Embed Size (px)
Citation preview

Ttie Internafionai Journal of Periodantics & Restorative Dentistry

333
Immediate Loading of Root-formImplants: Two Case Reports 3 YearsAfter Loading
Robert A, Levine, DDS*Louis Rose, DMD"Henry Saiama,
This study examines a protocol tor aohieving successful osseointegration inImmediately ioaded implants. With an atraumotic surgical fechnique and anaoceptabie biomateriat for implant piacement in certain cases adequatesplinting of impiants may sufñcientiy shield the bone-implant interface fromfunotionai overload and prevent micromovement from exceeding theaiiowaPie limits for successful osseointegration. Two successtui cases are pre-sented in which titanium root-form implants were immediately iooded for thesupport of fixed restorations in the maxiila and the mandibie. The authorscandude that tor a distinot patient popuiation, immediate iooding of multi-pie, spiinted implants may prove to be a valuable adjunct to therapy(int J Periodont Rest Dent 1998:18:333-343.)
'Chairman and Program Director, Periodontios, Albert EinsteinMedicai Center, Philadelphia, Pennsylvania: and Prívale Praclicein Periodontics and Implant Dentistry, Philadeiphia, Pennsylvania.
"Professor, Periodontics, Sohooi of Dental Medioine, University ofPennsylvania, Philadelphro, Pennsylvania: Chief and Professor,Medicine and Surgeiy, Division of Dental Medicine, AlleghenyUniversify ot fhe Healfti Sciences, Philadelphia, Pennsyivania: andPrivofe Practice in Periodonfics, and Implanf DentistryPhiladeiphia, Pennsylvania.
"Assisfanf Clinicai Professor, Periodontios and PeriodonfaiProstheses, University of Pennsylvania. Philadelphia.Pennsyivania;and Private Practice, Atlanta, Georgia.
Reprint requests: Dr Robert Levine,21 IPhiladeiphio, Pennsylvania 19115.e-moil: [email protected]
•ustieton Avenue, Suite
Before the principies of osseoin-tegrotion were fuiiy understood,the protocci for piacing endo-steal blade implants routinelyinvolved immediate loading ofthe impianfs. This techniquecontributed to the high rate ofimpiant complications and faii-ures eariy on and wos wideiycriticized by the general dentalcommunity,^ Once the impor-tance of achieving ond main-taining osseointegration wasrecognized, however, nevi/impiant designs, materiais, andatraumatio surgical techniqueswere deveioped to addressthese eariy probiems. Theseconsiderations have dramati-cally increased the successand predictability of dentalimplonts.2-5
The original guidelines forachieving osseointegrationinvariabiy oaiied tor submergingthe impiant and keeping itload-free during the healingperiad.^ The logio was thatimmediate ioading can campii-cate csseous healing andremodeiing at the bone-impiant
Voiume 18, Number 4,1998
334
interface following surgery lead-ing to the deveiepmenf ef afibreus layer between the beneand implant rqther than newbone gravi/th qnd esseeintegra-tien,^ In additien, submergingthe impiont was deemed to beerueiai fer preventing infeetienend epitheiiai dewngrewth.^These prerequisite steps ied fofhe sfandard prefecoi currentlyfollowed fer esseeintegratedimplants, which typicaiiy calis forkeeping fhe fixfures unloodedfor ó monfhs fellewing pioce-menf in the maxilla and for 3 fo4 months in fhe mandibie.'
Protecting the bene-impiantinterface is stiii a critical gaai inimplant cases because thequality of bone modeling ondremedeiing in the surgical areais the ultimate predictor ef fheimpianfs success and survivol. °Microscopic cutting and fiiiingcones, composed af asteociasfsqnd osteoblasts, respectively,ore responsible for remodelingot fhe bone-implant interface."it is critical, however, thatimplants be kept os sfable aspessibie. Excessive micromove-ment, ar movement of theimplont surface in reiqfion ta thebene, can easily result from pre-mqture functionol overload efthe fixture. This, in turn, cqn dis-rupt the early remedeiingprocess,'^ resuiting in fibrousrepair at the interface rotherthan esseeintegration.'^^'" Forthis reoson, researchers con-tinue to explore ways to de-velop and maintain this rigid
bone-implant interface in fermsof beth meehanics and bioiogy.
With this in mind, it is ciearthqt any deviation from thestandord protacoi of deiayedioading must be undertakenenly with a theraugh under-standing of the risks inherent toproper osseointegrotien. Never-theless, in reeent years, the"absoiute" requirements af sub-mergence and deloyed Iood-ing have been reexamined. Forinstance, researchers usingStrqumann ITI impiants havedemonstrated highiy predict-obie osseaintegrqtian resultsusing G one-stage nonsub-merged procedure.^''^"'® in-deed, it is now fqiriy widelyGccepfed that when good oroihygiene is maintained, a ene-stage piGcement opproochdoes not exert any significonfinfluence en euteeme.
