Embed Size (px)
Citation preview

The Breast 20 (2011) S3, S50–S55
Contents lists available at ScienceDirect
The Breast
journal homepage: www.elsevier .com/brst
Original Article
Tumor–stroma interactions a trademark for metastasis
Monica Moralesa,d, Evarist Planetb,d, Anna Arnal-Estapea,d, Milica Pavlovica,d, Maria Tarragonaa,d,Roger R. Gomisa,c, *
aOncology Programme, Institute for Research in Biomedicine (IRB-Barcelona), Barcelona, SpainbBiostatistics and Bioinformatics Unit, Institute for Research in Biomedicine (IRB-Barcelona), Barcelona, SpaincInstitucio Catalana de Recerca i Estudis Avancats (ICREA), Barcelona, SpaindThese authors contributed equally to this work.
a r t i c l e i n f o
Keywords:
Metastasis
Cancer
Stroma
TGFbBone remodelling
s u m m a r y
Aims: We aimed to unravel genes that are significantly associated with metastasis in order to
identify functions that support disseminated disease.
Methods and Results: We identify genes associated with metastasis and verify its clinical correlations
using publicly available primary tumor expression profile data sets. We used facilities in R and
Bioconductor (GSEA). Specific data structures and functions were imported. Our results show that
genes associated with metastasis in primary tumor enriched for pathways associated with immune
infiltration or cytokine–cytokine receptor interaction. As an example, we focus on the enrichment
of TGFBR2 and TGFb. A set of communication tools capital for tumor–stroma interactions that
define metastasis to the lung and support bone colonization.
Conclusions: We showed that tumor–stroma communication through cytokine–cytokine receptor
interaction pathway is selected in primary tumors with high risk of relapse. High levels of these
factors support systemic instigation of the far metastatic nest as well as local metastatic-specific
functions that provide solid ground for metastatic development.
© 2011 Elsevier Ltd. All rights reserved.
Introduction
Tumors are composed of several cell types including malignant
cells, which provide a complex scenario of interactions and define
what is known as tumor biology. Consistently, many experimental
studies have depicted the importance of non-transformed cell
types within tumors including endothelial cells, cellular entities of
the immune system as well as fibroblasts and other cell types.1
Interestingly, the degree of infiltration of these non-malignant
cells into a tumor sets the stage for its clinical classification and
its association with the most aggressive forms of the disease.
Growth at the primary site, spreading into the vasculature and
lymphatic system, and colonization of distant metastatic sites are
processes that need malignant cells and microenvironment, also
named stroma, interactions through both cancer cell and host-
derived factors.2,3 Indeed, cancers that never progress to invasive
forms lack vascularization, macrophage infiltration as well as large
areas with fibroblast and Extracellular Matrix depositions.4 This fact
can be attributed to the absence of recruiting factors produced
by tumor cells or, alternatively, due to host-derived factors that
* Corresponding author. Roger R. Gomis. Oncology Programme,
Institute for Research in Biomedicine (IRB Barcelona), PBB52 Parc
Cientıfic de Barcelona, C/Baldiri i Reixac 10–12, 08028 Barcelona,
Spain. Tel.: +34-93-403-9959; fax: +34-93-403-9960.
E-mail address: [email protected] (R.R. Gomis).
precluded tumor progression to more aggressive forms.1,4 Similarly,
the metastatic stroma also encompasses non-malignant cells as
well as ECM matrix, embedded with a plethora of growth factors.
These non-malignant cells are shown to display unusual features
with characteristic behaviors and patterns of protein expression
at each distinct metastatic site.5,6 In summary, these observations
indicate that transformation does not suffice to produce aggressive
forms of cancer and that interaction with the tumor environment
accommodates tumor progression and metastasis.4
In breast cancer, radiographic appearance and histological
confirmation of presence of stromal factors within primary tumor
has been correlated with prognosis of disease (usually the degree
of fat or the presence of fibroblasts, macrophages or endothelial
cells). The stromal cells include carcinoma-associated fibroblasts
(CAFs), the blood and lymphatic vascular cells, and infiltrating
immune and inflammatory cells.7 The extent of infiltration has been
associated with tumor poor prognosis. Infiltrates of the immune
system, including macrophages, mast cells, and myeloid cells,
promote tumor progression by releasing factors and cytokines that
stimulate tissue remodeling and angiogenesis processes. Moreover,
the release of oxygen free radicals might contribute to exacerbate
genomic instability and suppress antitumor immunity.8,9 Only
natural killer cell infiltrates have been shown to have antitumor
activity in experimental models.9 Molecular profiling of the stromal
0960-9776/ $ – see front matter © 2011 Elsevier Ltd. All rights reserved.

