Embed Size (px)
Citation preview
...........................................................................................................................
Insulin-like growth factor bindingprotein-1 in PCOS: a systematicreview and meta-analysisC.J. Kelly , S.R. Stenton , and H. Lashen *
Department of Reproductive and Developmental Medicine, University of Sheffield, New Jessop Wing, Sheffield S10 2SF, UK
*Correspondence address. Tel: +44-1142268317; Fax: +44-1142261074; E-mail: [email protected]
Submitted on July 12, 2009; resubmitted on May 19, 2010; accepted on May 28, 2010
table of contents
† Introduction† Methods
Selection of studiesStatistical analysis
† ResultsResults of the systematic literature reviewPrimary analysisSecondary analysesSubgroup analyses
† Discussion† Conclusion
background: Despite extensive research, the pathogenesis of polycystic ovary syndrome (PCOS) remains unclear. Putatively, an elev-ated circulating concentration of insulin inhibits the production of insulin-like growth factor binding protein-1 (IGFBP-1), thus increasing thelevel of free IGF-I in serum and stimulating ovarian androgen production. Decreased IGFBP-1 has been reported in PCOS and in obesity;however, there are inconsistencies in the evidence. This systematic review and meta-analysis aimed to determine whether IGFBP-1 isdecreased in PCOS when controlling for the influence of BMI.
methods: Articles published between 1988 and 2008 were searched using MEDLINE, PubMed, SCOPUS and Web of Knowledge.Unpublished literature, trials in progress, and recent reviews were also searched. Original articles were selected by two investigators. Tobe included, the study must have compared serum IGFBP-1 in two populations: either PCOS versus controls, or an overweight subgroupversus the normal weight subgroup in either population. From 617 identified articles, 12 were included in the meta-analysis. Data wereabstracted by two reviewers independently and standardized for errors.
results: The population difference is presented as the Weighted Mean Difference (95% CI). PCOS subjects had a significantly lowerserum concentrations of IGFBP-1 compared with controls [P , 0.00001; 236.6 (252.0, 221.2) mg/l]. Overweight PCOS subjects alsohad lower IGFBP-1 levels compared with normal weight PCOS subjects [P , 0.006; 230.6 (252.3, 28.8) mg/l]. No significant differencewas found between overweight PCOS patients and overweight controls [P ¼ 0.23; 25.1 (213.5, 3.2) mg/l] or between normal weightPCOS patients and normal weight controls [P ¼ 0.50; 23.8 (214.9, 7.3) mg/l]. Overweight controls had significantly lower IGFBP-1 con-centrations than normal weight controls [P ¼ 0.03; 218.0 (234.4, 2 1.5) mg/l].
conclusion: These data indicate that a decreased serum level of IGFBP-1 is unlikely to be a mechanism for ovarian hyperandrogenismin PCOS. BMI may be the major determinant of serum IGFBP-1.
Key words: polycystic ovary syndrome / insulin-like growth factor binding protein-1 / systematic review / meta-analysis / obesity
& The Author 2010. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved.For Permissions, please email: [email protected]
Human Reproduction Update, Vol.17, No.1 pp. 4–16, 2011
Advanced Access publication on July 15, 2010 doi:10.1093/humupd/dmq027
Dow
nloaded from https://academ
ic.oup.com/hum
upd/article-abstract/17/1/4/637745 by guest on 15 Novem
ber 2018

IntroductionPolycystic ovary syndrome (PCOS) is a heterogeneous disorder ofunknown aetiology. Characteristically, the spectrum of PCOS includesclinical and morphological ovarian features, intermittent or absentmenstrual cycles, and clinical or biochemical hyperandrogenism.Hyperandrogenism is widely believed to play a pivotal role in the defi-nition of PCOS despite the Rotterdam consensus (Azziz et al., 2006).
PCOS is believed to be strongly associated with insulin resistanceand hyperinsulinaemia (Dunaif, 1997), which has been shown insome studies to be independent of the obesity that is also prevalentamong PCOS women (Burghen et al., 1980; Dunaif et al., 1989).The evidence that insulin stimulates ovarian thecal and stromal andro-gen production in vitro (Barbieri et al., 1986; Bergh et al., 1993) and thedemonstration of a positive correlation between fasting insulin and cir-culating androgens (Burghen et al., 1980) gave rise to the hypothesisthat hyperinsulinaemia promotes hyperandrogenaemia in PCOS.This was supported clinically by the reported reduction in serum tes-tosterone and amelioration of hyperandrogenic symptoms afterinsulin-sensitizing therapy (Nestler and Jakubowicz, 1996).
It was proposed that insulin stimulates ovarian androgen synthesisthrough its interaction with the insulin-like growth factor (IGF)system and that IGF-I potentiates LH-stimulated ovarian androgen syn-thesis. The action of IGF-I action is modulated by the IGF-bindingprotein-1 (IGFBP-1; Rajaram et al., 1997), which has been reportedto correlate inversely with the serum level of free IGF-I (Thierry vanDessel et al., 1999). Insulin has also been shown to regulate theserum level of IGFBP-1 (Suikkari et al., 1988), decreasing its pro-duction by the liver (Brismar et al., 1994). Serum IGFBP-1 has beenfound to be decreased in women with PCOS (Conway et al., 1990;Iwashita et al., 1990; Thierry van Dessel et al., 1999). It was thereforehypothesized that hyperinsulinaemia in PCOS inhibits the productionof IGFBP-1, causing an increase in the level of free IGF-I in theserum and potentiating LH-stimulated androgen production.
The relationship between serum IGFBP-1, PCOS and BMI has beenthe focus of many studies. Several have reported that the serum levelof IGFBP-1 is significantly lower in PCOS women than in healthy(Pekonen et al., 1989; Conway et al., 1990; Morris and Falcone,1996; Thierry van Dessel et al., 1999) and anovulatory (Homburget al., 1992) control subjects. However, other studies have failed todemonstrate a significant difference in IGFBP-1 between the twogroups (Suikkari et al., 1991; Buyalos et al., 1995).
There is a strong inverse relationship between BMI and serumIGFBP-1 in the general population (Sandhu et al., 2004). This couldconfound the comparison of PCOS and non-PCOS yet obesewomen, and contribute towards discrepancies in the available evi-dence. Given the increased prevalence of overweight and obesity inPCOS (Pasquali and Casimirri, 1993), it is necessary to control forBMI in order to establish the independent effects of BMI and PCOS.This approach has been adopted by a number of studies (Buyaloset al., 1995; Morales et al., 1996; Morris and Falcone, 1996);however, there are various inconsistencies in the evidence.
Despite these inconsistencies in the literature there is a consensusthat serum IGFBP-1 is significantly lower in PCOS women (Poretskyet al., 1999; Wang and Wang, 2003) which suggests a role forIGFBP-1 in the pathogenesis of PCOS. However, many have arrivedat this conclusion based on selective evidence obtained from a
group of studies which are generally of small sample size, in diversepopulations and using different methodologies. It is possible thatthese factors have contributed to the discrepancies noted or con-founded the results.
In light of these points, a definitive conclusion on the role ofIGFBP-1 in PCOS has yet to be reached. This highlights the needfor an investigation into the serum level of IGFBP-1 in PCOS andcontrol women, controlling for the influence of BMI.
To date, meta-analyses have largely been used for dichotomousdata, and to pool the results of interventional trials. However, themethod also lends itself to continuous data. In order to determinethe verity of the current consensus and address the impact of BMIon IGFBP-1, we carried out a systematic review and meta-analysisof all the studies that compared the serum level of IGFBP-1 in aPCOS and control population. Further, we investigated the influenceof the assay used and of various population differences.
MethodsThe systematic review and meta-analysis were conducted according to adetailed protocol. Our null hypothesis was that serum IGFBP-1 was notsignificantly different in PCOS compared with control subjects. A second-ary null hypothesis was that serum IGFBP-1 is not significantly different inoverweight and obese subjects compared with normal weight subjects.
After inspection of the data, we hypothesized that population differ-ences affect serum IGFBP-1 and contribute towards the heterogeneitybetween studies. This factor was therefore investigated by several posthoc analyses.
Selection of studiesWe searched the following electronic databases: MEDLINE via Ovid SP(1950 to October 2008), PubMed, SCOPUS and Web of Knowledge.
