Embed Size (px)
Citation preview

Tuberkulosis Anak, DOTS, ISTC
Finny Fitry Yani
Courtesy :
UKK Respirologi Anak IDAI
World problems of Tuberculosis (TB)
• Global problem
• Neglected Childhood TB
• Low Case Detection Rate
• Lack of holistic approach of TB management
• Non-standardized management
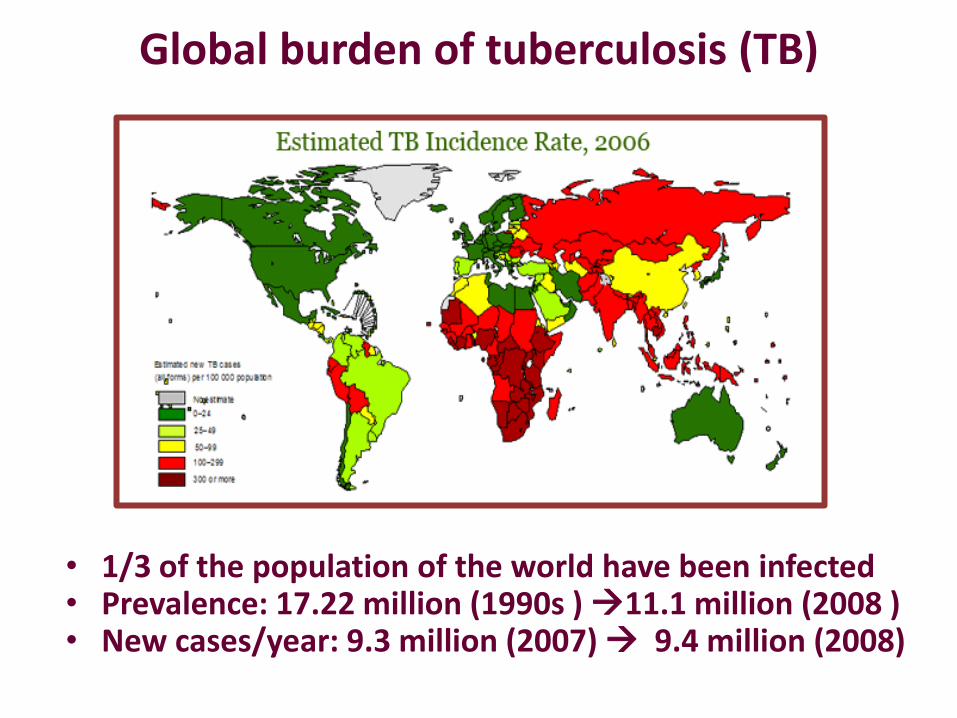
Global burden of tuberculosis (TB)
• 1/3 of the population of the world have been infected • Prevalence: 17.22 million (1990s ) 11.1 million (2008 ) • New cases/year: 9.3 million (2007) 9.4 million (2008)
TUBERCULOSIS PROGRAMS
GOAL:
• to break the chain of the transmission for eliminating the disease from society.
Strategies:
1)case finding and treatment of active disease
2)treatment of LTBI
3)vaccination with BCG
National TB Programs (NTPs)= P2 TB Kemenkes
Focus on adult cases
Pediatric TB
DOTS (Directly Observe Treatment Short-course)
• A global strategy to combat world TB problems
• Developed by WHO and IUATLD
• Introduced in early 1990, implemented in Indonesia since 1994s
DOTS coverage in 2006: 98%

Komitmen Politis dan dukungan
semua pihak
1
WHO 1991
5 KOMPONEN DOTS
2
Diagnosis
mikroskopik
ANAK??
