Embed Size (px)
Citation preview

11/13/2014
1
TB IntensiveSan Antonio, Texas
November 11‐14, 2014
Tuberculosis in Children Kim Smith, MD, MPHNovember 13, 2014
Kim Smith, MD, MPH has the following disclosures to make:
• No conflict of interests
• No relevant financial relationships with any commercial companies pertaining to this educational activity

11/13/2014
2
PEDIATRIC TUBERCULOSISKim Connelly Smith, MD, MPH
OUTLINE•Stages of tuberculosis•Differences of diseasein children and adults
•Diagnostic challengesof pediatric TB
•Treatment of TB in children•Clinical cases

11/13/2014
3
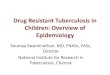
STAGES OF TUBERCULOSIS
Exposureto Contagious Adult with
Pulmonary Disease
Latent TB InfectionLTBI
Adult Active TB Disease
Child Active TB Disease
20-30%
5-10% Risk varies by age5-50%
Householdcontacts
0
10
20
30
40
50
60
0-12months
12-48months
4-11years
12-18years
HealthyAdults
Risk of Disease with no Treatmentby Age at Infection
Per
cen
t
Age at TB Infection

11/13/2014
4
RISK OF PROGRESSION TO TB DISEASE BY AGE
Age @ primary infectionBirth-12months
1-2 years
Risk of Disease
Disease 50%Pulmonary Dis 30-40%Miliary or TBM 10-20%
Disease 20-25%Pulmonary Dis 75%Miliary or TBM 2-5%
Marais BJ. Int J Tuberc Lung Dis 2004;8:392-402
TREATMENT OF TB IN CHILDREN
Stages of TB TST/IGRACXR/Lab Physical Symptoms Treatment
ExposureChild <4yrs (adult source)
Negative Normal None Window CPX 8-10 wksRepeat TST 8-10 wks after last contact
LTBI Positive Normal None INH x 9 months or Rif x 4-6 months
Disease 90% Positive
50% false negwith miliaryand TBM
AbnormalCXR, PE or labs
50% of children have symptoms
RIPE x 6-12 months, durationdepends on site

11/13/2014
5
Daycare Exposure
DAYCARE EXPOSURE
Index case, teacher assistant with AFB smear positive pulmonary disease and cough for 6 weeks
135 children < 4 years of age, plus adult staff members exposed
Smith, KC. Southern Medical Journal 93(9):877-880, 2000

11/13/2014
6
DAYCARE EXPOSURE MANAGEMENT
o Who is at risk?o Children and staff
o Who needs TST?o Everyone with significant contact with source case
o Who needs CXR?o All children less than 4 years of age even if TST negative o Any contacts with positive TST (> 5mm)
o Who needs treatment?o LTBI (positive TST >5mm and normal CXR) INH for 9 months or Rif x
4-6 monthso Exposed children less than 4 years of age (window prophylaxis)
o Follow up:o Skin test conversions: 4 adults and 3 childreno No TB disease
WINDOW PROPHYLAXIS FOR EXPOSURE
Household contact with contagious person Teen or adult with pulmonary TB disease Usually > 4 hours of contact
Initial TST negative Window period for TST conversion
(8-10 weeks) CXR and physical exam normal INH prophylaxis recommended:
For children <4 yrs of age Immunosuppressed patients May prevent progression to disease during
window period Repeat TST 8-10 wks after exposure May stop INH if 2nd TST negative <5mm in
immunocompetent patients

11/13/2014
7
PREVENTABLE CASE
PEDIATRIC TB CASE:MISSED OPPORTUNITY
15 mo old 10 days fussiness & decreased appetite 3 days inability to walk or sit up Lumbar puncture: CSF: 96 WBC (NL <7), 72% Lymphs,
198 Protein (NL <45), Glucose 8 Source case: mother of child Child’s diagnosis: TB Meningitis
Family history Mom with pulmonary TB diagnosed 5 mo earlier on
appropriate RIPE treatment Dad diagnosed with LTBI on INH Baby initial TST 0mm @ 10 months of age no CXR no treatment lost to follow up

11/13/2014
8
TB MENINGITIS
Youssef FG, et al. Diagn Microbiol Infect Dis 2006;55(4):275-8

11/13/2014
9
TB MENINGITISTREATMENT AND CLINICAL COURSE
9-12 months RIPE therapy Steroids for 1-2 month with 2-3 week taper
decreases CNS inflammation
Fever common for first month, symptoms may initially worsen followed by gradual improvement
Possible complications Seizures Hydrocephalus CNS tuberculoma, stroke, mental disabilities, CP Mortality high (>90%) if not diagnosed and treated
*Feigin & Cherry, Text of Pedi ID
TTimetable of Tuberculosis

