Embed Size (px)
Citation preview

UK guidelines on the management of varicealhaemorrhage in cirrhotic patientsDhiraj Tripathi1 Adrian J Stanley2 Peter C Hayes3 David Patch4 Charles Millson5
Homoyon Mehrzad6 Andrew Austin7 James W Ferguson1 Simon P Olliff6
Mark Hudson8 John M Christie9
1Liver Unit University HospitalsBirmingham NHS FoundationTrust Birmingham UK2GI Unit Glasgow RoyalInfirmary Glasgow UK3Liver Unit Royal Infirmary ofEdinburgh Edinburgh UK4The Royal Free Sheila SherlockLiver Centre Royal FreeHospital and University CollegeLondon London UK5Gastrointestinal and LiverServices York TeachingHospitals NHS FoundationTrust York UK6Department of InterventionalRadiology University HospitalsBirmingham NHS FoundationTrust Birmingham UK7Department ofGastroenterology DerbyHospitals NHS FoundationTrust Derby UK8Liver Unit Freeman HospitalNewcastle upon Tyne UK9Department ofGastroenterology Royal Devonand Exeter Hospital DevonUK
Correspondence toDr Dhiraj Tripathi Liver UnitQueen Elizabeth HospitalEdgbaston Birmingham B152TH UK DhirajTripathiuhbnhsuk dtripathibhamacuk
Received 28 January 2015Revised 11 March 2015Accepted 17 March 2015
To cite Tripathi DStanley AJ Hayes PC et alGut Published Online First[please include Day MonthYear] doi101136gutjnl-2015-309262
ABSTRACTThese updated guidelines on the management ofvariceal haemorrhage have been commissioned by theClinical Services and Standards Committee (CSSC) of theBritish Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG The originalguidelines which this document supersedes were writtenin 2000 and have undergone extensive revision by 13members of the Guidelines Development Group (GDG)The GDG comprises elected members of the BSG liversection representation from British Association for theStudy of the Liver (BASL) and Liver QuEST a nursingrepresentative and a patient representative The qualityof evidence and grading of recommendations wasappraised using the AGREE II toolThe nature of variceal haemorrhage in cirrhotic
patients with its complex range of complications makesrigid guidelines inappropriate These guidelines dealspecifically with the management of varices in patientswith cirrhosis under the following subheadings(1) primary prophylaxis (2) acute variceal haemorrhage(3) secondary prophylaxis of variceal haemorrhage and(4) gastric varices They are not designed to deal with(1) the management of the underlying liver disease(2) the management of variceal haemorrhage in childrenor (3) variceal haemorrhage from other aetiologicalconditions
Summary of all recommendationsRecommendations primary prophylaxis of varicealhaemorrhage in cirrhosis (Figure 2)1 What is the best method for primary prophylaxis11 We recommend non-cardioselective β
blockers (NSBB) or variceal band ligation(VBL) We suggest pharmacological treat-ment with propranolol as first line VBL isoffered if there are contraindications toNSBB The choice of VBL or NSBB shouldalso take into account patient choice (level1a grade A)
12 We suggest carvedilol or nadolol as alterna-tives to propranolol (level 1b grade A)
13 Dose131 Propranolol 40 mg twice daily Dose
titrated to maximum tolerated or onceheart rate (HR) of 50ndash55 bpm isreached to a maximum dose of320 mg (level 1a grade A)
132 Nadolol 40 mg daily dose Dosetitrated to maximum tolerated oronce HR of 50ndash55 bpm is reached a
maximum dose of 240 mg (level 1agrade A)
133 Carvedilol 625 mg once daily toincrease to maintenance of 125 mgafter a week if tolerated or once HRof lt50ndash55 bpm is reached (level 1agrade A)
134 It is suggested that NSBB are discon-tinued at the time of spontaneousbacterial peritonitis renal impair-ment and hypotension (level 2bgrade B)
14 In cases of contraindications or intoleranceto NSBB we recommend variceal bandligation (level 1a grade A)
2 Who should have surveillance for varicealbleeding21 We recommend all patients with cirrhosis
should be endoscoped at the time of diag-nosis (level 1a grade A) There is no indica-tion to repeat endoscopy in patientsreceiving NSBB
3 How often should cirrhotic patients beendoscoped31 If at the time of first endoscopy no varices
are seen we suggest that patientswith cirrhosis should be endoscoped at2ndash3-year intervals (level 2a grade B)
32 If grade I varices are diagnosed we suggestthat patients should be endoscoped at yearlyintervals (level 2a grade B)
33 If there is clear evidence of disease progres-sion we suggest that the intervals can bemodified by the clinician Endoscopy shouldalso be offered at time of decompensation(level 2a grade B)
4 Which patients with cirrhosis should haveprimary prophylaxis41 If grade I varices and red signs or grade 2ndash
3 varices are diagnosed we recommendthat patients have primary prophylaxis irre-spective of the severity of the liver disease(level 1a grade A)
5 Treatments not recommended51 Proton pump inhibitors are not recom-
mended unless otherwise required forpeptic ulcer disease (level 1b grade B)
52 Isosorbide mononitrate monotherapy is notrecommended as primary prophylaxis (level1b grade A) There is insufficient evidenceto recommend isosorbide mononitrate incombination with NSBB (level 1b grade A)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 1
Guidelines
53 Shunt surgery or transjugular intrahepatic portosystemicstent shunt (TIPSS) is not recommended as primaryprophylaxis (level 1a grade A)
54 Sclerotherapy is not recommended as primary prophy-laxis (level 1a grade A)
6 Areas requiring further study61 Role of NSBB in patients without varices with focus on
carvedilol62 Role of NSBB in patients with small varices with focus
on carvedilol63 Comparison of carvedilol versus propranolol in primary
prophylaxis64 Identification of and trials assessing new drugs for
primary prophylaxis such as statins7 Quality indicator
71 Percentage of patients at diagnosis of cirrhosis who havehad an endoscopy to screen for varices (level 1agrade A)Numerator patients diagnosed with cirrhosis who havehad an endoscopy either before or after diagnosis within6 monthsDenominator patients newly diagnosed with cirrhosis
72 Percentage of patients receiving primary prophylaxisamong those newly diagnosed with grade I varices andred signs or grade 2ndash3 varicesNumerator patients who have grade 1 varices with redsigns or grade 2ndash3 varices receiving primary prophylaxisDenominator patients diagnosed with cirrhosis whohave grade I varices with red signs or grade 2ndash3 varices
Recommendations control of active variceal haemorrhage incirrhosis (Figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with blood pla-telets and clotting factors in line with local protocols formanaging massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusion policyaiming for a haemoglobin of 70ndash80 gL is suggested inhaemodynamically stable patients (level 1b grade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable (level5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L (level5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to local cir-cumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with sus-
pected or confirmed variceal bleeding (level 1agrade A)
32 In all patients vasoconstrictors such as terlipressin orsomatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding41 If bleeding is difficult to control a Sengstakenndash
Blakemore tube should be inserted until furtherendoscopic treatment TIPSS or surgery is performeddepending on local resources and expertise (level 1bgrade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure(level 1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
2 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or whenmonotherapy with VBL or NSBB is used owing tointolerance or contraindications to combination therapy)and in selected cases owing to patient choice PTFE-covered stents are recommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
Recommendations management of active haemorrhage fromgastric varices (Figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices11 Gastro-oesophageal varices (GOV)-1 treat as for
oesophageal varices (level 2b grade B)12 GOV-2 and isolated gastric varices (IGV)
121 We recommend initial endoscopic therapy withcyanoacrylate injection (level 1a grade A)
122 Thrombin may also be considered (level 4 grade C)13 TIPSS can be considered depending on local resources
and clinical judgement (level 3a grade B)2 If control of bleeding fails
21 Balloon tamponade is suggested for GOV and IGV-1until definitive treatment is undertaken (level 2b grade B)
22 Salvage TIPSS is suggested as the first-line definite treat-ment where feasible (level 3a grade B)
23 Balloon-occluded retrograde transvenous obliteration(B-RTO) or surgical shunting can be considered if TIPSSis not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered into
a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (level2b grade B) Note the optimum endoscopic follow-upstrategy remains unclear Thrombin can also be consid-ered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 3
Guidelines
56 Role of endoscopic ultrasound-guided injection of tissueadhesives or thrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
INTRODUCTIONThe guidelines refer closely to the Baveno V consensus state-ment published in 20101 and the 2012 NICE Guidelines onAcute Upper GI bleeding (CG141)2 These documents arewidely used and offer useful evidence-based guidance Howeverwe feel that owing to significant recent advances further addi-tions and refinements to the published guidance with particularfocus on resource implications service development and thepatient pathway are necessary The previously mentioned docu-ments1 2 do not cover all the recent advancesmdashin particular inthe field of acute variceal bleeding and the role of transjugularintrahepatic portosystemic stent shunt (TIPSS) There have alsobeen developments and better insights into drug treatment forprevention of varices and variceal bleedingmdashin particular therole of non-cardioselective β blockers (NSBB)
Guideline developmentThese guidelines were drafted after discussions within the liversection of the British Society of Gastroenterology (BSG) andacceptance of the proposal by the Clinical Services andStandards Committee (CSSC) There followed division of sec-tions to be researched by designated authors and an exhaustiveliterature review The Baveno V consensus and NICE guidelineswere closely followed and guideline quality was assessed usingthe AGREE tool3 (section lsquoAssessing the quality of guidelinesthe AGREE II instrumentrsquo)
A preliminary guideline document was drafted by the authorsfollowing discussion and where necessary voting by membersof the Guidelines Development Group (GDG) The draft guide-lines were submitted for review by CSSG then BSG councilmembers Finally full peer review was undertaken by reviewersselected by the editor of Gut
Attempts were made to preserve the format of the originalguidelines with additional sections relating to service develop-ment the patient pathway and pre-primary prophylaxis Thesection on the management of acute variceal bleeding has beenextensively rewritten to take into account recent importantdevelopments in interventional radiology drug treatment andresuscitation
Assessing the quality of guidelines the AGREE II instrumentThe AGREE II instrument is an accepted method for appraisingclinical guidelines3 Six domains are listed
Scope and purposeThe guidelines are intended for use by clinicians and otherhealthcare professionals managing patients with cirrhosis andgastro-oesophageal varices in light of recent guidance publishedby NICE2 and the Baveno V Consensus1 Important subsequentdevelopments are covered in depth due to the potential impacton clinical practice The guidelines are primarily aimed at man-agement of adult patients
Guideline development group membership and stakeholderinvolvementMembership of the group includes gastroenterologists hepatolo-gists and interventional radiologists with nursing and patientrepresentation
Rigour of developmentThe published literature was searched using Pubmed MedlineWeb of Knowledge and the Cochrane database between October2013 and February 2015 The GDG met through a series of tel-econferences during that time The guidelines rely considerablyon consensus statements published by the Baveno V Consensusand NICE1 2 The style of graded recommendations is deter-mined by the level of supporting evidence (graded level 1 to 5)as described by the Oxford Centre For Evidence BasedMedicine4 (table 1) and is as followsA consistent level 1 studiesB consistent level 2 or 3 studies or extrapolations from level 1
studiesC level 4 studies or extrapolations from level 2 or 3 studiesD level 5 evidence or troublingly inconsistent or inconclusive
studies of any levelAreas of disagreement about the recommendation grade were
subjected to discussion and if necessary voting by members ofthe guidelines group Where possible the health benefits sideeffects and risks of recommendations have been discussed Theguidelines were subject to peer review after submission for con-sideration of publication in Gut
Clarity and presentationRecommendations are intended to be specific to particular situa-tions and patient groups where necessary different options arelisted Key recommendations are linked to discussion threads ona discussion forum hosted on the BSG website
ApplicabilityWhere necessary we have discussed organisational changes thatmay be needed in order to apply recommendations We haveattempted to identify key criteria for monitoring and auditpurposes
Editorial independence and conflict of interestGuideline group members have declared any conflicts ofinterest
Scheduled review of guidelinesThe proposed time for review of the guidelines is 5 years totake into account new developments To ensure that there is afacility for feedback after publication links to the BSG discus-sion forums corresponding to the particular section of theseguidelines are included with this document This facility toprovide new evidence is provided to all BSG members Inaccordance with the AGREE II tool the BSG forum will providefeedback
SERVICE DELIVERY AND DEVELOPMENTDespite improvements in outcomes following variceal bleedingthe need to optimise the management of acute variceal bleed-ing is highlighted in recent publications and national reportsIn a national audit5 variceal bleeding accounted for just over10 of all admissions with acute GI bleeding in the UK withtwo-thirds having a previous history of variceal bleeding andover 50 presenting during normal working hours Endoscopywithin 24 h of presentation was achieved in only 66 of allpatients and in 70 of patients with documented cirrhosisMost procedures were performed in the endoscopy depart-ment with just 14 performed under general anaestheticdespite high-risk stigmata and endoscopic therapy beingrequired in two-thirds of cases Notably antibiotics were
4 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
administered in only 27 of patients before endoscopy andadministration of vasoactive drugs before endoscopy was onlyslightly higher at 44 Furthermore only four patients (lt1)were referred for TIPSS which may reflect the lack of accessto interventional radiology and that the audit was conductedbefore the trial of early TIPSS6 The National ConfidentialEnquiry into Patient Outcome and Death (NCEPOD) reportlsquoMeasuring the unitsrsquo assessed clinical management beforedeath of 594 patients with alcoholic liver disease over a6-month period in the UK7 Gastrointestinal bleeding wasnoted in 35 of cases with approximately 50 having vari-ceal bleeding Delays in endoscopy were noted in 10 ofcases and several aspects of clinical andor organisational carewere judged to be poor or unacceptable in 18 of patientspresenting with GI bleeding There were deficiencies noted inthe out-of-hours rotas for GI bleeding with 27 of hospitalsnot having a dedicated-out-of hours GI bleeding serviceStudies from other countries have also reported deficiencieswith delays in admission to hospital and administration of anti-biotics Two observational studies showed that access to
emergency endoscopy and use of prophylactic antibiotics andvasoactive drugs was better in tertiary centres although thisdid not appear to affect survival8 9
Acute variceal haemorrhage refractory to endoscopic andpharmacological treatments where TIPSS is usually indicatedmust be managed with appropriate resources TIPSS is an estab-lished interventional treatment for refractory or recurrent vari-ceal haemorrhage It remains a highly specialised procedurerequiring adequate training and experience Knowledge of therelevant equipment anatomy and how to deal with any compli-cations is essential It should therefore be performed in centreswith adequate personnel multidisciplinary support and equip-ment required to optimise management and minimise risks10
Regional centres with easily accessible interventional radiologyservices are generally best equipped to perform this procedureSetting up regional agreements and pathways to allow transfer ofappropriate patients to hospitals that undertake TIPSS proce-dures is an important step These pathways could also be used toprovide emergency endoscopic management if necessary due toproblems with out-of-hours endoscopic cover in smaller
Table 1 Levels of evidence
LevelTherapyprevention aetiologyharm Prognosis Diagnosis DDXsymptom prevalence study
1a SR (with homogeneity) ofrandomised controlled trial (RCT)
SR (with homogeneity) of inceptioncohort studies CDRdagger validated indifferent populations
SR (with homogeneity) of level 1diagnostic studies CDRdagger with 1b studiesfrom different clinical centres
SR (with homogeneity) ofprospective cohort studies
1b Individual RCT (with narrow CI) Individual inception cohort study withge80 follow-up CDRdagger validated in asingle population
ValidatingDagger cohort study with goodsectreference standards or CDRdagger testedwithin one clinical centre
Prospective cohort study with goodfollow-uppara
1c All or none All or none case series Absolute SpPins and SnNoutsdaggerdagger All or none case series2a SR (with homogeneity) of cohort
studiesSR (with homogeneity) of eitherretrospective cohort studies or untreatedcontrol groups in RCTs
SR (with homogeneity) of level gt2diagnostic studies
SR (with homogeneity) of 2b andbetter studies
2b Individual cohort study (includinglow-quality RCT eg lt80follow-up)
Retrospective cohort study or follow-upof untreated control patients in an RCTderivation of CDRdagger or validated on splitsampleDaggerDagger only
ExploratoryDagger cohort study with goodsectreference standards CDRdagger afterderivation or validated only on splitsampleDaggerDagger or databases
Retrospective cohort study or poorfollow-up
2c lsquoOutcomesrsquo research ecologicalstudies
lsquoOutcomesrsquo research Ecological studies
3a SR (with homogeneity) of casendashcontrol studies
SR (with homogeneity) of 3b and betterstudies
SR (with homogeneity) of 3b andbetter studies
3b Individual casendashcontrol study Non-consecutive study or withoutconsistently applied reference standards
Non-consecutive cohort study orvery limited population
4 Case series (and poor qualitycohort and case-control studiessectsect)
Case series (and poor quality prognosticcohort studiesparapara)
Casendashcontrol study poor ornon-independent reference standard
Case series or superseded referencestandards
5 Expert opinion without explicitcritical appraisal or based onphysiology bench research or lsquofirstprinciplesrsquo
Expert opinion without explicit criticalappraisal or based on physiology benchresearch or lsquofirst principlesrsquo
Expert opinion without explicit criticalappraisal or based on physiology benchresearch or lsquofirst principlesrsquo
Expert opinion without explicitcritical appraisal or based onphysiology bench research or lsquofirstprinciplesrsquo
Homogeneity means a systematic review (SR) that is free of worrisome variations (heterogeneity) in the directions and degrees of results between individual studies Not all SRs withstatistically significant heterogeneity need be worrisome and not all worrisome heterogeneity need be statistically significantdaggerCDR Clinical Decision Rule (algorithms or scoring systems which lead to a prognostic estimation or a diagnostic category)DaggerValidating studies test the quality of a specific diagnostic test based on prior evidence An exploratory study collects information and trawls the data (eg using a regression analysis) tofind which factors are lsquosignificantrsquosectGood reference standards are independent of the test and applied blindly or objectively to all patients Poor reference standards are haphazardly applied but still independent of thetest Use of a non-independent reference standard (where the lsquotestrsquo is included in the lsquoreferencersquo or where the lsquotestingrsquo affects the lsquoreferencersquo) implies a level 4 studyparaGood follow-up in a differential diagnosis study is gt80 with adequate time for alternative diagnoses to emerge (eg 1ndash6 months acute 1ndash5 years chronic)Met when all patients died before the treatment became available but some now survive while receiving it or when some patients died before the treatment became available butnone now die while receiving itdaggerdaggerAn lsquoabsolute SpPinrsquo a diagnostic finding whose Specificity is so high that a Positive result rules in the diagnosis An lsquoAbsolute SnNoutrsquo a diagnostic finding whose Sensitivity is sohigh that a Negative result rules out the diagnosisDaggerDaggerSplit-sample validation is achieved by collecting all the information in a single tranche then artificially dividing this into lsquoderivationrsquo and lsquovalidationrsquo samplessectsectPoor quality cohort study one that failed to clearly define comparison groups andor failed to measure exposures and outcomes in the same (preferably blinded) objective way inboth exposed and non-exposed individuals andor failed to identify or appropriately control known confounders andor failed to carry out a sufficiently long and complete follow-up ofpatients Poor quality casendashcontrol study one that failed to clearly define comparison groups andor failed to measure exposures and outcomes in the same (preferably blinded)objective way in both cases and controls andor failed to identify or appropriately control known confoundersparaparaPoor quality prognostic cohort study one in which sampling was biased in favour of patients who already had the target outcome or the measurement of outcomes wasaccomplished in lt80 of study patients or outcomes were determined in an unblinded non-objective way or there was no correction for confounding factors
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 5
Guidelines
hospitals This model referred to as ldquospoke and wheelrdquo ornetwork model is well established for other complex proceduresand helps to expedite and streamline the process In theNCEPOD report lsquoMeasuring the unitsrsquo just 15 of hospitals hadon-site access to TIPSS while 72 had access to TIPSS in othercentres7
There have been significant efforts to address the need toimprove the upper GI bleeding (UGIB) service A toolkit wasproduced in collaboration with BSG Association of UpperGastrointestinal Surgeons (AUGIS) Royal Colleges ofPhysicians Radiology and Nursing and Academy of MedicalRoyal Colleges11 The key nine service standards recommendedby the document are detailed below1 There will be a nominated individual with the authority to
ensure implementation by the contracted provider2 Contracted providers will ensure the minimum service is
adequately resourced3 All patients with suspected UGIB should be properly
assessed and their risk scored on presentation4 All patients should be resuscitated before therapeutic
intervention5 All high-risk patients with UGIB should be endoscoped
within 24 h preferably on a planned list in the first instance6 For patients who require more urgent intervention either for
endoscopy interventional radiology or surgery formal 247arrangements must be available
7 The necessary team meeting an agreed competency levelshould be available throughout the complete patient pathway
8 Each stage of the patient pathway should be carried out inan area with lsquoappropriatersquo facilities equipment and supportincluding staff experienced in the management of UGIB
9 All hospitals must collect a minimum dataset in order tomeasure service provision against auditable outcomes(case-mix adjusted as appropriate)NICE recommendations for endoscopy provision are detailed
in the section lsquoManagement of active variceal haemorrhagersquorecommendations2 The BSG has also produced a care bundlefor patients admitted with decompensated cirrhosis in light ofthe NCEPOD report with a check list method which includesgastrointestinal bleeding12
Since the 2008 Darzi report quality has become a priorityfor the NHS13 With these guidelines there is real opportunityto introduce quality outcomes based on good clinical evidenceFurthermore by incorporating them into the liver accreditationscheme Liver Quest one can improve and assure quality inliver services across the UK14 Therefore a small number ofquality outcomes measures have been chosen and form part ofthe key recommendations15
DEFINITIONSIt is important to define the terms that should be used in thecontext of a variceal bleed These are the Baveno V consensusdefinitions1
Variceal haemorrhageVariceal haemorrhage is defined as bleeding from an oesopha-geal or gastric varix at the time of endoscopy or the presence oflarge oesophageal varices with blood in the stomach and noother recognisable cause of bleeding An episode of bleeding isclinically significant when there is a transfusion requirement for2 units of blood or more within 24 h of the time zero togetherwith a systolic blood pressure of lt100 mm Hg or a posturalchange of gt20 mm Hg andor pulse rate gt100 bpm at time
zero (time zero is the time of admission to the first hospital towhich the patient is taken)
Time frame of acute bleedingThe acute bleeding episode is represented by an interval of120 h (5 days) from time zero Evidence of any bleeding after120 h is the first rebleeding episode
Failure to control active bleedingFailure to control active bleeding is defined as death or need tochange treatment defined by one of the following criteria16 17
1 Fresh haematemesis or nasogastric aspiration of ge100 mL offresh blood ge2 h after the start of a specific drug treatmentor therapeutic endoscopy
2 Development of hypovolaemic shock3 30 gL drop in haemoglobin (9 drop of haematocrit)
within any 24 h period if no transfusion is given This timeframe needs to be further validated
Variceal rebleedingVariceal rebleeding is defined as the occurrence of a singleepisode of clinically significant rebleeding from portal hyperten-sive sources from day 5 Clinically significant rebleeding isdefined as recurrent melaena or haematemesis in any of the fol-lowing settings1 hospital admission2 blood transfusion3 30 gL drop in haemoglobin4 death within 6 weeks
Early mortalityDeath within 6 weeks of the initial episode of bleeding
NATURAL HISTORY OF VARICES IN CIRRHOSISDevelopment of varicesThe rise in portal pressure is associated with the developmentof collateral circulation which allows the portal blood to bediverted into the systemic circulation These spontaneous shuntsoccur (a) at the cardia through the intrinsic and extrinsic gastro-oesophageal veins (b) in the anal canal where the superiorhaemorrhoidal vein belonging to the portal system anastomoseswith the middle and inferior haemorrhoidal veins which belongto the caval system (c) in the falciform ligament of the liverthrough the para-umbilical veins which are the remains of theumbilical circulation of the fetus (d) in the abdominal wall andthe retroperitoneal tissues from the liver to the diaphragmveins in the lienorenal ligament in the omentum and lumbarveins and (e) blood diversion from the diaphragm gastric pan-creatic splenic and adrenal veins which may drain into the leftrenal vein
Numerous lines of evidence suggest that varices develop andenlarge with time Christensen et al18 followed up a cohort of532 patients with cirrhosis and showed that the cumulative inci-dence of patients with varices increased from 12 to 90 over12 years In a study involving 80 patients followed up for16 months Cales and Pascal19 showed that 20 of patientswho did not have varices developed new varices and 42 ofpatients with small varices showed definite enlargement Czajaet al20 also showed that the prevalence of varices increased from8 to 13 over 5 years in a cohort of patients with chronicactive hepatitis even though they were treated with prednisol-one Merli et al21 in a study of 213 patients with cirrhosis withno or small varices demonstrated that the annual progression ofvarices was 12 A recent database analysis by DrsquoAmico et al22
6 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
using a competing risk model showed that the cumulative inci-dence of varices at 10 and 20 years was 44 and 53 respect-ively suggesting an overestimation in previous studies not usinga competing risk model
The main factors that appear to determine the developmentof varices are continued hepatic injury the degree of portosyste-mic shunting endoscopic appearances and portal pressureEvidence for the role of hepatic injury is derived from studies inwhich varices were shown to regress with time Baker et al23 fol-lowed up a cohort of 115 patients with oesophageal varices andshowed that varices had disappeared in nine patients regressedin seven and remained unchanged in six They concluded thatthe disappearance and regression of varices might be related toabstinence from alcohol This observation was confirmed in astudy by Dagradi24 who followed up a cohort of patients withalcoholic cirrhosis over 3 years and showed a reduction in vari-ceal size in 12 of the 15 patients with alcoholic cirrhosis whostopped drinking and an enlargement in variceal size in 17patients who continued to drink On the other hand Cales andPascal19 showed that regression of varices occurred in 16 ofpatients with alcoholic cirrhosis who continued to imbibealcohol This might be related to the development of large por-tosystemic collaterals which decompress the portal system andreduce the risk of the development of large oesophageal varicesThe degree of portosystemic shunting can be quantified bymeasuring the diameter of portal veins and collaterals and canbe significant in those with gastrorenal or splenorenal shunt-ing25 26 Others have shown that the presence of alcoholic cir-rhosis Childrsquos B or C cirrhosis and red whale signs on indexendoscopy predicted progression of varices21 Groszmannet al27 in a placebo-controlled randomised trial of timolol in213 cirrhotic patients without varices showed that a baselinehepatic venous pressure gradient (HVPG) of gt10 mm Hg or age10 increase in HVPG during follow-up were both predictiveof the development of varices
Diagnosis of gastro-oesophageal varicesUntil recently endoscopy has been used exclusively to diagnosevarices Non-invasive methods of screening for varices includecapsule endoscopy transient elastography and use of laboratoryand radiological findings
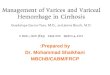
EndoscopyThere is universal acceptance that endoscopy is the lsquogold stand-ardrsquo for diagnosing gastro-oesophageal varices The main limita-tions are intraobserver variability in the diagnosis of small orgrade I oesophageal varices (figure 1AndashC) Recently unsedatednasal gastroscopy has been found to have similar accuracy toconventional endoscopy and has the advantage of tolerabilityand potential cost saving since it can be performed in the clinicsetting in some institutions28 29 However there are no con-trolled studies and banding of varices is not possible
Capsule endoscopyCapsule endoscopy uses a 26 mm pill-shaped device whichtransmits video footage which is stored and later analysedPatients are not sedated but patient cooperation is essentialIn a large study by de Franchis et al30 capsule endoscopy wascompared with standard gastroscopy The primary end point of90 or greater concordance was not achieved Lapalus et al31
in a prospective study of 120 patients demonstrated similarresults with capsule endoscopy Therefore capsule endoscopycannot be considered an alternative to standard endoscopyalthough may have a role in patient who refuse gastroscopy
Transient elastographyTransient elastography ((FibroScan Echosens Paris France) usesthe principles of ultrasound to derive tissue stiffness by measur-ing the speed of propagation of a low-frequency wave whichthen correlates with liver fibrosis Vizzutti et al32 in a study of61 patients with hepatitis C showed a sensitivity for predictionof oesophageal varices of 90 using a threshold 176 kPaHowever specificity was poor at 43 A study of 298 patientsfound the optimal cut-off point for the prediction of oesopha-geal varices was 215 kPa (sensitivity 76 and specificity78)33 In one uncontrolled study the use of transient elasto-graphy was found to be as effective as HVPG at predictingportal hypertension-related complications34 Therefore the roleof transient elastography in predicting varices is controversialdue to the lack of consistent results and controlled studies Thismodality may be more useful for predicting decompensation inpatients with cirrhosis
Radiological and serum parametersA prospective study of 311 patients with chronic hepatitis Cshowed that a platelet-to-spleen size ratio with a threshold of909 had positive and negative predictive values of 100 and94 respectively35 These good results have not been repro-duced by others as demonstrated in a meta-analysis36
Risk factors for first variceal bleedingThe factors that predispose to and precipitate variceal haemor-rhage are still not clear The suggestion that oesophagitis mayprecipitate variceal haemorrhage has been discarded37
Presently the most important factors that have been heldresponsible include (i) pressure within the varix (ii) varicealsize (iii) tension on the variceal wall and (iv) severity of theliver disease
Portal pressureIn most cases portal pressure reflects intravariceal pressure38
and a HVPG gt10 mm Hg is necessary for the development ofoesophageal varices27 There is no linear relationship betweenthe severity of portal hypertension and the risk of varicealhaemorrhage although HVPG gt12 mm Hg is an accepted
Figure 1 (A) Grade I oesophagealvarices These collapse to inflation ofthe oesophagus with air (B) Grade IIoesophageal varices These are varicesbetween grades 1 and 3 (C) Grade IIIoesophageal varices These are largeenough to occlude the lumen
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 7
Guidelines
threshold for variceal bleeding39 40 However the HVPG tendsto be higher in bleeders as well as in patients with larger varicesIn a prospective study comparing propranolol with placebo forthe prevention of first variceal haemorrhage Groszmann et al41
showed that bleeding from varices did not occur if the portalpressure gradient (PPG) could be reduced to lt12 mm HgOthers have shown that a 20 reduction in portal pressure pro-tects against further bleeding42 These haemodynamic goalshave been accepted as the aim of pharmacological treatment ofportal hypertension It is important to appreciate that gastricvarices can bleed at pressures lt12 mm Hg and the influence ofwall tension of the varix plays a greater role in the risk of bleed-ing43 A greater pressure reduction may be necessary to protectagainst bleeding This is further discussed in the section lsquoGastricvaricesrsquo At present measurement of portal pressure in guidingpharmacological treatments is limited to clinical trials in the UK
Variceal sizeVariceal size is best assessed endoscopically (figure 1AndashC)Published results are variable owing to the lack of a definition dis-tinguishing between large and small varices Small (grade I)varices tend to be narrow and flatten easily with air whereaslarger (grade 2 and 3) varices are usually broader and flatten withdifficulty if at all Numerous studies40 44 have shown that therisk of variceal haemorrhage increases with the size of varices45
Variceal wall and tensionPolio and Groszmann46 using an in vitro model showed thatrupture of varices was related to the tension on the varicealwall The tension depends on the radius of the varix In thismodel increasing the size of the varix and decreasing the thick-ness of the variceal wall caused variceal rupture Recently endo-scopic ultrasound and manometry have been used to estimatewall tension of varices47
Endoscopic features such as lsquored spotsrsquo and lsquowhalersquo markingswere first described by Dagradi24 They have been described asbeing important in the prediction of variceal haemorrhageThese features represent changes in variceal wall structure andtension associated with the development of microtelangiectasiasand reduced wall thickness In a retrospective study by theJapanese Research Society for Portal Hypertension Beppuet al48 showed that 80 of patients who had blue varices orcherry red spots bled from varices suggesting that this was animportant predictor of variceal haemorrhage in cirrhosis
Severity of liver disease and bleeding indicesTwo independent groups prospectively assessed factors predict-ing first variceal haemorrhage in cirrhosis (table 2) The NorthItalian Endoscopic Club (NIEC)49 reported their findings in1988 followed in 1990 by data from the Japanese50 Both thesestudies showed that the risk of bleeding was based on threefactors severity of liver disease as measured by Child class vari-ceal size and red wale markings The NIEC study showed awide range for the risk of bleeding of 6ndash76 depending on thepresence or absence of the different factors Using the same vari-ables the NIEC index was simplified by de Franchis et al51 andshown to correlate with the original index Further studiesshowed that the HVPG and intravariceal pressure were alsoindependent predictors of first variceal haemorrhage when ana-lysed in conjunction with the NIEC index52 53
In summary the most important factors that determine the risk ofvariceal haemorrhage are the severity of liver disease size of varicesand presence of red signs Measurement of HVPG is a useful guidefor selection of patients for treatment and their response to
treatment although the predictive value does not appear toimprove on the NIEC index and presence of red whale marking54
Risk and mortality of first variceal bleedData describing the overall risk of bleeding from varices must beviewed with caution and have some pitfalls in interpretationThe natural history of patients who have varices that are diag-nosed as part of their baseline investiations is different fromthat of patients who have complications of liver disease such asascites and encephalopathy Most studies do not comment oneither the severity of liver disease or whether patients with alco-holic cirrhosis are continuing to drink Both these factors have asignificant effect on the risk of variceal haemorrhage
Most studies report bleeding from varices in about 20ndash50of patients with cirrhosis during the period of follow-up Bakeret al23 reported variceal bleeding in 33 of 115 patients that theyfollowed up for a mean of 33 years with a mortality of 48from the first variceal haemorrhage These data were confirmedby Christensen et al18 About 70 of the episodes of bleedingoccur within 2 years of diagnosis Recent studies demonstrate adramatic reduction in mortality following variceal bleeding of20 6-week mortality55 and 15 in-hospital mortality5 withcontributions from improved endoscopic pharmacological andradiological therapies notably TIPSS Intensive care treatmenthas also improved with outcomes being particularly good forthose requiring minimal organ support
Analysis of the non-active treatment arms in the primaryprophylaxis trials comparing propranolol with placebo showresults similar to those of the primary prophylaxis shunt trialswith most episodes of bleeding occurring within the first 2 yearsof follow-up In these studies the rate of first variceal haemor-rhage ranged from 22 to 6156ndash60 This large difference inthe rate of first bleed relates almost certainly to the number ofpatients with severe liver disease included in the study (PascalChild Cmdash46 bleedingmdash61 Italian Multicenter Project forPropranolol in Prevention of Bleeding (IMPP) Child Cmdash6bleedingmdash32 Conn Child Cmdash6 bleedingmdash22)Mortality varied from 24 to 49 over 2 years (Pascal mortal-itymdash49 IMPP mortalitymdash24 Conn mortalitymdash24)
Primary prophylaxisSince 30ndash50 of patients with portal hypertension will bleedfrom varices and about 20 will die from the effects of the first
Table 2 Scoring systems for quantifying the severity of cirrhosisSeverity of liver disease can be described using the ChildndashPughscore or MELD scoreThe ChildndashPugh score is the sum of severity scores for Child classvariceal size and red wale markings the variables shown below
Category 1 2 3
Encephalopathy 0 III IIIIVAscites Absent Mild-moderate SevereBilirubin (μmolL) lt34 34ndash51 gt51Albumin (gL) gt35 28ndash35 lt28INR lt13 13ndash15 gt15
ChildndashPugh class A represents a score of le6 class B a score of 7ndash9 and class C ge10The MELD score is a formula that includes three laboratory-based variables reflectingthe severity of liver disease It was originally used to predict the short-term mortalityafter placement of a transjugular intrahepatic portosystemic stent-shunt for varicealbleeding Subsequently it has been used in selecting candidates for livertransplantationMELD score please use the online calculator httpswwwesotorgElitameldCalculatoraspxINR international normalised ratio
8 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleed it seems rational to develop prophylactic regimens toprevent the development of and bleeding from these varicesHowever most of the published trials do not have sufficientpower to identify favourable treatment effects Based on theexpected bleeding and death rates in the control group theminimum number of patients needed to detect a 50 reductionin bleeding would be 270 and 850 patients in each arm todetect the same reduction in mortality A proposed algorithmfor surveillance and prophylaxis of varices is shown in figure 2At this time there is insufficient evidence to support treatingpatients without varices or lsquopre-primary prophylaxisrsquo A largerandomised placebo-controlled trial of timolol in patientswithout varices and portal hypertension defined as HVPGgt6 mm Hg did not show any effect on the development ofvarices or variceal bleeding27 The role of drug treatment in pre-venting bleeding in patients with small varices is unclear Threerandomised placebo-controlled trials have studied this Caleset al61 showed that propranolol in patients with small or novarices resulted in greater development of varices Howeverpatients without varices were included and there was significantloss of patients to follow-up The second trial showed thatnadolol reduced variceal bleeding without survival benefit andincreased adverse events62 Sarin et al63 did not show any effectwith propranolol despite a significant effect on portal pressure
SurgeryPortacaval shuntsFour trials of portacaval shunts have been published which ran-domised a total of 302 patients64ndash67 either to prophylactic shuntsurgery or to non-active treatment A meta-analysis of thesestudies showed a significant benefit in the reduction of varicealbleeding (OR=031 95 CI 017 to 056) but also a signifi-cantly greater risk of hepatic encephalopathy (OR=2 95 CI12 to 31) and mortality (OR=16 95 CI 102 to 257) inpatients treated with shunt surgery68 At this time there is noevidence for the use of TIPSS for primary prophylaxis1
Devascularisation proceduresInokuchi50 showed that there was a significant reduction in vari-ceal bleeding and in mortality in patients treated with a varietyof devascularisation procedures There are however numerousproblems with the interpretation of this study because of theuse of different procedures in each of the 22 centres Theseresults require confirmation
Pharmacological treatmentNon-cardioselective β blockersThe mainstay of the pharmacological approach to the primaryprophylaxis of variceal haemorrhage has been NSBBPropranolol which has been shown to reduce the PPG reduceazygos blood flow and also variceal pressure It achieves this bycausing splanchnic vasoconstriction and reducing cardiacoutput There is no clear dose-related reduction in HVPG orcorrelation of HPVG reduction with reduction in heart rate69
Observational studies have shown that a 10ndash12 reduction inHVPG after acute administration of propranolol was associatedwith reduced bleeding and hepatic decompensation54 70
However HVPG monitoring is not routinely available in mostcentres outside of larger institutions A meta-analysis of nineplacebo-controlled randomised trials (964 patients) showed thatthe pooled risk difference for bleeding was minus11 (95 CIminus21 to minus1) and for death was minus9 (95 CI minus18 tominus1) in favour of propranolol71
Nadolol exerts similar effects on portal haemodynamicsalthough the effect on blood pressure may not be as pro-nounced Two placebo-controlled trials58 59 have shownreduced bleeding although in one study this was only seen onper protocol analysis59 There was no effect on overall survival
Carvedilol is a NSBB like propranolol and a vasodilator dueto α1 receptor blockade The latter reduces portocollateralresistance and by actions on hepatic stellate cells leads to areduction in intrahepatic resistance Haemodynamic studiesdemonstrate a greater reduction in portal pressure with
Figure 2 Algorithm for surveillance of varices and primary prophylaxis in cirrhosisndash If there is clear evidence of disease progression this interval can be modified by clinician Endoscopy should also be offered at time ofdecompensation
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 9
Guidelines
carvedilol than with propranolol although blood pressure isreduced72 73 The optimum dose is 625ndash125 mgday74 Higherdoses are not more effective and are associated with moreadverse eventsmdashin particular hypotension Carvedilol at a doseof 125 mgday at current UK prices is considerably cheaperthan propranolol 40 mg twice a day and nadolol 80 mgday(monthly cost pound120 pound562 and pound5 respectively) Two RCTs ofcarvedilol versus variceal band ligation (VBL) in primaryprophylaxis have been published75 76 The first study75 showedsignificantly reduced bleeding in the carvedilol arm (10 vs23 relative hazard 041 95 CI 019 to 096) with no effecton survival The second trial by Shah et al76 did not show anydifferences in bleeding or mortality Compliance with VBL wasbetter in the latter trial and unlike the first trial there were sig-nificantly more patients with viral hepatitis than alcoholic cir-rhosis A further study74 assessed the effect of carvedilol inpatients who were haemodynamic non-responders to propran-olol where haemodynamic response was defined as HVPGreduction to le12 mm Hg or by gt20 of baseline after 4 weeksof treatment Patients who were haemodynamic non-respondersor intolerant to carvedilol were treated with VBL Carvedilolresulted in significantly lower variceal bleeding compared withVBL and haemodynamic responders to carvedilol or propran-olol had significantly lower mortality than those treated withVBL It is worth noting that the study was not randomised
There have been recent suggestions based on low-level evi-dence that NSBB may result in a poorer outcome in patientswith cirrhosis and refractory ascites77 The lsquowindow hypothesisrsquofor β blockers in cirrhosis has also recently been described sug-gesting that NSBB are helpful in the compensated and earlydecompensated cirrhotic period but may not be helpful in veryearly cirrhosis such as in a patient with no varices and may beharmful in patients with end-stage cirrhosis with refractoryascites78 However recent large observational studies questionthe last hypothesis with improved survival seen in patients withrefractory ascites treated with NSBB79 unless patients have anepisode of spontaneous bacterial peritonitis80 Therefore untilthere are further prospective controlled studies NSBB should becontinued in patients with refractory ascites The clinician mustcarefully monitor haemodynamic parameters such as blood pres-sure and discontinue NSBB in patients with hypotension andrenal impairment as can occur after an episode of spontaneousbacterial peritonitis Other potentially severe adverse eventswith NSBB include symptomatic bradycardia asthma andcardiac failure Less severe side effects such as fatigue insomniaand sexual dysfunction may also result
Isosorbide mononitrateInterest in the use of vasodilators such as isosorbide mononitrate(ISMN) developed after the demonstration that it reduces portalpressure as effectively as propranolol81 but has subsequentlywaned A trial comparing ISMN with propranolol showed nosignificant difference between these agents82 Another rando-mised trial of ISMN versus placebo did show any difference inthe two arms83 Therefore ISMN is not recommended asmonotherapy in primary prophylaxis
β Blocker and ISMNThe combination of nadolol and ISMN has been compared withnadolol in a RCT The combination therapy reduced the fre-quency of bleeding significantly but no significant differenceswere detected in mortality84 However Garcia-Pagan et al85 in adouble-blind RCTof propranolol plus ISMN versus propranolol
plus placebo failed to show any differences between the twoarms Combination therapy is associated with more side effects
Proton pump inhibitorsA placebo-controlled randomised trial reported reduced bleed-ing and mortality with rabeprazole after eradication of varices86
However the study had a heterogeneous population with VBLperformed for both primary and secondary prophylaxis andsmall numbers (n=43) limiting the validity of the conclusionsFurthermore there was no arm comparing proton pump inhibi-tors with NSBB The use of proton pump inhibitors in patientswith cirrhosis and ascites was associated with increased risk ofspontaneous bacterial peritonitis in a large retrospective study87
This was not confirmed in a larger prospective non-randomisedstudy88 However a recent prospective observational study hasshown proton pump use to be associated with increased mortal-ity in cirrhosis89 Proton pump inhibitors are also associatedwith increased risk of Clostridium difficile infection90 Thereremains continuing concern about proton pump inhibitors inpatients with cirrhosis therefore caution should be used
Endoscopic therapyVariceal band ligationVBL has been compared with NSBB in 19 trials in a recentCochrane meta-analysis of 1504 patients91 Despite reducedbleeding (RR=067 95 CI 046 to 098) with VBL there wasno difference in overall mortality and bleeding-related mortalityThe difference in bleeding was not seen when only trials withlow selection or attrition bias were included Banding can haveserious complications The risk of fatal banding-induced bleed-ing was highlighted in a meta-analysis showing reduced fataladverse events with NSBB (OR=014 95 002 to 099)92
The optimal timing of banding intervals is discussed in thesection lsquoSecondary prophylaxis of variceal haemorrhagersquo A ran-domised trial of 96 patients who underwent endoscopic surveil-lance at 6 or 3 months after eradication of varices with VBL didnot demonstrate a difference in bleeding on mortality93
However the trial had a heterogeneous study group of patientswho underwent VBL both for primary (65) and secondaryprevention (35)
SclerotherapyNineteen trials have compared endoscopic variceal sclerotherapywith no treatment68 Owing to the marked heterogeneitybetween these studies a meta-analysis is clinically inappropri-ate68 Sclerotherapy does not offer any benefit in combinationwith NSBB or VBL compared with VBL or NSBB alone andincreases iatrogenic complications such as strictures94ndash96 At thistime sclerotherapy cannot be recommended for prophylaxis ofvariceal haemorrhage in patients with cirrhosis
Recommendations primary prophylaxis of variceal haemor-rhage in cirrhosis (figure 2)1 What is the best method for primary prophylaxis
11 We recommend NSBB or variceal band ligation (VBL)We suggest pharmacological treatment with propranololas first line VBL is offered if there are contraindicationsto NSBB The choice of VBL or NSBB should also takeinto account patient choice (level 1a grade A)
12 We suggest carvedilol or nadolol as alternatives to pro-pranolol (level 1b grade A)
13 Dose131 Propranolol 40 mg twice daily Dose titrated to
maximum tolerated or once heart rate (HR) of
10 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
50ndash55 bpm is reached to a maximum dose of320 mg (level 1a grade A)
132 Nadolol 40 mg daily dose Dose titrated tomaximum tolerated or once HR of 50ndash55 bpm isreached a maximum dose of 240 mg (level 1agrade A)
133 Carvedilol 625 mg once daily to increase tomaintenance of 125 mg after a week if toleratedor once HR of lt50ndash55 bpm is reached (level 1agrade A)
134 It is suggested that NSBB are discontinued at thetime of spontaneous bacterial peritonitis renalimpairment and hypotension (level 2b grade B)
14 In cases of contraindications or intolerance to NSBB werecommend variceal band ligation (level 1a grade A)
2 Who should have surveillance for variceal bleeding21 We recommend all patients with cirrhosis should be
endoscoped at the time of diagnosis (level 1a grade A)There is no indication to repeat endoscopy in patientsreceiving NSBB
3 How often should cirrhotic patients be endoscoped31 If at the time of first endoscopy no varices are seen we
suggest that patients with cirrhosis should be endos-coped at 2ndash3-year intervals (level 2a grade B)
32 If grade I varices are diagnosed we suggest that patientsshould be endoscoped at yearly intervals (level 2agrade B)
33 If there is clear evidence of disease progression wesuggest that the intervals can be modified by a clinicianEndoscopy should also be offered at time of decompen-sation (level 2a grade B)
4 Which patients with cirrhosis should have primaryprophylaxis41 If grade I varices and red signs or grade 2ndash3 varices are
diagnosed we recommend that patients have primaryprophylaxis irrespective of the severity of the liverdisease (level 1a grade A)
5 Treatments not recommended51 Proton pump inhibitors are not recommended unless
otherwise required for peptic ulcer disease (level 1bgrade B)
52 Isosorbide mononitrate monotherapy is not recommendedas primary prophylaxis (level 1b grade A) There is insuffi-cient evidence to recommend isosorbide mononitrate incombination with NSBB (level 1b grade A)
53 Shunt surgery or TIPSS is not recommended as primaryprophylaxis (level 1a grade A)
54 Sclerotherapy is not recommended as primary prophy-laxis (level 1a grade A)
6 Areas requiring further study61 Role of NSBB in patients without varices with focus on
carvedilol62 Role of NSBB in patients with small varices with focus
on carvedilol63 Comparison of carvedilol versus propranolol in primary
prophylaxis64 Identification of and trials assessing new drugs for
primary prophylaxis such as statins7 Quality indicator
71 Percentage of patients at diagnosis of cirrhosis who havehad an endoscopy to screen for varices (level 1agrade A)Numerator patients diagnosed with cirrhosis who havehad an endoscopy either before or after diagnosis within
6 monthsDenominator patients newly diagnosed with cirrhosis
72 Percentage of patients receiving primary prophylaxisamong those newly diagnosed with grade I varices andred signs or grade 2ndash3 varicesNumerator patients who have grade 1 varices with redsigns or grade 2ndash3 varices receiving primary prophy-laxisDenominator patients diagnosed with cirrhosis whohave grade I varices with red signs or grade 2ndash3 varices
MANAGEMENT OF ACTIVE VARICEAL HAEMORRHAGEThe average 6-week mortality of the first episode of varicealbleeding in most studies is reported to be up to 20 There hasbeen considerable improvement in survival since the early 1980swhen the in-hospital mortality was 40ndash5097 compared with15 from a recent UK audit5 Such is the improvement in out-comes that a patient with Childrsquos A cirrhosis is very unlikely tosuccumb to an index variceal bleed Studies have shown theChildndashPugh score MELD score and HVPG to be strong predic-tors of outcomes98ndash103 The MELD score has been shown tooutperform Childrsquos score in a recent study with a score gt19associated with 20 6 week mortality103 Furthermore theMELD score has been shown to perform as well as the trad-itional intensive care unit scores in predicting mortality inpatients admitted to intensive care in the UK104 MELD gt18active bleeding transfusing gt4 units of packed red blood cellshave been shown to be predictors of mortality and earlyrebleeding99 101 102 HVPG has also been shown to predictoutcome when measured at 2 weeks after a bleed44 and a valueof ge20 mm Hg when measured acutely within 48 h has beenshown to provide significant prognostic information100
However this technique is not used routinely in the manage-ment of patients around the world and substitution of clinicaldata in the latter study was shown to provide the same clinicalpredictive value100 These scoring systems are not purely aca-demic they allow the referring clinician to predict thosepatients with a high chance of rebleeding to be transferred to aspecialist centre offering for instance TIPSS before the patientrebleeds
Nonetheless probably the most important step in the man-agement of acute variceal haemorrhage is the initial resuscitationassessed according to standard lsquoABCrsquo practice together withprotection of the airway to prevent aspiration Although earlyendoscopy allows for accurate diagnosis of the bleeding site anddecisions about management (figure 3) therapeutic interventionin acute variceal bleeding can be initiated safely in most casesbefore diagnostic endoscopy As similar efficacy is demonstratedwith pharmacological treatment as with sclerotherapy theformer should be first-line therapy99 β Blockade should not bestarted in the acute setting and those already taking β blockersas prophylaxis should probably stop taking them for 48ndash72 h inorder that the patientrsquos physiological response to blood loss canbe allowed to manifest
General considerationsPatient evaluationThe majority of patients with a variceal bleed will be sufficientlystable to enable a full history and examination to take placeHistory of alcohol excess and or intravenous drug use should besought and may become particularly relevant if the patient haswithdrawal symptoms after admission Comorbidity is importantwhen estimating risk and deciding on use of vasopressors The
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 11
Guidelines
following risk factors doubled mortality after an acute varicealbleed in one US study older age comorbidities male gender andnot undergoing a gastroscopy within 24 h105
A full examination is helpful for the important negatives asmuch as the positives Baseline observations should include thetemperature as infection is a serious complication with signifi-cant mortality Confusion may be present because of encephal-opathy intoxication with alcohol or drugs or withdrawal fromalcohol or drugs The patient should be on continuous BP andpulse monitor and their haemodynamic status recordedAn oxygen saturation monitor is helpful Stigmata of chronicliver disease and concurrent jaundice provide insight into thecurrent status of a patientrsquos liver and also give warning ofpotential further decompensation if significant bleeding persists(see scoring systems above) Pneumonia must be actively
excluded Evidence of ascites requires a diagnostic tap to searchfor infection
Investigations including full blood count coagulationprofile liver and renal function and blood group and save andcross-match Blood and urine should also be cultured An ultra-sound scan later in the admission is helpful to identify subclin-ical ascites flow in portal vein and any obvious emergence of anhepatocellular carcinoma (HCC)
Location of patientA decision must be made as to where the patient is best managedVariceal bleeding is unpredictable generally occurs in patientswith significant liver disease and is associated with significant mor-tality Hence a high-dependency unit is usually the most appropri-ate initial location although a properly staffed lsquogastrointestinal
Figure 3 Algorithm for themanagement of acute varicealbleeding TIPSS transjugularintrahepatic portosystemic stent shunt
12 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleeding bedrsquo may be appropriate If a patient is vomiting bloodor there is a perceived risk of a haemodynamically unstable patienthaving blood in the stomach then the patient must be intubatedbefore endoscopy and return to an intensive care or high-dependency unit will be necessary until extubation
Volume resuscitation and blood productsIntravenous access (two 16ndash18G cannulae) should have beensecured on admission with a reported GI bleed Further intra-venous access may be necessary In patients with poor venousaccess advanced liver disease or renal failure associated withtheir liver disease central venous access may be helpful withguiding fluid infusions However the drawbacks include the riskof the procedure and a potential source of infection Thereforethere is no absolute requirement for a central line and no evi-dence of unequivocal benefit Intravenous fluid resuscitationshould be initiated with plasma expanders aiming to maintain asystolic blood pressure of 100 mm Hg Care with monitoring isparamount in this group of patients
Overtransfusion has been shown to have a deleterious effecton outcome In a recent single-centre RCT a restrictive transfu-sion policy of maintaining haemoglobin between 70 and 80 gLimproved the control of variceal bleeding (11 vs 22p=005) and lowered HVPG compared with a liberal transfu-sion policy without effect on 45-day survival106 However itshould be noted that these results were from a single Spanishcentre which was a tertiary unit for variceal bleeding where allpatients underwent endoscopy within 6 h Nonetheless arestrictive transfusion policy has been recommended for sometime1 and there is now good evidence to support not transfusinga stable patient with a haemoglobin of ge80 gL However under-resuscitation should also be avoided and while goal-orientedfluid replacement has generally not been useful in an intensivetherapy unit setting a venous saturation gt70 remains an easilymeasurable target with some evidence to support it107
Interpretation and management of clotting profile is challen-ging in liver disease where there is usually a balanced deficiencyof both procoagulant and anticoagulant factors108 The NICEguidelines recommend activation of a hospitalrsquos massive transfu-sion policy when there is major haemorrhage and plateletsupport when the value is lt50 and clotting factor supportwhen the international normalised ratio (INR) is gt15 timesnormal2 There is no evidence for the use of lsquoprophylacticrsquo clot-ting or platelet support to reduce the risk of rebleeding Thereis insufficient evidence to support the routine use of transexamicacid or recombinant factor VIIa109
Pharmacological treatmentThe two major classes of drugs that have been used in thecontrol of acute variceal bleeding are vasopressin or its analo-gues (either alone or in combination with nitroglycerine) andsomatostatin or its analogues Terlipressin is the only agent thathas been shown to reduce mortality in placebo-controlled trialsHowever in trials comparing terlipressin somatostatin andoctreotide no difference in efficacy was identified in a system-atic review110 and in a recent large RCT111 Prophylactic anti-biotics can result in a similar survival benefit following acutevariceal bleeding
VasopressinVasopressin reduces portal blood flow portal systemic collateralblood flow and variceal pressure It does however have signifi-cant systemic side effects such as an increase in peripheral resist-ance and reduction in cardiac output heart rate and coronary
blood flow In comparison with no active treatment the pooledresults of four randomised trials showed that it reduced failureto control variceal bleeding (OR=022 95 CI 012 to 043)although survival was unaffected68 Meta-analysis of five trialscomparing sclerotherapy with vasopressin has shown a signifi-cant effect on reduction in failure to control bleeding(OR=051 95 CI 027 to 097) with no effect on survival68
Vasopressin with nitroglycerineThe addition of nitroglycerine enhances the effect of vasopres-sin on portal pressure and reduces cardiovascular side effects112
Meta-analysis of three randomised trials comparing vasopressinalone with vasopressin and nitroglycerine showed that the com-bination was associated with a significant reduction in failure tocontrol bleeding (OR=039 95 CI 022 to 072) although nosurvival benefit was shown68
TerlipressinTerlipressin is a synthetic analogue of vasopressin which has animmediate systemic vasoconstrictor action followed by portalhaemodynamic effects due to slow conversion to vasopressin Ina Cochrane meta-analysis of seven placebo-controlled trials ter-lipressin was shown to reduce failure to control bleeding(RR=066 95 CI 055 to 093) and also to improve survival(RR=066 95 CI 049 to 088)113 In the same meta-analysisthere was no difference between terlipressin versus vasopressinballoon tamponade or endoscopic therapy in failure to controlbleeding or survival113 The role of terlipressin in combinationwith VBL is explored in the section lsquoEndoscopic therapy incombination with pharmacological therapyrsquo
The recommended dose of terlipressin is 2 mg IV every 4 halthough many units reduce the dose to 6 hourly as it may causeperipheral vasoconstriction which manifests as painful handsand feet While 5 days of IV treatment has been advocated inthe Baveno V guidelines1 this prolonged treatment has notbeen shown to have a survival benefit and for pragmaticreasons many units will stop treatment shortly after satisfactoryhaemostasis In a randomised trial terlipressin given for 24 hafter satisfactory haemostasis with VBL after oesophageal vari-ceal bleeding was as effective as 72 h of treatment114
In patients intolerant of terlipressin or in countries where ter-lipressin is not available alternatives should be considered
Somatostatin and octreotideSomatostatin causes selective splanchnic vasoconstriction andreduces portal pressure and portal blood flow115 Octreotide is asomatostatin analogue The mechanism of action of these twoagents is not clear Inhibition of glucagon increases vasodilatationrather than a direct vasoconstrictive effect and post-prandial guthyperaemia is also reduced The actions of octreotide on hepaticand systemic hemodynamics are transient making continuousinfusion necessary Octreotide is given as a 50 μg bolus followedby an infusion of 25ndash50 μgh Somatostatin is given as a 250 mgintravenous bolus followed by an infusion of 250 mghSomatostatin and octreotide have been shown to be aseffective as terlipressin in acute variceal bleeding in ameta-analysis110 Seo et al111 in a large RCTof 780 patients com-paring these three agents failed to show a difference in treatmentsuccess (range 838ndash862) rebleeding (range 34ndash44) andmortality (range 8ndash88) A low systolic blood pressure at pres-entation high serum creatinine level active bleeding in the emer-gency endoscopy gastric variceal bleeding and ChildndashPugh gradeC were independent factors predicting 5-day treatmentfailure111
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 13
Guidelines
AntibioticsAntibiotics that provide Gram-negative cover are one of the inter-ventions which positively influence survival in variceal haemor-rhage as shown in a Cochrane meta-analysis of 12placebo-controlled trials (RR=079 95 CI 063 to 098)116
Antibiotics were also shown to reduce bacterial infections(RR=043 95 CI 019 to 097) and early rebleeding (RR=05395 CI 038 to 074)116 Therefore short-term antibiotics shouldbe considered standard practice in all cirrhotic patients who have avariceal bleed irrespective of the presence of confirmed infectionThird-generation cephalosporins such as ceftriaxone (1 g IVdaily) have been shown to be more effective at reducingGram-negative sepsis than oral norfloxacin117 but choice of anti-biotics must be dictated by local resistance patterns and availability
Proton pump inhibitorsOne RCT compared a short course of proton pump inhibitorswith vasoconstrictor therapies after haemostasis in acute varicealbleeding118 Despite larger ulcers noted in the vasoconstrictorarm there were no differences in bleeding or survival Nearly50 of patients had ascites which might have implications inlight of the reports of increased incidence of spontaneous bac-terial peritonitis as mentioned earlier
Endoscopic therapyEndoscopy should take place within 24 h of admission andearlier if there is excessive bleeding based on low-level evi-dence105 While many guidelines and reviews suggest thatendoscopy should be carried out within 12 h the only study thatexamined the influence of timing on outcome failed to demon-strate any advantage of endoscopy before 12 h119 The optimaltime is after sufficient resuscitation and pharmacological treat-ment with the endoscopy performed by a skilled endoscopyteam in a suitably equipped theatre environment and withairway protection Airway protection is essential where risk ofaspiration is high and affords the endoscopist time for thoroughevaluation including complete clot aspiration and controlledapplication of treatment including tamponade if required Theendoscopy team must comprise an experienced endoscopynurse acquainted with the equipment necessary for endoscopytherapy of varices and a skilled endoscopist competent in usingbanding devices and deployment of balloon tamponade
Variceal band ligationThis technique is a modification of that used for the elastic bandligation of internal haemorrhoids Its use in humans was firstdescribed in 1988120 A meta-analysis of seven trials comparingVBL with sclerotherapy in acute bleeding showed that VBLreduced rebleeding from varices (OR=047 95 CI 029 to078) reduced mortality (OR=067 95 CI 046 to 098) andresulted in fewer oesophageal strictures (OR=010 95 CI003 to 029)121 The number of sessions required to obliteratevarices was lower with VBL (22 fewer sessions (95 CI 09to 35))
SclerotherapySclerotherapy has been replaced by VBL and should no longerbe offered as standard of care in acute variceal haemorrhage
Other endoscopic measuresIn an RCT cyanoacrylate offered no benefit over VBL with theadditional risk of embolisation and trend towards increasedrebleeding with cyanoacrylate122
Haemostatic powder (TC-325 Hemospray Cook MedicalUSA) has been described in a small study of nine patients whoreceived endoscopic spray treatment for acute variceal bleedingThe study reported no rebleeding within 24 h and no mortalityat 15 days123
Endoscopic therapy in combination with pharmacological therapyThe role of combining vasoactive drugs with endoscopictherapy (VBL or sclerotherapy) was reported in a meta-analysisof eight trials124 Combination therapy resulted in better initialcontrol of bleeding (RR=112 95 CI 102 to 123) and5-day haemostasis (RR=128 95 CI 118 to 139) withoutany difference in survival Adverse events were similar in bothgroups Two RCTs have compared VBL with sclerotherapy incombination with vasoactive agents in acute variceal bleed-ing125 126 Lo et al125 used vasopressin and found that VBLresulted in better 72 h haemostasis (97 vs 76 p=0009)with fewer complications (5 vs 29 p=0007) Villanuevaet al used somatostatin and reported lower failure to controlacute bleeding with VBL (4 vs 15 p=002) with fewerserious complications (4 vs 13 p=004) Overall survivalwas similar in both trials125 126
Balloon tamponadeBalloon tamponade is highly effective and controls acute bleed-ing in up to 90 of patients although about 50 rebleed whenthe balloon is deflated127 128 It is however associated withserious complications such as oesophageal ulceration and aspir-ation pneumonia in up to 15ndash20 of patients Despite this itmay be a life-saving treatment in cases of massive uncontrolledvariceal haemorrhage pending other forms of treatment Anappropriately placed SengstakenndashBlakemore tube allows forresuscitation safe transportation and either repeat endoscopy orradiological shunting in a patient with a stable cardiovascularsystem The oesophageal balloon is rarely required must neverbe used on its own and should be used only if there is continu-ing bleeding despite an adequately inflated gastric balloon cor-rectly placed and with appropriate tension Placement of thetube endoscopically or over a guide wire might reduce the riskof complications especially oesophageal rupture
Removable oesophageal stentsThe SX-Ella Danis stent (ELLA-CS Hradec Kralove CzechRepublic) is a removable covered metal mesh stent placed endo-scopically in the lower oesophagus without radiological screen-ing It has no role in the management of gastric varicealbleeding These stents can be left in situ for up to 2 weeksunlike the SengstakenndashBlakemore tube which should beremoved after a maximum of 24ndash48 h129 130 No published con-trolled trials have compared this modality with balloontamponade
Transjugular intrahepatic portosystemic stent-shuntSeveral uncontrolled studies have examined the role of salvagebare TIPSS in acute variceal bleeding In a review of 15 studiescontrol of bleeding was achieved in 90ndash100 with rebleedingin 6ndash16131 Mortality varied between 75 (in hospital) and15 (30 day) It is important to appreciate that sclerotherapywas used as first-line endoscopic therapy in most of thesestudies Long-term follow-up of a study that compared TIPSSwith H-graft portacaval shunts in patients for whom non-operative management had failed suggested that H-grafts were auseful method of reducing portal pressure and had a signifi-cantly lower failure rate (p=004) but had no significant
14 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
improvement in overall survival despite a benefit seen in ChildrsquosA and B disease132 A recent RCT compared emergency porto-caval surgery with bare TIPSS within 24 h of presenting withacute oesophageal variceal bleeding in unselected cirrhoticpatients Emergency portocaval surgery resulted in better out-comes for long-term bleeding control encephalopathy and sur-vival (plt0001)133 Before wider application of surgery foracute variceal bleeding more data are needed in light of therecent adoption of covered stents
There has also been a generalised established change in prac-tice in using covered TIPSS stents (polytetrafluoroethylene(PTFE)) rather than a bare metal stent with evidence to supportthis change In randomised controlled studies these stents wereshown to have higher primary patency rates than bare stentswithout significant differences in survival and the potential forreduced incidence of hepatic encephalopathy134 135
There is however growing evidence from two RCTs for theearlier use of TIPSS in selected patients stratified by HVPGChildndashPugh class and active bleeding and not just use as asalvage option6 136 Monescillo et al136 randomised patientspresenting with acute oesophageal variceal haemorrhage to bareTIPSS or standard of care if the HVPG was ge20 mm Hg within24 h of admission Significantly reduced treatment failure asdefined by failure to control acute bleeding andor early rebleed-ing (12 vs 50) was seen and improved survival (62 vs35) in the patients randomised to undergo a TIPSS procedureHowever the standard of care was sclerotherapy and not com-bination endoscopic and pharmacological treatment This limita-tion and the lack of availability of HVPG measurement in mostcentres meant this trial did not have a significant impact on clin-ical practice
Garcia-Pagan et al6 selected patients with active bleeding andChildrsquos B cirrhosis or patients with Childrsquos C cirrhosis (Childrsquosscore lt14) for randomisation to early PTFE-covered TIPSSwithin 72 h or standard of care with VBL and pharmacologicaltreatment This has shown encouraging results with reduced riskof treatment failure (3 vs 50) improved survival (86 vs61 at 1 year) yet without increased risk of hepatic encephal-opathy The results were supported by an observational studyfrom the same group although a survival benefit was notseen137 Furthermore a recent well-conducted observationalstudy did not demonstrate such high survival rates with earlyTIPSS with 11-year survival of 67 which was similar to thatof patients given endoscopic and pharmacological treatmentsonly138 Therefore larger multicentred RCTs need to be under-taken to further evaluate the role of early TIPSS It is importantto make the distinction between salvage TIPSS and early TIPSSto prevent rebleeding
Liver transplantationThis is probably appropriate only for patients who bleed whileawaiting liver transplantation although studies comparing VBLor TIPSS placement with urgent liver transplantation in thissituation need to be done Liver transplantation is an exceed-ingly rare option for the vast majority of patients both becauseit is not commonly available and because of shortages anddelays in organ procurement No controlled trials of liver trans-plantation in uncontrolledactive bleeding are available
Recommendations for the control of variceal bleeding in cir-rhosis are given below and in figure 3
Recommendations control of active variceal haemorrhage incirrhosis (figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with bloodplatelets and clotting factors in line with local protocolsfor managing massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusionpolicy aiming for a haemoglobin of 70ndash80 gL is sug-gested in haemodynamically stable patients (level 1bgrade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable(level 5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L(level 5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to localcircumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with suspected
or confirmed variceal bleeding (level 1a grade A)32 In all patients vasoconstrictors such as terlipressin or
somatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 15
Guidelines
41 If bleeding is difficult to control a SengstakenndashBlakemore tube should be inserted until further endo-scopic treatment TIPSS or surgery is performed depend-ing on local resources and expertise (level 1b grade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure (level1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
SECONDARY PROPHYLAXIS OF VARICEAL HAEMORRHAGEβ BlockersA meta-analysis of 12 trials comparing propranolol or nadolol139
with no active treatment showed a significant reduction inrebleeding but no significant reduction in mortality140 Thegreater reduction in portal pressure with carvedilol comparedwith propranolol has been described in the section lsquoPrimaryprophylaxisrsquo of this guideline
NitratesThe addition of ISMN to NSBB has been shown to reduce vari-ceal rebleeding compared with NSBB alone although no sur-vival benefit was seen141 In addition adverse events leading todrug withdrawal were more common in the group receivingcombined drug treatment A meta-analysis of ISMN alone orwith either NSBB or endoscopic therapy reported that there wasno mortality benefit from combining nitrates and NSBB com-pared with NSBB alone142
Side effects of ISMN include dizziness and headache Owingto the side effects and relative lack of data ISMN is not com-monly used in clinical practice
A recent RCT of 121 patients reported carvedilol to besimilar to combined ISMN and NSBB therapy in the preventionof variceal rebleeding and mortality although severe adverseevents were less common with carvedilol143
SimvastatinA recent abstract of a multicentre RCT of 158 patients reporteda survival benefit (91 vs 78 p=003) from adding simvasta-tin to VBL and NSBB compared with placebo VBL and NSBBas treatment for the prevention of variceal rebleeding144 Therewas no difference in rebleeding and the survival benefit wasrestricted to Child A and B patients Serious adverse events weresimilar in both groups More data are required to investigatethis interesting observation of a survival benefit from simvastatinin this situation which may relate to its effects on hepatocellularfunction fibrosis and portal pressure
Proton pump inhibitorsA double-blind randomised placebo-controlled trial showed thatpantoprazole reduced the size of ulcers in patients who under-went VBL However the total number of ulcers and other out-comes were similar in the two groups145
Endoscopic therapyVBL has been accepted as the preferred endoscopic treatmentfor the prevention of variceal rebleeding with a lower rate ofrebleeding mortality and complications than sclerother-apy146 147 The time interval between VBL sessions to achieveeradication of varices is debateable However a recent RCTcomparing monthly with biweekly VBL after initial haemostasiswith VBL in 70 patients suggested that there were fewerpost-VBL ulcers in the monthly group (11 vs 57plt0001)148 Variceal recurrence rebleeding and mortality weresimilar in both groups
Two meta-analyses showed there is no evidence that the add-ition of sclerotherapy to VBL improves clinically relevant out-comes including variceal rebleeding and death and thecombination led to higher stricture rates149 150
Endoscopic therapy versus drug therapyVBL has been reported to be more effective than combinedNSBB and ISMN drug therapy151 However an 8-yearfollow-up study of this RCT found that although VBL wassuperior in reducing variceal rebleeding survival rates were sig-nificantly higher in the group treated with combined drug treat-ment152 Other studies have found no superiority of VBL overcombined drug therapy for prevention of variceal rebleeding ormortality153 154 A recent small multicentre RCT reported carve-dilol to be similar to VBL in the prevention of variceal rebleed-ing with a trend in favour of survival with carvedilol (73 vs48 p=0110)155
Several meta-analyses have compared drug therapy with VBLin the prevention of variceal rebleeding One meta-analysis ofsix RCTs showed no significant difference in variceal rebleedingrates when comparing VBL alone with combined NSBB andISMN therapy However all-cause mortality was significantlyhigher in patients treated with the VBL (RR=125 95 CI101 to 155)156 Three meta-analyses comparing drug therapy(NSBB alone or with ISMN) with endoscopic therapy alonereported no difference in variceal rebleeding or mortality157ndash159
Endoscopic+drug therapy versus either aloneNumerous studies and several meta-analyses have comparedcombined endoscopic and drug therapy with monotherapy(endoscopic or drugs alone) in the prevention of varicealrebleeding A meta-analysis of 23 trials assessing sclerotherapyor VBL combined with NSBB reported that combinationtherapy reduced rebleeding more than either endoscopic
16 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines
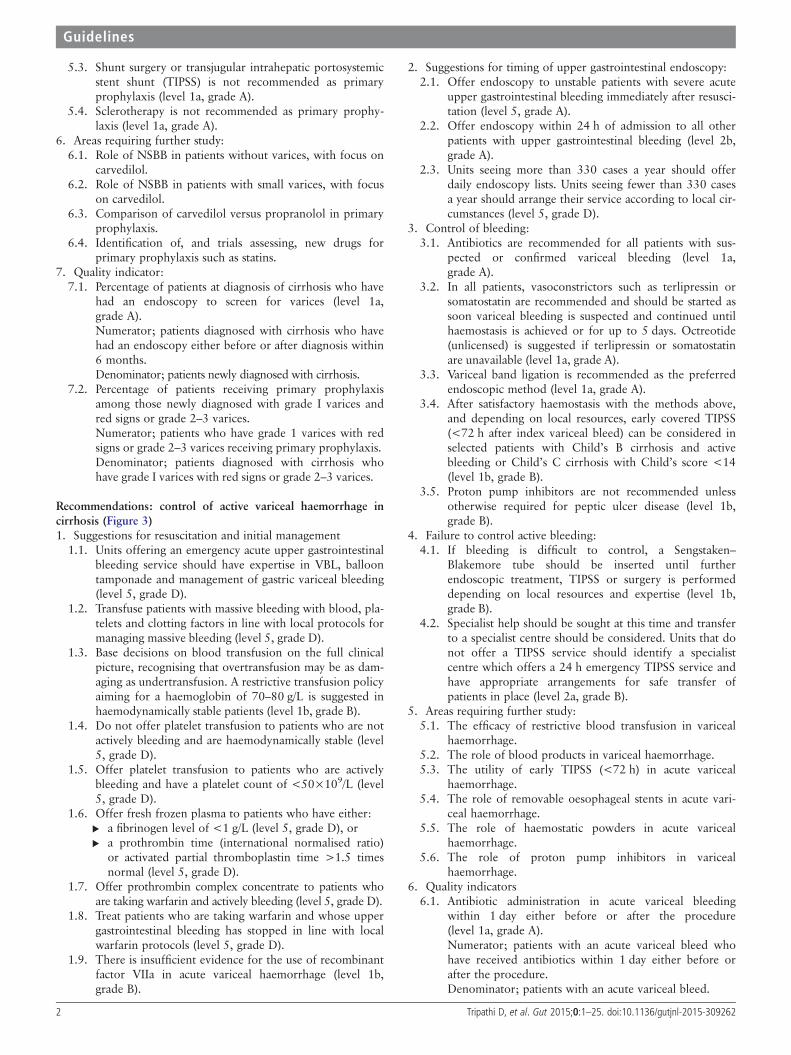
53 Shunt surgery or transjugular intrahepatic portosystemicstent shunt (TIPSS) is not recommended as primaryprophylaxis (level 1a grade A)
54 Sclerotherapy is not recommended as primary prophy-laxis (level 1a grade A)
6 Areas requiring further study61 Role of NSBB in patients without varices with focus on
carvedilol62 Role of NSBB in patients with small varices with focus
on carvedilol63 Comparison of carvedilol versus propranolol in primary
prophylaxis64 Identification of and trials assessing new drugs for
primary prophylaxis such as statins7 Quality indicator
71 Percentage of patients at diagnosis of cirrhosis who havehad an endoscopy to screen for varices (level 1agrade A)Numerator patients diagnosed with cirrhosis who havehad an endoscopy either before or after diagnosis within6 monthsDenominator patients newly diagnosed with cirrhosis
72 Percentage of patients receiving primary prophylaxisamong those newly diagnosed with grade I varices andred signs or grade 2ndash3 varicesNumerator patients who have grade 1 varices with redsigns or grade 2ndash3 varices receiving primary prophylaxisDenominator patients diagnosed with cirrhosis whohave grade I varices with red signs or grade 2ndash3 varices
Recommendations control of active variceal haemorrhage incirrhosis (Figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with blood pla-telets and clotting factors in line with local protocols formanaging massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusion policyaiming for a haemoglobin of 70ndash80 gL is suggested inhaemodynamically stable patients (level 1b grade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable (level5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L (level5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to local cir-cumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with sus-
pected or confirmed variceal bleeding (level 1agrade A)
32 In all patients vasoconstrictors such as terlipressin orsomatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding41 If bleeding is difficult to control a Sengstakenndash
Blakemore tube should be inserted until furtherendoscopic treatment TIPSS or surgery is performeddepending on local resources and expertise (level 1bgrade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure(level 1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
2 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or whenmonotherapy with VBL or NSBB is used owing tointolerance or contraindications to combination therapy)and in selected cases owing to patient choice PTFE-covered stents are recommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
Recommendations management of active haemorrhage fromgastric varices (Figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices11 Gastro-oesophageal varices (GOV)-1 treat as for
oesophageal varices (level 2b grade B)12 GOV-2 and isolated gastric varices (IGV)
121 We recommend initial endoscopic therapy withcyanoacrylate injection (level 1a grade A)
122 Thrombin may also be considered (level 4 grade C)13 TIPSS can be considered depending on local resources
and clinical judgement (level 3a grade B)2 If control of bleeding fails
21 Balloon tamponade is suggested for GOV and IGV-1until definitive treatment is undertaken (level 2b grade B)
22 Salvage TIPSS is suggested as the first-line definite treat-ment where feasible (level 3a grade B)
23 Balloon-occluded retrograde transvenous obliteration(B-RTO) or surgical shunting can be considered if TIPSSis not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered into
a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (level2b grade B) Note the optimum endoscopic follow-upstrategy remains unclear Thrombin can also be consid-ered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 3
Guidelines
56 Role of endoscopic ultrasound-guided injection of tissueadhesives or thrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
INTRODUCTIONThe guidelines refer closely to the Baveno V consensus state-ment published in 20101 and the 2012 NICE Guidelines onAcute Upper GI bleeding (CG141)2 These documents arewidely used and offer useful evidence-based guidance Howeverwe feel that owing to significant recent advances further addi-tions and refinements to the published guidance with particularfocus on resource implications service development and thepatient pathway are necessary The previously mentioned docu-ments1 2 do not cover all the recent advancesmdashin particular inthe field of acute variceal bleeding and the role of transjugularintrahepatic portosystemic stent shunt (TIPSS) There have alsobeen developments and better insights into drug treatment forprevention of varices and variceal bleedingmdashin particular therole of non-cardioselective β blockers (NSBB)
Guideline developmentThese guidelines were drafted after discussions within the liversection of the British Society of Gastroenterology (BSG) andacceptance of the proposal by the Clinical Services andStandards Committee (CSSC) There followed division of sec-tions to be researched by designated authors and an exhaustiveliterature review The Baveno V consensus and NICE guidelineswere closely followed and guideline quality was assessed usingthe AGREE tool3 (section lsquoAssessing the quality of guidelinesthe AGREE II instrumentrsquo)
A preliminary guideline document was drafted by the authorsfollowing discussion and where necessary voting by membersof the Guidelines Development Group (GDG) The draft guide-lines were submitted for review by CSSG then BSG councilmembers Finally full peer review was undertaken by reviewersselected by the editor of Gut
Attempts were made to preserve the format of the originalguidelines with additional sections relating to service develop-ment the patient pathway and pre-primary prophylaxis Thesection on the management of acute variceal bleeding has beenextensively rewritten to take into account recent importantdevelopments in interventional radiology drug treatment andresuscitation
Assessing the quality of guidelines the AGREE II instrumentThe AGREE II instrument is an accepted method for appraisingclinical guidelines3 Six domains are listed
Scope and purposeThe guidelines are intended for use by clinicians and otherhealthcare professionals managing patients with cirrhosis andgastro-oesophageal varices in light of recent guidance publishedby NICE2 and the Baveno V Consensus1 Important subsequentdevelopments are covered in depth due to the potential impacton clinical practice The guidelines are primarily aimed at man-agement of adult patients
Guideline development group membership and stakeholderinvolvementMembership of the group includes gastroenterologists hepatolo-gists and interventional radiologists with nursing and patientrepresentation
Rigour of developmentThe published literature was searched using Pubmed MedlineWeb of Knowledge and the Cochrane database between October2013 and February 2015 The GDG met through a series of tel-econferences during that time The guidelines rely considerablyon consensus statements published by the Baveno V Consensusand NICE1 2 The style of graded recommendations is deter-mined by the level of supporting evidence (graded level 1 to 5)as described by the Oxford Centre For Evidence BasedMedicine4 (table 1) and is as followsA consistent level 1 studiesB consistent level 2 or 3 studies or extrapolations from level 1
studiesC level 4 studies or extrapolations from level 2 or 3 studiesD level 5 evidence or troublingly inconsistent or inconclusive
studies of any levelAreas of disagreement about the recommendation grade were
subjected to discussion and if necessary voting by members ofthe guidelines group Where possible the health benefits sideeffects and risks of recommendations have been discussed Theguidelines were subject to peer review after submission for con-sideration of publication in Gut
Clarity and presentationRecommendations are intended to be specific to particular situa-tions and patient groups where necessary different options arelisted Key recommendations are linked to discussion threads ona discussion forum hosted on the BSG website
ApplicabilityWhere necessary we have discussed organisational changes thatmay be needed in order to apply recommendations We haveattempted to identify key criteria for monitoring and auditpurposes
Editorial independence and conflict of interestGuideline group members have declared any conflicts ofinterest
Scheduled review of guidelinesThe proposed time for review of the guidelines is 5 years totake into account new developments To ensure that there is afacility for feedback after publication links to the BSG discus-sion forums corresponding to the particular section of theseguidelines are included with this document This facility toprovide new evidence is provided to all BSG members Inaccordance with the AGREE II tool the BSG forum will providefeedback
SERVICE DELIVERY AND DEVELOPMENTDespite improvements in outcomes following variceal bleedingthe need to optimise the management of acute variceal bleed-ing is highlighted in recent publications and national reportsIn a national audit5 variceal bleeding accounted for just over10 of all admissions with acute GI bleeding in the UK withtwo-thirds having a previous history of variceal bleeding andover 50 presenting during normal working hours Endoscopywithin 24 h of presentation was achieved in only 66 of allpatients and in 70 of patients with documented cirrhosisMost procedures were performed in the endoscopy depart-ment with just 14 performed under general anaestheticdespite high-risk stigmata and endoscopic therapy beingrequired in two-thirds of cases Notably antibiotics were
4 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
administered in only 27 of patients before endoscopy andadministration of vasoactive drugs before endoscopy was onlyslightly higher at 44 Furthermore only four patients (lt1)were referred for TIPSS which may reflect the lack of accessto interventional radiology and that the audit was conductedbefore the trial of early TIPSS6 The National ConfidentialEnquiry into Patient Outcome and Death (NCEPOD) reportlsquoMeasuring the unitsrsquo assessed clinical management beforedeath of 594 patients with alcoholic liver disease over a6-month period in the UK7 Gastrointestinal bleeding wasnoted in 35 of cases with approximately 50 having vari-ceal bleeding Delays in endoscopy were noted in 10 ofcases and several aspects of clinical andor organisational carewere judged to be poor or unacceptable in 18 of patientspresenting with GI bleeding There were deficiencies noted inthe out-of-hours rotas for GI bleeding with 27 of hospitalsnot having a dedicated-out-of hours GI bleeding serviceStudies from other countries have also reported deficiencieswith delays in admission to hospital and administration of anti-biotics Two observational studies showed that access to
emergency endoscopy and use of prophylactic antibiotics andvasoactive drugs was better in tertiary centres although thisdid not appear to affect survival8 9
Acute variceal haemorrhage refractory to endoscopic andpharmacological treatments where TIPSS is usually indicatedmust be managed with appropriate resources TIPSS is an estab-lished interventional treatment for refractory or recurrent vari-ceal haemorrhage It remains a highly specialised procedurerequiring adequate training and experience Knowledge of therelevant equipment anatomy and how to deal with any compli-cations is essential It should therefore be performed in centreswith adequate personnel multidisciplinary support and equip-ment required to optimise management and minimise risks10
Regional centres with easily accessible interventional radiologyservices are generally best equipped to perform this procedureSetting up regional agreements and pathways to allow transfer ofappropriate patients to hospitals that undertake TIPSS proce-dures is an important step These pathways could also be used toprovide emergency endoscopic management if necessary due toproblems with out-of-hours endoscopic cover in smaller
Table 1 Levels of evidence
LevelTherapyprevention aetiologyharm Prognosis Diagnosis DDXsymptom prevalence study
1a SR (with homogeneity) ofrandomised controlled trial (RCT)
SR (with homogeneity) of inceptioncohort studies CDRdagger validated indifferent populations
SR (with homogeneity) of level 1diagnostic studies CDRdagger with 1b studiesfrom different clinical centres
SR (with homogeneity) ofprospective cohort studies
1b Individual RCT (with narrow CI) Individual inception cohort study withge80 follow-up CDRdagger validated in asingle population
ValidatingDagger cohort study with goodsectreference standards or CDRdagger testedwithin one clinical centre
Prospective cohort study with goodfollow-uppara
1c All or none All or none case series Absolute SpPins and SnNoutsdaggerdagger All or none case series2a SR (with homogeneity) of cohort
studiesSR (with homogeneity) of eitherretrospective cohort studies or untreatedcontrol groups in RCTs
SR (with homogeneity) of level gt2diagnostic studies
SR (with homogeneity) of 2b andbetter studies
2b Individual cohort study (includinglow-quality RCT eg lt80follow-up)
Retrospective cohort study or follow-upof untreated control patients in an RCTderivation of CDRdagger or validated on splitsampleDaggerDagger only
ExploratoryDagger cohort study with goodsectreference standards CDRdagger afterderivation or validated only on splitsampleDaggerDagger or databases
Retrospective cohort study or poorfollow-up
2c lsquoOutcomesrsquo research ecologicalstudies
lsquoOutcomesrsquo research Ecological studies
3a SR (with homogeneity) of casendashcontrol studies
SR (with homogeneity) of 3b and betterstudies
SR (with homogeneity) of 3b andbetter studies
3b Individual casendashcontrol study Non-consecutive study or withoutconsistently applied reference standards
Non-consecutive cohort study orvery limited population
4 Case series (and poor qualitycohort and case-control studiessectsect)
Case series (and poor quality prognosticcohort studiesparapara)
Casendashcontrol study poor ornon-independent reference standard
Case series or superseded referencestandards
5 Expert opinion without explicitcritical appraisal or based onphysiology bench research or lsquofirstprinciplesrsquo
Expert opinion without explicit criticalappraisal or based on physiology benchresearch or lsquofirst principlesrsquo
Expert opinion without explicit criticalappraisal or based on physiology benchresearch or lsquofirst principlesrsquo
Expert opinion without explicitcritical appraisal or based onphysiology bench research or lsquofirstprinciplesrsquo
Homogeneity means a systematic review (SR) that is free of worrisome variations (heterogeneity) in the directions and degrees of results between individual studies Not all SRs withstatistically significant heterogeneity need be worrisome and not all worrisome heterogeneity need be statistically significantdaggerCDR Clinical Decision Rule (algorithms or scoring systems which lead to a prognostic estimation or a diagnostic category)DaggerValidating studies test the quality of a specific diagnostic test based on prior evidence An exploratory study collects information and trawls the data (eg using a regression analysis) tofind which factors are lsquosignificantrsquosectGood reference standards are independent of the test and applied blindly or objectively to all patients Poor reference standards are haphazardly applied but still independent of thetest Use of a non-independent reference standard (where the lsquotestrsquo is included in the lsquoreferencersquo or where the lsquotestingrsquo affects the lsquoreferencersquo) implies a level 4 studyparaGood follow-up in a differential diagnosis study is gt80 with adequate time for alternative diagnoses to emerge (eg 1ndash6 months acute 1ndash5 years chronic)Met when all patients died before the treatment became available but some now survive while receiving it or when some patients died before the treatment became available butnone now die while receiving itdaggerdaggerAn lsquoabsolute SpPinrsquo a diagnostic finding whose Specificity is so high that a Positive result rules in the diagnosis An lsquoAbsolute SnNoutrsquo a diagnostic finding whose Sensitivity is sohigh that a Negative result rules out the diagnosisDaggerDaggerSplit-sample validation is achieved by collecting all the information in a single tranche then artificially dividing this into lsquoderivationrsquo and lsquovalidationrsquo samplessectsectPoor quality cohort study one that failed to clearly define comparison groups andor failed to measure exposures and outcomes in the same (preferably blinded) objective way inboth exposed and non-exposed individuals andor failed to identify or appropriately control known confounders andor failed to carry out a sufficiently long and complete follow-up ofpatients Poor quality casendashcontrol study one that failed to clearly define comparison groups andor failed to measure exposures and outcomes in the same (preferably blinded)objective way in both cases and controls andor failed to identify or appropriately control known confoundersparaparaPoor quality prognostic cohort study one in which sampling was biased in favour of patients who already had the target outcome or the measurement of outcomes wasaccomplished in lt80 of study patients or outcomes were determined in an unblinded non-objective way or there was no correction for confounding factors
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 5
Guidelines
hospitals This model referred to as ldquospoke and wheelrdquo ornetwork model is well established for other complex proceduresand helps to expedite and streamline the process In theNCEPOD report lsquoMeasuring the unitsrsquo just 15 of hospitals hadon-site access to TIPSS while 72 had access to TIPSS in othercentres7
There have been significant efforts to address the need toimprove the upper GI bleeding (UGIB) service A toolkit wasproduced in collaboration with BSG Association of UpperGastrointestinal Surgeons (AUGIS) Royal Colleges ofPhysicians Radiology and Nursing and Academy of MedicalRoyal Colleges11 The key nine service standards recommendedby the document are detailed below1 There will be a nominated individual with the authority to
ensure implementation by the contracted provider2 Contracted providers will ensure the minimum service is
adequately resourced3 All patients with suspected UGIB should be properly
assessed and their risk scored on presentation4 All patients should be resuscitated before therapeutic
intervention5 All high-risk patients with UGIB should be endoscoped
within 24 h preferably on a planned list in the first instance6 For patients who require more urgent intervention either for
endoscopy interventional radiology or surgery formal 247arrangements must be available
7 The necessary team meeting an agreed competency levelshould be available throughout the complete patient pathway
8 Each stage of the patient pathway should be carried out inan area with lsquoappropriatersquo facilities equipment and supportincluding staff experienced in the management of UGIB
9 All hospitals must collect a minimum dataset in order tomeasure service provision against auditable outcomes(case-mix adjusted as appropriate)NICE recommendations for endoscopy provision are detailed
in the section lsquoManagement of active variceal haemorrhagersquorecommendations2 The BSG has also produced a care bundlefor patients admitted with decompensated cirrhosis in light ofthe NCEPOD report with a check list method which includesgastrointestinal bleeding12
Since the 2008 Darzi report quality has become a priorityfor the NHS13 With these guidelines there is real opportunityto introduce quality outcomes based on good clinical evidenceFurthermore by incorporating them into the liver accreditationscheme Liver Quest one can improve and assure quality inliver services across the UK14 Therefore a small number ofquality outcomes measures have been chosen and form part ofthe key recommendations15
DEFINITIONSIt is important to define the terms that should be used in thecontext of a variceal bleed These are the Baveno V consensusdefinitions1
Variceal haemorrhageVariceal haemorrhage is defined as bleeding from an oesopha-geal or gastric varix at the time of endoscopy or the presence oflarge oesophageal varices with blood in the stomach and noother recognisable cause of bleeding An episode of bleeding isclinically significant when there is a transfusion requirement for2 units of blood or more within 24 h of the time zero togetherwith a systolic blood pressure of lt100 mm Hg or a posturalchange of gt20 mm Hg andor pulse rate gt100 bpm at time
zero (time zero is the time of admission to the first hospital towhich the patient is taken)
Time frame of acute bleedingThe acute bleeding episode is represented by an interval of120 h (5 days) from time zero Evidence of any bleeding after120 h is the first rebleeding episode
Failure to control active bleedingFailure to control active bleeding is defined as death or need tochange treatment defined by one of the following criteria16 17
1 Fresh haematemesis or nasogastric aspiration of ge100 mL offresh blood ge2 h after the start of a specific drug treatmentor therapeutic endoscopy
2 Development of hypovolaemic shock3 30 gL drop in haemoglobin (9 drop of haematocrit)
within any 24 h period if no transfusion is given This timeframe needs to be further validated
Variceal rebleedingVariceal rebleeding is defined as the occurrence of a singleepisode of clinically significant rebleeding from portal hyperten-sive sources from day 5 Clinically significant rebleeding isdefined as recurrent melaena or haematemesis in any of the fol-lowing settings1 hospital admission2 blood transfusion3 30 gL drop in haemoglobin4 death within 6 weeks
Early mortalityDeath within 6 weeks of the initial episode of bleeding
NATURAL HISTORY OF VARICES IN CIRRHOSISDevelopment of varicesThe rise in portal pressure is associated with the developmentof collateral circulation which allows the portal blood to bediverted into the systemic circulation These spontaneous shuntsoccur (a) at the cardia through the intrinsic and extrinsic gastro-oesophageal veins (b) in the anal canal where the superiorhaemorrhoidal vein belonging to the portal system anastomoseswith the middle and inferior haemorrhoidal veins which belongto the caval system (c) in the falciform ligament of the liverthrough the para-umbilical veins which are the remains of theumbilical circulation of the fetus (d) in the abdominal wall andthe retroperitoneal tissues from the liver to the diaphragmveins in the lienorenal ligament in the omentum and lumbarveins and (e) blood diversion from the diaphragm gastric pan-creatic splenic and adrenal veins which may drain into the leftrenal vein
Numerous lines of evidence suggest that varices develop andenlarge with time Christensen et al18 followed up a cohort of532 patients with cirrhosis and showed that the cumulative inci-dence of patients with varices increased from 12 to 90 over12 years In a study involving 80 patients followed up for16 months Cales and Pascal19 showed that 20 of patientswho did not have varices developed new varices and 42 ofpatients with small varices showed definite enlargement Czajaet al20 also showed that the prevalence of varices increased from8 to 13 over 5 years in a cohort of patients with chronicactive hepatitis even though they were treated with prednisol-one Merli et al21 in a study of 213 patients with cirrhosis withno or small varices demonstrated that the annual progression ofvarices was 12 A recent database analysis by DrsquoAmico et al22
6 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
using a competing risk model showed that the cumulative inci-dence of varices at 10 and 20 years was 44 and 53 respect-ively suggesting an overestimation in previous studies not usinga competing risk model
The main factors that appear to determine the developmentof varices are continued hepatic injury the degree of portosyste-mic shunting endoscopic appearances and portal pressureEvidence for the role of hepatic injury is derived from studies inwhich varices were shown to regress with time Baker et al23 fol-lowed up a cohort of 115 patients with oesophageal varices andshowed that varices had disappeared in nine patients regressedin seven and remained unchanged in six They concluded thatthe disappearance and regression of varices might be related toabstinence from alcohol This observation was confirmed in astudy by Dagradi24 who followed up a cohort of patients withalcoholic cirrhosis over 3 years and showed a reduction in vari-ceal size in 12 of the 15 patients with alcoholic cirrhosis whostopped drinking and an enlargement in variceal size in 17patients who continued to drink On the other hand Cales andPascal19 showed that regression of varices occurred in 16 ofpatients with alcoholic cirrhosis who continued to imbibealcohol This might be related to the development of large por-tosystemic collaterals which decompress the portal system andreduce the risk of the development of large oesophageal varicesThe degree of portosystemic shunting can be quantified bymeasuring the diameter of portal veins and collaterals and canbe significant in those with gastrorenal or splenorenal shunt-ing25 26 Others have shown that the presence of alcoholic cir-rhosis Childrsquos B or C cirrhosis and red whale signs on indexendoscopy predicted progression of varices21 Groszmannet al27 in a placebo-controlled randomised trial of timolol in213 cirrhotic patients without varices showed that a baselinehepatic venous pressure gradient (HVPG) of gt10 mm Hg or age10 increase in HVPG during follow-up were both predictiveof the development of varices
Diagnosis of gastro-oesophageal varicesUntil recently endoscopy has been used exclusively to diagnosevarices Non-invasive methods of screening for varices includecapsule endoscopy transient elastography and use of laboratoryand radiological findings
EndoscopyThere is universal acceptance that endoscopy is the lsquogold stand-ardrsquo for diagnosing gastro-oesophageal varices The main limita-tions are intraobserver variability in the diagnosis of small orgrade I oesophageal varices (figure 1AndashC) Recently unsedatednasal gastroscopy has been found to have similar accuracy toconventional endoscopy and has the advantage of tolerabilityand potential cost saving since it can be performed in the clinicsetting in some institutions28 29 However there are no con-trolled studies and banding of varices is not possible
Capsule endoscopyCapsule endoscopy uses a 26 mm pill-shaped device whichtransmits video footage which is stored and later analysedPatients are not sedated but patient cooperation is essentialIn a large study by de Franchis et al30 capsule endoscopy wascompared with standard gastroscopy The primary end point of90 or greater concordance was not achieved Lapalus et al31
in a prospective study of 120 patients demonstrated similarresults with capsule endoscopy Therefore capsule endoscopycannot be considered an alternative to standard endoscopyalthough may have a role in patient who refuse gastroscopy
Transient elastographyTransient elastography ((FibroScan Echosens Paris France) usesthe principles of ultrasound to derive tissue stiffness by measur-ing the speed of propagation of a low-frequency wave whichthen correlates with liver fibrosis Vizzutti et al32 in a study of61 patients with hepatitis C showed a sensitivity for predictionof oesophageal varices of 90 using a threshold 176 kPaHowever specificity was poor at 43 A study of 298 patientsfound the optimal cut-off point for the prediction of oesopha-geal varices was 215 kPa (sensitivity 76 and specificity78)33 In one uncontrolled study the use of transient elasto-graphy was found to be as effective as HVPG at predictingportal hypertension-related complications34 Therefore the roleof transient elastography in predicting varices is controversialdue to the lack of consistent results and controlled studies Thismodality may be more useful for predicting decompensation inpatients with cirrhosis
Radiological and serum parametersA prospective study of 311 patients with chronic hepatitis Cshowed that a platelet-to-spleen size ratio with a threshold of909 had positive and negative predictive values of 100 and94 respectively35 These good results have not been repro-duced by others as demonstrated in a meta-analysis36
Risk factors for first variceal bleedingThe factors that predispose to and precipitate variceal haemor-rhage are still not clear The suggestion that oesophagitis mayprecipitate variceal haemorrhage has been discarded37
Presently the most important factors that have been heldresponsible include (i) pressure within the varix (ii) varicealsize (iii) tension on the variceal wall and (iv) severity of theliver disease
Portal pressureIn most cases portal pressure reflects intravariceal pressure38
and a HVPG gt10 mm Hg is necessary for the development ofoesophageal varices27 There is no linear relationship betweenthe severity of portal hypertension and the risk of varicealhaemorrhage although HVPG gt12 mm Hg is an accepted
Figure 1 (A) Grade I oesophagealvarices These collapse to inflation ofthe oesophagus with air (B) Grade IIoesophageal varices These are varicesbetween grades 1 and 3 (C) Grade IIIoesophageal varices These are largeenough to occlude the lumen
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 7
Guidelines
threshold for variceal bleeding39 40 However the HVPG tendsto be higher in bleeders as well as in patients with larger varicesIn a prospective study comparing propranolol with placebo forthe prevention of first variceal haemorrhage Groszmann et al41
showed that bleeding from varices did not occur if the portalpressure gradient (PPG) could be reduced to lt12 mm HgOthers have shown that a 20 reduction in portal pressure pro-tects against further bleeding42 These haemodynamic goalshave been accepted as the aim of pharmacological treatment ofportal hypertension It is important to appreciate that gastricvarices can bleed at pressures lt12 mm Hg and the influence ofwall tension of the varix plays a greater role in the risk of bleed-ing43 A greater pressure reduction may be necessary to protectagainst bleeding This is further discussed in the section lsquoGastricvaricesrsquo At present measurement of portal pressure in guidingpharmacological treatments is limited to clinical trials in the UK
Variceal sizeVariceal size is best assessed endoscopically (figure 1AndashC)Published results are variable owing to the lack of a definition dis-tinguishing between large and small varices Small (grade I)varices tend to be narrow and flatten easily with air whereaslarger (grade 2 and 3) varices are usually broader and flatten withdifficulty if at all Numerous studies40 44 have shown that therisk of variceal haemorrhage increases with the size of varices45
Variceal wall and tensionPolio and Groszmann46 using an in vitro model showed thatrupture of varices was related to the tension on the varicealwall The tension depends on the radius of the varix In thismodel increasing the size of the varix and decreasing the thick-ness of the variceal wall caused variceal rupture Recently endo-scopic ultrasound and manometry have been used to estimatewall tension of varices47
Endoscopic features such as lsquored spotsrsquo and lsquowhalersquo markingswere first described by Dagradi24 They have been described asbeing important in the prediction of variceal haemorrhageThese features represent changes in variceal wall structure andtension associated with the development of microtelangiectasiasand reduced wall thickness In a retrospective study by theJapanese Research Society for Portal Hypertension Beppuet al48 showed that 80 of patients who had blue varices orcherry red spots bled from varices suggesting that this was animportant predictor of variceal haemorrhage in cirrhosis
Severity of liver disease and bleeding indicesTwo independent groups prospectively assessed factors predict-ing first variceal haemorrhage in cirrhosis (table 2) The NorthItalian Endoscopic Club (NIEC)49 reported their findings in1988 followed in 1990 by data from the Japanese50 Both thesestudies showed that the risk of bleeding was based on threefactors severity of liver disease as measured by Child class vari-ceal size and red wale markings The NIEC study showed awide range for the risk of bleeding of 6ndash76 depending on thepresence or absence of the different factors Using the same vari-ables the NIEC index was simplified by de Franchis et al51 andshown to correlate with the original index Further studiesshowed that the HVPG and intravariceal pressure were alsoindependent predictors of first variceal haemorrhage when ana-lysed in conjunction with the NIEC index52 53
In summary the most important factors that determine the risk ofvariceal haemorrhage are the severity of liver disease size of varicesand presence of red signs Measurement of HVPG is a useful guidefor selection of patients for treatment and their response to
treatment although the predictive value does not appear toimprove on the NIEC index and presence of red whale marking54
Risk and mortality of first variceal bleedData describing the overall risk of bleeding from varices must beviewed with caution and have some pitfalls in interpretationThe natural history of patients who have varices that are diag-nosed as part of their baseline investiations is different fromthat of patients who have complications of liver disease such asascites and encephalopathy Most studies do not comment oneither the severity of liver disease or whether patients with alco-holic cirrhosis are continuing to drink Both these factors have asignificant effect on the risk of variceal haemorrhage
Most studies report bleeding from varices in about 20ndash50of patients with cirrhosis during the period of follow-up Bakeret al23 reported variceal bleeding in 33 of 115 patients that theyfollowed up for a mean of 33 years with a mortality of 48from the first variceal haemorrhage These data were confirmedby Christensen et al18 About 70 of the episodes of bleedingoccur within 2 years of diagnosis Recent studies demonstrate adramatic reduction in mortality following variceal bleeding of20 6-week mortality55 and 15 in-hospital mortality5 withcontributions from improved endoscopic pharmacological andradiological therapies notably TIPSS Intensive care treatmenthas also improved with outcomes being particularly good forthose requiring minimal organ support
Analysis of the non-active treatment arms in the primaryprophylaxis trials comparing propranolol with placebo showresults similar to those of the primary prophylaxis shunt trialswith most episodes of bleeding occurring within the first 2 yearsof follow-up In these studies the rate of first variceal haemor-rhage ranged from 22 to 6156ndash60 This large difference inthe rate of first bleed relates almost certainly to the number ofpatients with severe liver disease included in the study (PascalChild Cmdash46 bleedingmdash61 Italian Multicenter Project forPropranolol in Prevention of Bleeding (IMPP) Child Cmdash6bleedingmdash32 Conn Child Cmdash6 bleedingmdash22)Mortality varied from 24 to 49 over 2 years (Pascal mortal-itymdash49 IMPP mortalitymdash24 Conn mortalitymdash24)