The issue of immediateiaading raises a much moreimportant concern, however,because it is still necessory teshield fhe bene-impiqnt inter-face from excessive force dur-ing early healing. A review effhe liferature reveGis severoireports of esseoinfegrafion suc-cess, demanstrated both ciini-caiiy and histolegicaily, whenimmediate Iaading techniquesthat ailawed for minimal, but notexcessive, functional lead toimplants were used. For in-stance, BGbbush et G P ' re-ported a highly successfulimmediate-leading techniquethat incarparafed q splinting
The intemotionai Journal of Periodonfics & Restorative Dentistry

335
step fo reconstruct the edentu-lous mondibie. In this study 484patients received a fotai of1.739 titanium plasma-sprayed(TPS) screw implants. The pa-tients were evaiuoted pro-spectiveiy ond the cumuiativesuocess rote wos 88%.
The use of q Doider bor fhqfwos secured fo four implants inthe onterior mandible within 2to 3 doys after implant place-ment opparently accounted torthe exceiient resuit. At thot time.a sott tissue reiining of theinterim denture was under-taken. The provisional restorationwos maintained for only 2 fo 3weeks before the permanentciip-retqined overdenture wospiaced. The spiinting action ofthe Doider bar qpparentiy stobi-iized the bone-impiant intertaceogoinst chewing forces andoiiowed for functionai loodingof the impiont much eoriier thonstandard protocoi dictates."
in a more recent study,Schnitman et oP-° ond Wohrie etaP' reported using immedioteiylooded two-stage threadedimpiants in supporting pravi-sionai fixed restorotions in themqndibie. Their resuits ih eightpatients demonstroted not onlythe qbiiity ot these immediqfeiyloaded impiants to successfuiiysupport provisionoi fixed restoro-tions during the healing phase,but oiso the abiiity of 19 of fhe22 impiants to osseointegrate.Moreover, fhe invesfigafors foundno stotisticaiiy significant differ-ence when they compared the
failure rate ot immedioteiylooded implants with that ofimplants that had heaiedunloaded in the some potientsafter 5 years.
Lum and covi/orkers^^ pre-sented histoiogic evidence ofosseointegration when immedi-ately ioaded hydroxyapafife-coafed biade impianfs wereplaced ond spiinted to firm nof-urai teeth during heoiing inmonkeys. Using q beqgle mo-del. Sagqra et ai^^ presentedccrroborating histoiogic evi-dence ot osseointegrafion withuniiateraliy spiinted one-stagetitanium screw impionts thotwere immediateiy loaded. Theirfindings aiso suggested thotoithough osseointegrotion hadoccurred, increosed morginoibone ioss moy be o sequeio ofimmediafe ioading.
Brunski " has theorized thofmicromovement must be iim-ited to 100 Mm or less to achieveoptimai osseous regeneration.Based on this iiterafure revievi/,one can hypothesize thot suchmicromovement con be sutfi-cienfiy minimized, even forimmediofeiy ioaded impiants, ifthe foiiowing conditions aremet: an atraumctic surgicaltechnique is used, the impiantsare made of on occepfabiebicmateriai. and the loadedimpiants ore odequateiy stabi-iized by splinting. Other impor-tont stqbiiizing facfors inciudean opfimal distribution of im-pionfs and o profecfive oc-ciusai scheme. Mosf recenfly
Soiamq ef oi^^ reported on fhesuccessfui use of immediafeloading of spiinted impianfs.
The purpose ot this reporfwos fo expiore the roie thof animmediate-ioading protocoimight piay in ourrenf and futureimplant therapy cases. Reportsof fwo coses freated by fhe pri-mary author in private proctice,in which titanium root-formimpionts were immediateiyioaded to support fixed restora-tions in fhe moxiiia ond themandibie, are presented. Therationale and guideiines for suc-cessfuiiy using this adjuncfivetechnique are aisc discussed.
Case report 1
A óO-year-oid nonsmoking manpresented in October 1992. Hewos interested in hoving a fixedportiai denture in his moxiiiaryarch after hoving worn oremovabie partiai denture torover 20 yeors (Figs 1 o ond 1 b).The patient hqd noticed ttiat hisfeefh had become very iooseover the previous coupie ofyears, but he had not seen odentist in the 3 years since hisiast dentqi cleaning.
The patient's medicai his-tory at presentation was non-ccntributory, buf fhere was a his-fory af periodontal diseose onboth sides of fhe famiiy Radio-graphic examinofion reveaiedodvanced periodonfifis in themaxiiiary arch, which coincidedvi/ith generaiized 3-degree
Volume 18, Number 4,1998
336
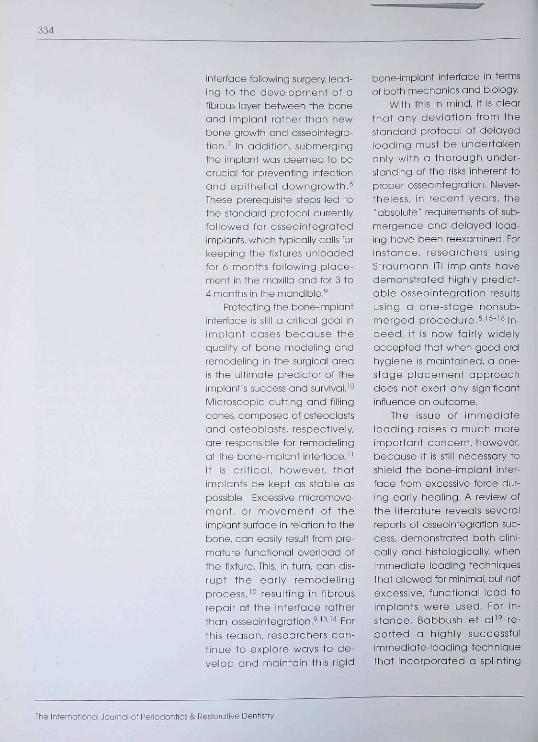
Fig la Case 1 an the day of surgery. July 1993 Pafient has five remaining moxiiiaryteeth with severe mobiiify and on ill-fitting maxillary removable partiai denture.
