Embed Size (px)
Citation preview
Tsunami-affected Scandinavian tourists: Disaster exposure and post-traumatic stress symptoms
TROND HEIR , SUSANNE ROSENDAL , KERSTIN BERGH-JOHANNESSON , PER-OLOF MICHEL , ERIK L. MORTENSEN , LARS WEIS Æ TH , HENRIK S. ANDERSEN , CHRISTINA M. HULTMAN
Heir T, Rosendal S, Bergh-Johannesson K, Michel P-O, Mortensen EL, Weis æ th L, Andersen HS, Hultman CM. Tsunami-affected Scandinavian tourists: Disaster exposure and post-traumatic stress symptoms. Nord J Psychiatry 2011;65:9–15.
Background: Studies of short- and long-term mental effects of natural disasters have reported a high prevalence of post-traumatic stress. Less is known about disaster-exposed tourists repatri-ated to stable societies. Aims: To examine the association between exposure to the 2004 South-east Asian tsunami and symptoms of post-traumatic stress in three Scandinavian tourist populations. Methods: Postal survey of Norwegian, Danish and Swedish Southeast Asia tourists registered by the police when arriving at national airports. Follow-up time was 6 (Norway), 10 (Denmark) and 14 months (Sweden) post-disaster; 6772 individuals were included and catego-rized according to disaster exposure: danger exposed (caught or chased by the waves), non-danger exposed (other disaster-related stressors) and non-exposed . Outcome measures were the Impact of Event Scale — Revised (IES-R) and Post Traumatic Stress Disorder Check List (PCL). Results: Danger exposed reported more post-traumatic stress than non-danger exposed , and the latter reported more symptoms than non-exposed (each P � 0.001). Comparison of the Norwegian and Swedish data suggested that symptoms were attenuated at 14 months follow-up ( P � 0.001). Female gender and low education, but not age, predicted higher levels of symp-toms. Conclusions: Disaster-exposed tourists repatriated to unaffected home environments show long-term post-traumatic stress disorder symptoms related to the severity of exposure.
Natural disasters, Psychological distress, Stress disorders, Posttraumatic stress .•
Trond Heir , Norwegian Centre for Violence and Traumatic Stress Studies , University of Oslo, Kirkeveien 166 , building 48 , N-0407 Oslo , Norway , E-mail: [email protected]; Accepted 16 March 2010.
The Southeast Asian earthquake-tsunami is one of the
largest human tragedies caused by natural disaster in
recent history. On the morning of 26 December 2004, the
tsunami hit the coast of 13 countries around the Indian
Ocean, causing damage and suffering in many regions. It
is estimated that over 2 million people were affected by
the tsunami, with over 230,000 dead and hundreds of
thousands of people injured. The majority of casualties
were among the local population. However, since South-
east Asia is a very popular vacation destination, a large
number of foreign tourists were in the area. It is esti-
mated that about 18,000 adult Scandinavian citizens,
many with children, were on Christmas holiday in South-
east Asia when the tsunami hit. Most were in tourist areas
along the coast, mainly in Thailand. The disaster was thus
exceptional in terms of the number of individuals involved
at a very distant site. A high number of Scandinavian cit-
izens perished in the tsunami: 543 from Sweden, 84 from
Norway and 46 from Denmark.
Studies of short- and long-term mental effects of fl oods,
mudslides, hurricanes and earthquakes have reported a high
prevalence of PTSD and comorbid depression in survivors
(1 – 3). Studies of adult local Thai survivors after the tsu-
nami have reported similar fi ndings (4 – 6). Many Thai
victims of the tsunami — like victims of other natural
disasters — also lost their homes and livelihood, and were
unable to return to their normal environment. Therefore,
the psychological consequences might be associated with
both the level of disaster exposure per se and with the
societal disruption and loss of normal life in the period
© 2011 Informa Healthcare DOI: 10.3109/08039481003786394
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 03
/16/
13Fo
r pe
rson
al u
se o
nly.

T HEIR ET AL.
10 NORD J PSYCHIATRY·VOL 65·NO 1·2011
excluded because of missing or inconsistent data: 40
for exposure data, 272 for the outcome variable Impact
of Event Scale — Revised (IES-R) or the Post Traumatic
Stress Disorder Check List (PCL), and fi ve for age or
gender. For the 6455 respondents included (Table 1),
the number of replies to individual exposure questions
varied between 92% and 99%. Comparing the respon-
dents with the non-respondents revealed only slight dif-
ferences. Respondents in all three countries had a small
overrepresentation of women, while no differences were
found with regard to age distribution. A study of non-
responders in the Norwegian study population showed
that non-responders were less likely to have been
exposed to the tsunami and had lower levels of post-
traumatic stress than those who responded (9).