Primary prophylaxisSince 30ndash50 of patients with portal hypertension will bleedfrom varices and about 20 will die from the effects of the first
Table 2 Scoring systems for quantifying the severity of cirrhosisSeverity of liver disease can be described using the ChildndashPughscore or MELD scoreThe ChildndashPugh score is the sum of severity scores for Child classvariceal size and red wale markings the variables shown below
Category 1 2 3
Encephalopathy 0 III IIIIVAscites Absent Mild-moderate SevereBilirubin (μmolL) lt34 34ndash51 gt51Albumin (gL) gt35 28ndash35 lt28INR lt13 13ndash15 gt15
ChildndashPugh class A represents a score of le6 class B a score of 7ndash9 and class C ge10The MELD score is a formula that includes three laboratory-based variables reflectingthe severity of liver disease It was originally used to predict the short-term mortalityafter placement of a transjugular intrahepatic portosystemic stent-shunt for varicealbleeding Subsequently it has been used in selecting candidates for livertransplantationMELD score please use the online calculator httpswwwesotorgElitameldCalculatoraspxINR international normalised ratio
8 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleed it seems rational to develop prophylactic regimens toprevent the development of and bleeding from these varicesHowever most of the published trials do not have sufficientpower to identify favourable treatment effects Based on theexpected bleeding and death rates in the control group theminimum number of patients needed to detect a 50 reductionin bleeding would be 270 and 850 patients in each arm todetect the same reduction in mortality A proposed algorithmfor surveillance and prophylaxis of varices is shown in figure 2At this time there is insufficient evidence to support treatingpatients without varices or lsquopre-primary prophylaxisrsquo A largerandomised placebo-controlled trial of timolol in patientswithout varices and portal hypertension defined as HVPGgt6 mm Hg did not show any effect on the development ofvarices or variceal bleeding27 The role of drug treatment in pre-venting bleeding in patients with small varices is unclear Threerandomised placebo-controlled trials have studied this Caleset al61 showed that propranolol in patients with small or novarices resulted in greater development of varices Howeverpatients without varices were included and there was significantloss of patients to follow-up The second trial showed thatnadolol reduced variceal bleeding without survival benefit andincreased adverse events62 Sarin et al63 did not show any effectwith propranolol despite a significant effect on portal pressure
SurgeryPortacaval shuntsFour trials of portacaval shunts have been published which ran-domised a total of 302 patients64ndash67 either to prophylactic shuntsurgery or to non-active treatment A meta-analysis of thesestudies showed a significant benefit in the reduction of varicealbleeding (OR=031 95 CI 017 to 056) but also a signifi-cantly greater risk of hepatic encephalopathy (OR=2 95 CI12 to 31) and mortality (OR=16 95 CI 102 to 257) inpatients treated with shunt surgery68 At this time there is noevidence for the use of TIPSS for primary prophylaxis1
Devascularisation proceduresInokuchi50 showed that there was a significant reduction in vari-ceal bleeding and in mortality in patients treated with a varietyof devascularisation procedures There are however numerousproblems with the interpretation of this study because of theuse of different procedures in each of the 22 centres Theseresults require confirmation
Pharmacological treatmentNon-cardioselective β blockersThe mainstay of the pharmacological approach to the primaryprophylaxis of variceal haemorrhage has been NSBBPropranolol which has been shown to reduce the PPG reduceazygos blood flow and also variceal pressure It achieves this bycausing splanchnic vasoconstriction and reducing cardiacoutput There is no clear dose-related reduction in HVPG orcorrelation of HPVG reduction with reduction in heart rate69
Observational studies have shown that a 10ndash12 reduction inHVPG after acute administration of propranolol was associatedwith reduced bleeding and hepatic decompensation54 70
However HVPG monitoring is not routinely available in mostcentres outside of larger institutions A meta-analysis of nineplacebo-controlled randomised trials (964 patients) showed thatthe pooled risk difference for bleeding was minus11 (95 CIminus21 to minus1) and for death was minus9 (95 CI minus18 tominus1) in favour of propranolol71
Nadolol exerts similar effects on portal haemodynamicsalthough the effect on blood pressure may not be as pro-nounced Two placebo-controlled trials58 59 have shownreduced bleeding although in one study this was only seen onper protocol analysis59 There was no effect on overall survival
Carvedilol is a NSBB like propranolol and a vasodilator dueto α1 receptor blockade The latter reduces portocollateralresistance and by actions on hepatic stellate cells leads to areduction in intrahepatic resistance Haemodynamic studiesdemonstrate a greater reduction in portal pressure with
Figure 2 Algorithm for surveillance of varices and primary prophylaxis in cirrhosisndash If there is clear evidence of disease progression this interval can be modified by clinician Endoscopy should also be offered at time ofdecompensation
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 9
Guidelines
carvedilol than with propranolol although blood pressure isreduced72 73 The optimum dose is 625ndash125 mgday74 Higherdoses are not more effective and are associated with moreadverse eventsmdashin particular hypotension Carvedilol at a doseof 125 mgday at current UK prices is considerably cheaperthan propranolol 40 mg twice a day and nadolol 80 mgday(monthly cost pound120 pound562 and pound5 respectively) Two RCTs ofcarvedilol versus variceal band ligation (VBL) in primaryprophylaxis have been published75 76 The first study75 showedsignificantly reduced bleeding in the carvedilol arm (10 vs23 relative hazard 041 95 CI 019 to 096) with no effecton survival The second trial by Shah et al76 did not show anydifferences in bleeding or mortality Compliance with VBL wasbetter in the latter trial and unlike the first trial there were sig-nificantly more patients with viral hepatitis than alcoholic cir-rhosis A further study74 assessed the effect of carvedilol inpatients who were haemodynamic non-responders to propran-olol where haemodynamic response was defined as HVPGreduction to le12 mm Hg or by gt20 of baseline after 4 weeksof treatment Patients who were haemodynamic non-respondersor intolerant to carvedilol were treated with VBL Carvedilolresulted in significantly lower variceal bleeding compared withVBL and haemodynamic responders to carvedilol or propran-olol had significantly lower mortality than those treated withVBL It is worth noting that the study was not randomised
There have been recent suggestions based on low-level evi-dence that NSBB may result in a poorer outcome in patientswith cirrhosis and refractory ascites77 The lsquowindow hypothesisrsquofor β blockers in cirrhosis has also recently been described sug-gesting that NSBB are helpful in the compensated and earlydecompensated cirrhotic period but may not be helpful in veryearly cirrhosis such as in a patient with no varices and may beharmful in patients with end-stage cirrhosis with refractoryascites78 However recent large observational studies questionthe last hypothesis with improved survival seen in patients withrefractory ascites treated with NSBB79 unless patients have anepisode of spontaneous bacterial peritonitis80 Therefore untilthere are further prospective controlled studies NSBB should becontinued in patients with refractory ascites The clinician mustcarefully monitor haemodynamic parameters such as blood pres-sure and discontinue NSBB in patients with hypotension andrenal impairment as can occur after an episode of spontaneousbacterial peritonitis Other potentially severe adverse eventswith NSBB include symptomatic bradycardia asthma andcardiac failure Less severe side effects such as fatigue insomniaand sexual dysfunction may also result
Isosorbide mononitrateInterest in the use of vasodilators such as isosorbide mononitrate(ISMN) developed after the demonstration that it reduces portalpressure as effectively as propranolol81 but has subsequentlywaned A trial comparing ISMN with propranolol showed nosignificant difference between these agents82 Another rando-mised trial of ISMN versus placebo did show any difference inthe two arms83 Therefore ISMN is not recommended asmonotherapy in primary prophylaxis
β Blocker and ISMNThe combination of nadolol and ISMN has been compared withnadolol in a RCT The combination therapy reduced the fre-quency of bleeding significantly but no significant differenceswere detected in mortality84 However Garcia-Pagan et al85 in adouble-blind RCTof propranolol plus ISMN versus propranolol
plus placebo failed to show any differences between the twoarms Combination therapy is associated with more side effects
Proton pump inhibitorsA placebo-controlled randomised trial reported reduced bleed-ing and mortality with rabeprazole after eradication of varices86
However the study had a heterogeneous population with VBLperformed for both primary and secondary prophylaxis andsmall numbers (n=43) limiting the validity of the conclusionsFurthermore there was no arm comparing proton pump inhibi-tors with NSBB The use of proton pump inhibitors in patientswith cirrhosis and ascites was associated with increased risk ofspontaneous bacterial peritonitis in a large retrospective study87
This was not confirmed in a larger prospective non-randomisedstudy88 However a recent prospective observational study hasshown proton pump use to be associated with increased mortal-ity in cirrhosis89 Proton pump inhibitors are also associatedwith increased risk of Clostridium difficile infection90 Thereremains continuing concern about proton pump inhibitors inpatients with cirrhosis therefore caution should be used
Endoscopic therapyVariceal band ligationVBL has been compared with NSBB in 19 trials in a recentCochrane meta-analysis of 1504 patients91 Despite reducedbleeding (RR=067 95 CI 046 to 098) with VBL there wasno difference in overall mortality and bleeding-related mortalityThe difference in bleeding was not seen when only trials withlow selection or attrition bias were included Banding can haveserious complications The risk of fatal banding-induced bleed-ing was highlighted in a meta-analysis showing reduced fataladverse events with NSBB (OR=014 95 002 to 099)92
The optimal timing of banding intervals is discussed in thesection lsquoSecondary prophylaxis of variceal haemorrhagersquo A ran-domised trial of 96 patients who underwent endoscopic surveil-lance at 6 or 3 months after eradication of varices with VBL didnot demonstrate a difference in bleeding on mortality93
However the trial had a heterogeneous study group of patientswho underwent VBL both for primary (65) and secondaryprevention (35)
SclerotherapyNineteen trials have compared endoscopic variceal sclerotherapywith no treatment68 Owing to the marked heterogeneitybetween these studies a meta-analysis is clinically inappropri-ate68 Sclerotherapy does not offer any benefit in combinationwith NSBB or VBL compared with VBL or NSBB alone andincreases iatrogenic complications such as strictures94ndash96 At thistime sclerotherapy cannot be recommended for prophylaxis ofvariceal haemorrhage in patients with cirrhosis
Recommendations primary prophylaxis of variceal haemor-rhage in cirrhosis (figure 2)1 What is the best method for primary prophylaxis
11 We recommend NSBB or variceal band ligation (VBL)We suggest pharmacological treatment with propranololas first line VBL is offered if there are contraindicationsto NSBB The choice of VBL or NSBB should also takeinto account patient choice (level 1a grade A)
12 We suggest carvedilol or nadolol as alternatives to pro-pranolol (level 1b grade A)
13 Dose131 Propranolol 40 mg twice daily Dose titrated to
maximum tolerated or once heart rate (HR) of
10 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
50ndash55 bpm is reached to a maximum dose of320 mg (level 1a grade A)
132 Nadolol 40 mg daily dose Dose titrated tomaximum tolerated or once HR of 50ndash55 bpm isreached a maximum dose of 240 mg (level 1agrade A)
133 Carvedilol 625 mg once daily to increase tomaintenance of 125 mg after a week if toleratedor once HR of lt50ndash55 bpm is reached (level 1agrade A)
134 It is suggested that NSBB are discontinued at thetime of spontaneous bacterial peritonitis renalimpairment and hypotension (level 2b grade B)
14 In cases of contraindications or intolerance to NSBB werecommend variceal band ligation (level 1a grade A)
2 Who should have surveillance for variceal bleeding21 We recommend all patients with cirrhosis should be
endoscoped at the time of diagnosis (level 1a grade A)There is no indication to repeat endoscopy in patientsreceiving NSBB
3 How often should cirrhotic patients be endoscoped31 If at the time of first endoscopy no varices are seen we
suggest that patients with cirrhosis should be endos-coped at 2ndash3-year intervals (level 2a grade B)
32 If grade I varices are diagnosed we suggest that patientsshould be endoscoped at yearly intervals (level 2agrade B)
33 If there is clear evidence of disease progression wesuggest that the intervals can be modified by a clinicianEndoscopy should also be offered at time of decompen-sation (level 2a grade B)
4 Which patients with cirrhosis should have primaryprophylaxis41 If grade I varices and red signs or grade 2ndash3 varices are
diagnosed we recommend that patients have primaryprophylaxis irrespective of the severity of the liverdisease (level 1a grade A)
5 Treatments not recommended51 Proton pump inhibitors are not recommended unless
otherwise required for peptic ulcer disease (level 1bgrade B)
52 Isosorbide mononitrate monotherapy is not recommendedas primary prophylaxis (level 1b grade A) There is insuffi-cient evidence to recommend isosorbide mononitrate incombination with NSBB (level 1b grade A)
53 Shunt surgery or TIPSS is not recommended as primaryprophylaxis (level 1a grade A)
54 Sclerotherapy is not recommended as primary prophy-laxis (level 1a grade A)
6 Areas requiring further study61 Role of NSBB in patients without varices with focus on
carvedilol62 Role of NSBB in patients with small varices with focus
on carvedilol63 Comparison of carvedilol versus propranolol in primary
prophylaxis64 Identification of and trials assessing new drugs for
primary prophylaxis such as statins7 Quality indicator
71 Percentage of patients at diagnosis of cirrhosis who havehad an endoscopy to screen for varices (level 1agrade A)Numerator patients diagnosed with cirrhosis who havehad an endoscopy either before or after diagnosis within
6 monthsDenominator patients newly diagnosed with cirrhosis
72 Percentage of patients receiving primary prophylaxisamong those newly diagnosed with grade I varices andred signs or grade 2ndash3 varicesNumerator patients who have grade 1 varices with redsigns or grade 2ndash3 varices receiving primary prophy-laxisDenominator patients diagnosed with cirrhosis whohave grade I varices with red signs or grade 2ndash3 varices
MANAGEMENT OF ACTIVE VARICEAL HAEMORRHAGEThe average 6-week mortality of the first episode of varicealbleeding in most studies is reported to be up to 20 There hasbeen considerable improvement in survival since the early 1980swhen the in-hospital mortality was 40ndash5097 compared with15 from a recent UK audit5 Such is the improvement in out-comes that a patient with Childrsquos A cirrhosis is very unlikely tosuccumb to an index variceal bleed Studies have shown theChildndashPugh score MELD score and HVPG to be strong predic-tors of outcomes98ndash103 The MELD score has been shown tooutperform Childrsquos score in a recent study with a score gt19associated with 20 6 week mortality103 Furthermore theMELD score has been shown to perform as well as the trad-itional intensive care unit scores in predicting mortality inpatients admitted to intensive care in the UK104 MELD gt18active bleeding transfusing gt4 units of packed red blood cellshave been shown to be predictors of mortality and earlyrebleeding99 101 102 HVPG has also been shown to predictoutcome when measured at 2 weeks after a bleed44 and a valueof ge20 mm Hg when measured acutely within 48 h has beenshown to provide significant prognostic information100
However this technique is not used routinely in the manage-ment of patients around the world and substitution of clinicaldata in the latter study was shown to provide the same clinicalpredictive value100 These scoring systems are not purely aca-demic they allow the referring clinician to predict thosepatients with a high chance of rebleeding to be transferred to aspecialist centre offering for instance TIPSS before the patientrebleeds
Nonetheless probably the most important step in the man-agement of acute variceal haemorrhage is the initial resuscitationassessed according to standard lsquoABCrsquo practice together withprotection of the airway to prevent aspiration Although earlyendoscopy allows for accurate diagnosis of the bleeding site anddecisions about management (figure 3) therapeutic interventionin acute variceal bleeding can be initiated safely in most casesbefore diagnostic endoscopy As similar efficacy is demonstratedwith pharmacological treatment as with sclerotherapy theformer should be first-line therapy99 β Blockade should not bestarted in the acute setting and those already taking β blockersas prophylaxis should probably stop taking them for 48ndash72 h inorder that the patientrsquos physiological response to blood loss canbe allowed to manifest
General considerationsPatient evaluationThe majority of patients with a variceal bleed will be sufficientlystable to enable a full history and examination to take placeHistory of alcohol excess and or intravenous drug use should besought and may become particularly relevant if the patient haswithdrawal symptoms after admission Comorbidity is importantwhen estimating risk and deciding on use of vasopressors The
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 11
Guidelines
following risk factors doubled mortality after an acute varicealbleed in one US study older age comorbidities male gender andnot undergoing a gastroscopy within 24 h105
A full examination is helpful for the important negatives asmuch as the positives Baseline observations should include thetemperature as infection is a serious complication with signifi-cant mortality Confusion may be present because of encephal-opathy intoxication with alcohol or drugs or withdrawal fromalcohol or drugs The patient should be on continuous BP andpulse monitor and their haemodynamic status recordedAn oxygen saturation monitor is helpful Stigmata of chronicliver disease and concurrent jaundice provide insight into thecurrent status of a patientrsquos liver and also give warning ofpotential further decompensation if significant bleeding persists(see scoring systems above) Pneumonia must be actively
excluded Evidence of ascites requires a diagnostic tap to searchfor infection
Investigations including full blood count coagulationprofile liver and renal function and blood group and save andcross-match Blood and urine should also be cultured An ultra-sound scan later in the admission is helpful to identify subclin-ical ascites flow in portal vein and any obvious emergence of anhepatocellular carcinoma (HCC)
Location of patientA decision must be made as to where the patient is best managedVariceal bleeding is unpredictable generally occurs in patientswith significant liver disease and is associated with significant mor-tality Hence a high-dependency unit is usually the most appropri-ate initial location although a properly staffed lsquogastrointestinal
Figure 3 Algorithm for themanagement of acute varicealbleeding TIPSS transjugularintrahepatic portosystemic stent shunt
12 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleeding bedrsquo may be appropriate If a patient is vomiting bloodor there is a perceived risk of a haemodynamically unstable patienthaving blood in the stomach then the patient must be intubatedbefore endoscopy and return to an intensive care or high-dependency unit will be necessary until extubation
Volume resuscitation and blood productsIntravenous access (two 16ndash18G cannulae) should have beensecured on admission with a reported GI bleed Further intra-venous access may be necessary In patients with poor venousaccess advanced liver disease or renal failure associated withtheir liver disease central venous access may be helpful withguiding fluid infusions However the drawbacks include the riskof the procedure and a potential source of infection Thereforethere is no absolute requirement for a central line and no evi-dence of unequivocal benefit Intravenous fluid resuscitationshould be initiated with plasma expanders aiming to maintain asystolic blood pressure of 100 mm Hg Care with monitoring isparamount in this group of patients
Overtransfusion has been shown to have a deleterious effecton outcome In a recent single-centre RCT a restrictive transfu-sion policy of maintaining haemoglobin between 70 and 80 gLimproved the control of variceal bleeding (11 vs 22p=005) and lowered HVPG compared with a liberal transfu-sion policy without effect on 45-day survival106 However itshould be noted that these results were from a single Spanishcentre which was a tertiary unit for variceal bleeding where allpatients underwent endoscopy within 6 h Nonetheless arestrictive transfusion policy has been recommended for sometime1 and there is now good evidence to support not transfusinga stable patient with a haemoglobin of ge80 gL However under-resuscitation should also be avoided and while goal-orientedfluid replacement has generally not been useful in an intensivetherapy unit setting a venous saturation gt70 remains an easilymeasurable target with some evidence to support it107
Interpretation and management of clotting profile is challen-ging in liver disease where there is usually a balanced deficiencyof both procoagulant and anticoagulant factors108 The NICEguidelines recommend activation of a hospitalrsquos massive transfu-sion policy when there is major haemorrhage and plateletsupport when the value is lt50 and clotting factor supportwhen the international normalised ratio (INR) is gt15 timesnormal2 There is no evidence for the use of lsquoprophylacticrsquo clot-ting or platelet support to reduce the risk of rebleeding Thereis insufficient evidence to support the routine use of transexamicacid or recombinant factor VIIa109
Pharmacological treatmentThe two major classes of drugs that have been used in thecontrol of acute variceal bleeding are vasopressin or its analo-gues (either alone or in combination with nitroglycerine) andsomatostatin or its analogues Terlipressin is the only agent thathas been shown to reduce mortality in placebo-controlled trialsHowever in trials comparing terlipressin somatostatin andoctreotide no difference in efficacy was identified in a system-atic review110 and in a recent large RCT111 Prophylactic anti-biotics can result in a similar survival benefit following acutevariceal bleeding
VasopressinVasopressin reduces portal blood flow portal systemic collateralblood flow and variceal pressure It does however have signifi-cant systemic side effects such as an increase in peripheral resist-ance and reduction in cardiac output heart rate and coronary
blood flow In comparison with no active treatment the pooledresults of four randomised trials showed that it reduced failureto control variceal bleeding (OR=022 95 CI 012 to 043)although survival was unaffected68 Meta-analysis of five trialscomparing sclerotherapy with vasopressin has shown a signifi-cant effect on reduction in failure to control bleeding(OR=051 95 CI 027 to 097) with no effect on survival68
Vasopressin with nitroglycerineThe addition of nitroglycerine enhances the effect of vasopres-sin on portal pressure and reduces cardiovascular side effects112
Meta-analysis of three randomised trials comparing vasopressinalone with vasopressin and nitroglycerine showed that the com-bination was associated with a significant reduction in failure tocontrol bleeding (OR=039 95 CI 022 to 072) although nosurvival benefit was shown68
TerlipressinTerlipressin is a synthetic analogue of vasopressin which has animmediate systemic vasoconstrictor action followed by portalhaemodynamic effects due to slow conversion to vasopressin Ina Cochrane meta-analysis of seven placebo-controlled trials ter-lipressin was shown to reduce failure to control bleeding(RR=066 95 CI 055 to 093) and also to improve survival(RR=066 95 CI 049 to 088)113 In the same meta-analysisthere was no difference between terlipressin versus vasopressinballoon tamponade or endoscopic therapy in failure to controlbleeding or survival113 The role of terlipressin in combinationwith VBL is explored in the section lsquoEndoscopic therapy incombination with pharmacological therapyrsquo
The recommended dose of terlipressin is 2 mg IV every 4 halthough many units reduce the dose to 6 hourly as it may causeperipheral vasoconstriction which manifests as painful handsand feet While 5 days of IV treatment has been advocated inthe Baveno V guidelines1 this prolonged treatment has notbeen shown to have a survival benefit and for pragmaticreasons many units will stop treatment shortly after satisfactoryhaemostasis In a randomised trial terlipressin given for 24 hafter satisfactory haemostasis with VBL after oesophageal vari-ceal bleeding was as effective as 72 h of treatment114
In patients intolerant of terlipressin or in countries where ter-lipressin is not available alternatives should be considered
Somatostatin and octreotideSomatostatin causes selective splanchnic vasoconstriction andreduces portal pressure and portal blood flow115 Octreotide is asomatostatin analogue The mechanism of action of these twoagents is not clear Inhibition of glucagon increases vasodilatationrather than a direct vasoconstrictive effect and post-prandial guthyperaemia is also reduced The actions of octreotide on hepaticand systemic hemodynamics are transient making continuousinfusion necessary Octreotide is given as a 50 μg bolus followedby an infusion of 25ndash50 μgh Somatostatin is given as a 250 mgintravenous bolus followed by an infusion of 250 mghSomatostatin and octreotide have been shown to be aseffective as terlipressin in acute variceal bleeding in ameta-analysis110 Seo et al111 in a large RCTof 780 patients com-paring these three agents failed to show a difference in treatmentsuccess (range 838ndash862) rebleeding (range 34ndash44) andmortality (range 8ndash88) A low systolic blood pressure at pres-entation high serum creatinine level active bleeding in the emer-gency endoscopy gastric variceal bleeding and ChildndashPugh gradeC were independent factors predicting 5-day treatmentfailure111
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 13
Guidelines
AntibioticsAntibiotics that provide Gram-negative cover are one of the inter-ventions which positively influence survival in variceal haemor-rhage as shown in a Cochrane meta-analysis of 12placebo-controlled trials (RR=079 95 CI 063 to 098)116
Antibiotics were also shown to reduce bacterial infections(RR=043 95 CI 019 to 097) and early rebleeding (RR=05395 CI 038 to 074)116 Therefore short-term antibiotics shouldbe considered standard practice in all cirrhotic patients who have avariceal bleed irrespective of the presence of confirmed infectionThird-generation cephalosporins such as ceftriaxone (1 g IVdaily) have been shown to be more effective at reducingGram-negative sepsis than oral norfloxacin117 but choice of anti-biotics must be dictated by local resistance patterns and availability
Proton pump inhibitorsOne RCT compared a short course of proton pump inhibitorswith vasoconstrictor therapies after haemostasis in acute varicealbleeding118 Despite larger ulcers noted in the vasoconstrictorarm there were no differences in bleeding or survival Nearly50 of patients had ascites which might have implications inlight of the reports of increased incidence of spontaneous bac-terial peritonitis as mentioned earlier
Endoscopic therapyEndoscopy should take place within 24 h of admission andearlier if there is excessive bleeding based on low-level evi-dence105 While many guidelines and reviews suggest thatendoscopy should be carried out within 12 h the only study thatexamined the influence of timing on outcome failed to demon-strate any advantage of endoscopy before 12 h119 The optimaltime is after sufficient resuscitation and pharmacological treat-ment with the endoscopy performed by a skilled endoscopyteam in a suitably equipped theatre environment and withairway protection Airway protection is essential where risk ofaspiration is high and affords the endoscopist time for thoroughevaluation including complete clot aspiration and controlledapplication of treatment including tamponade if required Theendoscopy team must comprise an experienced endoscopynurse acquainted with the equipment necessary for endoscopytherapy of varices and a skilled endoscopist competent in usingbanding devices and deployment of balloon tamponade
Variceal band ligationThis technique is a modification of that used for the elastic bandligation of internal haemorrhoids Its use in humans was firstdescribed in 1988120 A meta-analysis of seven trials comparingVBL with sclerotherapy in acute bleeding showed that VBLreduced rebleeding from varices (OR=047 95 CI 029 to078) reduced mortality (OR=067 95 CI 046 to 098) andresulted in fewer oesophageal strictures (OR=010 95 CI003 to 029)121 The number of sessions required to obliteratevarices was lower with VBL (22 fewer sessions (95 CI 09to 35))
SclerotherapySclerotherapy has been replaced by VBL and should no longerbe offered as standard of care in acute variceal haemorrhage
Other endoscopic measuresIn an RCT cyanoacrylate offered no benefit over VBL with theadditional risk of embolisation and trend towards increasedrebleeding with cyanoacrylate122
Haemostatic powder (TC-325 Hemospray Cook MedicalUSA) has been described in a small study of nine patients whoreceived endoscopic spray treatment for acute variceal bleedingThe study reported no rebleeding within 24 h and no mortalityat 15 days123
Endoscopic therapy in combination with pharmacological therapyThe role of combining vasoactive drugs with endoscopictherapy (VBL or sclerotherapy) was reported in a meta-analysisof eight trials124 Combination therapy resulted in better initialcontrol of bleeding (RR=112 95 CI 102 to 123) and5-day haemostasis (RR=128 95 CI 118 to 139) withoutany difference in survival Adverse events were similar in bothgroups Two RCTs have compared VBL with sclerotherapy incombination with vasoactive agents in acute variceal bleed-ing125 126 Lo et al125 used vasopressin and found that VBLresulted in better 72 h haemostasis (97 vs 76 p=0009)with fewer complications (5 vs 29 p=0007) Villanuevaet al used somatostatin and reported lower failure to controlacute bleeding with VBL (4 vs 15 p=002) with fewerserious complications (4 vs 13 p=004) Overall survivalwas similar in both trials125 126
Balloon tamponadeBalloon tamponade is highly effective and controls acute bleed-ing in up to 90 of patients although about 50 rebleed whenthe balloon is deflated127 128 It is however associated withserious complications such as oesophageal ulceration and aspir-ation pneumonia in up to 15ndash20 of patients Despite this itmay be a life-saving treatment in cases of massive uncontrolledvariceal haemorrhage pending other forms of treatment Anappropriately placed SengstakenndashBlakemore tube allows forresuscitation safe transportation and either repeat endoscopy orradiological shunting in a patient with a stable cardiovascularsystem The oesophageal balloon is rarely required must neverbe used on its own and should be used only if there is continu-ing bleeding despite an adequately inflated gastric balloon cor-rectly placed and with appropriate tension Placement of thetube endoscopically or over a guide wire might reduce the riskof complications especially oesophageal rupture
Removable oesophageal stentsThe SX-Ella Danis stent (ELLA-CS Hradec Kralove CzechRepublic) is a removable covered metal mesh stent placed endo-scopically in the lower oesophagus without radiological screen-ing It has no role in the management of gastric varicealbleeding These stents can be left in situ for up to 2 weeksunlike the SengstakenndashBlakemore tube which should beremoved after a maximum of 24ndash48 h129 130 No published con-trolled trials have compared this modality with balloontamponade
Transjugular intrahepatic portosystemic stent-shuntSeveral uncontrolled studies have examined the role of salvagebare TIPSS in acute variceal bleeding In a review of 15 studiescontrol of bleeding was achieved in 90ndash100 with rebleedingin 6ndash16131 Mortality varied between 75 (in hospital) and15 (30 day) It is important to appreciate that sclerotherapywas used as first-line endoscopic therapy in most of thesestudies Long-term follow-up of a study that compared TIPSSwith H-graft portacaval shunts in patients for whom non-operative management had failed suggested that H-grafts were auseful method of reducing portal pressure and had a signifi-cantly lower failure rate (p=004) but had no significant
14 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
improvement in overall survival despite a benefit seen in ChildrsquosA and B disease132 A recent RCT compared emergency porto-caval surgery with bare TIPSS within 24 h of presenting withacute oesophageal variceal bleeding in unselected cirrhoticpatients Emergency portocaval surgery resulted in better out-comes for long-term bleeding control encephalopathy and sur-vival (plt0001)133 Before wider application of surgery foracute variceal bleeding more data are needed in light of therecent adoption of covered stents
There has also been a generalised established change in prac-tice in using covered TIPSS stents (polytetrafluoroethylene(PTFE)) rather than a bare metal stent with evidence to supportthis change In randomised controlled studies these stents wereshown to have higher primary patency rates than bare stentswithout significant differences in survival and the potential forreduced incidence of hepatic encephalopathy134 135
There is however growing evidence from two RCTs for theearlier use of TIPSS in selected patients stratified by HVPGChildndashPugh class and active bleeding and not just use as asalvage option6 136 Monescillo et al136 randomised patientspresenting with acute oesophageal variceal haemorrhage to bareTIPSS or standard of care if the HVPG was ge20 mm Hg within24 h of admission Significantly reduced treatment failure asdefined by failure to control acute bleeding andor early rebleed-ing (12 vs 50) was seen and improved survival (62 vs35) in the patients randomised to undergo a TIPSS procedureHowever the standard of care was sclerotherapy and not com-bination endoscopic and pharmacological treatment This limita-tion and the lack of availability of HVPG measurement in mostcentres meant this trial did not have a significant impact on clin-ical practice
Garcia-Pagan et al6 selected patients with active bleeding andChildrsquos B cirrhosis or patients with Childrsquos C cirrhosis (Childrsquosscore lt14) for randomisation to early PTFE-covered TIPSSwithin 72 h or standard of care with VBL and pharmacologicaltreatment This has shown encouraging results with reduced riskof treatment failure (3 vs 50) improved survival (86 vs61 at 1 year) yet without increased risk of hepatic encephal-opathy The results were supported by an observational studyfrom the same group although a survival benefit was notseen137 Furthermore a recent well-conducted observationalstudy did not demonstrate such high survival rates with earlyTIPSS with 11-year survival of 67 which was similar to thatof patients given endoscopic and pharmacological treatmentsonly138 Therefore larger multicentred RCTs need to be under-taken to further evaluate the role of early TIPSS It is importantto make the distinction between salvage TIPSS and early TIPSSto prevent rebleeding
Liver transplantationThis is probably appropriate only for patients who bleed whileawaiting liver transplantation although studies comparing VBLor TIPSS placement with urgent liver transplantation in thissituation need to be done Liver transplantation is an exceed-ingly rare option for the vast majority of patients both becauseit is not commonly available and because of shortages anddelays in organ procurement No controlled trials of liver trans-plantation in uncontrolledactive bleeding are available
Recommendations for the control of variceal bleeding in cir-rhosis are given below and in figure 3
Recommendations control of active variceal haemorrhage incirrhosis (figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with bloodplatelets and clotting factors in line with local protocolsfor managing massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusionpolicy aiming for a haemoglobin of 70ndash80 gL is sug-gested in haemodynamically stable patients (level 1bgrade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable(level 5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L(level 5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to localcircumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with suspected
or confirmed variceal bleeding (level 1a grade A)32 In all patients vasoconstrictors such as terlipressin or
somatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 15
Guidelines
41 If bleeding is difficult to control a SengstakenndashBlakemore tube should be inserted until further endo-scopic treatment TIPSS or surgery is performed depend-ing on local resources and expertise (level 1b grade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure (level1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
SECONDARY PROPHYLAXIS OF VARICEAL HAEMORRHAGEβ BlockersA meta-analysis of 12 trials comparing propranolol or nadolol139
with no active treatment showed a significant reduction inrebleeding but no significant reduction in mortality140 Thegreater reduction in portal pressure with carvedilol comparedwith propranolol has been described in the section lsquoPrimaryprophylaxisrsquo of this guideline
NitratesThe addition of ISMN to NSBB has been shown to reduce vari-ceal rebleeding compared with NSBB alone although no sur-vival benefit was seen141 In addition adverse events leading todrug withdrawal were more common in the group receivingcombined drug treatment A meta-analysis of ISMN alone orwith either NSBB or endoscopic therapy reported that there wasno mortality benefit from combining nitrates and NSBB com-pared with NSBB alone142
Side effects of ISMN include dizziness and headache Owingto the side effects and relative lack of data ISMN is not com-monly used in clinical practice
A recent RCT of 121 patients reported carvedilol to besimilar to combined ISMN and NSBB therapy in the preventionof variceal rebleeding and mortality although severe adverseevents were less common with carvedilol143
SimvastatinA recent abstract of a multicentre RCT of 158 patients reporteda survival benefit (91 vs 78 p=003) from adding simvasta-tin to VBL and NSBB compared with placebo VBL and NSBBas treatment for the prevention of variceal rebleeding144 Therewas no difference in rebleeding and the survival benefit wasrestricted to Child A and B patients Serious adverse events weresimilar in both groups More data are required to investigatethis interesting observation of a survival benefit from simvastatinin this situation which may relate to its effects on hepatocellularfunction fibrosis and portal pressure
Proton pump inhibitorsA double-blind randomised placebo-controlled trial showed thatpantoprazole reduced the size of ulcers in patients who under-went VBL However the total number of ulcers and other out-comes were similar in the two groups145
Endoscopic therapyVBL has been accepted as the preferred endoscopic treatmentfor the prevention of variceal rebleeding with a lower rate ofrebleeding mortality and complications than sclerother-apy146 147 The time interval between VBL sessions to achieveeradication of varices is debateable However a recent RCTcomparing monthly with biweekly VBL after initial haemostasiswith VBL in 70 patients suggested that there were fewerpost-VBL ulcers in the monthly group (11 vs 57plt0001)148 Variceal recurrence rebleeding and mortality weresimilar in both groups
Two meta-analyses showed there is no evidence that the add-ition of sclerotherapy to VBL improves clinically relevant out-comes including variceal rebleeding and death and thecombination led to higher stricture rates149 150
Endoscopic therapy versus drug therapyVBL has been reported to be more effective than combinedNSBB and ISMN drug therapy151 However an 8-yearfollow-up study of this RCT found that although VBL wassuperior in reducing variceal rebleeding survival rates were sig-nificantly higher in the group treated with combined drug treat-ment152 Other studies have found no superiority of VBL overcombined drug therapy for prevention of variceal rebleeding ormortality153 154 A recent small multicentre RCT reported carve-dilol to be similar to VBL in the prevention of variceal rebleed-ing with a trend in favour of survival with carvedilol (73 vs48 p=0110)155
Several meta-analyses have compared drug therapy with VBLin the prevention of variceal rebleeding One meta-analysis ofsix RCTs showed no significant difference in variceal rebleedingrates when comparing VBL alone with combined NSBB andISMN therapy However all-cause mortality was significantlyhigher in patients treated with the VBL (RR=125 95 CI101 to 155)156 Three meta-analyses comparing drug therapy(NSBB alone or with ISMN) with endoscopic therapy alonereported no difference in variceal rebleeding or mortality157ndash159
Endoscopic+drug therapy versus either aloneNumerous studies and several meta-analyses have comparedcombined endoscopic and drug therapy with monotherapy(endoscopic or drugs alone) in the prevention of varicealrebleeding A meta-analysis of 23 trials assessing sclerotherapyor VBL combined with NSBB reported that combinationtherapy reduced rebleeding more than either endoscopic
16 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or whenmonotherapy with VBL or NSBB is used owing tointolerance or contraindications to combination therapy)and in selected cases owing to patient choice PTFE-covered stents are recommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
Recommendations management of active haemorrhage fromgastric varices (Figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices11 Gastro-oesophageal varices (GOV)-1 treat as for
oesophageal varices (level 2b grade B)12 GOV-2 and isolated gastric varices (IGV)
121 We recommend initial endoscopic therapy withcyanoacrylate injection (level 1a grade A)
122 Thrombin may also be considered (level 4 grade C)13 TIPSS can be considered depending on local resources
and clinical judgement (level 3a grade B)2 If control of bleeding fails
21 Balloon tamponade is suggested for GOV and IGV-1until definitive treatment is undertaken (level 2b grade B)
22 Salvage TIPSS is suggested as the first-line definite treat-ment where feasible (level 3a grade B)
23 Balloon-occluded retrograde transvenous obliteration(B-RTO) or surgical shunting can be considered if TIPSSis not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered into
a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (level2b grade B) Note the optimum endoscopic follow-upstrategy remains unclear Thrombin can also be consid-ered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 3
Guidelines
56 Role of endoscopic ultrasound-guided injection of tissueadhesives or thrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
INTRODUCTIONThe guidelines refer closely to the Baveno V consensus state-ment published in 20101 and the 2012 NICE Guidelines onAcute Upper GI bleeding (CG141)2 These documents arewidely used and offer useful evidence-based guidance Howeverwe feel that owing to significant recent advances further addi-tions and refinements to the published guidance with particularfocus on resource implications service development and thepatient pathway are necessary The previously mentioned docu-ments1 2 do not cover all the recent advancesmdashin particular inthe field of acute variceal bleeding and the role of transjugularintrahepatic portosystemic stent shunt (TIPSS) There have alsobeen developments and better insights into drug treatment forprevention of varices and variceal bleedingmdashin particular therole of non-cardioselective β blockers (NSBB)
Guideline developmentThese guidelines were drafted after discussions within the liversection of the British Society of Gastroenterology (BSG) andacceptance of the proposal by the Clinical Services andStandards Committee (CSSC) There followed division of sec-tions to be researched by designated authors and an exhaustiveliterature review The Baveno V consensus and NICE guidelineswere closely followed and guideline quality was assessed usingthe AGREE tool3 (section lsquoAssessing the quality of guidelinesthe AGREE II instrumentrsquo)
A preliminary guideline document was drafted by the authorsfollowing discussion and where necessary voting by membersof the Guidelines Development Group (GDG) The draft guide-lines were submitted for review by CSSG then BSG councilmembers Finally full peer review was undertaken by reviewersselected by the editor of Gut
Attempts were made to preserve the format of the originalguidelines with additional sections relating to service develop-ment the patient pathway and pre-primary prophylaxis Thesection on the management of acute variceal bleeding has beenextensively rewritten to take into account recent importantdevelopments in interventional radiology drug treatment andresuscitation
Assessing the quality of guidelines the AGREE II instrumentThe AGREE II instrument is an accepted method for appraisingclinical guidelines3 Six domains are listed
Scope and purposeThe guidelines are intended for use by clinicians and otherhealthcare professionals managing patients with cirrhosis andgastro-oesophageal varices in light of recent guidance publishedby NICE2 and the Baveno V Consensus1 Important subsequentdevelopments are covered in depth due to the potential impacton clinical practice The guidelines are primarily aimed at man-agement of adult patients
Guideline development group membership and stakeholderinvolvementMembership of the group includes gastroenterologists hepatolo-gists and interventional radiologists with nursing and patientrepresentation
Rigour of developmentThe published literature was searched using Pubmed MedlineWeb of Knowledge and the Cochrane database between October2013 and February 2015 The GDG met through a series of tel-econferences during that time The guidelines rely considerablyon consensus statements published by the Baveno V Consensusand NICE1 2 The style of graded recommendations is deter-mined by the level of supporting evidence (graded level 1 to 5)as described by the Oxford Centre For Evidence BasedMedicine4 (table 1) and is as followsA consistent level 1 studiesB consistent level 2 or 3 studies or extrapolations from level 1
studiesC level 4 studies or extrapolations from level 2 or 3 studiesD level 5 evidence or troublingly inconsistent or inconclusive
studies of any levelAreas of disagreement about the recommendation grade were
subjected to discussion and if necessary voting by members ofthe guidelines group Where possible the health benefits sideeffects and risks of recommendations have been discussed Theguidelines were subject to peer review after submission for con-sideration of publication in Gut
Clarity and presentationRecommendations are intended to be specific to particular situa-tions and patient groups where necessary different options arelisted Key recommendations are linked to discussion threads ona discussion forum hosted on the BSG website
ApplicabilityWhere necessary we have discussed organisational changes thatmay be needed in order to apply recommendations We haveattempted to identify key criteria for monitoring and auditpurposes
Editorial independence and conflict of interestGuideline group members have declared any conflicts ofinterest
Scheduled review of guidelinesThe proposed time for review of the guidelines is 5 years totake into account new developments To ensure that there is afacility for feedback after publication links to the BSG discus-sion forums corresponding to the particular section of theseguidelines are included with this document This facility toprovide new evidence is provided to all BSG members Inaccordance with the AGREE II tool the BSG forum will providefeedback
SERVICE DELIVERY AND DEVELOPMENTDespite improvements in outcomes following variceal bleedingthe need to optimise the management of acute variceal bleed-ing is highlighted in recent publications and national reportsIn a national audit5 variceal bleeding accounted for just over10 of all admissions with acute GI bleeding in the UK withtwo-thirds having a previous history of variceal bleeding andover 50 presenting during normal working hours Endoscopywithin 24 h of presentation was achieved in only 66 of allpatients and in 70 of patients with documented cirrhosisMost procedures were performed in the endoscopy depart-ment with just 14 performed under general anaestheticdespite high-risk stigmata and endoscopic therapy beingrequired in two-thirds of cases Notably antibiotics were
4 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
administered in only 27 of patients before endoscopy andadministration of vasoactive drugs before endoscopy was onlyslightly higher at 44 Furthermore only four patients (lt1)were referred for TIPSS which may reflect the lack of accessto interventional radiology and that the audit was conductedbefore the trial of early TIPSS6 The National ConfidentialEnquiry into Patient Outcome and Death (NCEPOD) reportlsquoMeasuring the unitsrsquo assessed clinical management beforedeath of 594 patients with alcoholic liver disease over a6-month period in the UK7 Gastrointestinal bleeding wasnoted in 35 of cases with approximately 50 having vari-ceal bleeding Delays in endoscopy were noted in 10 ofcases and several aspects of clinical andor organisational carewere judged to be poor or unacceptable in 18 of patientspresenting with GI bleeding There were deficiencies noted inthe out-of-hours rotas for GI bleeding with 27 of hospitalsnot having a dedicated-out-of hours GI bleeding serviceStudies from other countries have also reported deficiencieswith delays in admission to hospital and administration of anti-biotics Two observational studies showed that access to
emergency endoscopy and use of prophylactic antibiotics andvasoactive drugs was better in tertiary centres although thisdid not appear to affect survival8 9
Acute variceal haemorrhage refractory to endoscopic andpharmacological treatments where TIPSS is usually indicatedmust be managed with appropriate resources TIPSS is an estab-lished interventional treatment for refractory or recurrent vari-ceal haemorrhage It remains a highly specialised procedurerequiring adequate training and experience Knowledge of therelevant equipment anatomy and how to deal with any compli-cations is essential It should therefore be performed in centreswith adequate personnel multidisciplinary support and equip-ment required to optimise management and minimise risks10
Regional centres with easily accessible interventional radiologyservices are generally best equipped to perform this procedureSetting up regional agreements and pathways to allow transfer ofappropriate patients to hospitals that undertake TIPSS proce-dures is an important step These pathways could also be used toprovide emergency endoscopic management if necessary due toproblems with out-of-hours endoscopic cover in smaller
Table 1 Levels of evidence
LevelTherapyprevention aetiologyharm Prognosis Diagnosis DDXsymptom prevalence study
1a SR (with homogeneity) ofrandomised controlled trial (RCT)
SR (with homogeneity) of inceptioncohort studies CDRdagger validated indifferent populations
SR (with homogeneity) of level 1diagnostic studies CDRdagger with 1b studiesfrom different clinical centres
SR (with homogeneity) ofprospective cohort studies
1b Individual RCT (with narrow CI) Individual inception cohort study withge80 follow-up CDRdagger validated in asingle population
ValidatingDagger cohort study with goodsectreference standards or CDRdagger testedwithin one clinical centre
Prospective cohort study with goodfollow-uppara
1c All or none All or none case series Absolute SpPins and SnNoutsdaggerdagger All or none case series2a SR (with homogeneity) of cohort
studiesSR (with homogeneity) of eitherretrospective cohort studies or untreatedcontrol groups in RCTs
SR (with homogeneity) of level gt2diagnostic studies
SR (with homogeneity) of 2b andbetter studies
2b Individual cohort study (includinglow-quality RCT eg lt80follow-up)
Retrospective cohort study or follow-upof untreated control patients in an RCTderivation of CDRdagger or validated on splitsampleDaggerDagger only
ExploratoryDagger cohort study with goodsectreference standards CDRdagger afterderivation or validated only on splitsampleDaggerDagger or databases
Retrospective cohort study or poorfollow-up
2c lsquoOutcomesrsquo research ecologicalstudies
lsquoOutcomesrsquo research Ecological studies
3a SR (with homogeneity) of casendashcontrol studies
SR (with homogeneity) of 3b and betterstudies
SR (with homogeneity) of 3b andbetter studies
3b Individual casendashcontrol study Non-consecutive study or withoutconsistently applied reference standards
Non-consecutive cohort study orvery limited population
4 Case series (and poor qualitycohort and case-control studiessectsect)
Case series (and poor quality prognosticcohort studiesparapara)
Casendashcontrol study poor ornon-independent reference standard
Case series or superseded referencestandards
5 Expert opinion without explicitcritical appraisal or based onphysiology bench research or lsquofirstprinciplesrsquo
Expert opinion without explicit criticalappraisal or based on physiology benchresearch or lsquofirst principlesrsquo
Expert opinion without explicit criticalappraisal or based on physiology benchresearch or lsquofirst principlesrsquo
Expert opinion without explicitcritical appraisal or based onphysiology bench research or lsquofirstprinciplesrsquo
Homogeneity means a systematic review (SR) that is free of worrisome variations (heterogeneity) in the directions and degrees of results between individual studies Not all SRs withstatistically significant heterogeneity need be worrisome and not all worrisome heterogeneity need be statistically significantdaggerCDR Clinical Decision Rule (algorithms or scoring systems which lead to a prognostic estimation or a diagnostic category)DaggerValidating studies test the quality of a specific diagnostic test based on prior evidence An exploratory study collects information and trawls the data (eg using a regression analysis) tofind which factors are lsquosignificantrsquosectGood reference standards are independent of the test and applied blindly or objectively to all patients Poor reference standards are haphazardly applied but still independent of thetest Use of a non-independent reference standard (where the lsquotestrsquo is included in the lsquoreferencersquo or where the lsquotestingrsquo affects the lsquoreferencersquo) implies a level 4 studyparaGood follow-up in a differential diagnosis study is gt80 with adequate time for alternative diagnoses to emerge (eg 1ndash6 months acute 1ndash5 years chronic)Met when all patients died before the treatment became available but some now survive while receiving it or when some patients died before the treatment became available butnone now die while receiving itdaggerdaggerAn lsquoabsolute SpPinrsquo a diagnostic finding whose Specificity is so high that a Positive result rules in the diagnosis An lsquoAbsolute SnNoutrsquo a diagnostic finding whose Sensitivity is sohigh that a Negative result rules out the diagnosisDaggerDaggerSplit-sample validation is achieved by collecting all the information in a single tranche then artificially dividing this into lsquoderivationrsquo and lsquovalidationrsquo samplessectsectPoor quality cohort study one that failed to clearly define comparison groups andor failed to measure exposures and outcomes in the same (preferably blinded) objective way inboth exposed and non-exposed individuals andor failed to identify or appropriately control known confounders andor failed to carry out a sufficiently long and complete follow-up ofpatients Poor quality casendashcontrol study one that failed to clearly define comparison groups andor failed to measure exposures and outcomes in the same (preferably blinded)objective way in both cases and controls andor failed to identify or appropriately control known confoundersparaparaPoor quality prognostic cohort study one in which sampling was biased in favour of patients who already had the target outcome or the measurement of outcomes wasaccomplished in lt80 of study patients or outcomes were determined in an unblinded non-objective way or there was no correction for confounding factors
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 5
Guidelines
hospitals This model referred to as ldquospoke and wheelrdquo ornetwork model is well established for other complex proceduresand helps to expedite and streamline the process In theNCEPOD report lsquoMeasuring the unitsrsquo just 15 of hospitals hadon-site access to TIPSS while 72 had access to TIPSS in othercentres7
There have been significant efforts to address the need toimprove the upper GI bleeding (UGIB) service A toolkit wasproduced in collaboration with BSG Association of UpperGastrointestinal Surgeons (AUGIS) Royal Colleges ofPhysicians Radiology and Nursing and Academy of MedicalRoyal Colleges11 The key nine service standards recommendedby the document are detailed below1 There will be a nominated individual with the authority to
ensure implementation by the contracted provider2 Contracted providers will ensure the minimum service is
adequately resourced3 All patients with suspected UGIB should be properly
assessed and their risk scored on presentation4 All patients should be resuscitated before therapeutic
intervention5 All high-risk patients with UGIB should be endoscoped
within 24 h preferably on a planned list in the first instance6 For patients who require more urgent intervention either for
endoscopy interventional radiology or surgery formal 247arrangements must be available
7 The necessary team meeting an agreed competency levelshould be available throughout the complete patient pathway
8 Each stage of the patient pathway should be carried out inan area with lsquoappropriatersquo facilities equipment and supportincluding staff experienced in the management of UGIB
9 All hospitals must collect a minimum dataset in order tomeasure service provision against auditable outcomes(case-mix adjusted as appropriate)NICE recommendations for endoscopy provision are detailed
in the section lsquoManagement of active variceal haemorrhagersquorecommendations2 The BSG has also produced a care bundlefor patients admitted with decompensated cirrhosis in light ofthe NCEPOD report with a check list method which includesgastrointestinal bleeding12
Since the 2008 Darzi report quality has become a priorityfor the NHS13 With these guidelines there is real opportunityto introduce quality outcomes based on good clinical evidenceFurthermore by incorporating them into the liver accreditationscheme Liver Quest one can improve and assure quality inliver services across the UK14 Therefore a small number ofquality outcomes measures have been chosen and form part ofthe key recommendations15
DEFINITIONSIt is important to define the terms that should be used in thecontext of a variceal bleed These are the Baveno V consensusdefinitions1
Variceal haemorrhageVariceal haemorrhage is defined as bleeding from an oesopha-geal or gastric varix at the time of endoscopy or the presence oflarge oesophageal varices with blood in the stomach and noother recognisable cause of bleeding An episode of bleeding isclinically significant when there is a transfusion requirement for2 units of blood or more within 24 h of the time zero togetherwith a systolic blood pressure of lt100 mm Hg or a posturalchange of gt20 mm Hg andor pulse rate gt100 bpm at time
zero (time zero is the time of admission to the first hospital towhich the patient is taken)
Time frame of acute bleedingThe acute bleeding episode is represented by an interval of120 h (5 days) from time zero Evidence of any bleeding after120 h is the first rebleeding episode
Failure to control active bleedingFailure to control active bleeding is defined as death or need tochange treatment defined by one of the following criteria16 17
1 Fresh haematemesis or nasogastric aspiration of ge100 mL offresh blood ge2 h after the start of a specific drug treatmentor therapeutic endoscopy
2 Development of hypovolaemic shock3 30 gL drop in haemoglobin (9 drop of haematocrit)
within any 24 h period if no transfusion is given This timeframe needs to be further validated
Variceal rebleedingVariceal rebleeding is defined as the occurrence of a singleepisode of clinically significant rebleeding from portal hyperten-sive sources from day 5 Clinically significant rebleeding isdefined as recurrent melaena or haematemesis in any of the fol-lowing settings1 hospital admission2 blood transfusion3 30 gL drop in haemoglobin4 death within 6 weeks
Early mortalityDeath within 6 weeks of the initial episode of bleeding
NATURAL HISTORY OF VARICES IN CIRRHOSISDevelopment of varicesThe rise in portal pressure is associated with the developmentof collateral circulation which allows the portal blood to bediverted into the systemic circulation These spontaneous shuntsoccur (a) at the cardia through the intrinsic and extrinsic gastro-oesophageal veins (b) in the anal canal where the superiorhaemorrhoidal vein belonging to the portal system anastomoseswith the middle and inferior haemorrhoidal veins which belongto the caval system (c) in the falciform ligament of the liverthrough the para-umbilical veins which are the remains of theumbilical circulation of the fetus (d) in the abdominal wall andthe retroperitoneal tissues from the liver to the diaphragmveins in the lienorenal ligament in the omentum and lumbarveins and (e) blood diversion from the diaphragm gastric pan-creatic splenic and adrenal veins which may drain into the leftrenal vein
Numerous lines of evidence suggest that varices develop andenlarge with time Christensen et al18 followed up a cohort of532 patients with cirrhosis and showed that the cumulative inci-dence of patients with varices increased from 12 to 90 over12 years In a study involving 80 patients followed up for16 months Cales and Pascal19 showed that 20 of patientswho did not have varices developed new varices and 42 ofpatients with small varices showed definite enlargement Czajaet al20 also showed that the prevalence of varices increased from8 to 13 over 5 years in a cohort of patients with chronicactive hepatitis even though they were treated with prednisol-one Merli et al21 in a study of 213 patients with cirrhosis withno or small varices demonstrated that the annual progression ofvarices was 12 A recent database analysis by DrsquoAmico et al22
6 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
using a competing risk model showed that the cumulative inci-dence of varices at 10 and 20 years was 44 and 53 respect-ively suggesting an overestimation in previous studies not usinga competing risk model
The main factors that appear to determine the developmentof varices are continued hepatic injury the degree of portosyste-mic shunting endoscopic appearances and portal pressureEvidence for the role of hepatic injury is derived from studies inwhich varices were shown to regress with time Baker et al23 fol-lowed up a cohort of 115 patients with oesophageal varices andshowed that varices had disappeared in nine patients regressedin seven and remained unchanged in six They concluded thatthe disappearance and regression of varices might be related toabstinence from alcohol This observation was confirmed in astudy by Dagradi24 who followed up a cohort of patients withalcoholic cirrhosis over 3 years and showed a reduction in vari-ceal size in 12 of the 15 patients with alcoholic cirrhosis whostopped drinking and an enlargement in variceal size in 17patients who continued to drink On the other hand Cales andPascal19 showed that regression of varices occurred in 16 ofpatients with alcoholic cirrhosis who continued to imbibealcohol This might be related to the development of large por-tosystemic collaterals which decompress the portal system andreduce the risk of the development of large oesophageal varicesThe degree of portosystemic shunting can be quantified bymeasuring the diameter of portal veins and collaterals and canbe significant in those with gastrorenal or splenorenal shunt-ing25 26 Others have shown that the presence of alcoholic cir-rhosis Childrsquos B or C cirrhosis and red whale signs on indexendoscopy predicted progression of varices21 Groszmannet al27 in a placebo-controlled randomised trial of timolol in213 cirrhotic patients without varices showed that a baselinehepatic venous pressure gradient (HVPG) of gt10 mm Hg or age10 increase in HVPG during follow-up were both predictiveof the development of varices
Diagnosis of gastro-oesophageal varicesUntil recently endoscopy has been used exclusively to diagnosevarices Non-invasive methods of screening for varices includecapsule endoscopy transient elastography and use of laboratoryand radiological findings
EndoscopyThere is universal acceptance that endoscopy is the lsquogold stand-ardrsquo for diagnosing gastro-oesophageal varices The main limita-tions are intraobserver variability in the diagnosis of small orgrade I oesophageal varices (figure 1AndashC) Recently unsedatednasal gastroscopy has been found to have similar accuracy toconventional endoscopy and has the advantage of tolerabilityand potential cost saving since it can be performed in the clinicsetting in some institutions28 29 However there are no con-trolled studies and banding of varices is not possible
Capsule endoscopyCapsule endoscopy uses a 26 mm pill-shaped device whichtransmits video footage which is stored and later analysedPatients are not sedated but patient cooperation is essentialIn a large study by de Franchis et al30 capsule endoscopy wascompared with standard gastroscopy The primary end point of90 or greater concordance was not achieved Lapalus et al31
in a prospective study of 120 patients demonstrated similarresults with capsule endoscopy Therefore capsule endoscopycannot be considered an alternative to standard endoscopyalthough may have a role in patient who refuse gastroscopy
Transient elastographyTransient elastography ((FibroScan Echosens Paris France) usesthe principles of ultrasound to derive tissue stiffness by measur-ing the speed of propagation of a low-frequency wave whichthen correlates with liver fibrosis Vizzutti et al32 in a study of61 patients with hepatitis C showed a sensitivity for predictionof oesophageal varices of 90 using a threshold 176 kPaHowever specificity was poor at 43 A study of 298 patientsfound the optimal cut-off point for the prediction of oesopha-geal varices was 215 kPa (sensitivity 76 and specificity78)33 In one uncontrolled study the use of transient elasto-graphy was found to be as effective as HVPG at predictingportal hypertension-related complications34 Therefore the roleof transient elastography in predicting varices is controversialdue to the lack of consistent results and controlled studies Thismodality may be more useful for predicting decompensation inpatients with cirrhosis
Radiological and serum parametersA prospective study of 311 patients with chronic hepatitis Cshowed that a platelet-to-spleen size ratio with a threshold of909 had positive and negative predictive values of 100 and94 respectively35 These good results have not been repro-duced by others as demonstrated in a meta-analysis36
Risk factors for first variceal bleedingThe factors that predispose to and precipitate variceal haemor-rhage are still not clear The suggestion that oesophagitis mayprecipitate variceal haemorrhage has been discarded37
Presently the most important factors that have been heldresponsible include (i) pressure within the varix (ii) varicealsize (iii) tension on the variceal wall and (iv) severity of theliver disease
Portal pressureIn most cases portal pressure reflects intravariceal pressure38
and a HVPG gt10 mm Hg is necessary for the development ofoesophageal varices27 There is no linear relationship betweenthe severity of portal hypertension and the risk of varicealhaemorrhage although HVPG gt12 mm Hg is an accepted
Figure 1 (A) Grade I oesophagealvarices These collapse to inflation ofthe oesophagus with air (B) Grade IIoesophageal varices These are varicesbetween grades 1 and 3 (C) Grade IIIoesophageal varices These are largeenough to occlude the lumen
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 7
Guidelines
threshold for variceal bleeding39 40 However the HVPG tendsto be higher in bleeders as well as in patients with larger varicesIn a prospective study comparing propranolol with placebo forthe prevention of first variceal haemorrhage Groszmann et al41
showed that bleeding from varices did not occur if the portalpressure gradient (PPG) could be reduced to lt12 mm HgOthers have shown that a 20 reduction in portal pressure pro-tects against further bleeding42 These haemodynamic goalshave been accepted as the aim of pharmacological treatment ofportal hypertension It is important to appreciate that gastricvarices can bleed at pressures lt12 mm Hg and the influence ofwall tension of the varix plays a greater role in the risk of bleed-ing43 A greater pressure reduction may be necessary to protectagainst bleeding This is further discussed in the section lsquoGastricvaricesrsquo At present measurement of portal pressure in guidingpharmacological treatments is limited to clinical trials in the UK
Variceal sizeVariceal size is best assessed endoscopically (figure 1AndashC)Published results are variable owing to the lack of a definition dis-tinguishing between large and small varices Small (grade I)varices tend to be narrow and flatten easily with air whereaslarger (grade 2 and 3) varices are usually broader and flatten withdifficulty if at all Numerous studies40 44 have shown that therisk of variceal haemorrhage increases with the size of varices45
Variceal wall and tensionPolio and Groszmann46 using an in vitro model showed thatrupture of varices was related to the tension on the varicealwall The tension depends on the radius of the varix In thismodel increasing the size of the varix and decreasing the thick-ness of the variceal wall caused variceal rupture Recently endo-scopic ultrasound and manometry have been used to estimatewall tension of varices47
Endoscopic features such as lsquored spotsrsquo and lsquowhalersquo markingswere first described by Dagradi24 They have been described asbeing important in the prediction of variceal haemorrhageThese features represent changes in variceal wall structure andtension associated with the development of microtelangiectasiasand reduced wall thickness In a retrospective study by theJapanese Research Society for Portal Hypertension Beppuet al48 showed that 80 of patients who had blue varices orcherry red spots bled from varices suggesting that this was animportant predictor of variceal haemorrhage in cirrhosis
Severity of liver disease and bleeding indicesTwo independent groups prospectively assessed factors predict-ing first variceal haemorrhage in cirrhosis (table 2) The NorthItalian Endoscopic Club (NIEC)49 reported their findings in1988 followed in 1990 by data from the Japanese50 Both thesestudies showed that the risk of bleeding was based on threefactors severity of liver disease as measured by Child class vari-ceal size and red wale markings The NIEC study showed awide range for the risk of bleeding of 6ndash76 depending on thepresence or absence of the different factors Using the same vari-ables the NIEC index was simplified by de Franchis et al51 andshown to correlate with the original index Further studiesshowed that the HVPG and intravariceal pressure were alsoindependent predictors of first variceal haemorrhage when ana-lysed in conjunction with the NIEC index52 53
In summary the most important factors that determine the risk ofvariceal haemorrhage are the severity of liver disease size of varicesand presence of red signs Measurement of HVPG is a useful guidefor selection of patients for treatment and their response to
treatment although the predictive value does not appear toimprove on the NIEC index and presence of red whale marking54
Risk and mortality of first variceal bleedData describing the overall risk of bleeding from varices must beviewed with caution and have some pitfalls in interpretationThe natural history of patients who have varices that are diag-nosed as part of their baseline investiations is different fromthat of patients who have complications of liver disease such asascites and encephalopathy Most studies do not comment oneither the severity of liver disease or whether patients with alco-holic cirrhosis are continuing to drink Both these factors have asignificant effect on the risk of variceal haemorrhage
Most studies report bleeding from varices in about 20ndash50of patients with cirrhosis during the period of follow-up Bakeret al23 reported variceal bleeding in 33 of 115 patients that theyfollowed up for a mean of 33 years with a mortality of 48from the first variceal haemorrhage These data were confirmedby Christensen et al18 About 70 of the episodes of bleedingoccur within 2 years of diagnosis Recent studies demonstrate adramatic reduction in mortality following variceal bleeding of20 6-week mortality55 and 15 in-hospital mortality5 withcontributions from improved endoscopic pharmacological andradiological therapies notably TIPSS Intensive care treatmenthas also improved with outcomes being particularly good forthose requiring minimal organ support
Analysis of the non-active treatment arms in the primaryprophylaxis trials comparing propranolol with placebo showresults similar to those of the primary prophylaxis shunt trialswith most episodes of bleeding occurring within the first 2 yearsof follow-up In these studies the rate of first variceal haemor-rhage ranged from 22 to 6156ndash60 This large difference inthe rate of first bleed relates almost certainly to the number ofpatients with severe liver disease included in the study (PascalChild Cmdash46 bleedingmdash61 Italian Multicenter Project forPropranolol in Prevention of Bleeding (IMPP) Child Cmdash6bleedingmdash32 Conn Child Cmdash6 bleedingmdash22)Mortality varied from 24 to 49 over 2 years (Pascal mortal-itymdash49 IMPP mortalitymdash24 Conn mortalitymdash24)
Primary prophylaxisSince 30ndash50 of patients with portal hypertension will bleedfrom varices and about 20 will die from the effects of the first
Table 2 Scoring systems for quantifying the severity of cirrhosisSeverity of liver disease can be described using the ChildndashPughscore or MELD scoreThe ChildndashPugh score is the sum of severity scores for Child classvariceal size and red wale markings the variables shown below
Category 1 2 3
Encephalopathy 0 III IIIIVAscites Absent Mild-moderate SevereBilirubin (μmolL) lt34 34ndash51 gt51Albumin (gL) gt35 28ndash35 lt28INR lt13 13ndash15 gt15
ChildndashPugh class A represents a score of le6 class B a score of 7ndash9 and class C ge10The MELD score is a formula that includes three laboratory-based variables reflectingthe severity of liver disease It was originally used to predict the short-term mortalityafter placement of a transjugular intrahepatic portosystemic stent-shunt for varicealbleeding Subsequently it has been used in selecting candidates for livertransplantationMELD score please use the online calculator httpswwwesotorgElitameldCalculatoraspxINR international normalised ratio
8 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleed it seems rational to develop prophylactic regimens toprevent the development of and bleeding from these varicesHowever most of the published trials do not have sufficientpower to identify favourable treatment effects Based on theexpected bleeding and death rates in the control group theminimum number of patients needed to detect a 50 reductionin bleeding would be 270 and 850 patients in each arm todetect the same reduction in mortality A proposed algorithmfor surveillance and prophylaxis of varices is shown in figure 2At this time there is insufficient evidence to support treatingpatients without varices or lsquopre-primary prophylaxisrsquo A largerandomised placebo-controlled trial of timolol in patientswithout varices and portal hypertension defined as HVPGgt6 mm Hg did not show any effect on the development ofvarices or variceal bleeding27 The role of drug treatment in pre-venting bleeding in patients with small varices is unclear Threerandomised placebo-controlled trials have studied this Caleset al61 showed that propranolol in patients with small or novarices resulted in greater development of varices Howeverpatients without varices were included and there was significantloss of patients to follow-up The second trial showed thatnadolol reduced variceal bleeding without survival benefit andincreased adverse events62 Sarin et al63 did not show any effectwith propranolol despite a significant effect on portal pressure
SurgeryPortacaval shuntsFour trials of portacaval shunts have been published which ran-domised a total of 302 patients64ndash67 either to prophylactic shuntsurgery or to non-active treatment A meta-analysis of thesestudies showed a significant benefit in the reduction of varicealbleeding (OR=031 95 CI 017 to 056) but also a signifi-cantly greater risk of hepatic encephalopathy (OR=2 95 CI12 to 31) and mortality (OR=16 95 CI 102 to 257) inpatients treated with shunt surgery68 At this time there is noevidence for the use of TIPSS for primary prophylaxis1
Devascularisation proceduresInokuchi50 showed that there was a significant reduction in vari-ceal bleeding and in mortality in patients treated with a varietyof devascularisation procedures There are however numerousproblems with the interpretation of this study because of theuse of different procedures in each of the 22 centres Theseresults require confirmation
Pharmacological treatmentNon-cardioselective β blockersThe mainstay of the pharmacological approach to the primaryprophylaxis of variceal haemorrhage has been NSBBPropranolol which has been shown to reduce the PPG reduceazygos blood flow and also variceal pressure It achieves this bycausing splanchnic vasoconstriction and reducing cardiacoutput There is no clear dose-related reduction in HVPG orcorrelation of HPVG reduction with reduction in heart rate69
Observational studies have shown that a 10ndash12 reduction inHVPG after acute administration of propranolol was associatedwith reduced bleeding and hepatic decompensation54 70
However HVPG monitoring is not routinely available in mostcentres outside of larger institutions A meta-analysis of nineplacebo-controlled randomised trials (964 patients) showed thatthe pooled risk difference for bleeding was minus11 (95 CIminus21 to minus1) and for death was minus9 (95 CI minus18 tominus1) in favour of propranolol71
Nadolol exerts similar effects on portal haemodynamicsalthough the effect on blood pressure may not be as pro-nounced Two placebo-controlled trials58 59 have shownreduced bleeding although in one study this was only seen onper protocol analysis59 There was no effect on overall survival
Carvedilol is a NSBB like propranolol and a vasodilator dueto α1 receptor blockade The latter reduces portocollateralresistance and by actions on hepatic stellate cells leads to areduction in intrahepatic resistance Haemodynamic studiesdemonstrate a greater reduction in portal pressure with
Figure 2 Algorithm for surveillance of varices and primary prophylaxis in cirrhosisndash If there is clear evidence of disease progression this interval can be modified by clinician Endoscopy should also be offered at time ofdecompensation
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 9
Guidelines
carvedilol than with propranolol although blood pressure isreduced72 73 The optimum dose is 625ndash125 mgday74 Higherdoses are not more effective and are associated with moreadverse eventsmdashin particular hypotension Carvedilol at a doseof 125 mgday at current UK prices is considerably cheaperthan propranolol 40 mg twice a day and nadolol 80 mgday(monthly cost pound120 pound562 and pound5 respectively) Two RCTs ofcarvedilol versus variceal band ligation (VBL) in primaryprophylaxis have been published75 76 The first study75 showedsignificantly reduced bleeding in the carvedilol arm (10 vs23 relative hazard 041 95 CI 019 to 096) with no effecton survival The second trial by Shah et al76 did not show anydifferences in bleeding or mortality Compliance with VBL wasbetter in the latter trial and unlike the first trial there were sig-nificantly more patients with viral hepatitis than alcoholic cir-rhosis A further study74 assessed the effect of carvedilol inpatients who were haemodynamic non-responders to propran-olol where haemodynamic response was defined as HVPGreduction to le12 mm Hg or by gt20 of baseline after 4 weeksof treatment Patients who were haemodynamic non-respondersor intolerant to carvedilol were treated with VBL Carvedilolresulted in significantly lower variceal bleeding compared withVBL and haemodynamic responders to carvedilol or propran-olol had significantly lower mortality than those treated withVBL It is worth noting that the study was not randomised
There have been recent suggestions based on low-level evi-dence that NSBB may result in a poorer outcome in patientswith cirrhosis and refractory ascites77 The lsquowindow hypothesisrsquofor β blockers in cirrhosis has also recently been described sug-gesting that NSBB are helpful in the compensated and earlydecompensated cirrhotic period but may not be helpful in veryearly cirrhosis such as in a patient with no varices and may beharmful in patients with end-stage cirrhosis with refractoryascites78 However recent large observational studies questionthe last hypothesis with improved survival seen in patients withrefractory ascites treated with NSBB79 unless patients have anepisode of spontaneous bacterial peritonitis80 Therefore untilthere are further prospective controlled studies NSBB should becontinued in patients with refractory ascites The clinician mustcarefully monitor haemodynamic parameters such as blood pres-sure and discontinue NSBB in patients with hypotension andrenal impairment as can occur after an episode of spontaneousbacterial peritonitis Other potentially severe adverse eventswith NSBB include symptomatic bradycardia asthma andcardiac failure Less severe side effects such as fatigue insomniaand sexual dysfunction may also result
Isosorbide mononitrateInterest in the use of vasodilators such as isosorbide mononitrate(ISMN) developed after the demonstration that it reduces portalpressure as effectively as propranolol81 but has subsequentlywaned A trial comparing ISMN with propranolol showed nosignificant difference between these agents82 Another rando-mised trial of ISMN versus placebo did show any difference inthe two arms83 Therefore ISMN is not recommended asmonotherapy in primary prophylaxis
β Blocker and ISMNThe combination of nadolol and ISMN has been compared withnadolol in a RCT The combination therapy reduced the fre-quency of bleeding significantly but no significant differenceswere detected in mortality84 However Garcia-Pagan et al85 in adouble-blind RCTof propranolol plus ISMN versus propranolol
plus placebo failed to show any differences between the twoarms Combination therapy is associated with more side effects
Proton pump inhibitorsA placebo-controlled randomised trial reported reduced bleed-ing and mortality with rabeprazole after eradication of varices86
However the study had a heterogeneous population with VBLperformed for both primary and secondary prophylaxis andsmall numbers (n=43) limiting the validity of the conclusionsFurthermore there was no arm comparing proton pump inhibi-tors with NSBB The use of proton pump inhibitors in patientswith cirrhosis and ascites was associated with increased risk ofspontaneous bacterial peritonitis in a large retrospective study87
This was not confirmed in a larger prospective non-randomisedstudy88 However a recent prospective observational study hasshown proton pump use to be associated with increased mortal-ity in cirrhosis89 Proton pump inhibitors are also associatedwith increased risk of Clostridium difficile infection90 Thereremains continuing concern about proton pump inhibitors inpatients with cirrhosis therefore caution should be used
Endoscopic therapyVariceal band ligationVBL has been compared with NSBB in 19 trials in a recentCochrane meta-analysis of 1504 patients91 Despite reducedbleeding (RR=067 95 CI 046 to 098) with VBL there wasno difference in overall mortality and bleeding-related mortalityThe difference in bleeding was not seen when only trials withlow selection or attrition bias were included Banding can haveserious complications The risk of fatal banding-induced bleed-ing was highlighted in a meta-analysis showing reduced fataladverse events with NSBB (OR=014 95 002 to 099)92
The optimal timing of banding intervals is discussed in thesection lsquoSecondary prophylaxis of variceal haemorrhagersquo A ran-domised trial of 96 patients who underwent endoscopic surveil-lance at 6 or 3 months after eradication of varices with VBL didnot demonstrate a difference in bleeding on mortality93
However the trial had a heterogeneous study group of patientswho underwent VBL both for primary (65) and secondaryprevention (35)
SclerotherapyNineteen trials have compared endoscopic variceal sclerotherapywith no treatment68 Owing to the marked heterogeneitybetween these studies a meta-analysis is clinically inappropri-ate68 Sclerotherapy does not offer any benefit in combinationwith NSBB or VBL compared with VBL or NSBB alone andincreases iatrogenic complications such as strictures94ndash96 At thistime sclerotherapy cannot be recommended for prophylaxis ofvariceal haemorrhage in patients with cirrhosis
Recommendations primary prophylaxis of variceal haemor-rhage in cirrhosis (figure 2)1 What is the best method for primary prophylaxis
11 We recommend NSBB or variceal band ligation (VBL)We suggest pharmacological treatment with propranololas first line VBL is offered if there are contraindicationsto NSBB The choice of VBL or NSBB should also takeinto account patient choice (level 1a grade A)
12 We suggest carvedilol or nadolol as alternatives to pro-pranolol (level 1b grade A)
13 Dose131 Propranolol 40 mg twice daily Dose titrated to
maximum tolerated or once heart rate (HR) of
10 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
50ndash55 bpm is reached to a maximum dose of320 mg (level 1a grade A)
132 Nadolol 40 mg daily dose Dose titrated tomaximum tolerated or once HR of 50ndash55 bpm isreached a maximum dose of 240 mg (level 1agrade A)
133 Carvedilol 625 mg once daily to increase tomaintenance of 125 mg after a week if toleratedor once HR of lt50ndash55 bpm is reached (level 1agrade A)
134 It is suggested that NSBB are discontinued at thetime of spontaneous bacterial peritonitis renalimpairment and hypotension (level 2b grade B)
14 In cases of contraindications or intolerance to NSBB werecommend variceal band ligation (level 1a grade A)
2 Who should have surveillance for variceal bleeding21 We recommend all patients with cirrhosis should be
endoscoped at the time of diagnosis (level 1a grade A)There is no indication to repeat endoscopy in patientsreceiving NSBB
3 How often should cirrhotic patients be endoscoped31 If at the time of first endoscopy no varices are seen we
suggest that patients with cirrhosis should be endos-coped at 2ndash3-year intervals (level 2a grade B)
32 If grade I varices are diagnosed we suggest that patientsshould be endoscoped at yearly intervals (level 2agrade B)
33 If there is clear evidence of disease progression wesuggest that the intervals can be modified by a clinicianEndoscopy should also be offered at time of decompen-sation (level 2a grade B)
4 Which patients with cirrhosis should have primaryprophylaxis41 If grade I varices and red signs or grade 2ndash3 varices are
diagnosed we recommend that patients have primaryprophylaxis irrespective of the severity of the liverdisease (level 1a grade A)
5 Treatments not recommended51 Proton pump inhibitors are not recommended unless
otherwise required for peptic ulcer disease (level 1bgrade B)
52 Isosorbide mononitrate monotherapy is not recommendedas primary prophylaxis (level 1b grade A) There is insuffi-cient evidence to recommend isosorbide mononitrate incombination with NSBB (level 1b grade A)
53 Shunt surgery or TIPSS is not recommended as primaryprophylaxis (level 1a grade A)
54 Sclerotherapy is not recommended as primary prophy-laxis (level 1a grade A)
6 Areas requiring further study61 Role of NSBB in patients without varices with focus on
carvedilol62 Role of NSBB in patients with small varices with focus
on carvedilol63 Comparison of carvedilol versus propranolol in primary
prophylaxis64 Identification of and trials assessing new drugs for
primary prophylaxis such as statins7 Quality indicator
71 Percentage of patients at diagnosis of cirrhosis who havehad an endoscopy to screen for varices (level 1agrade A)Numerator patients diagnosed with cirrhosis who havehad an endoscopy either before or after diagnosis within
6 monthsDenominator patients newly diagnosed with cirrhosis
72 Percentage of patients receiving primary prophylaxisamong those newly diagnosed with grade I varices andred signs or grade 2ndash3 varicesNumerator patients who have grade 1 varices with redsigns or grade 2ndash3 varices receiving primary prophy-laxisDenominator patients diagnosed with cirrhosis whohave grade I varices with red signs or grade 2ndash3 varices
MANAGEMENT OF ACTIVE VARICEAL HAEMORRHAGEThe average 6-week mortality of the first episode of varicealbleeding in most studies is reported to be up to 20 There hasbeen considerable improvement in survival since the early 1980swhen the in-hospital mortality was 40ndash5097 compared with15 from a recent UK audit5 Such is the improvement in out-comes that a patient with Childrsquos A cirrhosis is very unlikely tosuccumb to an index variceal bleed Studies have shown theChildndashPugh score MELD score and HVPG to be strong predic-tors of outcomes98ndash103 The MELD score has been shown tooutperform Childrsquos score in a recent study with a score gt19associated with 20 6 week mortality103 Furthermore theMELD score has been shown to perform as well as the trad-itional intensive care unit scores in predicting mortality inpatients admitted to intensive care in the UK104 MELD gt18active bleeding transfusing gt4 units of packed red blood cellshave been shown to be predictors of mortality and earlyrebleeding99 101 102 HVPG has also been shown to predictoutcome when measured at 2 weeks after a bleed44 and a valueof ge20 mm Hg when measured acutely within 48 h has beenshown to provide significant prognostic information100
However this technique is not used routinely in the manage-ment of patients around the world and substitution of clinicaldata in the latter study was shown to provide the same clinicalpredictive value100 These scoring systems are not purely aca-demic they allow the referring clinician to predict thosepatients with a high chance of rebleeding to be transferred to aspecialist centre offering for instance TIPSS before the patientrebleeds
Nonetheless probably the most important step in the man-agement of acute variceal haemorrhage is the initial resuscitationassessed according to standard lsquoABCrsquo practice together withprotection of the airway to prevent aspiration Although earlyendoscopy allows for accurate diagnosis of the bleeding site anddecisions about management (figure 3) therapeutic interventionin acute variceal bleeding can be initiated safely in most casesbefore diagnostic endoscopy As similar efficacy is demonstratedwith pharmacological treatment as with sclerotherapy theformer should be first-line therapy99 β Blockade should not bestarted in the acute setting and those already taking β blockersas prophylaxis should probably stop taking them for 48ndash72 h inorder that the patientrsquos physiological response to blood loss canbe allowed to manifest
General considerationsPatient evaluationThe majority of patients with a variceal bleed will be sufficientlystable to enable a full history and examination to take placeHistory of alcohol excess and or intravenous drug use should besought and may become particularly relevant if the patient haswithdrawal symptoms after admission Comorbidity is importantwhen estimating risk and deciding on use of vasopressors The
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 11
Guidelines
following risk factors doubled mortality after an acute varicealbleed in one US study older age comorbidities male gender andnot undergoing a gastroscopy within 24 h105
A full examination is helpful for the important negatives asmuch as the positives Baseline observations should include thetemperature as infection is a serious complication with signifi-cant mortality Confusion may be present because of encephal-opathy intoxication with alcohol or drugs or withdrawal fromalcohol or drugs The patient should be on continuous BP andpulse monitor and their haemodynamic status recordedAn oxygen saturation monitor is helpful Stigmata of chronicliver disease and concurrent jaundice provide insight into thecurrent status of a patientrsquos liver and also give warning ofpotential further decompensation if significant bleeding persists(see scoring systems above) Pneumonia must be actively
excluded Evidence of ascites requires a diagnostic tap to searchfor infection
Investigations including full blood count coagulationprofile liver and renal function and blood group and save andcross-match Blood and urine should also be cultured An ultra-sound scan later in the admission is helpful to identify subclin-ical ascites flow in portal vein and any obvious emergence of anhepatocellular carcinoma (HCC)
Location of patientA decision must be made as to where the patient is best managedVariceal bleeding is unpredictable generally occurs in patientswith significant liver disease and is associated with significant mor-tality Hence a high-dependency unit is usually the most appropri-ate initial location although a properly staffed lsquogastrointestinal
Figure 3 Algorithm for themanagement of acute varicealbleeding TIPSS transjugularintrahepatic portosystemic stent shunt
12 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleeding bedrsquo may be appropriate If a patient is vomiting bloodor there is a perceived risk of a haemodynamically unstable patienthaving blood in the stomach then the patient must be intubatedbefore endoscopy and return to an intensive care or high-dependency unit will be necessary until extubation
Volume resuscitation and blood productsIntravenous access (two 16ndash18G cannulae) should have beensecured on admission with a reported GI bleed Further intra-venous access may be necessary In patients with poor venousaccess advanced liver disease or renal failure associated withtheir liver disease central venous access may be helpful withguiding fluid infusions However the drawbacks include the riskof the procedure and a potential source of infection Thereforethere is no absolute requirement for a central line and no evi-dence of unequivocal benefit Intravenous fluid resuscitationshould be initiated with plasma expanders aiming to maintain asystolic blood pressure of 100 mm Hg Care with monitoring isparamount in this group of patients
Overtransfusion has been shown to have a deleterious effecton outcome In a recent single-centre RCT a restrictive transfu-sion policy of maintaining haemoglobin between 70 and 80 gLimproved the control of variceal bleeding (11 vs 22p=005) and lowered HVPG compared with a liberal transfu-sion policy without effect on 45-day survival106 However itshould be noted that these results were from a single Spanishcentre which was a tertiary unit for variceal bleeding where allpatients underwent endoscopy within 6 h Nonetheless arestrictive transfusion policy has been recommended for sometime1 and there is now good evidence to support not transfusinga stable patient with a haemoglobin of ge80 gL However under-resuscitation should also be avoided and while goal-orientedfluid replacement has generally not been useful in an intensivetherapy unit setting a venous saturation gt70 remains an easilymeasurable target with some evidence to support it107
Interpretation and management of clotting profile is challen-ging in liver disease where there is usually a balanced deficiencyof both procoagulant and anticoagulant factors108 The NICEguidelines recommend activation of a hospitalrsquos massive transfu-sion policy when there is major haemorrhage and plateletsupport when the value is lt50 and clotting factor supportwhen the international normalised ratio (INR) is gt15 timesnormal2 There is no evidence for the use of lsquoprophylacticrsquo clot-ting or platelet support to reduce the risk of rebleeding Thereis insufficient evidence to support the routine use of transexamicacid or recombinant factor VIIa109
Pharmacological treatmentThe two major classes of drugs that have been used in thecontrol of acute variceal bleeding are vasopressin or its analo-gues (either alone or in combination with nitroglycerine) andsomatostatin or its analogues Terlipressin is the only agent thathas been shown to reduce mortality in placebo-controlled trialsHowever in trials comparing terlipressin somatostatin andoctreotide no difference in efficacy was identified in a system-atic review110 and in a recent large RCT111 Prophylactic anti-biotics can result in a similar survival benefit following acutevariceal bleeding
VasopressinVasopressin reduces portal blood flow portal systemic collateralblood flow and variceal pressure It does however have signifi-cant systemic side effects such as an increase in peripheral resist-ance and reduction in cardiac output heart rate and coronary
blood flow In comparison with no active treatment the pooledresults of four randomised trials showed that it reduced failureto control variceal bleeding (OR=022 95 CI 012 to 043)although survival was unaffected68 Meta-analysis of five trialscomparing sclerotherapy with vasopressin has shown a signifi-cant effect on reduction in failure to control bleeding(OR=051 95 CI 027 to 097) with no effect on survival68
Vasopressin with nitroglycerineThe addition of nitroglycerine enhances the effect of vasopres-sin on portal pressure and reduces cardiovascular side effects112
Meta-analysis of three randomised trials comparing vasopressinalone with vasopressin and nitroglycerine showed that the com-bination was associated with a significant reduction in failure tocontrol bleeding (OR=039 95 CI 022 to 072) although nosurvival benefit was shown68
TerlipressinTerlipressin is a synthetic analogue of vasopressin which has animmediate systemic vasoconstrictor action followed by portalhaemodynamic effects due to slow conversion to vasopressin Ina Cochrane meta-analysis of seven placebo-controlled trials ter-lipressin was shown to reduce failure to control bleeding(RR=066 95 CI 055 to 093) and also to improve survival(RR=066 95 CI 049 to 088)113 In the same meta-analysisthere was no difference between terlipressin versus vasopressinballoon tamponade or endoscopic therapy in failure to controlbleeding or survival113 The role of terlipressin in combinationwith VBL is explored in the section lsquoEndoscopic therapy incombination with pharmacological therapyrsquo
The recommended dose of terlipressin is 2 mg IV every 4 halthough many units reduce the dose to 6 hourly as it may causeperipheral vasoconstriction which manifests as painful handsand feet While 5 days of IV treatment has been advocated inthe Baveno V guidelines1 this prolonged treatment has notbeen shown to have a survival benefit and for pragmaticreasons many units will stop treatment shortly after satisfactoryhaemostasis In a randomised trial terlipressin given for 24 hafter satisfactory haemostasis with VBL after oesophageal vari-ceal bleeding was as effective as 72 h of treatment114
In patients intolerant of terlipressin or in countries where ter-lipressin is not available alternatives should be considered
Somatostatin and octreotideSomatostatin causes selective splanchnic vasoconstriction andreduces portal pressure and portal blood flow115 Octreotide is asomatostatin analogue The mechanism of action of these twoagents is not clear Inhibition of glucagon increases vasodilatationrather than a direct vasoconstrictive effect and post-prandial guthyperaemia is also reduced The actions of octreotide on hepaticand systemic hemodynamics are transient making continuousinfusion necessary Octreotide is given as a 50 μg bolus followedby an infusion of 25ndash50 μgh Somatostatin is given as a 250 mgintravenous bolus followed by an infusion of 250 mghSomatostatin and octreotide have been shown to be aseffective as terlipressin in acute variceal bleeding in ameta-analysis110 Seo et al111 in a large RCTof 780 patients com-paring these three agents failed to show a difference in treatmentsuccess (range 838ndash862) rebleeding (range 34ndash44) andmortality (range 8ndash88) A low systolic blood pressure at pres-entation high serum creatinine level active bleeding in the emer-gency endoscopy gastric variceal bleeding and ChildndashPugh gradeC were independent factors predicting 5-day treatmentfailure111
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 13
Guidelines
AntibioticsAntibiotics that provide Gram-negative cover are one of the inter-ventions which positively influence survival in variceal haemor-rhage as shown in a Cochrane meta-analysis of 12placebo-controlled trials (RR=079 95 CI 063 to 098)116
Antibiotics were also shown to reduce bacterial infections(RR=043 95 CI 019 to 097) and early rebleeding (RR=05395 CI 038 to 074)116 Therefore short-term antibiotics shouldbe considered standard practice in all cirrhotic patients who have avariceal bleed irrespective of the presence of confirmed infectionThird-generation cephalosporins such as ceftriaxone (1 g IVdaily) have been shown to be more effective at reducingGram-negative sepsis than oral norfloxacin117 but choice of anti-biotics must be dictated by local resistance patterns and availability
Proton pump inhibitorsOne RCT compared a short course of proton pump inhibitorswith vasoconstrictor therapies after haemostasis in acute varicealbleeding118 Despite larger ulcers noted in the vasoconstrictorarm there were no differences in bleeding or survival Nearly50 of patients had ascites which might have implications inlight of the reports of increased incidence of spontaneous bac-terial peritonitis as mentioned earlier
Endoscopic therapyEndoscopy should take place within 24 h of admission andearlier if there is excessive bleeding based on low-level evi-dence105 While many guidelines and reviews suggest thatendoscopy should be carried out within 12 h the only study thatexamined the influence of timing on outcome failed to demon-strate any advantage of endoscopy before 12 h119 The optimaltime is after sufficient resuscitation and pharmacological treat-ment with the endoscopy performed by a skilled endoscopyteam in a suitably equipped theatre environment and withairway protection Airway protection is essential where risk ofaspiration is high and affords the endoscopist time for thoroughevaluation including complete clot aspiration and controlledapplication of treatment including tamponade if required Theendoscopy team must comprise an experienced endoscopynurse acquainted with the equipment necessary for endoscopytherapy of varices and a skilled endoscopist competent in usingbanding devices and deployment of balloon tamponade
Variceal band ligationThis technique is a modification of that used for the elastic bandligation of internal haemorrhoids Its use in humans was firstdescribed in 1988120 A meta-analysis of seven trials comparingVBL with sclerotherapy in acute bleeding showed that VBLreduced rebleeding from varices (OR=047 95 CI 029 to078) reduced mortality (OR=067 95 CI 046 to 098) andresulted in fewer oesophageal strictures (OR=010 95 CI003 to 029)121 The number of sessions required to obliteratevarices was lower with VBL (22 fewer sessions (95 CI 09to 35))
SclerotherapySclerotherapy has been replaced by VBL and should no longerbe offered as standard of care in acute variceal haemorrhage
Other endoscopic measuresIn an RCT cyanoacrylate offered no benefit over VBL with theadditional risk of embolisation and trend towards increasedrebleeding with cyanoacrylate122
Haemostatic powder (TC-325 Hemospray Cook MedicalUSA) has been described in a small study of nine patients whoreceived endoscopic spray treatment for acute variceal bleedingThe study reported no rebleeding within 24 h and no mortalityat 15 days123
Endoscopic therapy in combination with pharmacological therapyThe role of combining vasoactive drugs with endoscopictherapy (VBL or sclerotherapy) was reported in a meta-analysisof eight trials124 Combination therapy resulted in better initialcontrol of bleeding (RR=112 95 CI 102 to 123) and5-day haemostasis (RR=128 95 CI 118 to 139) withoutany difference in survival Adverse events were similar in bothgroups Two RCTs have compared VBL with sclerotherapy incombination with vasoactive agents in acute variceal bleed-ing125 126 Lo et al125 used vasopressin and found that VBLresulted in better 72 h haemostasis (97 vs 76 p=0009)with fewer complications (5 vs 29 p=0007) Villanuevaet al used somatostatin and reported lower failure to controlacute bleeding with VBL (4 vs 15 p=002) with fewerserious complications (4 vs 13 p=004) Overall survivalwas similar in both trials125 126
Balloon tamponadeBalloon tamponade is highly effective and controls acute bleed-ing in up to 90 of patients although about 50 rebleed whenthe balloon is deflated127 128 It is however associated withserious complications such as oesophageal ulceration and aspir-ation pneumonia in up to 15ndash20 of patients Despite this itmay be a life-saving treatment in cases of massive uncontrolledvariceal haemorrhage pending other forms of treatment Anappropriately placed SengstakenndashBlakemore tube allows forresuscitation safe transportation and either repeat endoscopy orradiological shunting in a patient with a stable cardiovascularsystem The oesophageal balloon is rarely required must neverbe used on its own and should be used only if there is continu-ing bleeding despite an adequately inflated gastric balloon cor-rectly placed and with appropriate tension Placement of thetube endoscopically or over a guide wire might reduce the riskof complications especially oesophageal rupture
Removable oesophageal stentsThe SX-Ella Danis stent (ELLA-CS Hradec Kralove CzechRepublic) is a removable covered metal mesh stent placed endo-scopically in the lower oesophagus without radiological screen-ing It has no role in the management of gastric varicealbleeding These stents can be left in situ for up to 2 weeksunlike the SengstakenndashBlakemore tube which should beremoved after a maximum of 24ndash48 h129 130 No published con-trolled trials have compared this modality with balloontamponade
Transjugular intrahepatic portosystemic stent-shuntSeveral uncontrolled studies have examined the role of salvagebare TIPSS in acute variceal bleeding In a review of 15 studiescontrol of bleeding was achieved in 90ndash100 with rebleedingin 6ndash16131 Mortality varied between 75 (in hospital) and15 (30 day) It is important to appreciate that sclerotherapywas used as first-line endoscopic therapy in most of thesestudies Long-term follow-up of a study that compared TIPSSwith H-graft portacaval shunts in patients for whom non-operative management had failed suggested that H-grafts were auseful method of reducing portal pressure and had a signifi-cantly lower failure rate (p=004) but had no significant
14 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
improvement in overall survival despite a benefit seen in ChildrsquosA and B disease132 A recent RCT compared emergency porto-caval surgery with bare TIPSS within 24 h of presenting withacute oesophageal variceal bleeding in unselected cirrhoticpatients Emergency portocaval surgery resulted in better out-comes for long-term bleeding control encephalopathy and sur-vival (plt0001)133 Before wider application of surgery foracute variceal bleeding more data are needed in light of therecent adoption of covered stents
There has also been a generalised established change in prac-tice in using covered TIPSS stents (polytetrafluoroethylene(PTFE)) rather than a bare metal stent with evidence to supportthis change In randomised controlled studies these stents wereshown to have higher primary patency rates than bare stentswithout significant differences in survival and the potential forreduced incidence of hepatic encephalopathy134 135
There is however growing evidence from two RCTs for theearlier use of TIPSS in selected patients stratified by HVPGChildndashPugh class and active bleeding and not just use as asalvage option6 136 Monescillo et al136 randomised patientspresenting with acute oesophageal variceal haemorrhage to bareTIPSS or standard of care if the HVPG was ge20 mm Hg within24 h of admission Significantly reduced treatment failure asdefined by failure to control acute bleeding andor early rebleed-ing (12 vs 50) was seen and improved survival (62 vs35) in the patients randomised to undergo a TIPSS procedureHowever the standard of care was sclerotherapy and not com-bination endoscopic and pharmacological treatment This limita-tion and the lack of availability of HVPG measurement in mostcentres meant this trial did not have a significant impact on clin-ical practice
Garcia-Pagan et al6 selected patients with active bleeding andChildrsquos B cirrhosis or patients with Childrsquos C cirrhosis (Childrsquosscore lt14) for randomisation to early PTFE-covered TIPSSwithin 72 h or standard of care with VBL and pharmacologicaltreatment This has shown encouraging results with reduced riskof treatment failure (3 vs 50) improved survival (86 vs61 at 1 year) yet without increased risk of hepatic encephal-opathy The results were supported by an observational studyfrom the same group although a survival benefit was notseen137 Furthermore a recent well-conducted observationalstudy did not demonstrate such high survival rates with earlyTIPSS with 11-year survival of 67 which was similar to thatof patients given endoscopic and pharmacological treatmentsonly138 Therefore larger multicentred RCTs need to be under-taken to further evaluate the role of early TIPSS It is importantto make the distinction between salvage TIPSS and early TIPSSto prevent rebleeding
Liver transplantationThis is probably appropriate only for patients who bleed whileawaiting liver transplantation although studies comparing VBLor TIPSS placement with urgent liver transplantation in thissituation need to be done Liver transplantation is an exceed-ingly rare option for the vast majority of patients both becauseit is not commonly available and because of shortages anddelays in organ procurement No controlled trials of liver trans-plantation in uncontrolledactive bleeding are available
Recommendations for the control of variceal bleeding in cir-rhosis are given below and in figure 3
Recommendations control of active variceal haemorrhage incirrhosis (figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with bloodplatelets and clotting factors in line with local protocolsfor managing massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusionpolicy aiming for a haemoglobin of 70ndash80 gL is sug-gested in haemodynamically stable patients (level 1bgrade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable(level 5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L(level 5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to localcircumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with suspected
or confirmed variceal bleeding (level 1a grade A)32 In all patients vasoconstrictors such as terlipressin or
somatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 15
Guidelines
41 If bleeding is difficult to control a SengstakenndashBlakemore tube should be inserted until further endo-scopic treatment TIPSS or surgery is performed depend-ing on local resources and expertise (level 1b grade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure (level1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
SECONDARY PROPHYLAXIS OF VARICEAL HAEMORRHAGEβ BlockersA meta-analysis of 12 trials comparing propranolol or nadolol139
with no active treatment showed a significant reduction inrebleeding but no significant reduction in mortality140 Thegreater reduction in portal pressure with carvedilol comparedwith propranolol has been described in the section lsquoPrimaryprophylaxisrsquo of this guideline
NitratesThe addition of ISMN to NSBB has been shown to reduce vari-ceal rebleeding compared with NSBB alone although no sur-vival benefit was seen141 In addition adverse events leading todrug withdrawal were more common in the group receivingcombined drug treatment A meta-analysis of ISMN alone orwith either NSBB or endoscopic therapy reported that there wasno mortality benefit from combining nitrates and NSBB com-pared with NSBB alone142
Side effects of ISMN include dizziness and headache Owingto the side effects and relative lack of data ISMN is not com-monly used in clinical practice
A recent RCT of 121 patients reported carvedilol to besimilar to combined ISMN and NSBB therapy in the preventionof variceal rebleeding and mortality although severe adverseevents were less common with carvedilol143
SimvastatinA recent abstract of a multicentre RCT of 158 patients reporteda survival benefit (91 vs 78 p=003) from adding simvasta-tin to VBL and NSBB compared with placebo VBL and NSBBas treatment for the prevention of variceal rebleeding144 Therewas no difference in rebleeding and the survival benefit wasrestricted to Child A and B patients Serious adverse events weresimilar in both groups More data are required to investigatethis interesting observation of a survival benefit from simvastatinin this situation which may relate to its effects on hepatocellularfunction fibrosis and portal pressure
Proton pump inhibitorsA double-blind randomised placebo-controlled trial showed thatpantoprazole reduced the size of ulcers in patients who under-went VBL However the total number of ulcers and other out-comes were similar in the two groups145
Endoscopic therapyVBL has been accepted as the preferred endoscopic treatmentfor the prevention of variceal rebleeding with a lower rate ofrebleeding mortality and complications than sclerother-apy146 147 The time interval between VBL sessions to achieveeradication of varices is debateable However a recent RCTcomparing monthly with biweekly VBL after initial haemostasiswith VBL in 70 patients suggested that there were fewerpost-VBL ulcers in the monthly group (11 vs 57plt0001)148 Variceal recurrence rebleeding and mortality weresimilar in both groups
Two meta-analyses showed there is no evidence that the add-ition of sclerotherapy to VBL improves clinically relevant out-comes including variceal rebleeding and death and thecombination led to higher stricture rates149 150
Endoscopic therapy versus drug therapyVBL has been reported to be more effective than combinedNSBB and ISMN drug therapy151 However an 8-yearfollow-up study of this RCT found that although VBL wassuperior in reducing variceal rebleeding survival rates were sig-nificantly higher in the group treated with combined drug treat-ment152 Other studies have found no superiority of VBL overcombined drug therapy for prevention of variceal rebleeding ormortality153 154 A recent small multicentre RCT reported carve-dilol to be similar to VBL in the prevention of variceal rebleed-ing with a trend in favour of survival with carvedilol (73 vs48 p=0110)155
Several meta-analyses have compared drug therapy with VBLin the prevention of variceal rebleeding One meta-analysis ofsix RCTs showed no significant difference in variceal rebleedingrates when comparing VBL alone with combined NSBB andISMN therapy However all-cause mortality was significantlyhigher in patients treated with the VBL (RR=125 95 CI101 to 155)156 Three meta-analyses comparing drug therapy(NSBB alone or with ISMN) with endoscopic therapy alonereported no difference in variceal rebleeding or mortality157ndash159
Endoscopic+drug therapy versus either aloneNumerous studies and several meta-analyses have comparedcombined endoscopic and drug therapy with monotherapy(endoscopic or drugs alone) in the prevention of varicealrebleeding A meta-analysis of 23 trials assessing sclerotherapyor VBL combined with NSBB reported that combinationtherapy reduced rebleeding more than either endoscopic
16 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

