Embed Size (px)
Citation preview
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 1/28
TwinTwin--toto--twintwin
transfusion syndrometransfusion syndrome(TTTS)(TTTS)
::::
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 2/28
> 20% discordance in birthweight, and > > 20% discordance in birthweight, and >
55 g/dL discordance in cord haemoglobing/dL discordance in cord haemoglobin
levelslevels ± ±insufficientinsufficient
ultrasoundultrasound--based criteria, with particular based criteria, with particular
attention to amniotic fluid discordance,attention to amniotic fluid discordance,
bladder volumes, and fetal Doppler bladder volumes, and fetal Doppler studies.studies.
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 3/28
PathophysiologyPathophysiology
1. Placental architecture1. Placental architecture Almost all monochorionic twins have Almost all monochorionic twins have
intertwin vascular anastomoses.intertwin vascular anastomoses.
Arterio Arterio--arterial ( AA) anastomoses andarterial ( AA) anastomoses and
venoveno--venous (VV) anastomoses arevenous (VV) anastomoses are
superficial anastomoses, travellingsuperficial anastomoses, travelling
across the surface of the placentaacross the surface of the placentawithout interruption between the two cordwithout interruption between the two cord
insertions.insertions.
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 4/28
Arterio Arterio--venous ( AV) anastomoses arevenous ( AV) anastomoses are
deep anastomoses, where an unpaireddeep anastomoses, where an unpairedartery and vein pierce the chorionic plateartery and vein pierce the chorionic platein close adjacency to supply a sharedin close adjacency to supply a sharedplacental cotyledon.placental cotyledon. ----provideprovide
unidirectional flow of blood from theunidirectional flow of blood from thedonor to the recipient.donor to the recipient.
TTTS results from intertwin transfusionTTTS results from intertwin transfusionacross shared placental vascular across shared placental vascular
anastomosesanastomoses TTTS occurred uncommonly (15%) TTTS occurred uncommonly (15%) despite the high frequency of occurrencedespite the high frequency of occurrenceof crossof cross--placental vascular placental vascular communication.communication.
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 5/28
TTTS is more likely to develop when there is aTTTS is more likely to develop when there is apaucity of paucity of bibi--directional AAs and VVdirectional AAs and VVanastomosesanastomoses that can assist with regulation of that can assist with regulation of intertwin circulatory imbalances.intertwin circulatory imbalances.
The larger the number and type of intertwinThe larger the number and type of intertwinanastomoses, the less frequently clinical TTTSanastomoses, the less frequently clinical TTTSis observed.is observed.
the antenatal detection of the antenatal detection of AA anastomosesAA anastomosespredicts higher perinatal survival inpredicts higher perinatal survival inpregnancies complicated by TTTS.pregnancies complicated by TTTS.
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 6/28
Transfusion through the unidirectional AVTransfusion through the unidirectional AV
anastomoses createsanastomoses creates hydrostatichydrostatic
differencesdifferences between the twins.between the twins.
Atrial natriuretic peptide (ANP) andAtrial natriuretic peptide (ANP) and
vasopressinvasopressin levels in the twins diverge;levels in the twins diverge;
the donor responds with oliguria, and thethe donor responds with oliguria, and therecipient with polyuria andrecipient with polyuria and
polyhydramnios (Quintero stage 1).polyhydramnios (Quintero stage 1).
PathophysiologyPathophysiology
2. The fetal response2. The fetal response
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 7/28
The resultantThe resultant haemoconcentration inhaemoconcentration in
the recipientthe recipient creates an osmoticcreates an osmotic
gradient from the maternal compartment,gradient from the maternal compartment,worsening the polyhydramniosworsening the polyhydramnios
As donor perfusion pressure continues to As donor perfusion pressure continues to
fall urine production finally ceasesfall urine production finally ceases(Quintero stage 2), resulting in a µstuck(Quintero stage 2), resulting in a µstuck
twin¶.twin¶.
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 8/28
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 9/28
The resultantThe resultant inability to swallowinability to swallow
aggravates the donor twin's hypotension,aggravates the donor twin's hypotension,andand vasoconstrictor peptides, such asvasoconstrictor peptides, such as
the reninthe renin--angiotensin system (RAS)angiotensin system (RAS)
mediatorsmediators, increase dramatically, increase dramaticallyincreased arterial resistance in the donor'sincreased arterial resistance in the donor's
placental territoryplacental territory growth restriction.growth restriction.
