Embed Size (px)
Citation preview

Tungs' Medical Journal
Contents in Brief
EdiTorial
69 Simulation-based Training in Medical residency Training ProgramChing-Shiang Chi
rEViEW arTiClE
73 Transient receptor Potential Cation Channel Subfamily V Member 4 (TrPV4): a Multifunctional Channel and Potential Therapeutic Target for analgesiaHueng-Chuen Fan, Xuming Zhang, Peter A. McNaughton
original arTiClE
85 risk Factors for Methicillin-resistant Staphylococcus Aureus in Two regional HospitalsWang-Feng Shen, Ya-Hua Liang, Ming-Tsung Lee, Mei-Pei Ling, Yi-Ming Kuo, Yu-Ying Yang
95 Portfolio assessment for a Postgraduate Year one residency Training Program: a rasch analysisChin-Yi Huang, Ming-Tsung Lee, Jhin-Long Jiang, Yi-Cheng Liao, Lon-Yen Tsao
CaSE rEPorT
102 Traumatic rhabdomyolysis-induced acute renal Failure: a Case report and review of literatureWang Shih-Nung, Tung Yung-Wei
108 Complicated Meckel’s diverticulum initially Presenting with Small Bowel obstructionChun-Hsiang Chang, Min-Yung Kuo
113 a different Method for Treating Pseudoarthrosis of the Surgical neck of the Humerus: a Case reportSheng-Chi Chen, Shao-keh Hsu
118 Cervical Trachea Transection after neck Blunt Trauma: a Case reportPei-Hung Liao, Ming- Sheng Lin, Yung-Wei Chiu, Chao-Hsin Wu, Yung Wei Tung
123 neonatal Femoral Fracture: a Case reportHui-Chien Lai*
127 Sudden onset of Blisters during remisson from Stevens–Johnson Syndrome/Toxic Epidermal necrolysisChu-Ju Hung, Sheng-Wen Wu, Chin-Yin Liu
Vol. 11 no. 2 July-december 2017

PaTHologY PagE
131 nodular Histiocytic Prostatitis: a Case report and literature reviewLi-Hua Huang, Zhon-Min Huang, Min-Zhe Tung, Tang-Yi Tsao
iMagE
135 gas-forming Pyogenic liver abscesses Mimicking Bowel gasChao-Hsin Wu, Li-Hua Lu, Chen-kuo Chu
Vol. 11 no. 2 July-december 2017

69
Simulation-based Training in Medical Residency Training Program
Ching-Shiang Chi*
Tungs’ Taichung Metroharbor Hospital Taichung, Taiwan
Received: Nov. 29, 2017; Accepted: Nov. 29, 2017
Abstract
Improving patient safety is an important focus in medical field internationally. Raising resident’s competency before they deal with real patients is thus a crucial consideration in medical school curricula and residency training programs. As simulation-based training provides simulated scenarios with real-life features for medical students and residents to practice and master their clinical skills before they face real patients, many medical schools and teaching hospitals have started to use simulation-based training as a crucial and effective instrument in their curricula and training programs. Nevertheless, understanding different types of simulators will help the program instructors select an appropriate simulator based on student learning goals. In addition to having the proper tools chosen for the simulation-based training, a well-designed training process is also key for the success of the training program.
Key words: Simulation-based Training, Simulator, Competency
Residency training is a critical stage of medical education. In most countries, completing a residency training program is one of the prerequisites toward medical practice. The goal of a residency is to provide a learning environment for medical students to improve their competency. Under the supervision of experienced and knowledgeable physicians, students not only further develop their medical knowledge, but also practice several clinical skills in a hospital setting. Usually during residency training, students learn from real patients and deal with a variety of serious situations that they encounter while they are in the program. In recent years, the awareness of patient safety has shifted many medical education curricula and training programs. Aligning simulation-based training to residency program for improving patient safety is recognized by medical professionals to be the mainstream movement all over the world. Simulation-based training is not a brand-new concept
in medical education. However, with the advance-ment of modern technology, high fidelity simulators have been created to maximize training achieve-ments to help students develop their skills before they face real patients. Many medical schools and medical centers have started to set up laboratories or simulation centers for supporting school curricula or residency programs. The objective of this article is to review simulation-based training in residency programs through examining the types of simulators and discussing how to appropriately implement a simulation-based training so as to set up an effective learning environment.
In 2011, an in-depth analysis of 600 studies in evaluation of simulation-based training program shows that technology based simulation training has significant effects for medical students’ clinical skills and patient-related outcomes[1]. Simulation learning is an imitated real-life situation for obtaining educational objectives. It is usually implemented in an existing training program and alongside other traditional approaches simultaneously. Neverthe-less, the simulation-based training has to be an
Tungs’ Medical Journal 11 (2017) 69-72
Editorial
* Correspondence to: Dr. Ching-Shiang Chi, Tungs’ Taichung Metroharbor Hospital, No. 699, Sec. 1, Chungchi Road, Wuchi, Taichung, 435, Taiwan, (R.O.C.)

70 Ching-Shiang Chi / Tungs’ Medical Journal 11 (2017) 69-72
effective intervention for goals that traditional training methods cannot easily attain. By using simu-lators, program instructors can adhere to resident needs to plan clinical cases, thus allowing learners to explore different types of scenarios and diseases, including complicated and uncommon cases that are not likely to be found in patients in the region of the residency program. Through consistent simulation learning opportunities, a resident will be able to expe-rience every aspect of the medicine field that they are going to practice. As such, the training program as a whole become a more complete and thorough expe-rience for residents, as they are prepared for even the most extraordinary cases and circumstances. A study by Johns Hopkins Medicine research team has found that “medical errors are No. 3 cause of US deaths”[2]. To avoid the risks caused by the inexperience of residents, using simulators allows junior residents to practice the same skills repeatedly until they master the skills. In addition, they can learn from mistakes without harming a patient’s safety especially for inva-sive procedures and medical decisions related to life-threaten situations.
The core tool of simulation-based training is, of course, a simulator. The decision of choosing a suit-able simulator for a program depends on the focus of the training. A simulator can simulate patient’s condition or even interaction caused by users’ input. It also functions as a model used both for demonstra-tion and for residents to practice clinical skills. There are several types of simulators, based on the fidelity and complexity of simulation, commonly used in many medical training programs. The basic type of simulator is a 3-D mannequin model that has little to no interface with users’ input. Program instructors can use it to do demonstration or provide opportu-nities for learners to practice certain skills, such as Brain Structure Model, Circulatory System Model, Acupuncture Model…etc. Screen-based simulator is a simulator which may include video clips, com-puter software, or virtual reality (VR). For example, a computer software simulator in which a user can choose an intubated patient from a list will display a video showing the patient’s situation. A user will use his or her observation and the data provided from the video to make a clinical decision. Then the user can use a keyboard or a mouse to input an infusion rate; the software will provide feedback as well as the patient’s outcome according to the treatment
decision. This outcome can be automatically gener-ated by the computer program or an operation con-troller[3]. Screen-based simulators are considered to be low fidelity simulators because the unrealistic screen setting most likely only provides a practice for cognitive skills instead of allowing users to physically exercise their clinical motor skills. Due to the rapid updates of technology, modern medical simulators have been developed to the level of intermediate fidelity up to high fidelity. Both fidelity levels of simu-lators offer the types of training that can help stu-dents grow their competences and further develop their psychomotor, cognitive, and interpersonal skills. Those types of simulators are usually computer con-trolled with a full size or part of a body model. A high fidelity simulator has sets of pre-programed patient scenarios in the primary software but a simulation controller can create a new situation or complication to override the original design[3]. There are multiple sensors provided in high fidelity simulator systems to display the data resulting from users’ actions and treatments. In addition, some features such as breathing with coordinated breath sounds, realistic light reactive eyes, and detailed internal simulated body structure and organs are in a variety of simu-lator products in order to deliver an adequate and quality learning experience for users. In addition to the technology aspect for simulation trainings, a stan-dardized patient simulation training program is also used widely in many teaching hospitals for residency training purpose. When using a standardized patient simulation, a training center will carefully train actors to play a role as a patient. Therefore, trainees can practice their communication, physical exam, and other skills.
A full-scale simulation training should include certain essential elements. Besides choosing the appropriate simulators, an authentic simulated environment and specific meaningful feedbacks are other key components for the effectiveness of a sim-ulation-based training program. To start a simulation practice, the planned practice goals should be pre-defined and communicated clearly with the learners. The important prerequisite knowledge and founda-tion skills for the designed simulation practice should be fully taught to the residents before they begin the simulation practice. In order to meet their goals, learners might need to practice repeatedly until the focused learning skills are mastered. During practice,

71Ching-Shiang Chi / Tungs’ Medical Journal 11 (2017) 69-72
learners should handle the simulation in a careful and respectful manner, as they would do with real patients. After completing each practice, a debrief should be provided for learners. The feedback can be data and reaction acquired from the simulators after the learners perform their practice. The other more detailed feedback is coming from program instruc-tors. Learners’ self-reflection usually is the first step during post-debrief session. They should reflect on their decision making process, observation of patient reaction process, and self evaluate patient’s outcome. Following the learners’ self-reflection, program instructions will provide oral feedback regarding learners’ performance. This type of feedback will not just be limited in the psychomotor skills domain, it should also include the cognitive domain and how the learner implemented a medical practice guideline and handled a situation under a stressful environ-ment[4]. A complete simulation learning cycle will help learners make sense of the situation, promote problem-solving skills, practice critical clinical skills, and develop self-reflection techniques to enhance their clinical competence[5].
Simulation-based training for residency pro-grams in a teaching hospital is a rapidly growing teaching approach. It not only helps learners increase
their competency in their service areas, but also improve the patient safety. Along with new technolo-gies, high-level fidelity simulators have been created to improve the quality of simulation-based training. However, a successful simulation-based training needs to have a proper simulator and a well designed curriculum. Residents need to receive a pre-session to make sure they have the prerequisite knowledge and skill before starting the simulation practice. A fully constructed debrief will allow learners to reflect on their performance and get advice on ways to improve their future practice.
References
1. Cook DA, Hatala R, Brydges R, Zendejas B, Szostek JH, Wang AT, et.al. Technology-enhanced simulation for health professions education: a systematic review and meta-analysis. JAMA 2011; 306: 978-88.
2. Makary MA, Daniel M. Medical Error- the third leading cause of death in the US. BMJ 2016; 353: 2139.
3. Pott LM, Budde AO, Murry WB. A proposed classification of simulatos. Middle East J Anesth 2009; 20: 179-186.
4. Rudolph JW, Simon R, Raemer DB, Eppich WJ. Debriefing as formative assessment: closing performance gaps in medical education. Acad Emerg Med 2008; 15: 1010-6.
5. Burns CL. Using debrief and feedback in simulation to improve participant performance: an educator’s perspec-tive. Int J Med Educ 2015; 6: 118-120.

72 Ching-Shiang Chi / Tungs’ Medical Journal 11 (2017) 69-72
模擬本位訓練在住院醫師訓練的運用
遲景上*
童綜合醫院
受文日期:民國 106年 11月 29日;接受刊載:民國 106年 11月 29日
摘要
病人安全是近年來國際醫學界一重要議題。為了提升病人安全,在住院醫師真正面對病人前,培養
並確認住院醫師有足夠的知識及技能來處理病人的問題是各大醫學院及教學醫院一重大方向。模擬本位
學習是利用模擬器製造一個模擬真實情境的訓練環境,讓醫學院學生及醫院住院醫師在面對真正病人前
能有足夠的機會練習一些必要的技能,因此在現今許多醫學院及教學醫院已將模擬本位學習融入教學課
程及住院醫師訓練流程中。依照各訓練課程目標選擇適當模擬器是一個模擬本位訓練的要素。 然而課程訓練負責老師必須充分了解各項模擬器的功能及合併教學目標才能為訓練課程選擇一適當的模擬器。除
此之外,一個完善設計的訓練課程計畫更是一個成功模擬本位訓練不可或缺的決定因素。
關鍵詞:模擬本位訓練、技能、模擬器
*通訊作者:遲景上醫師 童綜合醫療社團法人童綜合醫院 43503臺中市梧棲區臺灣大道八段 699號

73
Transient Receptor Potential Cation Channel Subfamily V Member 4 (TRPV4): A Multifunctional Channel and Potential
Therapeutic Target for Analgesia
Hueng-Chuen Fan1,2,*, Xuming Zhang2,3, Peter A. McNaughton2,4
1Department of Pediatrics, Department of Medical research, Tungs' Taichung MetroHarbor Hospital, 43503, Taichung, Taiwan2Department of Pharmacology, University of Cambridge, Cambridge, CB2 1PD, UK
3Rowett Institute of Nutrition and Health & Institute of Medical Sciences; University of Aberdeen, Foresterhill, Aberdeen, UK4Wolfson Centre for Age-Related Research, King’s College London, Guy’s Campus, London Bridge, London, UK
Received: May. 19, 2016; Accepted: Aug. 29, 2016
Abstract
Transient receptor potential cation channel subfamily V member 4 (TRPV4), is a polymodal receptor activated by hypotonicity, innocuous heat, and phorbol esters. TRPV4 is expressed in several tissues, including the lungs, spleen, kidneys, testes, fat, cochleas, skin, smooth muscle, liver, vascular endothelium, central nervous system, and dorsal root ganglia. In addition to this wide distribution, it has a broad spectrum of activators and is a nociceptor in inflammatory hyperalgesia generated by inflammatory mediators in inflamed tissues. After tissue injury, inflammatory mediators activate downstream kinases, specifically protein kinase C (PKC) and protein kinase A (PKA), both of which sensitize TRPV4 through phosphorylation and cause hyperalgesia. Despite intensive efforts to develop pain-blocking therapy based on this pathway, several nonspecific effects and side effects have halted the development of TRPV4 blockers. AKAP79 (A kinase anchoring protein 79) can orchestrate distinct signaling molecules, such as PKA and PKC, and enhance their phosphorylation to modulate target proteins. Interestingly, the administration of small interfering RNA against AKAP79 can abolish inflammatory hyperalgesia and is a promising target for the development of a novel class of analgesics.
Key words: Transient Receptor Potential, Transient Receptor Potential Cation Channel Subfamily V Member 4, Protein Kinase A, Protein Kinase C, Small Interfering RNA, A Kinase Anchoring Protein
Introduction
The International Association for the Study of Pain defines pain as “an unpleasant sensory and emotional experience with actual or potential tissue damage, or described in terms of such damage”[1]. Pain is an essential early warning that protects us from injury, and people seek medical care if that pain is intense or becomes chronic or persistent. Although approximately one-third of the world’s population
suffer from chronic pain, many currently available therapies are either inadequate or laden with side effects. This is an unfortunate state of affairs because patients with chronic pain can return to normal life and regain normal function if their pain can be effec-tively controlled.
Understanding how pain is generated and becomes chronic is key to overcoming the suffering associated with pain. Advanced technologies, such as positron emission tomography and functional mag-netic resonance imaging, have helped us to identify specific cortical loci that process complex pain mes-sages. However, even greater progress has been made in understanding the molecular mechanisms
Tungs’ Medical Journal 11 (2017) 73-84
Review Article
* Correspondence to: Hueng-Chuen Fan, MD, Msc, PhD, Depart-ment of Pediarics, Tungs’ Taichung MetroHarbor Hospital, No. 699, Sec. 8, Taiwan Blvd., Wuqi Dist., Taichung City 43503, Taiwan (R.O.C.)

74 Hueng-Chuen Fan et al. / Tungs’ Medical Journal 11 (2017) 73-84
by which primary sensory neurons detect pain-pro-ducing stimuli during nociception.
Nociception, nociceptors, and hyperalgesiaNociception is not only an evolutionally con-
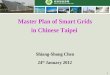
served mechanism in many species but also key to survival. The nociceptive system consists of nocicep-tors in peripheral nerves and neurons in the central nervous system. Nociceptors are primary sensory neurons activated by stimuli capable of causing tissue damage. They are thinly myelinated Aδ and unmy-elinated C fibers that terminate as sensory “free nerve endings.” Most nociceptors are polymodal and respond to mechanical, thermal, and chemical insults by generating action potentials that propagate via the dorsal horn of the spinal cord to higher brain centers to cause the sensation of pain. To facilitate this, several ion channels and receptors on cell mem-branes sense and transduce stimuli (Fig 1).
Hyperalgesia results from a dynamic process in
which the sensitivity of a nociceptor increases over time under the continued presence of a painful stim-ulus. Inflammatory mediators, such as prostaglan-dins, bradykinin, adenosine triphosphate, protons, and nerve growth factor, which are released from injured tissues, enhance the sensitivity of nocicep-tors. These nociceptors, in turn, can actively release neuropeptides like substance P and calcitonin gene-related peptide in response to external stimuli, leading to vasodilation, plasma extravasation, mac-rophage attraction, and mast cells degranulation[2]. Therefore, nociceptors can achieve nociception through both passive and active mechanisms.
Transient receptor potential channel superfamilyTransient receptor potential (TRP) channels are
a group of ion channels in the cell membrane com-prising six subfamilies and 28 channels in humans. These channels can sense changes in the environ-ment, such as cold or hot temperatures, chemical
Mastcell Tissue
damage
Marcophage
TRPV4EP/IP B1/B2 ASIC5HT H1
5HTHistamine PGE2
Bradykinin H+
TrkA TRPV1
?NGF
TTXR
PKA PKC
Gene regulationCGRP
SP
Heat
Hypo-tonic
Ca2+
Mastcell Tissue
damage
Marcophage
TRPV4EP/IP B1/B2 ASIC5HT H1
5HTHistamine PGE2
Bradykinin H+
TrkA TRPV1
?NGF
TTXR
PKA PKC
Gene regulationCGRP
SP
Heat
Hypo-tonic
Ca2+
Fig. 1 Mechanism of inflammatory pain (peripheral sensitization)Peripheral sensitization contributes to the pain hypersensitivity found at the site of tissue damage and inflammation, and the action of inflammatory chemicals or mediators, such as bradykinin, prostaglandin E2, and nerve growth factor (NGF) released around the site of tissue damage or inflammation cause hyperalgesia. The temperature threshold of the Transient Receptor Potential Vanilloid 1 (TRPV1) ion channel is lowered by these pro-inflammatory mediators, which activate protein kinase Cε (PKCε) and then in turn sensitizes TRPV1. Sensitization of the TRPV1 is an important cellular mechanism of inflammatory pain. Apart from by activating PLC leading to the metabolism of PIP2 to activate the TRPV1, NGF can sensitize TRPV1 by Src mediated tyrosine phosphorylation, by triggering the rapid movement of TRPV1 channels to the surface membrane. NGF also can up-regulate gene expression. Protons released from tissue damage can activate the Acid Sensitive Ion Channel (ASIC) and the TRPV1 channels, but the effect on TRPV4 is controversial. TRPV4 is also a nociceptor, and is activated by cell swelling. Whether pro-inflammatory mediators can sensitize this nociceptor is unclear. Substance P (SP) and Calcitonin Gene-Related Peptide (CGRP) released from the peripheral terminal, initiate plasma extravasation; increased tetrodotoxin resistant (TTX-R) sodium channel sensitivity enhances the cell’s capacity to be depolarized (central sensitization).

75Hueng-Chuen Fan et al. / Tungs’ Medical Journal 11 (2017) 73-84
compounds, mechanical stimuli, or acidity. Initially, they were identified in Drosophila melanogaster by mutations in the TRP gene that resulted in pheno-types with transient voltage responses of photore-ceptors to light stimulation[3]. The TRP superfamily is divided into at least seven subfamilies: TRPA (A for ankyrin), TRPC (C for canonical), TRPM (M for melastatin), TRPML (ML for mucolipin), TRPN (N for NOMPC (no mechanoreceptor potential C)), TRPP (P for polycystic), and TRPV (V for vanilloid). Classi-cally, thermo-TRP channels include TRPV1–4, TRPM8, and TRPA; although TRPM2, TRPM4, and TRPM5 also show temperature sensitivity, they are not included because none is expressed in primary somatosen-sory neurons. TRP channels have primary structures similar to those of voltage-gated channels and cyclic-nucleotide-gated channels[4].
The TRPV subfamily have key roles in physiolog-ical processes, such as thermoception, nociception, mechanoreception, renal Ca2+/Mg2+ balance, smooth muscle tone, and blood pressure regulation. This sub-family has six functional members, TRPV1–6[5]. Each protomer contains six transmembrane segments flanked by two intracellular domains that locate intracellularly: a large N-terminal domain containing
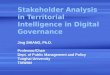
ankyrin repeats and a short C-terminal domain. Most of these proteins have a putative topology of six transmembrane domains with a pore loop between the fifth and sixth segments[6] (Fig 2). Amino acid sequences flanking the pore are highly conserved within the TRP superfamily, with approximately 25 amino acid residues per TRP domain. TRPV1–4 are heat sensitive and transduce different tempera-tures from warm temperature (TRPV4 and TRPV3) to noxious heat (TRPV1 and TRPV2), whereas TRPV5 and TRPV6 cannot be activated by either physical or chemical stimuli.
Capsaicin, the component of chili peppers responsible for topic burning or stinging pain, can produce nausea, vomiting, abdominal pain, and burning diarrhea if ingested in large amounts. Eye exposure produces intense tearing, pain, conjuncti-vitis, and blepharospasm. A specific capsaicin-sen-sitive receptor, vanilloid receptor 1, was first cloned from a rodent dorsal root ganglia cDNA library[2], and further study led to it being renamed TRPV1[7]. TRPV1 is a promiscuous channel activated by a wide range of stimuli, including capsaicin, acid, ethanol, anan-damide, lipoxygenase, and pain[7], making it a molec-ular integrator of many noxious stimuli.
i ii iii iV V Vi
nH2
CooH
extracellular
intracellular529
651
509
466
a812
831
486 571
551
573
593
637
617
691
711
663 676
798
809
a
aaa
a
162
175
189
824
i ii iii iV V Vi
nH2
CooH
extracellular
intracellular529
651
509
466
a812
831
486 571
551
573
593
637
617
691
711
663 676
798
809
a
aaa
a
162
175
189
824
Fig. 2 a predicted transmembrane topology with functional domains of TrPV4 and the corresponding sequence The predicted structure of TRPV4 is: N- and C- terminals; six ankyrin repeat domains (yellow; there are several small sequence insertions that affect the overall ARD structure); six transmembrane domains (from I to VI, gray); the pore region is marked in red. The glycosylation site locates at aa651 (green). The calmodulin binding site is in blue type. The microfilament associated protein 7 (MAP7) binding site is in brown type.

76 Hueng-Chuen Fan et al. / Tungs’ Medical Journal 11 (2017) 73-84
Within the TRPV subfamily, TRPV4 displays sig-nificantly stronger homology with TRPV1–TRPV3 than with TRPV5 and TRPV6. Indeed, TRPV4 is involved in several human physiological functions and diseases, such as shear stress-induced vasodilation, circulatory function, auditory function, neuropathic pain, cystic fibrosis, neuromuscular disorders, and cancer[8-12]. This review focuses on the structure and function of this novel channel and its role in human disease.
Distribution of TRPV4The gene for human TRPV4 is localized on chro-
mosome 12q23-q24.1 and has 15 exons that encode a protein with 871 amino acids. TRPV4 is expressed in neurons of the lamina terminalis, median pre-optic area, optic chiasm, subfornical organ, ventral hippocampal commissure, anterior hypothalamus, and dorsal root ganglia, and in ependymal cells of the choroid plexus in the lateral ventricles[13]. It is also detected in the kidney, particularly in the distal tubule, where it is mainly localized to the basolateral membrane of the renal epithelial cells that have low water permeability[14]. Its presence in respiratory epi-thelium and smooth muscle cells suggests that it may have a role in bronchoconstriction secondary to the inhalation of a hypotonic aerosol[15]. In blood vessels, TRPV4 is present in endothelium, where it is respon-sible for sensing blood flow shearing force[16]. TRPV4 may also be involved in hearing because its mRNA is present in the inner ear, the inner and outer hair cells of the organ of Corti, and the hair cells of the semi-circular canals and utricles[11]. Although it has been detected in the spleen, testis, fat, skin, and liver, its functions in these organs are unclear.
The structure of TRPV4The basic architecture of TRPV channels con-
tains four identical or similar subunits with six trans-membrane domains (TM1–6) and cytosolic N- and C-terminal tails that tetramerize to form a functional channel[17]. TM5, TM6, and the connecting pore loop form the central cation-conducting pore, whereas TM1–4 and the cytoplasmic N- and C-terminal parts are thought to contain the regulatory domains that control channel gating[18].
The N-terminal domain of TRPV4The N-terminal domain of TRPV4 spans from
amino acid 1 to 465. The ankyrin repeat domains
(ARDs) localize in this domain, with a predictive region from amino acid 236 to 314[19]. Each ARD con-sists of several small sequence insertions that affect the overall ARD structure: Ankyrin repeats 1–3 have unusually long and flexible fingers, whereas repeats 5–6 have unusually long outer helices. We previously identified that sites 162, 175, and 189 in the N-ter-minal of TRPV4 were crucial to the protein kinase C (PKC)-dependent phosphorylation in a model of inflammatory hyperalgesia[20]. A more recent pub-lication confirmed that the response of TRPV4 to phorbol 12-myristate 13-acetate was Src depen-dent, suggesting that tyrosine phosphorylation may underlie the mechanisms of action of TRPV4[21].
Ankyrin repeat domainsStructurally, ARDs are 33-residue sequence
motifs that fold into a helix–loop–helix structure in proteins. It has been shown that a single mutated residue in an individual repeat can affect the entire three-dimensional core structure[22], suggesting that ARDs stabilizes the associated ion channel. In a study of the design and biophysical characteristics of ARDs by in-house JAVA- or PERL-based programs, it was concluded that they might serve as a scaffold for protein–protein interactions[23]. However, the crystal structures of the ARDs in TRPV1 and TRPV2 suggested that they did not promote the tetrameric assembly of ion channels but were instead responsible for regula-tion[24]. Therefore, ARDs are versatile, with functions including stabilization of ion channels, cell–cell sig-naling, and regulation.
The C-terminal domain of TRPV4The carboxyl tail (i.e., C-terminal) of TRPV4 is
the docking site for at least two interacting proteins, calmodulin and microfilament-associated protein 7 (MAP7). Calmodulin is located at positions 814–829 in the C-terminal domain of TRPV4 (Fig 3, blue) and con-trols several Ca2+-dependent cellular reactions and modulates several ion channels, including TRPV4[25]. The binding for MAP7 is at sites 798–809 in the C-ter-minal domain of mouse TRPV4 (Fig 3, brown). Given that TRPV4 and MAP7 coexpression has been shown to increase TRPV4 membrane expression[26], TRPV4 may be involved in cytoskeletal interaction. Our group identified site 824 in the C-terminal domain of human TRPV4 as the phosphorylation site of protein kinase A (PKA)[20], and Peng et al.[27] used mass spectrometry

77Hueng-Chuen Fan et al. / Tungs’ Medical Journal 11 (2017) 73-84
to show that 824 is phosphorylated by both PKA and PKC. These findings highlight that activation or phos-phorylation by kinases on a target channel may con-tribute to the development of hyperalgesia. Interrup-tion of the interaction between these kinases and the channel may generate analgesia.
Membrane-spanning core region and pore loopThe membrane-spanning core region of TRPV4
spans from sites 466 to 711. The 245 amino acid central domain of TRPV4 comprises TM1–6, which, between TM5 and TM6, feature a short hydrophobic region that is the putative pore region or pore loop.
This may contain a highly hydrophobic pore helix, with ion selectivity serving as a filter. TRPV4 displays only a few predicted short extracellular domains: the amino acids between TM1 and TM2, an amino acid between TM3 and TM4, 25 amino acids upstream of the pore loop, and the 14 amino acids downstream of the pore loop. One glycosylation site (amino acid 651; see Fig 2, marked in green), in an extracellular stretch between TM5 and the pore region, has been shown to be glycosylated in heterologously expressed TRPV4[28].
Activation of TRPV4 may result in a significant influx of Ca2+ that triggers Ca2+-dependent signaling
L - Y P VV g Y g DT A - T TW W S V EY P R A LK c s a
A N Y V VI I D G PL F - L TF S T F EY P M A LT r P V 6
A N Y S VI I D G PL F - L TF S T F EY P T A LT r P V 5
l E M L Si g M g dL F K L TT F L L DS E T F ST r P V 4
l N I Q Qi g l g dL F K L TD A V L EY G S F ST r P V 3
l A F Q Ei g M g EL F K F TE A S L EY R G I LT r P V 2
l E F T Ei g M g dL F K F TS T C L EY N S L YT r P V 1
L - Y P VV g Y g DT A - T TW W S V EY P R A LK c s a
A N Y V VI I D G PL F - L TF S T F EY P M A LT r P V 6
A N Y S VI I D G PL F - L TF S T F EY P T A LT r P V 5
l E M L Si g M g dL F K L TT F L L DS E T F ST r P V 4
l N I Q Qi g l g dL F K L TD A V L EY G S F ST r P V 3
l A F Q Ei g M g EL F K F TE A S L EY R G I LT r P V 2
l E F T Ei g M g dL F K F TS T C L EY N S L YT r P V 1
Hydrophobic pore helix Selectivity pore S6 linker
a
B
Ti
gMg
d
Fig. 3 Alignment of the putative pore regions of the six mammalian TRPV channels and of the Streptomyces lividans potassium channel KcsA.(A) A homology model for the pore structure of TRPV1 is illustrated by using the Swiss-Model and the Swiss-Pdb Viewer software (www.expasy.ch/swissmod/SWISS-MODEL.html). The structure of the hydrophobic pore helix is in red colour, the selectivity pore in green and the S6 linker in yellow. (B) There are portions of sequences of putative pore regions of human TRPV1- TRPV6, and Streptomyces lividans KcsA. The pink box indicates the region with the highest homology among TRPV1 and TRPV4. The sequence similarities may indicate conserved pore structures for these cation channels. The letters marked red highlight the putative pore sequence of TRPV4. The grey box indicates the region of “K+ channel signature sequence” (TXXTXGYGD). The GYG motif in the pore of the K+ selective channel is changed into a GMG motif for TRPV1, -2, and -4 and a GLG motif for TRPV3. TRPV1 accession no.: NP_542435; TRPV2 accession no.: NP_057197; TRPV3 accession no.: NP_659505; TRPV4 accession no.: NP_067638.3; TRPV5 accession no.: NP_062815; TRPV6 accession no.: AAH34814; KcsA, S. lividans, accession no.: PIR S60172. Modified from Nilius et al. [19].