56 Role of endoscopic ultrasound-guided injection of tissueadhesives or thrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
INTRODUCTIONThe guidelines refer closely to the Baveno V consensus state-ment published in 20101 and the 2012 NICE Guidelines onAcute Upper GI bleeding (CG141)2 These documents arewidely used and offer useful evidence-based guidance Howeverwe feel that owing to significant recent advances further addi-tions and refinements to the published guidance with particularfocus on resource implications service development and thepatient pathway are necessary The previously mentioned docu-ments1 2 do not cover all the recent advancesmdashin particular inthe field of acute variceal bleeding and the role of transjugularintrahepatic portosystemic stent shunt (TIPSS) There have alsobeen developments and better insights into drug treatment forprevention of varices and variceal bleedingmdashin particular therole of non-cardioselective β blockers (NSBB)
Guideline developmentThese guidelines were drafted after discussions within the liversection of the British Society of Gastroenterology (BSG) andacceptance of the proposal by the Clinical Services andStandards Committee (CSSC) There followed division of sec-tions to be researched by designated authors and an exhaustiveliterature review The Baveno V consensus and NICE guidelineswere closely followed and guideline quality was assessed usingthe AGREE tool3 (section lsquoAssessing the quality of guidelinesthe AGREE II instrumentrsquo)
A preliminary guideline document was drafted by the authorsfollowing discussion and where necessary voting by membersof the Guidelines Development Group (GDG) The draft guide-lines were submitted for review by CSSG then BSG councilmembers Finally full peer review was undertaken by reviewersselected by the editor of Gut
Attempts were made to preserve the format of the originalguidelines with additional sections relating to service develop-ment the patient pathway and pre-primary prophylaxis Thesection on the management of acute variceal bleeding has beenextensively rewritten to take into account recent importantdevelopments in interventional radiology drug treatment andresuscitation
Assessing the quality of guidelines the AGREE II instrumentThe AGREE II instrument is an accepted method for appraisingclinical guidelines3 Six domains are listed
Scope and purposeThe guidelines are intended for use by clinicians and otherhealthcare professionals managing patients with cirrhosis andgastro-oesophageal varices in light of recent guidance publishedby NICE2 and the Baveno V Consensus1 Important subsequentdevelopments are covered in depth due to the potential impacton clinical practice The guidelines are primarily aimed at man-agement of adult patients
Guideline development group membership and stakeholderinvolvementMembership of the group includes gastroenterologists hepatolo-gists and interventional radiologists with nursing and patientrepresentation
Rigour of developmentThe published literature was searched using Pubmed MedlineWeb of Knowledge and the Cochrane database between October2013 and February 2015 The GDG met through a series of tel-econferences during that time The guidelines rely considerablyon consensus statements published by the Baveno V Consensusand NICE1 2 The style of graded recommendations is deter-mined by the level of supporting evidence (graded level 1 to 5)as described by the Oxford Centre For Evidence BasedMedicine4 (table 1) and is as followsA consistent level 1 studiesB consistent level 2 or 3 studies or extrapolations from level 1
studiesC level 4 studies or extrapolations from level 2 or 3 studiesD level 5 evidence or troublingly inconsistent or inconclusive
studies of any levelAreas of disagreement about the recommendation grade were
subjected to discussion and if necessary voting by members ofthe guidelines group Where possible the health benefits sideeffects and risks of recommendations have been discussed Theguidelines were subject to peer review after submission for con-sideration of publication in Gut
Clarity and presentationRecommendations are intended to be specific to particular situa-tions and patient groups where necessary different options arelisted Key recommendations are linked to discussion threads ona discussion forum hosted on the BSG website
ApplicabilityWhere necessary we have discussed organisational changes thatmay be needed in order to apply recommendations We haveattempted to identify key criteria for monitoring and auditpurposes
Editorial independence and conflict of interestGuideline group members have declared any conflicts ofinterest
Scheduled review of guidelinesThe proposed time for review of the guidelines is 5 years totake into account new developments To ensure that there is afacility for feedback after publication links to the BSG discus-sion forums corresponding to the particular section of theseguidelines are included with this document This facility toprovide new evidence is provided to all BSG members Inaccordance with the AGREE II tool the BSG forum will providefeedback
SERVICE DELIVERY AND DEVELOPMENTDespite improvements in outcomes following variceal bleedingthe need to optimise the management of acute variceal bleed-ing is highlighted in recent publications and national reportsIn a national audit5 variceal bleeding accounted for just over10 of all admissions with acute GI bleeding in the UK withtwo-thirds having a previous history of variceal bleeding andover 50 presenting during normal working hours Endoscopywithin 24 h of presentation was achieved in only 66 of allpatients and in 70 of patients with documented cirrhosisMost procedures were performed in the endoscopy depart-ment with just 14 performed under general anaestheticdespite high-risk stigmata and endoscopic therapy beingrequired in two-thirds of cases Notably antibiotics were
4 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
administered in only 27 of patients before endoscopy andadministration of vasoactive drugs before endoscopy was onlyslightly higher at 44 Furthermore only four patients (lt1)were referred for TIPSS which may reflect the lack of accessto interventional radiology and that the audit was conductedbefore the trial of early TIPSS6 The National ConfidentialEnquiry into Patient Outcome and Death (NCEPOD) reportlsquoMeasuring the unitsrsquo assessed clinical management beforedeath of 594 patients with alcoholic liver disease over a6-month period in the UK7 Gastrointestinal bleeding wasnoted in 35 of cases with approximately 50 having vari-ceal bleeding Delays in endoscopy were noted in 10 ofcases and several aspects of clinical andor organisational carewere judged to be poor or unacceptable in 18 of patientspresenting with GI bleeding There were deficiencies noted inthe out-of-hours rotas for GI bleeding with 27 of hospitalsnot having a dedicated-out-of hours GI bleeding serviceStudies from other countries have also reported deficiencieswith delays in admission to hospital and administration of anti-biotics Two observational studies showed that access to
emergency endoscopy and use of prophylactic antibiotics andvasoactive drugs was better in tertiary centres although thisdid not appear to affect survival8 9
Acute variceal haemorrhage refractory to endoscopic andpharmacological treatments where TIPSS is usually indicatedmust be managed with appropriate resources TIPSS is an estab-lished interventional treatment for refractory or recurrent vari-ceal haemorrhage It remains a highly specialised procedurerequiring adequate training and experience Knowledge of therelevant equipment anatomy and how to deal with any compli-cations is essential It should therefore be performed in centreswith adequate personnel multidisciplinary support and equip-ment required to optimise management and minimise risks10
Regional centres with easily accessible interventional radiologyservices are generally best equipped to perform this procedureSetting up regional agreements and pathways to allow transfer ofappropriate patients to hospitals that undertake TIPSS proce-dures is an important step These pathways could also be used toprovide emergency endoscopic management if necessary due toproblems with out-of-hours endoscopic cover in smaller
Table 1 Levels of evidence
LevelTherapyprevention aetiologyharm Prognosis Diagnosis DDXsymptom prevalence study
1a SR (with homogeneity) ofrandomised controlled trial (RCT)
SR (with homogeneity) of inceptioncohort studies CDRdagger validated indifferent populations
SR (with homogeneity) of level 1diagnostic studies CDRdagger with 1b studiesfrom different clinical centres
SR (with homogeneity) ofprospective cohort studies
1b Individual RCT (with narrow CI) Individual inception cohort study withge80 follow-up CDRdagger validated in asingle population
ValidatingDagger cohort study with goodsectreference standards or CDRdagger testedwithin one clinical centre
Prospective cohort study with goodfollow-uppara
1c All or none All or none case series Absolute SpPins and SnNoutsdaggerdagger All or none case series2a SR (with homogeneity) of cohort
studiesSR (with homogeneity) of eitherretrospective cohort studies or untreatedcontrol groups in RCTs
SR (with homogeneity) of level gt2diagnostic studies
SR (with homogeneity) of 2b andbetter studies
2b Individual cohort study (includinglow-quality RCT eg lt80follow-up)
Retrospective cohort study or follow-upof untreated control patients in an RCTderivation of CDRdagger or validated on splitsampleDaggerDagger only
ExploratoryDagger cohort study with goodsectreference standards CDRdagger afterderivation or validated only on splitsampleDaggerDagger or databases
Retrospective cohort study or poorfollow-up
2c lsquoOutcomesrsquo research ecologicalstudies
lsquoOutcomesrsquo research Ecological studies
3a SR (with homogeneity) of casendashcontrol studies
SR (with homogeneity) of 3b and betterstudies
SR (with homogeneity) of 3b andbetter studies
3b Individual casendashcontrol study Non-consecutive study or withoutconsistently applied reference standards
Non-consecutive cohort study orvery limited population
4 Case series (and poor qualitycohort and case-control studiessectsect)
Case series (and poor quality prognosticcohort studiesparapara)
Casendashcontrol study poor ornon-independent reference standard
Case series or superseded referencestandards
5 Expert opinion without explicitcritical appraisal or based onphysiology bench research or lsquofirstprinciplesrsquo
Expert opinion without explicit criticalappraisal or based on physiology benchresearch or lsquofirst principlesrsquo
Expert opinion without explicit criticalappraisal or based on physiology benchresearch or lsquofirst principlesrsquo
Expert opinion without explicitcritical appraisal or based onphysiology bench research or lsquofirstprinciplesrsquo
Homogeneity means a systematic review (SR) that is free of worrisome variations (heterogeneity) in the directions and degrees of results between individual studies Not all SRs withstatistically significant heterogeneity need be worrisome and not all worrisome heterogeneity need be statistically significantdaggerCDR Clinical Decision Rule (algorithms or scoring systems which lead to a prognostic estimation or a diagnostic category)DaggerValidating studies test the quality of a specific diagnostic test based on prior evidence An exploratory study collects information and trawls the data (eg using a regression analysis) tofind which factors are lsquosignificantrsquosectGood reference standards are independent of the test and applied blindly or objectively to all patients Poor reference standards are haphazardly applied but still independent of thetest Use of a non-independent reference standard (where the lsquotestrsquo is included in the lsquoreferencersquo or where the lsquotestingrsquo affects the lsquoreferencersquo) implies a level 4 studyparaGood follow-up in a differential diagnosis study is gt80 with adequate time for alternative diagnoses to emerge (eg 1ndash6 months acute 1ndash5 years chronic)Met when all patients died before the treatment became available but some now survive while receiving it or when some patients died before the treatment became available butnone now die while receiving itdaggerdaggerAn lsquoabsolute SpPinrsquo a diagnostic finding whose Specificity is so high that a Positive result rules in the diagnosis An lsquoAbsolute SnNoutrsquo a diagnostic finding whose Sensitivity is sohigh that a Negative result rules out the diagnosisDaggerDaggerSplit-sample validation is achieved by collecting all the information in a single tranche then artificially dividing this into lsquoderivationrsquo and lsquovalidationrsquo samplessectsectPoor quality cohort study one that failed to clearly define comparison groups andor failed to measure exposures and outcomes in the same (preferably blinded) objective way inboth exposed and non-exposed individuals andor failed to identify or appropriately control known confounders andor failed to carry out a sufficiently long and complete follow-up ofpatients Poor quality casendashcontrol study one that failed to clearly define comparison groups andor failed to measure exposures and outcomes in the same (preferably blinded)objective way in both cases and controls andor failed to identify or appropriately control known confoundersparaparaPoor quality prognostic cohort study one in which sampling was biased in favour of patients who already had the target outcome or the measurement of outcomes wasaccomplished in lt80 of study patients or outcomes were determined in an unblinded non-objective way or there was no correction for confounding factors
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 5
Guidelines
hospitals This model referred to as ldquospoke and wheelrdquo ornetwork model is well established for other complex proceduresand helps to expedite and streamline the process In theNCEPOD report lsquoMeasuring the unitsrsquo just 15 of hospitals hadon-site access to TIPSS while 72 had access to TIPSS in othercentres7
There have been significant efforts to address the need toimprove the upper GI bleeding (UGIB) service A toolkit wasproduced in collaboration with BSG Association of UpperGastrointestinal Surgeons (AUGIS) Royal Colleges ofPhysicians Radiology and Nursing and Academy of MedicalRoyal Colleges11 The key nine service standards recommendedby the document are detailed below1 There will be a nominated individual with the authority to
ensure implementation by the contracted provider2 Contracted providers will ensure the minimum service is
adequately resourced3 All patients with suspected UGIB should be properly
assessed and their risk scored on presentation4 All patients should be resuscitated before therapeutic
intervention5 All high-risk patients with UGIB should be endoscoped
within 24 h preferably on a planned list in the first instance6 For patients who require more urgent intervention either for
endoscopy interventional radiology or surgery formal 247arrangements must be available
7 The necessary team meeting an agreed competency levelshould be available throughout the complete patient pathway
8 Each stage of the patient pathway should be carried out inan area with lsquoappropriatersquo facilities equipment and supportincluding staff experienced in the management of UGIB
9 All hospitals must collect a minimum dataset in order tomeasure service provision against auditable outcomes(case-mix adjusted as appropriate)NICE recommendations for endoscopy provision are detailed
in the section lsquoManagement of active variceal haemorrhagersquorecommendations2 The BSG has also produced a care bundlefor patients admitted with decompensated cirrhosis in light ofthe NCEPOD report with a check list method which includesgastrointestinal bleeding12
Since the 2008 Darzi report quality has become a priorityfor the NHS13 With these guidelines there is real opportunityto introduce quality outcomes based on good clinical evidenceFurthermore by incorporating them into the liver accreditationscheme Liver Quest one can improve and assure quality inliver services across the UK14 Therefore a small number ofquality outcomes measures have been chosen and form part ofthe key recommendations15
DEFINITIONSIt is important to define the terms that should be used in thecontext of a variceal bleed These are the Baveno V consensusdefinitions1
Variceal haemorrhageVariceal haemorrhage is defined as bleeding from an oesopha-geal or gastric varix at the time of endoscopy or the presence oflarge oesophageal varices with blood in the stomach and noother recognisable cause of bleeding An episode of bleeding isclinically significant when there is a transfusion requirement for2 units of blood or more within 24 h of the time zero togetherwith a systolic blood pressure of lt100 mm Hg or a posturalchange of gt20 mm Hg andor pulse rate gt100 bpm at time
zero (time zero is the time of admission to the first hospital towhich the patient is taken)
Time frame of acute bleedingThe acute bleeding episode is represented by an interval of120 h (5 days) from time zero Evidence of any bleeding after120 h is the first rebleeding episode
Failure to control active bleedingFailure to control active bleeding is defined as death or need tochange treatment defined by one of the following criteria16 17
1 Fresh haematemesis or nasogastric aspiration of ge100 mL offresh blood ge2 h after the start of a specific drug treatmentor therapeutic endoscopy
2 Development of hypovolaemic shock3 30 gL drop in haemoglobin (9 drop of haematocrit)
within any 24 h period if no transfusion is given This timeframe needs to be further validated
Variceal rebleedingVariceal rebleeding is defined as the occurrence of a singleepisode of clinically significant rebleeding from portal hyperten-sive sources from day 5 Clinically significant rebleeding isdefined as recurrent melaena or haematemesis in any of the fol-lowing settings1 hospital admission2 blood transfusion3 30 gL drop in haemoglobin4 death within 6 weeks
Early mortalityDeath within 6 weeks of the initial episode of bleeding
NATURAL HISTORY OF VARICES IN CIRRHOSISDevelopment of varicesThe rise in portal pressure is associated with the developmentof collateral circulation which allows the portal blood to bediverted into the systemic circulation These spontaneous shuntsoccur (a) at the cardia through the intrinsic and extrinsic gastro-oesophageal veins (b) in the anal canal where the superiorhaemorrhoidal vein belonging to the portal system anastomoseswith the middle and inferior haemorrhoidal veins which belongto the caval system (c) in the falciform ligament of the liverthrough the para-umbilical veins which are the remains of theumbilical circulation of the fetus (d) in the abdominal wall andthe retroperitoneal tissues from the liver to the diaphragmveins in the lienorenal ligament in the omentum and lumbarveins and (e) blood diversion from the diaphragm gastric pan-creatic splenic and adrenal veins which may drain into the leftrenal vein
Numerous lines of evidence suggest that varices develop andenlarge with time Christensen et al18 followed up a cohort of532 patients with cirrhosis and showed that the cumulative inci-dence of patients with varices increased from 12 to 90 over12 years In a study involving 80 patients followed up for16 months Cales and Pascal19 showed that 20 of patientswho did not have varices developed new varices and 42 ofpatients with small varices showed definite enlargement Czajaet al20 also showed that the prevalence of varices increased from8 to 13 over 5 years in a cohort of patients with chronicactive hepatitis even though they were treated with prednisol-one Merli et al21 in a study of 213 patients with cirrhosis withno or small varices demonstrated that the annual progression ofvarices was 12 A recent database analysis by DrsquoAmico et al22
6 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
using a competing risk model showed that the cumulative inci-dence of varices at 10 and 20 years was 44 and 53 respect-ively suggesting an overestimation in previous studies not usinga competing risk model
The main factors that appear to determine the developmentof varices are continued hepatic injury the degree of portosyste-mic shunting endoscopic appearances and portal pressureEvidence for the role of hepatic injury is derived from studies inwhich varices were shown to regress with time Baker et al23 fol-lowed up a cohort of 115 patients with oesophageal varices andshowed that varices had disappeared in nine patients regressedin seven and remained unchanged in six They concluded thatthe disappearance and regression of varices might be related toabstinence from alcohol This observation was confirmed in astudy by Dagradi24 who followed up a cohort of patients withalcoholic cirrhosis over 3 years and showed a reduction in vari-ceal size in 12 of the 15 patients with alcoholic cirrhosis whostopped drinking and an enlargement in variceal size in 17patients who continued to drink On the other hand Cales andPascal19 showed that regression of varices occurred in 16 ofpatients with alcoholic cirrhosis who continued to imbibealcohol This might be related to the development of large por-tosystemic collaterals which decompress the portal system andreduce the risk of the development of large oesophageal varicesThe degree of portosystemic shunting can be quantified bymeasuring the diameter of portal veins and collaterals and canbe significant in those with gastrorenal or splenorenal shunt-ing25 26 Others have shown that the presence of alcoholic cir-rhosis Childrsquos B or C cirrhosis and red whale signs on indexendoscopy predicted progression of varices21 Groszmannet al27 in a placebo-controlled randomised trial of timolol in213 cirrhotic patients without varices showed that a baselinehepatic venous pressure gradient (HVPG) of gt10 mm Hg or age10 increase in HVPG during follow-up were both predictiveof the development of varices
Diagnosis of gastro-oesophageal varicesUntil recently endoscopy has been used exclusively to diagnosevarices Non-invasive methods of screening for varices includecapsule endoscopy transient elastography and use of laboratoryand radiological findings
EndoscopyThere is universal acceptance that endoscopy is the lsquogold stand-ardrsquo for diagnosing gastro-oesophageal varices The main limita-tions are intraobserver variability in the diagnosis of small orgrade I oesophageal varices (figure 1AndashC) Recently unsedatednasal gastroscopy has been found to have similar accuracy toconventional endoscopy and has the advantage of tolerabilityand potential cost saving since it can be performed in the clinicsetting in some institutions28 29 However there are no con-trolled studies and banding of varices is not possible
Capsule endoscopyCapsule endoscopy uses a 26 mm pill-shaped device whichtransmits video footage which is stored and later analysedPatients are not sedated but patient cooperation is essentialIn a large study by de Franchis et al30 capsule endoscopy wascompared with standard gastroscopy The primary end point of90 or greater concordance was not achieved Lapalus et al31
in a prospective study of 120 patients demonstrated similarresults with capsule endoscopy Therefore capsule endoscopycannot be considered an alternative to standard endoscopyalthough may have a role in patient who refuse gastroscopy
Transient elastographyTransient elastography ((FibroScan Echosens Paris France) usesthe principles of ultrasound to derive tissue stiffness by measur-ing the speed of propagation of a low-frequency wave whichthen correlates with liver fibrosis Vizzutti et al32 in a study of61 patients with hepatitis C showed a sensitivity for predictionof oesophageal varices of 90 using a threshold 176 kPaHowever specificity was poor at 43 A study of 298 patientsfound the optimal cut-off point for the prediction of oesopha-geal varices was 215 kPa (sensitivity 76 and specificity78)33 In one uncontrolled study the use of transient elasto-graphy was found to be as effective as HVPG at predictingportal hypertension-related complications34 Therefore the roleof transient elastography in predicting varices is controversialdue to the lack of consistent results and controlled studies Thismodality may be more useful for predicting decompensation inpatients with cirrhosis
Radiological and serum parametersA prospective study of 311 patients with chronic hepatitis Cshowed that a platelet-to-spleen size ratio with a threshold of909 had positive and negative predictive values of 100 and94 respectively35 These good results have not been repro-duced by others as demonstrated in a meta-analysis36
Risk factors for first variceal bleedingThe factors that predispose to and precipitate variceal haemor-rhage are still not clear The suggestion that oesophagitis mayprecipitate variceal haemorrhage has been discarded37
Presently the most important factors that have been heldresponsible include (i) pressure within the varix (ii) varicealsize (iii) tension on the variceal wall and (iv) severity of theliver disease
Portal pressureIn most cases portal pressure reflects intravariceal pressure38
and a HVPG gt10 mm Hg is necessary for the development ofoesophageal varices27 There is no linear relationship betweenthe severity of portal hypertension and the risk of varicealhaemorrhage although HVPG gt12 mm Hg is an accepted
Figure 1 (A) Grade I oesophagealvarices These collapse to inflation ofthe oesophagus with air (B) Grade IIoesophageal varices These are varicesbetween grades 1 and 3 (C) Grade IIIoesophageal varices These are largeenough to occlude the lumen
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 7
Guidelines
threshold for variceal bleeding39 40 However the HVPG tendsto be higher in bleeders as well as in patients with larger varicesIn a prospective study comparing propranolol with placebo forthe prevention of first variceal haemorrhage Groszmann et al41
showed that bleeding from varices did not occur if the portalpressure gradient (PPG) could be reduced to lt12 mm HgOthers have shown that a 20 reduction in portal pressure pro-tects against further bleeding42 These haemodynamic goalshave been accepted as the aim of pharmacological treatment ofportal hypertension It is important to appreciate that gastricvarices can bleed at pressures lt12 mm Hg and the influence ofwall tension of the varix plays a greater role in the risk of bleed-ing43 A greater pressure reduction may be necessary to protectagainst bleeding This is further discussed in the section lsquoGastricvaricesrsquo At present measurement of portal pressure in guidingpharmacological treatments is limited to clinical trials in the UK
Variceal sizeVariceal size is best assessed endoscopically (figure 1AndashC)Published results are variable owing to the lack of a definition dis-tinguishing between large and small varices Small (grade I)varices tend to be narrow and flatten easily with air whereaslarger (grade 2 and 3) varices are usually broader and flatten withdifficulty if at all Numerous studies40 44 have shown that therisk of variceal haemorrhage increases with the size of varices45
Variceal wall and tensionPolio and Groszmann46 using an in vitro model showed thatrupture of varices was related to the tension on the varicealwall The tension depends on the radius of the varix In thismodel increasing the size of the varix and decreasing the thick-ness of the variceal wall caused variceal rupture Recently endo-scopic ultrasound and manometry have been used to estimatewall tension of varices47
Endoscopic features such as lsquored spotsrsquo and lsquowhalersquo markingswere first described by Dagradi24 They have been described asbeing important in the prediction of variceal haemorrhageThese features represent changes in variceal wall structure andtension associated with the development of microtelangiectasiasand reduced wall thickness In a retrospective study by theJapanese Research Society for Portal Hypertension Beppuet al48 showed that 80 of patients who had blue varices orcherry red spots bled from varices suggesting that this was animportant predictor of variceal haemorrhage in cirrhosis
Severity of liver disease and bleeding indicesTwo independent groups prospectively assessed factors predict-ing first variceal haemorrhage in cirrhosis (table 2) The NorthItalian Endoscopic Club (NIEC)49 reported their findings in1988 followed in 1990 by data from the Japanese50 Both thesestudies showed that the risk of bleeding was based on threefactors severity of liver disease as measured by Child class vari-ceal size and red wale markings The NIEC study showed awide range for the risk of bleeding of 6ndash76 depending on thepresence or absence of the different factors Using the same vari-ables the NIEC index was simplified by de Franchis et al51 andshown to correlate with the original index Further studiesshowed that the HVPG and intravariceal pressure were alsoindependent predictors of first variceal haemorrhage when ana-lysed in conjunction with the NIEC index52 53
In summary the most important factors that determine the risk ofvariceal haemorrhage are the severity of liver disease size of varicesand presence of red signs Measurement of HVPG is a useful guidefor selection of patients for treatment and their response to
treatment although the predictive value does not appear toimprove on the NIEC index and presence of red whale marking54
Risk and mortality of first variceal bleedData describing the overall risk of bleeding from varices must beviewed with caution and have some pitfalls in interpretationThe natural history of patients who have varices that are diag-nosed as part of their baseline investiations is different fromthat of patients who have complications of liver disease such asascites and encephalopathy Most studies do not comment oneither the severity of liver disease or whether patients with alco-holic cirrhosis are continuing to drink Both these factors have asignificant effect on the risk of variceal haemorrhage
Most studies report bleeding from varices in about 20ndash50of patients with cirrhosis during the period of follow-up Bakeret al23 reported variceal bleeding in 33 of 115 patients that theyfollowed up for a mean of 33 years with a mortality of 48from the first variceal haemorrhage These data were confirmedby Christensen et al18 About 70 of the episodes of bleedingoccur within 2 years of diagnosis Recent studies demonstrate adramatic reduction in mortality following variceal bleeding of20 6-week mortality55 and 15 in-hospital mortality5 withcontributions from improved endoscopic pharmacological andradiological therapies notably TIPSS Intensive care treatmenthas also improved with outcomes being particularly good forthose requiring minimal organ support
Analysis of the non-active treatment arms in the primaryprophylaxis trials comparing propranolol with placebo showresults similar to those of the primary prophylaxis shunt trialswith most episodes of bleeding occurring within the first 2 yearsof follow-up In these studies the rate of first variceal haemor-rhage ranged from 22 to 6156ndash60 This large difference inthe rate of first bleed relates almost certainly to the number ofpatients with severe liver disease included in the study (PascalChild Cmdash46 bleedingmdash61 Italian Multicenter Project forPropranolol in Prevention of Bleeding (IMPP) Child Cmdash6bleedingmdash32 Conn Child Cmdash6 bleedingmdash22)Mortality varied from 24 to 49 over 2 years (Pascal mortal-itymdash49 IMPP mortalitymdash24 Conn mortalitymdash24)
Primary prophylaxisSince 30ndash50 of patients with portal hypertension will bleedfrom varices and about 20 will die from the effects of the first
Table 2 Scoring systems for quantifying the severity of cirrhosisSeverity of liver disease can be described using the ChildndashPughscore or MELD scoreThe ChildndashPugh score is the sum of severity scores for Child classvariceal size and red wale markings the variables shown below
Category 1 2 3
Encephalopathy 0 III IIIIVAscites Absent Mild-moderate SevereBilirubin (μmolL) lt34 34ndash51 gt51Albumin (gL) gt35 28ndash35 lt28INR lt13 13ndash15 gt15
ChildndashPugh class A represents a score of le6 class B a score of 7ndash9 and class C ge10The MELD score is a formula that includes three laboratory-based variables reflectingthe severity of liver disease It was originally used to predict the short-term mortalityafter placement of a transjugular intrahepatic portosystemic stent-shunt for varicealbleeding Subsequently it has been used in selecting candidates for livertransplantationMELD score please use the online calculator httpswwwesotorgElitameldCalculatoraspxINR international normalised ratio
8 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleed it seems rational to develop prophylactic regimens toprevent the development of and bleeding from these varicesHowever most of the published trials do not have sufficientpower to identify favourable treatment effects Based on theexpected bleeding and death rates in the control group theminimum number of patients needed to detect a 50 reductionin bleeding would be 270 and 850 patients in each arm todetect the same reduction in mortality A proposed algorithmfor surveillance and prophylaxis of varices is shown in figure 2At this time there is insufficient evidence to support treatingpatients without varices or lsquopre-primary prophylaxisrsquo A largerandomised placebo-controlled trial of timolol in patientswithout varices and portal hypertension defined as HVPGgt6 mm Hg did not show any effect on the development ofvarices or variceal bleeding27 The role of drug treatment in pre-venting bleeding in patients with small varices is unclear Threerandomised placebo-controlled trials have studied this Caleset al61 showed that propranolol in patients with small or novarices resulted in greater development of varices Howeverpatients without varices were included and there was significantloss of patients to follow-up The second trial showed thatnadolol reduced variceal bleeding without survival benefit andincreased adverse events62 Sarin et al63 did not show any effectwith propranolol despite a significant effect on portal pressure
SurgeryPortacaval shuntsFour trials of portacaval shunts have been published which ran-domised a total of 302 patients64ndash67 either to prophylactic shuntsurgery or to non-active treatment A meta-analysis of thesestudies showed a significant benefit in the reduction of varicealbleeding (OR=031 95 CI 017 to 056) but also a signifi-cantly greater risk of hepatic encephalopathy (OR=2 95 CI12 to 31) and mortality (OR=16 95 CI 102 to 257) inpatients treated with shunt surgery68 At this time there is noevidence for the use of TIPSS for primary prophylaxis1
Devascularisation proceduresInokuchi50 showed that there was a significant reduction in vari-ceal bleeding and in mortality in patients treated with a varietyof devascularisation procedures There are however numerousproblems with the interpretation of this study because of theuse of different procedures in each of the 22 centres Theseresults require confirmation
Pharmacological treatmentNon-cardioselective β blockersThe mainstay of the pharmacological approach to the primaryprophylaxis of variceal haemorrhage has been NSBBPropranolol which has been shown to reduce the PPG reduceazygos blood flow and also variceal pressure It achieves this bycausing splanchnic vasoconstriction and reducing cardiacoutput There is no clear dose-related reduction in HVPG orcorrelation of HPVG reduction with reduction in heart rate69
Observational studies have shown that a 10ndash12 reduction inHVPG after acute administration of propranolol was associatedwith reduced bleeding and hepatic decompensation54 70
However HVPG monitoring is not routinely available in mostcentres outside of larger institutions A meta-analysis of nineplacebo-controlled randomised trials (964 patients) showed thatthe pooled risk difference for bleeding was minus11 (95 CIminus21 to minus1) and for death was minus9 (95 CI minus18 tominus1) in favour of propranolol71
Nadolol exerts similar effects on portal haemodynamicsalthough the effect on blood pressure may not be as pro-nounced Two placebo-controlled trials58 59 have shownreduced bleeding although in one study this was only seen onper protocol analysis59 There was no effect on overall survival
Carvedilol is a NSBB like propranolol and a vasodilator dueto α1 receptor blockade The latter reduces portocollateralresistance and by actions on hepatic stellate cells leads to areduction in intrahepatic resistance Haemodynamic studiesdemonstrate a greater reduction in portal pressure with
Figure 2 Algorithm for surveillance of varices and primary prophylaxis in cirrhosisndash If there is clear evidence of disease progression this interval can be modified by clinician Endoscopy should also be offered at time ofdecompensation
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 9
Guidelines
carvedilol than with propranolol although blood pressure isreduced72 73 The optimum dose is 625ndash125 mgday74 Higherdoses are not more effective and are associated with moreadverse eventsmdashin particular hypotension Carvedilol at a doseof 125 mgday at current UK prices is considerably cheaperthan propranolol 40 mg twice a day and nadolol 80 mgday(monthly cost pound120 pound562 and pound5 respectively) Two RCTs ofcarvedilol versus variceal band ligation (VBL) in primaryprophylaxis have been published75 76 The first study75 showedsignificantly reduced bleeding in the carvedilol arm (10 vs23 relative hazard 041 95 CI 019 to 096) with no effecton survival The second trial by Shah et al76 did not show anydifferences in bleeding or mortality Compliance with VBL wasbetter in the latter trial and unlike the first trial there were sig-nificantly more patients with viral hepatitis than alcoholic cir-rhosis A further study74 assessed the effect of carvedilol inpatients who were haemodynamic non-responders to propran-olol where haemodynamic response was defined as HVPGreduction to le12 mm Hg or by gt20 of baseline after 4 weeksof treatment Patients who were haemodynamic non-respondersor intolerant to carvedilol were treated with VBL Carvedilolresulted in significantly lower variceal bleeding compared withVBL and haemodynamic responders to carvedilol or propran-olol had significantly lower mortality than those treated withVBL It is worth noting that the study was not randomised
There have been recent suggestions based on low-level evi-dence that NSBB may result in a poorer outcome in patientswith cirrhosis and refractory ascites77 The lsquowindow hypothesisrsquofor β blockers in cirrhosis has also recently been described sug-gesting that NSBB are helpful in the compensated and earlydecompensated cirrhotic period but may not be helpful in veryearly cirrhosis such as in a patient with no varices and may beharmful in patients with end-stage cirrhosis with refractoryascites78 However recent large observational studies questionthe last hypothesis with improved survival seen in patients withrefractory ascites treated with NSBB79 unless patients have anepisode of spontaneous bacterial peritonitis80 Therefore untilthere are further prospective controlled studies NSBB should becontinued in patients with refractory ascites The clinician mustcarefully monitor haemodynamic parameters such as blood pres-sure and discontinue NSBB in patients with hypotension andrenal impairment as can occur after an episode of spontaneousbacterial peritonitis Other potentially severe adverse eventswith NSBB include symptomatic bradycardia asthma andcardiac failure Less severe side effects such as fatigue insomniaand sexual dysfunction may also result
Isosorbide mononitrateInterest in the use of vasodilators such as isosorbide mononitrate(ISMN) developed after the demonstration that it reduces portalpressure as effectively as propranolol81 but has subsequentlywaned A trial comparing ISMN with propranolol showed nosignificant difference between these agents82 Another rando-mised trial of ISMN versus placebo did show any difference inthe two arms83 Therefore ISMN is not recommended asmonotherapy in primary prophylaxis
β Blocker and ISMNThe combination of nadolol and ISMN has been compared withnadolol in a RCT The combination therapy reduced the fre-quency of bleeding significantly but no significant differenceswere detected in mortality84 However Garcia-Pagan et al85 in adouble-blind RCTof propranolol plus ISMN versus propranolol
plus placebo failed to show any differences between the twoarms Combination therapy is associated with more side effects
Proton pump inhibitorsA placebo-controlled randomised trial reported reduced bleed-ing and mortality with rabeprazole after eradication of varices86
However the study had a heterogeneous population with VBLperformed for both primary and secondary prophylaxis andsmall numbers (n=43) limiting the validity of the conclusionsFurthermore there was no arm comparing proton pump inhibi-tors with NSBB The use of proton pump inhibitors in patientswith cirrhosis and ascites was associated with increased risk ofspontaneous bacterial peritonitis in a large retrospective study87
This was not confirmed in a larger prospective non-randomisedstudy88 However a recent prospective observational study hasshown proton pump use to be associated with increased mortal-ity in cirrhosis89 Proton pump inhibitors are also associatedwith increased risk of Clostridium difficile infection90 Thereremains continuing concern about proton pump inhibitors inpatients with cirrhosis therefore caution should be used
Endoscopic therapyVariceal band ligationVBL has been compared with NSBB in 19 trials in a recentCochrane meta-analysis of 1504 patients91 Despite reducedbleeding (RR=067 95 CI 046 to 098) with VBL there wasno difference in overall mortality and bleeding-related mortalityThe difference in bleeding was not seen when only trials withlow selection or attrition bias were included Banding can haveserious complications The risk of fatal banding-induced bleed-ing was highlighted in a meta-analysis showing reduced fataladverse events with NSBB (OR=014 95 002 to 099)92
The optimal timing of banding intervals is discussed in thesection lsquoSecondary prophylaxis of variceal haemorrhagersquo A ran-domised trial of 96 patients who underwent endoscopic surveil-lance at 6 or 3 months after eradication of varices with VBL didnot demonstrate a difference in bleeding on mortality93
However the trial had a heterogeneous study group of patientswho underwent VBL both for primary (65) and secondaryprevention (35)
SclerotherapyNineteen trials have compared endoscopic variceal sclerotherapywith no treatment68 Owing to the marked heterogeneitybetween these studies a meta-analysis is clinically inappropri-ate68 Sclerotherapy does not offer any benefit in combinationwith NSBB or VBL compared with VBL or NSBB alone andincreases iatrogenic complications such as strictures94ndash96 At thistime sclerotherapy cannot be recommended for prophylaxis ofvariceal haemorrhage in patients with cirrhosis
Recommendations primary prophylaxis of variceal haemor-rhage in cirrhosis (figure 2)1 What is the best method for primary prophylaxis
11 We recommend NSBB or variceal band ligation (VBL)We suggest pharmacological treatment with propranololas first line VBL is offered if there are contraindicationsto NSBB The choice of VBL or NSBB should also takeinto account patient choice (level 1a grade A)
12 We suggest carvedilol or nadolol as alternatives to pro-pranolol (level 1b grade A)
13 Dose131 Propranolol 40 mg twice daily Dose titrated to
maximum tolerated or once heart rate (HR) of
10 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
50ndash55 bpm is reached to a maximum dose of320 mg (level 1a grade A)
132 Nadolol 40 mg daily dose Dose titrated tomaximum tolerated or once HR of 50ndash55 bpm isreached a maximum dose of 240 mg (level 1agrade A)
133 Carvedilol 625 mg once daily to increase tomaintenance of 125 mg after a week if toleratedor once HR of lt50ndash55 bpm is reached (level 1agrade A)
134 It is suggested that NSBB are discontinued at thetime of spontaneous bacterial peritonitis renalimpairment and hypotension (level 2b grade B)
14 In cases of contraindications or intolerance to NSBB werecommend variceal band ligation (level 1a grade A)
2 Who should have surveillance for variceal bleeding21 We recommend all patients with cirrhosis should be
endoscoped at the time of diagnosis (level 1a grade A)There is no indication to repeat endoscopy in patientsreceiving NSBB
3 How often should cirrhotic patients be endoscoped31 If at the time of first endoscopy no varices are seen we
suggest that patients with cirrhosis should be endos-coped at 2ndash3-year intervals (level 2a grade B)
32 If grade I varices are diagnosed we suggest that patientsshould be endoscoped at yearly intervals (level 2agrade B)
33 If there is clear evidence of disease progression wesuggest that the intervals can be modified by a clinicianEndoscopy should also be offered at time of decompen-sation (level 2a grade B)
4 Which patients with cirrhosis should have primaryprophylaxis41 If grade I varices and red signs or grade 2ndash3 varices are
diagnosed we recommend that patients have primaryprophylaxis irrespective of the severity of the liverdisease (level 1a grade A)
5 Treatments not recommended51 Proton pump inhibitors are not recommended unless
otherwise required for peptic ulcer disease (level 1bgrade B)
52 Isosorbide mononitrate monotherapy is not recommendedas primary prophylaxis (level 1b grade A) There is insuffi-cient evidence to recommend isosorbide mononitrate incombination with NSBB (level 1b grade A)
53 Shunt surgery or TIPSS is not recommended as primaryprophylaxis (level 1a grade A)
54 Sclerotherapy is not recommended as primary prophy-laxis (level 1a grade A)
6 Areas requiring further study61 Role of NSBB in patients without varices with focus on
carvedilol62 Role of NSBB in patients with small varices with focus
on carvedilol63 Comparison of carvedilol versus propranolol in primary
prophylaxis64 Identification of and trials assessing new drugs for
primary prophylaxis such as statins7 Quality indicator
71 Percentage of patients at diagnosis of cirrhosis who havehad an endoscopy to screen for varices (level 1agrade A)Numerator patients diagnosed with cirrhosis who havehad an endoscopy either before or after diagnosis within
6 monthsDenominator patients newly diagnosed with cirrhosis
72 Percentage of patients receiving primary prophylaxisamong those newly diagnosed with grade I varices andred signs or grade 2ndash3 varicesNumerator patients who have grade 1 varices with redsigns or grade 2ndash3 varices receiving primary prophy-laxisDenominator patients diagnosed with cirrhosis whohave grade I varices with red signs or grade 2ndash3 varices
MANAGEMENT OF ACTIVE VARICEAL HAEMORRHAGEThe average 6-week mortality of the first episode of varicealbleeding in most studies is reported to be up to 20 There hasbeen considerable improvement in survival since the early 1980swhen the in-hospital mortality was 40ndash5097 compared with15 from a recent UK audit5 Such is the improvement in out-comes that a patient with Childrsquos A cirrhosis is very unlikely tosuccumb to an index variceal bleed Studies have shown theChildndashPugh score MELD score and HVPG to be strong predic-tors of outcomes98ndash103 The MELD score has been shown tooutperform Childrsquos score in a recent study with a score gt19associated with 20 6 week mortality103 Furthermore theMELD score has been shown to perform as well as the trad-itional intensive care unit scores in predicting mortality inpatients admitted to intensive care in the UK104 MELD gt18active bleeding transfusing gt4 units of packed red blood cellshave been shown to be predictors of mortality and earlyrebleeding99 101 102 HVPG has also been shown to predictoutcome when measured at 2 weeks after a bleed44 and a valueof ge20 mm Hg when measured acutely within 48 h has beenshown to provide significant prognostic information100
However this technique is not used routinely in the manage-ment of patients around the world and substitution of clinicaldata in the latter study was shown to provide the same clinicalpredictive value100 These scoring systems are not purely aca-demic they allow the referring clinician to predict thosepatients with a high chance of rebleeding to be transferred to aspecialist centre offering for instance TIPSS before the patientrebleeds
Nonetheless probably the most important step in the man-agement of acute variceal haemorrhage is the initial resuscitationassessed according to standard lsquoABCrsquo practice together withprotection of the airway to prevent aspiration Although earlyendoscopy allows for accurate diagnosis of the bleeding site anddecisions about management (figure 3) therapeutic interventionin acute variceal bleeding can be initiated safely in most casesbefore diagnostic endoscopy As similar efficacy is demonstratedwith pharmacological treatment as with sclerotherapy theformer should be first-line therapy99 β Blockade should not bestarted in the acute setting and those already taking β blockersas prophylaxis should probably stop taking them for 48ndash72 h inorder that the patientrsquos physiological response to blood loss canbe allowed to manifest
General considerationsPatient evaluationThe majority of patients with a variceal bleed will be sufficientlystable to enable a full history and examination to take placeHistory of alcohol excess and or intravenous drug use should besought and may become particularly relevant if the patient haswithdrawal symptoms after admission Comorbidity is importantwhen estimating risk and deciding on use of vasopressors The
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 11
Guidelines
following risk factors doubled mortality after an acute varicealbleed in one US study older age comorbidities male gender andnot undergoing a gastroscopy within 24 h105
A full examination is helpful for the important negatives asmuch as the positives Baseline observations should include thetemperature as infection is a serious complication with signifi-cant mortality Confusion may be present because of encephal-opathy intoxication with alcohol or drugs or withdrawal fromalcohol or drugs The patient should be on continuous BP andpulse monitor and their haemodynamic status recordedAn oxygen saturation monitor is helpful Stigmata of chronicliver disease and concurrent jaundice provide insight into thecurrent status of a patientrsquos liver and also give warning ofpotential further decompensation if significant bleeding persists(see scoring systems above) Pneumonia must be actively
excluded Evidence of ascites requires a diagnostic tap to searchfor infection
Investigations including full blood count coagulationprofile liver and renal function and blood group and save andcross-match Blood and urine should also be cultured An ultra-sound scan later in the admission is helpful to identify subclin-ical ascites flow in portal vein and any obvious emergence of anhepatocellular carcinoma (HCC)
Location of patientA decision must be made as to where the patient is best managedVariceal bleeding is unpredictable generally occurs in patientswith significant liver disease and is associated with significant mor-tality Hence a high-dependency unit is usually the most appropri-ate initial location although a properly staffed lsquogastrointestinal
Figure 3 Algorithm for themanagement of acute varicealbleeding TIPSS transjugularintrahepatic portosystemic stent shunt
12 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleeding bedrsquo may be appropriate If a patient is vomiting bloodor there is a perceived risk of a haemodynamically unstable patienthaving blood in the stomach then the patient must be intubatedbefore endoscopy and return to an intensive care or high-dependency unit will be necessary until extubation
Volume resuscitation and blood productsIntravenous access (two 16ndash18G cannulae) should have beensecured on admission with a reported GI bleed Further intra-venous access may be necessary In patients with poor venousaccess advanced liver disease or renal failure associated withtheir liver disease central venous access may be helpful withguiding fluid infusions However the drawbacks include the riskof the procedure and a potential source of infection Thereforethere is no absolute requirement for a central line and no evi-dence of unequivocal benefit Intravenous fluid resuscitationshould be initiated with plasma expanders aiming to maintain asystolic blood pressure of 100 mm Hg Care with monitoring isparamount in this group of patients
Overtransfusion has been shown to have a deleterious effecton outcome In a recent single-centre RCT a restrictive transfu-sion policy of maintaining haemoglobin between 70 and 80 gLimproved the control of variceal bleeding (11 vs 22p=005) and lowered HVPG compared with a liberal transfu-sion policy without effect on 45-day survival106 However itshould be noted that these results were from a single Spanishcentre which was a tertiary unit for variceal bleeding where allpatients underwent endoscopy within 6 h Nonetheless arestrictive transfusion policy has been recommended for sometime1 and there is now good evidence to support not transfusinga stable patient with a haemoglobin of ge80 gL However under-resuscitation should also be avoided and while goal-orientedfluid replacement has generally not been useful in an intensivetherapy unit setting a venous saturation gt70 remains an easilymeasurable target with some evidence to support it107
Interpretation and management of clotting profile is challen-ging in liver disease where there is usually a balanced deficiencyof both procoagulant and anticoagulant factors108 The NICEguidelines recommend activation of a hospitalrsquos massive transfu-sion policy when there is major haemorrhage and plateletsupport when the value is lt50 and clotting factor supportwhen the international normalised ratio (INR) is gt15 timesnormal2 There is no evidence for the use of lsquoprophylacticrsquo clot-ting or platelet support to reduce the risk of rebleeding Thereis insufficient evidence to support the routine use of transexamicacid or recombinant factor VIIa109
Pharmacological treatmentThe two major classes of drugs that have been used in thecontrol of acute variceal bleeding are vasopressin or its analo-gues (either alone or in combination with nitroglycerine) andsomatostatin or its analogues Terlipressin is the only agent thathas been shown to reduce mortality in placebo-controlled trialsHowever in trials comparing terlipressin somatostatin andoctreotide no difference in efficacy was identified in a system-atic review110 and in a recent large RCT111 Prophylactic anti-biotics can result in a similar survival benefit following acutevariceal bleeding
VasopressinVasopressin reduces portal blood flow portal systemic collateralblood flow and variceal pressure It does however have signifi-cant systemic side effects such as an increase in peripheral resist-ance and reduction in cardiac output heart rate and coronary
blood flow In comparison with no active treatment the pooledresults of four randomised trials showed that it reduced failureto control variceal bleeding (OR=022 95 CI 012 to 043)although survival was unaffected68 Meta-analysis of five trialscomparing sclerotherapy with vasopressin has shown a signifi-cant effect on reduction in failure to control bleeding(OR=051 95 CI 027 to 097) with no effect on survival68
Vasopressin with nitroglycerineThe addition of nitroglycerine enhances the effect of vasopres-sin on portal pressure and reduces cardiovascular side effects112
Meta-analysis of three randomised trials comparing vasopressinalone with vasopressin and nitroglycerine showed that the com-bination was associated with a significant reduction in failure tocontrol bleeding (OR=039 95 CI 022 to 072) although nosurvival benefit was shown68
TerlipressinTerlipressin is a synthetic analogue of vasopressin which has animmediate systemic vasoconstrictor action followed by portalhaemodynamic effects due to slow conversion to vasopressin Ina Cochrane meta-analysis of seven placebo-controlled trials ter-lipressin was shown to reduce failure to control bleeding(RR=066 95 CI 055 to 093) and also to improve survival(RR=066 95 CI 049 to 088)113 In the same meta-analysisthere was no difference between terlipressin versus vasopressinballoon tamponade or endoscopic therapy in failure to controlbleeding or survival113 The role of terlipressin in combinationwith VBL is explored in the section lsquoEndoscopic therapy incombination with pharmacological therapyrsquo
The recommended dose of terlipressin is 2 mg IV every 4 halthough many units reduce the dose to 6 hourly as it may causeperipheral vasoconstriction which manifests as painful handsand feet While 5 days of IV treatment has been advocated inthe Baveno V guidelines1 this prolonged treatment has notbeen shown to have a survival benefit and for pragmaticreasons many units will stop treatment shortly after satisfactoryhaemostasis In a randomised trial terlipressin given for 24 hafter satisfactory haemostasis with VBL after oesophageal vari-ceal bleeding was as effective as 72 h of treatment114
In patients intolerant of terlipressin or in countries where ter-lipressin is not available alternatives should be considered
Somatostatin and octreotideSomatostatin causes selective splanchnic vasoconstriction andreduces portal pressure and portal blood flow115 Octreotide is asomatostatin analogue The mechanism of action of these twoagents is not clear Inhibition of glucagon increases vasodilatationrather than a direct vasoconstrictive effect and post-prandial guthyperaemia is also reduced The actions of octreotide on hepaticand systemic hemodynamics are transient making continuousinfusion necessary Octreotide is given as a 50 μg bolus followedby an infusion of 25ndash50 μgh Somatostatin is given as a 250 mgintravenous bolus followed by an infusion of 250 mghSomatostatin and octreotide have been shown to be aseffective as terlipressin in acute variceal bleeding in ameta-analysis110 Seo et al111 in a large RCTof 780 patients com-paring these three agents failed to show a difference in treatmentsuccess (range 838ndash862) rebleeding (range 34ndash44) andmortality (range 8ndash88) A low systolic blood pressure at pres-entation high serum creatinine level active bleeding in the emer-gency endoscopy gastric variceal bleeding and ChildndashPugh gradeC were independent factors predicting 5-day treatmentfailure111
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 13
Guidelines
AntibioticsAntibiotics that provide Gram-negative cover are one of the inter-ventions which positively influence survival in variceal haemor-rhage as shown in a Cochrane meta-analysis of 12placebo-controlled trials (RR=079 95 CI 063 to 098)116
Antibiotics were also shown to reduce bacterial infections(RR=043 95 CI 019 to 097) and early rebleeding (RR=05395 CI 038 to 074)116 Therefore short-term antibiotics shouldbe considered standard practice in all cirrhotic patients who have avariceal bleed irrespective of the presence of confirmed infectionThird-generation cephalosporins such as ceftriaxone (1 g IVdaily) have been shown to be more effective at reducingGram-negative sepsis than oral norfloxacin117 but choice of anti-biotics must be dictated by local resistance patterns and availability
Proton pump inhibitorsOne RCT compared a short course of proton pump inhibitorswith vasoconstrictor therapies after haemostasis in acute varicealbleeding118 Despite larger ulcers noted in the vasoconstrictorarm there were no differences in bleeding or survival Nearly50 of patients had ascites which might have implications inlight of the reports of increased incidence of spontaneous bac-terial peritonitis as mentioned earlier
Endoscopic therapyEndoscopy should take place within 24 h of admission andearlier if there is excessive bleeding based on low-level evi-dence105 While many guidelines and reviews suggest thatendoscopy should be carried out within 12 h the only study thatexamined the influence of timing on outcome failed to demon-strate any advantage of endoscopy before 12 h119 The optimaltime is after sufficient resuscitation and pharmacological treat-ment with the endoscopy performed by a skilled endoscopyteam in a suitably equipped theatre environment and withairway protection Airway protection is essential where risk ofaspiration is high and affords the endoscopist time for thoroughevaluation including complete clot aspiration and controlledapplication of treatment including tamponade if required Theendoscopy team must comprise an experienced endoscopynurse acquainted with the equipment necessary for endoscopytherapy of varices and a skilled endoscopist competent in usingbanding devices and deployment of balloon tamponade
Variceal band ligationThis technique is a modification of that used for the elastic bandligation of internal haemorrhoids Its use in humans was firstdescribed in 1988120 A meta-analysis of seven trials comparingVBL with sclerotherapy in acute bleeding showed that VBLreduced rebleeding from varices (OR=047 95 CI 029 to078) reduced mortality (OR=067 95 CI 046 to 098) andresulted in fewer oesophageal strictures (OR=010 95 CI003 to 029)121 The number of sessions required to obliteratevarices was lower with VBL (22 fewer sessions (95 CI 09to 35))
SclerotherapySclerotherapy has been replaced by VBL and should no longerbe offered as standard of care in acute variceal haemorrhage
Other endoscopic measuresIn an RCT cyanoacrylate offered no benefit over VBL with theadditional risk of embolisation and trend towards increasedrebleeding with cyanoacrylate122
Haemostatic powder (TC-325 Hemospray Cook MedicalUSA) has been described in a small study of nine patients whoreceived endoscopic spray treatment for acute variceal bleedingThe study reported no rebleeding within 24 h and no mortalityat 15 days123
Endoscopic therapy in combination with pharmacological therapyThe role of combining vasoactive drugs with endoscopictherapy (VBL or sclerotherapy) was reported in a meta-analysisof eight trials124 Combination therapy resulted in better initialcontrol of bleeding (RR=112 95 CI 102 to 123) and5-day haemostasis (RR=128 95 CI 118 to 139) withoutany difference in survival Adverse events were similar in bothgroups Two RCTs have compared VBL with sclerotherapy incombination with vasoactive agents in acute variceal bleed-ing125 126 Lo et al125 used vasopressin and found that VBLresulted in better 72 h haemostasis (97 vs 76 p=0009)with fewer complications (5 vs 29 p=0007) Villanuevaet al used somatostatin and reported lower failure to controlacute bleeding with VBL (4 vs 15 p=002) with fewerserious complications (4 vs 13 p=004) Overall survivalwas similar in both trials125 126
Balloon tamponadeBalloon tamponade is highly effective and controls acute bleed-ing in up to 90 of patients although about 50 rebleed whenthe balloon is deflated127 128 It is however associated withserious complications such as oesophageal ulceration and aspir-ation pneumonia in up to 15ndash20 of patients Despite this itmay be a life-saving treatment in cases of massive uncontrolledvariceal haemorrhage pending other forms of treatment Anappropriately placed SengstakenndashBlakemore tube allows forresuscitation safe transportation and either repeat endoscopy orradiological shunting in a patient with a stable cardiovascularsystem The oesophageal balloon is rarely required must neverbe used on its own and should be used only if there is continu-ing bleeding despite an adequately inflated gastric balloon cor-rectly placed and with appropriate tension Placement of thetube endoscopically or over a guide wire might reduce the riskof complications especially oesophageal rupture
Removable oesophageal stentsThe SX-Ella Danis stent (ELLA-CS Hradec Kralove CzechRepublic) is a removable covered metal mesh stent placed endo-scopically in the lower oesophagus without radiological screen-ing It has no role in the management of gastric varicealbleeding These stents can be left in situ for up to 2 weeksunlike the SengstakenndashBlakemore tube which should beremoved after a maximum of 24ndash48 h129 130 No published con-trolled trials have compared this modality with balloontamponade
Transjugular intrahepatic portosystemic stent-shuntSeveral uncontrolled studies have examined the role of salvagebare TIPSS in acute variceal bleeding In a review of 15 studiescontrol of bleeding was achieved in 90ndash100 with rebleedingin 6ndash16131 Mortality varied between 75 (in hospital) and15 (30 day) It is important to appreciate that sclerotherapywas used as first-line endoscopic therapy in most of thesestudies Long-term follow-up of a study that compared TIPSSwith H-graft portacaval shunts in patients for whom non-operative management had failed suggested that H-grafts were auseful method of reducing portal pressure and had a signifi-cantly lower failure rate (p=004) but had no significant
14 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
improvement in overall survival despite a benefit seen in ChildrsquosA and B disease132 A recent RCT compared emergency porto-caval surgery with bare TIPSS within 24 h of presenting withacute oesophageal variceal bleeding in unselected cirrhoticpatients Emergency portocaval surgery resulted in better out-comes for long-term bleeding control encephalopathy and sur-vival (plt0001)133 Before wider application of surgery foracute variceal bleeding more data are needed in light of therecent adoption of covered stents
There has also been a generalised established change in prac-tice in using covered TIPSS stents (polytetrafluoroethylene(PTFE)) rather than a bare metal stent with evidence to supportthis change In randomised controlled studies these stents wereshown to have higher primary patency rates than bare stentswithout significant differences in survival and the potential forreduced incidence of hepatic encephalopathy134 135
There is however growing evidence from two RCTs for theearlier use of TIPSS in selected patients stratified by HVPGChildndashPugh class and active bleeding and not just use as asalvage option6 136 Monescillo et al136 randomised patientspresenting with acute oesophageal variceal haemorrhage to bareTIPSS or standard of care if the HVPG was ge20 mm Hg within24 h of admission Significantly reduced treatment failure asdefined by failure to control acute bleeding andor early rebleed-ing (12 vs 50) was seen and improved survival (62 vs35) in the patients randomised to undergo a TIPSS procedureHowever the standard of care was sclerotherapy and not com-bination endoscopic and pharmacological treatment This limita-tion and the lack of availability of HVPG measurement in mostcentres meant this trial did not have a significant impact on clin-ical practice
Garcia-Pagan et al6 selected patients with active bleeding andChildrsquos B cirrhosis or patients with Childrsquos C cirrhosis (Childrsquosscore lt14) for randomisation to early PTFE-covered TIPSSwithin 72 h or standard of care with VBL and pharmacologicaltreatment This has shown encouraging results with reduced riskof treatment failure (3 vs 50) improved survival (86 vs61 at 1 year) yet without increased risk of hepatic encephal-opathy The results were supported by an observational studyfrom the same group although a survival benefit was notseen137 Furthermore a recent well-conducted observationalstudy did not demonstrate such high survival rates with earlyTIPSS with 11-year survival of 67 which was similar to thatof patients given endoscopic and pharmacological treatmentsonly138 Therefore larger multicentred RCTs need to be under-taken to further evaluate the role of early TIPSS It is importantto make the distinction between salvage TIPSS and early TIPSSto prevent rebleeding
Liver transplantationThis is probably appropriate only for patients who bleed whileawaiting liver transplantation although studies comparing VBLor TIPSS placement with urgent liver transplantation in thissituation need to be done Liver transplantation is an exceed-ingly rare option for the vast majority of patients both becauseit is not commonly available and because of shortages anddelays in organ procurement No controlled trials of liver trans-plantation in uncontrolledactive bleeding are available
Recommendations for the control of variceal bleeding in cir-rhosis are given below and in figure 3
Recommendations control of active variceal haemorrhage incirrhosis (figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with bloodplatelets and clotting factors in line with local protocolsfor managing massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusionpolicy aiming for a haemoglobin of 70ndash80 gL is sug-gested in haemodynamically stable patients (level 1bgrade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable(level 5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L(level 5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to localcircumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with suspected
or confirmed variceal bleeding (level 1a grade A)32 In all patients vasoconstrictors such as terlipressin or
somatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 15
Guidelines
41 If bleeding is difficult to control a SengstakenndashBlakemore tube should be inserted until further endo-scopic treatment TIPSS or surgery is performed depend-ing on local resources and expertise (level 1b grade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure (level1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
SECONDARY PROPHYLAXIS OF VARICEAL HAEMORRHAGEβ BlockersA meta-analysis of 12 trials comparing propranolol or nadolol139
with no active treatment showed a significant reduction inrebleeding but no significant reduction in mortality140 Thegreater reduction in portal pressure with carvedilol comparedwith propranolol has been described in the section lsquoPrimaryprophylaxisrsquo of this guideline
NitratesThe addition of ISMN to NSBB has been shown to reduce vari-ceal rebleeding compared with NSBB alone although no sur-vival benefit was seen141 In addition adverse events leading todrug withdrawal were more common in the group receivingcombined drug treatment A meta-analysis of ISMN alone orwith either NSBB or endoscopic therapy reported that there wasno mortality benefit from combining nitrates and NSBB com-pared with NSBB alone142
Side effects of ISMN include dizziness and headache Owingto the side effects and relative lack of data ISMN is not com-monly used in clinical practice
A recent RCT of 121 patients reported carvedilol to besimilar to combined ISMN and NSBB therapy in the preventionof variceal rebleeding and mortality although severe adverseevents were less common with carvedilol143
SimvastatinA recent abstract of a multicentre RCT of 158 patients reporteda survival benefit (91 vs 78 p=003) from adding simvasta-tin to VBL and NSBB compared with placebo VBL and NSBBas treatment for the prevention of variceal rebleeding144 Therewas no difference in rebleeding and the survival benefit wasrestricted to Child A and B patients Serious adverse events weresimilar in both groups More data are required to investigatethis interesting observation of a survival benefit from simvastatinin this situation which may relate to its effects on hepatocellularfunction fibrosis and portal pressure
Proton pump inhibitorsA double-blind randomised placebo-controlled trial showed thatpantoprazole reduced the size of ulcers in patients who under-went VBL However the total number of ulcers and other out-comes were similar in the two groups145
Endoscopic therapyVBL has been accepted as the preferred endoscopic treatmentfor the prevention of variceal rebleeding with a lower rate ofrebleeding mortality and complications than sclerother-apy146 147 The time interval between VBL sessions to achieveeradication of varices is debateable However a recent RCTcomparing monthly with biweekly VBL after initial haemostasiswith VBL in 70 patients suggested that there were fewerpost-VBL ulcers in the monthly group (11 vs 57plt0001)148 Variceal recurrence rebleeding and mortality weresimilar in both groups
Two meta-analyses showed there is no evidence that the add-ition of sclerotherapy to VBL improves clinically relevant out-comes including variceal rebleeding and death and thecombination led to higher stricture rates149 150
Endoscopic therapy versus drug therapyVBL has been reported to be more effective than combinedNSBB and ISMN drug therapy151 However an 8-yearfollow-up study of this RCT found that although VBL wassuperior in reducing variceal rebleeding survival rates were sig-nificantly higher in the group treated with combined drug treat-ment152 Other studies have found no superiority of VBL overcombined drug therapy for prevention of variceal rebleeding ormortality153 154 A recent small multicentre RCT reported carve-dilol to be similar to VBL in the prevention of variceal rebleed-ing with a trend in favour of survival with carvedilol (73 vs48 p=0110)155
Several meta-analyses have compared drug therapy with VBLin the prevention of variceal rebleeding One meta-analysis ofsix RCTs showed no significant difference in variceal rebleedingrates when comparing VBL alone with combined NSBB andISMN therapy However all-cause mortality was significantlyhigher in patients treated with the VBL (RR=125 95 CI101 to 155)156 Three meta-analyses comparing drug therapy(NSBB alone or with ISMN) with endoscopic therapy alonereported no difference in variceal rebleeding or mortality157ndash159
Endoscopic+drug therapy versus either aloneNumerous studies and several meta-analyses have comparedcombined endoscopic and drug therapy with monotherapy(endoscopic or drugs alone) in the prevention of varicealrebleeding A meta-analysis of 23 trials assessing sclerotherapyor VBL combined with NSBB reported that combinationtherapy reduced rebleeding more than either endoscopic
16 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

