Embed Size (px)
Citation preview
THE RESPIRATORY SYSTEM
UEQ: How do we exchange oxygen to and carbon dioxide from the
human body?
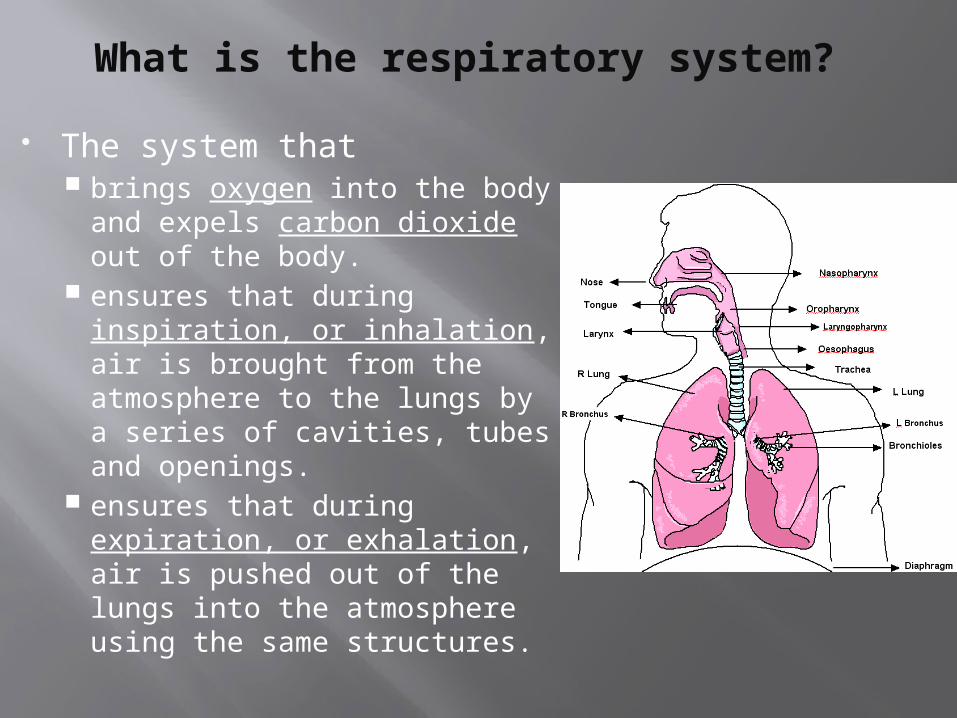
What is the respiratory system?
The system that brings oxygen into the body
and expels carbon dioxide out of the body.
ensures that during inspiration, or inhalation, air is brought from the atmosphere to the lungs by a series of cavities, tubes and openings.
ensures that during expiration, or exhalation, air is pushed out of the lungs into the atmosphere using the same structures.
THINK ABOUT IT:
WHAT ORGANS ARE APART OF THE UPPER RESPIRATORY TRACT?
Nasal cavities
Pharynx, or throat
Major Organs Accessory OrgansOral cavity , or mouth
Nose
Paranasal sinuses
The Upper Respiratory Tract
The nose
Bone and cartilage support the nose internally
Two nostrils or nares Air enters and leaves through here
Internal hairs guard nostrils Prevents larger particles carried in air
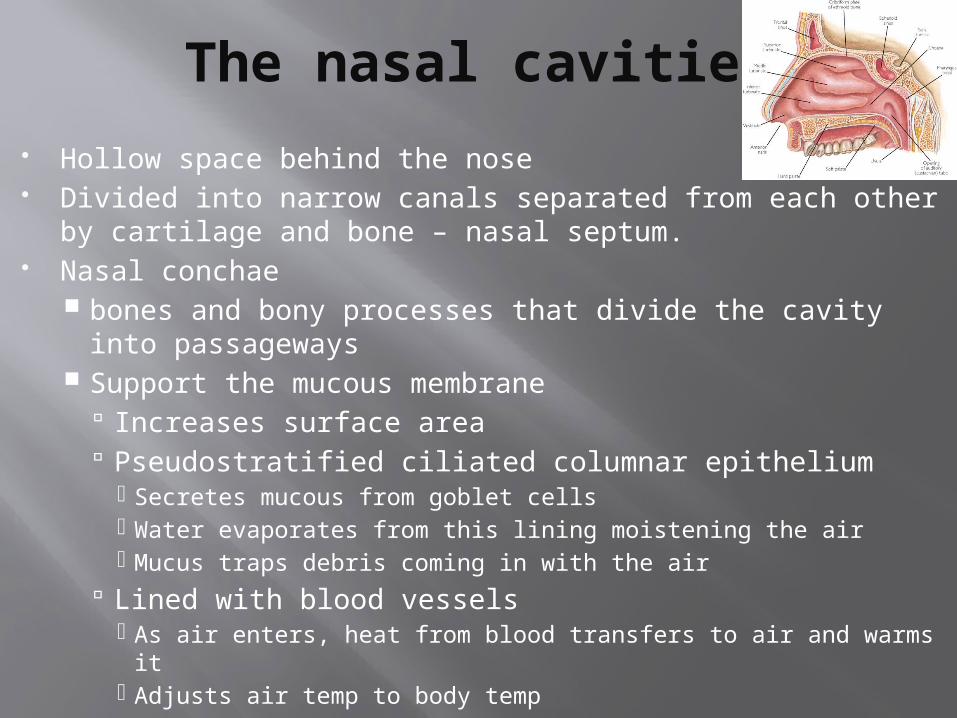
The nasal cavities
Hollow space behind the nose Divided into narrow canals separated from each other by
cartilage and bone – nasal septum. Nasal conchae
bones and bony processes that divide the cavity into passageways
Support the mucous membrane Increases surface area Pseudostratified ciliated columnar epithelium
Secretes mucous from goblet cells Water evaporates from this lining moistening the air Mucus traps debris coming in with the air
Lined with blood vessels As air enters, heat from blood transfers to air and warms it Adjusts air temp to body temp
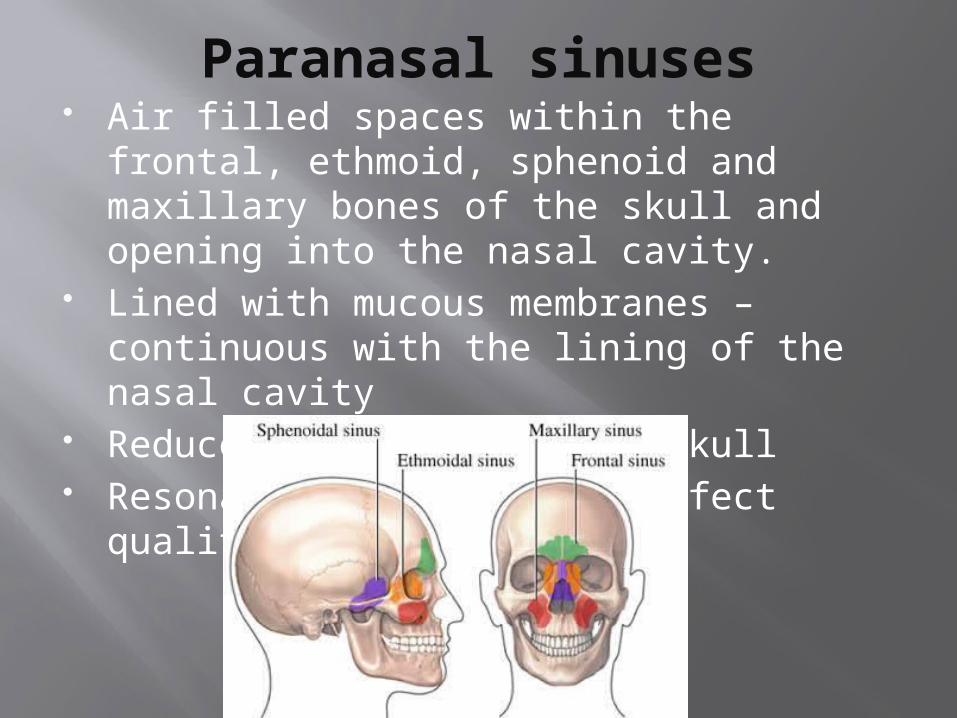
Paranasal sinuses Air filled spaces within the frontal,
ethmoid, sphenoid and maxillary bones of the skull and opening into the nasal cavity.
Lined with mucous membranes – continuous with the lining of the nasal cavity
Reduce the weight of the skull Resonance chambers that affect quality
of voice
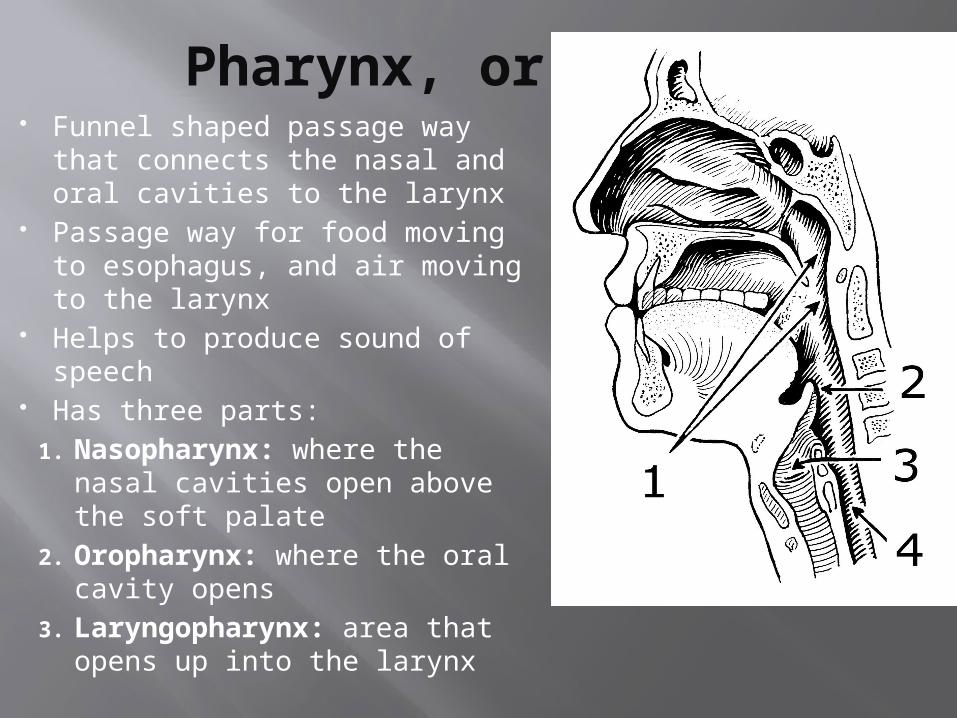
Pharynx, or Throat Funnel shaped passage way that
connects the nasal and oral cavities to the larynx
Passage way for food moving to esophagus, and air moving to the larynx
Helps to produce sound of speech
Has three parts: 1. Nasopharynx: where the
nasal cavities open above the soft palate
2. Oropharynx: where the oral cavity opens
3. Laryngopharynx: area that opens up into the larynx
Pathway of air through the upper respiratory
system.
