Embed Size (px)
Citation preview

INTERNATIONAL JOURNAL. OF LEPROSY^ Volume 47, Number 3Printed in the U.S.A.
Untreated Lepromatous Leprosy: HistopathologicalFindings in Cutaneous Blood Vessels'
GUIsen Coruh and A. Cohn McDougall 2
Referring to the earlier work of Neisserin 1881 and Touton in 1886, Metchnikoffdescribed the presence of leprosy bacilli inendothelial lining cells of blood vessels inhis lectures on — The Comparative Pathol-ogy of Inflammation'' in 1892, saying thatin some cases they occurred in such largenumbers as to obscure the nucleus ( 2 '). Inhis textbook of 1930, Klingmiiller ( 20) de-scribed and illustrated leprosy bacilli incapillaries and veins, and in 1941 Fite (")published a detailed account of the nature,frequency, and significance of vascular in-volvement in 77 patients suffering from var-ious types of leprosy. In his famous Athisof 1952, Mitsuda ( 2" ) illustrates marked vas-cular involvement with thickening of themedia and intima, and proliferating bacilliwithin intimal cells in a small artery andvein of the tunica alba in the tail of theepididymis. On the other hand, other stan-dard reference books, e.g., Cochrane andDavey ( 5) hardly refer to vascular involve-ment except perhaps in the context of theunusual Lucio-Latapi type of lepromatousleprosy, occurring mainly in Mexico. Thehistopathological findings in blood vesselsof skin were described in 205 patients withleprosy by Popov in 1966 ( 2") and in 90 se-lected biopsies by Santos and Beja in 1969("7). Other authors '7) have describedvascular changes in tissues infected withleprosy, often in the context of nerve in-volvement, while Skinsnes, et al. (m) andKaur, et al. ( 1 ") have given detailed ac-counts of the vascular defect in leprosy,mainly of the larger limb vessels, in relationto the dystrophic changes and mutilationswhich are so characteristic of this disease.
In recent years it has been a) re-empha-sized that there is a continuous bacteremia
' Received for publication on 29 January 1979.G. Coruh, M.D. and A. C. McDougall, M.D.,
M.R.C.P., The Slade Hospital, Headington, OxfordOX3, 7JH, U.K. Dr. Coruh's present address is EgeanUniversity, Medical Faculty, Department of Patholo-gy, Izmir, Turkey.
500
in lepromatous leprosy ("."")* and b) shownthat biting arthropods are, under experi-mental conditions, capable of taking up andtransferring leprosy bacilli from infectedpatients to the footpads of mice ("). Theseobservations, together with the possibilitythat endothelial cells may be an importantsite for the multiplication of leprosy bacilliand their seeding into the blood stream andthat the media of blood vessels may be asite in which bacilli persist despite adequatetherapy, have largely prompted the presentstudy. We report our findings in the skinvasculature of 100 patients with untreatedlepromatous leprosy.
PATIENTS AND METHODSThe majority of the patients (81 percent)
were taking part in a trial of rifampin (Ri-mactane") together with dapsone, orga-nized by Ciba-Geigy Ltd., Basle, Switzer-land, preliminary results of which havealready been communicated (ll), and theywere attending centers in India, Africa, andSouth America. The remainder (19 percent)were from the Medical Research CouncilUnit at the Sungei Buloh Leprosarium,Malaysia, and also entered drug trials aspreviously untreated patients. The biopsiesfrom these 100 patients of this study rep-resent the most recently received in thisunit up to the time of this writing (August1978). The lepromatous classification in-cluded polar lepromatous (LLp) and sub-polar lepromatous (LLs) (13 . 31 ."5) and wasestablished by clinical findings, multipleslit-skin smears, and the biopsy itself.
Skin biopsies were taken under local an-esthesia by standard technics (n), fixed ineither 10 percent formalin or a modificationof formol-Zenker, embedded in paraffin
Editor's Note: One of the reviewers of the manu-script points out that "Indice Bibliografico de Lepra, -
1500-1943, Vol. I, organized by Luiza Keffer, andpublished by the Biblioteca do Departamento de Pro-filaxia da Lepra do Estado de sao Paulo, Brazil, in1944, contains approximately 70 references to articlesdealing with bacillemia in leprosy published between1889 and 1940.
47, 3 Comb & McDougall: Untreated LL: Histopathology of Cutaneous Vessels 501
TABLE 1. Type of skin vessel, lesion ob-served, and numbers (percent) in skin biop-sies from 100 patients with untreated lep-romatous leprosy.
