Embed Size (px)
Citation preview

Section Two Section Two Section Two Section Two Section Two
Section TwoAn overview of occupational
therapy practice
Curtin_Ch005_main.indd 55 9/15/2009 2:16:35 PM

E
Curtin_Ch005_main.indd 56 9/15/2009 2:16:35 PM

E
5Chapter Five
Occupational reasoning
CHAPTER CONTENTS
The case method 58
Conceptual frameworks for occupational performance and engagement 58
Phases of the occupational therapy process 59
Assessment 59
Diagnosis 60
Intervention 61
Re-assessment 61
Occupational reasoning strategies 61
Comparative analysis 62
Hypothesising 63
Conditional reasoning 63
Inferential reasoning 63
Argumentative reasoning 64
Reframing 64
Evidence-based reasoning 64
Application of strategies 64
Sharpening occupational reasoning 64
Conclusion 65
SUMMARY
As humans, it is our nature to think Our thinking may be based on information or beliefs; it may be reality-based or distorted; it may be culturally appropriate or prejudicial As occupational therapy students, we learn a systematic method of thinking to ensure quality thinking in regard to
assessment and intervention We call this thinking occupational reasoning As therapists, we refine our occupational reasoning so that quality decisions are made expeditiously This chapter explores occupational reasoning The case method is introduced to establish the need for a systematic method of thinking Then, the role of a conceptual framework in transforming the case method to the occupational therapy process is presented Thinking strategies that are used throughout the occupational therapy process are described: comparative analysis, hypothesising, conditional reasoning, inferential reasoning, argumentative reasoning, reframing, and evidence-based reasoning The chapter concludes with suggestions for students and therapists to improve their occupational reasoning
KEY POINTS
• Occupational reasoning is a systematic method of thinking about the occupational performance and engagement of humans that supports the occupational therapy process
• From an historical perspective, the addition of occupational reasoning into the thinking patterns of occupational therapists enhanced occupational therapy’s professionalism and autonomy
• Each phase of the occupational therapy process involves multiple reasoning strategies to make decisions about assessment, diagnosis, intervention, and re-assessment
• Common reasoning strategies used by therapists are: comparing clients to textbook or real people, explaining facts through hypothesising, linking antecedents (ifs) with
Joan C. Rogers
Curtin_Ch005_main.indd 57 9/15/2009 2:16:35 PM

E
An overview of occupational therapy practices e c t i o n t w o
58
consequences (thens), projecting beyond the facts, debating all facets, re-interpreting and applying research findings to individual clients
• To improve their occupational reasoning, students and therapists may ‘think aloud’ about what they are doing and why and share this thinking with more experienced therapists
The case method
In 1969, Line challenged occupational therapists to discard their old ways of clinical thinking and embrace the case method, a scientific form of rea-soning. The ‘old ways of thinking’ Line alluded to were: (1) physician prescription of occupational therapy, in which physicians make decisions about occupational therapy goals and interventions; (2) standard operating procedures, which specify that all clients having a particular diagnosis receive a stan-dard, predetermined treatment; and, (3) customary thinking, whereby clients are treated in a certain way because ‘we have always done it this way’. These strategies limit the need for occupational therapists to think by allocating problem solving to prescriptions written by physicians or encoded in formal or informal traditions. By replacing pre-scribed thinking with the case method, occupational therapists assume responsibility for the thinking that guides their practice.
The case method provides a generic structure for professional thinking, and as such it supports the reasoning of many professions, including medicine and physical therapy. Each profession makes the process its own by the concepts it selects to think about in relation to clients and the actions it takes to benefit clients (Holm 1986). Physicians, for example, think about clients’ medical status and prescribe medications, surgery, or psychotherapy. Physical therapists focus on clients’ physical status and use exercise as their professional tool. Occupa-tional therapists concentrate on occupational perfor-mance and engagement, and use daily occupations when working with clients. It is the interaction of occupational performance and engagement with the case method that results in the occupational therapy process and, in turn, it is occupational reasoning that underlies the occupational therapy process.
