Embed Size (px)
Citation preview

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 1/38
TUBERCULOSIS
ANDCHRONIC RENAL
FAILURE
unior Resident Pulmonary Medicine

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 2/38
Magnitude Of The Problem:
Patientswithrenaldiseaseareatincreasedriskoftuberculosis(TB).Thisis
trueforallpatientswithchronickidneydisease(CKD),30timeshigher
prevalenceofTBinpatientswithCRF.YuanFH,GuanLX,ZhaoSJRenalFal2005;27:149-53
Ithasbeenestimatedpatientsundergoingdialysishave10to12foldhigher
riskofdevelopingTBcomparedtogeneralpopulationRutskyEA,RostandSGArchInternMed1980;140;57-61
TheincidenceofTBinIndianpatientsreceivingMaintenanceHemodialysis
hasbeenreportedtobe3.7to13.3percent.NarulaASetalIndianJNephrol1991;1;67
IncidenceofTBinrenaltransplantrecepientshasrangedfrom1to4%in
NorthernEurope,0.5-1%inNorthAmericaandnearly5to10%inIndia.McWhinneyN,KhanO,WilliamsGBrSurg1981;68:408-11
7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 3/38
Why increased incidence of TB in CKD patients
:Pathogenesis
UREMIA :
Acquiredimmunodeficiencystateleadingtoexcessivemorbidityand
mortalityrelatedtoinfections.
Granulocytefunctionslikechemotaxis,adherenceandphagocytosisare
defective.
DecreasedInterleukin2(IL2)productionbyactivatedTHelperCells
Adefectinthecostimulatoryfunctionofantigen-presentingcells,anda
persistentinflammatorystateofmonocytes,whichiscausedbythe
uremiaperse,aswellasbythedialysistreatment
ChatenoudL,Descamps-LatschaB:Immunologicaldisturbancesinuremia.In:MassrySG,
GlassockRJ(eds).TextbookofNephrology,4thed.Philadelphia:LippincottWilliams&
Wilkins,2001:1433 – 1438
Thehostresponseagainstintracellularpathogens,includingMycobacterium
tuberculosis,isdeterminedbythetype1helperT-cellresponsewiththeinvolvementof
interleukin(IL)-12,resultinginincreasedproductionofinterferon(IFN)-c

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 4/38
HEMODIALYSIS :
Leucocytechemotaxishasbeenshowntomarkedlydiminished
Conventionalcellulosemembranecausesalternatecomplementpathway
leadingtochangesingranulocytecelladhesionmoleculesCD11b,CD18
andLselectin,thiscorrelatewithleucopenia
Impairmentofphagocytosisisoftenencounteredwithcuprophane
membrane
WoeltjeKF,MathewA,RothsteinM,SeilerS,FraserVJ:Tuberculosis
infectionandanergyinhemodialysispatients.AmJKidneyDis31:848 – 852,1998
7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 5/38
IMMUNOSUPPRESSIVE THERAPY :
Immunosuppressionwithtacrolimusormycophenylatemofetil
is,however,associatedwiththedevelopmentofTBearlierinthepost-transplantperiodandinyoungerpatients.
PredisposingtoinfectionasCellmediatedandhumoral
immunitygotaffected
Other factors which might contribute to the decreased
immunity are
Malnutrition,
Vitamin D deficiency , andHyperparathyroidism

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 6/38
Clinical Features
Aninsidiousonsetofsymptoms,withfever,anorexia,andlossofweight
beingthemaincomplaints,mimickinguremicsymptoms.
Pienetal.foundfeveroccurringinameanof72%ofthecases(range29 –
100%),malaiseinameanof69%(range29 – 100%),andweightlossinameanof54%(range10 – 100%).
However,coughandhemoptysis,classicsymptomsofTBinthegeneral
population,arelessfrequentlyreportedindialysispatients(mean22%of
cases;range5 – 71%)

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 7/38
Clinical Presentation of Tuberculosis
during Maintenance Hemodialysis
•Malesnearlyaffectedtwiceascommonlyascomparedtofemales
•MajoritydevelopTBpriortoinitiationorwithinshortperiodfromthe
beiginingofMHD,atimewheneffectofuraemiaonimmunestatusisstill
pronounced
•ConstitutionalsymptomsattributabletoTBhavebeenreportedin30to92
percentpatientsinvariousseries
•Headache,chillsandshortnessofbreathwerelesscommon(lessthan
30%)
• Almost15%presentedwithPyrexiaofUnknownOrigin
•Malhotraetal(1981)pleuraleffusioninalmost50%ofcasesinonestudy.

