Embed Size (px)
Citation preview

Microenvironment and Immunology
Tumor-Surrogate Blood Vessel Subtypes Exhibit DifferentialSusceptibility to Anti-VEGF Therapy
Basel Sitohy, Janice A. Nagy, Shou-Ching Shih Jaminet, and Harold F. Dvorak
AbstractAntivascular therapy directed against VEGFor its receptors (VEGFR) has been successful when administered at
early stages of tumor vessel growth but is less effective when administered later. Tumor blood vessels areheterogeneous, so vessel subpopulations may differ in their requirements for tumor cell–secreted VEGF and intheir susceptibility to anti-VEGF/VEGFR therapy. Human cancers contain several distinct blood vessel types,including mother vessels (MV), glomeruloid microvascular proliferations (GMP), vascular malformations (VM),feeding arteries (FA), and draining veins (DV), all of which can be generated in mice in the absence of tumor cellsusing expression vectors for VEGF-A164. In this study, we investigated the sensitivity of eachof these vessel types toanti-VEGF therapy with Aflibercept (VEGF Trap), a potent inhibitor of VEGF-A164. Administering VEGF Traptreatment before or shortly after injection of a recombinant VEGF-A164–expressing adenovirus could prevent orregress tumor-free neovasculature, but it was progressively less effective if initiated at later times. Early-formingMVs and GMPs in which the lining endothelial cells expressed high levels of VEGFR-2 were highly susceptible toblockade by VEGF Trap. In contrast, late-forming VMs, FAs, and DVs that expressed low levels of VEGFR-2 werelargely resistant. Together, our findings define the susceptibility of different blood vessel subtypes to anti-VEGFtherapy, offering a possible explanation for the limited effectiveness of anti-VEGF-A/VEGFR treatment ofhuman cancers, which are typically present for months to years before discovery and are largely populatedby late-forming blood vessels. Cancer Res; 71(22); 7021–8. �2011 AACR.
Introduction
Most tumors need to induce the formation of new bloodvessels if they are to grow beyond minimal size (1). They arethought to do so, primarily, by expressing VEGF-A and par-ticularly VEGF-A164 (mouse; human VEGF-A165; refs. 2, 3).VEGF-A initiates signaling by binding to specific, plasmamembrane–associated receptors on vascular endothelial cells,particularly VEGF receptor-2 (VEGFR-2; Flk-1; ref. 4). Accord-ingly, VEGF and its receptors have been regarded as attractivetherapeutic targets. Antibodies against VEGF-A, as well astyrosine kinase inhibitors directed against VEGFR-2, are effec-tive as monotherapy against many rapidly growing mousetumors (3); however, they have been of less benefit when usedin treating cancer patients. Bevacizumab (Avastin; Genentech,a humanized anti-VEGF-A antibody) prolongs the life expec-tancy of patients with advanced colon cancer by an average ofonly 4 to 5 months, even when used in conjunction with triple
chemotherapy (5), and has not lengthened life expectancy inseveral other cancers (6).
It has been known for some time that tumor blood vesselsare not of a single type (7), and this heterogeneity raises thepossibility that different types of tumor blood vessels might bedifferentially sensitive to anti-VEGF or anti-VEGFR therapy.Human tumors are typically present formonths or years beforediscovery and therefore could be supplied by a differentpopulation of blood vessels than rapidly growing transplant-able mouse tumors. Thus, the difference in outcome betweenmany human and mouse cancers could reflect differences inblood vessel type, their differential requirements for tumor-secreted VEGF-A, and therefore their differential sensitivity toanti-VEGF/VEGFR therapies.
Testing this hypothesis requires detailed knowledge of thedifferent types of blood vessels present in tumors and theirproperties, and few attempts have beenmade to classify tumorblood vessels rigorously (7). Recently, we categorized thedifferent blood vessels present in several important humancancers (8, 9) and identified the following structurally distinctabnormal vessel types: mother vessels (MV), glomeruloidmicrovascular proliferations (GMP), and vascular malforma-tions (VM). Of these vessel types, GMPs were most prominentin glioblastoma multiforme, but the other vessel types were allprominently represented in human colon, kidney, and ovariancancers (8, 9). In addition, highly abnormal, enlarged feedingarteries (FA) and draining veins (DV) supply and drain theangiogenic, intratumor and immediately paratumor bloodvessels, that is, MVs, GMPs, and VMs.
Authors' Affiliations: The Center for Vascular Biology Research andDepartment of Pathology, Beth Israel Deaconess Medical Center andHarvard Medical School, Boston, Massachusetts
Note: J.A. Nagy and H.F. Dvorak contributed equally to the work.
Corresponding Author:Harold F. Dvorak, Department of Pathology, BethIsrael Deaconess Medical Center, 330 Brookline Ave, Boston, MA 02215.Phone: 617-667-8529; Fax: 617-667-3591; E-mail:[email protected]
doi: 10.1158/0008-5472.CAN-11-1693
�2011 American Association for Cancer Research.