Numberof cases
(alsoType of vessel and lesion^percent)
I. Small vessel lesiona. Presence of bacilli in the
endothelium^ 100
2. Large vessel lesionsa. Presence of bacilli in the
endothelium or vessel wall (media)^85
h. Hyalinization, fibrosis, and/orinfiltration of the vessel wallby macrophages (in differentdegrees) 85
c. Granuloma in the vessel wall^9
d. Thrombosis^ 2e. No abnormality found^ 15
wax, and cut in serial sections at 5 microns.These were stained with hematoxylin andeosin, the Fite-Faraco modification ofZiehl-Neelsen, or with a combined Massontrichrome and Fite-Faraco (TRIFF) ( 12 ).
RESULTSBlood vessel lesions were divided into
two groups according to the size of affectedvessels: a) small vessel lesions included le-sions of the papillary capillaries, arterioles,and venules of the subepidermal plexus andnew vessel formations in lepromatous infil-trates and b) larger vessel lesions consistedof lesions of arteries and veins of the sub-dermal vascular plexus and subcutaneoustissue.
The incidence of lesions in these twogroups of vessels and other cutaneousstructures is shown in Table I.
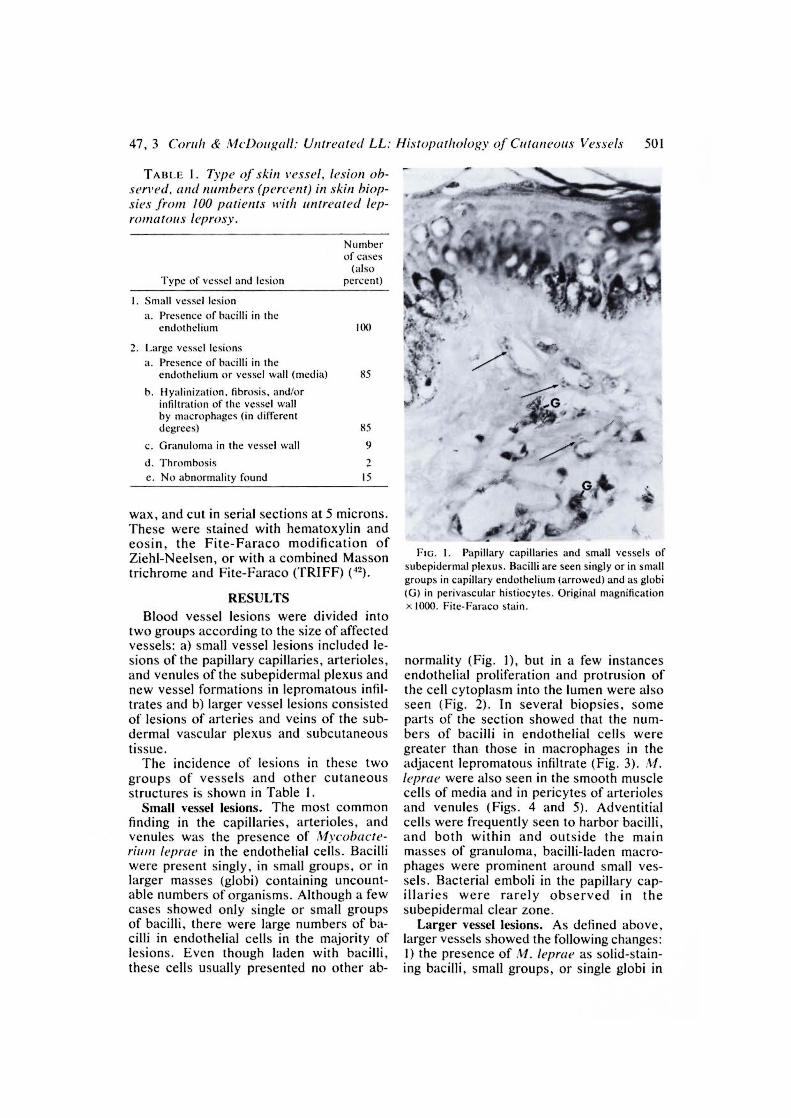
Small vessel lesions. The most commonfinding in the capillaries, arterioles, andvenules was the presence of Mycobacte-rium leprae in the endothelial cells. Bacilliwere present singly, in small groups, or inlarger masses (globi) containing uncount-able numbers of organisms. Although a fewcases showed only single or small groupsof bacilli, there were large numbers of ba-cilli in endothelial cells in the majority oflesions. Even though laden with bacilli,these cells usually presented no other ab-
FIG. I. Papillary capillaries and small vessels ofsubepidermal plexus. Bacilli are seen singly or in smallgroups in capillary endothelium (arrowed) and as globi(G) in perivascular histiocytes. Original magnificationx 1000. Fite-Faraco stain.
normality (Fig. 1), but in a few instancesendothelial proliferation and protrusion ofthe cell cytoplasm into the lumen were alsoseen (Fig. 2). In several biopsies, someparts of the section showed that the num-bers of bacilli in endothelial cells weregreater than those in macrophages in theadjacent lepromatous infiltrate (Fig. 3). Al./eprae were also seen in the smooth musclecells of media and in pericytes of arteriolesand venules (Figs. 4 and 5). Adventitialcells were frequently seen to harbor bacilli,and both within and outside the mainmasses of granuloma, bacilli-laden macro-phages were prominent around small ves-sels. Bacterial emboli in the papillary cap-illaries were rarely observed in thesubepidermal clear zone.