78 Hueng-Chuen Fan et al. / Tungs’ Medical Journal 11 (2017) 73-84
pathways. Because Ca2+ channels are as abundantly distributed in the nervous system as voltage-gated K+ channels, the pore structure of TRPV4 may be similar to that of the bacterial KcsA K+ channel19. Figure 3 shows an amino acid sequence alignment of the puta-tive pore regions of the six mammalian TRPV chan-nels, illustrating the high sequence conservation for TRPV1 to TPRV4. The sequences in the so-called K+ channel signature sequence also show homology with the pore sequences of the TRPV family (Fig 3, gray box, labeled). Amino acid sequences from 677 to 682 (TIGMGD) form the important part of the pore loop (similar to TXGYGD in the K+ channel) and deter-mine ion selectivity and permeability. The GYG motif in the K+-selective pore changes to a GMG motif for TRPV1, TRPV2, and TRPV4, but to a GLG motif for TRPV3, which may explain the different electrophysi-ological findings[29].
Voets et al.[30] reported a mutation in the TRPV4 residue (M680), which they considered equivalent to the GYG motif in the K+ channel, and stated that it strongly reduced current amplitude and impaired Ca2+ permeability in the whole cell. They found that mutated Asp 672 and Asp 682 resulted in stronger reductions in Ca2+ permeability and modification in the permeability to monovalent cations, suggesting that these sites were involved in determining Ca2+ permeability for the TRPV4 channel. The architecture of the bacterial KcsA channel may provide a model for investigating the pore and selectivity filtering of TRPV4.
TRPV4 is activated by a variety of stimuli, including the following:
1. Heat. The most studied thermo-TRPs are TRPV1 and TRPV4, which are activated at 43°C[31] and 27°C–35°C, respectively[32-34].
2. Acid. Heterologous TRPV4 expression in CHO cells has been shown to be activated at pH < 6, with maximum activation at pH 4[35]. Sequencing analysis (Fig 4) has also indicated that TRPV4 lacks a Glu at the equivalent position in the pore loop to Glu600, which is responsible for the potentiation of TRPV1 by protons[36]. However, TRPV4 does have a Glu at the position equivalent to Glu 648 that is involved in the activation of TRPV1 by protons.
3. Mucin. TRPV4 has been reported to be expressed in oviduct ciliated cells, which propel mucus over a wide range of viscosities[37]. The channel may also control ciliary beat frequency in airway ciliary movement[38].
4. Herbs. Bisandrographolide A is a traditional medicine in Asia, used for illnesses including upper respiratory tract infections, diarrhea, fever, tonsillitis, and snakebites. This traditional medicine can activate TRPV4 with a half-maximal effective concentration of 790–950 nM[39]. The wide distribution and roles of TRPV4 may explain the varied pharmacological effects of bisandrographolide A.
5. Phorbol esters. These plant-derived organic compounds can activate PKC[40], with the most com-monly used phorbol esters being phorbol 12-myristate 13-acetate and 12-O-tetradecanoylphorbol-13-ac-etate. PKC mediates different cellular processes, including proliferation, differentiation, apoptosis, and migration, as well as nociceptor excitation and sensiti-zation[41;42]. When activated, PKC can phosphorylate
TM5 TM6
E
E
600648H+
H+
H+H+
H+
H+
….AVVTLI EDGKNDSLPSESTSHRWRGPACRPPD-------------LFKFTIGMGDLE FTENYDFKAVF……..
....ALVSLLN PCANMKVCNEDQTNCTVPTYPSCRD-------------LFKLTIGMGDLEMLSSTKYPVVF…….
600 648
TRPV1
TRPV4637 684
TM5 TM6
E
E
600648H+
H+
H+H+
H+
H+
….AVVTLI EDGKNDSLPSESTSHRWRGPACRPPD-------------LFKFTIGMGDLE FTENYDFKAVF……..
....ALVSLLN PCANMKVCNEDQTNCTVPTYPSCRD-------------LFKLTIGMGDLEMLSSTKYPVVF…….
600 648
TRPV1
TRPV4637 684
Fig. 4 The proton-gating sites, E600 and E648 of TRPV1Top: Portions of sequence of TRPV1 containing the proton-gating sites, E600 and E648, and the equivalent positions of TRPV4. Sequence analysis shows that TRPV4, at the equivalent position of TRPV1, has a Glu at the position of 637, but lacks a Glu at the position 684 (circled in red). Bottom: Protons act on two residues of TRPV1, E600 and E648 (pink)

79Hueng-Chuen Fan et al. / Tungs’ Medical Journal 11 (2017) 73-84
several cellular proteins, including enzymes and ion channels. Our group and others[43] have confirmed that TRPV4 is activated or sensitized by phorbol 12-myristate 13-acetate through a PKC-dependent pathway. Thus, PKC is important to mechanical hyper-algesia during inflammation.
6. Hypotonicity. TRPV4 is highly sensitive to changes in extracellular osmolarity, especially hypo-tonicity[13], and can help a cell to restore its volume when this channel is expressed[44]. These features warrant further discussion, which is outlined in the following text.
The expression of TRPV4 in the heart[8] and lung[45] suggests that it may be involved in the patho-physiology of heart failure associated with lung con-gestion and other pathological conditions associated with symptoms of lung edema/congestion, such as ventilator-induced lung injury[46]. TRPV4 expressed within bladder smooth muscle cells probably acts as a sensor of bladder pressure/stretch/filling, ultimately contributing to bladder contraction and hyperac-tivity. Targeting TRPV4 channels could, therefore, be expected to provide therapeutic benefit for bladder overactivity[47].
TRPV4 is found in neurons with osmosensing properties[48] and is essential to water balance in humans. However, the mechanisms for sensing changes in osmolarity at a cellular level remain unclear. Tyrosine phosphorylation targeting Src by the actin of protein hu-li tai shao (HTS), as well as the phosphorylation site at residue 253 of TRPV4, has been reported. Also, a mutation at residue 253 can dramatically abolish the activation of TRPV4 by HTS[49] (Fig 5, path A). Although our group cannot replicate these findings, it has been shown that endocannabi-noid anandamide and its downstream metabolite, arachidonic acid, can activate TRPV4 through the end product of 5,6-epoxyeicosatrienoic acid (5,6-EET)[50]. PLA2 is the critical enzyme triggering the activation of TRPV4, and the inhibition of the CYP 450 epoxy-genase can strongly abolish the activation of TRPV4 by arachidonic acid[32].
The core concept is that hypotonicity stretches the membrane by activating an endogenous signaling cascade: swelling-induced activation of PLA2, arachi-donic acid release from membrane phospholipids, and CYP 450 epoxygenase-dependent metabolism of arachidonic acid to EETs (Fig 5, path B). However, mass spectrometry showed sites 110 and 805 of the
N- and C-terminal domain of TRPV4, respectively, to be tyrosine phosphorylation sites, with the mutated 110 attenuating the activation of TRPV4 by HTS. Thus, tyrosine phosphorylation may be part of the mecha-nism of activation of TRPV4 by HTS[21].
Chemotherapy-induced hyperalgesiaPaclitaxel (PTX), vincristine, and oxaliplatin are
often used in chemotherapy for cancer but can induce mechanical hyperalgesia. In models of painful periph-eral neuropathy associated with PTX or vincristine, the action of TRPV4 in mechanical hyperalgesia was elicited by the formation of a complex with integrin or Src tyrosine kinase. The mechanical hyperalgesia was then markedly reduced by intrathecal adminis-tration of oligodeoxynucleotides antisense to TRPV4 (ODN-TRPV4)[51]. Goshajinkigan (GJG), which contains plant components, is a traditional Japanese medicine used for pain relief and has been found to reduce PTX-induced hyperalgesia by suppressing TRPV4 expression[52]. GJG can also alleviate hypersensitivity
Cell Swelling
Traslocationand activation
of Pla2
aa released
5’, 6’- &
8’, 9’- EET
activation of TrPV4
Hypotonic stimulation
Src Kinaseactivated
Y253 Phosphorylation
Path APath B Cell Swelling
Traslocationand activation
of Pla2
aa released
5’, 6’- &
8’, 9’- EET
activation of TrPV4
Hypotonic stimulation
Src Kinaseactivated
Y253 Phosphorylation
Path APath B
Fig. 5 Alternative pathways for hypotonic stimulation acti-vating TRPV4.Path A with open arrow shows a summary of direct regulation of TRPV4 channel function through tyrosine phosphorylation. Xu et al.[49] concluded that hypotonic stress results in Src family tyrosine kinase-dependent tyrosine phosphorylation of the tonicity sensor TRPV4 at residue Tyr-253 and that this residue is essential for channel function. Path B with close arrow shows that cell swelling activates TRPV4 by means of the PLA(2)-dependent formation of AA, and its subsequent metabolization to 5’,6’-epoxyeicosatrienoic acid by means of a CYP-450 epoxygenase-dependent pathway[32].

80 Hueng-Chuen Fan et al. / Tungs’ Medical Journal 11 (2017) 73-84
to cold sensation induced by oxaliplatin, through the suppression of TRPM8 and TRPA1[53]. These results suggest that TRP channels may play a crucial role in chemotherapy-induced neuropathy.
Inflammatory hyperalgesiaDuring inflammation, injured tissues release
mediators, cytokines, and growth factors to heighten pain sensitivity, and these cause inflammatory hyper-algesia. Examples of common inflammatory media-tors are bradykinin and prostaglandin E2 (PGE2). Bra-dykinin (Fig 6, green triangle) activates Gq-coupled B1 and B2 receptors (Fig 6, gray cylinders) to initiate a cascade of intracellular messengers that sensi-tize target molecules. PGE2 (Fig 6, green oval) acti-vates PGE receptor 1 and PGE receptor 4 (Fig 6, red cylinders), which activate PKC (Gq coupled) and PKA (Gs coupled), respectively. These mediators form a complex network in the transmission of inflamma-tory signals under both physiological and patholog-ical conditions. However, it is important to know how these diverse signals pass to TRPV channels (Fig 6, blue cylinders) and decrease their firing thresholds,
thereby producing hypersensitivity to external stimuli and exacerbating pain.
Integrating the diverse signalsSignaling kinases are often widely distributed
and have broad substrate selectivity. Consequently, it can be unclear how signals interact and cooperate to modulate or activate target proteins. Numerous studies investigating the relationship between inflam-matory mediators and TRP channels have produced inconsistent or even contradictory results. Our poor understanding and the conflicting results may be due to the presence of different signaling pathways. If such pathways frequently and randomly act on a target protein to potentiate or sensitize the channel without control, cells will be unable to maintain their normal function and vitality. Cells must be specialized and equipped with “integrators” to navigate these stimuli and signals to proper destinations, prevent them from diffusing, and ensure a specific response. Subcellular targeting complexes associating with anchoring pro-teins has emerged as an important mechanism by which cells localize signaling molecules to sites where
COOHNH2
Gq/11
AA
PLA
BK
B2R
Lipids NH2
EP
Gs
HPETE
IP3 DAG
PGE2
COX
LOX
C-AMP
COOHAKAP
PKA
TRPV1
PKC
ER Ca2+
PKC
PKAAKAP PKC
TRPV4
PGE2
Gq
PLCβ
COOHNH2
Gq/11
AA
PLA
BK
B2R
Lipids NH2
EP
Gs
HPETE
IP3 DAG
PGE2
COX
LOX
C-AMP
COOHAKAP
PKA
TRPV1
PKC
ER Ca2+
PKC
PKAAKAP PKC
TRPV4
PGE2
Fig. 6 Modulation of the PKC and PKA phosphorylation by AKAP79Several proinflammatory mediators sensitize TRPV1 by PKC and/or PKA phosphorylation. Bradykinin, one of pro-inflammatory mediators, binds to the B2 receptor, which couples with Gq/11. A major target of this complex is PLCβ, which catalyses breakdown of PIP2 into IP3, causing a rise of calcium in the cell, and release of diacylglycerol (DAG), which in turn activates PKC, then targeting TRPV1. Prostaglandin E2 (PGE2) contributes to nociceptor sensitization by binding to PGE receptor subtypes EP1 or EP4. EP1 activates PKC. EP4 raises intracellular cAMP levels and activate cAMP-dependent protein kinase A (PKA), which in turn phosphorylates various proteins, include TRPV1. PKC and PKA are maintained adjacent to TRPV1 in a signalling complex by the scaffolding protein AKAP79. Preventing binding of AKAP 79 to TRPV1 by using a peptide or deleting the AKAP 79 binding sites on TRPV1, ablates the enhancement of TRPV1 channel activation. Over-expression of AKAP 79 enhances the sensitivity of TRPV1 to capsaicin. These suggest the mechanism of AKAP 79 regulating the sensitivity of TRPV1 by binding PKA and PKC so as to control their phosphorylations and activate their target protein. Manipulating this signalling integrator is a promising way for developing analgesics.

81Hueng-Chuen Fan et al. / Tungs’ Medical Journal 11 (2017) 73-84
they can be accessed by specific activators.The AKAP (A kinase anchoring protein) family
of scaffolding proteins were initially named for their targeting of PKA to specific substrates[54]. Later, AKAPs were found to be capable of assembling a wide range of kinases and phosphatases that fine-tune signaling molecules, such as PKC and PKA, and a number of ion channels, such as glutamate recep-tors, M-type potassium channels, and TRP chan-nels[54]. Our work in our lab has shown that PKA and PKC are anchored adjacent to TRPV1 and TRPV4 by AKAP79 (Fig 6, pink hexagon). The binding site of this complex has been identified. Functionally, the sensitizations, activations, and phosphorylations of TRPV1[55] and TRPV4[20] by both PKC and PKA were shown to be enhanced by cotransfection of AKAP79. Thus, the binding of AKAP79 to TRPV1 and TRPV4 may represent a “master switch,” the inhibition of which could be used to abolish hypersensitivity related to the PKA and PKC pathways. Indeed, administration of small interfering RNA (siRNA) AKAP may significantly reduce the sensitization of TRPV1 and TRPV4 by PKA and PKC[20,55].
Disrupting the binding between TRPV4 and AKAP79 inhibits inflammatory hyperalgesia
Heat hyperalgesia has been shown to reduce when TRPV1 was genetically deleted[31]. Tail with-drawal latency, for example, was increased fol-lowing moderately hot temperature exposure in TRPV4 knockout mice[56]. Rats treated by intrathecal ODN-TRPV4 also showed elimination of PTX-induced mechanical hyperalgesia[12], indicating that TRPV1 and TRPV4 could be promising targets for the develop-ment of a novel class of analgesics. However, blocking TRPV1 causes hyperthermia[57]. Moreover, attempts to develop TRPV4 blockers, such as gadolinium, lan-thanum, manganese, ruthenium red, HC-067047, RN-1734, RN-9893, and GSK 205, have largely halted because the agents lack specificity or have too many side effects[7,58]. Another strategy could be to con-struct a peptide that can block inflammatory signals. We originally identified that PKCε played a crucial role in sensitization of the TRPV1 response to painful heat, and that this response could be abolished by using a PKCε inhibitor peptide[59]. However, it is impractical to make an artificial pore on cell membranes to allow delivery of the peptide for an in vivo therapeutic effect.
Conclusion
AKAP79 can orchestrate distinct signaling mol-ecules, such as PKA and PKC, and enhance their phos-phorylation to modulate target proteins, whereas siRNA against AKAP79 can abolish inflammatory hyperalgesia in vitro. This is important because syn-thetic siRNAs hold promise for the creation of new therapeutic drug classes that can silence the target genes of cancers, viral infections, genetic diseases, and neuromuscular diseases[60]. In light of this, the use of siRNA against AKAP79 could be a prom-ising target for the development of a novel class of analgesics.
References
1. IASP. IASP (International Association for the Study of Pain). Pain Terminology. 1994.
2. Caterina MJ, Schumacher MA, Tominaga M, Rosen TA, Levine JD, Julius D. The capsaicin receptor: a heat-acti-vated ion channel in the pain pathway. Nature 1997; 389: 816-824.
3. Cosens DJ, Manning A. Abnormal electroretinogram from a Drosophila mutant. Nature 1969; 224: 285-287.
4. Moiseenkova-Bell VY, Wensel TG. Hot on the trail of TRP channel structure. J Gen Physiol 2009; 133: 239-244.
5. Ramsey IS, Delling M, Clapham DE. An introduction to TRP channels. Annu Rev Physiol 2006; 68: 619-647.
6. Lee H, Caterina MJ. TRPV channels as thermosensory receptors in epithelial cells. Pflugers Arch 2005; 451: 160-167.
7. Montell C, Birnbaumer L, Flockerzi V, et al. A unified nomenclature for the superfamily of TRP cation channels. Mol Cell 2002; 9: 229-231.
8. Baylie RL, Brayden JE. TRPV channels and vascular func-tion. Acta Physiol (Oxf) 2011; 203: 99-116.
9. Deng HX, Klein CJ, Yan J, et al. Scapuloperoneal spinal muscular atrophy and CMT2C are allelic disorders caused by alterations in TRPV4. Nat Genet 2010; 42: 165-169.
10. Lee WH, Choong LY, Mon NN, et al. TRPV4 Regulates Breast Cancer Cell Extravasation, Stiffness and Actin Cortex. Sci Rep 2016; 6: 27903.
11. Tabuchi K, Suzuki M, Mizuno A, Hara A. Hearing impair-ment in TRPV4 knockout mice. Neurosci Lett 2005; 382: 304-308.
12. Alessandri-Haber N, Dina OA, Yeh JJ, Parada CA, Reichling DB, Levine JD. Transient receptor potential vanilloid 4 is essential in chemotherapy-induced neuropathic pain in the rat. J Neurosci 2004; 24: 4444-4452.
13. Strotmann R, Harteneck C, Nunnenmacher K, Schultz G, Plant TD. OTRPC4, a nonselective cation channel that confers sensitivity to extracellular osmolarity. Nat Cell Biol 2000; 2: 695-702.
14. Tian W, Salanova M, Xu H, et al. Renal expression of osmotically responsive cation channel TRPV4 is restricted to water-impermeant nephron segments. Am J Physiol Renal Physiol 2004; 287: F17-F24.

82 Hueng-Chuen Fan et al. / Tungs’ Medical Journal 11 (2017) 73-84
15. Jia Y, Wang X, Varty L, et al. Functional TRPV4 channels are expressed in human airway smooth muscle cells. Am J Physiol Lung Cell Mol Physiol 2004; 287: L272-L278.
16. Inoue R, Jensen LJ, Shi J, et al. Transient receptor potential channels in cardiovascular function and disease. Circ Res 2006; 99: 119-131.
17. Yellen G. The voltage-gated potassium channels and their relatives. Nature 2002; 419: 35-42.
18. Voets T, Talavera K, Owsianik G, Nilius B. Sensing with TRP channels. Nat Chem Biol 2005; 1: 85-92.
19. Nilius B, Vriens J, Prenen J, Droogmans G, Voets T. TRPV4 calcium entry channel: a paradigm for gating diversity. Am J Physiol Cell Physiol 2004; 286: C195-C205.
20. Fan HC, Zhang X, McNaughton PA. Activation of the TRPV4 ion channel is enhanced by phosphorylation. J Biol Chem 2009; 284: 27884-27891.
21. Wegierski T, Lewandrowski U, Muller B, Sickmann A, Walz G. Tyrosine phosphorylation modulates the activity of TRPV4 in response to defined stimuli. J Biol Chem 2009; 284: 2923-2933.
22. Mosavi LK, Minor DL, Jr., Peng ZY. Consensus-derived structural determinants of the ankyrin repeat motif. Proc Natl Acad Sci U S A 2002; 99: 16029-16034.
23. Kohl A, Binz HK, Forrer P, Stumpp MT, Pluckthun A, Grutter MG. Designed to be stable: crystal structure of a consensus ankyrin repeat protein. Proc Natl Acad Sci U S A 2003; 100: 1700-1705.
24. Lishko PV, Procko E, Jin X, Phelps CB, Gaudet R. The ankyrin repeats of TRPV1 bind multiple ligands and modu-late channel sensitivity. Neuron 2007; 54: 905-918.
25. Strotmann R, Schultz G, Plant TD. Ca2+-dependent poten-tiation of the nonselective cation channel TRPV4 is medi-ated by a C-terminal calmodulin binding site. J Biol Chem 2003; 278: 26541-26549.
26. Suzuki M, Hirao A, Mizuno A. Microtubule-associated protein 7 increases the membrane expression of transient receptor potential vanilloid 4 (TRPV4). J Biol Chem 2003; 278: 51448-51453.
27. Peng H, Lewandrowski U, Muller B, Sickmann A, Walz G, Wegierski T. Identification of a Protein Kinase C-depen-dent phosphorylation site involved in sensitization of TRPV4 channel. Biochem Biophys Res Commun 2010; 391: 1721-1725.
28. Xu H, Fu Y, Tian W, Cohen DM. Glycosylation of the osmo-responsive transient receptor potential channel TRPV4 on Asn-651 influences membrane trafficking. Am J Physiol Renal Physiol 2006; 290: F1103-F1109.
29. Xu H, Ramsey IS, Kotecha SA et al. TRPV3 is a calcium-permeable temperature-sensitive cation channel. Nature 2002; 418: 181-186.
30. Voets T, Prenen J, Vriens J et al. Molecular determinants of permeation through the cation channel TRPV4. J Biol Chem 2002; 277: 33704-33710.
31. Davis JB, Gray J, Gunthorpe MJ et al. Vanilloid receptor-1 is essential for inflammatory thermal hyperalgesia. Nature 2000; 405: 183-187.
32. Vriens J, Watanabe H, Janssens A, Droogmans G, Voets T, Nilius B. Cell swelling, heat, and chemical agonists use distinct pathways for the activation of the cation channel TRPV4. Proc Natl Acad Sci U S A 2004; 101: 396-401.
33. Guler AD, Lee H, Iida T, Shimizu I, Tominaga M, Caterina M. Heat-evoked activation of the ion channel, TRPV4. J Neu-rosci 2002; 22: 6408-6414.
34. Watanabe H, Vriens J, Suh SH, Benham CD, Droogmans G,
Nilius B. Heat-evoked activation of TRPV4 channels in a HEK293 cell expression system and in native mouse aorta endothelial cells. J Biol Chem 2002; 277: 47044-47051.
35. Suzuki M, Mizuno A, Kodaira K, Imai M. Impaired pressure sensation in mice lacking TRPV4. J Biol Chem 2003; 278: 22664-22668.
36. Jordt SE, Tominaga M, Julius D. Acid potentiation of the capsaicin receptor determined by a key extracellular site. Proc Natl Acad Sci U S A 2000; 97: 8134-8139.
37. Andrade YN, Fernandes J, Vazquez E et al. TRPV4 channel is involved in the coupling of fluid viscosity changes to epi-thelial ciliary activity. J Cell Biol 2005; 168: 869-874.
38. Lorenzo IM, Liedtke W, Sanderson MJ, Valverde MA. TRPV4 channel participates in receptor-operated calcium entry and ciliary beat frequency regulation in mouse airway epithelial cells. Proc Natl Acad Sci U S A 2008; 105: 12611-12616.
39. Smith PL, Maloney KN, Pothen RG, Clardy J, Clapham DE. Bisandrographolide from Andrographis paniculata activates TRPV4 channels. J Biol Chem 2006; 281: 29897-29904.
40. Blumberg PM. Protein kinase C as the receptor for the phorbol ester tumor promoters: sixth Rhoads memorial award lecture. Cancer Res 1988; 48: 1-8.
41. Bhave G, Hu HJ, Glauner KS et al. Protein kinase C phos-phorylation sensitizes but does not activate the capsaicin receptor transient receptor potential vanilloid 1 (TRPV1). Proc Natl Acad Sci U S A 2003; 100: 12480-12485.
42. Vellani V, Mapplebeck S, Moriondo A, Davis JB, McNaughton PA. Protein kinase C activation potentiates gating of the vanilloid receptor VR1 by capsaicin, protons, heat and anandamide. J Physiol 2001; 534: 813-825.
43. Xu F, Satoh E, Iijima T. Protein kinase C-mediated Ca2+ entry in HEK 293 cells transiently expressing human TRPV4. Br J Pharmacol 2003; 140: 413-421.
44. Becker D, Blase C, Bereiter-Hahn J, Jendrach M. TRPV4 exhibits a functional role in cell-volume regulation. J Cell Sci 2005; 118: 2435-2440.
45. Yang XR, Lin MJ, McIntosh LS, Sham JS. Functional expres-sion of transient receptor potential melastatin- and vanil-loid-related channels in pulmonary arterial and aortic smooth muscle. Am J Physiol Lung Cell Mol Physiol 2006; 290: L1267-L1276.
46. Ferrer-Montiel A, Fernandez-Carvajal A, Planells-Cases R et al. Advances in modulating thermosensory TRP chan-nels. Expert Opin Ther Pat 2012; 22: 999-1017.
47. Birder L, Kullmann FA, Lee H et al. Activation of urothelial transient receptor potential vanilloid 4 by 4alpha-phorbol 12,13-didecanoate contributes to altered bladder reflexes in the rat. J Pharmacol Exp Ther 2007; 323: 227-235.
48. Liedtke W, Choe Y, Marti-Renom MA et al. Vanilloid receptor-related osmotically activated channel (VR-OAC), a candidate vertebrate osmoreceptor. Cell 2000; 103: 525-535.
49. Xu H, Zhao H, Tian W, Yoshida K, Roullet JB, Cohen DM. Regulation of a transient receptor potential (TRP) channel by tyrosine phosphorylation. SRC family kinase-depen-dent tyrosine phosphorylation of TRPV4 on TYR-253 mediates its response to hypotonic stress. J Biol Chem 2003; 278: 11520-11527.
50. Watanabe H, Vriens J, Prenen J, Droogmans G, Voets T, Nilius B. Anandamide and arachidonic acid use epoxyeico-satrienoic acids to activate TRPV4 channels. Nature 2003; 424: 434-438.