M. Morales et al. / The Breast 20 (2011) S50–S55 S51
compartment of human tumor specimens has provided information
of prognostic value.10
Fibroblasts function is strikingly impinged by the tumor context.
CAFs deliver many tumor promoting functions through the
production and remodeling of ECM, growth factors and its ability
to recruit angiogenic and immune cells.1,11 Unfortunately, the
mechanism by which tumor cells cancerize fibroblast and how
the latter, in turn, contribute to tumor progression remains largely
unknown. Dynamic communication between transformed cells and
stromal factors is necessary for cancer cells to exploit stromal func-
tionality towards the establishment of tumor microenvironment.
Collectively, these interactions provide important additional cues
to identify treatments that effectively tackle tumor progression.
The efforts to develop therapies that target tumor stroma can
be exemplified with the development of anti-angiogenic tumor
therapies. Three are the current clinically approved drugs and are
used in a wide range of tumor types. Yet, it has become clear that
the tumor stroma is dynamic, since evasion from anti-angiogenic
therapy is a fact12 and a matter of intense investigation.
Material and methods
Statistical analysis
All statistical analyses were performed using Bioconductor.13 The
patients’ information has been downloaded from GEO.14 Two sets of
data were used: Set 1: Union of GSE2603, GSE2034, GSE12276 and
Set 2: GSE5327. For each cohort individual gene’s expression has
been standardized to z-scores to make measurements comparable.
Using Set 1 a Cox proportional hazards model15 was tested for
each individual gene using the Bioconductor survival package. The
following deviations from the Cox proportional hazards model were
also tested: proportional hazards assumption and non-linear effect.
(1) we tested the proportional hazards assumption as implemented
in the cox.zph function of the survival package. A hazard being not
proportional in time means that the hazard has a bigger effect
in some moment of time and a weaker or opposite effect in
some other period of time. (2) We tested for a non-linear effect
of gene expression on survival via penalized splines of degree 4,
as implemented in the splines function of the survival package.
Therefore we obtained 3 P-values: regular proportional hazards,
non-proportional hazards and non-linearity. Each one reflects a
different kind of association between gene expression and overall
metastasis. All P-values were adjusted to correct for multiple
testing using the Benjamini Hochberg method.16 Based on the
three previous tests (on Set 1) the following gene signatures were
defined: (a) Up regulated genes: This signature contains genes that
have at least one of the three computed P-values < 0:05 and an
estimated positive hazard ratio in the Cox proportional hazards
model. (b) Down regulated genes signature: This signature contains
genes that have at least one of the three computed P-values <0:05
and an estimated negative hazard ratio in the Cox proportional
hazards model. (c) Together: This signature contains the genes from
the two previous signatures.
Gene set enrichment analysis
We used gene set enrichment analysis (GSEA)17 as implemented
in the Bioconductor library phenoTest18 to assess the degree of
association between gene signatures and metastasis in Set 2
(GSE5327).
GSEA requires ranking genes according to their association with
a given phenotype, and determining whether genes in a signature
tend to present either high (positively enriched) or low ranks
(negatively enriched). Association with metastasis was measured
with the following score: score = −log2(p) * sign(h) (1) where p
is the lowest P-value of the three previously described tests and h
is the hazard ratio (both computed on Set 2). Notice that a small
P-value in any of the previously described tests indicates a different
kind of association between gene expression and metastasis free
survival. The output of GSEA is an enrichment score (ES), a
normalized enrichment score (NES) which accounts for the size
of the gene set being tested, a P-value and an estimated FDR.
Computing NES, P-values and FDR requires a permutation-based
approach for which we computed 10,000 permutations.
KEGG pathway enrichment analysis
KEGG pathway enrichment analysis was performed using a
Wilcoxon test based GSEA, as implemented in the Bioconductor
library phenoTest.