Larger vessel lesions. As defined above,larger vessels showed the following changes:1) the presence of At leprae as solid-stain-ing bacilli, small groups, or single globi in

502^ International Journal of Leprosy^ 1979
FIG. 2. Terminal arteriole within the granuloma, showing proliferation and protrusion of endothelial cellsinto the lumen, and the presence of single, solid-staining bacilli within them. Original magnification x 1000.Fite-Faraco stain.
FIG. 3. Globi (G) in the endothelial cells of collapsed venules within the lepromatous granuloma. The densityof bacilli in the vessel is greater than in macrophages of the surrounding granuloma. Original magnificationx 1000. Fite-Faraco stain.

‘11111111P
e
4.•
47, 3 Condi^McDeo,,all: Untreated LL: Ilistopathology of Cutaneous Vessels^503
I'm. 4. Solid-staining bacilli are seen in the media of an arteriole in the lower (fermis. Original magnification
x 1000. Fite-Faraco stain.
a) the endothelium, b) smooth muscle (me-dia), and c) pericytes; 2) asymmetrical fi-brosis and homogenization of the vesselwall; 3) lepromatous infiltration in the ves-sel wall; 4) thrombosis and recanaliza-tion of the veins without any histologicalchanges in adjacent tissues.
Endothelial phagocytosis of A/. /epraewas also the commonest feature of largervessels, and here again the presence of ba-cilli was usually not accompanied by sig-nificant pathological changes in these hostcells (Fig. 6). However, the majority of ves-sels, especially veins (Figs. 7 and 8), con-tained bacilli in other layers in addition tothe endothelium. Hyalinization, fibrosisand infiltration of the vessel wall by mac-rophages were features in some arterieswhere the endothelium, loaded with bacilli,projected into the lumen (Figs. 9 and 10).
FIG. 5. Heavy endothelial bacillation in arteriole(A) and venule (V) in subepidermal plexus, obscuringmost of the nuclei. Bacilli are also present in pericytes
farrowed). Original magnification x 1000. "FRIFF stain.

•*A.
r
10iiP
•---oloy,„10.,...ev;iise-4,7.; 4,^b.
^Zla^e";:lY 00.40^sa
,^;144CAP Ira 4.4^111;N.^)110:".^AAP'^44^.401‘•
a.^•^.^ tap .4^4 1/0^41.'^•
•
gr:. "Or amp
4440
40*
*^414 IN^Pik^p.% ko44,8^sir
le•
• qv. 4•• ..486
411‘ A itik^Itt Nso
1•114
elf
‘1"°.14. sr
I^ot
•■•
504^ International Journal of Leprosy^ 1979
FIG. 6. Numerous bacilli farrowed) in endothelial cells of a vein in the subdermal plexus, with minimaledema and histiocytic infiltration of the vessel wall. Original magnification x400. TRIFF stain.
FIG. 7. Single bacilli and small globi are seen in media of a small venule in the mid-dermis. Original mag-nification x1000. TRIFF stain.
• --^'^•^'

47, 3 Coruh^.1I•Dodf,nill: Untreated LL: Ilistopathology of Cutaneous Vessels^505
FIG. 8. Globi in smooth muscle cells and pericytes of a larger vein in the subdermal plexus. Original
magnification x 1000. Fite-Faraco stain.
Lepromatous infiltrates in the vessel wallwere observed in 9 patients, and in some ofthese, lepra (Virchow) cells had accumu-lated in the intima and media, with narrow-ing of the lumen (Fig. 11). In one instance,intima and media were completely replacedby the infiltrate, the muscle layer beinghardly visible around the granuloma (Fig.12): the endothelial cells lining the narrowcleft-like lumen were packed with bacilli(Fig. 13).
Organized and recanalized thrombi wereobserved in biopsies from two patients, inone of which solid-staining bacilli werepresent in the shrunken, fibrotic intralumi-nal mass (Fig. 14). Fibrinoid necrosis, neu-trophil polymorphonuclear cell infiltrate orleukocytoclasis were not observed in anyof the 100 biopsies in this study.
Lesions of other structures of the skin.Nerves and arrector pili muscles contained
leprue in all of the biopsies. Hair folli-
Fic. 9. Asymmetrical fibrosis in an arteriole wall, which harbors single bacilli and a globus (G) which isprobably within the cytoplasm of an infiltrating macrophage. Original magnificati
ntro^EslQn x1(100. Fit.--itrudoS.co.stain.