REMEMBER!!!! Each time that you take a breath, there are three very important things that happen.
1. The air that you breathe in is cleaned by tiny hairs in your nose, trapping little bits of dirt and dust and germs that come in through your nose.
2. As you breathe, the air is made slightly wet. Your nose having damp passages does this.
3. The next thing that takes place when air enters your nose is that the air is warmed. This happens because the blood flows through the lining of the nose and gives off heat.
Snot and more.. Protecting us from harm Snot:
"Snot", is just another word for mucus. When bits of stuff get stuck in your nose hairs, it’s the mucus or snot that surrounds the stuff and traps it.
Boogers: Boogers are dried-up snot and dirty nose debris. Encrusted mucus is filled with the junk that’s in
the air you breathe - dust, pollen, germs, sand, fungi, smoke, small particles from outer space.
AND NOW FOR THE MUCUS MODEL…
Achoo…
Mucus model? – How does it compare to the real thing?
Model made up of gelatin (protein) and corn syrup (sugar)
Mucus is made mostly of sugars and protein.
The long, fine strings you could see inside your fake snot when you moved it around are protein strands.
These protein strands make snot sticky and capable of stretching

CHECK IT!Complete the questions for a stamp..
THINK ABOUT IT:
WHAT ORGANS ARE APART OF THE LOWER RESPIRATORY TRACT?
Trachea, or windpipeThe bronchial tree
Diaphragm
Major Organs Accessory Organs
The lungs
Larynx, or voicebox
Glottis
epiglottis
The Lower Respiratory System
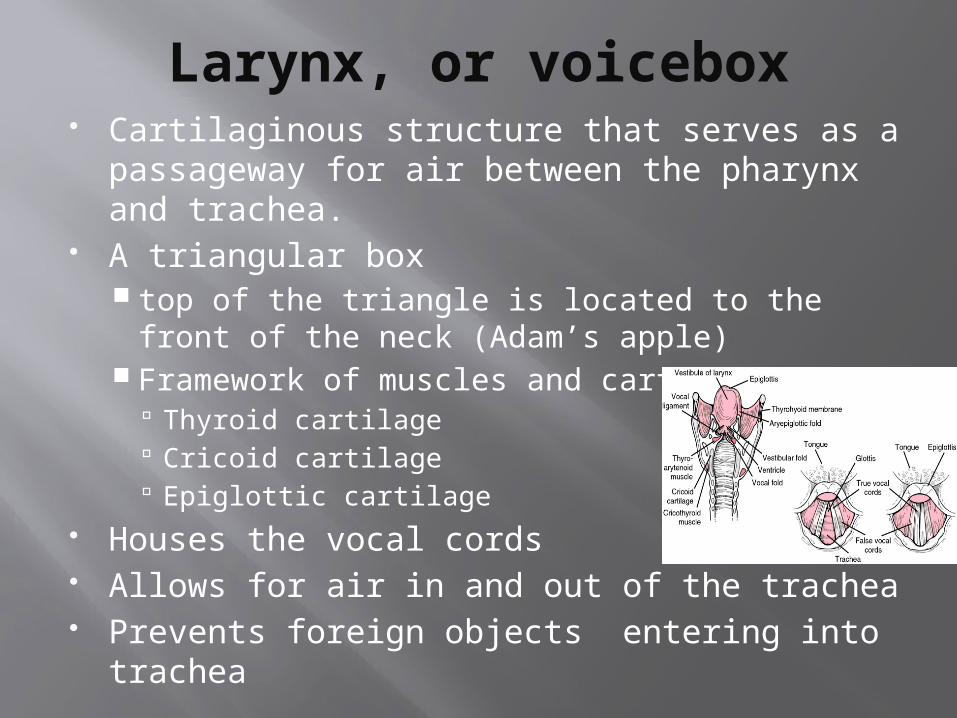
Larynx, or voicebox Cartilaginous structure that serves as a
passageway for air between the pharynx and trachea.
A triangular box top of the triangle is located to the front of
the neck (Adam’s apple) Framework of muscles and cartilage
Thyroid cartilage Cricoid cartilage Epiglottic cartilage
Houses the vocal cords Allows for air in and out of the trachea Prevents foreign objects entering into
trachea
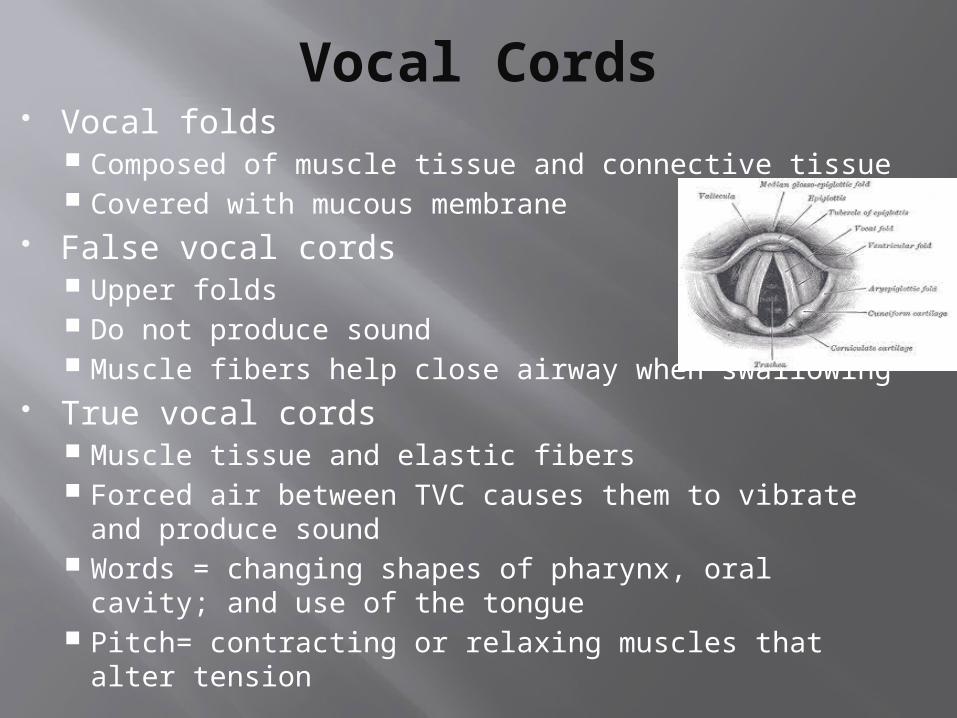
Vocal Cords Vocal folds
Composed of muscle tissue and connective tissue Covered with mucous membrane
False vocal cords Upper folds Do not produce sound Muscle fibers help close airway when swallowing
True vocal cords Muscle tissue and elastic fibers Forced air between TVC causes them to vibrate and
produce sound Words = changing shapes of pharynx, oral cavity;
and use of the tongue Pitch= contracting or relaxing muscles that alter
tension
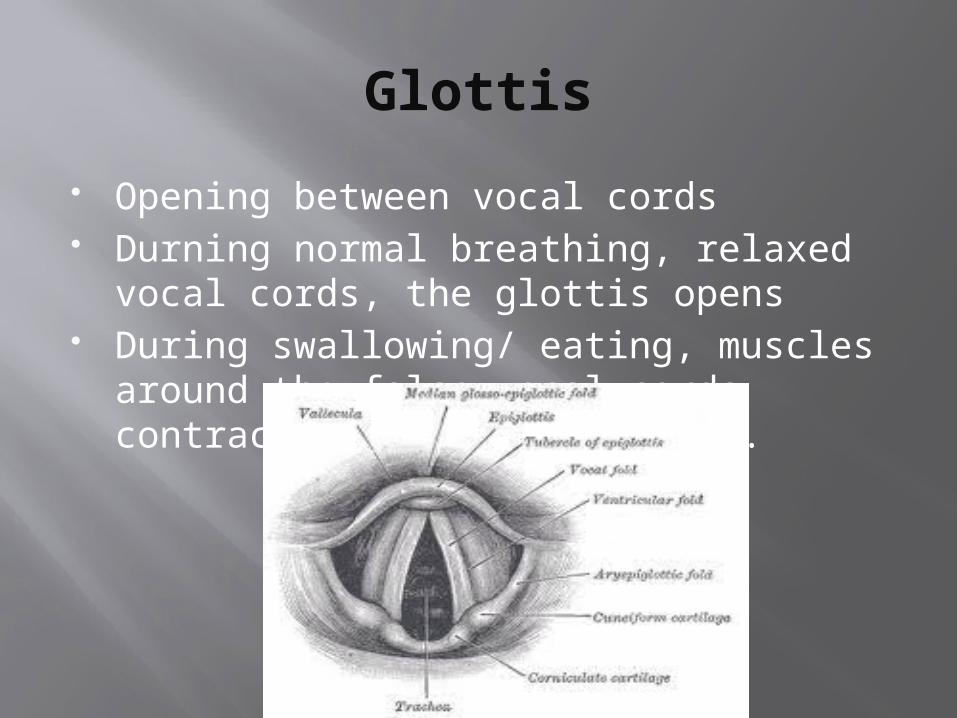
Glottis
Opening between vocal cords Durning normal breathing, relaxed vocal
cords, the glottis opens During swallowing/ eating, muscles
around the false vocal cords contract, the glottis closes.