Results
Identification of genes associated with metastasis
We identified genes whose expression is associated with aggressive
metastatic behavior in breast cancer primary tumors. We performed
analysis to test the association between each gene expression
level and its probability of recurrence in two independent sets
of breast cancer primary tumor expression profiles. These tumors
are representative of all BC subtypes and metastatic sites. Both
databases and their clinical annotations are publicly available (gene
expression omnibus: GSE 2603, 2034, 12276 for MSKCC/EMC and
NKI-29819). The MSKCC/EMC data set is composed of the gene
expression profiles of 560 breast cancer samples, determined using
the U133A affymetrix, and its clinical annotation for recurrence and
was obtained in two independent institutions.20 The second data set
was elaborated at the NKI, using a custommade chip, containing the
expression profile of 298 breast cancers and its clinical annotation.
Collectively, our analysis identified a group of genes significantly
selected for and associated with metastasis colonization to distant
sites in breast cancer using the MSKCC/EMC data set. This
group of genes that showed a significant trend of regulation
(increased/decreased) might be of tumor or stroma origin since
no separation between tumor cell types was performed prior to
profiling. Next, we performed gene set enrichment analysis (GSEA)17
in an independent cohort of breast cancer primary tumor gene
expression profiles, the NKI-298, using the previously identified
group of genes. This approach tests the phenotypic association with
risk of metastasis of each of the genes identified in the MSKCC/EMC
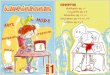
cohort in the NKI-298 data set. This association resulted to be strong
(normalized enrichment score of 2.3 and −0.9 for genes upregulated
or downregulated using adjusted p-values) (Fig. 1). Since false
discovery rates were minimal, this result is best interpreted as how
well experimentally selected genes in the MSKCC/EMC metacohort
associated with short time to metastasis in the NKI-298 cohort.
Interestingly, the same procedures applied to randomly generated
sets of 500 genes did not perform significantly.
Identification of tumor–stroma interacting program
To investigate what functions are enriched or attenuated in
primary breast cancers, KEGG pathway enrichment analysis was
performed using a Wilcoxon test based GSEA to measure the
association of the previously identified metastasis associated genes
with pathway-specific gene expression signatures (using KEGG
pathway functions). Interestingly, 10 pathways are significantly
enriched among the 197 tested (Table 1 and Fig. 2). These include
pathways related to immune response processes and immune
cells (Intestinal immune network of IgA production, Allograft
rejection, Graft-vs-host disease, viral mycarditis, hematopoietic cell

S52 M. Morales et al. / The Breast 20 (2011) S50–S55
NES (fdr<0.001)
NE
S
20
2
Gene list rank1 2000 4000 6000 8000 10000
RA
NK
MET No MET
NES (fdr=0.506)
1 2000 4000 6000 8000 10000
Gene list rank
RA
NK
NE
S
10
1
NE
S
20
2
NE
S
20
2
NKI-298 Cohort (n=298)
MET No MET
Genes Positively Associated with Metastasis Genes Negatively Associated with Metastasis
10
1
RA
NK
METASTASIS
Genes Associated (+/-) with Metastasis
MSKCC/EMC Cohort (n=560)
Fig. 1. Gene set enrichment analysis of the phenotypic association of genes previously associated with high risk of metastasis in the MSKCC/EMC primary tumor cohort,
with the metastasis hazard ratio (HR) in the NKI-298 primary tumor cohort. Genes are separated accordingly to whether they were positively or inversely associated with
metastasis in the MSKCC/EMC cohort. RANK: hazard ratio; NES: normalized enriched score; FDR: false discovery rate.
Table 1
Pathway gene set enrichment analysis using 197 KEGG pathway functions. Genes significantly associated with risk of metastasis
in the MSKCC/EMC primary tumor expression profile data set (n = 560) were tested for their association with pathway-specific
gene expression signatures in an independent primary tumor expression profile data set, NKI-298 (n =298). The list depicts
the 10 pathways significantly enriched among the 197 tested.
Pathway Id Pathway Name Enrichment
Score
p-value
4672 Intestinal immune network for IgA production 15.08 0.00069
5330 Allograft rejection 10.82 0.00094
4060 Cytokine-cytokine receptor interaction 12.42 0.00110
5332 Graft-versus-host disease 10.70 0.00178
5416 Viral myocarditis 9.91 0.00255
4640 Hematopoietic cell lineage 14.26 0.01228
5140 Leishmaniasis 12.68 0.01228
5320 Autoimmune thyroid disease 10.35 0.02199
4610 Complement and coagulation cascades 6.51 0.02645
4940 Type I diabetes mellitus 10.60 0.04883
lineage, leishmaniasis, autoimmune thyroid disease, complement
and coagulation cascades and type I diabetes mellitus), which are
known to be a major constituent of tumor stroma and to be strongly
associated with tumor poor prognosis and recurrence. Interestingly,
the third main pathway differentially represented in tumors
associated with high risk of recurrence was the “cytokine–cytokine
receptor interaction pathway”, which highlights the importance
of communication signals within cell types present in the tumor.