.•-e
Reinaldo Quagliat(I- -11"^ /-"N^/-,1^•

•• ••4,^-•r_st.2,„ •^• •
4 Z'l■^.• 4.
e *"4^'1'21^et- ),r, •••■/'^••••■^•..." 4°.
rg %Kr
506^ International Journal of Leprosy^ 1979
^. dr^*^1.°- •,„,^I ^-<^ -MI 4..,^_a
"0 .. Q11181°.•^,1 11 .1* / t "1,14 itio ., .., too•-• ,^or.
4rAga) ..,,....• fr. tr -Ag •%^ill
6
401114111W^106
■•14'°9 00'4elt
IP% jig, JO-‘IP.-
41^
FIG. 10. Proliferation and protrusion into the lumen (L) of endothelial cells containing numerous M. Ieprae,in a small arteriole. The wall was partly fibrotic and infiltrated by macrophages. Original magnification x 1000.Fite-Faraco stain.
Iles were present in 87 of the 100 biopsiesand in 67 (77 percent) of them, bacilli werepresent in the outer root sheath cells. Ba-cilli were also found in the inner root sheathcells on one occasion and around the hairshaft in the infundibulum in biopsies fromtwo patients.
FIG. 11. Accumulation of Virchow (lepra) cells inthe intima and media of a subcutaneous vein. Originalmagnification x400. Fite-Faraco stain.
No sweat glands could be found in thebiopsies of 9 patients, probably because ofobliteration by diffuse leprous infiltrate, butbacilli were found in the secretory or ductalcells, or in the lumen, in 54 out of the re-maining 91 biopsies (59 percent).
DISCUSSIONI. The incidence of vascular lesions. Al-
though the presence of M. /eprtie in vas-cular endothelial cells has been recognizedsince the work of Neisser in 1881 ( 2 - 1), sur-prisingly few detailed studies have been un-dertaken on the incidence of vessel involve-ment in skin biopsies.
Fite ( 10) and Kaur, el al. ('") examinedskin biopsies from different types of lep-rosy patients and found vascular lesions in42 and 50 percent respectively, while Des-ikan and Iyer ( 5 ) found an incidence of63 percent in lepromatous and borderlinecases. Our present findings are very muchin agreement with those of Fite who notedthe common occupation of small vessels by

..- --^- . 3, ' • 4,---r..:^-- ,^.• _; .-Afr". ' ° - '..—. „,:-^....." - ...a/.... e„ ,,..^. •^.......„,,....... A^' .../ . . leg.js^--.
p `/'' ...:'',..;;;::.''''':'i*: "f*44, .: .'7.:.' ii#:
,,,..tp,^,-.,,,,.:2Z.,.;'.... ,,...." .';.' ,^• :.^-,• -.,,,. .... ,..^.0,- ■^...„..., _ .^,,^r I , .^.•^.- __,. 4/r. it,. .,--4,,,,7-„ I . j,4 ,,,, •9 , -. ; ,..,,s,•,,,4,-,/,
: ?-.5 --(;--: --..f•Ze',,rtYPINN.,,.. ,
re4 • t. ' 4". ,.. .-• 4. v4I , - - ,...,e^; .,,:si .....^,„ .4,4 ..fli:...^4-^r. 4 .^- • 4'
• .2S# 4''%A
t .4v. to, .6,,^...- .,;s. - ..-, l..,..., e0,...,..,,^, . •^,..„,„..
,0 <at4.• C,1,1 ■Ir •^tt '172
47, 3 Coral, & McDougall: Untreated LL: Histopathology of Cutaneous Vessels 507
FIG. 12. Lepromatous infiltration in the wall of alarge subcutaneous vessel. Cleft-like lumen (L) is stillpresent. Original magnification x400. TRIFF stain.
bacilli and their presence in the media andadventitia in addition to the endothelium,together with lepromatous infiltration of thevascular wall. Popov ( 2") and Santos andBeja ( 7) studied cutaneous vessel lesions indifferent types of leprosy patients, usingthe terms "sclerosis and homogenization inthe vessel wall," "lepromatous endarteri-tis" and "lepromatous obliterative panar-teritis." Other authors (1.2.4,9,14,17.25,28,32)have described the presence of Al. lepraein the endothelium of blood vessels in skin,nerves, and nasal mucous membranes. Theincidence of vascular lesions in previous
studies which are comparable with our ownis shown in Table 2.