CancerResearch
www.aacrjournals.org 7021
Research. on March 10, 2021. © 2011 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 21, 2011; DOI: 10.1158/0008-5472.CAN-11-1693

Investigating the differential susceptibility of these vesselsubtypes to anti-VEGF/VEGFR therapies in human cancerpatients is difficult. Therefore, we developed an animal modelin which each of these blood vessel types is replicated in ahighly reproducible manner in nude mice in the absence oftumor cells using an adenoviral vector that expresses VEGF-A164 (10). This reductionist mouse model has allowed us toanalyze the sequential steps and mechanisms by which eachtype of new pathologic blood vessel forms and to characterizetheir functional properties (10). MVs, GMPs, and VMs devel-oped from preexisting postcapillary venules by a process ofangiogenesis, whereas FAs and DVs developed by arteriove-nogenesis from preexisting arteries and veins.
The present studies were undertaken to determine which ofthe different tumor-surrogate blood vessel types induced byAd-VEGF-A164 were or were not susceptible to anti-VEGF-Atherapy. To that end, we used Aflibercept (VEGF Trap), ahuman soluble decoy receptor protein created by fusion ofportions of VEGFR-1 and VEGFR-2 to the Fc segment of IgG1(11). VEGF Trap has high affinity for all of the isoforms ofVEGF-A, VEGF-B, and placental growth factor, but it does notbind VEGF-C. We now report that VEGF Trap potently inhib-ited both angiogenesis and arteriovenogenesis when admin-istered prior to Ad-VEGF-A164 and at least partially regressedangiogenic and arteriovenogenic blood vessels when admin-istered up to several weeks thereafter. However, VEGF Trapwaswithout significant effect when therapywas delayed until 2months after Ad-VEGF-A164 when "late" vessels, VMs, FAs, andDVs predominated. The endothelial cells lining these latevessels, in contrast to those of the highly susceptible MVs andGMPs, expressed little or no VEGFR-2. These findings couldhave important implications for understanding the limitedeffectiveness of anti-VEGF/VEGFR treatments in human can-cer, where "late" blood vessels that have acquired indepen-dence from tumor-secreted VEGF-A are likely to predominate.
Materials and Methods
Animal model, treatment with VEGF Trap, and histologyA total of 107 plaque-forming units (PFU) of Ad-VEGF-A164 in
10 mL PBS/3% glycerol were injected into the ears of femaleathymic nudemice (NationalCancer Institute) and 5� 108 PFUin 50 mL PBS/3% glycerol were injected into flank skin (12).Animals were injected subcutaneously with Aflibercept (VEGFTrap, 25 mg/kg; Regeneron) or equivalent control peptide(human Fc fragment that serves as the backbone of VEGFTrap) as in Table 1 (11). Twelve ormoremice, equallymatched,were used per group. Ears and flanks were viewed and photo-graphed in a dissecting microscope. All animal studies wereapproved by the Institutional Animal Care and Use Committeeof the Beth Israel Deaconess Medical Center, Boston, MA.
Histology and immunohistochemistryFor histology, tissueswerefixed inK2fixative and embedded
in Epon for Giemsa-stained, 1 mm-Epon sections (13). Immu-nohistochemistry was carried out on 4% paraformaldehyde-fixed, paraffin-embedded tissues with antibodies to VEGFR-2as previously described (13).
Vascular casting with MicrofilMice anesthetized with avertin (200 mg/kg) and injected
intravenously with 100 units of heparin were perfused throughthe left ventricle with 60 mL prewarmed, heparinized saline at80 mmHg, followed by sufficient Microfil (MV-122, Flow Tech,Inc.) at 120mmHg to fill the entire circulatory system. After 18to 24 hours at 4�C, tissues were dehydrated in glycerol as permanufacturer's instructions and photographed.
Quantification of intravascular plasma volume andplasma leak
We improved a 2-tracer method to quantify intravascularplasma volume and plasma albumin leakage, measures of totalblood vessel formation and vascular permeability, respectively(12). At time zero, mice were injected intravenously with 0.1 mLof 0.5% Evans blue dye, which binds to plasma albumin. Imme-diately thereafter, a sample of blood (100mL)was taken by retro-orbital puncture into 10 mL of heparin (1,000 units per mL).Twenty-five minutes later, a second intravenous injection wasadministered, this time of 10 mCi 125I-albumin (in 0.1 mL ofHanks' balanced salt solution containing 0.1% bovine serumalbumin as carrier), and another sample of blood (100 mL) wastaken immediately by retro-orbital puncture into 10 mL ofheparin (1,000 units per mL). Five minutes later, at time 30min-utes, mice were euthanized and Ad-VEGF-A164 injection siteswere carefully harvested to minimize blood loss (8-mm punchbiopsy for ear samples and 10-mm punch biopsy for flanksamples), weighed, and subjected to g-counting. The collectedblood samples were centrifuged (14,000 rpm, 10 minutes) topelletbloodcells, and theplasmawasremovedandstoredat4�C.Tissueswere extracted in1mLof formamide for at least 48hoursat 56�C. The absorbance at 620 nm of the tissue extract wasdeterminedby spectrophotometry and converted to the amount(micrograms) of Evans blue tracer in each sample using astandard curve. The concentrations of Evans blue dye and125I-albumin in the corresponding plasma samples were alsodetermined by spectrometry and g-counting, respectively, andthese values were used to convert the tissue tracer values intomicroliters of plasmaormicroliters of plasmaper gramof tissue.Anunderlying assumptionof thismethod is that even in the caseof highly leaky blood vessels only negligible amounts of 125I-albumin will have had time to extravasate at 5 minutes afterinjection. Therefore, the 125I-albumin value at 5 minutes pro-vides a quantitative measure of intravascular plasma volume,whereas the Evans blue albumin value at 30 minutes provides a
Table 1. VEGF Trap/Control treatment regimens
Group Treatment days(VEGF Trap orcontrol peptide)
Harvest day
Group 1 �1, þ2 5Group 2 þ5, 8, 11 12Group 3 þ11, 14, 17, 20 21Group 4 þ21, 24, 27, 30 31Group 5 þ51, 54, 57, 60 61
Sitohy et al.