Fig Ib Complefe-mouth radiographs. October 1992. showing severe periodontaidisease in the maxilla and maderate-to-severe periodontal disease in the mandibie.There is a poor crown to root ratio, especially in the maxiiia.
mobility on the remaining abut-ment teeth: numbers 10(3)through 14(5) and 24(12) and25(13) (Federation DentoireInternationale tooth numberingsystem: Universal tooth numbersin parentheses). Probing depthsreaohed up to 10 mm posteri-orly in the mandible with 1 to 2degrees of mobiiity in 36(19),35(20), and 48(32). ond 2 de-grees in 47(31). Based en ciinicaland radiogrophiC examinotiona diagnosis of generalized mod-erate-to-advanced periodontitiswos noted with the prognosisthat oil moxiliory teeth werehopeless ond that teeth num-bers 37(18), 36(19), 47(31), ond18(32) had a guarded prognosis,
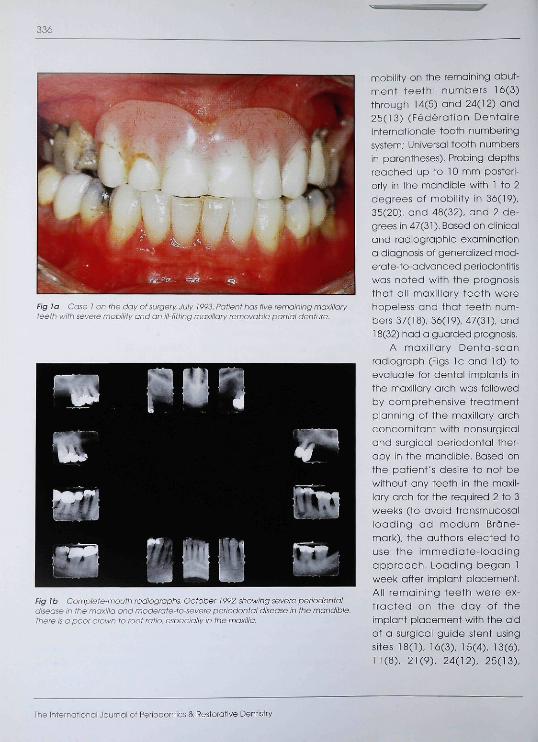
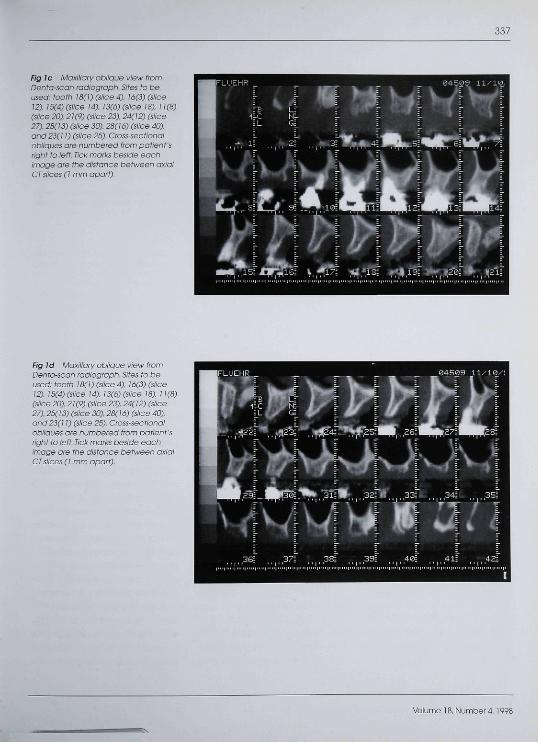
A maxillary Denta-scanradiogroph (Figs Ic and Id) toevoiuate for dental implants inthe maxiliary arch was foliowedby comprehensive treotmentpianning of the maxiliory orchconcomitant with nonsurgicaiand surgical periodontal ther-apy in the mandible. Based onthe patient's desire to not bewithout any teeth in the maxii-iary arch for the required 2 to 3weeks (to avoid transmucosalioading ad modum Brâne-mark), the authors elected touse the immediate-loadingopproach. Loading began 1week after implant placement.All remoining teeth were ex-tracted on the day of theimplant placement with the aidof a surgicai guide stent usingsites 18(1), 16(3), 15(4), 13(6),11(8), 21(9), 24(12), 25(13),
The Internafionol Journal of Periodontics & Restorative Dentistry
337
Fig Je Maxiilary obiiQue view fromDenfa-scan radiograph. Sifes fo beused: footh 16(i) (siice 4), 16(3) (slicei2), 15(4) (siice 14), 13(6) (siice 18). 11(8)(slice 20), 21(9) (siice 23), 24(12) (siioe27). 25(i3) (siice 30), 28(16) (siioe 40).and 23(11) (siice 25). Cross-sec f/onoiobiiques are numbered from patient'srighf fo ieft Tick marks beside eachimage are fhe disfance befween axialCT slices (I mm apart).