II. The significance of the presence of M.leprae in vessels walls: (A) Endothelial liningcell; inthna. The very considerable accu-mulation of bacilli within endothelial liningcells of blood vessels of skin, as confirmedin this study, is not seen in other mycobac-terial diseases, even in the miliary form oftuberculosis. The finding of organisms inthat location is unusual in other diseasesapart from those due to the Rickettsiae andcertain viral infections where the vascularendothelium may be an important site ofreplication and shedding ( 25). We associateit with the known, continuous, and totallyasymptomatic bacteremia of untreated lep-romatous leprosy ("• s") while acknowledg-ing the difficulty of knowing whether thisprocess occurs at an early stage in the de-velopment of this type of leprosy or only inthe later stages. Light and electron micro-scopic studies indicate that under normalconditions the vascular non-reticuloendo-thelial system is not phagocytic. On theother hand, some of the factors which maystimulate or activate endothelial cells to be-come phagocytic have been described byCotran ("), Florey ("), and Luk and Simon( 22). With regard to experimental materialsuch as colloidal carbon, "overloading" of
V-Jib^tr.-%; ,^ •^
40010611011P
11411416.44;"ELY4414
44,41;4144 , 41011t140„ 000%,• IPZ"d*^111J
ttFIG. 13. Acid-fast bacilli were present in virtually every endothelial lining cell of this section, from the same
vessel as shown in Fig. 12. Original magnification x 1000. 'MIFF stain.

508^ International Journal of Leprosy^ 1979
FIG. 14. Thrombosis and recanalization in a larger vessel of the subdermal plexus. Note solid bacilli (ar-
rowed) in the thrombotic mass. Original magnification x 1000. Fite-Faraco stain.
the circulation has been shown to be im-portant in achieving this. It may be that thecontinued presence of 10 5 ;11. leprae per mlof blood in a disease where the incubationperiod is commonly between two and fiveyears, and may be longer, accounts for thefinding of so many organisms in the endo-thelium of blood vessels in skin biopsiestaken when the disease is established. Us-ing a related organism, Mycobacterium lep-raemurium, the cause of rat leprosy, Kato
and Gozsy (") stated that in the earlystages, the endothelium was in fact activat-ed by injury or infections and so was notsubject to the entry of bacilli. In advancedinfection, they concluded that endothelialactivation broke down, contributing to thegeneral dissemination of the infection. Thepotentially damaging effect of stasis on theendothelial cell has been fully discussed byRyan (").
The finding of numerous solidly-staining
TABLE 2. The incidence of vascular lesions in previous publications compared with thepresent studs'.
Date ofpublication Author(s) Type of leprosy
Numberof
patients
Percentof vesselinvolve-
ment
1941 Fite ( 10 ) Different types, from lepromatousto tuberculoid 77 42
1972 Desikan and lyer ( 8 ) Lepromatous and borderline 100 63
1976 Kaur, et al. (IS) Different types, from lepromatousto borderline 35 .5()
1978 The present study Lepromatous (polar and sub-polar) 100 100

47, 3 Coruh^McDougall: Untreated LL: Ilistopathology of Cutaneous Vessels 509
organisms is indicative of bacillary viability(:w) and, taken with the presence of manyglobi, is strongly in favor of active prolif-eration of bacilli in the intimal layer. Fromendothelial cells, as pointed out by Desikanand lyer ('), spread could easily occur tomost parts of the body. Furthermore, it ispossible that large numbers of bacilli couldmove from one body site to another in viewof the known circulation of endothelial cells( 3 .'"). Recent experimental work on thepossible role of biting arthropods ( 27) and ofcertain flies, including the biting stable fly,,S7omoxys (l 2 ), in the transmission of lep-rosy raise the possibility that there may bemore to the localization of ..11. /eprae in su-perficially placed blood vessels than merephagocytosis due to overloading of theblood with bacilli or the selection of cellswhich happen to lie in a body plane wherethe temperature and other tissue factorsare conducive to survival. Just as the pro-liferation of leprosy bacilli in the nose oflepromatous patients is favorable for thespread of the organisms to the environment(""), so perhaps one should consider thattheir presence in large numbers in the en-dothelium of skin vessels is favorable fortransmission by biting insects, such as ap-pears to be the case for certain viruses andRickettsiae.
B. Smooth muscle cells; media. Both inthis study of 100 patients and in a widerange of other biopsies from lepromatouspatients seen in this unit during the pasteight years, including the examination ofvessels accompanying the biopsy of super-ficially placed peripheral nerves, we havebeen impressed by the numbers and densityof bacilli which may be seen in smoothmuscle cells of the media (Figs. 4, 7, 8, and9). Solidly-staining bacilli and globi are ascommon in this layer at the outset, i.e., be-fore treatment, as they are in other smoothmuscle tissues such as the arrector pili anddartos. The present study clearly does notdeal with the histopathological findings af-ter treatment, but in discussing the signifi-cance of bacilli in this layer as seen on thefirst biopsy, it is relevant to record that theyare liable to a) linger in this site, as they doin the arrector pili, hair follicles, and der-mal nerves, sometimes after many years oftreatment, thus persisting in the bacterio-logical sense ( 11 ) or b) give rise to an im-
mune-complex syndrome of which erythe-ma nodosum leprosum (ENL) in the skin isa well-known component.