Cancer Res; 71(22) November 15, 2011 Cancer Research7022
Research. on March 10, 2021. © 2011 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 21, 2011; DOI: 10.1158/0008-5472.CAN-11-1693

measure of the sum of both intravascular and extravascularplasmaalbuminvolume.The volumeofplasmaalbumin thathasextravasated can then be determined by subtracting the 5-minute value from the 30-minute value.
StatisticsData are presented asmean� SEM. Statistical analyseswere
conducted with InStat 3 software (GraphPad), using the non-parametric Mann–Whitney U test.
Results
Effect ofVEGFTrapon theneovascular response inducedby Ad-VEGF-A164
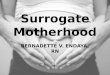
Ad-VEGF-A164 induces the formation of tumor-surrogateblood vessels in nudemice by 2 parallel processes: angiogenesisand arteriovenogenesis (9, 10). The response begins within aday, evolves over a period of weeks to months, and leavesbehind a substantial number of newly formed blood vesselsthat persist indefinitely (>1 year). VEGF Trap (or controlpeptide) was administered at various times before and afterAd-VEGF-A164 injection (Table 1). Ad-VEGF-A164 injected intomice treated with control peptide induced a strong neovas-cular response in both ears and flank skin that was identical tothat in mice receiving Ad-VEGF-A164 alone (Fig. 1). VEGF Trapprofoundly diminished the macroscopic vascular responseinduced by Ad-VEGF-A164 in groups 1 to 4 mice but had noapparent effect on group 5 mice (Fig. 1). Mice in none of thegroups exhibited any signs of toxicity.
Effect of VEGF Trap on the different subtypes of newblood vessels induced by Ad-VEGF-A164
In both ears and flank skin, MVs are the first new angiogenicvessel subtype to form (9, 10). They are greatly enlarged,
pericyte-poor, hyperpermeable blood vessels that develop frompreexisting normal venules as the result of basement mem-brane degradation and pericyte detachment (9, 10, 14). MVspeak on day 5, at the time ofmaximal intravascular volume andplasma protein leakage [Figs. 2, control peptide (C) group 1,and 3A]. Consistent with their hyperpermeability to plasmaproteins, injection sites exhibited extensive edema (Fig. 2,group 1 control). Subsequently, MVs evolved over 4 to 6 weeksinto several distinct types of "daughter" blood vessels, includingGMPs and VMs (Fig. 2, control group 4). GMPs are poorlyorganized vascular clusters that resemble renal glomerulimacroscopically (hence their name) and are composed ofpericyte-coated, endothelial cell–lined, minimally sized vascu-lar channels with reduplicated basement membranes (Fig. 3C;refs. 9, 10). VMs are large, tortuous vessels that derive fromMVsby acquiring an often asymmetrical smooth muscle coat andare the only angiogenic vessel subtype that persists beyond 2months (Fig. 3E; refs. 9, 10). Arteriovenogenesis develops inparallel with angiogenesis as preexisting small arteries andveins remodel and enlarge to form FAs andDVs that supply theangiogenic vasculature and, like VMs, persist indefinitely(Figs. 1, 2, and 3E and F). At 61 days and later times, VMs,FAs, and DVs were the predominant Ad-VEGF-A164–inducedblood vessel types present (Fig. 2, group 5).
VEGF Trap profoundly affected Ad-VEGF-A164–inducedangiogenesis and arteriovenogenesis, but its effectiveness washighly dependent on the time of administration.When injectedprior to Ad-VEGF-A164, MV formation, vascular permeabilityand edema were largely prevented [Figs. 2, treated (T) group 1,and 3B]. When injected up to one month after Ad-VEGF-A164
injection, VEGF Trap–treated mice exhibited only rare, smallGMPs, fewer VMs, and smaller FAs and DVs, and considerablyless edema than controls (Figs. 2, T group 4, and Fig. 3D).However, when treatment was delayed for 2 months (group 5),
Figure 1. Macroscopic images illustrating the effects of VEGFTrap on the angiogenic and arteriovenogenic response induced byAd-VEGF-A164 inmouse ears(A) and in flank skin after Microfil perfusion (B). For reference, areas of angiogenesis are outlined with dashed white lines in group 1, control peptide lesions;white arrows point to FAs and DVs.
