Embed Size (px)
Citation preview

Tubular secretion and renal Tubular secretion and renal handling of potassiumhandling of potassium
Tubular secretion and renal Tubular secretion and renal handling of potassiumhandling of potassium
Stephen P. DiBartola, DVMStephen P. DiBartola, DVM
Department of Veterinary Clinical SciencesDepartment of Veterinary Clinical Sciences
College of Veterinary MedicineCollege of Veterinary Medicine
Ohio State UniversityOhio State University
Columbus OH 43210Columbus OH 43210

TerminologyTerminology
Transepithelial versus Transepithelial versus transmembrane potential transmembrane potential differencedifference
Luminal versus basolateral Luminal versus basolateral membranesmembranes
Transcellular versus paracellular Transcellular versus paracellular transporttransport
Luminal surfaceLuminal surface
Basolateral surfaceBasolateral surface
Epithelial tight Epithelial tight junctionsjunctions
Just thinkof it as asix-pack
Substances secreted by the Substances secreted by the renal tubulesrenal tubules
Substances secreted by the Substances secreted by the renal tubulesrenal tubules
• Weak acids (organic anions) or weak Weak acids (organic anions) or weak bases (organic cations)bases (organic cations)
• Foreign substances (e.g. drugs, PAH, Foreign substances (e.g. drugs, PAH, PSP)PSP)
• Substances that are not metabolized Substances that are not metabolized and excreted unchanged in the urine and excreted unchanged in the urine (e.g., PAH, PSP)(e.g., PAH, PSP)
• Substances that are slowly metabolized Substances that are slowly metabolized (e.g. thiamine)(e.g. thiamine)

Evidence for tubular secretion: PSPEvidence for tubular secretion: PSPEvidence for tubular secretion: PSPEvidence for tubular secretion: PSP
• 70% of a dose of PSP is excreted after a 70% of a dose of PSP is excreted after a single circulation through the kidneyssingle circulation through the kidneys
• 75% of PSP is bound to plasma 75% of PSP is bound to plasma proteins (25% is free and available for proteins (25% is free and available for filtration)filtration)
• If FF = 20%, only 5% of dose can be If FF = 20%, only 5% of dose can be filtered in one circulation through the filtered in one circulation through the kidneys (20% of 25%)kidneys (20% of 25%)
• 65% of dose must have gotten into the 65% of dose must have gotten into the urine by secretion (70% - 5%)urine by secretion (70% - 5%)
Normal plasma constituents that Normal plasma constituents that undergo secretion at specific sites in undergo secretion at specific sites in
the renal tubulethe renal tubule
Normal plasma constituents that Normal plasma constituents that undergo secretion at specific sites in undergo secretion at specific sites in
the renal tubulethe renal tubule
• Hydrogen ionsHydrogen ions
• AmmoniumAmmonium
• PotassiumPotassium
• UrateUrate
Renal handling of potassiumRenal handling of potassiumRenal handling of potassiumRenal handling of potassium
• Kidneys are the primary regulator Kidneys are the primary regulator of potassium balanceof potassium balance
• Potassium is the only plasma Potassium is the only plasma electrolyte that is both electrolyte that is both reabsorbed and secreted by the reabsorbed and secreted by the tubulestubules
Renal handling of potassiumRenal handling of potassiumRenal handling of potassiumRenal handling of potassium
• Independent of state of balanceIndependent of state of balance• 60% reabsorbed passively in proximal tubule60% reabsorbed passively in proximal tubule• 20% reabsorbed in thick ascending limb of 20% reabsorbed in thick ascending limb of
Henle’s loop via NaHenle’s loop via Na++-K-K++-2Cl-2Cl-- carrier carrier
• Dependent on state of balanceDependent on state of balance• Secretion by principal cells in cortical collecting Secretion by principal cells in cortical collecting
duct and outer medullary collecting ductduct and outer medullary collecting duct• Reabsorption by HReabsorption by H++-K-K++ ATPase in Type A ( ATPase in Type A () )
intercalated cells in inner medullary collecting intercalated cells in inner medullary collecting ductduct