administered in only 27 of patients before endoscopy andadministration of vasoactive drugs before endoscopy was onlyslightly higher at 44 Furthermore only four patients (lt1)were referred for TIPSS which may reflect the lack of accessto interventional radiology and that the audit was conductedbefore the trial of early TIPSS6 The National ConfidentialEnquiry into Patient Outcome and Death (NCEPOD) reportlsquoMeasuring the unitsrsquo assessed clinical management beforedeath of 594 patients with alcoholic liver disease over a6-month period in the UK7 Gastrointestinal bleeding wasnoted in 35 of cases with approximately 50 having vari-ceal bleeding Delays in endoscopy were noted in 10 ofcases and several aspects of clinical andor organisational carewere judged to be poor or unacceptable in 18 of patientspresenting with GI bleeding There were deficiencies noted inthe out-of-hours rotas for GI bleeding with 27 of hospitalsnot having a dedicated-out-of hours GI bleeding serviceStudies from other countries have also reported deficiencieswith delays in admission to hospital and administration of anti-biotics Two observational studies showed that access to
emergency endoscopy and use of prophylactic antibiotics andvasoactive drugs was better in tertiary centres although thisdid not appear to affect survival8 9
Acute variceal haemorrhage refractory to endoscopic andpharmacological treatments where TIPSS is usually indicatedmust be managed with appropriate resources TIPSS is an estab-lished interventional treatment for refractory or recurrent vari-ceal haemorrhage It remains a highly specialised procedurerequiring adequate training and experience Knowledge of therelevant equipment anatomy and how to deal with any compli-cations is essential It should therefore be performed in centreswith adequate personnel multidisciplinary support and equip-ment required to optimise management and minimise risks10
Regional centres with easily accessible interventional radiologyservices are generally best equipped to perform this procedureSetting up regional agreements and pathways to allow transfer ofappropriate patients to hospitals that undertake TIPSS proce-dures is an important step These pathways could also be used toprovide emergency endoscopic management if necessary due toproblems with out-of-hours endoscopic cover in smaller
Table 1 Levels of evidence
LevelTherapyprevention aetiologyharm Prognosis Diagnosis DDXsymptom prevalence study
1a SR (with homogeneity) ofrandomised controlled trial (RCT)
SR (with homogeneity) of inceptioncohort studies CDRdagger validated indifferent populations
SR (with homogeneity) of level 1diagnostic studies CDRdagger with 1b studiesfrom different clinical centres
SR (with homogeneity) ofprospective cohort studies
1b Individual RCT (with narrow CI) Individual inception cohort study withge80 follow-up CDRdagger validated in asingle population
ValidatingDagger cohort study with goodsectreference standards or CDRdagger testedwithin one clinical centre
Prospective cohort study with goodfollow-uppara
1c All or none All or none case series Absolute SpPins and SnNoutsdaggerdagger All or none case series2a SR (with homogeneity) of cohort
studiesSR (with homogeneity) of eitherretrospective cohort studies or untreatedcontrol groups in RCTs
SR (with homogeneity) of level gt2diagnostic studies
SR (with homogeneity) of 2b andbetter studies
2b Individual cohort study (includinglow-quality RCT eg lt80follow-up)
Retrospective cohort study or follow-upof untreated control patients in an RCTderivation of CDRdagger or validated on splitsampleDaggerDagger only
ExploratoryDagger cohort study with goodsectreference standards CDRdagger afterderivation or validated only on splitsampleDaggerDagger or databases
Retrospective cohort study or poorfollow-up
2c lsquoOutcomesrsquo research ecologicalstudies
lsquoOutcomesrsquo research Ecological studies
3a SR (with homogeneity) of casendashcontrol studies
SR (with homogeneity) of 3b and betterstudies
SR (with homogeneity) of 3b andbetter studies
3b Individual casendashcontrol study Non-consecutive study or withoutconsistently applied reference standards
Non-consecutive cohort study orvery limited population
4 Case series (and poor qualitycohort and case-control studiessectsect)
Case series (and poor quality prognosticcohort studiesparapara)
Casendashcontrol study poor ornon-independent reference standard
Case series or superseded referencestandards
5 Expert opinion without explicitcritical appraisal or based onphysiology bench research or lsquofirstprinciplesrsquo
Expert opinion without explicit criticalappraisal or based on physiology benchresearch or lsquofirst principlesrsquo
Expert opinion without explicit criticalappraisal or based on physiology benchresearch or lsquofirst principlesrsquo
Expert opinion without explicitcritical appraisal or based onphysiology bench research or lsquofirstprinciplesrsquo
Homogeneity means a systematic review (SR) that is free of worrisome variations (heterogeneity) in the directions and degrees of results between individual studies Not all SRs withstatistically significant heterogeneity need be worrisome and not all worrisome heterogeneity need be statistically significantdaggerCDR Clinical Decision Rule (algorithms or scoring systems which lead to a prognostic estimation or a diagnostic category)DaggerValidating studies test the quality of a specific diagnostic test based on prior evidence An exploratory study collects information and trawls the data (eg using a regression analysis) tofind which factors are lsquosignificantrsquosectGood reference standards are independent of the test and applied blindly or objectively to all patients Poor reference standards are haphazardly applied but still independent of thetest Use of a non-independent reference standard (where the lsquotestrsquo is included in the lsquoreferencersquo or where the lsquotestingrsquo affects the lsquoreferencersquo) implies a level 4 studyparaGood follow-up in a differential diagnosis study is gt80 with adequate time for alternative diagnoses to emerge (eg 1ndash6 months acute 1ndash5 years chronic)Met when all patients died before the treatment became available but some now survive while receiving it or when some patients died before the treatment became available butnone now die while receiving itdaggerdaggerAn lsquoabsolute SpPinrsquo a diagnostic finding whose Specificity is so high that a Positive result rules in the diagnosis An lsquoAbsolute SnNoutrsquo a diagnostic finding whose Sensitivity is sohigh that a Negative result rules out the diagnosisDaggerDaggerSplit-sample validation is achieved by collecting all the information in a single tranche then artificially dividing this into lsquoderivationrsquo and lsquovalidationrsquo samplessectsectPoor quality cohort study one that failed to clearly define comparison groups andor failed to measure exposures and outcomes in the same (preferably blinded) objective way inboth exposed and non-exposed individuals andor failed to identify or appropriately control known confounders andor failed to carry out a sufficiently long and complete follow-up ofpatients Poor quality casendashcontrol study one that failed to clearly define comparison groups andor failed to measure exposures and outcomes in the same (preferably blinded)objective way in both cases and controls andor failed to identify or appropriately control known confoundersparaparaPoor quality prognostic cohort study one in which sampling was biased in favour of patients who already had the target outcome or the measurement of outcomes wasaccomplished in lt80 of study patients or outcomes were determined in an unblinded non-objective way or there was no correction for confounding factors
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 5
Guidelines
hospitals This model referred to as ldquospoke and wheelrdquo ornetwork model is well established for other complex proceduresand helps to expedite and streamline the process In theNCEPOD report lsquoMeasuring the unitsrsquo just 15 of hospitals hadon-site access to TIPSS while 72 had access to TIPSS in othercentres7
There have been significant efforts to address the need toimprove the upper GI bleeding (UGIB) service A toolkit wasproduced in collaboration with BSG Association of UpperGastrointestinal Surgeons (AUGIS) Royal Colleges ofPhysicians Radiology and Nursing and Academy of MedicalRoyal Colleges11 The key nine service standards recommendedby the document are detailed below1 There will be a nominated individual with the authority to
ensure implementation by the contracted provider2 Contracted providers will ensure the minimum service is
adequately resourced3 All patients with suspected UGIB should be properly
assessed and their risk scored on presentation4 All patients should be resuscitated before therapeutic
intervention5 All high-risk patients with UGIB should be endoscoped
within 24 h preferably on a planned list in the first instance6 For patients who require more urgent intervention either for
endoscopy interventional radiology or surgery formal 247arrangements must be available
7 The necessary team meeting an agreed competency levelshould be available throughout the complete patient pathway
8 Each stage of the patient pathway should be carried out inan area with lsquoappropriatersquo facilities equipment and supportincluding staff experienced in the management of UGIB
9 All hospitals must collect a minimum dataset in order tomeasure service provision against auditable outcomes(case-mix adjusted as appropriate)NICE recommendations for endoscopy provision are detailed
in the section lsquoManagement of active variceal haemorrhagersquorecommendations2 The BSG has also produced a care bundlefor patients admitted with decompensated cirrhosis in light ofthe NCEPOD report with a check list method which includesgastrointestinal bleeding12
Since the 2008 Darzi report quality has become a priorityfor the NHS13 With these guidelines there is real opportunityto introduce quality outcomes based on good clinical evidenceFurthermore by incorporating them into the liver accreditationscheme Liver Quest one can improve and assure quality inliver services across the UK14 Therefore a small number ofquality outcomes measures have been chosen and form part ofthe key recommendations15
DEFINITIONSIt is important to define the terms that should be used in thecontext of a variceal bleed These are the Baveno V consensusdefinitions1
Variceal haemorrhageVariceal haemorrhage is defined as bleeding from an oesopha-geal or gastric varix at the time of endoscopy or the presence oflarge oesophageal varices with blood in the stomach and noother recognisable cause of bleeding An episode of bleeding isclinically significant when there is a transfusion requirement for2 units of blood or more within 24 h of the time zero togetherwith a systolic blood pressure of lt100 mm Hg or a posturalchange of gt20 mm Hg andor pulse rate gt100 bpm at time
zero (time zero is the time of admission to the first hospital towhich the patient is taken)
Time frame of acute bleedingThe acute bleeding episode is represented by an interval of120 h (5 days) from time zero Evidence of any bleeding after120 h is the first rebleeding episode
Failure to control active bleedingFailure to control active bleeding is defined as death or need tochange treatment defined by one of the following criteria16 17
1 Fresh haematemesis or nasogastric aspiration of ge100 mL offresh blood ge2 h after the start of a specific drug treatmentor therapeutic endoscopy
2 Development of hypovolaemic shock3 30 gL drop in haemoglobin (9 drop of haematocrit)
within any 24 h period if no transfusion is given This timeframe needs to be further validated
Variceal rebleedingVariceal rebleeding is defined as the occurrence of a singleepisode of clinically significant rebleeding from portal hyperten-sive sources from day 5 Clinically significant rebleeding isdefined as recurrent melaena or haematemesis in any of the fol-lowing settings1 hospital admission2 blood transfusion3 30 gL drop in haemoglobin4 death within 6 weeks
Early mortalityDeath within 6 weeks of the initial episode of bleeding
NATURAL HISTORY OF VARICES IN CIRRHOSISDevelopment of varicesThe rise in portal pressure is associated with the developmentof collateral circulation which allows the portal blood to bediverted into the systemic circulation These spontaneous shuntsoccur (a) at the cardia through the intrinsic and extrinsic gastro-oesophageal veins (b) in the anal canal where the superiorhaemorrhoidal vein belonging to the portal system anastomoseswith the middle and inferior haemorrhoidal veins which belongto the caval system (c) in the falciform ligament of the liverthrough the para-umbilical veins which are the remains of theumbilical circulation of the fetus (d) in the abdominal wall andthe retroperitoneal tissues from the liver to the diaphragmveins in the lienorenal ligament in the omentum and lumbarveins and (e) blood diversion from the diaphragm gastric pan-creatic splenic and adrenal veins which may drain into the leftrenal vein
Numerous lines of evidence suggest that varices develop andenlarge with time Christensen et al18 followed up a cohort of532 patients with cirrhosis and showed that the cumulative inci-dence of patients with varices increased from 12 to 90 over12 years In a study involving 80 patients followed up for16 months Cales and Pascal19 showed that 20 of patientswho did not have varices developed new varices and 42 ofpatients with small varices showed definite enlargement Czajaet al20 also showed that the prevalence of varices increased from8 to 13 over 5 years in a cohort of patients with chronicactive hepatitis even though they were treated with prednisol-one Merli et al21 in a study of 213 patients with cirrhosis withno or small varices demonstrated that the annual progression ofvarices was 12 A recent database analysis by DrsquoAmico et al22
6 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
using a competing risk model showed that the cumulative inci-dence of varices at 10 and 20 years was 44 and 53 respect-ively suggesting an overestimation in previous studies not usinga competing risk model
The main factors that appear to determine the developmentof varices are continued hepatic injury the degree of portosyste-mic shunting endoscopic appearances and portal pressureEvidence for the role of hepatic injury is derived from studies inwhich varices were shown to regress with time Baker et al23 fol-lowed up a cohort of 115 patients with oesophageal varices andshowed that varices had disappeared in nine patients regressedin seven and remained unchanged in six They concluded thatthe disappearance and regression of varices might be related toabstinence from alcohol This observation was confirmed in astudy by Dagradi24 who followed up a cohort of patients withalcoholic cirrhosis over 3 years and showed a reduction in vari-ceal size in 12 of the 15 patients with alcoholic cirrhosis whostopped drinking and an enlargement in variceal size in 17patients who continued to drink On the other hand Cales andPascal19 showed that regression of varices occurred in 16 ofpatients with alcoholic cirrhosis who continued to imbibealcohol This might be related to the development of large por-tosystemic collaterals which decompress the portal system andreduce the risk of the development of large oesophageal varicesThe degree of portosystemic shunting can be quantified bymeasuring the diameter of portal veins and collaterals and canbe significant in those with gastrorenal or splenorenal shunt-ing25 26 Others have shown that the presence of alcoholic cir-rhosis Childrsquos B or C cirrhosis and red whale signs on indexendoscopy predicted progression of varices21 Groszmannet al27 in a placebo-controlled randomised trial of timolol in213 cirrhotic patients without varices showed that a baselinehepatic venous pressure gradient (HVPG) of gt10 mm Hg or age10 increase in HVPG during follow-up were both predictiveof the development of varices
Diagnosis of gastro-oesophageal varicesUntil recently endoscopy has been used exclusively to diagnosevarices Non-invasive methods of screening for varices includecapsule endoscopy transient elastography and use of laboratoryand radiological findings
EndoscopyThere is universal acceptance that endoscopy is the lsquogold stand-ardrsquo for diagnosing gastro-oesophageal varices The main limita-tions are intraobserver variability in the diagnosis of small orgrade I oesophageal varices (figure 1AndashC) Recently unsedatednasal gastroscopy has been found to have similar accuracy toconventional endoscopy and has the advantage of tolerabilityand potential cost saving since it can be performed in the clinicsetting in some institutions28 29 However there are no con-trolled studies and banding of varices is not possible
Capsule endoscopyCapsule endoscopy uses a 26 mm pill-shaped device whichtransmits video footage which is stored and later analysedPatients are not sedated but patient cooperation is essentialIn a large study by de Franchis et al30 capsule endoscopy wascompared with standard gastroscopy The primary end point of90 or greater concordance was not achieved Lapalus et al31
in a prospective study of 120 patients demonstrated similarresults with capsule endoscopy Therefore capsule endoscopycannot be considered an alternative to standard endoscopyalthough may have a role in patient who refuse gastroscopy
Transient elastographyTransient elastography ((FibroScan Echosens Paris France) usesthe principles of ultrasound to derive tissue stiffness by measur-ing the speed of propagation of a low-frequency wave whichthen correlates with liver fibrosis Vizzutti et al32 in a study of61 patients with hepatitis C showed a sensitivity for predictionof oesophageal varices of 90 using a threshold 176 kPaHowever specificity was poor at 43 A study of 298 patientsfound the optimal cut-off point for the prediction of oesopha-geal varices was 215 kPa (sensitivity 76 and specificity78)33 In one uncontrolled study the use of transient elasto-graphy was found to be as effective as HVPG at predictingportal hypertension-related complications34 Therefore the roleof transient elastography in predicting varices is controversialdue to the lack of consistent results and controlled studies Thismodality may be more useful for predicting decompensation inpatients with cirrhosis
Radiological and serum parametersA prospective study of 311 patients with chronic hepatitis Cshowed that a platelet-to-spleen size ratio with a threshold of909 had positive and negative predictive values of 100 and94 respectively35 These good results have not been repro-duced by others as demonstrated in a meta-analysis36
Risk factors for first variceal bleedingThe factors that predispose to and precipitate variceal haemor-rhage are still not clear The suggestion that oesophagitis mayprecipitate variceal haemorrhage has been discarded37
Presently the most important factors that have been heldresponsible include (i) pressure within the varix (ii) varicealsize (iii) tension on the variceal wall and (iv) severity of theliver disease
Portal pressureIn most cases portal pressure reflects intravariceal pressure38
and a HVPG gt10 mm Hg is necessary for the development ofoesophageal varices27 There is no linear relationship betweenthe severity of portal hypertension and the risk of varicealhaemorrhage although HVPG gt12 mm Hg is an accepted
Figure 1 (A) Grade I oesophagealvarices These collapse to inflation ofthe oesophagus with air (B) Grade IIoesophageal varices These are varicesbetween grades 1 and 3 (C) Grade IIIoesophageal varices These are largeenough to occlude the lumen
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 7
Guidelines
threshold for variceal bleeding39 40 However the HVPG tendsto be higher in bleeders as well as in patients with larger varicesIn a prospective study comparing propranolol with placebo forthe prevention of first variceal haemorrhage Groszmann et al41
showed that bleeding from varices did not occur if the portalpressure gradient (PPG) could be reduced to lt12 mm HgOthers have shown that a 20 reduction in portal pressure pro-tects against further bleeding42 These haemodynamic goalshave been accepted as the aim of pharmacological treatment ofportal hypertension It is important to appreciate that gastricvarices can bleed at pressures lt12 mm Hg and the influence ofwall tension of the varix plays a greater role in the risk of bleed-ing43 A greater pressure reduction may be necessary to protectagainst bleeding This is further discussed in the section lsquoGastricvaricesrsquo At present measurement of portal pressure in guidingpharmacological treatments is limited to clinical trials in the UK
Variceal sizeVariceal size is best assessed endoscopically (figure 1AndashC)Published results are variable owing to the lack of a definition dis-tinguishing between large and small varices Small (grade I)varices tend to be narrow and flatten easily with air whereaslarger (grade 2 and 3) varices are usually broader and flatten withdifficulty if at all Numerous studies40 44 have shown that therisk of variceal haemorrhage increases with the size of varices45
Variceal wall and tensionPolio and Groszmann46 using an in vitro model showed thatrupture of varices was related to the tension on the varicealwall The tension depends on the radius of the varix In thismodel increasing the size of the varix and decreasing the thick-ness of the variceal wall caused variceal rupture Recently endo-scopic ultrasound and manometry have been used to estimatewall tension of varices47
Endoscopic features such as lsquored spotsrsquo and lsquowhalersquo markingswere first described by Dagradi24 They have been described asbeing important in the prediction of variceal haemorrhageThese features represent changes in variceal wall structure andtension associated with the development of microtelangiectasiasand reduced wall thickness In a retrospective study by theJapanese Research Society for Portal Hypertension Beppuet al48 showed that 80 of patients who had blue varices orcherry red spots bled from varices suggesting that this was animportant predictor of variceal haemorrhage in cirrhosis
Severity of liver disease and bleeding indicesTwo independent groups prospectively assessed factors predict-ing first variceal haemorrhage in cirrhosis (table 2) The NorthItalian Endoscopic Club (NIEC)49 reported their findings in1988 followed in 1990 by data from the Japanese50 Both thesestudies showed that the risk of bleeding was based on threefactors severity of liver disease as measured by Child class vari-ceal size and red wale markings The NIEC study showed awide range for the risk of bleeding of 6ndash76 depending on thepresence or absence of the different factors Using the same vari-ables the NIEC index was simplified by de Franchis et al51 andshown to correlate with the original index Further studiesshowed that the HVPG and intravariceal pressure were alsoindependent predictors of first variceal haemorrhage when ana-lysed in conjunction with the NIEC index52 53
In summary the most important factors that determine the risk ofvariceal haemorrhage are the severity of liver disease size of varicesand presence of red signs Measurement of HVPG is a useful guidefor selection of patients for treatment and their response to
treatment although the predictive value does not appear toimprove on the NIEC index and presence of red whale marking54
Risk and mortality of first variceal bleedData describing the overall risk of bleeding from varices must beviewed with caution and have some pitfalls in interpretationThe natural history of patients who have varices that are diag-nosed as part of their baseline investiations is different fromthat of patients who have complications of liver disease such asascites and encephalopathy Most studies do not comment oneither the severity of liver disease or whether patients with alco-holic cirrhosis are continuing to drink Both these factors have asignificant effect on the risk of variceal haemorrhage
Most studies report bleeding from varices in about 20ndash50of patients with cirrhosis during the period of follow-up Bakeret al23 reported variceal bleeding in 33 of 115 patients that theyfollowed up for a mean of 33 years with a mortality of 48from the first variceal haemorrhage These data were confirmedby Christensen et al18 About 70 of the episodes of bleedingoccur within 2 years of diagnosis Recent studies demonstrate adramatic reduction in mortality following variceal bleeding of20 6-week mortality55 and 15 in-hospital mortality5 withcontributions from improved endoscopic pharmacological andradiological therapies notably TIPSS Intensive care treatmenthas also improved with outcomes being particularly good forthose requiring minimal organ support
Analysis of the non-active treatment arms in the primaryprophylaxis trials comparing propranolol with placebo showresults similar to those of the primary prophylaxis shunt trialswith most episodes of bleeding occurring within the first 2 yearsof follow-up In these studies the rate of first variceal haemor-rhage ranged from 22 to 6156ndash60 This large difference inthe rate of first bleed relates almost certainly to the number ofpatients with severe liver disease included in the study (PascalChild Cmdash46 bleedingmdash61 Italian Multicenter Project forPropranolol in Prevention of Bleeding (IMPP) Child Cmdash6bleedingmdash32 Conn Child Cmdash6 bleedingmdash22)Mortality varied from 24 to 49 over 2 years (Pascal mortal-itymdash49 IMPP mortalitymdash24 Conn mortalitymdash24)
Primary prophylaxisSince 30ndash50 of patients with portal hypertension will bleedfrom varices and about 20 will die from the effects of the first
Table 2 Scoring systems for quantifying the severity of cirrhosisSeverity of liver disease can be described using the ChildndashPughscore or MELD scoreThe ChildndashPugh score is the sum of severity scores for Child classvariceal size and red wale markings the variables shown below
Category 1 2 3
Encephalopathy 0 III IIIIVAscites Absent Mild-moderate SevereBilirubin (μmolL) lt34 34ndash51 gt51Albumin (gL) gt35 28ndash35 lt28INR lt13 13ndash15 gt15
ChildndashPugh class A represents a score of le6 class B a score of 7ndash9 and class C ge10The MELD score is a formula that includes three laboratory-based variables reflectingthe severity of liver disease It was originally used to predict the short-term mortalityafter placement of a transjugular intrahepatic portosystemic stent-shunt for varicealbleeding Subsequently it has been used in selecting candidates for livertransplantationMELD score please use the online calculator httpswwwesotorgElitameldCalculatoraspxINR international normalised ratio
8 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleed it seems rational to develop prophylactic regimens toprevent the development of and bleeding from these varicesHowever most of the published trials do not have sufficientpower to identify favourable treatment effects Based on theexpected bleeding and death rates in the control group theminimum number of patients needed to detect a 50 reductionin bleeding would be 270 and 850 patients in each arm todetect the same reduction in mortality A proposed algorithmfor surveillance and prophylaxis of varices is shown in figure 2At this time there is insufficient evidence to support treatingpatients without varices or lsquopre-primary prophylaxisrsquo A largerandomised placebo-controlled trial of timolol in patientswithout varices and portal hypertension defined as HVPGgt6 mm Hg did not show any effect on the development ofvarices or variceal bleeding27 The role of drug treatment in pre-venting bleeding in patients with small varices is unclear Threerandomised placebo-controlled trials have studied this Caleset al61 showed that propranolol in patients with small or novarices resulted in greater development of varices Howeverpatients without varices were included and there was significantloss of patients to follow-up The second trial showed thatnadolol reduced variceal bleeding without survival benefit andincreased adverse events62 Sarin et al63 did not show any effectwith propranolol despite a significant effect on portal pressure
SurgeryPortacaval shuntsFour trials of portacaval shunts have been published which ran-domised a total of 302 patients64ndash67 either to prophylactic shuntsurgery or to non-active treatment A meta-analysis of thesestudies showed a significant benefit in the reduction of varicealbleeding (OR=031 95 CI 017 to 056) but also a signifi-cantly greater risk of hepatic encephalopathy (OR=2 95 CI12 to 31) and mortality (OR=16 95 CI 102 to 257) inpatients treated with shunt surgery68 At this time there is noevidence for the use of TIPSS for primary prophylaxis1
Devascularisation proceduresInokuchi50 showed that there was a significant reduction in vari-ceal bleeding and in mortality in patients treated with a varietyof devascularisation procedures There are however numerousproblems with the interpretation of this study because of theuse of different procedures in each of the 22 centres Theseresults require confirmation
Pharmacological treatmentNon-cardioselective β blockersThe mainstay of the pharmacological approach to the primaryprophylaxis of variceal haemorrhage has been NSBBPropranolol which has been shown to reduce the PPG reduceazygos blood flow and also variceal pressure It achieves this bycausing splanchnic vasoconstriction and reducing cardiacoutput There is no clear dose-related reduction in HVPG orcorrelation of HPVG reduction with reduction in heart rate69
Observational studies have shown that a 10ndash12 reduction inHVPG after acute administration of propranolol was associatedwith reduced bleeding and hepatic decompensation54 70
However HVPG monitoring is not routinely available in mostcentres outside of larger institutions A meta-analysis of nineplacebo-controlled randomised trials (964 patients) showed thatthe pooled risk difference for bleeding was minus11 (95 CIminus21 to minus1) and for death was minus9 (95 CI minus18 tominus1) in favour of propranolol71
Nadolol exerts similar effects on portal haemodynamicsalthough the effect on blood pressure may not be as pro-nounced Two placebo-controlled trials58 59 have shownreduced bleeding although in one study this was only seen onper protocol analysis59 There was no effect on overall survival
Carvedilol is a NSBB like propranolol and a vasodilator dueto α1 receptor blockade The latter reduces portocollateralresistance and by actions on hepatic stellate cells leads to areduction in intrahepatic resistance Haemodynamic studiesdemonstrate a greater reduction in portal pressure with
Figure 2 Algorithm for surveillance of varices and primary prophylaxis in cirrhosisndash If there is clear evidence of disease progression this interval can be modified by clinician Endoscopy should also be offered at time ofdecompensation
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 9
Guidelines
carvedilol than with propranolol although blood pressure isreduced72 73 The optimum dose is 625ndash125 mgday74 Higherdoses are not more effective and are associated with moreadverse eventsmdashin particular hypotension Carvedilol at a doseof 125 mgday at current UK prices is considerably cheaperthan propranolol 40 mg twice a day and nadolol 80 mgday(monthly cost pound120 pound562 and pound5 respectively) Two RCTs ofcarvedilol versus variceal band ligation (VBL) in primaryprophylaxis have been published75 76 The first study75 showedsignificantly reduced bleeding in the carvedilol arm (10 vs23 relative hazard 041 95 CI 019 to 096) with no effecton survival The second trial by Shah et al76 did not show anydifferences in bleeding or mortality Compliance with VBL wasbetter in the latter trial and unlike the first trial there were sig-nificantly more patients with viral hepatitis than alcoholic cir-rhosis A further study74 assessed the effect of carvedilol inpatients who were haemodynamic non-responders to propran-olol where haemodynamic response was defined as HVPGreduction to le12 mm Hg or by gt20 of baseline after 4 weeksof treatment Patients who were haemodynamic non-respondersor intolerant to carvedilol were treated with VBL Carvedilolresulted in significantly lower variceal bleeding compared withVBL and haemodynamic responders to carvedilol or propran-olol had significantly lower mortality than those treated withVBL It is worth noting that the study was not randomised
There have been recent suggestions based on low-level evi-dence that NSBB may result in a poorer outcome in patientswith cirrhosis and refractory ascites77 The lsquowindow hypothesisrsquofor β blockers in cirrhosis has also recently been described sug-gesting that NSBB are helpful in the compensated and earlydecompensated cirrhotic period but may not be helpful in veryearly cirrhosis such as in a patient with no varices and may beharmful in patients with end-stage cirrhosis with refractoryascites78 However recent large observational studies questionthe last hypothesis with improved survival seen in patients withrefractory ascites treated with NSBB79 unless patients have anepisode of spontaneous bacterial peritonitis80 Therefore untilthere are further prospective controlled studies NSBB should becontinued in patients with refractory ascites The clinician mustcarefully monitor haemodynamic parameters such as blood pres-sure and discontinue NSBB in patients with hypotension andrenal impairment as can occur after an episode of spontaneousbacterial peritonitis Other potentially severe adverse eventswith NSBB include symptomatic bradycardia asthma andcardiac failure Less severe side effects such as fatigue insomniaand sexual dysfunction may also result
Isosorbide mononitrateInterest in the use of vasodilators such as isosorbide mononitrate(ISMN) developed after the demonstration that it reduces portalpressure as effectively as propranolol81 but has subsequentlywaned A trial comparing ISMN with propranolol showed nosignificant difference between these agents82 Another rando-mised trial of ISMN versus placebo did show any difference inthe two arms83 Therefore ISMN is not recommended asmonotherapy in primary prophylaxis
β Blocker and ISMNThe combination of nadolol and ISMN has been compared withnadolol in a RCT The combination therapy reduced the fre-quency of bleeding significantly but no significant differenceswere detected in mortality84 However Garcia-Pagan et al85 in adouble-blind RCTof propranolol plus ISMN versus propranolol
plus placebo failed to show any differences between the twoarms Combination therapy is associated with more side effects
Proton pump inhibitorsA placebo-controlled randomised trial reported reduced bleed-ing and mortality with rabeprazole after eradication of varices86
However the study had a heterogeneous population with VBLperformed for both primary and secondary prophylaxis andsmall numbers (n=43) limiting the validity of the conclusionsFurthermore there was no arm comparing proton pump inhibi-tors with NSBB The use of proton pump inhibitors in patientswith cirrhosis and ascites was associated with increased risk ofspontaneous bacterial peritonitis in a large retrospective study87
This was not confirmed in a larger prospective non-randomisedstudy88 However a recent prospective observational study hasshown proton pump use to be associated with increased mortal-ity in cirrhosis89 Proton pump inhibitors are also associatedwith increased risk of Clostridium difficile infection90 Thereremains continuing concern about proton pump inhibitors inpatients with cirrhosis therefore caution should be used
Endoscopic therapyVariceal band ligationVBL has been compared with NSBB in 19 trials in a recentCochrane meta-analysis of 1504 patients91 Despite reducedbleeding (RR=067 95 CI 046 to 098) with VBL there wasno difference in overall mortality and bleeding-related mortalityThe difference in bleeding was not seen when only trials withlow selection or attrition bias were included Banding can haveserious complications The risk of fatal banding-induced bleed-ing was highlighted in a meta-analysis showing reduced fataladverse events with NSBB (OR=014 95 002 to 099)92
The optimal timing of banding intervals is discussed in thesection lsquoSecondary prophylaxis of variceal haemorrhagersquo A ran-domised trial of 96 patients who underwent endoscopic surveil-lance at 6 or 3 months after eradication of varices with VBL didnot demonstrate a difference in bleeding on mortality93
However the trial had a heterogeneous study group of patientswho underwent VBL both for primary (65) and secondaryprevention (35)
SclerotherapyNineteen trials have compared endoscopic variceal sclerotherapywith no treatment68 Owing to the marked heterogeneitybetween these studies a meta-analysis is clinically inappropri-ate68 Sclerotherapy does not offer any benefit in combinationwith NSBB or VBL compared with VBL or NSBB alone andincreases iatrogenic complications such as strictures94ndash96 At thistime sclerotherapy cannot be recommended for prophylaxis ofvariceal haemorrhage in patients with cirrhosis
Recommendations primary prophylaxis of variceal haemor-rhage in cirrhosis (figure 2)1 What is the best method for primary prophylaxis
11 We recommend NSBB or variceal band ligation (VBL)We suggest pharmacological treatment with propranololas first line VBL is offered if there are contraindicationsto NSBB The choice of VBL or NSBB should also takeinto account patient choice (level 1a grade A)
12 We suggest carvedilol or nadolol as alternatives to pro-pranolol (level 1b grade A)
13 Dose131 Propranolol 40 mg twice daily Dose titrated to
maximum tolerated or once heart rate (HR) of
10 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
50ndash55 bpm is reached to a maximum dose of320 mg (level 1a grade A)
132 Nadolol 40 mg daily dose Dose titrated tomaximum tolerated or once HR of 50ndash55 bpm isreached a maximum dose of 240 mg (level 1agrade A)
133 Carvedilol 625 mg once daily to increase tomaintenance of 125 mg after a week if toleratedor once HR of lt50ndash55 bpm is reached (level 1agrade A)
134 It is suggested that NSBB are discontinued at thetime of spontaneous bacterial peritonitis renalimpairment and hypotension (level 2b grade B)
14 In cases of contraindications or intolerance to NSBB werecommend variceal band ligation (level 1a grade A)
2 Who should have surveillance for variceal bleeding21 We recommend all patients with cirrhosis should be
endoscoped at the time of diagnosis (level 1a grade A)There is no indication to repeat endoscopy in patientsreceiving NSBB
3 How often should cirrhotic patients be endoscoped31 If at the time of first endoscopy no varices are seen we
suggest that patients with cirrhosis should be endos-coped at 2ndash3-year intervals (level 2a grade B)
32 If grade I varices are diagnosed we suggest that patientsshould be endoscoped at yearly intervals (level 2agrade B)
33 If there is clear evidence of disease progression wesuggest that the intervals can be modified by a clinicianEndoscopy should also be offered at time of decompen-sation (level 2a grade B)
4 Which patients with cirrhosis should have primaryprophylaxis41 If grade I varices and red signs or grade 2ndash3 varices are
diagnosed we recommend that patients have primaryprophylaxis irrespective of the severity of the liverdisease (level 1a grade A)
5 Treatments not recommended51 Proton pump inhibitors are not recommended unless
otherwise required for peptic ulcer disease (level 1bgrade B)
52 Isosorbide mononitrate monotherapy is not recommendedas primary prophylaxis (level 1b grade A) There is insuffi-cient evidence to recommend isosorbide mononitrate incombination with NSBB (level 1b grade A)
53 Shunt surgery or TIPSS is not recommended as primaryprophylaxis (level 1a grade A)
54 Sclerotherapy is not recommended as primary prophy-laxis (level 1a grade A)
6 Areas requiring further study61 Role of NSBB in patients without varices with focus on
carvedilol62 Role of NSBB in patients with small varices with focus
on carvedilol63 Comparison of carvedilol versus propranolol in primary
prophylaxis64 Identification of and trials assessing new drugs for
primary prophylaxis such as statins7 Quality indicator
71 Percentage of patients at diagnosis of cirrhosis who havehad an endoscopy to screen for varices (level 1agrade A)Numerator patients diagnosed with cirrhosis who havehad an endoscopy either before or after diagnosis within
6 monthsDenominator patients newly diagnosed with cirrhosis
72 Percentage of patients receiving primary prophylaxisamong those newly diagnosed with grade I varices andred signs or grade 2ndash3 varicesNumerator patients who have grade 1 varices with redsigns or grade 2ndash3 varices receiving primary prophy-laxisDenominator patients diagnosed with cirrhosis whohave grade I varices with red signs or grade 2ndash3 varices
MANAGEMENT OF ACTIVE VARICEAL HAEMORRHAGEThe average 6-week mortality of the first episode of varicealbleeding in most studies is reported to be up to 20 There hasbeen considerable improvement in survival since the early 1980swhen the in-hospital mortality was 40ndash5097 compared with15 from a recent UK audit5 Such is the improvement in out-comes that a patient with Childrsquos A cirrhosis is very unlikely tosuccumb to an index variceal bleed Studies have shown theChildndashPugh score MELD score and HVPG to be strong predic-tors of outcomes98ndash103 The MELD score has been shown tooutperform Childrsquos score in a recent study with a score gt19associated with 20 6 week mortality103 Furthermore theMELD score has been shown to perform as well as the trad-itional intensive care unit scores in predicting mortality inpatients admitted to intensive care in the UK104 MELD gt18active bleeding transfusing gt4 units of packed red blood cellshave been shown to be predictors of mortality and earlyrebleeding99 101 102 HVPG has also been shown to predictoutcome when measured at 2 weeks after a bleed44 and a valueof ge20 mm Hg when measured acutely within 48 h has beenshown to provide significant prognostic information100
However this technique is not used routinely in the manage-ment of patients around the world and substitution of clinicaldata in the latter study was shown to provide the same clinicalpredictive value100 These scoring systems are not purely aca-demic they allow the referring clinician to predict thosepatients with a high chance of rebleeding to be transferred to aspecialist centre offering for instance TIPSS before the patientrebleeds
Nonetheless probably the most important step in the man-agement of acute variceal haemorrhage is the initial resuscitationassessed according to standard lsquoABCrsquo practice together withprotection of the airway to prevent aspiration Although earlyendoscopy allows for accurate diagnosis of the bleeding site anddecisions about management (figure 3) therapeutic interventionin acute variceal bleeding can be initiated safely in most casesbefore diagnostic endoscopy As similar efficacy is demonstratedwith pharmacological treatment as with sclerotherapy theformer should be first-line therapy99 β Blockade should not bestarted in the acute setting and those already taking β blockersas prophylaxis should probably stop taking them for 48ndash72 h inorder that the patientrsquos physiological response to blood loss canbe allowed to manifest
General considerationsPatient evaluationThe majority of patients with a variceal bleed will be sufficientlystable to enable a full history and examination to take placeHistory of alcohol excess and or intravenous drug use should besought and may become particularly relevant if the patient haswithdrawal symptoms after admission Comorbidity is importantwhen estimating risk and deciding on use of vasopressors The
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 11
Guidelines
following risk factors doubled mortality after an acute varicealbleed in one US study older age comorbidities male gender andnot undergoing a gastroscopy within 24 h105
A full examination is helpful for the important negatives asmuch as the positives Baseline observations should include thetemperature as infection is a serious complication with signifi-cant mortality Confusion may be present because of encephal-opathy intoxication with alcohol or drugs or withdrawal fromalcohol or drugs The patient should be on continuous BP andpulse monitor and their haemodynamic status recordedAn oxygen saturation monitor is helpful Stigmata of chronicliver disease and concurrent jaundice provide insight into thecurrent status of a patientrsquos liver and also give warning ofpotential further decompensation if significant bleeding persists(see scoring systems above) Pneumonia must be actively
excluded Evidence of ascites requires a diagnostic tap to searchfor infection
Investigations including full blood count coagulationprofile liver and renal function and blood group and save andcross-match Blood and urine should also be cultured An ultra-sound scan later in the admission is helpful to identify subclin-ical ascites flow in portal vein and any obvious emergence of anhepatocellular carcinoma (HCC)
Location of patientA decision must be made as to where the patient is best managedVariceal bleeding is unpredictable generally occurs in patientswith significant liver disease and is associated with significant mor-tality Hence a high-dependency unit is usually the most appropri-ate initial location although a properly staffed lsquogastrointestinal
Figure 3 Algorithm for themanagement of acute varicealbleeding TIPSS transjugularintrahepatic portosystemic stent shunt
12 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleeding bedrsquo may be appropriate If a patient is vomiting bloodor there is a perceived risk of a haemodynamically unstable patienthaving blood in the stomach then the patient must be intubatedbefore endoscopy and return to an intensive care or high-dependency unit will be necessary until extubation
Volume resuscitation and blood productsIntravenous access (two 16ndash18G cannulae) should have beensecured on admission with a reported GI bleed Further intra-venous access may be necessary In patients with poor venousaccess advanced liver disease or renal failure associated withtheir liver disease central venous access may be helpful withguiding fluid infusions However the drawbacks include the riskof the procedure and a potential source of infection Thereforethere is no absolute requirement for a central line and no evi-dence of unequivocal benefit Intravenous fluid resuscitationshould be initiated with plasma expanders aiming to maintain asystolic blood pressure of 100 mm Hg Care with monitoring isparamount in this group of patients
Overtransfusion has been shown to have a deleterious effecton outcome In a recent single-centre RCT a restrictive transfu-sion policy of maintaining haemoglobin between 70 and 80 gLimproved the control of variceal bleeding (11 vs 22p=005) and lowered HVPG compared with a liberal transfu-sion policy without effect on 45-day survival106 However itshould be noted that these results were from a single Spanishcentre which was a tertiary unit for variceal bleeding where allpatients underwent endoscopy within 6 h Nonetheless arestrictive transfusion policy has been recommended for sometime1 and there is now good evidence to support not transfusinga stable patient with a haemoglobin of ge80 gL However under-resuscitation should also be avoided and while goal-orientedfluid replacement has generally not been useful in an intensivetherapy unit setting a venous saturation gt70 remains an easilymeasurable target with some evidence to support it107
Interpretation and management of clotting profile is challen-ging in liver disease where there is usually a balanced deficiencyof both procoagulant and anticoagulant factors108 The NICEguidelines recommend activation of a hospitalrsquos massive transfu-sion policy when there is major haemorrhage and plateletsupport when the value is lt50 and clotting factor supportwhen the international normalised ratio (INR) is gt15 timesnormal2 There is no evidence for the use of lsquoprophylacticrsquo clot-ting or platelet support to reduce the risk of rebleeding Thereis insufficient evidence to support the routine use of transexamicacid or recombinant factor VIIa109
Pharmacological treatmentThe two major classes of drugs that have been used in thecontrol of acute variceal bleeding are vasopressin or its analo-gues (either alone or in combination with nitroglycerine) andsomatostatin or its analogues Terlipressin is the only agent thathas been shown to reduce mortality in placebo-controlled trialsHowever in trials comparing terlipressin somatostatin andoctreotide no difference in efficacy was identified in a system-atic review110 and in a recent large RCT111 Prophylactic anti-biotics can result in a similar survival benefit following acutevariceal bleeding
VasopressinVasopressin reduces portal blood flow portal systemic collateralblood flow and variceal pressure It does however have signifi-cant systemic side effects such as an increase in peripheral resist-ance and reduction in cardiac output heart rate and coronary
blood flow In comparison with no active treatment the pooledresults of four randomised trials showed that it reduced failureto control variceal bleeding (OR=022 95 CI 012 to 043)although survival was unaffected68 Meta-analysis of five trialscomparing sclerotherapy with vasopressin has shown a signifi-cant effect on reduction in failure to control bleeding(OR=051 95 CI 027 to 097) with no effect on survival68
Vasopressin with nitroglycerineThe addition of nitroglycerine enhances the effect of vasopres-sin on portal pressure and reduces cardiovascular side effects112
Meta-analysis of three randomised trials comparing vasopressinalone with vasopressin and nitroglycerine showed that the com-bination was associated with a significant reduction in failure tocontrol bleeding (OR=039 95 CI 022 to 072) although nosurvival benefit was shown68
TerlipressinTerlipressin is a synthetic analogue of vasopressin which has animmediate systemic vasoconstrictor action followed by portalhaemodynamic effects due to slow conversion to vasopressin Ina Cochrane meta-analysis of seven placebo-controlled trials ter-lipressin was shown to reduce failure to control bleeding(RR=066 95 CI 055 to 093) and also to improve survival(RR=066 95 CI 049 to 088)113 In the same meta-analysisthere was no difference between terlipressin versus vasopressinballoon tamponade or endoscopic therapy in failure to controlbleeding or survival113 The role of terlipressin in combinationwith VBL is explored in the section lsquoEndoscopic therapy incombination with pharmacological therapyrsquo
The recommended dose of terlipressin is 2 mg IV every 4 halthough many units reduce the dose to 6 hourly as it may causeperipheral vasoconstriction which manifests as painful handsand feet While 5 days of IV treatment has been advocated inthe Baveno V guidelines1 this prolonged treatment has notbeen shown to have a survival benefit and for pragmaticreasons many units will stop treatment shortly after satisfactoryhaemostasis In a randomised trial terlipressin given for 24 hafter satisfactory haemostasis with VBL after oesophageal vari-ceal bleeding was as effective as 72 h of treatment114
In patients intolerant of terlipressin or in countries where ter-lipressin is not available alternatives should be considered
Somatostatin and octreotideSomatostatin causes selective splanchnic vasoconstriction andreduces portal pressure and portal blood flow115 Octreotide is asomatostatin analogue The mechanism of action of these twoagents is not clear Inhibition of glucagon increases vasodilatationrather than a direct vasoconstrictive effect and post-prandial guthyperaemia is also reduced The actions of octreotide on hepaticand systemic hemodynamics are transient making continuousinfusion necessary Octreotide is given as a 50 μg bolus followedby an infusion of 25ndash50 μgh Somatostatin is given as a 250 mgintravenous bolus followed by an infusion of 250 mghSomatostatin and octreotide have been shown to be aseffective as terlipressin in acute variceal bleeding in ameta-analysis110 Seo et al111 in a large RCTof 780 patients com-paring these three agents failed to show a difference in treatmentsuccess (range 838ndash862) rebleeding (range 34ndash44) andmortality (range 8ndash88) A low systolic blood pressure at pres-entation high serum creatinine level active bleeding in the emer-gency endoscopy gastric variceal bleeding and ChildndashPugh gradeC were independent factors predicting 5-day treatmentfailure111
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 13
Guidelines
AntibioticsAntibiotics that provide Gram-negative cover are one of the inter-ventions which positively influence survival in variceal haemor-rhage as shown in a Cochrane meta-analysis of 12placebo-controlled trials (RR=079 95 CI 063 to 098)116
Antibiotics were also shown to reduce bacterial infections(RR=043 95 CI 019 to 097) and early rebleeding (RR=05395 CI 038 to 074)116 Therefore short-term antibiotics shouldbe considered standard practice in all cirrhotic patients who have avariceal bleed irrespective of the presence of confirmed infectionThird-generation cephalosporins such as ceftriaxone (1 g IVdaily) have been shown to be more effective at reducingGram-negative sepsis than oral norfloxacin117 but choice of anti-biotics must be dictated by local resistance patterns and availability
Proton pump inhibitorsOne RCT compared a short course of proton pump inhibitorswith vasoconstrictor therapies after haemostasis in acute varicealbleeding118 Despite larger ulcers noted in the vasoconstrictorarm there were no differences in bleeding or survival Nearly50 of patients had ascites which might have implications inlight of the reports of increased incidence of spontaneous bac-terial peritonitis as mentioned earlier
Endoscopic therapyEndoscopy should take place within 24 h of admission andearlier if there is excessive bleeding based on low-level evi-dence105 While many guidelines and reviews suggest thatendoscopy should be carried out within 12 h the only study thatexamined the influence of timing on outcome failed to demon-strate any advantage of endoscopy before 12 h119 The optimaltime is after sufficient resuscitation and pharmacological treat-ment with the endoscopy performed by a skilled endoscopyteam in a suitably equipped theatre environment and withairway protection Airway protection is essential where risk ofaspiration is high and affords the endoscopist time for thoroughevaluation including complete clot aspiration and controlledapplication of treatment including tamponade if required Theendoscopy team must comprise an experienced endoscopynurse acquainted with the equipment necessary for endoscopytherapy of varices and a skilled endoscopist competent in usingbanding devices and deployment of balloon tamponade
Variceal band ligationThis technique is a modification of that used for the elastic bandligation of internal haemorrhoids Its use in humans was firstdescribed in 1988120 A meta-analysis of seven trials comparingVBL with sclerotherapy in acute bleeding showed that VBLreduced rebleeding from varices (OR=047 95 CI 029 to078) reduced mortality (OR=067 95 CI 046 to 098) andresulted in fewer oesophageal strictures (OR=010 95 CI003 to 029)121 The number of sessions required to obliteratevarices was lower with VBL (22 fewer sessions (95 CI 09to 35))
SclerotherapySclerotherapy has been replaced by VBL and should no longerbe offered as standard of care in acute variceal haemorrhage
Other endoscopic measuresIn an RCT cyanoacrylate offered no benefit over VBL with theadditional risk of embolisation and trend towards increasedrebleeding with cyanoacrylate122
Haemostatic powder (TC-325 Hemospray Cook MedicalUSA) has been described in a small study of nine patients whoreceived endoscopic spray treatment for acute variceal bleedingThe study reported no rebleeding within 24 h and no mortalityat 15 days123
Endoscopic therapy in combination with pharmacological therapyThe role of combining vasoactive drugs with endoscopictherapy (VBL or sclerotherapy) was reported in a meta-analysisof eight trials124 Combination therapy resulted in better initialcontrol of bleeding (RR=112 95 CI 102 to 123) and5-day haemostasis (RR=128 95 CI 118 to 139) withoutany difference in survival Adverse events were similar in bothgroups Two RCTs have compared VBL with sclerotherapy incombination with vasoactive agents in acute variceal bleed-ing125 126 Lo et al125 used vasopressin and found that VBLresulted in better 72 h haemostasis (97 vs 76 p=0009)with fewer complications (5 vs 29 p=0007) Villanuevaet al used somatostatin and reported lower failure to controlacute bleeding with VBL (4 vs 15 p=002) with fewerserious complications (4 vs 13 p=004) Overall survivalwas similar in both trials125 126
Balloon tamponadeBalloon tamponade is highly effective and controls acute bleed-ing in up to 90 of patients although about 50 rebleed whenthe balloon is deflated127 128 It is however associated withserious complications such as oesophageal ulceration and aspir-ation pneumonia in up to 15ndash20 of patients Despite this itmay be a life-saving treatment in cases of massive uncontrolledvariceal haemorrhage pending other forms of treatment Anappropriately placed SengstakenndashBlakemore tube allows forresuscitation safe transportation and either repeat endoscopy orradiological shunting in a patient with a stable cardiovascularsystem The oesophageal balloon is rarely required must neverbe used on its own and should be used only if there is continu-ing bleeding despite an adequately inflated gastric balloon cor-rectly placed and with appropriate tension Placement of thetube endoscopically or over a guide wire might reduce the riskof complications especially oesophageal rupture
Removable oesophageal stentsThe SX-Ella Danis stent (ELLA-CS Hradec Kralove CzechRepublic) is a removable covered metal mesh stent placed endo-scopically in the lower oesophagus without radiological screen-ing It has no role in the management of gastric varicealbleeding These stents can be left in situ for up to 2 weeksunlike the SengstakenndashBlakemore tube which should beremoved after a maximum of 24ndash48 h129 130 No published con-trolled trials have compared this modality with balloontamponade
Transjugular intrahepatic portosystemic stent-shuntSeveral uncontrolled studies have examined the role of salvagebare TIPSS in acute variceal bleeding In a review of 15 studiescontrol of bleeding was achieved in 90ndash100 with rebleedingin 6ndash16131 Mortality varied between 75 (in hospital) and15 (30 day) It is important to appreciate that sclerotherapywas used as first-line endoscopic therapy in most of thesestudies Long-term follow-up of a study that compared TIPSSwith H-graft portacaval shunts in patients for whom non-operative management had failed suggested that H-grafts were auseful method of reducing portal pressure and had a signifi-cantly lower failure rate (p=004) but had no significant
14 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
improvement in overall survival despite a benefit seen in ChildrsquosA and B disease132 A recent RCT compared emergency porto-caval surgery with bare TIPSS within 24 h of presenting withacute oesophageal variceal bleeding in unselected cirrhoticpatients Emergency portocaval surgery resulted in better out-comes for long-term bleeding control encephalopathy and sur-vival (plt0001)133 Before wider application of surgery foracute variceal bleeding more data are needed in light of therecent adoption of covered stents
There has also been a generalised established change in prac-tice in using covered TIPSS stents (polytetrafluoroethylene(PTFE)) rather than a bare metal stent with evidence to supportthis change In randomised controlled studies these stents wereshown to have higher primary patency rates than bare stentswithout significant differences in survival and the potential forreduced incidence of hepatic encephalopathy134 135
There is however growing evidence from two RCTs for theearlier use of TIPSS in selected patients stratified by HVPGChildndashPugh class and active bleeding and not just use as asalvage option6 136 Monescillo et al136 randomised patientspresenting with acute oesophageal variceal haemorrhage to bareTIPSS or standard of care if the HVPG was ge20 mm Hg within24 h of admission Significantly reduced treatment failure asdefined by failure to control acute bleeding andor early rebleed-ing (12 vs 50) was seen and improved survival (62 vs35) in the patients randomised to undergo a TIPSS procedureHowever the standard of care was sclerotherapy and not com-bination endoscopic and pharmacological treatment This limita-tion and the lack of availability of HVPG measurement in mostcentres meant this trial did not have a significant impact on clin-ical practice
Garcia-Pagan et al6 selected patients with active bleeding andChildrsquos B cirrhosis or patients with Childrsquos C cirrhosis (Childrsquosscore lt14) for randomisation to early PTFE-covered TIPSSwithin 72 h or standard of care with VBL and pharmacologicaltreatment This has shown encouraging results with reduced riskof treatment failure (3 vs 50) improved survival (86 vs61 at 1 year) yet without increased risk of hepatic encephal-opathy The results were supported by an observational studyfrom the same group although a survival benefit was notseen137 Furthermore a recent well-conducted observationalstudy did not demonstrate such high survival rates with earlyTIPSS with 11-year survival of 67 which was similar to thatof patients given endoscopic and pharmacological treatmentsonly138 Therefore larger multicentred RCTs need to be under-taken to further evaluate the role of early TIPSS It is importantto make the distinction between salvage TIPSS and early TIPSSto prevent rebleeding
Liver transplantationThis is probably appropriate only for patients who bleed whileawaiting liver transplantation although studies comparing VBLor TIPSS placement with urgent liver transplantation in thissituation need to be done Liver transplantation is an exceed-ingly rare option for the vast majority of patients both becauseit is not commonly available and because of shortages anddelays in organ procurement No controlled trials of liver trans-plantation in uncontrolledactive bleeding are available
Recommendations for the control of variceal bleeding in cir-rhosis are given below and in figure 3
Recommendations control of active variceal haemorrhage incirrhosis (figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with bloodplatelets and clotting factors in line with local protocolsfor managing massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusionpolicy aiming for a haemoglobin of 70ndash80 gL is sug-gested in haemodynamically stable patients (level 1bgrade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable(level 5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L(level 5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to localcircumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with suspected
or confirmed variceal bleeding (level 1a grade A)32 In all patients vasoconstrictors such as terlipressin or
somatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 15
Guidelines
41 If bleeding is difficult to control a SengstakenndashBlakemore tube should be inserted until further endo-scopic treatment TIPSS or surgery is performed depend-ing on local resources and expertise (level 1b grade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure (level1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
SECONDARY PROPHYLAXIS OF VARICEAL HAEMORRHAGEβ BlockersA meta-analysis of 12 trials comparing propranolol or nadolol139
with no active treatment showed a significant reduction inrebleeding but no significant reduction in mortality140 Thegreater reduction in portal pressure with carvedilol comparedwith propranolol has been described in the section lsquoPrimaryprophylaxisrsquo of this guideline
NitratesThe addition of ISMN to NSBB has been shown to reduce vari-ceal rebleeding compared with NSBB alone although no sur-vival benefit was seen141 In addition adverse events leading todrug withdrawal were more common in the group receivingcombined drug treatment A meta-analysis of ISMN alone orwith either NSBB or endoscopic therapy reported that there wasno mortality benefit from combining nitrates and NSBB com-pared with NSBB alone142
Side effects of ISMN include dizziness and headache Owingto the side effects and relative lack of data ISMN is not com-monly used in clinical practice
A recent RCT of 121 patients reported carvedilol to besimilar to combined ISMN and NSBB therapy in the preventionof variceal rebleeding and mortality although severe adverseevents were less common with carvedilol143
SimvastatinA recent abstract of a multicentre RCT of 158 patients reporteda survival benefit (91 vs 78 p=003) from adding simvasta-tin to VBL and NSBB compared with placebo VBL and NSBBas treatment for the prevention of variceal rebleeding144 Therewas no difference in rebleeding and the survival benefit wasrestricted to Child A and B patients Serious adverse events weresimilar in both groups More data are required to investigatethis interesting observation of a survival benefit from simvastatinin this situation which may relate to its effects on hepatocellularfunction fibrosis and portal pressure
Proton pump inhibitorsA double-blind randomised placebo-controlled trial showed thatpantoprazole reduced the size of ulcers in patients who under-went VBL However the total number of ulcers and other out-comes were similar in the two groups145
Endoscopic therapyVBL has been accepted as the preferred endoscopic treatmentfor the prevention of variceal rebleeding with a lower rate ofrebleeding mortality and complications than sclerother-apy146 147 The time interval between VBL sessions to achieveeradication of varices is debateable However a recent RCTcomparing monthly with biweekly VBL after initial haemostasiswith VBL in 70 patients suggested that there were fewerpost-VBL ulcers in the monthly group (11 vs 57plt0001)148 Variceal recurrence rebleeding and mortality weresimilar in both groups
Two meta-analyses showed there is no evidence that the add-ition of sclerotherapy to VBL improves clinically relevant out-comes including variceal rebleeding and death and thecombination led to higher stricture rates149 150
Endoscopic therapy versus drug therapyVBL has been reported to be more effective than combinedNSBB and ISMN drug therapy151 However an 8-yearfollow-up study of this RCT found that although VBL wassuperior in reducing variceal rebleeding survival rates were sig-nificantly higher in the group treated with combined drug treat-ment152 Other studies have found no superiority of VBL overcombined drug therapy for prevention of variceal rebleeding ormortality153 154 A recent small multicentre RCT reported carve-dilol to be similar to VBL in the prevention of variceal rebleed-ing with a trend in favour of survival with carvedilol (73 vs48 p=0110)155
Several meta-analyses have compared drug therapy with VBLin the prevention of variceal rebleeding One meta-analysis ofsix RCTs showed no significant difference in variceal rebleedingrates when comparing VBL alone with combined NSBB andISMN therapy However all-cause mortality was significantlyhigher in patients treated with the VBL (RR=125 95 CI101 to 155)156 Three meta-analyses comparing drug therapy(NSBB alone or with ISMN) with endoscopic therapy alonereported no difference in variceal rebleeding or mortality157ndash159
Endoscopic+drug therapy versus either aloneNumerous studies and several meta-analyses have comparedcombined endoscopic and drug therapy with monotherapy(endoscopic or drugs alone) in the prevention of varicealrebleeding A meta-analysis of 23 trials assessing sclerotherapyor VBL combined with NSBB reported that combinationtherapy reduced rebleeding more than either endoscopic
16 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

