-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
1/22
PATHOLOGY & GENETICS
TUMOURS OF THE NERVOUS SYSTEM
Bethy Suryawathy, dr.,SpPA.,PhD
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
2/22
Tumors of the CNS
General
General - Statistics vary widelyPrimary tumors of the CNS is 9%
of all neoplasms.
Gliomas (50%), followed by Meningiomas (15%), andacoustic nerve
Schwannomas (5-10%). Of all
intracranial tumors, approximately 30% are metastatic.
Relative to site and age
70% of primary intracranial tumors in adults
aresupratentorial.
70% of primary intracranial tumors in children
areinfratentorial
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
3/22
The most common primary malignantintracerebral tumor inadults is
the glioblastoma
multiforme; in children is the medulloblastoma.
PATHOPHYSIOLOGY
Symptoms and Signs Produced by Brain Tumors
orTumor Mass Effect
In general, the signs & symptoms are due
primarily to the tumor Size and Location. Theseeffects are
expressed in two ways:
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
4/22
1. Compression: example - meningioma's compress theadjacent
brain
2. Infiltration: examples - low grade astrocytoma. In
thesecases, the tumor infiltrates and pushs apart importantneural
structures, and thus these structures fail tofunction properly.
Surrounding Edema
Metastatic tumors create most of their mass effects on
the adjacent brain by inducing cerebral edema Consequences:
Hemiation of cerebral and brain stem
structures.
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
5/22
METASTATIC TUMORS
Mode of metastatic extension is usually via the
blood stream to:
1. Bone
Vertebral body
Often metastasize to epidural space (top of column)
with compression of spinal cord.
Result of compression: paraplegia, failure of boweland bladder
control
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
6/22
2. Leptomeninges
Growth of carcinoma cells within leptomeninges =Carcinomatous
Meningitis.
3. Brain
Brain metastases can involve the cerebrum, cerebellum,
or uncommonly, the brain stem. Typically, they are at
thejunction of the cortex and white matter. 80% are from thelung,
breast, melanoma, kidney and Gl tract.
Metastases are discrete, and may be multiple.
Most important effect - surrounding edema, withsubsequent
swelling of white matter. This sometimesresponds to steroids or
hyperosmolar urea.
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
7/22
TUMORS OF MENINGES
Meningioma
A tumor of arachnoid cells, especially those within
the arachnoidal villi. The most common sites reflect
the areas where these villi are most numerous (e.g.
parasagittal area, falx cerebri, sphenoidal ridge, and
olfactory groove).
Age 45-60. Sex: F/M 1.5/1. These are wellcircumscribed benign
tumors which are attached to
and frequently invade the dura.
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
8/22
They cause symptoms by compression of theadjacent brain or by
invasion of the skull, which
commonly shows a reactive hyperostosis. There
are various histologic types.Microscopically : most have
meningothelial
whorls (resembling arachnoidal villi) with
laminated calcifications called psammoma bodies.
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
9/22
PRIMARY NEUROEPITHELIAL
TUMORS
Neuroglial Tumors (Gliomas)
Astrocytomas, anaplastic astrocytomas, and
glioblastoma multiforme together account forapproximately 80% of
primary brain tumors in adults.
Low grade astrocytomas may progress to the anaplastic
variant, which in turn may progress to glioblastoma
multiforme. These tumors occur primarily in the
cerebral hemispheres.
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
10/22
A. Astrocytoma
1. Fibrillary: Astrocytes abundant fibrillary processes
2. Gemistocytic: Large cells with eccentric nuclei and
swollen, glassy, eosinophilic cytoplasm
3. Pilocytic extremely low grade tumors, which tend
to occur in children, and generally are found in the
cerebellum or regron of the 3rd ventricle.
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
11/22
Glial fibrillary Acidic Protein (GFAP) is ahistologic aid in
confirming the astrocytic
origin of these neoplasms. The cytoplasm of
astrocytes contains glial filamentscomprised of GFAP. The
protein has been
isolated and antibodies have been prepared
against it and used to identify the protein in
tumor cells.