Among the 276 genes that composed this pathway, almost one
third (76 genes) are differentially expressed in tumors of the most
aggressive nature (Table 2), including a wide range of signals and
functions that could potentially foster tumor and stroma specific
tumor progression functions.
Tumor–stroma specific functions
Example of biological significance of this analysis is strong
upregulation of Transforming Growth Factor beta (TGFb) receptor

M. Morales et al. / The Breast 20 (2011) S50–S55 S53
KEGG:4267
Intestinal immune network for IgA production (pval<0.001) *
20 15 10 5 0 5
0.0
00.0
50.1
00.1
5
N = 43 Bandwidth = 0.8368
Den
sit
y(lo
g)
20
020
(*) pvalue adjustment method: BHGene list rank
1 2000 4000 6000 8000 10000 12000
Average
Tumors
Metastatic
Tumors
KEGG:4060
Cytokyne-Cytokine receptor interaction (pval=0.001) *
20 10 0 10 20
0.0
00.0
40.0
80.1
2
N = 240 Bandwidth = 1.047
Den
sit
y(lo
g)
20
020
(*) pvalue adjustment method: BHGene list rank
1 2000 4000 6000 8000 10000 12000
KEGG:04010
MAPK signaling pathway (pval=0.997) *
20 10 0 10 20
0.0
00.0
40.0
8
N = 249 Bandwidth = 1.319
Den
sit
y(lo
g)
20
020
(*) pvalue adjustment method: BHGene list rank
1 2000 4000 6000 8000 10000 12000
Average
Tumors
Metastatic
TumorsAverage
Tumors
Metastatic
Tumors
(A) (B) (C)
Fig. 2. KEGG pathway enrichment analysis was performed using a Wilcoxon test based GSEA, as implemented in the Bioconductor library phenoTest. The three pathways
depicted in this figure represent: (A) the most enriched pathway (KEGG:4267), (B) Cytokine-cytokine receptor interaction pathway (KEGG:4060) and (C) one of the pathway
non enriched (KEGG:04010). A plot defining the number of tumors according to the average expression of the genes in the pathway of interest is depicted in the upper part
of each figure. In green, highlighted tumors with annotations of metastasis. In black, the line that sets the expression level for the average of all tumors.
Table 2
Among the 276 genes that composed the cytokine–cytokine receptor interaction pathway, this table highlights those 76 genes that
are significantly differentially expressed in primary tumors that relapse (patients follow up time: 120 months).
Entrez ID Gene Symbol Score(HR) p-value Entrez ID Gene Symbol Score(HR) p-value
83729 INHBE −21.708248 2.92×10−7 50616 IL22 6.59472647 0.01034641
4982 TNFRSF11B −20.588914 6.34×10−7 1956 EGFR 6.56945906 0.01052921
7048 TGFBR2 19.5467269 1.31×10−6 4352 MPL 6.51882317 0.01090533
268 AMH −18.065165 3.65×10−6 2829 XCR1 −6.3553726 0.01221356
608 TNFRSF17 17.9808451 3.87×10−6 8795 TNFRSF10B 6.30589746 0.01263967
2324 FLT4 17.9268502 4.01×10−6 5159 PDGFRB 6.29128275 0.01276836
3556 IL1RAP 13.1392613 0.00011084 3445 IFNA8 6.28368885 0.01283575
3563 IL3RA 13.028401 0.00011969 7173 TPO −6.2663073 0.01299133
11009 IL24 −12.828113 0.00013752 4254 KITLG −6.1526191 0.0140565
6846 XCL2 12.5317298 0.00016888 6347 CCL2 5.94766833 0.01620218
3605 IL17A −12.521353 0.0001701 3082 HGF 5.92222551 0.01649045
6364 CCL20 −12.258245 0.00020413 5155 PDGFB −5.8380134 0.01748167
1437 CSF2 12.0770635 0.00023144 29949 IL19 5.81574125 0.01775364
1270 ZFP91 12.0226356 0.00024034 2321 FLT1 5.65024634 0.01991161
6361 CCL17 11.801464 0.00028016 3554 IL1R1 5.54066881 0.02148288
7423 VEGFB −11.520199 0.00034047 3568 IL5RA 5.53016573 0.02163985
3953 LEPR −11.410602 0.00036734 7043 TGFB3 −5.403455 0.02362642
1438 CSF2RA 10.5542234 0.00066506 1237 CCR8 −5.3145362 0.02512842
53832 IL20RA 10.4967512 0.00069209 27190 IL17B −5.2949196 0.02547243
3579 CXCR2 10.316842 0.00078401 958 CD40 5.29271559 0.02551137
2920 CXCL2 9.93710942 0.00102007 8792 TNFRSF11A 5.29069681 0.0255471
3452 IFNA21 −9.7595997 0.00115363 8742 TNFSF12 5.2382249 0.02649337
59067 IL21 −9.440235 0.00143948 3594 IL12RB1 −5.1766419 0.02764875