3
Pengawas Menelan Obat
4
Ketersediaan Obat
5
Pencatatan Pelaporan
Cure rate tinggi (pemutusan
rantai transmisi)
Paling cost effective (Bank
Dunia)
Rekomendasi WHO
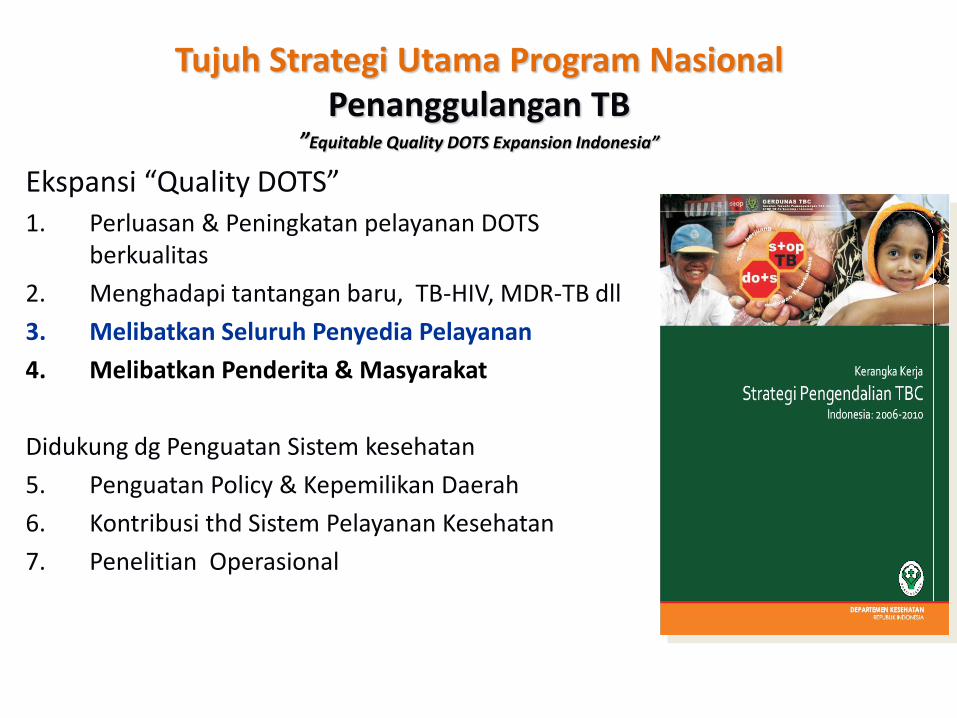
Tujuh Strategi Utama Program Nasional Penanggulangan TB
”Equitable Quality DOTS Expansion Indonesia”
Ekspansi “Quality DOTS” 1. Perluasan & Peningkatan pelayanan DOTS
berkualitas
2. Menghadapi tantangan baru, TB-HIV, MDR-TB dll
3. Melibatkan Seluruh Penyedia Pelayanan
4. Melibatkan Penderita & Masyarakat
Didukung dg Penguatan Sistem kesehatan
5. Penguatan Policy & Kepemilikan Daerah
6. Kontribusi thd Sistem Pelayanan Kesehatan
7. Penelitian Operasional
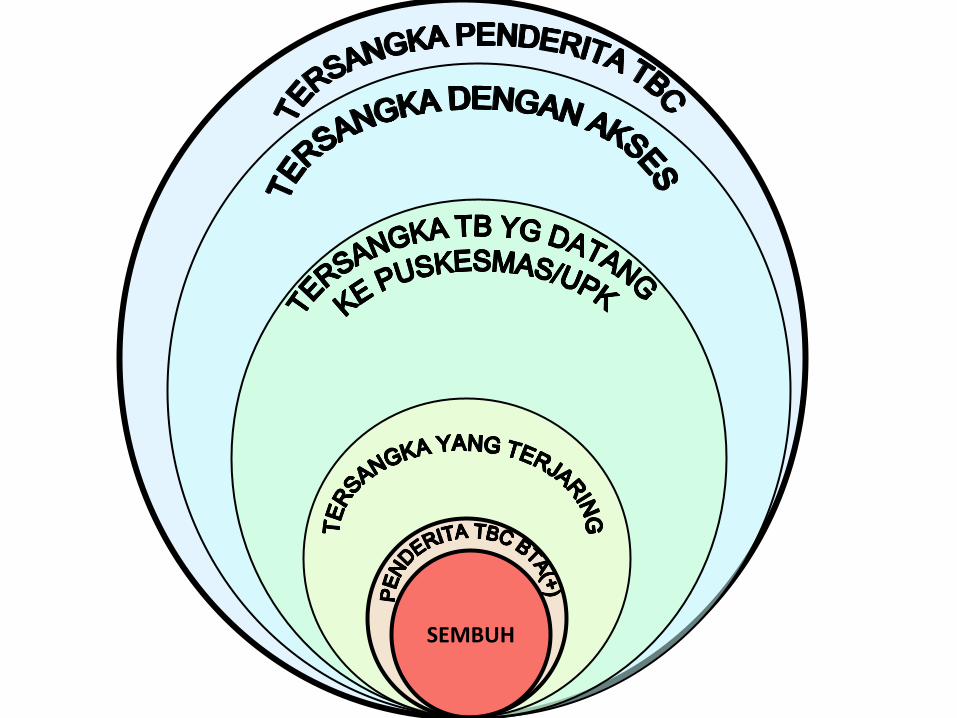
