-
8/2/2019 Tuberculous Abdomen 11062006
1/43
1
Tuberculous Abdomen
-
8/2/2019 Tuberculous Abdomen 11062006
2/43
2
Definition
Tuberculous abdomen is a condition inwhich there is tuberculous
infection of theperitoneum or other organs in theabdomen
-
8/2/2019 Tuberculous Abdomen 11062006
3/43
3
Robert Koch, a German Scientist who found outthe causative
organism for consumption and
revealed his invention in1882
-
8/2/2019 Tuberculous Abdomen 11062006
4/43
4
Gram negative bacillusMycobacterium tuberculosis
-
8/2/2019 Tuberculous Abdomen 11062006
5/43
5
Ways of presentation Acute tuberculous peritonitis
Chronic tuberculous peritonitis
Tuberculous stricture of the intestine(small) causing subacute
intestinalobstruction
Ileo caecal tuberculosis presenting with amass in the right
iliac fossa
-
8/2/2019 Tuberculous Abdomen 11062006
6/43
6
Acute tuberculous peritonitis Acute abdomen with severepain
Acute inflammation of the peritoneum
Straw coloured fluid Tubercles in the greater omentum and
peritoneum
Tubercles may casseate Anti tuberculous treatment
-
8/2/2019 Tuberculous Abdomen 11062006
7/43
7
Chronic tuberculous peritonitis The condition presents with
abdominal
pain
Fever
Loss of weight
Ascites
Nightsweats
Abdominalmass
-
8/2/2019 Tuberculous Abdomen 11062006
8/43
8
Origin of infection Tuberculous mesenteric lymph nodes
Tuberculosis of the ileocaecal region
Tuberculous pyosalpinx
Blood borne infection from pulmonarytuberculosis, usually the
miliary but
occasionally the cavitating form
-
8/2/2019 Tuberculous Abdomen 11062006
9/43
9
Varieties of tuberculous peritonitis Ascitic form peritoneal
fluid distension of
abdomen. Patient comes with the complaint of swelling
of the abdomen. increased abdominal pressureumbilical hernia,
inguinal hernia
Purulent form
Rare usually secondary to tuberculous salpingitispockets of
adherent intestines and omentum containingtuberculous pus. cold
abscesses
Encysted form
Inflammation and ascites are confined to one part of
theabdominal cavity
Fibrous form
Wide spread adhesions
adhesive obstruction
G
-
8/2/2019 Tuberculous Abdomen 11062006
10/43
10
GastrointestinalTuberculosis
Abdominal tuberculosis is usually secondary to
pulmonary tuberculosis, radiologic evaluation oftenshows no
evidence of lung disease
Ileocecum and ColonThe ileocecal region is the most common area
of
involvement in the gastrointestinal tract due to theabundance of
lymphoid tissue.
The natural course of gastrointestinal tuberculosismay
beulcerativehypertrophic orulcerohypertrophic.
G i i l T b l i
-
8/2/2019 Tuberculous Abdomen 11062006
11/43
11
Gastrointestinal Tuberculosis
Barium studies demonstrate spasm andhypermotility with edema of
the ileocecal valve inthe early stages
Later thickening of the ileocecal valve.
A widely gaping ileocecal valve with narrowing
of the terminal ileum (Fleischner sign) A narrowed terminal
ileum with rapidemptying
of the diseased segment through a gapingileocecal valve into a
shortened, rigid,
obliterated cecum (Stierlin sign) Focal or diffuse aphthous
ulcers : tend to be
linearorstellate, following the orientation oflymphoid follicles
(ie, longitudinal in the terminal
ileum and transverse in the colon)
-
8/2/2019 Tuberculous Abdomen 11062006
12/43
12
Gastrointestinal Tuberculosis
In advanced cases,symmetric annularstenosis and
obstructionassociated with shortening, retraction,
andpouchformation may be seen.
The cecum becomes conical, shrunken,and retractedout of the
iliac fossa due tofibrosis within the mesocolon,
Ileocecal valve becomes fixed, irregular,gaping, and
incompetent
-
8/2/2019 Tuberculous Abdomen 11062006
13/43
13
Investigations Blood routine
Urine routine - to detect diabetes mellitus
Plain X-ray of the abdomen
Laparoscopy
Laparoscopicbiopsy of tubercles foun inthe peritoneum or other
parts
-
8/2/2019 Tuberculous Abdomen 11062006
14/43
14
Treatment
Antituberculous treatmentdrugs : Akurit 4
Ripe Kit
isoniazid
rifampicin
pyrazinamide
ethambutol
Surgicalintervention as and whenneeded
C l i f M b t i
-
8/2/2019 Tuberculous Abdomen 11062006
15/43
15
Colonies of Mycobacterium
tuberculosisLowenstein-Jensen
med
Ch i l t b l i A h i t b l
-
8/2/2019 Tuberculous Abdomen 11062006
16/43
16
Chronic pulmonary tuberculosis.A chronic tuberculouscavity is
seen in the apical-posterior segment of theright upper lobe.
Peribronchial tubercles are present
throughout the remainder of the right lung.
-
8/2/2019 Tuberculous Abdomen 11062006
17/43
17
Circumferential ulceration is characteristic of
intestinal tuberculosis.
-
8/2/2019 Tuberculous Abdomen 11062006
18/43
18
TB is transmitted by airborne droplet nuclei,which may contain
fewer than 10 bacilli.
Exposure to TB occurs by sharing commonairspace with a patient
who is infectious. Wheninhaled, droplet nuclei are deposited within
theterminal airspaces of the lung. Upon
encountering the bacilli, macrophages ingestand transport the
bacteria to regional lymphnodes
-
8/2/2019 Tuberculous Abdomen 11062006
19/43
19
The bacilli have 4 potential fates:
(1) they may be killed by the immune system,
(2) they may multiply and cause primary TB,
(3) they may become dormant and remainasymptomatic, or
(4) they may proliferate after a latency period(reactivation
disease). Reactivation disease mayoccur following either (2) or (3)
above.