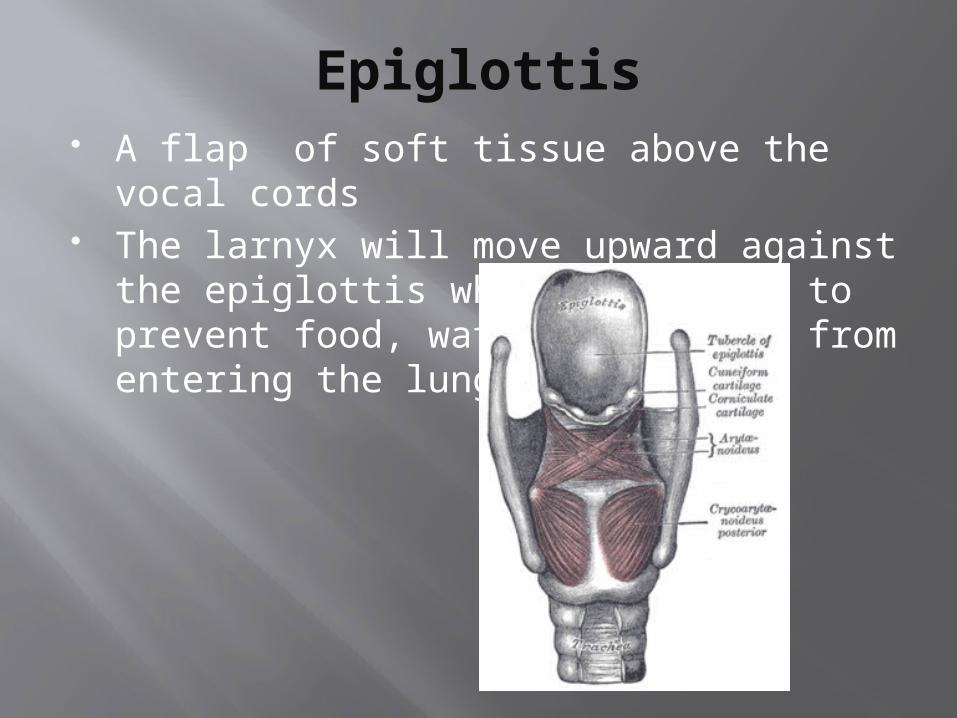
Epiglottis A flap of soft tissue above the vocal
cords The larnyx will move upward against the
epiglottis when swallowing to prevent food, water and saliva from entering the lungs.
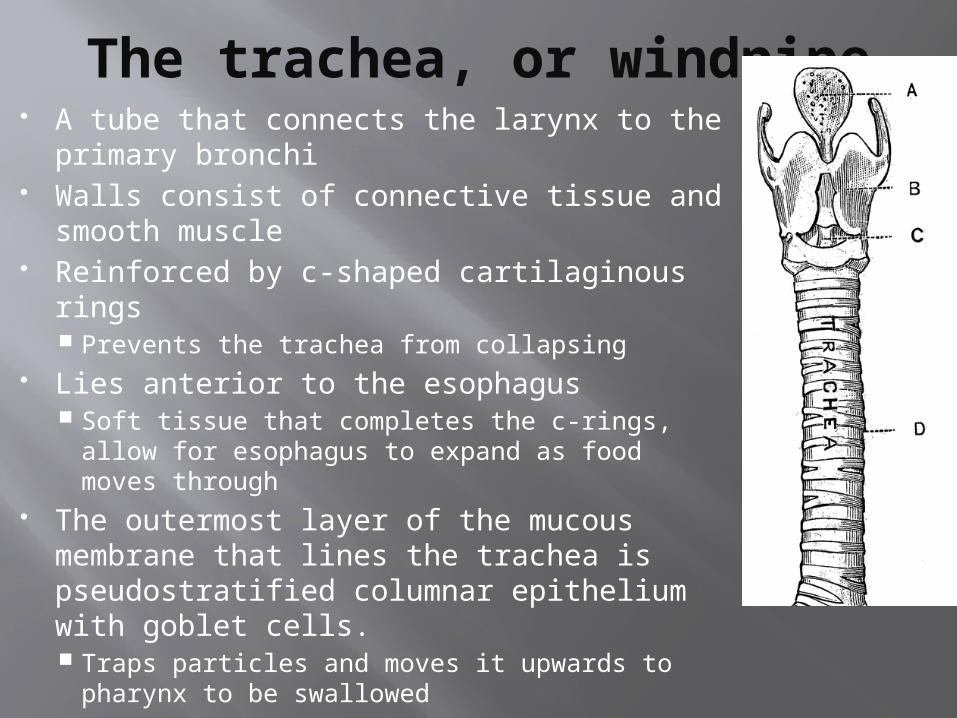
The trachea, or windpipe A tube that connects the larynx to the
primary bronchi Walls consist of connective tissue and
smooth muscle Reinforced by c-shaped cartilaginous rings
Prevents the trachea from collapsing Lies anterior to the esophagus
Soft tissue that completes the c-rings, allow for esophagus to expand as food moves through
The outermost layer of the mucous membrane that lines the trachea is pseudostratified columnar epithelium with goblet cells. Traps particles and moves it upwards to
pharynx to be swallowed
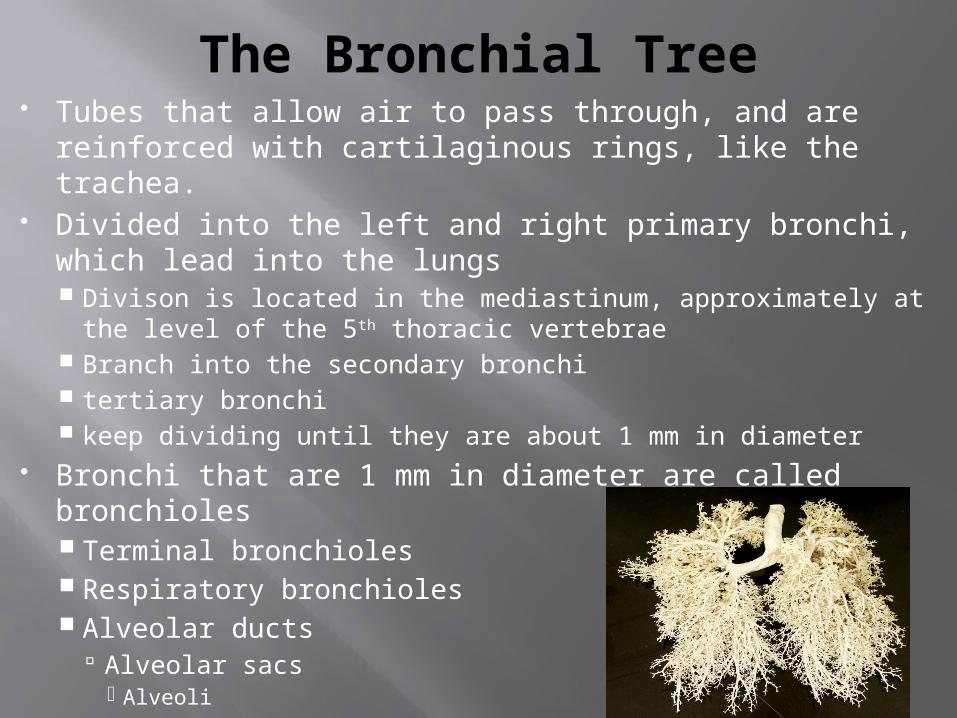
The Bronchial Tree Tubes that allow air to pass through, and are
reinforced with cartilaginous rings, like the trachea. Divided into the left and right primary bronchi, which
lead into the lungs Divison is located in the mediastinum, approximately at the
level of the 5th thoracic vertebrae Branch into the secondary bronchi tertiary bronchi keep dividing until they are about 1 mm in diameter
Bronchi that are 1 mm in diameter are called bronchioles Terminal bronchioles Respiratory bronchioles Alveolar ducts
Alveolar sacs Alveoli
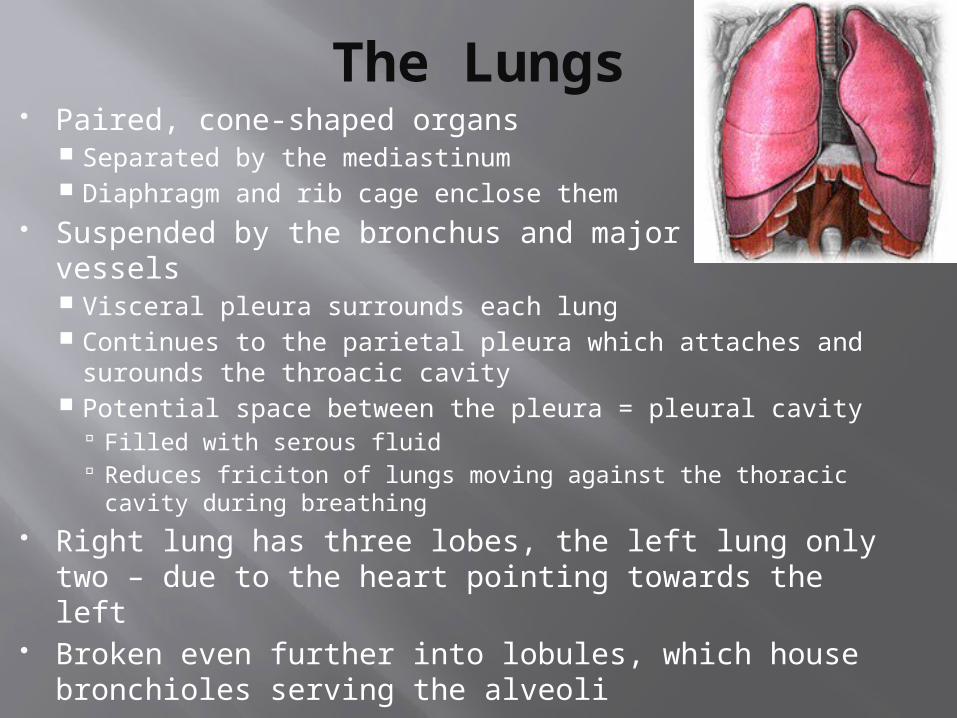
The Lungs Paired, cone-shaped organs
Separated by the mediastinum Diaphragm and rib cage enclose them