While reporting new clinical and bacte-riological data, Davey and Rees ( 7) havesummarized the published work on theoverwhelming importance of the nasal dis-charge in the dissemination of leprosy ba-cilli into the environment. As regards theroute of entry, however, despite the exper-imental work on inhalation quoted above,the commonest route of infection of humanbeings is, in fact, still unknown and difficultto investigate. Direct inoculation throughthe skin remains a distinct possibility. Indescribing histopathological findings in theearly lesions of leprosy, Ridley ( 31 . 32) hasreviewed the evidence for this route of en-try. The present study clearly deals withlepromatous patients at a relatively ad-vanced stage and sheds no light on the skinas a possible portal of entry. It neverthelessunderlines the enormous numbers of bacilliwhich have established themselves and aresuccessfully multiplying in this body tissue,many of them in blood vessel walls, includ-ing the proliferated capillaries of the lep-romatous infiltration. From the endothe-lium, bacilli may continuously contaminatethe blood stream; in the media, they maypersist despite many years of treatment."Escape" of viable bacilli from the skinand hence into the environment may ob-viously occur from cuts, abrasions,scratches, or as a result of skin ulcerationdue to secondary infection and possiblyalso in the sweat. An additional exit route,and one to which the present study lendssome support, concerns the vast numbersof bacilli which are present not only in skinmacrophages but also in the walls of bloodvessels, ideally situated for uptake by bitingarthropods. Particularly if the mode offeeding involves extravasation of bloodfrom a lacerated capillary to form a pool inthe tissues, as it may be in the case of mos-quitoes ("), heavy involvement of cuta-neous vessels could be advantageous to theleprosy bacillus in pursuing this route of in-fection.
SUMMARYSkin biopsies from 100 patients with un-
treated lepromatous leprosy from Malay-sia, India, Africa, and South America were

510^ International Journal of Leprosy^ 1979
examined with particular regard to patho-logical changes in intima, media, or adven-titia of blood vessels and to the presence ofleprosy bacilli in these layers.
Bacilli were found in capillaries, venules,or arterioles in all cases, and in many in-stances they were present in endothelial lin-ing cells or smooth muscle in large masses(globi). In several cases, solid-staining ba-cilli in endothelial lining cells were espe-cially prominent.
The findings are discussed in relation toa) the continuous bacteremia of leproma-tous leprosy, b) the role of endothelial cellsin phagocytosis, c) smooth muscle cells ofthe media as a site in which bacilli may per-sist, and d) the transmission of human lep-rosy by biting arthropods.
RESUMENSe examinaron biopsias de piel de 100 pacientes con
lepra lepromatosa, originarios de Malasia, India, Af-
rica y Sudamerica. El examen se hizo con particular
atenciOn a los cambios patoltigicos en Ia intima, mediay adventicia de los vasos sanguineos, y a Ia presencia
de bacilos de la lepra en estas capas.Se encontraron bacilos en capilares, venulas o ar-
terioles de todos los casos examinados. En muchos
casos los bacilos se encontraron presentes en las ce-lulas endoteliales o en el nnisculo liso en grandes ma-
sas o globi. En varios casos fue particularmente prom-inente Ia presencia de bacilos tenidos sOlidamente en
las celulas endoteliales.Los hallazgos se discuten en relaciOn a a) la bac-
teremia continua de la lepra lepromatosa, b) el papelde las celulas endoteliales en la fagocitosis, c) las ce-
lulas del nnisculo liso de la media, como un sitio en
el cual pueden persistir los bacilos y d) la transmisiOn
de la lepra humana a traves de la mordedura de artrti-
podos.
RESUME
On a examine tine serie de biopsies recueillies chez100 malades souffrant de lepre lepromateuse non trai-
tee, en Malaisie, en Inde, en Afrique, et en Ameriquedu Sud. Ces biopsies ont ete examinees afin d'etudier
les modifications pathologiques survenues au niveau
de l'intima, de Ia media ou de l'adventice des vais-
seaux sanguins, et egalement pour mettre en evidence
Ia presence de bacilles de Ia lepre dans ces tuniques.Des bacilles ont ete trouves dans les capillaires,
dans les venules et dans les arterioles, dans tons lescas; chez beaucoup de malades, on trouvait egalementdes amas de bacilles (globi) dans le revetement cellu-
laire endothelial ou dans les muscles lisses. Dans plu-
sieurs cas, Ia presence de bacilles colorables de faconmassive, dans les cellules du revetement endothelial,
etait particulierement notable.
Ces observations sont discutees en rapport avec a)
Ia bacteremie persistente dans Ia lepre lepromateuse,b) le role des cellules endotheliales dans la phagocy-
tose, c) lit localisation persistente des bacilles dansles cellules musculaires lisses de Ia media, et (I)Ia transmission de lepre humaine par la morsure
d'arthropodes.