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 8/38
•LungisthemostcommonsiteofinvolvementinpatientsonMHD,Pulmonary
TBrangedfrom40to92%
•LymphNodeinvolvementhasbeenfoundtobemostcommonextrapulmonary
siteofTBonMHD15to30%
•
Otherextrapulmonaryinvolvementinclude Abdomen
Meninges
BoneandJoints
•Disseminated/MiliaryTBrangedbetween10to15%
•TuberculosisPeritonitishasbeendescribedinpatientsonContinuous
AmbulatoryPeritonealDialysis

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 9/38
Clinical Presentation of Tuberculosis
following Renal Transplantation
Tuberculosisin
RenalTransplant
Patients
TBinPretransplant
phase..Havingpost
RTphasetoo
TBfirsttime
followingRT

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 10/38
PatientwhodevelopTBfollowingRTareusuallyyounger.Malearemore
oftenaffected.
PasthistoryofTBhasbeenreportedin5.6to8.9%patientsinstudies
reportedinIndia.
ConstitutionalSymptomsaremoreoftenencounteredinRTpatientsthan
inpatientsonMHD
LungismostcommonsiteRTpatientswhodevelopfollowedbyabdomen,pericardium,thalamus,boneandjoints
MiliaryTBhasalsobeenreportedin7to36%ofRTpatients
PUOpresentationisassociatedmorecommonlywithRTpatients
AbdominalTBmorecommonlyduringdialysis
NeurologicalTBmorecommonaftertransplantation
7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 11/38
Diagnosis
ThediagnosisofTBisbasedonthefindingofan acidfast bacilli-positive smear,
positive culture of M. tuberculosis, and typical histopathologic findings.Eff ortsshouldbemadetoobtainappropriatematerialsforculture,whichshould
includesensitivitytesting
ThediagnosisofTBishamperedbythecommonoccurrenceofanegative
purifiedproteinderivative(PPD)(Mantoux)skintest,whichwasfoundin40 – 100%ofthecases.
Routinebloodinvestigationsincludingrenalfunctiontestandsugarmonitoring
tokeepcheckonrenalfunctionanddiagnoseandkeepunderlyingpathology
underscanner.
7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 12/38
Paradoxically,anddespitethehighrateofanergytointracutaneously
administeredantigensinuremicpatients,highratesofpositiveMantouxtests(6.1 – 19%)havebeenfoundinroutinescreeningofdialysispatients
withoutahistoryoforactiveTB.
Thus,duetothefrequentextrapulmonarypresentationandnonspecific
symptomatology,a high index of suspicion is required, coupled with a
need for invasive procedures, including liver, bone, lymph node, andperitoneal biopsies
7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 13/38
Recommendations
1.Allpatientswithchronickidneydisease(CKD)consideredatriskfor
tuberculosis(TB)shouldhaveahistoryofpriorTBorTBcontactsought,anyhistoryofpriorTBtreatmentchecked(includingdrugstakenand
treatmentduration),anappropriateclinicalexamination,achestx-ray
2.AnypatientwithCKDwithanabnormalchestx-rayconsistentwith
pastTB,orprevioushistoryofextrapulmonaryTBbutwhohaspreviouslyreceivedadequatetreatmentshouldbemonitored
regularlyandconsideredforreferraltoandassessmentbya
specialistwithaninterestinTB,eitherathoracicorinfectious
diseasesphysician.
3.Thedecisiononchemoprophylaxisregimenshouldbemadebythe
thoracicorinfectiousdiseasephysicianafterdiscussionwithboththe
patientandrenalteam
7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 14/38
DIAGNOSIS OF LATENT TB INFECTION
ThediagnosisofLTBIisbasedoninformationgatheredfromthemedical
history,TSTorIGRAresult,chestradiograph,physicalexamination,andincertaincircumstances,sputumexaminations.
TimingofscreeningForpatientswithCKD,thereisnoevidenceonwhenorhowtoscreenfor
LTBI.ScreeningallpatientswithadvancedCKDorevenonlythoseonhaemodialysisorperitonealdialysiswouldbetime-consuming,expensiveand
unlikelytobecost-effective
Thecurrentpracticeinmostrenalunitsistogiveprophylaxistoallat-risktransplantpatientswithoutassessment.
Asignificantproportionofpatientswillbereceivingprophylaxiswithout
evidenceofLTBI.ChemoprophylaxiscouldbeofferedtothosewithLTBIbefore
transplantation,precludingtheneedforpost-transplantprophylaxis.
7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 15/38
Method of screening
AllpatientswithCKD,onhaemodialysisorCAPDandpriortorenal
transplantationshouldhaveachestx-rayandabnormalitiesinvestigated.
Mostpatientswillhavenormalx-raysandtheresponsetotuberculinor
TB-specificantigenswillbeneededforscreeningforLTBIinappropriate
patients.
TheTSTisunreliableinpatientswithadvancedCKDandinthoseon
immunosuppressiveagents.Apositivetestmaybeusefulbutanegative
resultcannotbeassumedtobeatruenegative.
7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 16/38
CHEMOPROPHYLAXIS
Therearethreepotentialchemoprophylaxisregimens:
Isoniazid for 6 months (6H),
Rifampicin plus isoniazid for 3 months (3RH)
Rifampicin alone for 4-6 months (4-6R).
Rifampicinandpyrazinamidefor2months(2RZ)wasaregimenusedin
theUSAbutitwasassociatedwithaveryhighrateofhepatitis,witha
numberoffatalitiesreported