Further, Google Scholar was used to maximize identification of relevantstudies by free-text searching. Unpublished literature was searched usingthe System for Information on Grey Literature in Europe (SIGLE). Relevanttrials in progress were investigated on the UK Clinical Research Networkportfolio database (UKCRN). The reference sections of five recent reviewarticles on IGFBP-1 were hand-searched (Poretsky, 1991; Poretsky et al.,1999; Lee et al., 1997; Fowler et al., 2000; Wang and Wang, 2003).Searches were limited to literature published during the past 20 years(1988–2008).
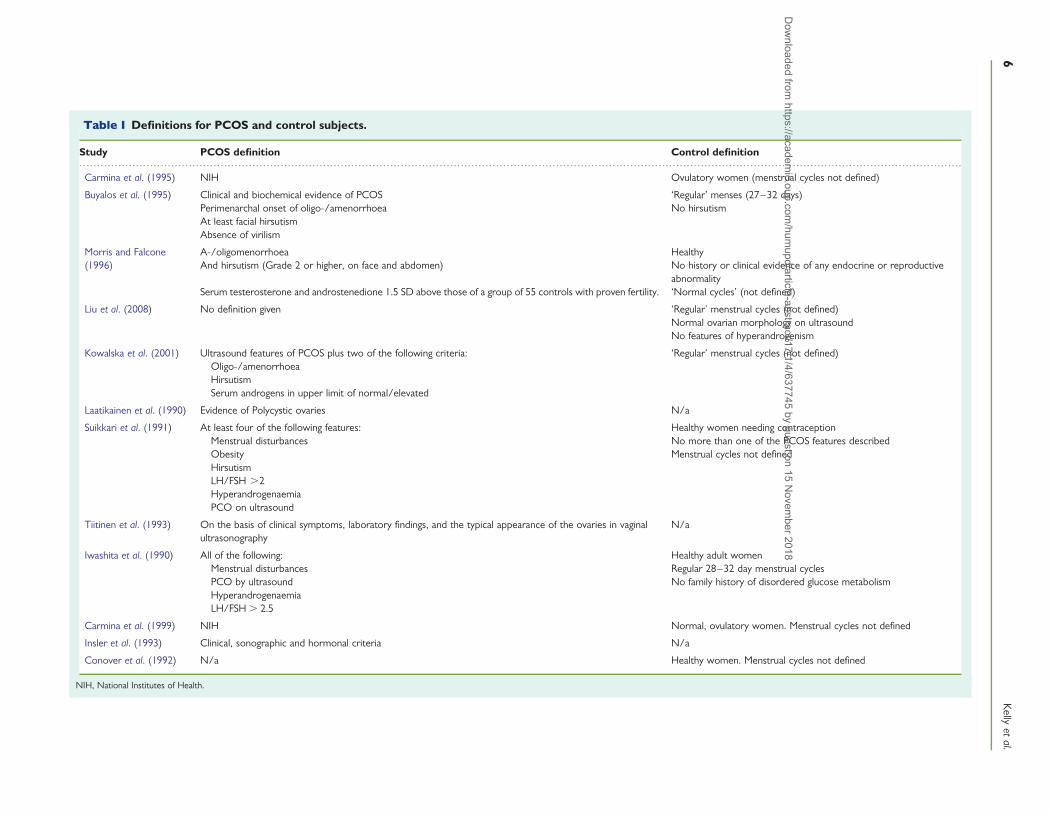
The search terms were ‘PCOS’, ‘IGF-I’ and ‘IGFBP-1’, including all acro-nyms and synonyms. Wild cards were used to allow for variation in punc-tuation and suffixes. We were unable to include articles that were notwritten in English due to cost limitations. We included studies thatmeasured fasting serum IGFBP-1 levels in PCOS women and non-PCOScontrols, or that compared overweight and normal weight subgroups ofeither population. We accepted PCOS women on the basis of a clinicaldiagnosis (Table I). Studies were excluded if subjects were post-menopausal. Control subjects were defined as non-PCOS. The definitionof ‘control’ used in each study is described in Table I. Subjects were sub-grouped according to their BMI. Normal BMI status was defined as≤25 kg/m2. Overweight was defined as a BMI . 25 kg/m2.
Articles were excluded from the analysis if it was stated that subjectswere taking hormone therapy or drugs known to affect carbohydratemetabolism. If it was explicit that subjects were tested in a non-fastingstate, the study was excluded from the analysis. In the absence of specificmention of fasting, a measurement of ‘fasting glucose/insulin’ or descrip-tion of a glucose tolerance test was accepted as proof of an overnightfast. Where either fasting or drugs were not mentioned, the study was
IGFBP-1 in PCOS: review and meta-analysis 5D
ownloaded from
https://academic.oup.com
/humupd/article-abstract/17/1/4/637745 by guest on 15 N
ovember 2018
..........................................................................................................................................................................................................................................................
Table I Definitions for PCOS and control subjects.
Study PCOS definition Control definition
Carmina et al. (1995) NIH Ovulatory women (menstrual cycles not defined)
Buyalos et al. (1995) Clinical and biochemical evidence of PCOS ‘Regular’ menses (27–32 days)Perimenarchal onset of oligo-/amenorrhoea No hirsutismAt least facial hirsutismAbsence of virilism
Morris and Falcone(1996)
A-/oligomenorrhoea HealthyAnd hirsutism (Grade 2 or higher, on face and abdomen) No history or clinical evidence of any endocrine or reproductive
abnormalitySerum testerosterone and androstenedione 1.5 SD above those of a group of 55 controls with proven fertility. ‘Normal cycles’ (not defined)
Liu et al. (2008) No definition given ‘Regular’ menstrual cycles (not defined)Normal ovarian morphology on ultrasoundNo features of hyperandrogenism
Kowalska et al. (2001) Ultrasound features of PCOS plus two of the following criteria: ‘Regular’ menstrual cycles (not defined)Oligo-/amenorrhoeaHirsutismSerum androgens in upper limit of normal/elevated
Laatikainen et al. (1990) Evidence of Polycystic ovaries N/a
Suikkari et al. (1991) At least four of the following features: Healthy women needing contraceptionMenstrual disturbances No more than one of the PCOS features describedObesity Menstrual cycles not definedHirsutismLH/FSH .2HyperandrogenaemiaPCO on ultrasound
Tiitinen et al. (1993) On the basis of clinical symptoms, laboratory findings, and the typical appearance of the ovaries in vaginalultrasonography
N/a
Iwashita et al. (1990) All of the following: Healthy adult womenMenstrual disturbances Regular 28–32 day menstrual cyclesPCO by ultrasound No family history of disordered glucose metabolismHyperandrogenaemiaLH/FSH . 2.5
Carmina et al. (1999) NIH Normal, ovulatory women. Menstrual cycles not defined
Insler et al. (1993) Clinical, sonographic and hormonal criteria N/a
Conover et al. (1992) N/a Healthy women. Menstrual cycles not defined
NIH, National Institutes of Health.
6K
ellyet
al.
Dow
nloaded from https://academ
ic.oup.com/hum
upd/article-abstract/17/1/4/637745 by guest on 15 Novem
ber 2018

included on the basis of assumption. IGFBP-1 mean values which were anaverage of multiple non-fasting samples (e.g. over a 24-h period) were notincluded.
All potential articles were first screened by their title and abstract byeither researcher (C.J.K. and S.R.S.) independently. Articles which wereclearly ineligible were discarded, and full text articles were obtained forthose studies fulfilling the inclusion criteria. These were screened byboth researchers to determine final eligibility for the study, with any dis-agreements resolved by a third researcher (H.L.). Data abstraction wascarried out by CJ.K. and S.R.S. independently and was standardized toeliminate errors.
Statistical analysisStatistical analysis was carried out using Review Manager 4.2 and SPSSVersion 15.0. The primary analysis was the meta-analysis of WeightedMean Differences (WMDs) for the studies comparing PCOS and controlsubjects. In the secondary analyses, we compared the BMI subgroups ofeach population: overweight PCOS versus Normal weight PCOS, Over-weight PCOS versus Overweight Control, Normal weight PCOS versusnormal weight control and Overweight control versus normal weightControl.