83Hueng-Chuen Fan et al. / Tungs’ Medical Journal 11 (2017) 73-84
51. Alessandri-Haber N, Dina OA, Joseph EK, Reichling DB, Levine JD. Interaction of transient receptor potential vanilloid 4, integrin, and SRC tyrosine kinase in mechan-ical hyperalgesia. J Neurosci 2008; 28: 1046-1057.
52. Matsumura K, Watanabe Y, Onoe H, Watanabe Y. Pros-tacyclin receptor in the brain and central terminals of the primary sensory neurons: an autoradiographic study using a stable prostacyclin analogue [3H]iloprost. Neuro-science 1995; 65: 493-503.
53. Kato Y, Tateai Y, Ohkubo M et al. Gosha-jinki-gan reduced oxaliplatin-induced hypersensitivity to cold sensation and its effect would be related to suppression of the expres-sion of TRPM8 and TRPA1 in rats. Anticancer Drugs 2014; 25: 39-43.
54. Smith FD, Langeberg LK, Scott JD. The where’s and when’s of kinase anchoring. Trends Biochem Sci 2006; 31: 316-323.
55. Zhang X, Li L, McNaughton PA. Proinflammatory media-tors modulate the heat-activated ion channel TRPV1 via the scaffolding protein AKAP79/150. Neuron 2008; 59: 450-461.
56. Lee H, Iida T, Mizuno A, Suzuki M, Caterina MJ. Altered thermal selection behavior in mice lacking transient receptor potential vanilloid 4. J Neurosci 2005; 25: 1304-1310.
57. Vay L. The thermo-TRP ion channel family: properties and therapeutic implications. 2012.
58. Everaerts W, Zhen X, Ghosh D et al. Inhibition of the cation channel TRPV4 improves bladder function in mice and rats with cyclophosphamide-induced cystitis. Proc Natl Acad Sci U S A 2010; 107: 19084-19089.
59. Cesare P, Dekker LV, Sardini A, Parker PJ, McNaughton PA. Specific involvement of PKC-epsilon in sensitization of the neuronal response to painful heat. Neuron 1999; 23: 617-624.
60. Lam JK, Chow MY, Zhang Y, Leung SW. siRNA Versus miRNA as Therapeutics for Gene Silencing. Mol Ther Nucleic Acids 2015; 4: e252.

84 Hueng-Chuen Fan et al. / Tungs’ Medical Journal 11 (2017) 73-84
瞬時感受器電位香草酸第四亞型離子通道 (Transient Receptor Potential Vanilloid, 4 Subfamily; TRPV4)
一個多功能的離子通道
范洪春1,2,*, Xuming Zhang2,3, Peter A. McNaughton2,4
1童綜合醫療社團法人童綜合醫院 醫學研究部 兒童醫學部2Department of Pharmacology, University of Cambridge, Cambridge, CB2 1PD, UK
3Rowett Institute of Nutrition and Health & Institute of Medical Sciences; University of Aberdeen, Foresterhill, Aberdeen, UK
4Wolfson Centre for Age-Related Research, King’s College London, Guy’s Campus, London Bridge, London, UK.
受文日期:民國 105年 05月 19日;接受刊載:民國 105年 08月 29日
摘要
瞬時感受器電位香草酸第四亞型離子通道蛋白(Transient Receptor Potential Vanilloid, 4 Subfamily; TRPV4)是可被低張力(hypotonicity)、溫熱(innocuous heat)、或者由佛波酯(phorbol esters)等所活化的多型受體(polymodal receptor)。TRPV4在人體分布廣泛,包括肺、脾臟、腎臟、睪丸、脂肪、耳蝸、皮膚、平滑肌、肝臟、血管內皮、中樞神經系統、以及背根神經元。TRPV4具有多樣的活化物以及廣泛的分布,它亦是發炎性痛覺過敏(in�ammatory hyperalgesia)的痛覺接受器。發炎性痛覺過敏是發炎組織內發炎的媒介物(in�ammatory mediators)的作用所致。當組織受損後,發炎的媒介物可以活化蛋白激酶 C(protein kinase C; PKC)和蛋白激酶 A(protein kinase A; PKA)。此兩種激酶在發炎性痛覺過敏(in�ammatory hyperalgesia)的過程中扮演關鍵性角色,因為此兩種激酶會磷酸化 TRPV1和 TRPV4,進而增加這些通道的敏感性,導致發炎性痛覺過敏的疼痛。雖然許多藥廠想要藉著發展 TRPV4的阻斷劑來治療疼痛,但因為阻斷劑的不精確性以及嚴重的副作用抑止了 TRPV4的阻斷劑的研發。由於 A型激酶錨定蛋白(A-kinase anchoring protein 79,AKAP79)可以整合像 PKC和 PKA等的訊息分子,透過增強磷酸化去調節目標蛋白,以小干擾核糖核酸(small interfering ribonucleic acid; siRNA)可抑制發炎性痛覺過敏。用小干擾核糖核酸抑制 AKAP79將是未來深具潛力的止痛藥。
關鍵詞:瞬時感受器電位離子通道蛋白、瞬時感受器電位香草酸第四亞型離子通道、蛋白蛋白激酶 C、蛋白激酶 A、小干擾核糖核酸、A型激酶錨定蛋白 79
* 通訊作者:范洪春 童綜合醫療社團法人童綜合醫院 醫學研究部 部主任 兒童醫學部 主治醫師 43503臺中市梧棲區臺灣大道 8段 699號

85
Risk Factors for Methicillin-Resistant Staphylococcus Aureus in Two Regional Hospitals
Wang-Feng Shen1, Ya-Hua Liang2, Ming-Tsung Lee3, Mei-Pei Ling4, Yi-Ming Kuo5, Yu-Ying Yang2,*
1Department of Emergency, 2Department of Laboratory, 3Research Assistant Center, Show Chwan Memorial Hospital 4Management Center, 5Foreign Business and Development Department, Show Chwan Health Care System
Received: May. 17, 2016; Accepted: Oct. 18, 2016
Abstract
Background: Drug resistance has become a critical issue in public health. Methicillin-resistant Staphylococcus aureus (MRSA), in particular, is one of the most significant infectious pathogens in hospitals. Healthcare staff can sometimes become carriers of MRSA, which can spread to and infect patients. MRSA is difficult to control if a hospital outbreak, or even a cluster outbreak, occurs.Methods: This study used a retrospective chart review to collect a total of 473 cases, 228 MRSA and 245 methicillin-sensitive Staphylococcus aureus (MSSA) cases, from two regional hospitals in central Taiwan during 2012–2013. The patients’ demographic data and information on potential risk factors for MRSA/MSSA were collected and compared to discriminate the factors associated with the highest risk.Results: After controlling for other factors, the results showed that significant risk factors for MRSA were a hospital stay of more than 30 days (OR 2.56, 95% CI 1.31–5.01, diabetes (OR 1.69, 95% CI 1.00–2.83), pneumonia during the previous year (OR 3.56, 95% CI 1.24–9.65), surgery during the previous year (OR 4.68, 95% CI 2.11–10.34), and catheterization with one tube (OR 2.19, 95% CI 1.19–4.03) or two tubes (OR 3.94, 95% CI 1.64–9.51). In addition, plural specimens (OR 6.41, 95% CI 1.30–31.57) and cultures taking more than 3 days (OR 2.41, 95% CI 1.34–4.34) were associated with MRSA.Conclusion: Patients at high risk of MRSA should be detected as early as possible, and MRSA awareness education for healthcare staff should be enhanced in order to reduce the spread of MRSA infection in hospitals and the incidence of cluster outbreaks.
Key words: Methicillin-resistant Staphylococcus aureus (MRSA); methicillin-sensitive Staphylococcus aureus (MSSA); risk factor
Introduction
Drug resistance has become a critical issue in public health. Methicillin-resistant Staphylococcus aureus (MRSA), in particular, is one of the most signif-icant infectious pathogens in hospitals. MRSA, which refers to Staphylococcus aureus bacteria that are resis-tant to methicillin, oxacillin, or nafcillin, usually exists in patients’ blood and/or other excreted body fluids.
Instruments and other articles can then become contaminated through hand contact by healthcare workers and spread among patients, causing infec-tions. MRSA is difficult to control once it leads to a hospital outbreak or a cluster outbreak[1,2].
Patients’ demographic and clinical characteris-tics have different impacts on the MRSA infection[3-5]. Empirical data are needed to help identify high-risk patients and prevent the spread of MRSA infec-tion. Greater understanding of the risk factors could provide a reference for the assessment of healthcare-associated infections in hospitals, as well as help to enhance awareness education for healthcare staff
Tungs’ Medical Journal 11 (2017) 85-94
Original Article
* Correspondence to: Yu-Ying Yang, Director of Department of Laboratory, Show Chwan Memorial Hospital, Changhua. No. 542, Sec. 1, Chung-Shan Rd., Changhua, 500, Taiwan (R.O.C.)

86 Wang-Feng Shen et al. / Tungs’ Medical Journal 11 (2017) 85-94
and provide on-the-job education regarding admis-sion assessment, spread pathway, and the infection prognosis of high-risk patients with MRSA, in order to reduce its spread and the incidence of cluster outbreak[6,7].
The aim of this study was to investigate the risk factors for MRSA by empirically examining the data from two regional hospitals in central Taiwan. We chose patients with methicillin-sensitive Staphylo-coccus aureus (MSSA) infections as the comparison group to study the hypothesis that factors that dif-fered significantly between the two groups would be the risk factors for MRSA. Demographic characteris-tics were compared between groups of patients with MRSA and MSSA, and the risk factors for MRSA and MSSA were evaluated.
Methods
Research SubjectsIn this retrospective study, we included all MRSA
or MSSA cases from January 2012 to December 2013 detected by bacterial culture during hospitalization in general wards, the intensive care unit (ICU), and the emergency room (ER) at two regional teaching hospi-tals in Changhua, Taiwan.
Study DesignThe patients’ chart included information about
MRSA and MSSA cultured from all inpatients in general wards, the ICU, and the ER during the study period. The first steps of the research process were to search the reports of bacterial cultures of MRSA and MSSA in the laboratory reporting system and then to collect patient demographics from electronic medical records. To record the data for each patient consis-tently, we designed a custom Staphylococcus aureus record sheet (SARS) on which potential risk factors obtained from a literature review were listed. Case data were then collected and recorded on SARSs for analysis of the relevant risk factors of MRSA. Patients’ demographic data and information on the potential risk factors were collected and compared between patients with MRSA and those with MSSA, hypoth-esizing that the factors that differed significantly would be the high risk factors for MRSA.
Data CollectionData were collected from patients’ electronic
medical records and recorded on SARSs. The informa-tion collected included the following:(A) Basic information: medical record number, year,
sex, age, hospital district, wards, divisions.(B) Admission information: length of stay and dis-
charge options. Length of stay indicates the period of hospitalization from admission to discharge (including transfer in, transfer out, against-advice discharge, and death).
(C) Disease history: cancer, diabetes, hemodialysis, immune disorders, pneumonia within the past year, cellulitis within the past year, surgery in the past year, readmission within 30 days after dis-charge, and previous MRSA infection.
(D) Medication history for the previous year: antibi-otics, steroids, and immunosuppressants.
(E) Invasive catheterization: nasogastric tubes, cath-eters, endotracheal tubes, tracheostomy, and the number of tubes used (zero, one, two, or three).
(F) The specimen source and days to issue reports: culture sites include blood, deep pus, ascites, bile, pleural fluid, cerebrospinal fluid, and joint fluid.
(G) Laboratory reports: white blood cell count (WBC) and C-reactive protein level (CRP).
Data AnalysisDescriptive statistics such as the number of
cases and percentages were used to describe the distribution of categorical data, whereas mean, stan-dard deviation, and range were used to describe continuous data. The chi-square test and t-test were used to analyze the relationships between two vari-ables. Analysis of the relevant factors related to MRSA and MSSA was performed using logistic regres-sion analysis and calculating odds ratios (ORs) with 95% confidence intervals (CIs) to estimate the risks of relevant factors, both in univariate and multivariate analyses. A p value < 0.05 was considered statistically significant.
Results
Demographic CharacteristicsIn total, 473 cases were included, including 228
cases in the MRSA group and 245 in the MSSA group. Table 1 presents the demographic characteristics of all the subjects. Individuals from A hospital comprised 54.1% of the research subjects, with the remaining 45.9% coming from B hospital. A significantly larger

87Wang-Feng Shen et al. / Tungs’ Medical Journal 11 (2017) 85-94
Table 1. Basic information of the research subjects.
MRSA (N=228) MSSA (N=245) Total (N=473) X2 p
Hospital 15.911 .000
A hospital 145 111 256
63.6% 45.3% 54.1%
B hospital 83 134 217
36.4% 54.7% 45.9%
Year
2012 135 121 256 4.202 .040
59.2% 49.4% 54.1%
2013 93 124 217
40.8% 50.6% 45.9%
Ward
General wards 131 175 306 9.492 .002
57.5% 71.4% 64.7%
ICU & ER 97 70 167
42.5% 28.6% 35.3%
Gender
Male 133 161 294 2.620 .106
58.3% 66.0% 62.3%
Female 95 83 178
41.7% 34.0% 37.7%
Age
<=40 y/o 23 42 65 8.719 .013
10.1% 17.1% 13.7%
41-64 y/o 63 81 144
27.6% 33.1% 30.4%
>=65 y/o 142 122 264
62.3% 49.8% 55.8%
Division
Medicine 138 138 276 .629 .428
61.1% 57.0% 59.0%
Surgery 88 104 192
38.9% 43.0% 41.0%
Length of stay
<=10 days 66 121 187 32.893 .000
29.6% 49.4% 40.0%
11-30 days 88 96 184
39.5% 39.2% 39.3%
>=31 days 69 28 97
30.9% 11.4% 20.7%
Discharge options
Routine 206 235 441 12.383a .001
90.4% 95.9% 93.2%
AAD 19 4 23
8.3% 1.6% 4.9%
Death 3 6 9
1.3% 2.4% 1.9%a Fisher’s Exact Test

88 Wang-Feng Shen et al. / Tungs’ Medical Journal 11 (2017) 85-94
proportion of the MRSA data was collected from A hospital (p < .001). Significantly more of the MRSA cases (59.2%) occurred in 2012 (p = .04). Chi-square tests showed no significant differences between the MRSA and MSSA groups in sex and divisions (p = .106 and .428, respectively); however, there were
significant differences between the groups in ward (p = .002), age (p = .013), length of stay (p < .001), and discharge options (p = .001) (p=.003).
Clinical CharacteristicsTable 2 shows the clinical differences between
Table 2. Clinical information of the research subjects.
MRSA (N=228) MSSA (N=245) Total (N=473) X2 p
Cancer 22 16 38 .917 .338
9.6% 6.8% 8.2%
Diabetes 100 59 159 17.484 .000
43.9% 25.0% 34.3%
Hemodialysis 33 28 61 .482 .488
14.5% 11.9% 13.1%
Autoimmune Disease 10 9 19 .006 .939
4.4% 3.8% 4.1%
Pneumonia in 1 year 32 8 40 15.466 .000
14.0% 3.4% 8.6%
Cellulitis 3 7 10 -a .339
1.3% 3.0% 2.2%
Surgery in 1 year 49 11 60 27.699 .000
21.5% 4.7% 12.9%
Readmission in 30 days 42 26 68 5.233 .022
18.4% 10.6% 14.4%
Previous MASA Infection 26 13 39 5.026 .025
11.4% 5.3% 8.2%
Antibiotics 201 154 355 15.337 .000
88.2% 73.0% 80.9%
Steroid 44 24 68 4.668 .031
19.3% 11.4% 15.5%
Immunosuppressive drug 4 1 5 —a .374
1.8% .5% 1.1%
WBC 1.310 .252
<=10000/uL 70 89 159
32.9% 38.5% 35.8%
>10000/uL 143 142 285
67.1% 61.5% 64.2%
CRP 1.330 .249
<=1.0 mg/dL 16 26 42
8.1% 12.0% 10.1%
>1.0 mg/dL 182 191 373
91.9% 88.0% 89.9%
Culture days 16.847 .000
1-3 days 85 138 223
37.4% 56.8% 47.4%
4-6 days 142 105 247
62.6% 43.2% 52.6%aFisher’s Exact Test

89Wang-Feng Shen et al. / Tungs’ Medical Journal 11 (2017) 85-94
the two groups in disease history and drug history. There were significant differences in diabetes (p < .001), pneumonia within the previous year (p < .001), surgery within the previous year (p < .001), readmis-sion within 30 days after discharge (p = .022), pre-vious MRSA infection (p = .025), the use of antibiotics within the previous year (p < .001), the use of ste-roids within the previous year (p = .031), and bacterial culture days (p < .001).
Risk Factors by Univariate Logistic Regression AnalysisTable 3 shows the results of univariate logistic
regression analysis of the demographic data to
evaluate potential risk factors. Significant demo-graphic risk factors for MRSA included admission to ICU or ER (OR 1.85, 95% CI 1.26–2.71), being older than 64 years (OR 2.13, 95% CI 1.21–3.73), a hospital stay of more than 30 days (OR 4.52, 95% CI 2.65–7.69), and against-advice discharge (OR 5.42, 95% CI 1.81–16.19). A significant protective factor against MRSA was being admitted to B hospital (OR 0.47, 95% CI 0.33–0.69). In addition, the risk of MRSA was lower in 2013 than in 2012 (OR 0.67, 95% CI 0.47–0.97). Sex and division were not significant predictors of MRSA.
Table 4 shows the results of univariate logistic regression analysis of the clinical data to evaluate potential risk factors. Significant risk factors for MRSA were diabetes (OR 2.34, 95% CI 1.58–3.48), pneumonia in the previous year (OR 4.67, 95% CI 2.10–10.38), surgery in the previous year (OR 5.60, 95% CI 2.83–11.08), readmission within 30 days (OR 1.90, 95% CI 1.12–3.22), previous MRSA infection (OR 2.30, 95% CI 1.15-4.59), the use of antibiotics in the previous year (OR 2.76, 95% CI 1.67–4.56), the use of steroids in the previous year (OR 1.86, 95% CI 1.09–3.19), and catheterization with one tube (OR 2.88, 95% CI 1.76–4.71) or two tubes (OR 4.76, 95% CI 2.40–9.47). In addition, MRSA was more likely when a pleural specimen was analyzed (OR 3.58, 95% CI 1.16–11.03), or the culture day took than 3 days (OR 2.20, 95% CI 1.52–3.18), and was less likely when the specimen was taken from deep pus (OR 0.51, 95% CI 0.33–0.79). Other factors including cancer, hemodial-ysis, autoimmune disease, cellulitis, immunosuppres-sive drug use, elevated WBC, and elevated CRP were not significant predictors.
Risk Factors by Multivariate Logistic Regression Analysis
The significant variables from the previous uni-variate analyses were then included in multivariate logistic regression analysis (Table 5). After control-ling for other factors, the results showed that the sig-nificant risk factors for MRSA were a hospital stay of more than 30 days (OR 2.56, 95% CI 1.31–5.01), dia-betes (OR 1.69, 95% CI 1.00–2.83), pneumonia in the previous year (OR 3.56, 95% CI 1.24–9.65), surgery in the previous year (OR 4.69, 95% CI 2.11–10.34), and catheterization with one tube (OR 2.19, 95% CI 1.19–4.03) or two tubes (OR 3.94, 95% CI 1.64–9.51). In addition, MRSA was more likely when a pleural specimen was taken (OR 6.41, 95% CI 1.30–31.57), or
Table 3. Comparison of the risks for MRSA on the demo-graphic factors by univariate logistic regression.
p OR95% C.I. for OR
Lower Upper
Hospital
A hospitala
B hospital .000 .474 .328 .686
Year
2012a
2013 .032 .672 .467 .967
Ward
General wardsa
ICU & ER .002 1.851 1.264 2.712
Gender
Malea
Female .087 1.386 .954 2.013
Age
<=40 y/oa
41-64 y/o .256 1.420 .775 2.603
>=65 y/o .009 2.125 1.210 3.732
Division
Medicinea
Surgery .375 .846 .585 1.224
Length of stay
<=10 daysa .
11-30 days .015 1.681 1.108 2.549
>=31 days .000 4.518 2.654 7.689
Discharge options
Routinea .
AAD .002 5.419 1.814 16.186
Death .431 .570 .141 2.310aReference category

90 Wang-Feng Shen et al. / Tungs’ Medical Journal 11 (2017) 85-94
the culture took more than 3 days (OR 2.41, 95% CI 1.34–4.34), and was less likely in the year 2013 (OR 0.34, 95% CI 0.20–0.59). Other variables showed no significant relationships with MRSA infection.
Discussion
This study analyzed a total of 473 cases for
which MRSA and MSSA infections had been detected by bacterial culture during hospitalization in 2012 and 2013. There were significantly more MRSA cases in 2012. After controlling for other factors, significant risk factors for MRSA were a hospital stay of more than 30 days, having diabetes, suffering pneumonia in the previous year, undergoing surgery in the pre-vious year, or undergoing catheterization. Pleural
Table 4. Comparison of the risks for MRSA on the clinical factors by univariate logistic regression.
p OR95% C.I. for OR
Lower Upper
Disease History
Cancer .262 1.468 .750 2.874
Diabetes .000 2.344 1.581 3.476
Hemodialysis .406 1.257 .732 2.158
Autoimmune Disease .756 1.157 .461 2.902
Pneumonia in 1 year .000 4.673 2.104 10.379
Cellulitis .234 .436 .111 1.708
Surgery in 1 year .000 5.599 2.829 11.083
Readmission in 30 days .017 1.902 1.123 3.221
Previous MASA Infection .018 2.297 1.150 4.589
Drugs
Antibiotics .000 2.755 1.665 4.560
Steroid .023 1.863 1.089 3.189
Immunosuppressive drug .239 3.750 .416 33.823
Tubing
No Tubea
1 Tube .000 2.876 1.757 4.707
2 Tubes .000 4.759 2.393 9.465
3 Tubes .456 1.393 .583 3.326
Specimen
Blooda
Deep pus .002 .507 .327 .786
Ascites .234 3.815 .421 34.536
Bile .156 4.768 .550 41.310
Pleural .027 3.576 1.159 11.030
CSF .365 2.861 .294 27.821
Joint .121 .477 .187 1.215
Culture days
1-3 daysa
4-6 days .000 2.196 1.517 3.178
WBC
<=10000/uLa
>10000/uL .214 1.280 .867 1.891
CRP
<=1.0 mg/dLa
>1.0 mg/dL .191 1.548 .804 2.981aReference category

91Wang-Feng Shen et al. / Tungs’ Medical Journal 11 (2017) 85-94
Table 5. Comparison of the risks for MRSA by multivariate logistic regression.
p OR95% C.I. for OR
Lower Upper
Hospital
A hospitala
B hospital .141 .588 .289 1.193
Year
2012a
2013 .000 .342 .199 .586
Ward
General wardsa
ICU & ER .556 1.186 .673 2.091
Age
<=40 y/oa
41-64 y/o .402 .714 .325 1.569
>=65 y/o .651 .836 .385 1.815
Length of stay
<=10 daysa
11-30 days .247 1.369 .804 2.331
>=31 days .006 2.557 1.306 5.005
Discharge options
Routinea
AAD .142 2.924 .699 12.232
Death .406 .446 .066 3.002
History
Diabetes .048 1.686 1.004 2.832
Pneumonia in 1 year .017 3.465 1.244 9.651
Sugery in 1 year .000 4.675 2.114 10.340
Readmission in 30 days .180 1.603 .804 3.197
Previous MASA Infection .279 1.673 .659 4.247
Antibiotics .895 .951 .453 1.997
Steroid .981 .991 .464 2.115
Tubing
No Tubea
1 Tube .012 2.190 1.190 4.029
2 Tubes .002 3.942 1.635 9.506
3 Tubes .357 .558 .161 1.931
Specimen
Blooda
Deep pus .226 1.603 .747 3.438
Ascites .097 14.008 .621 315.954
Bile .078 8.423 .788 90.058
Pleural .022 6.409 1.301 31.566
CSF .380 3.491 .214 57.028
Joint .581 1.422 .407 4.967
Culture days
1-3 daysa
4-6 days .003 2.411 1.340 4.339aReference category

92 Wang-Feng Shen et al. / Tungs’ Medical Journal 11 (2017) 85-94
specimens and cultures taking more than 3 days were also significantly associated with MRSA.
Staphylococcus aureus infection has become an important issue in health care, with drug-resis-tant Staphylococcus aureus a particular challenge for hospitals. In general, the incidence of MRSA in Asia is higher than in western countries. In Taiwan, the prevalence of MRSA increased from 16.3% in 1993 to 82% in 1998[8]. The main pathogens for distributing MRSA are the contaminated blood, body fluids, and excretion of patients, with the pathogens transferred from MRSA-infected patients to others via the hands of health care staff. Thus, the hands of medical staff have played a vital role in the delivery of the infec-tion. Infection with MRSA results in many diseases, such as bacteriuria, urinary tract infections, pneu-monia, myelitis, skin infection, sepsis, and endocar-ditis. These diseases resulted in patients experiencing a prolonged length of hospital stay, increasing the costs of medical care. The problem of drug resistance has resulted in the failure of antibiotic therapy, and in an increase in mortality. All of these issues have serious impacts on patient safety[9-11].
MRSA is a common cause of healthcare-associ-ated infections and is hard to control once an endemic outbreak occurs. A cluster infection in a hospital may have serious consequences. MRSA infection is an important hazard to the safety of patients receiving treatment in a hospital. The prevention of MRSA infections in hospitals needs the attention and collab-oration of the public and health care workers[1,2,12].
This study retrospectively collected empirical clinical data regarding MRSA and MSSA and analyzed the factors that influenced infection with MRSA. It is hoped that the results will be valuable references for infection control and prevention in hospital. There is still much that should be done for this issue. MRSA carriers can transmit to uncontaminated people due to the incompleteness of protective measures, which will increase the possibility of the spread of the disease. In an ICU, the severity of disease and the use of invasive catheterization are liable to result in MRSA colonization. The awareness of health care staff about MRSA infection should be increased and edu-cation provided. High-risk patients should be evalu-ated at admission. Continued medical education on the transmission route and prognosis of the infection should be enhanced to reduce dispense and cluster outbreaks of MRSA infection.
Our findings were consistent with those from other studies. One report noted that Taiwan’s prev-alence of MRSA are higher than other countries[13]. Studies have revealed that important risk factors for MRSA infection include medical history, being transferred from a long-term care facility, hemodi-alysis, MRSA colonization during the previous year, and readmission within 30 days[6,7]. Another study indicated other possible risk factors, including being transferred from ICU, undergoing a cardiac operation, admission to the neurosurgery ward, being trans-ferred from a nursing home or other institution, and being in a rehabilitation ward[14]. In addition, many studies have identified that having an open wound, undergoing an invasive procedure, being older than 65 years, pressure sores, having diabetes, operation history, and length of hospital stay were important factors related to MRSA colonization[3-5].
Another study, which observed a 15-year increasing trend of MRSA bacteremia, reported that length of hospital stay, age, malignant tumor, use of a respirator, and invasive catheterization were signifi-cant risk factors for MRSA infections, increasing mor-tality from MRSA to 1.78 times higher than that from MSSA[13]. A retrospective cohort study employed active screening of high-risk patients together with measures on contact prevention to control the spread of MRSA in a hospital. Even with the mea-sures adopted, the study found that a length of stay of more than 7 days, disease severity, the use of anti-biotics, the use of a respirator, and invasive cathe-terization were risk factors closely related to MRSA colonization[15].
This study had several limitations. We used a ret-rospective chart review of electronic medical records to collect data. The accuracy of the data largely depended on the completeness of the electronic medical records, but some information relevant to the risk factors of MRSA were not recorded in these records. This limited the scope of our analysis and interpretation. Furthermore, there are variables not included in this study that could potentially influence the results of the analysis. For example, we did not consider whether the MRSA was hospital-associated or community-associated, which limited the possi-bility of discriminating risk factors between these two types of MRSA. In addition, this study retrospectively collected inpatient data from general wards, the ICU, and the ER. The locations of our hospital and the

93Wang-Feng Shen et al. / Tungs’ Medical Journal 11 (2017) 85-94
specialties of the physicians may in part have affected the composition of patients who came to our hospital. There were obviously fewer children than patients in other age groups, which was the reason we catego-rized patients under 40 years to be a single age group in the data analysis. As a result, we were not able to provide evidence to support that children are highly susceptible to MRSA, which is another limitation of our study.
Conclusion
This study identified a number of risk factors for MRSA. It is suggested that risk factors such as these should be used to identify high-risk patients early, to help avoid outbreaks of MRSA in hospitals. In addi-tion, education and training should be provided to healthcare staff to increase awareness. Further studies on environmental MRSA screening and the development of clinical guidelines are needed.
References
1. Huang, S.S., et al., Impact of Routine Intensive Care Unit Surveillance Cultures and Resultant Barrier Precautions on Hospital-Wide Methicillin-Resistant Staphylococcus aureus Bacteremia. Clinical Infectious Diseases, 2006. 43(8): p. 971-978.
2. McGinigle, K.L., M.L. Gourlay, and I.B. Buchanan, The Use of Active Surveillance Cultures in Adult Intensive Care Units to Reduce Methicillin-Resistant Staphylococcus aureus-Related Morbidity, Mortality, and Costs: A System-atic Review. Clinical Infectious Diseases, 2008. 46(11): p. 1717-1725.
3. Lucet, J., et al., Prevalence and risk factors for carriage of methicillin-resistant staphylococcus aureus at admission to the intensive care unit: Results of a multicenter study. Archives of Internal Medicine, 2003. 163(2): p. 181-188.
4. Tomic, V., et al., COmprehensive strategy to prevent nos-ocomial spread of methicillin-resistant staphylococcus aureus in a highly endemic setting. Archives of Internal Medicine, 2004. 164(18): p. 2038-2043.
5. Wernitz, M.H., et al., Effectiveness of a hospital-wide selective screening programme for methicillin-resistant Staphylococcus aureus (MRSA) carriers at hospital admis-sion to prevent hospital-acquired MRSA infections. Clinical Microbiology and Infection, 2005. 11(6): p. 457-465.
6. Shitrit, P., et al., Active surveillance for methicillin-resistant Staphylococcus aureus (MRSA) decreases the incidence of MRSA bacteremia. Infection Control, 2006. 27(10): p. 1004-1008.
7. West, T.E., et al., Effect of targeted surveillance for control of methicillin-resistant Staphylococcus aureus in a com-munity hospital system. Infection Control, 2006. 27(03): p. 233-238.
8. Ho, M., et al., Surveillance of antibiotic resistance in Taiwan, 1998. Journal of microbiology, immunology, and infection= Wei mian yu gan ran za zhi, 1999. 32(4): p. 239-249.
9. Banning, M., Transmission and epidemiology of MRSA: current perspectives. British Journal of Nursing, 2005. 14(10): p. 548-554.
10. Klevens, R., et al., INvasive methicillin-resistant staphylo-coccus aureus infections in the united states. JAMA, 2007. 298(15): p. 1763-1771.
11. Weber, C.J., Update on methicillin-resistant Staphylo-coccus aureus (MRSA). Urologic nursing, 2008. 28(2): p. 143.
12. Lucet, J.-C., et al., Successful long-term program for con-trolling methicillin-resistant Staphylococcus aureus in intensive care units. Intensive Care Medicine, 2005. 31(8): p. 1051-1057.
13. Wang, F.-D., et al., Risk factors and mortality in patients with nosocomial Staphylococcus aureus bacteremia. American Journal of Infection Control, 2008. 36(2): p. 118-122.
14. Pan, A., et al., Trends in methicillin-resistant Staphylo-coccus aureus (MRSA) bloodstream infections: effect of the MRSA “search and isolate” strategy in a hospital in Italy with hyperendemic MRSA. Infection Control & Hos-pital Epidemiology, 2005. 26(02): p. 127-133.
15. Patel, M., et al., Active surveillance to determine the impact of methicillin-resistant Staphylococcus aureus col-onization on patients in intensive care units of a Veterans Affairs Medical Center. Infection Control & Hospital Epide-miology, 2008. 29(06): p. 503-509.