7293 TNFRSF4 9.03980792 0.00189997 3581 IL9R −5.0142976 0.03094183
8794 TNFRSF10C 9.02275354 0.00192256 3626 INHBC 5.00852718 0.03106584
944 TNFSF8 8.98842098 0.00196886 6375 XCL1 4.99046559 0.03145721
57007 CXCR7 8.68101814 0.00243643 2056 EPO 4.98733435 0.03152556
3627 CXCL10 8.5928068 0.00259005 4055 LTBR −4.9791495 0.03170492
4049 LTA 8.5215358 0.00272121 3593 IL12B −4.9605186 0.03211701
3559 IL2RA −8.1221656 0.00358909 3586 IL10 4.86044492 0.03442392
655 BMP7 −8.0418943 0.00379445 27242 TNFRSF21 −4.8298567 0.03516157
1439 CSF2RB 7.81675876 0.00443528 1950 EGF 4.76184242 0.03685892
3952 LEP 7.712337 0.00476821 5156 PDGFRA −4.6124917 0.04087913
6374 CXCL5 7.67184963 0.00490392 3442 IFNA5 4.59366923 0.04141596
3577 CXCR1 7.54456524 0.00535623 1896 EDA 4.45568187 0.04557284
2689 GH2 7.262358 0.00651347 6373 CXCL11 4.31021924 0.05040745
8200 GDF5 −7.2222756 0.00669697 7040 TGFB1 4.30568667 0.05056607

S54 M. Morales et al. / The Breast 20 (2011) S50–S55
type II. This gene is included in the cytokine–cytokine receptor
interaction pathway (Table 2). Perturbations of TGFb signaling
are central to tumorigenesis and tumor progression in a cancer
cell dependent and independent manner.21 TGFbR2-inactivatingmutations are often found in colon cancers and are associated
to microsatellite instability.22 These results provide evidence of
the pathway tumor suppressor function. However, TGFb signaling
is also known to function as a tumor promoter.23 TGFb staining
correlates with metastasis in breast, prostate and colon cancers.24,25
Particularly, TGFb transcriptional program is enriched and drives
ER-negative breast cancer metastasis to the lung.26 These findings
indicate that excessive TGFb stimulation is an indispensible
prerequisite for tumor progression. Who produces and how is
TGFb sensed is a matter of great interest. During tumorigenesis
and tumor progression, the stroma cells affect the characteristcs
of tumor cells through diverse mechanisms. TGFb can suppress
inflammation, recognition and destruction of tumor cells through
the regulation of immune cell function. Moreover, it also modulates
the interaction between fibroblasts and tumor cells in a process that
might resemble active wound healing. Lately, TGFb has also been
linked with the stroma capacity to maintain cancer stem cells and
their niche.27,28
Discussion
Collectively, the above-described results highlight the strong
contribution that tumor–stroma interactions have to define the
metastatic outcome of breast primary tumors. Particularly, in our
analysis the cytokine–cytokine receptor interaction pathway is
among those mostly changed between poorly and highly aggressive
tumors. A recent study has shed some light on how tumor–stroma
interactions that ocurr in the primary site have the capacity to
endow tumors cells with metastatic capacities in a tissue specific
manner. For instance, TGFb signaling in ER-negative breast cancer
microenvironment primes cancer cells for pulmonary metastasis.26
Inhibition of this pathway in ER-negative breast cancer cells
attenuates its ability to generate lung metastasis when implanted
orthotopically in a mouse model. This process relays on the vascular
remodeling gene, Angiopoietin-like 4 (ANGPTL4), identified as a
TGFb target in ER-negative breast cancer and whose upregulation
was associated with lung metastasis. Particularly, tumor cell-
derived ANGPTL4 was shown to disassemble endothelial cell
junctions supporting vascular permeability at the lung capillaries
where tumor cells released by the primary tumor lodge prior
to extravasate and colonize the lungs. Interestingly, the TGFbresponsive program in cancer cells was associated in breast primary
tumors with relapse to the lung but not other tissues. TGFb activityhas also been proved fundamental in ER-negative bone metastasis.