Where standard deviations were missing from the study report, theywere calculated from the standard error according to the formulae setout in the Cochrane Reviewers’ Handbook (Higgins, 2008).
Firstly, individual study data were combined using the fixed effectinverse variance model. There was significant heterogeneity in many ofthe analyses. This is unsurprising since the included studies investigatedethnically diverse populations and used different assays. Heterogeneousresults were then analysed by the random-effects model (Higgins, 2008).
Heterogeneity was examined by inspection of the forest plots and theresult of a x2 test. A P-value of ,0.10 was considered significant evidencefor heterogeneity. Heterogeneity was also investigated by subgroup analy-sis, where studies were grouped according to the IGFBP-1 assay used.Additionally, a sensitivity analysis was performed for each comparison.Each study was excluded in turn and the meta-analysis repeated inorder to evaluate the influence of each study on the summary WMD.
Within the text, the data are presented as the WMD (95% confidenceinterval).
Results
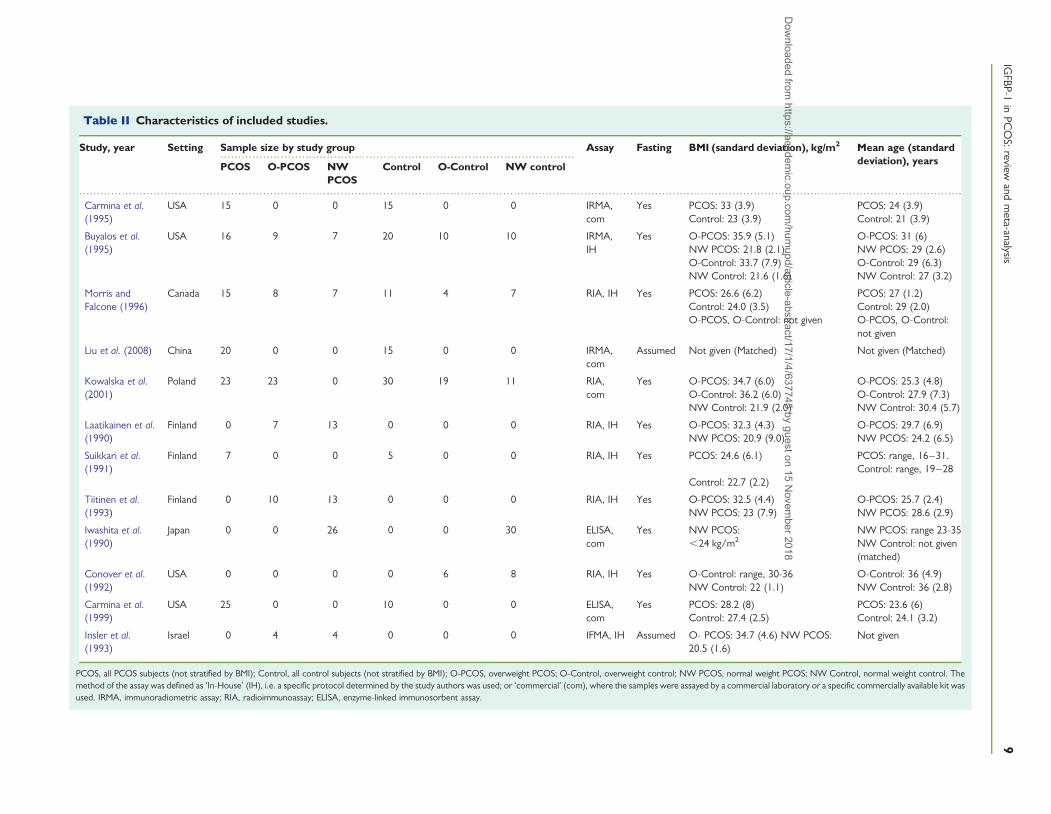
Results of the systematic literature reviewThe systematic retrieval process to identify eligible studies is summar-ized in Fig. 1. The characteristics of the included studies and their sub-jects are summarized in Table II.
Primary analysisComparison 1: PCOS versus controlFive studies compared the serum IGFBP-1 levels in a PCOS and acontrol population (Fig. 2; Suikkari et al., 1991; Carmina et al., 1995;Morris and Falcone, 1996; Carmina et al., 1999; Liu et al., 2008).The mean (SD) IGFBP-1 level in the PCOS populations ranged from6.4 mg/l (7.1) to 26.9 mg/l (16.3). In the control populations, therange was 26.1 mg/l (6.2) to 124.0 (38.0). With the exception ofSuikkari et al. (1991), all studies showed a significant mean differencebetween the IGFBP-1 levels in PCOS and control subjects. Thesummary WMD (95% CI) was 236.6 mg/l (252.0, 221.2). Serum
IGFBP-1 was significantly lower in PCOS subjects than in control sub-jects (P , 0.00001).
There was statistically significant heterogeneity between thesestudies (x2¼ 86.8, df ¼ 4, P , 0.00001, I2¼ 95.4%). In the sensitivityanalysis, the WMDs (95% CI) ranged from 224.4 (237.1, 211.7) to244.9 (269.2, 220.5) and the upper limits of the confidence inter-vals never crossed zero. This showed that the exclusion of any onestudy did not affect the overall direction of the result.
Secondary analysesComparison 2: overweight PCOS versus normal weight PCOSThere were five studies which compared the serum IGFBP-1 levels inan overweight PCOS and a normal weight PCOS population (Fig. 3;Laatikainen et al., 1990; Insler et al., 1993; Tiitinen et al., 1993;Buyalos et al., 1995; Morris and Falcone, 1996). In the overweightPCOS population, the IGFBP-1 mean (SD) ranged from 2.2 mg/l(1.8) to 24.3 mg/l (17.5). There was a wider range of meanIGFBP-1 values among the Normal Weight PCOS subjects; from6.2 mg/l (5.3) to 70.8 mg/l (41.5). Four of the five included studiesshowed IGFBP-1 to be significantly lower in the overweight subjectsin comparison to the controls (Laatikainen et al., 1990; Insler et al.,1993; Tiitinen et al., 1993; Morris and Falcone, 1996), whereasBuyalos et al. (1995) indicated that there was no significant differencebetween the two populations. This discrepancy may be explained bythe anomalously low mean value for IGFBP-1 in Buyalos’ normalweight PCOS population.
Meta-analysis of all trials confirmed that IGFBP-1 is significantlylower in overweight PCOS than in normal weight PCOS women(P ¼ 0.006). The summary WMD (95% CI) was 230.6 mg/l(252.3, 28.8).
There was significant heterogeneity between these studies (x2 ¼
54.3, df ¼ 4, P , 0.00001, I2¼ 92.6%). A sensitivity analysis wasundertaken. The WMDs (95% CI) ranged from 227.2 mg/l(249.6, 24.7) to 238.6 mg/l (247.0, 230.2) and the upper limitsof the confidence intervals never crossed zero.
Comparison 3: overweight PCOS versus overweight controlThere were three studies which compared overweight PCOS andcontrol populations (Fig. 4; Buyalos et al., 1995; Morris and Falcone,1996; Kowalska et al., 2001). In the overweight PCOS subjects, themean (SD) IGFBP-1 ranged from 2.2 mg/l (1.8) to 13.7 mg/l (5.4).Among the overweight control population the range was muchwider; 1.8 mg/l (1.3) to 50.6 mg/l (21.0). Kowalska et al. (2001) andBuyalos et al. (1995) found no significant difference between thetwo populations; WMD (95% CI) ¼ 22.3 mg/l (27.4, 2.8) and0.4 mg/l (21.0, 1.8), respectively. Conversely, Morris and Falcone(1996) reported that IGFBP-1 was significantly greater in overweightcontrol subjects than in overweight PCOS subjects, WMD (95%CI)¼ 236.9 ( 257.8, 215.99), P , 0.01.
Meta-analysis showed no significant difference between the IGFBP-1level in overweight PCOS subjects compared with overweight controlsubjects (P ¼ 0.23). The summary WMD (95% CI) was 25.1 mg/l(213.5, 3.2).