Renal potassium handling: Renal potassium handling: Proximal tubuleProximal tubule
Renal potassium handling: Renal potassium handling: Proximal tubuleProximal tubule
• Early proximal tubuleEarly proximal tubule• TEPD lumen negativeTEPD lumen negative• KK++ reabsorbed with reabsorbed with
water by solvent dragwater by solvent drag
• Late proximal tubuleLate proximal tubule• TEPD lumen positiveTEPD lumen positive
• Paracellular route Paracellular route importantimportant

Renal potassium handling: thick Renal potassium handling: thick ascending limb of Henle’s loopascending limb of Henle’s loop
Renal potassium handling: thick Renal potassium handling: thick ascending limb of Henle’s loopascending limb of Henle’s loop
• TEPD lumen TEPD lumen positivepositive
• Paracellular route Paracellular route importantimportant
• Basolateral exit via Basolateral exit via KK++ channels and channels and KK++-Cl-Cl-- cotransportercotransporter

Renal potassium handling: Late Renal potassium handling: Late distal tubule and collecting ductdistal tubule and collecting ductRenal potassium handling: Late Renal potassium handling: Late distal tubule and collecting ductdistal tubule and collecting duct
• Principal cells Principal cells responsible for responsible for KK++ secretion secretion
• TEPD lumen TEPD lumen negativenegative

Renal potassium handling: Late Renal potassium handling: Late distal tubule and collecting ductdistal tubule and collecting ductRenal potassium handling: Late Renal potassium handling: Late distal tubule and collecting ductdistal tubule and collecting duct
• Type A (Type A () intercalated ) intercalated cells reabsorb Kcells reabsorb K++ and and secrete Hsecrete H++
• KK++ enters at luminal enters at luminal membrane by Hmembrane by H++-K-K++ ATPaseATPase
• KK++ exits at basolateral exits at basolateral membrane by Kmembrane by K++ channelchannel
Major factors affecting KMajor factors affecting K++ movement movement across cortical collecting duct epitheliumacross cortical collecting duct epithelium
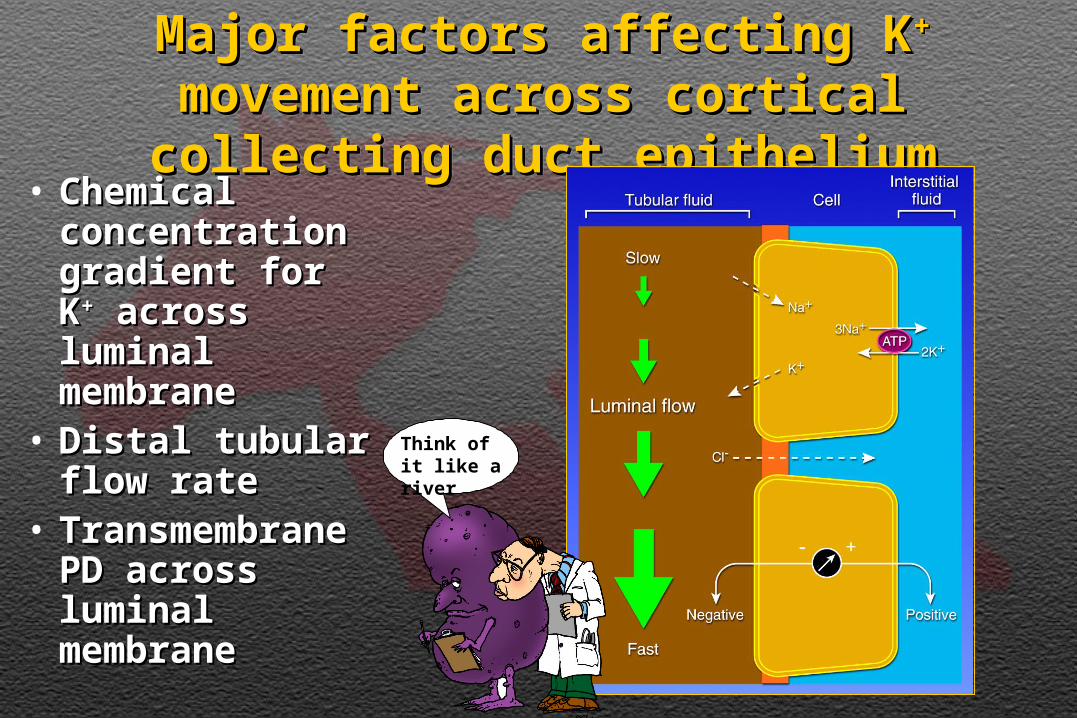
Major factors affecting KMajor factors affecting K++ movement movement across cortical collecting duct epitheliumacross cortical collecting duct epithelium• Chemical Chemical
concentration concentration gradient for Kgradient for K++ across luminal across luminal membranemembrane
• Distal tubular Distal tubular flow rateflow rate
• Transmembrane Transmembrane PD across PD across luminal luminal membranemembrane
Think of it like a river
Factors influencing renal Factors influencing renal excretion of potassiumexcretion of potassium
Factors influencing renal Factors influencing renal excretion of potassiumexcretion of potassium
• Sodium intakeSodium intake
• Potassium intakePotassium intake
• Mineralocorticoids (i.e. aldosterone)Mineralocorticoids (i.e. aldosterone)
• Hydrogen ion balanceHydrogen ion balance
• DiureticsDiuretics
Increased sodium intakeIncreased sodium intakeIncreased sodium intakeIncreased sodium intake
• More NaMore Na++ reaches distal tubules and reaches distal tubules and enters cells across luminal membranes enters cells across luminal membranes stimulating Nastimulating Na++-K-K++ ATPase in basolateral ATPase in basolateral membranes and increasing intracellular membranes and increasing intracellular KK++ concentration concentration
• Increased distal delivery of NaIncreased distal delivery of Na++ increases increases tubular flow rate and moves secreted tubular flow rate and moves secreted potassium downstreampotassium downstream
Increased potassium intakeIncreased potassium intakeIncreased potassium intakeIncreased potassium intake
• Increased numbers and activity of Increased numbers and activity of NaNa++-K-K++ ATPase and amplification of ATPase and amplification of basolateral membranes secondary to basolateral membranes secondary to aldosterone secretionaldosterone secretion
• Increased NaIncreased Na++-K-K++ ATPase activity ATPase activity increases intracellular Kincreases intracellular K++ concentration favoring secretionconcentration favoring secretion

