Embed Size (px)
Citation preview
7/28/2019 Trust in Physicians Published Paper
http://slidepdf.com/reader/full/trust-in-physicians-published-paper 1/9
Trust in Physicians and Elements of the MedicalInteraction in Patients With Rheumatoid Arthritisand Systemic Lupus ErythematosusJAVIER P. BERRIOS-RIVERA,1 RICHARD L. STREET, JR,2 MARIA G. GARCIA POPA-LISSEANU,1
MICHAEL A. KALLEN,1 MARSHA N. RICHARDSON,1 NAMIETA M. JANSSEN,1 DONALD M. MARCUS,1
JOHN D. REVEILLE,3 NORANNA B. WARNER,3 AND MARIA E. SUAREZ-ALMAZOR1
Objective. To identify components of the patient-doctor relationship associated with trust in physicians. Methods. We assessed 102 patients with systemic lupus erythematosus (SLE) or rheumatoid arthritis (RA) seen atpublicly funded hospitals in Houston, Texas. Patients completed a self-response survey examining patient perceptions of
the medical encounter and trust in their physicians. Evaluated components of physicians’ behaviors included: informa-tiveness, sensitivity to concerns, reassurance and support, patient-centeredness, and participatory decision-making style.Scales were scored 0 to 10, with higher numbers indicating more positive perceptions of communication. Results. Seventy patients had RA and 32 SLE; 25% were white, 43% Latino, 31% African American, and 75% werefemale. Mean scores for the medical interaction and trust scales ranged from 6.2–7.1, indicating moderate degrees of positive perceptions. All components were highly and positively correlated with each other, and with trust, suggestingthat these traits are all elements of a positive style of doctor-patient communication. In multivariate analysis, ethnicity,physicians’ informativeness, physicians’ sensitivity to concerns, patient-centeredness, disease activity, and patient trustin the US health care system were independent predictors of trust in physicians. A separate model examined thepredictors of patient disclosure of information. Patient perceptions of physicians’ patient-centeredness and severity of disease activity were independently predictive of patient disclosure of information.Conclusion. In patients with SLE and RA, trust in physicians is significantly associated with patients’ ethnicity and theirperceptions about specific components of physicians’ communication style. Trust in physicians can be improved by using apatient-centered approach, being sensitive to patient concerns, and providing adequate clinical information. Furthermore,patients appear to be more willing to disclose concerns when physicians use a patient-centered communication style.
KEY WORDS. Physician trust; Communication; Rheumatoid arthritis; Systemic lupus erythematosus.
INTRODUCTION
Trust is a key component of the patient-doctor relationship(1–6). It promotes improved patient quality of life, adher-ence to treatment, satisfaction with care, greater use of preventive clinical services, and better health outcomes(7–13). Without trust, the patient-doctor relationship may
not become firmly established, thus potentially hinderingphysicians’ ability to help patients. Previous studies haveshown that patient characteristics such as race (14–18),age (9,16,18–21), sex (18,19), and level of educationalattainment (9,19,20) are associated with trust. Other ele-ments of the patient-doctor relationship associated withtrust include continuity of care (22–24), length of patient-
Supported by the National Institute for Arthritis and Mus-culoskeletal and Skin Diseases (grant R01-AR-47858) and inpart by the Houston Center for Quality of Care & UtilizationStudies, Health Services Research and Development Ser-vice, Office of Research & Development, Department of Vet-erans Affairs.
1Javier P. Berrios-Rivera, MD, Maria G. Garcia Popa-Lisseanu, MD, Michael A. Kallen, PhD, MPH, MarshaN. Richardson, MSW, Namieta M. Janssen, MD, DonaldM. Marcus, MD, Maria E. Suarez-Almazor, MD, PhD:Baylor College of Medicine and Michael E. DeBakey
Veterans Affairs Medical Center, Houston, Texas;2Richard L. Street, Jr, PhD: Texas A & M University, CollegeStation; 3John D. Reveille, MD, Noranna B. Warner,MD, PhD: University of Texas Health Science Center, Hous-ton.
Address correspondence to Maria E. Suarez-Almazor,MD, PhD, Michael E. DeBakey Veterans Affairs MedicalCenter (152), 2002 Holcombe Boulevard, Houston, TX77030. E-mail: [email protected].
Submitted for publication May 11, 2005; accepted in re-vised form November 3, 2005.
Arthritis & Rheumatism (Arthritis Care & Research)Vol. 55, No. 3, June 15, 2006, pp 385–393DOI 10.1002/art.21988© 2006, American College of Rheumatology
ORIGINAL ARTICLE
385

7/28/2019 Trust in Physicians Published Paper
http://slidepdf.com/reader/full/trust-in-physicians-published-paper 2/9
doctor relationship (1,8,17,21,22), perceived seriousness of medical condition (25), comorbid conditions (21), sex con-cordance (19), concerns about medication adverse events(25), satisfaction with health care (25), poor physical health
(15,20,25), quality of the doctor-patient relationship(15,16,26,27), and physicians’ communicative style (27).
