Embed Size (px)
Citation preview

Actas Dermosifiliogr. 2014;105(10):891---899
REVIEW
Ultrasound Skin Imaging�
F. Alfageme Roldán
Servicio de Dermatología, Hospital Universitario Puerta de Hierro Majadahonda, Universidad Autónoma de Madrid, Madrid, Spain
Received 3 September 2013; accepted 24 November 2013Available online 4 November 2014
KEYWORDSEchography;Ultrasonography;Ultrasound skinimaging
Abstract The interaction of high-frequency ultrasound waves with the skin provides the basisfor noninvasive, fast, and accessible diagnostic imaging. This tool is increasingly used in skincancer and inflammatory conditions as well as in cosmetic dermatology. This article reviews thebasic principles of skin ultrasound and its applications in the different areas of dermatology.© 2013 Elsevier España, S.L.U. and AEDV. All rights reserved.
PALABRAS CLAVEEcografía;Ultrasonido;Ecografía cutánea
Ecografía cutánea
Resumen La ecografía cutánea es una técnica dermatológica de diagnóstico por imagenbasada en la interacción de los ultrasonidos de alta frecuencia con la piel. Su carácter noinvasivo, rápido y accesible hace que sus aplicaciones en la clínica sean cada vez más amplias,tanto en oncología cutánea como en afección inflamatoria o dermatología estética. En esteartículo se revisan los principios de la técnica y las aplicaciones en los distintos ámbitos de ladermatología.© 2013 Elsevier España, S.L.U. y AEDV. Todos los derechos reservados.
Introduction
Ultrasound skin imaging is a noninvasive diagnostic tech-nique in which the physical properties of ultrasound are usedto examine the skin and skin appendages.1
� Please cite this article as: Alfageme Roldán F. Ecografía cutánea.Actas Dermosifiliogr. 2014;105:891---899.
E-mail address: [email protected]
Both high-frequency (> 7 MHz) and very-high-frequencyultrasound (> 20 MHz) can provide a detailed diagnostic anal-ysis of the skin, as they offer sufficient resolution and depthto clearly identify skin structures.2
Application of the Doppler effect in ultrasound enablesthe visualization of physiological and pathological processesinvolving increased local blood flow, such as inflammationand neoangiogenesis.3
Ultrasound is a relatively new imaging modality in der-matology, and while more studies are needed to support its
1578-2190/© 2013 Elsevier España, S.L.U. and AEDV. All rights reserved.
Document downloaded from http://www.elsevier.es, day 06/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
892 F. Alfageme Roldán
EP
Der
Hyp
Fas
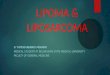
Figure 1 Structure of normal skin as seen on ultrasound. EPindicates epidermis; Der, dermis; Hyp, subcutaneous tissue; Fas,fascia.
integration into routine clinical practice, there is evidenceof its usefulness in different fields of dermatology.4
Normal Skin and Skin Appendages
In B-mode (bright mode) ultrasound imaging, the skin is seenas a series of lines and bands in varying shades of gray, black,and white that correspond to the different layers of the skin5
(Fig. 1).The epidermis appears as a hyperechoic line, or in certain
locations, such as acral sites, as a bilaminar hyperechoicline.6
The dermis also appears as a hyperechoic line but it isnot quite as echogenic as the epidermis. A more superficialhypoechoic area, corresponding to the papillary dermis, mayalso be seen.
Subcutaneous tissue appears under the dermal band asa network of hyperechoic lines that correspond to thesepta. Inside are hypoechoic areas that represent the fattylobules.1
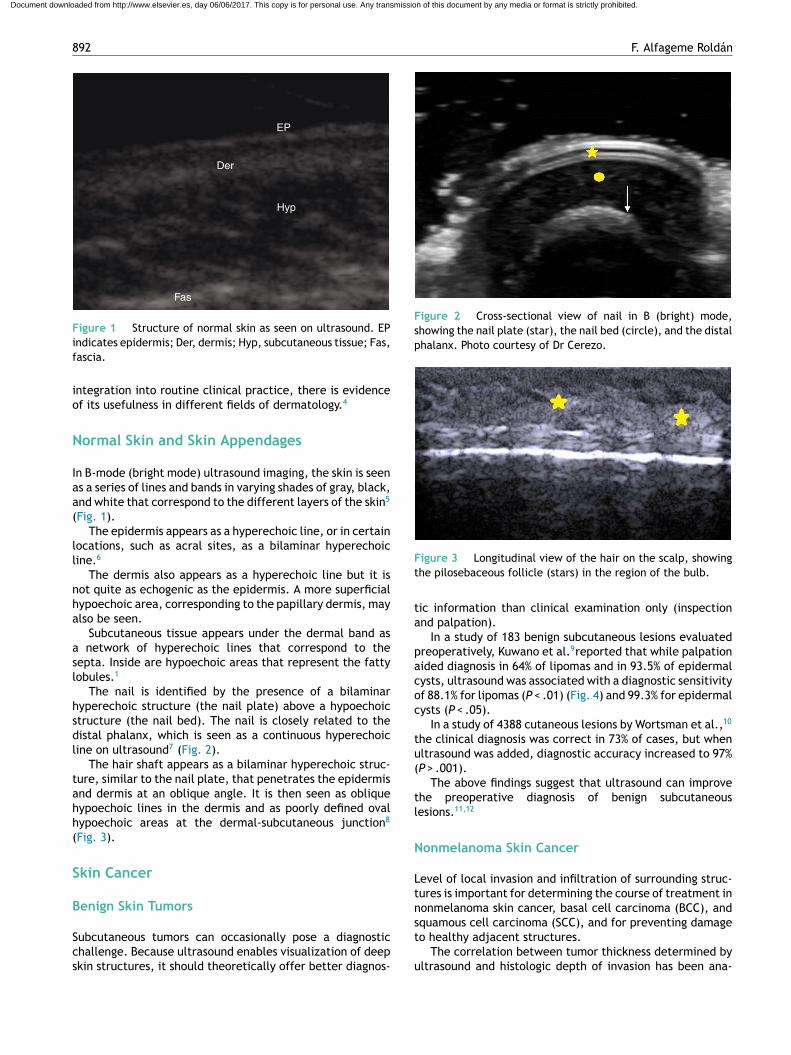
The nail is identified by the presence of a bilaminarhyperechoic structure (the nail plate) above a hypoechoicstructure (the nail bed). The nail is closely related to thedistal phalanx, which is seen as a continuous hyperechoicline on ultrasound7 (Fig. 2).
