Embed Size (px)
Citation preview

Two unsafe practices: Administration of a product with a precipitateand reuse of a saline flush syringe
Two events recently brought to our attention have again thrust unsafe injectionand infusion practices into the limelight. One involves the dispensing and in-travenous (IV) administration of a pharmacy-prepared product despite a
visible precipitate, and the other involves the reuse of prefilled saline flush syringesfor multiple patients, leading to the transmission of bloodborne diseases. We havenot previously published the scattered reports we received related to these unsafepractices, initially believing they were isolated cases. However, these recent eventsbrought to our attention that this may be a more widespread problem, whichhealthcare providers should address with clinical training programs and improvedmonitoring to ensure adherence with safe practices.
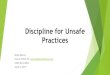
Dispensing and administering a product with a visible precipitateTo ensure the safe intravascular delivery of medications and solutions, practitionersmust be observant for potentially dangerous precipitates (Figure 1) often causedby drug or diluent incompatibilities (e.g., acid-base reactions, mixing oppositely
charged organic drug ions).1
In an analysis of more than300 drug incompatibilities re-ported to the PennsylvaniaPatient Safety Authority be-tween 2009 and 2016, almostone in five mentioned theformation of a precipitate.2
Precipitation reactions areusually rapid and can be ob-
served as crystals, haziness, or turbidity. If a precipitate is observed, the drug orsolution should not be administered. The precipitate can lead to drug inactivationand subsequent therapeutic failures, catheter occlusions, and varying levels of harmdue to particulate embolization, ranging from thrombophlebitis to multi-organ failureor even death.3The consequences can be particularly severe in pediatric patients.4
Since 1998, a total of 23 cases of precipitation have been reported to the ISMPNational Medication Errors Reporting Program (ISMP MERP). In 17 cases, a pharmacistor nurse (or patient/caregiver in the home setting) noticed the precipitate and imme-diately remedied the problem or stopped the injection or infusion. Some of thesecases involved compounding or flushing errors in which the wrong diluent, flush orbase solution, or concentration/dose was used, which resulted in the formation of aprecipitate. However, in 4 cases, the medication or solution was administereddespite observing the precipitate.
In one of these cases, a patient with no previous cardiac or pulmonary disease died.A bag of calcium gluconate and potassium phosphate mixed in saline in thepharmacy appeared cloudy prior to administration, but the nurse still started the in-
May 2017 Volume 15 Issue 5
continued on page 2—Unsafe practices >
Don’t dilute ProvayBlue in normalsaline. Due to the current drug shortageof methylene blue, a hospital switched fromthe generic product it normally used to thebrand product PROVAYBLUE, which theUS Food and Drug Administration (FDA)approved last year. This drug was prescribedfor a patient with encephalopathy fromifosfamide (www.ismp.org/sc?id=2895). Thepharmacist who built the electronic orderset for ProvayBlue in the computer systemnoticed that, in Lexicomp, under the prepa-ration for administration section for meth-ylene blue, it states: “For the treatment ofifosfamide-induced encephalopathy treat-ment (off-label use), case reports cite ad-ministering the dose undiluted, diluted in50 mL NS or D5W, or diluted in 250 mL ofD5W.” The hospital’s previous order setfor methylene blue listed 0.9% sodium chlo-ride injection as the diluent, so no changewas made for ProvayBlue. However, thepharmacist missed additional informationin the same section of the Lexicomp meth-ylene blue monograph that was more spe-cific to ProvayBlue. It states: “Dilution notrequired. In order to avoid local pain (es-pecially in pediatric patients), may be dilutedin 50 mL of D5W. Do not dilute in NS (thesolubility of methylene blue is reduced).”
Because the order set for ProvayBlue wasbuilt incorrectly, ProvayBlue was com-pounded using a base solution of 0.9%sodium chloride. This was dispensed, andonce administration began, a precipitateformed in the intravenous (IV) tubing. Be-cause the nurse did not report the precip-itation during the first round of therapy (itmay not have been readily visible becauseof the dark blue color of the product), theerror was not immediately identified. Later,another nurse reported the precipitate tothe pharmacy when a new bag was startedfor the same patient, at which time the di-lution discrepancy between the methylene
continued on page 2—SAFETY wires >
Supported by educational grants from Baxter, Novartis, and Fresenius Kabi
Figure 1. Example of precipitate (LORazepam) in IV tubing.