11/13/2014
10
DIFFERENCES INADULT AND PEDIATRIC TB
REACTIVATION DISEASE
Occurs years after primary infection
Typical of adult disease Occasionally seen in
teens Often cavitary disease High numbers of
organisms (AFB +) Usually symptomatic
and contagious

11/13/2014
11
PRIMARY TB DISEASE
Typical of childhood TBUsually not cavitary
Classic x-ray: Hilar lymphadenopathy +/-
infiltrates or Miliary pattern
Low numbers of organisms AFB smears negative (95%) Cultures negative in 60% of
cases
Most children <12 yrs not contagious
Often asymptomatic (50%)

11/13/2014
12

11/13/2014
13
RADIOGRAPHIC FINDINGS INPEDIATRIC TB DISEASE
Hilar and interthoraciclymphadenopathy
Miliary pattern
Basilar enhancement on brain imaging
Apical cavitary lesions in adults and teens
Lobar pneumonia
Pleural effusion in adults and teens
Typical of TB Not specific but common

11/13/2014
14
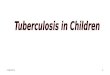
TB DISEASE
Pulmonary
Extrapulm
15%85%
Pulmonary
Extrapulmonary
25%75%
Adult TB Disease Pediatric TB Disease
Lymphatic25%
Pleural23%GU
16%
Meningeal4%
Bone/Joint10%
Miliary9%
Other13%
Adult Extrapulmonary TB Disease (15%)
Lymphatic
Pleural
GU
Meningeal
Bone/Joint
Miliary
Other

11/13/2014
15
Lymphatic65%
Meningeal14%
Pleural6%
Miliary 5%
Other5%
Bone/Joint5%
Extrapulmonary TB Disease in Children (25%)
Lymphatic
Meningeal
Pleural
Miliary
Other
Bone/Joint
COMMON SYMPTOMS OF TB DISEASE IN CHILDREN
(NONSPECIFIC)
Cough and/or respiratory distressPulmonary findings on examinationLymphadenopathy or lymphadenitisS/Sx of meningitis including seizuresPersistent fever (FUO)Weight loss or failure to thriveUnlike adults, up to 50% of children with
TB disease have no symptoms

11/13/2014
16
DIAGNOSIS OF TB IN CHILDREN
Gold Standard –Positive TB Culture
OR, Clinical Diagnosis:Abnormal CXR, laboratory,
or physical examination consistent with TB AND1 or more of the following: Positive tuberculin skin test or
IGRA Contagious adult source case
identified Clinical course consistent with
TB disease, or Improvement on TB therapy
DIAGNOSTIC TRIADPEDI TB DISEASE
1. Positive TST
2. Abnormal CXR
3. Infectious source case

11/13/2014
17
GASTRIC ASPIRATES
Inpatient procedure
Overnight fasting
Lavage with normal saline
Collected in morning x 3 days
Inpatient costs substantial
AFB smear yield: <5%
Sensitivity of culture 20-50%
Future: possible use of NAAT’s in children
INDUCED SPUTUM
Outpatient procedure 2-3h fasting period Pretreatment:
Nebulized bronchodilator and hypertonic saline
Chest physiotherapy (CPT) Nasopharynx suctioned One specimen sufficient Minimal costs Yield equivalent to GA’s
Lancet. 2005;365:130

11/13/2014
18
TB CULTURES FROM CHILDREN
Bronchoalveolar lavage (BAL) Single specimen with similar yield to 3 GA’s Sensitivity 40% (20-50% range)
Lymph nodes Biopsy or FNA for path and culture Sensitivity 30-70% on culture
CSF in TB meningitis High volume (> 6 ml) improves yield Sensitivity 20% average (12-50% range)
Nucleic acid amplification tests (NAAT) in children Data limited especially from U.S. Sensitivity estimated at 60-85%
Bottom line Negative test does not rule out
disease
TUBERCULIN SKIN TEST AND
INTERFERON GAMA RELEASE ASSAYS (IGRA)
Sensitivity 90% 50% in disseminated TB
Specificity 85% Lower in BCG
vaccinated
Cross reacts with BCG vaccine Many NTM
Sensitivity 75-90% Children 90% Lower in developing
countries and children <5 years of age (50-90%)
Specificity 90-99%
Cross reactions None with BCG Only 3 NTM
M. kansasii, M. marinum, M. szulgai
Tuberculin Skin Test IGRA (QFT or TSPOT)
Both TST and IGRA tests may be helpful in difficult cases