Suspended by the bronchus and major blood vessels Visceral pleura surrounds each lung Continues to the parietal pleura which attaches and
surounds the throacic cavity Potential space between the pleura = pleural cavity
Filled with serous fluid Reduces friciton of lungs moving against the thoracic cavity
during breathing Right lung has three lobes, the left lung only two –
due to the heart pointing towards the left Broken even further into lobules, which house
bronchioles serving the alveoli
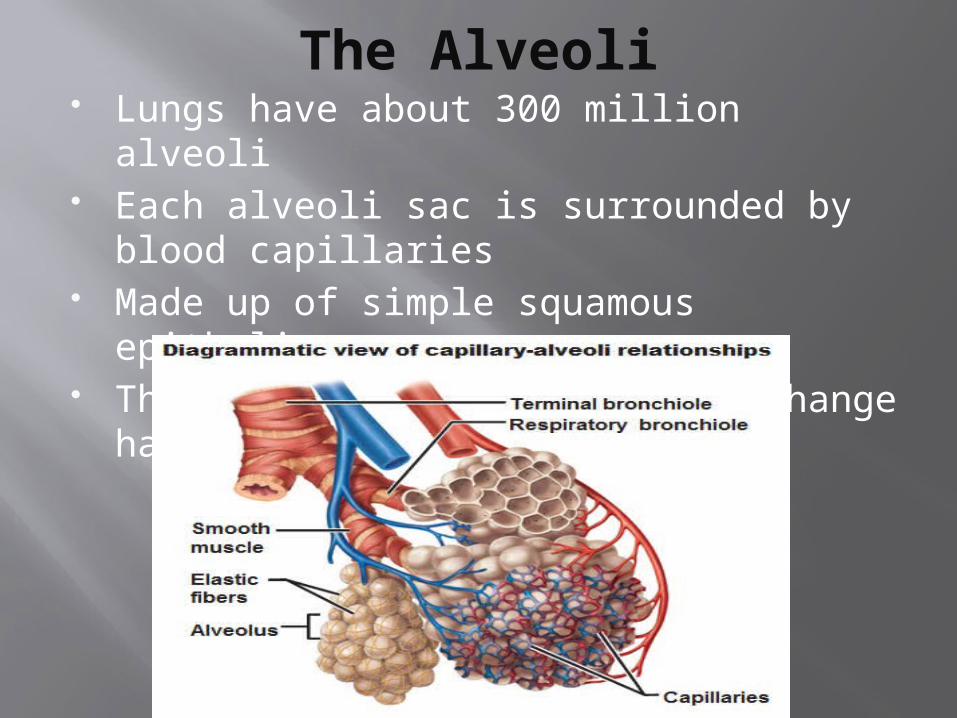
The Alveoli Lungs have about 300 million alveoli Each alveoli sac is surrounded by blood
capillaries Made up of simple squamous epithelium This is the site where gas exchange
happens
Be sure to complete the following
Your check it questions The diagram at the back of the packet
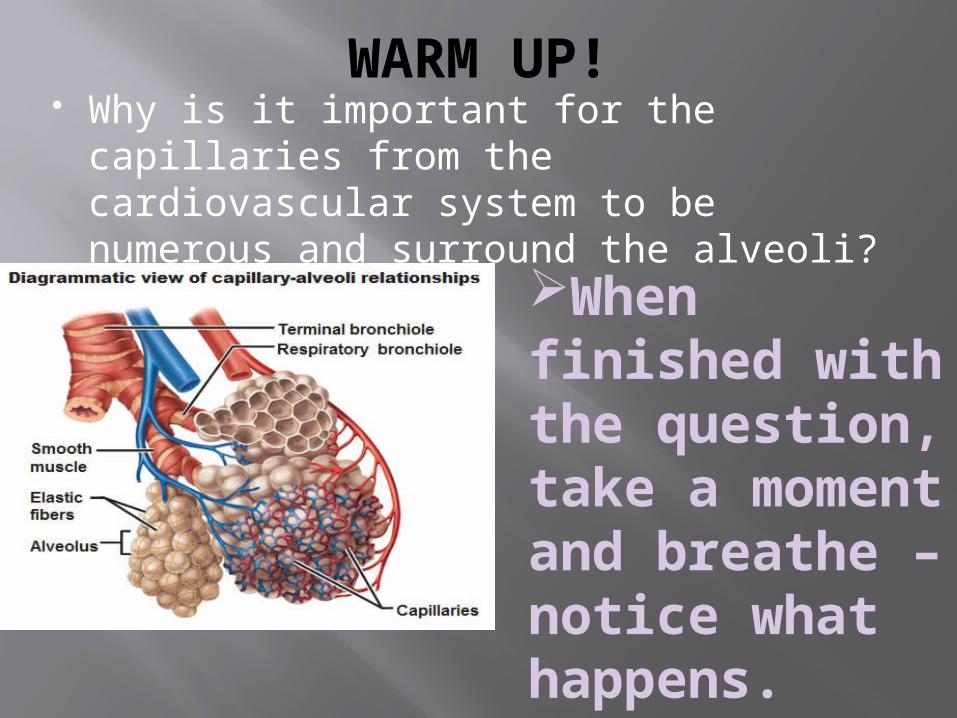
WARM UP! Why is it important for the capillaries
from the cardiovascular system to be numerous and surround the alveoli?
When finished with the question, take a moment and breathe – notice what happens. Write it down.
Cardio/ Respiratory connection
Oxygen diffuses from alveolar walls and enters the blood.(where it can now go to other cells in the body)
Carbon Dioxide diffuses from the blood through the walls and enters the alveoli. (where it can be exhaled and released)
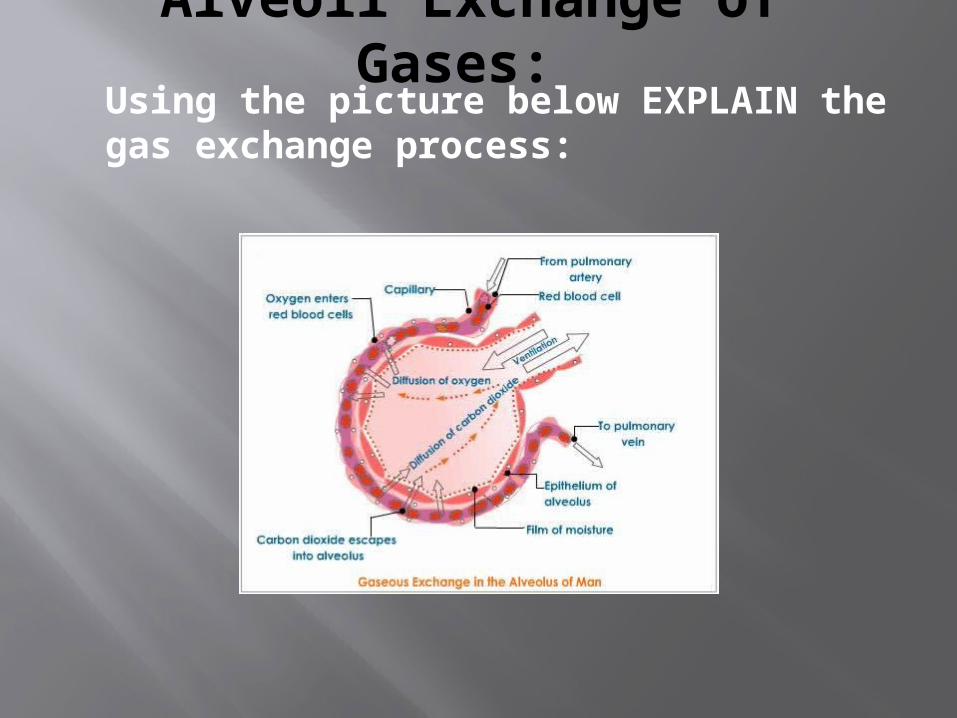
Alveoli Exchange of Gases: Using the picture below EXPLAIN the gas exchange process:
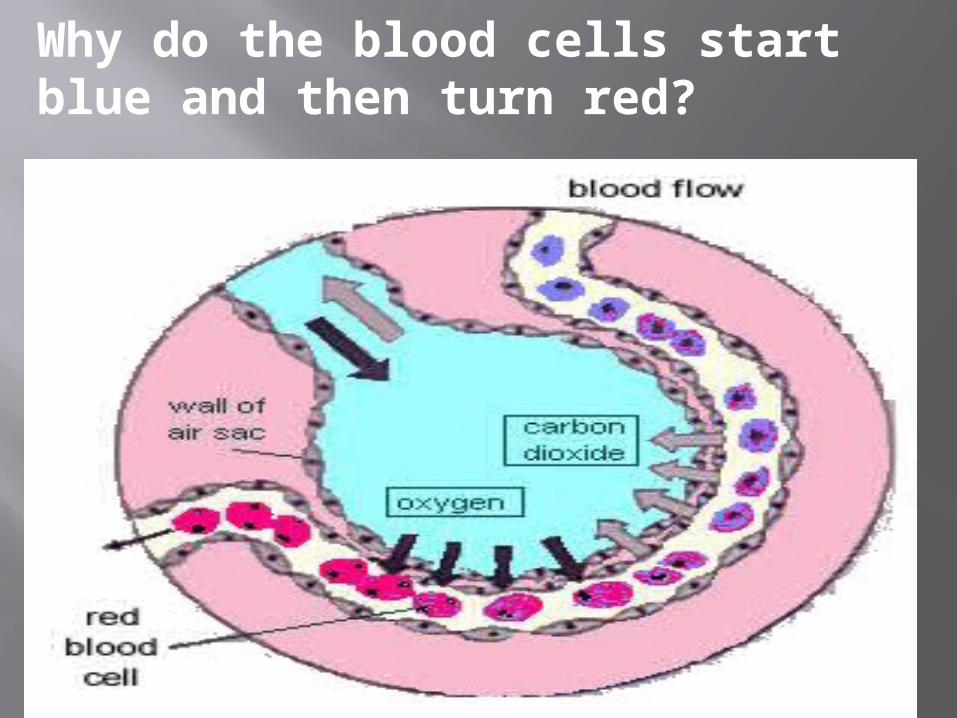
Why do the blood cells start blue and then turn red?

CHECK IT!