Acknowledgments. We are indebted to Professor S.
J. Yawalkar and the Medical Department of Ciba-Gei-
gy, Basle, Switzerland for the permission to reportfindings in patients taking part in a trial of rifampin
(Rimactane'), and to Dr. R. J. W. Rees of the NationalInstitute for Medical Research, Mill Hill, London, for
permission to refer to patients under treatment in Sun-gei Buloh Leprosarium, Malaysia. A. C. McDougall
is supported by the British Leprosy Relief Association
(LEPRA) and by a grant from the Oxfordshire AreaHealth Authority (Teaching).
REFERENCESI. BINI.ORD, C. H. and M1.51.1t, W. M. Pathology of
tropical and extraordinary diseases. In: An Atlas,
Vol. I. C. H. Binford and D. H. Connor, eds.,Washington, D.C.: Armed Forces Institute of Pa-
thology, 1976, pp 205-225.2. Bormusiolus, J. Ultrastructural changes in blood
vessels of peripheral nerves in leprous neuropa-thy. II. Borderline, borderline-lepromatous lep-
rosy patients. Acta Neuropathol. (Berl.) 40 (1977)
21-39.3. BOUVIER, C. A., MAURICE, P. A. and Rocit, R.
Resultes obtenus par la leucoconcentration. Bull.
Schweiz. Akad. Med. Wiss. 20 (1964) 15-26.4. BROWNE, S. G. Leprosy. Basle: Documenta Gei-
gy, 1970.
5. COCHRANE, R. G. and DAVEY, T. F. Leprosy in
Theory and Practice. Bristol: John Wright and
Sons Ltd., 1964.
6. Co FRAN, R. S. Endothelial phagocytosis: An elec-
tron microscopic study. Exp. Mol. Pathol. 4(1965) 217-231.
7. DAvi:v, F. F. and REFS, R. J. W. The nasal dis-charge in leprosy; clinical and bacteriological as-
pects. Lepr. Rev. 45 (1974) 121-134.8. DESIKAN, K. V. and IsER, C. G. S. The distri-
bution of .1/. leprae in different structures of the
skin. Lepr. Rev. 43 (1972) 30-37.
9. DRUrz, D. J., CHEN, T. S. N. and WEN-HSIAN,
L. The continuous bacteremia of lepromatous lep-rosy. N. Engl. J. Med. 287 (1972) 159-164.
10. FITE, G. L. The vascular lesions of leprosy. Int.
J. Lepr. 9 (1941) 193-202.I. FLORLY, L. The uptake of particulate matter of
endothelial cells. Proc. R. Soc. 166 (1967) 375-
383.
12. GLATER, J. G. The fly as potential vector in the
transmission of leprosy. Lepr. Rev. 46 (1967) 279-286.
13. GogpoN, R. M. and LUN1SDEN, W. H. R. A study
s
•

47, 3 Corral & McDougall: Untreated LL: Histopatholos,q of Cutaneous Vessels 511
4
of the behavior of the mouth-parts of mosquitoeswhen taking up blood from living tissue: togetherwith some observations on the ingestion of micro-filariae. Ann. Trop. Med. 33 (1939) 259-278.
14. HAENSCII, R. and SCHNIALBRUCH, H. Ziir Mor-
phologie der Leprazelle. Arch. Dermatol. Forsch.241 (1971) 179-187.
15. HARMAN, D. J. Biopsies in leprosy. Lepr. Rev.46 (1975) 125-134.
16. HLRHEUVAL, H. and Fouum, M. Etude compar-ative de l'endothelium vasculaire et de sa basalesur coupe et en concentration. C. R. Soc. Biol.158 (1964) 137-141.
17. Jou, C. K. Pathology of peripheral nerve lesionsin lepromatous leprosy: a light and electron mi-croscopic study. Int. J. Lepr. 39 (1971) 251-268.
18. KA o, L. and GOZSY, B. Studies on the physio-pathology of experimental murine leprosy. Retic-uloendothelial, capillary, and mast cells response.Rev. Canad. Biol. 23 (1964) 217-226.
19. KAUR, S., WAIII, P. L., CIIAKRAVARTI, R. N.,Sooui, J. S., VADHWA, M. B. and KUER, A. S.Peripheral vascular deposit in leprosy. Int. J.Lepr. 44 (1976) 332-339.
20. KLINGMOLLER, V. Die Lepra. Vol. X, Part 2 inJadassohn's Handbuch der Haut- and Ge-schlechtskrankheiten. Berlin: Julius Springer,1930, pp 542-546.
21. LANGUILLON, J., YAWALKAR, S. J. and Mc-DOUGALL, A. C. Therapeutic effects of addingRimactane" (rifampicin) 450 mg daily or 1200 mgonce monthly in a single dose to dapsone 50 mgdaily in patients with lepromatous leprosy. Paper292, Abstracts of the XI International LeprosyCongress, Mexico City, 1978.
