Embed Size (px)
Citation preview
UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Falls in the Elderly
C. Bree Johnston, MD MPHC. Bree Johnston, MD MPH
Copyright May 2001Copyright May 2001
UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Overview PrevalencePrevalence Clinical ImportanceClinical Importance Risk Factors & EtiologyRisk Factors & Etiology Evaluation Evaluation Prevention & ManagementPrevention & Management Falls & restraint useFalls & restraint use SummarySummary

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Falls: Mrs. F. Mrs. F. is an 80 year old woman who lives Mrs. F. is an 80 year old woman who lives
alone. She just came in to your office for alone. She just came in to your office for follow up of a fall resulting in a Colles’ follow up of a fall resulting in a Colles’ fracture. She has had two other falls over the fracture. She has had two other falls over the past year and a half. She is scared of falling past year and a half. She is scared of falling again. She has a history of osteoarthritis and again. She has a history of osteoarthritis and anxiety/depressison. She is on naproxen anxiety/depressison. She is on naproxen 500mg BID and diazepam 5mg BID prn500mg BID and diazepam 5mg BID prn
UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Falls in the Elderly PrevalencePrevalence Clinical ImportanceClinical Importance Risk Factors & EtiologyRisk Factors & Etiology Evaluation Evaluation Prevention & ManagementPrevention & Management Falls & restraint useFalls & restraint use SummarySummary

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Prevalence
30% of those over 65 fall annually30% of those over 65 fall annually Half are repeat fallersHalf are repeat fallers Falls go up with each decade of lifeFalls go up with each decade of life Over half of those in nursing homes and hospitals Over half of those in nursing homes and hospitals
will fall each yearwill fall each year

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Falls in the Elderly PrevalencePrevalence Clinical ImportanceClinical Importance Risk Factors & EtiologyRisk Factors & Etiology Evaluation Evaluation Prevention & ManagementPrevention & Management Falls & restraint useFalls & restraint use SummarySummary

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Impact of Hip Fractures 1% of falls result in hip fracture1% of falls result in hip fracture $2 billion + in medical costs annually$2 billion + in medical costs annually 25% die within 6 months25% die within 6 months 60% have restricted mobility60% have restricted mobility 25% remain functionally more dependent25% remain functionally more dependent

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Falls Cause Morbidity and Mortality
Mortality: found down syndrome, indirect effectsMortality: found down syndrome, indirect effects Fractures: 6% of fallsFractures: 6% of falls Soft tissue injury, head injury, subdural hematomaSoft tissue injury, head injury, subdural hematoma Fear of falling can result in decreased activity, Fear of falling can result in decreased activity,
isolation, and further functional declineisolation, and further functional decline Nursing home placement and loss of Nursing home placement and loss of
independenceindependence

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Falls in the Elderly PrevalencePrevalence Clinical ImportanceClinical Importance Risk Factors & EtiologyRisk Factors & Etiology Evaluation Evaluation Prevention & ManagementPrevention & Management Falls & restraint useFalls & restraint use SummarySummary

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Falls are Multifactorial
Intrinsic Factors Extrinsic Factors
FALLS
Medical conditions
Impaired vision and hearing
Age related changes
Medications
Improper use of assistive devices
Environment

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Normal Changes with Aging NeurologicNeurologic
Increased reaction timeIncreased reaction time Decreased righting reflexesDecreased righting reflexes Decreased proprioceptionDecreased proprioception
Vision ChangesVision Changes Decreased accommodation & dark adaptationDecreased accommodation & dark adaptation
Decreased muscle massDecreased muscle mass

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Normal changes of Gait
Slower gaitSlower gait Decreased stride length and arm swingDecreased stride length and arm swing Forward flexion at head and torsoForward flexion at head and torso Increased flexion at shoulders and kneesIncreased flexion at shoulders and knees Increased lateral swayIncreased lateral sway