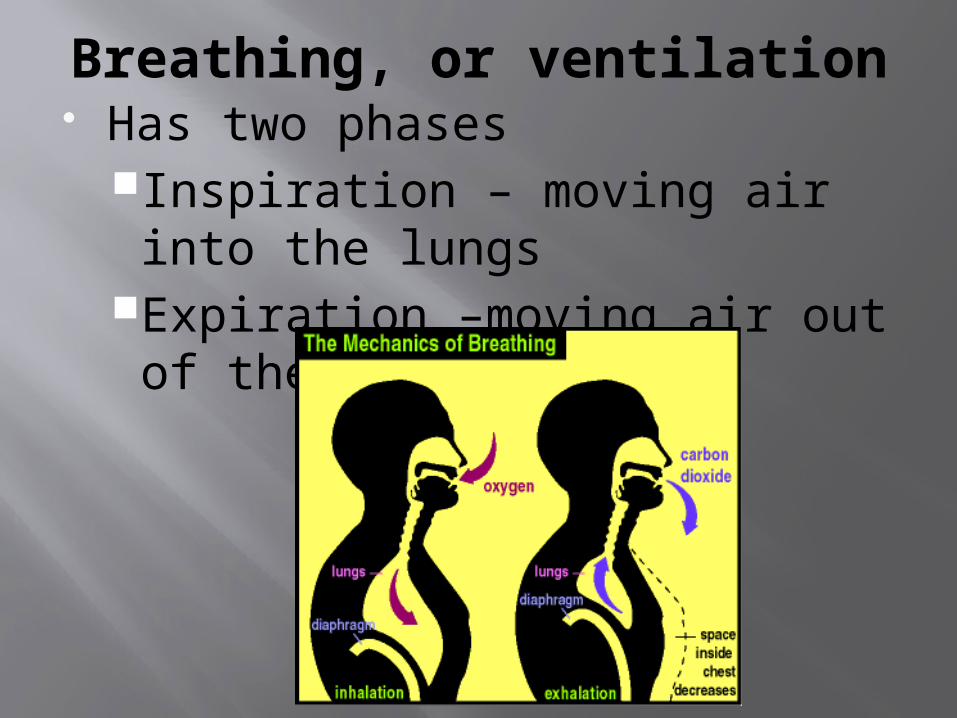
Breathing, or ventilation Has two phases
Inspiration – moving air into the lungs
Expiration –moving air out of the lungs
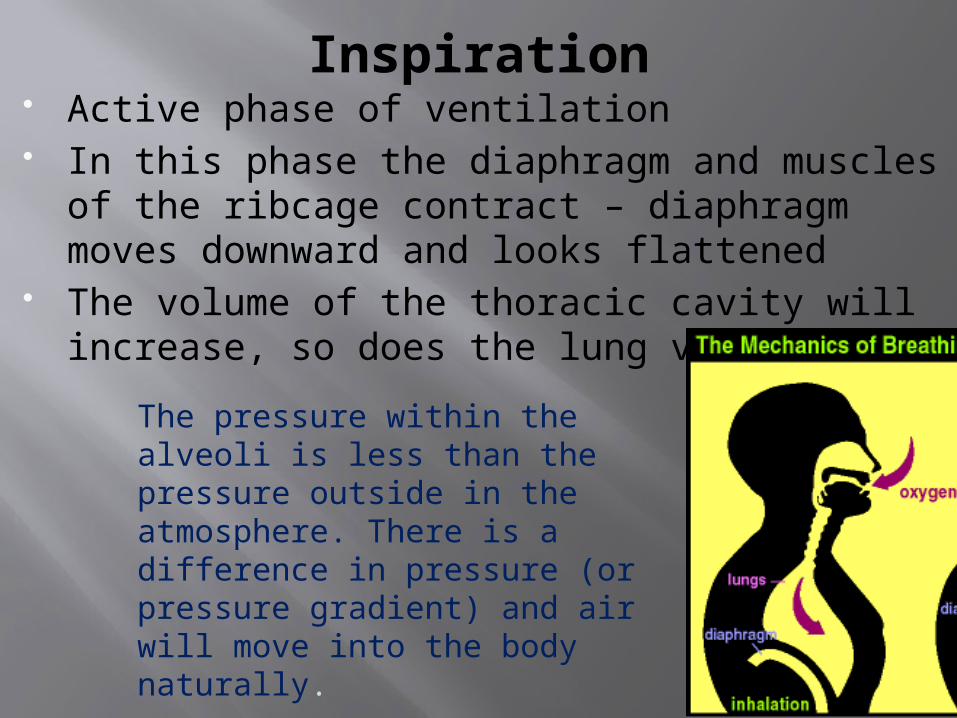
Inspiration Active phase of ventilation In this phase the diaphragm and muscles of
the ribcage contract – diaphragm moves downward and looks flattened
The volume of the thoracic cavity will increase, so does the lung volume
The pressure within the alveoli is less than the pressure outside in the atmosphere. There is a difference in pressure (or pressure gradient) and air will move into the body naturally.
Pressure and volume have an inverse relationship
Pressure inside the lungs and alveoli decrease, atmospheric pressure will push outside air into airways
During this time the pressure in the alveoli drops 2mmHg below atmospheric pressure
In response, atmospheric pressure forces air into the airways
The external intercostal muscles between ribs are stimulated and move the ribs and sternum upwards
Enlarges thoracic cavity even further Internal pressure is further reduced;
increases amount of air into the lungs
Water within the serous fluid found in between the visceral and parietal pleura creates an attraction between the pleura, and the membranes move upward during inspiration
This expands the lung in all directions. Too much water in the alveolar sacs
creates a surface tension that may collapse the alveoli.
Certain cells within the alveoli secrete a surfactant – lipids and proteins
Fills the alveolar air spaces – reducing the tendency to collaspe, especially when lung volumes are low
Makes it easier to inflate alveoli
Expiration Passive phase of ventilation Come from elastic recoil and surface
tension No effort is required for air to leave
the body Diaphragm and muscles of the
ribcage relax – diaphragm looks cone shaped
Pressure within the alveoli increases to about 1mmHg above atmospheric pressure
Forces the air out of the lungs The volume of the thoracic cavity will
decrease, so does the lung volume
Maximum inspiration and forced expiration
MAXIMUM INSPIRATION FORCED EXPIRATION Involves muscles of
the back, chest, and neck
Thoracic cavity increases more than normal, for maximum lung capacity
Usually during exercise
Contraction of the ribcage muscles forces the ribcage to move downward and inward
Involves the abdominal muscles pushing against the abdominal organs which pushes against the diaphragm, pushing more out of the lungs
Usually during exercise, singing, playing an instrument, or blowing out a candle
CHECK IT!And then the activity.
Volumes of Air in the LungsWarm UP: Are our lungs ever void of air? Why or why not?
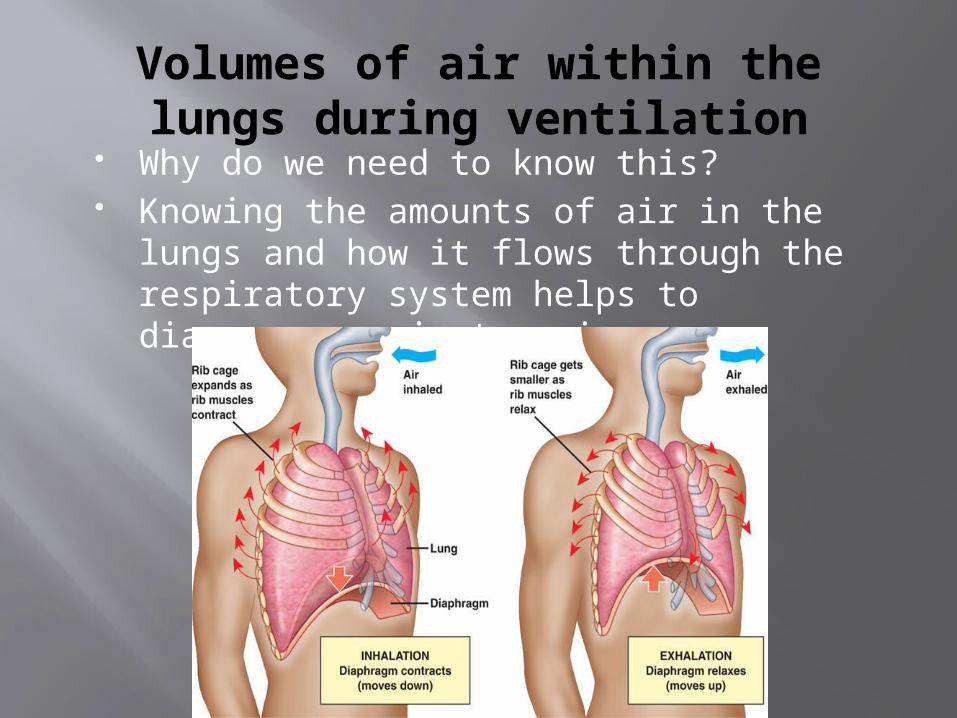
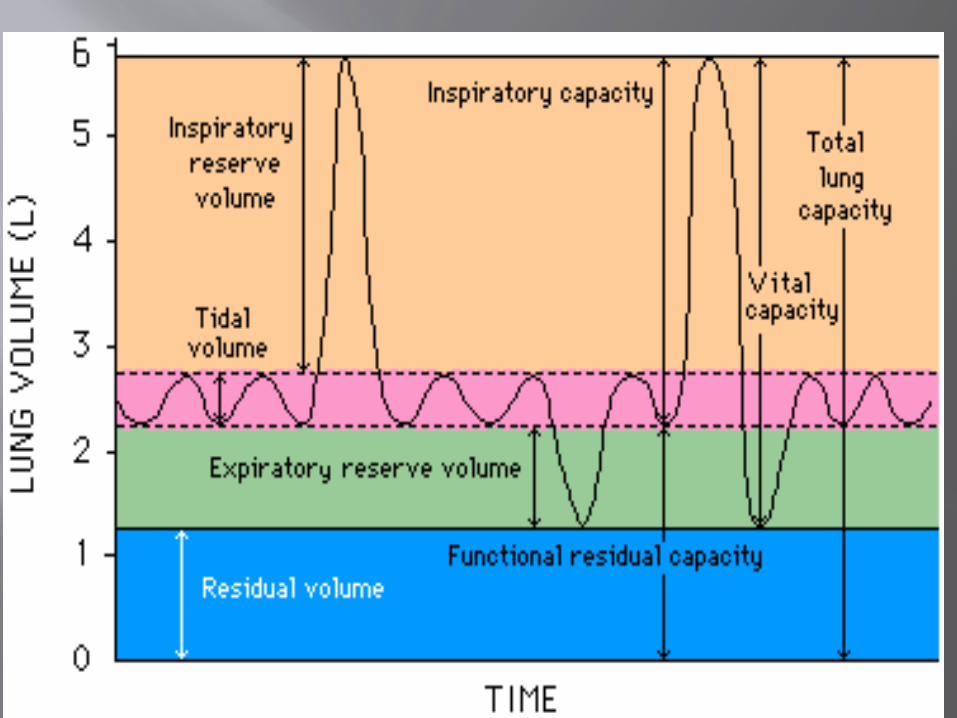
Volumes of air within the lungs during ventilation
Why do we need to know this? Knowing the amounts of air in the lungs
and how it flows through the respiratory system helps to diagnose respiratory issues
Respiratory Air Volumes and Capacities
Spirometry is the test that measures air volumes in or out of the lungs. Three distinct repiratory volumes can be
measured: Resting Tidal volume Inspiratory reserve volume Expiratory reserve volume
One inspiration + one expiration = respiratory cycle. Air that enters of leaves during a respiratory
cycle is the tidal volume
Respiratory cycle: One inspiration plus one expiriation. (Breathe in- breathe out)
1. Resting Tidal volume- the normal amount of air that enters the lungs and leaves the lungs during a respiratory cycle.
The average is about 500 milliliters of air per breath in and the same amount out.