hospitals This model referred to as ldquospoke and wheelrdquo ornetwork model is well established for other complex proceduresand helps to expedite and streamline the process In theNCEPOD report lsquoMeasuring the unitsrsquo just 15 of hospitals hadon-site access to TIPSS while 72 had access to TIPSS in othercentres7
There have been significant efforts to address the need toimprove the upper GI bleeding (UGIB) service A toolkit wasproduced in collaboration with BSG Association of UpperGastrointestinal Surgeons (AUGIS) Royal Colleges ofPhysicians Radiology and Nursing and Academy of MedicalRoyal Colleges11 The key nine service standards recommendedby the document are detailed below1 There will be a nominated individual with the authority to
ensure implementation by the contracted provider2 Contracted providers will ensure the minimum service is
adequately resourced3 All patients with suspected UGIB should be properly
assessed and their risk scored on presentation4 All patients should be resuscitated before therapeutic
intervention5 All high-risk patients with UGIB should be endoscoped
within 24 h preferably on a planned list in the first instance6 For patients who require more urgent intervention either for
endoscopy interventional radiology or surgery formal 247arrangements must be available
7 The necessary team meeting an agreed competency levelshould be available throughout the complete patient pathway
8 Each stage of the patient pathway should be carried out inan area with lsquoappropriatersquo facilities equipment and supportincluding staff experienced in the management of UGIB
9 All hospitals must collect a minimum dataset in order tomeasure service provision against auditable outcomes(case-mix adjusted as appropriate)NICE recommendations for endoscopy provision are detailed
in the section lsquoManagement of active variceal haemorrhagersquorecommendations2 The BSG has also produced a care bundlefor patients admitted with decompensated cirrhosis in light ofthe NCEPOD report with a check list method which includesgastrointestinal bleeding12
Since the 2008 Darzi report quality has become a priorityfor the NHS13 With these guidelines there is real opportunityto introduce quality outcomes based on good clinical evidenceFurthermore by incorporating them into the liver accreditationscheme Liver Quest one can improve and assure quality inliver services across the UK14 Therefore a small number ofquality outcomes measures have been chosen and form part ofthe key recommendations15
DEFINITIONSIt is important to define the terms that should be used in thecontext of a variceal bleed These are the Baveno V consensusdefinitions1
Variceal haemorrhageVariceal haemorrhage is defined as bleeding from an oesopha-geal or gastric varix at the time of endoscopy or the presence oflarge oesophageal varices with blood in the stomach and noother recognisable cause of bleeding An episode of bleeding isclinically significant when there is a transfusion requirement for2 units of blood or more within 24 h of the time zero togetherwith a systolic blood pressure of lt100 mm Hg or a posturalchange of gt20 mm Hg andor pulse rate gt100 bpm at time
zero (time zero is the time of admission to the first hospital towhich the patient is taken)
Time frame of acute bleedingThe acute bleeding episode is represented by an interval of120 h (5 days) from time zero Evidence of any bleeding after120 h is the first rebleeding episode
Failure to control active bleedingFailure to control active bleeding is defined as death or need tochange treatment defined by one of the following criteria16 17
1 Fresh haematemesis or nasogastric aspiration of ge100 mL offresh blood ge2 h after the start of a specific drug treatmentor therapeutic endoscopy
2 Development of hypovolaemic shock3 30 gL drop in haemoglobin (9 drop of haematocrit)
within any 24 h period if no transfusion is given This timeframe needs to be further validated
Variceal rebleedingVariceal rebleeding is defined as the occurrence of a singleepisode of clinically significant rebleeding from portal hyperten-sive sources from day 5 Clinically significant rebleeding isdefined as recurrent melaena or haematemesis in any of the fol-lowing settings1 hospital admission2 blood transfusion3 30 gL drop in haemoglobin4 death within 6 weeks
Early mortalityDeath within 6 weeks of the initial episode of bleeding
NATURAL HISTORY OF VARICES IN CIRRHOSISDevelopment of varicesThe rise in portal pressure is associated with the developmentof collateral circulation which allows the portal blood to bediverted into the systemic circulation These spontaneous shuntsoccur (a) at the cardia through the intrinsic and extrinsic gastro-oesophageal veins (b) in the anal canal where the superiorhaemorrhoidal vein belonging to the portal system anastomoseswith the middle and inferior haemorrhoidal veins which belongto the caval system (c) in the falciform ligament of the liverthrough the para-umbilical veins which are the remains of theumbilical circulation of the fetus (d) in the abdominal wall andthe retroperitoneal tissues from the liver to the diaphragmveins in the lienorenal ligament in the omentum and lumbarveins and (e) blood diversion from the diaphragm gastric pan-creatic splenic and adrenal veins which may drain into the leftrenal vein
Numerous lines of evidence suggest that varices develop andenlarge with time Christensen et al18 followed up a cohort of532 patients with cirrhosis and showed that the cumulative inci-dence of patients with varices increased from 12 to 90 over12 years In a study involving 80 patients followed up for16 months Cales and Pascal19 showed that 20 of patientswho did not have varices developed new varices and 42 ofpatients with small varices showed definite enlargement Czajaet al20 also showed that the prevalence of varices increased from8 to 13 over 5 years in a cohort of patients with chronicactive hepatitis even though they were treated with prednisol-one Merli et al21 in a study of 213 patients with cirrhosis withno or small varices demonstrated that the annual progression ofvarices was 12 A recent database analysis by DrsquoAmico et al22
6 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
using a competing risk model showed that the cumulative inci-dence of varices at 10 and 20 years was 44 and 53 respect-ively suggesting an overestimation in previous studies not usinga competing risk model
The main factors that appear to determine the developmentof varices are continued hepatic injury the degree of portosyste-mic shunting endoscopic appearances and portal pressureEvidence for the role of hepatic injury is derived from studies inwhich varices were shown to regress with time Baker et al23 fol-lowed up a cohort of 115 patients with oesophageal varices andshowed that varices had disappeared in nine patients regressedin seven and remained unchanged in six They concluded thatthe disappearance and regression of varices might be related toabstinence from alcohol This observation was confirmed in astudy by Dagradi24 who followed up a cohort of patients withalcoholic cirrhosis over 3 years and showed a reduction in vari-ceal size in 12 of the 15 patients with alcoholic cirrhosis whostopped drinking and an enlargement in variceal size in 17patients who continued to drink On the other hand Cales andPascal19 showed that regression of varices occurred in 16 ofpatients with alcoholic cirrhosis who continued to imbibealcohol This might be related to the development of large por-tosystemic collaterals which decompress the portal system andreduce the risk of the development of large oesophageal varicesThe degree of portosystemic shunting can be quantified bymeasuring the diameter of portal veins and collaterals and canbe significant in those with gastrorenal or splenorenal shunt-ing25 26 Others have shown that the presence of alcoholic cir-rhosis Childrsquos B or C cirrhosis and red whale signs on indexendoscopy predicted progression of varices21 Groszmannet al27 in a placebo-controlled randomised trial of timolol in213 cirrhotic patients without varices showed that a baselinehepatic venous pressure gradient (HVPG) of gt10 mm Hg or age10 increase in HVPG during follow-up were both predictiveof the development of varices
Diagnosis of gastro-oesophageal varicesUntil recently endoscopy has been used exclusively to diagnosevarices Non-invasive methods of screening for varices includecapsule endoscopy transient elastography and use of laboratoryand radiological findings
EndoscopyThere is universal acceptance that endoscopy is the lsquogold stand-ardrsquo for diagnosing gastro-oesophageal varices The main limita-tions are intraobserver variability in the diagnosis of small orgrade I oesophageal varices (figure 1AndashC) Recently unsedatednasal gastroscopy has been found to have similar accuracy toconventional endoscopy and has the advantage of tolerabilityand potential cost saving since it can be performed in the clinicsetting in some institutions28 29 However there are no con-trolled studies and banding of varices is not possible
Capsule endoscopyCapsule endoscopy uses a 26 mm pill-shaped device whichtransmits video footage which is stored and later analysedPatients are not sedated but patient cooperation is essentialIn a large study by de Franchis et al30 capsule endoscopy wascompared with standard gastroscopy The primary end point of90 or greater concordance was not achieved Lapalus et al31
in a prospective study of 120 patients demonstrated similarresults with capsule endoscopy Therefore capsule endoscopycannot be considered an alternative to standard endoscopyalthough may have a role in patient who refuse gastroscopy
Transient elastographyTransient elastography ((FibroScan Echosens Paris France) usesthe principles of ultrasound to derive tissue stiffness by measur-ing the speed of propagation of a low-frequency wave whichthen correlates with liver fibrosis Vizzutti et al32 in a study of61 patients with hepatitis C showed a sensitivity for predictionof oesophageal varices of 90 using a threshold 176 kPaHowever specificity was poor at 43 A study of 298 patientsfound the optimal cut-off point for the prediction of oesopha-geal varices was 215 kPa (sensitivity 76 and specificity78)33 In one uncontrolled study the use of transient elasto-graphy was found to be as effective as HVPG at predictingportal hypertension-related complications34 Therefore the roleof transient elastography in predicting varices is controversialdue to the lack of consistent results and controlled studies Thismodality may be more useful for predicting decompensation inpatients with cirrhosis
Radiological and serum parametersA prospective study of 311 patients with chronic hepatitis Cshowed that a platelet-to-spleen size ratio with a threshold of909 had positive and negative predictive values of 100 and94 respectively35 These good results have not been repro-duced by others as demonstrated in a meta-analysis36
Risk factors for first variceal bleedingThe factors that predispose to and precipitate variceal haemor-rhage are still not clear The suggestion that oesophagitis mayprecipitate variceal haemorrhage has been discarded37
Presently the most important factors that have been heldresponsible include (i) pressure within the varix (ii) varicealsize (iii) tension on the variceal wall and (iv) severity of theliver disease
Portal pressureIn most cases portal pressure reflects intravariceal pressure38
and a HVPG gt10 mm Hg is necessary for the development ofoesophageal varices27 There is no linear relationship betweenthe severity of portal hypertension and the risk of varicealhaemorrhage although HVPG gt12 mm Hg is an accepted
Figure 1 (A) Grade I oesophagealvarices These collapse to inflation ofthe oesophagus with air (B) Grade IIoesophageal varices These are varicesbetween grades 1 and 3 (C) Grade IIIoesophageal varices These are largeenough to occlude the lumen
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 7
Guidelines
threshold for variceal bleeding39 40 However the HVPG tendsto be higher in bleeders as well as in patients with larger varicesIn a prospective study comparing propranolol with placebo forthe prevention of first variceal haemorrhage Groszmann et al41
showed that bleeding from varices did not occur if the portalpressure gradient (PPG) could be reduced to lt12 mm HgOthers have shown that a 20 reduction in portal pressure pro-tects against further bleeding42 These haemodynamic goalshave been accepted as the aim of pharmacological treatment ofportal hypertension It is important to appreciate that gastricvarices can bleed at pressures lt12 mm Hg and the influence ofwall tension of the varix plays a greater role in the risk of bleed-ing43 A greater pressure reduction may be necessary to protectagainst bleeding This is further discussed in the section lsquoGastricvaricesrsquo At present measurement of portal pressure in guidingpharmacological treatments is limited to clinical trials in the UK
Variceal sizeVariceal size is best assessed endoscopically (figure 1AndashC)Published results are variable owing to the lack of a definition dis-tinguishing between large and small varices Small (grade I)varices tend to be narrow and flatten easily with air whereaslarger (grade 2 and 3) varices are usually broader and flatten withdifficulty if at all Numerous studies40 44 have shown that therisk of variceal haemorrhage increases with the size of varices45
Variceal wall and tensionPolio and Groszmann46 using an in vitro model showed thatrupture of varices was related to the tension on the varicealwall The tension depends on the radius of the varix In thismodel increasing the size of the varix and decreasing the thick-ness of the variceal wall caused variceal rupture Recently endo-scopic ultrasound and manometry have been used to estimatewall tension of varices47
Endoscopic features such as lsquored spotsrsquo and lsquowhalersquo markingswere first described by Dagradi24 They have been described asbeing important in the prediction of variceal haemorrhageThese features represent changes in variceal wall structure andtension associated with the development of microtelangiectasiasand reduced wall thickness In a retrospective study by theJapanese Research Society for Portal Hypertension Beppuet al48 showed that 80 of patients who had blue varices orcherry red spots bled from varices suggesting that this was animportant predictor of variceal haemorrhage in cirrhosis
Severity of liver disease and bleeding indicesTwo independent groups prospectively assessed factors predict-ing first variceal haemorrhage in cirrhosis (table 2) The NorthItalian Endoscopic Club (NIEC)49 reported their findings in1988 followed in 1990 by data from the Japanese50 Both thesestudies showed that the risk of bleeding was based on threefactors severity of liver disease as measured by Child class vari-ceal size and red wale markings The NIEC study showed awide range for the risk of bleeding of 6ndash76 depending on thepresence or absence of the different factors Using the same vari-ables the NIEC index was simplified by de Franchis et al51 andshown to correlate with the original index Further studiesshowed that the HVPG and intravariceal pressure were alsoindependent predictors of first variceal haemorrhage when ana-lysed in conjunction with the NIEC index52 53
In summary the most important factors that determine the risk ofvariceal haemorrhage are the severity of liver disease size of varicesand presence of red signs Measurement of HVPG is a useful guidefor selection of patients for treatment and their response to
treatment although the predictive value does not appear toimprove on the NIEC index and presence of red whale marking54
Risk and mortality of first variceal bleedData describing the overall risk of bleeding from varices must beviewed with caution and have some pitfalls in interpretationThe natural history of patients who have varices that are diag-nosed as part of their baseline investiations is different fromthat of patients who have complications of liver disease such asascites and encephalopathy Most studies do not comment oneither the severity of liver disease or whether patients with alco-holic cirrhosis are continuing to drink Both these factors have asignificant effect on the risk of variceal haemorrhage
Most studies report bleeding from varices in about 20ndash50of patients with cirrhosis during the period of follow-up Bakeret al23 reported variceal bleeding in 33 of 115 patients that theyfollowed up for a mean of 33 years with a mortality of 48from the first variceal haemorrhage These data were confirmedby Christensen et al18 About 70 of the episodes of bleedingoccur within 2 years of diagnosis Recent studies demonstrate adramatic reduction in mortality following variceal bleeding of20 6-week mortality55 and 15 in-hospital mortality5 withcontributions from improved endoscopic pharmacological andradiological therapies notably TIPSS Intensive care treatmenthas also improved with outcomes being particularly good forthose requiring minimal organ support
Analysis of the non-active treatment arms in the primaryprophylaxis trials comparing propranolol with placebo showresults similar to those of the primary prophylaxis shunt trialswith most episodes of bleeding occurring within the first 2 yearsof follow-up In these studies the rate of first variceal haemor-rhage ranged from 22 to 6156ndash60 This large difference inthe rate of first bleed relates almost certainly to the number ofpatients with severe liver disease included in the study (PascalChild Cmdash46 bleedingmdash61 Italian Multicenter Project forPropranolol in Prevention of Bleeding (IMPP) Child Cmdash6bleedingmdash32 Conn Child Cmdash6 bleedingmdash22)Mortality varied from 24 to 49 over 2 years (Pascal mortal-itymdash49 IMPP mortalitymdash24 Conn mortalitymdash24)
Primary prophylaxisSince 30ndash50 of patients with portal hypertension will bleedfrom varices and about 20 will die from the effects of the first
Table 2 Scoring systems for quantifying the severity of cirrhosisSeverity of liver disease can be described using the ChildndashPughscore or MELD scoreThe ChildndashPugh score is the sum of severity scores for Child classvariceal size and red wale markings the variables shown below
Category 1 2 3
Encephalopathy 0 III IIIIVAscites Absent Mild-moderate SevereBilirubin (μmolL) lt34 34ndash51 gt51Albumin (gL) gt35 28ndash35 lt28INR lt13 13ndash15 gt15
ChildndashPugh class A represents a score of le6 class B a score of 7ndash9 and class C ge10The MELD score is a formula that includes three laboratory-based variables reflectingthe severity of liver disease It was originally used to predict the short-term mortalityafter placement of a transjugular intrahepatic portosystemic stent-shunt for varicealbleeding Subsequently it has been used in selecting candidates for livertransplantationMELD score please use the online calculator httpswwwesotorgElitameldCalculatoraspxINR international normalised ratio
8 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleed it seems rational to develop prophylactic regimens toprevent the development of and bleeding from these varicesHowever most of the published trials do not have sufficientpower to identify favourable treatment effects Based on theexpected bleeding and death rates in the control group theminimum number of patients needed to detect a 50 reductionin bleeding would be 270 and 850 patients in each arm todetect the same reduction in mortality A proposed algorithmfor surveillance and prophylaxis of varices is shown in figure 2At this time there is insufficient evidence to support treatingpatients without varices or lsquopre-primary prophylaxisrsquo A largerandomised placebo-controlled trial of timolol in patientswithout varices and portal hypertension defined as HVPGgt6 mm Hg did not show any effect on the development ofvarices or variceal bleeding27 The role of drug treatment in pre-venting bleeding in patients with small varices is unclear Threerandomised placebo-controlled trials have studied this Caleset al61 showed that propranolol in patients with small or novarices resulted in greater development of varices Howeverpatients without varices were included and there was significantloss of patients to follow-up The second trial showed thatnadolol reduced variceal bleeding without survival benefit andincreased adverse events62 Sarin et al63 did not show any effectwith propranolol despite a significant effect on portal pressure
SurgeryPortacaval shuntsFour trials of portacaval shunts have been published which ran-domised a total of 302 patients64ndash67 either to prophylactic shuntsurgery or to non-active treatment A meta-analysis of thesestudies showed a significant benefit in the reduction of varicealbleeding (OR=031 95 CI 017 to 056) but also a signifi-cantly greater risk of hepatic encephalopathy (OR=2 95 CI12 to 31) and mortality (OR=16 95 CI 102 to 257) inpatients treated with shunt surgery68 At this time there is noevidence for the use of TIPSS for primary prophylaxis1
Devascularisation proceduresInokuchi50 showed that there was a significant reduction in vari-ceal bleeding and in mortality in patients treated with a varietyof devascularisation procedures There are however numerousproblems with the interpretation of this study because of theuse of different procedures in each of the 22 centres Theseresults require confirmation
Pharmacological treatmentNon-cardioselective β blockersThe mainstay of the pharmacological approach to the primaryprophylaxis of variceal haemorrhage has been NSBBPropranolol which has been shown to reduce the PPG reduceazygos blood flow and also variceal pressure It achieves this bycausing splanchnic vasoconstriction and reducing cardiacoutput There is no clear dose-related reduction in HVPG orcorrelation of HPVG reduction with reduction in heart rate69
Observational studies have shown that a 10ndash12 reduction inHVPG after acute administration of propranolol was associatedwith reduced bleeding and hepatic decompensation54 70
However HVPG monitoring is not routinely available in mostcentres outside of larger institutions A meta-analysis of nineplacebo-controlled randomised trials (964 patients) showed thatthe pooled risk difference for bleeding was minus11 (95 CIminus21 to minus1) and for death was minus9 (95 CI minus18 tominus1) in favour of propranolol71
Nadolol exerts similar effects on portal haemodynamicsalthough the effect on blood pressure may not be as pro-nounced Two placebo-controlled trials58 59 have shownreduced bleeding although in one study this was only seen onper protocol analysis59 There was no effect on overall survival
Carvedilol is a NSBB like propranolol and a vasodilator dueto α1 receptor blockade The latter reduces portocollateralresistance and by actions on hepatic stellate cells leads to areduction in intrahepatic resistance Haemodynamic studiesdemonstrate a greater reduction in portal pressure with
Figure 2 Algorithm for surveillance of varices and primary prophylaxis in cirrhosisndash If there is clear evidence of disease progression this interval can be modified by clinician Endoscopy should also be offered at time ofdecompensation
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 9
Guidelines
carvedilol than with propranolol although blood pressure isreduced72 73 The optimum dose is 625ndash125 mgday74 Higherdoses are not more effective and are associated with moreadverse eventsmdashin particular hypotension Carvedilol at a doseof 125 mgday at current UK prices is considerably cheaperthan propranolol 40 mg twice a day and nadolol 80 mgday(monthly cost pound120 pound562 and pound5 respectively) Two RCTs ofcarvedilol versus variceal band ligation (VBL) in primaryprophylaxis have been published75 76 The first study75 showedsignificantly reduced bleeding in the carvedilol arm (10 vs23 relative hazard 041 95 CI 019 to 096) with no effecton survival The second trial by Shah et al76 did not show anydifferences in bleeding or mortality Compliance with VBL wasbetter in the latter trial and unlike the first trial there were sig-nificantly more patients with viral hepatitis than alcoholic cir-rhosis A further study74 assessed the effect of carvedilol inpatients who were haemodynamic non-responders to propran-olol where haemodynamic response was defined as HVPGreduction to le12 mm Hg or by gt20 of baseline after 4 weeksof treatment Patients who were haemodynamic non-respondersor intolerant to carvedilol were treated with VBL Carvedilolresulted in significantly lower variceal bleeding compared withVBL and haemodynamic responders to carvedilol or propran-olol had significantly lower mortality than those treated withVBL It is worth noting that the study was not randomised
There have been recent suggestions based on low-level evi-dence that NSBB may result in a poorer outcome in patientswith cirrhosis and refractory ascites77 The lsquowindow hypothesisrsquofor β blockers in cirrhosis has also recently been described sug-gesting that NSBB are helpful in the compensated and earlydecompensated cirrhotic period but may not be helpful in veryearly cirrhosis such as in a patient with no varices and may beharmful in patients with end-stage cirrhosis with refractoryascites78 However recent large observational studies questionthe last hypothesis with improved survival seen in patients withrefractory ascites treated with NSBB79 unless patients have anepisode of spontaneous bacterial peritonitis80 Therefore untilthere are further prospective controlled studies NSBB should becontinued in patients with refractory ascites The clinician mustcarefully monitor haemodynamic parameters such as blood pres-sure and discontinue NSBB in patients with hypotension andrenal impairment as can occur after an episode of spontaneousbacterial peritonitis Other potentially severe adverse eventswith NSBB include symptomatic bradycardia asthma andcardiac failure Less severe side effects such as fatigue insomniaand sexual dysfunction may also result
Isosorbide mononitrateInterest in the use of vasodilators such as isosorbide mononitrate(ISMN) developed after the demonstration that it reduces portalpressure as effectively as propranolol81 but has subsequentlywaned A trial comparing ISMN with propranolol showed nosignificant difference between these agents82 Another rando-mised trial of ISMN versus placebo did show any difference inthe two arms83 Therefore ISMN is not recommended asmonotherapy in primary prophylaxis
β Blocker and ISMNThe combination of nadolol and ISMN has been compared withnadolol in a RCT The combination therapy reduced the fre-quency of bleeding significantly but no significant differenceswere detected in mortality84 However Garcia-Pagan et al85 in adouble-blind RCTof propranolol plus ISMN versus propranolol
plus placebo failed to show any differences between the twoarms Combination therapy is associated with more side effects
Proton pump inhibitorsA placebo-controlled randomised trial reported reduced bleed-ing and mortality with rabeprazole after eradication of varices86
However the study had a heterogeneous population with VBLperformed for both primary and secondary prophylaxis andsmall numbers (n=43) limiting the validity of the conclusionsFurthermore there was no arm comparing proton pump inhibi-tors with NSBB The use of proton pump inhibitors in patientswith cirrhosis and ascites was associated with increased risk ofspontaneous bacterial peritonitis in a large retrospective study87
This was not confirmed in a larger prospective non-randomisedstudy88 However a recent prospective observational study hasshown proton pump use to be associated with increased mortal-ity in cirrhosis89 Proton pump inhibitors are also associatedwith increased risk of Clostridium difficile infection90 Thereremains continuing concern about proton pump inhibitors inpatients with cirrhosis therefore caution should be used
Endoscopic therapyVariceal band ligationVBL has been compared with NSBB in 19 trials in a recentCochrane meta-analysis of 1504 patients91 Despite reducedbleeding (RR=067 95 CI 046 to 098) with VBL there wasno difference in overall mortality and bleeding-related mortalityThe difference in bleeding was not seen when only trials withlow selection or attrition bias were included Banding can haveserious complications The risk of fatal banding-induced bleed-ing was highlighted in a meta-analysis showing reduced fataladverse events with NSBB (OR=014 95 002 to 099)92
The optimal timing of banding intervals is discussed in thesection lsquoSecondary prophylaxis of variceal haemorrhagersquo A ran-domised trial of 96 patients who underwent endoscopic surveil-lance at 6 or 3 months after eradication of varices with VBL didnot demonstrate a difference in bleeding on mortality93
However the trial had a heterogeneous study group of patientswho underwent VBL both for primary (65) and secondaryprevention (35)
SclerotherapyNineteen trials have compared endoscopic variceal sclerotherapywith no treatment68 Owing to the marked heterogeneitybetween these studies a meta-analysis is clinically inappropri-ate68 Sclerotherapy does not offer any benefit in combinationwith NSBB or VBL compared with VBL or NSBB alone andincreases iatrogenic complications such as strictures94ndash96 At thistime sclerotherapy cannot be recommended for prophylaxis ofvariceal haemorrhage in patients with cirrhosis
Recommendations primary prophylaxis of variceal haemor-rhage in cirrhosis (figure 2)1 What is the best method for primary prophylaxis
11 We recommend NSBB or variceal band ligation (VBL)We suggest pharmacological treatment with propranololas first line VBL is offered if there are contraindicationsto NSBB The choice of VBL or NSBB should also takeinto account patient choice (level 1a grade A)
12 We suggest carvedilol or nadolol as alternatives to pro-pranolol (level 1b grade A)
13 Dose131 Propranolol 40 mg twice daily Dose titrated to
maximum tolerated or once heart rate (HR) of
10 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
50ndash55 bpm is reached to a maximum dose of320 mg (level 1a grade A)
132 Nadolol 40 mg daily dose Dose titrated tomaximum tolerated or once HR of 50ndash55 bpm isreached a maximum dose of 240 mg (level 1agrade A)
133 Carvedilol 625 mg once daily to increase tomaintenance of 125 mg after a week if toleratedor once HR of lt50ndash55 bpm is reached (level 1agrade A)
134 It is suggested that NSBB are discontinued at thetime of spontaneous bacterial peritonitis renalimpairment and hypotension (level 2b grade B)
14 In cases of contraindications or intolerance to NSBB werecommend variceal band ligation (level 1a grade A)
2 Who should have surveillance for variceal bleeding21 We recommend all patients with cirrhosis should be
endoscoped at the time of diagnosis (level 1a grade A)There is no indication to repeat endoscopy in patientsreceiving NSBB
3 How often should cirrhotic patients be endoscoped31 If at the time of first endoscopy no varices are seen we
suggest that patients with cirrhosis should be endos-coped at 2ndash3-year intervals (level 2a grade B)
32 If grade I varices are diagnosed we suggest that patientsshould be endoscoped at yearly intervals (level 2agrade B)
33 If there is clear evidence of disease progression wesuggest that the intervals can be modified by a clinicianEndoscopy should also be offered at time of decompen-sation (level 2a grade B)
4 Which patients with cirrhosis should have primaryprophylaxis41 If grade I varices and red signs or grade 2ndash3 varices are
diagnosed we recommend that patients have primaryprophylaxis irrespective of the severity of the liverdisease (level 1a grade A)
5 Treatments not recommended51 Proton pump inhibitors are not recommended unless
otherwise required for peptic ulcer disease (level 1bgrade B)
52 Isosorbide mononitrate monotherapy is not recommendedas primary prophylaxis (level 1b grade A) There is insuffi-cient evidence to recommend isosorbide mononitrate incombination with NSBB (level 1b grade A)
53 Shunt surgery or TIPSS is not recommended as primaryprophylaxis (level 1a grade A)
54 Sclerotherapy is not recommended as primary prophy-laxis (level 1a grade A)
6 Areas requiring further study61 Role of NSBB in patients without varices with focus on
carvedilol62 Role of NSBB in patients with small varices with focus
on carvedilol63 Comparison of carvedilol versus propranolol in primary
prophylaxis64 Identification of and trials assessing new drugs for
primary prophylaxis such as statins7 Quality indicator
71 Percentage of patients at diagnosis of cirrhosis who havehad an endoscopy to screen for varices (level 1agrade A)Numerator patients diagnosed with cirrhosis who havehad an endoscopy either before or after diagnosis within
6 monthsDenominator patients newly diagnosed with cirrhosis
72 Percentage of patients receiving primary prophylaxisamong those newly diagnosed with grade I varices andred signs or grade 2ndash3 varicesNumerator patients who have grade 1 varices with redsigns or grade 2ndash3 varices receiving primary prophy-laxisDenominator patients diagnosed with cirrhosis whohave grade I varices with red signs or grade 2ndash3 varices
MANAGEMENT OF ACTIVE VARICEAL HAEMORRHAGEThe average 6-week mortality of the first episode of varicealbleeding in most studies is reported to be up to 20 There hasbeen considerable improvement in survival since the early 1980swhen the in-hospital mortality was 40ndash5097 compared with15 from a recent UK audit5 Such is the improvement in out-comes that a patient with Childrsquos A cirrhosis is very unlikely tosuccumb to an index variceal bleed Studies have shown theChildndashPugh score MELD score and HVPG to be strong predic-tors of outcomes98ndash103 The MELD score has been shown tooutperform Childrsquos score in a recent study with a score gt19associated with 20 6 week mortality103 Furthermore theMELD score has been shown to perform as well as the trad-itional intensive care unit scores in predicting mortality inpatients admitted to intensive care in the UK104 MELD gt18active bleeding transfusing gt4 units of packed red blood cellshave been shown to be predictors of mortality and earlyrebleeding99 101 102 HVPG has also been shown to predictoutcome when measured at 2 weeks after a bleed44 and a valueof ge20 mm Hg when measured acutely within 48 h has beenshown to provide significant prognostic information100
However this technique is not used routinely in the manage-ment of patients around the world and substitution of clinicaldata in the latter study was shown to provide the same clinicalpredictive value100 These scoring systems are not purely aca-demic they allow the referring clinician to predict thosepatients with a high chance of rebleeding to be transferred to aspecialist centre offering for instance TIPSS before the patientrebleeds
Nonetheless probably the most important step in the man-agement of acute variceal haemorrhage is the initial resuscitationassessed according to standard lsquoABCrsquo practice together withprotection of the airway to prevent aspiration Although earlyendoscopy allows for accurate diagnosis of the bleeding site anddecisions about management (figure 3) therapeutic interventionin acute variceal bleeding can be initiated safely in most casesbefore diagnostic endoscopy As similar efficacy is demonstratedwith pharmacological treatment as with sclerotherapy theformer should be first-line therapy99 β Blockade should not bestarted in the acute setting and those already taking β blockersas prophylaxis should probably stop taking them for 48ndash72 h inorder that the patientrsquos physiological response to blood loss canbe allowed to manifest
General considerationsPatient evaluationThe majority of patients with a variceal bleed will be sufficientlystable to enable a full history and examination to take placeHistory of alcohol excess and or intravenous drug use should besought and may become particularly relevant if the patient haswithdrawal symptoms after admission Comorbidity is importantwhen estimating risk and deciding on use of vasopressors The
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 11
Guidelines
following risk factors doubled mortality after an acute varicealbleed in one US study older age comorbidities male gender andnot undergoing a gastroscopy within 24 h105
A full examination is helpful for the important negatives asmuch as the positives Baseline observations should include thetemperature as infection is a serious complication with signifi-cant mortality Confusion may be present because of encephal-opathy intoxication with alcohol or drugs or withdrawal fromalcohol or drugs The patient should be on continuous BP andpulse monitor and their haemodynamic status recordedAn oxygen saturation monitor is helpful Stigmata of chronicliver disease and concurrent jaundice provide insight into thecurrent status of a patientrsquos liver and also give warning ofpotential further decompensation if significant bleeding persists(see scoring systems above) Pneumonia must be actively
excluded Evidence of ascites requires a diagnostic tap to searchfor infection
Investigations including full blood count coagulationprofile liver and renal function and blood group and save andcross-match Blood and urine should also be cultured An ultra-sound scan later in the admission is helpful to identify subclin-ical ascites flow in portal vein and any obvious emergence of anhepatocellular carcinoma (HCC)
Location of patientA decision must be made as to where the patient is best managedVariceal bleeding is unpredictable generally occurs in patientswith significant liver disease and is associated with significant mor-tality Hence a high-dependency unit is usually the most appropri-ate initial location although a properly staffed lsquogastrointestinal
Figure 3 Algorithm for themanagement of acute varicealbleeding TIPSS transjugularintrahepatic portosystemic stent shunt
12 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleeding bedrsquo may be appropriate If a patient is vomiting bloodor there is a perceived risk of a haemodynamically unstable patienthaving blood in the stomach then the patient must be intubatedbefore endoscopy and return to an intensive care or high-dependency unit will be necessary until extubation
Volume resuscitation and blood productsIntravenous access (two 16ndash18G cannulae) should have beensecured on admission with a reported GI bleed Further intra-venous access may be necessary In patients with poor venousaccess advanced liver disease or renal failure associated withtheir liver disease central venous access may be helpful withguiding fluid infusions However the drawbacks include the riskof the procedure and a potential source of infection Thereforethere is no absolute requirement for a central line and no evi-dence of unequivocal benefit Intravenous fluid resuscitationshould be initiated with plasma expanders aiming to maintain asystolic blood pressure of 100 mm Hg Care with monitoring isparamount in this group of patients
Overtransfusion has been shown to have a deleterious effecton outcome In a recent single-centre RCT a restrictive transfu-sion policy of maintaining haemoglobin between 70 and 80 gLimproved the control of variceal bleeding (11 vs 22p=005) and lowered HVPG compared with a liberal transfu-sion policy without effect on 45-day survival106 However itshould be noted that these results were from a single Spanishcentre which was a tertiary unit for variceal bleeding where allpatients underwent endoscopy within 6 h Nonetheless arestrictive transfusion policy has been recommended for sometime1 and there is now good evidence to support not transfusinga stable patient with a haemoglobin of ge80 gL However under-resuscitation should also be avoided and while goal-orientedfluid replacement has generally not been useful in an intensivetherapy unit setting a venous saturation gt70 remains an easilymeasurable target with some evidence to support it107
Interpretation and management of clotting profile is challen-ging in liver disease where there is usually a balanced deficiencyof both procoagulant and anticoagulant factors108 The NICEguidelines recommend activation of a hospitalrsquos massive transfu-sion policy when there is major haemorrhage and plateletsupport when the value is lt50 and clotting factor supportwhen the international normalised ratio (INR) is gt15 timesnormal2 There is no evidence for the use of lsquoprophylacticrsquo clot-ting or platelet support to reduce the risk of rebleeding Thereis insufficient evidence to support the routine use of transexamicacid or recombinant factor VIIa109
Pharmacological treatmentThe two major classes of drugs that have been used in thecontrol of acute variceal bleeding are vasopressin or its analo-gues (either alone or in combination with nitroglycerine) andsomatostatin or its analogues Terlipressin is the only agent thathas been shown to reduce mortality in placebo-controlled trialsHowever in trials comparing terlipressin somatostatin andoctreotide no difference in efficacy was identified in a system-atic review110 and in a recent large RCT111 Prophylactic anti-biotics can result in a similar survival benefit following acutevariceal bleeding
VasopressinVasopressin reduces portal blood flow portal systemic collateralblood flow and variceal pressure It does however have signifi-cant systemic side effects such as an increase in peripheral resist-ance and reduction in cardiac output heart rate and coronary
blood flow In comparison with no active treatment the pooledresults of four randomised trials showed that it reduced failureto control variceal bleeding (OR=022 95 CI 012 to 043)although survival was unaffected68 Meta-analysis of five trialscomparing sclerotherapy with vasopressin has shown a signifi-cant effect on reduction in failure to control bleeding(OR=051 95 CI 027 to 097) with no effect on survival68
Vasopressin with nitroglycerineThe addition of nitroglycerine enhances the effect of vasopres-sin on portal pressure and reduces cardiovascular side effects112
Meta-analysis of three randomised trials comparing vasopressinalone with vasopressin and nitroglycerine showed that the com-bination was associated with a significant reduction in failure tocontrol bleeding (OR=039 95 CI 022 to 072) although nosurvival benefit was shown68
TerlipressinTerlipressin is a synthetic analogue of vasopressin which has animmediate systemic vasoconstrictor action followed by portalhaemodynamic effects due to slow conversion to vasopressin Ina Cochrane meta-analysis of seven placebo-controlled trials ter-lipressin was shown to reduce failure to control bleeding(RR=066 95 CI 055 to 093) and also to improve survival(RR=066 95 CI 049 to 088)113 In the same meta-analysisthere was no difference between terlipressin versus vasopressinballoon tamponade or endoscopic therapy in failure to controlbleeding or survival113 The role of terlipressin in combinationwith VBL is explored in the section lsquoEndoscopic therapy incombination with pharmacological therapyrsquo
The recommended dose of terlipressin is 2 mg IV every 4 halthough many units reduce the dose to 6 hourly as it may causeperipheral vasoconstriction which manifests as painful handsand feet While 5 days of IV treatment has been advocated inthe Baveno V guidelines1 this prolonged treatment has notbeen shown to have a survival benefit and for pragmaticreasons many units will stop treatment shortly after satisfactoryhaemostasis In a randomised trial terlipressin given for 24 hafter satisfactory haemostasis with VBL after oesophageal vari-ceal bleeding was as effective as 72 h of treatment114
In patients intolerant of terlipressin or in countries where ter-lipressin is not available alternatives should be considered
Somatostatin and octreotideSomatostatin causes selective splanchnic vasoconstriction andreduces portal pressure and portal blood flow115 Octreotide is asomatostatin analogue The mechanism of action of these twoagents is not clear Inhibition of glucagon increases vasodilatationrather than a direct vasoconstrictive effect and post-prandial guthyperaemia is also reduced The actions of octreotide on hepaticand systemic hemodynamics are transient making continuousinfusion necessary Octreotide is given as a 50 μg bolus followedby an infusion of 25ndash50 μgh Somatostatin is given as a 250 mgintravenous bolus followed by an infusion of 250 mghSomatostatin and octreotide have been shown to be aseffective as terlipressin in acute variceal bleeding in ameta-analysis110 Seo et al111 in a large RCTof 780 patients com-paring these three agents failed to show a difference in treatmentsuccess (range 838ndash862) rebleeding (range 34ndash44) andmortality (range 8ndash88) A low systolic blood pressure at pres-entation high serum creatinine level active bleeding in the emer-gency endoscopy gastric variceal bleeding and ChildndashPugh gradeC were independent factors predicting 5-day treatmentfailure111
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 13
Guidelines
AntibioticsAntibiotics that provide Gram-negative cover are one of the inter-ventions which positively influence survival in variceal haemor-rhage as shown in a Cochrane meta-analysis of 12placebo-controlled trials (RR=079 95 CI 063 to 098)116
Antibiotics were also shown to reduce bacterial infections(RR=043 95 CI 019 to 097) and early rebleeding (RR=05395 CI 038 to 074)116 Therefore short-term antibiotics shouldbe considered standard practice in all cirrhotic patients who have avariceal bleed irrespective of the presence of confirmed infectionThird-generation cephalosporins such as ceftriaxone (1 g IVdaily) have been shown to be more effective at reducingGram-negative sepsis than oral norfloxacin117 but choice of anti-biotics must be dictated by local resistance patterns and availability
Proton pump inhibitorsOne RCT compared a short course of proton pump inhibitorswith vasoconstrictor therapies after haemostasis in acute varicealbleeding118 Despite larger ulcers noted in the vasoconstrictorarm there were no differences in bleeding or survival Nearly50 of patients had ascites which might have implications inlight of the reports of increased incidence of spontaneous bac-terial peritonitis as mentioned earlier
Endoscopic therapyEndoscopy should take place within 24 h of admission andearlier if there is excessive bleeding based on low-level evi-dence105 While many guidelines and reviews suggest thatendoscopy should be carried out within 12 h the only study thatexamined the influence of timing on outcome failed to demon-strate any advantage of endoscopy before 12 h119 The optimaltime is after sufficient resuscitation and pharmacological treat-ment with the endoscopy performed by a skilled endoscopyteam in a suitably equipped theatre environment and withairway protection Airway protection is essential where risk ofaspiration is high and affords the endoscopist time for thoroughevaluation including complete clot aspiration and controlledapplication of treatment including tamponade if required Theendoscopy team must comprise an experienced endoscopynurse acquainted with the equipment necessary for endoscopytherapy of varices and a skilled endoscopist competent in usingbanding devices and deployment of balloon tamponade
Variceal band ligationThis technique is a modification of that used for the elastic bandligation of internal haemorrhoids Its use in humans was firstdescribed in 1988120 A meta-analysis of seven trials comparingVBL with sclerotherapy in acute bleeding showed that VBLreduced rebleeding from varices (OR=047 95 CI 029 to078) reduced mortality (OR=067 95 CI 046 to 098) andresulted in fewer oesophageal strictures (OR=010 95 CI003 to 029)121 The number of sessions required to obliteratevarices was lower with VBL (22 fewer sessions (95 CI 09to 35))
SclerotherapySclerotherapy has been replaced by VBL and should no longerbe offered as standard of care in acute variceal haemorrhage
Other endoscopic measuresIn an RCT cyanoacrylate offered no benefit over VBL with theadditional risk of embolisation and trend towards increasedrebleeding with cyanoacrylate122
Haemostatic powder (TC-325 Hemospray Cook MedicalUSA) has been described in a small study of nine patients whoreceived endoscopic spray treatment for acute variceal bleedingThe study reported no rebleeding within 24 h and no mortalityat 15 days123
Endoscopic therapy in combination with pharmacological therapyThe role of combining vasoactive drugs with endoscopictherapy (VBL or sclerotherapy) was reported in a meta-analysisof eight trials124 Combination therapy resulted in better initialcontrol of bleeding (RR=112 95 CI 102 to 123) and5-day haemostasis (RR=128 95 CI 118 to 139) withoutany difference in survival Adverse events were similar in bothgroups Two RCTs have compared VBL with sclerotherapy incombination with vasoactive agents in acute variceal bleed-ing125 126 Lo et al125 used vasopressin and found that VBLresulted in better 72 h haemostasis (97 vs 76 p=0009)with fewer complications (5 vs 29 p=0007) Villanuevaet al used somatostatin and reported lower failure to controlacute bleeding with VBL (4 vs 15 p=002) with fewerserious complications (4 vs 13 p=004) Overall survivalwas similar in both trials125 126
Balloon tamponadeBalloon tamponade is highly effective and controls acute bleed-ing in up to 90 of patients although about 50 rebleed whenthe balloon is deflated127 128 It is however associated withserious complications such as oesophageal ulceration and aspir-ation pneumonia in up to 15ndash20 of patients Despite this itmay be a life-saving treatment in cases of massive uncontrolledvariceal haemorrhage pending other forms of treatment Anappropriately placed SengstakenndashBlakemore tube allows forresuscitation safe transportation and either repeat endoscopy orradiological shunting in a patient with a stable cardiovascularsystem The oesophageal balloon is rarely required must neverbe used on its own and should be used only if there is continu-ing bleeding despite an adequately inflated gastric balloon cor-rectly placed and with appropriate tension Placement of thetube endoscopically or over a guide wire might reduce the riskof complications especially oesophageal rupture
Removable oesophageal stentsThe SX-Ella Danis stent (ELLA-CS Hradec Kralove CzechRepublic) is a removable covered metal mesh stent placed endo-scopically in the lower oesophagus without radiological screen-ing It has no role in the management of gastric varicealbleeding These stents can be left in situ for up to 2 weeksunlike the SengstakenndashBlakemore tube which should beremoved after a maximum of 24ndash48 h129 130 No published con-trolled trials have compared this modality with balloontamponade
Transjugular intrahepatic portosystemic stent-shuntSeveral uncontrolled studies have examined the role of salvagebare TIPSS in acute variceal bleeding In a review of 15 studiescontrol of bleeding was achieved in 90ndash100 with rebleedingin 6ndash16131 Mortality varied between 75 (in hospital) and15 (30 day) It is important to appreciate that sclerotherapywas used as first-line endoscopic therapy in most of thesestudies Long-term follow-up of a study that compared TIPSSwith H-graft portacaval shunts in patients for whom non-operative management had failed suggested that H-grafts were auseful method of reducing portal pressure and had a signifi-cantly lower failure rate (p=004) but had no significant
14 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
improvement in overall survival despite a benefit seen in ChildrsquosA and B disease132 A recent RCT compared emergency porto-caval surgery with bare TIPSS within 24 h of presenting withacute oesophageal variceal bleeding in unselected cirrhoticpatients Emergency portocaval surgery resulted in better out-comes for long-term bleeding control encephalopathy and sur-vival (plt0001)133 Before wider application of surgery foracute variceal bleeding more data are needed in light of therecent adoption of covered stents
There has also been a generalised established change in prac-tice in using covered TIPSS stents (polytetrafluoroethylene(PTFE)) rather than a bare metal stent with evidence to supportthis change In randomised controlled studies these stents wereshown to have higher primary patency rates than bare stentswithout significant differences in survival and the potential forreduced incidence of hepatic encephalopathy134 135
There is however growing evidence from two RCTs for theearlier use of TIPSS in selected patients stratified by HVPGChildndashPugh class and active bleeding and not just use as asalvage option6 136 Monescillo et al136 randomised patientspresenting with acute oesophageal variceal haemorrhage to bareTIPSS or standard of care if the HVPG was ge20 mm Hg within24 h of admission Significantly reduced treatment failure asdefined by failure to control acute bleeding andor early rebleed-ing (12 vs 50) was seen and improved survival (62 vs35) in the patients randomised to undergo a TIPSS procedureHowever the standard of care was sclerotherapy and not com-bination endoscopic and pharmacological treatment This limita-tion and the lack of availability of HVPG measurement in mostcentres meant this trial did not have a significant impact on clin-ical practice
Garcia-Pagan et al6 selected patients with active bleeding andChildrsquos B cirrhosis or patients with Childrsquos C cirrhosis (Childrsquosscore lt14) for randomisation to early PTFE-covered TIPSSwithin 72 h or standard of care with VBL and pharmacologicaltreatment This has shown encouraging results with reduced riskof treatment failure (3 vs 50) improved survival (86 vs61 at 1 year) yet without increased risk of hepatic encephal-opathy The results were supported by an observational studyfrom the same group although a survival benefit was notseen137 Furthermore a recent well-conducted observationalstudy did not demonstrate such high survival rates with earlyTIPSS with 11-year survival of 67 which was similar to thatof patients given endoscopic and pharmacological treatmentsonly138 Therefore larger multicentred RCTs need to be under-taken to further evaluate the role of early TIPSS It is importantto make the distinction between salvage TIPSS and early TIPSSto prevent rebleeding
Liver transplantationThis is probably appropriate only for patients who bleed whileawaiting liver transplantation although studies comparing VBLor TIPSS placement with urgent liver transplantation in thissituation need to be done Liver transplantation is an exceed-ingly rare option for the vast majority of patients both becauseit is not commonly available and because of shortages anddelays in organ procurement No controlled trials of liver trans-plantation in uncontrolledactive bleeding are available
Recommendations for the control of variceal bleeding in cir-rhosis are given below and in figure 3
Recommendations control of active variceal haemorrhage incirrhosis (figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with bloodplatelets and clotting factors in line with local protocolsfor managing massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusionpolicy aiming for a haemoglobin of 70ndash80 gL is sug-gested in haemodynamically stable patients (level 1bgrade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable(level 5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L(level 5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to localcircumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with suspected
or confirmed variceal bleeding (level 1a grade A)32 In all patients vasoconstrictors such as terlipressin or
somatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 15
Guidelines
41 If bleeding is difficult to control a SengstakenndashBlakemore tube should be inserted until further endo-scopic treatment TIPSS or surgery is performed depend-ing on local resources and expertise (level 1b grade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure (level1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
SECONDARY PROPHYLAXIS OF VARICEAL HAEMORRHAGEβ BlockersA meta-analysis of 12 trials comparing propranolol or nadolol139
with no active treatment showed a significant reduction inrebleeding but no significant reduction in mortality140 Thegreater reduction in portal pressure with carvedilol comparedwith propranolol has been described in the section lsquoPrimaryprophylaxisrsquo of this guideline
NitratesThe addition of ISMN to NSBB has been shown to reduce vari-ceal rebleeding compared with NSBB alone although no sur-vival benefit was seen141 In addition adverse events leading todrug withdrawal were more common in the group receivingcombined drug treatment A meta-analysis of ISMN alone orwith either NSBB or endoscopic therapy reported that there wasno mortality benefit from combining nitrates and NSBB com-pared with NSBB alone142
Side effects of ISMN include dizziness and headache Owingto the side effects and relative lack of data ISMN is not com-monly used in clinical practice
A recent RCT of 121 patients reported carvedilol to besimilar to combined ISMN and NSBB therapy in the preventionof variceal rebleeding and mortality although severe adverseevents were less common with carvedilol143
SimvastatinA recent abstract of a multicentre RCT of 158 patients reporteda survival benefit (91 vs 78 p=003) from adding simvasta-tin to VBL and NSBB compared with placebo VBL and NSBBas treatment for the prevention of variceal rebleeding144 Therewas no difference in rebleeding and the survival benefit wasrestricted to Child A and B patients Serious adverse events weresimilar in both groups More data are required to investigatethis interesting observation of a survival benefit from simvastatinin this situation which may relate to its effects on hepatocellularfunction fibrosis and portal pressure
Proton pump inhibitorsA double-blind randomised placebo-controlled trial showed thatpantoprazole reduced the size of ulcers in patients who under-went VBL However the total number of ulcers and other out-comes were similar in the two groups145
Endoscopic therapyVBL has been accepted as the preferred endoscopic treatmentfor the prevention of variceal rebleeding with a lower rate ofrebleeding mortality and complications than sclerother-apy146 147 The time interval between VBL sessions to achieveeradication of varices is debateable However a recent RCTcomparing monthly with biweekly VBL after initial haemostasiswith VBL in 70 patients suggested that there were fewerpost-VBL ulcers in the monthly group (11 vs 57plt0001)148 Variceal recurrence rebleeding and mortality weresimilar in both groups
Two meta-analyses showed there is no evidence that the add-ition of sclerotherapy to VBL improves clinically relevant out-comes including variceal rebleeding and death and thecombination led to higher stricture rates149 150
Endoscopic therapy versus drug therapyVBL has been reported to be more effective than combinedNSBB and ISMN drug therapy151 However an 8-yearfollow-up study of this RCT found that although VBL wassuperior in reducing variceal rebleeding survival rates were sig-nificantly higher in the group treated with combined drug treat-ment152 Other studies have found no superiority of VBL overcombined drug therapy for prevention of variceal rebleeding ormortality153 154 A recent small multicentre RCT reported carve-dilol to be similar to VBL in the prevention of variceal rebleed-ing with a trend in favour of survival with carvedilol (73 vs48 p=0110)155
Several meta-analyses have compared drug therapy with VBLin the prevention of variceal rebleeding One meta-analysis ofsix RCTs showed no significant difference in variceal rebleedingrates when comparing VBL alone with combined NSBB andISMN therapy However all-cause mortality was significantlyhigher in patients treated with the VBL (RR=125 95 CI101 to 155)156 Three meta-analyses comparing drug therapy(NSBB alone or with ISMN) with endoscopic therapy alonereported no difference in variceal rebleeding or mortality157ndash159
Endoscopic+drug therapy versus either aloneNumerous studies and several meta-analyses have comparedcombined endoscopic and drug therapy with monotherapy(endoscopic or drugs alone) in the prevention of varicealrebleeding A meta-analysis of 23 trials assessing sclerotherapyor VBL combined with NSBB reported that combinationtherapy reduced rebleeding more than either endoscopic
16 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

using a competing risk model showed that the cumulative inci-dence of varices at 10 and 20 years was 44 and 53 respect-ively suggesting an overestimation in previous studies not usinga competing risk model
The main factors that appear to determine the developmentof varices are continued hepatic injury the degree of portosyste-mic shunting endoscopic appearances and portal pressureEvidence for the role of hepatic injury is derived from studies inwhich varices were shown to regress with time Baker et al23 fol-lowed up a cohort of 115 patients with oesophageal varices andshowed that varices had disappeared in nine patients regressedin seven and remained unchanged in six They concluded thatthe disappearance and regression of varices might be related toabstinence from alcohol This observation was confirmed in astudy by Dagradi24 who followed up a cohort of patients withalcoholic cirrhosis over 3 years and showed a reduction in vari-ceal size in 12 of the 15 patients with alcoholic cirrhosis whostopped drinking and an enlargement in variceal size in 17patients who continued to drink On the other hand Cales andPascal19 showed that regression of varices occurred in 16 ofpatients with alcoholic cirrhosis who continued to imbibealcohol This might be related to the development of large por-tosystemic collaterals which decompress the portal system andreduce the risk of the development of large oesophageal varicesThe degree of portosystemic shunting can be quantified bymeasuring the diameter of portal veins and collaterals and canbe significant in those with gastrorenal or splenorenal shunt-ing25 26 Others have shown that the presence of alcoholic cir-rhosis Childrsquos B or C cirrhosis and red whale signs on indexendoscopy predicted progression of varices21 Groszmannet al27 in a placebo-controlled randomised trial of timolol in213 cirrhotic patients without varices showed that a baselinehepatic venous pressure gradient (HVPG) of gt10 mm Hg or age10 increase in HVPG during follow-up were both predictiveof the development of varices
Diagnosis of gastro-oesophageal varicesUntil recently endoscopy has been used exclusively to diagnosevarices Non-invasive methods of screening for varices includecapsule endoscopy transient elastography and use of laboratoryand radiological findings
EndoscopyThere is universal acceptance that endoscopy is the lsquogold stand-ardrsquo for diagnosing gastro-oesophageal varices The main limita-tions are intraobserver variability in the diagnosis of small orgrade I oesophageal varices (figure 1AndashC) Recently unsedatednasal gastroscopy has been found to have similar accuracy toconventional endoscopy and has the advantage of tolerabilityand potential cost saving since it can be performed in the clinicsetting in some institutions28 29 However there are no con-trolled studies and banding of varices is not possible
Capsule endoscopyCapsule endoscopy uses a 26 mm pill-shaped device whichtransmits video footage which is stored and later analysedPatients are not sedated but patient cooperation is essentialIn a large study by de Franchis et al30 capsule endoscopy wascompared with standard gastroscopy The primary end point of90 or greater concordance was not achieved Lapalus et al31
in a prospective study of 120 patients demonstrated similarresults with capsule endoscopy Therefore capsule endoscopycannot be considered an alternative to standard endoscopyalthough may have a role in patient who refuse gastroscopy
Transient elastographyTransient elastography ((FibroScan Echosens Paris France) usesthe principles of ultrasound to derive tissue stiffness by measur-ing the speed of propagation of a low-frequency wave whichthen correlates with liver fibrosis Vizzutti et al32 in a study of61 patients with hepatitis C showed a sensitivity for predictionof oesophageal varices of 90 using a threshold 176 kPaHowever specificity was poor at 43 A study of 298 patientsfound the optimal cut-off point for the prediction of oesopha-geal varices was 215 kPa (sensitivity 76 and specificity78)33 In one uncontrolled study the use of transient elasto-graphy was found to be as effective as HVPG at predictingportal hypertension-related complications34 Therefore the roleof transient elastography in predicting varices is controversialdue to the lack of consistent results and controlled studies Thismodality may be more useful for predicting decompensation inpatients with cirrhosis
Radiological and serum parametersA prospective study of 311 patients with chronic hepatitis Cshowed that a platelet-to-spleen size ratio with a threshold of909 had positive and negative predictive values of 100 and94 respectively35 These good results have not been repro-duced by others as demonstrated in a meta-analysis36
Risk factors for first variceal bleedingThe factors that predispose to and precipitate variceal haemor-rhage are still not clear The suggestion that oesophagitis mayprecipitate variceal haemorrhage has been discarded37
Presently the most important factors that have been heldresponsible include (i) pressure within the varix (ii) varicealsize (iii) tension on the variceal wall and (iv) severity of theliver disease
Portal pressureIn most cases portal pressure reflects intravariceal pressure38
and a HVPG gt10 mm Hg is necessary for the development ofoesophageal varices27 There is no linear relationship betweenthe severity of portal hypertension and the risk of varicealhaemorrhage although HVPG gt12 mm Hg is an accepted
Figure 1 (A) Grade I oesophagealvarices These collapse to inflation ofthe oesophagus with air (B) Grade IIoesophageal varices These are varicesbetween grades 1 and 3 (C) Grade IIIoesophageal varices These are largeenough to occlude the lumen
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 7
Guidelines
threshold for variceal bleeding39 40 However the HVPG tendsto be higher in bleeders as well as in patients with larger varicesIn a prospective study comparing propranolol with placebo forthe prevention of first variceal haemorrhage Groszmann et al41
showed that bleeding from varices did not occur if the portalpressure gradient (PPG) could be reduced to lt12 mm HgOthers have shown that a 20 reduction in portal pressure pro-tects against further bleeding42 These haemodynamic goalshave been accepted as the aim of pharmacological treatment ofportal hypertension It is important to appreciate that gastricvarices can bleed at pressures lt12 mm Hg and the influence ofwall tension of the varix plays a greater role in the risk of bleed-ing43 A greater pressure reduction may be necessary to protectagainst bleeding This is further discussed in the section lsquoGastricvaricesrsquo At present measurement of portal pressure in guidingpharmacological treatments is limited to clinical trials in the UK
Variceal sizeVariceal size is best assessed endoscopically (figure 1AndashC)Published results are variable owing to the lack of a definition dis-tinguishing between large and small varices Small (grade I)varices tend to be narrow and flatten easily with air whereaslarger (grade 2 and 3) varices are usually broader and flatten withdifficulty if at all Numerous studies40 44 have shown that therisk of variceal haemorrhage increases with the size of varices45
Variceal wall and tensionPolio and Groszmann46 using an in vitro model showed thatrupture of varices was related to the tension on the varicealwall The tension depends on the radius of the varix In thismodel increasing the size of the varix and decreasing the thick-ness of the variceal wall caused variceal rupture Recently endo-scopic ultrasound and manometry have been used to estimatewall tension of varices47
Endoscopic features such as lsquored spotsrsquo and lsquowhalersquo markingswere first described by Dagradi24 They have been described asbeing important in the prediction of variceal haemorrhageThese features represent changes in variceal wall structure andtension associated with the development of microtelangiectasiasand reduced wall thickness In a retrospective study by theJapanese Research Society for Portal Hypertension Beppuet al48 showed that 80 of patients who had blue varices orcherry red spots bled from varices suggesting that this was animportant predictor of variceal haemorrhage in cirrhosis
Severity of liver disease and bleeding indicesTwo independent groups prospectively assessed factors predict-ing first variceal haemorrhage in cirrhosis (table 2) The NorthItalian Endoscopic Club (NIEC)49 reported their findings in1988 followed in 1990 by data from the Japanese50 Both thesestudies showed that the risk of bleeding was based on threefactors severity of liver disease as measured by Child class vari-ceal size and red wale markings The NIEC study showed awide range for the risk of bleeding of 6ndash76 depending on thepresence or absence of the different factors Using the same vari-ables the NIEC index was simplified by de Franchis et al51 andshown to correlate with the original index Further studiesshowed that the HVPG and intravariceal pressure were alsoindependent predictors of first variceal haemorrhage when ana-lysed in conjunction with the NIEC index52 53
In summary the most important factors that determine the risk ofvariceal haemorrhage are the severity of liver disease size of varicesand presence of red signs Measurement of HVPG is a useful guidefor selection of patients for treatment and their response to
treatment although the predictive value does not appear toimprove on the NIEC index and presence of red whale marking54
Risk and mortality of first variceal bleedData describing the overall risk of bleeding from varices must beviewed with caution and have some pitfalls in interpretationThe natural history of patients who have varices that are diag-nosed as part of their baseline investiations is different fromthat of patients who have complications of liver disease such asascites and encephalopathy Most studies do not comment oneither the severity of liver disease or whether patients with alco-holic cirrhosis are continuing to drink Both these factors have asignificant effect on the risk of variceal haemorrhage
Most studies report bleeding from varices in about 20ndash50of patients with cirrhosis during the period of follow-up Bakeret al23 reported variceal bleeding in 33 of 115 patients that theyfollowed up for a mean of 33 years with a mortality of 48from the first variceal haemorrhage These data were confirmedby Christensen et al18 About 70 of the episodes of bleedingoccur within 2 years of diagnosis Recent studies demonstrate adramatic reduction in mortality following variceal bleeding of20 6-week mortality55 and 15 in-hospital mortality5 withcontributions from improved endoscopic pharmacological andradiological therapies notably TIPSS Intensive care treatmenthas also improved with outcomes being particularly good forthose requiring minimal organ support
Analysis of the non-active treatment arms in the primaryprophylaxis trials comparing propranolol with placebo showresults similar to those of the primary prophylaxis shunt trialswith most episodes of bleeding occurring within the first 2 yearsof follow-up In these studies the rate of first variceal haemor-rhage ranged from 22 to 6156ndash60 This large difference inthe rate of first bleed relates almost certainly to the number ofpatients with severe liver disease included in the study (PascalChild Cmdash46 bleedingmdash61 Italian Multicenter Project forPropranolol in Prevention of Bleeding (IMPP) Child Cmdash6bleedingmdash32 Conn Child Cmdash6 bleedingmdash22)Mortality varied from 24 to 49 over 2 years (Pascal mortal-itymdash49 IMPP mortalitymdash24 Conn mortalitymdash24)
Primary prophylaxisSince 30ndash50 of patients with portal hypertension will bleedfrom varices and about 20 will die from the effects of the first
Table 2 Scoring systems for quantifying the severity of cirrhosisSeverity of liver disease can be described using the ChildndashPughscore or MELD scoreThe ChildndashPugh score is the sum of severity scores for Child classvariceal size and red wale markings the variables shown below
Category 1 2 3
Encephalopathy 0 III IIIIVAscites Absent Mild-moderate SevereBilirubin (μmolL) lt34 34ndash51 gt51Albumin (gL) gt35 28ndash35 lt28INR lt13 13ndash15 gt15
ChildndashPugh class A represents a score of le6 class B a score of 7ndash9 and class C ge10The MELD score is a formula that includes three laboratory-based variables reflectingthe severity of liver disease It was originally used to predict the short-term mortalityafter placement of a transjugular intrahepatic portosystemic stent-shunt for varicealbleeding Subsequently it has been used in selecting candidates for livertransplantationMELD score please use the online calculator httpswwwesotorgElitameldCalculatoraspxINR international normalised ratio
8 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleed it seems rational to develop prophylactic regimens toprevent the development of and bleeding from these varicesHowever most of the published trials do not have sufficientpower to identify favourable treatment effects Based on theexpected bleeding and death rates in the control group theminimum number of patients needed to detect a 50 reductionin bleeding would be 270 and 850 patients in each arm todetect the same reduction in mortality A proposed algorithmfor surveillance and prophylaxis of varices is shown in figure 2At this time there is insufficient evidence to support treatingpatients without varices or lsquopre-primary prophylaxisrsquo A largerandomised placebo-controlled trial of timolol in patientswithout varices and portal hypertension defined as HVPGgt6 mm Hg did not show any effect on the development ofvarices or variceal bleeding27 The role of drug treatment in pre-venting bleeding in patients with small varices is unclear Threerandomised placebo-controlled trials have studied this Caleset al61 showed that propranolol in patients with small or novarices resulted in greater development of varices Howeverpatients without varices were included and there was significantloss of patients to follow-up The second trial showed thatnadolol reduced variceal bleeding without survival benefit andincreased adverse events62 Sarin et al63 did not show any effectwith propranolol despite a significant effect on portal pressure
SurgeryPortacaval shuntsFour trials of portacaval shunts have been published which ran-domised a total of 302 patients64ndash67 either to prophylactic shuntsurgery or to non-active treatment A meta-analysis of thesestudies showed a significant benefit in the reduction of varicealbleeding (OR=031 95 CI 017 to 056) but also a signifi-cantly greater risk of hepatic encephalopathy (OR=2 95 CI12 to 31) and mortality (OR=16 95 CI 102 to 257) inpatients treated with shunt surgery68 At this time there is noevidence for the use of TIPSS for primary prophylaxis1
Devascularisation proceduresInokuchi50 showed that there was a significant reduction in vari-ceal bleeding and in mortality in patients treated with a varietyof devascularisation procedures There are however numerousproblems with the interpretation of this study because of theuse of different procedures in each of the 22 centres Theseresults require confirmation
Pharmacological treatmentNon-cardioselective β blockersThe mainstay of the pharmacological approach to the primaryprophylaxis of variceal haemorrhage has been NSBBPropranolol which has been shown to reduce the PPG reduceazygos blood flow and also variceal pressure It achieves this bycausing splanchnic vasoconstriction and reducing cardiacoutput There is no clear dose-related reduction in HVPG orcorrelation of HPVG reduction with reduction in heart rate69
Observational studies have shown that a 10ndash12 reduction inHVPG after acute administration of propranolol was associatedwith reduced bleeding and hepatic decompensation54 70
However HVPG monitoring is not routinely available in mostcentres outside of larger institutions A meta-analysis of nineplacebo-controlled randomised trials (964 patients) showed thatthe pooled risk difference for bleeding was minus11 (95 CIminus21 to minus1) and for death was minus9 (95 CI minus18 tominus1) in favour of propranolol71
Nadolol exerts similar effects on portal haemodynamicsalthough the effect on blood pressure may not be as pro-nounced Two placebo-controlled trials58 59 have shownreduced bleeding although in one study this was only seen onper protocol analysis59 There was no effect on overall survival
Carvedilol is a NSBB like propranolol and a vasodilator dueto α1 receptor blockade The latter reduces portocollateralresistance and by actions on hepatic stellate cells leads to areduction in intrahepatic resistance Haemodynamic studiesdemonstrate a greater reduction in portal pressure with
Figure 2 Algorithm for surveillance of varices and primary prophylaxis in cirrhosisndash If there is clear evidence of disease progression this interval can be modified by clinician Endoscopy should also be offered at time ofdecompensation
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 9
Guidelines
carvedilol than with propranolol although blood pressure isreduced72 73 The optimum dose is 625ndash125 mgday74 Higherdoses are not more effective and are associated with moreadverse eventsmdashin particular hypotension Carvedilol at a doseof 125 mgday at current UK prices is considerably cheaperthan propranolol 40 mg twice a day and nadolol 80 mgday(monthly cost pound120 pound562 and pound5 respectively) Two RCTs ofcarvedilol versus variceal band ligation (VBL) in primaryprophylaxis have been published75 76 The first study75 showedsignificantly reduced bleeding in the carvedilol arm (10 vs23 relative hazard 041 95 CI 019 to 096) with no effecton survival The second trial by Shah et al76 did not show anydifferences in bleeding or mortality Compliance with VBL wasbetter in the latter trial and unlike the first trial there were sig-nificantly more patients with viral hepatitis than alcoholic cir-rhosis A further study74 assessed the effect of carvedilol inpatients who were haemodynamic non-responders to propran-olol where haemodynamic response was defined as HVPGreduction to le12 mm Hg or by gt20 of baseline after 4 weeksof treatment Patients who were haemodynamic non-respondersor intolerant to carvedilol were treated with VBL Carvedilolresulted in significantly lower variceal bleeding compared withVBL and haemodynamic responders to carvedilol or propran-olol had significantly lower mortality than those treated withVBL It is worth noting that the study was not randomised
There have been recent suggestions based on low-level evi-dence that NSBB may result in a poorer outcome in patientswith cirrhosis and refractory ascites77 The lsquowindow hypothesisrsquofor β blockers in cirrhosis has also recently been described sug-gesting that NSBB are helpful in the compensated and earlydecompensated cirrhotic period but may not be helpful in veryearly cirrhosis such as in a patient with no varices and may beharmful in patients with end-stage cirrhosis with refractoryascites78 However recent large observational studies questionthe last hypothesis with improved survival seen in patients withrefractory ascites treated with NSBB79 unless patients have anepisode of spontaneous bacterial peritonitis80 Therefore untilthere are further prospective controlled studies NSBB should becontinued in patients with refractory ascites The clinician mustcarefully monitor haemodynamic parameters such as blood pres-sure and discontinue NSBB in patients with hypotension andrenal impairment as can occur after an episode of spontaneousbacterial peritonitis Other potentially severe adverse eventswith NSBB include symptomatic bradycardia asthma andcardiac failure Less severe side effects such as fatigue insomniaand sexual dysfunction may also result
Isosorbide mononitrateInterest in the use of vasodilators such as isosorbide mononitrate(ISMN) developed after the demonstration that it reduces portalpressure as effectively as propranolol81 but has subsequentlywaned A trial comparing ISMN with propranolol showed nosignificant difference between these agents82 Another rando-mised trial of ISMN versus placebo did show any difference inthe two arms83 Therefore ISMN is not recommended asmonotherapy in primary prophylaxis
β Blocker and ISMNThe combination of nadolol and ISMN has been compared withnadolol in a RCT The combination therapy reduced the fre-quency of bleeding significantly but no significant differenceswere detected in mortality84 However Garcia-Pagan et al85 in adouble-blind RCTof propranolol plus ISMN versus propranolol
plus placebo failed to show any differences between the twoarms Combination therapy is associated with more side effects
Proton pump inhibitorsA placebo-controlled randomised trial reported reduced bleed-ing and mortality with rabeprazole after eradication of varices86
However the study had a heterogeneous population with VBLperformed for both primary and secondary prophylaxis andsmall numbers (n=43) limiting the validity of the conclusionsFurthermore there was no arm comparing proton pump inhibi-tors with NSBB The use of proton pump inhibitors in patientswith cirrhosis and ascites was associated with increased risk ofspontaneous bacterial peritonitis in a large retrospective study87
This was not confirmed in a larger prospective non-randomisedstudy88 However a recent prospective observational study hasshown proton pump use to be associated with increased mortal-ity in cirrhosis89 Proton pump inhibitors are also associatedwith increased risk of Clostridium difficile infection90 Thereremains continuing concern about proton pump inhibitors inpatients with cirrhosis therefore caution should be used
Endoscopic therapyVariceal band ligationVBL has been compared with NSBB in 19 trials in a recentCochrane meta-analysis of 1504 patients91 Despite reducedbleeding (RR=067 95 CI 046 to 098) with VBL there wasno difference in overall mortality and bleeding-related mortalityThe difference in bleeding was not seen when only trials withlow selection or attrition bias were included Banding can haveserious complications The risk of fatal banding-induced bleed-ing was highlighted in a meta-analysis showing reduced fataladverse events with NSBB (OR=014 95 002 to 099)92
The optimal timing of banding intervals is discussed in thesection lsquoSecondary prophylaxis of variceal haemorrhagersquo A ran-domised trial of 96 patients who underwent endoscopic surveil-lance at 6 or 3 months after eradication of varices with VBL didnot demonstrate a difference in bleeding on mortality93
However the trial had a heterogeneous study group of patientswho underwent VBL both for primary (65) and secondaryprevention (35)
SclerotherapyNineteen trials have compared endoscopic variceal sclerotherapywith no treatment68 Owing to the marked heterogeneitybetween these studies a meta-analysis is clinically inappropri-ate68 Sclerotherapy does not offer any benefit in combinationwith NSBB or VBL compared with VBL or NSBB alone andincreases iatrogenic complications such as strictures94ndash96 At thistime sclerotherapy cannot be recommended for prophylaxis ofvariceal haemorrhage in patients with cirrhosis
Recommendations primary prophylaxis of variceal haemor-rhage in cirrhosis (figure 2)1 What is the best method for primary prophylaxis
11 We recommend NSBB or variceal band ligation (VBL)We suggest pharmacological treatment with propranololas first line VBL is offered if there are contraindicationsto NSBB The choice of VBL or NSBB should also takeinto account patient choice (level 1a grade A)
12 We suggest carvedilol or nadolol as alternatives to pro-pranolol (level 1b grade A)
13 Dose131 Propranolol 40 mg twice daily Dose titrated to
maximum tolerated or once heart rate (HR) of
10 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
50ndash55 bpm is reached to a maximum dose of320 mg (level 1a grade A)
132 Nadolol 40 mg daily dose Dose titrated tomaximum tolerated or once HR of 50ndash55 bpm isreached a maximum dose of 240 mg (level 1agrade A)
133 Carvedilol 625 mg once daily to increase tomaintenance of 125 mg after a week if toleratedor once HR of lt50ndash55 bpm is reached (level 1agrade A)
134 It is suggested that NSBB are discontinued at thetime of spontaneous bacterial peritonitis renalimpairment and hypotension (level 2b grade B)
14 In cases of contraindications or intolerance to NSBB werecommend variceal band ligation (level 1a grade A)
2 Who should have surveillance for variceal bleeding21 We recommend all patients with cirrhosis should be
endoscoped at the time of diagnosis (level 1a grade A)There is no indication to repeat endoscopy in patientsreceiving NSBB
3 How often should cirrhotic patients be endoscoped31 If at the time of first endoscopy no varices are seen we
suggest that patients with cirrhosis should be endos-coped at 2ndash3-year intervals (level 2a grade B)
32 If grade I varices are diagnosed we suggest that patientsshould be endoscoped at yearly intervals (level 2agrade B)
33 If there is clear evidence of disease progression wesuggest that the intervals can be modified by a clinicianEndoscopy should also be offered at time of decompen-sation (level 2a grade B)
4 Which patients with cirrhosis should have primaryprophylaxis41 If grade I varices and red signs or grade 2ndash3 varices are
diagnosed we recommend that patients have primaryprophylaxis irrespective of the severity of the liverdisease (level 1a grade A)
5 Treatments not recommended51 Proton pump inhibitors are not recommended unless
otherwise required for peptic ulcer disease (level 1bgrade B)
52 Isosorbide mononitrate monotherapy is not recommendedas primary prophylaxis (level 1b grade A) There is insuffi-cient evidence to recommend isosorbide mononitrate incombination with NSBB (level 1b grade A)
53 Shunt surgery or TIPSS is not recommended as primaryprophylaxis (level 1a grade A)
54 Sclerotherapy is not recommended as primary prophy-laxis (level 1a grade A)
6 Areas requiring further study61 Role of NSBB in patients without varices with focus on
carvedilol62 Role of NSBB in patients with small varices with focus
on carvedilol63 Comparison of carvedilol versus propranolol in primary
prophylaxis64 Identification of and trials assessing new drugs for
primary prophylaxis such as statins7 Quality indicator
71 Percentage of patients at diagnosis of cirrhosis who havehad an endoscopy to screen for varices (level 1agrade A)Numerator patients diagnosed with cirrhosis who havehad an endoscopy either before or after diagnosis within
6 monthsDenominator patients newly diagnosed with cirrhosis
72 Percentage of patients receiving primary prophylaxisamong those newly diagnosed with grade I varices andred signs or grade 2ndash3 varicesNumerator patients who have grade 1 varices with redsigns or grade 2ndash3 varices receiving primary prophy-laxisDenominator patients diagnosed with cirrhosis whohave grade I varices with red signs or grade 2ndash3 varices
MANAGEMENT OF ACTIVE VARICEAL HAEMORRHAGEThe average 6-week mortality of the first episode of varicealbleeding in most studies is reported to be up to 20 There hasbeen considerable improvement in survival since the early 1980swhen the in-hospital mortality was 40ndash5097 compared with15 from a recent UK audit5 Such is the improvement in out-comes that a patient with Childrsquos A cirrhosis is very unlikely tosuccumb to an index variceal bleed Studies have shown theChildndashPugh score MELD score and HVPG to be strong predic-tors of outcomes98ndash103 The MELD score has been shown tooutperform Childrsquos score in a recent study with a score gt19associated with 20 6 week mortality103 Furthermore theMELD score has been shown to perform as well as the trad-itional intensive care unit scores in predicting mortality inpatients admitted to intensive care in the UK104 MELD gt18active bleeding transfusing gt4 units of packed red blood cellshave been shown to be predictors of mortality and earlyrebleeding99 101 102 HVPG has also been shown to predictoutcome when measured at 2 weeks after a bleed44 and a valueof ge20 mm Hg when measured acutely within 48 h has beenshown to provide significant prognostic information100
However this technique is not used routinely in the manage-ment of patients around the world and substitution of clinicaldata in the latter study was shown to provide the same clinicalpredictive value100 These scoring systems are not purely aca-demic they allow the referring clinician to predict thosepatients with a high chance of rebleeding to be transferred to aspecialist centre offering for instance TIPSS before the patientrebleeds
Nonetheless probably the most important step in the man-agement of acute variceal haemorrhage is the initial resuscitationassessed according to standard lsquoABCrsquo practice together withprotection of the airway to prevent aspiration Although earlyendoscopy allows for accurate diagnosis of the bleeding site anddecisions about management (figure 3) therapeutic interventionin acute variceal bleeding can be initiated safely in most casesbefore diagnostic endoscopy As similar efficacy is demonstratedwith pharmacological treatment as with sclerotherapy theformer should be first-line therapy99 β Blockade should not bestarted in the acute setting and those already taking β blockersas prophylaxis should probably stop taking them for 48ndash72 h inorder that the patientrsquos physiological response to blood loss canbe allowed to manifest
General considerationsPatient evaluationThe majority of patients with a variceal bleed will be sufficientlystable to enable a full history and examination to take placeHistory of alcohol excess and or intravenous drug use should besought and may become particularly relevant if the patient haswithdrawal symptoms after admission Comorbidity is importantwhen estimating risk and deciding on use of vasopressors The
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 11
Guidelines
following risk factors doubled mortality after an acute varicealbleed in one US study older age comorbidities male gender andnot undergoing a gastroscopy within 24 h105
A full examination is helpful for the important negatives asmuch as the positives Baseline observations should include thetemperature as infection is a serious complication with signifi-cant mortality Confusion may be present because of encephal-opathy intoxication with alcohol or drugs or withdrawal fromalcohol or drugs The patient should be on continuous BP andpulse monitor and their haemodynamic status recordedAn oxygen saturation monitor is helpful Stigmata of chronicliver disease and concurrent jaundice provide insight into thecurrent status of a patientrsquos liver and also give warning ofpotential further decompensation if significant bleeding persists(see scoring systems above) Pneumonia must be actively
excluded Evidence of ascites requires a diagnostic tap to searchfor infection
Investigations including full blood count coagulationprofile liver and renal function and blood group and save andcross-match Blood and urine should also be cultured An ultra-sound scan later in the admission is helpful to identify subclin-ical ascites flow in portal vein and any obvious emergence of anhepatocellular carcinoma (HCC)
Location of patientA decision must be made as to where the patient is best managedVariceal bleeding is unpredictable generally occurs in patientswith significant liver disease and is associated with significant mor-tality Hence a high-dependency unit is usually the most appropri-ate initial location although a properly staffed lsquogastrointestinal
Figure 3 Algorithm for themanagement of acute varicealbleeding TIPSS transjugularintrahepatic portosystemic stent shunt
12 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleeding bedrsquo may be appropriate If a patient is vomiting bloodor there is a perceived risk of a haemodynamically unstable patienthaving blood in the stomach then the patient must be intubatedbefore endoscopy and return to an intensive care or high-dependency unit will be necessary until extubation
Volume resuscitation and blood productsIntravenous access (two 16ndash18G cannulae) should have beensecured on admission with a reported GI bleed Further intra-venous access may be necessary In patients with poor venousaccess advanced liver disease or renal failure associated withtheir liver disease central venous access may be helpful withguiding fluid infusions However the drawbacks include the riskof the procedure and a potential source of infection Thereforethere is no absolute requirement for a central line and no evi-dence of unequivocal benefit Intravenous fluid resuscitationshould be initiated with plasma expanders aiming to maintain asystolic blood pressure of 100 mm Hg Care with monitoring isparamount in this group of patients
Overtransfusion has been shown to have a deleterious effecton outcome In a recent single-centre RCT a restrictive transfu-sion policy of maintaining haemoglobin between 70 and 80 gLimproved the control of variceal bleeding (11 vs 22p=005) and lowered HVPG compared with a liberal transfu-sion policy without effect on 45-day survival106 However itshould be noted that these results were from a single Spanishcentre which was a tertiary unit for variceal bleeding where allpatients underwent endoscopy within 6 h Nonetheless arestrictive transfusion policy has been recommended for sometime1 and there is now good evidence to support not transfusinga stable patient with a haemoglobin of ge80 gL However under-resuscitation should also be avoided and while goal-orientedfluid replacement has generally not been useful in an intensivetherapy unit setting a venous saturation gt70 remains an easilymeasurable target with some evidence to support it107
Interpretation and management of clotting profile is challen-ging in liver disease where there is usually a balanced deficiencyof both procoagulant and anticoagulant factors108 The NICEguidelines recommend activation of a hospitalrsquos massive transfu-sion policy when there is major haemorrhage and plateletsupport when the value is lt50 and clotting factor supportwhen the international normalised ratio (INR) is gt15 timesnormal2 There is no evidence for the use of lsquoprophylacticrsquo clot-ting or platelet support to reduce the risk of rebleeding Thereis insufficient evidence to support the routine use of transexamicacid or recombinant factor VIIa109
Pharmacological treatmentThe two major classes of drugs that have been used in thecontrol of acute variceal bleeding are vasopressin or its analo-gues (either alone or in combination with nitroglycerine) andsomatostatin or its analogues Terlipressin is the only agent thathas been shown to reduce mortality in placebo-controlled trialsHowever in trials comparing terlipressin somatostatin andoctreotide no difference in efficacy was identified in a system-atic review110 and in a recent large RCT111 Prophylactic anti-biotics can result in a similar survival benefit following acutevariceal bleeding
VasopressinVasopressin reduces portal blood flow portal systemic collateralblood flow and variceal pressure It does however have signifi-cant systemic side effects such as an increase in peripheral resist-ance and reduction in cardiac output heart rate and coronary
blood flow In comparison with no active treatment the pooledresults of four randomised trials showed that it reduced failureto control variceal bleeding (OR=022 95 CI 012 to 043)although survival was unaffected68 Meta-analysis of five trialscomparing sclerotherapy with vasopressin has shown a signifi-cant effect on reduction in failure to control bleeding(OR=051 95 CI 027 to 097) with no effect on survival68
Vasopressin with nitroglycerineThe addition of nitroglycerine enhances the effect of vasopres-sin on portal pressure and reduces cardiovascular side effects112
Meta-analysis of three randomised trials comparing vasopressinalone with vasopressin and nitroglycerine showed that the com-bination was associated with a significant reduction in failure tocontrol bleeding (OR=039 95 CI 022 to 072) although nosurvival benefit was shown68
TerlipressinTerlipressin is a synthetic analogue of vasopressin which has animmediate systemic vasoconstrictor action followed by portalhaemodynamic effects due to slow conversion to vasopressin Ina Cochrane meta-analysis of seven placebo-controlled trials ter-lipressin was shown to reduce failure to control bleeding(RR=066 95 CI 055 to 093) and also to improve survival(RR=066 95 CI 049 to 088)113 In the same meta-analysisthere was no difference between terlipressin versus vasopressinballoon tamponade or endoscopic therapy in failure to controlbleeding or survival113 The role of terlipressin in combinationwith VBL is explored in the section lsquoEndoscopic therapy incombination with pharmacological therapyrsquo
The recommended dose of terlipressin is 2 mg IV every 4 halthough many units reduce the dose to 6 hourly as it may causeperipheral vasoconstriction which manifests as painful handsand feet While 5 days of IV treatment has been advocated inthe Baveno V guidelines1 this prolonged treatment has notbeen shown to have a survival benefit and for pragmaticreasons many units will stop treatment shortly after satisfactoryhaemostasis In a randomised trial terlipressin given for 24 hafter satisfactory haemostasis with VBL after oesophageal vari-ceal bleeding was as effective as 72 h of treatment114
In patients intolerant of terlipressin or in countries where ter-lipressin is not available alternatives should be considered
Somatostatin and octreotideSomatostatin causes selective splanchnic vasoconstriction andreduces portal pressure and portal blood flow115 Octreotide is asomatostatin analogue The mechanism of action of these twoagents is not clear Inhibition of glucagon increases vasodilatationrather than a direct vasoconstrictive effect and post-prandial guthyperaemia is also reduced The actions of octreotide on hepaticand systemic hemodynamics are transient making continuousinfusion necessary Octreotide is given as a 50 μg bolus followedby an infusion of 25ndash50 μgh Somatostatin is given as a 250 mgintravenous bolus followed by an infusion of 250 mghSomatostatin and octreotide have been shown to be aseffective as terlipressin in acute variceal bleeding in ameta-analysis110 Seo et al111 in a large RCTof 780 patients com-paring these three agents failed to show a difference in treatmentsuccess (range 838ndash862) rebleeding (range 34ndash44) andmortality (range 8ndash88) A low systolic blood pressure at pres-entation high serum creatinine level active bleeding in the emer-gency endoscopy gastric variceal bleeding and ChildndashPugh gradeC were independent factors predicting 5-day treatmentfailure111
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 13
Guidelines
AntibioticsAntibiotics that provide Gram-negative cover are one of the inter-ventions which positively influence survival in variceal haemor-rhage as shown in a Cochrane meta-analysis of 12placebo-controlled trials (RR=079 95 CI 063 to 098)116
Antibiotics were also shown to reduce bacterial infections(RR=043 95 CI 019 to 097) and early rebleeding (RR=05395 CI 038 to 074)116 Therefore short-term antibiotics shouldbe considered standard practice in all cirrhotic patients who have avariceal bleed irrespective of the presence of confirmed infectionThird-generation cephalosporins such as ceftriaxone (1 g IVdaily) have been shown to be more effective at reducingGram-negative sepsis than oral norfloxacin117 but choice of anti-biotics must be dictated by local resistance patterns and availability
Proton pump inhibitorsOne RCT compared a short course of proton pump inhibitorswith vasoconstrictor therapies after haemostasis in acute varicealbleeding118 Despite larger ulcers noted in the vasoconstrictorarm there were no differences in bleeding or survival Nearly50 of patients had ascites which might have implications inlight of the reports of increased incidence of spontaneous bac-terial peritonitis as mentioned earlier
Endoscopic therapyEndoscopy should take place within 24 h of admission andearlier if there is excessive bleeding based on low-level evi-dence105 While many guidelines and reviews suggest thatendoscopy should be carried out within 12 h the only study thatexamined the influence of timing on outcome failed to demon-strate any advantage of endoscopy before 12 h119 The optimaltime is after sufficient resuscitation and pharmacological treat-ment with the endoscopy performed by a skilled endoscopyteam in a suitably equipped theatre environment and withairway protection Airway protection is essential where risk ofaspiration is high and affords the endoscopist time for thoroughevaluation including complete clot aspiration and controlledapplication of treatment including tamponade if required Theendoscopy team must comprise an experienced endoscopynurse acquainted with the equipment necessary for endoscopytherapy of varices and a skilled endoscopist competent in usingbanding devices and deployment of balloon tamponade
Variceal band ligationThis technique is a modification of that used for the elastic bandligation of internal haemorrhoids Its use in humans was firstdescribed in 1988120 A meta-analysis of seven trials comparingVBL with sclerotherapy in acute bleeding showed that VBLreduced rebleeding from varices (OR=047 95 CI 029 to078) reduced mortality (OR=067 95 CI 046 to 098) andresulted in fewer oesophageal strictures (OR=010 95 CI003 to 029)121 The number of sessions required to obliteratevarices was lower with VBL (22 fewer sessions (95 CI 09to 35))
SclerotherapySclerotherapy has been replaced by VBL and should no longerbe offered as standard of care in acute variceal haemorrhage
Other endoscopic measuresIn an RCT cyanoacrylate offered no benefit over VBL with theadditional risk of embolisation and trend towards increasedrebleeding with cyanoacrylate122
Haemostatic powder (TC-325 Hemospray Cook MedicalUSA) has been described in a small study of nine patients whoreceived endoscopic spray treatment for acute variceal bleedingThe study reported no rebleeding within 24 h and no mortalityat 15 days123
Endoscopic therapy in combination with pharmacological therapyThe role of combining vasoactive drugs with endoscopictherapy (VBL or sclerotherapy) was reported in a meta-analysisof eight trials124 Combination therapy resulted in better initialcontrol of bleeding (RR=112 95 CI 102 to 123) and5-day haemostasis (RR=128 95 CI 118 to 139) withoutany difference in survival Adverse events were similar in bothgroups Two RCTs have compared VBL with sclerotherapy incombination with vasoactive agents in acute variceal bleed-ing125 126 Lo et al125 used vasopressin and found that VBLresulted in better 72 h haemostasis (97 vs 76 p=0009)with fewer complications (5 vs 29 p=0007) Villanuevaet al used somatostatin and reported lower failure to controlacute bleeding with VBL (4 vs 15 p=002) with fewerserious complications (4 vs 13 p=004) Overall survivalwas similar in both trials125 126
Balloon tamponadeBalloon tamponade is highly effective and controls acute bleed-ing in up to 90 of patients although about 50 rebleed whenthe balloon is deflated127 128 It is however associated withserious complications such as oesophageal ulceration and aspir-ation pneumonia in up to 15ndash20 of patients Despite this itmay be a life-saving treatment in cases of massive uncontrolledvariceal haemorrhage pending other forms of treatment Anappropriately placed SengstakenndashBlakemore tube allows forresuscitation safe transportation and either repeat endoscopy orradiological shunting in a patient with a stable cardiovascularsystem The oesophageal balloon is rarely required must neverbe used on its own and should be used only if there is continu-ing bleeding despite an adequately inflated gastric balloon cor-rectly placed and with appropriate tension Placement of thetube endoscopically or over a guide wire might reduce the riskof complications especially oesophageal rupture
Removable oesophageal stentsThe SX-Ella Danis stent (ELLA-CS Hradec Kralove CzechRepublic) is a removable covered metal mesh stent placed endo-scopically in the lower oesophagus without radiological screen-ing It has no role in the management of gastric varicealbleeding These stents can be left in situ for up to 2 weeksunlike the SengstakenndashBlakemore tube which should beremoved after a maximum of 24ndash48 h129 130 No published con-trolled trials have compared this modality with balloontamponade
Transjugular intrahepatic portosystemic stent-shuntSeveral uncontrolled studies have examined the role of salvagebare TIPSS in acute variceal bleeding In a review of 15 studiescontrol of bleeding was achieved in 90ndash100 with rebleedingin 6ndash16131 Mortality varied between 75 (in hospital) and15 (30 day) It is important to appreciate that sclerotherapywas used as first-line endoscopic therapy in most of thesestudies Long-term follow-up of a study that compared TIPSSwith H-graft portacaval shunts in patients for whom non-operative management had failed suggested that H-grafts were auseful method of reducing portal pressure and had a signifi-cantly lower failure rate (p=004) but had no significant
14 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
improvement in overall survival despite a benefit seen in ChildrsquosA and B disease132 A recent RCT compared emergency porto-caval surgery with bare TIPSS within 24 h of presenting withacute oesophageal variceal bleeding in unselected cirrhoticpatients Emergency portocaval surgery resulted in better out-comes for long-term bleeding control encephalopathy and sur-vival (plt0001)133 Before wider application of surgery foracute variceal bleeding more data are needed in light of therecent adoption of covered stents
There has also been a generalised established change in prac-tice in using covered TIPSS stents (polytetrafluoroethylene(PTFE)) rather than a bare metal stent with evidence to supportthis change In randomised controlled studies these stents wereshown to have higher primary patency rates than bare stentswithout significant differences in survival and the potential forreduced incidence of hepatic encephalopathy134 135
There is however growing evidence from two RCTs for theearlier use of TIPSS in selected patients stratified by HVPGChildndashPugh class and active bleeding and not just use as asalvage option6 136 Monescillo et al136 randomised patientspresenting with acute oesophageal variceal haemorrhage to bareTIPSS or standard of care if the HVPG was ge20 mm Hg within24 h of admission Significantly reduced treatment failure asdefined by failure to control acute bleeding andor early rebleed-ing (12 vs 50) was seen and improved survival (62 vs35) in the patients randomised to undergo a TIPSS procedureHowever the standard of care was sclerotherapy and not com-bination endoscopic and pharmacological treatment This limita-tion and the lack of availability of HVPG measurement in mostcentres meant this trial did not have a significant impact on clin-ical practice
Garcia-Pagan et al6 selected patients with active bleeding andChildrsquos B cirrhosis or patients with Childrsquos C cirrhosis (Childrsquosscore lt14) for randomisation to early PTFE-covered TIPSSwithin 72 h or standard of care with VBL and pharmacologicaltreatment This has shown encouraging results with reduced riskof treatment failure (3 vs 50) improved survival (86 vs61 at 1 year) yet without increased risk of hepatic encephal-opathy The results were supported by an observational studyfrom the same group although a survival benefit was notseen137 Furthermore a recent well-conducted observationalstudy did not demonstrate such high survival rates with earlyTIPSS with 11-year survival of 67 which was similar to thatof patients given endoscopic and pharmacological treatmentsonly138 Therefore larger multicentred RCTs need to be under-taken to further evaluate the role of early TIPSS It is importantto make the distinction between salvage TIPSS and early TIPSSto prevent rebleeding
Liver transplantationThis is probably appropriate only for patients who bleed whileawaiting liver transplantation although studies comparing VBLor TIPSS placement with urgent liver transplantation in thissituation need to be done Liver transplantation is an exceed-ingly rare option for the vast majority of patients both becauseit is not commonly available and because of shortages anddelays in organ procurement No controlled trials of liver trans-plantation in uncontrolledactive bleeding are available
Recommendations for the control of variceal bleeding in cir-rhosis are given below and in figure 3
Recommendations control of active variceal haemorrhage incirrhosis (figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with bloodplatelets and clotting factors in line with local protocolsfor managing massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusionpolicy aiming for a haemoglobin of 70ndash80 gL is sug-gested in haemodynamically stable patients (level 1bgrade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable(level 5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L(level 5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to localcircumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with suspected
or confirmed variceal bleeding (level 1a grade A)32 In all patients vasoconstrictors such as terlipressin or
somatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 15
Guidelines
41 If bleeding is difficult to control a SengstakenndashBlakemore tube should be inserted until further endo-scopic treatment TIPSS or surgery is performed depend-ing on local resources and expertise (level 1b grade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure (level1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
SECONDARY PROPHYLAXIS OF VARICEAL HAEMORRHAGEβ BlockersA meta-analysis of 12 trials comparing propranolol or nadolol139
with no active treatment showed a significant reduction inrebleeding but no significant reduction in mortality140 Thegreater reduction in portal pressure with carvedilol comparedwith propranolol has been described in the section lsquoPrimaryprophylaxisrsquo of this guideline
NitratesThe addition of ISMN to NSBB has been shown to reduce vari-ceal rebleeding compared with NSBB alone although no sur-vival benefit was seen141 In addition adverse events leading todrug withdrawal were more common in the group receivingcombined drug treatment A meta-analysis of ISMN alone orwith either NSBB or endoscopic therapy reported that there wasno mortality benefit from combining nitrates and NSBB com-pared with NSBB alone142
Side effects of ISMN include dizziness and headache Owingto the side effects and relative lack of data ISMN is not com-monly used in clinical practice
A recent RCT of 121 patients reported carvedilol to besimilar to combined ISMN and NSBB therapy in the preventionof variceal rebleeding and mortality although severe adverseevents were less common with carvedilol143
SimvastatinA recent abstract of a multicentre RCT of 158 patients reporteda survival benefit (91 vs 78 p=003) from adding simvasta-tin to VBL and NSBB compared with placebo VBL and NSBBas treatment for the prevention of variceal rebleeding144 Therewas no difference in rebleeding and the survival benefit wasrestricted to Child A and B patients Serious adverse events weresimilar in both groups More data are required to investigatethis interesting observation of a survival benefit from simvastatinin this situation which may relate to its effects on hepatocellularfunction fibrosis and portal pressure
Proton pump inhibitorsA double-blind randomised placebo-controlled trial showed thatpantoprazole reduced the size of ulcers in patients who under-went VBL However the total number of ulcers and other out-comes were similar in the two groups145
Endoscopic therapyVBL has been accepted as the preferred endoscopic treatmentfor the prevention of variceal rebleeding with a lower rate ofrebleeding mortality and complications than sclerother-apy146 147 The time interval between VBL sessions to achieveeradication of varices is debateable However a recent RCTcomparing monthly with biweekly VBL after initial haemostasiswith VBL in 70 patients suggested that there were fewerpost-VBL ulcers in the monthly group (11 vs 57plt0001)148 Variceal recurrence rebleeding and mortality weresimilar in both groups
Two meta-analyses showed there is no evidence that the add-ition of sclerotherapy to VBL improves clinically relevant out-comes including variceal rebleeding and death and thecombination led to higher stricture rates149 150
Endoscopic therapy versus drug therapyVBL has been reported to be more effective than combinedNSBB and ISMN drug therapy151 However an 8-yearfollow-up study of this RCT found that although VBL wassuperior in reducing variceal rebleeding survival rates were sig-nificantly higher in the group treated with combined drug treat-ment152 Other studies have found no superiority of VBL overcombined drug therapy for prevention of variceal rebleeding ormortality153 154 A recent small multicentre RCT reported carve-dilol to be similar to VBL in the prevention of variceal rebleed-ing with a trend in favour of survival with carvedilol (73 vs48 p=0110)155
Several meta-analyses have compared drug therapy with VBLin the prevention of variceal rebleeding One meta-analysis ofsix RCTs showed no significant difference in variceal rebleedingrates when comparing VBL alone with combined NSBB andISMN therapy However all-cause mortality was significantlyhigher in patients treated with the VBL (RR=125 95 CI101 to 155)156 Three meta-analyses comparing drug therapy(NSBB alone or with ISMN) with endoscopic therapy alonereported no difference in variceal rebleeding or mortality157ndash159
Endoscopic+drug therapy versus either aloneNumerous studies and several meta-analyses have comparedcombined endoscopic and drug therapy with monotherapy(endoscopic or drugs alone) in the prevention of varicealrebleeding A meta-analysis of 23 trials assessing sclerotherapyor VBL combined with NSBB reported that combinationtherapy reduced rebleeding more than either endoscopic
16 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