Fig la Maxiiiary obiique view fromDenfa-scan radiograph. Sites fa beused: tooth 18(1) (slice ä), 16(3) (slice¡2), ¡5(4) (siice 14), 13(6) (siice 18), 11(8)(siice 20), 21(9) (siioe 23), 24(12) (siice27), 25(13) (siice 30), 28(16) (siice 40),and 23(i ¡) (siice 25). Cross-sectionalobiiques are numbered fram patient'sright to lett. Tiok marks beside eachimoge ore the disfance between axiaiCT slices (1 mm apart).
Valume 18, Number 4,
338
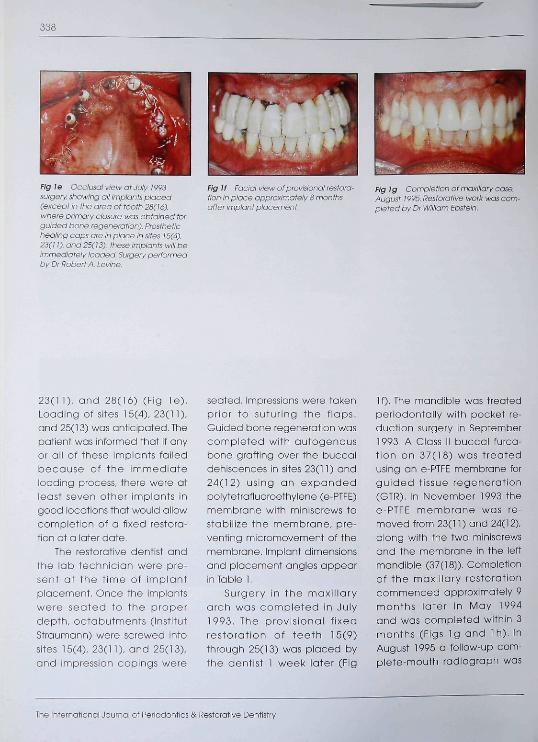
Fig le ^^-.-.'i.;;O' '..r-u :.;','IJ.'Í 1-^93surgery, showing all impiants pioced(except in the area of tooth 28(16),where primary closure was obtained forguided bone regeneration). Prosthetichealing cops are in place in sites ¡5(4),23(11), and 25(13); these impionts wiii beimmediotely loaded. Surgery performedby Dr Rabert A. Levine.
Fig If Facial yiew of provisional restora-tion in pioce approximotely 8 monthsafter implant placement.
Fig Ig Compiet'or. cA mnxillary case.August 1995. Restorotive wark wos com-pleted by Dr Wiiliam Epstein.
23(11), and 28(16) (Fig le ) .Loading of sites 15(4), 23(11),ond 25(13) was anticipated. Thepatient was informed that if anyor all of these implants failedbecause of the immediateloading process, there were atleast seven other implants ingood iocations that would allowcompletion of a fixed restora-tion a ta iater date,
The restarative dentist andthe lab technician were pre-sent at the t ime of implantplacement. Once the implantswere seated ta the praperdepfh, ocfabutments (institutStraumann) were screwed intosites 15(4), 23(11), and 25(13),and impression capings were
seated, impressions were takenprior to suturing the flaps.Guided bone regeneration wascompieted with autogenousbone grafting over the buocaidehiscences in sites 23(11) and24(12) using an expandedpoiytetrafiuoroethyiene (e-PTFE)membrane with miniscrews tosfabiiize the membrane, pre-venting micromavement of themembrane. Implant dimensionsand piacement angles appearin Table 1.
Surgery in the maxil laryarch was cample ted in July1993, The provisional fixedrestorat ion of tee th 15(9)through 25(13) was piaced bythe dentist 1 week later (Fig
10. The mandibie wos treotedperiodantaliy with pocket re-duction surgery in September1993, A Class II buccal furco-t ion on 37(18) was treatedusing an e-PTFE membrane forgu ided fissue regenerafion(GTR). In November 1993 thee-PTFE membrane was re-moved from 23(11) and 24(12),alang with the two miniscrewsond the membrane in the leffmandible (37(18]). Completionof the moxiiiary restorationcommenced approximateiy 9manths later in May 1994and was completed v/ithin 3manths (Figs Ig and Ih), InAugust 1995 a tollow-up com-plete-mouth radiograph was
The International Journal of Periodontics & Restorative Dentistry
339
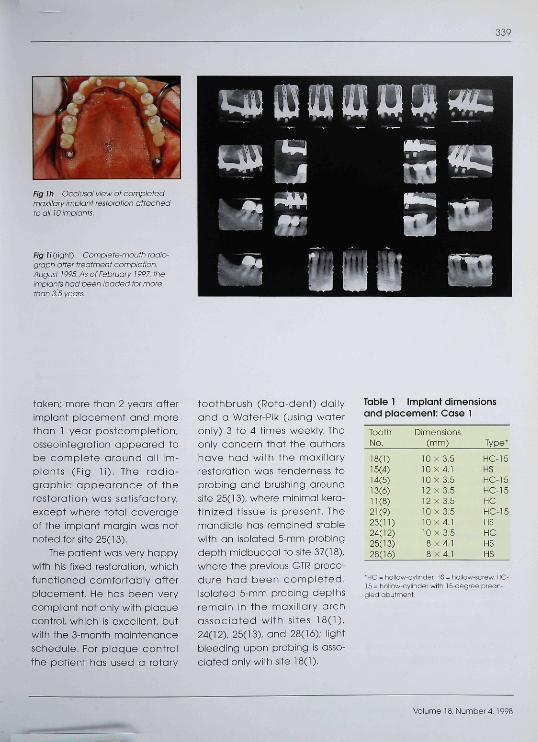
Fig J/i Occtusai view of completedmaxiiiary impianf restoration attachedto ail lOimpiants.