Aflibercept (VEGF Trap)-Resistant Tumor-Surrogate Blood Vessels
www.aacrjournals.org Cancer Res; 71(22) November 15, 2011 7023
Research. on March 10, 2021. © 2011 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 21, 2011; DOI: 10.1158/0008-5472.CAN-11-1693

VEGF Trap had almost no inhibitory effect. VMs, FAs, and DVswere indistinguishable from controls in VEGF Trap–treatedmice (Fig. 3E and F) and both treated and control groupsdeveloped an equivalent mast cell–rich, fibrous connectivetissue stroma, similar to that found in desmoplastic tumors(Fig. 2, group 5).
VEGFR-2 (Flk-1) expression levels in different bloodvessel types induced by Ad-VEGF-A164
A possible reason for the failure of late vessels to respond toVEGF Trap is a loss of their dependence on exogenous (i.e., Ad-VEGF-A164–induced) VEGF-A. To test this possibility, we car-ried out immunohistochemistry on the different vessel types toassess changes in VEGFR-2 expression. MV and GMP endo-thelial cells stained strongly for VEGFR-2 whereas those liningVMs, FAs and DVs stained weakly or not at all (Fig. 4).
Quantification of intravascular volume and vascularleak
We refined a double tracer method that we had developedearlier (12) to provide an unbiased, quantitative measure ofboth the extent of new blood vessel formation (intravascularvolume) and the extent of vascular leakage. This method issuperior to measures evaluating vascular density for quanti-fying angiogenesis in that it the takes into account the entirevasculature within a prescribed tissue volume, thus avoidingthe problems of vascular variability in different regions and theassociated risk of sampling bias. It is also superior to the classicMiles assay in that it clearly distinguishes between dye–albu-min complex that is within versus that which is outside thevasculature. Using this method, we showed that Ad-VEGF-A164
induced a dramatic increase in intravascular plasma volume in
both ear and flank skin of mice receiving control peptide(Fig. 5); peak levels were observed on day 5, at the height ofMV formation, and persisted thereafter, though at somewhatlower levels. By day 61, intravascular plasma volume remainedsignificantly elevated, approximately twice that of normalplasma volumes in both ear and flank skin. Leakage of plasmaalbumin was also dramatically increased in Ad-VEGF-A164–injected mice receiving control peptide; again maximum leak-age was observed at 5 days and declined progressively there-after until little (ears) or no (flank skin) leakage was detected at31 days and none at 61 days (both ears and flank skin). This wasexpected as MVs and GMPs, hyperpermeable blood vessels,had by that time been largely replaced by "late" vessels (VMs,FAs, and DVs) that are not hyperpermeable (9, 10).
VEGF Trap substantially reduced both intravascular plasmavolume and plasma albumin leak in both ear and flank skin ofgroups 1 to 4 mice (Fig. 5). However, at 61 days, intravascularplasma volumes in both ears and flank skin of group 5 controlpeptide mice remained elevated approximately 2-fold abovethose of normal levels, and these volumes were not signifi-cantly diminished by VEGF Trap.
Discussion
VEGF Trap effectively prevented both angiogenesis andarteriovenogenesis when administered prior to injection ofAd-VEGF-A164. In group 1 VEGFTrap–treatedmice, new bloodvessels largely failed to develop and increases in intravascularplasma volume, permeability, and edema were minimal(Figs. 1–3 and 5). When VEGF Trap was instead administeredat intervals up to one month after Ad-VEGF-A164 injection, theMVs, GMPs, and early VMs that had formed regressed, and
Figure 2. Histology of the new blood vessels and stroma induced by Ad-VEGF-A164 in ear skin, and the effects of VEGF Trap on that response. RepresentativeGiemsa-stained, 1-mm Epon sections at various intervals after Ad-VEGF-A164 injection and treatment with VEGF Trap or control peptide. Group 1 (5 days),control peptide (C)–treated ears exhibit numerous large MVs and extensive edema, whereas ears from VEGF Trap (T)-treated mice exhibit few MVs and littleedema (compare lengths of red vertical arrows). Group 4 (31 days), control peptide–treated ears remain thickened and exhibit extensiveGMPs aswell as VMs(FAs andDVs not shown). Ears of VEGF Trap–treatedmice are of near normal thickness and show fewer and smaller newblood vessels. Group 5 (61 days), earthickness, VMs, FAs, and DVs are equivalent in VEGF Trap- and control peptide–treated mice. Both show extensive fibrous connective tissue stroma andnumerous mast cells (arrows). L, lymphatics; C, ear cartilage. Magnification bars, 50 mm.
Sitohy et al.