threshold for variceal bleeding39 40 However the HVPG tendsto be higher in bleeders as well as in patients with larger varicesIn a prospective study comparing propranolol with placebo forthe prevention of first variceal haemorrhage Groszmann et al41
showed that bleeding from varices did not occur if the portalpressure gradient (PPG) could be reduced to lt12 mm HgOthers have shown that a 20 reduction in portal pressure pro-tects against further bleeding42 These haemodynamic goalshave been accepted as the aim of pharmacological treatment ofportal hypertension It is important to appreciate that gastricvarices can bleed at pressures lt12 mm Hg and the influence ofwall tension of the varix plays a greater role in the risk of bleed-ing43 A greater pressure reduction may be necessary to protectagainst bleeding This is further discussed in the section lsquoGastricvaricesrsquo At present measurement of portal pressure in guidingpharmacological treatments is limited to clinical trials in the UK
Variceal sizeVariceal size is best assessed endoscopically (figure 1AndashC)Published results are variable owing to the lack of a definition dis-tinguishing between large and small varices Small (grade I)varices tend to be narrow and flatten easily with air whereaslarger (grade 2 and 3) varices are usually broader and flatten withdifficulty if at all Numerous studies40 44 have shown that therisk of variceal haemorrhage increases with the size of varices45
Variceal wall and tensionPolio and Groszmann46 using an in vitro model showed thatrupture of varices was related to the tension on the varicealwall The tension depends on the radius of the varix In thismodel increasing the size of the varix and decreasing the thick-ness of the variceal wall caused variceal rupture Recently endo-scopic ultrasound and manometry have been used to estimatewall tension of varices47
Endoscopic features such as lsquored spotsrsquo and lsquowhalersquo markingswere first described by Dagradi24 They have been described asbeing important in the prediction of variceal haemorrhageThese features represent changes in variceal wall structure andtension associated with the development of microtelangiectasiasand reduced wall thickness In a retrospective study by theJapanese Research Society for Portal Hypertension Beppuet al48 showed that 80 of patients who had blue varices orcherry red spots bled from varices suggesting that this was animportant predictor of variceal haemorrhage in cirrhosis
Severity of liver disease and bleeding indicesTwo independent groups prospectively assessed factors predict-ing first variceal haemorrhage in cirrhosis (table 2) The NorthItalian Endoscopic Club (NIEC)49 reported their findings in1988 followed in 1990 by data from the Japanese50 Both thesestudies showed that the risk of bleeding was based on threefactors severity of liver disease as measured by Child class vari-ceal size and red wale markings The NIEC study showed awide range for the risk of bleeding of 6ndash76 depending on thepresence or absence of the different factors Using the same vari-ables the NIEC index was simplified by de Franchis et al51 andshown to correlate with the original index Further studiesshowed that the HVPG and intravariceal pressure were alsoindependent predictors of first variceal haemorrhage when ana-lysed in conjunction with the NIEC index52 53
In summary the most important factors that determine the risk ofvariceal haemorrhage are the severity of liver disease size of varicesand presence of red signs Measurement of HVPG is a useful guidefor selection of patients for treatment and their response to
treatment although the predictive value does not appear toimprove on the NIEC index and presence of red whale marking54
Risk and mortality of first variceal bleedData describing the overall risk of bleeding from varices must beviewed with caution and have some pitfalls in interpretationThe natural history of patients who have varices that are diag-nosed as part of their baseline investiations is different fromthat of patients who have complications of liver disease such asascites and encephalopathy Most studies do not comment oneither the severity of liver disease or whether patients with alco-holic cirrhosis are continuing to drink Both these factors have asignificant effect on the risk of variceal haemorrhage
Most studies report bleeding from varices in about 20ndash50of patients with cirrhosis during the period of follow-up Bakeret al23 reported variceal bleeding in 33 of 115 patients that theyfollowed up for a mean of 33 years with a mortality of 48from the first variceal haemorrhage These data were confirmedby Christensen et al18 About 70 of the episodes of bleedingoccur within 2 years of diagnosis Recent studies demonstrate adramatic reduction in mortality following variceal bleeding of20 6-week mortality55 and 15 in-hospital mortality5 withcontributions from improved endoscopic pharmacological andradiological therapies notably TIPSS Intensive care treatmenthas also improved with outcomes being particularly good forthose requiring minimal organ support
Analysis of the non-active treatment arms in the primaryprophylaxis trials comparing propranolol with placebo showresults similar to those of the primary prophylaxis shunt trialswith most episodes of bleeding occurring within the first 2 yearsof follow-up In these studies the rate of first variceal haemor-rhage ranged from 22 to 6156ndash60 This large difference inthe rate of first bleed relates almost certainly to the number ofpatients with severe liver disease included in the study (PascalChild Cmdash46 bleedingmdash61 Italian Multicenter Project forPropranolol in Prevention of Bleeding (IMPP) Child Cmdash6bleedingmdash32 Conn Child Cmdash6 bleedingmdash22)Mortality varied from 24 to 49 over 2 years (Pascal mortal-itymdash49 IMPP mortalitymdash24 Conn mortalitymdash24)
Primary prophylaxisSince 30ndash50 of patients with portal hypertension will bleedfrom varices and about 20 will die from the effects of the first
Table 2 Scoring systems for quantifying the severity of cirrhosisSeverity of liver disease can be described using the ChildndashPughscore or MELD scoreThe ChildndashPugh score is the sum of severity scores for Child classvariceal size and red wale markings the variables shown below
Category 1 2 3
Encephalopathy 0 III IIIIVAscites Absent Mild-moderate SevereBilirubin (μmolL) lt34 34ndash51 gt51Albumin (gL) gt35 28ndash35 lt28INR lt13 13ndash15 gt15
ChildndashPugh class A represents a score of le6 class B a score of 7ndash9 and class C ge10The MELD score is a formula that includes three laboratory-based variables reflectingthe severity of liver disease It was originally used to predict the short-term mortalityafter placement of a transjugular intrahepatic portosystemic stent-shunt for varicealbleeding Subsequently it has been used in selecting candidates for livertransplantationMELD score please use the online calculator httpswwwesotorgElitameldCalculatoraspxINR international normalised ratio
8 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleed it seems rational to develop prophylactic regimens toprevent the development of and bleeding from these varicesHowever most of the published trials do not have sufficientpower to identify favourable treatment effects Based on theexpected bleeding and death rates in the control group theminimum number of patients needed to detect a 50 reductionin bleeding would be 270 and 850 patients in each arm todetect the same reduction in mortality A proposed algorithmfor surveillance and prophylaxis of varices is shown in figure 2At this time there is insufficient evidence to support treatingpatients without varices or lsquopre-primary prophylaxisrsquo A largerandomised placebo-controlled trial of timolol in patientswithout varices and portal hypertension defined as HVPGgt6 mm Hg did not show any effect on the development ofvarices or variceal bleeding27 The role of drug treatment in pre-venting bleeding in patients with small varices is unclear Threerandomised placebo-controlled trials have studied this Caleset al61 showed that propranolol in patients with small or novarices resulted in greater development of varices Howeverpatients without varices were included and there was significantloss of patients to follow-up The second trial showed thatnadolol reduced variceal bleeding without survival benefit andincreased adverse events62 Sarin et al63 did not show any effectwith propranolol despite a significant effect on portal pressure
SurgeryPortacaval shuntsFour trials of portacaval shunts have been published which ran-domised a total of 302 patients64ndash67 either to prophylactic shuntsurgery or to non-active treatment A meta-analysis of thesestudies showed a significant benefit in the reduction of varicealbleeding (OR=031 95 CI 017 to 056) but also a signifi-cantly greater risk of hepatic encephalopathy (OR=2 95 CI12 to 31) and mortality (OR=16 95 CI 102 to 257) inpatients treated with shunt surgery68 At this time there is noevidence for the use of TIPSS for primary prophylaxis1
Devascularisation proceduresInokuchi50 showed that there was a significant reduction in vari-ceal bleeding and in mortality in patients treated with a varietyof devascularisation procedures There are however numerousproblems with the interpretation of this study because of theuse of different procedures in each of the 22 centres Theseresults require confirmation
Pharmacological treatmentNon-cardioselective β blockersThe mainstay of the pharmacological approach to the primaryprophylaxis of variceal haemorrhage has been NSBBPropranolol which has been shown to reduce the PPG reduceazygos blood flow and also variceal pressure It achieves this bycausing splanchnic vasoconstriction and reducing cardiacoutput There is no clear dose-related reduction in HVPG orcorrelation of HPVG reduction with reduction in heart rate69
Observational studies have shown that a 10ndash12 reduction inHVPG after acute administration of propranolol was associatedwith reduced bleeding and hepatic decompensation54 70
However HVPG monitoring is not routinely available in mostcentres outside of larger institutions A meta-analysis of nineplacebo-controlled randomised trials (964 patients) showed thatthe pooled risk difference for bleeding was minus11 (95 CIminus21 to minus1) and for death was minus9 (95 CI minus18 tominus1) in favour of propranolol71
Nadolol exerts similar effects on portal haemodynamicsalthough the effect on blood pressure may not be as pro-nounced Two placebo-controlled trials58 59 have shownreduced bleeding although in one study this was only seen onper protocol analysis59 There was no effect on overall survival
Carvedilol is a NSBB like propranolol and a vasodilator dueto α1 receptor blockade The latter reduces portocollateralresistance and by actions on hepatic stellate cells leads to areduction in intrahepatic resistance Haemodynamic studiesdemonstrate a greater reduction in portal pressure with
Figure 2 Algorithm for surveillance of varices and primary prophylaxis in cirrhosisndash If there is clear evidence of disease progression this interval can be modified by clinician Endoscopy should also be offered at time ofdecompensation
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 9
Guidelines
carvedilol than with propranolol although blood pressure isreduced72 73 The optimum dose is 625ndash125 mgday74 Higherdoses are not more effective and are associated with moreadverse eventsmdashin particular hypotension Carvedilol at a doseof 125 mgday at current UK prices is considerably cheaperthan propranolol 40 mg twice a day and nadolol 80 mgday(monthly cost pound120 pound562 and pound5 respectively) Two RCTs ofcarvedilol versus variceal band ligation (VBL) in primaryprophylaxis have been published75 76 The first study75 showedsignificantly reduced bleeding in the carvedilol arm (10 vs23 relative hazard 041 95 CI 019 to 096) with no effecton survival The second trial by Shah et al76 did not show anydifferences in bleeding or mortality Compliance with VBL wasbetter in the latter trial and unlike the first trial there were sig-nificantly more patients with viral hepatitis than alcoholic cir-rhosis A further study74 assessed the effect of carvedilol inpatients who were haemodynamic non-responders to propran-olol where haemodynamic response was defined as HVPGreduction to le12 mm Hg or by gt20 of baseline after 4 weeksof treatment Patients who were haemodynamic non-respondersor intolerant to carvedilol were treated with VBL Carvedilolresulted in significantly lower variceal bleeding compared withVBL and haemodynamic responders to carvedilol or propran-olol had significantly lower mortality than those treated withVBL It is worth noting that the study was not randomised
There have been recent suggestions based on low-level evi-dence that NSBB may result in a poorer outcome in patientswith cirrhosis and refractory ascites77 The lsquowindow hypothesisrsquofor β blockers in cirrhosis has also recently been described sug-gesting that NSBB are helpful in the compensated and earlydecompensated cirrhotic period but may not be helpful in veryearly cirrhosis such as in a patient with no varices and may beharmful in patients with end-stage cirrhosis with refractoryascites78 However recent large observational studies questionthe last hypothesis with improved survival seen in patients withrefractory ascites treated with NSBB79 unless patients have anepisode of spontaneous bacterial peritonitis80 Therefore untilthere are further prospective controlled studies NSBB should becontinued in patients with refractory ascites The clinician mustcarefully monitor haemodynamic parameters such as blood pres-sure and discontinue NSBB in patients with hypotension andrenal impairment as can occur after an episode of spontaneousbacterial peritonitis Other potentially severe adverse eventswith NSBB include symptomatic bradycardia asthma andcardiac failure Less severe side effects such as fatigue insomniaand sexual dysfunction may also result
Isosorbide mononitrateInterest in the use of vasodilators such as isosorbide mononitrate(ISMN) developed after the demonstration that it reduces portalpressure as effectively as propranolol81 but has subsequentlywaned A trial comparing ISMN with propranolol showed nosignificant difference between these agents82 Another rando-mised trial of ISMN versus placebo did show any difference inthe two arms83 Therefore ISMN is not recommended asmonotherapy in primary prophylaxis
β Blocker and ISMNThe combination of nadolol and ISMN has been compared withnadolol in a RCT The combination therapy reduced the fre-quency of bleeding significantly but no significant differenceswere detected in mortality84 However Garcia-Pagan et al85 in adouble-blind RCTof propranolol plus ISMN versus propranolol
plus placebo failed to show any differences between the twoarms Combination therapy is associated with more side effects
Proton pump inhibitorsA placebo-controlled randomised trial reported reduced bleed-ing and mortality with rabeprazole after eradication of varices86
However the study had a heterogeneous population with VBLperformed for both primary and secondary prophylaxis andsmall numbers (n=43) limiting the validity of the conclusionsFurthermore there was no arm comparing proton pump inhibi-tors with NSBB The use of proton pump inhibitors in patientswith cirrhosis and ascites was associated with increased risk ofspontaneous bacterial peritonitis in a large retrospective study87
This was not confirmed in a larger prospective non-randomisedstudy88 However a recent prospective observational study hasshown proton pump use to be associated with increased mortal-ity in cirrhosis89 Proton pump inhibitors are also associatedwith increased risk of Clostridium difficile infection90 Thereremains continuing concern about proton pump inhibitors inpatients with cirrhosis therefore caution should be used
Endoscopic therapyVariceal band ligationVBL has been compared with NSBB in 19 trials in a recentCochrane meta-analysis of 1504 patients91 Despite reducedbleeding (RR=067 95 CI 046 to 098) with VBL there wasno difference in overall mortality and bleeding-related mortalityThe difference in bleeding was not seen when only trials withlow selection or attrition bias were included Banding can haveserious complications The risk of fatal banding-induced bleed-ing was highlighted in a meta-analysis showing reduced fataladverse events with NSBB (OR=014 95 002 to 099)92
The optimal timing of banding intervals is discussed in thesection lsquoSecondary prophylaxis of variceal haemorrhagersquo A ran-domised trial of 96 patients who underwent endoscopic surveil-lance at 6 or 3 months after eradication of varices with VBL didnot demonstrate a difference in bleeding on mortality93
However the trial had a heterogeneous study group of patientswho underwent VBL both for primary (65) and secondaryprevention (35)
SclerotherapyNineteen trials have compared endoscopic variceal sclerotherapywith no treatment68 Owing to the marked heterogeneitybetween these studies a meta-analysis is clinically inappropri-ate68 Sclerotherapy does not offer any benefit in combinationwith NSBB or VBL compared with VBL or NSBB alone andincreases iatrogenic complications such as strictures94ndash96 At thistime sclerotherapy cannot be recommended for prophylaxis ofvariceal haemorrhage in patients with cirrhosis
Recommendations primary prophylaxis of variceal haemor-rhage in cirrhosis (figure 2)1 What is the best method for primary prophylaxis
11 We recommend NSBB or variceal band ligation (VBL)We suggest pharmacological treatment with propranololas first line VBL is offered if there are contraindicationsto NSBB The choice of VBL or NSBB should also takeinto account patient choice (level 1a grade A)
12 We suggest carvedilol or nadolol as alternatives to pro-pranolol (level 1b grade A)
13 Dose131 Propranolol 40 mg twice daily Dose titrated to
maximum tolerated or once heart rate (HR) of
10 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
50ndash55 bpm is reached to a maximum dose of320 mg (level 1a grade A)
132 Nadolol 40 mg daily dose Dose titrated tomaximum tolerated or once HR of 50ndash55 bpm isreached a maximum dose of 240 mg (level 1agrade A)
133 Carvedilol 625 mg once daily to increase tomaintenance of 125 mg after a week if toleratedor once HR of lt50ndash55 bpm is reached (level 1agrade A)
134 It is suggested that NSBB are discontinued at thetime of spontaneous bacterial peritonitis renalimpairment and hypotension (level 2b grade B)
14 In cases of contraindications or intolerance to NSBB werecommend variceal band ligation (level 1a grade A)
2 Who should have surveillance for variceal bleeding21 We recommend all patients with cirrhosis should be
endoscoped at the time of diagnosis (level 1a grade A)There is no indication to repeat endoscopy in patientsreceiving NSBB
3 How often should cirrhotic patients be endoscoped31 If at the time of first endoscopy no varices are seen we
suggest that patients with cirrhosis should be endos-coped at 2ndash3-year intervals (level 2a grade B)
32 If grade I varices are diagnosed we suggest that patientsshould be endoscoped at yearly intervals (level 2agrade B)
33 If there is clear evidence of disease progression wesuggest that the intervals can be modified by a clinicianEndoscopy should also be offered at time of decompen-sation (level 2a grade B)
4 Which patients with cirrhosis should have primaryprophylaxis41 If grade I varices and red signs or grade 2ndash3 varices are
diagnosed we recommend that patients have primaryprophylaxis irrespective of the severity of the liverdisease (level 1a grade A)
5 Treatments not recommended51 Proton pump inhibitors are not recommended unless
otherwise required for peptic ulcer disease (level 1bgrade B)
52 Isosorbide mononitrate monotherapy is not recommendedas primary prophylaxis (level 1b grade A) There is insuffi-cient evidence to recommend isosorbide mononitrate incombination with NSBB (level 1b grade A)
53 Shunt surgery or TIPSS is not recommended as primaryprophylaxis (level 1a grade A)
54 Sclerotherapy is not recommended as primary prophy-laxis (level 1a grade A)
6 Areas requiring further study61 Role of NSBB in patients without varices with focus on
carvedilol62 Role of NSBB in patients with small varices with focus
on carvedilol63 Comparison of carvedilol versus propranolol in primary
prophylaxis64 Identification of and trials assessing new drugs for
primary prophylaxis such as statins7 Quality indicator
71 Percentage of patients at diagnosis of cirrhosis who havehad an endoscopy to screen for varices (level 1agrade A)Numerator patients diagnosed with cirrhosis who havehad an endoscopy either before or after diagnosis within
6 monthsDenominator patients newly diagnosed with cirrhosis
72 Percentage of patients receiving primary prophylaxisamong those newly diagnosed with grade I varices andred signs or grade 2ndash3 varicesNumerator patients who have grade 1 varices with redsigns or grade 2ndash3 varices receiving primary prophy-laxisDenominator patients diagnosed with cirrhosis whohave grade I varices with red signs or grade 2ndash3 varices
MANAGEMENT OF ACTIVE VARICEAL HAEMORRHAGEThe average 6-week mortality of the first episode of varicealbleeding in most studies is reported to be up to 20 There hasbeen considerable improvement in survival since the early 1980swhen the in-hospital mortality was 40ndash5097 compared with15 from a recent UK audit5 Such is the improvement in out-comes that a patient with Childrsquos A cirrhosis is very unlikely tosuccumb to an index variceal bleed Studies have shown theChildndashPugh score MELD score and HVPG to be strong predic-tors of outcomes98ndash103 The MELD score has been shown tooutperform Childrsquos score in a recent study with a score gt19associated with 20 6 week mortality103 Furthermore theMELD score has been shown to perform as well as the trad-itional intensive care unit scores in predicting mortality inpatients admitted to intensive care in the UK104 MELD gt18active bleeding transfusing gt4 units of packed red blood cellshave been shown to be predictors of mortality and earlyrebleeding99 101 102 HVPG has also been shown to predictoutcome when measured at 2 weeks after a bleed44 and a valueof ge20 mm Hg when measured acutely within 48 h has beenshown to provide significant prognostic information100
However this technique is not used routinely in the manage-ment of patients around the world and substitution of clinicaldata in the latter study was shown to provide the same clinicalpredictive value100 These scoring systems are not purely aca-demic they allow the referring clinician to predict thosepatients with a high chance of rebleeding to be transferred to aspecialist centre offering for instance TIPSS before the patientrebleeds
Nonetheless probably the most important step in the man-agement of acute variceal haemorrhage is the initial resuscitationassessed according to standard lsquoABCrsquo practice together withprotection of the airway to prevent aspiration Although earlyendoscopy allows for accurate diagnosis of the bleeding site anddecisions about management (figure 3) therapeutic interventionin acute variceal bleeding can be initiated safely in most casesbefore diagnostic endoscopy As similar efficacy is demonstratedwith pharmacological treatment as with sclerotherapy theformer should be first-line therapy99 β Blockade should not bestarted in the acute setting and those already taking β blockersas prophylaxis should probably stop taking them for 48ndash72 h inorder that the patientrsquos physiological response to blood loss canbe allowed to manifest
General considerationsPatient evaluationThe majority of patients with a variceal bleed will be sufficientlystable to enable a full history and examination to take placeHistory of alcohol excess and or intravenous drug use should besought and may become particularly relevant if the patient haswithdrawal symptoms after admission Comorbidity is importantwhen estimating risk and deciding on use of vasopressors The
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 11
Guidelines
following risk factors doubled mortality after an acute varicealbleed in one US study older age comorbidities male gender andnot undergoing a gastroscopy within 24 h105
A full examination is helpful for the important negatives asmuch as the positives Baseline observations should include thetemperature as infection is a serious complication with signifi-cant mortality Confusion may be present because of encephal-opathy intoxication with alcohol or drugs or withdrawal fromalcohol or drugs The patient should be on continuous BP andpulse monitor and their haemodynamic status recordedAn oxygen saturation monitor is helpful Stigmata of chronicliver disease and concurrent jaundice provide insight into thecurrent status of a patientrsquos liver and also give warning ofpotential further decompensation if significant bleeding persists(see scoring systems above) Pneumonia must be actively
excluded Evidence of ascites requires a diagnostic tap to searchfor infection
Investigations including full blood count coagulationprofile liver and renal function and blood group and save andcross-match Blood and urine should also be cultured An ultra-sound scan later in the admission is helpful to identify subclin-ical ascites flow in portal vein and any obvious emergence of anhepatocellular carcinoma (HCC)
Location of patientA decision must be made as to where the patient is best managedVariceal bleeding is unpredictable generally occurs in patientswith significant liver disease and is associated with significant mor-tality Hence a high-dependency unit is usually the most appropri-ate initial location although a properly staffed lsquogastrointestinal
Figure 3 Algorithm for themanagement of acute varicealbleeding TIPSS transjugularintrahepatic portosystemic stent shunt
12 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleeding bedrsquo may be appropriate If a patient is vomiting bloodor there is a perceived risk of a haemodynamically unstable patienthaving blood in the stomach then the patient must be intubatedbefore endoscopy and return to an intensive care or high-dependency unit will be necessary until extubation
Volume resuscitation and blood productsIntravenous access (two 16ndash18G cannulae) should have beensecured on admission with a reported GI bleed Further intra-venous access may be necessary In patients with poor venousaccess advanced liver disease or renal failure associated withtheir liver disease central venous access may be helpful withguiding fluid infusions However the drawbacks include the riskof the procedure and a potential source of infection Thereforethere is no absolute requirement for a central line and no evi-dence of unequivocal benefit Intravenous fluid resuscitationshould be initiated with plasma expanders aiming to maintain asystolic blood pressure of 100 mm Hg Care with monitoring isparamount in this group of patients
Overtransfusion has been shown to have a deleterious effecton outcome In a recent single-centre RCT a restrictive transfu-sion policy of maintaining haemoglobin between 70 and 80 gLimproved the control of variceal bleeding (11 vs 22p=005) and lowered HVPG compared with a liberal transfu-sion policy without effect on 45-day survival106 However itshould be noted that these results were from a single Spanishcentre which was a tertiary unit for variceal bleeding where allpatients underwent endoscopy within 6 h Nonetheless arestrictive transfusion policy has been recommended for sometime1 and there is now good evidence to support not transfusinga stable patient with a haemoglobin of ge80 gL However under-resuscitation should also be avoided and while goal-orientedfluid replacement has generally not been useful in an intensivetherapy unit setting a venous saturation gt70 remains an easilymeasurable target with some evidence to support it107
Interpretation and management of clotting profile is challen-ging in liver disease where there is usually a balanced deficiencyof both procoagulant and anticoagulant factors108 The NICEguidelines recommend activation of a hospitalrsquos massive transfu-sion policy when there is major haemorrhage and plateletsupport when the value is lt50 and clotting factor supportwhen the international normalised ratio (INR) is gt15 timesnormal2 There is no evidence for the use of lsquoprophylacticrsquo clot-ting or platelet support to reduce the risk of rebleeding Thereis insufficient evidence to support the routine use of transexamicacid or recombinant factor VIIa109
Pharmacological treatmentThe two major classes of drugs that have been used in thecontrol of acute variceal bleeding are vasopressin or its analo-gues (either alone or in combination with nitroglycerine) andsomatostatin or its analogues Terlipressin is the only agent thathas been shown to reduce mortality in placebo-controlled trialsHowever in trials comparing terlipressin somatostatin andoctreotide no difference in efficacy was identified in a system-atic review110 and in a recent large RCT111 Prophylactic anti-biotics can result in a similar survival benefit following acutevariceal bleeding
VasopressinVasopressin reduces portal blood flow portal systemic collateralblood flow and variceal pressure It does however have signifi-cant systemic side effects such as an increase in peripheral resist-ance and reduction in cardiac output heart rate and coronary
blood flow In comparison with no active treatment the pooledresults of four randomised trials showed that it reduced failureto control variceal bleeding (OR=022 95 CI 012 to 043)although survival was unaffected68 Meta-analysis of five trialscomparing sclerotherapy with vasopressin has shown a signifi-cant effect on reduction in failure to control bleeding(OR=051 95 CI 027 to 097) with no effect on survival68
Vasopressin with nitroglycerineThe addition of nitroglycerine enhances the effect of vasopres-sin on portal pressure and reduces cardiovascular side effects112
Meta-analysis of three randomised trials comparing vasopressinalone with vasopressin and nitroglycerine showed that the com-bination was associated with a significant reduction in failure tocontrol bleeding (OR=039 95 CI 022 to 072) although nosurvival benefit was shown68
TerlipressinTerlipressin is a synthetic analogue of vasopressin which has animmediate systemic vasoconstrictor action followed by portalhaemodynamic effects due to slow conversion to vasopressin Ina Cochrane meta-analysis of seven placebo-controlled trials ter-lipressin was shown to reduce failure to control bleeding(RR=066 95 CI 055 to 093) and also to improve survival(RR=066 95 CI 049 to 088)113 In the same meta-analysisthere was no difference between terlipressin versus vasopressinballoon tamponade or endoscopic therapy in failure to controlbleeding or survival113 The role of terlipressin in combinationwith VBL is explored in the section lsquoEndoscopic therapy incombination with pharmacological therapyrsquo
The recommended dose of terlipressin is 2 mg IV every 4 halthough many units reduce the dose to 6 hourly as it may causeperipheral vasoconstriction which manifests as painful handsand feet While 5 days of IV treatment has been advocated inthe Baveno V guidelines1 this prolonged treatment has notbeen shown to have a survival benefit and for pragmaticreasons many units will stop treatment shortly after satisfactoryhaemostasis In a randomised trial terlipressin given for 24 hafter satisfactory haemostasis with VBL after oesophageal vari-ceal bleeding was as effective as 72 h of treatment114
In patients intolerant of terlipressin or in countries where ter-lipressin is not available alternatives should be considered
Somatostatin and octreotideSomatostatin causes selective splanchnic vasoconstriction andreduces portal pressure and portal blood flow115 Octreotide is asomatostatin analogue The mechanism of action of these twoagents is not clear Inhibition of glucagon increases vasodilatationrather than a direct vasoconstrictive effect and post-prandial guthyperaemia is also reduced The actions of octreotide on hepaticand systemic hemodynamics are transient making continuousinfusion necessary Octreotide is given as a 50 μg bolus followedby an infusion of 25ndash50 μgh Somatostatin is given as a 250 mgintravenous bolus followed by an infusion of 250 mghSomatostatin and octreotide have been shown to be aseffective as terlipressin in acute variceal bleeding in ameta-analysis110 Seo et al111 in a large RCTof 780 patients com-paring these three agents failed to show a difference in treatmentsuccess (range 838ndash862) rebleeding (range 34ndash44) andmortality (range 8ndash88) A low systolic blood pressure at pres-entation high serum creatinine level active bleeding in the emer-gency endoscopy gastric variceal bleeding and ChildndashPugh gradeC were independent factors predicting 5-day treatmentfailure111
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 13
Guidelines
AntibioticsAntibiotics that provide Gram-negative cover are one of the inter-ventions which positively influence survival in variceal haemor-rhage as shown in a Cochrane meta-analysis of 12placebo-controlled trials (RR=079 95 CI 063 to 098)116
Antibiotics were also shown to reduce bacterial infections(RR=043 95 CI 019 to 097) and early rebleeding (RR=05395 CI 038 to 074)116 Therefore short-term antibiotics shouldbe considered standard practice in all cirrhotic patients who have avariceal bleed irrespective of the presence of confirmed infectionThird-generation cephalosporins such as ceftriaxone (1 g IVdaily) have been shown to be more effective at reducingGram-negative sepsis than oral norfloxacin117 but choice of anti-biotics must be dictated by local resistance patterns and availability
Proton pump inhibitorsOne RCT compared a short course of proton pump inhibitorswith vasoconstrictor therapies after haemostasis in acute varicealbleeding118 Despite larger ulcers noted in the vasoconstrictorarm there were no differences in bleeding or survival Nearly50 of patients had ascites which might have implications inlight of the reports of increased incidence of spontaneous bac-terial peritonitis as mentioned earlier
Endoscopic therapyEndoscopy should take place within 24 h of admission andearlier if there is excessive bleeding based on low-level evi-dence105 While many guidelines and reviews suggest thatendoscopy should be carried out within 12 h the only study thatexamined the influence of timing on outcome failed to demon-strate any advantage of endoscopy before 12 h119 The optimaltime is after sufficient resuscitation and pharmacological treat-ment with the endoscopy performed by a skilled endoscopyteam in a suitably equipped theatre environment and withairway protection Airway protection is essential where risk ofaspiration is high and affords the endoscopist time for thoroughevaluation including complete clot aspiration and controlledapplication of treatment including tamponade if required Theendoscopy team must comprise an experienced endoscopynurse acquainted with the equipment necessary for endoscopytherapy of varices and a skilled endoscopist competent in usingbanding devices and deployment of balloon tamponade
Variceal band ligationThis technique is a modification of that used for the elastic bandligation of internal haemorrhoids Its use in humans was firstdescribed in 1988120 A meta-analysis of seven trials comparingVBL with sclerotherapy in acute bleeding showed that VBLreduced rebleeding from varices (OR=047 95 CI 029 to078) reduced mortality (OR=067 95 CI 046 to 098) andresulted in fewer oesophageal strictures (OR=010 95 CI003 to 029)121 The number of sessions required to obliteratevarices was lower with VBL (22 fewer sessions (95 CI 09to 35))
SclerotherapySclerotherapy has been replaced by VBL and should no longerbe offered as standard of care in acute variceal haemorrhage
Other endoscopic measuresIn an RCT cyanoacrylate offered no benefit over VBL with theadditional risk of embolisation and trend towards increasedrebleeding with cyanoacrylate122
Haemostatic powder (TC-325 Hemospray Cook MedicalUSA) has been described in a small study of nine patients whoreceived endoscopic spray treatment for acute variceal bleedingThe study reported no rebleeding within 24 h and no mortalityat 15 days123
Endoscopic therapy in combination with pharmacological therapyThe role of combining vasoactive drugs with endoscopictherapy (VBL or sclerotherapy) was reported in a meta-analysisof eight trials124 Combination therapy resulted in better initialcontrol of bleeding (RR=112 95 CI 102 to 123) and5-day haemostasis (RR=128 95 CI 118 to 139) withoutany difference in survival Adverse events were similar in bothgroups Two RCTs have compared VBL with sclerotherapy incombination with vasoactive agents in acute variceal bleed-ing125 126 Lo et al125 used vasopressin and found that VBLresulted in better 72 h haemostasis (97 vs 76 p=0009)with fewer complications (5 vs 29 p=0007) Villanuevaet al used somatostatin and reported lower failure to controlacute bleeding with VBL (4 vs 15 p=002) with fewerserious complications (4 vs 13 p=004) Overall survivalwas similar in both trials125 126
Balloon tamponadeBalloon tamponade is highly effective and controls acute bleed-ing in up to 90 of patients although about 50 rebleed whenthe balloon is deflated127 128 It is however associated withserious complications such as oesophageal ulceration and aspir-ation pneumonia in up to 15ndash20 of patients Despite this itmay be a life-saving treatment in cases of massive uncontrolledvariceal haemorrhage pending other forms of treatment Anappropriately placed SengstakenndashBlakemore tube allows forresuscitation safe transportation and either repeat endoscopy orradiological shunting in a patient with a stable cardiovascularsystem The oesophageal balloon is rarely required must neverbe used on its own and should be used only if there is continu-ing bleeding despite an adequately inflated gastric balloon cor-rectly placed and with appropriate tension Placement of thetube endoscopically or over a guide wire might reduce the riskof complications especially oesophageal rupture
Removable oesophageal stentsThe SX-Ella Danis stent (ELLA-CS Hradec Kralove CzechRepublic) is a removable covered metal mesh stent placed endo-scopically in the lower oesophagus without radiological screen-ing It has no role in the management of gastric varicealbleeding These stents can be left in situ for up to 2 weeksunlike the SengstakenndashBlakemore tube which should beremoved after a maximum of 24ndash48 h129 130 No published con-trolled trials have compared this modality with balloontamponade
Transjugular intrahepatic portosystemic stent-shuntSeveral uncontrolled studies have examined the role of salvagebare TIPSS in acute variceal bleeding In a review of 15 studiescontrol of bleeding was achieved in 90ndash100 with rebleedingin 6ndash16131 Mortality varied between 75 (in hospital) and15 (30 day) It is important to appreciate that sclerotherapywas used as first-line endoscopic therapy in most of thesestudies Long-term follow-up of a study that compared TIPSSwith H-graft portacaval shunts in patients for whom non-operative management had failed suggested that H-grafts were auseful method of reducing portal pressure and had a signifi-cantly lower failure rate (p=004) but had no significant
14 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
improvement in overall survival despite a benefit seen in ChildrsquosA and B disease132 A recent RCT compared emergency porto-caval surgery with bare TIPSS within 24 h of presenting withacute oesophageal variceal bleeding in unselected cirrhoticpatients Emergency portocaval surgery resulted in better out-comes for long-term bleeding control encephalopathy and sur-vival (plt0001)133 Before wider application of surgery foracute variceal bleeding more data are needed in light of therecent adoption of covered stents
There has also been a generalised established change in prac-tice in using covered TIPSS stents (polytetrafluoroethylene(PTFE)) rather than a bare metal stent with evidence to supportthis change In randomised controlled studies these stents wereshown to have higher primary patency rates than bare stentswithout significant differences in survival and the potential forreduced incidence of hepatic encephalopathy134 135
There is however growing evidence from two RCTs for theearlier use of TIPSS in selected patients stratified by HVPGChildndashPugh class and active bleeding and not just use as asalvage option6 136 Monescillo et al136 randomised patientspresenting with acute oesophageal variceal haemorrhage to bareTIPSS or standard of care if the HVPG was ge20 mm Hg within24 h of admission Significantly reduced treatment failure asdefined by failure to control acute bleeding andor early rebleed-ing (12 vs 50) was seen and improved survival (62 vs35) in the patients randomised to undergo a TIPSS procedureHowever the standard of care was sclerotherapy and not com-bination endoscopic and pharmacological treatment This limita-tion and the lack of availability of HVPG measurement in mostcentres meant this trial did not have a significant impact on clin-ical practice
Garcia-Pagan et al6 selected patients with active bleeding andChildrsquos B cirrhosis or patients with Childrsquos C cirrhosis (Childrsquosscore lt14) for randomisation to early PTFE-covered TIPSSwithin 72 h or standard of care with VBL and pharmacologicaltreatment This has shown encouraging results with reduced riskof treatment failure (3 vs 50) improved survival (86 vs61 at 1 year) yet without increased risk of hepatic encephal-opathy The results were supported by an observational studyfrom the same group although a survival benefit was notseen137 Furthermore a recent well-conducted observationalstudy did not demonstrate such high survival rates with earlyTIPSS with 11-year survival of 67 which was similar to thatof patients given endoscopic and pharmacological treatmentsonly138 Therefore larger multicentred RCTs need to be under-taken to further evaluate the role of early TIPSS It is importantto make the distinction between salvage TIPSS and early TIPSSto prevent rebleeding
Liver transplantationThis is probably appropriate only for patients who bleed whileawaiting liver transplantation although studies comparing VBLor TIPSS placement with urgent liver transplantation in thissituation need to be done Liver transplantation is an exceed-ingly rare option for the vast majority of patients both becauseit is not commonly available and because of shortages anddelays in organ procurement No controlled trials of liver trans-plantation in uncontrolledactive bleeding are available
Recommendations for the control of variceal bleeding in cir-rhosis are given below and in figure 3
Recommendations control of active variceal haemorrhage incirrhosis (figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with bloodplatelets and clotting factors in line with local protocolsfor managing massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusionpolicy aiming for a haemoglobin of 70ndash80 gL is sug-gested in haemodynamically stable patients (level 1bgrade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable(level 5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L(level 5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to localcircumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with suspected
or confirmed variceal bleeding (level 1a grade A)32 In all patients vasoconstrictors such as terlipressin or
somatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 15
Guidelines
41 If bleeding is difficult to control a SengstakenndashBlakemore tube should be inserted until further endo-scopic treatment TIPSS or surgery is performed depend-ing on local resources and expertise (level 1b grade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure (level1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
SECONDARY PROPHYLAXIS OF VARICEAL HAEMORRHAGEβ BlockersA meta-analysis of 12 trials comparing propranolol or nadolol139
with no active treatment showed a significant reduction inrebleeding but no significant reduction in mortality140 Thegreater reduction in portal pressure with carvedilol comparedwith propranolol has been described in the section lsquoPrimaryprophylaxisrsquo of this guideline
NitratesThe addition of ISMN to NSBB has been shown to reduce vari-ceal rebleeding compared with NSBB alone although no sur-vival benefit was seen141 In addition adverse events leading todrug withdrawal were more common in the group receivingcombined drug treatment A meta-analysis of ISMN alone orwith either NSBB or endoscopic therapy reported that there wasno mortality benefit from combining nitrates and NSBB com-pared with NSBB alone142
Side effects of ISMN include dizziness and headache Owingto the side effects and relative lack of data ISMN is not com-monly used in clinical practice
A recent RCT of 121 patients reported carvedilol to besimilar to combined ISMN and NSBB therapy in the preventionof variceal rebleeding and mortality although severe adverseevents were less common with carvedilol143
SimvastatinA recent abstract of a multicentre RCT of 158 patients reporteda survival benefit (91 vs 78 p=003) from adding simvasta-tin to VBL and NSBB compared with placebo VBL and NSBBas treatment for the prevention of variceal rebleeding144 Therewas no difference in rebleeding and the survival benefit wasrestricted to Child A and B patients Serious adverse events weresimilar in both groups More data are required to investigatethis interesting observation of a survival benefit from simvastatinin this situation which may relate to its effects on hepatocellularfunction fibrosis and portal pressure
Proton pump inhibitorsA double-blind randomised placebo-controlled trial showed thatpantoprazole reduced the size of ulcers in patients who under-went VBL However the total number of ulcers and other out-comes were similar in the two groups145
Endoscopic therapyVBL has been accepted as the preferred endoscopic treatmentfor the prevention of variceal rebleeding with a lower rate ofrebleeding mortality and complications than sclerother-apy146 147 The time interval between VBL sessions to achieveeradication of varices is debateable However a recent RCTcomparing monthly with biweekly VBL after initial haemostasiswith VBL in 70 patients suggested that there were fewerpost-VBL ulcers in the monthly group (11 vs 57plt0001)148 Variceal recurrence rebleeding and mortality weresimilar in both groups
Two meta-analyses showed there is no evidence that the add-ition of sclerotherapy to VBL improves clinically relevant out-comes including variceal rebleeding and death and thecombination led to higher stricture rates149 150
Endoscopic therapy versus drug therapyVBL has been reported to be more effective than combinedNSBB and ISMN drug therapy151 However an 8-yearfollow-up study of this RCT found that although VBL wassuperior in reducing variceal rebleeding survival rates were sig-nificantly higher in the group treated with combined drug treat-ment152 Other studies have found no superiority of VBL overcombined drug therapy for prevention of variceal rebleeding ormortality153 154 A recent small multicentre RCT reported carve-dilol to be similar to VBL in the prevention of variceal rebleed-ing with a trend in favour of survival with carvedilol (73 vs48 p=0110)155
Several meta-analyses have compared drug therapy with VBLin the prevention of variceal rebleeding One meta-analysis ofsix RCTs showed no significant difference in variceal rebleedingrates when comparing VBL alone with combined NSBB andISMN therapy However all-cause mortality was significantlyhigher in patients treated with the VBL (RR=125 95 CI101 to 155)156 Three meta-analyses comparing drug therapy(NSBB alone or with ISMN) with endoscopic therapy alonereported no difference in variceal rebleeding or mortality157ndash159
Endoscopic+drug therapy versus either aloneNumerous studies and several meta-analyses have comparedcombined endoscopic and drug therapy with monotherapy(endoscopic or drugs alone) in the prevention of varicealrebleeding A meta-analysis of 23 trials assessing sclerotherapyor VBL combined with NSBB reported that combinationtherapy reduced rebleeding more than either endoscopic
16 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

bleed it seems rational to develop prophylactic regimens toprevent the development of and bleeding from these varicesHowever most of the published trials do not have sufficientpower to identify favourable treatment effects Based on theexpected bleeding and death rates in the control group theminimum number of patients needed to detect a 50 reductionin bleeding would be 270 and 850 patients in each arm todetect the same reduction in mortality A proposed algorithmfor surveillance and prophylaxis of varices is shown in figure 2At this time there is insufficient evidence to support treatingpatients without varices or lsquopre-primary prophylaxisrsquo A largerandomised placebo-controlled trial of timolol in patientswithout varices and portal hypertension defined as HVPGgt6 mm Hg did not show any effect on the development ofvarices or variceal bleeding27 The role of drug treatment in pre-venting bleeding in patients with small varices is unclear Threerandomised placebo-controlled trials have studied this Caleset al61 showed that propranolol in patients with small or novarices resulted in greater development of varices Howeverpatients without varices were included and there was significantloss of patients to follow-up The second trial showed thatnadolol reduced variceal bleeding without survival benefit andincreased adverse events62 Sarin et al63 did not show any effectwith propranolol despite a significant effect on portal pressure
SurgeryPortacaval shuntsFour trials of portacaval shunts have been published which ran-domised a total of 302 patients64ndash67 either to prophylactic shuntsurgery or to non-active treatment A meta-analysis of thesestudies showed a significant benefit in the reduction of varicealbleeding (OR=031 95 CI 017 to 056) but also a signifi-cantly greater risk of hepatic encephalopathy (OR=2 95 CI12 to 31) and mortality (OR=16 95 CI 102 to 257) inpatients treated with shunt surgery68 At this time there is noevidence for the use of TIPSS for primary prophylaxis1
Devascularisation proceduresInokuchi50 showed that there was a significant reduction in vari-ceal bleeding and in mortality in patients treated with a varietyof devascularisation procedures There are however numerousproblems with the interpretation of this study because of theuse of different procedures in each of the 22 centres Theseresults require confirmation
Pharmacological treatmentNon-cardioselective β blockersThe mainstay of the pharmacological approach to the primaryprophylaxis of variceal haemorrhage has been NSBBPropranolol which has been shown to reduce the PPG reduceazygos blood flow and also variceal pressure It achieves this bycausing splanchnic vasoconstriction and reducing cardiacoutput There is no clear dose-related reduction in HVPG orcorrelation of HPVG reduction with reduction in heart rate69
Observational studies have shown that a 10ndash12 reduction inHVPG after acute administration of propranolol was associatedwith reduced bleeding and hepatic decompensation54 70
However HVPG monitoring is not routinely available in mostcentres outside of larger institutions A meta-analysis of nineplacebo-controlled randomised trials (964 patients) showed thatthe pooled risk difference for bleeding was minus11 (95 CIminus21 to minus1) and for death was minus9 (95 CI minus18 tominus1) in favour of propranolol71
Nadolol exerts similar effects on portal haemodynamicsalthough the effect on blood pressure may not be as pro-nounced Two placebo-controlled trials58 59 have shownreduced bleeding although in one study this was only seen onper protocol analysis59 There was no effect on overall survival
Carvedilol is a NSBB like propranolol and a vasodilator dueto α1 receptor blockade The latter reduces portocollateralresistance and by actions on hepatic stellate cells leads to areduction in intrahepatic resistance Haemodynamic studiesdemonstrate a greater reduction in portal pressure with
Figure 2 Algorithm for surveillance of varices and primary prophylaxis in cirrhosisndash If there is clear evidence of disease progression this interval can be modified by clinician Endoscopy should also be offered at time ofdecompensation
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 9
Guidelines
carvedilol than with propranolol although blood pressure isreduced72 73 The optimum dose is 625ndash125 mgday74 Higherdoses are not more effective and are associated with moreadverse eventsmdashin particular hypotension Carvedilol at a doseof 125 mgday at current UK prices is considerably cheaperthan propranolol 40 mg twice a day and nadolol 80 mgday(monthly cost pound120 pound562 and pound5 respectively) Two RCTs ofcarvedilol versus variceal band ligation (VBL) in primaryprophylaxis have been published75 76 The first study75 showedsignificantly reduced bleeding in the carvedilol arm (10 vs23 relative hazard 041 95 CI 019 to 096) with no effecton survival The second trial by Shah et al76 did not show anydifferences in bleeding or mortality Compliance with VBL wasbetter in the latter trial and unlike the first trial there were sig-nificantly more patients with viral hepatitis than alcoholic cir-rhosis A further study74 assessed the effect of carvedilol inpatients who were haemodynamic non-responders to propran-olol where haemodynamic response was defined as HVPGreduction to le12 mm Hg or by gt20 of baseline after 4 weeksof treatment Patients who were haemodynamic non-respondersor intolerant to carvedilol were treated with VBL Carvedilolresulted in significantly lower variceal bleeding compared withVBL and haemodynamic responders to carvedilol or propran-olol had significantly lower mortality than those treated withVBL It is worth noting that the study was not randomised
There have been recent suggestions based on low-level evi-dence that NSBB may result in a poorer outcome in patientswith cirrhosis and refractory ascites77 The lsquowindow hypothesisrsquofor β blockers in cirrhosis has also recently been described sug-gesting that NSBB are helpful in the compensated and earlydecompensated cirrhotic period but may not be helpful in veryearly cirrhosis such as in a patient with no varices and may beharmful in patients with end-stage cirrhosis with refractoryascites78 However recent large observational studies questionthe last hypothesis with improved survival seen in patients withrefractory ascites treated with NSBB79 unless patients have anepisode of spontaneous bacterial peritonitis80 Therefore untilthere are further prospective controlled studies NSBB should becontinued in patients with refractory ascites The clinician mustcarefully monitor haemodynamic parameters such as blood pres-sure and discontinue NSBB in patients with hypotension andrenal impairment as can occur after an episode of spontaneousbacterial peritonitis Other potentially severe adverse eventswith NSBB include symptomatic bradycardia asthma andcardiac failure Less severe side effects such as fatigue insomniaand sexual dysfunction may also result
Isosorbide mononitrateInterest in the use of vasodilators such as isosorbide mononitrate(ISMN) developed after the demonstration that it reduces portalpressure as effectively as propranolol81 but has subsequentlywaned A trial comparing ISMN with propranolol showed nosignificant difference between these agents82 Another rando-mised trial of ISMN versus placebo did show any difference inthe two arms83 Therefore ISMN is not recommended asmonotherapy in primary prophylaxis
β Blocker and ISMNThe combination of nadolol and ISMN has been compared withnadolol in a RCT The combination therapy reduced the fre-quency of bleeding significantly but no significant differenceswere detected in mortality84 However Garcia-Pagan et al85 in adouble-blind RCTof propranolol plus ISMN versus propranolol
plus placebo failed to show any differences between the twoarms Combination therapy is associated with more side effects
Proton pump inhibitorsA placebo-controlled randomised trial reported reduced bleed-ing and mortality with rabeprazole after eradication of varices86
However the study had a heterogeneous population with VBLperformed for both primary and secondary prophylaxis andsmall numbers (n=43) limiting the validity of the conclusionsFurthermore there was no arm comparing proton pump inhibi-tors with NSBB The use of proton pump inhibitors in patientswith cirrhosis and ascites was associated with increased risk ofspontaneous bacterial peritonitis in a large retrospective study87
This was not confirmed in a larger prospective non-randomisedstudy88 However a recent prospective observational study hasshown proton pump use to be associated with increased mortal-ity in cirrhosis89 Proton pump inhibitors are also associatedwith increased risk of Clostridium difficile infection90 Thereremains continuing concern about proton pump inhibitors inpatients with cirrhosis therefore caution should be used
Endoscopic therapyVariceal band ligationVBL has been compared with NSBB in 19 trials in a recentCochrane meta-analysis of 1504 patients91 Despite reducedbleeding (RR=067 95 CI 046 to 098) with VBL there wasno difference in overall mortality and bleeding-related mortalityThe difference in bleeding was not seen when only trials withlow selection or attrition bias were included Banding can haveserious complications The risk of fatal banding-induced bleed-ing was highlighted in a meta-analysis showing reduced fataladverse events with NSBB (OR=014 95 002 to 099)92
The optimal timing of banding intervals is discussed in thesection lsquoSecondary prophylaxis of variceal haemorrhagersquo A ran-domised trial of 96 patients who underwent endoscopic surveil-lance at 6 or 3 months after eradication of varices with VBL didnot demonstrate a difference in bleeding on mortality93
However the trial had a heterogeneous study group of patientswho underwent VBL both for primary (65) and secondaryprevention (35)
SclerotherapyNineteen trials have compared endoscopic variceal sclerotherapywith no treatment68 Owing to the marked heterogeneitybetween these studies a meta-analysis is clinically inappropri-ate68 Sclerotherapy does not offer any benefit in combinationwith NSBB or VBL compared with VBL or NSBB alone andincreases iatrogenic complications such as strictures94ndash96 At thistime sclerotherapy cannot be recommended for prophylaxis ofvariceal haemorrhage in patients with cirrhosis
Recommendations primary prophylaxis of variceal haemor-rhage in cirrhosis (figure 2)1 What is the best method for primary prophylaxis
11 We recommend NSBB or variceal band ligation (VBL)We suggest pharmacological treatment with propranololas first line VBL is offered if there are contraindicationsto NSBB The choice of VBL or NSBB should also takeinto account patient choice (level 1a grade A)
12 We suggest carvedilol or nadolol as alternatives to pro-pranolol (level 1b grade A)
13 Dose131 Propranolol 40 mg twice daily Dose titrated to
maximum tolerated or once heart rate (HR) of
10 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
50ndash55 bpm is reached to a maximum dose of320 mg (level 1a grade A)
132 Nadolol 40 mg daily dose Dose titrated tomaximum tolerated or once HR of 50ndash55 bpm isreached a maximum dose of 240 mg (level 1agrade A)
133 Carvedilol 625 mg once daily to increase tomaintenance of 125 mg after a week if toleratedor once HR of lt50ndash55 bpm is reached (level 1agrade A)
134 It is suggested that NSBB are discontinued at thetime of spontaneous bacterial peritonitis renalimpairment and hypotension (level 2b grade B)
14 In cases of contraindications or intolerance to NSBB werecommend variceal band ligation (level 1a grade A)
2 Who should have surveillance for variceal bleeding21 We recommend all patients with cirrhosis should be
endoscoped at the time of diagnosis (level 1a grade A)There is no indication to repeat endoscopy in patientsreceiving NSBB
3 How often should cirrhotic patients be endoscoped31 If at the time of first endoscopy no varices are seen we
suggest that patients with cirrhosis should be endos-coped at 2ndash3-year intervals (level 2a grade B)
32 If grade I varices are diagnosed we suggest that patientsshould be endoscoped at yearly intervals (level 2agrade B)
33 If there is clear evidence of disease progression wesuggest that the intervals can be modified by a clinicianEndoscopy should also be offered at time of decompen-sation (level 2a grade B)
4 Which patients with cirrhosis should have primaryprophylaxis41 If grade I varices and red signs or grade 2ndash3 varices are
diagnosed we recommend that patients have primaryprophylaxis irrespective of the severity of the liverdisease (level 1a grade A)
5 Treatments not recommended51 Proton pump inhibitors are not recommended unless
otherwise required for peptic ulcer disease (level 1bgrade B)
52 Isosorbide mononitrate monotherapy is not recommendedas primary prophylaxis (level 1b grade A) There is insuffi-cient evidence to recommend isosorbide mononitrate incombination with NSBB (level 1b grade A)
53 Shunt surgery or TIPSS is not recommended as primaryprophylaxis (level 1a grade A)
54 Sclerotherapy is not recommended as primary prophy-laxis (level 1a grade A)
6 Areas requiring further study61 Role of NSBB in patients without varices with focus on
carvedilol62 Role of NSBB in patients with small varices with focus
on carvedilol63 Comparison of carvedilol versus propranolol in primary
prophylaxis64 Identification of and trials assessing new drugs for
primary prophylaxis such as statins7 Quality indicator
71 Percentage of patients at diagnosis of cirrhosis who havehad an endoscopy to screen for varices (level 1agrade A)Numerator patients diagnosed with cirrhosis who havehad an endoscopy either before or after diagnosis within
6 monthsDenominator patients newly diagnosed with cirrhosis
72 Percentage of patients receiving primary prophylaxisamong those newly diagnosed with grade I varices andred signs or grade 2ndash3 varicesNumerator patients who have grade 1 varices with redsigns or grade 2ndash3 varices receiving primary prophy-laxisDenominator patients diagnosed with cirrhosis whohave grade I varices with red signs or grade 2ndash3 varices
MANAGEMENT OF ACTIVE VARICEAL HAEMORRHAGEThe average 6-week mortality of the first episode of varicealbleeding in most studies is reported to be up to 20 There hasbeen considerable improvement in survival since the early 1980swhen the in-hospital mortality was 40ndash5097 compared with15 from a recent UK audit5 Such is the improvement in out-comes that a patient with Childrsquos A cirrhosis is very unlikely tosuccumb to an index variceal bleed Studies have shown theChildndashPugh score MELD score and HVPG to be strong predic-tors of outcomes98ndash103 The MELD score has been shown tooutperform Childrsquos score in a recent study with a score gt19associated with 20 6 week mortality103 Furthermore theMELD score has been shown to perform as well as the trad-itional intensive care unit scores in predicting mortality inpatients admitted to intensive care in the UK104 MELD gt18active bleeding transfusing gt4 units of packed red blood cellshave been shown to be predictors of mortality and earlyrebleeding99 101 102 HVPG has also been shown to predictoutcome when measured at 2 weeks after a bleed44 and a valueof ge20 mm Hg when measured acutely within 48 h has beenshown to provide significant prognostic information100
However this technique is not used routinely in the manage-ment of patients around the world and substitution of clinicaldata in the latter study was shown to provide the same clinicalpredictive value100 These scoring systems are not purely aca-demic they allow the referring clinician to predict thosepatients with a high chance of rebleeding to be transferred to aspecialist centre offering for instance TIPSS before the patientrebleeds
Nonetheless probably the most important step in the man-agement of acute variceal haemorrhage is the initial resuscitationassessed according to standard lsquoABCrsquo practice together withprotection of the airway to prevent aspiration Although earlyendoscopy allows for accurate diagnosis of the bleeding site anddecisions about management (figure 3) therapeutic interventionin acute variceal bleeding can be initiated safely in most casesbefore diagnostic endoscopy As similar efficacy is demonstratedwith pharmacological treatment as with sclerotherapy theformer should be first-line therapy99 β Blockade should not bestarted in the acute setting and those already taking β blockersas prophylaxis should probably stop taking them for 48ndash72 h inorder that the patientrsquos physiological response to blood loss canbe allowed to manifest
General considerationsPatient evaluationThe majority of patients with a variceal bleed will be sufficientlystable to enable a full history and examination to take placeHistory of alcohol excess and or intravenous drug use should besought and may become particularly relevant if the patient haswithdrawal symptoms after admission Comorbidity is importantwhen estimating risk and deciding on use of vasopressors The
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 11
Guidelines
following risk factors doubled mortality after an acute varicealbleed in one US study older age comorbidities male gender andnot undergoing a gastroscopy within 24 h105
A full examination is helpful for the important negatives asmuch as the positives Baseline observations should include thetemperature as infection is a serious complication with signifi-cant mortality Confusion may be present because of encephal-opathy intoxication with alcohol or drugs or withdrawal fromalcohol or drugs The patient should be on continuous BP andpulse monitor and their haemodynamic status recordedAn oxygen saturation monitor is helpful Stigmata of chronicliver disease and concurrent jaundice provide insight into thecurrent status of a patientrsquos liver and also give warning ofpotential further decompensation if significant bleeding persists(see scoring systems above) Pneumonia must be actively
excluded Evidence of ascites requires a diagnostic tap to searchfor infection
Investigations including full blood count coagulationprofile liver and renal function and blood group and save andcross-match Blood and urine should also be cultured An ultra-sound scan later in the admission is helpful to identify subclin-ical ascites flow in portal vein and any obvious emergence of anhepatocellular carcinoma (HCC)
Location of patientA decision must be made as to where the patient is best managedVariceal bleeding is unpredictable generally occurs in patientswith significant liver disease and is associated with significant mor-tality Hence a high-dependency unit is usually the most appropri-ate initial location although a properly staffed lsquogastrointestinal
Figure 3 Algorithm for themanagement of acute varicealbleeding TIPSS transjugularintrahepatic portosystemic stent shunt
12 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleeding bedrsquo may be appropriate If a patient is vomiting bloodor there is a perceived risk of a haemodynamically unstable patienthaving blood in the stomach then the patient must be intubatedbefore endoscopy and return to an intensive care or high-dependency unit will be necessary until extubation
Volume resuscitation and blood productsIntravenous access (two 16ndash18G cannulae) should have beensecured on admission with a reported GI bleed Further intra-venous access may be necessary In patients with poor venousaccess advanced liver disease or renal failure associated withtheir liver disease central venous access may be helpful withguiding fluid infusions However the drawbacks include the riskof the procedure and a potential source of infection Thereforethere is no absolute requirement for a central line and no evi-dence of unequivocal benefit Intravenous fluid resuscitationshould be initiated with plasma expanders aiming to maintain asystolic blood pressure of 100 mm Hg Care with monitoring isparamount in this group of patients
Overtransfusion has been shown to have a deleterious effecton outcome In a recent single-centre RCT a restrictive transfu-sion policy of maintaining haemoglobin between 70 and 80 gLimproved the control of variceal bleeding (11 vs 22p=005) and lowered HVPG compared with a liberal transfu-sion policy without effect on 45-day survival106 However itshould be noted that these results were from a single Spanishcentre which was a tertiary unit for variceal bleeding where allpatients underwent endoscopy within 6 h Nonetheless arestrictive transfusion policy has been recommended for sometime1 and there is now good evidence to support not transfusinga stable patient with a haemoglobin of ge80 gL However under-resuscitation should also be avoided and while goal-orientedfluid replacement has generally not been useful in an intensivetherapy unit setting a venous saturation gt70 remains an easilymeasurable target with some evidence to support it107
Interpretation and management of clotting profile is challen-ging in liver disease where there is usually a balanced deficiencyof both procoagulant and anticoagulant factors108 The NICEguidelines recommend activation of a hospitalrsquos massive transfu-sion policy when there is major haemorrhage and plateletsupport when the value is lt50 and clotting factor supportwhen the international normalised ratio (INR) is gt15 timesnormal2 There is no evidence for the use of lsquoprophylacticrsquo clot-ting or platelet support to reduce the risk of rebleeding Thereis insufficient evidence to support the routine use of transexamicacid or recombinant factor VIIa109
Pharmacological treatmentThe two major classes of drugs that have been used in thecontrol of acute variceal bleeding are vasopressin or its analo-gues (either alone or in combination with nitroglycerine) andsomatostatin or its analogues Terlipressin is the only agent thathas been shown to reduce mortality in placebo-controlled trialsHowever in trials comparing terlipressin somatostatin andoctreotide no difference in efficacy was identified in a system-atic review110 and in a recent large RCT111 Prophylactic anti-biotics can result in a similar survival benefit following acutevariceal bleeding
VasopressinVasopressin reduces portal blood flow portal systemic collateralblood flow and variceal pressure It does however have signifi-cant systemic side effects such as an increase in peripheral resist-ance and reduction in cardiac output heart rate and coronary
blood flow In comparison with no active treatment the pooledresults of four randomised trials showed that it reduced failureto control variceal bleeding (OR=022 95 CI 012 to 043)although survival was unaffected68 Meta-analysis of five trialscomparing sclerotherapy with vasopressin has shown a signifi-cant effect on reduction in failure to control bleeding(OR=051 95 CI 027 to 097) with no effect on survival68
Vasopressin with nitroglycerineThe addition of nitroglycerine enhances the effect of vasopres-sin on portal pressure and reduces cardiovascular side effects112
Meta-analysis of three randomised trials comparing vasopressinalone with vasopressin and nitroglycerine showed that the com-bination was associated with a significant reduction in failure tocontrol bleeding (OR=039 95 CI 022 to 072) although nosurvival benefit was shown68
TerlipressinTerlipressin is a synthetic analogue of vasopressin which has animmediate systemic vasoconstrictor action followed by portalhaemodynamic effects due to slow conversion to vasopressin Ina Cochrane meta-analysis of seven placebo-controlled trials ter-lipressin was shown to reduce failure to control bleeding(RR=066 95 CI 055 to 093) and also to improve survival(RR=066 95 CI 049 to 088)113 In the same meta-analysisthere was no difference between terlipressin versus vasopressinballoon tamponade or endoscopic therapy in failure to controlbleeding or survival113 The role of terlipressin in combinationwith VBL is explored in the section lsquoEndoscopic therapy incombination with pharmacological therapyrsquo
The recommended dose of terlipressin is 2 mg IV every 4 halthough many units reduce the dose to 6 hourly as it may causeperipheral vasoconstriction which manifests as painful handsand feet While 5 days of IV treatment has been advocated inthe Baveno V guidelines1 this prolonged treatment has notbeen shown to have a survival benefit and for pragmaticreasons many units will stop treatment shortly after satisfactoryhaemostasis In a randomised trial terlipressin given for 24 hafter satisfactory haemostasis with VBL after oesophageal vari-ceal bleeding was as effective as 72 h of treatment114
In patients intolerant of terlipressin or in countries where ter-lipressin is not available alternatives should be considered
Somatostatin and octreotideSomatostatin causes selective splanchnic vasoconstriction andreduces portal pressure and portal blood flow115 Octreotide is asomatostatin analogue The mechanism of action of these twoagents is not clear Inhibition of glucagon increases vasodilatationrather than a direct vasoconstrictive effect and post-prandial guthyperaemia is also reduced The actions of octreotide on hepaticand systemic hemodynamics are transient making continuousinfusion necessary Octreotide is given as a 50 μg bolus followedby an infusion of 25ndash50 μgh Somatostatin is given as a 250 mgintravenous bolus followed by an infusion of 250 mghSomatostatin and octreotide have been shown to be aseffective as terlipressin in acute variceal bleeding in ameta-analysis110 Seo et al111 in a large RCTof 780 patients com-paring these three agents failed to show a difference in treatmentsuccess (range 838ndash862) rebleeding (range 34ndash44) andmortality (range 8ndash88) A low systolic blood pressure at pres-entation high serum creatinine level active bleeding in the emer-gency endoscopy gastric variceal bleeding and ChildndashPugh gradeC were independent factors predicting 5-day treatmentfailure111
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 13
Guidelines
AntibioticsAntibiotics that provide Gram-negative cover are one of the inter-ventions which positively influence survival in variceal haemor-rhage as shown in a Cochrane meta-analysis of 12placebo-controlled trials (RR=079 95 CI 063 to 098)116
Antibiotics were also shown to reduce bacterial infections(RR=043 95 CI 019 to 097) and early rebleeding (RR=05395 CI 038 to 074)116 Therefore short-term antibiotics shouldbe considered standard practice in all cirrhotic patients who have avariceal bleed irrespective of the presence of confirmed infectionThird-generation cephalosporins such as ceftriaxone (1 g IVdaily) have been shown to be more effective at reducingGram-negative sepsis than oral norfloxacin117 but choice of anti-biotics must be dictated by local resistance patterns and availability
Proton pump inhibitorsOne RCT compared a short course of proton pump inhibitorswith vasoconstrictor therapies after haemostasis in acute varicealbleeding118 Despite larger ulcers noted in the vasoconstrictorarm there were no differences in bleeding or survival Nearly50 of patients had ascites which might have implications inlight of the reports of increased incidence of spontaneous bac-terial peritonitis as mentioned earlier
Endoscopic therapyEndoscopy should take place within 24 h of admission andearlier if there is excessive bleeding based on low-level evi-dence105 While many guidelines and reviews suggest thatendoscopy should be carried out within 12 h the only study thatexamined the influence of timing on outcome failed to demon-strate any advantage of endoscopy before 12 h119 The optimaltime is after sufficient resuscitation and pharmacological treat-ment with the endoscopy performed by a skilled endoscopyteam in a suitably equipped theatre environment and withairway protection Airway protection is essential where risk ofaspiration is high and affords the endoscopist time for thoroughevaluation including complete clot aspiration and controlledapplication of treatment including tamponade if required Theendoscopy team must comprise an experienced endoscopynurse acquainted with the equipment necessary for endoscopytherapy of varices and a skilled endoscopist competent in usingbanding devices and deployment of balloon tamponade
Variceal band ligationThis technique is a modification of that used for the elastic bandligation of internal haemorrhoids Its use in humans was firstdescribed in 1988120 A meta-analysis of seven trials comparingVBL with sclerotherapy in acute bleeding showed that VBLreduced rebleeding from varices (OR=047 95 CI 029 to078) reduced mortality (OR=067 95 CI 046 to 098) andresulted in fewer oesophageal strictures (OR=010 95 CI003 to 029)121 The number of sessions required to obliteratevarices was lower with VBL (22 fewer sessions (95 CI 09to 35))
SclerotherapySclerotherapy has been replaced by VBL and should no longerbe offered as standard of care in acute variceal haemorrhage
Other endoscopic measuresIn an RCT cyanoacrylate offered no benefit over VBL with theadditional risk of embolisation and trend towards increasedrebleeding with cyanoacrylate122
Haemostatic powder (TC-325 Hemospray Cook MedicalUSA) has been described in a small study of nine patients whoreceived endoscopic spray treatment for acute variceal bleedingThe study reported no rebleeding within 24 h and no mortalityat 15 days123
Endoscopic therapy in combination with pharmacological therapyThe role of combining vasoactive drugs with endoscopictherapy (VBL or sclerotherapy) was reported in a meta-analysisof eight trials124 Combination therapy resulted in better initialcontrol of bleeding (RR=112 95 CI 102 to 123) and5-day haemostasis (RR=128 95 CI 118 to 139) withoutany difference in survival Adverse events were similar in bothgroups Two RCTs have compared VBL with sclerotherapy incombination with vasoactive agents in acute variceal bleed-ing125 126 Lo et al125 used vasopressin and found that VBLresulted in better 72 h haemostasis (97 vs 76 p=0009)with fewer complications (5 vs 29 p=0007) Villanuevaet al used somatostatin and reported lower failure to controlacute bleeding with VBL (4 vs 15 p=002) with fewerserious complications (4 vs 13 p=004) Overall survivalwas similar in both trials125 126
Balloon tamponadeBalloon tamponade is highly effective and controls acute bleed-ing in up to 90 of patients although about 50 rebleed whenthe balloon is deflated127 128 It is however associated withserious complications such as oesophageal ulceration and aspir-ation pneumonia in up to 15ndash20 of patients Despite this itmay be a life-saving treatment in cases of massive uncontrolledvariceal haemorrhage pending other forms of treatment Anappropriately placed SengstakenndashBlakemore tube allows forresuscitation safe transportation and either repeat endoscopy orradiological shunting in a patient with a stable cardiovascularsystem The oesophageal balloon is rarely required must neverbe used on its own and should be used only if there is continu-ing bleeding despite an adequately inflated gastric balloon cor-rectly placed and with appropriate tension Placement of thetube endoscopically or over a guide wire might reduce the riskof complications especially oesophageal rupture
Removable oesophageal stentsThe SX-Ella Danis stent (ELLA-CS Hradec Kralove CzechRepublic) is a removable covered metal mesh stent placed endo-scopically in the lower oesophagus without radiological screen-ing It has no role in the management of gastric varicealbleeding These stents can be left in situ for up to 2 weeksunlike the SengstakenndashBlakemore tube which should beremoved after a maximum of 24ndash48 h129 130 No published con-trolled trials have compared this modality with balloontamponade
Transjugular intrahepatic portosystemic stent-shuntSeveral uncontrolled studies have examined the role of salvagebare TIPSS in acute variceal bleeding In a review of 15 studiescontrol of bleeding was achieved in 90ndash100 with rebleedingin 6ndash16131 Mortality varied between 75 (in hospital) and15 (30 day) It is important to appreciate that sclerotherapywas used as first-line endoscopic therapy in most of thesestudies Long-term follow-up of a study that compared TIPSSwith H-graft portacaval shunts in patients for whom non-operative management had failed suggested that H-grafts were auseful method of reducing portal pressure and had a signifi-cantly lower failure rate (p=004) but had no significant
14 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
improvement in overall survival despite a benefit seen in ChildrsquosA and B disease132 A recent RCT compared emergency porto-caval surgery with bare TIPSS within 24 h of presenting withacute oesophageal variceal bleeding in unselected cirrhoticpatients Emergency portocaval surgery resulted in better out-comes for long-term bleeding control encephalopathy and sur-vival (plt0001)133 Before wider application of surgery foracute variceal bleeding more data are needed in light of therecent adoption of covered stents
There has also been a generalised established change in prac-tice in using covered TIPSS stents (polytetrafluoroethylene(PTFE)) rather than a bare metal stent with evidence to supportthis change In randomised controlled studies these stents wereshown to have higher primary patency rates than bare stentswithout significant differences in survival and the potential forreduced incidence of hepatic encephalopathy134 135
There is however growing evidence from two RCTs for theearlier use of TIPSS in selected patients stratified by HVPGChildndashPugh class and active bleeding and not just use as asalvage option6 136 Monescillo et al136 randomised patientspresenting with acute oesophageal variceal haemorrhage to bareTIPSS or standard of care if the HVPG was ge20 mm Hg within24 h of admission Significantly reduced treatment failure asdefined by failure to control acute bleeding andor early rebleed-ing (12 vs 50) was seen and improved survival (62 vs35) in the patients randomised to undergo a TIPSS procedureHowever the standard of care was sclerotherapy and not com-bination endoscopic and pharmacological treatment This limita-tion and the lack of availability of HVPG measurement in mostcentres meant this trial did not have a significant impact on clin-ical practice
Garcia-Pagan et al6 selected patients with active bleeding andChildrsquos B cirrhosis or patients with Childrsquos C cirrhosis (Childrsquosscore lt14) for randomisation to early PTFE-covered TIPSSwithin 72 h or standard of care with VBL and pharmacologicaltreatment This has shown encouraging results with reduced riskof treatment failure (3 vs 50) improved survival (86 vs61 at 1 year) yet without increased risk of hepatic encephal-opathy The results were supported by an observational studyfrom the same group although a survival benefit was notseen137 Furthermore a recent well-conducted observationalstudy did not demonstrate such high survival rates with earlyTIPSS with 11-year survival of 67 which was similar to thatof patients given endoscopic and pharmacological treatmentsonly138 Therefore larger multicentred RCTs need to be under-taken to further evaluate the role of early TIPSS It is importantto make the distinction between salvage TIPSS and early TIPSSto prevent rebleeding
Liver transplantationThis is probably appropriate only for patients who bleed whileawaiting liver transplantation although studies comparing VBLor TIPSS placement with urgent liver transplantation in thissituation need to be done Liver transplantation is an exceed-ingly rare option for the vast majority of patients both becauseit is not commonly available and because of shortages anddelays in organ procurement No controlled trials of liver trans-plantation in uncontrolledactive bleeding are available
Recommendations for the control of variceal bleeding in cir-rhosis are given below and in figure 3
Recommendations control of active variceal haemorrhage incirrhosis (figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with bloodplatelets and clotting factors in line with local protocolsfor managing massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusionpolicy aiming for a haemoglobin of 70ndash80 gL is sug-gested in haemodynamically stable patients (level 1bgrade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable(level 5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L(level 5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to localcircumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with suspected
or confirmed variceal bleeding (level 1a grade A)32 In all patients vasoconstrictors such as terlipressin or
somatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 15
Guidelines
41 If bleeding is difficult to control a SengstakenndashBlakemore tube should be inserted until further endo-scopic treatment TIPSS or surgery is performed depend-ing on local resources and expertise (level 1b grade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure (level1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
SECONDARY PROPHYLAXIS OF VARICEAL HAEMORRHAGEβ BlockersA meta-analysis of 12 trials comparing propranolol or nadolol139
with no active treatment showed a significant reduction inrebleeding but no significant reduction in mortality140 Thegreater reduction in portal pressure with carvedilol comparedwith propranolol has been described in the section lsquoPrimaryprophylaxisrsquo of this guideline
NitratesThe addition of ISMN to NSBB has been shown to reduce vari-ceal rebleeding compared with NSBB alone although no sur-vival benefit was seen141 In addition adverse events leading todrug withdrawal were more common in the group receivingcombined drug treatment A meta-analysis of ISMN alone orwith either NSBB or endoscopic therapy reported that there wasno mortality benefit from combining nitrates and NSBB com-pared with NSBB alone142
Side effects of ISMN include dizziness and headache Owingto the side effects and relative lack of data ISMN is not com-monly used in clinical practice
A recent RCT of 121 patients reported carvedilol to besimilar to combined ISMN and NSBB therapy in the preventionof variceal rebleeding and mortality although severe adverseevents were less common with carvedilol143
SimvastatinA recent abstract of a multicentre RCT of 158 patients reporteda survival benefit (91 vs 78 p=003) from adding simvasta-tin to VBL and NSBB compared with placebo VBL and NSBBas treatment for the prevention of variceal rebleeding144 Therewas no difference in rebleeding and the survival benefit wasrestricted to Child A and B patients Serious adverse events weresimilar in both groups More data are required to investigatethis interesting observation of a survival benefit from simvastatinin this situation which may relate to its effects on hepatocellularfunction fibrosis and portal pressure
Proton pump inhibitorsA double-blind randomised placebo-controlled trial showed thatpantoprazole reduced the size of ulcers in patients who under-went VBL However the total number of ulcers and other out-comes were similar in the two groups145
Endoscopic therapyVBL has been accepted as the preferred endoscopic treatmentfor the prevention of variceal rebleeding with a lower rate ofrebleeding mortality and complications than sclerother-apy146 147 The time interval between VBL sessions to achieveeradication of varices is debateable However a recent RCTcomparing monthly with biweekly VBL after initial haemostasiswith VBL in 70 patients suggested that there were fewerpost-VBL ulcers in the monthly group (11 vs 57plt0001)148 Variceal recurrence rebleeding and mortality weresimilar in both groups
Two meta-analyses showed there is no evidence that the add-ition of sclerotherapy to VBL improves clinically relevant out-comes including variceal rebleeding and death and thecombination led to higher stricture rates149 150
Endoscopic therapy versus drug therapyVBL has been reported to be more effective than combinedNSBB and ISMN drug therapy151 However an 8-yearfollow-up study of this RCT found that although VBL wassuperior in reducing variceal rebleeding survival rates were sig-nificantly higher in the group treated with combined drug treat-ment152 Other studies have found no superiority of VBL overcombined drug therapy for prevention of variceal rebleeding ormortality153 154 A recent small multicentre RCT reported carve-dilol to be similar to VBL in the prevention of variceal rebleed-ing with a trend in favour of survival with carvedilol (73 vs48 p=0110)155
Several meta-analyses have compared drug therapy with VBLin the prevention of variceal rebleeding One meta-analysis ofsix RCTs showed no significant difference in variceal rebleedingrates when comparing VBL alone with combined NSBB andISMN therapy However all-cause mortality was significantlyhigher in patients treated with the VBL (RR=125 95 CI101 to 155)156 Three meta-analyses comparing drug therapy(NSBB alone or with ISMN) with endoscopic therapy alonereported no difference in variceal rebleeding or mortality157ndash159
Endoscopic+drug therapy versus either aloneNumerous studies and several meta-analyses have comparedcombined endoscopic and drug therapy with monotherapy(endoscopic or drugs alone) in the prevention of varicealrebleeding A meta-analysis of 23 trials assessing sclerotherapyor VBL combined with NSBB reported that combinationtherapy reduced rebleeding more than either endoscopic
16 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

carvedilol than with propranolol although blood pressure isreduced72 73 The optimum dose is 625ndash125 mgday74 Higherdoses are not more effective and are associated with moreadverse eventsmdashin particular hypotension Carvedilol at a doseof 125 mgday at current UK prices is considerably cheaperthan propranolol 40 mg twice a day and nadolol 80 mgday(monthly cost pound120 pound562 and pound5 respectively) Two RCTs ofcarvedilol versus variceal band ligation (VBL) in primaryprophylaxis have been published75 76 The first study75 showedsignificantly reduced bleeding in the carvedilol arm (10 vs23 relative hazard 041 95 CI 019 to 096) with no effecton survival The second trial by Shah et al76 did not show anydifferences in bleeding or mortality Compliance with VBL wasbetter in the latter trial and unlike the first trial there were sig-nificantly more patients with viral hepatitis than alcoholic cir-rhosis A further study74 assessed the effect of carvedilol inpatients who were haemodynamic non-responders to propran-olol where haemodynamic response was defined as HVPGreduction to le12 mm Hg or by gt20 of baseline after 4 weeksof treatment Patients who were haemodynamic non-respondersor intolerant to carvedilol were treated with VBL Carvedilolresulted in significantly lower variceal bleeding compared withVBL and haemodynamic responders to carvedilol or propran-olol had significantly lower mortality than those treated withVBL It is worth noting that the study was not randomised
There have been recent suggestions based on low-level evi-dence that NSBB may result in a poorer outcome in patientswith cirrhosis and refractory ascites77 The lsquowindow hypothesisrsquofor β blockers in cirrhosis has also recently been described sug-gesting that NSBB are helpful in the compensated and earlydecompensated cirrhotic period but may not be helpful in veryearly cirrhosis such as in a patient with no varices and may beharmful in patients with end-stage cirrhosis with refractoryascites78 However recent large observational studies questionthe last hypothesis with improved survival seen in patients withrefractory ascites treated with NSBB79 unless patients have anepisode of spontaneous bacterial peritonitis80 Therefore untilthere are further prospective controlled studies NSBB should becontinued in patients with refractory ascites The clinician mustcarefully monitor haemodynamic parameters such as blood pres-sure and discontinue NSBB in patients with hypotension andrenal impairment as can occur after an episode of spontaneousbacterial peritonitis Other potentially severe adverse eventswith NSBB include symptomatic bradycardia asthma andcardiac failure Less severe side effects such as fatigue insomniaand sexual dysfunction may also result
Isosorbide mononitrateInterest in the use of vasodilators such as isosorbide mononitrate(ISMN) developed after the demonstration that it reduces portalpressure as effectively as propranolol81 but has subsequentlywaned A trial comparing ISMN with propranolol showed nosignificant difference between these agents82 Another rando-mised trial of ISMN versus placebo did show any difference inthe two arms83 Therefore ISMN is not recommended asmonotherapy in primary prophylaxis
β Blocker and ISMNThe combination of nadolol and ISMN has been compared withnadolol in a RCT The combination therapy reduced the fre-quency of bleeding significantly but no significant differenceswere detected in mortality84 However Garcia-Pagan et al85 in adouble-blind RCTof propranolol plus ISMN versus propranolol
plus placebo failed to show any differences between the twoarms Combination therapy is associated with more side effects
Proton pump inhibitorsA placebo-controlled randomised trial reported reduced bleed-ing and mortality with rabeprazole after eradication of varices86
However the study had a heterogeneous population with VBLperformed for both primary and secondary prophylaxis andsmall numbers (n=43) limiting the validity of the conclusionsFurthermore there was no arm comparing proton pump inhibi-tors with NSBB The use of proton pump inhibitors in patientswith cirrhosis and ascites was associated with increased risk ofspontaneous bacterial peritonitis in a large retrospective study87
This was not confirmed in a larger prospective non-randomisedstudy88 However a recent prospective observational study hasshown proton pump use to be associated with increased mortal-ity in cirrhosis89 Proton pump inhibitors are also associatedwith increased risk of Clostridium difficile infection90 Thereremains continuing concern about proton pump inhibitors inpatients with cirrhosis therefore caution should be used
Endoscopic therapyVariceal band ligationVBL has been compared with NSBB in 19 trials in a recentCochrane meta-analysis of 1504 patients91 Despite reducedbleeding (RR=067 95 CI 046 to 098) with VBL there wasno difference in overall mortality and bleeding-related mortalityThe difference in bleeding was not seen when only trials withlow selection or attrition bias were included Banding can haveserious complications The risk of fatal banding-induced bleed-ing was highlighted in a meta-analysis showing reduced fataladverse events with NSBB (OR=014 95 002 to 099)92
The optimal timing of banding intervals is discussed in thesection lsquoSecondary prophylaxis of variceal haemorrhagersquo A ran-domised trial of 96 patients who underwent endoscopic surveil-lance at 6 or 3 months after eradication of varices with VBL didnot demonstrate a difference in bleeding on mortality93
However the trial had a heterogeneous study group of patientswho underwent VBL both for primary (65) and secondaryprevention (35)
SclerotherapyNineteen trials have compared endoscopic variceal sclerotherapywith no treatment68 Owing to the marked heterogeneitybetween these studies a meta-analysis is clinically inappropri-ate68 Sclerotherapy does not offer any benefit in combinationwith NSBB or VBL compared with VBL or NSBB alone andincreases iatrogenic complications such as strictures94ndash96 At thistime sclerotherapy cannot be recommended for prophylaxis ofvariceal haemorrhage in patients with cirrhosis
Recommendations primary prophylaxis of variceal haemor-rhage in cirrhosis (figure 2)1 What is the best method for primary prophylaxis
11 We recommend NSBB or variceal band ligation (VBL)We suggest pharmacological treatment with propranololas first line VBL is offered if there are contraindicationsto NSBB The choice of VBL or NSBB should also takeinto account patient choice (level 1a grade A)
12 We suggest carvedilol or nadolol as alternatives to pro-pranolol (level 1b grade A)
13 Dose131 Propranolol 40 mg twice daily Dose titrated to
maximum tolerated or once heart rate (HR) of
10 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
50ndash55 bpm is reached to a maximum dose of320 mg (level 1a grade A)
132 Nadolol 40 mg daily dose Dose titrated tomaximum tolerated or once HR of 50ndash55 bpm isreached a maximum dose of 240 mg (level 1agrade A)
133 Carvedilol 625 mg once daily to increase tomaintenance of 125 mg after a week if toleratedor once HR of lt50ndash55 bpm is reached (level 1agrade A)
134 It is suggested that NSBB are discontinued at thetime of spontaneous bacterial peritonitis renalimpairment and hypotension (level 2b grade B)
14 In cases of contraindications or intolerance to NSBB werecommend variceal band ligation (level 1a grade A)
2 Who should have surveillance for variceal bleeding21 We recommend all patients with cirrhosis should be
endoscoped at the time of diagnosis (level 1a grade A)There is no indication to repeat endoscopy in patientsreceiving NSBB
3 How often should cirrhotic patients be endoscoped31 If at the time of first endoscopy no varices are seen we
suggest that patients with cirrhosis should be endos-coped at 2ndash3-year intervals (level 2a grade B)
32 If grade I varices are diagnosed we suggest that patientsshould be endoscoped at yearly intervals (level 2agrade B)
33 If there is clear evidence of disease progression wesuggest that the intervals can be modified by a clinicianEndoscopy should also be offered at time of decompen-sation (level 2a grade B)
4 Which patients with cirrhosis should have primaryprophylaxis41 If grade I varices and red signs or grade 2ndash3 varices are
diagnosed we recommend that patients have primaryprophylaxis irrespective of the severity of the liverdisease (level 1a grade A)
5 Treatments not recommended51 Proton pump inhibitors are not recommended unless
otherwise required for peptic ulcer disease (level 1bgrade B)
52 Isosorbide mononitrate monotherapy is not recommendedas primary prophylaxis (level 1b grade A) There is insuffi-cient evidence to recommend isosorbide mononitrate incombination with NSBB (level 1b grade A)
53 Shunt surgery or TIPSS is not recommended as primaryprophylaxis (level 1a grade A)
54 Sclerotherapy is not recommended as primary prophy-laxis (level 1a grade A)
6 Areas requiring further study61 Role of NSBB in patients without varices with focus on
carvedilol62 Role of NSBB in patients with small varices with focus
on carvedilol63 Comparison of carvedilol versus propranolol in primary
prophylaxis64 Identification of and trials assessing new drugs for
primary prophylaxis such as statins7 Quality indicator
71 Percentage of patients at diagnosis of cirrhosis who havehad an endoscopy to screen for varices (level 1agrade A)Numerator patients diagnosed with cirrhosis who havehad an endoscopy either before or after diagnosis within
6 monthsDenominator patients newly diagnosed with cirrhosis
72 Percentage of patients receiving primary prophylaxisamong those newly diagnosed with grade I varices andred signs or grade 2ndash3 varicesNumerator patients who have grade 1 varices with redsigns or grade 2ndash3 varices receiving primary prophy-laxisDenominator patients diagnosed with cirrhosis whohave grade I varices with red signs or grade 2ndash3 varices
MANAGEMENT OF ACTIVE VARICEAL HAEMORRHAGEThe average 6-week mortality of the first episode of varicealbleeding in most studies is reported to be up to 20 There hasbeen considerable improvement in survival since the early 1980swhen the in-hospital mortality was 40ndash5097 compared with15 from a recent UK audit5 Such is the improvement in out-comes that a patient with Childrsquos A cirrhosis is very unlikely tosuccumb to an index variceal bleed Studies have shown theChildndashPugh score MELD score and HVPG to be strong predic-tors of outcomes98ndash103 The MELD score has been shown tooutperform Childrsquos score in a recent study with a score gt19associated with 20 6 week mortality103 Furthermore theMELD score has been shown to perform as well as the trad-itional intensive care unit scores in predicting mortality inpatients admitted to intensive care in the UK104 MELD gt18active bleeding transfusing gt4 units of packed red blood cellshave been shown to be predictors of mortality and earlyrebleeding99 101 102 HVPG has also been shown to predictoutcome when measured at 2 weeks after a bleed44 and a valueof ge20 mm Hg when measured acutely within 48 h has beenshown to provide significant prognostic information100
However this technique is not used routinely in the manage-ment of patients around the world and substitution of clinicaldata in the latter study was shown to provide the same clinicalpredictive value100 These scoring systems are not purely aca-demic they allow the referring clinician to predict thosepatients with a high chance of rebleeding to be transferred to aspecialist centre offering for instance TIPSS before the patientrebleeds
Nonetheless probably the most important step in the man-agement of acute variceal haemorrhage is the initial resuscitationassessed according to standard lsquoABCrsquo practice together withprotection of the airway to prevent aspiration Although earlyendoscopy allows for accurate diagnosis of the bleeding site anddecisions about management (figure 3) therapeutic interventionin acute variceal bleeding can be initiated safely in most casesbefore diagnostic endoscopy As similar efficacy is demonstratedwith pharmacological treatment as with sclerotherapy theformer should be first-line therapy99 β Blockade should not bestarted in the acute setting and those already taking β blockersas prophylaxis should probably stop taking them for 48ndash72 h inorder that the patientrsquos physiological response to blood loss canbe allowed to manifest
General considerationsPatient evaluationThe majority of patients with a variceal bleed will be sufficientlystable to enable a full history and examination to take placeHistory of alcohol excess and or intravenous drug use should besought and may become particularly relevant if the patient haswithdrawal symptoms after admission Comorbidity is importantwhen estimating risk and deciding on use of vasopressors The
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 11
Guidelines
following risk factors doubled mortality after an acute varicealbleed in one US study older age comorbidities male gender andnot undergoing a gastroscopy within 24 h105
A full examination is helpful for the important negatives asmuch as the positives Baseline observations should include thetemperature as infection is a serious complication with signifi-cant mortality Confusion may be present because of encephal-opathy intoxication with alcohol or drugs or withdrawal fromalcohol or drugs The patient should be on continuous BP andpulse monitor and their haemodynamic status recordedAn oxygen saturation monitor is helpful Stigmata of chronicliver disease and concurrent jaundice provide insight into thecurrent status of a patientrsquos liver and also give warning ofpotential further decompensation if significant bleeding persists(see scoring systems above) Pneumonia must be actively
excluded Evidence of ascites requires a diagnostic tap to searchfor infection
Investigations including full blood count coagulationprofile liver and renal function and blood group and save andcross-match Blood and urine should also be cultured An ultra-sound scan later in the admission is helpful to identify subclin-ical ascites flow in portal vein and any obvious emergence of anhepatocellular carcinoma (HCC)
Location of patientA decision must be made as to where the patient is best managedVariceal bleeding is unpredictable generally occurs in patientswith significant liver disease and is associated with significant mor-tality Hence a high-dependency unit is usually the most appropri-ate initial location although a properly staffed lsquogastrointestinal
Figure 3 Algorithm for themanagement of acute varicealbleeding TIPSS transjugularintrahepatic portosystemic stent shunt
12 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleeding bedrsquo may be appropriate If a patient is vomiting bloodor there is a perceived risk of a haemodynamically unstable patienthaving blood in the stomach then the patient must be intubatedbefore endoscopy and return to an intensive care or high-dependency unit will be necessary until extubation
Volume resuscitation and blood productsIntravenous access (two 16ndash18G cannulae) should have beensecured on admission with a reported GI bleed Further intra-venous access may be necessary In patients with poor venousaccess advanced liver disease or renal failure associated withtheir liver disease central venous access may be helpful withguiding fluid infusions However the drawbacks include the riskof the procedure and a potential source of infection Thereforethere is no absolute requirement for a central line and no evi-dence of unequivocal benefit Intravenous fluid resuscitationshould be initiated with plasma expanders aiming to maintain asystolic blood pressure of 100 mm Hg Care with monitoring isparamount in this group of patients
Overtransfusion has been shown to have a deleterious effecton outcome In a recent single-centre RCT a restrictive transfu-sion policy of maintaining haemoglobin between 70 and 80 gLimproved the control of variceal bleeding (11 vs 22p=005) and lowered HVPG compared with a liberal transfu-sion policy without effect on 45-day survival106 However itshould be noted that these results were from a single Spanishcentre which was a tertiary unit for variceal bleeding where allpatients underwent endoscopy within 6 h Nonetheless arestrictive transfusion policy has been recommended for sometime1 and there is now good evidence to support not transfusinga stable patient with a haemoglobin of ge80 gL However under-resuscitation should also be avoided and while goal-orientedfluid replacement has generally not been useful in an intensivetherapy unit setting a venous saturation gt70 remains an easilymeasurable target with some evidence to support it107
Interpretation and management of clotting profile is challen-ging in liver disease where there is usually a balanced deficiencyof both procoagulant and anticoagulant factors108 The NICEguidelines recommend activation of a hospitalrsquos massive transfu-sion policy when there is major haemorrhage and plateletsupport when the value is lt50 and clotting factor supportwhen the international normalised ratio (INR) is gt15 timesnormal2 There is no evidence for the use of lsquoprophylacticrsquo clot-ting or platelet support to reduce the risk of rebleeding Thereis insufficient evidence to support the routine use of transexamicacid or recombinant factor VIIa109
Pharmacological treatmentThe two major classes of drugs that have been used in thecontrol of acute variceal bleeding are vasopressin or its analo-gues (either alone or in combination with nitroglycerine) andsomatostatin or its analogues Terlipressin is the only agent thathas been shown to reduce mortality in placebo-controlled trialsHowever in trials comparing terlipressin somatostatin andoctreotide no difference in efficacy was identified in a system-atic review110 and in a recent large RCT111 Prophylactic anti-biotics can result in a similar survival benefit following acutevariceal bleeding
VasopressinVasopressin reduces portal blood flow portal systemic collateralblood flow and variceal pressure It does however have signifi-cant systemic side effects such as an increase in peripheral resist-ance and reduction in cardiac output heart rate and coronary
blood flow In comparison with no active treatment the pooledresults of four randomised trials showed that it reduced failureto control variceal bleeding (OR=022 95 CI 012 to 043)although survival was unaffected68 Meta-analysis of five trialscomparing sclerotherapy with vasopressin has shown a signifi-cant effect on reduction in failure to control bleeding(OR=051 95 CI 027 to 097) with no effect on survival68
Vasopressin with nitroglycerineThe addition of nitroglycerine enhances the effect of vasopres-sin on portal pressure and reduces cardiovascular side effects112
Meta-analysis of three randomised trials comparing vasopressinalone with vasopressin and nitroglycerine showed that the com-bination was associated with a significant reduction in failure tocontrol bleeding (OR=039 95 CI 022 to 072) although nosurvival benefit was shown68
TerlipressinTerlipressin is a synthetic analogue of vasopressin which has animmediate systemic vasoconstrictor action followed by portalhaemodynamic effects due to slow conversion to vasopressin Ina Cochrane meta-analysis of seven placebo-controlled trials ter-lipressin was shown to reduce failure to control bleeding(RR=066 95 CI 055 to 093) and also to improve survival(RR=066 95 CI 049 to 088)113 In the same meta-analysisthere was no difference between terlipressin versus vasopressinballoon tamponade or endoscopic therapy in failure to controlbleeding or survival113 The role of terlipressin in combinationwith VBL is explored in the section lsquoEndoscopic therapy incombination with pharmacological therapyrsquo
The recommended dose of terlipressin is 2 mg IV every 4 halthough many units reduce the dose to 6 hourly as it may causeperipheral vasoconstriction which manifests as painful handsand feet While 5 days of IV treatment has been advocated inthe Baveno V guidelines1 this prolonged treatment has notbeen shown to have a survival benefit and for pragmaticreasons many units will stop treatment shortly after satisfactoryhaemostasis In a randomised trial terlipressin given for 24 hafter satisfactory haemostasis with VBL after oesophageal vari-ceal bleeding was as effective as 72 h of treatment114
In patients intolerant of terlipressin or in countries where ter-lipressin is not available alternatives should be considered
Somatostatin and octreotideSomatostatin causes selective splanchnic vasoconstriction andreduces portal pressure and portal blood flow115 Octreotide is asomatostatin analogue The mechanism of action of these twoagents is not clear Inhibition of glucagon increases vasodilatationrather than a direct vasoconstrictive effect and post-prandial guthyperaemia is also reduced The actions of octreotide on hepaticand systemic hemodynamics are transient making continuousinfusion necessary Octreotide is given as a 50 μg bolus followedby an infusion of 25ndash50 μgh Somatostatin is given as a 250 mgintravenous bolus followed by an infusion of 250 mghSomatostatin and octreotide have been shown to be aseffective as terlipressin in acute variceal bleeding in ameta-analysis110 Seo et al111 in a large RCTof 780 patients com-paring these three agents failed to show a difference in treatmentsuccess (range 838ndash862) rebleeding (range 34ndash44) andmortality (range 8ndash88) A low systolic blood pressure at pres-entation high serum creatinine level active bleeding in the emer-gency endoscopy gastric variceal bleeding and ChildndashPugh gradeC were independent factors predicting 5-day treatmentfailure111
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 13
Guidelines
AntibioticsAntibiotics that provide Gram-negative cover are one of the inter-ventions which positively influence survival in variceal haemor-rhage as shown in a Cochrane meta-analysis of 12placebo-controlled trials (RR=079 95 CI 063 to 098)116
Antibiotics were also shown to reduce bacterial infections(RR=043 95 CI 019 to 097) and early rebleeding (RR=05395 CI 038 to 074)116 Therefore short-term antibiotics shouldbe considered standard practice in all cirrhotic patients who have avariceal bleed irrespective of the presence of confirmed infectionThird-generation cephalosporins such as ceftriaxone (1 g IVdaily) have been shown to be more effective at reducingGram-negative sepsis than oral norfloxacin117 but choice of anti-biotics must be dictated by local resistance patterns and availability
Proton pump inhibitorsOne RCT compared a short course of proton pump inhibitorswith vasoconstrictor therapies after haemostasis in acute varicealbleeding118 Despite larger ulcers noted in the vasoconstrictorarm there were no differences in bleeding or survival Nearly50 of patients had ascites which might have implications inlight of the reports of increased incidence of spontaneous bac-terial peritonitis as mentioned earlier
Endoscopic therapyEndoscopy should take place within 24 h of admission andearlier if there is excessive bleeding based on low-level evi-dence105 While many guidelines and reviews suggest thatendoscopy should be carried out within 12 h the only study thatexamined the influence of timing on outcome failed to demon-strate any advantage of endoscopy before 12 h119 The optimaltime is after sufficient resuscitation and pharmacological treat-ment with the endoscopy performed by a skilled endoscopyteam in a suitably equipped theatre environment and withairway protection Airway protection is essential where risk ofaspiration is high and affords the endoscopist time for thoroughevaluation including complete clot aspiration and controlledapplication of treatment including tamponade if required Theendoscopy team must comprise an experienced endoscopynurse acquainted with the equipment necessary for endoscopytherapy of varices and a skilled endoscopist competent in usingbanding devices and deployment of balloon tamponade
Variceal band ligationThis technique is a modification of that used for the elastic bandligation of internal haemorrhoids Its use in humans was firstdescribed in 1988120 A meta-analysis of seven trials comparingVBL with sclerotherapy in acute bleeding showed that VBLreduced rebleeding from varices (OR=047 95 CI 029 to078) reduced mortality (OR=067 95 CI 046 to 098) andresulted in fewer oesophageal strictures (OR=010 95 CI003 to 029)121 The number of sessions required to obliteratevarices was lower with VBL (22 fewer sessions (95 CI 09to 35))
SclerotherapySclerotherapy has been replaced by VBL and should no longerbe offered as standard of care in acute variceal haemorrhage
Other endoscopic measuresIn an RCT cyanoacrylate offered no benefit over VBL with theadditional risk of embolisation and trend towards increasedrebleeding with cyanoacrylate122
Haemostatic powder (TC-325 Hemospray Cook MedicalUSA) has been described in a small study of nine patients whoreceived endoscopic spray treatment for acute variceal bleedingThe study reported no rebleeding within 24 h and no mortalityat 15 days123
Endoscopic therapy in combination with pharmacological therapyThe role of combining vasoactive drugs with endoscopictherapy (VBL or sclerotherapy) was reported in a meta-analysisof eight trials124 Combination therapy resulted in better initialcontrol of bleeding (RR=112 95 CI 102 to 123) and5-day haemostasis (RR=128 95 CI 118 to 139) withoutany difference in survival Adverse events were similar in bothgroups Two RCTs have compared VBL with sclerotherapy incombination with vasoactive agents in acute variceal bleed-ing125 126 Lo et al125 used vasopressin and found that VBLresulted in better 72 h haemostasis (97 vs 76 p=0009)with fewer complications (5 vs 29 p=0007) Villanuevaet al used somatostatin and reported lower failure to controlacute bleeding with VBL (4 vs 15 p=002) with fewerserious complications (4 vs 13 p=004) Overall survivalwas similar in both trials125 126
Balloon tamponadeBalloon tamponade is highly effective and controls acute bleed-ing in up to 90 of patients although about 50 rebleed whenthe balloon is deflated127 128 It is however associated withserious complications such as oesophageal ulceration and aspir-ation pneumonia in up to 15ndash20 of patients Despite this itmay be a life-saving treatment in cases of massive uncontrolledvariceal haemorrhage pending other forms of treatment Anappropriately placed SengstakenndashBlakemore tube allows forresuscitation safe transportation and either repeat endoscopy orradiological shunting in a patient with a stable cardiovascularsystem The oesophageal balloon is rarely required must neverbe used on its own and should be used only if there is continu-ing bleeding despite an adequately inflated gastric balloon cor-rectly placed and with appropriate tension Placement of thetube endoscopically or over a guide wire might reduce the riskof complications especially oesophageal rupture
Removable oesophageal stentsThe SX-Ella Danis stent (ELLA-CS Hradec Kralove CzechRepublic) is a removable covered metal mesh stent placed endo-scopically in the lower oesophagus without radiological screen-ing It has no role in the management of gastric varicealbleeding These stents can be left in situ for up to 2 weeksunlike the SengstakenndashBlakemore tube which should beremoved after a maximum of 24ndash48 h129 130 No published con-trolled trials have compared this modality with balloontamponade
Transjugular intrahepatic portosystemic stent-shuntSeveral uncontrolled studies have examined the role of salvagebare TIPSS in acute variceal bleeding In a review of 15 studiescontrol of bleeding was achieved in 90ndash100 with rebleedingin 6ndash16131 Mortality varied between 75 (in hospital) and15 (30 day) It is important to appreciate that sclerotherapywas used as first-line endoscopic therapy in most of thesestudies Long-term follow-up of a study that compared TIPSSwith H-graft portacaval shunts in patients for whom non-operative management had failed suggested that H-grafts were auseful method of reducing portal pressure and had a signifi-cantly lower failure rate (p=004) but had no significant
14 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
improvement in overall survival despite a benefit seen in ChildrsquosA and B disease132 A recent RCT compared emergency porto-caval surgery with bare TIPSS within 24 h of presenting withacute oesophageal variceal bleeding in unselected cirrhoticpatients Emergency portocaval surgery resulted in better out-comes for long-term bleeding control encephalopathy and sur-vival (plt0001)133 Before wider application of surgery foracute variceal bleeding more data are needed in light of therecent adoption of covered stents
There has also been a generalised established change in prac-tice in using covered TIPSS stents (polytetrafluoroethylene(PTFE)) rather than a bare metal stent with evidence to supportthis change In randomised controlled studies these stents wereshown to have higher primary patency rates than bare stentswithout significant differences in survival and the potential forreduced incidence of hepatic encephalopathy134 135
There is however growing evidence from two RCTs for theearlier use of TIPSS in selected patients stratified by HVPGChildndashPugh class and active bleeding and not just use as asalvage option6 136 Monescillo et al136 randomised patientspresenting with acute oesophageal variceal haemorrhage to bareTIPSS or standard of care if the HVPG was ge20 mm Hg within24 h of admission Significantly reduced treatment failure asdefined by failure to control acute bleeding andor early rebleed-ing (12 vs 50) was seen and improved survival (62 vs35) in the patients randomised to undergo a TIPSS procedureHowever the standard of care was sclerotherapy and not com-bination endoscopic and pharmacological treatment This limita-tion and the lack of availability of HVPG measurement in mostcentres meant this trial did not have a significant impact on clin-ical practice
Garcia-Pagan et al6 selected patients with active bleeding andChildrsquos B cirrhosis or patients with Childrsquos C cirrhosis (Childrsquosscore lt14) for randomisation to early PTFE-covered TIPSSwithin 72 h or standard of care with VBL and pharmacologicaltreatment This has shown encouraging results with reduced riskof treatment failure (3 vs 50) improved survival (86 vs61 at 1 year) yet without increased risk of hepatic encephal-opathy The results were supported by an observational studyfrom the same group although a survival benefit was notseen137 Furthermore a recent well-conducted observationalstudy did not demonstrate such high survival rates with earlyTIPSS with 11-year survival of 67 which was similar to thatof patients given endoscopic and pharmacological treatmentsonly138 Therefore larger multicentred RCTs need to be under-taken to further evaluate the role of early TIPSS It is importantto make the distinction between salvage TIPSS and early TIPSSto prevent rebleeding
Liver transplantationThis is probably appropriate only for patients who bleed whileawaiting liver transplantation although studies comparing VBLor TIPSS placement with urgent liver transplantation in thissituation need to be done Liver transplantation is an exceed-ingly rare option for the vast majority of patients both becauseit is not commonly available and because of shortages anddelays in organ procurement No controlled trials of liver trans-plantation in uncontrolledactive bleeding are available
Recommendations for the control of variceal bleeding in cir-rhosis are given below and in figure 3
Recommendations control of active variceal haemorrhage incirrhosis (figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with bloodplatelets and clotting factors in line with local protocolsfor managing massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusionpolicy aiming for a haemoglobin of 70ndash80 gL is sug-gested in haemodynamically stable patients (level 1bgrade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable(level 5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L(level 5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to localcircumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with suspected
or confirmed variceal bleeding (level 1a grade A)32 In all patients vasoconstrictors such as terlipressin or
somatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 15
Guidelines
41 If bleeding is difficult to control a SengstakenndashBlakemore tube should be inserted until further endo-scopic treatment TIPSS or surgery is performed depend-ing on local resources and expertise (level 1b grade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure (level1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
SECONDARY PROPHYLAXIS OF VARICEAL HAEMORRHAGEβ BlockersA meta-analysis of 12 trials comparing propranolol or nadolol139
with no active treatment showed a significant reduction inrebleeding but no significant reduction in mortality140 Thegreater reduction in portal pressure with carvedilol comparedwith propranolol has been described in the section lsquoPrimaryprophylaxisrsquo of this guideline
NitratesThe addition of ISMN to NSBB has been shown to reduce vari-ceal rebleeding compared with NSBB alone although no sur-vival benefit was seen141 In addition adverse events leading todrug withdrawal were more common in the group receivingcombined drug treatment A meta-analysis of ISMN alone orwith either NSBB or endoscopic therapy reported that there wasno mortality benefit from combining nitrates and NSBB com-pared with NSBB alone142
Side effects of ISMN include dizziness and headache Owingto the side effects and relative lack of data ISMN is not com-monly used in clinical practice
A recent RCT of 121 patients reported carvedilol to besimilar to combined ISMN and NSBB therapy in the preventionof variceal rebleeding and mortality although severe adverseevents were less common with carvedilol143
SimvastatinA recent abstract of a multicentre RCT of 158 patients reporteda survival benefit (91 vs 78 p=003) from adding simvasta-tin to VBL and NSBB compared with placebo VBL and NSBBas treatment for the prevention of variceal rebleeding144 Therewas no difference in rebleeding and the survival benefit wasrestricted to Child A and B patients Serious adverse events weresimilar in both groups More data are required to investigatethis interesting observation of a survival benefit from simvastatinin this situation which may relate to its effects on hepatocellularfunction fibrosis and portal pressure
Proton pump inhibitorsA double-blind randomised placebo-controlled trial showed thatpantoprazole reduced the size of ulcers in patients who under-went VBL However the total number of ulcers and other out-comes were similar in the two groups145
Endoscopic therapyVBL has been accepted as the preferred endoscopic treatmentfor the prevention of variceal rebleeding with a lower rate ofrebleeding mortality and complications than sclerother-apy146 147 The time interval between VBL sessions to achieveeradication of varices is debateable However a recent RCTcomparing monthly with biweekly VBL after initial haemostasiswith VBL in 70 patients suggested that there were fewerpost-VBL ulcers in the monthly group (11 vs 57plt0001)148 Variceal recurrence rebleeding and mortality weresimilar in both groups
Two meta-analyses showed there is no evidence that the add-ition of sclerotherapy to VBL improves clinically relevant out-comes including variceal rebleeding and death and thecombination led to higher stricture rates149 150
Endoscopic therapy versus drug therapyVBL has been reported to be more effective than combinedNSBB and ISMN drug therapy151 However an 8-yearfollow-up study of this RCT found that although VBL wassuperior in reducing variceal rebleeding survival rates were sig-nificantly higher in the group treated with combined drug treat-ment152 Other studies have found no superiority of VBL overcombined drug therapy for prevention of variceal rebleeding ormortality153 154 A recent small multicentre RCT reported carve-dilol to be similar to VBL in the prevention of variceal rebleed-ing with a trend in favour of survival with carvedilol (73 vs48 p=0110)155
Several meta-analyses have compared drug therapy with VBLin the prevention of variceal rebleeding One meta-analysis ofsix RCTs showed no significant difference in variceal rebleedingrates when comparing VBL alone with combined NSBB andISMN therapy However all-cause mortality was significantlyhigher in patients treated with the VBL (RR=125 95 CI101 to 155)156 Three meta-analyses comparing drug therapy(NSBB alone or with ISMN) with endoscopic therapy alonereported no difference in variceal rebleeding or mortality157ndash159
Endoscopic+drug therapy versus either aloneNumerous studies and several meta-analyses have comparedcombined endoscopic and drug therapy with monotherapy(endoscopic or drugs alone) in the prevention of varicealrebleeding A meta-analysis of 23 trials assessing sclerotherapyor VBL combined with NSBB reported that combinationtherapy reduced rebleeding more than either endoscopic
16 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