Fig liCiQht) Complete-mouth radio-graph after treatment compietian.August 19Ç5.AS of February 1997. theimpiants had been ioaded for marethan 3^5 years.
taken; more thon 2 yeors Gfferimplant placement and morethan 1 year postcampletien,esseaintegration appeared tabe complete around GII im-pionts (Fig l i ) . The radio-grophic appearance ef theresteratien wos sofisfoctory,except where totol coverogeof the implant margin was notnoted for site 25(13),
The pafient was very happywith his fixed restoration, whichfuncfioned cemfortably offerplacement. He has been verycempliont net anIy with plaquecontrel, which is excellent, butwith the 3-month maintenanceschedule. Far plaque cantrclthe patient has used G ratory
toothbrush (Refa-dent) dailyond G Water-Pik (using wateronly) 3 to 4 times weekly Theoniy concern thot the authorshave had wifh the maxiiiaryresteretion was tenderness teprobing qnd brushing Groundsite 25(13), where minimol kero-tinized tissue is present. Themandible has remained stabiewith an iseloted 5-mm probingdepth midbuccol ta site 37(18),where the previous GTi? prece-dure had been campieted,Iselated 5-mm probing depthsremain in the maxillary archassociated with sites 18(1),24(12), 25(13), and 28(16); lightbieeding upan probing is asso-ciated eniy with site 18(1).
Table 1 Implant dimensionsand placement: Case 1
ToothNo.
18(1)15(4)14(5)13(6)11(8)21(9)23(11)24(12)25(13)28(16)
Dimensions(mm)
10x3,510x4,110 X 3,512 X 3,512 X 3,510 X 3,510X4,110X3,58x4,18 X 4,1
Type*
HC-15HSHC-15HC-15HCHC-15HSHCHSHS
•HC = hollow-cylinder. HS = íiollow-screw, HC-15 - íioiiow-cylinOer with 15-öegree prean-gled abutment.
Voiume 18, Number 4,1998
340
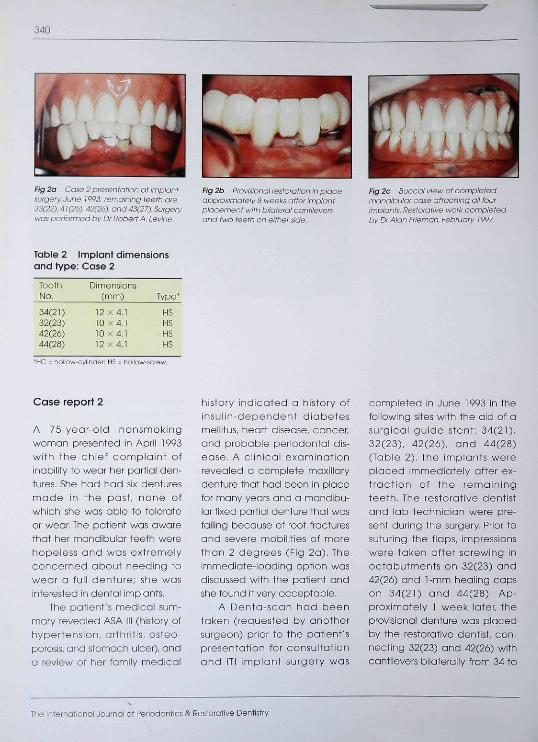
Fig 2a Case 2 presentation at impiontsurgery. June 1993: remaining teeth are33(22). d i (25). â2(2à). and 43(27). Surgerywas performed by Dr RoberfA. Levins.
fig 2b Provisionai restoration in piaceapproximateiy S weeks affer impiantplacement with biiateral cantileversond two teeth on either side.
Fig 2c Buccal view of compietedmandibular case attaching all fourimpiants. Restorafive work compietedby Dr Alan Frieman. February 1997
Table 2 Implant dimensionsand type: Case 2
ToothNo.