Cancer Res; 71(22) November 15, 2011 Cancer Research7024
Research. on March 10, 2021. © 2011 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 21, 2011; DOI: 10.1158/0008-5472.CAN-11-1693

vascular volumes and associated leakage were greatly reduced;arteriovenogenesis was also inhibited. However, VEGF Trapwas largely ineffective when treatment was delayed until 2months after Ad-VEGF-A164 injection (Figs. 1–3 and 5). At thislate time, angiogenesis had largely passed through the stages ofMVs and GMPs to form fully developed VMs, and arteriove-nogenesis had proceeded to formwell-developed FAs and DVs.Thus, VEGF Trap prevented new blood vessel formation andefficiently regressed "early" blood vessels (MVs and GMPs)induced by Ad-VEGF-A164; however, it had essentially no effecton the "late" blood vessels induced either by angiogenesis(VMs) or arteriovenogenesis (FAs and DVs). Thus, althoughall of the new blood vessels were induced by VEGF-A, not allremained sensitive to anti-VEGF-A therapy. Results consistentwith ours were recently reported in amodel involving hypoxia-inducible factor 1a (HIF-1a)-overexpressing keratinocytes;antibodies against VEGFR-2 were quite effective in preventingangiogenesis induction but were much less effective whenadministration was delayed for 2 weeks after the onset ofangiogenesis (15).One possible explanation for the insensitivity of VMs, FAs,
andDVs to VEGFTrap is that their lining endothelial cells havelost dependence on exogenous VEGF-A and that any require-ment for VEGF-A as a survival factor has been met by thepericytes or smooth muscle cells that closely envelop them.
VEGF-A delivered to endothelial cells by a paracellular mech-anism from closely apposed smooth muscle cells would likelynot be accessible to VEGF Trap. Evidence in favor of thispossibility was obtained from immunohistochemistry; MVsand GMPs expressed extremely high levels of VEGFR-2 stain-ing, whereas VMs, FAs, and DVs expressed very low or unde-tectable levels (Fig. 4).
Insufficient attention has been paid in the literature to theheterogeneity of the tumor vasculature and to the origins andspecific properties of the different types of tumor blood vesselsand their susceptibility to anti-VEGF/VEGFR therapy. A num-ber of reports indicate that vessel types variously describedas "pericyte-coated," "a-smooth muscle actin (a-SMA)–posi-tive," "mature," "normalized," "stable," "established," or "large"are resistant to such therapy in mouse and/or human cancers(16–22), whereas vessels described as "immature," "dilated," or"unstable" are sensitive (17, 23–25). However, there are excep-tions to this pattern of differential sensitivity, as VEGFTrap hasbeen reported to regress smooth muscle–coated blood vesselsin at least some tumormodels (26, 27). In any event, the specifictypes of resistant or sensitive vessels, their mode of formation,their detailed properties, and their relationships to the vascularcategories we have described in human tumors and in thetumor-surrogate vessels induced by Ad-VEGF-A164 have notpreviously been well-defined.
Figure 3. Higher magnification ofthe different types of blood vesselsinduced by Ad-VEGF-A164,following treatment with VEGF Trapor control peptide. MVs (A and B)and GMPs (C and D) are muchlarger and more frequent in controlpeptide–treated than in VEGFTrap–treated mice, whereas onceformed, VMs, FAs, and DVs are notdistinguishable (E and F). h, hairfollicle; L, lymphatic; N, nerve.Magnification bars, 25 mm.
A B
C D
E F
Aflibercept (VEGF Trap)-Resistant Tumor-Surrogate Blood Vessels
www.aacrjournals.org Cancer Res; 71(22) November 15, 2011 7025
Research. on March 10, 2021. © 2011 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 21, 2011; DOI: 10.1158/0008-5472.CAN-11-1693

Our results with VEGF Trap agree with reports of anti-VEGF/VEGFR therapy in a number of different mouse cancers.Anti-VEGF antibodies and/or small molecule VEGFR inhibi-tors have been found to inhibit the growth of many trans-plantable, VEGF-secreting mouse tumors and tumor xeno-grafts (3, 17, 28, 29). Review of the literature and our own dataindicate that MVs are the predominant vessel type, at leastduring early stages of growth, in at least the following tumors,many of which have been treated effectively with anti-VEGF/VEGFR approaches: mouse B16 melanomas, Lewis lung car-cinomas, MOT, TA3/St mammary carcinoma, guinea pig line 1and 10 bile duct carcinomas (refs. 30, 31; our unpublished data),and, as best as can be determined from published photomi-crographs, early stages of the autochthonous Rip-Tag2 tumor(29). Therefore, it may be safely presumed that MVs are theprimary vessel subtype susceptible to anti-VEGF/VEGFR treat-ment. Additional strong evidence for this conclusion comesfrom the finding that anti-VEGF/VEGFR drugs potently inhibittumor vascular hyperpermeability (24, 32, 33). In the pathologicangiogenesis induced by tumors or Ad-VEGF-A164,MVs (and toa lesser extent GMPs) are the only hyperpermeable bloodvessels (9, 10).