AldosteroneAldosteroneStimuli for releaseStimuli for releaseAldosteroneAldosterone
Stimuli for releaseStimuli for release• Volume depletion RAS activation Volume depletion RAS activation
Angiotensin II stimulates zona Angiotensin II stimulates zona glomerulosa of adrenal gland to release glomerulosa of adrenal gland to release aldosteronealdosterone
• Hyperkalemia also stimulates zona Hyperkalemia also stimulates zona glomerulosaglomerulosa
• Other (minor) stimuliOther (minor) stimuli• ACTHACTH• HyponatremiaHyponatremia• Decreased extracellular pH (acidosis)Decreased extracellular pH (acidosis)

AldosteroneAldosteroneEffectsEffects
AldosteroneAldosteroneEffectsEffects
• Main effect is to Main effect is to increase the number increase the number of open Naof open Na++ channels channels in luminal membranes in luminal membranes of principal cellsof principal cells
• Also stimulates HAlso stimulates H++ ATPase in ATPase in luminal membranes of Type luminal membranes of Type A (A () intercalated cells) intercalated cells

AldosteroneAldosteroneInhibition of releaseInhibition of release
AldosteroneAldosteroneInhibition of releaseInhibition of release
• Dopamine (released in response Dopamine (released in response to increased ECF volume)to increased ECF volume)
• Atrial natriuretic peptide Atrial natriuretic peptide (released in response to (released in response to increased ECF volume)increased ECF volume)