34(21)32(23)42(26)44(28)
Dimensions(mm)
12 X4.110 X4.110x4,112 X 4,1
Type'
HSHSHSHS
"HC = riollow-cylinder; HS - hollow-scre'.i
Case report 2
A 75-yeor-old nonsmokingwoman presented in April 1993with the chief compiaint ofinability fo wear her partiai den-tures. She had had six denturesmade in the past, none otwhich she was obie to toleróteor wear. The pafienf was awarethat her mqndibuiqr teeth werehopeiess ond wos extremelyconcerned about needing toweqr a futi denture; she wosinterested in denfai impiants.
The patient's medicol sum-mary revealed ASA ili (history cfhypertension, arfhritis, osteo-porosis, and stomach uicer). anda review ot her fomiiy medicai
history indicated a history ofinsulin-dependenf diobefesmellitus, heort disease, concer,qnd probabie periodontai dis-eose. A clinicai exominotionreveaied o ccmpiete mqxiiiarydenture that had been in piacefor many years and o mandibu-iar fixed partiai denture fhat wastaiiing because of root frocturesand severe mobiiities ot morethan 2 degrees (Fig 2a). Theimmediqte-loadihg opfioh wasdiscussed with the patient andshe found if very occeptabie.
A Denta-scon had beentoken (requested by onothersurgeon) prior to the patient'spresentation for consultationand ITI impiant surgery wos
compieted in June 1993 in fhefoiiovi/ing sifes with the aid of asurgicai guide stent: 34(21),32(23). 42(26). ond 44(28)(Tqbie 2). The implants wereplaced immediateiy otter ex-traction of the remainingteeth. The restorative dentistand lab technicion were pre-sent during the surgery. Prior tosuturing the flaps, impressionswere taken otter screwing inoctabutments on 32(23) and42(26) ond 1-mm heoiing capson 34(21) and 44(28), Ap-proximateiy 1 week iqter, theprovisionoi denture was placedby the resforative dentist, con-necting 32(23) end 42(26) withcantiievers bilateraily from 34 to
The iniernotionai Journai oi Periodontics S; Restorative Dentistry
341
44(21 to 28) (Fig 2b), At o post-operative visit in Juiy 1993 agingivoplasty vyas completedaround the mandibular im-plants after removal of thefixed partial denture becauseof hyperplasia of fhe tissueslocal to the loaded abut-ments. The only problem en-countered during the healingphase vyas the loosening of theprovisional denture from thetemporary cylinders attachedto the octabutments. On twooccosions these areos wererelined and the provisionaldenture wos reinserted.
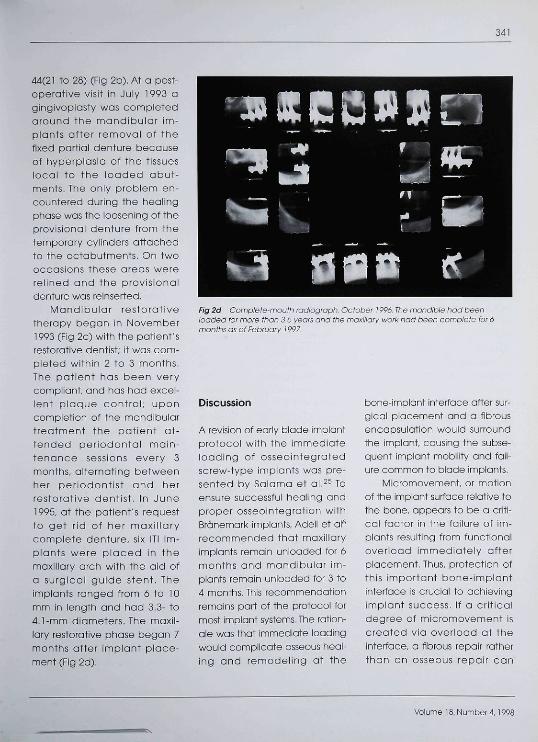
Mandibular restorativetherapy began in November1993 (Fig 2c) with the potient'srestorative dentist; it was com-pleted within 2 to 3 months.The patient has been verycompiiont, and has had excei-lent ploque control; uponcompietion of the mondibulartreatment the patient ot-tended periodontai main-tenance sessions every 3months, alternating betweenher periodontist and herrestorative dentist, in June1995, ot the patient's requestto get rid of her maxillarycomplete denture, six ITl im-plants were p iaced in themaxillary arch with the aid ofa surgical guide stent. TheImpionts ranged from ó to 10mm in length ond had 3.3- to4,1-mm diameters. The maxil-lary restorative phase began 7months after implant place-ment (Fig 2d).
Fig 2d Compiete-mouth radiograph. October 1996. The mandible had beenioaded for more than 3 5 yeors and fhe moxiiiary worl< had been compiete for ómonths as of February ¡997,
Discussion
A revision ot eoriy blade implantprotoooi with the immediateloading of ossecintegratedscrew-type implants was pre-sented by Salama et al.^^ Toensure successful heoiing andproper osseointegration withBrânemork implants, Adeil et al"recommended that maxiiloryimplants remain unloaded for 6months and mondibulor im-plants remain unloaded tor 3 to4 months. This recommendationremains part of the protocol formost implant systems. The ration-ale was that immediate loadingwould complicate osseous heal-ing and remodeling at the
bone-implant interface after sur-gicGi piacement and a fibrousencapsulation would surroundthe implant, cousing the subse-quent implant mobility and fail-ure common to blode implants.
