Embed Size (px)
Citation preview

Archives of Medical Research 33 (2002) 261–264
0188-4409/02 $–see front matter. Copyright © 2002 IMSS. Published by Elsevier Science Inc.PII S0188-4409(02)00354-5
ORIGINAL ARTICLE
Types of Obstructions in Double-Chambered Right Ventricle: Mid-Term Results
Carlos Alva,
a
José Ortegón,
a
Fernando Herrera,
a
Carlos Meléndez,
b
Felipe David,
a
Santiago Jiménez,
a
David Jiménez,
a
Agustín Sánchez,
a
Martha Hernández,
a
Mariano Ledesma
c
and Rubén Argüero
d
a
Departamento de Enfermedades Congénitas del Corazón,
b
División de Cirugía Cardiaca,
c
Departamento de Cardiología Intervencional,
d
Dirección, Hospital de Cardiología, Centro Médico Nacional Siglo XXI (CMN-SXXI), Instituto Mexicano del Seguro Social (IMSS), Mexico City, Mexico
Received for publication June 6, 2001; accepted December 12, 2001 (01/085).
Background.
The double-chambered right ventricle (DCRV) is increasingly recognizedas a distinct obstruction entity. The nature of the obstruction is not well defined.
Methods.
Patients with DCRV were prospectively studied during the last 4 years accord-ing to the following criteria: 1) pressure gradient by echo Doppler and cardiac catheteriza-tion within the right ventricle; 2) angiographic demonstration, and 3) surgical confirmation.
Results.
From March 1997 to March 2001, 10 new cases were included. Age ranged from 2to 14 years (mean 9.5
�
4.4 years), weight ranged from 9.9 to 75 kg (mean 23
�
13.6 kg),and height from 0.85 to 1.48 m (mean 114
�
19 cm). Systolic gradient by echo Dopplerranged from 20 to 135 mmHg (mean 86
�
44 mmHg) and by cardiac catheterization, 18 to130 mmHg (mean 78
�
35 mmHg). In terms of angiographic findings, in six patients theright ventriculogram showed an oblique and low obstruction; in four patients the obstruc-tion was high and horizontal. With regard to surgical findings, angiographic findings wereconfirmed by the surgeon except in one patient, in whom both types of obstruction werepresent. No mortality was observed. With follow-up 4 to 40 months after surgery (mean 24
�
15 months), 8 of 10 patients were evaluated; all corresponded to class I NYHA. Systolicgradient by echo Doppler ranged from 0 to 11 mmHg (mean 4
�
6 mmHg).
Conclusions.
DCRV is produced by the following three types of muscular obstructions:low and oblique obstruction; high and horizontal obstruction, and mixed obstruction. Mid-term surgical results are satisfactory. © 2002 IMSS. Published by Elsevier Science Inc.
Key Words:
Double-chambered right ventricle, Divided right ventricle, Abnormal muscle bundles inright ventricle, Right intraventricular obstruction, Outflow tract obstruction.
Introduction
The double-chambered right ventricle (DCRV) is being rec-ognized as a distinct entity in which the right ventricle cav-ity is divided into two chambers by anomalous muscle bun-dles (1–4). DCRV tends to produce symptoms such ascongestive heart failure in infants and children, given its as-
sociation with a ventricular septal defect. However, inadults the clinical picture is related with pulmonary obstruc-tion (3,5–7). DCRV is recognized as an important associationwith ventricular septal defects and its progressive evolution(8–10). The nature of the obstruction is not well defined;some authors have related it with abnormal displacement ofthe moderator band (11). We have recently reported ourfindings in English patients (12). In this retrospective study,there were two types of muscular obstructions within theright ventricle: the first, an oblique and low obstruction, anda second type with a horizontal and high obstruction. Treat-ment for this lesion is surgical. Cardiopulmonary bypass is
Address reprint requests to: Carlos Alva, M.D., Ph.D., Departamentode Enfermedades Congénitas del Corazón, Hospital de Cardiología, CMN-SXXI, IMSS, Av. Cuauhtémoc 330, Col. Doctores, 06725 México, D.F.,México. Tel.: (
�
52) (55) 5627-6900, ext. 2500; FAX: (
�
52) (55) 5761-4867; E-mail: [email protected]

262
Alva et al./ Archives of Medical Research 33 (2002) 261–264
required, and resection of the anomalous muscle bundles isperformed either through right ventriculotomy (12) or bytricuspid approach (13,14). This study was designed to pro-spectively analyze the angiographic details and surgicalfindings of all new cases with DCRV and to observe possi-ble restenosis in the mid-term.