94 Wang-Feng Shen et al. / Tungs’ Medical Journal 11 (2017) 85-94
抗藥性金黃色葡萄球菌感染之危險因子探討
沈萬豐1 梁雅畫2 李銘宗3 凌美貝4 郭依明5 楊玉英2,*
秀傳紀念醫院 1急診醫學部 2檢驗科 3研究輔導中心秀傳醫療體系 4營運中心 5國外事業發展組
受文日期:民國 105年 05月 17日;接受刊載:民國 105年 10月 18日
摘要
背景:抗藥性是公衛重要議題,抗藥性金黃色葡萄球菌(MRSA)感染是院內感染重要因素。醫護人員會成為MRSA帶原者且傳染給病患。如院內大流行或群聚感染則難以控制。方法:本研究採病例回溯研究,收集 473名病患資料,其中 228位MRSA,245位非抗藥性金黃色葡萄球菌(MSSA)感染病患,2012至 2013年兩家區域醫院之病歷資料,包括人口學資料及臨床潛在危險因子。比較MRSA與MSSA之危險因子,作為預防方法依據。結果:多變項分析顯示MRSA之危險因子:住院超過 30天(OR 2.56, 95% CI 1.31-5.01)、糖尿病(OR 1.69, 95% CI 1.00-2.83)、一年內肺炎(OR 3.56, 95% CI 1.24-9.65)、一年內手術(OR 4.68, 95% CI 2.11-10.34)、一條管路(OR 2.19, 95% CI 1.19-4.03)及兩條管路(OR 3.94, 95% CI 1.64-9.51)、腹膜檢體(OR 6.41, 95% CI 1.30-31.57)及培養超過 3天(OR 2.41, 95% CI 1.34-4.34)。結論:MRSA高危險群須儘早檢測,加強醫護感控教育以降低傳播。
關鍵詞:抗藥性金黃色葡萄球菌、非抗藥性金黃色葡萄球菌、危險因子
*通訊作者:楊玉英檢驗科主任 秀傳紀念醫院檢驗科主任 彰化縣彰化市中山路一段 542號

95
Portfolio Assessment for a Postgraduate Year One Residency Training Program: A Rasch Analysis
Chin-Yi Huang1,†, Ming-Tsung Lee2,†, Jhin-Long Jiang1, Yi-Cheng Liao1,*, Lon-Yen Tsao3
1Department of Medical Education, Changhua Christian Hospital, Changhua, Taiwan2Research Assistant Center, Show Chwan Memorial Hospital, Changhua, Taiwan
3Department of Pediatrics, Changhua Christian Hospital, Changhua, Taiwan
Received: Jun. 20, 2016; Accepted: Oct. 18, 2016
Abstract
Background and purpose: In clinical practice, portfolio assessment is becoming more acceptable as both a learning and assessment tool. However, the validity and reliability of the application of portfolio assessment to personal development and reflection for postgraduate year one (PGY1) residency training in Taiwan have been evaluated in very few studies. Therefore, this study aimed to develop a valid scoring rubric and examine its validity and reliability using the Rasch model.Methods: A scoring rubric with clear criteria was developed for the portfolio assessment procedure. Five assessment items were included in the rubric to evaluate competences. The Rasch model was used to determine the validity and reliability of the rubric. Infit and outfit mean square statistics (MNSQ) were used to identify misfit items and subjects. Person reliability was used to analyze the response patterns of the subjects.Results: Fifty-one residents who participated in the PGY1 residency training program during the 2012–2013 academic year participated in the study. The infit MNSQ ranged from 0.73 to 1.19, and the outfit MNSQ ranged from 0.72 to 1.20. The estimated test reliability and person separation indices were 0.89 and 2.88, respectively.Conclusion: The rubric provided the learners with much clearer criteria for assessment. All developed items fitted the Rasch model well, confirming desirable validity and reliability of the evaluation rubric.
Key words: Evaluation; Medical Education; Medical Residency; Training Programs; Rasch Model
Introduction
In recent years, experts in medical education have been developing new methodologies and cur-ricula emphasizing outcome-based education[1-4]. Simultaneously, assessment strategies have been rapidly developed to keep pace with the innova-tions in education[5], and it was noted that proficient assessment tools would be capable of both evaluating performance and enhancing the learning process[5,6]. Portfolio assessment appears to be a solution to such a demand[7]. A portfolio is a collection of papers and
other forms of evidence that represents students’ progress toward the achievement of the curriculum over time, and it charts students’ progress toward the expected standard for each learning outcome[2,6,8-10]. According to the Accreditation Council for Graduate Medical Education (ACGME) Tool Box for Assessment, portfolio assessment is a powerful tool suitable for formative or summative assessment that differs from general quantitative assessment tools. Thus, a port-folio is a useful tool for assessing performance and enhancing learning[11].
However, judging the quality of portfolios is a critical issue[7]. Reliability is a common problem for raters when they retrospectively judge the perfor-mance of the residents in ACGME competency areas. One study systematically reviewed prior research and suggested that the average reliability across six
Tungs’ Medical Journal 11 (2017) 95-101
Original Article
* Correspondence to: Dr. Yi-Cheng Liao, Department of Medical Education, Changhua Christian Hospital, No. 135 Nanxiao Street, Changhua City, Changhua County, 500, Taiwan (R.O.C.)
† Chin-Yi Huang and Ming-Tsung Lee contributed equally to this work.

96 Chin-Yi Huang et al. / Tungs’ Medical Journal 11 (2017) 95-101
studies was 0.63, which indicated that only a fair inter-rater reliability could be achieved by individual assessors grading the same portfolio[12]. Additionally, available coding systems for analyzing portfolios are limited. These limitations restrict the ability to dis-criminate the extents and levels of portfolio content.
A scoring rubric is a more objective method to solve this problem. Precise criteria are adopted by this uniform method to rate the performance of the learners. Recent studies reported that scoring rubrics have been applied to postgraduate resi-dents to evaluate their reflective abilities and perfor-mances; however, the strengths of these tools were restricted by undesirable reliabilities[13,14]. Learman and coworkers[13] developed a scoring schema for reflection, but the internal consistency reliability was low (Cronbach’s α = 0.4). The quality of the assess-ment tool by Webb and Merkley [14] was restrained by suboptimal inter-rater reliability (inter-rater reli-ability = 0.63).
Although the reliability of an instrument is most commonly represented by Cronbach’s α, it can be increased by adding items or including more rating scale categories. Applications of Rasch models in medical research have been reported in the scientific literature [15,16]. Rasch models are superior for trans-forming ordinal measures into interval measures, identifying items with poor functionality, and gener-alizing results across samples and items. Therefore, we conducted this study to standardize the scoring rubric measures via Rasch model analysis.
In Taiwan, a postgraduate year one (PGY1) residency training program is completed prior to the usual resident training. Both training programs are required by health administration authorities. However, the application of a portfolio scoring rubric to the personal performance development and core competence reflection for PGY1 training was of concern as it has not been previously studied. There-fore, the aim of the present study was to develop an ideal tool that was simple and concise and that could be used by multiple assessors. In this study, a rubric for portfolio assessment was developed. Further-more, to examine the validity and reliability of the scoring rubric, Rasch model analysis was used. The developed rubric is expected to add new information to our existing resident evaluation profile.
Methods
SettingThe participants of this cross-sectional study
were 51 residents trained in the PGY1 residency training program of a teaching hospital in central Taiwan during the 2012–2013 academic year. At the beginning of the training program, the residents received a structured portfolio booklet and port-folio assessment scoring rubric. The portfolio booklet mainly aimed to support the learning process of the residents, and the scoring rubric was designed to set clear expectations for the portfolio. Moreover, other key aims of the scoring rubric were to broaden the scope of the expected competences and assist the learners in selecting appropriate material for inclusion in the portfolio. In addition, the rubric was created to provide an objective, feasible, and user-friendly method that would facilitate acceptable agreement among the raters. The assessment of portfolios was commenced at the end of the training program. Each portfolio was independently assessed by two clinical teachers of the residents, resulting in a total of 104 evaluations. The score for each resident’s portfolio was derived from the average scores provided by the two clinical teachers.
Scoring Rubric DevelopmentSeveral studies suggested that the use of global
criteria with rubrics had a positive impact on inter-rater agreement[17-19]. At the same time, the litera-ture suggested useful items for portfolio assessment in medical education[11,13,14,18]. After reviewing the literature, we summarized and drafted a list of pre-liminary portfolio assessment standards. Then, the clinical teachers and we held many discussions and completed several revisions before the portfolio assessment scale was completed. Afterward, five clinical teachers were invited to assist in the establish-ment of content validity (Content Validity Index = 1).
The evaluation items of the rubric comprised two facets: (1) personal development planning and (2) core courses reflection and practice. There were three items in the measure of personal development planning, namely specific development require-ments, plan execution approaches, and outcomes and evaluation. Meanwhile, there were two items in the measure of core courses reflection and practice: (1) reflection and practice and (2) self-assessment

97Chin-Yi Huang et al. / Tungs’ Medical Journal 11 (2017) 95-101
of the learning process. Five rating scale categories were included in the rubric, and four in-between cat-egories were inserted as means of scores, giving a total of nine categories in the analysis. For each item, five different levels were rated on a Likert scale from 1 (lowest) to 5 (highest) points. Each quality level for each item was clearly defined to distinguish between the performances to allow the medical teacher to assign appropriate score points.
Finally, a scoring rubric was developed in an effort to increase the objectivity of the rubric as the assessment tool for the present study. This rubric pro-vided stricter definitions for each measured quality, thus decreasing the likelihood of subjectivity. Guide-lines for personal development planning and core courses reflection and practice were prepared and provided to support the residents[6,7,10,11,20].
Rater TrainingA rater training program was designed to
improve rater performance and increase the reli-ability and validity of the rating[4]. Example portfolios and the scoring rubric were provided to the raters during the training workshop. The example portfo-lios were generated from our experience with actual examples and were contrived as materials for training purposes. During the training workshop, the raters first had a general discussion about the scoring rubric. Then, they reviewed each level of the scoring rubric individually and discussed the interpretations of each level as well as differences between each level and its preceding and succeeding levels. After the discussion, the raters were asked to rate the example portfolios according to the scoring rubric. All rating data were collected for reliability calculation.
AnalysisWe conducted statistical analyses using SPSS
software (version 15.0; SPSS Inc, Chicago, IL). We calculated the intra-class correlation coefficient to measure the inter-rater reliability. Furthermore, to standardize the scoring rubric measures via Rasch model analysis, Minstep (version 3.70.0.1) was used for the data analysis. Rasch analysis advocates that the respondent’s ability interacts with the parame-ters of the item scale, resulting in an item response. Rasch analysis, independent of the sample distribu-tion, estimates the reliability and validity of both persons and items.
ValidityValidity refers to how well an instrument can
evaluate what it is meant to measure. Rasch analysis is a one-dimensional model that assumes that all scale items have discriminating power. The infit and outfit mean square statistics (MNSQ) are two indices to justify unidimensionality. Therefore, fit statistics are the bases of validity analysis in Rasch models. Infit and outfit MNSQ are also used to identify misfit items and subjects. According to the preset criteria, one misfit item was excluded according to the order in which it was identified, and the process was continued until no further misfit item was found. Then, examinees who met the preset misfit criteria were excluded from the next step of the analysis. An item or subject was con-sidered to fit the Rasch model and meet unidimen-sionality if it had infit and outfit MNSQ ranging from 0.5 to 1.5 and a Z-score between −2 and 2[21].
ReliabilityReliability refers to the ability of an assessment
tool to generate stable results. Person reliability in Rasch analysis analyzes the response patterns of the subjects independently of item reliability, which is equivalent to the Cronbach’s α coefficient. In addi-tion, the separation index reported by Rasch analysis, another source of reliability information, illustrates how well the examination can discriminate subject ability. The person separation index for the rubric score can detect distinct groups of residents within the sample. A lower person separation index (<2) implies that the instrument may not be sufficiently sensitive to distinguish between high and low performance. The logit map identifies the location of the items along the scale on the right, with the distribution of the residents on the left side of the scale. In the Rasch scale map, the mean of the item values is set at zero, with more difficult scale items located above the item mean and easier scale items below the item mean.
Results
Fifty-one residents who were trained in the PGY1 residency training program during the 2012–2013 academic year participated in the study. Table 1 shows the descriptive statistics for the scores of the portfolio assessment. The residents received scores exceeding the median (mean = 3.24, SD = 0.71) on the evaluations of specific development requirements

98 Chin-Yi Huang et al. / Tungs’ Medical Journal 11 (2017) 95-101
and received the lowest average score (mean = 2.31, SD = 0.87) for outcomes and evaluation.
The inter-rater reliability based on the intra-class correlation coefficient was 0.85, which can be inter-preted to indicate good reliability. This demonstrated good consistency between the two raters. In addi-tion, we used Rasch model analysis to examine the quality of the measurement tool. Table 1 also lists the results of Rasch analysis. During the fit analysis, three examinees were excluded from further analysis. The infit MNSQ of items ranged between 0.73 and 1.19. To the contrary, the outfit MNSQ of the remaining examinees varied from 0.72 to 1.20. The estimated test reliability and person separation indices were 0.89 and 2.88, respectively, through the process of exclusion of misfit examinees and items.
Figure 1 presents the results of item analysis. The item difficulty values fell between −1.10 and 1.46, and the range of examinee ability scores was −3.40–4.75. There were four items located at the section from M (0 logit) downward to T (2 SD) set by the Rasch model. After examining the parameter distributions of the subjects and items on the two sides of the map, it was found that 40% of the resi-dents had competences above the four items. Nearly 72% of the residents had competences above item I0001. Approximately 22% of the residents had com-petences below all of the items, indicating that the items were too difficult for them to complete. On the other hand, only one item (I0003) was located in the section from M (0 logit) upward to T (2 SD) set by the Rasch model. The item was difficult for 87% of the residents to complete. However, nearly 13% of the residents had higher competences than the item, indicating that they could complete all of the items in this study.
Table 1 Raw score means, Item measures and fit statistics of portfolio scoring rubric
ItemsRaw score
Measure SEInfit Outfit
Mean SD MNSQ Z-value MNSQ Z-value
1 3.24 0.71 -1.10 .18 .92 -.30 .99 .00
2 2.87 0.71 -.16 .17 .96 -.10 1.05 .30
3 2.31 0.87 1.46 .17 1.19 .90 1.20 1.00
4 2.87 0.84 -.01 .17 1.02 .20 1.02 .10
5 2.93 0.77 -.19 .17 .73 -1.30 .72 -1.40
Items: 1. Specific Development Requirements; 2. Plan Execution Approaches; 3. Outcomes and Evaluation; 4. Reflection and Practice; 5. Self-assessment of Learning Process.
Fig. 1 Residence ability/item difficulty map of the 5 items of portfolio scoring rubric.

99Chin-Yi Huang et al. / Tungs’ Medical Journal 11 (2017) 95-101
Discussion
This study focused on the application of a port-folio scoring rubric to a PGY1 residency training program in Taiwan using a Rasch analysis. From this empirical study, we have several findings that pro-vided valuable information for improving the exam-ination. First, all items fitted the Rasch model well, implying passable item development quality and acceptable construct validity for the scoring rubric. Second, the reliability of the scoring rubric was 0.89, meaning that the measured results were reliable. This scoring rubric can be useful for raters to assess port-folios and allow the learners to better understand the criteria by which they are evaluated. It is also feasible to incorporate the rubric as one of the summative assessment tools for PGY1 residency training.
Competence is recognized as both the gain of knowledge and the application of knowledge in prac-tice. A portfolio is a collection of learning achieve-ments with unlimited formats presented by the learners to demonstrate their competences[8]. Port-folio assessment is desirable for facilitating self-reflection through peer feedback during the learning process[2,7,10,22,23]. Therefore, the portfolio has become a popular tool in medical education for both learning and assessment. At the same time, the use of evaluation tools with much higher precision, such as portfolios, will facilitate the development of effective educational methods for delivering essential compe-tences in medical education[5,13,24-26].
A major challenge for integrating portfolio assessment into medical education is the assess-ment quality of individual portfolios. Several studies suggested that a number of measures had a positive impact on inter-rater agreement, such as the use of a small group of trained assessors[17-19,27], discussion among the raters before the actual assessment[18,19,27] and after assessing part of the portfolios[18,19], and the use of global criteria with rubrics[17-19]. Our study illustrated that via discussion and consensus between assessors, together with creating a rubric for grading, the inter-rater reliability achieved the desired level needed for summative assessment.
Another challenge of incorporating portfolio assessment into medical education is that its effec-tiveness depends largely on the assessed students. In introducing a new assessment process, both the PGY1 students and clinical teachers could feel increasingly
stressed about the use of portfolios in the practical training program. Thus, supportive resources and clear guidelines should be prepared to facilitate the teaching and learning process[7,10,20,28]. The port-folio assessment scoring rubric clarified the expec-tations for the portfolio and improved residents’ understanding of the assessment criteria. However, the quality of the portfolio could decrease owing to the busy and stressful clinical tasks of the residents. Such resistance from trainees was also reported by a previous studies[2,7]. Currently, we are struggling to provide incentives to ensure that the trainees con-tinue to optimize the content of their portfolios.
Some previous studies reported that only mod-erate inter-rater reliabilities could be achieved when portfolios were assessed[12]. Another study that examined the reliability of assessors in providing ratings for portfolios demonstrated that the inter-rater reliability for the global assessment of the port-folios was 0.38 and that the intra-rater reliability was 0.54[29]. In a trial assessing the performances of pedi-atric specialist registrars via portfolio assessment, the inter-rater correlation coefficient of the portfolio assessment was 0.52, and the internal consistency generalizability coefficient was 0.65[27]. A study that adopted portfolio assessment in a surgical residency learning program revealed that the inter-rater reli-ability remained less than 0.7 even with extensive negotiation and collaboration between assessors and the creation of a more objective scoring rubric[14].
We recognize that this study has several limi-tations. The participants consisted of only 51 PGY1 residents trained in one teaching medical center in central Taiwan during a single academic year. The sample size limits the generalizability of the findings to other training programs in other hospitals in other parts of Taiwan. In addition, the items of the port-folio scoring rubric were set by the medical teachers according to their curricula and expectations for the students. Over time, the goals and environments of clinical education will change, and the criteria of the portfolio scoring rubric will have to be revised regu-larly based on the suggestions of the clinical teachers.
Other medical education institutions can design their own portfolio scoring rubrics matching their curricula and expectations, in line with the principles and spirit of the scoring rubric. To date, the profes-sionalism and career performances of clinical educa-tion are difficult to collect, present, and assess via

100 Chin-Yi Huang et al. / Tungs’ Medical Journal 11 (2017) 95-101
portfolios. We await further developments on port-folio assessment in our hospital, and a well-designed portfolio scoring rubric should be applied to assess the professionalism or career performances in broader real-life situations in clinical education.
To conclude, this study demonstrated the devel-opment of a valid portfolio assessment scoring rubric for a PGY1 residency training program. The devel-oped scoring rubric increased the validity and reli-ability of portfolio assessment. The rubric also pro-vided the learners with much clearer criteria for the assessment. These efforts have improved medical education in our hospital, and they represent a useful example for other hospitals seeking to achieve similar progress.
References
1. Moonen-van Loon, J.M.W., et al., Composite reliability of a workplace-based assessment toolbox for postgraduate medical education. Advances in Health Sciences Educa-tion: Theory and Practice, 2013. 18(5): p. 1087-1102.
2. Ben-David, M.F., et al., AMEE Medical Education Guide No. 24: Portfolios as a method of student assessment. Medical Teacher, 2001. 23(6): p. 535-551.
3. Koretz, D., Large-scale portfolio assessments in the US: evidence pertaining to the quality of measurement. Assessment in Education: Principles, Policy & Practice, 1998. 5(3): p. pp.309-334.
4. Feldman, M., et al., Rater training to support high-stakes simulation-based assessments. Journal of Continuing Edu-cation in the Health Professions, 2012. 32(4): p. 279-286.
5. McArdle, P.J., Innovations in undergraduate medical edu-cation and in graduate medical training. Journal of Con-tinuing Education in the Health Professions, 1997. 17(4): p. 214-223.
6. Albanese, M.A., et al., Building a competency-based cur-riculum: the agony and the ecstasy. Advances in Health Sciences Education: Theory and Practice, 2010. 15(3): p. 439-454.
7. Tompkins, M. and D. Paquette-Frenette, Learning port-folio models in health regulatory colleges of Ontario, Canada. Journal of Continuing Education in the Health Professions, 2010. 30(1): p. 57-64.
8. Carraccio, C. and R. Englander, ANALYSES/LITERATURE REVIEWS: Evaluating Competence Using a Portfolio: A Lit-erature Review and Web-Based Application to the ACGME Competencies. Teaching and Learning in Medicine, 2004. 16(4): p. 381-387.
9. Davis MH, P.G., Portfolio assessment. Journal of Veteri-nary Medical Education, 2005. 32(3): p. 279-284.
10. Green, M.L., S.G. Reddy, and E. Holmboe, Teaching and evaluating point of care learning with an Internet-based clinical-question portfolio. Journal of Continuing Educa-tion in the Health Professions, 2009. 29(4): p. 209-219.
11. McNeill, H., J.M. Brown, and N.J. Shaw, First year spe-cialist trainees’ engagement with reflective practice in the e-portfolio. Advances in Health Sciences Education:
Theory and Practice, 2010. 15(4): p. 547-558.12. Driessen, E., et al., Portfolios in medical education: why
do they meet with mixed success? A systematic review. Medical Education, 2007. 41(12): p. 1224-1233.
13. Learman, L.A., A.M. Autry, and P. O’Sullivan, Reliability and validity of reflection exercises for obstetrics and gynecology residents. American Journal of Obstetrics and Gynecology, 2008. 198(4): p. 461.e1-461.e10.
14. Webb, T.P. and T.R. Merkley, An Evaluation of the Success of a Surgical Resident Learning Portfolio. Journal of Sur-gical Education, 2012. 69(1): p. 1-7.
15. Yang, S.C., et al., Statistical item analysis of the exami-nation in anesthesiology for medical students using the Rasch model. Journal of the Chinese Medical Association, 2011. 74(3): p. 125-129.
16. Huang, Y.F., et al., Item response analysis on an examina-tion in anesthesiology for medical students in Taiwan: A comparison of one- and two-parameter logistic models. Journal of the Chinese Medical Association, 2013. 76(6): p. 344-349.
17. Tate P, F.J., Neighbour R, Campion P, Field S., Assessing Physicians’ Interpersonal Skills via Videotaped Encounters: A New Approach for the Royal College of General Practi-tioners Membership Examination. Journal of Health Com-munication, 1999. 4(2): p. 143-152.
18. O’Sullivan, P., et al., Demonstration of Portfolios to Assess Competency of Residents. Advances in Health Sciences Education: Theory and Practice, 2004. 9(4): p. 309-323.
19. Rees, C.E. and C.E. Sheard, The reliability of assessment criteria for undergraduate medical students’ communica-tion skills portfolios: the Nottingham experience. Medical Education, 2004. 38(2): p. 138-144.
20. Dornan, T., Self-assessment in CPD: Lessons from the UK undergraduate and postgraduate education domains. Journal of Continuing Education in the Health Professions, 2008. 28(1): p. 32-37.
21. Linacre, J.M., A User’s Guide to W I N S T E P S® M I N I S T E P Rasch-Model Computer Programs. 2015, Chicago; .
22. Parboosingh, J., Role of self-assessment in identification of learning needs. Journal of Continuing Education in the Health Professions, 1998. 18(4): p. 213-219.
23. Lockyer, J., S.T. Gondocz, and R.L. Thivierge, Knowledge translation: The role and place of practice reflection. Journal of Continuing Education in the Health Professions, 2004. 24(1): p. 50-56.
24. Grant, J., Measurement of learning outcomes in continuing professional development. Journal of Continuing Educa-tion in the Health Professions, 1999. 19(4): p. 214-221.
25. Ben-David, M.F., The role of assessment in expanding pro-fessional horizons. Medical Teacher, 2000. 22(5): p. 472-477.
26. Wass, V., et al., Assessment of clinical competence. The Lancet, 2001. 357(9260): p. 945-949.
27. Melville, C., et al., Portfolios for assessment of paediatric specialist registrars. Medical Education, 2004. 38(10): p. 1117-1125.
28. McMullan, M., Students’ perceptions on the use of portfo-lios in pre-registration nursing education: A questionnaire survey. International Journal of Nursing Studies, 2006. 43(3): p. 333-343.
29. Pitts J, C.C., Thomas P., Enhancing reliability in portfolio assessment: ‘shaping’ the portfolio. Medical Teacher, 2001. 23(4): p. 351-356.

