Embed Size (px)
Citation preview

Ultrasound Guided MSK Procedures in Children
Mahesh Thapa, MD Associate Professor
Seattle Children’s University of Washington School of
Medicine

ANDREW KISHORE THAPA * - BORN APRIL 14, 2012
*NAUGHTIER THAN THIS PICTURE SUGGESTS

Disclosures
Under contract with Lippincott Williams and Wilkins (LWW) for Pediatric Radiology - A Teaching File Textbook
Simulation workshop for Ultrasound-guided MSK procedures

Acknowledgment
• William Shiels, DO
• Nationwide Children’s Hospital

Objectives
• At the end of this lecture the audience will be able to:
reiterate three basic US techniques to increase needle conspicuity.
define the key steps in performing arthrograms of the shoulder, hip, elbow, and ankle.
explain the concept of hydrodisection and how to remove a foreign body.

Needle Visualization
Direct visualization is most important for success & safety
Insertion angle and needle gauge
Steeper the angle of insertion, the more difficult it is to visualize the needle.
Large bore needle has larger surface of reflection and less flexible (resists bending out of plane of US beam)
If background echogenic, lower gain

Small Angle = Better Visualization

Cyst Aspiration/Mass Bx
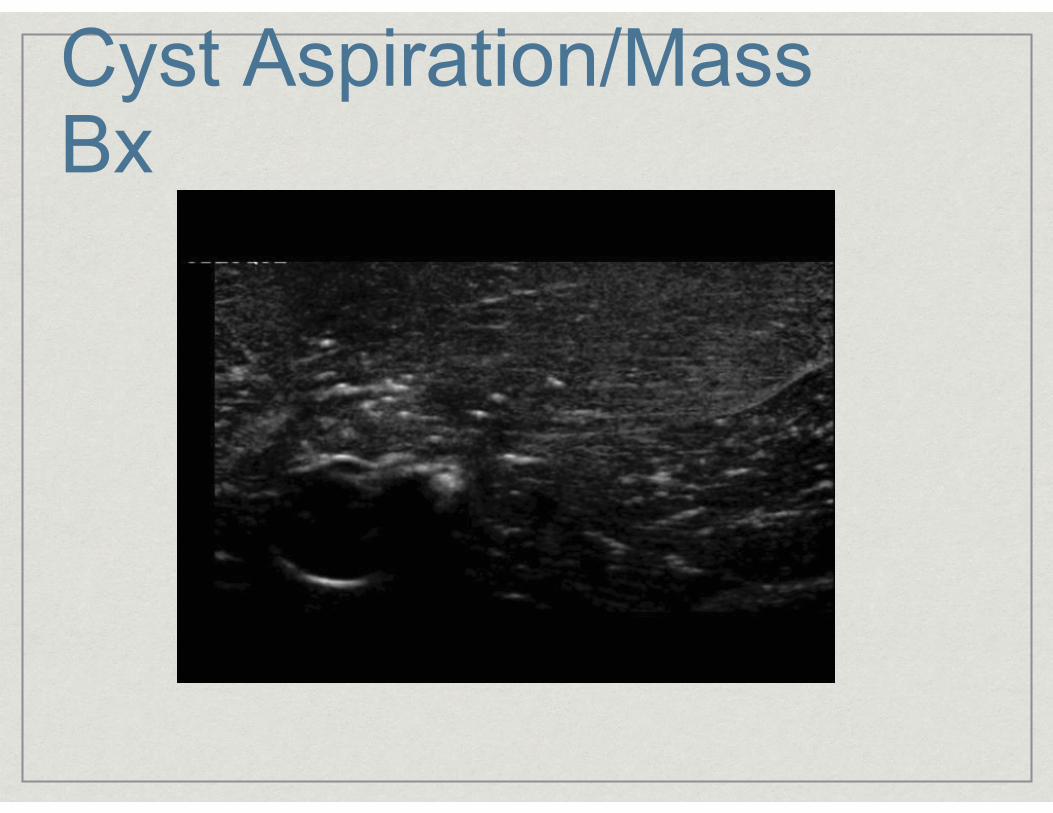
Cyst Aspiration/Mass Bx