Nephron segments affected Nephron segments affected by aldosteroneby aldosterone
Nephron segments affected Nephron segments affected by aldosteroneby aldosterone
• Connecting segment (late distal Connecting segment (late distal tubule)tubule)
•Cortical collecting ductCortical collecting duct• Outer medullary collecting ductOuter medullary collecting duct

Glomerulus…Glomerulus…Proximal tubule…Proximal tubule…
Thin descending LH…Thin descending LH…Thin ascending LH…Thin ascending LH…
Thick ascending LH…Thick ascending LH…Distal convoluted tubule…Distal convoluted tubule…
Connecting segment…Connecting segment…Cortical collecting duct…Cortical collecting duct…
Outer medullary collecting Outer medullary collecting duct…duct…
Inner medullary collecting Inner medullary collecting duct…duct…
Could you remind me again … what are the parts of the nephron?
… What a bozo …

Hydrogen ion balanceHydrogen ion balanceHydrogen ion balanceHydrogen ion balance
• Alkalosis increases urinary excretion of Alkalosis increases urinary excretion of potassiumpotassium
• ACUTE MINERAL METABOLIC acidosis ACUTE MINERAL METABOLIC acidosis decreases urinary excretion of potassiumdecreases urinary excretion of potassium• ORGANIC METABOLIC acidosis does notORGANIC METABOLIC acidosis does not
• CHRONIC METABOLIC acidosis may increase CHRONIC METABOLIC acidosis may increase urinary excretion of potassiumurinary excretion of potassium
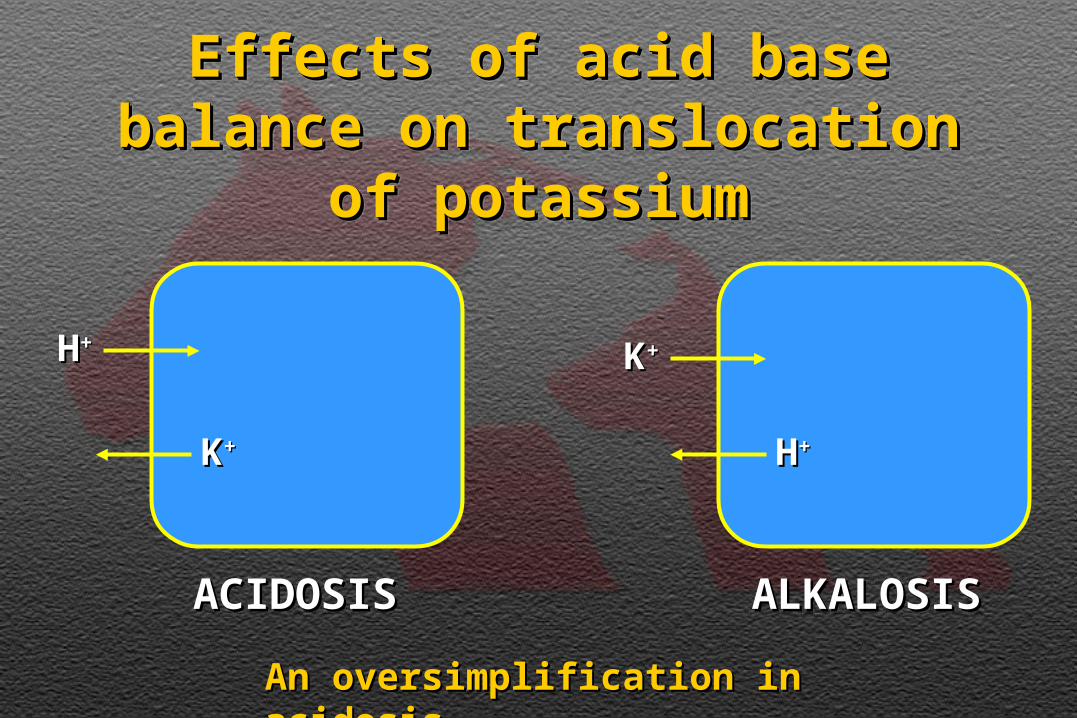
Effects of acid base balance on Effects of acid base balance on translocation of potassiumtranslocation of potassium