In contrast to their effectiveness in early mouse tumorspopulated largely by MVs, anti-VEGF/VEGFR therapies havebeen much less effective at later stages of growth in mousetumors and have had only limited effectiveness in treatinghuman cancers (5, 6). One explanation is that tumor cells
exposed to these therapies begin to express new growth factorssuch as members of the fibroblast growth factor family,angiopoietins, and interleukin-6, thereby circumventing theneed for VEGF-A (17, 28, 34, 35). However, an additionalexplanation is that, over time, the tumor vasculature evolvesto form "late" blood vessels (VMs, FAs, and DVs) that are notsusceptible to VEGF/VEGFR inhibition. Human cancers inparticular are commonly present for many months or yearsbefore they are discovered and so have sufficient time to formlarge numbers of "late" blood vessels. Quantification of therelative numbers of each vessel type in resected human car-cinomas is an impossible task, but we have shown that, at thevery least, important human carcinomas (e.g., colon, breast,ovary, and kidney) contain large numbers of VMs, FAs, andDVs(8, 9).
Our data also offer an alternative interpretation of the"normalizing" effect that anti-VEGF/VEGFR therapies have onthe tumor vasculature. Normalization refers to the decrease invascular permeability, edema, and interstitial tissue pressureinduced by anti-VEGF/VEGFR therapies (36, 37). We suggest
A
B
C
Figure 4. VEGFR-2 immunostaining of flank skin reactions. MV and GMPendothelial cells stain intensely,whereasFA,VM, andDVendothelial cellsstain much less so. Mast cells (MC) stain nonspecifically. Arrows in (C)indicate capillaries, which stainmore intensely for VEGFR-2 than doDVs.Magnification bars, 25 mm.
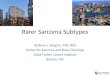
Figure 5. Quantification of angiogenesis (total intravascular plasmavolume, red bars) and plasma leakage (blue bars) in VEGF Trap- versuscontrol peptide–treatedmice. VEGF Trap treatment significantly reducedintravascular plasma volumes in both ears (51%–78%) and flank skin(52%–94%) of groups 1 to 4 mice as compared with control peptide buthad no effect on group 5mice. Intravascular volumes of both control andVEGF Trap–treated groups were significantly greater than those ofnormal ears in all groups. VEGF Trap significantly reduced plasmaleakage in groups 1 to 4 ears (79%–100%) and in groups 1 to 3 flank(86%–97%) skin. No leakage was detected in group 4 control peptide–orVEGFTrap–treated flank skin. ���,P� 0.001; ��,P�0.01; and �,P� 0.05;ns, not significant, Mann–Whitney U test.
Sitohy et al.
Cancer Res; 71(22) November 15, 2011 Cancer Research7026
Research. on March 10, 2021. © 2011 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 21, 2011; DOI: 10.1158/0008-5472.CAN-11-1693

that these therapies, as here with Ad-VEGF-A164–inducedangiogenesis, selectively attack MVs (and GMPs when pres-ent), as these are the only tumor blood vessels known to behyperpermeable to plasma proteins; edema and increasedinterstitial hyperpermeability, of course, result from increasedvascular permeability. Left behind, then are relatively unaf-fected pericyte- and smooth muscle–coated VMs, FAs, andDVs; that is, vessels that by radiological examination andimmunocytochemistry seem relatively normal in that they aresmooth muscle cell coated, smaller on average than MVs, andnot hyperpermeable to circulating macromolecules.In summary, we have shown that specific, well-defined
subsets of VEGF-A–induced blood vessels (MVs and GMPs)are sensitive to VEGF Trap therapy whereas other vesselsubsets (VMs, FAs, and DVs) are not. Because VEGF Trappotently binds to and inactivates VEGF-A, these data arelikely representative of data obtained with Avastin or VEGFRinhibitors and thus may help to explain the limited benefit ofanti-VEGF/VEGFR therapy in treating human cancers. We
suggest that antivascular therapy could be improved byfinding new targets on late tumor blood vessels, that is,those vessels that are not susceptible to anti-VEGF/VEGFRtherapy.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Grant Support
This work was supported by U.S. Public Health Service grants P01 CA92644,CA-142262 and by a contract from the National Foundation for Cancer Research(to H.F. Dvorak), and by The Swedish Research Council and The Swedish Societyof Medicine (to B. Sitohy).
The costs of publication of this article were defrayed in part by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received May 20, 2011; revised August 23, 2011; accepted September 7, 2011;published OnlineFirst September 21, 2011.
References1. Folkman J. Tumor angiogenesis: therapeutic implications. N Engl J
Med 1971;285:1182–6.2. Dvorak HF. Vascular permeability factor/vascular endothelial growth
factor: a critical cytokine in tumor angiogenesis and a potential targetfor diagnosis and therapy. J Clin Oncol 2002;20:4368–80.
3. FerraraN. Role of vascular endothelial growth factor in physiologic andpathologic angiogenesis: therapeutic implications. Semin Oncol2002;29:10–4.