Absent or reversed endAbsent or reversed end--diastolic flowdiastolic flow
(A/REDF) in the donor umbilical arter y (A/REDF) in the donor umbilical arter y
(UA)(UA) may be seen (Quintero stage 3: donor ).may be seen (Quintero stage 3: donor ).
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 10/28
These R AS mediators are also transfused toThese R AS mediators are also transfused to
the recipient via placental anastomosesthe recipient via placental anastomoses
similar cord levels of renin and aldosteronesimilar cord levels of renin and aldosterone
despite discordant renal expression of renindespite discordant renal expression of renin
between donors and recipients.between donors and recipients.
Systemic hypertension in the recipient fetus,Systemic hypertension in the recipient fetus,initiated by the increase in cardiac output, nowinitiated by the increase in cardiac output, now
worsens.worsens.
[endothelin and fetal natriuretic peptides]:[endothelin and fetal natriuretic peptides]:
higher in recipient twinshigher in recipient twins----these mediators likelythese mediators likely
work synergistically to induce pressurework synergistically to induce pressure--
overload cardiomyopathy.overload cardiomyopathy.
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 11/28
Fetal echocardiography in recipientFetal echocardiography in recipientthethe
presence of presence of cardiomegaly secondar y tocardiomegaly secondar y tobiventricular hypertrophybiventricular hypertrophy, with the, with the
majority exhibitingmajority exhibiting right ventricular right ventricular
systolic and biventricular diastolicsystolic and biventricular diastolic
dysfunctiondysfunction..
Right ventricular outflow tract obstructionRight ventricular outflow tract obstruction
may evolvemay evolve10% of recipient fetuses10% of recipient fetuses
Venous DopplersVenous Dopplers ± ± ductus venosus (DV)ductus venosus (DV)and umbilical vein (UV)and umbilical vein (UV) ± ± may nowmay now
deteriorate (Quintero stage 3: recipient).deteriorate (Quintero stage 3: recipient).
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 12/28
Continuing fetoContinuing feto± ±fetal transfusion in the face of fetal transfusion in the face of
such cardiac dysfunctionsuch cardiac dysfunction progression to fetalprogression to fetalhydrops (Quintero stage 4).hydrops (Quintero stage 4).
Whether by terminal hypoperfusion in the donor, or Whether by terminal hypoperfusion in the donor, or by cardiac failure in the recipient, single fetalby cardiac failure in the recipient, single fetal
demise may ensue (Quintero stage 5).demise may ensue (Quintero stage 5). At or around the time of this death, acute feto At or around the time of this death, acute feto± ±fetalfetal
haemorrhage from the survivor haemorrhage from the survivor into the placentalinto the placentaland fetal vascular compartment of the deadand fetal vascular compartment of the dead
twintwin can occur through the patent intertwincan occur through the patent intertwinvascular anastomoses.vascular anastomoses. profound hypotensionprofound hypotension
high risk of death or severe neurological injuryhigh risk of death or severe neurological injury(approximately 30% for each) in the co(approximately 30% for each) in the co--twin.twin.