Better Visualization
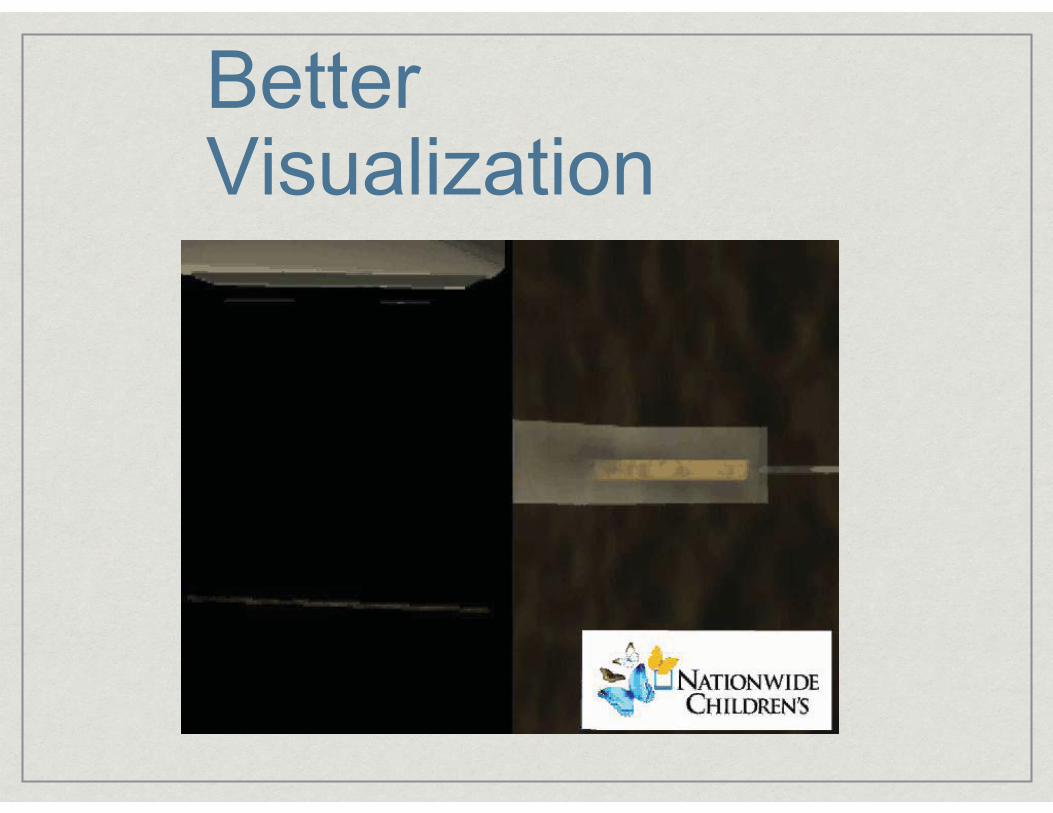
Better Visualization

Advancing Needle
DON’T advance blindly
Always know where needle tip is
Jiggling the needle slightly may help identify the tip, but only make tiny movements
In general hold probe hand steady; try to move only the needle
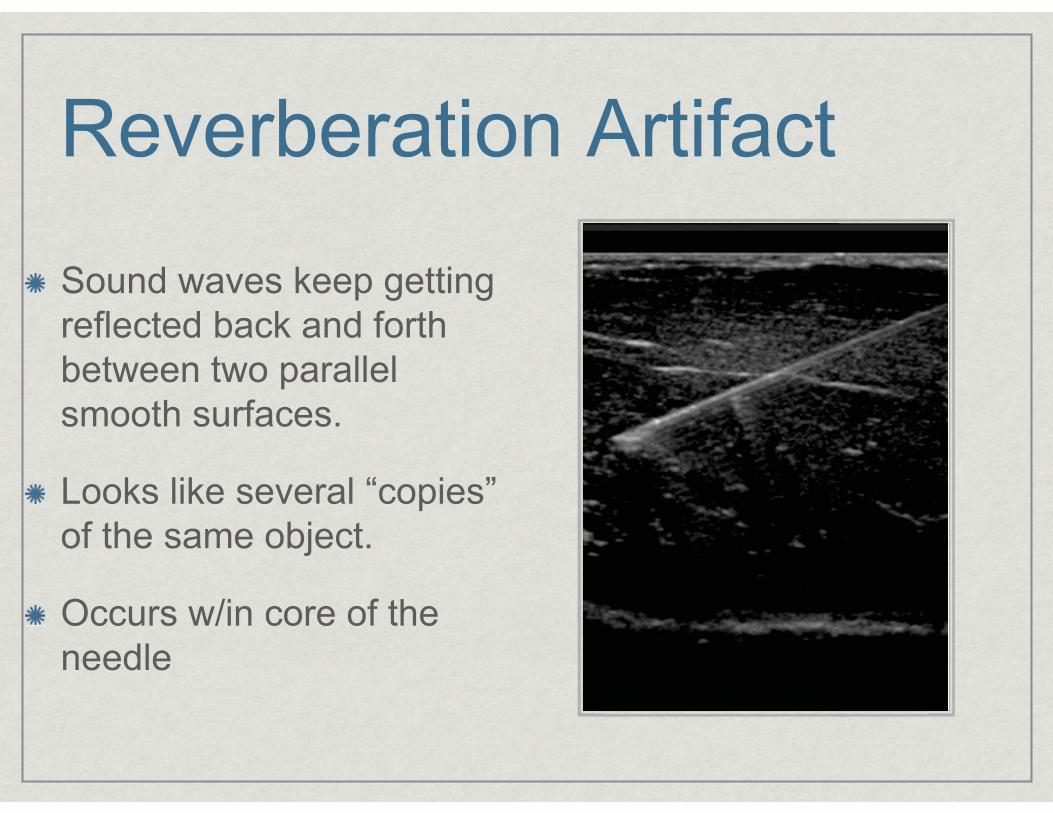
Reverberation Artifact
Sound waves keep getting reflected back and forth between two parallel smooth surfaces.
Looks like several “copies” of the same object.
Occurs w/in core of the needle