101Chin-Yi Huang et al. / Tungs’ Medical Journal 11 (2017) 95-101
畢業後一般醫學訓練醫師課程學習歷程檔案評量:Rasch 模式分析
黃靜宜1,† 李銘宗2,† 蔣志隆1 廖以誠1,* 曹龍彥3
1彰化基督教醫院 教學部2彰化秀傳醫院 研究輔佐中心
3彰化基督教醫院 兒科部
受文日期:民國 105年 06月 20日;接受刊載:民國 105年 10月 18日
摘要
背景及目的:學習歷程在臨床實務已漸採用取為學習及評量之工具。然以學習歷程來評量畢業後一般醫
學訓練醫師個人發展與反思,其信度與效度台灣少有研究。本研究目的為發展一評分規範,並以 Rasch模式評估其信度與效度。
方法:建立具有清楚基準之評分規範,做為學習歷程評量。評分規範中有五個評分項目以評量學員能力。
以 Rasch模式來評估評分規範的信度與效度。內與外適合度均方可找出不適配的項目與答題者,以受試者信度分析答題者之答題型態。
結果:2012-2013學年間,51位畢業後一般醫學訓練醫師參與本研究。內適合度均方 0.73-1.19,外適合度均方 0.72-1.20。估計測驗信度及受試者分離指標,依序為 0.89 及 2.88。結論:此評分規範提供學員清楚之評量基準,該評量基準具有良好之效度與信度。
關鍵詞:評估、醫學教育、住院訓練、訓練課程、Rasch模式
*通訊作者:廖以誠醫師 彰化基督教醫院教學部 彰化市南校街 135號 † 黃靜宜與李銘宗為共同第一作者。

102
Traumatic Rhabdomyolysis-Induced Acute Renal Failure: A Case Report and Review of Literature
Wang Shih-Nung*, Tung Yung-Wei
Division of Critical care Medicine, Division of Thoracic Surgery, Tung’s Taichung MetroHarbor Hospital
Received: Jan. 19, 2016; Accepted: Jun. 24, 2016
Abstract
Trauma is often the cause of elevated creatine kinase, but in most cases, serum values are <5,000 IU/L. Here we present a case report of a 78-year-old man who was compressed by a tiller for >2 h and sustained a crush injury of his bilateral lower limbs. He suffered a hypovolemic shock. Resuscitation and an emergency operation were performed after assessment. His vital signs stabilized after fluid resuscitation, alkalinization of urine, and hemodialysis. His initial serum creatine kinase level was >220,000 IU/L; the level declined to 8,000 IU/L after treatment. Muscle necrosis persisted. He refused to undergo a further operation. He suffered with hyperkalemia and hemodynamic collapse and expired despite cardiopulmonary resuscitation.
If creatine kinase levels increase out of proportion or do not decline as expected after treatment, continued muscle injury or compartment syndrome should be suspected and debridement and fasciotomy should be considered; furthermore, hemodialysis should be administered as early as possible to alleviate the impact of electrolyte imbalance and myoglobinemia in rhabdomyolysis-related acute kidney injury instead of treating the condition just by methods such as fluid resuscitation, alkalinization, and administration of diuretics. In this article, the pathologic mechanism and treatment of rhabdomyolysis are reviewed. We also discuss the possible methods for improving the condition.
Key words: creatine kinase, rhabdomyolysis, acute renal failure
Introduction
Rhabdomyolysis is a syndrome characterized by muscle necrosis and release of intracellular muscle constituents into the circulation. Elevated creatine kinase (CK) level, muscle pain, and myoglobinuria may also be present. High circulating plasma myo-globin levels can lead to heme pigment-associated acute tubular necrosis or acute kidney injury (AKI)[1,2]. The severity of illness ranges from asymptomatic elevations in serum muscle enzymes to life-threat-ening disease associated with extreme enzyme eleva-tions, electrolyte imbalances, and AKI. The benefit of hemodialysis is yet to be determined, but it should
be considered if the initial CK level is high or rapidly increasing.
Case Report
A 78-year-old man sustained a crush injury of his bilateral lower limbs in a traffic accident. Severe soft tissue damage of the right leg and foot and deformity of bilateral thighs were noted (Fig. 1). Fluid resusci-tation was administered. Imaging studies revealed fractures of the tibia, fibula, and femur of both lower limbs. Emergency surgical intervention, including amputation and debridement, was performed because of severe soft tissue damage and compart-ment syndrome of the right leg. Postoperatively, the patient was admitted to the surgical intensive care unit. Vancomycin was administered. Pus culture revealed Enterococcus faecium. Prothrombin time
Tungs’ Medical Journal 11 (2017) 102-107
Case Report
* Correspondence to: Dr. Wang Shih-Nung, Division of Critical care Medicine, Division of Thoracic Surgery, Tung’s Taichung MetroHarbor Hospital, No. 699, Sec. 8, Taiwan Blvd., Wuqi Dist., Taichung City 43503, Taiwan, (R.O.C.)

103Wang Shih-Nung et al. / Tungs’ Medical Journal 11 (2017) 102-107
was 14.2 s. Activated partial thromboplastin time was 45.9 s. Fresh frozen plasma and platelets were admin-istered for coagulopathy. The serum creatinine level had worsened from an initial level of 1.4 mg/dL to 4.7 mg/dL on day 4. Serum CK level had rapidly increased: 8,425 U/L (day 1), 35,492 U/L (day 2), 145,480 U/L (day 3), and 226,116 U/L (day 4). Fluid resuscitation of >5000 mL/day was administered. Sodium bicar-bonate was administered to alkalinize the urine. Mannitol was administered to control diuresis and protect renal tubular cells but was stopped on day 3 because of anuria. An inotropic agent was admin-istered to maintain systemic blood pressure, which was >80 mmHg. On day 4, hemodialysis therapy was administered because of anuria, metabolic acidosis, and hyperkalemia (6.1 mEq/L). Serum CK levels pro-gressively declined to 8,523 units/L on day 8 after the treatment, but hyperkalemia (6.1 to 7.7 mEq/L) and hypocalcemia (5.2 to 6.8 mg/dL) were refractory to correction. The patient’s family refused fasciotomy and debridement for compartment syndrome of the right thigh. The patient showed sudden arrhythmia and hemodynamic collapse on day 8 of hospitalization and expired despite cardiopulmonary resuscitation.
Discussion
Approximately 26,000 cases of rhabdomyol-ysis are diagnosed annually in the United States [3]. Among these cases, approximately 15% to over 50% are complicated by AKI [2].
Rhabdomyolysis can result from trauma or muscle compression (for instance, crush syndrome
or prolonged immobilization), nontraumatic exertion (for instance, marked exertion in untrained individ-uals or hyperthermia), toxins, infections, or electro-lyte disorders. Traumatic rhabdomyolysis develops in 30%–50% of cases of crush syndrome and is fre-quently observed after catastrophic earthquakes [4,5].
Rhabdomyolysis should be suspected following prolonged immobilization in any stuporous or coma-tose patient or in a patient who is otherwise unable to provide a medical history and has muscle tender-ness, pressure necrosis of the skin, multiple trauma, or a crush injury, and blood chemistry abnormalities, suggesting the possibility of increased cell break-down, such as hyperkalemia, hyperphosphatemia, hypocalcemia, and/or AKI.
DiagnosisThe diagnosis of rhabdomyolysis is markedly
elevated serum CK levels (that is, >20,000 units/L) or myoglobinuria [6]. Other symptoms include myalgia, muscle stiffness and cramping, malaise, fever, tachy-cardia, nausea and vomiting, and abdominal pain. Limb induration and ischemic skin changes, such as discoloration and blisters, are present in <10% of patients [7].
The serum CK levels at presentation are usually at least five times the upper limit of the normal level, but can range from approximately 1,500 IU/L to >100,000 IU/L. The mean peak CK levels ranged from approximately 10,000 to 25,000 IU/L in the largest series [2]. CK levels may be lower in patients with liver disease or multiple organ failure because of decreased half-life of the enzyme due to extracellular glutathione depletion. Elevations in serum amino-transferases are common and can cause confusion if attributed to liver disease. CK has a serum half-life of approximately 1.5 days and declines at a relative con-stant rate of approximately 40%–50% of the previous day’s value [7,8]. Serum CK levels begin to rise within 2–12 h following the onset of muscle injury, reaching their maximum within 24–72 h. A decline of 50% per 48 h is usually observed within 3–5 days of resolu-tion of the muscle injury. If CK levels do not decline as expected, continued muscle injury or compartment syndrome should be suspected [7,8].
Myoglobinuria is observed in only half of the cases; thus, its absence does not exclude the diag-nosis. Myoglobin, a small molecule monomer and heme-containing respiratory protein, is released
Fig. 1 Severe crushed wounds over bilateral feet.

104 Wang Shih-Nung et al. / Tungs’ Medical Journal 11 (2017) 102-107
from damaged muscles in parallel with CK, is rapidly filtered and excreted in the urine, and often results in the production of red to brown urine and normal color plasma unless renal failure limits myoglobin excre-tion. It can be detected by the urine (orthotolidine) dipstick test at concentrations of just 0.5–1 mg/dL [9]. Myoglobin has a half-life of only 2–3 h. Because of its rapid excretion and metabolism to bilirubin, serum levels may return to normal within 6–8 h [9]. There-fore, routine urine testing for myoglobin by urine dip-stick evaluation may be negative in up to half of the patients with rhabdomyolysis [1]. Pigmenturia will be missed in rhabdomyolysis if the filtered load of myo-globin is insufficient or has largely resolved before the patient seeks medical attention due to its rapid clearance. Both hemoglobin and myoglobin can be detected on the urine dipstick, appearing as “blood,” although microscopic evaluation of urine generally shows few red blood cells (RBCs). Such testing is not a reliable method for the rapid detection of myoglobin if RBCs are present or in patients with hemolysis due to its lack of specificity for myoglobin.
Hypovolemia results from the influx of extra-cellular fluid into injured muscles and induces acute renal ischemic damage. Hyperkalemia and hyper-phosphatemia result from the release of potassium and phosphorus, respectively, from damaged muscle cells. Hyperkalemia may develop early, even in the absence of AKI. Its severity may appear dispropor-tionate to the degree of renal injury. The daily rate of rise in the plasma potassium concentration can exceed 1.0 mEq/L in patients with rhabdomyolysis, much greater than that typically occurring even in patients with renal failure [10]. The levels of potas-sium and phosphate decrease as they are excreted in the urine.
Hypocalcemia occurs in up to two-thirds of patients with significant rhabdomyolysis in the first few days because of calcium entry into damaged myocytes, and causes both the deposition of calcium salts in damaged muscle and decreased bone respon-siveness to parathyroid hormone [11]. Hypercalcemia occurs during the recovery phase of rhabdomyolysis in up to 20%–30% of patients [11]. It results from the mobilization of calcium that has been deposited in the injured muscle [12], mild secondary hyperparathy-roidism from acute renal failure, correction of hyper-phosphatemia (resulting from the rise in GFR), and an increase in 1,25-dihydroxyvitamin D [11]. To minimize
this complication, the administration of calcium should be avoided during the renal failure phase.
Hyperuricemia may develop due to the release of nucleosides from damaged myocyte nuclei, which are metabolized in the liver into purines and then converted to uric acid, and reduced urinary excretion in impaired renal function.
ComplicationsThe complications of rhabdomyolysis include
acute kidney injury, electrolyte abnormalities (hyper-kalemia, hyperphosphatemia, hypocalcemia, and hyperuricemia), compartment syndrome, and dis-seminated intravascular coagulation.
AKI is a common complication of rhabdomyol-ysis, with a frequency from 15% to >50% [2]. The risk of AKI is lower in patients with CK levels < 15,000–20,000 units/L at admission; the risk factors for AKI in patients with lower CK levels include dehydration, sepsis, and acidosis [13]. Heme pigment may injure the kidney via tubular obstruction, possibly in association with uric acid, direct proximal tubular cell injury from free chelatable iron, or vasoconstriction [14]. Despite its toxic properties, heme pigment rarely causes kidney injury in the absence of predisposing condi-tions. Volume depletion enhances both vasoconstric-tion and formation of obstructing casts. This is very important for the development of heme-induced AKI.
The degree of CK elevation does not always predict the development of AKI, although there is a weak correlation between the peak CK level and serum creatinine [14]. AKI is uncommon when the peak CK levels are <5,000–10,000 units/L [8,15].
Compartment syndrome is a potential compli-cation of severe rhabdomyolysis that may develop after fluid resuscitation, with worsening edema of the damaged limb [16]. Disseminated intravascular coagulation may occur due to the release of throm-boplastin and other prothrombotic substances from the damaged muscle [7].
TreatmentThe goals for treatment include correction of
volume depletion and prevention of intratubular cast formation. Volume repletion is necessary to enhance renal perfusion, minimize ischemic injury, and increase the urine flow rate, which will limit intratubular cast formation and increase urinary potassium excretion. Fluid resuscitation should be

105Wang Shih-Nung et al. / Tungs’ Medical Journal 11 (2017) 102-107
administered as soon as possible and continued until the muscle injury has resolved. The optimal fluid and rate of repletion remain unclear. The use of chloride-restrictive fluid administration strategies in critically ill patients has been associated with a significant decrease in the incidence of AKI and use of renal replacement therapy [17]. Initial fluid resuscitation with isotonic saline at a rate of 1–2 L/h is suggested, until the plasma CK level is stable and not increasing [8]. Patients who have a stable plasma CK level < 5000 unit/L do not require intravenous fluid. The volume status of the patient should be carefully assessed and the urine output monitored.
Forced alkaline diuresis, in which the urine pH is raised to >6.5, may diminish the renal toxicity of heme, intratubular pigment cast formation, release of free iron from myoglobin, and risk for tubular pre-cipitation of uric acid [2]. Despite these potential ben-efits, there is no clear clinical evidence that an alka-line diuresis is more effective than a saline diuresis in preventing AKI [7]. Bicarbonate could be administered if severe hypocalcemia is absent, arterial pH is <7.5, and serum bicarbonate is <30 mEq/L. It is mandatory to monitor the arterial pH and serum calcium every 2 h during the infusion.
The benefit of mannitol in rhabdomyolysis is not established, although experimental studies have sug-gested that mannitol is protective by causing diuresis, which minimizes intratubular heme pigment deposi-tion and cast formation, and/or by acting as a free radical scavenger, thereby minimizing cell injury [18]. The use of mannitol administration may be benefi-cial in patients with marked CK elevations (>30,000 unit/L) [19]. Mannitol is contraindicated in patients with oligouria or anuria because there is a risk of hyperosmolality, volume overload, and hyperkalemia.
The benefit of hemodialysis in removing myo-globin, hemoglobin, or uric acid to prevent the devel-opment of renal injury is unclear [2]. Temporary dialysis can be administered for one week since the epithelium of the renal tubule regenerates in this period.
The overall prognosis for patients with heme-induced AKI is favorable, and several patients will recover to normal or near-normal kidney function.
Our patient had rhabdomyolysis-related kidney injury resulting from his severe soft tissue damage. His unstable hemodynamic status persisted despite fluid resuscitation and inotropic treatment. Though
his CK levels declined progressively after hemodialysis being administered daily since the fourth day after operation, hypocalcemia and hyperkalemia wors-ened progressively and were refractory to correction by administration of insulin, bicarbonate, or calcium polystyrene sulfonate (kayexalate). This implied that more muscle necrosis or compartment syndrome had developed. Debridement and fasciotomy should have been considered, but the patient’s family refused further surgical intervention, including fasciotomy and amputation. Uncontrolled electrolyte imbalance and profound sepsis caused hemodynamic collapse and death.
Enough fluid supplementation should have been administered to maintain the hemodynamic status and adequate renal perfusion. The serum lactate levels should have been checked to monitor tissue perfusion. Fluid resuscitation seemed to be inade-quate. More fluid supplementation should have been administered.
His CK levels increased rapidly—2,460 U/h (4-fold) at the initial 12 h and 4,582 U/h (4-fold) at the next 24 h. In other mild rhabdomyolysis cases, the increased rate is about 0.5-fold to 1.5-fold per day. This implied a high possibility of developing rhabdo-myolysis-related AKI. The initial time of hemodialysis was day 4 of hospitalization, which may have been too late. Although prophylactic hemodialysis could not have prevented the development of rhabdomyolysis-related AKI, it should be administered as early as pos-sible to alleviate the impact of electrolyte imbalance if the initial CK level was >10,000–15,000 units/L or the CK rate was increasing out of proportion. In other words, all treatments of rhabdomyolysis, including fluid supplementation and alkalization of urine and mannitol, are to be administered to decrease myoglo-binemia and prevent kidney injury. If renal function worsens, hemodialysis should be administered early to salvage remnant renal function and alleviate the complication of acute renal failure.
SummaryA major cause of rhabdomyolysis is traumatic
muscle injury. The clinical manifestations and com-plications of rhabdomyolysis result from muscle cell death, with the release of intracellular muscle con-stituents into the circulation. Hypovolemia, increased plasma CK, hyperkalemia, hyperphosphatemia, hypo-calcemia, hyperuricemia, and metabolic acidosis

106 Wang Shih-Nung et al. / Tungs’ Medical Journal 11 (2017) 102-107
can also occur. The clinical manifestations of heme-induced AKI include oliguria or anuria, red or brown urine, and pigmented granular casts on urinalysis. Serum CK levels begin to rise within 2–12 h following muscle injury and reach their maximum within 3 days and then progressively decrease. Early and aggressive fluid resuscitation is the major preventive therapy. Fluid resuscitation is recommended in patients with rhabdomyolysis who have plasma CK levels >5000 unit/L and in those who have increasing CK levels regardless of the baseline value. Limited data suggest that alkalinization of the urine and mannitol treat-ment benefit patients with severe rhabdomyolysis. Plasma potassium and calcium should be monitored until the levels become stable. Calcium supplemen-tation should be administered only for symptomatic hypocalcemia or severe hyperkalemia. The serum CK levels and electrolytes (such as potassium) should be monitored closely during treatment. If the CK level increases out of proportion or does not decline as expected after treatment, continued muscle necrosis or compartment syndrome should be suspected. Debridement and fasciotomy should be considered. Hemodialysis may be necessary for controlling hyper-kalemia and the correction of acidosis or for the treat-ment of volume overload; it should be administered as early as possible to prevent electrolyte imbalance if the initial CK level is >10,000–15,000 units/L or increasing at a rapid rate.
References
1. Giannoglou GD, Chatzizisis YS, Misirli G. The syndrome of rhabdomyolysis: Pathophysiology and diagnosis. Eur J Intern Med 2007; 18:90.
2. Melli G, Chaudhry V, Cornblath DR. Rhabdomyolysis: an evaluation of 475 hospitalized patients. Medicine (Balti-more) 2005; 84: 377.
3. Sauret JM, Marinides G, Wang GK. Rhabdomyolysis. Am Fam Physician 2002; 65:907.
4. Bartal C, Zeller L, Miskin I, et al. Crush syndrome: saving more lives in disasters: lessons learned from the early-response phase in Haiti. Arch Intern Med 2011; 171: 694.
5. Sever MS, Erek E, Vanholder R, et al. The Marmara earthquake: epidemiological analysis of the victims with nephrological problems. Kidney Int 2001; 60: 1114.
6. Huerta-Alardín AL, Varon J, Marik PE. Bench-to-bedside review: Rhabdomyolysis – an overview for clinicians. Crit Care 2005; 9: 158.
7. Bagley WH, Yang H, Shah KH. Rhabdomyolysis. Intern Emerg Med 2007; 2: 210.
8. Mikkelsen TS, Toft P. Prognostic value, kinetics and effect of CVVHDF on serum of the myoglobin and creatine kinase in critically ill patients with rhabdomyolysis. Acta Anaes-thesiol Scand 2005; 49: 859.
9. Llach F, Felsenfeld AJ, Haussler MR. The pathophysiology of altered calcium metabolism in rhabdomyolysis-induced acute renal failure. Interactions of parathyroid hormone, 25-hydroxycholecalciferol, and 1,25-dihydroxycholecal-ciferol. N Engl J Med 1981; 305: 117.
10. Lane JT, Boudreau RJ, Kinlaw WB. Disappearance of mus-cular calcium deposits during resolution of prolonged rhabdomyolysis-induced hypercalcemia. Am J Med 1990; 89: 523.
11. Zager RA. Rhabdomyolysis and myohemoglobinuric acute renal failure. Kidney Int 1996; 49: 314.
12. Hatamizadeh P, Najafi I, Vanholder R, et al. Epidemiologic aspects of the Bam earthquake in Iran: the nephrologic perspective. Am J Kidney Dis 2006; 47: 428.
13. Paletta CE, Lynch R, Knutsen AP. Rhabdomyolysis and lower extremity compartment syndrome due to influenza B virus. Ann Plast Surg 1993; 30: 272.
14. Yunos NM, Bellomo R, Hegarty C, et al. Association between a chloride-liberal vs chloride-restrictive intra-venous fluid administration strategy and kidney injury in critically ill adults. JAMA 2012; 308: 1566.
15. Zager RA. Combined mannitol and deferoxamine therapy for myohemoglobinuric renal injury and oxidant tubular stress. Mechanistic and therapeutic implications. J Clin Invest 1992; 90: 711.

107Wang Shih-Nung et al. / Tungs’ Medical Journal 11 (2017) 102-107
外傷性橫紋肌溶解症導致急性腎衰竭:一病例報告暨文獻回顧
王世農* 童詠偉
童綜合醫院 重症醫學科 胸腔外科
受文日期:民國 105年 01月 19日;接受刊載:民國 105年 06月 24日
摘要
外傷常常導致肌酸激酶升高,但一般血清值大多低於 5000 IU/L. 超過 10000 IU/L 者並不多見。在此我們報告一位 78歲老者,其於工作時,不慎耕耘機壓傷下肢,達兩個多小時,方被救出。送醫到院時,已有脫水休克現象。經急救與緊急手術後,經輸液鹼化尿液血液透析等治療,生命徵象一度穩定。
其肌酸激酶一度超過 220000IU/L. 雖其逐漸下降至 8000IU/L. 最後仍然因高血鉀導致血行動力衰竭死亡。 治療橫紋肌溶解症效果之追蹤,端視肌酸激酶與血鉀之變化。若兩者異常升高,意味發生持續
性肌肉壞死或腔室症候群,必須施以清創或肌膜切開等外科治療。當肌酸激酶異常快速升高(高於
10,000–15,000 units/L或高於 2倍 /天)或治療中血鉀持續升高,預期腎衰竭可能發生,應儘早施以血液透析,以期儘快降低肌球蛋白所造成之破壞,而不單只是先施以輸液,鹼化尿液,利尿劑等基本的內科治
療,這樣或許對於嚴重肢體壓傷之病患,尚且有一線生機。文中也回顧橫紋肌溶解症之致病機轉及治療
原則,並討論此病例治療之改善空間。
關鍵詞:肌酸激酶、橫紋肌溶解症、急性腎衰竭
*通訊作者:王世農醫師 童綜合醫療社團法人童綜合醫院 重症醫學科 胸腔外科 43503臺中市梧棲區臺灣大道八段 699號

108
Complicated Meckel’s Diverticulum Initially Presenting with Small Bowel Obstruction
Chun-Hsiang Chang, Min-Yung Kuo*
Department of Surgery, Tungs’ Taichung MetroHarbor Hospital, Taichung, Taiwan
Received: Apr. 08, 2016; Accepted: Mar. 13, 2017
Abstract
Meckel’s diverticulum, which is the most common congenital abnormality of the gastrointestinal tract, results from an incomplete obliteration of the vitelline duct. Axial torsion of Meckel’s diverticulum is the rarest reported complication, particularly in children. Owing to insignificant findings in laboratory tests or computed tomography scans, surgery for Meckel’s diverticulum tends to be delayed. In our case, early exploratory laparotomy allowed an early diagnosis and treatment of the complicated Meckel’s diverticulum.
Key words: Meckel’s diverticulum, Axial torsion, Small bowel obstruction
Introduction
Meckel’s diverticulum is the most common congenital abnormality of the gastrointestinal tract, which results from an incomplete obliteration of the vitelline duct. Symptoms of Meckel’s divertic-ulum occur because of complications. This condition more frequently occurs in children than in adults and includes hemorrhage and intestinal obstruction[1]. One out of five cases reportedly develops life-threat-ening complications requiring surgical treatment, and approximately 50% of the cases are reported in chil-dren aged <2 years[2]. The omphalomesenteric band is a remnant of the omphalomesenteric duct, and the mesodiverticular band is an embryologic remnant of the vitelline circulation[3]. The torsion of Meckel’s diverticulum is associated with either of these bands. Here we describe the case of a child with axial torsion of Meckel’s diverticulum, which is the rarest reported complication particularly in children.
Case Report
A boy aged 1 year and 3 months, with a normal birth history, was admitted to our pediatric emer-gency department with fever, abdominal distension, and bilious vomiting for 3 d; he defecated at the time of visit. His family had visited a local clinic for medical treatment, but his symptoms and signs con-tinued to progress. His body temperature at admis-sion was 37.3°C, heart rate was 130 beats per min, and respiratory rate was 30 breaths per min. Physical examination revealed a severe abdominal distension with decreased bowel sounds, but no abdominal or rebound tenderness was present. Laboratory tests at admission revealed a normal white blood cell count of 4100/μl with 89.5% neutrophils and a C-reactive protein level of 22.9 mg/dl. Abdominal radiography showed dilated small bowel loops and a scanty colon gas pattern (Fig. 1A, 1B). Because of suspected small bowel obstruction, he was admitted to the inten-sive care unit where he underwent nasogastric tube insertion with NPO for gastrointestinal decompres-sion, fluid resuscitation for dehydration, and antibi-otic therapy with ceftriaxone for preventing bacte-rial translocation from the gastrointestinal tract to the bloodstream. A complete abdominal computed
Tungs’ Medical Journal 11 (2017) 108-112
Case Report
* Correspondence to: Dr. Min-Yung Kuo. Department of Surgery, Tungs’ Taichung MetroHarbor Hospital, Taichung, Taiwan, No. 699, Sec. 8, Taiwan Blvd.,Wuqi Dist., Taichung City, 43503, Taiwan (R.O.C)

109Chun-Hsiang Chang et al. / Tungs’ Medical Journal 11 (2017) 108-112
Fig. 2 Computed tomography revealed pneumatosis intesinalis of proximal jejunum; with suspicion of incarcerated internal herniation and ischemic gangrene of jejunum small bowels.
Fig. 3 Upper GI and small bowel series revealed diffuse dila-tation with suspicious obstruction level in ileum.
(A)
Fig. 1 (A) Plain KUB with supine ap view revealed distension of stomach and dilated small bowel loops. (B) Plain abdomen with left decubital view revealed dilated small bowel loops in abdomen and scanty colon gas pattenn.
(B)

110 Chun-Hsiang Chang et al. / Tungs’ Medical Journal 11 (2017) 108-112
tomography (CT) showed pneumatosis intestinalis of the proximal jejunum and dilatation of the bowel loop (Fig. 2). In the following days, his clinical condi-tions improved without fever; however, these wors-ened on day 3 with further abdominal distension. We obtained upper gastrointestinal and small bowel series, which revealed a diffuse dilatation of the small intestine (Fig. 3). Owing to progressive small bowel obstruction, exploratory laparotomy was performed on day. At exploration, Meckel’s tip was attached to the retroperitoneum with internal loop formation, the small intestine from Meckel’s diverticulum to the ileocecal region was incarcerated into the internal loop, and an internal hernia was formed with isch-emic change and gangrene (Fig. 4A, 4B). Thus, ileo-colostomy was performed. Pathological analysis con-firmed Meckel’s diverticulum with gastric mucosa and a transmural infarct. The patient recovered without complications and was discharged on postoperative day 8. The postoperative course was uneventful.
Discussion
Meckel’s diverticulum is asymptomatic in the majority of the cases. Despite advances in radiolog-ical techniques, Meckel’s diverticulum remains dif-ficult to diagnose, and a preoperative diagnosis is made only in 4% of the cases[4]. Owing to insignificant findings in laboratory tests or CT scans, surgery for Meckel’s diverticulum tends to be delayed.
The most common small bowel obstruction
related to Meckel’s diverticulum is intussusception or invagination, with Meckel’s diverticulum being the lead point, and other obstructions include volvulus around fibrous bands adherent to the umbilicus, inflammatory adhesions, Littre’s hernias, and diver-ticular strictures[5,6]. Axial torsion of Meckel’s diver-ticulum is a rare complication resulting from the axial twisting of Meckel’s diverticulum around its narrow base, which is related to the attachment of the diver-ticulum to the umbilicus or to the ileal mesentery[7,8].
Because of unspecific symptoms associated with the complications of Meckel’s diverticulum, preop-erative diagnosis is challenging, even with a CT scan. Therefore, early intervention with exploratory lapa-rotomy can be helpful. In our case, the use of explor-atory laparotomy allowed the complications of Meck-el’s diverticulum to be accurately diagnosed early and reduced the possibility of morbidity and mor-tality resulting from an unclear etiology of an acute abdomen. In other cases, diagnostic laparoscopy yielded the same outcome, but the postoperative wound was smaller[9]. Diagnostic laparoscopy can help avoid delayed surgery, which carries substantial risks[10].
In conclusion, axial torsion of Meckel’s divertic-ulum is very rare, and the preoperative diagnosis is challenging. When the cause of small bowel obstruc-tion is unknown, early exploratory laparotomy can help in the early diagnosis and treatment of Meckel’s diverticulum.
Fig. 4 (A) Meckel’s diverticulum torsion with gangrenous formation. (B) Small intestines from Meckel’s diverticulum to ileocecal region incarcerated into internal loop caused incarcerated internal herniation
(A) (B)

111Chun-Hsiang Chang et al. / Tungs’ Medical Journal 11 (2017) 108-112
References
1. Limas C, Seretis K, Soultanidis C, Anagnostoulis S. Axial torsion and gangrene of a giant Meckel’s diverticulum. J Gastrointestin Liver Dis 2006; 15: 67-8.
2. Tassinari D, Cimatti AG, Tani G, Lima M. A common case of gastroenteritis in a child followed by an axial torsion of Meckel diverticulum: a rare and unusual complication. BMJ Case Rep 2013 22; 2013. pii: bcr2012006656. doi: 10.1136/bcr-2012-006656.
3. Hadeed AA, Azar RR, Azar NN, Benninger B. Meckel’s diverticulum complicated by axial torsion and gangrene. J Surg Case Rep 2015; 3: 1-3
4. Ludtke FE, Mende V, Kohler H, Lepsien G. Incidence and frequency or complications and management of Meckel’s diverticulum. Surg Gynecol Obstet 1989; 169: 537-42.
5. Dumper J, Mackenzie S, Mitchell P, Sutherland F, Quan ML, Mew D. Complications of Meckel’s diverticula in adults. Can J Surg 2006; 49: 353-7.
6. Cartanese C, Petitt Ti, Marinelli E, Pignatelli A, Martignetti D, Zuccarino M, et al. Intestinal obstruction caused by torsed gangrenous Meckel’s diverticulum encircling terminal ileum. World J Gastrointest Surg 2011; 3: 106-9.
7. Malhotra S, Roth DA, Gouge TH, Hofstetter SR, Sidhu G, Newman E. Gangrene of Meckel’s diverticulum secondary to axial torsion: a rare complication. Am J Gastroenterol 1998; 93: 1373-5.
8. Kiyak G, Ergul E, Sarikaya SM, Kusdemir A. Axial torsion and gangrene of a giant Meckel’s diverticulum mimicking acute appendicitis. J Pak Med Assoc 2009; 59: 408-9.
9. Chan KW, Lee KH, Mou JW, Cheung ST, Tam YH. Lapa-roscopic management of complicated Meckel’s diver-ticulum in children: a 10-year review. Surg Endosc 2008; 22: 1509-12.
10. Nose S, Okuyama H, Sasaki T, Nishimura M. Torsion of Meckel’s diverticulum in a child. Case Rep Gastroenterol 2013; 7: 14-8.