The case method provides a structure for prob-lem-setting and problem-solving by organising infor-mation about individual clients and relating it to occupational therapy knowledge. It facilitates the process whereby therapists learn what they need to
know about clients to make informed decisions about the strategies that may assist the clients. This learning is accomplished collaboratively with clients in four overlapping and interdependent phases. First, therapists gather information about clients so that they can understand their clients’ occupational chal-lenges and what they might be able to do to assist them. Second, therapists organise and interpret the information gathered and diagnose problems. Third, therapists plan outcomes and actions to assist clients to achieve the outcomes. Fourth, therapists evaluate the actions taken to see if they accomplished the outcomes. These four phases are labelled assess-ment, diagnosis, intervention, and re-assessment, respectively, and comprise the occupational therapy process.
Conceptual frameworks for occupational performance and engagement
Each phase of the occupational therapy process is guided by the conceptual framework of occupa-tional performance and engagement selected by the therapist. Application of an occupational therapy framework to the case method transforms into the occupational therapy process. Occupational therapy, like many professions, uses many conceptual frame-works. In this context, conceptual framework is intended to be all inclusive of related terms such as theory, model, frame of reference, or paradigm. Holm (1986) grouped occupational therapy frame-works into five fundamental classifications: acquisi-tional, biomechanical, developmental, occupational behaviour, and rehabilitation. Each framework guides therapists to evaluate different aspects of occupational performance and engagement, diag-nose different occupational challenges, intervene using different approaches and procedures, and evaluate improvement in occupational performance and engagement differently.
Some frameworks (e.g. biomechanical) focus only on the enablers of occupation, that is, on factors within clients. From the perspective of the Interna-tional Classification of Functioning, Disability and Health (ICF) (World Health Organization 2001), they address body structures and functions and their impairments. Other frameworks (e.g. rehabilitation) highlight clients performing their valued daily living activities. In the language of the ICF, they address
Curtin_Ch005_main.indd 58 9/15/2009 2:16:35 PM

E
Occupational reasoning c h a p t e r 5
59
activities and their limitations. Still other frame-works use a panoramic lens to capture clients per-forming occupations where they are typically performed, whether the location is the home, school or workplace. Thus, they emphasise participation and its restrictions as defined in the ICF.
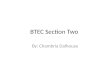
Occupational therapy needs different conceptual frameworks of occupational performance and engagement to serve the differential needs of clients. During the acute stage of a burn injury, the biome-chanical framework may be the most appropriate to guide intervention aimed at preserving range of motion and strength and preventing scar tissue for-mation. However, upon discharge from acute care the acquisitional or developmental framework may be more applicable for managing return to work or school despite disfigurement and pain. Strategies implemented under the biomechanical framework, such as active range of motion exercises and wearing pressure garments may still be employed. Hence, the various frameworks of occupational performance and engagement are not necessarily mutually exclu-sive and it is often appropriate to operate from different, but compatible, frameworks, simultane-ously or sequentially. Commonly, intervention for people who have had a stroke includes constraint induced movement therapy for the paralysed extremity and assistive technology devices (e.g. one-handed knife) for use by the non-paralysed extrem-ity. Constraint induced movement therapy emanates from an acquisitional framework and assistive tech-nology from a rehabilitation framework. As depicted in Figure 5.1, the conceptual framework selected by the therapist influences each step of the occupa-tional therapy process.
Phases of the occupational therapy process
Although each phase of the occupational therapy process is discussed separately, there are no clear distinctions between assessment, diagnosis, inter-vention, and re-assessment. The process is divided into phases to highlight key decisions that are required to support occupational reasoning. The occupational framework selected by the therapist permeates each phase.