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Dysmobility Dysmobility and falling closely relatedDysmobility and falling closely related 15% of those over 65 have trouble walking15% of those over 65 have trouble walking 1/4 men and 1/3 women over age 85 have 1/4 men and 1/3 women over age 85 have
difficulty with walkingdifficulty with walking 2/3 of people in hospital or NH unable to 2/3 of people in hospital or NH unable to
ambulate without assistanceambulate without assistance
UCSF Division of Geriatrics Primary Care Lecture Series May 2001
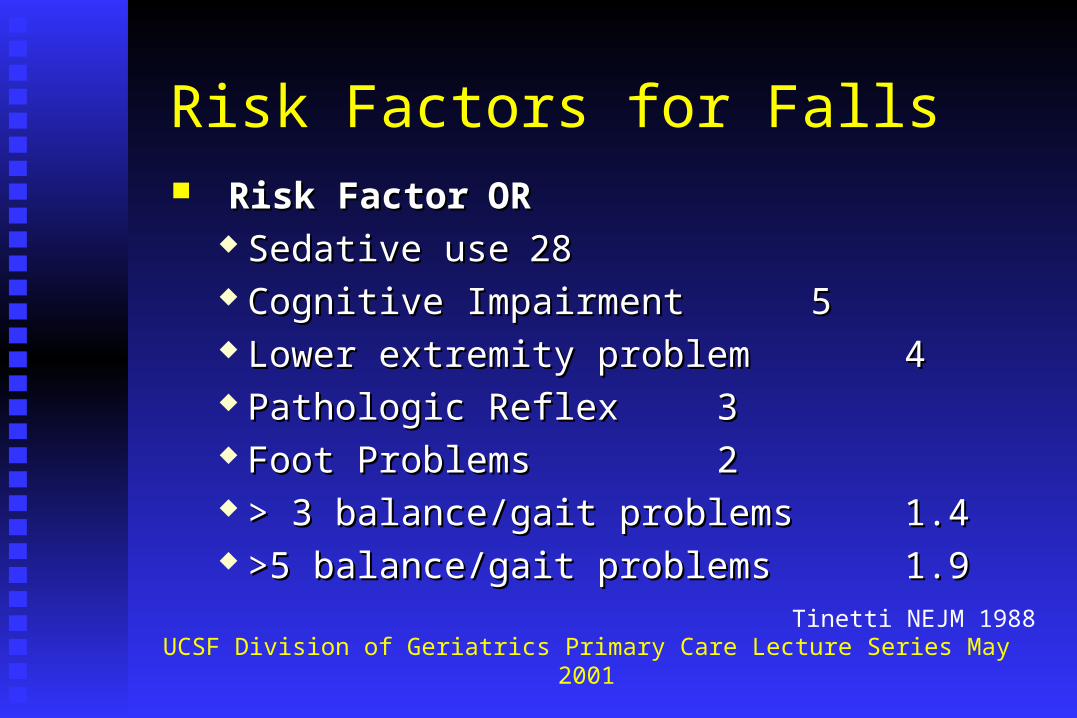
Risk Factors for Falls Risk FactorRisk Factor OROR
Sedative useSedative use 2828 Cognitive ImpairmentCognitive Impairment 55 Lower extremity problemLower extremity problem 44 Pathologic ReflexPathologic Reflex 33 Foot ProblemsFoot Problems 22 > 3 balance/gait problems> 3 balance/gait problems 1.41.4 >5 balance/gait problems>5 balance/gait problems 1.91.9
Tinetti NEJM 1988

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Common Pathologies associated with Falls Ophthalmologic diseasesOphthalmologic diseases Arthritis Arthritis Foot problems Foot problems Neurologic illnessNeurologic illness
Parkinson’s & related disordersParkinson’s & related disorders StrokesStrokes Peripheral neuropathyPeripheral neuropathy
Dizziness and dysequilibriumDizziness and dysequilibrium
UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Dizziness: A Multifactorial Syndrome Vertigo: BPV, Posterior CVA/TIA, Cervical Vertigo: BPV, Posterior CVA/TIA, Cervical Presyncope: Orthostatic, Dysrythmia, AnemiaPresyncope: Orthostatic, Dysrythmia, Anemia Dysequilibrium: Peripheral neuropathy, VisualDysequilibrium: Peripheral neuropathy, Visual Other: Anxiety, depressionOther: Anxiety, depression In older people, usually multifactorial In older people, usually multifactorial
Tinetti, Annals of Internal Med 2000Tinetti, Annals of Internal Med 2000

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Falls in the Community Accidents/environmentAccidents/environment 37%37% Weakness, balance, gaitWeakness, balance, gait 12%12% Drop attackDrop attack 11%11% Dizziness or vertigoDizziness or vertigo 8%8% Orthostatic hypotensionOrthostatic hypotension 5%5% Acute illness, confusion, drugs, Acute illness, confusion, drugs,
decreased vision decreased vision 18%18%
UnknownUnknown 8% 8%
Rubenstein JAGS 1988

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Falls in Residential Care
Generalized weaknessGeneralized weakness 31%31% Environmental hazardEnvironmental hazard 27%27% Orthostatic hypotensionOrthostatic hypotension 16%16% Acute illnessAcute illness 5%5% Gait or balance disorderGait or balance disorder 4%4% DrugsDrugs 5%5% Other or unknownOther or unknown 10% 10%
Rubenstein Ann Int Med 1990