Tip Scatter

Before the procedure
Review prior imaging
Obtain informed consent
Time-out
Ready US machine; choose appropriate probe
Scan area and plan approach. Make marks as needed
Prep and drape
A GODDESS AMONG MORTALS - LESCHI, SEATTLE
LIGHT OF MY LIFE - CARKEEK PARK, SEATTLE

US guided arthrograms Is it just as effective as as fluoro guided arthrograms?
Choudur, et. al. Ultrasound Guided Gadolinium Joint Injections for Magnetic Resonance Arthrography. Journal of Clinical US. 2010.
99/100 joints successfully injected under US (shoulder, hip, knee, wrists)
1 patient has vasovagal reaction after local anesthetic and procedure aborted.
No studies in kids, AFAIK

US guided arthrograms
How to know the needle is in the joint
Visualize and feel needle tip “hitting” bone/cartilage
Visualize contrast solution flowing away from needle tip.
Minimal resistance to injection
Until comfortable with technique, I suggest using fluoro to verify contrast is in joint

US guided arthrograms Shoulder
Elbow
Wrist - I prefer fluoro
Hip
Knee
Ankle

My Arthrogram Cocktail
15 cc NS
5 cc Optiray (isoversol) 320 - if fluoro used for verification
0.1 cc Magnevist (.5 mol/L solution)
? Lidocaine: Although less profound than the effects of bupivacaine, lidocaine 1% and lidocaine 2% also exhibit dose-dependent and time-dependent toxic effects on bovine articular chondrocytes.*
Karpie JC, Chu CR. Lidocaine exhibits dose- and time-dependent cytotoxic effects on bovine articular chondrocytes in vitro. Am J Sports Med 2007;35:1622-7

Shoulder arthrogram
Patient positioning
Similar to conventional arthrogram
Supine, elbow extended, forearm supinated
22 G Spinal needle (20 G if very muscular)

