Embed Size (px)
Citation preview

The Journal of Emergency Medicine, Vol. 43, No. 1, pp. 87–92, 2012Copyright � 2012 Elsevier Inc.
Printed in the USA. All rights reserved0736-4679/$ - see front matter
doi:10.1016/j.jemermed.2011.06.034
This work wasSociety for Acadident AcademicMedicine, Caroli
Currently, Dr.Gastonia, NC andCenter, Winston-
RECEIVED: 7 DeACCEPTED: 5 Jun
Ultrasound inEmergency Medicine
ULTRASOUND MEASUREMENTS OF THE SAPHENOUS VEIN IN THE PEDIATRICEMERGENCY DEPARTMENT POPULATION WITH COMPARISON
TO I.V. CATHETER SIZE
Ian Cole, MD,* Casey Glass, MD,* H. James Norton, PHD,† and Vivek Tayal, MD*
*Department of Emergency Medicine and †Department of Biostatistics, Carolinas Medical Center, Charlotte, North Carolina
Reprint Address: Vivek Tayal, MD, Department of Emergency Medicine, Carolinas Medical Center, Box 32861, Charlotte, NC 28232
, Abstract—Background: Saphenous vein cutdown isa rare venous access procedure. Ultrasound (US) can assistwith many vascular access procedures. Objectives: Ourobjective was to identify the saphenous veins (SVs) usingUS in pediatric emergency department (ED) patients, andto determine if the SV size allows for potential cannulationby different standard-size intravenous (i.v.) catheters.Methods: This study was a prospective, observational conve-nience sample of 60 pediatric patients at an urban, regionalreferral pediatric ED. Inclusion criteria were children ages 1through 12 years categorized into four age groups: 1–<2,2–4, 5–7, and 8–12 years, with informed consent and assent.Investigators performed US examination using a 10-MHzmulti-frequency transducer to identify the SV on both legsand measure the SV in short-axis view. The US measure-ments were then used to calculate the SV areas. Diametersof typical pediatric gauge (G) catheters (24G, 22G, 20G,18G) were used to calculate catheter areas. Results: Sixtypatients were enrolled, with five SVs unable to be measuredin 4 patients (1 patient with both SVs). For the remaining115 (96%) SVs available for further analysis, the medianage was 4 years (interquartile range [IQR] 2) and medianweight was 22.7 kg (IQR 14.5). Mean area (mm2) of the right
presented at the 2010 Annual Meeting of theemic Emergency Medicine and the 2010 Res-Day presentation (Department of Emergencynas Medical Center).Cole works at Gaston Memorial Hospital,Dr. Glass works at the Wake Forest Medical
Salem, NC.
cember 2010; FINAL SUBMISSION RECEIVED: 28 Ae 2011
87
SV was 2.85 ± 1.9 and for the left SV, 2.88 ± 1.8. Forour study group, the compatibility rates of differentsize i.v. catheters to fit the measured SV areas were asfollows: 24G = 100%, 22G = 100%, 20G = 97.3%, and18G = 86.1%. Conclusions: US can localize the SV in pediat-ric ED patients. US size of the SV in various pediatric ageranges suggests that the SVmay be a potential US venous ac-cess site with multiple-size i.v. catheters up to 18G. � 2012Elsevier Inc.
, Keywords—US guidance; peripheral venous access;saphenous vein
INTRODUCTION
Peripheral intravenous (i.v.) access is often a criticalcomponent of emergency department (ED) patient care.In 2006 there were over 119 million ED visits in theUnited States, with over 21 million of those visits fromchildren under the age of 15 years (1). Many of thesevisits may require i.v. access for various reasons, includ-ing i.v. volume resuscitation, phlebotomy, and medica-tion administration. However, obtaining i.v. access inpediatric patients can be difficult for many reasons; theirperipheral veins may not be palpable or visible at times.Failure to obtain i.v. access in a timely fashion can leadto delay in treatment and diagnosis.