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 13/28
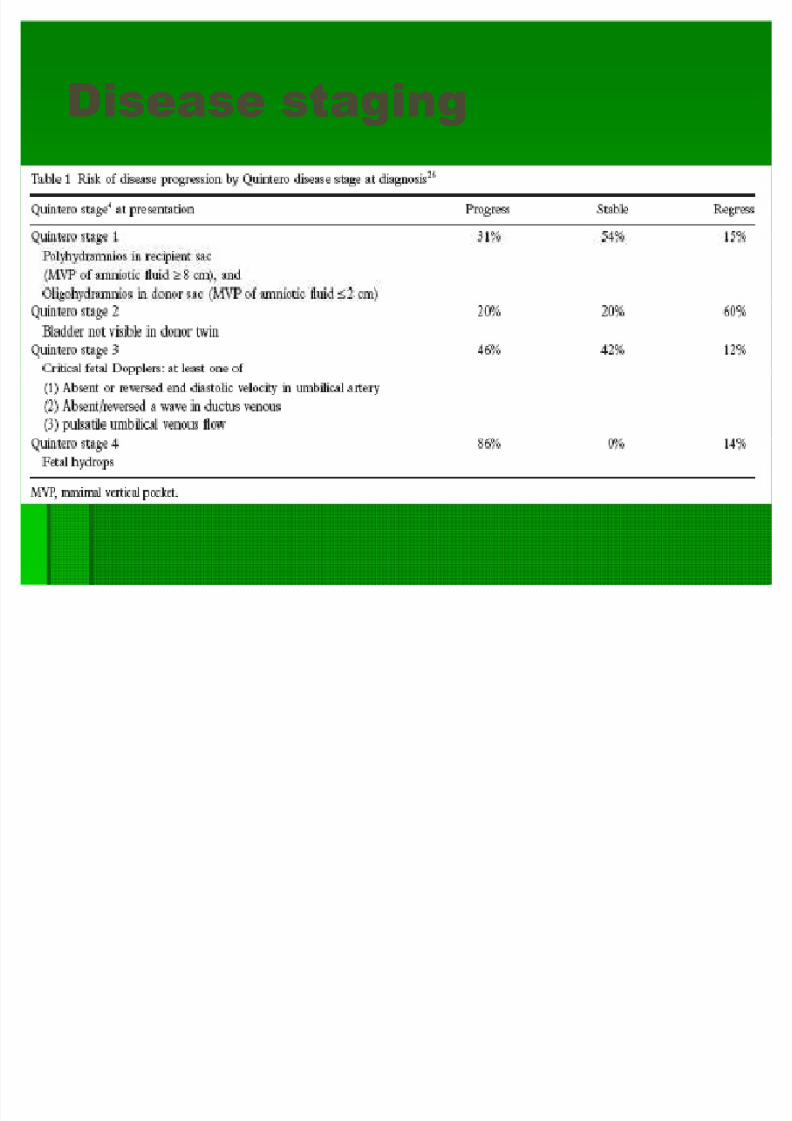
Disease stagingDisease staging
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 14/28
Screening for TTTSScreening for TTTS
1. nuchal translucency1. nuchal translucency Discordant crownDiscordant crown± ±rump length in the first trimester rump length in the first trimester
doesdoes notnot identify those pregnancies destined toidentify those pregnancies destined to
develop TTTS, butdevelop TTTS, but increased nuchalincreased nuchal
translucency (NT) and/or NT discordancetranslucency (NT) and/or NT discordance ininmonochorionicmonochorionic twins is associated with antwins is associated with an
increased risk for subsequent development of increased risk for subsequent development of
TTTS.TTTS.
Increased NT (>Increased NT (> 95th centile) at 1095th centile) at 10± ±14 weeks a/w14 weeks a/w
a likelihood ratio of 3.5 (95% CI, 1.9a likelihood ratio of 3.5 (95% CI, 1.9 ± ±6.2) for the6.2) for the
development of severe TTTS.development of severe TTTS.SebireSebire et et al al . Hum. Hum
Reprod 2000Reprod 2000
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 15/28
This transient finding probably reflectsThis transient finding probably reflects
impaired ventricular function of theimpaired ventricular function of the
immature fetal heart in the hypervolaemicimmature fetal heart in the hypervolaemicrecipient twin;recipient twin;
thethe improvement with advancingimprovement with advancing
gestationgestation is likely because of is likely because of improvedimprovedventricular complianceventricular compliance and theand the
establishment of diuresis.establishment of diuresis.
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 16/28
Among twin with discordant NTAmong twin with discordant NT,,
discordant reversal of the µa¶ wave in thediscordant reversal of the µa¶ wave in the
DV was useful in identifying those twinsDV was useful in identifying those twinsthat went on to develop TTTS.that went on to develop TTTS.MatiasMatias
et et al al . J Matern Fetal Med 2005. J Matern Fetal Med 2005
Screening for TTTSScreening for TTTS
2.2. First trimester ductus venosus (DV)First trimester ductus venosus (DV)
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 17/28
an early ultrasound marker of amniotican early ultrasound marker of amniotic
fluid discordancefluid discordance
the likelihood ratio of membrane foldingthe likelihood ratio of membrane folding
on ultrasound aton ultrasound at between 15 and 17between 15 and 17
weeks gestationweeks gestation for the subsequentfor the subsequent
development of TTTS was 4.2 (95% CI development of TTTS was 4.2 (95% CI 3.03.0± ±6.0).6.0).SebireSebire et et al al . Hum Reprod. Hum Reprod
20002000
Screening for TTTSScreening for TTTS
3. Intertwin membrane folding3. Intertwin membrane folding
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 18/28
Surveillance for TTTSSurveillance for TTTS
BIW after NT assessment for monochorionicBIW after NT assessment for monochorionic
twinstwins
amniotic fluid discordance, intertwinamniotic fluid discordance, intertwin
membrane folding, bladder volumes, andmembrane folding, bladder volumes, and
Doppler studies.Doppler studies.