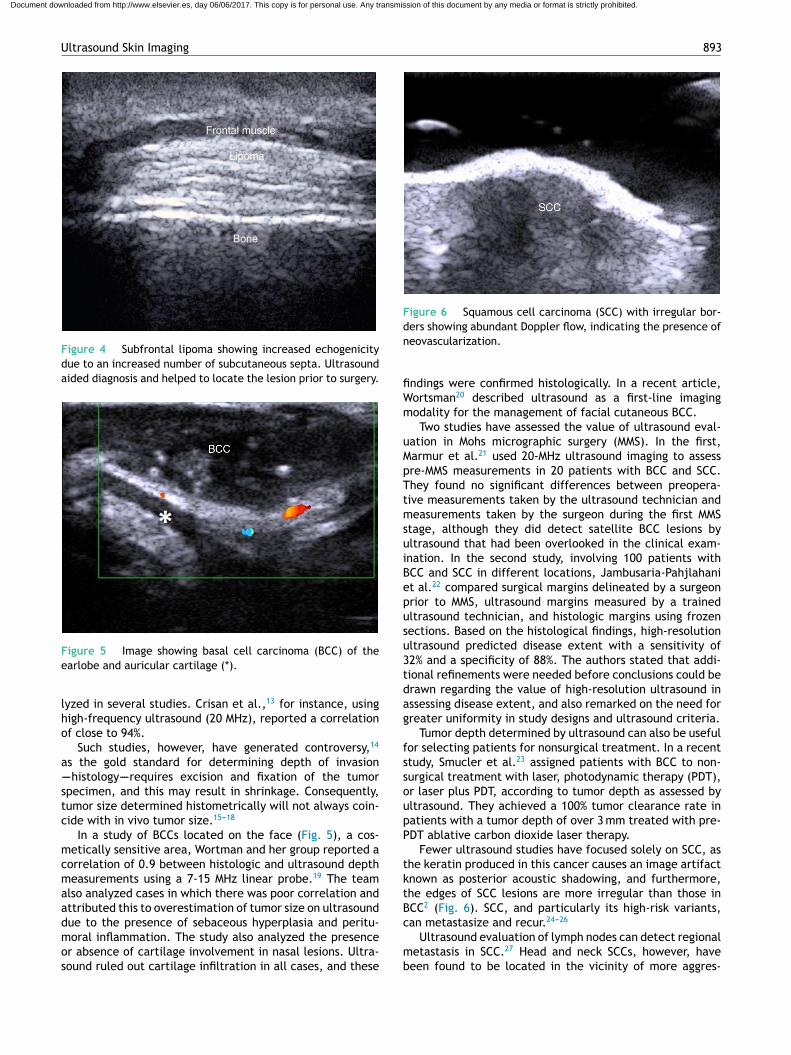
The hair shaft appears as a bilaminar hyperechoic struc-ture, similar to the nail plate, that penetrates the epidermisand dermis at an oblique angle. It is then seen as obliquehypoechoic lines in the dermis and as poorly defined ovalhypoechoic areas at the dermal-subcutaneous junction8
(Fig. 3).
Skin Cancer
Benign Skin Tumors
Subcutaneous tumors can occasionally pose a diagnosticchallenge. Because ultrasound enables visualization of deepskin structures, it should theoretically offer better diagnos-
Figure 2 Cross-sectional view of nail in B (bright) mode,showing the nail plate (star), the nail bed (circle), and the distalphalanx. Photo courtesy of Dr Cerezo.
Figure 3 Longitudinal view of the hair on the scalp, showingthe pilosebaceous follicle (stars) in the region of the bulb.
tic information than clinical examination only (inspectionand palpation).
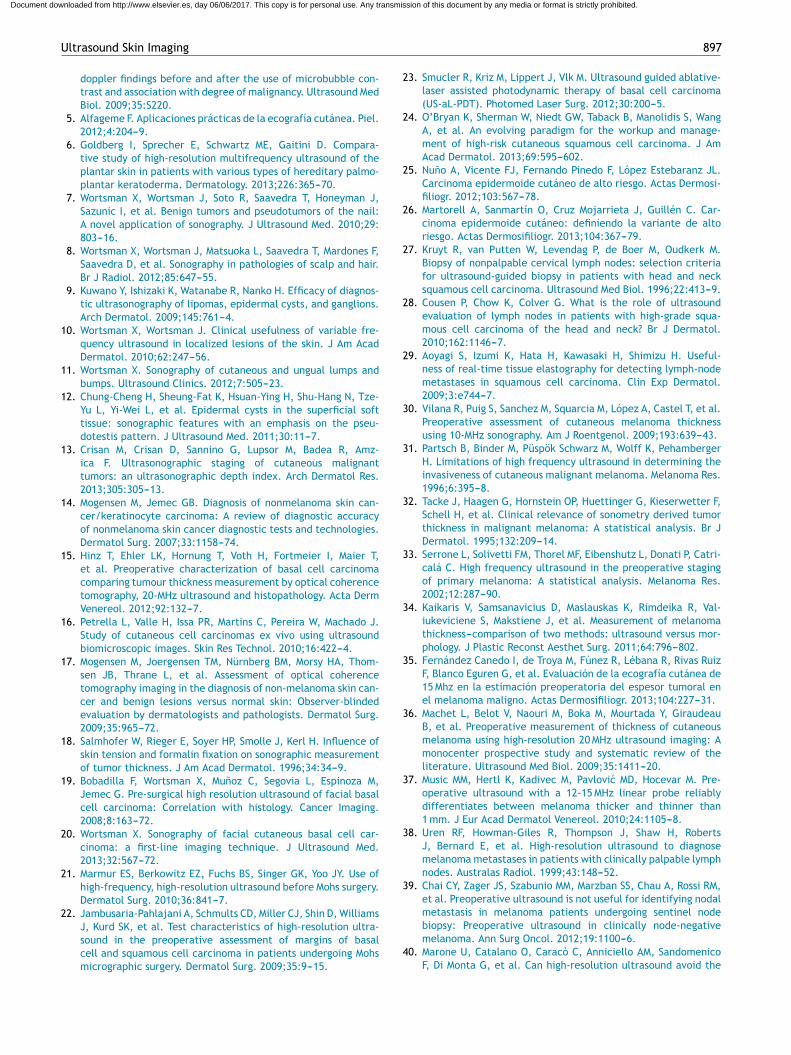
In a study of 183 benign subcutaneous lesions evaluatedpreoperatively, Kuwano et al.9reported that while palpationaided diagnosis in 64% of lipomas and in 93.5% of epidermalcysts, ultrasound was associated with a diagnostic sensitivityof 88.1% for lipomas (P < .01) (Fig. 4) and 99.3% for epidermalcysts (P < .05).