Alternative routes and techniques have been sought toobtain rapid i.v. access. Ultrasound (US)-guided i.v.placement has been one of the alternatives to traditional
pril 2011;

88 I. Cole et al.
techniques for i.v. placement in patients with difficult i.v.access (2–9). In the pediatric literature, the saphenousvein (SV) is mostly identified with venous cutdown andnot with US guidance i.v. access. Therefore, we soughtto identify the SV using US in pediatric ED patients,and to determine if the vein size allows for potentialcannulation by different standard-size i.v. catheters.
Figure 1. Ten-MHz multi-frequency transducer was placedapproximately 1 cm anterior and 1 cm superior to the medialmalleolus to locate the saphenous vein (SV).
METHODS
Study Design
This studywas a prospective observational study of a con-venience sample of 60 pediatric ED patients. All patientsenrolled in this study had parental informed consent and,in addition, gave assent for their participation if age6 years or older. The Institutional Review Board at thestudy site approved this study.
Study Setting and Population
This study was done in a single urban, regional referralpediatric ED with approximately 30,000 annual visits.The pediatric ED is part of a 3-year emergency medicine(EM) residency program that has a pediatric EM and USfellowship. The study sonographers were an experiencedthird-year EM resident and a US fellow. Patients wereenrolled when one of these sonographers were present.Patients age 1 through 12 years were eligible if parentswere able to provide informed consent, and in addition,children 6 years or older provided assent. Patients weregrouped into categories by age; 1–<2, 2–4, 5–7, and8–12 years. Patients were excluded if there was evidenceof pathologic changes to the leg, including fracture, am-putation, congenital or acquired deformity/contractures,skin infection, and history of operative repair. In addition,unstable patients—defined as any one of these beingpresent: hypotension, respiratory distress, altered mentalstatus, and cardiorespiratory arrest—were excluded.
Study Protocol
Before the start of the study, study sonographers met thetraining requirements of being a faculty physician of theUS division or an EM resident who had performed over150 EM US scans and had completed a month of USintern rotation with dedicated peripheral vein trainingby the US director.
After consent and assent were obtained, demographicinformation (age, sex, height, weight, and chief complaint)was recorded directly on a paper form by the sonographer.
The patient was then placed in a supine position and astandard i.v. tourniquet was placed at the calf (Figure 1).The primary study objective was successful identification
and measurements of the diameters of the SV in the trans-verse plane. The SV was identified using Ultrasonix CEPor Sonixtouch (Ultrasonix Corporations, Vancouver, BC,Canada) with the same 10-MHz multi-frequency trans-ducer (Figure 1). The transducer was placed approxi-mately 1 cm anterior and 1 cm superior to the medialmalleolus to locate the SV. Once the SV was identifiedand confirmed to be anechoic and compressible, a stillimage in the transverse plane was obtained. The studysonographer measured the diameter in millimeters(mm) of the SV in transverse plane in both the horizontaland vertical axes (Figure 2). The same steps describedabove were repeated on the contralateral leg. The mea-surements were then recorded directly onto the samepaper form that contained the demographic information.The director of EM US reviewed images and data collec-tion forms to ensure quality and consistency and thenentered the information into a Microsoft Access database(Microsoft Corporation, Redmond, WA).
Diameters of typical pediatric gauge (G) i.v. cathe-ters—24G, 22G, 20G, and 18G—were used to calculatei.v. catheter areas using the standard geometric formulafor a circle (pr2). US measurements of the diameters ofthe SV in transverse plane were used to calculate SVareasusing the standard geometric formula p1/2 D11/2D2 foran oval. The calculated SV areas (per measured dimen-sions and with a 20% reduction in vein area) and thei.v. catheter areas were then compared with descriptivestatistics.
Data Analysis
The study subjects were divided into four age categories:1–<2, 2–4, 5–7, and 8–12 years. Fisher exact test wasused to determine significance of association between

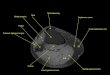
Figure 2. Ultrasound image of the saphenous vein with measurements of the saphenous vein in transverse plane both in thehorizontal and vertical axis.