Assessment
The purpose of assessment is for therapists to learn about the client’s occupational performance and engagement so that they can formulate a diagnosis to direct intervention and re-assessment. Data are gathered about occupational performance and engagement through questioning, testing, and observing. Data may also be collected from the cli-ent’s medical or school records or from case confer-ences; however, these data have their origins in questioning, testing, or observing. Questioning may be done orally through interviews or in writing through questionnaires. Interview tools like the Canadian Occupational Performance Measure (Law et al 2005) and questionnaires, like the Health Assessment Questionnaire (Fries et al 1982) are formal, standardised measures that yield informa-tion about clients’ perceptions of their performance. If clients are unwilling to provide data (e.g. clients who are paranoid), unable to provide data (e.g. infants or clients who are comatose), or unable to provide reliable data (e.g. clients with severe demen-tia), proxies become the best source of information. Proxies who live with clients, spend considerable time with them, or are their caregivers are preferred.
Testing involves examining clients’ performance under standardised conditions. This is accomplished by having clients demonstrate how they perform activities (e.g. cooking, typing) or how they perform components of those activities, such as the physical or cognitive actions that enable or restrict activities. Tests like the FIM™ Instrument (Uniform Data System for Medical Rehabilitation 1997) and the Performance Assessment of Self-Care Skills (Rogers & Holm 1989a) are activity measures and require therapists to observe and describe the client’s per-formance in terms of independence–dependence. Tests such as the Keitel Function Test (Eberl et al Figure 5.1 • the occupational therapy process
Evaluation
FRAME OF REFERENCE
Diagnosis
Intervention
Re-evaluation
Curtin_Ch005_main.indd 59 9/15/2009 2:16:35 PM

E
An overview of occupational therapy practices e c t i o n t w o
60
1976), Mini-Mental State Examination (Folstein et al 1975), and Geriatric Depression Scale (Yesavage 1988) are impairment measures used to indicate the extent to which physical, cognitive, and affective factors, respectively, may be negatively influencing performance. For most observational measures, clients are requested to perform the desired activities during a scheduled assessment. Hence, clients may demonstrate bathing in the middle of the afternoon, even though they may usually bathe at bedtime. This procedure allows therapists to use their time efficiently. However, observation may also be carried out informally during daily activities. Settings like assisted living facilities, nursing homes, and schools are particularly suited for informal observation.
Commonly, an occupational therapy assessment incorporates more than one data-gathering method. Therapists may use interviewing to assess perceived performance problems and observation to assess actual performance problems. The conceptual framework selected by the therapist identifies the concepts to be assessed and suggests how data should be organised to facilitate interpretation. However, it does not indicate the method to be used to assess each concept, the extent to which each concept warrants assessment, the tool to be used to measure each concept, the order in which the con-cepts should be measured, or the means to validate data and resolve inconsistencies.
Diagnosis
As assessment data are ‘fitted’ to the conceptual framework, the therapist develops a working image of this client’s occupational performance and engagement. The endpoint of assessment is an occu-pational diagnosis that defines the client’s occupa-tional problem(s) (Rogers 2004). Clients come to
occupational therapy because they have a problem or need. They may report that they are unable to bathe them selves or prepare their meals adequately. Although professional judgement may not be required to recognise a bathing or cooking impair-ment, to diagnose a bathing or cooking impairment does require occupational therapy knowledge, judgement, and skill.
The occupational diagnosis marks the transition between assessment and planning outcomes and strategies. Hence, the diagnosis must contain suffi-cient information to provide sound direction. To do this, the occupational diagnostic statement should give an indication of: the nature of the impairment, the presumed cause of the impairment, the evalua-tive cue supporting the impairment, and, if appli-cable the health condition(s) associated with the impairment (Rogers 2004). Unlike medicine, which has the ICD-10 (World Health Organization 2005), psychiatry, which has the DSM-IV-TR™ (American Psychiatric Association 2000), and nursing, which has NANDA International (2007), occupational therapy lacks a diagnostic taxonomy. Occupational therapy does not have a label, for example, to dis-tinguish a limitation in dressing associated with cog-nitive impairment from a limitation in dressing associated with physical impairment. Because of this deficiency, the occupational therapy diagnosis is for-mulated as a descriptive statement.