Shoulder arthrogram
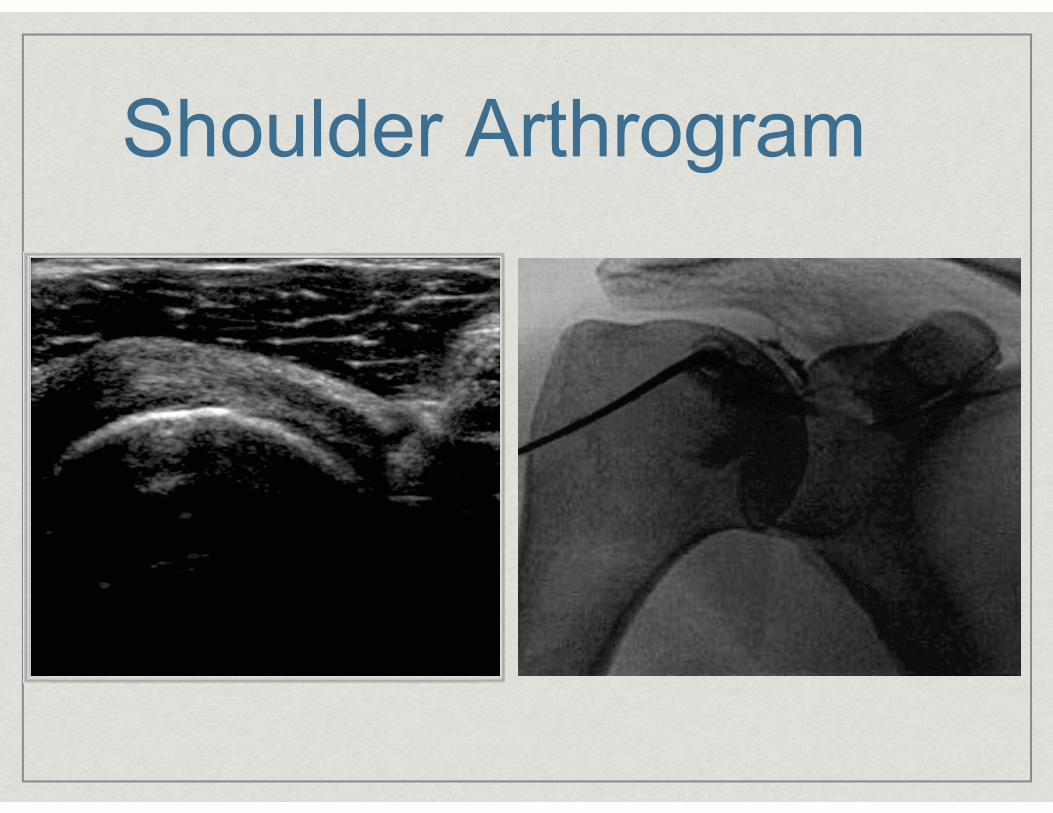
Shoulder Arthrogram

Shoulder arthrogram
Landmarks
Identify Coracoid process
Aim for humeral head just inferior and lateral to Coracoid process
Best to place needle between subscapularis and biceps tendons

DISCOVERING THE LIGHT - DISCOVERY PARK, SEATTLE

Elbow arthrogram Patient positioning
Whichever position is most comfortable for patient and operator (eg, prone with with elbow flexed by head; sitting with elbow on table)
Visualize the radial head/capitellum joint as best you can
25 G Injection needle adequate for both local anesthesia and contrast injection

Elbow arthrogram

Elbow Arthrogram

Elbow Arthrogram

Elbow arthrogram
Landmarks
I prefer to approach from the lateral aspect of the radio-capitellar joint
Carefully examine radiographs, especially if hx of fracture. Look for osteophytes
Remember joint is very superficial.

THE RED BRIDGE OF COURAGKUBOTA GARDEN, SEATTLE
Hip arthrogram
Patient positioning
Leg fully extended with foot in slight internal rotation
22 G Spinal needle (20 G if very muscular)

Hip arthrogram/tap

Hip arthrogram

Hip arthrogram

Hip arthrogram Landmarks
Locate the femoral artery and stay at least 3 finger widths lateral to it.
Method 1: Locate the Greater Tuberosity in transverse plane
Aim for femoral neck at level of the mid aspect of the greater tuberosity
Method 2: Parallel to femoral neck and aim for neck “concavity”

GOING, GOING, GOING... - RIZAL PARK, SEATTLE
Ankle arthrogram
Patient positioning
I find the “mortise view” (extension and slight adduction of foot) position best opens up the lateral tibiotalar joint.
22 G spinal needle

Ankle arthrogram

Ankle arthrogram

Ankle arthrogram
Landmarks
Must locate dorsalis pedis and avoid it.
Aim for the lateral gutter of the tibiotalar joint
I find it easiest to find the lateral malleolus with the US probe and work medially until the joint space is observed.
Pitfalls How easy it is to find the needle tip depends on
Body habitus
e.g. obese patients
Type of joint injected
e.g. Shoulder: difficult to localize needle between biceps and subscapularis tendons
Capacity of the joint
Presence of intra-articular fluid

Benefits of US guided arthrograms
No radiation to patient or radiologist
Realtime visualization of needle tip entering joint space
Plane of orientation of joint space varies in different individuals. With US, probe and needle can be tailored to individual joint orientation.
Benefits of US guided arthrograms No need to inject radiopaque contrast prior to Gad
Avoids rare complication of allergic reaction to inadvertent venous injection of iodinated contrast *
Jordan RM, Mintz RD. Fatal reaction to gadopentetate dimeglumine. AJR Am J Roentgenol 1999;172: 1141.
If intra-articular fluid present, US guided injection much easier
Can be performed in any room
Disadvantages of US guided arthrograms
Entire joint is not depicted on a single image
Only subchondral surfaces are visualized
Learning curve longer with MSK US than with fluoro
Narrowed joint space & presence of osteophytes better assessed with fluoro, but these are not common issues in pediatric population.