The test for heterogeneity was significant (x2¼ 13.1, df ¼ 2, P ¼0.001, I2 ¼ 84.7%). In the sensitivity analysis the WMDs (95% CI)ranged from 0.2 (21.2, 1.6) to 218.1 (251.8, 15.7). The sensitivity
IGFBP-1 in PCOS: review and meta-analysis 7D
ownloaded from
https://academic.oup.com
/humupd/article-abstract/17/1/4/637745 by guest on 15 N
ovember 2018

analyses confirmed that IGFBP-1 is not significantly different in over-weight PCOS and overweight control subjects.
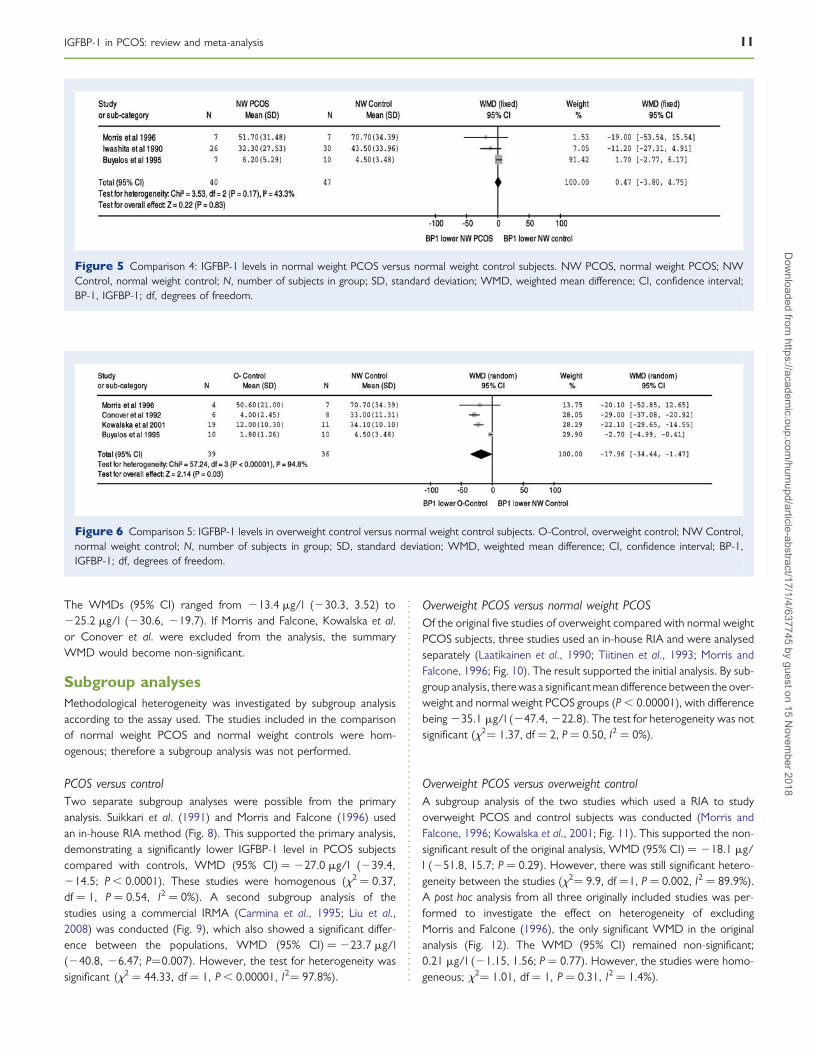
Comparison 4: normal weight PCOS versus normal weight controlThere were three studies which compared the serum IGFBP-1 levels inNormal Weight PCOS and Normal Weight control populations (Fig. 5;Iwashita et al., 1990; Buyalos et al., 1995; Morris and Falcone, 1996). Themean IGFBP-1 value (SD) in the Normal Weight PCOS populationranged from 6.2 mg/l (5.3) to 51.7 mg/l (31.5). There was also a widerange in the Normal Weight controls: 4.5 mg/l (3.5) to 70.7 mg/l(34.4). None of the included studies found a significant difference inmean IGFBP-1 between the two populations. This was reflected bythe summary WMD (95% CI): 0.47 mg/l (23.8, 4.8). There was no
significant difference between normal weight PCOS and normalweight control subjects (P ¼ 0.83). These studies were shown to behomogenous (x2 ¼ 3.53, df ¼ 2, P ¼ 0.17, I2¼ 43.3%).
Comparison 5: overweight control versus normal weight controlThere were four studies which compared overweight and normalweight control populations (Fig. 6; Conover et al., 1992; Buyaloset al., 1995; Morris and Falcone, 1996; Kowalska et al., 2001). Themean IGFBP-1 values (SD) were wide-ranging for both overweightcontrol and normal weight control subjects; 1.8 mg/l (1.3) to50.6 mg/l (21.0) and 4.5 mg/l (3.5) to 70.7 mg/l (34.4), respectively.IGFBP-1 was significantly lower in overweight controls in three ofthe studies (Conover et al., 1992; Buyalos et al., 1995; Kowalska
Figure 1 Summary of the systematic retrieval process. A literature search was conducted using a variety of sources. These were primarily screenedby title, which identified 617 articles. Of these, 12 were deemed suitable to include in the meta-analysis based on their adherence to the inclusioncriteria. The numbers in parentheses represent the number of studies included in each comparison. Articles were sub-grouped according to BMI andthe assay method used. RIA, radioimmunoassay; IRMA, immunoradiometric assay; IH, in-house assay; Com, commercial assay.
8 Kelly et al.
Dow
nloaded from https://academ
ic.oup.com/hum
upd/article-abstract/17/1/4/637745 by guest on 15 Novem
ber 2018
....................................................................................................
..........................................................................................................................................................................................................................................................
Table II Characteristics of included studies.
Study, year Setting Sample size by study group Assay Fasting BMI (sandard deviation), kg/m2 Mean age (standarddeviation), yearsPCOS O-PCOS NW
PCOSControl O-Control NW control
Carmina et al.(1995)
USA 15 0 0 15 0 0 IRMA,com
Yes PCOS: 33 (3.9) PCOS: 24 (3.9)Control: 23 (3.9) Control: 21 (3.9)
Buyalos et al.(1995)
USA 16 9 7 20 10 10 IRMA,IH
Yes O-PCOS: 35.9 (5.1) O-PCOS: 31 (6)NW PCOS: 21.8 (2.1) NW PCOS: 29 (2.6)O-Control: 33.7 (7.9) O-Control: 29 (6.3)NW Control: 21.6 (1.6) NW Control: 27 (3.2)
Morris andFalcone (1996)
Canada 15 8 7 11 4 7 RIA, IH Yes PCOS: 26.6 (6.2) PCOS: 27 (1.2)Control: 24.0 (3.5) Control: 29 (2.0)O-PCOS, O-Control: not given O-PCOS, O-Control:
not given
Liu et al. (2008) China 20 0 0 15 0 0 IRMA,com
Assumed Not given (Matched) Not given (Matched)
Kowalska et al.(2001)
Poland 23 23 0 30 19 11 RIA,com
Yes O-PCOS: 34.7 (6.0) O-PCOS: 25.3 (4.8)O-Control: 36.2 (6.0) O-Control: 27.9 (7.3)NW Control: 21.9 (2.0) NW Control: 30.4 (5.7)
Laatikainen et al.(1990)
Finland 0 7 13 0 0 0 RIA, IH Yes O-PCOS: 32.3 (4.3) O-PCOS: 29.7 (6.9)NW PCOS: 20.9 (9.0) NW PCOS: 24.2 (6.5)
Suikkari et al.(1991)
Finland 7 0 0 5 0 0 RIA, IH Yes PCOS: 24.6 (6.1) PCOS: range, 16–31.Control: range, 19–28
Control: 22.7 (2.2)
Tiitinen et al.(1993)
Finland 0 10 13 0 0 0 RIA, IH Yes O-PCOS: 32.5 (4.4) O-PCOS: 25.7 (2.4)NW PCOS: 23 (7.9) NW PCOS: 28.6 (2.9)
Iwashita et al.(1990)
Japan 0 0 26 0 0 30 ELISA,com
Yes NW PCOS: NW PCOS: range 23-35,24 kg/m2 NW Control: not given
(matched)
Conover et al.(1992)
USA 0 0 0 0 6 8 RIA, IH Yes O-Control: range, 30-36 O-Control: 36 (4.9)NW Control: 22 (1.1) NW Control: 36 (2.8)
Carmina et al.(1999)
USA 25 0 0 10 0 0 ELISA,com
Yes PCOS: 28.2 (8) PCOS: 23.6 (6)Control: 27.4 (2.5) Control: 24.1 (3.2)
Insler et al.(1993)
Israel 0 4 4 0 0 0 IFMA, IH Assumed O- PCOS: 34.7 (4.6) NW PCOS:20.5 (1.6)
Not given
PCOS, all PCOS subjects (not stratified by BMI); Control, all control subjects (not stratified by BMI); O-PCOS, overweight PCOS; O-Control, overweight control; NW PCOS, normal weight PCOS; NW Control, normal weight control. Themethod of the assay was defined as ‘In-House’ (IH), i.e. a specific protocol determined by the study authors was used; or ‘commercial’ (com), where the samples were assayed by a commercial laboratory or a specific commercially available kit wasused. IRMA, immunoradiometric assay; RIA, radioimmunoassay; ELISA, enzyme-linked immunosorbent assay.