Study questionnaire A comprehensive questionnaire was initially developed by
the Norwegian research group. In Norway and Sweden, the
22-item IES-R (10) was incorporated in the questionnaire,
following the disaster. Furthermore, generalization of
fi ndings is complicated by the fact that natural disasters
often strike populations with diffi cult and unfavorable
life-circumstances. The poorest countries are most severely
affected (7), and the poorest and most disadvantaged
members of a disaster-affected community are likely to
experience the most serious consequences (8). In contrast,
the Scandinavian tourists who were struck by the tsunami
represented a reasonably well-to-do population on vaca-
tion. They were hit by a single, unexpected and danger-
ous natural disaster and were rapidly repatriated to their
stable societies and generally favorable life-circumstances.
Consequently, this population offers a unique opportunity
to evaluate the effects of being exposed to a sudden-onset
natural disaster, but without experiencing the secondary
disaster stressors.
Initiated by the Norwegian Centre for Violence and
Traumatic Stress Studies, a Scandinavian multi-centre col-
laboration was established to assess the mental health con-
sequences of the tsunami disaster. The aim of the present
study was to examine the association between exposure
to the tsunami and symptoms of post-traumatic stress in
three large Scandinavian tourist populations. An impor-
tant research question was whether exposure to the tsu-
nami that included danger to one ’ s own life was a stronger
predictor of post-traumatic stress symptoms than other
types of disaster experiences. In addition, the study offered
the opportunity to illuminate the possible bearing of the
time interval between exposure to the tsunami and the dif-
ferent follow-up periods on symptom severity.
Subjects and Methods Participants Scandinavian tourists from the tsunami-affected parts of
South-East Asia were repatriated in the days following
the tsunami. The national police in each of the three
countries registered and made lists of their citizens upon
their arrival at Scandinavian airports during the fi rst 3
weeks after the disaster, a total of 2640 Norwegian, 2254
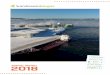
Danes and 12840 Swedes over the age of 18. Figure 1
presents a chart of the population of interest, i.e. all
registered individuals with the minimum age of 18. The
Norwegian and Danish study populations represent all
registered citizens. In Sweden, for formal reasons, the 21
national healthcare regions were asked to take part in the
study. Ten regions accepted, three major and seven minor
regions, accounting for 75% (9614 individuals) of those
12,840 totally registered. The fi nal study populations
comprised 2468 Norwegian, 2174 Danish and 9592 Swed-
ish citizens.
A total of 6772 returned the questionnaire. The
response rates in the three countries are presented in
Figure 1. From this sample, a total of 317 respondents
(55 Norwegians, 175 Danes and 87 Swedes) were
Scandinavian evacuees (>18 years old) registered by the national police when arrival to their home countries from Southeast Asia:
2640 Norwegian, 2254 Danes, 12840 Swedes*
The final study population: Norwegians: 2468 Danes: 2174 Swedes: 9592
Not traceable: Norwegian: 172 Danes: 80 Swedes: 22
Response: 899(36%)
Response: 1055(49%)
Response: 4818(50%)
6 months post
disaster 14 months
post disaster
10 months post
disaster
The Tsunami Disaster 26 December 2004
Dead among Scandinavian citizens: 84 Norwegians, 46 Danes, 543 Swedes
*Of whom 9614 evacuees belonged to the health care regions that participated in the study
Fig. 1. The Scandinavian study population.
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 03
/16/
13Fo
r pe
rson
al u
se o
nly.
TSUNAMI-AFFECTED SCANDINAVIAN TOURISTS
NORD J PSYCHIATRY·VOL 65·NO 1·2011 11
all ” to “ extremely ” regarding their experience with the
tsunami (IES-R items were scored 0 – 4 and PCL 1 – 5).
Scandinavian versions of the IES-R and the PCL have
been translated and back-translated, and a panel of
researchers has approved the fi nal versions. The IES-R
has been used in Norway and Sweden as a research
instrument for many years, and several studies have been
published showing high scale construct validity (12, 13).
The IES-R and the PCL scales were not scored for
individuals with 30% or more unanswered items. Other-
wise, missing data were replaced by the mean value of
the other items. The IES-R mean item score and the
PCL sum score were used as semi-continuous measures
of PTSD symptom severity.
Data analysis The association between the three exposure levels and
PTSD symptoms was analyzed for each country. First,
one-way analyses of variance (ANOVAs) with logarithmic
transformation of the scores and subsidiary Bonferroni-
corrected post hoc t -tests were performed to compare
symptom scores between groups within each country.