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Medications and Falls Sedative-hypnotics, especially long acting Sedative-hypnotics, especially long acting
benzodiazepines, increase fallsbenzodiazepines, increase falls Small association between most psychotropics Small association between most psychotropics
and fallsand falls SSRIs and TCAs both incrsease fallsSSRIs and TCAs both incrsease falls Weak association between Type 1A Weak association between Type 1A
antiarrythmics, digoxin, diuretics, and fallsantiarrythmics, digoxin, diuretics, and fallsLeipzig JAGS 1999
Thapa NEJM 1998

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Falls in the Elderly PrevalencePrevalence Clinical ImportanceClinical Importance Risk Factors & EtiologyRisk Factors & Etiology EvaluationEvaluation Prevention & ManagementPrevention & Management Falls & restraint useFalls & restraint use SummarySummary

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Evaluation of Falls: History Location & circumstances of FallLocation & circumstances of Fall Associated symptomsAssociated symptoms Other falls or near fallsOther falls or near falls Medications (including nonprescription) and Medications (including nonprescription) and
alcoholalcohol Injury & ability to get upInjury & ability to get up

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Evaluation of Falls: Physical Examination
Supine and standing BP - alwaysSupine and standing BP - always Routine physical examinationRoutine physical examination
Focus on cardiovascular, MS, neuro, feetFocus on cardiovascular, MS, neuro, feet Vision and hearing evaluationVision and hearing evaluation Consider acute medical illness & deliriumConsider acute medical illness & delirium Formal gait and balance assessmentFormal gait and balance assessment

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Evaluation of Falls: Home Evaluation Can be performed by nurse, OT, PT, othersCan be performed by nurse, OT, PT, others StairsStairs LightingLighting ClutterClutter BathroomBathroom Specific hazards: cords, throw rugsSpecific hazards: cords, throw rugs

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Evaluation of Falls: Risk Factors for Injury
Osteoporosis assessmentOsteoporosis assessment Anticoagulation: Usual benefits outweigh risks Anticoagulation: Usual benefits outweigh risks
unless repeat or high risk fallerunless repeat or high risk faller Can the person get up from fall?Can the person get up from fall? Is there a way to notify others in case of falling?Is there a way to notify others in case of falling?

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Mrs. F. History reveals that she fell at home in the History reveals that she fell at home in the
bathroom at night, tripping over a bathmat. bathroom at night, tripping over a bathmat. Both other falls have been in similar Both other falls have been in similar circumstances. She was able to get up.circumstances. She was able to get up.
On PE, she has visual acuity of 20/100 with On PE, she has visual acuity of 20/100 with bilateral cataracts. She has mild OA of the bilateral cataracts. She has mild OA of the knees, with bunyon deformities of her feet and knees, with bunyon deformities of her feet and poor fitting shoes.poor fitting shoes.

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Mrs. F.
Her gait assessment shoes that she is unable to Her gait assessment shoes that she is unable to get up out of the chair without help. Her gait get up out of the chair without help. Her gait is hesitant and slightly wide based. is hesitant and slightly wide based.
Home evaluation reveals poor lighting in all Home evaluation reveals poor lighting in all rooms, multiple throw rugs in every room, rooms, multiple throw rugs in every room, and no grab bars or safety equipment in the and no grab bars or safety equipment in the bathroom.bathroom.
UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Mrs. F. She is weaned off of her diazepam over 3 monthsShe is weaned off of her diazepam over 3 months T-score on dexa is –3.0, and she is begun on T-score on dexa is –3.0, and she is begun on
alendronate, vitamin D, and calciumalendronate, vitamin D, and calcium She goes to ophthalmology and podiatry She goes to ophthalmology and podiatry PT begins exercises, followed by weight lifting PT begins exercises, followed by weight lifting
and exercise 3X a week at a Senior Centerand exercise 3X a week at a Senior Center She gets home safety equipment, improved She gets home safety equipment, improved
lighting, and gives away her throw rugs lighting, and gives away her throw rugs

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Formal Gait Evaluation
Get up and Go TestGet up and Go Test Tinetti Gait and Balance Evaluation (POMA)Tinetti Gait and Balance Evaluation (POMA)
Tinetti JAGS 1986
Podsiallo jAGS 1991
Mathias Arch Phys Med 1986