US Measurements of Pediatric Saphenous Vein 89
age and compatibility rates for each i.v. catheter size. Inaddition, the Fisher exact test was used to assess the asso-ciation between i.v. catheter size and compatibility to fitinto the SV within each age category. Each calculatedSV area was compared to the areas of the respectivedifferent i.v. catheter sizes (24G, 22G, 20G, and 18G),and if the SV area was larger than the i.v. catheter area,it was considered compatible. Calculated vein area wasthen reduced by 20% and compared to catheter size ina separate analysis.
Demographic characteristics are presented descrip-tively as medians with interquartile range (IQR) and num-bers, when appropriate. A p-value of < 0.05 wasconsidered significant. SAS version 9.1 (SAS InstituteInc., Cary, NC) was used for analysis.
Table 1. Body and Saphenous Vein (SV) Characteristics of the Stu
1–<2 2–4
n = 12 n = 20
Median IQR (25%–75%) Median IQR (25%
Weight (kg) 12.1 (10.8–12.8) 16.6 (15–21Height (cm) 77 (75–81) 98 (94–10Right SV area (mm2) 2.96 (1.88–3.06) 2.15 (1.53–Left SV area (mm2) 1.98 (1.43–2.83) 1.88 (1.32–
IQR = interquartile range.
RESULTS
Sixty patients were enrolled during the study, with a totalof 120 extremities available for US visualization andmeasurement of the SV. The distribution of subjects andidentified SV were as follows: 1–<2 years: 12 subjectswith 23 SV measured; 2–4 years: 20 subjects with37 SV measured; 5–7 years: 14 subjects with 27 SV mea-sured; 8–12 years: 14 patients and 28 SVmeasured. Over-all, the SV was not measured or identified in fiveextremities involving a total of 4 patients.
For the remaining 115 (96%) SVs available for furtheranalysis, the median age was 4 years (IQR 2) and medianweight 22.7 kg (IQR 14.5). Twenty-six (40%) of theenrolled patients were female. For our study group the
dy Population per Age Group
Age, Years
5–7 8–12
n = 14 n = 14
–75%) Median IQR (25%–75%) Median IQR (25%–75%)
.6) 27.5 (25–35) 34.5 (31–51)7) 125 (121–132) 148 (134–154)2.71) 2.63 (1.53–3.73) 2.8 (2.2–3.8)3.39) 2.64 (2.25–4.1) 2.9 (2.4–4.1)

Table 2. Compatibility Rate (%) of Ultrasound-measuredSaphenous Vein in Different Pediatric Age Groupswith Regard to Different i.v. Catheter Size (Area)
1–<2 Years 2–4 Years 5–7 Years 8–12 Years
24 Gauge 100 100 100 10022 Gauge 100 100 100 10020 Gauge 100 95 100 9618 Gauge 87 78 89 93
Table 3. Compatibility Rate (%) of Ultrasound-measuredSaphenous Vein in Different Pediatric Age Groupswith Regard to Different i.v. Catheter Size (Area)Using a 20% ‘‘Wiggle Room’’ Difference betweenVein Size and Catheter
1–<2 Years 2–4 Years 5–7 Years 8–12 Years
24 Gauge 100 100 100 10022 Gauge 100 97.3 100 10020 Gauge 95.7 86.5 88.9 92.918 Gauge 74 59.5 66.7 85.7
90 I. Cole et al.
compatibility rate of different size IV catheters to fit themeasured SV areas was as follows: 24G = 100%, 22G =100%, 20G = 97.3%, 18G = 86.1%. Table 1 describesbody and saphenous vein characteristics per age category.Table 2 describes the high compatibility rates of the dif-ferent catheter gauges in regards to the US-measuredarea of SV per age group. In Table 3, using a 20% reduc-tion in vein area for each age group and catheter size,there continued to be high compatibility rates up to the18G catheter size.
Age did not have a significant effect on the compati-bility rate of different size i.v. catheters to fit theUS-measured SV (24G, p = 1.00; 22G, p = 1.00; 20G,p = 0.697; 18G, p = 0.504). Intravenous catheter size didnot significantly affect the compatibility rate of fittinginto the measured SV within each age group (1–<2,p = 0.057; 5–7, p = 0.058; and 8–12, p = 0.615) exceptin the 2–4 years of age group (p = 0.004).