Second, a linear regression model was used to adjust for
age, gender and education. The beta coeffi cient value
( β -value) in the regression model was used as measure of
the association, i.e. the difference in the outcome variable
related to a one-step/categorical change in the exposure
variable with other variables kept constant. Education was
included as a binary (high and low) measure, using 13
years ’ education as cut-off. Also, IES-R scores in identi-
cal Norwegian and Swedish exposure groups were com-
pared using t -tests. To enable an illustrative comparison
of symptom levels between all three countries, the Nor-
wegian and Swedish IES-R scores and the Danish PCL
scores were linearly transformed to a scale with a mean
while the Danish study preferred the 17-item PCL (11).
The current study focuses on the relationship between
disaster exposure and post-traumatic stress symptoms.
The questionnaire was mailed to the three Scandina-
vian study populations at three different points in time
after the tsunami. In Norway, the questionnaire was
mailed 6 months, in Denmark 10 months and in Sweden
14 months after the disaster. One reminder was mailed
to non-respondents after 2 – 3 weeks. For the back recep-
tion of questionnaires, the mean number of months since
trauma were 6.4 in Norway, 10.4 in Denmark and 14.5
in Sweden.
Assessment of exposure The questionnaires included detailed registration of expo-
sure to stressful aspects of the tsunami. For the present
analysis, the sample of each country was classifi ed into
three exposure groups: danger exposure , non-danger expo-sure and no exposure . Participants were classifi ed as “ not
exposed ” if they had no contact with the waves or the
fl ood, no physical injuries to themselves or a close rela-
tive, no fear for the safety of relatives and had not wit-
nessed death or suffering others. “ Non-danger exposed ”
was defi ned as having had some of the above-mentioned
disaster-related exposure, but without danger to self.
“ Danger exposed ” was defi ned as having been caught,
touched or chased by waves, which also included possi-
ble exposure to other aspects of the disaster.
Assessment of tsunami effects The presence and intensity of the PTSD symptoms
intrusion, avoidance, numbness and arousal were exam-
ined over the past week (IES-R) or month (PCL). The
participants were instructed to respond to each item,
based on a 5-point Likert scale ranging from “ not at
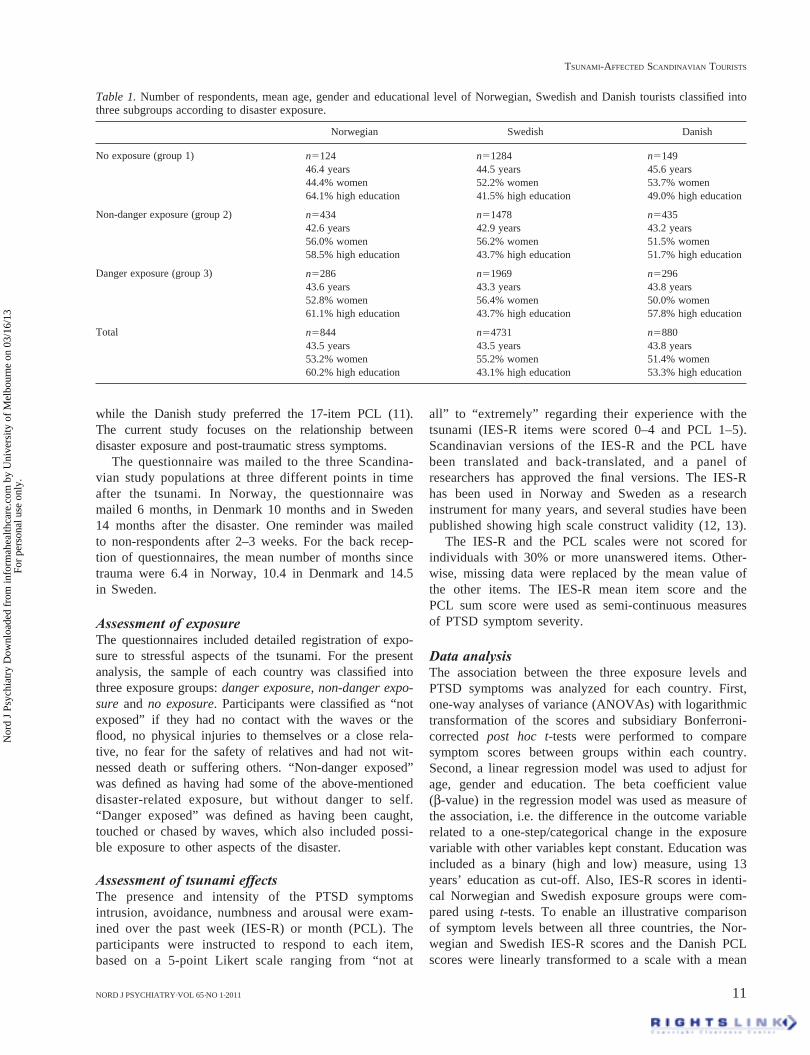
Table 1. Number of respondents, mean age, gender and educational level of Norwegian, Swedish and Danish tourists classifi ed into three subgroups according to disaster exposure.