In a study of 4388 cutaneous lesions by Wortsman et al.,10
the clinical diagnosis was correct in 73% of cases, but whenultrasound was added, diagnostic accuracy increased to 97%(P > .001).
The above findings suggest that ultrasound can improvethe preoperative diagnosis of benign subcutaneouslesions.11,12
Nonmelanoma Skin Cancer
Level of local invasion and infiltration of surrounding struc-tures is important for determining the course of treatment innonmelanoma skin cancer, basal cell carcinoma (BCC), andsquamous cell carcinoma (SCC), and for preventing damageto healthy adjacent structures.
The correlation between tumor thickness determined byultrasound and histologic depth of invasion has been ana-
Document downloaded from http://www.elsevier.es, day 06/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Ultrasound Skin Imaging 893
Frontal muscle
Lipoma
Bone
Figure 4 Subfrontal lipoma showing increased echogenicitydue to an increased number of subcutaneous septa. Ultrasoundaided diagnosis and helped to locate the lesion prior to surgery.
Figure 5 Image showing basal cell carcinoma (BCC) of theearlobe and auricular cartilage (*).
lyzed in several studies. Crisan et al.,13 for instance, usinghigh-frequency ultrasound (20 MHz), reported a correlationof close to 94%.
Such studies, however, have generated controversy,14
as the gold standard for determining depth of invasion----histology----requires excision and fixation of the tumorspecimen, and this may result in shrinkage. Consequently,tumor size determined histometrically will not always coin-cide with in vivo tumor size.15---18
In a study of BCCs located on the face (Fig. 5), a cos-metically sensitive area, Wortman and her group reported acorrelation of 0.9 between histologic and ultrasound depthmeasurements using a 7-15 MHz linear probe.19 The teamalso analyzed cases in which there was poor correlation andattributed this to overestimation of tumor size on ultrasounddue to the presence of sebaceous hyperplasia and peritu-moral inflammation. The study also analyzed the presenceor absence of cartilage involvement in nasal lesions. Ultra-sound ruled out cartilage infiltration in all cases, and these
Figure 6 Squamous cell carcinoma (SCC) with irregular bor-ders showing abundant Doppler flow, indicating the presence ofneovascularization.
findings were confirmed histologically. In a recent article,Wortsman20 described ultrasound as a first-line imagingmodality for the management of facial cutaneous BCC.
Two studies have assessed the value of ultrasound eval-uation in Mohs micrographic surgery (MMS). In the first,Marmur et al.21 used 20-MHz ultrasound imaging to assesspre-MMS measurements in 20 patients with BCC and SCC.They found no significant differences between preopera-tive measurements taken by the ultrasound technician andmeasurements taken by the surgeon during the first MMSstage, although they did detect satellite BCC lesions byultrasound that had been overlooked in the clinical exam-ination. In the second study, involving 100 patients withBCC and SCC in different locations, Jambusaria-Pahjlahaniet al.22 compared surgical margins delineated by a surgeonprior to MMS, ultrasound margins measured by a trainedultrasound technician, and histologic margins using frozensections. Based on the histological findings, high-resolutionultrasound predicted disease extent with a sensitivity of32% and a specificity of 88%. The authors stated that addi-tional refinements were needed before conclusions could bedrawn regarding the value of high-resolution ultrasound inassessing disease extent, and also remarked on the need forgreater uniformity in study designs and ultrasound criteria.
Tumor depth determined by ultrasound can also be usefulfor selecting patients for nonsurgical treatment. In a recentstudy, Smucler et al.23 assigned patients with BCC to non-surgical treatment with laser, photodynamic therapy (PDT),or laser plus PDT, according to tumor depth as assessed byultrasound. They achieved a 100% tumor clearance rate inpatients with a tumor depth of over 3 mm treated with pre-PDT ablative carbon dioxide laser therapy.
Fewer ultrasound studies have focused solely on SCC, asthe keratin produced in this cancer causes an image artifactknown as posterior acoustic shadowing, and furthermore,the edges of SCC lesions are more irregular than those inBCC2 (Fig. 6). SCC, and particularly its high-risk variants,can metastasize and recur.24---26
Ultrasound evaluation of lymph nodes can detect regionalmetastasis in SCC.27 Head and neck SCCs, however, havebeen found to be located in the vicinity of more aggres-
Document downloaded from http://www.elsevier.es, day 06/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

894 F. Alfageme Roldán
Figure 7 Melanoma (M). Hypoechoic dermal-subcutaneousarea with abundant neovascularization.
sive tumors, such as those in the maxillofacial region.27 Inthe only preliminary study of head and neck SCC, Cousenet al.28 did not find postoperative ultrasound evaluation tobe of prognostic value in 47 patients with histologic grade 3and 4 SCC according to Broders’ classification. Perhaps newultrasound techniques, such as elastography, will improvedetection of very early stages of lymph node metasases.29
Melanoma
Breslow depth and the presence of local or distance metas-tases are prognostic indicators in melanoma and help toguide treatment.30(Fig. 7)
Two key factors influence the correlation between Bres-low depth measured by ultrasound and by histology: themean Breslow depth of the melanomas being studied and theultrasound equipment used.31 Although numerous studieshave been performed, a lack of uniformity in terms of equip-ment and criteria used to measure Breslow depth makes itdifficult to draw clear conclusions.32---34
Researchers at Hospital Costa del Sol in Marbella, Spainrecently published a study in which they analyzed 79 cuta-neous melanomas using a 15-Mhz ultrasound probe.35 Theyobtained a mean Breslow depth of 0.8 mm, and com-pared this with mean depth assessed histometrically. Theyreported moderate correlation for thin melanomas (< 1 mm)and lower correlation for thicker melanomas. Ultrasoundwas able to detect stage 1B melanomas with a sensitivity of82%, a specificity of 80%, a positive predictive power (PPV)of 54%, and a negative predictive power (NPV) of 94%.