As portrayed in Table 5.1, the occupational diag-nostic statement has four components – descriptive, cue, explanatory, and health condition (Rogers 2004, Rogers & Holm 1991). The descriptive com-ponent identifies the occupational challenge to be targeted for intervention and against which the success of the intervention will be measured. In Table 5.1, the diagnostic statement specifies an inability to write. The cue component identifies the observable sign or signs of the problem. It indicates
Table 5.1 Occupational therapy diagnostic statement
Component Phrase ICF
Descriptive Unable to write telephone messages without pain d170.3 Writing. Severe difficulty
Cue As evidenced by increase in number of Tylenol® taken per day
Explanatory Inflammation of the metacarpal phalangeal joint of the right thumb
b280 14.2 Pain in upper limb, moderate
Health condition Rheumatoid arthritis ICD M05.3
Curtin_Ch005_main.indd 60 9/15/2009 2:16:36 PM

E
Occupational reasoning c h a p t e r 5
61
the significant slice of evaluative data that led the therapist to know that a writing limitation was present. The explanatory component gives the reason the therapist hypothesises as the cause of the writing limitation. In the example, insufficient hand strength to hold a writing utensil is thought to be the cause of the writing limitation. The health condition component addresses factors arising from pathology that need to be taken into account in the intervention plan. For a writing limitation secondary to rheumatoid arthritis, therapists would want infor-mation about pain, joint deformity, and the use of disease-modifying medications. ICF and ICD-10 codes have been added to Table 5.1 to illustrate their potential usefulness for developing an occupa-tional diagnostic taxonomy.
Occupational diagnostic decisions centre on: for-mulating plausible hypotheses; determining the support for each occupational diagnosis, including the validity of the explanatory component, which often determines the intervention; and, prioritising occupational diagnoses.
Intervention
The intervention phase responds to the question: How will occupational therapy intervention help alleviate this client’s problem or achieve the targeted outcomes? In the intervention phase, data from the occupational diagnosis and assessment phase are used to formulate intervention outcomes and plans to achieve them. Outcome statements are devised that describe occupational performance and engage-ment after occupational therapy intervention has had its effect. For Mrs. Trippit, a receptionist who exhibited a writing limitation, an occupational goal might be to enable message taking without diffi-culty. At the beginning of therapy, Mrs. Trippit could not hold a pen long enough to write telephone messages because of hand weakness and pain. An outcome statement might read: within one week (estimated time required for change), Mrs. Trippit will write (desired action) three telephone messages within five minutes, completely and legibly, and report no difficulty holding the pen or pain interfer-ence (performance criteria). Occupational outcomes specify how therapists will know if the strategies they plan are achieving the intended results; hence, they must be observable and measurable.
Having determined the endpoint of therapy, the therapist moves to deciding the techniques, and
modalities that can be brought to bear on the problem. Of the feasible strategies, which are most appropriate for this client with this health condition? If insufficient hand strength is the cause of Mrs. Trippitt’s writing limitation, then weak hand strength must be improved or circumvented to alleviate the problem in writing. For some clients with rheuma-toid arthritis, a restorative approach to improve hand strength may be appropriate, while for other clients a compensatory approach incorporating assis-tive technology (e.g. enlarged pen for better grasp) may be preferable. For pain interference, a biomech-nical approach may be beneficial, namely a rigid or soft thumb post splint to protect the inflamed meta-carpal–phalangeal joint of her right thumb. Selecting the most judicious intervention to use with a client, from available options, is the pivotal decision for the intervention phase. Decision-making includes decid-ing on the therapy: dose (how intense?), frequency (how often?), and duration (how long?).
Re-assessment
The purpose of re-assessment is to ascertain if tar-geted outcomes have been achieved. To do this, therapists compare clients’ current occupational performance and engagement to that predicted at the outset of therapy. Improvement, stability, or deterioration is based on the same measures that were used during assessment to determine that there was a problem. When data indicate that the outcomes were achieved, more advanced outcomes may be proposed or the client may be discharged. When data indicate that the outcomes were not achieved, the time for achieving the outcomes may be extended, outcomes may be revised to reflect more achievable ones, a different intervention may be initiated, or the client may be discharged from services because maximum benefit has been achieved.