112 Chun-Hsiang Chang et al. / Tungs’ Medical Journal 11 (2017) 108-112
複雜性梅克爾憩室初始以小腸阻塞呈現
張竣翔 郭敏勇*
童綜合醫院 外科部
受文日期:民國 105年 04月 08日;接受刊載:民國 106年 03月 13日
摘要
梅克爾憩室,是由於卵黃管不完全的退化所形成的,而它也是最常見的腸胃道的先天性異常。
梅克爾憩室的軸向旋轉是很罕見的併發症,尤其在兒童族群裡。由於梅克爾憩室,不論在實驗室檢驗或
者是電腦斷層掃描,均不具有特異性的表現,所以在手術的介入時間點上,往往有所延誤。在我們的個
案裡,剖腹探查可以對於梅克爾憩室做出早期的診斷及治療。
關鍵詞:梅克爾憩室、軸向旋轉
*通訊作者:郭敏勇醫師 童綜合醫療社團法人童綜合醫院外科部 43503台中市梧棲區台灣大道八段 699號

113
A Different Method for Treating Pseudoarthrosis of the Surgical Neck of the Humerus: A Case Report
Sheng-Chi Chen*, Shao-keh Hsu
Department of orthopedics, Tung’s Taichung MetroHarbor Hospital
Received: Nov. 25, 2015; Accepted: Mar. 02, 2016
Abstract
Pseudoarthrosis of the surgical neck of the humerus is a very rare condition which comprises humeral neck fracture nonunion with deficient bone stock. Treatment can be challenging, and many surgical techniques have been described in the literature, but each technique has its own drawbacks. We describe a new and far simpler technique to treat pseudoarthrosis of the surgical neck of the humerus using a femoral head allograft, bone marrow aspiration, and proximal humerus locking plate fixation, which resulted in both bony union and markedly improved clinical outcomes.
Key words: Pseudoarthrosis, surgical neck of the humerus, allograft, bone marrow aspirate, locking plate
Introduction
Pseudoarthrosis of the surgical neck of the humerus is a rare condition which can be associ-ated with pain and major limitation of shoulder func-tion[1,2]. Treatment is challenging owing to excessive fracture site mobility, humeral head cavitation with deficient bone stock, concomitant osteoporosis, and head-shaft size mismatch[3].
Both reconstructive and replacement type sur-geries have been described; however, reconstructive methods with any form of open reduction internal fixation and bone grafting are preferred because the reported results of replacement surgeries have been poor[3].
Several reconstructive techniques were described, such as impaling the shaft onto the head[4], placing a tension suture through the rotator cuffs[4,5], or using an intramedullary corticocancellous auto-graft to improve construct stability[6]. However, each technique has its own drawbacks, such as donor site
morbidity, ongoing nonunion, and the need for metal ware removal[4,5,6].
Here we present a case of pseudoarthrosis of the surgical neck of the humerus treated with a com-bination of femoral head allograft, bone marrow aspi-rate, and a locking plate, which resulted in bony union and improved clinical outcomes. Combined allograft and bone marrow aspirate have previously been described for treating long bone nonunions[7], but, to the best of our knowledge, its use in treating pseudo-arthrosis of the surgical neck of the humerus has not been reported in literature.
Case Report
A 63-year-old housewife fell on her right shoulder in March 2014 with resultant right humerus surgical neck fracture, which was initially treated conserva-tively. She presented to our clinic 4 months later com-plaining of ongoing pain and an inability to elevate her shoulder. Clinically, she had an abduction of only 30° and forward elevation of only 40°. Radiographs of her right shoulder showed pseudoarthrosis of the right humeral neck with resorption and cavitation of the head fragment (Fig. 1). The risks and benefits of sur-gical management were discussed with her in detail.
Tungs’ Medical Journal 11 (2017) 113-117
Case Report
* Correspondence to: Dr. Sheng-Chi Chen. Department of orthopedics, Tungs’ Taichung MetroHarbor Hospital, Taic-hung, Taiwan, No. 699, Sec. 8, Taiwan Blvd., Wuqi Dist., Taic-hung City, 43503, Taiwan (R.O.C)

114 Sheng-Chi Chen et al. / Tungs’ Medical Journal 11 (2017) 113-117
The deltopectoral approach was utilized to expose the fracture after the skin incision was made. There was severe cavitation of the head fragment with little cancellous bone remaining, leaving a near egg-shell head wrapped around by rotator cuffs. The fibrous scarring tissue was excised, and both ends of the fractured surface were decorticated with a high-speed burr.
An allograft femoral head was prepared by removing its overlying cartilage and shaped so that it could be fitted into the head fragment cavity. Bone marrow aspirate was obtained simultaneously from the ipsilateral iliac crest using a large bore needle and syringe. The prepared allograft was then socked in the bone marrow aspirate before being placed into the head fragment cavity. The head fragment containing the allograft was reduced onto the shaft and tempo-rarily fixed with two Kirschner wires. Once a satisfac-tory reduction was confirmed using an image inten-sifier, the rotator cuffs were sutured onto the shaft using Ethibond through drill holes. Lastly, a proximal humerus locking plate was applied with the proximal locking screws purchasing into both the head frag-ment and allograft. The two Kirschne wires were then removed, and the stability and range of motion of the shoulder was checked. The wound was irrigated with saline, and the remaining bone marrow aspirate was injected into the fracture site before wound closure. An immediate postoperative radiograph confirmed satisfactory overall alignment. (Fig. 2)
Postoperative management included 24 h of prophylactic antibiotics and 2 days of hospital stay. The shoulder was immobilized in a brace for 6 weeks with gentle pendulum exercises initiated at home after 2 weeks. Active shoulder range of motion was initiated at 8 weeks.
At 2 months, the femoral head allograft seemed to be incorporated into both the head and shaft
Fig. 2 Immediate post-operative radiograph confirmed satis-factory implant and allograft position with good overall align-ment.
Fig. 1 Anteroposterior radiograph of right shoulder joint with shoulder joint in (A) internal rotation (B) external rotation showing deficient bone stock with humeral head cavitation.
(A) (B)

115Sheng-Chi Chen et al. / Tungs’ Medical Journal 11 (2017) 113-117
properly, with only a fine fracture line visible over the shaft-graft junction (Fig. 3). At 5 months, the right shoulder was pain-free and had regained motion to a 110° of abduction and 100° of forward elevation. Radiographs taken at the time showed complete bony union (Fig. 4).
Discussion
Nonunion of the surgical neck of the humerus is an uncommon condition. It can be divided into two types: nonunion with preserved bone stock, more commonly observed, and nonunion with deficient bone stock, the other rare type which is termed as pseudoarthrosis[1,2].
Treatment of pseudoarthrosis can be chal-lenging; therefore, several methods of reconstruc-tion were described. Scheck[4] described a technique of improving fracture stability by impaling the distal fragment into the head followed by tension-band wiring of the rotator cuffs to the shaft and use of a lateral extramedullary strut to enhance overall sta-bility. However, most of these cases needed spica immobilization and secondary implant removal. Neer and Rockwood[5] reported better union rates with the use of the tension band technique with intra-medullary rods to improve stability through fracture site compression. However, 20% of their patients
Fig. 4 Anteroposterior right shoulder radiograph taken at 5 months showing complete bony union.
Fig. 3 Two months post-operative radiographs showing good incorporation of allograft with head and shaft fragment and new bone formation. (A) Anteroposterior and (B) lateral view.
(A) (B)

116 Sheng-Chi Chen et al. / Tungs’ Medical Journal 11 (2017) 113-117
had ongoing nonunion and 80% required hardware removal because of irritation. An intramedullary bone peg technique with a corticocancellous auto-graft harvested from the patient’s iliac crest, anterior tibia, or fibula to supplement fixation was described by Walchet al.[6]; this technique showed a very high union rate of 96%. However, it was associated with significant donor site morbidity: 50% of the patients developed pathological fracture after bone har-vesting from the anterior tibial crest. Some authors used the iliac crest autograft alone, but they also reported a high incidence of donor site morbidity with a significant percentage of the patients experi-encing postoperative donor site pain[8.9.10].
In our case, we used a much more simple tech-nique to treat pseudoarthrosis of the surgical neck of the humerus. The femoral head allograft used pro-vided good medial support against varus collapse of the humeral head, and the construct was further strengthened by the use of a locking plate. The com-bined allograft and bone marrow aspirate helps promote new bone formation without the associated donor site morbidity secondary to autograft har-vesting. However, more cases should be performed to accurately assess the limitations and potential complications of this new technique.
Conclusion
Locking plate fixation combined with femoral head allograft and bone marrow aspirate appears to be a valid option for treating pseudoarthrosis of the surgical neck of the humerus.
References
1. Einarsson F. Fracture of the upper end of the humerus.Discussion based on the follow-up of 302 cases. Acta Orthop Scand Suppl. 1958; 32: 1-215.
2. Mills KL. Severe injuries of the upper end of the humerus. Injury. 1974; 6: 13.
3. Antuna SA, Sperling JW, Sánchez-Sotelo J, Cofield RH. Shoulder arthroplasty for proximal humeral nonunions. J Shoulder Elbow Surg. 2002; 11: 114-121.
4. Scheck M. Surgical treatment of nonunions of the surgical neck of humerus. Clin Orthop Relat Res. 1982; 167: 255-259.
5. Walch G, Badet R, Nové-Josserand L, Levigne C. Nonunions of the surgical neck of the humerus: Surgical treatment with an intramedullary bone peg, internal fixation, and cancellous bone grafting. J Shoulder Elbow Surg. 1996; 5: 161-168.
6. Neer CS II, Rockwood CA. Fractures and dislocations of the shoulder. In: Rockwood CA Jr, Green DD eds. Frac-tures, vol. 1. Philadelphia, PA: J. B. Lippincott, 1975: 610.
7. Scaglione M, Fabbri L, Dell’Omo D, Gambini F, Guido G. Long bone nonunions treated with autologous concen-trated bone marrow-derived cells combined with dried bone allograft. Musculoskeletal Surg. 2014; 98 (2): 101-106.
8. Healy WL, Jupiter JP, Kristiansen TK, et al. Nonunion of the proximal humerus. A review of 25 cases. J Orthop Trauma. 1990; 4: 424-43.
9. Norris TR, Turner JA, Bovill D. Nonunion of the upper humerus: an analysis of the etiology and treatment in 28 cases. In: Post M, Morrey BF, Hawkins RJ eds. Surgery of the Shoulder. St Louis, MO: Mosby, 1990: 63-67.
10. Ring D, McKee M, Perey B, et al. The use of a blade plate and autogenous cancellous bone graft in the treatment of ununited fractures of the proximal humerus. J Shoulder Elbow Surg. 2001; 10: 501-507.

117Sheng-Chi Chen et al. / Tungs’ Medical Journal 11 (2017) 113-117
治療肱骨外科頸假性關節的另類方法:病例報告
陳聖祺* 徐少克
童綜合醫院 骨科部
受文日期:民國 104年 11月 25日;接受刊載:民國 105年 03月 02日
摘要
肱骨外科頸假性關節是一種非常罕見的疾病,它包括肱骨外科頸骨折不癒合合併骨量的缺乏。治療
通常具有挑戰性,文獻中記載了許多手術治療的技術,但每個都有各自的缺點。我們採用了一個新的簡
單技術治療肱骨外科頸假性關節且得到不錯的結果,不但骨折處癒合並顯著的改善了病人的臨床症狀。
關鍵詞:假性關節、肱骨外科頸骨折、異體骨、骨髓穿刺、互鎖式鋼板
*通訊作者:陳聖祺醫師 童綜合醫療社團法人童綜合醫院骨科部 43503台中市梧棲區台灣大道八段 699號

118
Cervical Trachea Transection after Neck Blunt Trauma: A Case Report
Pei-Hung Liao1, Ming- Sheng Lin1,*, Yung-Wei Chiu1, Chao-Hsin Wu1, Yung Wei Tung2
1Department of Emergency Medicine, 2Division of Thoracic Surgery, Department of Surgery, Tungs’ Taichung Metro Harbor Hospital, Taiwan
Received: Feb. 05, 2016; Accepted: Apr. 06, 2016
Abstract
Tracheal transection is relatively rare but can occur as a result of fatal chest injury and neck blunt trauma. Emergency diagnosis and management is challenging for emergency physicians because of rapid respiratory distress and hypoxemia. Here we describe a 37-year-old male with total tracheal transection due to neck blunt injury resulting from a road traffic accident. An endobronchial tube was inserted because of rapid respiratory distress. Bronchoscopy of the endotracheal tube confirmed a tracheal rupture, and the patient was moved to the operating room for surgical tracheal repair and reconstruction with tracheostomy. Timely and appropriate airway management is essential for a favorable outcome. The present case describes the importance of early airway assessment for patients with occult traumatic tracheobronchial injury.
Key words: Blunt trauma, Tracheal transection
Introduction
Tracheobronchial injury (TBI) commonly occurs after neck and chest blunt trauma or iatrogenic pos-tintubation tracheal injury. It is a rare, serious event accounting for approximately 0.5%–2% of thoracic and neck blunt trauma and 14% of penetrating neck injuries[1]. In most cases, TBI is not recognized early because of a lack of specific clinical signs and radio-logic manifestations. Delayed diagnosis of tracheal injury may be life-threatening and is associated with a high mortality rate because of severe complica-tions such as mediastinitis, ventilator failure, sepsis, airway stenosis, bronchiectasis, pulmonary infec-tions, and permanent pulmonary function impair-ment. The location of the tracheal transection can be subdivided two groups: above clavicles (cervical tracheal) and below clavicles (thoracic tracheal)[1,8].
linical manifestations of TBI include subcutaneous emphysema, inspiratory stridor, and hoarseness of voice. Tracheal transections are usually accompanied by vascular injury, esophagus injury, and surrounding tissue injury; therefore, it is important to also consider the recurrent laryngeal nerves and spinal injuries[2].
Case Report
A 37-year-old patient was involved in a high-velocity road traffic accident that involved crashing his car into a telegraph pole. The patient was uncon-scious at the scene (Coma Glasgow Scale = 8/15 E2V2M4) and presented with respiratory distress and neck blunt trauma with a huge hematoma. In addition, an 18-cm-deep laceration and type IIIC open fracture was noted on the right tibia/fibula. According to the retrieval team, he was sitting and leaning forward on the dashboard with his seat belt unfastened. He had a hoarse voice, was unable to speak, and occasionally spit blood. He was unable to lie flat and showed increased dyspnea and aphonia
Tungs’ Medical Journal 11 (2017) 118-122
Case Report
* Correspondence to: Ming- Sheng Lin, Department of Emer-gency Medicine, Tungs’ Taichung MetroHarbor Hospital, No. 699, Sec. 8, Taiwan Boulevard, Wuchi, Taichung, 43503, Taiwan (R.O.C.)

119Pei-Hung Liao et al. / Tungs’ Medical Journal 11 (2017) 118-122
with oxygen saturation of approximately 85%. He was administered supplementary oxygen via a face mask and sent to the nearest community hospital by ambulance. On arrival, the anterior compartment of the neck was diffusely swollen and tender. Palpation of the laryngotracheal skeleton below the cricoid car-tilages revealed that it was movable and depressed, and palpable crepitus was present bilaterally around the soft tissue of the neck. The initial diagnosis was traumatic tracheal injury due to rapid airway compro-mise. However, tracheostomy or cricothyrotomy were not possible because of a lack of surgical expertise at the hospital. The patient reached critical status, and a size 7.0 cuffed oral endotracheal tube was inserted to secure the airway to maintain his airway as an emer-gency procedure.
Brain computed tomography (CT) scan per-formed at the community hospital revealed no intra-cranial hemorrhage. Furthermore, no alcohol was detectable in serum. The rapid desaturation and tem-porary loss of consciousness may have been related to development of hypoxia and breathing difficul-ties. Details of the history of the injury and valuable information were provided by phone call. The patient was transferred to the emergency department at our hospital 2 h later. Subcutaneous emphysema around the neck progressed and chest radiography revealed massive pneumomediastinum with soft tissue emphysema bilaterally across the lower neck. Cervicothoracic CT scan confirmed extrapulmonary free air from the cervix to the mediastinum and cer-vical trachea transection above the thoracic inlet. The distal end of the trachea was completely sepa-rated at the level of the first to the third tracheal ring. Endotracheal tube was secured to the distal end of the trachea. Bronchoscopy via the endotracheal tube confirmed laceration of the membrane portion of the tracheal rings with transection and gross supralaryn-geal to laryngeal edema; therefore, emergent neck exploratory surgical intervention was required. A collar incision of approximately 8 cm was performed along the stab wound. By blunt dissection, the upper flap was elevated to the notch of the thyroid cartilage and the lower flap to the sternal notch. The pretra-cheal soft tissue was separated and the trachea was exposed. Total transection of the trachea was found between the first and third membrane portion of tracheal rings. The two tracheal wounds were con-nected together and an Armond tube was placed into
the distal trachea for ventilation. The trachea was repaired with 3-0 PDS sutures. Sterile water was irri-gated to check for any air leakage or bleeding. Due to defects in the cartilaginous part of the tracheal ring, a 7-mm tracheostomy tube was indicated and placed for postoperative management and ventilator support, with a drain placed over the pretracheal area. In addi-tion, esopahgoscopy was performed, with no specific findings. The subcutaneous emphysema and pneu-momediastinum gradually resolved after chest tube drainage. The patient also received external fixation
Fig. 2 CT scan showing above thoracic inlet cervical trachea extensive transection with paratracheal air and soft-tissue air around thoracic trachea.
Fig. 1 Chest radiograph showing massive pneumomedias-tinum and soft tissue emphysema over bilateral lower neck.

120 Pei-Hung Liao et al. / Tungs’ Medical Journal 11 (2017) 118-122
for the tibia/fibula open fracture and open reduction and internal fixation with split-thickness skin grafts for the huge skin defect. The patient was alert and conscious after surgery recovery, and no secondary brain insults were found following head injury. There was no respiratory infection or mediastenitis, and the patient’s recovery was uneventful. Repeat bronchos-copy performed on the postoperative day 10 dem-onstrated suspected bilateral recurrent laryngeal nerve injury due to vocal cord immobility. Injury to the recurrent nerve may have been related to laryn-gotracheal separation or initial blunt trauma. Perma-nent recurrent laryngeal nerve injury is avoidable fol-lowing these injuries. Tracheostomy decannulation failed following fully independent breathing due to immobile and paralyzed vocal cords. The patient was discharged on postoperative day 29 and returned to clinic for follow-up. He was doing well and showed no evidence of respiratory compromise. Laryngeal nerve damage repair was suggested by an otolaryngologist; however, the patient was reluctant.
Discussion
Blunt traumatic tracheal laceration injury is rare, and reports of complete tracheal transection are uncommon because of rapid hypoxemia and high
mortality at the scene of the accident, implying that most individuals die before reaching hospital. Among those arriving at hospital alive, young age is predomi-nant; however, the recorded mortality rate is approx-imately 30%–60%. Therefore, timely airway manage-ment is important and can be lifesaving[1,2]. Initial minor injury is not easily identified, and delayed recognition is associated with poor prognosis. Emer-gency physicians should be alert to nonspecific clin-ical signs, such as dyspnea, hoarseness, persistent cough or hemoptysis, and cyanosis. Subcutaneous emphysema and aphonia are important indicators of thoracic tracheal injuries following blunt or penetra-tion injury[2,9]. Neck blunt trauma is frequently com-bined with esophagus injury, spinal cord injury, recur-rent laryngeal nerve injury, and carotid vessel injury. Most complete tracheal transection injuries occur at the level of the cricoid cartilage because the cricotra-cheal ligament is composed of a thin elastic mem-brane and is relatively weak. A systematic clinical approach may identify these as supraglottic, glottic, or subglottic, and assessment of injured structures can identify hyoid bone, thyroid cartilage, cricoid cartilage, or arytenoids. Schaefer–Fuhrman classifi-cation is recently a more commonly referenced clas-sification for laryngotracheal injury, which separates the degree of injury into five groups, where total complete tracheal separation is classified as grade 5, as in the present case[2,5]. Early assessment of laryn-gotracheal injury may focus on primary survey of the airway, breathing, and circulation. Therefore, estab-lishing a definitive airway and protecting the cervical spine should be a priority, and adequate and spon-taneous ventilation should be maintained until laryn-goscopy or bronchoscopy can identify the location of the injury.
The mode of initial airway management remains controversial and needs to be tailored to suit each individual case. Compared with intubation, trache-ostomy is preferred for primary airway management because intubation may further aggravate the laryn-geal injury. However, if the patient is unstable and tracheostomy or cricothroidotomy are not available, an endotracheal tube can still maintain positive ven-tilation and oxygenation under adequate inflation of the cuff distal to the tear site[3,5]. Furthermore, if the injury is at the distal tracheal or bronchial level, emer-gency tracheostomy is of no benefit under local anes-thesia. Initial chest X-ray and lateral cervical spine
Fig. 3 Diffuse ecchymosis of neck soft tissue with total tran-section of trachea between membrane portion of 1st to 3rd tracheal rings .Orally Endo-tracheal tube was inserted at lower part of completely transected trachea.