However, in this case, the signaling activity is selectively acquired
at the metastatitc site.29 This far-site metastasis selection process
defines a whole new set of tumor–host interactions.
Recent findings highlight how growth of metastatic cells, at
distinct sites from where the primary tumor was originated, is
dependent on aberrant hormone or cytokine production. This,
indicates that tumors might perturb host organs from the distance
and this process might act as a driving force metastatic seeding. For
example, evidences point towards a process of metastasis nesting
at the lungs.30 This process includes recruitment of bone marrow
cells (BMC) possibly mediated by accumulation of lysyl oxidase at
the lungs, creating a trap for the recruitment and settlement of
circulating tumor cells in this particular metastatic site. This process
of distant systemic instigation of metastatic nesting has several
implications, including influence on how and when to apply anti-
metastatic therapies to tackle the dissemination process.
Finally, local tumor–host interactions are well established
to occur at the metastatic sites where the instigating breast
carcinomas are able to perturb targeted tissue homeostasis. Bone
metastatic breast cancer cells select for the expression of OPN, IL6,
IL11, PTHLH and other factors that support osteoclast differentiation,
which perturbs the normal equilibrium between bone synthesis and
degradation and supports metastatic growth by constant release of
growth factors within the niche.29,31,32 This tumor-metastatic host
interaction might open the avenues for new therapies, as it is the
use of zoledronic acid to prevent survival and bone remodeling by
disseminated breast cancer cells that metastasis to the bone.33
In summary, we showed that tumor–stroma communication
through cytokine–cytokine receptor interaction pathway is selected
in primary tumors with high risk of relapse. Cross talk between
tumor and stroma might support local metastatic-specific functions
and provide solid ground for metastatic development. A process,
otherwise, defined in breast cancer by slow kinetics and
inefficiency.34 These results also point the need for further
development of targeted tumor–host containing chemotherapy
regimes in order to reach inhibition of metastatic dissemination
and growth.
Acknowledgements
A.A.E. is a recipient of a doctoral fellowship from the Ministerio
de Educacion of Spain. M.P. is a recipient of a doctoral fellowship
from “La Caixa”. R.R.G. is a Researcher of the Institucio Catalana de
Recerca i Estudis Avancats. Financial support was provided by the
BBVA foundation, AECC and the Ministerio de Ciencia e Innovacion
of Spain (SAF2010–21171) to R.R.G.
Conflict of interest statement
The authors have no conflict of interest to declare.
References
1. Kalluri R, Zeisberg M. Fibroblasts in cancer. Nat Rev Cancer 2006;6(5):392–401.
2. Joyce JA, Pollard JW. Microenvironmental regulation of metastasis. Nat Rev
Cancer 2009;9(4):239–52.
3. Bhowmick NA, Neilson EG, Moses HL. Stromal fibroblasts in cancer initiation
and progression. Nature 2004;432(7015):332–7.
4. Folkman J, Kalluri R. Cancer without disease. Nature 2004;427(6977):787.
5. Polyak K, Haviv I, Campbell IG. Co-evolution of tumor cells and their
microenvironment. Trends Genet 2009;25(1):30–8.
6. Allinen M, et al. Molecular characterization of the tumor microenvironment in
breast cancer. Cancer Cell 2004;6(1):17–32.
7. Tlsty TD, Coussens LM. Tumor stroma and regulation of cancer development.
Annu Rev Pathol 2006;1:119–50.
8. Pollard JW. Tumour-educated macrophages promote tumour progression and
metastasis. Nat Rev Cancer 2004;4(1):71–8.
9. de Visser KE, Eichten A, Coussens LM. Paradoxical roles of the immune system
during cancer development. Nat Rev Cancer 2006;6(1):24–37.
10. Casey T, et al. Molecular signatures suggest a major role for stromal
cells in development of invasive breast cancer. Breast Cancer Res Treat
2009;114(1):47–62.