Occupational reasoning strategies
Although the occupational therapy process outlines the phases that therapists progress through when working with clients, it does not indicate how thera-pists select, analyse, synthesise, and evaluate data to make decisions. The sequential and iterative cogni-tive processes therapists use to assess, diagnose, intervene, and re-assess occupational performance
Curtin_Ch005_main.indd 61 9/15/2009 2:16:36 PM

E
An overview of occupational therapy practices e c t i o n t w o
62
and engagement are collectively called occupational reasoning. Although it is easy to delineate the phases in the occupational therapy process, describing the dynamics of moving forward and backward from one phase to another, while continuing to advance toward diagnostic and therapeutic decisions, is extremely complex. As is apparent from Table 5.2, in which key decisions involved in the occupational therapy process are outlined, efficient and effective management of these decisions requires consider-able professional expertise. Although we do not know exactly how occupational reasoning occurs, research on health care professionals, including occupational therapists, has furnished some indications of its dynamics. We will discuss common thinking strate-gies that therapists use in occupational reasoning:
comparative analysis, hypothesising, conditional rea-soning, inferential reasoning, argumentative reason-ing, reframing, and evidence-based reasoning (Pesut & Herman 1999).
Comparative analysis
Comparative analysis involves examining similarities and differences between new clients and textbook scenarios or former clients to gain insight about diag-noses and strategies to apply to new clients (Holm & Rogers 1989). During didactic education, stu-dents use textbook scenarios to develop images of impairment in ‘typical’ clients with a particular diag-nosis. They learn to expect clients with severe strokes to have hemiplegia and have difficulty with bilateral activities; clients with obsessive compulsive disorder to manifest disordered thinking and make unusual repetitive movements; children with autism to exhibit rocking and other self-stimulating behav-iours and to be unaware of their environment, and so on. They also learn an array of occupational therapy strategies appropriate for the occupational challenges associated with these health conditions and the results that can be expected from their application.
These textbook descriptions of typical clients, strategies, and outcomes serve as prototypes for client comparisons. When students engage in field-work, they compare the characteristics of their clients to the defining features of these prototypes. Students’ reasoning goes something like this: ‘My client had a left hemisphere stroke with resultant hemiplegia, and, therefore, if I work with my client using the same strategies used for people following a stroke, I learned about in the classroom, I will get the same outcomes in the same time limits.’
As students observe and work with ‘real’ people, prototypes are modified based on the occupational performance and engagement, and recovery patterns observed in ‘real’ clients. Students develop a cogni-tive or client library based on their caseload. In future encounters with clients with stroke, these stored clients replace the prototypes for compari-sons. As professional experience accumulates, stu-dents not only add more clients to their cognitive library, they organise their library for easy retrieval. For example, within the stroke library, clients may be classified according to: those with and without sensory impairment, with and without lower-extremity involvement, and with and without a
Table 5.2 Decisions central to occupational reasoning
Phase Decisions
Assessment • What concepts should be assessed?• How extensively should each concept
be assessed?• What method(s) should be used?• What assessment tools should be used?• In what order should the assessment
tools be used?• How should data be validated and
inconsistencies resolved?
Diagnosis • What are the client’s occupational diagnoses?
• Which occupational diagnosis is best supported by assessment data?
• How should occupational diagnoses be prioritised?
Intervention • What occupational therapy interventions could be used?
• What occupational therapy interventions should be used for this client?
• How intense should each intervention session be?
• How many times per week should intervention be?
• How long should each intervention be?
Re-assessment • Was each stated goal achieved?• Should intervention be terminated?• Should intervention be continued or
changed?• Are new outcomes appropriate?
Curtin_Ch005_main.indd 62 9/15/2009 2:16:36 PM

E
Occupational reasoning c h a p t e r 5
63
flaccid upper extremity. The functionality of these classifications for comparative reasoning becomes evident when Mrs. Swanson, who has no lower-extremity impairment, is able to grasp large objects in the affected extremity, but has no sensation in the affected hand, comes to occupational therapy. Using comparative reasoning, therapists search for the client in their cognitive library that provides the best, although not perfect, match for Mrs. Swanson. The reference client(s) would be called to mind and would provide therapists with guidance about the most enabling strategies.