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 19/28
Diagnosis and assessmentDiagnosis and assessment
of TTTSof TTTS Minimum sonographic criteriaMinimum sonographic criteria
(i) (i) monochorionicmonochorionic twins, that is,twins, that is, singlesingle
placenta, same sex twins, and absence of placenta, same sex twins, and absence of intervening chorion (µtwin peak¶ sign);intervening chorion (µtwin peak¶ sign);
(ii) oligohydramnios (maximal vertical pocket(ii) oligohydramnios (maximal vertical pocket
(MVP) (MVP) 22 cm) in the donor sac; andcm) in the donor sac; and
(iii) polyhydramnios (MVP (iii) polyhydramnios (MVP 88 cm) in thecm) in the
recipient sac.recipient sac.
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 20/28
Differential diagnosesDifferential diagnoses
1.1. selective intrauterine growth restrictionselective intrauterine growth restriction(IUGR), which also affects 15% of (IUGR), which also affects 15% of monochorionic twins, and may result inmonochorionic twins, and may result inoligohydramnios, delayed growth andoligohydramnios, delayed growth andabnormal umbilical Dopplers in one twin.abnormal umbilical Dopplers in one twin.
2.2. monochorionic twins discordant for anomalymonochorionic twins discordant for anomaly(particularly(particularly renal agenesisrenal agenesis) may result in) may result in
anhydramnios around one twin.anhydramnios around one twin.
---- neither of these conditions is associatedneither of these conditions is associatedwith polyhydramnios in the other twinwith polyhydramnios in the other twin
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 21/28
Treatment optionsTreatment options
untreated perinatal mortality for severeuntreated perinatal mortality for severe
midtrimester TTTS is up to 90%.midtrimester TTTS is up to 90%.
1.1. Selective laser photocoagulationSelective laser photocoagulation
(SLPC) of intertwin vascular (SLPC) of intertwin vascular
anastomosesanastomoses
2.2. Amnioreduction and septostomyAmnioreduction and septostomy3.3. cord occlusion in TTTScord occlusion in TTTS
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 22/28
TTTS in monochorionicTTTS in monochorionic
monoamniotic (MCMA)monoamniotic (MCMA) much less commonmuch less common nearly all MCM A placentasnearly all MCM A placentas
have AA anastomoses, and a decreased number have AA anastomoses, and a decreased number of AV anastomoses, when compared to MCD A of AV anastomoses, when compared to MCD A placentas.placentas.
may still occur may still occur ----will lack the classic sign of will lack the classic sign of discordant sac size.discordant sac size.
----The combination of polyhydramnios in the singleThe combination of polyhydramnios in the single
amniotic cavity withamniotic cavity with discordant bladder sizediscordant bladder size isisusually sufficient to make the diagnosis,usually sufficient to make the diagnosis,particularly where there are discordant cordparticularly where there are discordant corddiameters and abnormal Doppler waveformsdiameters and abnormal Doppler waveforms..
---- S tage 1 disease, however, may escape detectionS tage 1 disease, however, may escape detection..

8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 23/28
TTTS inTTTS in
Dichorionic diamnion?Dichorionic diamnion?Dizygotic twins?Dizygotic twins?
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 24/28
1. monochorionic dizygotic1. monochorionic dizygotic
twins seems increase after twins seems increase after
pregnancy by ART(?)pregnancy by ART(?)
Monochorionic (MC) dizygotic twins (DZT) areMonochorionic (MC) dizygotic twins (DZT) areextremely rare in natural pregnancyextremely rare in natural pregnancy
1.1. Unusual monochorionic placentation withUnusual monochorionic placentation withheterosexual twins.heterosexual twins. ObstetGynecol 1970;36:621ObstetGynecol 1970;36:621--5.5.