SEMBUH
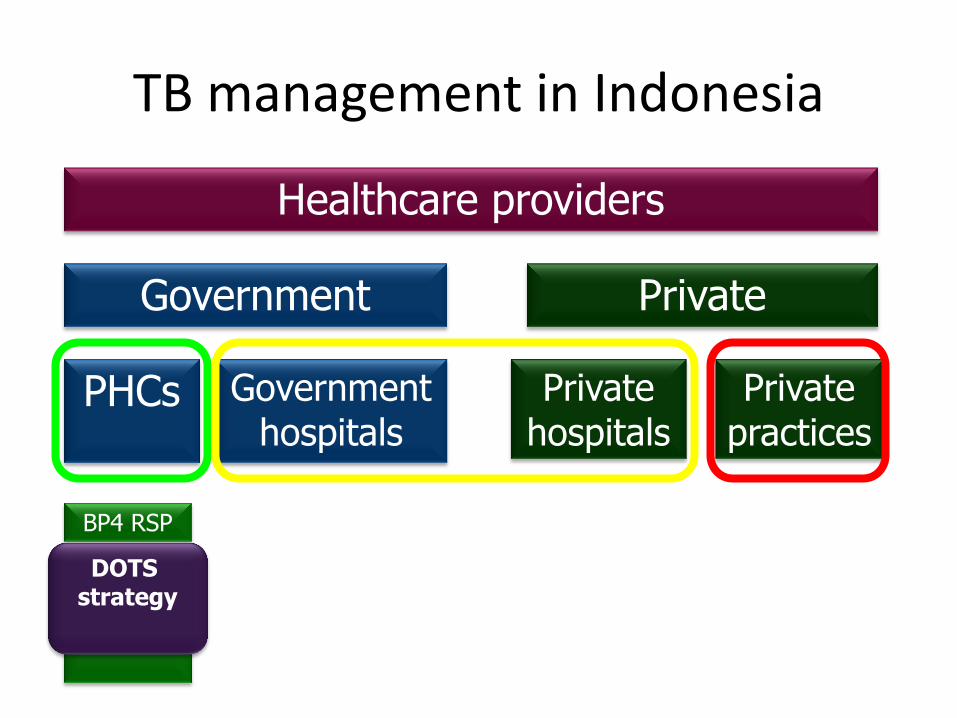
TB management in Indonesia
PHCs
Government Private
Private practices
Private hospitals
Government hospitals
Healthcare providers
BP4 RSP
GP Pulm
DOTS strategy
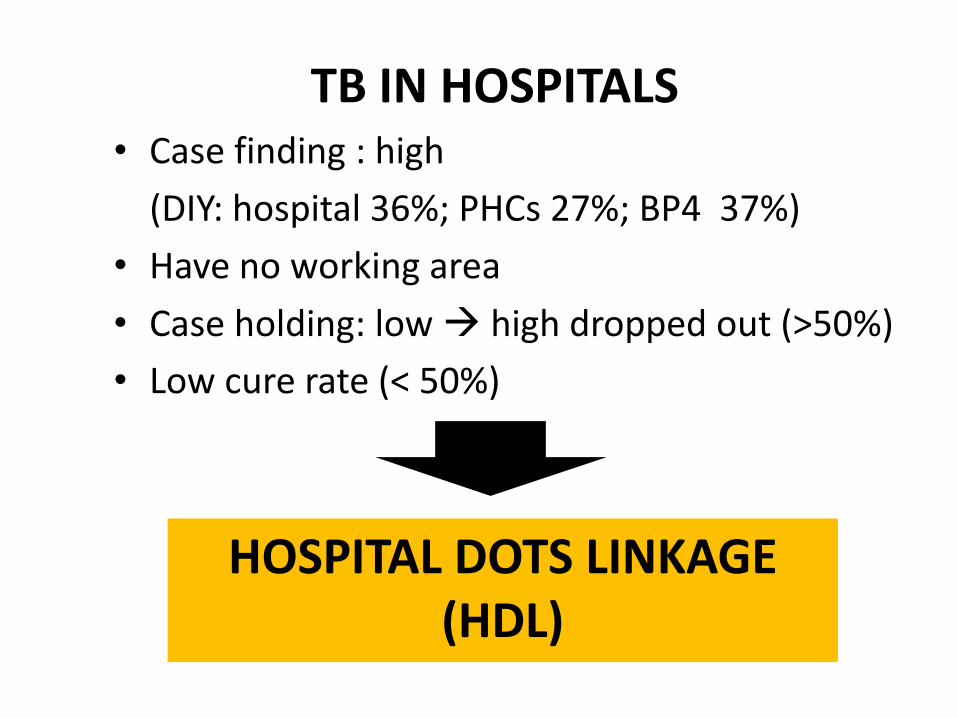
HOSPITAL DOTS LINKAGE (HDL)
TB IN HOSPITALS • Case finding : high
(DIY: hospital 36%; PHCs 27%; BP4 37%)
• Have no working area
• Case holding: low high dropped out (>50%)
• Low cure rate (< 50%)
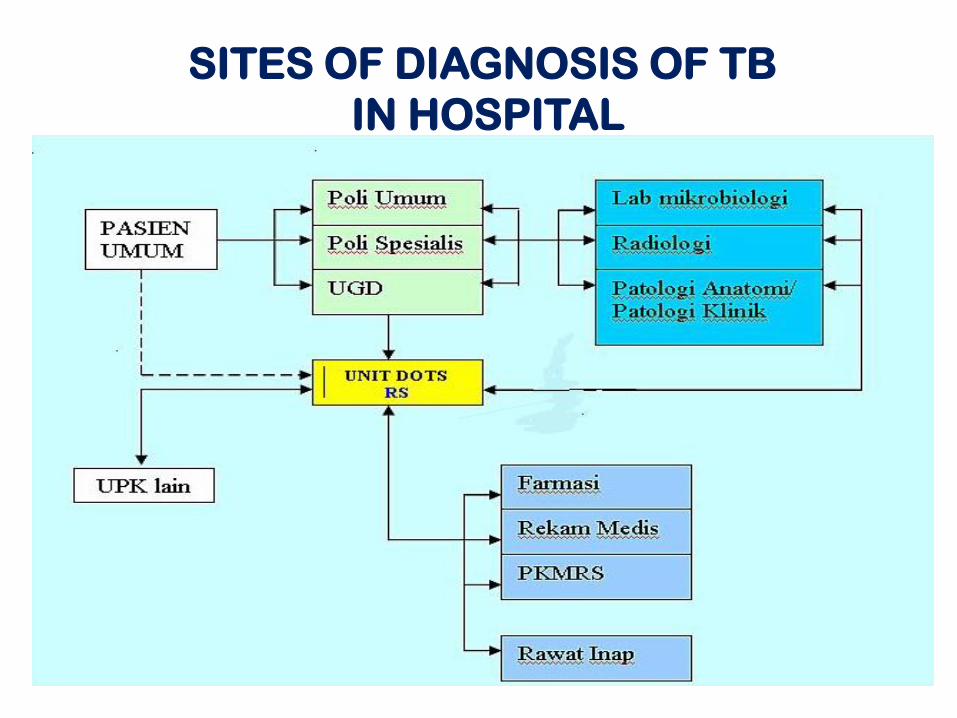
SITES OF DIAGNOSIS OF TB
IN HOSPITAL
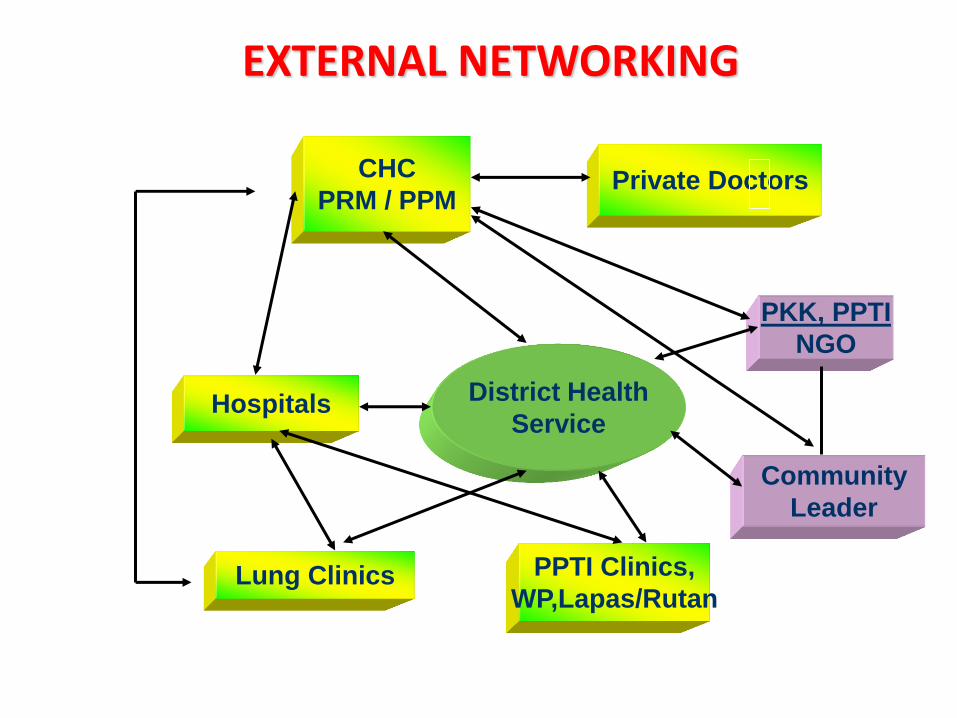
District Health
Service Hospitals
Lung Clinics PPTI Clinics,
WP,Lapas/Rutan
Community
Leader
PKK, PPTI
NGO