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 17/38
Thechoiceofregimen
6H [ Isoniazid for 6 months] ,whichhasalowerhepatitisrate.
3RHwhichmayhaveadvantagesintermsofshorterdurationandthus
possiblybetteradherenceandalsolessriskofdrugresistancedevelopingif
activediseaseispresent.
4-6R whichalsohasthedisadvantageofasingleagentbutwasbetter
toleratedthan9monthsofisoniazidaloneandcanbeusedfollowingcontact
withisoniazid-resistantdisease.
Nochemoprophylaxisregimeniswhollyeffective;protectiveefficaciesof60-65%havebeenreportedfor6Handof50%for3RH.
Thereisstrongevidencethatregimenslongerthan6Hhaveonlyvery
minimaladditionaladvantageatthecostofanincreaseintheriskof
hepatitis

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 18/38
ANTITUBERCULOSIS DRUGS IN CHRONIC KIDNEY
DISEASE
Thepharmacologicalpropertiesofantituberculosisdrugsdeterminehowtheirlevelsarelikelytobeinfluencedbyrenalfailure,clearanceduring
dialysisandalsotheirinteractionwithimmunosuppressivedrugsusedin
patientsundergoingrenaltransplantation.
Theexacttimingofadministrationinrelationtodialysisandconcomitant
useofimmunosuppressivedrugsfollowingrenaltransplantation.
Treatmentdurationshould,however,followguidelines,6monthsformost
casesoffullysensitivedisease,withtheexceptionofTBinvolvingtheCNSwhentreatmentshouldbefor1year.

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 19/38
Isoniazid (H)
Isoniazidismetabolisedbytheliverintolessactivecompoundswhicharethen
excretedbythekidneys.Themostrecentevidenceavailablesuggeststhatisoniazidisdialysableinonlyverysmallamountsandmostclearanceoccurs
fromhepaticmetabolism.
Pharmacokineticstudiesofisoniazidinrenalfailure,however,suggestthat
eventhoughthehalf-lifeofisoniazidisincreasedbyabout45%inslow
acetylators,thisdoesnotleadtosignificantadverseeventsnecessitating
dosagereduction,andtherapeuticdrugmonitoringisnotthoughttobe
necessary.Furthermore,thereisevidencetosuggestthatadministering
isoniazidinreduceddosesmayleadtoreducedpotencyandriskthe
developmentofresistance.
Stage1-3ofCKDIsoniazid300mg
Stage4-5ofCKDIsoniazid300mg
RenalTransplantRecipients15mg/kgmax900mg3X/week