Materials and Methods
All new consecutive cases with DCRV were prospectivelystudied over the last 4 years. Diagnosis of DCRV and surgi-cal indications were based on the following criteria: 1) apressure gradient of at least 20 mmHg by echo Doppler in-terrogation or in cardiac catheterization between the twochambers within the right ventricle; 2) angiographic demon-stration of anomalous obstruction within the right ventricle.Performance of selective right ventriculogram in frontal andlateral view was planned simultaneously in all cases; 3) nor-mal right ventricular infundibulum, and 4) surgical confir-mation of DCRV in the operating room.
All patients were required to have clinical and echo Dop-pler evaluation during the last 2 months of this study toassess any residual lesion. Cardiac catheterization andechocardiographic studies were performed and interpretedby at least two pediatric cardiologists. All angiographic andecho images were recorded on VHS video tapes.
Results
From March 1997 to March 2001, 10 new cases, six female,fulfilled the inclusion criteria. Ages ranged from 2 to 14years (mean 9.5
�
4.4 years), weight ranged from 9.9 to 75kg (mean 23
�
13.6 kg), and height, from 0.85 to 1.48 m(mean 114
�
19 cm). Maximum systolic gradient measuredby continuous echo Doppler ranged from 20 to 135 mmHg(mean 86
�
44 mmHg) and peak systolic gradient by cardiaccatheterization ranged from 18 to 130 mmHg (mean 78
�
35mmHg). In one case, reduction of the ventricular septal de-fect was detected; in contrast, in two patients gradient pro-gression was documented from 32 to 39 mmHg and from 40to 49 mmHg, respectively.
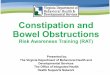
Angiographic findings.
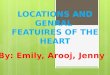
In six cases, either in the frontal orlateral view the right venticulogram showed an oblique andlow muscular obstruction (Figure 1). In contrast, in fourcases obstruction was high and horizontal, immediately be-low the infundibulum (Figure 2). As to associated lesions, aventricular septal defect was present in seven cases (70%),an atrial septal defect in one (10%), and membranous sub-aortic stenosis in another (10%). In all cases, frontal viewwas superior to lateral view in demonstrating muscular ob-structions.
Surgical findings.
In all patients, angiographic findings wereconfirmed by the surgeon, except one, in which both types
of obstructions were present. This patient was initially con-sidered to have a diagonal and low obstruction. Cardiopul-monary bypass time ranged from 48 to 127 min (mean 86
�
27 min), while aortic clamp time ranged from 29 to 117 min(range 62
�
25 min). Anomalous muscle bundles were re-sected by means of right ventriculotomy in all cases. Nomortality was observed. Three patients (30%) developedcomplete atrioventricular heart block after the surgery; tworecovered eventually while the third patient required a per-manent pacemaker.
Follow-up.
Eight of 10 patients were reviewed at the end ofthis study 4–60 months after the surgery (mean 24
�
15months). Two patients living outside of Mexico City were
Figure 1. a) Frontal view of the right ventriculogram showing a low andoblique muscular obstruction (arrow); b) corresponding lateral view of thesame patient. RV: right ventricle.

Types of Obstructions in Double-Chambered Right Ventricle
263
not found, but the remaining patients were in good condi-tion and in class I of the NYHA. Maximum systolic gradientby echo Doppler interrogation ranged from 0 to 11 mmHg(mean 4
�
6 mmHg). Three patients had zero gradient.
Discussion
Clinical recognition of DCRV is difficult due to the differ-ent degrees of obstruction and to various other defects asso-ciated with this anomaly. Failure to recognize and correctDCRV at time of surgery has resulted in an adverse out-come (1,15). Correct diagnosis is usually made by echocar-diography in children, while cardiac catheterization is addi-tionally required in atypical cases or adult patients.