IGFBP-1
inPC
OS:
reviewand
meta-analysis
9
Dow
nloaded from https://academ
ic.oup.com/hum
upd/article-abstract/17/1/4/637745 by guest on 15 Novem
ber 2018

et al., 2001), while Morris and Falcone (1996) found no significantdifference between the two populations [WMD (95% CI) ¼ 220.1(252.9, 12.7)]. From the meta-analysis, the summary WMD (95%CI) was 218.0 mg/l (234.4, 21.5), demonstrating that IGFBP-1 is
significantly lower in overweight control subjects compared withnormal weight controls (P ¼ 0.03).
The test for heterogeneity was significant (x2¼ 57.2, df ¼ 3, P ,
0.00001, I2¼ 94.8%). A sensitivity analysis was undertaken (Fig. 7).
Figure 2 Comparison 1: IGFBP-1 levels in PCOS versus control subjects. N, number of subjects in group; SD, standard deviation; WMD, weightedmean difference, CI, confidence interval; BP-1, IGFBP-1, df, degrees of freedom.
Figure 3 Comparison 2: IGFBP-1 levels in overweight PCOS versus normal weight PCOS subjects. O-PCOS, overweight PCOS; NW PCOS,normal weight PCOS; N, number of subjects in group; SD, standard deviation; WMD, weighted mean difference; CI, confidence interval; BP-1,IGFBP-1; df, degrees of freedom.
Figure 4 Comparison 3: IGFBP-1 levels in overweight PCOS versus overweight control subjects. O-PCOS, overweight PCOS; O-Control, over-weight control; N, number of subjects in group; SD, standard deviation; WMD, weighted mean difference; CI, confidence interval; BP-1, IGFBP-1;df, degrees of freedom.
10 Kelly et al.
Dow
nloaded from https://academ
ic.oup.com/hum
upd/article-abstract/17/1/4/637745 by guest on 15 Novem
ber 2018
The WMDs (95% CI) ranged from 213.4 mg/l (230.3, 3.52) to225.2 mg/l (230.6, 219.7). If Morris and Falcone, Kowalska et al.or Conover et al. were excluded from the analysis, the summaryWMD would become non-significant.
Subgroup analysesMethodological heterogeneity was investigated by subgroup analysisaccording to the assay used. The studies included in the comparisonof normal weight PCOS and normal weight controls were hom-ogenous; therefore a subgroup analysis was not performed.
PCOS versus controlTwo separate subgroup analyses were possible from the primaryanalysis. Suikkari et al. (1991) and Morris and Falcone (1996) usedan in-house RIA method (Fig. 8). This supported the primary analysis,demonstrating a significantly lower IGFBP-1 level in PCOS subjectscompared with controls, WMD (95% CI) ¼ 227.0 mg/l (239.4,214.5; P , 0.0001). These studies were homogenous (x2 ¼ 0.37,df ¼ 1, P ¼ 0.54, I2 ¼ 0%). A second subgroup analysis of thestudies using a commercial IRMA (Carmina et al., 1995; Liu et al.,2008) was conducted (Fig. 9), which also showed a significant differ-ence between the populations, WMD (95% CI) ¼ 223.7 mg/l(240.8, 26.47; P¼0.007). However, the test for heterogeneity wassignificant (x2 ¼ 44.33, df ¼ 1, P , 0.00001, I2¼ 97.8%).
Overweight PCOS versus normal weight PCOSOf the original five studies of overweight compared with normal weightPCOS subjects, three studies used an in-house RIA and were analysedseparately (Laatikainen et al., 1990; Tiitinen et al., 1993; Morris andFalcone, 1996; Fig. 10). The result supported the initial analysis. By sub-group analysis, there was a significant mean difference between the over-weight and normal weight PCOS groups (P , 0.00001), with differencebeing 235.1 mg/l (247.4, 222.8). The test for heterogeneity was notsignificant (x2¼ 1.37, df ¼ 2, P ¼ 0.50, I2 ¼ 0%).
Overweight PCOS versus overweight controlA subgroup analysis of the two studies which used a RIA to studyoverweight PCOS and control subjects was conducted (Morris andFalcone, 1996; Kowalska et al., 2001; Fig. 11). This supported the non-significant result of the original analysis, WMD (95% CI) ¼ 218.1 mg/l (251.8, 15.7; P ¼ 0.29). However, there was still significant hetero-geneity between the studies (x2¼ 9.9, df ¼1, P ¼ 0.002, I2 ¼ 89.9%).A post hoc analysis from all three originally included studies was per-formed to investigate the effect on heterogeneity of excludingMorris and Falcone (1996), the only significant WMD in the originalanalysis (Fig. 12). The WMD (95% CI) remained non-significant;0.21 mg/l (21.15, 1.56; P ¼ 0.77). However, the studies were homo-geneous; x2¼ 1.01, df ¼ 1, P ¼ 0.31, I2 ¼ 1.4%).
Figure 5 Comparison 4: IGFBP-1 levels in normal weight PCOS versus normal weight control subjects. NW PCOS, normal weight PCOS; NWControl, normal weight control; N, number of subjects in group; SD, standard deviation; WMD, weighted mean difference; CI, confidence interval;BP-1, IGFBP-1; df, degrees of freedom.
Figure 6 Comparison 5: IGFBP-1 levels in overweight control versus normal weight control subjects. O-Control, overweight control; NW Control,normal weight control; N, number of subjects in group; SD, standard deviation; WMD, weighted mean difference; CI, confidence interval; BP-1,IGFBP-1; df, degrees of freedom.
IGFBP-1 in PCOS: review and meta-analysis 11D
ownloaded from
https://academic.oup.com
/humupd/article-abstract/17/1/4/637745 by guest on 15 N
ovember 2018

Figure 7 Sensitivity analysis: IGFBP-1 levels in overweight control versus normal weight control subjects. WMD, weighted mean difference.
Figure 8 IGFBP-1 levels in PCOS versus control subjects: in-house RIA method. N, number of subjects in group; SD, standard deviation; WMD,weighted mean difference; CI, confidence interval; BP-1, IGFBP-1; df, degrees of freedom.
Figure 9 IGFBP-1 levels in PCOS versus control subjects: commercial IRMA method. BP-1, IGFBP-1; N, number of subjects in group; SD, standarddeviation; WMD, weighted mean difference; CI, confidence interval; BP-1, IGFBP-1; df, degrees of freedom.