Norwegian Swedish Danish
No exposure (group 1) n�124 n�1284 n�149
46.4 years 44.5 years 45.6 years
44.4% women 52.2% women 53.7% women
64.1% high education 41.5% high education 49.0% high education
Non-danger exposure (group 2) n�434 n�1478 n�435
42.6 years 42.9 years 43.2 years
56.0% women 56.2% women 51.5% women
58.5% high education 43.7% high education 51.7% high education
Danger exposure (group 3) n�286 n�1969 n�296
43.6 years 43.3 years 43.8 years
52.8% women 56.4% women 50.0% women
61.1% high education 43.7% high education 57.8% high education
Total n�844 n�4731 n�880
43.5 years 43.5 years 43.8 years
53.2% women 55.2% women 51.4% women
60.2% high education 43.1% high education 53.3% high education
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 03
/16/
13Fo
r pe
rson
al u
se o
nly.

T HEIR ET AL.
12 NORD J PSYCHIATRY·VOL 65·NO 1·2011
the waves, and those exposed to severe disaster stres-
sors other than danger. Our fi ndings suggest a strong
relationship between severity of exposure and PTSD
symptoms at 6, 10 and 14 months follow-up independent
of age, gender and education. This pattern was observed
in all three Scandinavian study populations assessed at
different follow-up intervals and with two different symp-
tom assessment instruments. Our data included control
populations of Scandinavian tourists visiting places in the
Southeast Asia not directly hit by the tsunami, but simul-
taneously repatriated. While the control populations had
similar levels of distress symptoms irrespective of follow-
up time, the severity of PTSD symptoms was related to
follow-up time in the exposed populations.
The published peer-reviewed literature (14 – 17, 21) is
consistent in showing that the extent of exposure to a
disaster is probably the most important risk factor for the
development of post-traumatic stress. In this respect, our
fi ndings resemble those in a substantial number of stud-
ies that have been conducted in the aftermath of natural
disasters (1, 22), technological disasters (17, 23) and
mass violence (24).
For the tourists, the tsunami was a totally unexpected
natural fl ood disaster with an extreme suddenness of onset
and a high intensity of impact. It is unusual that natural
disasters are categorized as high-impact disasters, with the
exception of some disasters that have caused extraordinary
destruction and disruption (1, 25). What makes the tourist
population ’ s experiences with the tsunami quite different
and unique is the time-limited stress exposure that con-
trasts with the experience of the indigenous Southeast
Asian population (4 – 6) and of victims of other natural
disasters that have been studied (26). Rapid repatriation of
tourists to stable societies and unaffected home environ-
ments makes their disaster exposure more like large-scale
accidents, human-made or technological disasters such as
shipwrecks, oil rig breakdowns, factory explosions, large
fi res, etc. (17, 27 – 30). These disasters types have high
mortality, are geographically circumscribed and time-
limited, and occur within intact communities.
An evident limitation in the epidemiology of psycho-
traumatology is that a variety of instruments have been
of 0 and a standard deviation of 1 for each country ( Z -
score transformation). Regression analyses were repeated
on the transformed symptom scores. All tests were two-
tailed, and differences were considered signifi cant if
P � 0.05. The statistical analysis was performed using the
software package SPSS version 14.0.
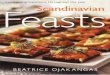
Results Table 2 presents the mean IES-R or PCL scores for the
three exposure groups in each country. In all three coun-
tries, respondents who had been exposed to danger reported
more PTSD symptoms than the non-danger exposure
group, and the latter reported more symptoms than the no exposure group (each P � 0.001).
When comparing the Norwegian and Swedish samples,
similar IES-R scores were found in the no exposure
groups. Among participants in the danger and non-danger
exposure groups, however, the symptom scores were
higher in the Norwegian 6-months data than in the Swed-
ish 14-months data (Table 2).
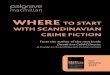
The differences in PTSD symptoms between no exposure and exposure groups remained similar after
adjusting for age, gender and education (Table 3). The
symptom level was higher in women than in men and
higher among those with lower education. Effects of
gender and education were similar across national popu-
lations and follow-up time. The effects of age were
slight and not consistent.
Adjusted effect sizes of exposure after Z -score trans-
formation of symptom scores showed highly signifi cant
differences between the countries: Norway 6 months (non-
danger 0.77, 95% CI 0.59 – 0.95; and danger 1.26, 1.06 –
1.45), Denmark 10 months (non-danger 0.58, 0.41 – 0.75;
and danger 1.14, 0.96 – 1.33) and Sweden 14 months (non-
danger 0.50, 0.43 – 0.56; and danger 0.96, 0.89 – 1.02).