50ndash55 bpm is reached to a maximum dose of320 mg (level 1a grade A)
132 Nadolol 40 mg daily dose Dose titrated tomaximum tolerated or once HR of 50ndash55 bpm isreached a maximum dose of 240 mg (level 1agrade A)
133 Carvedilol 625 mg once daily to increase tomaintenance of 125 mg after a week if toleratedor once HR of lt50ndash55 bpm is reached (level 1agrade A)
134 It is suggested that NSBB are discontinued at thetime of spontaneous bacterial peritonitis renalimpairment and hypotension (level 2b grade B)
14 In cases of contraindications or intolerance to NSBB werecommend variceal band ligation (level 1a grade A)
2 Who should have surveillance for variceal bleeding21 We recommend all patients with cirrhosis should be
endoscoped at the time of diagnosis (level 1a grade A)There is no indication to repeat endoscopy in patientsreceiving NSBB
3 How often should cirrhotic patients be endoscoped31 If at the time of first endoscopy no varices are seen we
suggest that patients with cirrhosis should be endos-coped at 2ndash3-year intervals (level 2a grade B)
32 If grade I varices are diagnosed we suggest that patientsshould be endoscoped at yearly intervals (level 2agrade B)
33 If there is clear evidence of disease progression wesuggest that the intervals can be modified by a clinicianEndoscopy should also be offered at time of decompen-sation (level 2a grade B)
4 Which patients with cirrhosis should have primaryprophylaxis41 If grade I varices and red signs or grade 2ndash3 varices are
diagnosed we recommend that patients have primaryprophylaxis irrespective of the severity of the liverdisease (level 1a grade A)
5 Treatments not recommended51 Proton pump inhibitors are not recommended unless
otherwise required for peptic ulcer disease (level 1bgrade B)
52 Isosorbide mononitrate monotherapy is not recommendedas primary prophylaxis (level 1b grade A) There is insuffi-cient evidence to recommend isosorbide mononitrate incombination with NSBB (level 1b grade A)
53 Shunt surgery or TIPSS is not recommended as primaryprophylaxis (level 1a grade A)
54 Sclerotherapy is not recommended as primary prophy-laxis (level 1a grade A)
6 Areas requiring further study61 Role of NSBB in patients without varices with focus on
carvedilol62 Role of NSBB in patients with small varices with focus
on carvedilol63 Comparison of carvedilol versus propranolol in primary
prophylaxis64 Identification of and trials assessing new drugs for
primary prophylaxis such as statins7 Quality indicator
71 Percentage of patients at diagnosis of cirrhosis who havehad an endoscopy to screen for varices (level 1agrade A)Numerator patients diagnosed with cirrhosis who havehad an endoscopy either before or after diagnosis within
6 monthsDenominator patients newly diagnosed with cirrhosis
72 Percentage of patients receiving primary prophylaxisamong those newly diagnosed with grade I varices andred signs or grade 2ndash3 varicesNumerator patients who have grade 1 varices with redsigns or grade 2ndash3 varices receiving primary prophy-laxisDenominator patients diagnosed with cirrhosis whohave grade I varices with red signs or grade 2ndash3 varices
MANAGEMENT OF ACTIVE VARICEAL HAEMORRHAGEThe average 6-week mortality of the first episode of varicealbleeding in most studies is reported to be up to 20 There hasbeen considerable improvement in survival since the early 1980swhen the in-hospital mortality was 40ndash5097 compared with15 from a recent UK audit5 Such is the improvement in out-comes that a patient with Childrsquos A cirrhosis is very unlikely tosuccumb to an index variceal bleed Studies have shown theChildndashPugh score MELD score and HVPG to be strong predic-tors of outcomes98ndash103 The MELD score has been shown tooutperform Childrsquos score in a recent study with a score gt19associated with 20 6 week mortality103 Furthermore theMELD score has been shown to perform as well as the trad-itional intensive care unit scores in predicting mortality inpatients admitted to intensive care in the UK104 MELD gt18active bleeding transfusing gt4 units of packed red blood cellshave been shown to be predictors of mortality and earlyrebleeding99 101 102 HVPG has also been shown to predictoutcome when measured at 2 weeks after a bleed44 and a valueof ge20 mm Hg when measured acutely within 48 h has beenshown to provide significant prognostic information100
However this technique is not used routinely in the manage-ment of patients around the world and substitution of clinicaldata in the latter study was shown to provide the same clinicalpredictive value100 These scoring systems are not purely aca-demic they allow the referring clinician to predict thosepatients with a high chance of rebleeding to be transferred to aspecialist centre offering for instance TIPSS before the patientrebleeds
Nonetheless probably the most important step in the man-agement of acute variceal haemorrhage is the initial resuscitationassessed according to standard lsquoABCrsquo practice together withprotection of the airway to prevent aspiration Although earlyendoscopy allows for accurate diagnosis of the bleeding site anddecisions about management (figure 3) therapeutic interventionin acute variceal bleeding can be initiated safely in most casesbefore diagnostic endoscopy As similar efficacy is demonstratedwith pharmacological treatment as with sclerotherapy theformer should be first-line therapy99 β Blockade should not bestarted in the acute setting and those already taking β blockersas prophylaxis should probably stop taking them for 48ndash72 h inorder that the patientrsquos physiological response to blood loss canbe allowed to manifest
General considerationsPatient evaluationThe majority of patients with a variceal bleed will be sufficientlystable to enable a full history and examination to take placeHistory of alcohol excess and or intravenous drug use should besought and may become particularly relevant if the patient haswithdrawal symptoms after admission Comorbidity is importantwhen estimating risk and deciding on use of vasopressors The
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 11
Guidelines
following risk factors doubled mortality after an acute varicealbleed in one US study older age comorbidities male gender andnot undergoing a gastroscopy within 24 h105
A full examination is helpful for the important negatives asmuch as the positives Baseline observations should include thetemperature as infection is a serious complication with signifi-cant mortality Confusion may be present because of encephal-opathy intoxication with alcohol or drugs or withdrawal fromalcohol or drugs The patient should be on continuous BP andpulse monitor and their haemodynamic status recordedAn oxygen saturation monitor is helpful Stigmata of chronicliver disease and concurrent jaundice provide insight into thecurrent status of a patientrsquos liver and also give warning ofpotential further decompensation if significant bleeding persists(see scoring systems above) Pneumonia must be actively
excluded Evidence of ascites requires a diagnostic tap to searchfor infection
Investigations including full blood count coagulationprofile liver and renal function and blood group and save andcross-match Blood and urine should also be cultured An ultra-sound scan later in the admission is helpful to identify subclin-ical ascites flow in portal vein and any obvious emergence of anhepatocellular carcinoma (HCC)
Location of patientA decision must be made as to where the patient is best managedVariceal bleeding is unpredictable generally occurs in patientswith significant liver disease and is associated with significant mor-tality Hence a high-dependency unit is usually the most appropri-ate initial location although a properly staffed lsquogastrointestinal
Figure 3 Algorithm for themanagement of acute varicealbleeding TIPSS transjugularintrahepatic portosystemic stent shunt
12 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleeding bedrsquo may be appropriate If a patient is vomiting bloodor there is a perceived risk of a haemodynamically unstable patienthaving blood in the stomach then the patient must be intubatedbefore endoscopy and return to an intensive care or high-dependency unit will be necessary until extubation
Volume resuscitation and blood productsIntravenous access (two 16ndash18G cannulae) should have beensecured on admission with a reported GI bleed Further intra-venous access may be necessary In patients with poor venousaccess advanced liver disease or renal failure associated withtheir liver disease central venous access may be helpful withguiding fluid infusions However the drawbacks include the riskof the procedure and a potential source of infection Thereforethere is no absolute requirement for a central line and no evi-dence of unequivocal benefit Intravenous fluid resuscitationshould be initiated with plasma expanders aiming to maintain asystolic blood pressure of 100 mm Hg Care with monitoring isparamount in this group of patients
Overtransfusion has been shown to have a deleterious effecton outcome In a recent single-centre RCT a restrictive transfu-sion policy of maintaining haemoglobin between 70 and 80 gLimproved the control of variceal bleeding (11 vs 22p=005) and lowered HVPG compared with a liberal transfu-sion policy without effect on 45-day survival106 However itshould be noted that these results were from a single Spanishcentre which was a tertiary unit for variceal bleeding where allpatients underwent endoscopy within 6 h Nonetheless arestrictive transfusion policy has been recommended for sometime1 and there is now good evidence to support not transfusinga stable patient with a haemoglobin of ge80 gL However under-resuscitation should also be avoided and while goal-orientedfluid replacement has generally not been useful in an intensivetherapy unit setting a venous saturation gt70 remains an easilymeasurable target with some evidence to support it107
Interpretation and management of clotting profile is challen-ging in liver disease where there is usually a balanced deficiencyof both procoagulant and anticoagulant factors108 The NICEguidelines recommend activation of a hospitalrsquos massive transfu-sion policy when there is major haemorrhage and plateletsupport when the value is lt50 and clotting factor supportwhen the international normalised ratio (INR) is gt15 timesnormal2 There is no evidence for the use of lsquoprophylacticrsquo clot-ting or platelet support to reduce the risk of rebleeding Thereis insufficient evidence to support the routine use of transexamicacid or recombinant factor VIIa109
Pharmacological treatmentThe two major classes of drugs that have been used in thecontrol of acute variceal bleeding are vasopressin or its analo-gues (either alone or in combination with nitroglycerine) andsomatostatin or its analogues Terlipressin is the only agent thathas been shown to reduce mortality in placebo-controlled trialsHowever in trials comparing terlipressin somatostatin andoctreotide no difference in efficacy was identified in a system-atic review110 and in a recent large RCT111 Prophylactic anti-biotics can result in a similar survival benefit following acutevariceal bleeding
VasopressinVasopressin reduces portal blood flow portal systemic collateralblood flow and variceal pressure It does however have signifi-cant systemic side effects such as an increase in peripheral resist-ance and reduction in cardiac output heart rate and coronary
blood flow In comparison with no active treatment the pooledresults of four randomised trials showed that it reduced failureto control variceal bleeding (OR=022 95 CI 012 to 043)although survival was unaffected68 Meta-analysis of five trialscomparing sclerotherapy with vasopressin has shown a signifi-cant effect on reduction in failure to control bleeding(OR=051 95 CI 027 to 097) with no effect on survival68
Vasopressin with nitroglycerineThe addition of nitroglycerine enhances the effect of vasopres-sin on portal pressure and reduces cardiovascular side effects112
Meta-analysis of three randomised trials comparing vasopressinalone with vasopressin and nitroglycerine showed that the com-bination was associated with a significant reduction in failure tocontrol bleeding (OR=039 95 CI 022 to 072) although nosurvival benefit was shown68
TerlipressinTerlipressin is a synthetic analogue of vasopressin which has animmediate systemic vasoconstrictor action followed by portalhaemodynamic effects due to slow conversion to vasopressin Ina Cochrane meta-analysis of seven placebo-controlled trials ter-lipressin was shown to reduce failure to control bleeding(RR=066 95 CI 055 to 093) and also to improve survival(RR=066 95 CI 049 to 088)113 In the same meta-analysisthere was no difference between terlipressin versus vasopressinballoon tamponade or endoscopic therapy in failure to controlbleeding or survival113 The role of terlipressin in combinationwith VBL is explored in the section lsquoEndoscopic therapy incombination with pharmacological therapyrsquo
The recommended dose of terlipressin is 2 mg IV every 4 halthough many units reduce the dose to 6 hourly as it may causeperipheral vasoconstriction which manifests as painful handsand feet While 5 days of IV treatment has been advocated inthe Baveno V guidelines1 this prolonged treatment has notbeen shown to have a survival benefit and for pragmaticreasons many units will stop treatment shortly after satisfactoryhaemostasis In a randomised trial terlipressin given for 24 hafter satisfactory haemostasis with VBL after oesophageal vari-ceal bleeding was as effective as 72 h of treatment114
In patients intolerant of terlipressin or in countries where ter-lipressin is not available alternatives should be considered
Somatostatin and octreotideSomatostatin causes selective splanchnic vasoconstriction andreduces portal pressure and portal blood flow115 Octreotide is asomatostatin analogue The mechanism of action of these twoagents is not clear Inhibition of glucagon increases vasodilatationrather than a direct vasoconstrictive effect and post-prandial guthyperaemia is also reduced The actions of octreotide on hepaticand systemic hemodynamics are transient making continuousinfusion necessary Octreotide is given as a 50 μg bolus followedby an infusion of 25ndash50 μgh Somatostatin is given as a 250 mgintravenous bolus followed by an infusion of 250 mghSomatostatin and octreotide have been shown to be aseffective as terlipressin in acute variceal bleeding in ameta-analysis110 Seo et al111 in a large RCTof 780 patients com-paring these three agents failed to show a difference in treatmentsuccess (range 838ndash862) rebleeding (range 34ndash44) andmortality (range 8ndash88) A low systolic blood pressure at pres-entation high serum creatinine level active bleeding in the emer-gency endoscopy gastric variceal bleeding and ChildndashPugh gradeC were independent factors predicting 5-day treatmentfailure111
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 13
Guidelines
AntibioticsAntibiotics that provide Gram-negative cover are one of the inter-ventions which positively influence survival in variceal haemor-rhage as shown in a Cochrane meta-analysis of 12placebo-controlled trials (RR=079 95 CI 063 to 098)116
Antibiotics were also shown to reduce bacterial infections(RR=043 95 CI 019 to 097) and early rebleeding (RR=05395 CI 038 to 074)116 Therefore short-term antibiotics shouldbe considered standard practice in all cirrhotic patients who have avariceal bleed irrespective of the presence of confirmed infectionThird-generation cephalosporins such as ceftriaxone (1 g IVdaily) have been shown to be more effective at reducingGram-negative sepsis than oral norfloxacin117 but choice of anti-biotics must be dictated by local resistance patterns and availability
Proton pump inhibitorsOne RCT compared a short course of proton pump inhibitorswith vasoconstrictor therapies after haemostasis in acute varicealbleeding118 Despite larger ulcers noted in the vasoconstrictorarm there were no differences in bleeding or survival Nearly50 of patients had ascites which might have implications inlight of the reports of increased incidence of spontaneous bac-terial peritonitis as mentioned earlier
Endoscopic therapyEndoscopy should take place within 24 h of admission andearlier if there is excessive bleeding based on low-level evi-dence105 While many guidelines and reviews suggest thatendoscopy should be carried out within 12 h the only study thatexamined the influence of timing on outcome failed to demon-strate any advantage of endoscopy before 12 h119 The optimaltime is after sufficient resuscitation and pharmacological treat-ment with the endoscopy performed by a skilled endoscopyteam in a suitably equipped theatre environment and withairway protection Airway protection is essential where risk ofaspiration is high and affords the endoscopist time for thoroughevaluation including complete clot aspiration and controlledapplication of treatment including tamponade if required Theendoscopy team must comprise an experienced endoscopynurse acquainted with the equipment necessary for endoscopytherapy of varices and a skilled endoscopist competent in usingbanding devices and deployment of balloon tamponade
Variceal band ligationThis technique is a modification of that used for the elastic bandligation of internal haemorrhoids Its use in humans was firstdescribed in 1988120 A meta-analysis of seven trials comparingVBL with sclerotherapy in acute bleeding showed that VBLreduced rebleeding from varices (OR=047 95 CI 029 to078) reduced mortality (OR=067 95 CI 046 to 098) andresulted in fewer oesophageal strictures (OR=010 95 CI003 to 029)121 The number of sessions required to obliteratevarices was lower with VBL (22 fewer sessions (95 CI 09to 35))
SclerotherapySclerotherapy has been replaced by VBL and should no longerbe offered as standard of care in acute variceal haemorrhage
Other endoscopic measuresIn an RCT cyanoacrylate offered no benefit over VBL with theadditional risk of embolisation and trend towards increasedrebleeding with cyanoacrylate122
Haemostatic powder (TC-325 Hemospray Cook MedicalUSA) has been described in a small study of nine patients whoreceived endoscopic spray treatment for acute variceal bleedingThe study reported no rebleeding within 24 h and no mortalityat 15 days123
Endoscopic therapy in combination with pharmacological therapyThe role of combining vasoactive drugs with endoscopictherapy (VBL or sclerotherapy) was reported in a meta-analysisof eight trials124 Combination therapy resulted in better initialcontrol of bleeding (RR=112 95 CI 102 to 123) and5-day haemostasis (RR=128 95 CI 118 to 139) withoutany difference in survival Adverse events were similar in bothgroups Two RCTs have compared VBL with sclerotherapy incombination with vasoactive agents in acute variceal bleed-ing125 126 Lo et al125 used vasopressin and found that VBLresulted in better 72 h haemostasis (97 vs 76 p=0009)with fewer complications (5 vs 29 p=0007) Villanuevaet al used somatostatin and reported lower failure to controlacute bleeding with VBL (4 vs 15 p=002) with fewerserious complications (4 vs 13 p=004) Overall survivalwas similar in both trials125 126
Balloon tamponadeBalloon tamponade is highly effective and controls acute bleed-ing in up to 90 of patients although about 50 rebleed whenthe balloon is deflated127 128 It is however associated withserious complications such as oesophageal ulceration and aspir-ation pneumonia in up to 15ndash20 of patients Despite this itmay be a life-saving treatment in cases of massive uncontrolledvariceal haemorrhage pending other forms of treatment Anappropriately placed SengstakenndashBlakemore tube allows forresuscitation safe transportation and either repeat endoscopy orradiological shunting in a patient with a stable cardiovascularsystem The oesophageal balloon is rarely required must neverbe used on its own and should be used only if there is continu-ing bleeding despite an adequately inflated gastric balloon cor-rectly placed and with appropriate tension Placement of thetube endoscopically or over a guide wire might reduce the riskof complications especially oesophageal rupture
Removable oesophageal stentsThe SX-Ella Danis stent (ELLA-CS Hradec Kralove CzechRepublic) is a removable covered metal mesh stent placed endo-scopically in the lower oesophagus without radiological screen-ing It has no role in the management of gastric varicealbleeding These stents can be left in situ for up to 2 weeksunlike the SengstakenndashBlakemore tube which should beremoved after a maximum of 24ndash48 h129 130 No published con-trolled trials have compared this modality with balloontamponade
Transjugular intrahepatic portosystemic stent-shuntSeveral uncontrolled studies have examined the role of salvagebare TIPSS in acute variceal bleeding In a review of 15 studiescontrol of bleeding was achieved in 90ndash100 with rebleedingin 6ndash16131 Mortality varied between 75 (in hospital) and15 (30 day) It is important to appreciate that sclerotherapywas used as first-line endoscopic therapy in most of thesestudies Long-term follow-up of a study that compared TIPSSwith H-graft portacaval shunts in patients for whom non-operative management had failed suggested that H-grafts were auseful method of reducing portal pressure and had a signifi-cantly lower failure rate (p=004) but had no significant
14 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
improvement in overall survival despite a benefit seen in ChildrsquosA and B disease132 A recent RCT compared emergency porto-caval surgery with bare TIPSS within 24 h of presenting withacute oesophageal variceal bleeding in unselected cirrhoticpatients Emergency portocaval surgery resulted in better out-comes for long-term bleeding control encephalopathy and sur-vival (plt0001)133 Before wider application of surgery foracute variceal bleeding more data are needed in light of therecent adoption of covered stents
There has also been a generalised established change in prac-tice in using covered TIPSS stents (polytetrafluoroethylene(PTFE)) rather than a bare metal stent with evidence to supportthis change In randomised controlled studies these stents wereshown to have higher primary patency rates than bare stentswithout significant differences in survival and the potential forreduced incidence of hepatic encephalopathy134 135
There is however growing evidence from two RCTs for theearlier use of TIPSS in selected patients stratified by HVPGChildndashPugh class and active bleeding and not just use as asalvage option6 136 Monescillo et al136 randomised patientspresenting with acute oesophageal variceal haemorrhage to bareTIPSS or standard of care if the HVPG was ge20 mm Hg within24 h of admission Significantly reduced treatment failure asdefined by failure to control acute bleeding andor early rebleed-ing (12 vs 50) was seen and improved survival (62 vs35) in the patients randomised to undergo a TIPSS procedureHowever the standard of care was sclerotherapy and not com-bination endoscopic and pharmacological treatment This limita-tion and the lack of availability of HVPG measurement in mostcentres meant this trial did not have a significant impact on clin-ical practice
Garcia-Pagan et al6 selected patients with active bleeding andChildrsquos B cirrhosis or patients with Childrsquos C cirrhosis (Childrsquosscore lt14) for randomisation to early PTFE-covered TIPSSwithin 72 h or standard of care with VBL and pharmacologicaltreatment This has shown encouraging results with reduced riskof treatment failure (3 vs 50) improved survival (86 vs61 at 1 year) yet without increased risk of hepatic encephal-opathy The results were supported by an observational studyfrom the same group although a survival benefit was notseen137 Furthermore a recent well-conducted observationalstudy did not demonstrate such high survival rates with earlyTIPSS with 11-year survival of 67 which was similar to thatof patients given endoscopic and pharmacological treatmentsonly138 Therefore larger multicentred RCTs need to be under-taken to further evaluate the role of early TIPSS It is importantto make the distinction between salvage TIPSS and early TIPSSto prevent rebleeding
Liver transplantationThis is probably appropriate only for patients who bleed whileawaiting liver transplantation although studies comparing VBLor TIPSS placement with urgent liver transplantation in thissituation need to be done Liver transplantation is an exceed-ingly rare option for the vast majority of patients both becauseit is not commonly available and because of shortages anddelays in organ procurement No controlled trials of liver trans-plantation in uncontrolledactive bleeding are available
Recommendations for the control of variceal bleeding in cir-rhosis are given below and in figure 3
Recommendations control of active variceal haemorrhage incirrhosis (figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with bloodplatelets and clotting factors in line with local protocolsfor managing massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusionpolicy aiming for a haemoglobin of 70ndash80 gL is sug-gested in haemodynamically stable patients (level 1bgrade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable(level 5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L(level 5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to localcircumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with suspected
or confirmed variceal bleeding (level 1a grade A)32 In all patients vasoconstrictors such as terlipressin or
somatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 15
Guidelines
41 If bleeding is difficult to control a SengstakenndashBlakemore tube should be inserted until further endo-scopic treatment TIPSS or surgery is performed depend-ing on local resources and expertise (level 1b grade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure (level1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
SECONDARY PROPHYLAXIS OF VARICEAL HAEMORRHAGEβ BlockersA meta-analysis of 12 trials comparing propranolol or nadolol139
with no active treatment showed a significant reduction inrebleeding but no significant reduction in mortality140 Thegreater reduction in portal pressure with carvedilol comparedwith propranolol has been described in the section lsquoPrimaryprophylaxisrsquo of this guideline
NitratesThe addition of ISMN to NSBB has been shown to reduce vari-ceal rebleeding compared with NSBB alone although no sur-vival benefit was seen141 In addition adverse events leading todrug withdrawal were more common in the group receivingcombined drug treatment A meta-analysis of ISMN alone orwith either NSBB or endoscopic therapy reported that there wasno mortality benefit from combining nitrates and NSBB com-pared with NSBB alone142
Side effects of ISMN include dizziness and headache Owingto the side effects and relative lack of data ISMN is not com-monly used in clinical practice
A recent RCT of 121 patients reported carvedilol to besimilar to combined ISMN and NSBB therapy in the preventionof variceal rebleeding and mortality although severe adverseevents were less common with carvedilol143
SimvastatinA recent abstract of a multicentre RCT of 158 patients reporteda survival benefit (91 vs 78 p=003) from adding simvasta-tin to VBL and NSBB compared with placebo VBL and NSBBas treatment for the prevention of variceal rebleeding144 Therewas no difference in rebleeding and the survival benefit wasrestricted to Child A and B patients Serious adverse events weresimilar in both groups More data are required to investigatethis interesting observation of a survival benefit from simvastatinin this situation which may relate to its effects on hepatocellularfunction fibrosis and portal pressure
Proton pump inhibitorsA double-blind randomised placebo-controlled trial showed thatpantoprazole reduced the size of ulcers in patients who under-went VBL However the total number of ulcers and other out-comes were similar in the two groups145
Endoscopic therapyVBL has been accepted as the preferred endoscopic treatmentfor the prevention of variceal rebleeding with a lower rate ofrebleeding mortality and complications than sclerother-apy146 147 The time interval between VBL sessions to achieveeradication of varices is debateable However a recent RCTcomparing monthly with biweekly VBL after initial haemostasiswith VBL in 70 patients suggested that there were fewerpost-VBL ulcers in the monthly group (11 vs 57plt0001)148 Variceal recurrence rebleeding and mortality weresimilar in both groups
Two meta-analyses showed there is no evidence that the add-ition of sclerotherapy to VBL improves clinically relevant out-comes including variceal rebleeding and death and thecombination led to higher stricture rates149 150
Endoscopic therapy versus drug therapyVBL has been reported to be more effective than combinedNSBB and ISMN drug therapy151 However an 8-yearfollow-up study of this RCT found that although VBL wassuperior in reducing variceal rebleeding survival rates were sig-nificantly higher in the group treated with combined drug treat-ment152 Other studies have found no superiority of VBL overcombined drug therapy for prevention of variceal rebleeding ormortality153 154 A recent small multicentre RCT reported carve-dilol to be similar to VBL in the prevention of variceal rebleed-ing with a trend in favour of survival with carvedilol (73 vs48 p=0110)155
Several meta-analyses have compared drug therapy with VBLin the prevention of variceal rebleeding One meta-analysis ofsix RCTs showed no significant difference in variceal rebleedingrates when comparing VBL alone with combined NSBB andISMN therapy However all-cause mortality was significantlyhigher in patients treated with the VBL (RR=125 95 CI101 to 155)156 Three meta-analyses comparing drug therapy(NSBB alone or with ISMN) with endoscopic therapy alonereported no difference in variceal rebleeding or mortality157ndash159
Endoscopic+drug therapy versus either aloneNumerous studies and several meta-analyses have comparedcombined endoscopic and drug therapy with monotherapy(endoscopic or drugs alone) in the prevention of varicealrebleeding A meta-analysis of 23 trials assessing sclerotherapyor VBL combined with NSBB reported that combinationtherapy reduced rebleeding more than either endoscopic
16 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

following risk factors doubled mortality after an acute varicealbleed in one US study older age comorbidities male gender andnot undergoing a gastroscopy within 24 h105
A full examination is helpful for the important negatives asmuch as the positives Baseline observations should include thetemperature as infection is a serious complication with signifi-cant mortality Confusion may be present because of encephal-opathy intoxication with alcohol or drugs or withdrawal fromalcohol or drugs The patient should be on continuous BP andpulse monitor and their haemodynamic status recordedAn oxygen saturation monitor is helpful Stigmata of chronicliver disease and concurrent jaundice provide insight into thecurrent status of a patientrsquos liver and also give warning ofpotential further decompensation if significant bleeding persists(see scoring systems above) Pneumonia must be actively
excluded Evidence of ascites requires a diagnostic tap to searchfor infection
Investigations including full blood count coagulationprofile liver and renal function and blood group and save andcross-match Blood and urine should also be cultured An ultra-sound scan later in the admission is helpful to identify subclin-ical ascites flow in portal vein and any obvious emergence of anhepatocellular carcinoma (HCC)
Location of patientA decision must be made as to where the patient is best managedVariceal bleeding is unpredictable generally occurs in patientswith significant liver disease and is associated with significant mor-tality Hence a high-dependency unit is usually the most appropri-ate initial location although a properly staffed lsquogastrointestinal
Figure 3 Algorithm for themanagement of acute varicealbleeding TIPSS transjugularintrahepatic portosystemic stent shunt
12 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
bleeding bedrsquo may be appropriate If a patient is vomiting bloodor there is a perceived risk of a haemodynamically unstable patienthaving blood in the stomach then the patient must be intubatedbefore endoscopy and return to an intensive care or high-dependency unit will be necessary until extubation
Volume resuscitation and blood productsIntravenous access (two 16ndash18G cannulae) should have beensecured on admission with a reported GI bleed Further intra-venous access may be necessary In patients with poor venousaccess advanced liver disease or renal failure associated withtheir liver disease central venous access may be helpful withguiding fluid infusions However the drawbacks include the riskof the procedure and a potential source of infection Thereforethere is no absolute requirement for a central line and no evi-dence of unequivocal benefit Intravenous fluid resuscitationshould be initiated with plasma expanders aiming to maintain asystolic blood pressure of 100 mm Hg Care with monitoring isparamount in this group of patients
Overtransfusion has been shown to have a deleterious effecton outcome In a recent single-centre RCT a restrictive transfu-sion policy of maintaining haemoglobin between 70 and 80 gLimproved the control of variceal bleeding (11 vs 22p=005) and lowered HVPG compared with a liberal transfu-sion policy without effect on 45-day survival106 However itshould be noted that these results were from a single Spanishcentre which was a tertiary unit for variceal bleeding where allpatients underwent endoscopy within 6 h Nonetheless arestrictive transfusion policy has been recommended for sometime1 and there is now good evidence to support not transfusinga stable patient with a haemoglobin of ge80 gL However under-resuscitation should also be avoided and while goal-orientedfluid replacement has generally not been useful in an intensivetherapy unit setting a venous saturation gt70 remains an easilymeasurable target with some evidence to support it107
Interpretation and management of clotting profile is challen-ging in liver disease where there is usually a balanced deficiencyof both procoagulant and anticoagulant factors108 The NICEguidelines recommend activation of a hospitalrsquos massive transfu-sion policy when there is major haemorrhage and plateletsupport when the value is lt50 and clotting factor supportwhen the international normalised ratio (INR) is gt15 timesnormal2 There is no evidence for the use of lsquoprophylacticrsquo clot-ting or platelet support to reduce the risk of rebleeding Thereis insufficient evidence to support the routine use of transexamicacid or recombinant factor VIIa109
Pharmacological treatmentThe two major classes of drugs that have been used in thecontrol of acute variceal bleeding are vasopressin or its analo-gues (either alone or in combination with nitroglycerine) andsomatostatin or its analogues Terlipressin is the only agent thathas been shown to reduce mortality in placebo-controlled trialsHowever in trials comparing terlipressin somatostatin andoctreotide no difference in efficacy was identified in a system-atic review110 and in a recent large RCT111 Prophylactic anti-biotics can result in a similar survival benefit following acutevariceal bleeding
VasopressinVasopressin reduces portal blood flow portal systemic collateralblood flow and variceal pressure It does however have signifi-cant systemic side effects such as an increase in peripheral resist-ance and reduction in cardiac output heart rate and coronary
blood flow In comparison with no active treatment the pooledresults of four randomised trials showed that it reduced failureto control variceal bleeding (OR=022 95 CI 012 to 043)although survival was unaffected68 Meta-analysis of five trialscomparing sclerotherapy with vasopressin has shown a signifi-cant effect on reduction in failure to control bleeding(OR=051 95 CI 027 to 097) with no effect on survival68
Vasopressin with nitroglycerineThe addition of nitroglycerine enhances the effect of vasopres-sin on portal pressure and reduces cardiovascular side effects112
Meta-analysis of three randomised trials comparing vasopressinalone with vasopressin and nitroglycerine showed that the com-bination was associated with a significant reduction in failure tocontrol bleeding (OR=039 95 CI 022 to 072) although nosurvival benefit was shown68
TerlipressinTerlipressin is a synthetic analogue of vasopressin which has animmediate systemic vasoconstrictor action followed by portalhaemodynamic effects due to slow conversion to vasopressin Ina Cochrane meta-analysis of seven placebo-controlled trials ter-lipressin was shown to reduce failure to control bleeding(RR=066 95 CI 055 to 093) and also to improve survival(RR=066 95 CI 049 to 088)113 In the same meta-analysisthere was no difference between terlipressin versus vasopressinballoon tamponade or endoscopic therapy in failure to controlbleeding or survival113 The role of terlipressin in combinationwith VBL is explored in the section lsquoEndoscopic therapy incombination with pharmacological therapyrsquo
The recommended dose of terlipressin is 2 mg IV every 4 halthough many units reduce the dose to 6 hourly as it may causeperipheral vasoconstriction which manifests as painful handsand feet While 5 days of IV treatment has been advocated inthe Baveno V guidelines1 this prolonged treatment has notbeen shown to have a survival benefit and for pragmaticreasons many units will stop treatment shortly after satisfactoryhaemostasis In a randomised trial terlipressin given for 24 hafter satisfactory haemostasis with VBL after oesophageal vari-ceal bleeding was as effective as 72 h of treatment114
In patients intolerant of terlipressin or in countries where ter-lipressin is not available alternatives should be considered
Somatostatin and octreotideSomatostatin causes selective splanchnic vasoconstriction andreduces portal pressure and portal blood flow115 Octreotide is asomatostatin analogue The mechanism of action of these twoagents is not clear Inhibition of glucagon increases vasodilatationrather than a direct vasoconstrictive effect and post-prandial guthyperaemia is also reduced The actions of octreotide on hepaticand systemic hemodynamics are transient making continuousinfusion necessary Octreotide is given as a 50 μg bolus followedby an infusion of 25ndash50 μgh Somatostatin is given as a 250 mgintravenous bolus followed by an infusion of 250 mghSomatostatin and octreotide have been shown to be aseffective as terlipressin in acute variceal bleeding in ameta-analysis110 Seo et al111 in a large RCTof 780 patients com-paring these three agents failed to show a difference in treatmentsuccess (range 838ndash862) rebleeding (range 34ndash44) andmortality (range 8ndash88) A low systolic blood pressure at pres-entation high serum creatinine level active bleeding in the emer-gency endoscopy gastric variceal bleeding and ChildndashPugh gradeC were independent factors predicting 5-day treatmentfailure111
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 13
Guidelines
AntibioticsAntibiotics that provide Gram-negative cover are one of the inter-ventions which positively influence survival in variceal haemor-rhage as shown in a Cochrane meta-analysis of 12placebo-controlled trials (RR=079 95 CI 063 to 098)116
Antibiotics were also shown to reduce bacterial infections(RR=043 95 CI 019 to 097) and early rebleeding (RR=05395 CI 038 to 074)116 Therefore short-term antibiotics shouldbe considered standard practice in all cirrhotic patients who have avariceal bleed irrespective of the presence of confirmed infectionThird-generation cephalosporins such as ceftriaxone (1 g IVdaily) have been shown to be more effective at reducingGram-negative sepsis than oral norfloxacin117 but choice of anti-biotics must be dictated by local resistance patterns and availability
Proton pump inhibitorsOne RCT compared a short course of proton pump inhibitorswith vasoconstrictor therapies after haemostasis in acute varicealbleeding118 Despite larger ulcers noted in the vasoconstrictorarm there were no differences in bleeding or survival Nearly50 of patients had ascites which might have implications inlight of the reports of increased incidence of spontaneous bac-terial peritonitis as mentioned earlier
Endoscopic therapyEndoscopy should take place within 24 h of admission andearlier if there is excessive bleeding based on low-level evi-dence105 While many guidelines and reviews suggest thatendoscopy should be carried out within 12 h the only study thatexamined the influence of timing on outcome failed to demon-strate any advantage of endoscopy before 12 h119 The optimaltime is after sufficient resuscitation and pharmacological treat-ment with the endoscopy performed by a skilled endoscopyteam in a suitably equipped theatre environment and withairway protection Airway protection is essential where risk ofaspiration is high and affords the endoscopist time for thoroughevaluation including complete clot aspiration and controlledapplication of treatment including tamponade if required Theendoscopy team must comprise an experienced endoscopynurse acquainted with the equipment necessary for endoscopytherapy of varices and a skilled endoscopist competent in usingbanding devices and deployment of balloon tamponade
Variceal band ligationThis technique is a modification of that used for the elastic bandligation of internal haemorrhoids Its use in humans was firstdescribed in 1988120 A meta-analysis of seven trials comparingVBL with sclerotherapy in acute bleeding showed that VBLreduced rebleeding from varices (OR=047 95 CI 029 to078) reduced mortality (OR=067 95 CI 046 to 098) andresulted in fewer oesophageal strictures (OR=010 95 CI003 to 029)121 The number of sessions required to obliteratevarices was lower with VBL (22 fewer sessions (95 CI 09to 35))
SclerotherapySclerotherapy has been replaced by VBL and should no longerbe offered as standard of care in acute variceal haemorrhage
Other endoscopic measuresIn an RCT cyanoacrylate offered no benefit over VBL with theadditional risk of embolisation and trend towards increasedrebleeding with cyanoacrylate122
Haemostatic powder (TC-325 Hemospray Cook MedicalUSA) has been described in a small study of nine patients whoreceived endoscopic spray treatment for acute variceal bleedingThe study reported no rebleeding within 24 h and no mortalityat 15 days123
Endoscopic therapy in combination with pharmacological therapyThe role of combining vasoactive drugs with endoscopictherapy (VBL or sclerotherapy) was reported in a meta-analysisof eight trials124 Combination therapy resulted in better initialcontrol of bleeding (RR=112 95 CI 102 to 123) and5-day haemostasis (RR=128 95 CI 118 to 139) withoutany difference in survival Adverse events were similar in bothgroups Two RCTs have compared VBL with sclerotherapy incombination with vasoactive agents in acute variceal bleed-ing125 126 Lo et al125 used vasopressin and found that VBLresulted in better 72 h haemostasis (97 vs 76 p=0009)with fewer complications (5 vs 29 p=0007) Villanuevaet al used somatostatin and reported lower failure to controlacute bleeding with VBL (4 vs 15 p=002) with fewerserious complications (4 vs 13 p=004) Overall survivalwas similar in both trials125 126
Balloon tamponadeBalloon tamponade is highly effective and controls acute bleed-ing in up to 90 of patients although about 50 rebleed whenthe balloon is deflated127 128 It is however associated withserious complications such as oesophageal ulceration and aspir-ation pneumonia in up to 15ndash20 of patients Despite this itmay be a life-saving treatment in cases of massive uncontrolledvariceal haemorrhage pending other forms of treatment Anappropriately placed SengstakenndashBlakemore tube allows forresuscitation safe transportation and either repeat endoscopy orradiological shunting in a patient with a stable cardiovascularsystem The oesophageal balloon is rarely required must neverbe used on its own and should be used only if there is continu-ing bleeding despite an adequately inflated gastric balloon cor-rectly placed and with appropriate tension Placement of thetube endoscopically or over a guide wire might reduce the riskof complications especially oesophageal rupture
Removable oesophageal stentsThe SX-Ella Danis stent (ELLA-CS Hradec Kralove CzechRepublic) is a removable covered metal mesh stent placed endo-scopically in the lower oesophagus without radiological screen-ing It has no role in the management of gastric varicealbleeding These stents can be left in situ for up to 2 weeksunlike the SengstakenndashBlakemore tube which should beremoved after a maximum of 24ndash48 h129 130 No published con-trolled trials have compared this modality with balloontamponade
Transjugular intrahepatic portosystemic stent-shuntSeveral uncontrolled studies have examined the role of salvagebare TIPSS in acute variceal bleeding In a review of 15 studiescontrol of bleeding was achieved in 90ndash100 with rebleedingin 6ndash16131 Mortality varied between 75 (in hospital) and15 (30 day) It is important to appreciate that sclerotherapywas used as first-line endoscopic therapy in most of thesestudies Long-term follow-up of a study that compared TIPSSwith H-graft portacaval shunts in patients for whom non-operative management had failed suggested that H-grafts were auseful method of reducing portal pressure and had a signifi-cantly lower failure rate (p=004) but had no significant
14 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
improvement in overall survival despite a benefit seen in ChildrsquosA and B disease132 A recent RCT compared emergency porto-caval surgery with bare TIPSS within 24 h of presenting withacute oesophageal variceal bleeding in unselected cirrhoticpatients Emergency portocaval surgery resulted in better out-comes for long-term bleeding control encephalopathy and sur-vival (plt0001)133 Before wider application of surgery foracute variceal bleeding more data are needed in light of therecent adoption of covered stents
There has also been a generalised established change in prac-tice in using covered TIPSS stents (polytetrafluoroethylene(PTFE)) rather than a bare metal stent with evidence to supportthis change In randomised controlled studies these stents wereshown to have higher primary patency rates than bare stentswithout significant differences in survival and the potential forreduced incidence of hepatic encephalopathy134 135
There is however growing evidence from two RCTs for theearlier use of TIPSS in selected patients stratified by HVPGChildndashPugh class and active bleeding and not just use as asalvage option6 136 Monescillo et al136 randomised patientspresenting with acute oesophageal variceal haemorrhage to bareTIPSS or standard of care if the HVPG was ge20 mm Hg within24 h of admission Significantly reduced treatment failure asdefined by failure to control acute bleeding andor early rebleed-ing (12 vs 50) was seen and improved survival (62 vs35) in the patients randomised to undergo a TIPSS procedureHowever the standard of care was sclerotherapy and not com-bination endoscopic and pharmacological treatment This limita-tion and the lack of availability of HVPG measurement in mostcentres meant this trial did not have a significant impact on clin-ical practice
Garcia-Pagan et al6 selected patients with active bleeding andChildrsquos B cirrhosis or patients with Childrsquos C cirrhosis (Childrsquosscore lt14) for randomisation to early PTFE-covered TIPSSwithin 72 h or standard of care with VBL and pharmacologicaltreatment This has shown encouraging results with reduced riskof treatment failure (3 vs 50) improved survival (86 vs61 at 1 year) yet without increased risk of hepatic encephal-opathy The results were supported by an observational studyfrom the same group although a survival benefit was notseen137 Furthermore a recent well-conducted observationalstudy did not demonstrate such high survival rates with earlyTIPSS with 11-year survival of 67 which was similar to thatof patients given endoscopic and pharmacological treatmentsonly138 Therefore larger multicentred RCTs need to be under-taken to further evaluate the role of early TIPSS It is importantto make the distinction between salvage TIPSS and early TIPSSto prevent rebleeding
Liver transplantationThis is probably appropriate only for patients who bleed whileawaiting liver transplantation although studies comparing VBLor TIPSS placement with urgent liver transplantation in thissituation need to be done Liver transplantation is an exceed-ingly rare option for the vast majority of patients both becauseit is not commonly available and because of shortages anddelays in organ procurement No controlled trials of liver trans-plantation in uncontrolledactive bleeding are available
Recommendations for the control of variceal bleeding in cir-rhosis are given below and in figure 3
Recommendations control of active variceal haemorrhage incirrhosis (figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with bloodplatelets and clotting factors in line with local protocolsfor managing massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusionpolicy aiming for a haemoglobin of 70ndash80 gL is sug-gested in haemodynamically stable patients (level 1bgrade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable(level 5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L(level 5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to localcircumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with suspected
or confirmed variceal bleeding (level 1a grade A)32 In all patients vasoconstrictors such as terlipressin or
somatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 15
Guidelines
41 If bleeding is difficult to control a SengstakenndashBlakemore tube should be inserted until further endo-scopic treatment TIPSS or surgery is performed depend-ing on local resources and expertise (level 1b grade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure (level1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
SECONDARY PROPHYLAXIS OF VARICEAL HAEMORRHAGEβ BlockersA meta-analysis of 12 trials comparing propranolol or nadolol139
with no active treatment showed a significant reduction inrebleeding but no significant reduction in mortality140 Thegreater reduction in portal pressure with carvedilol comparedwith propranolol has been described in the section lsquoPrimaryprophylaxisrsquo of this guideline
NitratesThe addition of ISMN to NSBB has been shown to reduce vari-ceal rebleeding compared with NSBB alone although no sur-vival benefit was seen141 In addition adverse events leading todrug withdrawal were more common in the group receivingcombined drug treatment A meta-analysis of ISMN alone orwith either NSBB or endoscopic therapy reported that there wasno mortality benefit from combining nitrates and NSBB com-pared with NSBB alone142
Side effects of ISMN include dizziness and headache Owingto the side effects and relative lack of data ISMN is not com-monly used in clinical practice
A recent RCT of 121 patients reported carvedilol to besimilar to combined ISMN and NSBB therapy in the preventionof variceal rebleeding and mortality although severe adverseevents were less common with carvedilol143
SimvastatinA recent abstract of a multicentre RCT of 158 patients reporteda survival benefit (91 vs 78 p=003) from adding simvasta-tin to VBL and NSBB compared with placebo VBL and NSBBas treatment for the prevention of variceal rebleeding144 Therewas no difference in rebleeding and the survival benefit wasrestricted to Child A and B patients Serious adverse events weresimilar in both groups More data are required to investigatethis interesting observation of a survival benefit from simvastatinin this situation which may relate to its effects on hepatocellularfunction fibrosis and portal pressure
Proton pump inhibitorsA double-blind randomised placebo-controlled trial showed thatpantoprazole reduced the size of ulcers in patients who under-went VBL However the total number of ulcers and other out-comes were similar in the two groups145
Endoscopic therapyVBL has been accepted as the preferred endoscopic treatmentfor the prevention of variceal rebleeding with a lower rate ofrebleeding mortality and complications than sclerother-apy146 147 The time interval between VBL sessions to achieveeradication of varices is debateable However a recent RCTcomparing monthly with biweekly VBL after initial haemostasiswith VBL in 70 patients suggested that there were fewerpost-VBL ulcers in the monthly group (11 vs 57plt0001)148 Variceal recurrence rebleeding and mortality weresimilar in both groups
Two meta-analyses showed there is no evidence that the add-ition of sclerotherapy to VBL improves clinically relevant out-comes including variceal rebleeding and death and thecombination led to higher stricture rates149 150
Endoscopic therapy versus drug therapyVBL has been reported to be more effective than combinedNSBB and ISMN drug therapy151 However an 8-yearfollow-up study of this RCT found that although VBL wassuperior in reducing variceal rebleeding survival rates were sig-nificantly higher in the group treated with combined drug treat-ment152 Other studies have found no superiority of VBL overcombined drug therapy for prevention of variceal rebleeding ormortality153 154 A recent small multicentre RCT reported carve-dilol to be similar to VBL in the prevention of variceal rebleed-ing with a trend in favour of survival with carvedilol (73 vs48 p=0110)155
Several meta-analyses have compared drug therapy with VBLin the prevention of variceal rebleeding One meta-analysis ofsix RCTs showed no significant difference in variceal rebleedingrates when comparing VBL alone with combined NSBB andISMN therapy However all-cause mortality was significantlyhigher in patients treated with the VBL (RR=125 95 CI101 to 155)156 Three meta-analyses comparing drug therapy(NSBB alone or with ISMN) with endoscopic therapy alonereported no difference in variceal rebleeding or mortality157ndash159
Endoscopic+drug therapy versus either aloneNumerous studies and several meta-analyses have comparedcombined endoscopic and drug therapy with monotherapy(endoscopic or drugs alone) in the prevention of varicealrebleeding A meta-analysis of 23 trials assessing sclerotherapyor VBL combined with NSBB reported that combinationtherapy reduced rebleeding more than either endoscopic
16 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

bleeding bedrsquo may be appropriate If a patient is vomiting bloodor there is a perceived risk of a haemodynamically unstable patienthaving blood in the stomach then the patient must be intubatedbefore endoscopy and return to an intensive care or high-dependency unit will be necessary until extubation
Volume resuscitation and blood productsIntravenous access (two 16ndash18G cannulae) should have beensecured on admission with a reported GI bleed Further intra-venous access may be necessary In patients with poor venousaccess advanced liver disease or renal failure associated withtheir liver disease central venous access may be helpful withguiding fluid infusions However the drawbacks include the riskof the procedure and a potential source of infection Thereforethere is no absolute requirement for a central line and no evi-dence of unequivocal benefit Intravenous fluid resuscitationshould be initiated with plasma expanders aiming to maintain asystolic blood pressure of 100 mm Hg Care with monitoring isparamount in this group of patients
Overtransfusion has been shown to have a deleterious effecton outcome In a recent single-centre RCT a restrictive transfu-sion policy of maintaining haemoglobin between 70 and 80 gLimproved the control of variceal bleeding (11 vs 22p=005) and lowered HVPG compared with a liberal transfu-sion policy without effect on 45-day survival106 However itshould be noted that these results were from a single Spanishcentre which was a tertiary unit for variceal bleeding where allpatients underwent endoscopy within 6 h Nonetheless arestrictive transfusion policy has been recommended for sometime1 and there is now good evidence to support not transfusinga stable patient with a haemoglobin of ge80 gL However under-resuscitation should also be avoided and while goal-orientedfluid replacement has generally not been useful in an intensivetherapy unit setting a venous saturation gt70 remains an easilymeasurable target with some evidence to support it107
Interpretation and management of clotting profile is challen-ging in liver disease where there is usually a balanced deficiencyof both procoagulant and anticoagulant factors108 The NICEguidelines recommend activation of a hospitalrsquos massive transfu-sion policy when there is major haemorrhage and plateletsupport when the value is lt50 and clotting factor supportwhen the international normalised ratio (INR) is gt15 timesnormal2 There is no evidence for the use of lsquoprophylacticrsquo clot-ting or platelet support to reduce the risk of rebleeding Thereis insufficient evidence to support the routine use of transexamicacid or recombinant factor VIIa109
Pharmacological treatmentThe two major classes of drugs that have been used in thecontrol of acute variceal bleeding are vasopressin or its analo-gues (either alone or in combination with nitroglycerine) andsomatostatin or its analogues Terlipressin is the only agent thathas been shown to reduce mortality in placebo-controlled trialsHowever in trials comparing terlipressin somatostatin andoctreotide no difference in efficacy was identified in a system-atic review110 and in a recent large RCT111 Prophylactic anti-biotics can result in a similar survival benefit following acutevariceal bleeding
VasopressinVasopressin reduces portal blood flow portal systemic collateralblood flow and variceal pressure It does however have signifi-cant systemic side effects such as an increase in peripheral resist-ance and reduction in cardiac output heart rate and coronary
blood flow In comparison with no active treatment the pooledresults of four randomised trials showed that it reduced failureto control variceal bleeding (OR=022 95 CI 012 to 043)although survival was unaffected68 Meta-analysis of five trialscomparing sclerotherapy with vasopressin has shown a signifi-cant effect on reduction in failure to control bleeding(OR=051 95 CI 027 to 097) with no effect on survival68
Vasopressin with nitroglycerineThe addition of nitroglycerine enhances the effect of vasopres-sin on portal pressure and reduces cardiovascular side effects112
Meta-analysis of three randomised trials comparing vasopressinalone with vasopressin and nitroglycerine showed that the com-bination was associated with a significant reduction in failure tocontrol bleeding (OR=039 95 CI 022 to 072) although nosurvival benefit was shown68
TerlipressinTerlipressin is a synthetic analogue of vasopressin which has animmediate systemic vasoconstrictor action followed by portalhaemodynamic effects due to slow conversion to vasopressin Ina Cochrane meta-analysis of seven placebo-controlled trials ter-lipressin was shown to reduce failure to control bleeding(RR=066 95 CI 055 to 093) and also to improve survival(RR=066 95 CI 049 to 088)113 In the same meta-analysisthere was no difference between terlipressin versus vasopressinballoon tamponade or endoscopic therapy in failure to controlbleeding or survival113 The role of terlipressin in combinationwith VBL is explored in the section lsquoEndoscopic therapy incombination with pharmacological therapyrsquo
The recommended dose of terlipressin is 2 mg IV every 4 halthough many units reduce the dose to 6 hourly as it may causeperipheral vasoconstriction which manifests as painful handsand feet While 5 days of IV treatment has been advocated inthe Baveno V guidelines1 this prolonged treatment has notbeen shown to have a survival benefit and for pragmaticreasons many units will stop treatment shortly after satisfactoryhaemostasis In a randomised trial terlipressin given for 24 hafter satisfactory haemostasis with VBL after oesophageal vari-ceal bleeding was as effective as 72 h of treatment114
In patients intolerant of terlipressin or in countries where ter-lipressin is not available alternatives should be considered
Somatostatin and octreotideSomatostatin causes selective splanchnic vasoconstriction andreduces portal pressure and portal blood flow115 Octreotide is asomatostatin analogue The mechanism of action of these twoagents is not clear Inhibition of glucagon increases vasodilatationrather than a direct vasoconstrictive effect and post-prandial guthyperaemia is also reduced The actions of octreotide on hepaticand systemic hemodynamics are transient making continuousinfusion necessary Octreotide is given as a 50 μg bolus followedby an infusion of 25ndash50 μgh Somatostatin is given as a 250 mgintravenous bolus followed by an infusion of 250 mghSomatostatin and octreotide have been shown to be aseffective as terlipressin in acute variceal bleeding in ameta-analysis110 Seo et al111 in a large RCTof 780 patients com-paring these three agents failed to show a difference in treatmentsuccess (range 838ndash862) rebleeding (range 34ndash44) andmortality (range 8ndash88) A low systolic blood pressure at pres-entation high serum creatinine level active bleeding in the emer-gency endoscopy gastric variceal bleeding and ChildndashPugh gradeC were independent factors predicting 5-day treatmentfailure111
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 13
Guidelines
AntibioticsAntibiotics that provide Gram-negative cover are one of the inter-ventions which positively influence survival in variceal haemor-rhage as shown in a Cochrane meta-analysis of 12placebo-controlled trials (RR=079 95 CI 063 to 098)116
Antibiotics were also shown to reduce bacterial infections(RR=043 95 CI 019 to 097) and early rebleeding (RR=05395 CI 038 to 074)116 Therefore short-term antibiotics shouldbe considered standard practice in all cirrhotic patients who have avariceal bleed irrespective of the presence of confirmed infectionThird-generation cephalosporins such as ceftriaxone (1 g IVdaily) have been shown to be more effective at reducingGram-negative sepsis than oral norfloxacin117 but choice of anti-biotics must be dictated by local resistance patterns and availability
Proton pump inhibitorsOne RCT compared a short course of proton pump inhibitorswith vasoconstrictor therapies after haemostasis in acute varicealbleeding118 Despite larger ulcers noted in the vasoconstrictorarm there were no differences in bleeding or survival Nearly50 of patients had ascites which might have implications inlight of the reports of increased incidence of spontaneous bac-terial peritonitis as mentioned earlier
Endoscopic therapyEndoscopy should take place within 24 h of admission andearlier if there is excessive bleeding based on low-level evi-dence105 While many guidelines and reviews suggest thatendoscopy should be carried out within 12 h the only study thatexamined the influence of timing on outcome failed to demon-strate any advantage of endoscopy before 12 h119 The optimaltime is after sufficient resuscitation and pharmacological treat-ment with the endoscopy performed by a skilled endoscopyteam in a suitably equipped theatre environment and withairway protection Airway protection is essential where risk ofaspiration is high and affords the endoscopist time for thoroughevaluation including complete clot aspiration and controlledapplication of treatment including tamponade if required Theendoscopy team must comprise an experienced endoscopynurse acquainted with the equipment necessary for endoscopytherapy of varices and a skilled endoscopist competent in usingbanding devices and deployment of balloon tamponade
Variceal band ligationThis technique is a modification of that used for the elastic bandligation of internal haemorrhoids Its use in humans was firstdescribed in 1988120 A meta-analysis of seven trials comparingVBL with sclerotherapy in acute bleeding showed that VBLreduced rebleeding from varices (OR=047 95 CI 029 to078) reduced mortality (OR=067 95 CI 046 to 098) andresulted in fewer oesophageal strictures (OR=010 95 CI003 to 029)121 The number of sessions required to obliteratevarices was lower with VBL (22 fewer sessions (95 CI 09to 35))
SclerotherapySclerotherapy has been replaced by VBL and should no longerbe offered as standard of care in acute variceal haemorrhage
Other endoscopic measuresIn an RCT cyanoacrylate offered no benefit over VBL with theadditional risk of embolisation and trend towards increasedrebleeding with cyanoacrylate122
Haemostatic powder (TC-325 Hemospray Cook MedicalUSA) has been described in a small study of nine patients whoreceived endoscopic spray treatment for acute variceal bleedingThe study reported no rebleeding within 24 h and no mortalityat 15 days123
Endoscopic therapy in combination with pharmacological therapyThe role of combining vasoactive drugs with endoscopictherapy (VBL or sclerotherapy) was reported in a meta-analysisof eight trials124 Combination therapy resulted in better initialcontrol of bleeding (RR=112 95 CI 102 to 123) and5-day haemostasis (RR=128 95 CI 118 to 139) withoutany difference in survival Adverse events were similar in bothgroups Two RCTs have compared VBL with sclerotherapy incombination with vasoactive agents in acute variceal bleed-ing125 126 Lo et al125 used vasopressin and found that VBLresulted in better 72 h haemostasis (97 vs 76 p=0009)with fewer complications (5 vs 29 p=0007) Villanuevaet al used somatostatin and reported lower failure to controlacute bleeding with VBL (4 vs 15 p=002) with fewerserious complications (4 vs 13 p=004) Overall survivalwas similar in both trials125 126
Balloon tamponadeBalloon tamponade is highly effective and controls acute bleed-ing in up to 90 of patients although about 50 rebleed whenthe balloon is deflated127 128 It is however associated withserious complications such as oesophageal ulceration and aspir-ation pneumonia in up to 15ndash20 of patients Despite this itmay be a life-saving treatment in cases of massive uncontrolledvariceal haemorrhage pending other forms of treatment Anappropriately placed SengstakenndashBlakemore tube allows forresuscitation safe transportation and either repeat endoscopy orradiological shunting in a patient with a stable cardiovascularsystem The oesophageal balloon is rarely required must neverbe used on its own and should be used only if there is continu-ing bleeding despite an adequately inflated gastric balloon cor-rectly placed and with appropriate tension Placement of thetube endoscopically or over a guide wire might reduce the riskof complications especially oesophageal rupture
Removable oesophageal stentsThe SX-Ella Danis stent (ELLA-CS Hradec Kralove CzechRepublic) is a removable covered metal mesh stent placed endo-scopically in the lower oesophagus without radiological screen-ing It has no role in the management of gastric varicealbleeding These stents can be left in situ for up to 2 weeksunlike the SengstakenndashBlakemore tube which should beremoved after a maximum of 24ndash48 h129 130 No published con-trolled trials have compared this modality with balloontamponade
Transjugular intrahepatic portosystemic stent-shuntSeveral uncontrolled studies have examined the role of salvagebare TIPSS in acute variceal bleeding In a review of 15 studiescontrol of bleeding was achieved in 90ndash100 with rebleedingin 6ndash16131 Mortality varied between 75 (in hospital) and15 (30 day) It is important to appreciate that sclerotherapywas used as first-line endoscopic therapy in most of thesestudies Long-term follow-up of a study that compared TIPSSwith H-graft portacaval shunts in patients for whom non-operative management had failed suggested that H-grafts were auseful method of reducing portal pressure and had a signifi-cantly lower failure rate (p=004) but had no significant
14 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
improvement in overall survival despite a benefit seen in ChildrsquosA and B disease132 A recent RCT compared emergency porto-caval surgery with bare TIPSS within 24 h of presenting withacute oesophageal variceal bleeding in unselected cirrhoticpatients Emergency portocaval surgery resulted in better out-comes for long-term bleeding control encephalopathy and sur-vival (plt0001)133 Before wider application of surgery foracute variceal bleeding more data are needed in light of therecent adoption of covered stents
There has also been a generalised established change in prac-tice in using covered TIPSS stents (polytetrafluoroethylene(PTFE)) rather than a bare metal stent with evidence to supportthis change In randomised controlled studies these stents wereshown to have higher primary patency rates than bare stentswithout significant differences in survival and the potential forreduced incidence of hepatic encephalopathy134 135
There is however growing evidence from two RCTs for theearlier use of TIPSS in selected patients stratified by HVPGChildndashPugh class and active bleeding and not just use as asalvage option6 136 Monescillo et al136 randomised patientspresenting with acute oesophageal variceal haemorrhage to bareTIPSS or standard of care if the HVPG was ge20 mm Hg within24 h of admission Significantly reduced treatment failure asdefined by failure to control acute bleeding andor early rebleed-ing (12 vs 50) was seen and improved survival (62 vs35) in the patients randomised to undergo a TIPSS procedureHowever the standard of care was sclerotherapy and not com-bination endoscopic and pharmacological treatment This limita-tion and the lack of availability of HVPG measurement in mostcentres meant this trial did not have a significant impact on clin-ical practice
Garcia-Pagan et al6 selected patients with active bleeding andChildrsquos B cirrhosis or patients with Childrsquos C cirrhosis (Childrsquosscore lt14) for randomisation to early PTFE-covered TIPSSwithin 72 h or standard of care with VBL and pharmacologicaltreatment This has shown encouraging results with reduced riskof treatment failure (3 vs 50) improved survival (86 vs61 at 1 year) yet without increased risk of hepatic encephal-opathy The results were supported by an observational studyfrom the same group although a survival benefit was notseen137 Furthermore a recent well-conducted observationalstudy did not demonstrate such high survival rates with earlyTIPSS with 11-year survival of 67 which was similar to thatof patients given endoscopic and pharmacological treatmentsonly138 Therefore larger multicentred RCTs need to be under-taken to further evaluate the role of early TIPSS It is importantto make the distinction between salvage TIPSS and early TIPSSto prevent rebleeding
Liver transplantationThis is probably appropriate only for patients who bleed whileawaiting liver transplantation although studies comparing VBLor TIPSS placement with urgent liver transplantation in thissituation need to be done Liver transplantation is an exceed-ingly rare option for the vast majority of patients both becauseit is not commonly available and because of shortages anddelays in organ procurement No controlled trials of liver trans-plantation in uncontrolledactive bleeding are available
Recommendations for the control of variceal bleeding in cir-rhosis are given below and in figure 3
Recommendations control of active variceal haemorrhage incirrhosis (figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with bloodplatelets and clotting factors in line with local protocolsfor managing massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusionpolicy aiming for a haemoglobin of 70ndash80 gL is sug-gested in haemodynamically stable patients (level 1bgrade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable(level 5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L(level 5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to localcircumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with suspected
or confirmed variceal bleeding (level 1a grade A)32 In all patients vasoconstrictors such as terlipressin or
somatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 15
Guidelines
41 If bleeding is difficult to control a SengstakenndashBlakemore tube should be inserted until further endo-scopic treatment TIPSS or surgery is performed depend-ing on local resources and expertise (level 1b grade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure (level1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
SECONDARY PROPHYLAXIS OF VARICEAL HAEMORRHAGEβ BlockersA meta-analysis of 12 trials comparing propranolol or nadolol139
with no active treatment showed a significant reduction inrebleeding but no significant reduction in mortality140 Thegreater reduction in portal pressure with carvedilol comparedwith propranolol has been described in the section lsquoPrimaryprophylaxisrsquo of this guideline
NitratesThe addition of ISMN to NSBB has been shown to reduce vari-ceal rebleeding compared with NSBB alone although no sur-vival benefit was seen141 In addition adverse events leading todrug withdrawal were more common in the group receivingcombined drug treatment A meta-analysis of ISMN alone orwith either NSBB or endoscopic therapy reported that there wasno mortality benefit from combining nitrates and NSBB com-pared with NSBB alone142
Side effects of ISMN include dizziness and headache Owingto the side effects and relative lack of data ISMN is not com-monly used in clinical practice
A recent RCT of 121 patients reported carvedilol to besimilar to combined ISMN and NSBB therapy in the preventionof variceal rebleeding and mortality although severe adverseevents were less common with carvedilol143
SimvastatinA recent abstract of a multicentre RCT of 158 patients reporteda survival benefit (91 vs 78 p=003) from adding simvasta-tin to VBL and NSBB compared with placebo VBL and NSBBas treatment for the prevention of variceal rebleeding144 Therewas no difference in rebleeding and the survival benefit wasrestricted to Child A and B patients Serious adverse events weresimilar in both groups More data are required to investigatethis interesting observation of a survival benefit from simvastatinin this situation which may relate to its effects on hepatocellularfunction fibrosis and portal pressure
Proton pump inhibitorsA double-blind randomised placebo-controlled trial showed thatpantoprazole reduced the size of ulcers in patients who under-went VBL However the total number of ulcers and other out-comes were similar in the two groups145
Endoscopic therapyVBL has been accepted as the preferred endoscopic treatmentfor the prevention of variceal rebleeding with a lower rate ofrebleeding mortality and complications than sclerother-apy146 147 The time interval between VBL sessions to achieveeradication of varices is debateable However a recent RCTcomparing monthly with biweekly VBL after initial haemostasiswith VBL in 70 patients suggested that there were fewerpost-VBL ulcers in the monthly group (11 vs 57plt0001)148 Variceal recurrence rebleeding and mortality weresimilar in both groups
Two meta-analyses showed there is no evidence that the add-ition of sclerotherapy to VBL improves clinically relevant out-comes including variceal rebleeding and death and thecombination led to higher stricture rates149 150
Endoscopic therapy versus drug therapyVBL has been reported to be more effective than combinedNSBB and ISMN drug therapy151 However an 8-yearfollow-up study of this RCT found that although VBL wassuperior in reducing variceal rebleeding survival rates were sig-nificantly higher in the group treated with combined drug treat-ment152 Other studies have found no superiority of VBL overcombined drug therapy for prevention of variceal rebleeding ormortality153 154 A recent small multicentre RCT reported carve-dilol to be similar to VBL in the prevention of variceal rebleed-ing with a trend in favour of survival with carvedilol (73 vs48 p=0110)155
Several meta-analyses have compared drug therapy with VBLin the prevention of variceal rebleeding One meta-analysis ofsix RCTs showed no significant difference in variceal rebleedingrates when comparing VBL alone with combined NSBB andISMN therapy However all-cause mortality was significantlyhigher in patients treated with the VBL (RR=125 95 CI101 to 155)156 Three meta-analyses comparing drug therapy(NSBB alone or with ISMN) with endoscopic therapy alonereported no difference in variceal rebleeding or mortality157ndash159
Endoscopic+drug therapy versus either aloneNumerous studies and several meta-analyses have comparedcombined endoscopic and drug therapy with monotherapy(endoscopic or drugs alone) in the prevention of varicealrebleeding A meta-analysis of 23 trials assessing sclerotherapyor VBL combined with NSBB reported that combinationtherapy reduced rebleeding more than either endoscopic
16 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