Therapists use multiple classification principles to organise their cognitive client libraries, not just diag-nosis. For instance, they may classify based on culture or religious beliefs. When a Muslim person who has had a stroke, is assigned to them, they might call to mind past clients who were Muslim, not just those with stroke. These reference clients would remind them to be sensitive to gender (pref-erence for males working with males), fasting sched-ules (during Ramadan fasting sun up to sun down), and dress (female preference for head scarf) among other factors.
Comparative analysis may be used within, as well as between, client comparisons. During re-assess-ment, a client’s present occupational performance and engagement may be compared to the predicted outcome status. Similarly, actual engagement may be compared two or more times: preadmission, admission, interim, and discharge. These compari-sons allow therapists to know if occupational therapy intervention is having the anticipated effect on occu-pational performance and engagement.
Hypothesising
To hypothesise is to give an explanation for a set of facts that can be tested through the use of experi-mentation. Early in the assessment phase, therapists may put forth several diagnostic hypotheses (Elstein & Schwarz 2002). An occupational diagnosis is an educated guess, which is based on foundational knowledge. It explains a set of data about a client’s occupational performance and engagement and can be tested. Data collection is guided by hypotheses and data are organised to support or dispute each hypothesis (Rogers & Holm 1989). By interviewing Mrs. Ming, the therapist may ascertain that she is dependent in dressing. Observation of Mrs. Ming performing dressing activities, leads the therapist to
think that the reason Mrs. Ming has difficulty dress-ing is due to hand weakness and lack of range of motion at the shoulder. The therapist then evaluates Mrs. Ming’s hand strength and upper extremity joint range of motion to ascertain if the hypothesis about the cause of the dressing limitation is viable. Hand strength might be evaluated by testing grip strength on a dynamometer and pinch strength on a pinch meter. Range of motion might be evaluated with the Keitel Function Test. The results of these impair-ment tests would be compared to normal values for strength and movement to ascertain if they are defi-cient. If both values are deficient, the therapist’s hypothesis about the cause of dressing dependency remains highly probable. However, it still needs to be tested through such means as progressive active and passive range of motion exercises.
Conditional reasoning
Conditional reasoning reflects an ‘if–then’ thinking strategy in which antecedents are linked to their consequences. When therapists link diagnoses or impairments to activity limitations or participation restrictions, conditional reasoning may be used. For example: if Mrs. Jones is hearing voices, then she may have difficulty concentrating on typing and will make errors; and if Mr. Book is visually impaired, then he is at risk for falls.
Inferential reasoning
Inferential reasoning involves drawing conclusions from facts. Facts have been or can be verified through observation or examination. Inferences are derived from facts. Therapists commonly make inferences about activity limitations based on facts about impairments. For example, a therapist may reason that because goniometry indicated that Mr. Goodman’s external rotation at the hip was severely restricted, he would be dependent in donning socks. ‘Dependence in donning socks’ is a conclusion that was logically derived from the fact of restricted hip external rotation (movement restricted to: 0 to 20 degrees). This conclusion could be examined through performance testing, and if it were shown to be valid, ‘dependence in sock donning’ would become a fact rather than an inference. Because the thera-pist’s inference fails to take into account adaptive techniques that circumvent decreased hip motion, such as a sock aid, it may be invalid.
Curtin_Ch005_main.indd 63 9/15/2009 2:16:36 PM

E
An overview of occupational therapy practices e c t i o n t w o
64
Argumentative reasoning
Argumentative reasoning examines the reasons that support and fail to support a position or action. For example, a therapist may weigh the advantages and disadvantages associated with a home programme plus bi-weekly or monthly hospital-based sessions, for a client who lives in a rural area and has a severe upper-extremity crush injury. Advantages of bi-weekly sessions are that the therapy is supervised, occupation can be graded more effectively, and there is frequent opportunity to monitor infection and progress. The disadvantages are that bi-weekly ses-sions are expensive, the client lacks insurance, and the client may cancel sessions, especially in wintry weather. The advantages for bi-weekly sessions become disadvantages for monthly sessions and vice-versa for its disadvantages. Explicating the strengths and weaknesses of each stance heightens awareness of all factors that need to be taken into account, facilitates collaboration between therapists and clients, and fosters making quality decisions (Rogers 1983). This strategy is also beneficial for considering risks and benefits associated with client preferences.