Discussion This multi-centre study of a Scandinavian tourist popu-
lation has shown substantial differences in aftermath
reactions between those who were caught or chased by
Table 2. Post-disaster stress in Norwegian, Swedish and Danish tourists classifi ed in three subgroups according to disaster exposure.
Time after disaster
Norwegian, n�844
6 months
Swedish, n�4731
14 months
Danish, n�880
10 months
IES-R mean score, 5 point scale: 0–4 IES-R mean score, 5 point scale: 0–4 PCL sum score Sum range: 17–85
Non-danger exposure (group 1) 0.39 (0.47) 0.40 (0.48) 19.3 (5.0)
Non-danger exposure (group 2) 1.07 (0.80)∗ 0.80 (0.72)∗‡ 26.5 (11.2)∗Danger exposure (group 3) 1.47 (0.80)∗† 1.17 (0.86)∗†‡ 33.6 (14.7)∗†
The different national populations are assessed at different times after the tsunami. The Norwegian and Swedish population are assessed by IES-R mean
item scores; the Danish by PCL sum score. Results are given as mean values with standard deviations in brackets.
∗Signifi cant difference for group 2 or 3 vs. group 1, P�0.001.
†Signifi cant difference also for group 3 vs. group 2, P�0.001.
‡Signifi cant diff. for the Swedish vs. the corresponding Norwegian exposure group, P�0.001.
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 03
/16/
13Fo
r pe
rson
al u
se o
nly.

TSUNAMI-AFFECTED SCANDINAVIAN TOURISTS
NORD J PSYCHIATRY·VOL 65·NO 1·2011 13
As in most postal surveys of disaster victims, we
achieved response rates close to 50% or lower (14 – 16).
The respondents and non-respondents were similar as
regards age and gender. However, the questionnaires were
focused on exposure to the tsunami, and this resulted in
relatively low response rates among tourists with low or
no direct exposure (9). The most frequently reported rea-
sons for not participating in the study were lack of inter-
est or time and not being directly affected by the disaster
(9). The low response rate among tourists with low or no
direct exposure is more likely to affect estimates of the
frequency of the different types of exposure than the esti-
mates of the differences in PTSD symptom levels between
exposure groups. A biased direction or magnitude of the
effect would imply that the exposed non-respondents
should have shown the opposite pattern provided they had
taken part in the study (18).
Our study is based on a large sample size, comprising
a total of 6455 tourists, presumably healthy before the
disaster, from three Scandinavian countries, and offers
the possibility of evaluating the effect of disaster
exposure without the additional effect of disruption of
home environment and broken societal infra-structure.
While the sheer size of the study population strength-
ens the survey fi ndings, it precluded detailed clinical
examinations at the fi rst follow-up. Accordingly, we have
refrained from estimating the diagnostic prevalence of
PTSD and other trauma-related disorders.
The study includes appropriate no exposure control
groups. The two categories of exposed individuals were
defi ned according to whether they had been exposed to
danger or not. We used a priori defi ned objective criteria
of danger exposure (caught, touched or chased by the
waves) to minimize self-report and recall bias. Non-dan-ger exposure versus no exposure was likewise defi ned on
the basis of what may be considered objective events.
However, exposure to a natural disaster like the tsunami
will typically include a many-faceted disaster impact, and
it is likely that many individuals within the two exposed
applied for the assessment of post-traumatic distress during
the past decades (21, 26). The IES-R and PCL are both
constructed to measure the core symptoms of PTSD and
have been shown to have good psychometric properties
(10, 11). However, they have only been available for a
relatively short time and have not been applied in many
studies of disaster survivors. The interpretation of previ-
ous research is also challenged by the large differences in
sampling strategies and follow-up times, which compli-
cate cross-study comparisons (21). Taking these limita-
tions into consideration, the level of PTSD symptoms
estimated in our danger-exposed group seems to be some-
what lower than among treatment-seeking motor vehicle
accident survivors (31), temporarily relocated earthquake
survivors (32) or Vietnam veterans (19).
The fi ndings suggesting an overall attenuation in PTSD
symptoms between 6 and 14 months are consistent with
the general rule for victim samples to improve as time
passes. In general, longitudinal data suggest that the fi rst
year is the time of peak symptoms or effects (3, 33 – 35).
However, the relatively high burden of PTSD symptoms
observed at 14 months could be a manifestation of pos-
sible long-lasting psychiatric morbidity, which has been
reported after some very high-impact technological disas-
ters (23, 28, 29).
Methodological considerations Two different instruments were used to measure PTSD
symptoms, and demonstrated very consistent and simi-
lar associations with exposure. Although IES-R and
PCL have somewhat different time frames, they share
similar items and conceptual backgrounds and they
have been reported to be highly correlated in compari-
son studies (19, 20). After standardization of the out-
come measures, the effect of exposure declined from
the Norwegian 6-month assessment to the Swedish
14-month assessment with the Danish 10-month assess-
ment in between.
