bilical resistan ce was not significantly different until 9 days, These results illustratethe difference between calculated res istance (meanpressure difference/rnean flow) for steady flow and theflow velocity waveform res istance indices. T he latter arernor e directly deterrnined by the ext ent of wave reflec-
, tion at the periphery of th e arte rial tree rather thanresistan ce. Embolization could be expected to decreasethe cro ss-sectional area of the umbilical placental vascular bed and so increase reflectio n. Resistan ce may bedefined as the en ergy lost in forcing blood through thearterial tree ." This cne rgyloss iricludes compone ntsdue to thc pulsatile nature of bloodflow (this can be
Embolizat ion of umbilical circulatlon 1447
assessed by measuring impedance), the dimensions ofthe arterial tree and the viscoelasti c properties of itswalls (d istensibility), physical properties of the blood,and the reflected waves . The change in systolicldiastolicratio preceding the change in caJculated vascular resistance can be explained if there is an alteration in an yof the other factors affecting re sistance opposite to thewaveforrn refleetion effect, It is also possible that someof the effect of microsphere embolization ma y havebeen hidden by the cont inued grow th and expansionof the umbilical placental bed with gestational age . Thiswas the explanation sug gested when the same observations were made about the rnaternal uterine bloodflow after ernbolization of the matemal uteroplacentalbed." Against this explanation is the rise in the flowvelocity waveform systolic/diastolic (Al B) ratio wefound afte r embolization. It is also possible that thefetal cotyledon circul at ion has a greater potential foropening collateral ch annels than observed in someother tissues in' response to microsphere embolization.However, this explanation is not likely because there 'was a downward alterat ion in flow in the embolizedgroup.
There was a change in umbilical flow at 9 days th atwas not significant at 4 days, although the urnbilical/spl an chnic flow rati o was decreased . Evidence of thepreservat ion of umbilical flow despite an increase insystolic/dia stolic ratio in human pregn an cy exists." Volume flow in the thoracic ao rta and umbilical vein wascompared in human fetuses with su bsequent birthweight appropriate and sma ll-fo r-gestational age. Theumbilical flow was sho wn to be 40 % of ao r tic flow inappropriate for gestational age fetuses, but 21% in thesmall for gestational age group. The umbilical volumeflow was of the same magnitude in the two groups, yetthe systolic/diastolic rati o was increased in the small forgestation al age group. Similar findings were reportedin grow th-re ta rded fetal lambs." These observationssuggest an increase in card iac outp~L
The urnbili cal artery flow velocity waveforms are similar in normal ovine and human pregnancy. In humanpregnanc y the two urnbilical arteries run fro m the fetusto the placental disc. In ovine pregnancy the umbilicalvessels branch to the manycotyledons. For this reasonit is necessary to make multiple observations of theumbilical art ery at different sites to d er ive an ave ragedsystolicldiasto lic ratio.
We are not aware of any previous reports of embolizat ion of the umbilical circulation. Embo lization of th euterine circulation?.• has been used to pro vide a modelof feta l growth failure or asphyxia. Ligation of oneumbilical .ar tcrv has also been stud ied for a similarreas on . Because an alteration in umbilical flow velocity waveform as indicated by an increase in the sys-

1448 Trudinger et al.
tolicldiastolie (A l B) ratio is an early feature of fe talgrow th reta rd ation , with definite plaeental pathologiecor relation" and only some tim es a eoexistent altera tionin the uterine circ ulation ," umbi lieal artery em bolization may providea better model for the study of intrauterine growth reta rdation than does uterine ern
bolization. Our study pe riod (9 days) was too sho rt toaffeet signifieantly the feta l weight.
REFERENCES
I. T rudinger BJ, Giles WB, Coo k CM, Bombardieri J, Col!ins L Fetal umbilical artery fiow velocity waveforms andplacental resistance: Clini cal significa nce . BI'J Obstet Gynaecol 1985 ;92:23-30.