May 2017 Volume 15 Issue 5 Page 2
fusion. About an hour later, the patient was found in respiratory distress whichquickly progressed to a fatal cardiac arrest. A different nurse had previouslyabandoned an attempt to administer the same solution due to its cloudy appearance,although she had not yet contacted the pharmacy. The nurse who then administeredthe solution decided to hang it after referencing a flawed hospital protocol thatstated products with precipitates could be infused under “close observation” due tothe risk of “sudden death.” An autopsy showed scattered pulmonary emboli, andthe death was determined to be accidental and related to the infusion of theprecipitated electrolyte infusion.
In the ISMP MERP database, there were two additional events in which nursesattempted to administer solutions despite observed precipitates. But fortunately,rapid IV line occlusions led to their discontinuation, although in one case, thesolution was reinfused into another vein until that line also became occluded.
In 2015, ISMP learned of another event in which an 11-month-old baby receiveddaily etoposide infusions over a 5-day period despite the presence of visibleprecipitates within the solution. The baby had a rare form of cancer, and fouroncologists had worked together to create a custom chemotherapy treatment plan.Unfortunately, the dose of etoposide was mistranscribed as 33 mg per kg per day,instead of the correct dose of 3.3 mg per kg per day, for 5 days. The high concentrationof the etoposide, which was diluted in 100 mL of normal saline, caused the drug toprecipitate. Despite frequent occlusions and the need to constantly flush andreaccess the IV access port, none of the nurses reported the precipitate to apharmacist or oncologist or stopped the infusion. Had they done so, perhaps the 10-fold dosing error could have been detected before the 5 days of therapy had beenadministered. When we learned of the error, the baby was being closely monitoredfor possible liver, renal, bone marrow, neurologic, and respiratory damage secondaryto etoposide toxicity and particulate administration.
ISMP recently received another report about a compounding error with PROVAYBLUE(methylene blue) that led to precipitation of the drug and IV administration despitepotentially visible particulates in the solution or IV tubing (see the SAFETY wirestarting in the right column on page 1).
Reuse of prefilled saline flush syringesAccording to the Centers for Disease Control and Prevention (CDC), unsafe injectionpractices have affected more than 150,000 patients since 2001, including more than50 documented outbreaks of viral hepatitis or bacterial infections.5 While manypractitioners follow the CDC safe injection practices guideline,6 a survey of morethan 5,000 practitioners about the use of needles, syringes, and vials suggests thatsome may be placing patients at risk for transmission of bloodborne diseases.7 Forexample, 1% of the survey respondents admitted to sometimes or always reusing asyringe for more than one patient.
We first learned about the unsafe practice of reusing a prefilled saline flush syringefrom a 2013 press release issued by a New York hospital that was investigatingpossible disease transmission in 236 patients hospitalized during a 3-month period.8
In that case, a single nurse had been reusing prefilled saline syringes to flush the IVlines of multiple patients, mistakenly believing that the practice was safe. Luckily, nocases of disease transmission had been identified at the time of the press release.
More recently, the March 10, 2017, issue of Morbidity and Mortality Weekly Report(MMWR) described a very similar event, this time in a Texas hospital. A nurse whoworked in a telemetry unit had been reusing prefilled saline syringes to flush thelines of multiple patients, which led to a case of hepatitis C transmission.9 The
> Unsafe practices—continued from page 1
continued on page 3—Unsafe practices >
blue products was discovered. Fortunately,the patient was not harmed and the errorwas caught before any additional patientsreceived the incorrectly compounded prod-uct. Strangely, it may not be that uncommonfor IV infusions to continue even if a pre-cipitate is noticed, without reporting theevent to the pharmacy. For more on thistopic, please see the feature article.
Tresiba U-200 won’t allow odd numberdosing of insulin units. With the intro-duction of the TRESIBA (insulin degludec)U-200 pens comes a chance for dosingerrors. A pharmacist recently reportedthat a physician prescribed 25 units dailyof Tresiba U-200. This product is only avail-able in the Novo Nordisk FlexTouch insulinpen. An odd numbered dose is not possiblewith U-200 because the pen only allowsdosing increments in even numbers, startingat 2 units and going up to 160 units. In thiscase, an elderly patient tried to dial 25units by estimating the proper position be-tween 24 units (marked on the pen) and anotch or score that represents 26 units(Figure 1). Due to the design of the pen,the insulin will not be administered unlessthe pen is correctly set to a dose—24 or26 units in this case.