Table 3. Adjusted differences in IES-R or PCL according to exposure group, age, gender and education in Scandinavian tsunami victims.
Time after disaster
Norwegiann�844
6 months
Swedishn�4731
14 months
Danishn�880
10 months
β of IES-R mean score β of IES-R mean score β of PCL sum score
Non-danger exposure(vs. no exposure) 0.65 (0.39)∗∗(0.50–0.80) 0.37 (0.22)∗∗(0.32–0.41) 7.37 (0.29)∗∗(5.19–9.55)
Danger exposure(vs. no exposure) 1.05 (0.60)∗∗(0.90–1.21) 0.76 (0.47)∗∗(0.71–0.81) 14.63 (0.54)∗∗(12.32–16.94)
Age (increase of 10 years) 0.05 (0.75)∗(0.01–0.09) 0.01 (0.12)(–0.01–0.02) –0.13 (–0.14)(–0.74–0.48)
Gender (women vs. men) 0.29 (0.17)∗∗(0.19–0.39) 0.31 (0.19)∗∗(0.26–0.35) 3.35 (0.13)∗∗(1.76–4.93)
Education (low vs. high) 0.21 (0.13)∗∗(0.10–0.31) 0.21 (0.13)∗∗(0.17–0.25) 2.15 (0.11)∗(0.50–3.80)
Results are given as β-values, standardized beta and 95% confi dence intervals of β, according to multiple linear regression performed in each country
population separately.
∗Signifi cant association, P�0.05.
∗∗Signifi cant association, P�0.001.
Adjusted R-square�0.22 (Norwegian), 0.20 (Swedish) and 0.17 (Danish sample).
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 03
/16/
13Fo
r pe
rson
al u
se o
nly.

T HEIR ET AL.
14 NORD J PSYCHIATRY·VOL 65·NO 1·2011
Clinical examinations are needed to establish the
prevalence of PTSD and other disaster-related disorders
in the tsunami-exposed tourist population. Repeated
follow-up surveys are necessary to examine recovery
rates and factors that may infl uence prognosis.
Conclusion Disaster-exposed tourists repatriated to unaffected home
environments show long-term PTSD symptoms related to
the severity of exposure. There was a strong relationship
between severity of exposure and PTSD symptoms. Also,
female gender and low education predicted higher levels
of symptoms. Screening for danger exposure would have
been a possible method for implementing a preventive
strategy against high risk.
Declaration of interest : The authors report no confl icts of
interest. The authors alone are responsible for the content
and writing of the paper.
Funding The Norwegian Directorate of Health and Social Welfare,
The Danish Ministry of Interior and Health and the
Swedish National Board of Health and Welfare funded
this study. The funders had no involvement in the research
process.
Ethical approval The Medical Ethical Board in Uppsala and Oslo. Not
required in Denmark.
Data protection Approval given from the Norwegian, Swedish and Danish
Data Protection Agencies.
References Ironson G, Wynings C, Schneiderman N, Baum A, Rodriguez M, 1. Greenwood D, et al. Posttraumatic stress symptoms, intrusive thoughts, loss, and immune function after Hurricane Andrew. Psychosom Med 1997;59:128 – 41. Basoglu M, Kilic C, Salcioglu E, Livanou M. Prevalence of post-2. traumatic stress disorder and comorbid depression in earthquake survivors in Turkey: An epidemiological study. J Trauma Stress 2004;17:133 – 41. Norris FH, Murphy AD, Baker CK, Perilla JL. Postdisaster PTSD 3. over four waves of a panel study of Mexico ’ s 1999 fl ood. J Trauma Stress 2004;17:283 – 92. Tang CS. Positive and negative postdisaster psychological adjust-4. ment among adult survivors of the Southeast Asian earthquake-tsunami. J Psychosom Res 2006;61:699 – 705. Tang CS. Trajectory of traumatic stress symptoms in the aftermath 5. of extreme natural disaster: A study of adult Thai survivors of the 2004 Southeast Asian earthquake and tsunami. J Nerv Ment Dis 2007;195:54 – 9.
categories had experienced several stressful aspects of
the disaster. Although we are unable to estimate the
effect of single disaster stressors, our analysis suggests
that exposure to danger is an important predictor of
PTSD symptoms at follow-up.
Cultural and social differences among the Scandina-
vian countries are relatively small. The symptom level
was similar in Norwegian and Swedish tourists who had
not been directly exposed. Thus, it is likely that the
observed differences between the Norwegian and Swed-
ish victims who had been exposed to the tsunami —
whether this included danger or not — are related to the
follow-up periods of 6 or 14 months.
Implications The documentation of long-term stress reactions after
the tsunami indicates that the return of citizens to sta-
ble societies, unaffected environments and everyday life
in no way eliminates the impact of such a disaster on
mental health. Even a good recovery environment does
not secure a spontaneous recovery in all of the exposed.