In a review of 14 studies analyzing the correlationbetween melanoma thickness measured by ultrasound andby histology, Machet et al.36 reported correlation rates ofaround 0.9. Based on the findings of 7 studies with fullpatient data (869 patients in total), the authors reportedthat ultrasound-determined margins accurately predictedsurgical margins in 72% of cases.
Music et al.,37 in turn, studied 70 melanomas to seewhether ultrasound imaging with a probe of 12 to 15 MHzwould be capable of distinguishing melanomas thicker than1 mm. They reported sensitivity, specificity, PPV, and NPVvalues of 92%, 92%, 95%, and 81%, respectively, and con-cluded that ultrasound was a reliable means of distinguishing
between melanomas with a thickness of over 1 mm and thin-ner melanomas.
Ultrasound characteristics of enlarged lymphnodes----length to width ratio < 2, hyperechoic center,and absence of hilar vessels----can be used to distinguishbetween inflammatory nodes and nodes affected bymelanoma with a sensitivity of 100% and a specificity of96%.38
Sentinel lymph node biopsy (SLNB) is a technique usedto determine melanoma involvement in the sentinel lymphnode, which is the preferential site of metastasis in thisdisease. The technique involves the injection of radioac-tive isotopes, followed by surgery to remove the affectednode. Preoperative ultrasound has not proven to be supe-rior to SLNB for the identification of melanoma metastasis.39
On comparing ultrasound and SLNB in 623 patients withmelanoma, Marone et al.40 showed that ultrasound char-acteristics were predictive of nodal involvement with asensitivity of 15%, a specificity of 100%, a PPV of 100%, andan NPV of 87%.
However, in a study of 707 patients with melanoma whounderwent preoperative ultrasound assessment, patientswith negative lymph nodes on ultrasound had a lower tumorburden and longer overall survival than those with lymphnode metastases.41
In a study of 123 patients with melanoma that comparedpositron emission tomography and ultrasound in the detec-tion of sentinel lymph nodes, ultrasound identified 2 out of19 positive nodes, while PET detected none.42
Doppler ultrasound of melanomas also has a role to playin the assessment of cutaneous melanomas. Lassau et al.43
showed that detection of neoangiogenesis on ultrasound waspredictive of the metastatic potential of melanoma. In arecent study by Srivastava et al.44 of melanomas analyzedby Doppler ultrasound flowmetry (10 MHz), neovasculariza-tion and higher peak systolic frequency were found to bepredictive of survival at 15 years.
The introduction of new ultrasound contrast agents45 andultrasound elastography46 will probably lead to improvedcharacterization and detection of metastatic lymph nodes.Elastography, and in particular quantification of flow usingcontrast-enhanced ultrasound, can help to predict responseto chemotherapy in patients with advanced melanoma.47
Other Skin Tumors
Most of the studies on the use of ultrasound in otherskin tumors, such as dermatofibrosarcoma protuberans,48,49
Merkel cell carcinoma,50,51 and cutaneous lymphoma52,53 aremainly descriptive case series.
Inflammatory Skin Disorders
Ultrasound findings in inflammatory skin disorders include2:
• Hypoechogenic areas in the subepidermal portion of thedermis
• Increased local blood flow shown by Doppler ultrasound• Hypoechogenic septae when the subcutaneous tissue is
affected• Hyperechoic fatty lobules
Document downloaded from http://www.elsevier.es, day 06/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

Ultrasound Skin Imaging 895
Papillary dermis
Thenar muscles
Epidermis
Figure 8 Palmar psoriasis. Increased blood flow in hypoechoicsubepidermal area indicating inflammation.
The above characteristics help to determine the level andextent of inflammation in inflammatory disorders of the skin,hair, and nails.
Infectious Diseases
Ultrasound can be used to assess the extent of plantar wartsand to monitor treatment response in human papillomavirusinfections.54
Ultrasound assessment of abscesses has also becomewidespread in emergency departments in the United States.According to a report published by a pediatric emergencydepartment in Michigan, ultrasound evaluation led to achange in treatment strategy (drainage vs no drainage) in15% of cases that had been evaluated by physical exami-nation only.55 An additional advantage of ultrasound in thediagnosis of abscesses is that it can be performed with min-imal training.56,57
Psoriasis
Ultrasound characteristics of psoriasis include epidermaland dermal thickening and a subepidermal hypoechoic areawith increased blood flow (Fig. 8).58
These ultrasound findings, and in particular, dermalthickness, have been found to be correlated with dis-ease severity measured using the Psoriasis Area SeverityIndex and other scales assessing the severity or extent ofdisease.59,60
The effects of topical61 and systemic treatments59,62 forpsoriasis can be determined by analyzing changes to theabove-described ultrasound characteristics.
In a multicenter study by the Spanish RheumatologySociety, high-frequency ultrasound evaluation showed areduction in plaque thickness and Doppler signal intensityin the dermis of patients treated with infliximab.62
Nails appear thicker on ultrasound in patients with nailpsoriasis than in either healthy patients or patients withatopic dermatitis.63 Nail disease in psoriasis has been cor-related with the presence of enthesopathy, even in theabsence of clinical signs.63
In an ultrasound study investigating systemic inflam-mation in psoriasis, researchers at the Universidad deGranada in Spain demonstrated that, compared with
Figure 9 Hidradenitis. Irregular hypoechoic area at thedermal-subcutaneous junction with increased perilesional flow.
controls, patients with psoriasis, and in particular thosewith nail disease, had lower blood flow in the nails, whichwas attributed to increased nailflow vessel resistance.64 Theauthors suggested that psoriasis could be an independentrisk factor for microvascular damage.64
Within the concept of psoriasis as an inflammatory sys-temic disease, ultrasound has been used to evaluate thepotential of carotid intima-media thickness as a marker ofcardiovascular risk.65,66 In one recent pilot study, intima-media thickness was found to be higher in patients treatedwith anti-tumor necrosis factor.67 The implications of ultra-sound evaluations of systemic inflammation in psoriasis haveyet to be clarified.