2.2. sexsex--discordant monochorionic twins conceived by indiscordant monochorionic twins conceived by invitro fertilizationvitro fertilization The New England Journal of The New England Journal of
Medicine.Medicine. 2003. 349(2): 1542003. 349(2): 154--159 159 3.3. DZ monochorionic twins conceived by ART, of whichDZ monochorionic twins conceived by ART, of whichone has both Klinefelter syndrome and Beckwithone has both Klinefelter syndrome and Beckwith--Wiedemann syndrome (BWS).Wiedemann syndrome (BWS).Journal of Journal of PediatricsPediatrics.2005, 146(4):565.2005, 146(4):565--567567
----J Hum Genet. 2005;50(1):1J Hum Genet. 2005;50(1):1--6.6.
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 25/28
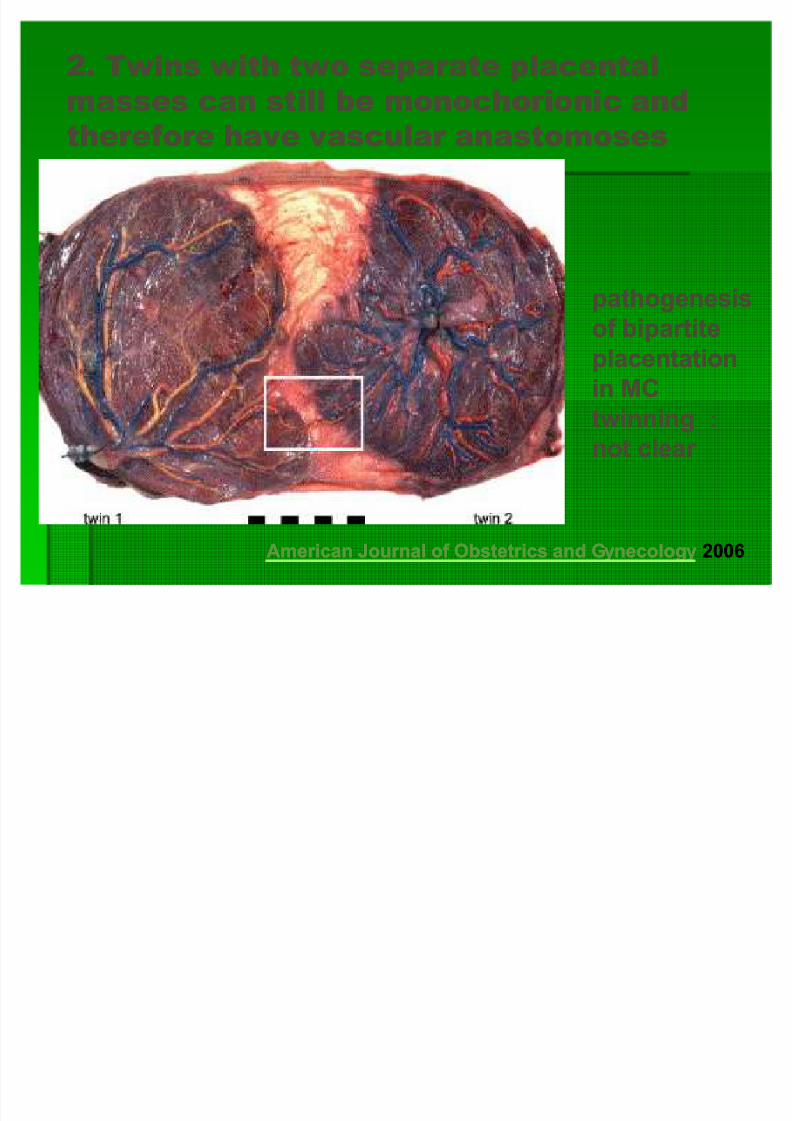
2. Twins with two separate placental2. Twins with two separate placental
masses can still bemasses can still be monochorionicmonochorionic andand
therefore have vascular anastomosestherefore have vascular anastomoses
American Journal of Obstetrics and GynecologyAmerican Journal of Obstetrics and Gynecology 20062006
pathogenesispathogenesis
of bipartiteof bipartite
placentationplacentation
in MCin MC
twinningtwinningnot clear not clear
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 26/28
True DADC?True DADC?