This has implications both for clinicians who should be
aware of possible long-term symptoms in survivors and
for policy makers who should be prepared for future
events. Although natural disasters are increasing in fre-
quency and in terms of number of people affected,
developed countries seem to have reduced the risk to
life by means of solid buildings, warning systems and
evacuation procedures (36). The enormous difference
between industrial countries and the third world in the
number of people killed in the same type of natural
disaster demonstrates this possibility of controlling the
consequences of harmful events (37). Nevertheless,
large numbers of citizens from developed countries may
be exposed to life-threatening disasters through the
extensive and rapidly increasing tourist industry that
often favors destinations in poor countries. Thus, it is
important that national health services have knowledge
and resources to deal with victims of international
disasters.
In all Scandinavian countries, the police and health
services mobilized at the national airports to receive the
repatriated tourists. While their physical health was exam-
ined, no screening was conducted with regard to disaster
stress exposure or stress reactions. The Norwegian Minis-
ter of Health directed the Regular General Practitioners to
contact persons on their patient lists who had been regis-
tered as repatriated. Although the strategy was well
received by the majority of those who were contacted, the
effectiveness of the outreach was reduced because no
high-risk group had been defi ned (38). Screening for dan-
ger exposure upon arrival at national airports would have
been a possible method for implementing a preventive
strategy against high risk.
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 03
/16/
13Fo
r pe
rson
al u
se o
nly.

TSUNAMI-AFFECTED SCANDINAVIAN TOURISTS
NORD J PSYCHIATRY·VOL 65·NO 1·2011 15
Katrina-displaced persons in shelters: A population-based cluster sample. Ann Emerg Med 2007 Jun 19; Epub ahead of print. Norris FH, Friedman MJ, Watson PJ, Byrne CM, Diaz E, Kaniasty 26. K. 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981 – 2001. Psychiatry 2002;65:207 – 39. Eriksson NG, Lundin T. Early traumatic stress reactions among 27. Swedish survivors of the m/s Estonia disaster. Br J Psychiatry 1996;169:713 – 6. Holen A. A longitudinal-study of the occurrence and persistence of 28. posttraumatic health-problems in disaster survivors. Stress Med 1991;7:11 – 7. Hull AM, Alexander DA, Klein S. Survivors of the Piper Alpha oil 29. platform disaster: Long-term follow-up study. Br J Psychiatry 2002;181:433 – 8. Turner SW, Thompson J, Rosser RM. The Kings Cross fi re: Psycho-30. logical reactions. J Traum Stress 1995;8:419 – 27. Beck JG, Grant DM, Read JP, Clapp JD, Coffey SF, Miller LM, 31. et al. The Impact of Event Scale-Revised: Psychometric properties in a sample of motor vehicle accident survivors. J Anxiety Disord 2008;22:187 – 98. Asukai N, Kato H, Kawamura N, Kim Y, Yamamoto K, Kishimoto J, 32. et al. Reliability and validity of the Japanese-language version of the impact of event scale-revised (IES-R-J): Four studies of different traumatic events. J Nerv Ment Dis 2002;190:175 – 82. Parker G. Cyclone Tracy and Darwin evacuees: On the restoration 33. of the species. Br J Psychiatry 1977;130:548 – 55. Steinglass P, Gerrity E. Natural disasters and posttraumatic-stress-34. disorder — Short-term versus long-term recovery in 2 disaster-affected communities. J Appl Soc Psychol 1990;20:1746 – 65. Carr VJ, Lewin TJ, Webster RA, Kenardy JA, Hazell PL, Carter GL. 35. Psychosocial sequelae of the 1989 Newcastle earthquake: II. Expo-sure and morbidity profi les during the fi rst 2 years post-disaster. Psychol Med 1997;27:167 – 78. Weisaeth L. Disasters: Psychological and psychiatric aspects. In: 36. Goldberger L, Breznitz S, editors. Handbook of stress: Theoretical and clinical aspects. New York: The Free Press; 1993. Guha-Sapir D, Hargitt D, Hoyois P. Thirty years of natural disasters 37. 1974 – 2003: The numbers. Louvain-la-Neuve, Belgium: Presses Uni-versitaires de Louvain; 2004. Hjemdal O. Follow up of tsunami victims: The role of the general 38. practitioners. Oslo: Norwegian Center for Violence and Traumatic Stress Studies; 2007. Report No. 1/2007.