It’s important for healthcare professionalsto be aware of the difference between U-100 pens and the U-200 Tresiba pen. Al-though the U-200 pen WILL allow dosesfrom 2 to 160 units (in even numbers only,2 units at a time), prescribers should con-sider providing a U-100 pen when smalleror odd numbered doses must be adminis-tered, reserving U-200 pens for patientsrequiring larger, even numbered doses.
Why color-coding injectables by drugclass can be dangerous. A hospital re-cently converted from ePHEDrine ampulsto vials from Éclat Pharmaceuticals. Sincethen, there have been several instancesat the hospital where the drug vial was
continued on page 3—SAFETY wires >
© 2017 ISMP. Reproduction of the newsletter or its content for use outside your facility, including republication of articles/excerpts or posting on a public-access website, is prohibited without written permission from ISMP.
continued from page 1
Figure 1. Tresiba U-200 pen allows dosing incre-ments of 2 units, so only even numbered dosescan be delivered.

May 2017 Volume 15 Issue 5 Page 3
unsafe practice was discovered after noticing that the nurse would often leave apartially filled saline flush syringe near a computer work station. When a nursemanager investigated this practice, the nurse voluntarily reported reusing syringesduring the previous 6 months, believing it was cost-effective and safe if no fluidshad been withdrawn into the syringe prior to injecting the saline. The nurse hadbeen working on the unit for 18 months but had not been taught that this was anunsafe practice.
Because all telemetry unit patients were required to have IV access, all 392 livingpatients potentially exposed to this unsafe practice were notified about the possibleexposure to bloodborne diseases and the need for laboratory testing. One of twopatients who tested positive for hepatitis C had been admitted to the unit during thesame time as a patient with known preexisting chronic hepatitis C infection.Genotyping and molecular sequencing identified that both were infected with anidentical strain, which accounts for only about 1% of all hepatitis C infections in theUS. The CDC concluded that at least one of the hepatitis C infections was likelytransmitted as a result of inappropriate reuse and sharing of the saline flushesbetween multiple patients.9
ISMP is concerned that the reports of IV drug administration despite observed par-ticulates, and the reuse of prefilled saline flush syringes, are signals of morewidespread unsafe practices that illustrate the need for ongoing education andimproved monitoring. Given the potential for harm associated with these unsafepractices, several opportunities exist to reduce the risk of errors.
EducationProvide initial orientation and annual education on injection and infusion safety,and include new and temporary nurses. Assess and reinforce practitioner competenceassociated with even the most basic concepts of infection control and aseptictechnique, including recognition that any form of syringe and/or needle reuse isdangerous and should be prohibited. All nurses, pharmacists, and pharmacytechnicians should also be taught to observe medications and solutions forprecipitates, and to avoid dispensing or administering an injection or infusion if pre-cipitates are visible or a solution that should be clear is cloudy. Provide actualexamples or pictures of drugs that have precipitated10 so practitioners who havenever seen this reaction know exactly what to look for.
Also, be sure practitioners understand how to identify and avoid drug incompatibilitieswhen preparing and administering medications or solutions or flushing IV lines(e.g., thoroughly flushing the line before administering an incompatible drug, ad-ministering certain medications through a separate injection port or site). The use ofan in-line filter for solutions that are prone to precipitation can also help preventparticulates from entering the body; however, precipitates can still form in thetubing below the filter, and filters may become blocked, signaling a need to investi-gate.2
Policies and proceduresReview organizational policies and procedures related to safe injection and infusionpractices to ensure that the principles of infection control, aseptic technique, theCDC safe injection practices guideline,6 and the ISMP Safe Practice Guidelines forAdult IV Push Medications11 have been incorporated. Policies and protocols shouldalso be very clear regarding the need to avoid or immediately discontinue anyinjection or infusion if particulates are observed in medications or solutions.
SurveillanceIt is essential to monitor adherence with proper injection and infusion techniques in
> Unsafe practices—continued from page 2mistaken as EPINEPHrine, manufacturedby PAR Pharmaceutical. Both productsare available in small vials with purplecaps, as noted by the person who sent usthe report. Purple is also on the vial labels,and the generic names of the drugs canlook similar, especially with the narrowprint used by Éclat on its ePHEDrine label(Figure 1). Also, these drugs are oftenstored near each other in areas such aslabor and delivery and the operating room.