US guided arthrograms Personal Experience at Seattle Children’s (December 2010 - June 2012)
Shoulder: 22/22. Average 15 min
Elbow: 12/12. Average 5 min
Hip: 19/19. Average 15 min
Ankle (tibio-talar) 3/3. Average 10 min
Subtalar: 0
SI: 0
EACH FOR THE SKY - POINT OF ARCHES, OLYMPIC NATIONAL PAR

Foreign Body Removal
Can be very time intensive & fruitless - set a time limit
Make sure to visualize the longest axis of foreign body
Look carefully for small FB
Pre-scan to visualize important structures to avoid

Foreign body appearance
TX OBLIQUE LONGITUDINAL

Foreign Body Removal (Hydrodisection)

Foreign Body Removal (Hydrodisection)

Foreign Body Removal (Hydrodisection)

Foreign Body Removal (incorrect method)

Foreign Body Removal (correct method)

Foreign Body Removal
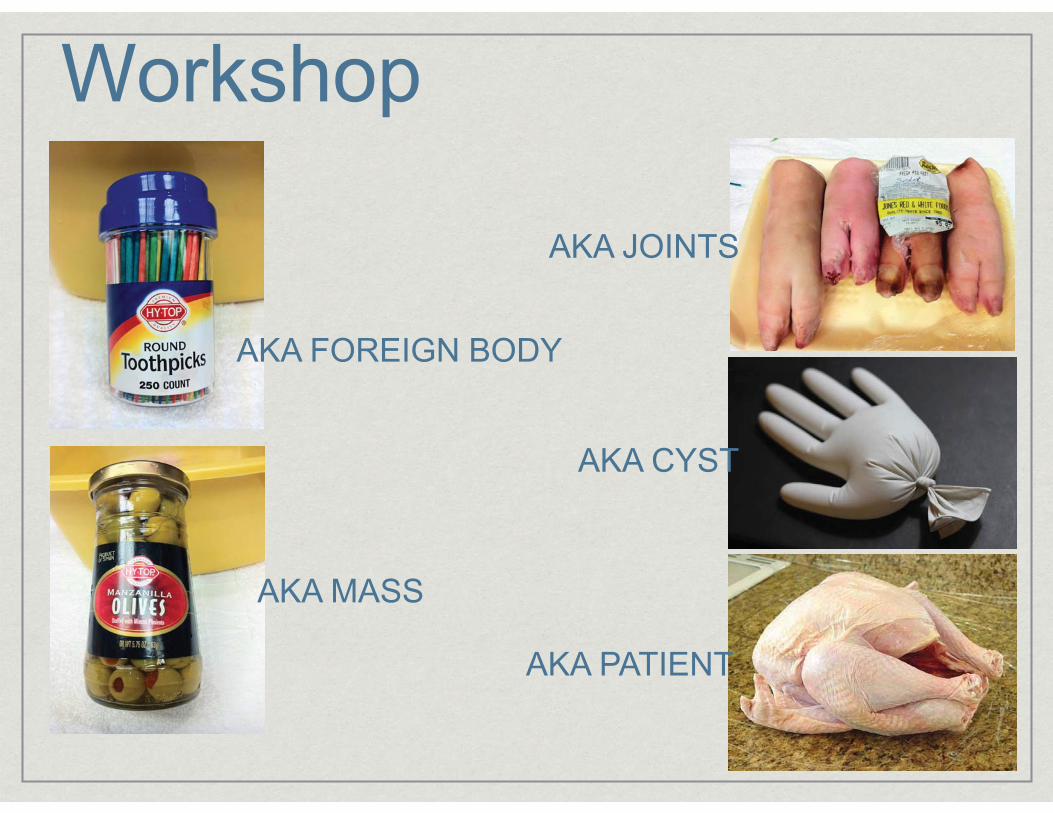
Workshop
AKA FOREIGN BODY
AKA MASS
AKA JOINTS
AKA CYST
AKA PATIENT

FREED WILLIES - SAN JUAN ISLANDS, WATHANK YOU [email protected]