Trond Heir, Ph.D., Norwegian Centre for Violence and Traumatic Stress Studies, University of Oslo, Oslo, Norway. Susanne Rosendal, M.D., Centre for Crisis and Disaster psychiatry, Copenhagen University Hospital, Rigshospitalet, Denmark. Kerstin Bergh-Johannesson, Psy.D., Department of Neuroscience, Psychiatry, Uller å ker, Uppsala University, Sweden. Per-Olof Michel, M.D., Ph.D., Department of Neuroscience, Psychiatry, Uller å ker, Uppsala University, Sweden. Erik L Mortensen, Cand.Psych., Department of Health Psychology, University of Copenhagen, Denmark. Lars Weis æ th, M.D., Ph.D., Norwegian Centre for Violence and Traumatic Stress Studies, University of Oslo, Oslo, Norway. Henrik S Andersen, M.D., Ph.D., Centre for Crisis and Disaster psychiatry, Copenhagen University Hospital, Rigshospitalet, Denmark. Christina M Hultman, Ph.D., Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden.
vanGriensven F, Chakkraband ML, Thienkrua W, Pengjuntr W, 6. Lopes CB, Tantipiwatanaskul P, et al. Mental health problems among adults in tsunami-affected areas in southern Thailand. JAMA 2006;296:537 – 48. Hansson K, Danielson M, Ekenberg L. A framework for evalua-7. tion of fl ood management strategies. J Environ Manage 2008;86:465 – 80. Fothergill A, Peek LA. Poverty and disasters in the United States: 8. A review of recent sociological fi ndings. Natural Hazards 2004;32:89 – 110. Hussain A, Weis æ th L, Heir T. Non-response to a population 9. based post disaster questionnaire study. J Trauma Stress 2009;22:324 – 328. Weiss D, Marmar C. The Impact of Event Scale — Revised. In: 10. Wilson J, Keane T, editors. Assessing psychological trauma and PTSD, 2nd edition. New York: Guildford Press; 2004. p. 168 – 89. Weathers F, Litz B, Herman D, Huska J, Keane T. The PTSD Check-11. list (PCL): Reliability, validity, and diagnostic utility. The Annual Convention of the International Society for Traumatic Stress Studies 1993; Paper presentation. Paunovi c12. ´ N, Ost LG. Psychometric properties of a Swedish transla-tion of the clinician-administered PTSD scale-diagnostic version. J Trauma Stress 2005;18:161 – 4. Johansen VA, Wahl AK, Eilertsen DE, Weisaeth L. Prevalence and 13. predictors of post-traumatic stress disorder (PTSD) in physically injured victims of non-domestic violence: A longitudinal study. Soc Psychiatry Psychiatr Epidemiol 2007;42:583 – 93. Clayer JR, Bookless-Pratz C, Harris RL. Some health consequences 14. of a natural disaster. Med J Aust 1985;143:182 – 4. Selly C, King E, Peveler R, Osola K, Martin N, Thompson C. Post-15. traumatic stress disorder symptoms and the Clapham rail accident. Br J Psychiatry 1997;171:478 – 82. Arata CM, Picou JS, Johnson GD, McNally TS. Coping with tech-16. nological disaster: An application of the conservation of resources model to the Exxon Valdez oil spill. J Traum Stress 2000;13:23 – 39. Weisaeth L. The stressors and the post-traumatic stress syndrome 17. after an industrial disaster. Acta Psychiatr Scand Suppl 1989;355:25 – 37. Sogaard AJ, Selmer R, Bjertness E, Thelle D. The Oslo Health 18. Study: The impact of self-selection in a large, population-based survey. Int J Equity Health 2004;3:3. Creamer M, Bell R, Failla S. Psychometric properties of the Impact 19. of Event Scale — Revised. Behav Res Ther 2003;41:1489 – 96. Mehnert A, Koch U. Prevalence of acute and post-traumatic stress 20. disorder and comorbid mental disorders in breast cancer patients during primary cancer care: A prospective study. Psychooncology 2007;16:181 – 8. Galea S, Nandi A, Vlahov D. The epidemiology of post-traumatic 21. stress disorder after disasters. Epidemiol Rev 2005;27:78 – 91. Verger P, Rotily M, Hunault C, Breno t J, Baruffol E, Bard D. 22. Assessment of exposure to a fl ood disaster in a mental-health study. J Expo Anal Environ Epidemiol 2003;13:436 – 42. Green BL, Lindy JD, Grace MC, Gleser GC, Leonard AC, Korol M, 23. et al. Buffalo Creek survivors in the second decade: Stability of stress symptoms. Am J Orthopsychiatry 1990;60:43 – 54. Abenhaim L, Dab W, Salmi LR. Study of civilian victims of terrorist 24. attacks (France 1982 – 1987). J Clin Epidemiol 1992;45:103 – 9. Greenough PG, Lappi MD, Hsu EB, Fink S, Hsieh YH, Vu A, 25. et al. Burden of disease and health status among Hurricane
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 03
/16/
13Fo
r pe
rson
al u
se o
nly.