Gastrointestinal TB: Any site along the
-
8/2/2019 Tuberculous Abdomen 11062006
20/43
20
Gastrointestinal TB: Any site along thegastrointestinal tract
may become infected.Symptoms are referable to the site
infected,including the following:
nonhealing ulcers of the mouth or anus;
difficulty swallowing with esophageal disease;
abdominal pain mimicking peptic ulcer diseasewith stomach or
duodenal infection;
malabsorption with infection of the smallintestine;
and pain, diarrhea, or hematochezia with
infection of the colon.
-
8/2/2019 Tuberculous Abdomen 11062006
21/43
21
Emaciation due to TB
-
8/2/2019 Tuberculous Abdomen 11062006
22/43
22
Tuberculosis of the skin
-
8/2/2019 Tuberculous Abdomen 11062006
23/43
23
Lupus vulgaris on the face of an 88 y-o female (gross
findings).@Thefacial skin is the most common site of reinfection
tuberculosis of this
form.
http://www.yamagiku.co.jp/pathology/photo/photo163-3.htm
-
8/2/2019 Tuberculous Abdomen 11062006
24/43
-
8/2/2019 Tuberculous Abdomen 11062006
25/43
25
Mantoux Test
-
8/2/2019 Tuberculous Abdomen 11062006
26/43
26
Mantoux positive
M i th i d ti M t t
-
8/2/2019 Tuberculous Abdomen 11062006
27/43
27
Measuring the induration Mx test
-
8/2/2019 Tuberculous Abdomen 11062006
28/43
28
Tuberculous ulcers in the intestine
-
8/2/2019 Tuberculous Abdomen 11062006
29/43
29
Bilateral Extensive Tuberculosis
-
8/2/2019 Tuberculous Abdomen 11062006
30/43
30
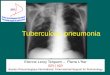
Tuberculouspneumonitic
patch
T b l
http://www.emedicine.com/med/images/2324Dsc00001.jpg
-
8/2/2019 Tuberculous Abdomen 11062006
31/43
31
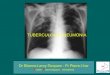
Tuberculousinfiltration
withcavitation
http://www.emedicine.com/med/images/2324Dsc00001.jpg
-
8/2/2019 Tuberculous Abdomen 11062006
32/43
32
Tuberculouspneumonitis
http://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpg
-
8/2/2019 Tuberculous Abdomen 11062006
33/43
33
http://www.emedicine.com/med/images/2324Dsc00001.jpg
-
8/2/2019 Tuberculous Abdomen 11062006
34/43
34
http://www.emedicine.com/med/images/2324Dsc00001.jpg
-
8/2/2019 Tuberculous Abdomen 11062006
35/43
35
Tuberculousperitonitis
USGM Intestinesfloating inperitoneal
fluid - ascites
Mycobacterium tuberculosis Acid-fast stain
http://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpg
-
8/2/2019 Tuberculous Abdomen 11062006
36/43
36
Mycobacterium tuberculosis. Acid-fast stain
http://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpg
-
8/2/2019 Tuberculous Abdomen 11062006
37/43
37
Gram negative bacilli in sputum
http://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpg
-
8/2/2019 Tuberculous Abdomen 11062006
38/43
38
Caseation
L h i t ll
http://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpg
-
8/2/2019 Tuberculous Abdomen 11062006
39/43
39
Langhans giant cells
http://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.emedicine.com/med/images/2324Dsc00001.jpghttp://www.microscopyu.com/galleries/pathology/tuberculosis.html
-
8/2/2019 Tuberculous Abdomen 11062006
40/43
40
http://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.html
-
8/2/2019 Tuberculous Abdomen 11062006
41/43
41
Drugs used to treat TB disease. From left to rightisoniazid,
rifampin, pyrazinamide, and ethambutol.
Streptomycin (not shown) is given by injection
http://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.html
-
8/2/2019 Tuberculous Abdomen 11062006
42/43
42
Gastrointestinal Tuberculosis: This is uncommontoday because
routine pasteurization of milk haseliminated Mycobacterium bovis
infections. However, M.
tuberculosis organisms coughed up in sputum may beswallowed into
the GI tract. The classic lesions arecircumferential ulcerations
with stricture of the smallintestine. There is a predilection for
ileocecalinvolvement because of the abundant lymphoid tissue
and slower rate of passage of lumenal contents.
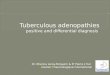
Scrofula: Tuberculous lymphadenitis of the cervicalnodes may
produce a mass of firm, matted nodes just
under the mandible. There can be chronic drainingfistulous
tracts to overlying skin. This complication mayappear in children,
and Mycobacterium scrofulaceummay be cultured.
http://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.html
-
8/2/2019 Tuberculous Abdomen 11062006
43/43
43
The name tuberculosis comes from tubercles. These are
small, hard lumps that form when the immune systembuilds a wall
around the TB bacteria in the lungs.
There are two kinds of active TB.
Primary TB occurs soon after a person is first exposedto TB.
Reactivation TB occurs in people who were previouslyexposed to
TB. If their immune system is weakened, TBcan break out of the
tubercles and cause active disease.Most of the cases of TB in
people with HIV are due toreactivation of a previous TB
infection.
Active TB can cause the following symptoms: coughingfor more
than 3 weeks, weight loss, constant fatigue,night sweats, and
fevers, especially in the evening
http://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.htmlhttp://www.microscopyu.com/galleries/pathology/tuberculosis.html