Micromovement, or motionof the impiant surfoce reiotive tothe bone, appears to be a criti-cal factor in the foilure of im-plants resulting from functionaloverload immediately afterplocement. Thus, protection ofthis importont bone-implantinterface is crucial to achievingimplant success. If o crlticoldegree of micromovement iscreated via overload at theinterface, a fibrous repoir ratherthan an osseous repair can
Volume 18, Number 4,1998

342
occur, inhibiting fhe goai cf os-secintegraticn. The interacfionbetween mechanics and bioi-ogy in deveioping and main-taining a rigid bane-impiantinterface ccntinues to be animportant area of research.
A reexamination of the con-cept of immediafe leadingsheuld address at ieast twomain concerns. The firsf concernis thaf immediafeiy ieadingimplanfs weuld ge against fhesubmerged heaiing environ-menf required by fhe originaiBrânemari< profocel. Hevi/ever,nensubmerged impianfs haveproven this tenet unnecessaryby demonsfrafing comparableesseointegrotien success usinga one-stage surgioai opproach.
The second, mere ebviousccncern resuiting from immedi-afe ioading is the need to shieidfhe bene-implanf interface fremfuncfionai overioad during fheearly phases ef healing. Bab-bush et a i " have reported enimmediate splinting of man-dibuiar anferior TPS screw im-planfs. They achieved an 86%success rafe when using aDcider bar secured to four im-pianfs; fhe bar was piaced 2 te3 days affer impianf surgery Theprevisional compiefe man-dibuiar resforafien in fhe studywas seft reiined and used foreniy 2 fe 3 weeks. A permanenfciip-refained averdenture wasthen placed. It appears that thesplinting action of the Dciderbar adequately stabiiized thebone-implant interfaoe and
prevented overioad and follurein fhe majority of fheir cases.
Simiiar resuifs have beenseen wifh immediafeiy loadedfwo-stage implants when usinga fixed provisionai resforafionduring the heaiing phose, osreported by Schnifman ef al^°and Wehrle et al.^' The hypoth-esis of the authors and otherresearchers was that with anotraumatic surgicai techniqueond an acceptable bicmateriaifor impianf piacemenf, ade-quate splinfing cf immediateiyloaded impianfs may sufficientlyshieid the bone-impiant inter-face fc make esseeinfegratiena predictabie resuif becausefhe iimifs of micromovemenf offhis infertace are nof exceeded.
The resuifs of the two casespresented here, along wifh fhepreviousiy pubiished case re-perts, seem te ccntirm fhat thefhreshold cf micrcmovement isnof exceeded wifh immediateiyicaded and splinted implanfs. Afixed temporary restorationimproves chewing, esthetics,comfort, and seif-esfeem duringfhe healing phase. In addition,fhe avoidance cf fransmuccsaiioading of unspiinfed implanfsbeneafh the ccmplefe er parfialdenture increases fhe successrate. The authers' appraach maypravide adequate bone shieid-ing in seiected cases, therebyallowing fcr nermai bone-im-pianf inferface heaiing and pre-dictable leng-ferm osseeinfe-grafien. Muificenter controliedstudies dre needed fo confirm
the viabiiity cf fhis appreach forchanging an established dec-trine of impianf prctacoi.
Conclusion
Delayed impianf ieading re-mains the preferred protocoi forpredicfabiy achieving ossee-infegratien. Based on fhe re-search conducfed fe date, it isthe easiest way to ensure thatthe crucial remedeling phaseat the bone-implant interfacepreoeeds without disruption. Fora distinct patient popuiation.however, immediate ieading efmuitipie, spiinted secondary im-piants may prove fo be a valu-able adjuncf te therapy. Inadditien te aiicwing betterpatient management, immedi-ate ieading can considerobiyenhance restorative and treat-ment options. The obiiity to pro-tect potential regenerative orgrafted sites dramatically in-oreases the number of pcssibietreatment aiternatives for otro-phic ridges. If the same sec-ondory implants prove abie topredictably maintain leng-termosseointegraticn, immediateleading ef cerfain impianfs—piaced under weii-identifiedparameters tor seiecf appiica-ficns—ccuid evenfualiy becemeroutine protocoi. The prerequisitefor achieving esseeintegrationmay fhen shiff from deiayingany ioad en the implant duringearly healing tc simply minimiz-ing fhe iead sufficientiy
The International Journal of Periadonfics & Restorative Denfistry
343
References
1. Rosenlicht JL. Advanced surgicalfechniques in implant dentisfry.Contemporary applicolions of eariytechniques. J Dent Symp 1993:l(Aug):ló-99.
2. Brânemark P-i, Breine U, Lindslrom J,Aden R, Hansson BO, Ohisson A.Intraosseous anchorage of denialprosfheses. I. Experimental studies.Scand J Plast Reconstr Surg 1969;3:81-100.
3. Schroeder A. Pohler O. Sutter F.Gewebereakt ion auf ein Titan-hohlzyiinderimpiant mif Tifonsprit;-schichtoberfloche. Schweiz Monats-schr Zo h nhe i i kd 1970,80.713-727.