DISCUSSION
SV cutdown is well described in the pediatric literature,although it is becoming an obsolete procedure due to ad-vances in central line placement and intraosseous access(10–14). However, there are potential disadvantages tothese techniques. Complications can occur in central lineplacement, including pneumothorax, arterial puncture,and central venous thrombosis, as well as bloodstreaminfection (15,16). In addition, central line placementcan be time-consuming and technically difficult in criti-cally ill pediatric patients. Intraosseous needle placementcan also lead to potential complications, including subcu-taneous infiltration, needle clogging, infection (cellulitisor osteomyelitis), and compartment syndrome (17).
Intravenous access with peripheral i.v. access beingthe preferred route is still one of the most critical compo-nents in ED pediatric care. One retrospective studyrevealed that lack of peripheral venous access (64%)was the most common indicated reason for placementof central venous catheters (18). When traditional tech-niques for peripheral i.v. access fail, we need alternativemethods such as ultrasound guidance that will providerapid access. We chose the SV as a site for potentialUS-guidance i.v. placement for several reasons. The SV
anatomy and path is predictable and has a superficiallocation at the ankle. In addition, during resuscitation,the ankle site is distant from the primary resuscitativeefforts usually centered on the head and torso region,allowing for possible unhindered access to the SV at theankle for i.v. placement.
Our hypothesis was that the SV would be compatiblein terms of size with standard i.v. catheters (24G, 22G,20G, 18G). Although our study focus was comparingSVareas to i.v. catheter areas, having a peripheral vesselcompatible in size to the i.v. catheter may not translate tosuccessful US-guided peripheral i.v. placement. There-fore, the next logical step will be to attempt to cannulatethe SV using US guidance in further research.
The scope of future studies can be broad and not justlimited to identification and cannulation of the SV.Panebianco et al. concluded that successful US-guidedperipheral i.v. placement in adult patients was solelyrelated to vessel characteristics detected with US andnot to patient characteristics (19). It is not clear whetherthe same will be true in pediatric patients; it will be im-portant to assess if there are associations between vesseldiameter and vessel depth from the skin surface as wellas patient’s age, weight, height, body mass index, andhydration status to successful US-guided SV i.v. place-ment in pediatric patients.
Limitations
Lack of cannulation is a significant limitation in ourstudy, although we have demonstrated that the SV sizecan allow for potential cannulation by various size cath-eters. Actual cannulation and placement of a functioningi.v. will be the ideal clinical endpoint.
Study was limited to a single site. The study had onlytwo sonographers, which allowed for consistency andensured a level of quality in performing the objectivesof the study. But this may have provided several limita-tions. First, it could limit the applicability to other EDsbecause other providers may not have attained the skilllevel of the study sonographers, especially as they couldhave refined and improved their skill level as the studyprogressed. Second, patients were enrolled only when

US Measurements of Pediatric Saphenous Vein 91
these sonographers were available, which was mostlyduring daytime and hence were a convenience sample.The sonographers were not blinded to the study objec-tives, which potentially exposes the results to severalbiases, including selection bias.
Although this was an observational study, the exclu-sion of unstable patients could have positively affectedour outcome data. In addition, it excludes a group thatwould eventually be a target for US-guided i.v. place-ment.We did not account for the effect of hydration statuson the SV size.
CONCLUSIONS
US can localize the SV in pediatric ED patients. US sizeof the SV in various pediatric age ranges suggests that theSV may be a potential US venous access site withmultiple-size i.v. catheters, with only 18G catheters hav-ing potential size limitations. Future US-guided SV stud-ies in pediatric patients are justified.
REFERENCES
1. Pitts SR, Niska RW, Xu J, Burt CW. National Hospital AmbulatoryMedical Care Survey: 2006 emergency department summary[Table 2]. Natl Health Stat Report 2008;(7):1–38.
2. Resnick JR, Cydulka RK, Donato J, Jones RA, Werner SL. Successof ultrasound-guided peripheral intravenous access with skin mark-ing. Acad Emerg Med 2008;15:723–30.