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
POMA: Balance Component
Sitting (in hard, armless chair)
Arising
Standing balance (immediate and delayed)
Balance with Nudge
Balance with Eyes closed
Balance with 360 degree turn Tinetti JAGS 1986

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
POMA: Gait Component
InitiationInitiation
Step length and heightStep length and height
Step symmetry & continuityStep symmetry & continuity
PathPath
Stance Stance
Ability to pick up speedAbility to pick up speed Tinetti JAGS 1986Tinetti JAGS 1986

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Common Causes of Abnormal Gait Difficulty arising from chairDifficulty arising from chair WeaknessWeakness
ArthritisArthritis Instability on first standingInstability on first standing Hypotension, Hypotension,
Weakness Weakness Instability with eyes closedInstability with eyes closed Proprioception Proprioception
Step height/lengthStep height/length ParkinsonismParkinsonism
Frontal lobe Frontal lobe Fear Fear

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Falls in the Elderly PrevalencePrevalence Clinical ImportanceClinical Importance Risk Factors & EtiologyRisk Factors & Etiology Evaluation Evaluation Prevention & ManagementPrevention & Management Falls & restraint useFalls & restraint use SummarySummary

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Prevention & Treatment Treat acute injury & underlying medical Treat acute injury & underlying medical
conditionsconditions Remove unnecessary medicationsRemove unnecessary medications Rehab, exercises, assistive devicesRehab, exercises, assistive devices Correct sensory impairmentsCorrect sensory impairments Environmental modifications & safetyEnvironmental modifications & safety Evaluate for osteoporosis treatmentEvaluate for osteoporosis treatment
UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Osteoporosis Calcium and vitamin D for most elders at riskCalcium and vitamin D for most elders at risk
Dawson-Hughes, NEJM, 1997Dawson-Hughes, NEJM, 1997
Osteoporosis evaluation and treatment Osteoporosis evaluation and treatment Hip protectors appear to protect from hip Hip protectors appear to protect from hip
fractures in those who wear themfractures in those who wear them Kannus, NEJM, 2000 Kannus, NEJM, 2000
Thiazides may help slightlyThiazides may help slightly Statins?Statins?

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Change Estimated Change in Risk
Quit smoking 38%
Treat impaired vision 50%
Stop sedatives 40%
Add 1 Gram Calcium 24%
Hip Protectors 50%?
Adapted from Stteve Cummings
Risk Factor Modifications for Fractures

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Hip pads to prevent hip fracture
““RCT” of 1801 frail subjects in FinlandRCT” of 1801 frail subjects in Finland Nursing home or frail community patients Nursing home or frail community patients Mean age 81Mean age 81 78% women78% women 63% assisted walking63% assisted walking
Kannus. NEJM;2000;343;1506-1513.Kannus. NEJM;2000;343;1506-1513.

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Fractures with Hip ProtectorsFractures with Hip Protectors 2.1% per year vs. 4.6% per year 2.1% per year vs. 4.6% per year
(p<.01) (p<.01) 40 patients needed to be treated with 40 patients needed to be treated with
hip protector for 1 year to prevent one hip protector for 1 year to prevent one fracturefracture
2.4% of falls resulted in hip fracture 2.4% of falls resulted in hip fracture when not wearing protectorwhen not wearing protector
0.4% resulted in hip fracture when 0.4% resulted in hip fracture when wearing protector (80% risk reduction)wearing protector (80% risk reduction)
But patient acceptance lowBut patient acceptance lowKannus. NEJM;2000;343;1506-1513Kannus. NEJM;2000;343;1506-1513

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
www.hipsavers.com

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Prevention of “Found Down” Syndrome
Lifelines
Accessible telephones
Teach in getting up off floor
Friendly phone calls or visitors for isolated elderly

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Falls: Primary Prevention
301 community dwelling elders with 1+ 301 community dwelling elders with 1+ risk factors for fallingrisk factors for falling
Intervention: adjustment in medications, Intervention: adjustment in medications, behavioral instructions, exercise programs behavioral instructions, exercise programs aimed at modifying risk factorsaimed at modifying risk factors
One year follow upOne year follow upTinetti et al. 1994 NEJMTinetti et al. 1994 NEJM

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Multifactorial Intervention
0
10
20
30
40
50
0 3 6 9 12
Months
% Falling
Control
InterventMoi
P = .04
Tinetti et al 1994 NEJM