12 Kelly et al.
Dow
nloaded from https://academ
ic.oup.com/hum
upd/article-abstract/17/1/4/637745 by guest on 15 Novem
ber 2018

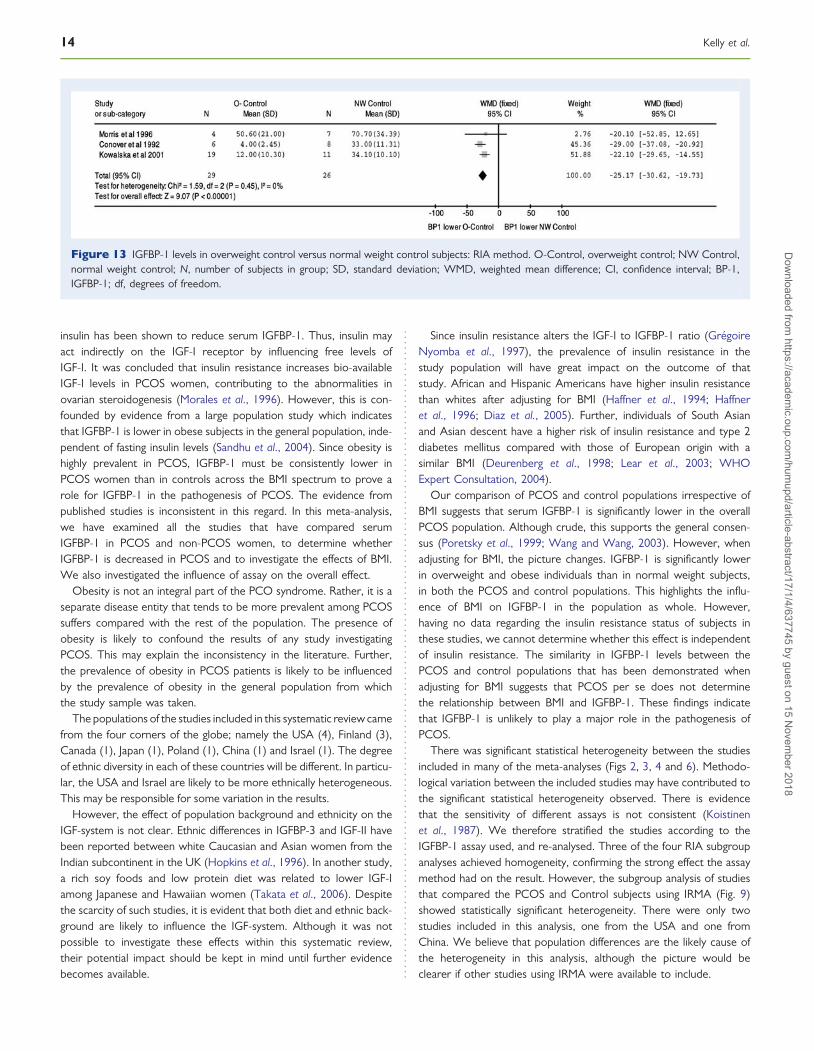
Overweight control versus normal weight controlA subgroup analysis of the three studies which used an RIA assay tostudy overweight and normal weight contros was conducted(Conover et al., 1992, Morris and Falcone, 1996; Kowalska et al.,2001; Fig. 13). This supported the original analysis, indicating thatIGFBP-1 is significantly lower among overweight controls, WMD(95% CI) ¼ 225.2 mg/l (230.6, 219.7). The test for heterogeneitywas non-significant (x2¼ 1.59, df ¼ 2, P ¼ 0.45, I2 ¼ 0%).
DiscussionThe mechanism for excess androgen production in PCOS is yet to befully elucidated. One theory is that an elevated serum concentration ofinsulin could act directly via the IGF-I receptor to increase androgenproduction (Barbieri and Rayan, 1983). However, the IGF-I receptorhas a greater affinity for IGF-I than for insulin (Froesch and Zapf,1985). In healthy individuals (Gregoire Nyomba et al., 1997) and indiabetic patients (Brismar and Hall, 1993), the administration of
Figure 10 IGFBP-1 levels in overweight PCOS versus normal weight PCOS subjects: in-house RIA method. O-PCOS, overweight PCOS; NWPCOS, normal weight PCOS; N, number of subjects in group; SD, standard deviation; WMD, weighted mean difference; CI, confidence interval;BP-1, IGFBP-1; df, degrees of freedom.
Figure 11 IGFBP-1 levels in overweight PCOS versus overweight control subjects: RIA method. O-PCOS, overweight PCOS; O-Control, over-weight control; N, number of subjects in group; SD, standard deviation; WMD, weighted mean difference; CI, confidence interval; BP-1, IGFBP-1;df, degrees of freedom.
Figure 12 IGFBP-1 levels in overweight PCOS versus overweight control subjects: post hoc analysis excluding Morris and Falcone. O-PCOS, over-weight PCOS. O-Control, overweight control; N, number of subjects in group; SD, standard deviation; WMD, weighted mean difference;CI, confidence interval; BP-1, IGFBP-1; df, degrees of freedom.
IGFBP-1 in PCOS: review and meta-analysis 13D
ownloaded from
https://academic.oup.com
/humupd/article-abstract/17/1/4/637745 by guest on 15 N
ovember 2018
insulin has been shown to reduce serum IGFBP-1. Thus, insulin mayact indirectly on the IGF-I receptor by influencing free levels ofIGF-I. It was concluded that insulin resistance increases bio-availableIGF-I levels in PCOS women, contributing to the abnormalities inovarian steroidogenesis (Morales et al., 1996). However, this is con-founded by evidence from a large population study which indicatesthat IGFBP-1 is lower in obese subjects in the general population, inde-pendent of fasting insulin levels (Sandhu et al., 2004). Since obesity ishighly prevalent in PCOS, IGFBP-1 must be consistently lower inPCOS women than in controls across the BMI spectrum to prove arole for IGFBP-1 in the pathogenesis of PCOS. The evidence frompublished studies is inconsistent in this regard. In this meta-analysis,we have examined all the studies that have compared serumIGFBP-1 in PCOS and non-PCOS women, to determine whetherIGFBP-1 is decreased in PCOS and to investigate the effects of BMI.We also investigated the influence of assay on the overall effect.
Obesity is not an integral part of the PCO syndrome. Rather, it is aseparate disease entity that tends to be more prevalent among PCOSsuffers compared with the rest of the population. The presence ofobesity is likely to confound the results of any study investigatingPCOS. This may explain the inconsistency in the literature. Further,the prevalence of obesity in PCOS patients is likely to be influencedby the prevalence of obesity in the general population from whichthe study sample was taken.
The populations of the studies included in this systematic review camefrom the four corners of the globe; namely the USA (4), Finland (3),Canada (1), Japan (1), Poland (1), China (1) and Israel (1). The degreeof ethnic diversity in each of these countries will be different. In particu-lar, the USA and Israel are likely to be more ethnically heterogeneous.This may be responsible for some variation in the results.
However, the effect of population background and ethnicity on theIGF-system is not clear. Ethnic differences in IGFBP-3 and IGF-II havebeen reported between white Caucasian and Asian women from theIndian subcontinent in the UK (Hopkins et al., 1996). In another study,a rich soy foods and low protein diet was related to lower IGF-Iamong Japanese and Hawaiian women (Takata et al., 2006). Despitethe scarcity of such studies, it is evident that both diet and ethnic back-ground are likely to influence the IGF-system. Although it was notpossible to investigate these effects within this systematic review,their potential impact should be kept in mind until further evidencebecomes available.
Since insulin resistance alters the IGF-I to IGFBP-1 ratio (GregoireNyomba et al., 1997), the prevalence of insulin resistance in thestudy population will have great impact on the outcome of thatstudy. African and Hispanic Americans have higher insulin resistancethan whites after adjusting for BMI (Haffner et al., 1994; Haffneret al., 1996; Diaz et al., 2005). Further, individuals of South Asianand Asian descent have a higher risk of insulin resistance and type 2diabetes mellitus compared with those of European origin with asimilar BMI (Deurenberg et al., 1998; Lear et al., 2003; WHOExpert Consultation, 2004).
Our comparison of PCOS and control populations irrespective ofBMI suggests that serum IGFBP-1 is significantly lower in the overallPCOS population. Although crude, this supports the general consen-sus (Poretsky et al., 1999; Wang and Wang, 2003). However, whenadjusting for BMI, the picture changes. IGFBP-1 is significantly lowerin overweight and obese individuals than in normal weight subjects,in both the PCOS and control populations. This highlights the influ-ence of BMI on IGFBP-1 in the population as whole. However,having no data regarding the insulin resistance status of subjects inthese studies, we cannot determine whether this effect is independentof insulin resistance. The similarity in IGFBP-1 levels between thePCOS and control populations that has been demonstrated whenadjusting for BMI suggests that PCOS per se does not determinethe relationship between BMI and IGFBP-1. These findings indicatethat IGFBP-1 is unlikely to play a major role in the pathogenesis ofPCOS.
