Embed Size (px)
Citation preview

Tutorial on Breast Pathology Part I: Ductal and Lobular Neoplasias
Thomas J Lawton MD, Director Seattle Breast Pathology Consultants, LLC
Seattle, WA

• There are two main types of epithelial cells in the breast: Ductal and Lobular.
• The distinction is based on how the cells look and how they grow, not necessarily on their location in the breast.
• So ductal cells can travel into the lobules and lobular cells can travel up the ducts.

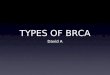
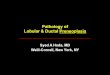
Normal breast duct and lobules
lobule
duct
lobule

Let’s start with ductal….

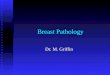
There are three main ductal lesions: 1) ductal hyperplasia, usual type; 2) atypical ductal
hyperplasia; and 3) ductal carcinoma in situ Ductal hyperplasia Atypical ductal hyperplasia Ductal carcinoma in situ

Ductal hyperplasia, usual type
• This basically means there are too many ductal cells in the ducts but they are not atypical.
• Often graded as mild, moderate, or severe (florid). • Studies show there is an increased relative risk
(1.5-2 times) for the subsequent development of invasive carcinoma with moderate to florid ductal hyperplasia.
• This risk applies to both breasts.

Ductal hyperplasia: What does it mean if my biopsy shows this? • If found on core needle biopsy and the
findings are concordant to the radiologist, no need for surgical excision.
• If found on a surgical excision and nothing more significant is found, no need for the pathologist to comment on margins and no need for surgical re-excision.

Atypical ductal hyperplasia • This term describes a proliferation of ductal cells
that has “some, but not all” of the features of low grade ductal carcinoma in situ.
• Studies show there is an increased relative risk (4-5 times) for the subsequent development of invasive carcinoma.
• This risk applies to both breasts.

Atypical ductal hyperplasia: What does it mean if my biopsy shows this? • If found on core needle biopsy, surgical excision
is warranted because of an approximate 20-30% chance of finding carcinoma in situ or invasive carcinoma based on most studies.
• If found on a surgical excision and nothing more significant is found, no need for the pathologist to comment on margins and no need for re-excision in the vast majority of cases.

Ductal carcinoma in situ • This term refers to a neoplastic proliferation of
ductal cells that has not invaded beyond the confines of the duct.
• Studies show there is an increased relative risk (8-10 times) for the subsequent development of invasive carcinoma.
• This risk applies to both breasts. • However, ductal carcinoma is situ is also felt to be
a precursor lesion, unlike atypical ductal hyperplasia and usual type ductal hyperplasia.

• Risk lesions imply a relative increased risk for the development of invasive carcinoma which applies to both breasts, not just the breast involved by the diagnostic risk lesion.
• A precursor lesion is thought to also be able to proceed to invasive carcinoma in the same part of the breast if it is not treated appropriately.
• This is why surgeons try to get clear margins around ductal carcinoma in situ and often patients receive radiation therapy and/or endocrine therapy. The reason is to try to reduce the risk of this precursor lesion proceeding to invasive carcinoma at a later time.

Ductal carcinoma in situ: What does it mean if my biopsy shows this? • If found on core needle biopsy, surgical excision is
necessary. • If found on a surgical excision, the size of DCIS,
nuclear grade, presence of necrosis, and distance from all surgical margins should be reported by the pathologist.
• If margins are close, additional surgery may be needed. • Radiation therapy may also be needed. • In many cases, a medical oncologist may ask the
pathologist to determine if the DCIS is estrogen receptor positive.

Now on to lobular…

Lobular hyperplasia
• Not a well-defined pathologic term • Diagnosis not generally used

Atypical lobular hyperplasia • A proliferation of small cells that begin to fill up
but do not expand the milk-producing glands in the lobules.
• Studies show there is an increased relative risk (4-5 times) for the subsequent development of invasive carcinoma, similar to atypical ductal hyperplasia.
• This risk applies to both breasts.

Atypical lobular hyperplasia: What does it mean if my biopsy shows this?
• If found on core needle biopsy, most doctors will recommend a surgical excision but this is somewhat controversial.
• If found on a surgical excision and nothing more significant is found, the pathologist does not need to comment on surgical margins, and no surgical re-excision is needed.

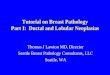
Lobular carcinoma in situ
• A proliferation of bland cells that fill up and expand at least 50% of the milk-producing glands in the lobules.
• Studies shows there is an increased relative risk (8-10 times) for the subsequent development of invasive carcinoma.
• This risk applies to both breasts.

Lobular carcinoma in situ

Lobular carcinoma in situ: What does it mean if my biopsy shows this?
• If found on core needle biopsy, most doctors will recommend a surgical excision but this is somewhat controversial.
• If found on a surgical excision and nothing more significant is found, the pathologist does not need to comment on surgical margins, and no surgical re-excision is needed.

Stay tuned for Part II which will cover invasive carcinomas…