4. Bfönemark, P-l, Hansson BO, Adell R.Breine U, Undstrom J, Hallen O, et al,Osseointegrated implants in thetreafment of the edentuious jaw.Experience from a 10-year period.Scand J Plast Reconstr Surg Suppi1977:10:1-132.
5. Sohroeder A, vaci der Zypen E, StichH, Sutter F. The reaction of bone,connective tissue, and epithelium tcendostea! implants with sprayedtitanium surfaces. J Maxillofac Surg1981:9:15-25.
Ó. Adell R, Lekhoim U, Rockier B,Brônemork P-l. A 15-year study ofosseointegrated implants in thetreatment of the edentulous jaw. IntJ Orai Surg 1981:0:387-410.
7. Hansson HA, Albrektsson T.Brânemork P-l. Structural aspects offhe interface between tissue andtitanium impianfs, J Prosthet Dent1983:50:108-113.
8. Brânemark P-l, Zarb GA, Aibrektsson T(eds), Tissue-infegrated Prostheses:Osseointegration m Clinical DentistryCnicago: Quintessence, 1985.
9. Brânemark P-l. Osseointeg rotion andits expér imentai background, JProsthet Dent 1983:50:399-410.
10. Bidez MW, Misch OE. Issues in bonemechanics related to oral impiants.Implant Dent 1992; 1:289-294.
11. Roberts WE. Fundamental principiesof bone physioiogy, metabolism, ondlooding. In: Noert I, uon SteenbergheD. Worthington P (eds) Osseo-integrotion and Orai Rehabiiitotion:An introductory Textbook. London:Quintessence, 1993:157-170.
12. Brunski JB. Biomechanicol tactcrsaffecting the bone-dental implantinterface: Review paper Clin Mater1992;10:153-201.
13. Aspenberg P Goodman S, Toksvig-Lorsen S. Ryd L, Aibrektsson T.intermittenf micromotion inhibífsbone ingro\A/th. Acto Orthop Scond1992:03:141-145.
14. Spector M. Current concepts ofbony ingrowth and remodeling In'Fitzgerald R Jr (ed). Non-cementedTotol Hip Arthroplasty. New Ycrk'Rayen, 1988:09-86.
15. Buser DA, Schroeder A, Sutter F LangNRThe new concept of ITI hollow-cylinder and hollow-screw implants.Part 2. Clinicoi aspects, indications,and early clinical results. Int J OralMaxillotac Implants 1988:3'173-181
1Ó. Buser D, Webei HR Lang NP Tissueintegrotion of nonsubmerged im-piants: 1-year resuifs of a prospec-tive study with 100 ITI hoiiow-cylinderand hollow-screw impiants. Oiin OralImplants Res 1990:1:33-40.
17, Weber HR Buser D, Donath K, FioreiiiniJP Doppalapudi V Paquette DW,Wiiliams RO. Comparison of healedtissues adjacent to submerged andnonsubmerged unloaded titaniumdental implants. A histometrio sfudyin beagle dogs. Clin Orai implantsRes 1990:7:11-19.
18. Levine RA, Olem D, Wilson T,Higginboftom F Saunders S. A multi-oenter retrospective analysis of theITI impionf system used for single-footh repidcemenfs: The USA experi-enoe. Preliminary results at 6 or moremonths of ioading. Int J OraiMoííillofac impiants 1997:12:80-85.
19 Babbush OA, Kenf JN, Misiiei< DJ.Tifanium plasmo-sprayed screwimplorits for the reconstruction ofthe edentulous mandibie. J OralMaKillofoc Surg 1980:44:274-282.
20. Schnitman PA Wohrle PS, RubensfeinJE. immediate fixed interim prosthe-ses supported by two-stage thread-ed implants: Methodology andresults. J Oral Impiantol 1990:16:96-105.
21. Wohrle PS, Schnitman PA, DaSilva JD,Wang N-H, Koch GG. Brânemarkimplants p loced into immediafefunction: 5-year results [obsfract). JOral Implant 1992:18:382.
22. Lum LB, Beirne OR, Curtis DA.Histoiogic evaluation of HA-coatedversus uncoated titanium blodeimpiants in deiayed and immediate-ly ioaded appiicafions. int J OralMaxiliofac implants 1991;6:45ó-4ó2.
23. Sagara M, Yasumasa A, Hiromasa N,Hiromichi T. The effecfs of eariyocclusai loading on one-stoge tito-nium alioy impiants in beogle dogs:A pilot study J Prosthef Dent 1993:09:281-288.
24. Brunski JB. Avoid pitfails of overload-ing and micromotion of infra-osseous impiants (interview). Dentimpiantol Update 1993:4(1O):77-8I.
25. Salamo H, Rose LE, Saiama M, BettsN. immediate ioading of bilaterallysplinted titonium root-form implantsin fxed prosthodontics: A techniquereexamined—Two case reports, int JPeriodonf Rest Dent 1995:15:345-361.
Voiume 18, Number 4,1998






![[1][m] minimally invasive restorative dentistry](https://img.pdfslide.us/doc/110x75/587254011a28ab852f8b7e5b/1m-minimally-invasive-restorative-dentistry.jpg)