AntibioticsAntibiotics that provide Gram-negative cover are one of the inter-ventions which positively influence survival in variceal haemor-rhage as shown in a Cochrane meta-analysis of 12placebo-controlled trials (RR=079 95 CI 063 to 098)116
Antibiotics were also shown to reduce bacterial infections(RR=043 95 CI 019 to 097) and early rebleeding (RR=05395 CI 038 to 074)116 Therefore short-term antibiotics shouldbe considered standard practice in all cirrhotic patients who have avariceal bleed irrespective of the presence of confirmed infectionThird-generation cephalosporins such as ceftriaxone (1 g IVdaily) have been shown to be more effective at reducingGram-negative sepsis than oral norfloxacin117 but choice of anti-biotics must be dictated by local resistance patterns and availability
Proton pump inhibitorsOne RCT compared a short course of proton pump inhibitorswith vasoconstrictor therapies after haemostasis in acute varicealbleeding118 Despite larger ulcers noted in the vasoconstrictorarm there were no differences in bleeding or survival Nearly50 of patients had ascites which might have implications inlight of the reports of increased incidence of spontaneous bac-terial peritonitis as mentioned earlier
Endoscopic therapyEndoscopy should take place within 24 h of admission andearlier if there is excessive bleeding based on low-level evi-dence105 While many guidelines and reviews suggest thatendoscopy should be carried out within 12 h the only study thatexamined the influence of timing on outcome failed to demon-strate any advantage of endoscopy before 12 h119 The optimaltime is after sufficient resuscitation and pharmacological treat-ment with the endoscopy performed by a skilled endoscopyteam in a suitably equipped theatre environment and withairway protection Airway protection is essential where risk ofaspiration is high and affords the endoscopist time for thoroughevaluation including complete clot aspiration and controlledapplication of treatment including tamponade if required Theendoscopy team must comprise an experienced endoscopynurse acquainted with the equipment necessary for endoscopytherapy of varices and a skilled endoscopist competent in usingbanding devices and deployment of balloon tamponade
Variceal band ligationThis technique is a modification of that used for the elastic bandligation of internal haemorrhoids Its use in humans was firstdescribed in 1988120 A meta-analysis of seven trials comparingVBL with sclerotherapy in acute bleeding showed that VBLreduced rebleeding from varices (OR=047 95 CI 029 to078) reduced mortality (OR=067 95 CI 046 to 098) andresulted in fewer oesophageal strictures (OR=010 95 CI003 to 029)121 The number of sessions required to obliteratevarices was lower with VBL (22 fewer sessions (95 CI 09to 35))
SclerotherapySclerotherapy has been replaced by VBL and should no longerbe offered as standard of care in acute variceal haemorrhage
Other endoscopic measuresIn an RCT cyanoacrylate offered no benefit over VBL with theadditional risk of embolisation and trend towards increasedrebleeding with cyanoacrylate122
Haemostatic powder (TC-325 Hemospray Cook MedicalUSA) has been described in a small study of nine patients whoreceived endoscopic spray treatment for acute variceal bleedingThe study reported no rebleeding within 24 h and no mortalityat 15 days123
Endoscopic therapy in combination with pharmacological therapyThe role of combining vasoactive drugs with endoscopictherapy (VBL or sclerotherapy) was reported in a meta-analysisof eight trials124 Combination therapy resulted in better initialcontrol of bleeding (RR=112 95 CI 102 to 123) and5-day haemostasis (RR=128 95 CI 118 to 139) withoutany difference in survival Adverse events were similar in bothgroups Two RCTs have compared VBL with sclerotherapy incombination with vasoactive agents in acute variceal bleed-ing125 126 Lo et al125 used vasopressin and found that VBLresulted in better 72 h haemostasis (97 vs 76 p=0009)with fewer complications (5 vs 29 p=0007) Villanuevaet al used somatostatin and reported lower failure to controlacute bleeding with VBL (4 vs 15 p=002) with fewerserious complications (4 vs 13 p=004) Overall survivalwas similar in both trials125 126
Balloon tamponadeBalloon tamponade is highly effective and controls acute bleed-ing in up to 90 of patients although about 50 rebleed whenthe balloon is deflated127 128 It is however associated withserious complications such as oesophageal ulceration and aspir-ation pneumonia in up to 15ndash20 of patients Despite this itmay be a life-saving treatment in cases of massive uncontrolledvariceal haemorrhage pending other forms of treatment Anappropriately placed SengstakenndashBlakemore tube allows forresuscitation safe transportation and either repeat endoscopy orradiological shunting in a patient with a stable cardiovascularsystem The oesophageal balloon is rarely required must neverbe used on its own and should be used only if there is continu-ing bleeding despite an adequately inflated gastric balloon cor-rectly placed and with appropriate tension Placement of thetube endoscopically or over a guide wire might reduce the riskof complications especially oesophageal rupture
Removable oesophageal stentsThe SX-Ella Danis stent (ELLA-CS Hradec Kralove CzechRepublic) is a removable covered metal mesh stent placed endo-scopically in the lower oesophagus without radiological screen-ing It has no role in the management of gastric varicealbleeding These stents can be left in situ for up to 2 weeksunlike the SengstakenndashBlakemore tube which should beremoved after a maximum of 24ndash48 h129 130 No published con-trolled trials have compared this modality with balloontamponade
Transjugular intrahepatic portosystemic stent-shuntSeveral uncontrolled studies have examined the role of salvagebare TIPSS in acute variceal bleeding In a review of 15 studiescontrol of bleeding was achieved in 90ndash100 with rebleedingin 6ndash16131 Mortality varied between 75 (in hospital) and15 (30 day) It is important to appreciate that sclerotherapywas used as first-line endoscopic therapy in most of thesestudies Long-term follow-up of a study that compared TIPSSwith H-graft portacaval shunts in patients for whom non-operative management had failed suggested that H-grafts were auseful method of reducing portal pressure and had a signifi-cantly lower failure rate (p=004) but had no significant
14 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
improvement in overall survival despite a benefit seen in ChildrsquosA and B disease132 A recent RCT compared emergency porto-caval surgery with bare TIPSS within 24 h of presenting withacute oesophageal variceal bleeding in unselected cirrhoticpatients Emergency portocaval surgery resulted in better out-comes for long-term bleeding control encephalopathy and sur-vival (plt0001)133 Before wider application of surgery foracute variceal bleeding more data are needed in light of therecent adoption of covered stents
There has also been a generalised established change in prac-tice in using covered TIPSS stents (polytetrafluoroethylene(PTFE)) rather than a bare metal stent with evidence to supportthis change In randomised controlled studies these stents wereshown to have higher primary patency rates than bare stentswithout significant differences in survival and the potential forreduced incidence of hepatic encephalopathy134 135
There is however growing evidence from two RCTs for theearlier use of TIPSS in selected patients stratified by HVPGChildndashPugh class and active bleeding and not just use as asalvage option6 136 Monescillo et al136 randomised patientspresenting with acute oesophageal variceal haemorrhage to bareTIPSS or standard of care if the HVPG was ge20 mm Hg within24 h of admission Significantly reduced treatment failure asdefined by failure to control acute bleeding andor early rebleed-ing (12 vs 50) was seen and improved survival (62 vs35) in the patients randomised to undergo a TIPSS procedureHowever the standard of care was sclerotherapy and not com-bination endoscopic and pharmacological treatment This limita-tion and the lack of availability of HVPG measurement in mostcentres meant this trial did not have a significant impact on clin-ical practice
Garcia-Pagan et al6 selected patients with active bleeding andChildrsquos B cirrhosis or patients with Childrsquos C cirrhosis (Childrsquosscore lt14) for randomisation to early PTFE-covered TIPSSwithin 72 h or standard of care with VBL and pharmacologicaltreatment This has shown encouraging results with reduced riskof treatment failure (3 vs 50) improved survival (86 vs61 at 1 year) yet without increased risk of hepatic encephal-opathy The results were supported by an observational studyfrom the same group although a survival benefit was notseen137 Furthermore a recent well-conducted observationalstudy did not demonstrate such high survival rates with earlyTIPSS with 11-year survival of 67 which was similar to thatof patients given endoscopic and pharmacological treatmentsonly138 Therefore larger multicentred RCTs need to be under-taken to further evaluate the role of early TIPSS It is importantto make the distinction between salvage TIPSS and early TIPSSto prevent rebleeding
Liver transplantationThis is probably appropriate only for patients who bleed whileawaiting liver transplantation although studies comparing VBLor TIPSS placement with urgent liver transplantation in thissituation need to be done Liver transplantation is an exceed-ingly rare option for the vast majority of patients both becauseit is not commonly available and because of shortages anddelays in organ procurement No controlled trials of liver trans-plantation in uncontrolledactive bleeding are available
Recommendations for the control of variceal bleeding in cir-rhosis are given below and in figure 3
Recommendations control of active variceal haemorrhage incirrhosis (figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with bloodplatelets and clotting factors in line with local protocolsfor managing massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusionpolicy aiming for a haemoglobin of 70ndash80 gL is sug-gested in haemodynamically stable patients (level 1bgrade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable(level 5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L(level 5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to localcircumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with suspected
or confirmed variceal bleeding (level 1a grade A)32 In all patients vasoconstrictors such as terlipressin or
somatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 15
Guidelines
41 If bleeding is difficult to control a SengstakenndashBlakemore tube should be inserted until further endo-scopic treatment TIPSS or surgery is performed depend-ing on local resources and expertise (level 1b grade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure (level1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
SECONDARY PROPHYLAXIS OF VARICEAL HAEMORRHAGEβ BlockersA meta-analysis of 12 trials comparing propranolol or nadolol139
with no active treatment showed a significant reduction inrebleeding but no significant reduction in mortality140 Thegreater reduction in portal pressure with carvedilol comparedwith propranolol has been described in the section lsquoPrimaryprophylaxisrsquo of this guideline
NitratesThe addition of ISMN to NSBB has been shown to reduce vari-ceal rebleeding compared with NSBB alone although no sur-vival benefit was seen141 In addition adverse events leading todrug withdrawal were more common in the group receivingcombined drug treatment A meta-analysis of ISMN alone orwith either NSBB or endoscopic therapy reported that there wasno mortality benefit from combining nitrates and NSBB com-pared with NSBB alone142
Side effects of ISMN include dizziness and headache Owingto the side effects and relative lack of data ISMN is not com-monly used in clinical practice
A recent RCT of 121 patients reported carvedilol to besimilar to combined ISMN and NSBB therapy in the preventionof variceal rebleeding and mortality although severe adverseevents were less common with carvedilol143
SimvastatinA recent abstract of a multicentre RCT of 158 patients reporteda survival benefit (91 vs 78 p=003) from adding simvasta-tin to VBL and NSBB compared with placebo VBL and NSBBas treatment for the prevention of variceal rebleeding144 Therewas no difference in rebleeding and the survival benefit wasrestricted to Child A and B patients Serious adverse events weresimilar in both groups More data are required to investigatethis interesting observation of a survival benefit from simvastatinin this situation which may relate to its effects on hepatocellularfunction fibrosis and portal pressure
Proton pump inhibitorsA double-blind randomised placebo-controlled trial showed thatpantoprazole reduced the size of ulcers in patients who under-went VBL However the total number of ulcers and other out-comes were similar in the two groups145
Endoscopic therapyVBL has been accepted as the preferred endoscopic treatmentfor the prevention of variceal rebleeding with a lower rate ofrebleeding mortality and complications than sclerother-apy146 147 The time interval between VBL sessions to achieveeradication of varices is debateable However a recent RCTcomparing monthly with biweekly VBL after initial haemostasiswith VBL in 70 patients suggested that there were fewerpost-VBL ulcers in the monthly group (11 vs 57plt0001)148 Variceal recurrence rebleeding and mortality weresimilar in both groups
Two meta-analyses showed there is no evidence that the add-ition of sclerotherapy to VBL improves clinically relevant out-comes including variceal rebleeding and death and thecombination led to higher stricture rates149 150
Endoscopic therapy versus drug therapyVBL has been reported to be more effective than combinedNSBB and ISMN drug therapy151 However an 8-yearfollow-up study of this RCT found that although VBL wassuperior in reducing variceal rebleeding survival rates were sig-nificantly higher in the group treated with combined drug treat-ment152 Other studies have found no superiority of VBL overcombined drug therapy for prevention of variceal rebleeding ormortality153 154 A recent small multicentre RCT reported carve-dilol to be similar to VBL in the prevention of variceal rebleed-ing with a trend in favour of survival with carvedilol (73 vs48 p=0110)155
Several meta-analyses have compared drug therapy with VBLin the prevention of variceal rebleeding One meta-analysis ofsix RCTs showed no significant difference in variceal rebleedingrates when comparing VBL alone with combined NSBB andISMN therapy However all-cause mortality was significantlyhigher in patients treated with the VBL (RR=125 95 CI101 to 155)156 Three meta-analyses comparing drug therapy(NSBB alone or with ISMN) with endoscopic therapy alonereported no difference in variceal rebleeding or mortality157ndash159
Endoscopic+drug therapy versus either aloneNumerous studies and several meta-analyses have comparedcombined endoscopic and drug therapy with monotherapy(endoscopic or drugs alone) in the prevention of varicealrebleeding A meta-analysis of 23 trials assessing sclerotherapyor VBL combined with NSBB reported that combinationtherapy reduced rebleeding more than either endoscopic
16 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

improvement in overall survival despite a benefit seen in ChildrsquosA and B disease132 A recent RCT compared emergency porto-caval surgery with bare TIPSS within 24 h of presenting withacute oesophageal variceal bleeding in unselected cirrhoticpatients Emergency portocaval surgery resulted in better out-comes for long-term bleeding control encephalopathy and sur-vival (plt0001)133 Before wider application of surgery foracute variceal bleeding more data are needed in light of therecent adoption of covered stents
There has also been a generalised established change in prac-tice in using covered TIPSS stents (polytetrafluoroethylene(PTFE)) rather than a bare metal stent with evidence to supportthis change In randomised controlled studies these stents wereshown to have higher primary patency rates than bare stentswithout significant differences in survival and the potential forreduced incidence of hepatic encephalopathy134 135
There is however growing evidence from two RCTs for theearlier use of TIPSS in selected patients stratified by HVPGChildndashPugh class and active bleeding and not just use as asalvage option6 136 Monescillo et al136 randomised patientspresenting with acute oesophageal variceal haemorrhage to bareTIPSS or standard of care if the HVPG was ge20 mm Hg within24 h of admission Significantly reduced treatment failure asdefined by failure to control acute bleeding andor early rebleed-ing (12 vs 50) was seen and improved survival (62 vs35) in the patients randomised to undergo a TIPSS procedureHowever the standard of care was sclerotherapy and not com-bination endoscopic and pharmacological treatment This limita-tion and the lack of availability of HVPG measurement in mostcentres meant this trial did not have a significant impact on clin-ical practice
Garcia-Pagan et al6 selected patients with active bleeding andChildrsquos B cirrhosis or patients with Childrsquos C cirrhosis (Childrsquosscore lt14) for randomisation to early PTFE-covered TIPSSwithin 72 h or standard of care with VBL and pharmacologicaltreatment This has shown encouraging results with reduced riskof treatment failure (3 vs 50) improved survival (86 vs61 at 1 year) yet without increased risk of hepatic encephal-opathy The results were supported by an observational studyfrom the same group although a survival benefit was notseen137 Furthermore a recent well-conducted observationalstudy did not demonstrate such high survival rates with earlyTIPSS with 11-year survival of 67 which was similar to thatof patients given endoscopic and pharmacological treatmentsonly138 Therefore larger multicentred RCTs need to be under-taken to further evaluate the role of early TIPSS It is importantto make the distinction between salvage TIPSS and early TIPSSto prevent rebleeding
Liver transplantationThis is probably appropriate only for patients who bleed whileawaiting liver transplantation although studies comparing VBLor TIPSS placement with urgent liver transplantation in thissituation need to be done Liver transplantation is an exceed-ingly rare option for the vast majority of patients both becauseit is not commonly available and because of shortages anddelays in organ procurement No controlled trials of liver trans-plantation in uncontrolledactive bleeding are available
Recommendations for the control of variceal bleeding in cir-rhosis are given below and in figure 3
Recommendations control of active variceal haemorrhage incirrhosis (figure 3)1 Suggestions for resuscitation and initial management
11 Units offering an emergency acute upper gastrointestinalbleeding service should have expertise in VBL balloontamponade and management of gastric variceal bleeding(level 5 grade D)
12 Transfuse patients with massive bleeding with bloodplatelets and clotting factors in line with local protocolsfor managing massive bleeding (level 5 grade D)
13 Base decisions on blood transfusion on the full clinicalpicture recognising that overtransfusion may be as dam-aging as undertransfusion A restrictive transfusionpolicy aiming for a haemoglobin of 70ndash80 gL is sug-gested in haemodynamically stable patients (level 1bgrade B)
14 Do not offer platelet transfusion to patients who are notactively bleeding and are haemodynamically stable(level 5 grade D)
15 Offer platelet transfusion to patients who are activelybleeding and have a platelet count of lt50times109L(level 5 grade D)
16 Offer fresh frozen plasma to patients who have either a fibrinogen level of lt1 gL (level 5 grade D) or a prothrombin time (international normalised ratio)
or activated partial thromboplastin time gt15 timesnormal (level 5 grade D)
17 Offer prothrombin complex concentrate to patients whoare taking warfarin and actively bleeding (level 5 grade D)
18 Treat patients who are taking warfarin and whose uppergastrointestinal bleeding has stopped in line with localwarfarin protocols (level 5 grade D)
19 There is insufficient evidence for the use of recombinantfactor VIIa in acute variceal haemorrhage (level 1bgrade B)
2 Suggestions for timing of upper gastrointestinal endoscopy21 Offer endoscopy to unstable patients with severe acute
upper gastrointestinal bleeding immediately after resusci-tation (level 5 grade A)
22 Offer endoscopy within 24 h of admission to all otherpatients with upper gastrointestinal bleeding (level 2bgrade A)
23 Units seeing more than 330 cases a year should offerdaily endoscopy lists Units seeing fewer than 330 casesa year should arrange their service according to localcircumstances (level 5 grade D)
3 Control of bleeding31 Antibiotics are recommended for all patients with suspected
or confirmed variceal bleeding (level 1a grade A)32 In all patients vasoconstrictors such as terlipressin or
somatostatin are recommended and should be started assoon variceal bleeding is suspected and continued untilhaemostasis is achieved or for up to 5 days Octreotide(unlicensed) is suggested if terlipressin or somatostatinare unavailable (level 1a grade A)
33 Variceal band ligation is recommended as the preferredendoscopic method (level 1a grade A)
34 After satisfactory haemostasis with the methods aboveand depending on local resources early covered TIPSS(lt72 h after index variceal bleed) can be considered inselected patients with Childrsquos B cirrhosis and activebleeding or Childrsquos C cirrhosis with Childrsquos score lt14(level 1b grade B)
35 Proton pump inhibitors are not recommended unlessotherwise required for peptic ulcer disease (level 1bgrade B)
4 Failure to control active bleeding
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 15
Guidelines
41 If bleeding is difficult to control a SengstakenndashBlakemore tube should be inserted until further endo-scopic treatment TIPSS or surgery is performed depend-ing on local resources and expertise (level 1b grade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure (level1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
SECONDARY PROPHYLAXIS OF VARICEAL HAEMORRHAGEβ BlockersA meta-analysis of 12 trials comparing propranolol or nadolol139
with no active treatment showed a significant reduction inrebleeding but no significant reduction in mortality140 Thegreater reduction in portal pressure with carvedilol comparedwith propranolol has been described in the section lsquoPrimaryprophylaxisrsquo of this guideline
NitratesThe addition of ISMN to NSBB has been shown to reduce vari-ceal rebleeding compared with NSBB alone although no sur-vival benefit was seen141 In addition adverse events leading todrug withdrawal were more common in the group receivingcombined drug treatment A meta-analysis of ISMN alone orwith either NSBB or endoscopic therapy reported that there wasno mortality benefit from combining nitrates and NSBB com-pared with NSBB alone142
Side effects of ISMN include dizziness and headache Owingto the side effects and relative lack of data ISMN is not com-monly used in clinical practice
A recent RCT of 121 patients reported carvedilol to besimilar to combined ISMN and NSBB therapy in the preventionof variceal rebleeding and mortality although severe adverseevents were less common with carvedilol143
SimvastatinA recent abstract of a multicentre RCT of 158 patients reporteda survival benefit (91 vs 78 p=003) from adding simvasta-tin to VBL and NSBB compared with placebo VBL and NSBBas treatment for the prevention of variceal rebleeding144 Therewas no difference in rebleeding and the survival benefit wasrestricted to Child A and B patients Serious adverse events weresimilar in both groups More data are required to investigatethis interesting observation of a survival benefit from simvastatinin this situation which may relate to its effects on hepatocellularfunction fibrosis and portal pressure
Proton pump inhibitorsA double-blind randomised placebo-controlled trial showed thatpantoprazole reduced the size of ulcers in patients who under-went VBL However the total number of ulcers and other out-comes were similar in the two groups145
Endoscopic therapyVBL has been accepted as the preferred endoscopic treatmentfor the prevention of variceal rebleeding with a lower rate ofrebleeding mortality and complications than sclerother-apy146 147 The time interval between VBL sessions to achieveeradication of varices is debateable However a recent RCTcomparing monthly with biweekly VBL after initial haemostasiswith VBL in 70 patients suggested that there were fewerpost-VBL ulcers in the monthly group (11 vs 57plt0001)148 Variceal recurrence rebleeding and mortality weresimilar in both groups
Two meta-analyses showed there is no evidence that the add-ition of sclerotherapy to VBL improves clinically relevant out-comes including variceal rebleeding and death and thecombination led to higher stricture rates149 150
Endoscopic therapy versus drug therapyVBL has been reported to be more effective than combinedNSBB and ISMN drug therapy151 However an 8-yearfollow-up study of this RCT found that although VBL wassuperior in reducing variceal rebleeding survival rates were sig-nificantly higher in the group treated with combined drug treat-ment152 Other studies have found no superiority of VBL overcombined drug therapy for prevention of variceal rebleeding ormortality153 154 A recent small multicentre RCT reported carve-dilol to be similar to VBL in the prevention of variceal rebleed-ing with a trend in favour of survival with carvedilol (73 vs48 p=0110)155
Several meta-analyses have compared drug therapy with VBLin the prevention of variceal rebleeding One meta-analysis ofsix RCTs showed no significant difference in variceal rebleedingrates when comparing VBL alone with combined NSBB andISMN therapy However all-cause mortality was significantlyhigher in patients treated with the VBL (RR=125 95 CI101 to 155)156 Three meta-analyses comparing drug therapy(NSBB alone or with ISMN) with endoscopic therapy alonereported no difference in variceal rebleeding or mortality157ndash159
Endoscopic+drug therapy versus either aloneNumerous studies and several meta-analyses have comparedcombined endoscopic and drug therapy with monotherapy(endoscopic or drugs alone) in the prevention of varicealrebleeding A meta-analysis of 23 trials assessing sclerotherapyor VBL combined with NSBB reported that combinationtherapy reduced rebleeding more than either endoscopic
16 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

41 If bleeding is difficult to control a SengstakenndashBlakemore tube should be inserted until further endo-scopic treatment TIPSS or surgery is performed depend-ing on local resources and expertise (level 1b grade B)
42 Specialist help should be sought at this time and transferto a specialist centre should be considered Units that donot offer a TIPSS service should identify a specialistcentre which offers a 24 h emergency TIPSS service andhave appropriate arrangements for safe transfer ofpatients in place (level 2a grade B)
5 Areas requiring further study51 The efficacy of restrictive blood transfusion in variceal
haemorrhage52 The role of blood products in variceal haemorrhage53 The utility of early TIPSS (lt72 h) in acute variceal
haemorrhage54 The role of removable oesophageal stents in acute vari-
ceal haemorrhage55 The role of haemostatic powders in acute variceal
haemorrhage56 The role of proton pump inhibitors in variceal
haemorrhage6 Quality indicators
61 Antibiotic administration in acute variceal bleedingwithin 1 day either before or after the procedure (level1a grade A)Numerator patients with an acute variceal bleed whohave received antibiotics within 1 day either before orafter the procedureDenominator patients with an acute variceal bleed
62 Endoscopy performed within 24 h of presentation of anacute variceal bleed (level 2b grade A)Numerator patients with an acute variceal bleed whohave received endoscopy within 24 h of presentationDenominator patients with an acute variceal bleed
SECONDARY PROPHYLAXIS OF VARICEAL HAEMORRHAGEβ BlockersA meta-analysis of 12 trials comparing propranolol or nadolol139
with no active treatment showed a significant reduction inrebleeding but no significant reduction in mortality140 Thegreater reduction in portal pressure with carvedilol comparedwith propranolol has been described in the section lsquoPrimaryprophylaxisrsquo of this guideline
NitratesThe addition of ISMN to NSBB has been shown to reduce vari-ceal rebleeding compared with NSBB alone although no sur-vival benefit was seen141 In addition adverse events leading todrug withdrawal were more common in the group receivingcombined drug treatment A meta-analysis of ISMN alone orwith either NSBB or endoscopic therapy reported that there wasno mortality benefit from combining nitrates and NSBB com-pared with NSBB alone142
Side effects of ISMN include dizziness and headache Owingto the side effects and relative lack of data ISMN is not com-monly used in clinical practice
A recent RCT of 121 patients reported carvedilol to besimilar to combined ISMN and NSBB therapy in the preventionof variceal rebleeding and mortality although severe adverseevents were less common with carvedilol143
SimvastatinA recent abstract of a multicentre RCT of 158 patients reporteda survival benefit (91 vs 78 p=003) from adding simvasta-tin to VBL and NSBB compared with placebo VBL and NSBBas treatment for the prevention of variceal rebleeding144 Therewas no difference in rebleeding and the survival benefit wasrestricted to Child A and B patients Serious adverse events weresimilar in both groups More data are required to investigatethis interesting observation of a survival benefit from simvastatinin this situation which may relate to its effects on hepatocellularfunction fibrosis and portal pressure
Proton pump inhibitorsA double-blind randomised placebo-controlled trial showed thatpantoprazole reduced the size of ulcers in patients who under-went VBL However the total number of ulcers and other out-comes were similar in the two groups145
Endoscopic therapyVBL has been accepted as the preferred endoscopic treatmentfor the prevention of variceal rebleeding with a lower rate ofrebleeding mortality and complications than sclerother-apy146 147 The time interval between VBL sessions to achieveeradication of varices is debateable However a recent RCTcomparing monthly with biweekly VBL after initial haemostasiswith VBL in 70 patients suggested that there were fewerpost-VBL ulcers in the monthly group (11 vs 57plt0001)148 Variceal recurrence rebleeding and mortality weresimilar in both groups
Two meta-analyses showed there is no evidence that the add-ition of sclerotherapy to VBL improves clinically relevant out-comes including variceal rebleeding and death and thecombination led to higher stricture rates149 150
Endoscopic therapy versus drug therapyVBL has been reported to be more effective than combinedNSBB and ISMN drug therapy151 However an 8-yearfollow-up study of this RCT found that although VBL wassuperior in reducing variceal rebleeding survival rates were sig-nificantly higher in the group treated with combined drug treat-ment152 Other studies have found no superiority of VBL overcombined drug therapy for prevention of variceal rebleeding ormortality153 154 A recent small multicentre RCT reported carve-dilol to be similar to VBL in the prevention of variceal rebleed-ing with a trend in favour of survival with carvedilol (73 vs48 p=0110)155
Several meta-analyses have compared drug therapy with VBLin the prevention of variceal rebleeding One meta-analysis ofsix RCTs showed no significant difference in variceal rebleedingrates when comparing VBL alone with combined NSBB andISMN therapy However all-cause mortality was significantlyhigher in patients treated with the VBL (RR=125 95 CI101 to 155)156 Three meta-analyses comparing drug therapy(NSBB alone or with ISMN) with endoscopic therapy alonereported no difference in variceal rebleeding or mortality157ndash159
Endoscopic+drug therapy versus either aloneNumerous studies and several meta-analyses have comparedcombined endoscopic and drug therapy with monotherapy(endoscopic or drugs alone) in the prevention of varicealrebleeding A meta-analysis of 23 trials assessing sclerotherapyor VBL combined with NSBB reported that combinationtherapy reduced rebleeding more than either endoscopic
16 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

therapy or NSBB alone (pooled RR=068 95 CI 052 to089) although no difference in mortality was detected160
A meta-analysis of fewer studies suggested no significant dif-ference in rebleeding between combined drug and VBL therapyand either alone157 A further meta-analysis reported reducedvariceal rebleeding (RR=0601 95 CI 0440 to 0820) butsimilar mortality with combined drug and endoscopic therapyversus endoscopic therapy alone159 Another meta-analysis of17 trials (14 using sclerotherapy and three using VBL) reportedthat combined endoscopic and NSBB therapy reduced rebleed-ing (OR=220 95 CI 169 to 285) and overall mortality(OR=143 95 CI 103 to 198) compared with endoscopictherapy alone161
A further meta-analysis of 10 RCTs suggested that combin-ation therapy reduces the risk of rebleeding from oesophagealvarices compared with VBL (RR=068 95 CI 045 to 093)or medical treatment (RR=060 95 CI 043 to 084)162 Thismeta-analysis included seven trials comparing combinationtherapy with VBL and three trials comparing combinationtherapy with drug treatment Combined VBL and drug therapygave a survival benefit when compared with VBL alone(RR=052 95 CI 027 to 099) but not when compared withmedical treatment alone
Another recent meta-analysis assessed five studies comparingVBL alone with combination VBL and drug therapy and fourstudies comparing drugs alone or combined with VBL163 Thisfound that adding drugs to VBL reduced rebleeding (RR=04495 CI 028 to 069) with a trend towards reduced mortalitybut adding VBL to drug treatment did not significantly affecteither rebleeding or mortality
The meta-analyses are not entirely consistent although itwould appear that combined VBL and drug treatment mightimprove survival but is likely to increase adverse effects com-pared with VBL alone There appears to be less clear benefitfrom combined VBL and drug treatment compared with drugtreatment alone
Transjugular intrahepatic portosystemic stent-shuntThree meta-analyses comparing TIPSS with endoscopic treat-ment (sclerotherapy or VBL) have been published164ndash166 Theresults are similar with the largest meta-analysis of 12 RCTsshowing that (bare) TIPSS reduces variceal rebleeding(OR=032 95 CI 024 to 043) but is associated with anincreased risk of encephalopathy (OR=221 95 CI 161 to303)166 No differences in survival were seen164ndash166 Despitethe problem of shunt insufficiency and the cost of shunt surveil-lance TIPSS has been shown to be more cost-effective thanendoscopic therapy167
A meta-analysis of six studies comparing TIPSS (both bareand covered) with or without variceal embolisation showed thatadjuvant embolisation during TIPSS reduced rebleeding(OR=202 95 CI 129 to 317) with similar shunt dysfunc-tion encephalopathy and mortality rates168 However owing toheterogeneity of the study methodology the authors recom-mended larger randomised studies using covered stents toconfirm the findings Generally TIPSS placement usingPTFE-covered stents134 is recommended for patients for whomendoscopic and pharmacological treatment for the preventionof variceal rebleeding fails1
The evidence for undertaking an lsquoearlyrsquo TIPSS procedure6 inpatients shortly after a first variceal bleed has been discussed inthe ldquoManagement of acute variceal bleedingrdquo section of thisguideline
SurgeryA meta-analysis demonstrated that non-selective shunts reducedrebleeding compared with no active treatment or sclerotherapyat the expense of increased encephalopathy with no survivalbenefit68 Non-selective shunts resulted in similar outcomescompared with distal splenorenal shunts68 Extended follow-upof a randomised study comparing portocaval shunt surgery withsclerotherapy following acute variceal bleeding reported betterlong-term bleeding control (100 vs 20 plt0001) andimproved survival (5-year survival 71 vs 21 plt0001) inthe portocaval shunt arm169 Distal splenorenal shunt surgerywas compared with TIPSS in a multicentre RCT including 140patients with Childrsquos A and B cirrhosis170 Results showedsimilar rebleeding and survival but higher rates of shunt dys-function and re-intervention in the TIPSS group althoughcovered stents were not used A follow-up study suggested thatTIPSS was more cost-effective171
Portosystemic shunts (total surgical distal splenorenal or bareTIPSS) were compared with endoscopic therapy for varicealrebleeding in a Cochrane database systematic review172
Twenty-two trials incorporating 1409 patients were included Allshunt therapies reduced rebleeding (OR=024 95 CI 018 to030) at the expense of higher rates of encephalopathy(OR=209 95 CI 120 to 362) with no survival advantageTIPSS was complicated by a high incidence of shunt dysfunction
Laparoscopic splenectomy plus VBL was also compared withTIPSS for variceal rebleeding in a recent non-randomised trialof 83 patients173 This reported surgery plus VBL to be betterthan TIPSS in preventing variceal rebleeding with low rates ofencephalopathy
Liver transplantation should be considered in eligible patientsfollowing a variceal bleed determined by the selection criteria ofthe country174 There is no clear evidence that prior shuntsurgery has a significant impact on transplant outcome169
Recommendations for the secondary prophylaxis of varicealbleeding in cirrhosis are given below and in figure 3
Recommendations secondary prophylaxis of variceal haemor-rhage in cirrhosis (figure 3)1 Should VBL be used in combination with NSBB
11 NSBB (propranolol or nadolol)+VBL combinationtherapy are recommended as secondary prophylaxis(level 1a grade A)
12 NSBB or VBL monotherapy are suggested as alternativeoptions taking into account patient preference and clin-ical judgement (level 1a grade B)
13 Carvedilol is suggested as an alternative to propranololand nadolol (level 1b grade B)
14 If NSBB alone are used there is no need to undertakefurther endoscopy unless clinically indicated (level 1agrade A)
15 We recommend that VBL alone is used to eradicatevarices if there are contraindications or intolerance tocombined use with NSBB (level 1a grade A)
2 What is the optimal protocol for VBL21 It is suggested that varices are banded at 2ndash4-weekly
intervals until eradication (level 1b grade B)22 After successful eradication of the varices patients
should be endoscoped at 3 months then 6 monthlythereafter Any recurrent varices should be treated withfurther VBL until eradication (level 1b grade B)
23 Proton pump inhibitors are not recommended unlessotherwise required for peptic disease (level 1b grade B)
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 17
Guidelines
3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

3 When is TIPSS indicated31 We suggest that TIPSS is used for patients who rebleed
despite combined VBL and NSBB therapy (or when mono-therapy with VBL or NSBB is used owing to intolerance orcontraindications to combination therapy) and in selectedcases owing to patient choice PTFE-covered stents arerecommended (level 1a grade A)
32 Where TIPSS is not feasible in Childrsquos A and B patientswe suggest shunt surgery can be used where localexpertise and resources allow (level 1b grade B)
4 Areas requiring further study41 Combination of VBL and carvedilol (or other NSBB)
versus carvedilol as monotherapy42 Comparison of carvedilol with propranolol in secondary
prophylaxis43 Optimum time interval between VBL sessions44 Strategy of VBL or NSBB discontinuation after variceal
eradication during combination therapy with VBL+NSBB
45 Strategy of VBL add-on therapy to failure of NSBBmonotherapy
46 Strategy of NSBB add-on therapy to failure of VBLmonotherapy
47 Role of early TIPSS in secondary prophylaxis48 Role of statins in secondary prophylaxis
5 Quality indicator51 Institution of secondary prophylaxis after acute variceal
bleeding (level 1a grade A)Numerator patients with an acute variceal bleed whohave received either NSBB or banding or both within4 weeks of the index bleedDenominator patients with an acute variceal bleed
GASTRIC VARICESNatural historyAt first endoscopy in patients with portal hypertension 20 areshown to have gastric varices175 They are commonly seen inpatients with portal hypertension due to portal or splenic veinobstruction175 Only 10ndash20 of all variceal bleeding occursfrom gastric varices but outcome is worse than with bleedingfrom oesophageal varices175 176
Gastric varices can be classified on the basis of their locationin the stomach and relationship with oesophageal varices Thisclassification has implications for management The commonlyused Sarin classification divides them into (a) gastro-oesophagealvarices (GOV) which are associated with oesophageal varicesand (b) isolated gastric varices (IGV) which occur independ-ently of oesophageal varices175 Both GOV and IGV are subdi-vided into two groups Type 1 GOV are continuous withoesophageal varices and extend for 2ndash5 cm below the gastro-oesophageal junction along the lesser curvature of the stomachType 2 GOV extend beyond the gastro-oesophageal junctioninto the fundus of the stomach Type 1 IGV refers to varicesthat occur in the fundus of the stomach and type 2 IGVdescribes varices anywhere else in the stomach including thebody antrum and pylorus The most common type of varicesseen in cirrhosis is GOV type 1 Patients who bleed from IGVare at a significantly higher risk of dying from an episode ofvariceal bleeding than patients bleeding from GOV177
Management of acute gastric variceal bleedingAlthough no studies have reported the use of vasopressors andantibiotics specifically for the initial management of gastric vari-ceal haemorrhage any patient with suspected variceal bleeding
should be managed as described above (see sectionlsquoManagement of active variceal haemorrhagersquo) Once endoscopyhas identified the source of bleeding as gastric varices thera-peutic options include endoscopic methods TIPSS other radio-logical procedures surgery and long-term NSBB Splenic veinthrombosis should be considered and appropriate investigationsundertaken in patients presenting with gastric variceal bleeding
Endoscopic therapyEndoscopic sclerotherapySclerotherapy has been largely replaced by VBL and tissue adhe-sives or thrombin when appropriate for gastric varices owing tothe lower complication and rebleeding rates
Endoscopic VBLStandard VBL or the use of detachable snares has been shownto control active bleeding from gastric varices but rebleedingand recurrence rates are high178 179 As GOV-1 are generallyconsidered extensions of oesophageal varices VBL is often usedto treat bleeding from here However given the larger diameterand the anatomy of other types of gastric varices and thelimited data on use of VBL in this situation this technique isgenerally not recommended for these
Endoscopic injection therapy with tissue adhesivesNumerous studies have reported the use of tissue adhesivesmost commonly histoacryl (N-butyl-cyanoacrylate) in the treat-ment of gastric varices180ndash194 Variations in technique dilutionwith lipiodol and follow-up strategy have been described Thesestudies have reported an initial haemostasis success rate withtissue glue of 86ndash100 with rebleeding rates of 7ndash28Uncommon but severe complications including emboli to thepulmonary and cerebral circulations have been described181
A randomised study compared cyanoacrylate injection withVBL in 60 patients with gastric variceal bleeding186 Patientstreated with cyanoacrylate had a higher haemostasis rate (87vs 45) lower rebleeding (31 vs 54) and lower mortality(29 vs 48) than those treated with VBL Another rando-mised study comparing cyanoacrylate with VBL in 97 patientswith gastric variceal bleeding reported equal haemostasis ratesat 93 but significantly higher rebleeding with VBL (72 vs27)193 This study reported no difference in survival or com-plications between groups
A non-randomised study comparing cyanoacrylate with VBLfor gastric variceal bleeding reported similar haemostasis ratesbut lower rebleeding with cyanoacrylate (32 vs 72)194
Survival and complication rates were similar in both groups Ina controlled but non-randomised study comparing cyanoacrylatewith sclerotherapy for gastric variceal bleeding Oho et al188
showed that the haemostasis rate was significantly higher in thecyanoacrylate group Survival was also significantly greater inpatients treated with cyanoacrylate
Mishra et al187 reported a randomised study comparingcyanoacrylate injection with β blockers in the prevention ofrebleeding in 67 patients with bleeding GOV-2 or IGV-1During a median 26-month follow-up patients in the cyano-acrylate group had significantly lower rates of both varicealrebleeding (15 vs 55) and mortality (3 vs 25)Treatment modality presence of portal hypertensive gastropathyand gastric variceal size gt20 mm correlated with mortalityAnother recent RCT compared repeated gastric variceal obtura-tion with or without NSBB in patients with bleeding GOV-2 orIGV-1182 Mortality and rebleeding rates were similar in the two
18 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

groups although adverse effects were more common in thecombination group
In a non-randomised study Lee et al185 suggested that endo-scopic ultrasound (EUS)-guided biweekly cyanoacrylate injectionversus lsquoon demandrsquo injection after recurrent bleeding led to sig-nificantly lower rebleeding (19 vs 45) from gastric varicesalthough survival was similar However others have not con-firmed this approach189 EUS-guided coil therapy has recentlybeen described as having similar efficacy but fewer adverseevents compared with cyanoacrylate injection in a small non-randomised study191
Binmoeller et al180 described a new method for the manage-ment of fundal gastric varices in 30 patients using EUS and acombination of 2-octyl-cyanoacrylate and coils Haemostasiswas achieved in 100 of patients with no procedure-relatedcomplications Use of coils appeared to reduce the volume ofcyanoacrylate required to obliterate varices
Endoscopic injection of thrombinInjection of bovine thrombin to successfully control gastric vari-ceal bleeding was initially described in a small cohort in1994195 Varices were eradicated in all patients after a mean oftwo injections Przemioslo et al196 reported 94 haemostasisand 18 rebleeding in 52 patients with gastric variceal bleedingtreated with bovine thrombin Ramesh et al197 also studiedbovine thrombin for bleeding gastric varices They reported92 haemostasis with no rebleeding during follow-up Noadverse events or technical problems were noted More recentstudies have used human rather than bovine thrombin becauseof safety concerns with the latter McAvoy et al198 reported onthe largest series of patients treated with human thrombin injec-tion for gastric or ectopic variceal bleeding They reported 11rebleeding in the 33 patients who had gastric variceal haemor-rhage with no significant adverse events A recent series bySmith et al199 reported a high rate of initial haemostasis in acutebleeding However failure to control bleeding or rebleeding wasreported in gt50 suggesting that thrombin has a role in bridg-ing to definitive treatment in acute bleeding Where thrombinwas used as prophylaxis rebleeding occurred in 20 To dateno randomised studies assessing thrombin injection for gastricvariceal bleeding have been reported
New endoscopic therapiesTwo recent reports have described the successful use ofHemospray (Cook Medical USA) in the management of activegastric variceal bleeding refractory to cyanoacrylate injectiontherapy200 201 In the latter case this was used as a bridge to aTIPSS procedure201 but in the former case TIPSS was notundertaken owing to pre-existing cardiomyopathy200 Norebleeding was reported in either case at a 30-day follow-upFurther data on the use of haemostatic powders in gastric vari-ceal bleeding are required
Balloon tamponadeInsertion of a SengstakenndashBlakemore or LintonndashNachlas tubemay sometimes help to temporarily stabilise the patient withsevere gastric variceal bleeding which is uncontrolled by stand-ard endoscopic methods as described above127 The LintonndashNachlas tube has been reported to have greater efficacy ingastric varices haemorrhage in a controlled trial128 Howeverrebleeding is almost universal if another treatment modality isnot instituted
Transjugular intrahepatic portosystemic stent-shuntAn initial TIPSS series using bare stents reported control ofactive bleeding from gastric varices in almost all patients inwhom the shunt was performed successfully202ndash206 Tripathiet al43 described 272 patients who had a TIPSS procedure foreither gastric or oesophageal variceal bleeding They reportedsimilar rebleeding rates after TIPSS for either gastric oroesophageal varices Initial PPG was lower in patients withbleeding from gastric varices In addition mortality was lowerin those patients with initial PPG gt12 mm Hg who had TIPSSfor gastric compared with oesophageal variceal bleeding Shuntinsufficiency and encephalopathy rates were similar in bothgroups The authors suggested aiming to reduce HVPG tolt7 mm Hg in gastric variceal bleeding
Lo et al207 undertook a randomised trial in 72 patients com-paring TIPSS with cyanoacrylate injection in the prevention ofgastric variceal rebleeding Control of active bleeding hadbeen achieved with cyanoacrylate in all patients before random-isation They reported a significantly lower rate of gastric vari-ceal rebleeding with TIPSS (11 vs 38) although overallupper gastrointestinal rebleeding was similar in both groupsEncephalopathy was more common in those patients treatedwith TIPSS (26 vs 3) but overall complications and survivalwere similar in both groups
A non-randomised study compared TIPSS with cyanoacrylateinjection for gastric variceal bleeding208 No differences were foundin haemostasis rebleeding or survival but the group treated withTIPSS had increased encephalopathy Another comparative studydescribed lower rebleeding with TIPSS but reduced in-patientlength of stay with cyanoacrylate and similar mortality209 Thisstudy also reported cyanoacrylate to be more cost-effective
Other radiological proceduresThe use of balloon-occluded retrograde transvenous obliteration(B-RTO) for the treatment of bleeding gastric varices was pio-neered by the Japanese184 210 This procedure involves insertionof a balloon catheter into an outflow shunt (gastrorenal orgastric-inferior vena caval) via the femoral or internal jugularvein Blood flow is blocked by balloon inflation then the veinsdraining gastric varices are embolised with microcoils and asclerosant injected to obliterate the varices
In a small randomised study B-RTO was compared withTIPSS in the management of 14 patients with active gastric vari-ceal bleeding and gastrorenal shunts211 Immediate haemostasisrebleeding and encephalopathy were similar in both groups In anon-randomised study of 27 high-risk patients Hong et al212
compared B-RTO with cyanoacrylate injection in acute gastricvariceal bleeding Active bleeding at baseline was more commonin the cyanoacrylate group Haemostasis rates after B-RTO andcyanoacrylate were similar at 77 and 100 Rebleeding washigher in the cyanoacrylate group (71 vs 15) with compli-cations and mortality similar in both groups This rebleedingrate after cyanoacrylate is much higher than figures reportedfrom other studies
A large Korean retrospective study evaluated B-RTO for themanagement of gastric variceal haemorrhage213 Technicalsuccess of B-RTO was 97 with procedure-related complica-tions seen in 4 and rebleeding in 22 Another retrospectivestudy of B-RTO for bleeding gastric varices described 95 tech-nical success and 50 5-year survival214 Cho et al215 assessedB-RTO in 49 patients who had gastric varices with spontaneousgastro-systemic shunts Procedural success rate was 84 but twoprocedure-related deaths occurred No variceal recurrence or
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 19
Guidelines
rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

rebleeding was noted It has been reported that B-RTO canincrease PPG and may aggravate pre-existing oesophagealvarices and ascites215 216 Although B-RTO appears to be aneffective alternative to TIPSS in patients with gastric varicealbleeding who have appropriate shunts217 it is rarely performedoutside Asian centres218
Percutaneous transhepatic variceal embolisation with cyano-acrylate and standard endoscopic cyanoacrylate injection have alsobeen compared in a non-randomised study of 77 patients219 Theauthors reported lower rebleeding with the percutaneousapproach although mortality was similar in both groups
SurgerySurgery for portal hypertension should be performed by experi-enced surgeons in lower-risk patients ideally in specialistunits220 Because of the increasing use of simpler endoscopicand radiological procedures as described above the need forsuch an intervention has reduced dramatically and is mainlyconfined to splenectomy or splenic artery embolisation inpatients with splenic vein thrombosis221 222
Under-running of gastric varices has been shown to controlactive bleeding but is followed by recurrence of bleeding in50 of patients and is associated with a perioperative mortalityof gt40223 Complete devascularisation of the cardia stomachand distal oesophagus for bleeding from gastric varices is asso-ciated with good control of bleeding but is followed by rebleed-ing in gt40 of patients and early mortality in about 50224
The use of distal splenorenal shunting for bleeding from gastricvarices in patients with cirrhosis was reported in six patientswith Child class A or B cirrhosis225 Although good control ofbleeding was attained two patients died in the postoperativeperiod Orloff et al169 reported that a portal-systemic shunt canbe an effective treatment for bleeding varices in patients withportal vein thrombosis and preserved liver function
Primary prophylaxis of gastric variceal bleedingA randomised study of 89 patients compared β blockers cyano-acrylate injection and no active treatment in the primary preven-tion of bleeding from larger (gt10 mm) GOV-2 and IGV-1226
Over a 26-month follow-up period bleeding occurred in 3810 and 53 of patients in the β blocker cyanoacrylate andno-treatment groups respectively The cyanoacrylate group hadsignificantly lower bleeding rates than the other groups forGOV-2 but not for IGV-1 patients Mortality was lower in thegroup treated with cyanoacrylate (7) than in those given notreatment (26) but was similar to that in the β blocker group(17) However this was a small single-centre study with anunusually high failure rate for NSBB Many clinicians have sig-nificant concerns about the safety of cyanoacrylate injection inthe context of primary prophylaxis
In a retrospective study Kang et al suggested that cyanoacryl-ate injection may be an effective prophylactic treatment forhigher-risk gastric varices227
A retrospective study evaluated the clinical outcomes ofB-RTO for gastric varices in which the procedure was per-formed as a primary prophylactic treatment in 40 patients228
The procedure was successful in 79 of patients although pro-cedural complications were reported in 9 Survival at 1 and 5years was 92 and 73 respectively
Recommendations management of active haemorrhage fromgastric varices (figure 3)1 What is the optimal management of bleeding gastro-
oesophageal varices
11 GOV-1 treat as for oesophageal varices (level 2bgrade B)
12 GOV-2 and IGV121 We recommend initial endoscopic therapy with
cyanoacrylate injection (level 1a grade A)122 Thrombin may also be considered (level 4 grade C)
13 TIPSS can be considered depending on local resourcesand clinical judgement (level 3a grade B)
2 In control of bleeding fails21 Balloon tamponade is suggested for GOV IGV-1 until
definitive treatment is undertaken (level 2b grade B)22 Salvage TIPSS is suggested as the first-line definite treat-
ment where feasible (level 3a grade B)23 B-RTO or surgical shunting can be considered if TIPSS
is not possible (eg portal vein thrombosis present) anddepending on local resources (level 3a grade B)
3 What are the therapeutic options for prevention of rebleed-ing from gastric varices31 We recommend that patients with GOV-1 are entered
into a VBL surveillance programme (level 2b grade B)32 We recommend endoscopic surveillance with cyano-
acrylate injection as needed for GOV-2 and IGV (notethe optimum endoscopic follow-up strategy remainsunclear)(level 2b grade B) Thrombin can also be con-sidered (level 4 grade C)
33 NSBB can be considered in certain circumstances aftertaking into account the patientrsquos preferences and clinicaljudgement (level 1b grade B)
34 We suggest TIPSS if patients rebleed despite cyanoacryl-ate injection TIPSS can also be considered in otherselected patients (eg those with large or multiple gastricvarices) (level 1b grade B)
35 Shunt surgery may be used in selected patients withwell-compensated cirrhosis and depending on localresources (level 3c grade B)
36 Splenectomy or splenic artery embolisation should beconsidered in all patients where there is splenic veinthrombosis or left-sided portal hypertension (level 4grade C)
4 Is there a role for primary prophylaxis of gastric varicealbleeding41 NSBB (level 2a grade B) can be considered in selected
high-risk patients with large GOV-2 after taking intoaccount the patientrsquos preferences and clinical judgement
42 Cyanoacrylate injection is not recommended outsideclinical trials (level 2a grade A)
5 Areas requiring further study51 Role of thrombin in gastric varices comparing this with
tissue adhesives in both acute gastric variceal bleedingand secondary prophylaxis
52 Role of TIPSS in acute gastric variceal bleeding and sec-ondary prophylaxis
53 Role of haemostatic powders in controlling refractoryactive gastric variceal bleeding
54 Role of NSBB in the prevention of rebleeding fromgastric varices
55 Role of B-RTO as monotherapy or in combination withendoscopic injection of tissue adhesives in prevention ofbleeding from gastric varices
56 Role of EUS-guided injection of tissue adhesives orthrombin
57 Primary prevention of gastric variceal bleeding withtissues adhesives and NSBB
20 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

Acknowledgements BSG Liver Section 2013ndash2015mdashin particular Dr GraceDolman trainee member of the BSG liver section for review of the guideline onbehalf of BSG liver section and Dr Stuart McPherson member of the BSG liversection for review of the guideline on behalf of the BSG liver section
Collaborators Mr Benedict Lowsley-Williams UK Patient representative Memberof guidelines development group Sister Kathy Guo research nurse UniversityHospitals Birmingham Birmingham UK Member of guidelines development group
Contributors DT consultant hepatologist University Hospitals BirminghamMember of BSG liver section Chair of GDG and lead author AJS consultantgastroenterologist Glasgow Royal Infirmary Coauthor of sections lsquoSecondaryprophylaxis of variceal haemorrhagersquo and lsquoGastric varicesrsquo Review of entireguideline PCH consultant hepatologist Royal Infirmary of Edinburgh Coauthor ofsections lsquoNatural history of varices in cirrhosisrsquo and lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline DP consultant hepatologist Royal FreeHospital London Coauthor of section lsquoManagement of active varicealhaemorrhagersquo Review of entire guideline CM consultant hepatologist The YorkHospital Member of BSG liver section Coauthor of section lsquoManagement of activevariceal haemorrhagersquo Review of entire guideline HM consultant interventionalradiologist University Hospitals Birmingham Coauthor of sections lsquoService deliveryand developmentrsquo and lsquoManagement of active variceal haemorrhagersquo in relation toTIPSS AA consultant hepatologist Royal Derby Hospital Derby Chair of BSG liversection Contribution to sections lsquoSecondary prophylaxis of variceal haemorrhagersquoand lsquoGastric varicesrsquo Review of entire guideline JWF consultant hepatologistUniversity Hospitals Birmingham Clinical lead of Liver QuEST Development ofquality indicators and implementation through Liver QuEST SPO consultantinterventional radiologist University Hospitals Birmingham Review of entireguideline with focus on radiological aspects MH consultant hepatologist TheFreeman Hospital Newcastle Member of BSG liver section and BASL Review ofentire guideline JMC consultant gastroenterologist Royal Devon and ExeterHospital Member of BSG liver section Review of entire guideline BenedictLowsley-Williams patient representative Advice given relating to patient aspectsSister Kathy Guo RGN research nurse University Hospitals Birmingham Nursingrepresentative Advice given relating to nursing aspects
Funding This guideline was commissioned by Clinical Services and StandardsCommittee (CSSC) of the British Society of Gastroenterology (BSG) under theauspices of the liver section of the BSG
Competing interests DT speaker fees for Gore Medical AA educational grantfrom Ferring Pharmaceuticals PCH speaker fees for Gore Medical SPO speakerfees for Gore Medical DP involvement in NICE guidelines on Acute GI Bleeding
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 de Franchis R Revising consensus in portal hypertension report of the Baveno V
consensus workshop on methodology of diagnosis and therapy in portalhypertension J Hepatol 201053762ndash8
2 Acute upper gastrointestinal bleeding management NICE 2012 httpwwwniceorgukGuidanceCG141
3 Brouwers MC Kho ME Browman GP et al AGREE II advancing guidelinedevelopment reporting and evaluation in health care CMAJ 2010182E839ndash42
4 Centre for evidence-based medicine Oxford Oxford University 20095 Jairath V Rehal S Logan R et al Acute variceal haemorrhage in the United
Kingdom patient characteristics management and outcomes in a nationwideaudit Dig Liver Dis 201446419ndash26
6 Garcia-Pagan JC Caca K Bureau C et al Early use of TIPS in patients withcirrhosis and variceal bleeding N Engl J Med 20103622370ndash9
7 Measuring the Units A review of patients who died with alcohol-related liverdisease NCEPOD 2013 httpwwwncepodorguk2013report1downloadsMeasuring20the20Units_full20reportpdf
8 Hobolth L Krag A Malchow-Moller A et al Adherence to guidelines in bleedingoesophageal varices and effects on outcome comparison between a specializedunit and a community hospital Eur J Gastroenterol Hepatol 2010221221ndash7
9 Schlansky B Lee B Hartwell L et al Guideline adherence and outcomes inesophageal variceal hemorrhage comparison of tertiary care and non-tertiary caresettings J Clin Gastroenterol 201246235ndash42
10 Krajina A Hulek P Fejfar T et al Quality improvement guidelines for transjugularintrahepatic portosystemic shunt (TIPS) Cardiovasc Intervent Radiol2012351295ndash300
11 Scope for improvement a toolkit for a safer upper gastrointestinal bleeding (UGIB)service 2011 httpwww aomrc org ukdoc_download9338-upper-gastrointestinal-bleeding-toolkit
12 McPherson S Dyson J Austin A et al Response to the NCEPOD report developmentof a care bundle for patients admitted with decompensated cirrhosismdashthe first 24 hFrontline Gastroenterology Published Online First 2 Dec 2014 doi101136flgastro-2014-100491
13 Darzi A High quality care for all NHS Next Stage Review final report LondonDoH 2008
14 Liver Quality Enhancement Service Tool (QuEST) 2015 httpwww liverquest org uk15 [No authors listed] Tackling liver disease in the UK a Lancet Commission Lancet
2014384190216 Thabut D Rudler M Dib N et al Multicenter prospective validation of the Baveno
IV and Baveno IIIII criteria in cirrhosis patients with variceal bleeding Hepatology2015611024ndash32
17 Ahn SY Park SY Tak WY et al Prospective validation of Baveno V definitions andcriteria for failure to control bleeding in portal hypertension Hepatology2015611033ndash40
18 Christensen E Fauerholdt L Schlichting P et al Aspects of the natural history ofgastrointestinal bleeding in cirrhosis and the effect of prednisone Gastroenterology198181944ndash52
19 Cales P Pascal JP [Natural history of esophageal varices in cirrhosis (from originto rupture)] Gastroenterol Clin Biol 198812245ndash54
20 Czaja AJ Wolf AM Summerskill WH Development and early prognosis ofesophageal varices in severe chronic active liver disease (CALD) treated withprednisone Gastroenterology 197977(4 Pt 1)629ndash33
21 Merli M Nicolini G Angeloni S et al Incidence and natural history of smallesophageal varices in cirrhotic patients J Hepatol 200338266ndash72
22 DrsquoAmico G Pasta L Morabito A et al Competing risks and prognostic stages ofcirrhosis a 25-year inception cohort study of 494 patients Aliment PharmacolTher 2014391180ndash93
23 Baker LA Smith C Lieberman G The natural history of esophageal varices astudy of 115 cirrhotic patients in whom varices were diagnosed prior to bleedingAm J Med 195926228ndash37
24 Dagradi AE The natural history of esophageal varices in patients with alcoholicliver cirrhosis An endoscopic and clinical study Am J Gastroenterol197257520ndash40
25 Ohnishi K Sato S Saito M et al Clinical and portal hemodynamic features incirrhotic patients having a large spontaneous splenorenal andor gastrorenal shuntAm J Gastroenterol 198681450ndash5
26 Takashi M Igarashi M Hino S et al Portal hemodynamics in chronic portal-systemic encephalopathy Angiographic study in seven cases J Hepatol19851467ndash76
27 Groszmann RJ Garcia-Tsao G Bosch J et al Beta-blockers to preventgastroesophageal varices in patients with cirrhosis N Engl J Med20053532254ndash61
28 Chung JW Park S Chung MJ et al A novel disposable transnasalesophagoscope a pilot trial of feasibility safety and tolerance Endoscopy201244206ndash9
29 Choe WH Kim JH Ko SY et al Comparison of transnasal small-caliber vs peroralconventional esophagogastroduodenoscopy for evaluating varices in unsedatedcirrhotic patients Endoscopy 201143649ndash56
30 de Franchis R Eisen GM Laine L et al Esophageal capsule endoscopy forscreening and surveillance of esophageal varices in patients with portalhypertension Hepatology 2008471595ndash603
31 Lapalus MG Ben Soussan E Gaudric M et al Esophageal capsule endoscopy vsEGD for the evaluation of portal hypertension a French prospective multicentercomparative study Am J Gastroenterol 20091041112ndash18
32 Vizzutti F Arena U Romanelli RG et al Liver stiffness measurement predictssevere portal hypertension in patients with HCV-related cirrhosis Hepatology2007451290ndash7
33 Castera L Le Bail B Roudot-Thoraval F et al Early detection in routine clinicalpractice of cirrhosis and oesophageal varices in chronic hepatitis C comparison oftransient elastography (FibroScan) with standard laboratory tests and non-invasivescores J Hepatol 20095059ndash68
34 Robic MA Procopet B Metivier S et al Liver stiffness accurately predicts portalhypertension related complications in patients with chronic liver diseasea prospective study J Hepatol 2011551017ndash24
35 Giannini EG Zaman A Kreil A et al Platelet countspleen diameter ratio for thenoninvasive diagnosis of esophageal varices results of a multicenter prospectivevalidation study Am J Gastroenterol 20061012511ndash19
36 Chawla S Katz A Attar BM et al Platelet countspleen diameter ratio to predictthe presence of esophageal varices in patients with cirrhosis a systematic reviewEur J Gastroenterol Hepatol 201224431ndash6
37 MacDougall BR Westaby D Theodossi A et al Increased long-term survival invariceal haemorrhage using injection sclerotherapy Results of a controlled trialLancet 19821124ndash7
38 Dawson J Gertsch P Mosimann F et al Endoscopic variceal pressuremeasurements response to isosorbide dinitrate Gut 198526843ndash7
39 Garcia-Tsao G Groszmann RJ Fisher RL et al Portal pressure presenceof gastroesophageal varices and variceal bleeding Hepatology 19855419ndash24
40 Lebrec D De Fleury P Rueff B et al Portal hypertension size of esophagealvarices and risk of gastrointestinal bleeding in alcoholic cirrhosis Gastroenterology1980791139ndash44
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 21
Guidelines
41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

41 Groszmann RJ Bosch J Grace ND et al Hemodynamic events in a prospectiverandomized trial of propranolol versus placebo in the prevention of a first varicealhemorrhage Gastroenterology 1990991401ndash7
42 Feu F Garcia-Pagan JC Bosch J et al Relation between portal pressure responseto pharmacotherapy and risk of recurrent variceal haemorrhage in patients withcirrhosis Lancet 19953461056ndash9
43 Tripathi D Therapondos G Jackson E et al The role of the transjugularintrahepatic portosystemic stent shunt (TIPSS) in the management of bleedinggastric varices clinical and haemodynamic correlations Gut 200251270ndash4
44 Vinel JP Cassigneul J Levade M et al Assessment of short-term prognosis aftervariceal bleeding in patients with alcoholic cirrhosis by early measurement ofportohepatic gradient Hepatology 19866116ndash17
45 Palmer ED Brick IB Correlation between the severity of esophageal varices inportal cirrhosis and their propensity toward hemorrhage Gastroenterology19563085ndash90
46 Polio J Groszmann RJ Hemodynamic factors involved in the development andrupture of esophageal varices a pathophysiologic approach to treatment SeminLiver Dis 19866318ndash31
47 Vegesna AK Chung CY Bajaj A et al Minimally invasive measurement ofesophageal variceal pressure and wall tension (with video) Gastrointest Endosc200970407ndash13
48 Beppu K Inokuchi K Koyanagi N et al Prediction of variceal hemorrhage byesophageal endoscopy Gastrointest Endosc 198127213ndash18
49 North Italian Endoscopic Club for the Study and Treatment of Esophageal VaricesPrediction of the first variceal hemorrhage in patients with cirrhosis of the liverand esophageal varices A prospective multicenter study N Engl J Med1988319983ndash9
50 Inokuchi K Improved survival after prophylactic portal nondecompression surgeryfor esophageal varices a randomized clinical trial Cooperative Study Group ofPortal Hypertension of Japan Hepatology 1990121ndash6
51 de Franchis R Primignani M Arcidiacono PG et al Prophylactic sclerotherapy inhigh-risk cirrhotics selected by endoscopic criteria A multicenter randomizedcontrolled trial Gastroenterology 19911011087ndash93
52 Feu F Ruiz del Arbol L Banares R et al Double-blind randomized controlled trialcomparing terlipressin and somatostatin for acute variceal hemorrhage VaricealBleeding Study Group Gastroenterology 19961111291ndash9
53 Merkel C Bolognesi M Bellon S et al Prognostic usefulness of hepatic veincatheterization in patients with cirrhosis and esophageal varices Gastroenterology1992102973ndash9
54 Villanueva C Aracil C Colomo A et al Acute hemodynamic response to beta-blockers and prediction of long-term outcome in primary prophylaxis of varicealbleeding Gastroenterology 2009137119ndash28
55 Stokkeland K Brandt L Ekbom A et al Improved prognosis for patientshospitalized with esophageal varices in Sweden 1969ndash2002 Hepatology200643500ndash5
56 [No authors listed] Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients Final report of a multicenter randomized trial The ItalianMulticenter Project for Propranolol in Prevention of Bleeding (IMPP) J Hepatol1989975ndash83
57 Conn HO Grace ND Bosch J et al Propranolol in the prevention of the firsthemorrhage from esophagogastric varices a multicenter randomized clinical trialThe Boston-New Haven-Barcelona Portal Hypertension Study Group Hepatology199113902ndash12
58 Ideo G Bellati G Fesce E et al Nadolol can prevent the first gastrointestinalbleeding in cirrhotics a prospective randomized study Hepatology 198886ndash9
59 Lebrec D Poynard T Capron JP et al Nadolol for prophylaxis of gastrointestinalbleeding in patients with cirrhosis A randomized trial J Hepatol 19887118ndash25
60 Pascal JP Cales P Propranolol in the prevention of first upper gastrointestinal tracthemorrhage in patients with cirrhosis of the liver and esophageal varices N Engl JMed 1987317856ndash61
61 Cales P Oberti F Payen JL et al Lack of effect of propranolol in the prevention oflarge oesophageal varices in patients with cirrhosis a randomized trial French-Speaking Club for the Study of Portal Hypertension Eur J Gastroenterol Hepatol199911741ndash5
62 Merkel C Marin R Angeli P et al A placebo-controlled clinical trial of nadolol inthe prophylaxis of growth of small esophageal varices in cirrhosisGastroenterology 2004127476ndash84
63 Sarin SK Misra SR Sharma P et al Early primary prophylaxis with beta-blockersdoes not prevent the growth of small esophageal varices in cirrhosisa randomized controlled trial Hepatol Intl 20137248ndash56
64 Conn HO Lindenmuth WW Prophylactic portacaval anastomosis in cirrhoticpatients with esophageal varices a progress report of a continuing study N Engl JMed 19652721255ndash63
65 Conn HO Lindenmuth WW May CJ et al Prophylactic portacaval anastomosisMedicine (Baltimore) 19725127ndash40
66 Jackson FC Perrin EB Smith AG et al A clinical investigation of the portacavalshunt II Survival analysis of the prophylactic operation Am J Surg196811522ndash42
67 Resnick RH Chalmers TC Ishihara AM et al A controlled study of theprophylactic portacaval shunt A final report Ann Intern Med 196970675ndash88
68 DrsquoAmico G Pagliaro L Bosch J The treatment of portal hypertension a meta-analytic review Hepatology 199522332ndash54
69 Garcia-Tsao G Grace ND Groszmann RJ et al Short-term effects of propranololon portal venous pressure Hepatology 19866101ndash6
70 La Mura V Abraldes JG Raffa S et al Prognostic value of acute hemodynamicresponse to iv propranolol in patients with cirrhosis and portal hypertensionJ Hepatol 200951279ndash87
71 Cheng JW Zhu L Gu MJ et al Meta analysis of propranolol effects ongastrointestinal hemorrhage in cirrhotic patients World J Gastroenterol200391836ndash9
72 Banares R Moitinho E Matilla A et al Randomized comparison of long-termcarvedilol and propranolol administration in the treatment of portal hypertension incirrhosis Hepatology 2002361367ndash73
73 Hobolth L Moller S Gronbaek H et al Carvedilol or propranolol in portalhypertension A randomized comparison Scand J Gastroenterol 201247467ndash74
74 Reiberger T Ulbrich G Ferlitsch A et al Carvedilol for primary prophylaxis ofvariceal bleeding in cirrhotic patients with haemodynamic non-response topropranolol Gut 2013621634ndash41
75 Tripathi D Ferguson JW Kochar N et al Randomized controlled trial of carvedilolversus variceal band ligation for the prevention of the first variceal bleedHepatology 200950825ndash33
76 Shah HA Azam Z Rauf J et al Carvedilol vs esophageal variceal band ligation inthe primary prophylaxis of variceal hemorrhage a multicentre randomizedcontrolled trial J Hepatol 201460757ndash64
77 Serste T Melot C Francoz C et al Deleterious effects of beta-blockers onsurvival in patients with cirrhosis and refractory ascites Hepatology2010521017ndash22
78 Krag A Wiest R Albillos A et al The window hypothesis haemodynamic andnon-haemodynamic effects of beta-blockers improve survival of patients withcirrhosis during a window in the disease Gut 201261967ndash9
79 Leithead JA Rajoriya N Tehami N et al Non-selective beta-blockers areassociated with improved survival in patients with ascites listed for livertransplantation Gut 2014 Published Online First 3 Oct 2014Doi101136gutjnl-2013-306502
80 Mandorfer M Bota S Schwabl P et al Nonselective beta blockers increase riskfor hepatorenal syndrome and death in patients with cirrhosis and spontaneousbacterial peritonitis Gastroenterology 20141461680ndash90
81 Navasa M Chesta J Bosch J et al Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis Effects on splanchnic and systemichemodynamics and liver function Gastroenterology 1989961110ndash18
82 Angelico M Carli L Piat C et al Isosorbide-5-mononitrate versus propranolol inthe prevention of first bleeding in cirrhosis Gastroenterology 19931041460ndash5
83 Garcia-Pagan JC Isosorbide-5-monitrate (ISMN) vs placebo (PLA) in the preventionof the first variceal bleeding (FVB) in patients with contraindications or intoleranceto beta-blockers J Hepatol 20003228
84 Merkel C Marin R Enzo E et al Randomised trial of nadolol alone or with isosorbidemononitrate for primary prophylaxis of variceal bleeding in cirrhosis Gruppo-Trivenetoper Lrsquoipertensione portale (GTIP) Lancet 19963481677ndash81
85 Garcia-Pagan JC Morillas R Banares R et al Propranolol plus placebo versuspropranolol plus isosorbide-5-mononitrate in the prevention of a first varicealbleed a double-blind RCT Hepatology 2003371260ndash6
86 Hidaka H Nakazawa T Wang G et al Long-term administration of PPI reducestreatment failures after esophageal variceal band ligation a randomized controlledtrial J Gastroenterol 201247118ndash26
87 Min YW Lim KS Min BH et al Proton pump inhibitor use significantly increasesthe risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis andascites a propensity score matched cohort study Aliment Pharmacol Ther201440695ndash704
88 Terg R Casciato P Garbe C et al Proton pump inhibitor therapy doesnot increase the incidence of spontaneous bacterial peritonitis in cirrhosisa multicenter prospective study J Hepatol 2014 Doi101016jjhep201411036
89 Dultz G Piiper A Zeuzem S et al Proton pump inhibitor treatment is associatedwith the severity of liver disease and increased mortality in patients with cirrhosisAliment Pharmacol Ther 201541459ndash66
90 Janarthanan S Ditah I Adler DG et al Clostridium difficile-associated diarrheaand proton pump inhibitor therapy a meta-analysis Am J Gastroenterol20121071001ndash10
91 Gluud LL Krag A Banding ligation versus beta-blockers for primary prevention inoesophageal varices in adults Cochrane Database Syst Rev 20128CD004544
92 Funakoshi N Duny Y Valats JC et al Meta-analysis beta-blockers versus bandingligation for primary prophylaxis of esophageal variceal bleeding Ann Hepatol201211369ndash83
93 Debernardi VW Elia C Stradella D et al Prospective randomized trial endoscopicfollow up 3 vs 6 months after esophageal variceal eradication by band ligation incirrhosis Eur J Intern Med 201425674ndash9
22 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

94 Avgerinos A Armonis A Manolakopoulos S et al Endoscopic sclerotherapy pluspropranolol versus propranolol alone in the primary prevention of bleeding in highrisk cirrhotic patients with esophageal varices a prospective multicenterrandomized trial Gastrointest Endosc 200051652ndash8
95 Gotoh Y Iwakiri R Sakata Y et al Evaluation of endoscopic variceal ligation inprophylactic therapy for bleeding of oesophageal varices a prospective controlledtrial compared with endoscopic injection sclerotherapy J Gastroenterol Hepatol199914241ndash4
96 Masumoto H Toyonaga A Oho K et al Ligation plus low-volume sclerotherapyfor high-risk esophageal varices comparisons with ligation therapy orsclerotherapy alone J Gastroenterol 1998331ndash5
97 Graham DY Smith JL The course of patients after variceal hemorrhageGastroenterology 198180800ndash9
98 Kamath PS Wiesner RH Malinchoc M et al A model to predict survival inpatients with end-stage liver disease Hepatology 200133464ndash70
99 DrsquoAmico G de Franchis R Upper digestive bleeding in cirrhosis Post-therapeuticoutcome and prognostic indicators Hepatology 200338599ndash612
100 Abraldes JG Villanueva C Banares R et al Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated with pharmacologic andendoscopic therapy J Hepatol 200848229ndash36
101 Bambha K Kim WR Pedersen R et al Predictors of early re-bleeding andmortality after acute variceal haemorrhage in patients with cirrhosis Gut200857814ndash20
102 Hunter SS Hamdy S Predictors of early re-bleeding and mortality after acutevariceal haemorrhage Arab J Gastroenterol 20131463ndash7
103 Reverter E Tandon P Augustin S et al A MELD-based model to determine risk ofmortality among patients with acute variceal bleeding Gastroenterology2014146412ndash19
104 Al Freah MA Gera A Martini S et al Comparison of scoring systems andoutcome of patients admitted to a liver intensive care unit of a tertiary referralcentre with severe variceal bleeding Aliment Pharmacol Ther 2014391286ndash300
105 Chen PH Chen WC Hou MC et al Delayed endoscopy increases re-bleeding andmortality in patients with hematemesis and active esophageal variceal bleedinga cohort study J Hepatol 2012571207ndash13
106 Villanueva C Colomo A Bosch A et al Transfusion strategies for acute uppergastrointestinal bleeding N Engl J Med 201336811ndash21
107 Scalea TM Holman M Fuortes M et al Central venous blood oxygen saturationan early accurate measurement of volume during hemorrhage J Trauma198828725ndash32
108 Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med2011365147ndash56
109 Bendtsen F DrsquoAmico G Rusch E et al Effect of recombinant Factor VIIa onoutcome of acute variceal bleeding an individual patient based meta-analysis oftwo controlled trials J Hepatol 201461252ndash9
110 Wells M Chande N Adams P et al Meta-analysis vasoactive medications forthe management of acute variceal bleeds Aliment Pharmacol Ther 2012351267ndash78
111 Seo YS Park SY Kim MY et al Lack of difference among terlipressinsomatostatin and octreotide in the control of acute gastroesophageal varicealhemorrhage Hepatology 201460954ndash63
112 Groszmann RJ Kravetz D Bosch J et al Nitroglycerin improves the hemodynamicresponse to vasopressin in portal hypertension Hepatology 19822757ndash62
113 Ioannou G Doust J Rockey DC Terlipressin for acute esophageal varicealhemorrhage Cochrane Database Syst Rev 2003(1)CD002147
114 Azam Z Hamid S Jafri W et al Short course adjuvant terlipressin in acutevariceal bleeding a randomized double blind dummy controlled trial J Hepatol201256819ndash24
115 Bosch J Kravetz D Rodes J Effects of somatostatin on hepatic and systemichemodynamics in patients with cirrhosis of the liver comparison with vasopressinGastroenterology 198180518ndash25
116 Chavez-Tapia NC Barrientos-Gutierrez T Tellez-Avila F et al Meta-analysisantibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleedingmdashan updated Cochrane review Aliment Pharmacol Ther 201134509ndash18
117 Fernandez J Ruiz del Arbol L Gomez C et al Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhageGastroenterology 20061311049ndash56
118 Lo GH Perng DS Chang CY et al Controlled trial of ligation plus vasoconstrictorversus proton pump inhibitor in the control of acute esophageal variceal bleedingJ Gastroenterol Hepatol 201328684ndash9
119 Cheung J Soo I Bastiampillai R et al Urgent vs non-urgent endoscopy in stableacute variceal bleeding Am J Gastroenterol 20091041125ndash9
120 Van Stiegmann G Goff JS Endoscopic esophageal varix ligation preliminaryclinical experience Gastrointest Endosc 198834113ndash17
121 Laine L Cook D Endoscopic ligation compared with sclerotherapy for treatmentof esophageal variceal bleeding A meta-analysis Ann Intern Med1995123280ndash7
122 Ljubicic N Biscanin A Nikolic M et al A randomized-controlled trial of endoscopictreatment of acute esophageal variceal hemorrhage N-butyl-2-cyanoacrylateinjection vs variceal ligation Hepatogastroenterology 201158438ndash43
123 Ibrahim M El Mikkawy A Mostafa I et al Endoscopic treatment of acute varicealhemorrhage by using hemostatic powder TC-325 a prospective pilot studyGastrointest Endosc 201378769ndash73
124 Banares R Albillos A Rincon D et al Endoscopic treatment versus endoscopicplus pharmacologic treatment for acute variceal bleeding a meta-analysisHepatology 200235609ndash15
125 Lo GH Lai KH Cheng JS et al Emergency banding ligation versus sclerotherapyfor the control of active bleeding from esophageal varices Hepatology1997251101ndash4
126 Villanueva C Piqueras M Aracil C et al A randomized controlled trial comparingligation and sclerotherapy as emergency endoscopic treatment added tosomatostatin in acute variceal bleeding J Hepatol 200645560ndash7
127 Panes J Teres J Bosch J et al Efficacy of balloon tamponade in treatment ofbleeding gastric and esophageal varices Results in 151 consecutive episodesDig Dis Sci 198833454ndash9
128 Teres J Cecilia A Bordas JM et al Esophageal tamponade for bleeding varicesControlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlastube Gastroenterology 197875566ndash9
129 Dechene A El Fouly AH Bechmann LP et al Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents Digestion201285185ndash91
130 Wright G Lewis H Hogan B et al A self-expanding metal stent for complicatedvariceal hemorrhage experience at a single center Gastrointest Endosc 20107171ndash8
131 Vangeli M Patch D Burroughs AK Salvage tips for uncontrolled variceal bleedingJ Hepatol 200237703ndash4
132 Rosemurgy AS Frohman HA Teta AF et al Prosthetic H-graft portacaval shunts vstransjugular intrahepatic portasystemic stent shunts 18-year follow-up of arandomized trial J Am Coll Surg 2012214445ndash53
133 Orloff MJ Vaida F Haynes KS et al Randomized controlled trial of emergencytransjugular intrahepatic portosystemic shunt versus emergency portacaval shunttreatment of acute bleeding esophageal varices in cirrhosis J Gastrointest Surg2012162094ndash111
134 Bureau C Pagan JC Layrargues GP et al Patency of stents covered withpolytetrafluoroethylene in patients treated by transjugular intrahepaticportosystemic shunts long-term results of a randomized multicentre study Liver Int200727742ndash7
135 Perarnau JM Le Gouge A Nicolas C et al Covered vs uncovered stents fortransjugular intrahepatic portosystemic shunt a randomized controlled trialJ Hepatol 201460962ndash8
136 Monescillo A Martinez-Lagares F Ruiz-del-Arbol L et al Influence of portalhypertension and its early decompression by TIPS placement on the outcome ofvariceal bleeding Hepatology 200440793ndash801
137 Garcia-Pagan JC Di Pascoli M Caca K et al Use of early-TIPS for high-riskvariceal bleeding results of a post-RCT surveillance study J Hepatol20135845ndash50
138 Rudler M Cluzel P Corvec TL et al Early-TIPSS placement prevents rebleeding inhigh-risk patients with variceal bleeding without improving survival AlimentPharmacol Ther 2014401074ndash80
139 Gatta A Merkel C Sacerdoti D et al Nadolol for prevention of variceal rebleedingin cirrhosis a controlled clinical trial Digestion 19873722ndash8
140 DrsquoAmico G Pagliaro L Bosch J Pharmacological treatment of portal hypertensionan evidence-based approach Semin Liver Dis 199919475ndash505
141 Gournay J Masliah C Martin T et al Isosorbide mononitrate and propranololcompared with propranolol alone for the prevention of variceal rebleedingHepatology 2000311239ndash45
142 Gluud LL Langholz E Krag A Meta-analysis isosorbide-mononitrate alone or witheither beta-blockers or endoscopic therapy for the management of oesophagealvarices Aliment Pharmacol Ther 201032859ndash71
143 Lo GH Chen WC Wang HM et al Randomized controlled trial of carvedilolversus nadolol plus isosorbide mononitrate for the prevention of varicealrebleeding J Gastroenterol Hepatol 2012271681ndash7
144 Abraldes JG Villanueva C Aracil C et al Addition of simvastatin to standardtreatment improves survival after variceal bleeding in patients with cirrhosisA double-blind randomized trial J Hepatol 201460S525
145 Shaheen NJ Stuart E Schmitz SM et al Pantoprazole reduces the size ofpostbanding ulcers after variceal band ligation a randomized controlled trialHepatology 200541588ndash94
146 de Franchis R Primignani M Endoscopic treatments for portal hypertensionSemin Liver Dis 199919439ndash55
147 Laine L Ligation endoscopic treatment of choice for patients with bleedingesophageal varices Hepatology 199522663ndash5
148 Wang HM Lo GH Chen WC et al Randomized controlled trial of monthly versusbiweekly endoscopic variceal ligation for the prevention of esophageal varicealrebleeding J Gastroenterol Hepatol 2014291229ndash36
149 Karsan HA Morton SC Shekelle PG et al Combination endoscopic band ligationand sclerotherapy compared with endoscopic band ligation alone for thesecondary prophylaxis of esophageal variceal hemorrhage a meta-analysis Dig DisSci 200550399ndash406
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 23
Guidelines
150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

150 Singh P Pooran N Indaram A et al Combined ligation and sclerotherapy versusligation alone for secondary prophylaxis of esophageal variceal bleeding a meta-analysis Am J Gastroenterol 200297623ndash9
151 Lo GH Chen WC Chen MH et al Banding ligation versus nadolol and isosorbidemononitrate for the prevention of esophageal variceal rebleeding Gastroenterology2002123728ndash34
152 Lo GH Chen WC Lin CK et al Improved survival in patients receiving medicaltherapy as compared with banding ligation for the prevention of esophagealvariceal rebleeding Hepatology 200848580ndash7
153 Patch D Sabin CA Goulis J et al A randomized controlled trial of medicaltherapy versus endoscopic ligation for the prevention of variceal rebleeding inpatients with cirrhosis Gastroenterology 20021231013ndash19
154 Romero G Kravetz D Argonz J et al Comparative study between nadolol and5-isosorbide mononitrate vs endoscopic band ligation plus sclerotherapy in theprevention of variceal rebleeding in cirrhotic patients a randomized controlledtrial Aliment Pharmacol Ther 200624601ndash11
155 Stanley AJ Dickson S Hayes PC et al Multicentre randomised controlled studycomparing carvedilol with variceal band ligation in the prevention of varicealrebleeding J Hepatol 2014611014ndash19
156 Li L Yu C Li Y Endoscopic band ligation versus pharmacological therapy for varicealbleeding in cirrhosis a meta-analysis Can J Gastroenterol 201125147ndash55
157 Cheung J Zeman M van Zanten SV et al Systematic review secondaryprevention with band ligation pharmacotherapy or combination therapy afterbleeding from oesophageal varices Aliment Pharmacol Ther 200930577ndash88
158 Ding SH Liu J Wang JP Efficacy of beta-adrenergic blocker plus 5-isosorbidemononitrate and endoscopic band ligation for prophylaxis of esophageal varicealrebleeding a meta-analysis World J Gastroenterol 2009152151ndash5
159 Ravipati M Katragadda S Swaminathan PD et al Pharmacotherapy plusendoscopic intervention is more effective than pharmacotherapy or endoscopyalone in the secondary prevention of esophageal variceal bleeding a meta-analysisof randomized controlled trials Gastrointest Endosc 200970658ndash64
160 Gonzalez R Zamora J Gomez-Camarero J et al Meta-analysis combinationendoscopic and drug therapy to prevent variceal rebleeding in cirrhosis Ann InternMed 2008149109ndash22
161 Funakoshi N Segalas-Largey F Duny Y et al Benefit of combination beta-blockerand endoscopic treatment to prevent variceal rebleeding a meta-analysis World JGastroenterol 2010165982ndash92
162 Thiele M Krag A Rohde U et al Meta-analysis banding ligation and medicalinterventions for the prevention of rebleeding from oesophageal varices AlimentPharmacol Ther 2012351155ndash65
163 Puente A Hernaacutendez-Gea V Graupera I et al Drugs plus ligation to preventrebleeding in cirrhosis an updated systematic review Liver Int 201434823ndash33
164 Luca A DrsquoAmico G La Galla R et al TIPS for prevention of recurrent bleeding inpatients with cirrhosis meta-analysis of randomized clinical trials Radiology1999212411ndash21
165 Papatheodoridis GV Goulis J Leandro G et al Transjugular intrahepaticportosystemic shunt compared with endoscopic treatment for prevention of varicealrebleeding a meta-analysis Hepatology 199930612ndash22
166 Zheng M Chen Y Bai J et al Transjugular intrahepatic portosystemic shunt versusendoscopic therapy in the secondary prophylaxis of variceal rebleeding in cirrhoticpatients meta-analysis update J Clin Gastroenterol 200842507ndash16
167 Garcia-Villarreal L Martinez-Lagares F Sierra A et al Transjugular intrahepaticportosystemic shunt versus endoscopic sclerotherapy for the prevention of varicealrebleeding after recent variceal hemorrhage Hepatology 19992927ndash32
168 Qi X Liu L Bai M et al Transjugular intrahepatic portosystemic shunt incombination with or without variceal embolization for the prevention of varicealrebleeding a meta-analysis J Gastroenterol Hepatol 201429688ndash96
169 Orloff MJ Isenberg JI Wheeler HO et al Liver transplantation in a randomizedcontrolled trial of emergency treatment of acutely bleeding esophageal varices incirrhosis Transplant Proc 2010424101ndash8
170 Henderson JM Boyer TD Kutner MH et al Distal splenorenal shunt versustransjugular intrahepatic portal systematic shunt for variceal bleedinga randomized trial Gastroenterology 20061301643ndash51
171 Boyer TD Henderson JM Heerey AM et al Cost of preventing variceal rebleedingwith transjugular intrahepatic portal systemic shunt and distal splenorenal shuntJ Hepatol 200848407ndash14
172 Khan S Tudur SC Williamson P et al Portosystemic shunts versus endoscopictherapy for variceal rebleeding in patients with cirrhosis Cochrane Database SystRev 2006(4)CD000553
173 Zhou J Wu Z Wu J et al Transjugular intrahepatic portosystemic shunt (TIPS)versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation(EVL) in the treatment of recurrent variceal bleeding Surg Endosc2013272712ndash20
174 Neuberger J Gimson A Davies M et al Selection of patients for livertransplantation and allocation of donated livers in the UK Gut 200857252ndash7
175 Sarin SK Lahoti D Saxena SP et al Prevalence classification and natural historyof gastric varices a long-term follow-up study in 568 portal hypertension patientsHepatology 1992161343ndash9
176 Trudeau W Prindiville T Endoscopic injection sclerosis in bleeding gastric varicesGastrointest Endosc 198632264ndash8
177 Gimson AE Westaby D Williams R Endoscopic sclerotherapy in the managementof gastric variceal haemorrhage J Hepatol 199113274ndash8
178 Harada T Yoshida T Shigemitsu T et al Therapeutic results of endoscopic varicealligation for acute bleeding of oesophageal and gastric varices J GastroenterolHepatol 199712331ndash5
179 Takeuchi M Nakai Y Syu A et al Endoscopic ligation of gastric varices Lancet19963481038
180 Binmoeller KF Weilert F Shah JN et al EUS-guided transesophageal treatment ofgastric fundal varices with combined coiling and cyanoacrylate glue injection (withvideos) Gastrointest Endosc 2011741019ndash25
181 Cheng LF Wang ZQ Li CZ et al Low incidence of complications from endoscopicgastric variceal obturation with butyl cyanoacrylate Clin Gastroenterol Hepatol20108760ndash6
182 Hung HH Chang CJ Hou MC et al Efficacy of non-selective beta-blockers asadjunct to endoscopic prophylactic treatment for gastric variceal bleedinga randomized controlled trial J Hepatol 2012561025ndash32
183 Kahloon A Chalasani N Dewitt J et al Endoscopic therapy with 2-octyl-cyanoacrylate for the treatment of gastric varices Dig Dis Sci 2014592178ndash83
184 Kanagawa H Mima S Kouyama H et al Treatment of gastric fundal varices byballoon-occluded retrograde transvenous obliteration J Gastroenterol Hepatol19961151ndash8
185 Lee YT Chan FK Ng EK et al EUS-guided injection of cyanoacrylate for bleedinggastric varices Gastrointest Endosc 200052168ndash74
186 Lo GH Lai KH Cheng JS et al A prospective randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices Hepatology 2001331060ndash4
187 Mishra SR Chander SB Kumar A et al Endoscopic cyanoacrylate injection versusbeta-blocker for secondary prophylaxis of gastric variceal bleed a randomisedcontrolled trial Gut 201059729ndash35
188 Oho K Iwao T Sumino M et al Ethanolamine oleate versus butylcyanoacrylate for bleeding gastric varices a nonrandomized study Endoscopy199527349ndash54
189 Rajoriya N Forrest EH Gray J et al Long-term follow-up of endoscopic histoacrylglue injection for the management of gastric variceal bleeding QJM201110441ndash7
190 Ramond MJ Valla D Mosnier JF et al Successful endoscopic obturation of gastricvarices with butyl cyanoacrylate Hepatology 198910488ndash93
191 Romero-Castro R Ellrichmann M Ortiz-Moyano C et al EUS-guided coil versuscyanoacrylate therapy for the treatment of gastric varices a multicenter study (withvideos) Gastrointest Endosc 201378711ndash21
192 Soehendra N Grimm H Nam VC et al N-butyl-2-cyanoacrylate a supplement toendoscopic sclerotherapy Endoscopy 198719221ndash4
193 Tan PC Hou MC Lin HC et al A randomized trial of endoscopic treatment ofacute gastric variceal hemorrhage N-butyl-2-cyanoacrylate injection versus bandligation Hepatology 200643690ndash7
194 Tantau M Crisan D Popa D et al Band ligation vs N-butyl-2-cyanoacrylateinjection in acute gastric variceal bleeding a prospective follow-up study AnnHepatol 20131375ndash83
195 Williams SG Peters RA Westaby D Thrombinndashan effective treatment for gastricvariceal haemorrhage Gut 1994351287ndash9
196 Przemioslo RT McNair A Williams R Thrombin is effective in arresting bleedingfrom gastric variceal hemorrhage Dig Dis Sci 199944778ndash81
197 Ramesh J Limdi JK Sharma V et al The use of thrombin injections in themanagement of bleeding gastric varices a single-center experience GastrointestEndosc 200868877ndash82
198 McAvoy NC Plevris JN Hayes PC Human thrombin for the treatment of gastricand ectopic varices World J Gastroenterol 2012185912ndash17
199 Smith MR Tidswell R Tripathi D Outcomes of endoscopic human thrombininjection in the management of gastric varices Eur J Gastroenterol Hepatol201426846ndash52
200 Holster IL Poley JW Kuipers EJ et al Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray) J Hepatol2012571397ndash8
201 Stanley AJ Smith LA Morris AJ Use of hemostatic powder (Hemospray) in themanagement of refractory gastric variceal hemorrhage Endoscopy 201345(Suppl2 UCTN)E86ndash7
202 Kuradusenge P Rousseau H Vinel JP et al [Treatment of hemorrhages by ruptureof cardio-tuberous varices with transjugular intrahepatic portasystemic shunt]Gastroenterol Clin Biol 199317431ndash4
203 Sanyal AJ Freedman AM Luketic VA et al Transjugular intrahepatic portosystemicshunts for patients with active variceal hemorrhage unresponsive to sclerotherapyGastroenterology 1996111138ndash46
204 Stanley AJ Jalan R Ireland HM et al A comparison between gastric andoesophageal variceal haemorrhage treated with transjugular intrahepaticportosystemic stent shunt (TIPSS) Aliment Pharmacol Ther 199711171ndash6
24 Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262
Guidelines
205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines

205 Barange K Peron JM Imani K et al Transjugular intrahepatic portosystemic shuntin the treatment of refractory bleeding from ruptured gastric varices Hepatology1999301139ndash43
206 Chau TN Patch D Chan YW et al ldquoSalvagerdquo transjugular intrahepaticportosystemic shunts gastric fundal compared with esophageal variceal bleedingGastroenterology 1998114981ndash7
207 Lo GH Liang HL Chen WC et al A prospective randomized controlled trial oftransjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in theprevention of gastric variceal rebleeding Endoscopy 200739679ndash85
208 Procaccini NJ Al Osaimi AM Northup P et al Endoscopic cyanoacrylate versustransjugular intrahepatic portosystemic shunt for gastric variceal bleeding a single-center US analysis Gastrointest Endosc 200970881ndash7
209 Mahadeva S Bellamy MC Kessel D et al Cost-effectiveness of N-butyl-2-cyanoacrylate (histoacryl) glue injections versus transjugular intrahepaticportosystemic shunt in the management of acute gastric variceal bleeding Am JGastroenterol 2003982688ndash93
210 Koito K Namieno T Nagakawa T et al Balloon-occluded retrograde transvenousobliteration for gastric varices with gastrorenal or gastrocaval collaterals AJR Am JRoentgenol 19961671317ndash20
211 Choi YH Yoon CJ Park JH et al Balloon-occluded retrograde transvenousobliteration for gastric variceal bleeding its feasibility compared with transjugularintrahepatic portosystemic shunt Korean J Radiol 20034109ndash16
212 Hong CH Kim HJ Park JH et al Treatment of patients with gastric varicealhemorrhage endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occludedretrograde transvenous obliteration J Gastroenterol Hepatol 200924372ndash8
213 Jang SY Kim GH Park SY et al Clinical outcomes of balloon-occluded retrogradetransvenous obliteration for the treatment of gastric variceal hemorrhage in Koreanpatients with liver cirrhosis a retrospective multicenter study Clin Mol Hepatol201218368ndash74
214 Naeshiro N Aikata H Kakizawa H et al Long-term outcome of patients withgastric varices treated by balloon-occluded retrograde transvenous obliterationJ Gastroenterol Hepatol 2014291035ndash42
215 Cho SK Shin SW Lee IH et al Balloon-occluded retrograde transvenousobliteration of gastric varices outcomes and complications in 49 patients AJR AmJ Roentgenol 2007189W365ndash72
216 Tanihata H Minamiguchi H Sato M et al Changes in portal systemic pressuregradient after balloon-occluded retrograde transvenous obliteration of gastric
varices and aggravation of esophageal varices Cardiovasc Intervent Radiol2009321209ndash16
217 Sabri SS Abi-Jaoudeh N Swee W et al Short-term rebleeding rates for isolatedgastric varices managed by transjugular intrahepatic portosystemic shunt versusballoon-occluded retrograde transvenous obliteration J Vasc Interv Radiol201425355ndash61
218 Saad WE The history and evolution of balloon-occluded retrograde transvenousobliteration (BRTO) from the United States to Japan and back Semin InterventRadiol 201128283ndash7
219 Wang J Tian XG Li Y et al Comparison of modified percutaneous transhepaticvariceal embolization and endoscopic cyanoacrylate injection for gastric varicealrebleeding World J Gastroenterol 201319706ndash14
220 Orozco H Mercado MA The evolution of portal hypertension surgery lessonsfrom 1000 operations and 50 yearsrsquo experience Arch Surg 20001351389ndash93
221 Jaroszewski DE Schlinkert RT Gray RJ Laparoscopic splenectomy for the treatmentof gastric varices secondary to sinistral portal hypertension Surg Endosc20001487
222 Stone PA Phang D Richmond B et al Splenic artery embolization for thetreatment of bleeding gastric varices secondary to splenic vein thrombosisAnn Vasc Surg 201428737ndash11
223 Greig JD Garden OJ Anderson JR et al Management of gastric varicealhaemorrhage Br J Surg 199077297ndash9
224 Riemenschneider T Bermel RE Hirner A [Results of devascularization surgery ofthe gastroesophageal junction in recurrent hemorrhage of esophageal and fundusvarices] Zentralbl Chir 1994119291ndash7
225 Thomas PG DrsquoCruz AJ Distal splenorenal shunting for bleeding gastric varicesBr J Surg 199481241ndash4
226 Mishra SR Sharma BC Kumar A et al Primary prophylaxis of gastric varicealbleeding comparing cyanoacrylate injection and beta-blockers a randomizedcontrolled trial J Hepatol 2011541161ndash7
227 Kang EJ Jeong SW Jang JY et al Long-term result of endoscopic Histoacryl(N-butyl-2-cyanoacrylate) injection for treatment of gastric varices World JGastroenterol 2011171494ndash500
228 Katoh K Sone M Hirose A et al Balloon-occluded retrograde transvenousobliteration for gastric varices the relationship between the clinical outcome andgastrorenal shunt occlusion BMC Med Imaging 2010102
Tripathi D et al Gut 201501ndash25 doi101136gutjnl-2015-309262 25
Guidelines