4. ShibuyaM, Claesson-Welsh L. Signal transduction by VEGF receptorsin regulation of angiogenesis and lymphangiogenesis. Exp Cell Res2006;312:549–60.
5. Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J,Heim W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucov-orin formetastatic colorectal cancer. NEngl JMed 2004;350:2335–42.
6. Jain RK. Lessons from multidisciplinary translational trials on anti-angiogenic therapy of cancer. Nat Rev Cancer 2008;8:309–16.
7. Warren B. The vascular morphology of tumors. In:Peterson H-I, editor.Tumor blood circulation: angiogenesis, vascular morphology andblood flow of experimental and human tumors. Boca Raton, FL: CRCPress; 1979. p. 1–47.
8. Fu Y, Nagy JA, Dvorak AM, Dvorak HF. Tumor blood vessels. Struc-ture, function and classification. In:Teicher BA, Ellis LM, editors.Cancer drug discovery and development antiangiogenic agents incancer therapy. Totowa, NJ: Humana Press; 2007. p. 205–24.
9. Nagy JA,ChangSH,ShihSC,DvorakAM,DvorakHF.Heterogeneity ofthe tumor vasculature. Semin Thromb Hemost 2010;36:321–31.
10. Nagy JA, Dvorak AM, Dvorak HF. VEGF-A and the induction ofpathological angiogenesis. Annu Rev Pathol 2007;2:251–75.
11. Holash J, Davis S, Papadopoulos N, Croll SD, Ho L, Russell M, et al.VEGF-Trap: a VEGF blocker with potent antitumor effects. Proc NatlAcad Sci U S A 2002;99:11393–8.
12. Nagy JA, Shih SC, Wong WH, Dvorak AM, Dvorak HF. Chapter 3. Theadenoviral vector angiogenesis/lymphangiogenesis assay. MethodsEnzymol 2008;444:43–64.
13. FengD,Nagy JA,BrekkenRA,PetterssonA,ManseauEJ,PyneK, et al.Ultrastructural localization of the vascular permeability factor/vascularendothelial growth factor (VPF/VEGF) receptor-2 (FLK-1, KDR) innormal mouse kidney and in the hyperpermeable vessels induced byVPF/VEGF-expressing tumors and adenoviral vectors. J HistochemCytochem 2000;48:545–56.
14. ChangSH, Kanasaki K, Gocheva V, BlumG,Harper J,MosesMA, et al.VEGF-A induces angiogenesis by perturbing the cathepsin-cysteineprotease inhibitor balance in venules, causing basement membrane
degradation and mother vessel formation. Cancer Res 2009;69:4537–44.
15. Oladipupo SS, Hu S, Santeford AC, Yao J, Kovalski JR, Shohet RV,et al. Conditional HIF-1 induction produces multistage neovascular-ization with stage-specific sensitivity to VEGFR inhibitors and myeloidcell independence. Blood 2011;117:4142–53.
16. Benjamin LE, Golijanin D, Itin A, PodeD, Keshet E. Selective ablation ofimmature blood vessels in established human tumors follows vascularendothelial growth factor withdrawal. J Clin Invest 1999;103:159–65.
17. BergersG, SongS,Meyer-MorseN, Bergsland E, HanahanD. Benefitsof targeting both pericytes and endothelial cells in the tumor vascu-lature with kinase inhibitors. J Clin Invest 2003;111:1287–95.
18. Dor Y, Djonov V, Abramovitch R, Itin A, Fishman GI, Carmeliet P, et al.Conditional switching of VEGF provides new insights into adult neo-vascularization and pro-angiogenic therapy. EMBO J 2002;21:1939–47.
19. Frischer JS, Huang J, Serur A, Kadenhe-Chiweshe A,McCrudden KW,O'Toole K, et al. Effects of potent VEGF blockade on experimentalWilms tumor and its persisting vasculature. Int J Oncol 2004;25:549–53.
20. Helfrich I, Scheffrahn I, Bartling S, Weis J, von Felbert V, Middleton M,et al. Resistance to antiangiogenic therapy is directed by vascularphenotype, vessel stabilization, and maturation in malignant melano-ma. J Exp Med 2010;207:491–503.
21. Tafuro S, Ayuso E, Zacchigna S, Zentilin L, Moimas S, Dore F, et al.Inducible adeno-associated virus vectors promote functional angio-genesis in adult organisms via regulated vascular endothelial growthfactor expression. Cardiovasc Res 2009;83:663–71.
22. Lu C, Kamat AA, Lin YG, Merritt WM, Landen CN, Kim TJ, et al. Dualtargeting of endothelial cells and pericytes in antivascular therapy forovarian carcinoma. Clin Cancer Res 2007;13:4209–17.
23. Dor Y, Djonov V, Keshet E. Induction of vascular networks in adultorgans: implications to proangiogenic therapy. Ann N Y Acad Sci2003;995:208–16.