3. Mills CN, Liebmann O, Stone MB, Frazee BW. Ultrasonographi-cally guided insertion of a 15-cm catheter into the deep brachialor basilic vein in patients with difficult intravenous access. AnnEmerg Med 2007;50:68–72.
4. Constantino TG, Parikh AK, Satz WA, Fojtik JP. Ultrasonography-guided peripheral intravenous access versus traditional approachesin patients with difficult intravenous access. Ann Emerg Med 2005;46:456–61.
5. Brannam L, Blaivas M, Lyon M, Flake M. Emergency nurses’utilization of ultrasound guidance for placement of peripheralintravenous lines in difficult-access patients. Acad Emerg Med2004;11:1361–3.
6. Keyes LE, Frazee BW, Snoey ER, Simon BC, Christy D. Ultra-sound-guided brachial and basilic vein cannulation in emergencydepartment patients with difficult intravenous access. Ann EmergMed 1999;34:711–4.
7. Doniger SJ, Ishimine P, Fox JC, Kanegaye JT. Randomized con-trolled trial of ultrasound-guided peripheral intravenous catheterplacement versus traditional techniques in difficult-access pediatricpatients. Pediatr Emerg Care 2009;25:154–9.
8. Bauman M, Braude D, Crandall C. Ultrasound-guidance vs. stan-dard technique in difficult vascular access patients by ED techni-cians. Am J Emerg Med 2009;27:135–40.
9. Costantino TG, Kirtz JF, Satz WA. Ultrasound-guided peripheralvenous access vs. the external jugular vein as the initial approachto the patient with difficult vascular access. J Emerg Med 2010;39:462–7.
10. Adelman S. An emergency intravenous route for the pediatricpatient. JACEP 1976;5:596–8.
11. Gauderer MW. Vascular access techniques and devices in the pedi-atric patient. Surg Clin North America 1992;72:1267–84.
12. Johnson EM, Saltzman DA, Suh G, Dahmus RA, Leonard AS.Complications and risks of central venous catheter placement inchildren. Surgery 1998;124:911–6.
13. LaRocco BG, Wang HE. Intraosseous infusion. Prehosp EmergCare 2003;7:280–5.
14. DeBoer S, Russell T, Seaver M, Vardi A. Infant intraosseous infu-sion. Neonatal Netw 2008;27:25–32.
15. Karapinar B, Cura A. Complications of central venous catherizationin critically ill children. Pediatr Int 2007;49:593–9.
16. Goede MR, Coopersmith CM. Catheter-related bloodstream infec-tion. Surg Clin North Am 2009;89:463–74.
17. Eslami P. Pediatric intraosseous access. Available at: http://emedicine.medscape.com/article/940993-overview. Accessed November 1,2010.
18. Chiang VW, Baskin MN. Uses and complications of central venouscatheters inserted in a pediatric emergency department. PediatrEmerg Care 2000;16:230–2.
19. Panebianco NL, Fredette JM, Szyld D, Sagalyn EB, Pines JM,Dean AJ. What you see (sonographically) is what you get: veinand patient characteristics associated with successful ultrasound-guided peripheral intravenous placement in patients with difficultaccess. Acad Emerg Med 2009;16:1298–303.

92 I. Cole et al.
ARTICLE SUMMARY
1. Why is this topic important?Saphenous vein access is performed by cutdown. Many
emergency physicians have limited experience with cut-down. Ultrasound has been found to assist with vascularaccess, including central and peripheral venous access.2. What does this study attempt to show?
We attempt to show that we could find the distal saphe-nous vein near the ankle in different pediatric ranges. Sec-ondly, we measured the dimensions of the veins todeterminewhether various different size intravenous cath-eters would fit within such veins.3. What are the key findings?
Saphenous veins were able to be seen near the ankle inchildren, and their size may fit typical intravenous cathe-ters up to 18 gauge.4. How is patient care impacted?
Ultrasound-guided saphenous vein cannulation shouldbe considered as a potential site for an intravenous cathe-ter in children.