121Pei-Hung Liao et al. / Tungs’ Medical Journal 11 (2017) 118-122
X-ray examinations are essential to screen possible TBI-related presence of pneumothorax, subcutaneous emphysema, pneumomediastinum, or abnormal air surrounding the mainstem bronchi. Neck-to-chest CT scan should be used for high sensitivity tracheal tran-section diagnosis (up to 85%) and to provide further associated unsuspected thoracic and laryngeal tissue injuries[4]. However, CT scan should not delay the time of surgical exploration and is contraindicated in hemodynamically unstable trauma patients and in those with unstable airway status. However, bron-choscopy is the best diagnostic tool to determine the location and definitive extent of the injury. Flexible bronchoscopy is a useful guide for intubation to the distal tracheal segment. Small lacerations without obvious air leak might be conservatively managed successfully, and treatment may include drainage of air secretions and adequate mechanical ventilation with minimal pressure[5]. Following confirmation of trachea transection with transmural tear of more than one-third of the circumference or of more than 1 cm using bronchoscopy and air leak needing posi-tive pressure ventilation, emergency tracheal primary repair is the treatment of choice[6]. The best manage-ment is complete repair of the trachea with end-to-end anastomosis using a nonabsorbable suture mate-rial. This may avoid tracheostomy; however, in our patient, the trachea was lacerated, with defects in the cartilaginous tracheal ring and complete anastomosis was not possible. Therefore, tracheostomy was indi-cated. Removal of the tracheostomy tube along with reconstruction was performed later. Tracheostomy after airway reconstruction may be performed under the following conditions: (1) obstruction of the mouth or throat; (2) breathing difficulty caused by edema, injury, or pulmonary conditions; (3) airway recon-struction following tracheal or laryngeal surgery; (4) airway protection from secretions or food because of swallowing problems; and (5) long-term need for ven-tilator support.
In the neck, trachea transection laparotomy management should avoid recurrent laryngeal nerve damage. After surgery, the patient should be instructed to rest the voice for at least 2 days and take antireflux and antitussive medication to prevent irri-tation and scar formation. Laryngostroboscopy and laryngeal electromyography are the most common clinical evaluation methods used to determine the main underlying pathology. Injection laryngoplasty
with hyaluronic acid may improve the quality of the voice during the recovery period. To improve revers-ible injuries and vocal cord paralysis, corrective pro-cedures may be delayed for at least 6 months unless the nerve was definitely transected. Surgical treat-ment options include medialization (most common) and reinnervation. Tracheotomy may be required to treat severe vocal cord paralysis. Cordotomy and arytenoidectomy are the most commonly performed surgical procedures because they enlarge the airway and may permit decannulation of tracheostomy. Pro-phylactic antibiotics could prevent secondary infec-tion. Long-term complications, such as tracheal ste-nosis and dysphonia[7], may occur. Tracheal stenosis may be managed by secondary surgical reconstruc-tion or interventional bronchoscopy. Recurrent laryn-geal nerve injury-related dysphonia requires speech and language therapy[8,9].
In conclusion, in patients with complete tracheal transection, prognosis is mostly dependent on early diagnosis and initial airway management in the emer-gency room. Emergent airway management is the most important, and bronchoscopy intervention and immediate neck exploration are lifesaving and should not be delayed.
References
1. Karmy-Jones R, Wood DE. Traumatic injury to the trachea and bronchus. Thorac Surg Clin 2007; 17: 35-46.
2. Fuhrman GM, Stieg 3rd FH, Buerk CA. Blunt laryngeal trauma: classification and management protocol. J Trauma 1990; 30: 87-92.
3. Norwood SH, McAuley CE, VallinaVL, Berne JD, Moore WL. Complete cervical tracheal transection from blunt trauma. JTrauma 2001; 51: 568-571.
4. Chen JD, Shanmuganathan K, Mirvis SE, Killeen KL, Dutton RP. Using CT to diagnose tracheal rupture. AJR Am J Roentgenol 2001; 176(5): 1273-1280.
5. Chang CY, Cheng SL, Chang SC. Conservative treatment of severe tracheal laceration after endotracheal intubation. Respir Care 2011; 56(6): 861-862.
6. Ye D, Shen Z, Zhang Y, Qiu S, Kang C. Clinical features and management of closed injury of the cervical trachea due to blunt trauma. Scand J Trauma Resusc Emerg Med 2013; 21(1): 60.
7. Shweikh A. Laryngotracheal separation with pneumo-pericardium after a blunt trauma to the neck. Emerg Med J. 2001; 410-411.
8. O’Neill JP, Shine N, Timon C. Complete traumatic laryngo-tracheal separation. Irish medical journal.2009; 102(9): 291-292
9. Barmada H, Gibbons JR. Tracheobronchial injury in blunt and penetrating chest Trauma. Chest 1994; 106(1): 74-78

122 Pei-Hung Liao et al. / Tungs’ Medical Journal 11 (2017) 118-122
頸部鈍傷導致氣管斷裂:個案報告
廖培宏1 林明聖1,* 邱永偉1 吳肇鑫1 童詠偉2
童綜合醫療社團法人童綜合醫院 1急診部 2胸腔外科
受文日期:民國 105年 02月 05日;接受刊載:民國 105年 04月 06日
摘要
喉部氣管斷裂為罕見的胸頸部鈍傷併發症,由於快速呼吸窘迫會造成立即性腦部缺氧,所以立即診
斷及處置對於急診醫護人員是一大挑戰,我們報告一名 37歲男性因車禍造成多重器官創傷合併氣管完全斷裂案例,經緊急呼吸建立且支氣管鏡確認診斷後,立即接受氣管修復重建合手術和氣切造口,術後恢
復順利。緊急且適當的呼吸道處置對於預後有很大的關係,早期的呼吸道氣管創傷並不容易被查覺,所
以早期察覺診斷及呼吸道建立是最重要的。
關鍵詞:胸頸部鈍傷、氣管斷裂、氣道處置
*通訊作者:林明聖醫師 童綜合醫療社團法人童綜合醫院急診部 43503台中市梧棲區台灣大道八段 699號

123
Neonatal Femoral Fracture: A Case Report
Hui-Chien Lai*
Department of Pediatrics, Show Chwan Memorial Hospital, Changhua City, Taiwan
Received: Mar. 01, 2016; Accepted: May. 24, 2016
Abstract
Birth-related fractures are relatively uncommon. They generally occur during a difficult delivery, particularly with breech presentation. In neonates, femoral fractures are rare. We encountered a female neonate with a femoral fracture who had been delivered by cesarean section due to breech presentation. The gestational age was 38 weeks, and the birth weight was 2.885 kg. A left footling presentation was noted during delivery, and limited range of motion of the right leg was found soon after delivery. An X-ray revealed a fracture of the right femoral shaft with slight displacement. A cast was applied to the right thigh immediately after orthopedic consultation. However, it was replaced with Bryant traction of both legs, because the fracture became more displaced and there was persistent painful swelling of the thigh. An X-ray showed good alignment with callus formation and no shortening or deformity of the right femur at four weeks of age.
Key words: femoral fracture, Bryant traction, cesarean section
Introduction
Femoral fractures in neonates are relatively uncommon. Predisposing factors include twin preg-nancies, breech presentation, and fetal osteopo-rosis. Infants feel pain and discomfort, which causes parental distress, and the hospital stay is longer. Fixa-tion of femoral shaft fractures in newborns presents a difficult challenge to the orthopedic surgeon. We encountered a female neonate with a right femoral fracture who was delivered by cesarean section (C/S) due to breech presentation.
Case Report
A woman complaining of frequent uterine con-tractions for four weeks before delivery was admitted for tocolysis. Prenatal examination on admission revealed a breech presentation. The mother had fre-quent labor pains on the morning of delivery, which
was carried out by C/S due to breech presentation. The gestational age was 38 weeks. A left footling breech was noted during delivery. The baby’s birth weight was 2.885 kg, and the Apgar scores were 8 and 9 at 1 and 5 min, respectively. Immediately after delivery, we noted limited range of motion of the right leg; therefore, the neonate was transferred to the sick baby room for further evaluation. Physical examination revealed normal vital signs, clear breath sounds, normal heart beat with no murmur, and a soft and flat abdomen. There was a tender swelling of the right thigh. Laboratory examinations showed a white blood cell count of 16,200/cmm and a hemo-globin level of 17.0 g/dL. An X-ray revealed right femoral shaft fracture with slight displacement and a radiolucent line in the left femoral shaft. A cast was applied to the right thigh after orthopedic consulta-tion. However, there was persistent painful swelling of the thigh, and the fracture became more displaced (Fig. 1). Therefore, the cast was replaced with Bryant traction of both legs (Fig. 2). On a follow-up X-ray 18 days later, overriding callus formation of the fracture was noted. Good alignment with callus formation and no shortening or deformity of the right femur was
Tungs’ Medical Journal 11 (2017) 123-126
Case Report
* Correspondence to: Dr. Hui-Chien Lai, Department of Pediat-rics, Show Chwan Memorial Hospital, No. 542, Sec. 1, Chung-Shang Rd., 886, Taiwan (R.O.C.)

124 Hui-Chien Lai / Tungs’ Medical Journal 11 (2017) 123-126
noted on X-ray when the infant was four weeks old (Fig. 3).
Discussion
The reported incidence of birth-related fractures varies from less than 1–6 per 1000 live births[1,2], the most common type being fracture of the clavicle[3]. Previous studies have shown that planned C/S for term breech pregnancies lead to significant reduc-tions in perinatal and infant mortality[4]. However, while C/S avoids the danger of head entrapment, it does not reduce the risk of long bone trauma because the delivery maneuvers for a breech presentation are similar in both C/S and vaginal delivery[5]. Femoral
fractures resulting from birth injuries are rare, with a reported incidence of 0.13 per 1,000 live births[6]. Predisposing factors include twin pregnancies, breech presentation, and fetal osteoporosis (including that due to prematurity, osteogenesis imperfecta, or disuse osteoporosis)[6,7]. The typical pattern of neonatal femoral fracture is a spiral fracture in the proximal half of the diaphysis, but it may occur in the epiphysis [8]. Sudden or forced traction of limbs during delivery may cause femoral fracture[8].
The presentations of neonatal femoral fracture are soft tissue swelling, knee stiffness, focal tender-ness, and irritability. In our case, we noted limited range of motion of the right leg immediately after delivery, and after a few hours after birth, there was
Fig. 1 Fracture at the right femoral shaft with mild displace-ment (A). More displacement of right femoral shaft fracture after cast fixation (B).
Fig. 2 Bryant traction. Note improvised use of infusion stands to hold traction weights.
Fig. 3 Well aligment with callus formation without deformity of the right femur.

125Hui-Chien Lai / Tungs’ Medical Journal 11 (2017) 123-126
a tender swelling of the thigh. However, a fracture may be asymptomatic and inapparent on an imme-diate postnatal examination, only to be discovered later, as described by Morris et al.[6]; they reported a mean time to diagnosis of 6.3 days (range 1–21 days). A crack may be caused by the previous production process [9].
Neonatal femoral fractures pose a challenge to the orthopedic surgeon. The recommended treat-ment modes include a spica cast, the Pavlik harness, and Bryant traction[6]. Casting may be complicated by malalignment, as was the initial situation in our case, requiring a change of cast or discontinuation of casting altogether. Casts may also result in skin exco-riation or ulceration. The Pavlik harness addresses the flexed, abducted, and externally rotated position of the proximal fragment, but a poorly fitting harness can lead to femoral nerve palsy and avascular necrosis of the hip. Bryant traction is applied without any spe-cialized equipment, using simple devices available in any neonatal unit. Givon et al. reported that treating infants in the hospital with Bryant traction allows the family to adjust better rather than having the baby at home in a Pavlik harness[10]. The outcome of neonatal femoral fracture is excellent, with evidence of callus formation usually examined on a follow-up X-ray. Clinical evidence of fracture healing was obvious by four weeks in our case, which is consistent with pre-vious reports[8-10].
To prevent femoral fracture related to breech presentations during C/S delivery, forced traction on the extremities should be avoided by appropriate extension of the uterine incision, if necessary. After delivery, a femoral fracture should be suspected in the presence of clinical signs such as limitation of movement, knee stiffness, soft tissue swelling, focal tenderness, and irritability.
References
1. Perlow JH, Wigton T, Hart J, Strassner HT, Nageotte MP, Wolk BM. Birth trauma. A five-year review of incidence and associated perinatal trauma. J Reprod Med 1996; 41: 754-60.
2. Salomen IS, Uusitalo R. Birth injuries: incidence and pre-disposing factors. Z Kinderchir 1990; 45: 133-5.
3. Hsu TY, Hung FC, Lu YJ, Ou CY, Roan CJ, Kung FT, et al. Neonatal clavicular fracture: Clinical analysis of incidence, predisposing factors, diagnosis and outcome. Am J Peri-natol 2002; 19: 17-21.
4. Swedish Collaborative Breech Study Group. Term breech delivery in Sweden: mortality relative to fetal presenta-tion and planned mode of delivery. Acta Obstet Gynecol Scand 2005; 84: 593-601.
5. Vasa R, Kim MR. Fracture of the femur at cesarean section: case report and review of literature. Am J Perinatol 1990; 7: 46-8.
6. Morris S, Cassidy N, Stephens M, McCormack D, McManus F. Birth-associated femoral fractures: incidence and outcome. J Pediatr Orthop 2002; 22: 27-30.
7. Phillips RR, Lee SH. Fractures of the long bones occurring in neonatal intensive therapy units. BMJ 1990;301:225-6.
8. Jain R, Bielski RJ. Fracture of lower femoral epiphysis in an infant at birth: a rare obstetrical injury. J Perinatol 2001; 21: 550-2.
9. Matsubara S, Izumi A, Nagai T, Kikkawa I, Suzuki M. Femur fracture during abdominal breech delivery. Arch Gynecol Obstet 2008; 278: 195-7.
10. Givon U, Sherr-Lurie N, Schindler A, Blankstein A, Ganel A. Treatment of Femoral Fractures in Neonates. Isr Med Assoc J 2007; 9: 28-9.

126 Hui-Chien Lai / Tungs’ Medical Journal 11 (2017) 123-126
新生兒股骨骨折之病例報告
賴輝謙*
秀傳紀念醫院 小兒科
受文日期:民國 105年 03月 01日;接受刊載:民國 105年 05月 24日
摘要
生產時發生骨折較罕見,難產過程中可能會出這情形,尤其是臀位。新生兒股骨骨折更是罕見,本
篇報告一個剖腹產的女嬰股骨骨折之病例報告。胎齡 38週,出生時體重為 2885克,在分娩過程中注意到右腿關節活動範圍有問題,經 X光檢驗,右股骨幹有輕度骨折。於是與骨科會診,將她右大腿以石膏固定,因右股骨幹骨折,所以右大腿持久疼痛腫脹。運用科比牽引法後,在滿一個月時之 X光片,檢查顯示女嬰右股骨畸形幾乎沒有發生。
關鍵詞:股骨骨折、科比牽引、剖腹產
*通訊作者:賴輝謙醫師 秀傳紀念醫院小兒科 彰化市中山路一段 542 號

127
Sudden Onset of Blisters During Remisson from Stevens–Johnson Syndrome/Toxic Epidermal Necrolysis
Chu-Ju Hung1,2, Sheng-Wen Wu2,3, Chin-Yin Liu1,2,*
1Department of Dermatology, 3The Institute of Medicine, Chung Shan Medical University Hospital, Taiwan2Division of Nephrology, Chung Shan Medical University Hospital, Taiwan
Received: Mar. 10, 2016; Accepted: Jun. 24, 2016
Abstract
Stevens–Johnson syndrome/toxic epidermal necrolysis (SJS/TEN) is an extensive, life-threatening, drug-induced skin eruption. Common sequelae among survivors are xerotic eczema and heat intolerance, but recurrent blisters during the remission period are rare. Here, we report a 65-year-old women who presented with multiple blisters during remission from SJS/TEN. Miliaria crystallina, a self-limiting disease, was eventually diagnosed after excluding many diseases, such as autoimmune bullous disease, herpes virus infection, bullous impetigo, transient acanyholytic dermatosis, and SJS/TEN recurrence. We show that blisters occurred because of eccrine duct disruption and fluid accumulation beneath the necrotic epidermis and that this presentation can mimic SJS/TEN. It is important to consider this self-limiting condition to avoid unnecessary worry and intervention.
Key words: femoral fracture, Bryant traction, cesarean section
Introduction
Stevens–Johnson syndrome/toxic epidermal necrolysis (SJS/TEN) is a rare, life-threatening con-dition. Typically triggered by specific medications, including carbamazepine, allopurinol, antibiotics, and nonsteroidal anti-inflammatory drugs, they have an associated mortality of 5%–30%. Pathologically, they are characterized by widespread apoptosis of kera-tinocytes provoked by activation of cell-mediated cytotoxic reactions amplified by cytokines, mainly granulysin. Although recurrent blister eruption during remission is uncommon, when present, SJS/TEN recurrence, viral infection, and other bullous dis-eases should be taken into consideration.
Case Report
A 65-year-old woman was admitted to our ward because of carbamazepine-induced SJS/TEN. She had one episode of SJS/TEN a decade ago. At this instance, carbamazepine had been introduced to treat head-ache 3 days before the rash developed. On admission, we discontinued the carbamazepine and prescribed a short course of intravenous steroid (methylpredniso-lone, 40 mg every 8 hours) and nutritional support, fluid replacement, and wound dressings. The muco-sitis and detached skin gradually healed without further progression.
On day 7 of admission, there was a sudden onset eruption of asymptomatic blisters after the patient took a hot shower. Physical examination revealed multiple clear, drop-like crops of vesicles and bullae, measuring 2 mm–5 cm, accentuated on the neck, trunk, and arms (Fig. 1a–c). The largeest blisters con-tained clear fluid and were mainly present on the pre-viously damaged skin. Her oral mucosa and conjunc-tiva were spared, with no new targetoid lesions at any
Tungs’ Medical Journal 11 (2017) 127-130
Case Report
* Correspondence to: Chin-Yin Liu MD, Department of Derma-tology, Chung Shan Medical University Hospital, No. 110, Sec. 1, Chien-Kuo N. Road, Taichung 402, Taiwan (R.O.C.)

128 Chu-Ju Hung et al. / Tungs’ Medical Journal 11 (2017) 127-130
site. Laboratory data of complete blood count, meta-bolic panel, and test for antinuclear antibodies were normal. Tzanck’s smear from the vesicle base was negative, indicating that acantholytic or giant cells were absent. In addition, no bacteria were found by Gram staining, and skin biopsy revealed subcorneal blisters not only overlying the acrosyringium of the eccrine sweat duct but also between the re-epitheli-alization and upper necrotic skin (Fig. 2). Direct immu-nofluorescence (DIF) was negative for IgG, C3, IgM, and IgA.
Based on the cutaneous and pathological find-ings, we diagnosed miliaria crystallina. After diag-nosis, she was advised to wear loose-fitting, light clothes. The vesicles subsequently dried up and dis-appeared spontaneously within 16 hours (Fig. 1d);
Fig. 1 (A, B, C) multiple vesicles and bullae over the neck, chest, upper arms, abdomen and back. (D) 16 hours after cooling down, the vesicle and bullae disappeared spontaneously.
Fig. 2 Subcorneal blister overlies acrosyringium and between the previous necrotic skin and re-epithelialization (arrow: eccrine duct, star sign: previous necrotic skin, Hematoxylin & Eosin, original magnification 40x)

129Chu-Ju Hung et al. / Tungs’ Medical Journal 11 (2017) 127-130
however, but large areas of desquamation were observed on day 12.
Discussion
On the basis of the occlusion of the eccrine sweat duct at various levels of the skin, miliaria pres-ents in three forms: miliaria crystallina, miliaria rubra, and miliaria profunda. Miliaria crystallina is the most superficial form and is caused by obstruction or dis-ruption of sweat ducts in the stratum corneum. It is identified as a diffuse eruption of asymptomatic crops of clear, drop-like vesicles measuring 1–3 mm on a non-inflamed base, which appear preferentially on the head, neck, and trunk[1]. Large bullae and blis-ters are rare, but they have been reported in patients with intensive skin eruptions, such as those with staphylococcal scaled skin syndrome[2]. Therefore, when present, autoimmune bullous disease, herpes virus infection, bullous impetigo, Grover’s disease, and recurrent SJS/TEN should be considered. In the present case, however, pathology did not reveal acan-tholytic cells, giant cells, apoptotic keratinocytes, or new necrotic epidermis. Therefore, we satisfactorily excluded herpes virus infection, Grover’s disease, and SJS/TEN recurrence. DIF was also negative, which excluded autoimmune bullous diseases.
Miliaria crystallina occurs particularly under high temperatures and high humidity. It has also been observed during febrile illness associated with profuse sweating and in response to drugs that affect innervation (bethanechol)[3,4].Sweat duct necrosis and disruption without affecting the secretory glands were detected pathologically in the cases of TEN[5]. This disruption could be responsible for the common problems of dry skin and poor heat tolerance among
survivors of SJS/TEN[6]. Shuster hypothesized that mil-iaria occurs when there is sweat duct disruption and when a potential space develops between the upper necrotic epidermis and re-epithelialize tissue[7]. We believe that the humid conditions of the hot shower combined with the potential space and eccrine duct disruption because of the healing lesions of SJS/TEN caused the miliaria to present as large blisters in this patient.
In conclusion, the present case highlights that recurrent blistering due to eccrine duct disrup-tion and fluid accumulation beneath a necrotic epi-dermis could result in severe-looking form of miliaria crystallina after SJS/TEN. However, because this is essentially a self-limiting condition, prompt recog-nition is important to avoid unnecessary worry and intervention. Indeed, it can be effectively managed by simple measures, such as removing close-fitting items of clothing, avoiding overheating, and avoiding air-conditioning.
References
1. Wenzel FG, Horn TD. Nonneoplastic disorders of the eccrine glands. J Am Acad Dermatol. 1998; 38: 1-17.
2. Anbu AT, Williams S. Miliaria crystallina complicating staphylococcal scalded skin syndrome. Arch Dis Child. 2004; 89: 94.
3. Haas N, Martens F, Henz BM. Miliaria crystallina in an intensive care setting. Clin Exp Dermatol. 2004; 29: 32-4.
4. Rochmis PG, Koplan BS. Iatrogenic miliaria crystallina due to bethanechol. Arch Dermatol. 1967; 95: 499-500.
5. Akosa AB, Elhag AM. Toxic epidermal necrolysis. A study of the sweat glands. Journal of cutaneous pathology. 1995; 22: 359-64.
6. Kano Y, Shiohara T. Long-term outcome of patients with severe cutaneous adverse reactions. Dermatologica Sinica. 2013; 31: 211-6.
7. Shuster S. Duct disruption, a new explanation of miliaria. Acta Derm Venereol. 1997; 77: 1-3.

130 Chu-Ju Hung et al. / Tungs’ Medical Journal 11 (2017) 127-130
在史蒂芬強生症候群/毒性表皮壞死溶解症患者的緩解期突然又產生水泡
洪琡茹1,2 吳勝文2,3 劉親穎1,2,*
中山醫學大學附設醫院 1皮膚科 3腎臟科 2中山醫學大學醫學系
受文日期:民國 105年 03月 10日;接受刊載:民國 105年 06月 24日
摘要
史蒂文強生症候群 /毒性表皮壞死溶解症是一個嚴重及可致死的藥物疹。常見的後遺症包括皮膚乾燥及熱耐受性不良。在史蒂文強生症候群 /毒性表皮壞死溶解症的緩解期又反覆出現水泡是很少見的。我們報告一個 65歲的女性在史蒂文強生症候群 /毒性表皮壞死溶解症的緩解期又反覆出現水泡。在排除其他疾病,如自體免疫性水泡病,單純性皰疹,水泡型膿痂疹,暫時性棘皮鬆解皮膚病以及復發性史蒂
文強生症候群 /毒性表皮壞死溶解症後,診斷為一自限性的晶狀汗疹。我們的病例報告提醒在史蒂文強生症候群 /毒性表皮壞死溶解症的患者上,因為汗腺管的破壞及體液堆積在壞死上皮之下會造成反覆的水泡發生。了解這是自限性且無害的情況是重要的,因可必免不必要的擔心和處置。
關鍵詞:股骨骨折、科比牽引、剖腹產
*通訊作者:劉親穎醫師 中山醫學大學附設醫院皮膚科 台中市南區建國北路一段 110號

131
Nodular Histiocytic Prostatitis: A Case Report and Literature Review
Li-Hua Huang1, Zhon-Min Huang1, Min-Zhe Tung1, Tang-Yi Tsao2,*
1Division of Urology, 2Departmant of Pathology, Tungs’ Taichung MetroHarbor Hospital, Taichung, Taiwan
Received: Jun. 04, 2015; Accepted: Oct. 19, 2015
Abstract
Nodular histiocytic prostatitis is a rare benign prostatic inflammatory lesion. It is usually diagnosed as prostate cancer before operation because it is generally associated with an elevation in serum PSA levels. We describe a 63-year-old man with significant LUTS and a high serum PSA level (60.6 ng/mL). The primary clinical consideration was prostate carcinoma. However, the final pathological diagnosis was nodular histiocytic prostatitis. One and a half months after the operation, the patient’s serum PSA level decreased to 0.1 ng/ml. The recognition of this rare phenomenon is important in avoiding unnecessary radical surgical procedures.
Key words: nodular, histiocytic, prostatitis
Pathology Page
A 63-year-old man without any previous sys-temic disease history was examined after benign nodular hyperplasia with pathologic evidence was noted in 2009. He presented to our urology outpa-tient department with 1-year history of frequent acute dysuria and 4-month history of repeated attacks of acute urine retention with two episodes of gross hematuria. A surgical intervention was accord-ingly suggested.
Because he was diagnosed with suspected pros-tate cancer, the patient was refused a needle biopsy and referred straight for a da Vinci robot-assisted radical prostatectomy. He was admitted to our ward and prepared for a robot-assisted prostatectomy. On admission, the digital rectal examination revealed that the prostate was nodular and hard, with an estimated weight of around 80 g. The laboratory data showed a PSA level of 60.6 ng/mL. Other data, including the
routine urine test, white blood cell count, and body temperature, were within normal range.
Grossly, the prostate appeared brown in color and rubbery-to-firm in consistency and weighed around 82 g. The bladder neck, apex, and capsule were unremarkable. On serial cut sections, there were numerous small brown tan lesions in the periphery zone of the whole prostate tissue, measuring around 3–5 mm in size (Fig 1). Histopathology revealed that all these lesions showed a picture of nodular pat-terns, mixed hemorrhage, and focal acinar necrosis (Fig 2). The lesions also showed a marked infiltration of lymphocytes, epitheloid histiocytes, and foamy cells with basal cells hyperplasia in most of the acini. The foamy cells showed large amounts of clear cyto-plasm with prominent central small nucleoli and absent eosinophilic inclusion bodies, which mimicked malignant acinar cells (Fig 3), but the immunohisto-chemical stains were negative for PSA and AMACR and positive for CK5, CD43, and CD68. The CK5 stain was positive in hyperplasia basal cells, the CD43 stain was positive in lymphocytes, and the CD68 stain was diffusely positive in epitheloid histiocytes and foamy cells (Fig 4). The pathological diagnosis was nodular histiocytic prostatitis.
Tungs’ Medical Journal 11 (2017) 131-134
Pathology Page
* Correspondence to: Dr. Tang-Yi, Tsao, Department of Pathology, Tungs’ Taichung MetroHarbor Hospital, No. 699, Sec. 8, Taiwan Blvd, Wuqi Dist., Taichung City 43503, Taiwan (R.O.C.)

132 Li-Hua Huang et al. / Tungs’ Medical Journal 11 (2017) 131-134
Granulomatous prostatitis (GnP) accounts for 0.8%–1% of benign inflammatory conditions of the prostate [1], and it mimics prostate cancer clinically, histologically, biochemically, ultrasonographically, and radiologically. Carcinoma was clinically sus-pected in up to 59% of cases of GnP, and the rate of histological similarity with carcinoma in one series was 20%[1]. Carcinoma also coexists in 10%–14% of patients with clinically diagnosed GnP[1]. The spec-trum of morphologic abnormalities in nonspecific granulomatous prostatitis includes xanthogranulo-matous prostatitis, nodular histiocytic prostatitis, and prostatic xanthoma[2]. Nodular histiocytic pros-tatitis is a rare benign prostate inflammatory lesion, first reported by Fox [3]. It is usually diagnosed as
prostate cancer before operation, because it is nor-mally associated with elevations in serum PSA level. This is a rare entity that is usually an incidental finding in the periphery zone tissue removed to evaluate for BPH or carcinoma[2]. Our case was also distributed in the periphery zone tissue, and a correlation was found between gross findings (brown tan lesions) and microscopic findings (hemorrhage) (Figures 1 & 2). This is the first case report with a prostate gross gallery presentation. Histopathologically, it has a patch nodular pattern (not diffuse) infiltration of lymphocytes, plasma cells, and epitheloid histio-cytes with clear cytoplasm mimicking xanthoma cells, in which were revealed CD68+, PSA−, AMACR− and absent eosinophilic inclusion bodies[3]. Misdiagnosis
Fig. 1 The cut surfaces of normal prostatic tissue showed white-gray color. The nodular inflammatory lesions were brown tan color in the periphery zone and measured around 3-5 mm in size.
Fig. 4 The histiocytes and foamy cells showed diffuse positive for CD68 immunostain (IHC stain x 200).
Fig. 2 Nodualr pattern with hemorrhage, necrosis and infiltra-tion of lymphocytes, histiocytes and foamy cells (H & E stain x 20).
Fig. 3 The acini showed infiltration of lymphocytes, histio-cytes and foamy cells with focal basal cells hyperplasia (arrow head). The foamy cells showed amount of clear cytoplasm with proiment central small nucleoli in which mimicked the malignant acinar cells (arrow) (H & E stain x 400).