Hidradenitis
Hidradenitis is a predominantly subcutaneous inflamma-tion (Fig. 9) that can be studied in detail by ultrasound.68
On comparing epidermal and dermal thickness in patientswith hidradenitis and healthy controls, Wortsman and hergroup69 found that areas of the body affected by hidradeni-tis exhibited increased dermal-epidermal thickness andlower echogenicity. Finally, ultrasound can also be usedto detect subclinical lesions and occult fistulas in thissetting.69
Collagenosis
Scleroderma is the most widely studied disease by ultra-sound, as treatment varies according to the stage of disease(inflammatory or sclerotic).70 In a study of 104 morpheaplaques in 59 patients, Wortsman et al.71 showed that ultra-sound had a sensitivity of 100% and a specificity of 98.4% fordifferentiating between the inflammatory and the scleroticphases. In the same study, ultrasound detected subclinicalinflammation in 5 patients with Parry-Romberg syndrome.Attempts have been made to standardize these results tocreate semi-quantitative scales72 to assess the effectivenessof treatments such as phototherapy.73
Document downloaded from http://www.elsevier.es, day 06/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

896 F. Alfageme Roldán
Table 1 Ultrasound Patterns of the Most Common Dermal Fillers.
Location Pattern Echogenicity Differential Characteristics
Hyaluronic acid (R) Dermal Vacuolar Hypoechoic Disappears with timePolyacrylamide (NR) Dermal-subcutaneous Vacuolar Hypoechoic RemainsSilicone oil (NR) Dermal-subcutaneous Snowstorm Variable Posterior reverberationMethylmethacrylate
(NR)Dermal-subcutaneous Snowstorm Hyperechoic Similar to silicone
Calciumhydroxyapatite (R)
Dermal-subcutaneous Hyperechoic Hyperechoic Occasional posterioracoustic shadowing
Polylactic acid (R) Dermal-subcutaneous Hypoechoic,increased tissue
Variable May be undetectable
Abbreviations: NR, nonresorbable; R, resorbable.
Other Inflammatory Disorders
In a recent study comparing features of atopic dermatitisseen by ultrasound and histology, Polanska et al.74 observeda correlation between the thickness of the hypoechogenicsubepidermal band and epidermal hyperplasia, parakerato-sis, spongiosis, and intensity of inflammatory infiltrates.This band might therefore have potential as a cutaneousinflammation marker. Ultrasound could also be used detectsubclinical cutaneous inflammation in normal-appearing skinin patients with atopic dermatitis.75
Ultrasound in Cosmetic Dermatology
In recent years, ultrasound has become an important tool forthe noninvasive study of cosmetic fillers (Fig. 10) and theirpotential complications and medico-legal implications.76---78
Dermal fillers have distinguishing ultrasound features(Table 1) that can help to identify the nature of the filler,as well as any changes or complications (e.g., migration,clot formation)79 that can occur postinfiltration. Ultrasoundcan also be used to assess skin aging through the measure-ment of the hypoechoic subcutaneous band in sun-exposedareas,80,81 as this reflects the degree of dermal elastosis.
Several studies have used subcutaneous band thicknessmeasurement as a quick, noninvasive, and reproduciblemeans of assessing different skin rejuvenation techniques,such as mesotherapy, growth factors,82 and ablative andfractional laser resurfacing.83
Figure 10 Hyaluronic acid implants (H). The pattern is ini-tially vesicular.
The Future of Ultrasound Imaging of the Skin
The future of ultrasound skin imaging is closely linked to thepresent. On the one hand, dermatologists need to spreadword of their experiences with the technique and to con-tinue to learn and experiment, and on the other hand, justas in other areas such as rheumatology, dermatologists per-forming ultrasound need to standardize terminology andcriteria for evaluating skin cancers and inflammatory skindisorders.
The value of recent advances such as elastography andcontrast-enhanced ultrasound in dermatology has yet to bedetermined. The increasing availability of affordable ultra-sound equipment specifically designed for dermatologistswill also help to foster the use of ultrasound imaging in ourfield.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Acknowledgments
We thank Dr Cerezo (President of SEECO), Dr Villegas ofHospital Sanitas Moraleja, and Dr Roustán and Dr Suárez atHospital Universitario Puerta de Hierro for their support inthe early and later stages of cutaneous ultrasound and fortheir contributions to this article.
References
1. Wortsman X, Wortsmann J, Carreno L, Morales C, Sazunic I,Jemec G. Sonographic anatomy of the skin appendages andadjacent structures. In: Wortsmann X, Jemec G, editors. Der-matologic ultrasound with clinical and histological correlations.1st ed Berlin: Springer-Verlag; 2013. p. 15---35.
2. Alfageme F. ¿Cómo utilizar un ecógrafo? Botonología. In:Alfageme F, editor. Manual de ecografía cutánea. 1a edi-ción Charleston: Create Space Independent Platform Publisher;2013. p. 7---13.
3. Wortsman X. Common applications of dermatologic sonography.J Ultrasound Med. 2012;31:97---111.
4. Bouer M, Chammas M, Messina M, Cerri G. Squamous cell car-cinoma (SCC) of the skin: Description of ultrasound and power
Document downloaded from http://www.elsevier.es, day 06/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Ultrasound Skin Imaging 897
doppler findings before and after the use of microbubble con-trast and association with degree of malignancy. Ultrasound MedBiol. 2009;35:S220.
5. Alfageme F. Aplicaciones prácticas de la ecografía cutánea. Piel.2012;4:204---9.
6. Goldberg I, Sprecher E, Schwartz ME, Gaitini D. Compara-tive study of high-resolution multifrequency ultrasound of theplantar skin in patients with various types of hereditary palmo-plantar keratoderma. Dermatology. 2013;226:365---70.
7. Wortsman X, Wortsman J, Soto R, Saavedra T, Honeyman J,Sazunic I, et al. Benign tumors and pseudotumors of the nail:A novel application of sonography. J Ultrasound Med. 2010;29:803---16.
8. Wortsman X, Wortsman J, Matsuoka L, Saavedra T, Mardones F,Saavedra D, et al. Sonography in pathologies of scalp and hair.Br J Radiol. 2012;85:647---55.
9. Kuwano Y, Ishizaki K, Watanabe R, Nanko H. Efficacy of diagnos-tic ultrasonography of lipomas, epidermal cysts, and ganglions.Arch Dermatol. 2009;145:761---4.
10. Wortsman X, Wortsman J. Clinical usefulness of variable fre-quency ultrasound in localized lesions of the skin. J Am AcadDermatol. 2010;62:247---56.