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 20/38
Side Effects of ISONIAZID
1.Neurotoxicity:grandmalseizures(withnopriorhistory),depressive
psychosis,confusion,nightmares,hallucinations,peripheralneuropathy,
twitchinganddizziness.Encephalopathywasalsoreportedin3of48
dialysispatientswithTB
2.Afewofthosereceivingdialysisalsoexperiencedsignificant
gastrointestinaladverseeffects(jaundice,nauseaandvomiting).
3.Ototoxicityhasbeendescribedovera10-yearperiodinsevenpatientswithCKDreceivingisoniazidtogetherwithotherdrugsbutnot
aminoglycosides.
4.RenalFailure
SiskindMS,ThienemannD,KirlinL.Isoniazid-inducedneurotoxicityinchronicdialysis
patients:reportofthreecasesandareviewoftheliterature.Nephron1993;64:303e6 .
WangHY,ChienCC,ChenYM,etal.Encephalopathycausedbyisoniazidinapatient
withendstagerenaldiseasewithextrapulmonarytuberculosis.RenFail2003;25:135e8.
7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 21/38
Rifampicin (R)
Rifampicinisalsometabolisedbytheliver.Itsinactivemetabolite,
formylrifampicin,isexcretedintheurineanditsmajormetabolite,desacetyl-
rifampicin,isexcretedinbile.
Urinaryexcretionaccountsforverylittleofitseliminationfromthebody,with
onlyabout10%ofagivendosebeingfoundunchangedintheurine.Rifampicin
doesnotappearinsignificantamountsindialysate.
Reportedsideeffectsforrifampicindonotappeartooccurwithsignificantly
increasedfrequencyinpatientswithCKDorondialysis,althoughrifampicinhas
beencitedasararecauseofacuterenalfailure.Assuch,thereiswidespread
agreementthatthedoseofrifampicinneednotbealteredinrenalimpairment
andthatdruglevelsneednotbemonitored
RekhaVV,SanthaT,JawaharMS.Rifampicin-inducedrenaltoxicityduring
retreatmentofpatientswithpulmonarytuberculosis.JAssocPhysiciansIndia
2005;53:811-13

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 22/38
Pyrazinamide (Z)
Pyrazinamideismetabolisedintheliver.Only3-4%isrenallyexcretedin
unaltered.Althoughthepharmacokineticsofthedrugareunalteredinitiallyin
patientswithrenalfailure,onestudyofitseliminationfoundmuchhigherlevelsdetectableforupto48hafteradministration.Owingtoitseffectonuricacid
retention,thismayleadtohyperuricaemiaandgout.
Pyrazinamideanditsmetabolitesaresignificantlyeliminatedfromthebodyby
haemodialysis,45%appearinginthedialysate.
Nodataareavailableforperitonealdialysis.Duetopossibledelayed
eliminationofthedruganditsmetabolite,thedosageintervalshouldbealtered
instages4and5CKDandinpatientsonhaemodialysis.Therearenocleardataforperitonealdialysis
20 -35 mg/kg per dose three timer per week
EllardGA.Chemotherapyoftuberculosisforpatientswithrenalimpairment.
Nephron1993;64:169e81.(2++)
7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 23/38
Ethambutol (E)
Around80%ofethambutolisexcretedunchangedbythekidneys.
Inpatientswithrenalfailure,excretionofethambutolwassignificantlyreduced
followingtheusualdoseof15mg/kg.
Itisrenallyexcretedandoculartoxicityislargelydose-dependent.Ethambutol
hasbeendetectedindialysate.
Ithasimprovedefficacywhenadministeredinhighdoseslessoftenthaninadailylowerdose.Serummonitoringshouldbedoneandtroughlevelsshouldbe
lessthan1.0mg/mlat24hpost-dosewithoutdialysis
Recommendation : 15-25 mg/kg per dose three times per week
VarugheseA,BraterDC,BenetLZ,etal.Ethambutolkineticsinpatientswith
impairedrenalfunction.AmRevRespirDis1986;134:34e8.(2+).
CitronK.Ethambutol:areviewwithspecialreferencetooculartoxicity.
Tubercle1969;50(Suppl):32e6.(2++).

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 24/38
Aminoglycosides
Around80%ofstreptomycin,kanamycin,amikacinandcapreomycinare
excretedunchangedintheurinewithouthavingundergonesignificant
metabolism.
Streptomycincausessignificantvestibulartoxicitybutlessnephrotoxicity
comparedwiththeotheraminoglycosides.
Thereisanincreaseineliminationtimewithincreasingageanddecliningrenalfunction.Approximately40%ofstreptomycin,amikacin,capreomycinand
kanamycinareremovedbyhaemodialysiswhenthesedrugsaregivenjust
beforehaemodialysis.
TheAmericanThoracicSociety(ATS)recommends12-15
mg/kg/dose2or3times/weekforallofthesedrugs.
Druglevelsshouldbemonitored.