24. Yuan F, Chen Y, Dellian M, Safabakhsh N, Ferrara N, Jain RK. Time-dependent vascular regression and permeability changes in estab-lished human tumor xenografts induced by an anti-vascular endothe-lial growth factor/vascular permeability factor antibody. ProcNatl AcadSci U S A 1996;93:14765–70.
25. Escorcia FE,HenkeE,McDevittMR, VillaCH,Smith-JonesP,BlasbergRG, et al. Selective killing of tumor neovasculature paradoxicallyimproves chemotherapy delivery to tumors. Cancer Res 2010;70:9277–86.
Aflibercept (VEGF Trap)-Resistant Tumor-Surrogate Blood Vessels
www.aacrjournals.org Cancer Res; 71(22) November 15, 2011 7027
Research. on March 10, 2021. © 2011 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 21, 2011; DOI: 10.1158/0008-5472.CAN-11-1693

26. Kadenhe-Chiweshe A, Papa J, McCrudden KW, Frischer J, Bae JO,Huang J, et al. Sustained VEGF blockade results in microenvironmen-tal sequestration of VEGF by tumors and persistent VEGF receptor-2activation. Mol Cancer Res 2008;6:1–9.
27. Gomez-Manzano C, Holash J, Fueyo J, Xu J, Conrad CA, Aldape KD,et al. VEGF Trap induces antiglioma effect at different stages ofdisease. Neuro Oncol 2008;10:940–5.
28. Casanovas O, Hicklin DJ, Bergers G, Hanahan D. Drug resistance byevasion of antiangiogenic targeting of VEGF signaling in late-stagepancreatic islet tumors. Cancer Cell 2005;8:299–309.
29. Ryschich E, Schmidt J, Hammerling GJ, Klar E, Ganss R. Transfor-mation of the microvascular system during multistage tumorigenesis.Int J Cancer 2002;97:719–25.
30. Dvorak HF. Rous-Whipple Award Lecture. How tumors make badblood vessels and stroma. Am J Pathol 2003;162:1747–57.
31. ZengH,Qin L, ZhaoD, Tan X,Manseau EJ, VanHoangM, et al. Orphannuclear receptor TR3/Nur77 regulates VEGF-A-induced angiogenesisthrough its transcriptional activity. J Exp Med 2006;203:719–29.
32. Verheul HM, Hammers H, van Erp K, Wei Y, Sanni T, Salumbides B,et al. Vascular endothelial growth factor trap blocks tumor growth,
metastasis formation, and vascular leakage in an orthotopic murinerenal cell cancer model. Clin Cancer Res 2007;13:4201–8.
33. Zhu AX, Sahani DV, Duda DG, di Tomaso E, Ancukiewicz M, CatalanoOA, et al. Efficacy, safety, and potential biomarkers of sunitinib mono-therapy in advanced hepatocellular carcinoma: a phase II study. J ClinOncol 2009;27:3027–35.
34. Jain RK, Duda DG, Willett CG, Sahani DV, Zhu AX, Loeffler JS, et al.Biomarkers of response and resistance to antiangiogenic therapy. NatRev Clin Oncol 2009;6:327–38.
35. Willett CG, Duda DG, di Tomaso E, Boucher Y, AncukiewiczM, SahaniDV, et al. Efficacy, safety, and biomarkers of neoadjuvant bevacizu-mab, radiation therapy, and fluorouracil in rectal cancer: a multidisci-plinary phase II study. J Clin Oncol 2009;27:3020–6.
36. Jain RK. Normalization of tumor vasculature: an emerging concept inantiangiogenic therapy. Science 2005;307:58–62.
37. Kamoun WS, Ley CD, Farrar CT, Duyverman AM, Lahdenranta J,Lacorre DA, et al. Edema control by cediranib, a vascular endothelialgrowth factor receptor-targeted kinase inhibitor, prolongs survivaldespite persistent brain tumor growth in mice. J Clin Oncol 2009;27:2542–52.
Sitohy et al.
Cancer Res; 71(22) November 15, 2011 Cancer Research7028
Research. on March 10, 2021. © 2011 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 21, 2011; DOI: 10.1158/0008-5472.CAN-11-1693

2011;71:7021-7028. Published OnlineFirst September 21, 2011.Cancer Res Basel Sitohy, Janice A. Nagy, Shou-Ching Shih Jaminet, et al. Susceptibility to Anti-VEGF TherapyTumor-Surrogate Blood Vessel Subtypes Exhibit Differential
Updated version
10.1158/0008-5472.CAN-11-1693doi:
Access the most recent version of this article at:
Cited articles
http://cancerres.aacrjournals.org/content/71/22/7021.full#ref-list-1
This article cites 35 articles, 16 of which you can access for free at:
Citing articles
http://cancerres.aacrjournals.org/content/71/22/7021.full#related-urls
This article has been cited by 8 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
SubscriptionsReprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://cancerres.aacrjournals.org/content/71/22/7021To request permission to re-use all or part of this article, use this link
Research. on March 10, 2021. © 2011 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 21, 2011; DOI: 10.1158/0008-5472.CAN-11-1693