Most authors have considered DCRV as abnormal mus-cle bands; however, for some groups hypertrophy and upperdisplacement of the moderator band, a normal structure inthe right ventricle, have been considered the basis for DCRV(11). In contrast, the prospective findings in this work re-vealed that DCRV is due to abnormal muscle bundles divid-
ing the right ventricle into two chambers. This obstructionhas the following two basic types not previously describedby other authors: 1) a diagonal and low obstruction, and 2) ahorizontal and high obstruction. One patient had a mixedobstruction that could possibly be considered a third type.These results confirm our previous observations (12). Ab-normal muscle bundles probably have a congenital origin.Left-to-right shunt occurring due to the ventricular septaldefect could be the stimulus for the muscle bundles to de-velop obstruction with time. Echo Doppler studies shouldrecognize the two types of obstruction; further echo studiesare needed. Surgical resection by right ventriculotomy re-vealed good results with no mortality at mid-term. Com-plete atrioventicular block seen in three patients postopera-tively was the main concern. Careful resection of musclebundles avoiding conducting tissue is required. Right atrialapproach should be an alternative to reduce risk for com-plete atrioventricular block. Further extensive research stud-ies are required to confirm our findings and to ascertainwhether the type of obstruction has implications in the sur-gical procedure.
Acknowledgments
We would like to thank Antonio Sánchez Bolaños for excellenttechnical support in the preparation of the figures.
References
1. Lucas RV, Varco RL, Lillehei CW, Adams P, Anderson RC, EdwardsJE. Anomalous muscle bundles of the right ventricle. Hemodynamicconsequences and surgical considerations. Circulation 1962;25:443–455.
2. Hartman AF, Goldring D, Carlsson E. Development of right ventricu-lar observant muscular bands. Circulation 1964;30:679–685.
3. Forster JW, Humphries JD. Right ventricular anomalous muscle bun-dle: clinical and laboratory presentation and natural history. Circula-tion 1971;43:115–128.
4. Restivo A, Cameron AH, Anderson RH, Allwork SP. Divided rightventricle: a review of its anatomical varieties. Pediatr Cardiol 1984;5:197–204.
5. McElhinney DB, Chatterjee KM, Reddy VM. Double-chambered rightventricle presenting in adulthood. Ann Thorac Surg 2000;70:124–127.
6. Osborn RC, Taylor J, Soto B, Burunum JF. Double chambered rightventricle in a 70-year-old woman. Ala J Med Sci 1984;21:73–77.
7. Kalaria VG, Mendelson A, Peterson J, Ling FS. Double-chamberedright ventricle in an adult patient. J Invasive Cardiol 2001;13:111–113.
8. Pongiglione G, Freedom RM, Cook D, Rowe RD. Mechanism of ac-quired right ventricular outflow tract obstruction in patients with ven-tricular septal defect on angiocardiographic study. Am J Cardiol 1982;50:776–780.
9. Maron BJ, Ferrans VJ, White IR. Unusual evolution of acquired in-fundibular stenosis in patients with ventricular septal defect: clinicaland morphologic observations. Circulation 1973;48:1092–1103.
10. Cil E, Saraclar M, Ozkutlu S, Osme S, Bilgic A, Ozer S, Celiker A,Tokel K, Demircin M. Double-chambered right ventricle: experiencewith 52 cases. Int J Cardiol 1995;50:19–29.
11. Wong PC, Saunders SP, Jonas RA, Colan SD, Parness IA, Gera T, VanPraagh R, Spevak PJ. Pulmonary valve-moderator and band distanceand association with development of double-chambered right ventri-cle. Am J Cardiol 1991;68:1681–1686.
Figure 2. a) Frontal view of right ventriculogram revealing a horizontaland high obstruction; b) corresponding lateral view of the same patient.RV: right ventricle.

264
Alva et al./ Archives of Medical Research 33 (2002) 261–264
12. Alva C, Ho SY, Lincoln CR, Rigby ML, Wright A, Anderson RH. Thenature of the obstructive muscular bundles in double-chambered rightventricle. J Thorac Cardiovasc Surg 1999;117:1180–1189.
13. Cabrera A, Martínez P, Rumoroso JR, Alcívar J, Arriola J, Pastor E,Galdeano JM. Double-chambered right ventricle. Eur Heart J 1995;16:682–686.
14. Penkoske PA, Duncan N, Collins-Nakai RL. Surgical repair at double-chambered right ventricle with or without ventriculotomy. J ThoracCardiovasc Surg 1987;93:385–393.
15. Rowland TW, Rosenthal A, Castañeda AR. Double chamber right ven-tricle: experience with 17 cases. Am Heart J 1975;89:445–462.