Reframing
Reframing involves reinterpretation. It provokes a new view or perspective. For instance, a therapist may reason that Mr. Brown’s failure to follow instructions consistently is due to dementia, and, hence, focus on caregiver training. However, after additional sessions, the therapist realises that Mr. Brown has a hearing impairment. Replacing oral instructions with written ones addresses the incon-sistency. This solution was made possible by framing the problem as an auditory versus cognitive impair-ment. Importantly, reframing shapes what we do as well as how we think. Reframing is employed every time a therapist switches a conceptual framework when working with a client.
Evidence-based reasoning
Evidence-based reasoning is similar to comparative analysis, except that clients are compared with study samples versus prototype or actual clients. Assuming that the study meets criteria for internal validity, therapists question its external validity: Can the find -ings be generalised to this client in my practice? To answer this question, key characteristics, related to
clients (e.g. age, diagnosis), therapists (e.g. compe-tence in specific strategies) and settings (e.g. hospital, school) are matched to those of study subjects. Suppose that following a home-safety programme for community-dwelling older people, a participant asks you about the benefits of hip protectors for preventing hip fractures. Because the daily activities of community-dwelling older adults are more exten-sive than those living in nursing homes, place of residence would be a key variable on which to match. By reading research, especially systematic reviews and meta-analyses, therapists stock their evidence-based library.
Application of strategies
A therapists’ use of these reasoning strategies is highly dependent on their foundational and evi-dence-based knowledge, professional experience, and reasoning skill. Experienced therapists (experts) formulate more salient hypotheses, and formulate them earlier in the occupational therapy process, than novices (e.g. students and new practitioners). Novices need more data before they can recognise patterns, potentially because they have more diffi-culty sorting relevant and irrelevant data. Drawing on their professional experience, the thinking of experts is more automatic and less effortful. Experts reserve the more laborious ‘if–then’ thinking and hypothesis testing for unfamiliar situations or when the ‘usual intervention’ approach fails. Novices, lacking this depth of experience, rely on more delib-erate problem solving. Each repetition of the occu-pational therapy process incorporates multiple occupational reasoning strategies.
Sharpening occupational reasoning
Professional self-talk provides an approach to improving one’s occupational reasoning. It refers to the stream of thoughts that therapists communicate to themselves about a client, before, during, and after they interact with clients (Newell & Simon 1972, Rogers 1982). While it encompasses the occu-pational reasoning strategies discussed above, the emphasis is on thinking about your thinking while you are thinking. It encourages therapists to identify the thinking strategies that they usually use in prac-tice and to reflect on their adequacy. By sharing self-talk, students can learn best-practice reasoning
Curtin_Ch005_main.indd 64 9/15/2009 2:16:36 PM

E
Occupational reasoning c h a p t e r 5
65
skills from their supervisors, and therapists can learn them from expert therapists.
Conclusion
Occupational reasoning underlies each profes-sional decision. Although this chapter emphasised
thinking skills commonly associated with the scientific method, other perspectives may also be usefully applied to elucidate the decision-making process. Quantitative and qualitative studies of occupational reasoning will advance the science, art, and practice of the occupational therapy process.
References
American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders, (4th ed.), Text revision. Washington, DC, American Psychiatric Association.
Eberl, D. R., Fasching, V., Rahlfs, V. et al (1976). Repeatability and objectivity of various measurements in rheumatoid arthritis: a comparative study. Arthritis & Rheumatism 19, 1278–1286.