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Exercise Training & Nutrition
-20
0
20
40
60
80
100
120
140
Exer Exer +Su
Sup Control
STUDY GROUP
% Change Muscle
strength
Exer
Exer + Su
Sup
Control
Fiatarone et al NEJM 1994
UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Tai Chi and Falling Atlanta FICSIT Trial Atlanta FICSIT Trial
200 community dwelling elders 70+200 community dwelling elders 70+ Intervention: 15 weeks of education, balance training, Intervention: 15 weeks of education, balance training,
or Tai Chior Tai Chi Outcomes at 4 months: Strength, flexibility, CV Outcomes at 4 months: Strength, flexibility, CV
endurance, composition, IADL, well being, fallsendurance, composition, IADL, well being, falls Falls reduced by 47% in Tai Chi groupFalls reduced by 47% in Tai Chi group
Wolf JAGS 1996Wolf JAGS 1996

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Exercise, Falls, and FrailtyFICSIT TrialsFICSIT Trials
8 independent prospective RCTs8 independent prospective RCTsGoal: reduction in falls and frailtyGoal: reduction in falls and frailty
Pre-planned Meta-analysisPre-planned Meta-analysisInterventionIntervention RRRR CICIAny ExerciseAny Exercise .90.90 (.81-.99)(.81-.99)Balance ComponentBalance Component .83.83 (.70-.98)(.70-.98)
Province JAMA 1995Province JAMA 1995

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Campbell BMJ 1997
Training frail older persons: The New Zealand Study of Women
223 women >80 years223 women >80 yearsIntervention: PT tailored to individual needs, with Intervention: PT tailored to individual needs, with
resistance and balance trainingresistance and balance trainingResults:Results:
Clinical balance, chair rise improvedClinical balance, chair rise improvedRR for falls .47 (CI .04-.90)RR for falls .47 (CI .04-.90)RR for injurious falls .61 (.39-.97)RR for injurious falls .61 (.39-.97)

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Falls in the Elderly
PrevalencePrevalence Clinical ImportanceClinical Importance Risk Factors & EtiologyRisk Factors & Etiology Evaluation Evaluation Prevention & ManagementPrevention & Management Falls & restraint useFalls & restraint use SummarySummary

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Restraint Reduction and Injury
No evidence that restraints reduce fall injuries No evidence that restraints reduce fall injuries Restraints increase morbidity and may cause Restraints increase morbidity and may cause
deathdeath Reported strangulation deaths from restraints Reported strangulation deaths from restraints
every yearevery year Risk factor for delirium, decubitus ulcers, Risk factor for delirium, decubitus ulcers,
malnutrition, aspiration pneumoniamalnutrition, aspiration pneumonia

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Restraint Reduction Decreases Injuries
816 bed Jewish Home for the Aged816 bed Jewish Home for the Aged- Restraints decreased from 39% to 4% over 3 years- Restraints decreased from 39% to 4% over 3 years - No change in falls, injuries, psychotropic use- No change in falls, injuries, psychotropic use
2 year educational intervention covering 2000+ 2 year educational intervention covering 2000+ bedsbeds - Restraint reduction 41% to 4% - Restraint reduction 41% to 4% - Decrease in serious injuries from 7.5% to 4.4%- Decrease in serious injuries from 7.5% to 4.4%
Tinetti 1992, Capezuti, Neufeld 1999, Evans 1997

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Alternatives to Restraints For Patients with Lines and Tubes
Sedation (especially in ICU)Sedation (especially in ICU) Reducing delirium risk factors (drugs, Reducing delirium risk factors (drugs,
dehydration)dehydration) Does the benefit of tubes and lines (or Does the benefit of tubes and lines (or
hospitalization) outweigh the risks of restraints?hospitalization) outweigh the risks of restraints? Geriatric Consultation TeamGeriatric Consultation Team Sometimes restraints may be unavoidable in this Sometimes restraints may be unavoidable in this
settingsetting

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Alternatives to Restraints for Patients Who Fall or Wander
Accept the risk of fallingAccept the risk of falling Hip protectorsHip protectors Environmental modifications, day rooms, Environmental modifications, day rooms,
low bedslow beds Least restrictive alternativesLeast restrictive alternatives AlarmsAlarms Sitters or familySitters or family Geriatric consultation team Geriatric consultation team

UCSF Division of Geriatrics Primary Care Lecture Series May 2001
Summary
Falls are common in the elderly & may lead to Falls are common in the elderly & may lead to injuries and decline in functioninjuries and decline in function
Evaluation should included risk factor Evaluation should included risk factor assessment, gait assessment, and home assessment, gait assessment, and home assessmentassessment
Exercise can improve outcomesExercise can improve outcomes We have no evidence that restraints reduce fall We have no evidence that restraints reduce fall
related injuriesrelated injuries