133Li-Hua Huang et al. / Tungs’ Medical Journal 11 (2017) 131-134
may occur especially in the microscopic examination of transrectal needle biopsy material, since the histio-cytic infiltration observed in nodular histiocytic pros-tatitis resembles the tumor cells in clear-cell pros-tate carcinoma (CD68−, PSA+, and AMACR+). Thus, a careful histopathological examination should accom-pany immunohistochemical tests.
Cases that morphologically resemble malako-plakia but do not contain Michaelis-Gutmann bodies (MGBs) are referred to as nodular histiocytic prosta-titis[4]. The xanthoma cells also can be confused with carcinoma with hormone treatment effect and foamy gland carcinoma. However, immunohistochemical stains can easily be for in differential diagnosis of these two entities. Our patent’s serum PSA level 1.5 months after the operation had decreased to 0.1 ng/ml. The etiology and pathogenesis of this morpholog-ically distinct lesion remains unknown. Nodular his-tiocytic prostatitis is likely caused by blockage of the prostate ducts and stasis of secretions. The resulting epithelial disruption leads to the escape of cellular debris, bacterial toxins, and prostate secretions into the stroma, leading to an intense localized inflam-matory response. [5] On transrectal ultrasonography and magnetic resonance imaging, there is no pattern that allows a specific diagnosis of this prostatitis or differentiates it from prostate carcinoma.[6] Hence, diagnosing nodular histiocytic prostatitis on histo-pathological examination of a transrectal prostate needle biopsy specimen or a TURP specimen is essen-tial, especially before radical surgical procedures are
undertaken. Nodular histiocytic prostatitis is treated mainly by supportive therapy and, for cases with severe lower urinary tract obstruction, TURP can be employed. Follow-up must be performed by the examination of PSA serum levels and, if necessary, needle biopsy of the prostate.[7]
In conclusion, nodular histiocytic prostatitis is a rare diagnosis, which should be kept in mind in cases presenting with clinical features of prostatitis or pros-tate carcinoma. It is necessary to collect and docu-ment more clinical cases to evaluate the pathogen-esis and long-term features of this rare condition.
References
1. Uzoh CC, Uff JS, Okeke AA: Granulomatous prostatitis.BJU Int.2007; 99(3): 510-2.
2. Peter A. Humphrey, J. Carlos Manivel, Robert Young: Neo-plastic Mimics in Genitourinary Pathology.2013:p127-30.
3. Fox H:Nodular histiocytic prostatitis: J Urol. 1966; 96(3): 372-4.
4. Dudu Solakoglu Kahraman, Sevil Sayan, Gulden Diniz, Duygu Ayaz, Tugua Karadeniz, Ertan Can: A Pitfall in Tran-srectal Prostate Biopsy: Malakoplakia Evaluation of Two Cases Based on the Literature Review. Case Reports in Pathology Volume 2014, Article ID 150972, 3 pages.
5. Srigley JR:Benign mimickers of prostatic adenocarcinoma: Mod Pathol. 2004; 17(3): 328-48.
6. Naik KS, Carey BM: The transrectal ultrasound and MRI appearances of granulomatous prostatitis and its differ-entiation from carcinoma:Clin Radiol. 1999; 54: 173–175.
7.Wang Y, Hu HL, Liu ZF, Sun WZ, Chen XX, Wu CL: Diagnosis and treatment of xanthogranulomatous prostatitis: a case report and review of the literature: Zhonghua Nan Ke Xue. 2013; 19(2): 149-52.

134 Li-Hua Huang et al. / Tungs’ Medical Journal 11 (2017) 131-134
結節狀組織球前列腺炎:一病例報告及文獻回顧
黃立華1 許兆畬1 童敏哲1 曹唐義2,*
童綜合醫院 泌尿科1 病理部2
受文日期:民國 104年 06月 04日;接受刊載:民國 104年 10月 19日
摘要
一位 63歲男性無系統性疾病史,在 2009年時病理診斷患有良性結節狀前列腺增生,大約最近一年開始有尿急、尿顏、排尿困難及尿痛現象,最近四個月內發生兩次急性尿滯留及血尿現象,因此病人到
泌尿科門診求助,建議病人住院進一步檢查急治療。理學檢查發現前列腺成結節狀且較硬,約 80克,血中 PSA值為 60.6 ng/mL,其它檢查包括尿液,白血球及體溫均正常。在臨床診斷為前列腺癌下,病患接受達文西機械手臂協助前列腺根除手術,病理診斷結節狀組織球前列腺炎。結節狀組織球前列腺炎
是一非常少見的良性前列腺發炎病變,因為此病變會合併血中 PSA值上升,所以在開刀前常被診斷為前列腺癌。病人在開刀後一個半月抽血檢查血中 PSA值降到 0.1 ng/ml。認識此一少見的良性病變是非常重要,以避免過度的外科手術治療。
關鍵詞:結節狀組織球前列腺炎
*通訊作者:曹唐義醫師 童綜合醫院 病理部 43053台中市梧棲區台灣大道八段 699號

135
Gas-forming Pyogenic Liver Abscesses Mimicking Bowel Gas
Chao-Hsin Wu1, Li-Hua Lu1, Chen-kuo Chu2,*
1Department of Emergency Medicine, Tungs’ Taichung MetroHarbor Hospital2Department of Emergency Medicine, Taichung Veterans General Hospital
Received: Dec. 31, 2015; Accepted: Apr. 28, 2015
Abstract
A 52-year-old man visited our emergency department after experiencing dizziness for a few days. He had a past history of diabetes mellitus, hypertension, and chronic cholangitis following cholecystectomy, choledocholithotomy, and T-tube drainage approximately 2 years ago. He was afebrile, and physical examination revealed no tenderness of the abdomen, although leukocytosis was noted. A chest X-ray revealed an abnormal air collection with an air–fluid level in the central upper abdomen and a coarse heterogeneous air collection in the right upper abdomen; however, no attention was paid to these abnormal air collections. Under the suspicion of diabetes mellitus with poor control and urinary tract infection, the patient was admitted to the ward, and intravenous ceftriaxone sodium 2 g was administered. Abdominal ultrasound conducted 2 days later revealed two air-containing liver abscesses. Two drainage catheters were inserted by the radiologist. Subsequently, the patient’s condition improved, and he was discharged in a stable condition 26 days later.
Key words: gas-forming, liver abscess, bowel gas
A 52-year-old man visited our emergency depart-ment after experiencing dizziness for a few days. He had a past history of diabetes mellitus, hypertension, and chronic cholangitis following cholecystectomy, choledocholithotomy, and T-tube drainage approxi-mately 2 year ago. He was afebrile, and physical examination revealed no tenderness of the abdomen. Laboratory data revealed a white blood cell (WBC) count of 14.9 ×103 cells/μL (normal range, 4.0–10 ×103 cells/μL) with a differential of 92.9% neutrophils and 3.5% lymphocytes; Hemoglobin, 10.8 g/dL; plate-lets, 18 ×103/μL (normal range 140–520 × 103/μL); glucose, 595 mg/dL (normal range, 70–100 mg/dL); SGOT/SGPT 488/282 IU/L (normal range, 8–40 IU/L); blood urea nitrogen, 43 mg/dL (normal range, 7–22 mg/dL); creatinine, 2.6 mg/dL (normal range, 0.6–1.3 mg/dL); and urine WBC, 5–10/HPF. A standing chest X-ray revealed air collection in RUQ and epigastric area of the abdomen, as shown Fig. 1.
Under the suspicion of diabetes mellitus with poor control and urinary tract infection, the patient was admitted to the ward for further evaluation and treatment and was administered 2-g intravenous cef-triaxone sodium. Delayed abdominal ultrasound con-ducted 2 days later revealed air-containing abscesses in the right and left lobes of the liver (7.0 and 5.7 cm in diameter, respectively) (Fig. 2) and ascites. Inten-sive care was arranged because of sepsis (Fig. 3). Intravenous vancomycin was administered for 4 days and then changed to ertapenem sodium and vanco-mycin 6 days later because of the presence of Klebsi-ella pneumoniae (producing ESBLs) and Enterococcus faecalis in the blood culture. Two drainage cathe-ters were inserted under the guidance of computer tomography (CT) (Fig. 4) by a radiologist 4 days later. The patient’s condition gradually improved, and he was discharged in a stable condition 26 days later.
Discussion
The annual incidence of pyogenic liver abscess for all age groups has gradually increased in Taiwan
Tungs’ Medical Journal 11 (2017) 135-138
Image
* Correspondence to: Chen-kuo Chu, Department of Emergency Medicine, Taichung Veterans General Hospital, No. 1650 Taiwan Boulevard Sec. 4, Taichung, 40705, Taiwan (R.O.C.)

136 Chao-Hsin Wu et al. / Tungs’ Medical Journal 11 (2017) 135-138
from 10.83 per 100,000 person-years in 2000 to 15.45 per 100,000 person-years in 2011. Pyogenic liver abscesses occur more commonly in men, in patients >50 years old, and in those with a lower family income[1]. Diabetes is the major predis-posing factor of liver abscess, and K. pneumoniae is
the primary pathogen[2]. CT and ultrasound are the diagnostic modalities of choice. CT usually shows a fluid collection with surrounding edema. Stranding and loculated subcollections may also be revealed. However, a pyogenic liver abscess cannot be reliably distinguished from an amebic abscess by imaging studies, and abscesses need to be distinguished from tumors and cysts. Tumors have a solid radiographic appearance and may contain areas of calcification. Necrosis and bleeding within a tumor may result in a fluid-filled appearance; in such circumstances, its radiographic differentiation from an abscess can be challenging. Cysts appear as fluid collections without
Fig. 2 Sonography of the liver: Air-containing abscesses in the right and left lobes of liver, small amount of ascites was seen.
Fig. 3 Chest roentgenogram in supine AP view 4 days later: Bilateral parahilar, middle & lower lung heterogeneous consol-idation, pneumonia was suspected. Two air collection remain at the same region.
Fig.4 CT of abemen: Two large liver abscess with air col-lection were seen in both lobes of the liver, minimal ascites were noted in the abdomen, too. Pulmonary infiltrations and consolidation in posterior regions of bilateral lungs, suggesting pneumonia.
Fig. 1 Chest roentgenogram in standing PA projection: One abnormal air collection with air-fluid level in the central part of upper abdomen (black arrow). Another coarse heteroge-neous air collection in right upper abdomen (white arrow).

137Chao-Hsin Wu et al. / Tungs’ Medical Journal 11 (2017) 135-138
surrounding stranding or hyperemia[3].The most dramatic change in the treatment of
pyogenic liver abscess has been the introduction of drainage guided by CT. Before this development, open surgical drainage was the most often employed treatment, which was associated with mortality rate as high as 70%. If the abscess is multiloculated, mul-tiple catheters may be needed to achieve adequate drainage[4].
References
1. Chen YC1, Lin CH2, Chang SN2, et al. Epidemiology and clinical outcome of pyogenic liver abscess: an analysis from the National Health Insurance Research Database of Taiwan, 2000-2011. J Microbiol Immunol Infect. 2014 Nov 20.
2. Feng-Chiao Tsai, Yu-Tsung Huang, Luan-Yin Chang, et al. Pyogenic Liver Abscess as Endemic Disease, Taiwan. Emerg Infect Dis. 2008 Oct; 14(10): 1592-1600.
3. http://www.uptodate.com/contents/pyogenic-liver-abscess4. Todd A Nickloes, DO, FACOS. Pyogenic Hepatic Abscesses
Treatment & Management. http://emedicine.medscape.com/article/193182-treatment.

138 Chao-Hsin Wu et al. / Tungs’ Medical Journal 11 (2017) 135-138
產氣性肝膿瘍被誤認為只是一般腸氣
吳肇鑫1 盧立華1 朱振國2,*
1童綜合醫院 急診醫學部2台中榮民總醫院急診部
受文日期:民國 104年 12月 31日;接受刊載:民國 105年 04月 28日
摘要
一位 52歲男性,過去病史有糖尿病、高血壓、慢性膽管炎經膽囊切除、結石取出及 T型管置入引流術後已兩年。他因為頭暈不適來急診就醫,身體檢查呈現無發燒、無腹痛,但是血液檢查白血球偏
高。初步的胸部 X光檢查顯示於腹部有異常氣體形成,但是臨床醫師沒有注意到。當天是在診斷為糖尿病血糖控制不佳及泌尿道感染下安排住院,先以 ceftriaxone 抗生素治療。2天後的腹部超音波顯示肝臟有兩處產氣性肝膿瘍,隨後由放射科醫師置放兩條膿瘍引流管。幸運地病人病情改善,並於 26天後出院。
關鍵詞:產氣性、肝膿瘍、腸氣
*通訊作者:朱振國醫師 台中榮民總醫院急診部 40705台灣台中市台灣大道四段 1650號

instruction to contributors
The Tungs’ Medical Journal provides a forum for all fields of medicine, including Editorials, Review Articles, Original Articles, Case Reports, Brief Communications, Images, and Pathology Page. Authors are welcome to submit manuscripts to Tungs’ Medical Journal.
Preparing Your Manuscript:1. Three copies of the manuscript must be submitted as a Word document to the Editor, Tungs’
Medical Journal, Tungs’ Taichung MetroHarbor Hospital, No.699, Sec.8, Taiwan Blvd., Wuqi Dist., Taichung 43503, Taiwan (R.O.C.) and an electronic copy of the manuscript to E-mail address: [email protected].
2. The author is responsible for the content of the manuscript. If the content is related to copyright, author needs to obtain the right to use and is legally responsible for it.
3. Please attached the copyright and consent form on submission. All author(s) listed must actually participate in and agree with the conclusion. Upon receiving and completion of printing, the author(s) will receive 20 free copies and compensation. If extra copy is needed, please notify during editing, and this is subjected to charges.
4. The manuscript may be rejected if incompatible with the journal’s mission. After acquiring consent from the author(s), the editor may edit the manuscript.
5. For any the manuscript related to “the human specimen for research” or “clinical trial”, must follow the guidelines to obtain an IRB approval for the right of participants.
6. For any the manuscript related to the use of animals, it needs to be approval of The Institutional Animal Care and Use Committee to ensure the humane management.
Manuscript format:1. Editorials are limited to 2000 words, with 150 words of abstract and 7 references.
2. Review articles should provide the reader with a balanced overview of an important and topical subject in the field. This should be limited to 3500 words, with 300 words of abstract and 40 references.
3. Original articles should be presented in the following order: Abstract, Introduction, Materials and Methods, Results, Discussion and Conclusion, Acknowledgements, References, Attachments, Tables, Legends for illustration, and Figures (photographs). This should be limited to 3000 words, with 300 words of abstract and 40 references.
4. Case reports should be arranged by the following sequence: Abstract, Introduction, the Clinical case, Discussion, References, Attachments, Table, Legends for illustration, and Figures. Patients’ eyes should be covered for privacy. Diagnosis information or the chart of clinical process should be within 6 months. This should be limited to 1500 words, with 150 words of abstract and 10 references.
5. Brief communications should be concise presentations of preliminary clinical results and technological improvements. This should be exceeded 750 words, 150 words of abstract and 7

references.
6. Images and Pathology page should be limited to 500 words, with 150 words of abstract and 3 references.
7. For other details, please refer to International Steering Committee, for Uniform Requirements for Manuscripts Submitted to Biomedical Journals, please refer to The New England Journal of Medicine 336:309-315,1997.
Specifications for the different article categories
Article CategoryWord count limit No. of references
allowedNo. of tables/
figures allowedAbstract Min text*Original Articles 300 3000 40 5Case Reports 150 1500 10 3Review Articles 300 3500 60 6Brief Communications 150 750 7 1Images, Pathology Page 150 500 3 2Editorials 150 2000 7 1
* Refers to the main body of text only, i.e., does not include article title, abstract, table headings/tables, figure legends and references.
Manuscript preparation:Manuscript should be double-spaced and numbered pages, and comply with the “uniform requirements for manuscripts submitted to biomedical journals”. The first page is the title page, which include title, name of author(s), organization and unit, contact name, phone number, e-mail address and mail address (in both Chinese and English). The second and the third page is for abstract (Chinese content needs to consist with English content) and key words (please include 3 to 5 keywords or phrases in Chinese and English), and should be written in paragraphs following by background and purpose, methods, results and discussion.
Co-corresponding author should mention the contributions on manuscript, such as initiation of research topics, the study design, statistical analysis, interpretation of findings, chapters writing involved, et al.
Please attach two original copies including attachments, charts and legends. Chart should be professional, with only one figure or one table per page, and is arranged in consecutive orders and numbered in Arabic characters. Table should have a title and appropriate interpretation. Picture should be 5” x 7” in size, black and white, glossy and numbered in consecutive orders of appearance.
reference:Unpublished articles or abstracts cannot be listed as references, but could be noted as “unpublished observations”. Doctoral dissertation or master thesis can be used. Any articles being accepted by magazines but not published yet, please note the name of magazine, year and note “in press”.
Original researches, case reports, review articles, communications (includes brief communications), images in clinical medicine, editorial follows the following format:

1. Abbreviations used should follow the format of Index Medicus for all journal titles. When authors are less than 6 people, list all author(s), when more than 6, only list the first 6 followed by “et al.” for the rest.
2. References in the text should be placed where relevant. When a reference article is cited, only the primary author is cited; however, if only two authors are present, both should be listed.
3. Example of references:
Examples of reference:1. Periodicals:
Yang KTA, Chen HD: A semi-automated method for edge detection in the evaluation of left ventricular function using ECG-gated single-photon emission tomography. Eur J Nucl Med 1994;21:1206-11.
2. Monographs:Plum F, Posner JB: Diagnosis of Stupor and Coma. 3rd ed. Philadelphia: Davis, 1980:132-3.
3. Monographs with multiple authors:Levinsky NG: Fluid and electrolytes. In: Thorn GW, Adams RD, Braunwald E, Isselbacher K, Petersdprf RG eds. Harrison’s Principles of Internal Medicine, 8th ed. New York: Mcgraw-Hill, 1977:364-75.
4. References from websiteplease indicate the title, source, and the retrieving date
(Accessed Month day, 2016, at http://www.house.gov/xxxx/min/inves_xxx/index_accord.htm.)
Copyright:If any submission being accepted by Tungs’ Taichung MetroHarbor Hospital Medical Journal, the author(s) agree to grant the Medical Journal the right to sublicense the National Central Library or any other database providers to reproduce, transmit publicly by internet, download, print and browse by authorized users. The submission may be changed to meet the requirement of databases.

童綜合醫學雜誌投稿相關規則
95.9.01製訂 99.08.17修訂
100.07.11修訂 102.07.08修訂 102.12.27修訂 103.07.14修訂 103.12.12修訂 104.03.13修訂 104.11.19修訂
本雜誌刊載與醫學有關之論述,包括原著論文(Original Articles)、病例報告(Case Reports)、綜論(Review Articles)、短論(Communications、包括 Brief Communications)、影像判讀(Images)、臨床病理討論(Pathology Page)、編著的話(Editorials)等。惠稿請送 43503臺中市梧棲區臺灣大道八段 699號童綜合醫學雜誌編審委員會。(E-mail:[email protected])
壹、投稿前注意事項
1. 惠稿請以英文撰寫,本雜誌接受電子檔投稿或紙本投稿,電子檔投稿請直接將稿件WORD 檔寄至編審委員會信箱 [email protected]),紙本投稿需檢附紙本稿件三份及電子檔一份寄至編審委員會(43503臺中市梧棲區臺灣大道八段 699號童綜合醫學雜誌編審委員會)。
2. 文件內容需清晰,內容與原稿一致,若複印稿與原稿有差異或遺漏,由作者自行負責。著作中若牽扯到版權所有之內容,作者需取得其使用權,法律責任由作者負責。
3. 投稿同時請附上著作權讓與同意書。所有作者必須實際參與並同意該論述。本院於接受稿件且印刷完成後,將致贈稿酬並贈送 20份抽印本給通訊作者,如需額外抽印本請於校稿時言明,並酌收成本費用。第一作者若需抽印本可提出申請,依份數酌收成本費用。
4. 本刊對於原稿經徵得著者之同意得伸縮或修改之。如不合本刊宗旨者,得退還之。5. 凡刊載於本雜誌之著作,若涉及「研究用人體檢體採集」及「人體試驗」等情事,應遵守該注意事項,以落實保障受檢人權益。詳文請參考須附上相關審議認可之文件。
6. 論文中如涉及使用脊椎動物進行科學應用計畫者,應檢附該計畫業經所屬機構動物實驗管理小組審議認可之文件,以落實實驗動物之人道管理。
貳、寫作原則
1. 原著論文(Original Articles)按下列順序撰寫:摘要、前言、材料與方法、結果、討論與結論、誌謝、參考文獻、附表、圖片說明、圖片(含照片)。每篇字數 3000字以內,摘要 300字以內,參考文獻 40篇以內。
2. 病例報告(Case Reports)按下列順序撰寫:摘要、前言、病例、討論、參考文獻、附表、圖片說明、附圖、照片。凡病患顏面部位之相片必須遮去眼睛部位,表示尊重隱私。診療資料或臨床經過之圖表,原則上均限六個月以內。每篇字數 1500字以內,摘要 150字以內,參考文獻 10篇以內。
3. 綜論(Review Articles)不必按原著論文格式撰寫,但每篇字數 3500字以內,摘要300字以內,參考文獻 60篇以內。
4. 短論(Brief Communications),臨床上、技術上的精簡論著,每篇字數 750字以內,摘要 150字以內,參考文獻 7篇以內。
5. 影像判讀(Images)、臨床病理討論(Pathology Page)圖例說明每篇字數 500字以內,

摘要 150字以內,參考文獻 3篇以內。6. 編者的話(Editorials),每篇字數 2000字以內,摘要 150字以內,參考文獻 7篇以內。
7. 其他細節,請參閱國際指導委員會(International Steering Committee)發表之生物醫學雜誌稿件統一規格(Uniform Requirements for Manuscripts Submitted to Biomedical Journals,見 The New England Journal of Medicine 336:309-315,1997)。
8. 將可接受投稿之稿件種類之摘要字數、字數、參考文獻及圖表相關上限規定,整理於下表:
稿件種類字數限制
參考文獻 圖 /表摘 要 內文字數
原著論文 (Original Article) ≦ 300 ≦ 3000 ≦ 40 ≦ 5病例報告 (Case Report) ≦ 150 ≦ 1500 ≦ 10 ≦ 3綜論 (Review Article) ≦ 300 ≦ 3500 ≦ 60 ≦ 6短論 (Brief Communication) ≦ 150 ≦ 750 ≦ 7 ≦ 1影像判讀 (Images)、 臨床病理討論 (Pathology Page) ≦ 150 ≦ 500 ≦ 3 ≦ 2
編者的話 (Editorial) ≦ 150 ≦ 2000 ≦ 7 ≦ 1
參、投稿須知
1. 稿件須符合「生物醫學雜誌投稿之統一規定」1,請以電腦隔行 double space書寫,並編頁碼,中文字型以標楷體,英文字型以 Time New Roman 12號字大小,稿紙之左右緣為 2.54公分,上下緣為 3.17公分。
2. 第一頁為標題頁,須列出中文及英文之論文題目、中英文作者姓名、所屬機構及單位之中英文稱號(分屬不同單位,請以阿拉伯數字標出作者與單位)、聯絡人姓名、電話及中英文通
訊錄。
3. 第二、三頁為中文及英文之摘要及關鍵詞(請提供 3至 5個關鍵詞或簡短片語),中英文摘要須完全相同,摘要分段撰寫,依序為背景及目的(Background and purpose)、方法(Methods)、結果(Results)及討論(Discussion)。
4. 相同貢獻作者請加註說明,如研究主題的設定、參與決定研究設計、進行統計分析、詮釋研究結果、以及各章節撰稿等貢獻。
5. 圖表應專業製作,一張紙僅一個附圖或附表,依引用順序以阿拉伯數字標出排列。附表須有標題及說明且不可以照片形式。圖片或照片電子檔(.jpg)必須清晰、分明。附圖須有簡單說明(Legend),並另頁撰寫。光學或電子顯微鏡照片,請註明擴大倍率或比例。
註: 1根據「生物醫學雜誌投稿之統一規定」第五版,刊載於 Annals of Internal Medicine 1997;126(1): 36-47.
肆、參考文獻
未經發表之論文或摘要不得列為參考文獻,但可於本文中說明並註明「未發表」(unpublished observations)。博碩士論文可引用。已被任何雜誌接受刊發但仍未發表之著作,請列出雜誌名稱及年份,並註明「in press」。原著論文、病例報告、綜論、短論、影像判讀、臨床病理討論、編著的話按下列格式撰寫:
A. 雜誌及期刊 中文例〔作者姓名:題目。雜誌簡稱 年號;卷數:起訖頁數〕

薛玉梅、陳建仁:皮膚砷癌之流行性病學特徵與危險因子。中華衛誌 1996; 15: 1-26。 英文例〔英文原稿中引用的參考文獻,其雜誌或期刊之簡稱應參照 Index Medicus型式〕 1. Feely J, Wilkinson GR, Wood AJ. Reduction of liver blood flow and propranonol metabolism by
cimetidine. N Engl J Med 1981;304:691-6. 2. Kaplan NM. Coronary heart disease risk factors and antihypertensive drug selection. J cardiovasc
Pharmacol 1982; 4(suppl 2): 186-365.(引用雜誌附冊時) 3. Tada A, Hisada K, Suzuki T, Kadoya S. Volume measurement of intracranial hematoma by
computedtomography. Neurol surg (Tokyo) 1981; 9: 251-6. 〔In Japanese: English abstract〕(引用文獻之作者之本文為非英文,但有英文摘要)。
4. Bhasin S, Storer TW, Berman N, Callegari C, Clecenger B, Phillips J, et al. The effects of supraphysiologic doses of testosterone on muscle size and strength in normal men. N Engl J Med 1996; 335: 1-7.(作者超過 6位時,只須列出前 6位,其它以「等」(et al)代替)
*期刊若有「數位物件識別碼 (digital object identifier, DOI)」,則於文獻未。B. 單行本: 中文例 [作者姓名:書名,版數(卷數)。發行地;出版公司,年代:引用部份頁數 ]。 楊志良:生物統計學新論,一版。台北;巨流圖書公司,1984:33-8. 英文例 [英文單行本的書名,除介系詞及連接詞外,第一字母需大寫 ] (1) Plum F, Posner JB. Diagnosis of Stupor and Coma. 3rd ed., Philadelphia: Davis, 1980:132-3.C. 多重作者之單行本: 中文例 [有關文章作者姓名:題目。編輯者姓名 :書名。版數(卷數)。發行地 :出版公司,年代 ;引用部份頁數 ]。
蔣欣欣:護理與健康。顧乃平:護理專業導論。一版。台北 : 匯華出版公司,1991:83-121。
英文例 Levinsky NG: Fluid and electrolytes. In: Thorn GW, Adams RD, Braunwald E, lsselbacher K, Petersdprf RG eds. Harrison’s Principles of Internal Medicine. 8th ed. New York: Mcgraw-Hill, 1977;364-75.
D. 參考文獻引用時,若兩名以下作者請列出姓氏。兩名以上則列出第一名之姓氏,其他以「等」 (et al)代替,並以阿拉伯數字方括弧表示於引用之後。
例:One of the first well documented reports of ECH poisoning with fatality in young children was reported by Miller et al. in 1970[2].
E. 參考文獻引用網路資料請列出文獻名稱及出處以及引用時間 (Accessed Month day, 2016, at http://www.house.gov/xxxx/min/inves_xxx/index_accord.htm.)
伍、 著作權 若著作人投稿於本刊經收錄後,同意授權本刊得再授權國家圖書館或其他資料庫業者,進行重
製、透過網路提供服務、授權用戶下載、列印、瀏覽等行為。並得為符合各資料庫之需求,酌作格
式之修改。若為摘譯、譯稿或改寫稿,需附原作者之正本同意書,並附原文影本一份;來稿如涉及
版權,概由作者自負文責。

童 綜 合 醫 學 雜 誌
編著的話
69 模擬本位訓練在住院醫師訓練的運用
遲景上
綜 論
73 瞬時感受器電位香草酸第四亞型離子通道(Transient receptor Potential Vanilloid, 4 Subfamily; TrPV4)一個多功能的離子通道范洪春 , Xuming Zhang, Peter A. McNaughton
原 著
85 抗藥性金黃色葡萄球菌感染之危險因子探討
沈萬豐 梁雅畫 李銘宗 凌美貝 郭依明 楊玉英
95 畢業後一般醫學訓練醫師課程學習歷程檔案評量:rasch模式分析黃靜宜 李銘宗 蔣志隆 廖以誠 曹龍彥
病例報告
102 外傷性橫紋肌溶解症導致急性腎衰竭:一病例報告暨文獻回顧
王世農 童詠偉
108 複雜性梅克爾憩室初始以小腸阻塞呈現
張竣翔 郭敏勇
113 治療肱骨外科頸假性關節的另類方法:病例報告
陳聖祺 徐少克
118 頸部鈍傷導致氣管斷裂:個案報告
廖培宏 林明聖 邱永偉 吳肇鑫 童詠偉
123 新生兒股骨骨折之病例報告
賴輝謙
第十一卷 第二期 民國 106年 07-12月

127 在史蒂芬強生症候群/毒性表皮壞死溶解症患者的緩解期突然又產生水泡
洪琡茹 吳勝文 劉親穎
臨床病理討論
131 結節狀組織球前列腺炎:一病例報告及文獻回顧
黃立華 許兆畬 童敏哲 曹唐義
影像判讀
135 產氣性肝膿瘍被誤認為只是一般腸氣
吳肇鑫 盧立華 朱振國
第十一卷 第二期 民國 106年 07-12月