22. LUK, S. C. and SIMON, G. T. Phagocytosis of col-loidal carbon and heterologous red blood cells inthe bone marrow of rats and rabbits. Am. J. Pa-thol. 77 (1974) 423-438.
23. McDouGAI.E, A. C., RI:Es, R. J. W., WEDDELE.,A. G. M. and KANAN, M. W. The histopathologyof lepromatous leprosy in the nose. J. Pathol. 115(1975) 215-226.
24. METCHNIKOFF, E. Lecture on the comparativepathology of inflammation. London: Dover, 1893.
25. MINIS, C. A. The Pathogenesis of Infectious Dis-eases. London: Academic Press, 1977, p 132.
26. Mt rsuon, K. Atlas of Leprosy. Okayama, Japan:Chotokai Foundation, 1952, p 20.
27. NARAYANAN, E., SHANKARA MANJA, K., BEDI,B. M. S., KIRCHHEIMER, W. F. and BALASU-
BRAtiNtANYAm, NI. Arthropod feeding experi-ments in lepromatous leprosy. Lepr. Rev. 43(1972) 188-193.
28. PANIKAROVSKY, V. V., GRIGORIYAN, A. S. andBUSYGINA, M. V. Histochemical characteristicsof leprous lesions of the buccal mucosa. Vestn.Dermatol. Venerol. 44 (1970) 32-38.
29. POPOV, K. P. Veranderungen in ein Blutgefassendes Derma bei Lepra. Derm. Wschr. 152 (1966)945-950.
30. REEs, R. J. W. and VALENTINE, R. C. The ap-pearance of dead leprosy bacilli by light and elec-tron microscopy. Int. J. Lepr. 30 (1962) 1-9.
31. RIDLEY, D. S. Pathology and bacteriology of earlylesions in leprosy. Int. J. Lepr. 39 (1971) 217-224.
32. RtotELY, D. S. The pathogenesis of the early skinlesion in leprosy. J. Pathol. 111 (1973) 191-206.
33. RinEEY, D. S. and JOPLING, W. H. A classifica-tion of leprosy for research purposes. Lepr. Rev.33 (1962) 119-128.
34. RIDLEY, D. S. and JOPLING, W. H. Classificationof leprosy according to immunity: a five groupsystem. Int. J. Lepr. 34 (1966) 255-273.
35. RIDLLN", D. S. and WATERS, M. F. R. Significanceof variations within the lepromatous group. Lepr.Rev. 40 (1969) 143-152.
36. RYAN, T. J. Vasculitis. In: Physiology and Patho-physiology of the Skin, Vol. 3., A. Jarrett, ed.,London: Academic Press, 1974.
37. SANTOS, H. S. and BEJA, M. L. C. Histopatho-logia dos vasos cutaneous na lepra. Rovisco Pais8 (1969) 3.
38. SHANKARA MANJA, K., BEDI, B. M. S., KASTURI,
G., KIRCFIIIEINtER, W. F. and BALASUBRAHNIAN-
YAM, NI. Demonstration of .Ifycobacterium lepraein the peripheral blood of leprosy patients. Lepr.Rev. 43 (1972) 181-187.
39. SHEPARD, C. C. Temperature optimum of .Viyea-bacterium leprae in mice. J. Bacteriol. 90 (1965)1271-1275.
40. SKINSNES, 0. K., SAKURAI, I. and AQUINO, 'f. I.Pathogenesis of extremity deformity in leprosy. Apathological study on large sections of amputatedextremities in relation to radiological appearance.Int. J. Lepr. 40 (1972) 375-388.
41. WATERS, M. F. R., REES, R. J. W., MCDOUGALL,A. C. and WEDDELL, A. G. M. Ten years of dap-sone in lepromatous leprosy: clinical, bacteriolog-ical, and histological assessment and the findingof viable leprosy bacilli. Lepr. Rev. 45 (1974) 288-298.
42. WHEELER, E. A., HAMILTON, E. G. and HAR-
MAN, D. J. An improved technique for the histo-pathological diagnosis and classification of lepro-sy. Lepr. Rev. 36 (1965) 37-39.




![eimiay Eiece o aua esisace o - ILSLila.ilsl.br/pdfs/v52n2a02.pdf40 0 1 ^ Intrntnl rnl f pr ^ 19 1 5 ^5 ^ 1 CG E WE [0 6] E IGUE. In vtr fft f rph-CG ntrtn n 3 rl nrprtn nt bll Mnlr](https://img.pdfslide.us/doc/110x75/60bc01efeeb29a485f147a4f/eimiay-eiece-o-aua-esisace-o-40-0-1-intrntnl-rnl-f-pr-19-1-5-5-1-cg-e-we.jpg)
