11. Wortsman X. Sonography of cutaneous and ungual lumps andbumps. Ultrasound Clinics. 2012;7:505---23.
12. Chung-Cheng H, Sheung-Fat K, Hsuan-Ying H, Shu-Hang N, Tze-Yu L, Yi-Wei L, et al. Epidermal cysts in the superficial softtissue: sonographic features with an emphasis on the pseu-dotestis pattern. J Ultrasound Med. 2011;30:11---7.
13. Crisan M, Crisan D, Sannino G, Lupsor M, Badea R, Amz-ica F. Ultrasonographic staging of cutaneous malignanttumors: an ultrasonographic depth index. Arch Dermatol Res.2013;305:305---13.
14. Mogensen M, Jemec GB. Diagnosis of nonmelanoma skin can-cer/keratinocyte carcinoma: A review of diagnostic accuracyof nonmelanoma skin cancer diagnostic tests and technologies.Dermatol Surg. 2007;33:1158---74.
15. Hinz T, Ehler LK, Hornung T, Voth H, Fortmeier I, Maier T,et al. Preoperative characterization of basal cell carcinomacomparing tumour thickness measurement by optical coherencetomography, 20-MHz ultrasound and histopathology. Acta DermVenereol. 2012;92:132---7.
16. Petrella L, Valle H, Issa PR, Martins C, Pereira W, Machado J.Study of cutaneous cell carcinomas ex vivo using ultrasoundbiomicroscopic images. Skin Res Technol. 2010;16:422---4.
17. Mogensen M, Joergensen TM, Nürnberg BM, Morsy HA, Thom-sen JB, Thrane L, et al. Assessment of optical coherencetomography imaging in the diagnosis of non-melanoma skin can-cer and benign lesions versus normal skin: Observer-blindedevaluation by dermatologists and pathologists. Dermatol Surg.2009;35:965---72.
18. Salmhofer W, Rieger E, Soyer HP, Smolle J, Kerl H. Influence ofskin tension and formalin fixation on sonographic measurementof tumor thickness. J Am Acad Dermatol. 1996;34:34---9.
19. Bobadilla F, Wortsman X, Munoz C, Segovia L, Espinoza M,Jemec G. Pre-surgical high resolution ultrasound of facial basalcell carcinoma: Correlation with histology. Cancer Imaging.2008;8:163---72.
20. Wortsman X. Sonography of facial cutaneous basal cell car-cinoma: a first-line imaging technique. J Ultrasound Med.2013;32:567---72.
21. Marmur ES, Berkowitz EZ, Fuchs BS, Singer GK, Yoo JY. Use ofhigh-frequency, high-resolution ultrasound before Mohs surgery.Dermatol Surg. 2010;36:841---7.
22. Jambusaria-Pahlajani A, Schmults CD, Miller CJ, Shin D, WilliamsJ, Kurd SK, et al. Test characteristics of high-resolution ultra-sound in the preoperative assessment of margins of basalcell and squamous cell carcinoma in patients undergoing Mohsmicrographic surgery. Dermatol Surg. 2009;35:9---15.
23. Smucler R, Kriz M, Lippert J, Vlk M. Ultrasound guided ablative-laser assisted photodynamic therapy of basal cell carcinoma(US-aL-PDT). Photomed Laser Surg. 2012;30:200---5.
24. O’Bryan K, Sherman W, Niedt GW, Taback B, Manolidis S, WangA, et al. An evolving paradigm for the workup and manage-ment of high-risk cutaneous squamous cell carcinoma. J AmAcad Dermatol. 2013;69:595---602.
25. Nuno A, Vicente FJ, Fernando Pinedo F, López Estebaranz JL.Carcinoma epidermoide cutáneo de alto riesgo. Actas Dermosi-filiogr. 2012;103:567---78.
26. Martorell A, Sanmartín O, Cruz Mojarrieta J, Guillén C. Car-cinoma epidermoide cutáneo: definiendo la variante de altoriesgo. Actas Dermosifiliogr. 2013;104:367---79.
27. Kruyt R, van Putten W, Levendag P, de Boer M, Oudkerk M.Biopsy of nonpalpable cervical lymph nodes: selection criteriafor ultrasound-guided biopsy in patients with head and necksquamous cell carcinoma. Ultrasound Med Biol. 1996;22:413---9.
28. Cousen P, Chow K, Colver G. What is the role of ultrasoundevaluation of lymph nodes in patients with high-grade squa-mous cell carcinoma of the head and neck? Br J Dermatol.2010;162:1146---7.
29. Aoyagi S, Izumi K, Hata H, Kawasaki H, Shimizu H. Useful-ness of real-time tissue elastography for detecting lymph-nodemetastases in squamous cell carcinoma. Clin Exp Dermatol.2009;3:e744---7.
30. Vilana R, Puig S, Sanchez M, Squarcia M, López A, Castel T, et al.Preoperative assessment of cutaneous melanoma thicknessusing 10-MHz sonography. Am J Roentgenol. 2009;193:639---43.
31. Partsch B, Binder M, Püspök Schwarz M, Wolff K, PehambergerH. Limitations of high frequency ultrasound in determining theinvasiveness of cutaneous malignant melanoma. Melanoma Res.1996;6:395---8.
32. Tacke J, Haagen G, Hornstein OP, Huettinger G, Kieserwetter F,Schell H, et al. Clinical relevance of sonometry derived tumorthickness in malignant melanoma: A statistical analysis. Br JDermatol. 1995;132:209---14.
33. Serrone L, Solivetti FM, Thorel MF, Eibenshutz L, Donati P, Catri-calá C. High frequency ultrasound in the preoperative stagingof primary melanoma: A statistical analysis. Melanoma Res.2002;12:287---90.
34. Kaikaris V, Samsanavicius D, Maslauskas K, Rimdeika R, Val-iukeviciene S, Makstiene J, et al. Measurement of melanomathickness---comparison of two methods: ultrasound versus mor-phology. J Plastic Reconst Aesthet Surg. 2011;64:796---802.
35. Fernández Canedo I, de Troya M, Fúnez R, Lébana R, Rivas RuizF, Blanco Eguren G, et al. Evaluación de la ecografía cutánea de15 Mhz en la estimación preoperatoria del espesor tumoral enel melanoma maligno. Actas Dermosifiliogr. 2013;104:227---31.