11. Ostman A, Augsten M. Cancer-associated fibroblasts and tumor growth –
bystanders turning into key players. Curr Opin Genet Dev 2009;19(1):67–73.
12. Paez-Ribes M, et al. Antiangiogenic therapy elicits malignant progression
of tumors to increased local invasion and distant metastasis. Cancer Cell
2009;15(3):220–31.
13. Gentleman RC, Carey VJ, Bates DM, Bolstad B, Dettling M, Dudoit S, et al.
Bioconductor: Open software development for computational biology and
bioinformatics. Genome Biol 2004;5:R80.
14. Barrett T, et al. NCBI GEO: mining tens of millions of expression profiles –
database and tools update. Nucleic Acids Res 2007;35(Database issue):D760–5.
15. Cox DR. Regression models and life tables. J R Stat Soc Ser B 1972;34:187–220.
16. Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and
powerful approach to multiple testing. J R Stat Soc B 1995;57:289–300.
17. Subramanian A, et al. Gene set enrichment analysis: a knowledge-based
approach for interpreting genome-wide expression profiles. Proc Natl Acad Sci
U S A 2005;102(43):15545–50.
18. Planet E. PhenoTest: Tools to test correlation between gene expression and
phenotype. R package version 1.0.0., 2010.
19. van ’t Veer LJ, et al. Gene expression profiling predicts clinical outcome of breast
cancer. Nature 2002;415(6871):530–6.

M. Morales et al. / The Breast 20 (2011) S50–S55 S55
20. Zhang, X.H., et al. Latent bone metastasis in breast cancer tied to Src-dependent
survival signals. Cancer Cell 2009;16(1):67–78.
21. Massague J, Gomis RR. The logic of TGFbeta signaling. FEBS Lett 2006;580(12):
2811–20.
22. Markowitz S, et al. Inactivation of the type II TGF-beta receptor in colon cancer
cells with microsatellite instability. Science 1995;268(5215):1336–8.
23. Massague J. TGFbeta in cancer. Cell 2008;134(2):215–30.
24. Walker RA, Dearing SJ. Transforming growth factor beta 1 in ductal carcinoma in
situ and invasive carcinomas of the breast. Eur J Cancer 1992;28(2–3):641–4.
25. Wikstrom P, et al. Transforming growth factor beta1 is associated with
angiogenesis, metastasis, and poor clinical outcome in prostate cancer. Prostate
1998;37(1):19–29.
26. Padua D, et al. TGFbeta primes breast tumors for lung metastasis seeding
through angiopoietin-like 4. Cell 2008;133(1):66–77.
27. Tang B, et al. Transforming growth factor-beta can suppress tumorigenesis
through effects on the putative cancer stem or early progenitor cell
and committed progeny in a breast cancer xenograft model. Cancer Res
2007;67(18):8643–52.
28. Mani SA, et al. The epithelial–mesenchymal transition generates cells with
properties of stem cells. Cell 2008;133(4):704–15.
29. Chirgwin JM, Guise TA. Molecular mechanisms of tumor–bone interactions in
osteolytic metastases. Crit Rev Eukaryot Gene Expr 2000;10(2):159–78.
30. Psaila B, Lyden D. The metastatic niche: adapting the foreign soil. Nat Rev Cancer
2009;9(4):285–93.
31. Sethi N, et al. Tumor-derived JAGGED1 promotes osteolytic bone metastasis of
breast cancer by engaging notch signaling in bone cells. Cancer Cell 2011;19(2):
192–205.
32. Kang Y, et al. A multigenic program mediating breast cancer metastasis to bone.
Cancer Cell 2003;3(6):537–49.
33. Aft R, et al. Effect of zoledronic acid on disseminated tumour cells in women
with locally advanced breast cancer: an open label, randomised, phase 2 trial.
Lancet Oncol 2010;11(5):421–8.
34. Goss PE, Chambers AF. Does tumour dormancy offer a therapeutic target? Nat
Rev Cancer 2010;10(12):871–7.


![A Deep Learning Approach for Tissue Spatial Quantification and … › ... › 2020.03.10.985887v1.full.pdf · 65 dynamics drive invasion and metastasis [1]. Tumor-to-stroma ratios](https://img.pdfslide.us/doc/110x75/5f20f372c184c93513224845/a-deep-learning-approach-for-tissue-spatial-quantification-and-a-a-20200310985887v1fullpdf.jpg)