11/13/2014
19
Machingaidze et al. PIDJ 2011; 30: epub
Quantiferon and TST in Children
IGRA SENSITIVITY IN CHILDREN < 5 YRSOF AGE INSUFFICIENT TO REPLACE TST
Test Sensitivity <5 years (CI)
Sensitivity >5 years (CI)
Specificity
TST 90% (79-100) 98% (93-100) NA, ref standard
QFT-G-IT 73% (58-89) 93% (84-100) 93% (88-99)
T-SPOT.TB 63% (46-80) 83% (75-90) 92% (87-99)
Chiappini E. PIDJ. 2014:33:1291-1293.338 children total, 210 not infected, 58 LTBI, 42 probable TB disease by clinical criteria, 28 culture confirmed disease

11/13/2014
20
TB Risk Questionnaire
positive?
Age < 5 years?
BCG Vaccinated?
Screening Complete
TST Preferred
IGRA Preferred
TST or IGRA Acceptable
No
No
Yes
No
Yes
Yes
Algorithm for TB Testing in Children
Consider•Cost•Confidence in test •Ability to return
WHAT TO DO WITH DISCORDANT IGRA AND TST RESULTS?
For healthy patients (5 yrs or older) without high risk for disease Choose the more specific test (IGRA)
If the patient is sick, under 5 years of age or at high risk of disease Consider either test positive for highest sensitivity
Indeterminate results means the control failed Repeat the test

11/13/2014
21
EXPECTED CLINICAL COURSEFOR TB DISEASE IN CHILDREN
Pulmonary CXR takes months to improve
Hilar lymphadenopathy May take a year or more to regress on x-ray
Cervical lymphadenitis Gets worse before improvement over months-years
Meningitis Inflammation and symptoms sometime increase
initially with treatment
MONITORING CHILDRENON TB TREATMENT
Risk of drug toxicity very low Monitor clinical signs
regular clinical visits (4-6 wks) patient education
Routine blood work not necessary unless symptoms risk factors for toxicity
Monitor and reinforce adherenceWhen to follow up CXR’s for pulmonary TB
Beginning and end of therapy Anytime if clinical change
Completion of therapy certificate

11/13/2014
22
TB MEDICATIONS IN KIDS
Hepatotoxicity rare INH liquid vs tabletsMedication refusal in children Crush tablets, medication sandwich
Vitamin B6 Not needed for all kids Important for
Breastfed infants Teens and/or picky eaters Patients with symptoms of peripheral neuropathy
Going back to school Children <12 yrs of age are not contagious
CENTRAL NERVOUS SYSTEMTB DRUG PENETRATION
Isoniazid Rifampin PZA Ethambutol Ethionamide Aminoglycosides Fluoroquinolones
Good Inflamed meninges only Good Inflamed meninges only Good Inflamed meninges only Good except Cipro poor
Drug CNS Penetration

11/13/2014
23
ETHAMBUTOL IN CHILDREN
Risk of optic neuritis: Visual acuity Color perception Dose related Usually reversible Risk around 1-3% in adults Risk in children about the same
EMB safe in children with monitoring Monitor vision on treatment Infants – visual evoked potentials (VEP)
Table 2. Studies that have specifically sought optical toxicity in children treated with Ethambutol
Reference Patients (n) Age range Method of evaluation Length of follow up Number with(months) toxicity
2425
Fox*262728
4736
4530276
3-13 years4 months to 16 years1-15 years4-5 years5-15 years9-16 years
Visual evoked responsesAcuity/field/colour
Acuity/field/colourAcuity/field/colourAcuity/field/colourComputerized visual fieldexamination
15-1824-48
9-18612-369
00
0000
*Fox W, unpublished data quoted in Tubercle 1986; 67:27.
SM Graham. Arch Dis child 1998; 79:274-278.
Ethambutol in Children

11/13/2014
24
*B Hampel. Pediatr Inf Dis J, 1997;16:127-9.
FLUOROQUINOLONES IN CHILDREN
Initial clinical trials in children not done Some children have been treated without
problems: CF, chronic UTI, shigellosis and TB
Most consider safe in children: Some case series and RCT with good results Germany study: 2030 patients treated, 31 (1.5%)
with self resolving arthralgia*
Not indicated for routine infections in children Consider risks and benefits Monitor clinically for joint and tendon
problems
Comparison of Side Effects with Ciprofloxacin vs Ceftazidime/Tobramycin in Children
No. of Patients
Event CiprofloxacinCeftazidime/TobramycinN = 62 (%)N = 67 (%)
P
Any 52 (78) 43 (69) 0.288Abnormal liver function tests 17 (25) 13 (21) 0.554Injection 16 (24) 5 (8) 0.015Injection site pain 13 (19) 7 (11) 0.203Rash 10 (15) 5 (8) 0.225Phlebitis 7 (10) 1 (2) 0.063Vomiting 11(16) 4 (6) 0.078Central nervous system, any 1 (1) 6 (10) 0.055Respiratory, any 7 (10) 3 (5) 0.328Musculoskeletal, any 15 (22) 13 (21) 0.845
Joint Disorder 8 (12) 10 (16) 0.493Arthralgia 7 (10) 7 (11) 0.878Arthritis 1 (1) 0 (0) 1.0Leg cramps 0 (0) 1 (2) 0.481Myalgia 1 (1) 0 (0) 1.000
DA Church. Pediatr Infec Dis J 1997 Jan; 16 (1): 97-105