What’s important to know is that this reportrepresents our first notification about amedication error where drug class color-coding may have played a role, at least in-directly. Purple is the standard color foruser-applied labels on syringes of vaso-pressors in the operating room (OR) (ASTMD4774-06 Standard Specification for UserApplied Drug Labels in Anesthesiology).However, “user-applied” (in the control ofindividual anesthesiologists or anesthetists)does not mean the standard should be ap-plied by manufacturers for commercialdrug vials that contain vasopressors, which,whether by design or coincidence, seemsto be the case here. Although both drugsare vasopressors, mix-ups betweenePHEDrine and EPINEPHrine are dangerous,as noted in our April 17, 2003 issue(www.ismp.org/sc?id=2864).
Many hospitals also purchase prefilled sy-ringes from 503b compounding pharmaciesthat unnecessarily use the standard colorsfor user-applied labels. But what may besafe on syringes within the OR environmentmay not be safe in other areas of thehospital. With commercial vials, similarity
continued on page 4—Unsafe practices >
continued from page 2
Newsletter also partially supported by an educational grant from
continued on page 4—SAFETY wires >
Figure 1. Although somewhat different in overallappearance, the purple cap and label may havecontributed to several mix-ups.

May 2017 Volume 15 Issue 5 Page 4
all settings where medications are prepared and administered. Consider developinga checklist12 based on the CDC safe injection practices guideline6 that can be used toconduct the surveillance process and collect the data. Syringe reuse, if identified,should be immediately corrected, and patients should always be notified of anypotential exposures and the need for testing.9
ReferencesNewton DW. Drug incompatibility chemistry. Am J Health Syst Pharm. 2009;66(4):348-57. 1)Grissinger M. Analysis of reported drug interactions: a recipe for harm to patients. Pa Pat Saf2)Advis. 2016;13(4):137-48.US Food and Drug Administration. Information for healthcare professionals: ceftriaxone (marketed3)as Rocephin and generics). April 21, 2009. www.ismp.org/sc?id=2896Höpner JH, Schulte A, Thiessen J, Knuf M, Huth RG. Preparation of a compatibility chart for intra-4)venous drug therapy in neonatal and pediatric intensive care units. Klin Padiatr. 2007;219(1):37-43.Centers for Disease Control and Prevention. The One & Only Campaign. 2017. www.ismp.org/5)sc?id=2889Siegel JD, Rhinehart E, Jackson M, Chiarello L, Healthcare Infection Control Practices Advisory6)Committee. Safe injection practices to prevent transmission of infections to patients. In: 2007guideline for isolation precautions: preventing transmission of infectious agents in healthcaresettings. Atlanta: US Department of Health and Human Services; 2007. www.ismp.org/sc?id=2890Pugliese G, Gosnell C, Bartley JM, Robinson S. Injection practices among clinicians in United7)States health care settings. Am J Infect Control. 2010;38(10):789-98. Guthrie Health. Guthrie Corning Hospital alerts patients to possible saline flush syringe reuse.8)February 7, 2013. www.ismp.org/sc?id=2891Arnold S, Melville SK, Morehead B, Vaughan G, Moorman A, Crist MB. Notes from the field: hep-9)atitis C transmission from inappropriate reuse of saline flush syringes for multiple patients in anacute care general hospital—Texas, 2015. MMWR. 2017;66(9):258-60. www.ismp.org/sc?id=2894B. Braun. Drug incompatibility. Risk prevention in infusion therapy. www.ismp.org/sc?id=289210)ISMP. ISMP safe practice guidelines for adult IV push medications. 2015. www.ismp.org/sc?id=56311)ASC Quality Collaboration. Safe injection practices toolkit. 2017. www.ismp.org/sc?id=289312)
> Unsafe practices—continued from page 3 continued from page 3in appearance is enhanced by the use ofsimilar colors across a drug class.
The ASTM color scheme is used for otherdrug classes such as opioids, neuromus-cular blockers, beta blockers, and inductionagents. It was never meant for commercialdrug vials, especially high-alert drugs whereindividual agents within the class may havevarying potencies and pharmacologic ef-fects. We agree with the reporter’s concernabout the potential for mix-ups attributedto the purple caps. We hope that the USFood and Drug Administration (FDA), Éclat,PAR, and other manufacturers of commer-cial drug vials will stay away from anytype of color-coding by drug class.
