Embed Size (px)
Citation preview

t
ULTRASONIC APPEARANCE OF ACUTE POSTSTREPTOCOCCAL GLOMERULONEPHRITIS
by David Rochester, MD*t; Andrew J. Aronson, MD $;James D. Bowie, MD*; and Axel Kunzmann, MD*
ABSTRACT We have described a case of acute post-streptococcal glomerulonephritis in which the ultrasound findings resemble multiple solid renal masses. The diagnosis of this inflam- matory lesion should be considered in the proper clinical setting.
Indexing Words Renal Ultrasound Renal Masses Glomerulonephritis
INTRODUCTION
The ultrasonic appearance of renal solid and cystic masses has been well described (1-3), but as yet there have been few descriptions of renal inflammatory lesions. A lack of familiarity with the ultrasonic appearance of glomerulone- phritis led us to an erroneous diagnosis of tumor.
CASE REPORT
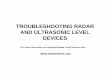
The patient was admitted to The University of Chicago Hospitals and Clinics at the age of 3 in 1971, when she was found to have a Wilms' tumor involving the right kidney and underwent a right nephrectomy. After doing 'well for five years, she was admitted in renal failure two weeks after an episode of pharyngitis. The ultra- sound examination of the remaining kidney demonstrated what appeared to be solid renal masses (Figs. 1A and 1B). To exclude a diagnosis of recurrent Wilms' tumor, an open biopsy was performed. The biopsy revealed a large, smooth left kidney with no evidence of masses. The biopsy indicated acute poststreptococcal glomer- ulonephritis. Postoperatively, she did well with the gradual return of renal function. The ultra- sound examination was repeated 10 months later, showing a return of the normal appearance of the kidney (Figs. 2A and 2B).
IA
From the Departments of Radiology* and Pediatrics. $ The
?Present Position (as of 7/1/77): Evanston Hospital, North-
Received June 30, 1977; revision accepted August 22, 1977. For reprints contact: David R ~ ~ ~ ~ ~ ~ ~ ~ , MD, ~~~~~t~~ ~ ~ ~ ~ i -
16
FIGURES 1A AND 16. Longitudinal and transverse scans of the left kidney show enlargement of the kidney with multiple "masses" containing low-level echoes. The "masses" are separ- ated by dense echo-producing bands.
University of Chicago.
western University, Evanston, Illinois.
tal, 2650 Ridge Avenue, Evanston, Illinois 60201.
JCU, Vol. 6 , 1-72 (1978).@1978, John Wiley and Sons, Inc.. 0091-2751/78/0006-0049 $01.00.
49

FIGURES 2A AND 2B. Ten months later the appearance of the kidney has returned to normal. The "masses" are no longer
DISCUSSION
Most cystic-appearing masses shown by renal ultrasound represent benign simple cysts, and most solid masses represent tumors. There are, however, execeptions to this generalization. A cyst-like appearance has been reported in hydronephrosis, xanthogranulomatous pyelone- phritis, renal hematoma, transitional cell carcin- oma, lymphoma, and adenocarcinoma with cen- tral necrosis or hemorrhage (1). Fewer solid- appearing lesions are not neoplastic : hemorrha- gic, infarcted, or multilobular cysts; xanthogran- ulomatous pyelonephritis; and lobar dysmorph- ism (2). Our case adds a further item to this list: acute glomerulonephritis. We speculate that the most likely explanation for this appearance is that focal differences in the amount of edema produce a mass-like effect, resulting in a variable appearance of the parenchyma from one portion
present, and the size of the kidney, particularly the anteroposter- ior dimension, has decreased.
of the organ to another. It may be that this same appearance will be found in other inflammatory diseases of the kidney.
SUMMARY
We have described a case of acute glomeru- lonephritis which had the ultrasonic appearance of multiple solid renal masses. In the proper age group and clinical setting, the ultrasonographer should consider this diagnosis when presented with the finding of multiple masses in the kid- ney.
REFERENCES 1. Green WM, King DC, Casarella WJ:A reappraisal of
sonolucent renal masses. Radiology 121:163, 1976. 2. Green WM, King DC: Diagnostic ultrasound of the
urinary tract. J Clin Ultrasound 4:35,1976. 3. Sanders RC: Renal ultrasound. Radio1 Clin North Am
13:505,1975.
50 JOURNAL OF CLINICAL ULTRASOUND