- IntroBone tumors are very diverse in morphology and biological
potential (can be no big deal or rapidly fatal)MOST bone tumors are
benign lesionsMost benign lesions are seen
-
Bone neoplasms are very difficult to diagnose specifically on
radiologic testing aloneSo why is radiology important?Exact
location of lesionExtent of growth/metastasisAggressivenessBest
test for Dx= X-rayBest test for staging= CT or MRIQuick shout out
to the pathologists histologic grade is the most important
prognostic feature of bone sarcomas and essential for staging most
of the bone tumor types.
-
CasesFind the lesionExample:
-
CasesFind the lesionExample:RIGHT THERE!
-
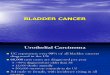
Case I16 yr old white male with pain in his left upper arm.Mild
swelling and tendernessPain progressively getting worse for ~ 3
monthsRecent onset of mild fever
-
Imaging:
-
Imaging:**
-
Biopsy material showed a highly cellular, infiltrative neoplasm
consisting of sheets of tightly packed, round cells with very scant
cytoplasm ("round blue cell tumor"). Occasional Homer-Wright
rosettes were identified. Other fields showed extensive
necrosis.
-
Dx: Ewings Sarcoma (or PNET)#2 primary bone malignancy in kids
(5-15 is most common age groupMuch more common in
CaucasiansTypically in the diaphysis of long tubular bones or in
large flat boneLytic tumor w/ permeative margins extending into the
soft tissuePeriostial rxn creates sheets of reactive bone in an
onion-skin fashion
-
Another most excellent example of onion-skinning
-
Case II33 yr old black female with sudden severe hand pain after
very minor trauma.Completely healthy otherwise.All labs normal
-
Dx: EnchondromaBenign cartilagenous tumors but hard to
distinguish from a low grade chondrosarcomaAcral bones-- the most
common primary hand tumorUsually solitary, usually incidental
finding (non-painful unless associated with fracture)Get hand films
and look for dec. lucency but not so much as a cyst (more
ground-glass) w/ or w/o areas of stippled calcifications or
rings
-
For boards and wards:Multiple enchondromas =
____________Multiple enchondromas + hemanigiomas of soft tissue =
_____________
-
For boards and wards:Multiple enchondromas = Olliers DzMultiple
enchondromas + hemangiomas of soft tissue = Maffucci syndrome
-
Case III50 yr old white male with back pain Mainly lower
spine/sacral pain, progressive ~ 8 monthsNew onset rectal pain and
constipation
-
CT guided FNA confirmed
-
Dx: ChordomaArises from notochord remnants. Thus is typically
midline along the spine and usually at the ends (Sacrococc or
occ/cervical jxn)Males>Females, middle age+ staining w/ S-100
and epithelial markersLocally invasive until very late in disease
where mets can go to the lungs, LN, skin.
-
Case IV21 yr old male with new onset chest pain today, worse on
inhalation. ROS significant for an ongoing aching leg pain for the
past 6 months which he has put off seeing a doctor for.
- Dx: The dreaded Osteosarcoma#1 primary bone
malignancyAssociated with RB1 and p53 gene mutations1000x greater
risk w/ Hx of hereditary retinoblastomaMember of the Li-Fraumeni
Syndrome familyBimodal age spike: young and elderly75%
-
Metaphysial tumor60% at the knee (distal femur or prox
tibia)Radiographic terms to know:Codmans Triangle:
Sunburst periostial formation:AKA Hair on end
-
For the future Surgeons:Rotationplasty is a new solution to
disfiguring surgical resections of lower limb sarcomas:
-
Quick Hits:Gout
-
Incidental finding on knee xrayFabella = posterior sesmoids or
little confused knee caps
-
13 yr old boy with superior tibial pain, r/o neoplasm w/ xray
shows:Osgood Schlatter
-
Metastatic DiseaseMost common malignant lesion of boneBone is #
3 on the list of favorite places for mobile cancers to goMalignant
lesions are more likely to be in axial bonesTypically multifocal
BUT renal and thyroid carcinomas are notorious for producing only a
solitary lesionCan be lytic, blastic, or both:Lung is Lytic,
Prostate Produces, Breast does Both
-
Mets
(cont)AdultsLungProstateBreastKidneyKidsNBWilmsOSEwingsRhabdomyosarcoma
-
The EndThanks for your attention and good luck on
applications!
-
BibliographyRobbins and Cotran, Pathological Basis of Disease,
7th EditionMD Murphey, MR Robbin, GA McRae, DJ Flemming, HT Temple,
and MJ Kransdorf The Many Faces of Osteosarcoma RadioGraphics 1997;
17: 1205 William R. Reinus, Louis A. Gilula IESS Committee
Radiology of Ewing's sarcoma: Intergroup Ewing's Sarcoma Study
(IESS) RadioGraphics 1984; 4: 929-944. Washington Univ. in St.
Louis (website)Harvard Medical School (website)Learning
Radiology.com (website duh)Bonetumor.org (Youre not even reading
this are you?)