2. Dawes GS. The um bilical circulat ion . In : Fetal and neonatal ph ysiolog y. Chicago : Year Book , 1968:66-78 .
3. Rudolph AM,H eymann MA. Circulatory changes duringgrowth in the fetal lam b. Circ Res 1970;26:289-99.
4. Giles WB, Trudinger BJ, Cook CM. Umbilical artery velocity waveforms in pregnancy. J Ultrasound Med 1982;I(suppl):98.
5. Trudinger BJ, Giles WB, Cook CM. Flow velocity waveforms in the m ate rn al uteroplacental and fetal um bilicalplacental circ u larion , AM J OBSTET GYNECOL 1985;152 :155-63.
6. Giles WB, Trud inger BJ , Baird P. Fetal umbilical ar teryflow veloci ty waveforms and placental resistan ce : Pathological correlation. BI' J Obstet Gynae col 1985;92 :31-8 .
December 1987Am J Ob slei Gynecol
7. Creasy RK, Barren CT, de Swiet M, Kahan paa KV, Rudolph AM. Experim e ntal int ra-u ter ine growth retardation in the sheep. AM J OBSTET GYN ECOL 1972;1 12:566-73 . .
8. Clapp JF, McLa ughlin MK, Larrow R, Farnharn J , MannLI. The uterine haemod yna mic response 10 re pet itive unilateral vascular em bolizat iton in the pregn an t ewe. AMJOBSTET GVNECOL 1982;144 :309-18.
9. Block BSB, Llanos AJ , Creasy RK. Response o f the growthretarded fetu s to ac ute hypoxem ia . AMJ OBSTET GVNECOL1984;148:879-85.
10. Boyle J W, Lot gering FK, Longo 1.D. Acute emboliza tionof the utero placental circulation : uter ine blood flow andplacen tal CO diffusing ca pacity. J Dev Physiol 1984;6:377-86 .
11. HaIes J RS. Radioactive microsphere technique for studiesof the circulation. Clin Exp Pharmacol Physiol 1974;I(suppl 1):31-46.
12. Zar JH. Multiple compari so ns. In: Biostatistical analysis. En glewood Cliffs, New J ersey: Prentice-Hall , 1984 :185-98.
13. Harnilton WF. The pat tern s of the arteri al pressure pul se.Am J Ph ysiol 1944;14 1:235 -4 I.
14 . T ho mpson RS, T ru dinger BJ, Cook CM. A compari sonof Dop pler ult rasound wavefo rm ind ices in the umb ilicalartery. I. In d ices derive d fro m the maximum veloci tywavefor rn. Ultrasound Med Biol 1986;12.
15. Milnor WR. Pulsa tile blood flow, N Eng l J Med1 972;287 :27-34 .
16. Giles WB, Ling man G, Marsa l K, T rudinger BJ. Fetalvolume bloodflow and umbilical artery flow velocity waveform analysis: a comparison . BI' J Obstet Gynaecol1986;93:461-5.
Bound volumes available to subscribersBound volumes of the AMERICANJ OURNAL OF OBSTETRICS AND GYNECOLOGY are avai l
able to subseribe rs (only) für the 1987 issues from the Publisher, at a cost of $5 1.00 ($74.00int ernation al) for Val. 156 (january-J une) an d Vol. 157 (july-Deeember). Shi p ping eha rgesare included . Eae h bo un d volume con tains a su bjcet an d au thor index and all advertisingis re mov ed. Co pics are shipped within 60 days after pu blicati on of th e last issu e in th evolu me . T he bin di n g is durable buck ram with th e J OURNAL name, volume nu m ber, andyea r stamped in gold on th e spi ne . Payment must accompany alt orders. Contact T he C. V.Mosby Company, Circu lation Department, 11830 Westl ine Industrial Dr ive , SI. Louis,Missouri 63146, USA; ph one (800) 325-41 77, ex t. 35 1.
Subscriptions must be in force to qualify. Bound volumes are not available in placeof a regular JOURNAL subscrip tion .