Effects of acid base balance on Effects of acid base balance on translocation of potassiumtranslocation of potassium
HH++ KK++
HH++KK++
ACIDOSISACIDOSIS ALKALOSISALKALOSIS
An oversimplification in acidosisAn oversimplification in acidosis
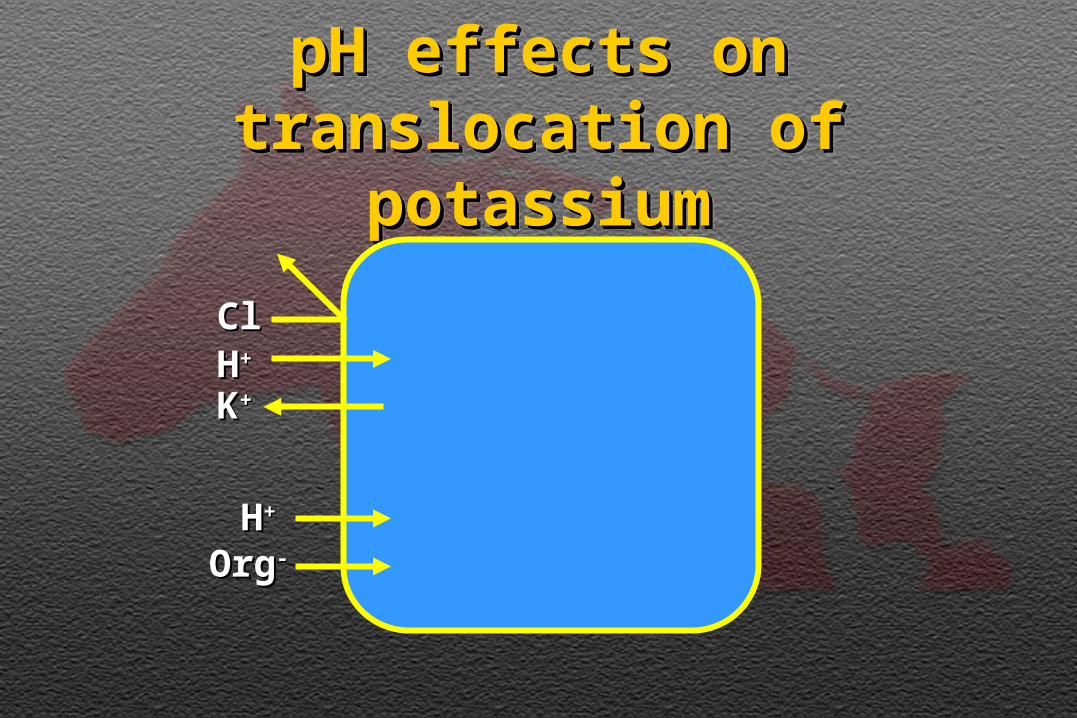
pH effects on translocation pH effects on translocation of potassiumof potassium
pH effects on translocation pH effects on translocation of potassiumof potassium
HH++
ClCl--
OrgOrg--
HH++
KK++
DiureticsDiureticsDiureticsDiuretics
• Many diuretics increase urinary Many diuretics increase urinary excretion of potassium (e.g. excretion of potassium (e.g. furosemide, thiazides, mannitol)furosemide, thiazides, mannitol)
• They do so by increasing distal They do so by increasing distal delivery of sodium and distal delivery of sodium and distal tubular flow ratetubular flow rate

Renal handling of urateRenal handling of urateRenal handling of urateRenal handling of urate
• In veterinary medicine, primarily In veterinary medicine, primarily important in Dalmatian dogsimportant in Dalmatian dogs
• Urate is both reabsorbed and Urate is both reabsorbed and secreted in the renal tubulesecreted in the renal tubule
• Secretion resembles that of PAHSecretion resembles that of PAH• Co-transported into cell with NaCo-transported into cell with Na++ at at
basolateral membranebasolateral membrane• Exits cell at luminal membrane by Exits cell at luminal membrane by
facilitated diffusion down its facilitated diffusion down its concentration gradientconcentration gradient