36. Machet L, Belot V, Naouri M, Boka M, Mourtada Y, GiraudeauB, et al. Preoperative measurement of thickness of cutaneousmelanoma using high-resolution 20 MHz ultrasound imaging: Amonocenter prospective study and systematic review of theliterature. Ultrasound Med Biol. 2009;35:1411---20.
37. Music MM, Hertl K, Kadivec M, Pavlovic MD, Hocevar M. Pre-operative ultrasound with a 12-15 MHz linear probe reliablydifferentiates between melanoma thicker and thinner than1 mm. J Eur Acad Dermatol Venereol. 2010;24:1105---8.
38. Uren RF, Howman-Giles R, Thompson J, Shaw H, RobertsJ, Bernard E, et al. High-resolution ultrasound to diagnosemelanoma metastases in patients with clinically palpable lymphnodes. Australas Radiol. 1999;43:148---52.
39. Chai CY, Zager JS, Szabunio MM, Marzban SS, Chau A, Rossi RM,et al. Preoperative ultrasound is not useful for identifying nodalmetastasis in melanoma patients undergoing sentinel nodebiopsy: Preoperative ultrasound in clinically node-negativemelanoma. Ann Surg Oncol. 2012;19:1100---6.
40. Marone U, Catalano O, Caracò C, Anniciello AM, SandomenicoF, Di Monta G, et al. Can high-resolution ultrasound avoid the
Document downloaded from http://www.elsevier.es, day 06/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
898 F. Alfageme Roldán
sentinel lymph-node biopsy procedure in the staging process ofpatients with stage i-ii cutaneous melanoma? Ultraschall Med.2012;33:E179---85.
41. Pilko G, Zgajnar J, Music M, Hocevar M. Lower tumour burdenand better overall survival in melanoma patients with regionallymph node metastases and negative preoperative ultrasound.Radiol Oncol. 2012;46:60---8.
42. Hinz T, Voth H, Ahmadzadehfar H, Hoeller T, Wenzel J, BieberT, et al. Role of high-resolution ultrasound and PET/CT imagingfor preoperative characterization of sentinel lymph nodes incutaneous melanoma. Ultrasound Med Biol. 2013;39:30---6.
43. Lassau N, Lamuraglia M, Koscielny S, Spatz A, Roche A, LeclereJ, et al. Prognostic value of angiogenesis evaluated with high-frequency and colour doppler sonography for preoperativeassessment of primary cutaneous melanomas: correlation withrecurrence after a 5 year follow-up period. Cancer Imaging.2006;6:24---9.
44. Srivastava A, Woodcock JP, Mansel RE, Webster DJ, Laidler P,Hughes LE, et al. Doppler ultrasound flowmetry predicts 15year outcome in patients with skin melanoma. Indian J Surg.2012;74:278---83.
45. Rubaltelli L, Beltrame V, Scagliori E, Bezzon E, Frigo AC, Ras-trelli M, et al. Potential use of contrast-enhanced ultrasound(CEUS) in the detection of metastatic superficial lymph nodesin melanoma patients. Ultraschall Med. 2014;35:67---71.
46. Ogata D, Uematsu T, Yoshikawa S, Kiyohara Y. Accuracy of real-time ultrasound elastography in the differential diagnosis oflymph nodes in cutaneous malignant melanoma (CMM): A pilotstudy. Int J Clin Oncol. 2013 [Epub ahead of print].
47. Chami L, Lassau N, Chebil M, Robert C. Imaging of melanoma:Usefulness of ultrasonography before and after contrast injec-tion for diagnosis and early evaluation of treatment. ClinCosmet Investig Dermatol. 2011;4:1---6.
48. Kilian KJ, Ruzicka T, Flaig M, Berking C, Kunte C. Recurrentfibrosarcomatous dermatofibrosarcoma protuberans ultrasoundimaging. Hautarzt. 2013;64:512---5.
49. Shin YR, Kim JY, Sung MS, Jung JH. Sonographic findings of der-matofibrosarcoma protuberans with pathologic correlation. JUltrasound Med. 2008;27:269---74.
50. Enzenhofer E, Ubl P, Czerny C, Erovic BM. Imaging in patientswith Merkel cell carcinoma. J Skin Cancer. 2013;2013:9731---823.
51. Righi A, Asioli S, Caliendo V, Macripò G, Picciotto F, Risio M, et al.An ultrasonography-cytology protocol for the diagnostic man-agement of regional nodes in a subset of patients with Merkelcell carcinoma of the skin. Br J Dermatol. 2013;168:563---70.
52. Giovagnorio F. Sonography of cutaneous non-Hodgkin’s lym-phomas. Clin Radiol. 1997;52:301---3.
53. Terhorst D, Mestel DS, Humme D, Sterry W, Beyer M. Evaluationof different methods in the follow-up of patients with indo-lent types of primary cutaneous lymphomas. Br J Dermatol.2012;166:1295---300.
54. Wortsman X, Jemec GBE, Sazunic I. Anatomical detection ofinflammatory changes associated to plantar warts. Dermatol-ogy. 2010;220:213---7.
55. Iverson K, Haritos D, Thomas R, Kannikeswaran N. The effect ofbedside ultrasound on diagnosis and management of soft tissueinfections in a pediatric ED. Am J Emerg Med. 2012;30:1347---51.
56. Ramirez-Schrempp D, Dorfman DH, Baker W, Liteplo AS. Ultra-sound soft-tissue applications in the pediatric emergencydepartment: To drain or not to drain? Pediatr Emerg Care.2009;25:44---8.
57. Squire BT, Fox JC, Anderson C. ABSCESS: Applied bedsidesonography for convenient evaluation of superficial soft tissueinfections. Acad Emerg Med. 2005;12:601---6.
58. Gutierrez M, Wortsman X, Filippucci E, de Angelis R, FilosaG, Grassi W. High-frequency sonography in the evaluationof psoriasis: Nail and skin involvement. J Ultrasound Med.2009;28:1569---74.
59. Gutierrez M, de Angelis R, Bernardini ML, Filippucci E, GoteriG, Brandozzi G, et al. Clinical, power doppler sonographyand histological assessment of the psoriatic plaque: Short-termmonitoring in patients treated with etanercept. Br J Dermatol.2011;164:33---7.
60. Gutierrez M, Filippucci E, Bertolazzi C, Grassi W. Sonographicmonitoring of psoriatic plaque. J Rheumatol. 2009;36:850---1.