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 25/38
Aswithethambutolandpyrazinamide,thedosingintervalshouldbe
increasedratherthanthedosedecreasedasthedrugsexhibitconcentration
dependentbactericidalaction,andlowerdosesmayreducedrugefficacy.Itispreferabletogivestreptomycintwiceorthriceweeklywithoutdecreasingthe
usualdose.
15mg/kg(max1gdaily).Doseisreducedin<50kgand>40yearstomax500to750mgdailyor12-15mg/kg2-3times/week.
Peakplasmaconcentrationsofstreptomycinshouldbebetween15and40
mg/mlandtroughconcentrations<3-5mg/mlor<1mg/mlinCKDorthose
>50years.

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 26/38
HOW TO CALCULATE CREATININE
CLEARANCE
Cockcroft and Gault equation:
CrCl = [(140 - age) x TBW] / (Scr x 72) (x 0.85 for females)
Where
CrClisCreatinineclearance
TBWisTotalBodyWeight
ScrisSerumCreatininine

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 27/38
Stage1CKD:Normalcreatinineclearanceandfunctionbuturinary
tractabnormality,forexample,polycystickidney,structuralabnormality.
Stage2CKD:Creatinineclearance60to90ml/min
Stage3CKD:Creatinineclearance30to60ml/min
Stage4CKD:Creatinineclearance15to30ml/min
Stage5CKD:Creatinineclearance<15ml/minwithorwithoutdialysis.

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 28/38
SECOND-LINE DRUGS USED IN THE MANAGEMENT OF
RESISTANT DISEASE
FLUOROQUINOLONES
•Bothofloxacinandciprofloxacinarealsodependentonrenal
clearanceanddosesshouldbereducedaccordingly.Other
fluoroquinolonesundergosomedegreeofrenalclearancewhichvaries
fromdrugtodrug.
•Levofloxacinundergoesgreaterrenalclearancethanmoxifloxacin.
•FluoroquinolonesdecreasethemetabolismofciclosporinAand
displaceitfromtheboundform,thusincreasingitstoxicity
FishDN,ChowAT.Theclinicalpharmacokineticsof
levofloxacin.ClinPharmacokinet1997;32:101-19.(l+).

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 29/38
CYCLOSERINE
Upto70%ofcycloserineisexcretedbythekidneyand56%removedby
haemodialysis.
Giventhatdose-relatedneurologicalandpsychiatricsideeffectsofcycloserine
havebeenreportedinupto50%ofpatients,doseadjustmentinthesettingof
renalfailureisrecommended.
TheATSrecommendsincreasingthedoseintervalandsuggests250mgonce
daily
orpreferably500mg3times/week.
Again,itshouldbegivenafterhaemodialysistoavoidunder-dosingand
monitoredforneurotoxicity.
MaloneRS,FishDN,SpiegelDM,etal.Theeffectofhemodialysison
cycloserine,ethionamide,para-aminosalicylate,andclofazimine.
Chest1999;116:984-90.(2+).

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 30/38
Para-amino salicylic acid (PAS)
AmodestamountofPAS(6.3%)isclearedbyhaemodialysisbutitsmetabolite,
acetyl-PAS,issubstantiallyremoved.
8-12g/dayintwoorthreedivideddosestwiceshouldbeadequate..
Ethionamide/prothionamide
Ethionamideandprothionamidearenotclearedbythekidneysnorarethey
removedbyhaemodialysis,sonoadjustmenttodosingisneeded.
15to20mg/kg/day(maximum1g;usually500to750mg)insingledailydose
ortwodivideddose
7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 31/38
Clofazimine
Clofazimineisavailableonanamedpatientbasis.ItcanaccumulateinCKD
andcausesskinandhairdiscolouration,photosensitivityandocular
problems.Pharmaceuticaladviceshouldbesought.
Thenormaldoseis100-300mgdailyandthisshouldbereducedtothree
timesweeklyinpatientswithCKDandthoseondialysis.
Linezolid
Ahigherincidenceofblooddisordersandopticneuropathyhasbeen
reportediflinezolidisusedforlongerthan28days,makingitsuseinthe
managementofTBdifficult.Linezolidisareversiblenon-selectivemonoamineoxidaseinhibitorand
patientsshouldavoideatingtyramine-richfoodssuchascheeseand
productscontainingyeast.Thenormaldoseis600mgevery12h.