There was significant statistical heterogeneity between the studiesincluded in many of the meta-analyses (Figs 2, 3, 4 and 6). Methodo-logical variation between the included studies may have contributed tothe significant statistical heterogeneity observed. There is evidencethat the sensitivity of different assays is not consistent (Koistinenet al., 1987). We therefore stratified the studies according to theIGFBP-1 assay used, and re-analysed. Three of the four RIA subgroupanalyses achieved homogeneity, confirming the strong effect the assaymethod had on the result. However, the subgroup analysis of studiesthat compared the PCOS and Control subjects using IRMA (Fig. 9)showed statistically significant heterogeneity. There were only twostudies included in this analysis, one from the USA and one fromChina. We believe that population differences are the likely cause ofthe heterogeneity in this analysis, although the picture would beclearer if other studies using IRMA were available to include.
Figure 13 IGFBP-1 levels in overweight control versus normal weight control subjects: RIA method. O-Control, overweight control; NW Control,normal weight control; N, number of subjects in group; SD, standard deviation; WMD, weighted mean difference; CI, confidence interval; BP-1,IGFBP-1; df, degrees of freedom.
14 Kelly et al.
Dow
nloaded from https://academ
ic.oup.com/hum
upd/article-abstract/17/1/4/637745 by guest on 15 Novem
ber 2018

The diagnostic criteria for PCOS are another cause of the lack ofconsistency in the literature. Prior to the Rotterdam criteria (Rotter-dam ESHRE/ASRM, 2004), there had been two different sets of cri-teria upon which the diagnosis of PCOS was made, the NIH(Zawadzki and Dunaif, 1992) and the European criteria (Adamset al., 1985). The formerly accepted hyperandrogenism and oligo/anovulation as the main criteria for the diagnosis whereas the latterhad the radiological morphological appearance of the ovaries as man-datory to the diagnosis. Neither set of criteria were deemed adequate,hence the Rotterdam consensus. However, even the Rotterdam con-sensus has been the subject of criticism; mainly from those whobelieve that hyperandrogenism should be the cornerstone of PCOSdiagnosis (Azziz et al., 2006). Several subsets or phenotypes ofPCOS have emerged as a result of the introduction of the Rotterdamcriteria (Welt et al., 2006). Given such disagreement, the variation inPCOS definitions is likely to be a contributor to the heterogeneity inour meta-analyses.
ConclusionThis meta-analysis suggests that a decreased serum level of IGFBP-1does not have a role in the pathogenesis of PCOS but is likely toresult from the high prevalence of obesity in the PCOS population.However, we are limited by the retrospective nature of the includedstudies. Since they did not address temporality, we cannot excludethe possibility of reverse causality between obesity and IGFBP-1.
Although homogeneity was not achieved in all the analyses, weidentified assay method as a potential source of heterogeneity andadjusted for this factor. The inherent variation in the PCOS pheno-type, ethnic differences and the prevalence of obesity and insulinresistance are likely sources of heterogeneity which cannot beavoided in a meta-analysis. Prospective studies are needed to fullyinvestigate the impact of these factors.
Authors’ rolesC.J.K.: Acquisition of data, analysis and interpretation of data, draftingthe article. S.R.S.: Acquisition of data, analysis and interpretation ofdata. H.L.: Conception and design of article, analysis and interpret-ation of data, revising the article for intellectual content.
ReferencesAdams J, Franks S, Polson DW, Mason HS, Abdulwahid N, Tucker M, Morris DV,
Price J, Jacobs HS. Multifollicular ovaries: clinical and endocrine features andresponse to pulsatile gonadotrophin releasing hormone. Lancet 1985;ii:1375–1378.
Azziz R, Carmina E, Dewailly D, Diamanti-Kandarakis E, Escobar-Morreale HF,Futterweit W, Janssen OE, Legro RS, Norman RJ, Taylor AE et al. Positionsstatement: criteria for defining polycystic ovary syndrome as a predominantlyhyperandrogenic syndrome: an Androgen Excess Society guideline. J ClinEndocrinol Metab 2006;91:4237–4245.
Barbieri RL, Rayan KJ. Hyperandrogenism, insulin resistance and acanthosis nigricanssyndrome: a common endocrinopathy with distinct pathophysiologic features. AmJ obstet Gynecol 1983;147:90–101.
Barbieri RL, Makris A, Randall RW, Daniels G, Kistner RW, Ryan KJ. Insulinstimulates androgen accumulation in incubations of ovarian stroma obtainedfrom women with hyperandrogenism. J Clin Endocrinol Metab 1986;62:904–910.
Bergh C, Carlsson B, Olsson JH, Selleskog U, Hillensjo T. Regulation of androgenproduction in cultured human thecal cells by insulin-like growth factor I andinsulin. Fertil Steril 1993;59:323–331.
Brismar K, Hall K. Clinical applications of IGFBP-1 and its regulation. Growth Regul1993;3:98–100.
Brismar K, Fernqvist-Forbes E, Wahren J, Hall K. Effect of insulin on the hepaticproduction of insulin-like growth factor-binding protein-1 (IGFBP-1), IGFBP-3,and IGF-I in insulin-dependent diabetes. J Clin Endocrinol Metab 1994;79:872–878.
Burghen GA, Givens JR, Kitabchi AE. Correlation of hyperandrogenism withhyperinsulinism in polycystic ovarian disease. J Clin Endocrinol Metab 1980;50:113–116.
Buyalos RP, Pekonen F, Halme JK, Judd HL, Rutanen EM. The relationship betweencirculating androgens, obesity, and hyperinsulinemia on serum insulin-like growthfactor binding protein-1 in the polycystic ovarian syndrome. Am J Obstet Gynecol1995;172:932–939.
Carmina E, Stanczyk FZ, Morris RS, Lee PD, Savjani G, Lobo RA. Altered regulationof insulin-like growth factor binding protein-1 in patients with polycystic ovarysyndrome. J Soc Gynecol Investig 1995;2:743–747.
Carmina E, Gonzalez F, Vidali A, Stanczyk FZ, Ferin M, Lobo RA. The contributionsof oestrogen and growth factors to increased adrenal androgen secretion inpolycystic ovary syndrome. Hum Reprod 1999;14:307–311.
Conover CA, Lee PD, Kanaley JA, Clarkson JT, Jensen MD. Insulin regulation ofinsulin-like growth factor binding protein-1 in obese and nonobese humans.J Clin Endocrinol Metab 1992;74:1355–1360.
Conway GS, Jacobs HS, Holly JM, Wass JA. Effects of luteinizing hormone, insulin,insulin-like growth factor-I and insulin-like growth factor small binding protein 1in the polycystic ovary syndrome. Clin Endocrinol (Oxf) 1990;33:593–603.
Deurenberg P, Yap M, van Staveren WA. Body mass index and percent body fat: ameta-analysis among different ethnic groups. Int J Obes Relat Metab Disord 1998;22:1164–1171.
Diaz VA, Mainous AG III, Koopman RJ. Are ethnic differences in insulin sensitivityexplained by variation in carbohydrate intake? Diabetologia 2005;48:1264–1268.
Dunaif A. Insulin resistance and the polycystic ovary syndrome: mechanism andimplications for pathogenesis. Endocr Rev 1997;18:774–800.
Dunaif A, Segal KR, Futterweit W, Dobrjansky A. Profound peripheral insulinresistance, independent of obesity, in polycystic ovary syndrome. Diabetes1989;38:1165–1174.
Fowler DJ, Nicolaides KH, Miell JP. Insulin-like growth factor binding protein-1(IGFBP-1): a multifunctional role in the human female reproductive tract. HumReprod Update 2000;6:495–504.
Froesch ER, Zapf J. Insulin like growth factors and insulin: comparative aspects.Diabetologia 1985;28:485–493.
Gregoire Nyomba BL, Berard L, Murphy LJ. Free insulin like growth factor I (IGF-I) inhealthy subjects: relationship with IGF-binding proteins and insulin sensitivity. J ClinEndocrinol Metab 1997;82:2177–2181.