Elstein, A. S. & Schwarz A. (2002). Clinical problem solving and diagnostic decision making: Selective review of the cognitive literature. British Journal of Medicine, 324, 729–732.
Folstein. M. F., Folstein, S. E. & McHugh, P. R. (1975). ‘Mini-Mental State’: A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research, 12, 189–198.
Fries, J. F., Spitz, P. W. & Young, D. Y. (1982). The dimensions of health outcomes: the health assessment questionnaire, disability and pain scale. Journal of Rheumatology, 9(5), 789–793.
Holm, M. B. (1986). Frames of reference: guides for action – occupational therapist. In: H. Schmid (Ed.). Project for independent living in occupational therapy (PILOT). Rockville, MD, American Occupational Therapy Association, pp. 69–78.
Holm, M. B. & Rogers, J. C. (1989). The therapist’s thinking behind functional assessment II. In: C. B. Royeen (Ed.). AOTA self study series: assessing function. Rockville, MD, American Occupational Therapy Association.
Law, M., Baptiste, S. & Carswell A. et al (2005). The Canadian Occupational Performance Measure, (4th ed). Toronto, CAOT Publications ACE.
Line, J. (1969). Case method as a scientific form of clinical thinking. American Journal of Occupational Therapy 23, 308–313.
NANDA International (2007). Nursing diagnoses: definitions & classification 2007–2008, (7th ed.). Philadelphia: NANDA International.
Newell A. & Simon, H. A. (1972). Human problem solving. Englewood Cliffs, NJ, Prentice-Hall.
Pesut, D. J. & Herman, J. (1999). Clinical reasoning: The art & science of critical & creative thinking. Albany, Delmar.
Rogers, J. C. (1982). Teaching clinical reasoning for practice in geriatrics. Physical & Occupational Therapy in Geriatrics, 1(4), 29–37.
Rogers, J. C. (1983). Clinical reasoning: the ethics, science, and art. American Journal of Occupational Therapy, 37, 601–616.
Rogers, J. C. (2004) Occupational diagnosis. In: M. Molineux (Ed.). Occupation for occupational
therapists (pp. 17–31). Oxford, UK, Blackwell.
Rogers, J. C. & Holm, M. B. (1989a). Performance assessment of self-care skills. Pittsburgh, PA, University of Pittsburgh, Department of Occupational Therapy.
Rogers, J. C. & Holm, M. B. (1989b). The therapist’s thinking behind functional assessment. I. In: C. B. Royeen (Ed.). AOTA self study series: assessing function. Rockville, MD, American Occupational Therapy Association.
Rogers, J. C. & Holm, M. B. (1991). Occupational therapy diagnostic reasoning: a component of clinical reasoning. American Journal of Occupational Therapy 45(11), 1045–1053.
Uniform Data System for Medical Rehabilitation (1997). The Guide for the Uniform Data Set for Medical Rehabilitation (Including the FIM Instrument), Version 5.1. Buffalo: UDSMR.
World Health Organization (2001). International Classification of Functioning, Disability and Health. Geneva,World Health Organization.
World Health Organization (2005). International Statistical Classification of Disease and Related Health Problems, 10th Revision, (2nd ed). Geneva, World Health Organization.
Yesavage, J. A. (1988). Geriatric depression scale. Psychopharmacology Bulletin, 24, 709.
Curtin_Ch005_main.indd 65 9/15/2009 2:16:36 PM

E
Curtin_Ch005_main.indd 66 9/15/2009 2:16:36 PM







![Welcome [booksite.elsevier.com]booksite.elsevier.com/9780123745149/appendices/CD-ROM_Menu_Bo… · Welcome to the Programming Language Pragmatics, ... Scopes, and BindingsNa ... 8.2.2](https://img.pdfslide.us/doc/110x75/5aa6559c7f8b9ae7438ea65f/welcome-welcome-to-the-programming-language-pragmatics-scopes-and-bindingsna.jpg)











![Section Two: Poetry [60]](https://img.pdfslide.us/doc/110x75/61bd383561276e740b108b09/section-two-poetry-60.jpg)