Private Doctors CHC
PRM / PPM
EXTERNAL NETWORKING
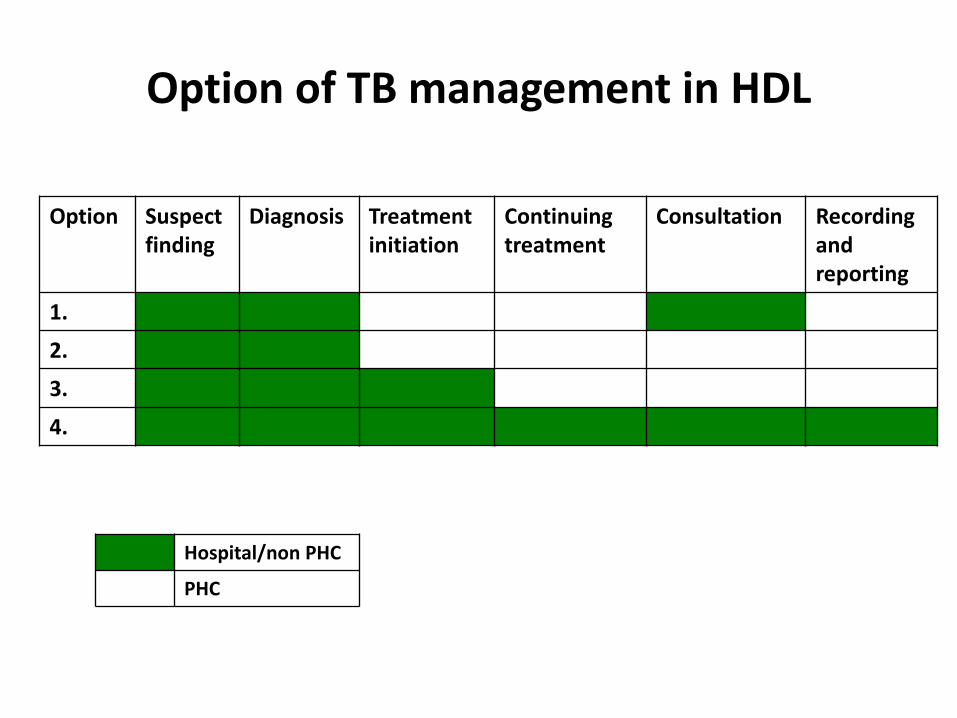
Option of TB management in HDL
Option Suspect finding
Diagnosis Treatment initiation
Continuing treatment
Consultation Recording and reporting
1.
2.
3.
4.
Hospital/non PHC
PHC
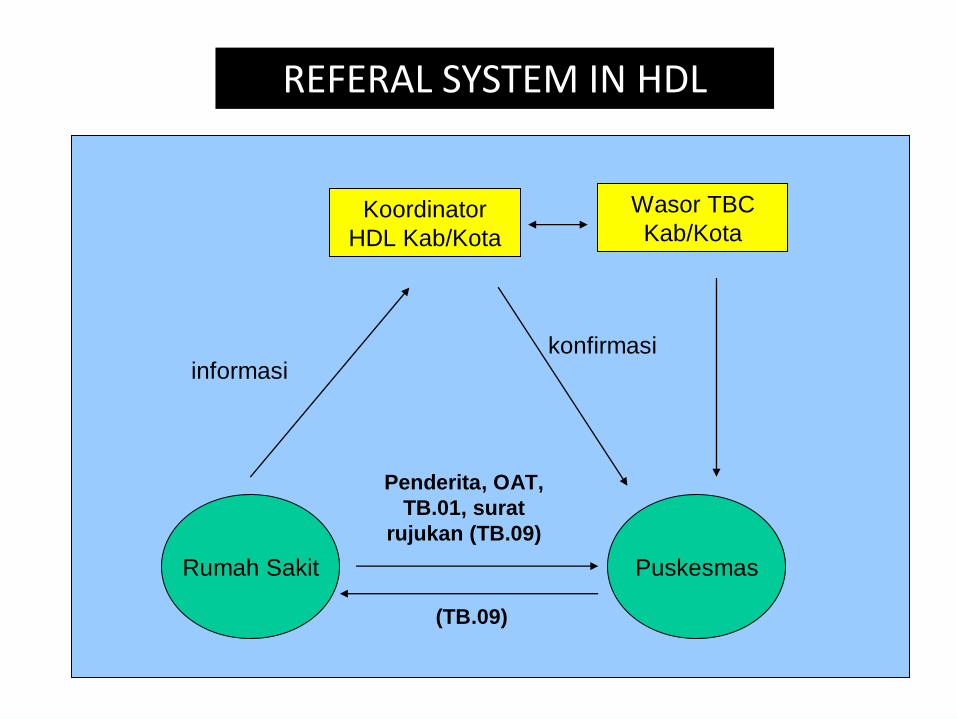
Alur Rujukan Penderita Tuberkulosis
Rumah Sakit Puskesmas
Koordinator
HDL Kab/Kota
Penderita, OAT,
TB.01, surat
rujukan (TB.09)
Wasor TBC
Kab/Kota
informasikonfirmasi
(TB.09)
REFERAL SYSTEM IN HDL
World problems of Tuberculosis (TB)
• The second global cause of death from infectious
agents
• Neglected Childhood TB
• Low Case Detection Rate
• Lack of holistic approach of TB management