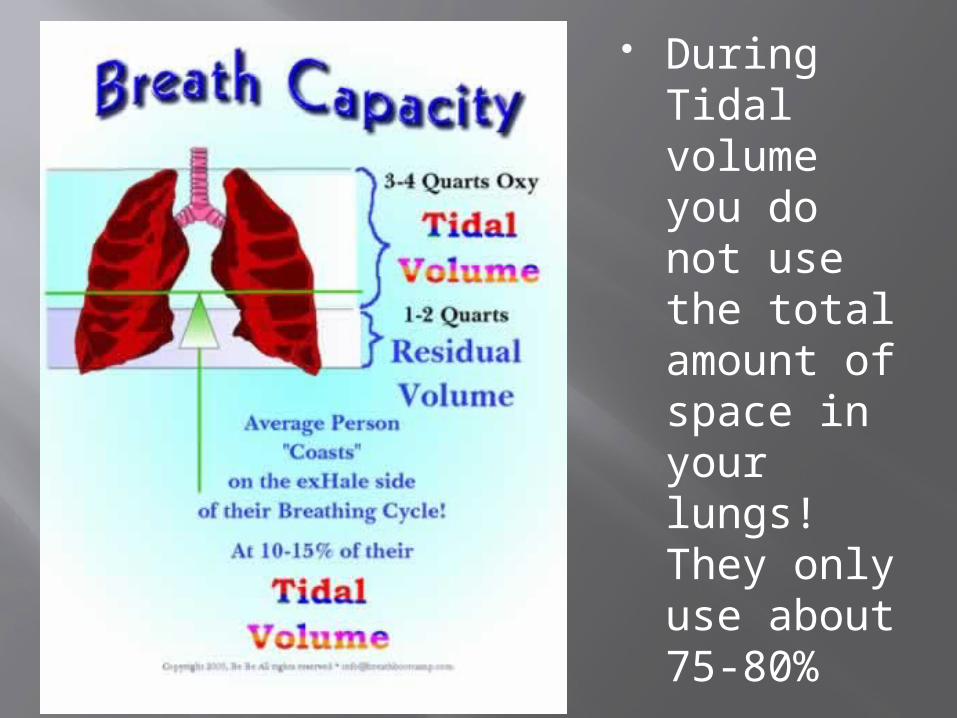
During Tidal volume you do not use the total amount of space in your lungs! They only use about 75-80%
2. Inspiratory Reserve Volume: When you take a deep breath in to hold more air than a usual breath. “Forced inhalation”.
3. Expiratory Reserve Volume: Forced expiration. Expelling air beyond the tidal volume. Even after the most forceful exhale however you still have air left in your lungs.
This left over air is called the Residual Volume.
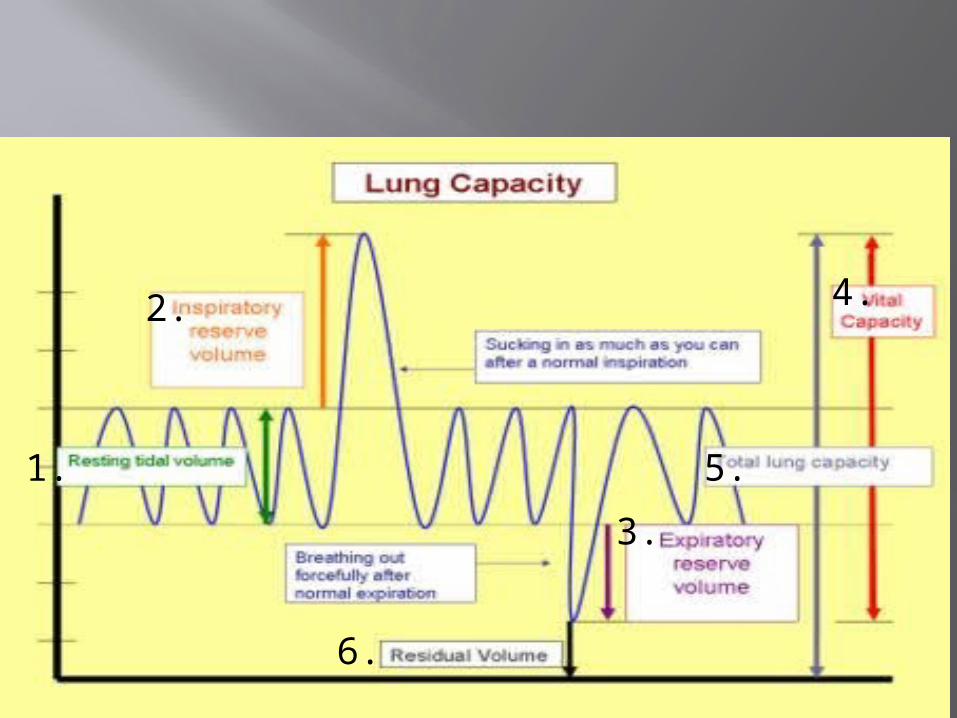
2.
3.
4.
5. 1.
6.
4. Vital Capacity: Combining the tidal volume with both the inspiratory reserve volume and the expiratory reserve volume.
5. Total Lung Capacity: The vital capacity plus the residual volume. All the possible air that can come into or out of the lungs, including the air that never leaves the lungs.
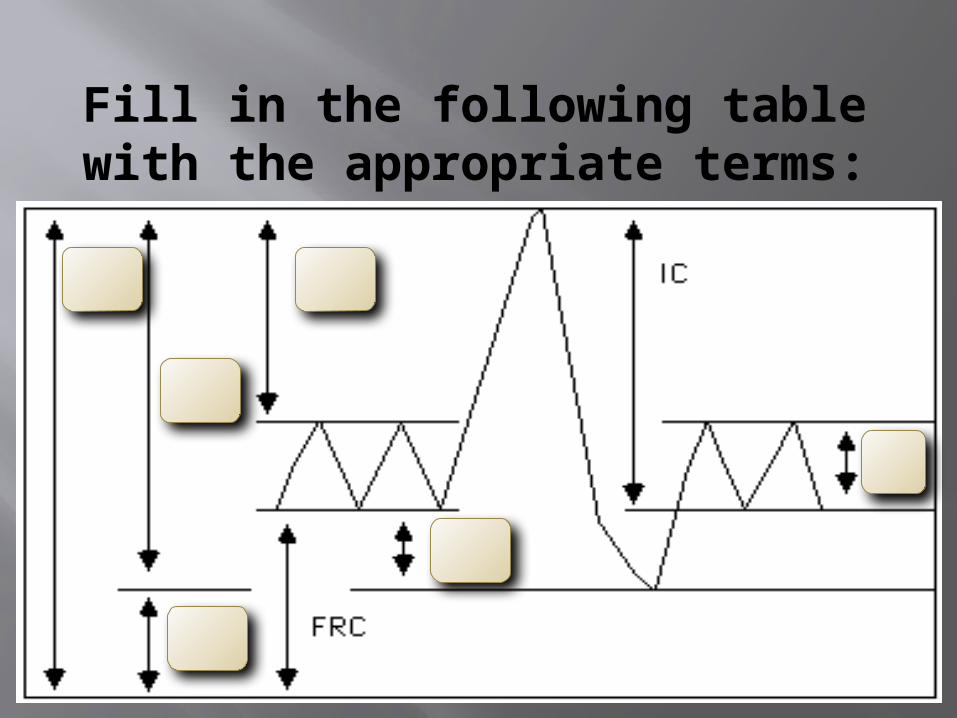
Fill in the following table with the appropriate terms:
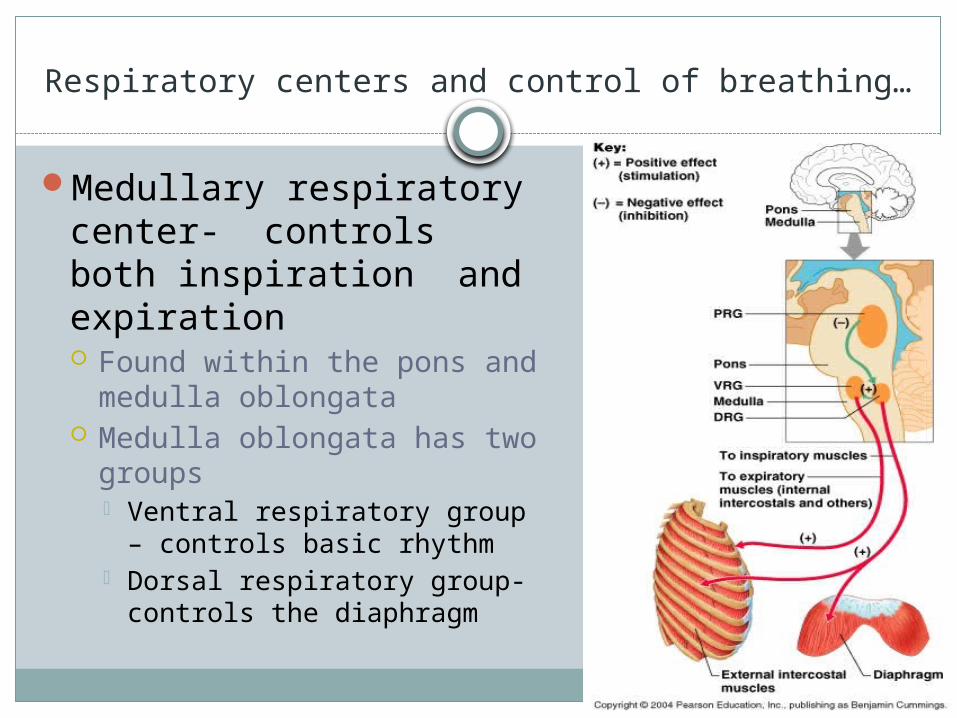
Respiratory centers and control of breathing…
Medullary respiratory center- controls both inspiration and expiration Found within the pons and
medulla oblongata Medulla oblongata has two
groups Ventral respiratory group –
controls basic rhythm Dorsal respiratory group-
controls the diaphragm
Factors that Affect breathingflow charts.. CHECK IT!