No, not methotrexate. Despite its name,MTX TOPICAL PAIN does not containmethotrexate or mitoXANTRONE, both cancerdrugs associated with the dangerous ab-breviation “MTX” which has led to mix-upsbetween them. When we saw “MTX” usedfor this over-the-counter (OTC) topical lidocaine4% and menthol 1% patch sold by UnikPharmaceuticals, we were taken aback.Perhaps more concerning is that arthritissufferers are commonly treated withmethotrexate and may be misled by the“MTX” on this patch. The image on theproduct’s package also implies that it is usedto treat joint pain, which it does not. Methotrex-ate is also used to treat psoriasis, a diseasecharacterized by skin lesions, while the MTXTopical Pain product specifically warnsagainst use in patients with damaged skin.
This combination of lidocaine and mentholingredients is marketed under the OTCDrug Monograph process “for temporaryrelief of pain and itching associated withminor burns, cuts, scrapes, and minor skinirritations.” OTC products in compliancewith an OTC Drug Monograph may bemarketed without submitting a productname for review or undergoing a preap-proval review by the US Food and DrugAdministration (FDA). According to FDA,the monographs establish conditions underwhich certain OTC active ingredients are“generally recognized as safe and effective.”FDA has been alerted to this error-proneabbreviation. We would appreciate hearingfrom readers who may have experiencedan issue with this OTC product.
If you would like to subscribe to this newsletter, visit: www.ismp.org/sc?id=382
ISMP Nurse AdviseERR (ISSN 1550-6304) © 2017 Institute for Safe Med-ication Practices (ISMP). Subscribers are granted permission to redistributethe newsletter or reproduce its contents within their practice site or facilityonly. Other reproduction, including posting on a public-access website, isprohibited without written permission from ISMP. This is a peer reviewedpublication.
Report medication and vaccine errors to ISMP: Call 1-800-FAIL-SAF(E), or visit www.ismp.org/MERPor www.ismp.org/VERP. ISMP guarantees the confidentiality of information received and respects the re-porters’ wishes regarding the level of detail included in publications.
ismp.org consumermedsafety.org twitter.com/ISMP1 facebook.com/ismp1 medsafetyofficer.org
Editors: Ann Shastay, MSN, RN, AOCN; Judy Smetzer, BSN, RN, FISMP; Michael Cohen, RPh, MS, ScD(hon), DPS (hon); Russell Jenkins, MD; Ronald S. Litman, DO. ISMP, 200 Lakeside Drive, Suite 200, Hor-sham, PA 19044. Email: [email protected]; Tel: 215-947-7797; Fax: 215-914-1492.
Join ISMP in celebrating National Nurses Week
May 6-12, 2017

How to Apply
Information, a course outline, and an application can be found at:www.ismp.org/sc?id=2898.
Applications can also be requested by calling 215-947-7797.
The application deadline for the International Fellowship is June 30, 2017.
Safe Medication Management Fellowship
ISMP International
ISMP is now accepting applications for a unique 2-year International Fellowship
Sponsored by: Baxter International
Location and Term:The 2-year International Fellowship, sponsored by Baxter International,begins on September 1, 2017, at the Horsham, Pennsylvania (near Philadelphia) office ofthe Institute for Safe Medication Practices (ISMP). Relocation to the Horsham/Philadelphia areais required.
Qualifications:The International Fellow must:
Have an advanced degree in healthcare (e.g., PharmD, master’s degree)Have at least 1 year of experience in a clinical role in an acute care settingBe fluent in written and spoken EnglishBe a US citizen or have official documentation that allows him or her to remain in theUS for 2 years and travel internationally for a week or more at a time
Description:The International Fellowship will help train a medication safety leader seekinga long-term career at an international level. The Fellow will be involved in global medicationsafety initiatives, address worldwide safety issues, and help increase global reporting of med-ication errors. They also will work directly with international professional organizations andmedication safety centers, and attend multi-country medication safety meetings and events.The Fellowship offers an unparalleled opportunity to learn from and work collaboratively withUS and international experts in medication safety to assess and develop global medicationerror-prevention strategies.
< >