11/13/2014
25
PEDIATRIC TB CASES
LYMPHADENOPATHY

11/13/2014
26
CLINICAL CASE
CERVICAL LYMPHADENOPATHY
8 yr old with cervical lymphadenopathy
History: LAN for 3 months PMHx: HealthyBCG vaccine at birth
TB skin test 10 mmPhysical Exam:
3 cm anterior cervical LAN 1.5 cm supraclavicular
lymphadenopathy CXR:
Hilar LAN, no infiltratesIs this TB disease?What else could it be?
HILAR & CERVICALLYMPHADENOPATHY
Differential Dx Tuberculosis Non TB mycobacteria (NTM) Lymphoma/Leukemia HIV Other causes
Diagnostic tests Biopsy (FNA or surgical for
culture and path) Interferon blood test for TB
infection

11/13/2014
27
RESULTS
Fine needle aspirate of node: Pathology: lymphoma, no TB by culture or microscopy
Interferon Blood test for TB Positive Diagnostic for latent TB infection or disease
Diagnoses: LTBI
AND Hodgkin’s Lymphoma
Treatment: Chemotherapy for lymphoma AND INH daily for 9 months for LTBI
consider prolonged treatment during immunosuppresion
Skin Test in Foreign Born

11/13/2014
28
SKIN TEST IN FOREIGN BORN
6 year old with positive TST for school entry Born in Asia BCG documented on vaccination records at birth
and BCG scar present TST measures 12mm
CXR NORMAL
How do you interpret the 12 mm skin test?
Is this BCG effect or LTBI?
Are there any other tests that may help?

11/13/2014
29
TB IN NEWBORN NURSERY

11/13/2014
30
NEW MOTHER WITH POSITIVE TST
Newborn infant in hospital nursery Mother with 15 mm TST CXR: calcified granuloma no active disease Not on treatment
What is mother’s diagnosis? Do mother or baby need isolation? May baby breast feed and room with mother?
Maternal TB disease or LTBI during pregnancy
Is mother contagious?
Exposure to contagious household TB contact:• Window prophylaxis
for baby• Multivitamin for baby• Okay to breastfeed
If no exposure to contagious household TB contacts:• No treatment for
baby• Okay to breastfeed
No Yes

11/13/2014
31
PREVENTION OF TB DISEASEIN CHILDREN
Contact Investigation
INH Window Prophylaxis
Treatment of LTBI
RESOURCES
HNTC Pedi TB Toolbox Guidelines and clinical tools Reference materials Patient education materials
TB Testing in Children Brochure
Pediatric Radiology for Clinicians

11/13/2014
32
TREATMENT OF TUBERCULOSIS IN CHILDRENStages of TB Skin Test or
IGRACXR SXs Treatment
Exposure Child < 4 years of age Household contact with adult with active pulmonary disease
TST Negative Normal None Meds: INH window prophylaxisDuration: 8-10 weeksRepeat skin test: 8-10 wks after expif positive > 5mm, see LTBI
Latent TB infection (LTBI) Positive Normal None Meds: INHDuration: INH 9 mo or RIF 4-6 mo
DiseasePulmonary and extrapulmonary(except disseminated disease and meningitis, see below)
90% positive Abnormal +/- Meds: INH, RIF, PZA(consider EMB or an aminoglycoside) Duration: 6 mo total, Stop PZA after 2 mo, continue INH & RIF for susceptible disease
DiseaseDisseminated including miliary, bone/joint and multi-site disease
TST may be negative early in disseminated TB, most positive by end of treatment
+/- Yes Meds: INH, RIF, PZA and EMB or an aminoglycosideDuration: 9-12 mo total Stop PZA and EMB or aminoglycoside after 2 mo for susceptible disease
DiseaseMeningitis
Often negative early in meningitis and miliary disease90% positive by end of tx
+/- Yes Meds: INH, RIF, PZA and Ethionamide, or an aminoglycosideor EMB daily for 2 mo, then INH and RIF for 7-10 moDuration: 9-12 mo total for drug susceptible diseaseSteroids recommended for first 1-2 mo for meningitis