PP. 456- 458Create flow charts for the following factors
that affect breathing CO2 levels O2 levels Depth of breathing Emotional upset Holding your breath Hyperventilation
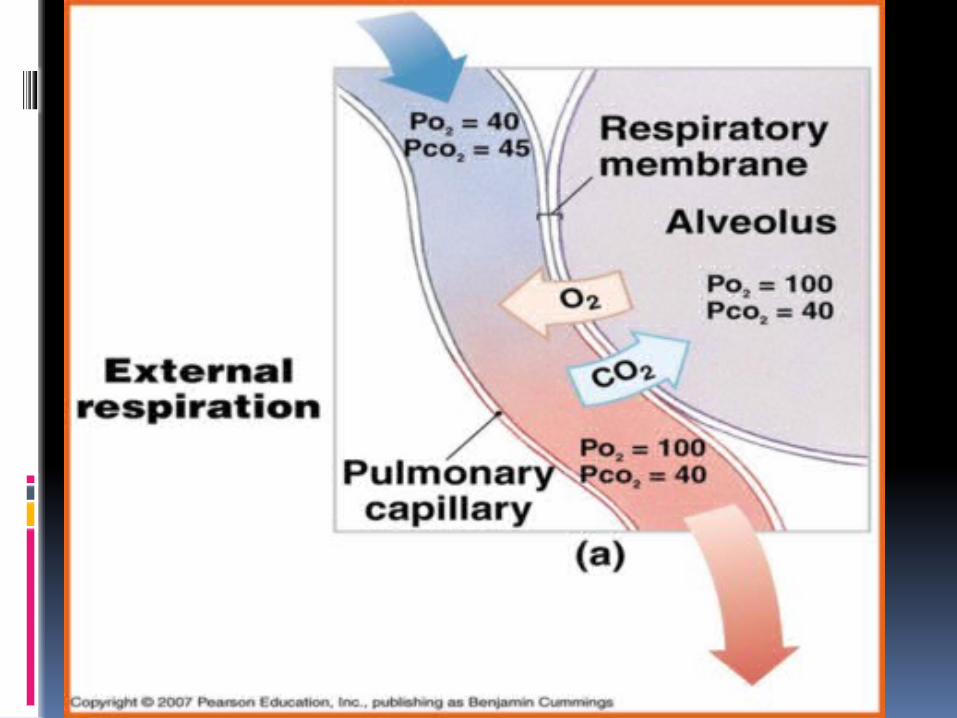
HOW AND WHY GAS EXCHANGE HAPPENS:
Location: The alveoliMethod: Diffusion
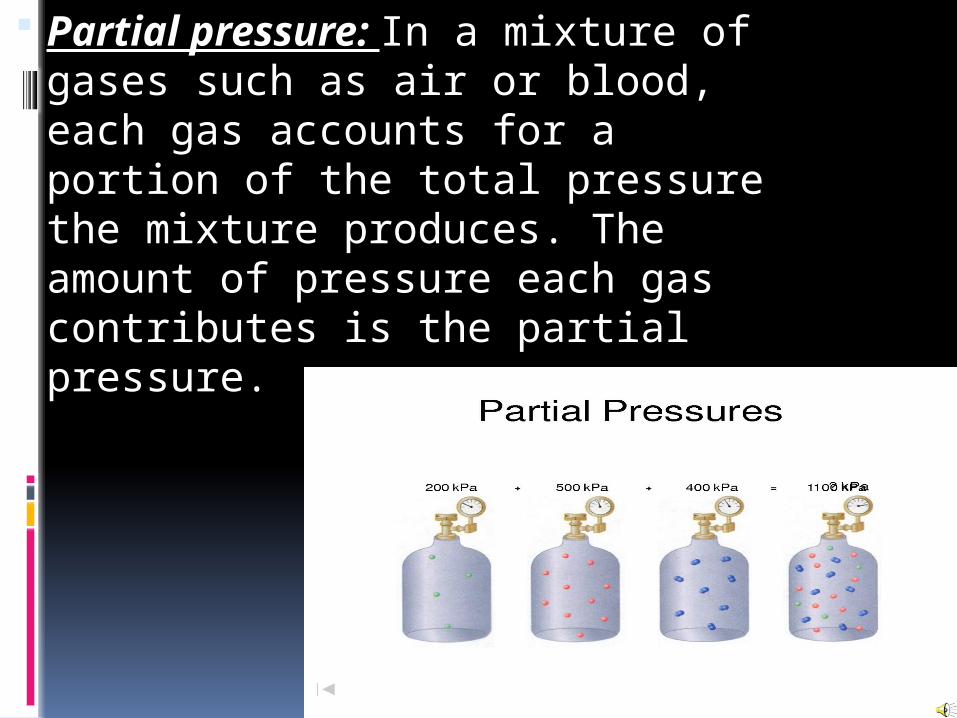
Partial pressure: In a mixture of gases such as air or blood, each gas accounts for a portion of the total pressure the mixture produces. The amount of pressure each gas contributes is the partial pressure.
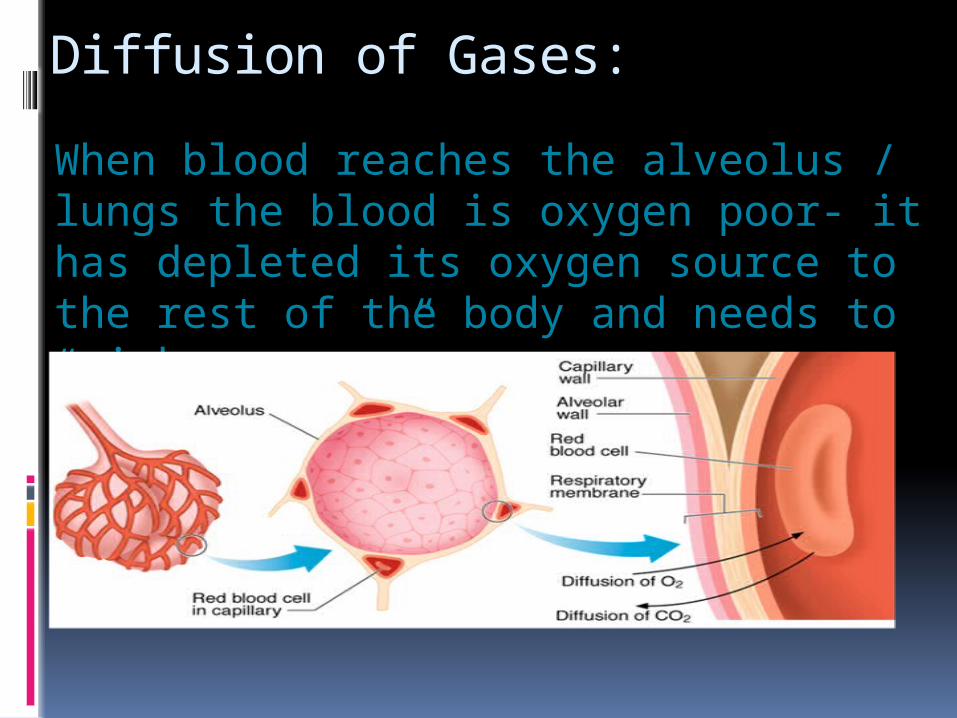
Diffusion of Gases:
When blood reaches the alveolus / lungs the blood is oxygen poor- it has depleted its oxygen source to the rest of the body and needs to “pick up more”.
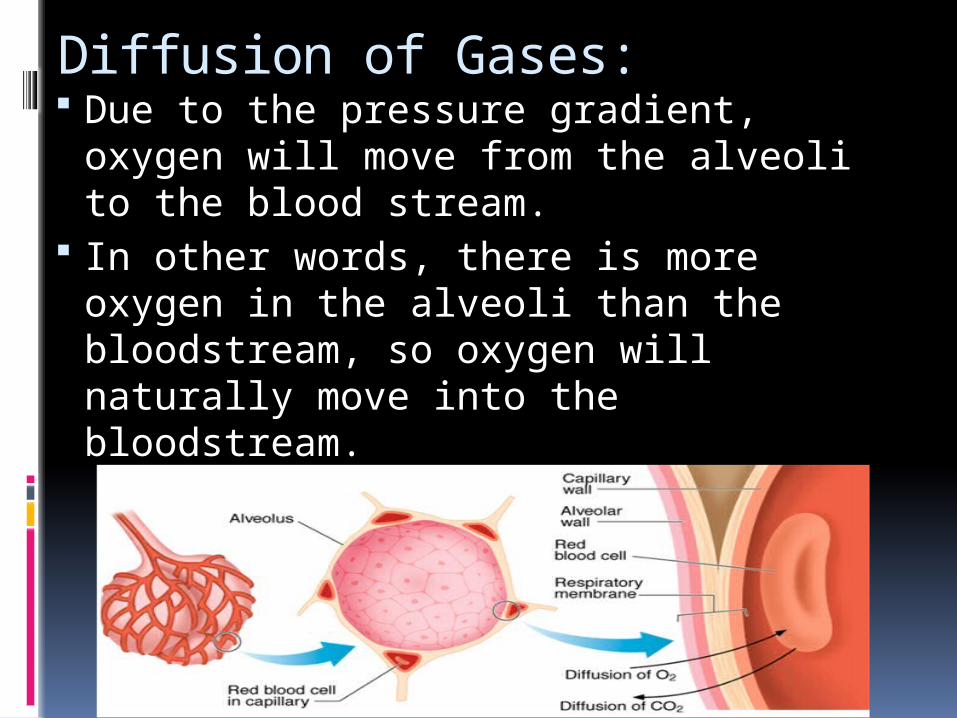
Diffusion of Gases: Due to the pressure gradient,
oxygen will move from the alveoli to the blood stream.
In other words, there is more oxygen in the alveoli than the bloodstream, so oxygen will naturally move into the bloodstream.