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 32/38
Patients with CKD not on dialysis
Forpatientswithstages4and5CKD,dosingintervalsshouldbeincreasedto
threetimesweeklyforethambutol,pyrazinamideandtheaminoglycosides.
Isoniazid(H),rifampicin(R)andpyrazinamide(Z)canbeusedinnormal
dosesinrenalimpairment.Controlledclinicaltrialshaveshownthatthree
timesweeklytreatmentwithpyrazinamideistherapeuticallymoreeffective
thandailyadministration.
Pyridoxinesupplementationshouldbegivenwithisoniazidtopreventthe
developmentofperipheralneuropathy.
Ethambutolandtheaminoglycosideshavethedisadvantageofrenal
clearance,theneedforincreaseddoseintervalsorreduceddosageand
drugmonitoring.

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 33/38
HAEMODIALYSIS
Treatmentcanbegivenimmediatelyafterhaemodialysistoavoidpremature
drugremoval.Withthisstrategythereisapossibleriskofraiseddruglevelsof
ethambutolandpyrazinamidebetweendialysissessions.
1.BothrifampicinandisoniazidmaybegivenintheirusualdailyDoses
2.Haemodialysisremovesasignificantamountofpyrazinamideandthe
primarymetaboliteofpyrazinamide,pyrazinoicacid,accumulatesinpatientswithrenalfailure.Advicevariesoverwhetherreductionorspacingofthedose
ofpryazinamideisbestforpatientsonhaemodialysis.Variabledosesof25-30
mg/kgthreetimesweeklyor40mg/kgthreetimesweeklyhavebeen
Recommended.
3.Pyrazinamideshouldbeadministeredimmediatelyafterhaemodialysisor4-6
hbeforehand.
Ethambutolcanbegivenatadoseof15-25mg/kgthreetimesweeklyfor
patientsonregularhaemodialysis.

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 34/38
PERITONEAL DIALYSIS
Mechanismsfordrugremovaldifferbetweenhaemodialysisandperitoneal
dialysissoitcannotbeassumedthatrecommendationsforhaemodialysisalso
applytoperitonealdialysis.
Onestudyhasshownthatnodoseadjustmentisneededforisoniazid,
rifampicinorpyrazinmideforthetreatmentofsystemicorpulmonaryTBin
patientsonCAPD.
Rifampicinhasahighmolecularweight,lipidsolubilityandproteinbindingcapacityandthesepropertiesmakeitlessdialysablethroughtheperitoneal
membranesothatonlyminimalamountsarerecoveredinthedialysate,
implyingthatoraltherapywithrifampicinmaynotbeadequatefortreatmentof
peritonealTB.Ahnandcolleaguessuggestintraperitonealadministrationof
rifampicinshouldbeconsideredwhentreatingperitonealTB
AhnC,OhK-H,KimK,etal.Effectofperitonealdialysisonplasmaand
peritonealfluidconcentrationsofisoniazid,pyrazinamideandrifampicin.Perit
DialInt2003;23:362e7 .

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 35/38
RENAL TRANSPLANTATION
Rifampicininparticularcaninteractwithimmunosuppressiveregimens,
increasingthechanceofgraftrejection,anddosesofmycophenolatemofetil,
tacrolimusandciclosporinmayneedadjustment.Corticosteroiddosesshould
bedoubledinpatientsreceiving
rifampicin.
Rifampicinisthedrugmostlikelytointerferewithimmunosuppressivetreatment
byinductionofanumberofliverenzymesincludinguridinediphosphate-
glucuronosyltransferases,monoamineoxidases,glutathioneS-transferasesandcytochromeP450.
Thedailycorticosteroiddoseshouldbeincreasedtotwicethebaselinedosage
inpatientstakingrifampicin.
Oncerifampicinhasbeenstopped,liverenzymeinductionusuallytakes
2weekstoreturntonormal.
Azathioprinesometimescauseshepatotoxicity,whichhastobe
differentiatedfromthehepatotoxicityduetoantituberculosisdrugs.