• Non-standardized management
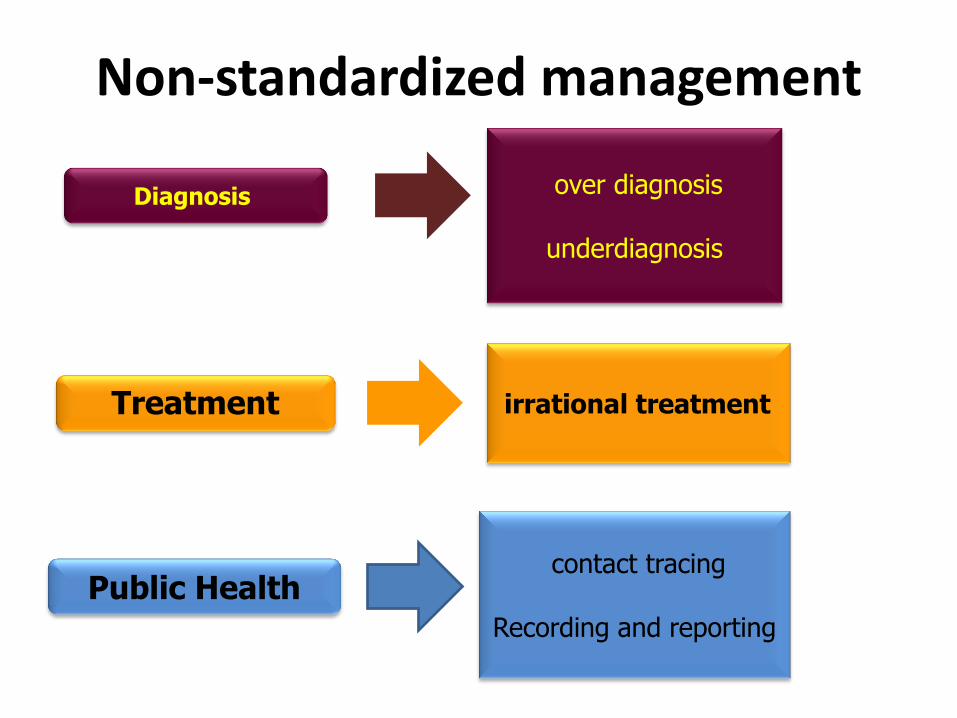
Non-standardized management
Diagnosis
Treatment
Public Health
irrational treatment
over diagnosis
underdiagnosis
contact tracing
Recording and reporting
ISTC (International Standard for TB care)
• Differ from existing guidelines
– standards what should be done
– guidelines how the action is to be accomplished
• Evidence-based, living document
• As a complementary of the existing guideline
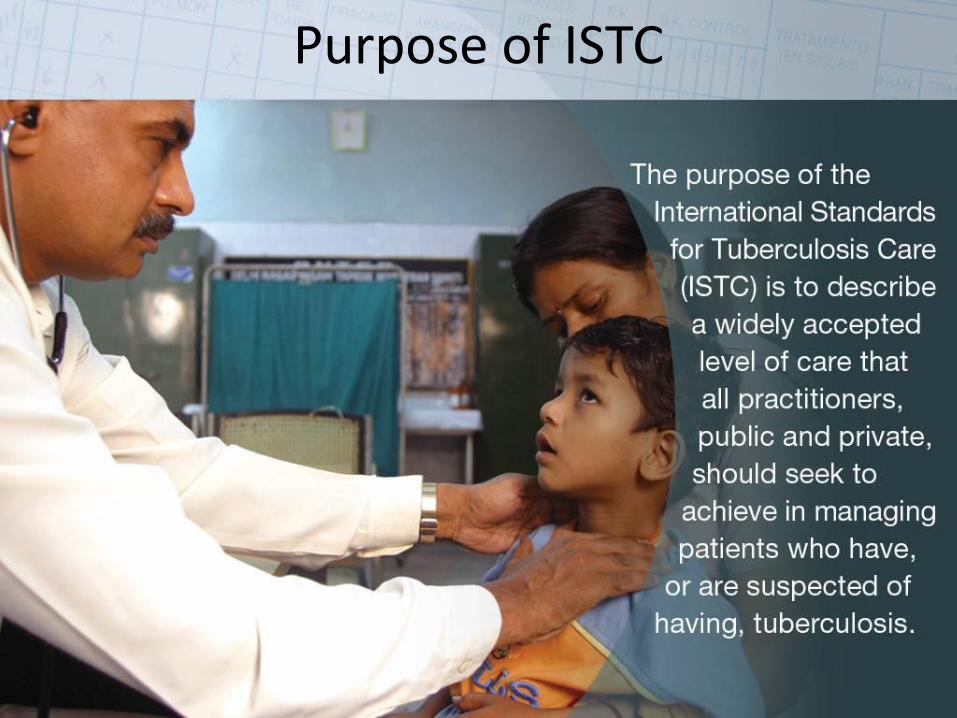
Purpose of ISTC
ISTC
Diagnosis
Treatment
2 standards Public Health
6 standards
9 standards
Standards for Diagnosis Pediatric considerations
Standard 1