Haffner SM, Bowsher RR, Mykkanen L, Hazuda HP, Mitchell BD, Valdez RA, Gingerich R,Monterossa A, Stern MP. Proinsulin and specific insulin concentration in high- andlow-risk populations for NIDDM. Diabetes 1994;43:1490–1493.
Haffner SM, D’Agostino R, Saad MF, Rewers M, Mykkanen L, Selby J, Howard G,Savage PJ, Hamman RF, Wagenknecht LE et al. Increased insulin resistance andinsulin secretion in nondiabetic African-Americans and Hispanics compared withnon-Hispanic whites. The Insulin Resistance Atherosclerosis Study. Diabetes1996;45:742–748.
Higgins JPT (ed). Cochrane Handbook for Systematic Reviews of Interventions. TheCochrane Collaboration, 2008, www.cochrane-handbook.org.
Homburg R, Pariente C, Lunenfeld B, Jacobs HS. The role of insulin-like growthfactor-1 (IGF-1) and IGF binding protein-1 (IGFBP-1) in the pathogenesis ofpolycystic ovary syndrome. Hum Reprod 1992;7:1379–1383.
Hopkins KD, Lehmann ED, Jones RL, Holly JM, Cwyfan-Huges SC, Turay RC, Teale JD,Gosling RG. Ethnicity affects IGFBP-3 and IGF-II in normal healthy young adultsubjects. Clin Endocrinol (Oxf) 1996;45:327–331.
Insler V, Shoham Z, Barash A, Koistinen R, Seppala M, Hen M, Lunenfeld B, Zadik.Polycystic ovaries in non-obese and obese patients: possible pathophysiologicalmechanism based on new interpretation of facts and findings. Hum Reprod1993;8:379–384.
Iwashita M, Mimuro T, Watanabe M, Setoyama T, Matsuo A, Adachi T, Takeda Y,Sakamoto S. Plasma levels of insulin-like growth factor-I and its binding protein inpolycystic ovary syndrome. Horm Res 1990;33(Suppl. 2):21–26.
IGFBP-1 in PCOS: review and meta-analysis 15D
ownloaded from
https://academic.oup.com
/humupd/article-abstract/17/1/4/637745 by guest on 15 N
ovember 2018

Koistinen R, Stenman UH, Alfthan H, Seppala M. Time-resolvedimmunofluorometric assay of 34-kDa somatomedin-binding protein. Clin Chem1987;33:1126–1128.
Kowalska I, Kinalski M, Straczkowski M, Wolczyski S, Kinalska I. Insulin, leptin, IGF-Iand insulin-dependent protein concentrations after insulin-sensitizing therapy inobese women with polycystic ovary syndrome. Eur J Endocrinol 2001;144:509–515.
Laatikainen T, Anttila L, Suikkari AM, Ruutiain K, Erkkola R, Seppala M. Effect ofnaloxone on plasma insulin, insulin-like growth factor I, and its binding protein1 in patients with polycystic ovarian disease. Fertil Steril 1990;54:434–437.
Lear SA, Toma M, Birmingham CL, Frolich JJ. Modification of the relationshipbetween simple and anthropometric indices and risk factors by ethnicbackground. Metab Clin Exp 2003;52:1295–1301.
Lee PD, Giudice LC, Conover CA, Powell DR. Insulin-like growth factor bindingprotein-1: recent findings and new directions. Proc Soc Exp Biol Med 1997;216:319–357.
Liu B, Cai L-Y, LV H-M, Xia L, Zhang Y-J, Zhang H-X, Guan Y-M. Raised serumlevels of matrix metalloproteinase-9 in women with polycystic ovary syndromeand its association with insulin-like growth factor binding protein-1. GynecolEndocrinol 2008;24:285–288.
Morales AJ, Laughlin GA, Butzow T, Maheshwari H, Baumann G, Yen SS. Insulin,somatotropic, and luteinizing hormone axes in lean and obese women withpolycystic ovary syndrome: common and distinct features. J Clin EndocrinolMetab 1996;81:2854–2864.
Morris DV, Falcone T. The relationship between insulin sensitivity and insulin-likegrowth factor-binding protein-1. Gynecol Endocrinol 1996;10:407–412.
Nestler JE, Jakubowicz DJ. Decreases in ovarian cytochrome P450c17 alpha activityand serum free testosterone after reduction of insulin secretion in polycysticovary syndrome.[see comment]. N Engl J Med 1996;335:617–623.
Pasquali R, Casimirri F. The impact of obesity on hyperandrogenism and polycysticovary syndrome in premenopausal women. Clin Endocrinol (Oxf) 1993;39:1–16.
Pekonen F, Laatikainen T, Buyalos R, Rutanen EM. Decreased 34 K insulin-likegrowth factor binding protein in polycystic ovarian disease. Fertil Steril 1989;51:972–975.
Poretsky L. On the paradox of insulin-induced hyperandrogenism in insulin-resistantstates. Endocr Rev 1991;12:3–13.
Poretsky L, Cataldo NA, Rosenwaks Z, Giudice LC. The insulin-related ovarianregulatory system in health and disease. Endocr Rev 1999;20:535–582.
Rajaram S, Baylink DJ, Mohan S. Insulin-like growth factor-binding proteins in serumand other biological fluids: regulation and functions. Endocr Rev 1997;18:801–831.
Rotterdam ESHRE/ASRM-sponsored PCOS consensus workshop group. Revised2003 consensus on diagnostic criteria and long term health risks related topolycystic ovary syndrome (PCOS). Hum Reprod 2004;19:41–47.
Sandhu MS, Gibson JM, Heald AH, Dunger DB, Wareham NJ. Association betweeninsulin-like growth factor-I: insulin-like growth factor-binding protein-1 ratio andmetabolic and anthropometric factors in men and women. Cancer EpidemiolBiomarkers Prev 2004;13:166–170.
Suikkari AM, Koivisto VA, Rutanen EM, Yki-Jarvinen H, Karonen SL, Seppala M.Insulin regulates the serum levels of low molecular weight insulin-like growthfactor-binding protein. J Clin Endocrinol Metab 1988;66:266–272.
Suikkari AM, Tiitinen A, Stenman UH, Seppala M, Laatikainen T. Oral contraceptivesincrease insulin-like growth factor binding protein-1 concentration in women withpolycystic ovarian disease. Fertil Steril 1991;55:895–899.
Takata Y, Maskarinec G, Rindali S, Kaaks R, Nagata C. Serum insulin-like growthfactor-1 levels among women in Hawaii and Japan with different levels of tofuintake. Nutr Cancer 2006;56:136–142.
Thierry Van Dessel HJ, Lee PD, Faessen G, Fauser BC, Giudice LC. Elevated serumlevels of free insulin-like growth factor I in polycystic ovary syndrome. J ClinEndocrinol Metab 1999;84:3030–3035.
Tiitinen AE, Laatikainen TJ, Seppala MT. Serum levels of insulin-like growth factor bindingprotein-1 and ovulatory responses to clomiphene citrate in women with polycysticovarian disease. Fertil Steril 1993;60:58–62.
Wang H-S, Wang T-H. Polycystic ovary syndrome (PCOS), insulin resistance andinsulin-like growth factors (IGfs)/IGF-binding proteins (IGFBPs). Chang GungMed J 2003;26:540–553.
Welt CK, Gudmundsson JA, Arason G, Adams J, Palsdottir H, Gudlaugsdottir G,Ingadottir G, Crowley WF. Characterizing discrete subsets of polycystic ovarysyndrome as defined by the Rotterdam criteria: the impact of weighton phenotype and metabolic features. J Clin Endocrinol Metab 2006;91:4842–4848.
WHO Expert Consultation. Appropriate body mass index for Asian population andits implications for policy and intervention strategies. Lancet 2004;363:157–163.
Zawadzki JK, Dunaif A. Diagnostic criteria for polycystc ovary syndrome in anunselected population. In: Dunaif A, Givens JR, Haseltine FP, Merriam GR(ed)., Polycystic Ovary Syndrome. Boston: Blackwell Scientific, 1992, 377–384.
16 Kelly et al.
Dow
nloaded from https://academ
ic.oup.com/hum
upd/article-abstract/17/1/4/637745 by guest on 15 Novem
ber 2018