61. Lacarrubba F, Nardone B, Musumeci ML, Micali G. Ultrasoundevaluation of clobetasol propionate 0.05% foam application inpsoriatic and healthy skin: A pilot study. Dermatol Ther. 2009;22Suppl 1:S19---21.
62. De Agustín JJ, Moragues C, de Miguel E, Möller I, AcebesC, Naredo E, et al. A multicentre study on high-frequencyultrasound evaluation of the skin and joints in patients withpsoriatic arthritis treated with infliximab. Clin Exp Rheumatol.2012;30:879---85.
63. Aydin SZ, Castillo-Gallego C, Ash ZR, Abignano G, Marzo-OrtegaH, Wittmann M, et al. Ultrasonographic assessment of nail inpsoriatic disease shows a link between onychopathy and distalinterphalangeal joint extensor tendon enthesopathy. Dermatol-ogy. 2012;225:231---5.
64. Husein El-Ahmed H, Garrido-Pareja F, Ruiz-Carrascosa JC,Naranjo-Sintes R. Vessel resistance to blood flow in the nail-fold in patients with psoriasis: A prospective case-control echoDoppler-based study. Br J Dermatol. 2012;166:54---8.
65. Antonucci VA, Tengattini V, Balestri R, Patrizi A, Filippini M,et al. Intima-media thickness in an Italian psoriatic population:correlation with lipidic serum levels PASI and BMI. J Eur AcadDermatol Venereol. 2014;28:512---5.
66. Arias-Santiago S, Orgaz-Molina J, Castellote-Caballero L,Arrabal-Polo MÁ, García-Rodriguez S, Perandrés-López R, et al.Atheroma plaque, metabolic syndrome and inflammation inpatients with psoriasis. Eur J Dermatol. 2012;22:337---44.
67. Jókai H, Szakonyi J, Kontár O, Marschalkó M, Szalai K, Kár-páti S, et al. Impact of effective tumor necrosis factor-alfainhibitor treatment on arterial intima-media thickness in pso-riasis: Results of a pilot study. J Am Acad Dermatol. 2013;69:523---9.
68. Kelekis NL, Efstathopoulos E, Balanika A, Spyridopoulos TN,Pelekanou A, Kanni T, et al. Ultrasound aids in diagnosis andseverity assessment of hidradenitis suppurativa. Br J Dermatol.2010;1:1400---2.
69. Wortsman X, Jemec GBE. High frequency ultrasound forthe assessment of hidradenitis suppurativa. Dermatol Surg.2007;33:1---3.
70. Wortsman X, Jemec G. Common inflammatory diseases of theskin: From the skin to the screen. Adv Psoriasis InflammatorySkin Dis. 2010;2:9---15.
71. Wortsman X, Wortsman J, Sazunic I, Carreno L. Activity assess-ment in morphea using color doppler ultrasound. J Am AcadDermatol. 2011;65:942---8.
72. Li SC, Liebling MS, Haines KA, Weiss JE, Prann A. Initial eval-uation of an ultrasound measure for assessing the activity ofskin lesions in juvenile localized scleroderma. Arthritis Care Res(Hoboken). 2011;63:735---42.
73. Sator PG, Radakovic S, Schulmeister K, Hönigsmann H, TanewA. Medium-dose is more effective than low-dose ultraviolet A1phototherapy for localized scleroderma as shown by 20-MHzultrasound assessment. J Rheumatol. 2009;3:2819---29.
74. Polanska A, Danczak-Pazdrowska A, Silny W, Wozniak A, MaksinK, Jenerowicz D, et al. Comparison between high-frequencyultrasonography (Dermascan C, version 3) and histopathologyin atopic dermatitis. Skin Res Technol. 2013;19:432---7.
75. Danczak-Pazdrowska A, Polanska A, Silny W, Sadowska A,Osmola-Mankowska A, Czarnecka-Operacz M, et al. Seeminglyhealthy skin in atopic dermatitis: observations with the useof high-frequency ultrasonography, preliminary study. Skin ResTechnol. 2012;18:162---7.
Document downloaded from http://www.elsevier.es, day 06/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

Ultrasound Skin Imaging 899
76. De Cabo-Frances FM, Alcolea JM, Bové-Farré L, Pedret C, TrellesMA. Ecografía de los materiales de relleno inyectables y suinterés en el seguimiento diagnóstico. Cir Plást Iberolatinoam.2012;38:179---87.
77. Schelke LW, Elzen HJ, Erkamp PP, Neumann HA. Use of ultra-sound to provide overall information on facial fillers andsurrounding tissue. Dermatol Surg. 2010;36 Suppl 3:1843.
78. Wortsman X, Wortsman J, Orlandi C, Cardenas G, Sazunic I,Jemec G. Ultrasound detection and identification of cosmeticfillers in the skin. J Eur Acad Dermatol Venereol. 2012;26:293.
79. Wortsman X, Wortsman J. Sonographic outcomes of cosmeticprocedures. Am J Roentgenol. 2011;197:W910---8.
80. Gniadecka M, Gniadecki R, Serup J, Sondergaard J. Ultra-sound structure and digital image analysis of the subepidermal
low echogenic band in aged human skin: Diurnal changesand interindividual variability. J Invest Dermatol. 1994;102:362---5.
81. Alfageme F, Tresguerres Fernandez A, Buron I, Villegas C. Méto-dos ecográficos de evaluación del envejecimiento cutáneo y sutratamiento. Piel. 2011;26:517---22.
82. Fernández-Tresguerres A, Alfageme F, Burón I, RodríguezR, Villegas C. Bioestimulación cutánea con plasma rico enplaquetas autólogo: estudio controlado con ecografía. Piel.2013;28:69---74.
83. Tierny E, Hanke C, Petersen J, Bartley T, Eckert JR, McCutchenC. Clinical and echographic analysis of ablative fractionatedcarbon dioxide laser in the treatment of photodamaged facialskin. Dermatol Surg. 2010;36:2009---21.
Document downloaded from http://www.elsevier.es, day 06/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.










![Large buccal fat pad lipoma: A rare case report...gland lipoma in 2 cases, angiolipoma in 2 cases, and spindle cell lipoma in 3 cases [10]. The most common presentation of BFP lipoma](https://img.pdfslide.us/doc/110x75/5e610a1252021369db53e163/large-buccal-fat-pad-lipoma-a-rare-case-report-gland-lipoma-in-2-cases-angiolipoma.jpg)