All persons with otherwise unexplained productive cough lasting two-three weeks or more should be evaluated for TB
•COUGH is NOT the main symptom of TB •Other symptoms should be considered:
•weight loss or FTT in the last two months •fever >2 weeks with unexplained causes •Close contact with adult Pulmonary TB
Pediatric consideration
Standard 4
All persons with
chest radiographic
findings suggestive
of TB should have
sputum specimens
submitted for
microbiological
examination.
Collecting sputum in children is challenging
If possible, perform induced sputum
or gastric lavage
Pediatric consideration
Standard 6
The diagnosis of
intra-thoracic TB in
symptomatic
children with
negative sputum
smears should be
based on the
finding of chest
radiograph
The appearance of
lymphadenopathy is
subtle and may be
difficult to detect
especially in
malnourished children
and when there is HIV-
related pulmonary disease.
Pediatric consideration

Standards for Treatment pediatric considerations
Standard 8
All patients (incl those
with HIV infection) .....
regimen using drugs of
known bioavailability.
The initial phase should
consist of two months
of isoniazid, rifampicin,
pyrazinamide, and
ethambutol.
•Triple drugs:
INH, Rif and PZA
•Four or five drugs for severe TB
Pediatric consideration
Standards for Public Health
ISTC Standard 16
All providers of care for patients with TB should ensure that persons (especially children under 5
year of age and persons with HIV infection) who are in close contact with patients who have infectious
TB are evaluated and managed in line with international recommendations.
ISTC Standard 16
Children under 5 years of age and persons with HIV infection who have been in contact with an infectious case should be evaluated for both latent infection with M. tb and for active TB.
ISTC Standard 17
All providers must report both new and retreatment TB cases and their treatment outcomes to local public health authorities, in conformance with applicable legal requirements and policies.

Together in partnership we are more than the sum of our parts!





