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
12/22
B. Glioblastoma Multiforme
Most arise from pre-existing AnaplasticAstrocytomas.
They produce VEGF AND FDGF factors which
encourages blood vessel growth with strikingendothelial
hyperplasia resulting in formation of
glomeruloid and angiomatoid structures.
Local ischemia causes the diagnostic "stellate" foci
of necrosis, which are surrounded by palisadedtumor cells,
(pseudopalisading necrosis)
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
13/22
C. Ependymoma Ependymomas are derived from ependymal cells,
which line all ventricles.
In the first two decades, they constitute 5 -10% ofbrain tumors,
and are found typically in the 4th
ventricle where they form solid/papillary masses
projecting from the floor of the ventricle. They
often cause obstruction of the 4th ventricle with
obstructive hydrocephalus. The prognosis is poor
because their location prevents complete removal.
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
14/22
D. Oligodendroglioma These tumors arise in the cerebral
hemispheres
of adults, where they appear as well-
circumscribed gelatinous grey masses. There
are sheets of monotonous cells with uniform
central nuclei, surrounded by a clear halo of
cytoplasm. These resemble a "fried-egg".
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
15/22
E. Meduloblastoma A primitive, undifferentiated embryonal
tumor
derived from neuroepithelial stem cells.
They are the most commom primary intracranialtumor of childhood
and account for 25% of all
primary brain tumors in the first 2 decades. They
typically arise in the cerebellum usually in the
midline vermis in young children.
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
16/22
PRIMARY CEREBRAL
LYMPHOMA
Systemic lymphomas/leukemias can secondarily
involve the brain - typically the meninges. Patients in
the late late stages of AIDS frequently developprimary lymphomas
of the CNS. Sporadic cerebral
lymphoma (unasssociated with HIV) typically affects
older adults. Typically, the tumor is deep-seated and
periventricular in distribution (masses, ant. horns oflateral
ventricle), may be nodular or diffuse, and
multiple masses are commom.
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
17/22
Microscopically, these are always
large cell lymphomas which
typically infiltrate and expand the
walls of blood vessels. These have
a poor prognosis with a mean
survival of 18 months. Dramatic
but temporary shrinkage of the
mass follows administration of
corticosteroids.
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
18/22
TUMORS OF PERIPHERAL
NERVES
Schwannoma
Antoni A PatternAntoni B Pattern
*Neurofibroma
Neurofibromatosis type 1 (Von Recklinghausensdisease)
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
19/22
Differentiated astrocytes or precursor cells
Low grade astrocytoma
P53 Mutation (>65%)
PDGF-A, PDGFR-a
Overexpression ( ~ 60%)
LOH 19q (~ 50%)
RB alteration (~25%)
Anaplastic astrocytoma
Secondary glioblastoma
LOH 10q
PTEN mutation (5%)
DCC loss of expression (~50%)PDGFR-a amplification (
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
20/22
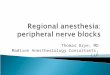
Oligodendrocyte or precursor cells
Oligodendroglioma WHO Grade II
Anaplastic Oligodendroglioma WHO Grade III
EGFRPDGF/PDGFR
overexpression
LOH 1pLOH 19q
LOH 4q
CDK4, EGFR, MYC
Amplification (rare)
VEGF overexpression
CDKN2A deletion
CDKN2C mut./del.
LOH 9p and 10q
Fig.2 Flowchart showing molecular alterations identified in
oligodendrogliomas and
Anaplastic oligodendrogliomas
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
21/22
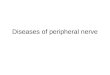
Arachnoidal cells
Meningioma, WHO grade I
Atypical meningioma, WHO grade II
Anaplastic (malignant) meningioma, WHO grade III
NF2 gene mutation / chromosome
22q lost? Other loci
Loses of 1q, 6q, 10q,14q and 18q
Gains of 1q, 9q 12q, 15q, 17q and 20q
Loses of 6q, 9p,10 and 14q
17q amplification
Rare mutation: TP53, PTEN
Rare deletion: CDKN2A
Fig. 3 Genetic changes associated with meningioma
progression
-
7/30/2019 Tumor of CNS and Peripheral Nerve(Dr.betty)
22/22