The combination of the lambda sign or 2The combination of the lambda sign or 2
separate placentas on sono in twin pregnanciesseparate placentas on sono in twin pregnancies
predicts dichorionicity with a sensitivity of 97%predicts dichorionicity with a sensitivity of 97%
and a specificity of 100% ; ³T´ signand a specificity of 100% ; ³T´ sign ---- the mostthe mostuseful sign in predicting monochorionicity with auseful sign in predicting monochorionicity with a
sensitivity of 100% and a specificity of 98%.sensitivity of 100% and a specificity of 98%.
G A 10G A 10--14 wks14 wks
2 separate placental masses are not per se DC 2 separate placental masses are not per se DC
Microscopic examination of the intertwinMicroscopic examination of the intertwin
membrane after deliverymembrane after delivery ---- the gold standard for the gold standard for
chorionicitychorionicity
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 27/28
If true DADCIf true DADC
Anastomotic communication was found Anastomotic communication was foundalmost universally in monochorionicalmost universally in monochorionicplacentation and very rarely withplacentation and very rarely withdichorionic placentas.dichorionic placentas. Placental injectionPlacental injectionstudies in twin gestation.studies in twin gestation. Robertson EG.Robertson EG. Am J Am J Obstet Gynecol Obstet Gynecol 1983; 147(2): 1701983; 147(2): 170--174174
Vascular Anastomoses in DichorionicVascular Anastomoses in Dichorionic
DiamnioticDiamniotic--Fused PlacentasFused Placentas
sideside--toto--side connections between smallside connections between smallsubchorionic vessels.subchorionic vessels. International Journal of International Journal of Gynecological Pathology. 22(4):359Gynecological Pathology. 22(4):359--361, October 361, October 20032003
8/8/2019 TTTS discussion1
http://slidepdf.com/reader/full/ttts-discussion1 28/28
NonNon--immune hydrops fetalisimmune hydrops fetalis
1.1. Cardiac failureCardiac failure
2.2. Anemia Anemia
3.3. Arteriovenous shunts Arteriovenous shunts
4.4. Mediastinal compressionMediastinal compression
5.5. Metabolic disorder Metabolic disorder
6.6. Fetal infection/tumor Fetal infection/tumor 7.7. Congenital renal/pulmonary/GI/skeletal defectCongenital renal/pulmonary/GI/skeletal defect
8.8. Chromosomal anomaliesChromosomal anomalies




![=58t2 1W352 D - Wing On Travel€¦ · M@F RSQTPCBABGADBCH MKN?N?NIK?GDF TiCU[vjSUST TTTS JLNIKBGON 8F mj SR5Q+j6F]Zd3L~cC nj 0XP3{jF]6[/yO}ZtDIA1](https://img.pdfslide.us/doc/110x75/5e993d2717c1be5e1c1e0e5d/58t2-1w352-d-wing-on-travel-mf-rsqtpcbabgadbch-mknnnikgdf-ticuvjsust-ttts.jpg)














![^mt%:m' mm mmmitm - NYS Historic Newspapersnyshistoricnewspapers.org/lccn/sn83031566/1865-09-14/ed-1/seq-3.pdf · if % C *-~ s&frgtet^ttts*! 1865] ^iLi,-.4. — y ... i I •» •](https://img.pdfslide.us/doc/110x75/5e2429f61f2c01561513a97e/mtm-mm-mmmitm-nys-historic-newspapersn-if-c-sfrgtetttts-1865.jpg)


![,V O - Wing On Travel · BV^dbR\ H_caeV 0JedcZUV PZVg1 > q]kN?fG]@2|GcqE] ... =JN/=} /2 O8.8 mwkN~c?SUST TTTS ... 9:;8 iRDDJFbtUjKDG+E3hB *RHE>O>p7LIF 2>ILKp:](https://img.pdfslide.us/doc/110x75/5b4e41427f8b9ab7608b4898/v-o-wing-on-travel-bvdbr-hcaev-0jedczuv-pzvg1-qknfg2gcqe-jn.jpg)