7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 36/38
SUMMARY1. Closecooperationbetweenrenalphysiciansandspecialistsinthe
managementofTBisstronglyrecommended.
2. ActiveTBshouldbeexcludedinpatientswithCKDbyappropriate
investigationsinpatientswhohaveanabnormalchestx-rayorahistoryof
priorpulmonaryorextrapulmonaryTBthathasbeeneitherinadequatelyor
notpreviouslytreated.Chemoprophylaxisshouldbegiven
3. Forpatientswithstages4and5CKD,dosingintervalsshouldbeincreased
tothreetimesweeklyforethambutol,pyrazinamideandthe
aminoglycosides.
4. Treatmentcanbegivenimmediatelyafterhaemodialysistoavoidpremature
drugremoval.
5. Rifampicininparticularcaninteractwithimmunosuppressiveregimens,
increasingthechanceofgraftrejection,anddosesofmycophenolatemofetil,
tacrolimusandciclosporinmayneedadjustment.Corticosteroiddoses
shouldbedoubledinpatientsreceivingrifampicin.
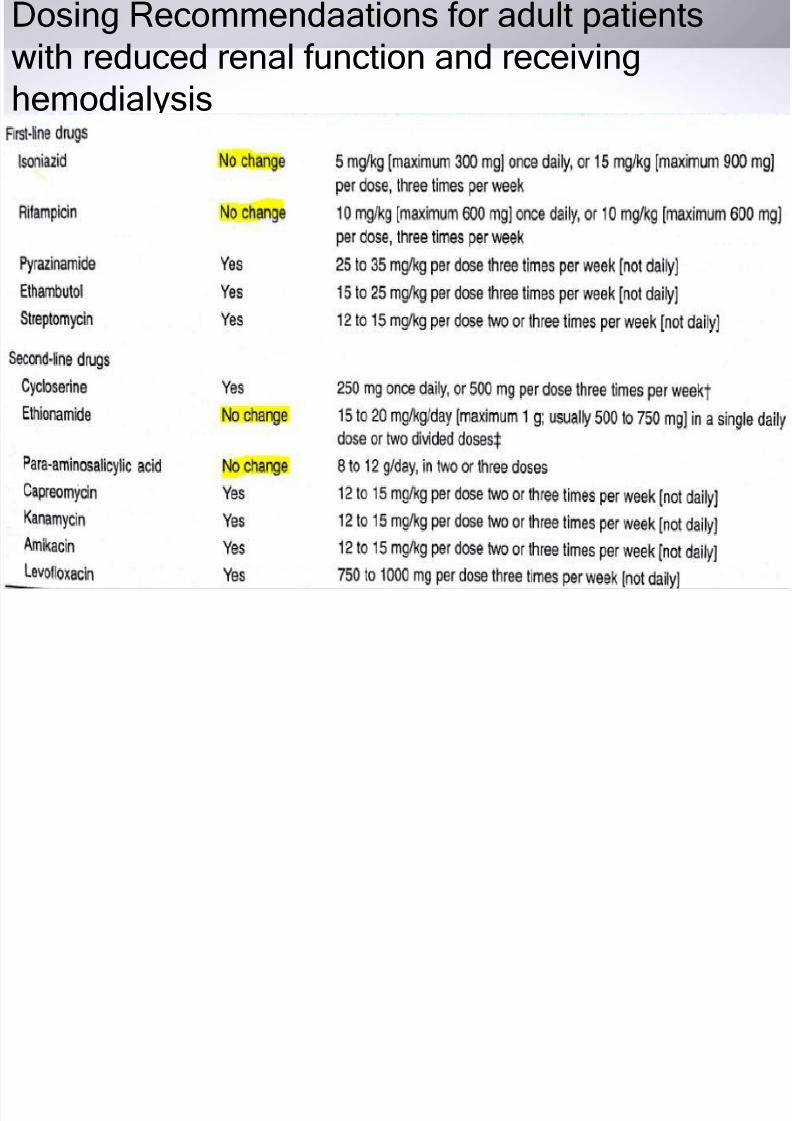
Dosing Recommendaations for adult patients
7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 37/38
DosingRecommendaationsforadultpatientswithreducedrenalfunctionandreceiving
hemodialysis
7/29/2019 Tuberculosis And Chronic Renal failure
http://slidepdf.com/reader/full/tuberculosis-and-chronic-renal-failure 38/38
THANK YOU