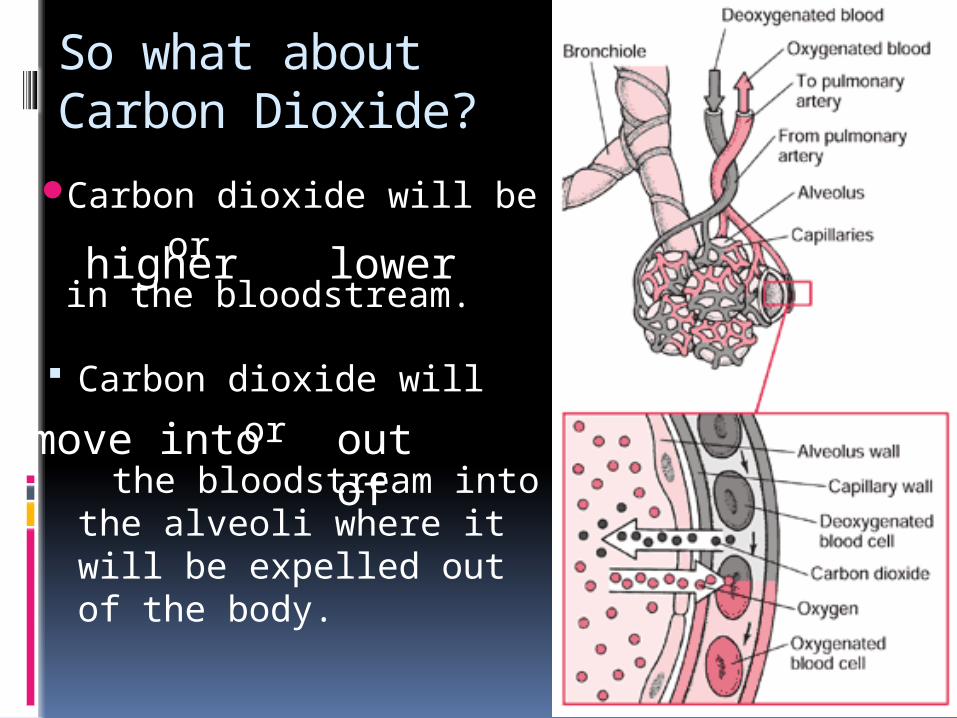
Carbon dioxide will be orin the bloodstream.
So what about Carbon Dioxide?
Carbon dioxide will or
the bloodstream into the alveoli where it will be expelled out of the body.
higher lower
move into out of

Color and label the diagram

GAS TRANSPORT
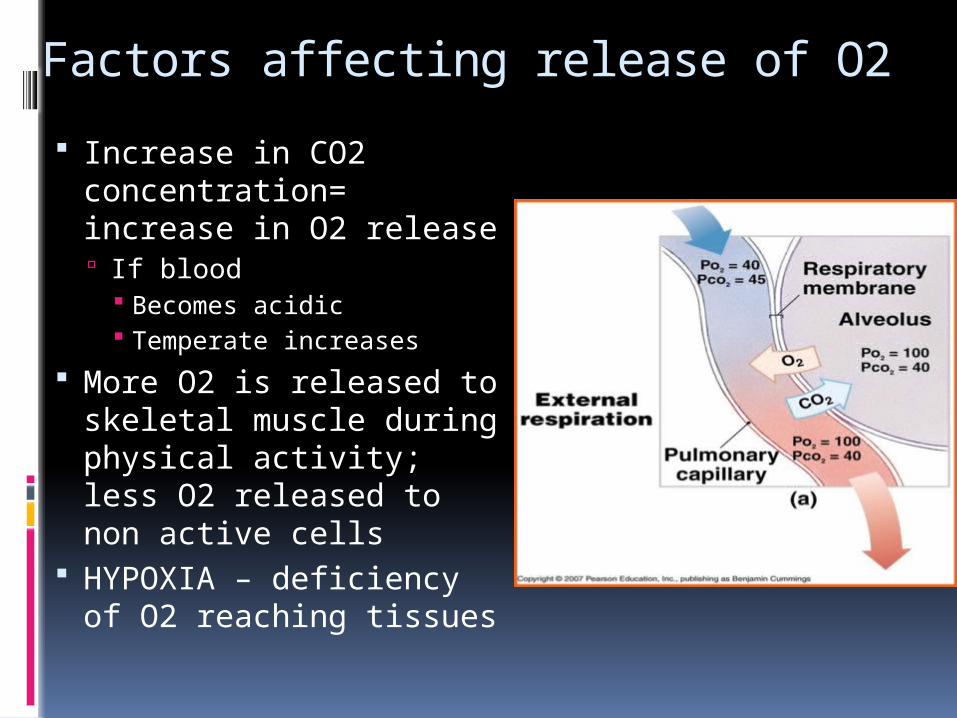
Factors affecting release of O2
Increase in CO2 concentration= increase in O2 release If blood
Becomes acidic Temperate increases
More O2 is released to skeletal muscle during physical activity; less O2 released to non active cells
HYPOXIA – deficiency of O2 reaching tissues
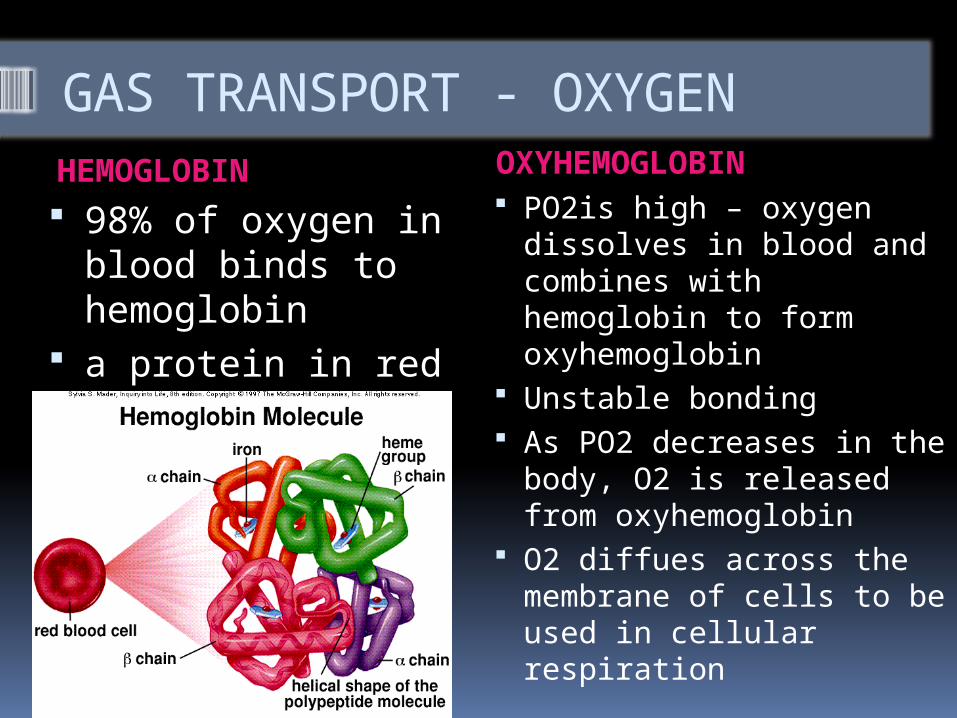
GAS TRANSPORT - OXYGENHEMOGLOBIN OXYHEMOGLOBIN
98% of oxygen in blood binds to hemoglobin
a protein in red blood cells that carries oxygen
PO2is high – oxygen dissolves in blood and combines with hemoglobin to form oxyhemoglobin
Unstable bonding As PO2 decreases in the
body, O2 is released from oxyhemoglobin
O2 diffues across the membrane of cells to be used in cellular respiration
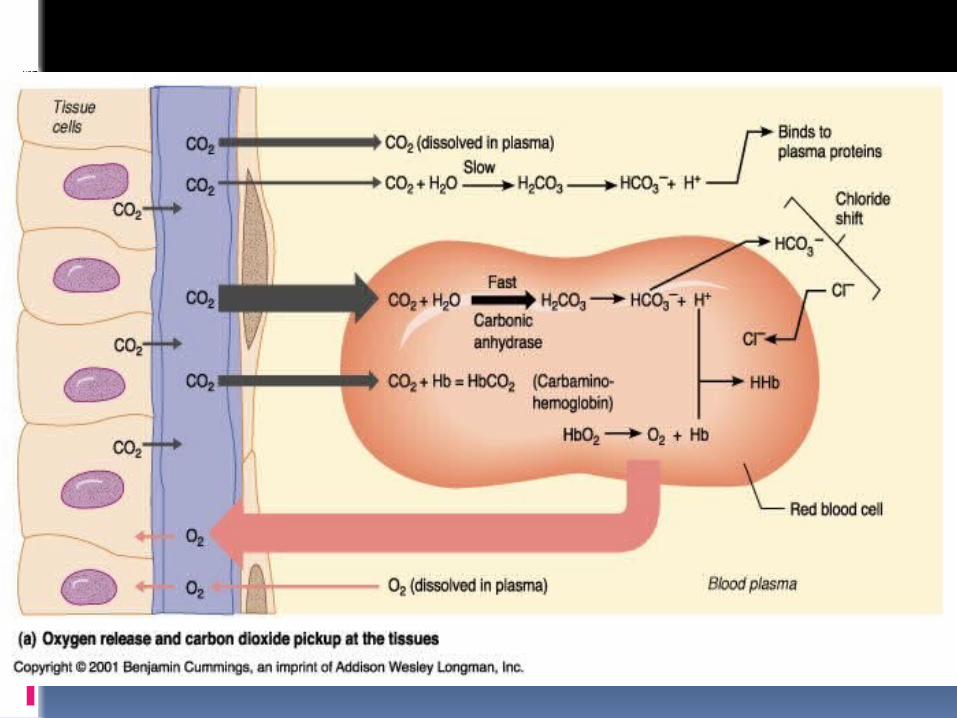
CO2 Transport
Capillary blood gains CO2, as tissues have increased levels of PCO2
Transported in three ways to the lungs: Dissolved in plasma Bound to hemoglobin Bicarbonate ions
Amount of CO2 dissolved in plasma dependent on its partial pressure Increased PCO2 = more CO2 in solution Only 7% of CO2 transports in this form
GAS TRANSPORTCarbaminohemoglobin Bicarbonate Ions
CO2 loosely bonds with hemoglobin = carbaminohemoglobin
Decomposes readily in regions of low PCO2 – releasing CO2
Only about 23% of the CO2 carried in the blood is formed in molecule, as this reaction happens slowly
Most important CO2 transport mechanism
CO2+ H2O => H2CO3 (carbonic acid)
Occurs slowly in plasma Carbonic anhydrase
speeds up reaction, releasing H+ and HCO3- (bicarbonate ions)
Bicarbonate ions diffuse into the plasma – 70% of all CO2 in blood is transported this way
CO2 Transport Continued
Plasma release CO2 Dissolved CO2 diffuses into the alveoli (alveoli
PCO2 is low
Bicarbonate Ions Release CO2 As blood passes through the capillaries of the
lungs At same time H+ and HCO3- combine to make
H2CO3 under influence of carbonic anhydrase H2CO3 breaks down quickly to form CO2 and
H2O CO2 then diffuses into the alveolus
Carbaminohemoglobin release of CO2 As blood passes through the
capillaries of the lungs Release of CO2 happens Will continue until PCO2 of blood and
alveolar air are at equilibrium
CO2 Transport Continued