Despite the importance of trust in physicians as a deter-minant of patients’ health-related attitudes and behaviors,few studies have examined the effect of specific compo-nents of the medical care interaction on the developmentof such trust. Rheumatic diseases are chronic and patient-doctor relationships need to be established over a lifetimewith disease. Therefore, it is important that studies beconducted to identify the communicative correlates of trust. Few studies, however, have evaluated these issues inrheumatic patients. One study has evaluated the use of thetrust-in-physicians scale in a group of predominatelywhite patients with rheumatoid arthritis (RA), osteoarthri-
tis, or fibromyalgia (20). This study showed that highereducational attainment, poorer health, and older age wereassociated with decreased trust, but did not examine pa-tients’ perceptions of their doctors’ communicative styles.The objective of our study was to identify and evaluate thecommunicative correlates of trust, and their associationwith trust in physicians in a multiethnic sample of pa-tients with RA and systemic lupus erythematosus (SLE)attending publicly funded health clinics. We used theconceptual framework depicted in Figure 1, examiningconstructs such as doctor patient-centeredness, doctor in-formativeness, doctor sensitivity to concerns, and reassur-ance and support. To our knowledge, this is the first studyto examine these issues in this population.
PATIENTS AND METHODS
Recruitment and data collection. We conducted thiscross-sectional study as part of an ongoing longitudinalstudy of patients with SLE and RA. Participants werepatients receiving medical care at outpatient rheumatologyclinics at publicly funded hospitals in Houston, Texas(Ben Taub General Hospital, Lyndon B. Johnson Hospital,and the Michael E. DeBakey Veterans Affairs Hospital).These institutions are staffed by fellows and residents
under the supervision of attending physicians, and pro-vide medical care to mostly low-income patients of vari-ous ethnic backgrounds who have limited or no healthinsurance. Inclusion criteria included age 18 – 80 years;fulfillment of the American College of Rheumatology RAor SLE diagnostic criteria (28,29); disease duration Ն1year; current treatment with disease-modifying antirheu-
matic drugs, steroids, or biologic agents; adequate mentalstatus; white, African American, or Latino ethnicity; andlanguage proficiency in English or Spanish. The physi-cians and research staff identified all patients with RA orSLE from clinic rosters and reviewed their charts to assesseligibility and ensure that they met the inclusion criteria.With the attending physician’s consent, the research assis-tant approached eligible patients between September 4,2003 and November 11, 2003 to provide information aboutthe study and the content of the questionnaires. Eligiblepatients were approached by letter, phone, or at the time of the clinic visit. If the patient agreed to participate, theresearch assistant proceeded to review the consent form
with the patient and answer any questions. The researchassistant then conducted a brief interview to elicit lan-guage preference and verify the patient’s data from themedical records. Adequate mental status was determined
by the research assistant at the time of the initial contacton the basis of recall memory and initial questioning. Atotal of 119 participants were approached. Of these, 3 weresubsequently found to be ineligible, 9 refused, and 5 whoinitially agreed could not be subsequently reached, leavinga total of 102 subjects (86% participation rate) to partici-pate in the survey. The questionnaire was completed inthe clinic (self-response) by 87 subjects, and on the tele-phone by 15 subjects. Patients were reassured that theresults of the survey were confidential and would not be
shared with their physicians. Institutional Review Boardapproval was obtained from Baylor College of Medicine,Ben Taub General Hospital, Lyndon B. Johnson Hospital,and the Michael E. DeBakey Veterans Affairs prior to thestart of the study. Written informed consent was obtainedfrom all participants at the time of enrollment, includingthose subjects who were interviewed by phone.
Questionnaire. The selection of relevant domains was based on the literature (4,7,17,22,30–37), expert opinion,concurrent related studies at our institution (38,39), andfocus groups (40). Constructs measured using previouslypublished validated scales included Hall’s Trust in Physi-cians Scale (4,7) and Kaplan’s Physicians’ Participatory
Decision-Making Style Scale (30). For components forwhich no suitable scale was identified we created specificitems based on the information gathered during the focusgroup sessions. All subscales were validated using factoranalysis and reliability coefficients (Cronbach’s alpha) todrop redundant or unrelated items. The constructs that wemeasured using the newly created scales included doctors’informativeness (e.g., “I feel that my doctors don’t keep meinformed about rheumatoid arthritis”), doctors’ sensitivityto concerns (e.g., “My doctors seem to care about myproblems”), doctors’ reassurance and support (e.g., “I feelthat my doctors comfort me”), and patient-centered behav-
Figure 1. Conceptual framework depicting the relationship be-tween patient-doctor communication, trust, and outcomes.
386 Berrios-Rivera et al

7/28/2019 Trust in Physicians Published Paper
http://slidepdf.com/reader/full/trust-in-physicians-published-paper 3/9
ior (e.g., “My doctors always ask me what I need”). We alsocreated a 2-item scale to assess patients’ willingness todisclose information (e.g., “I am not comfortable telling mydoctors that I stopped my medication”), and a 2-item scaleto assess patients’ trust in the US health care system (e.g.,“How much trust do you have in the US health care sys-tem?”). All items were scored on a 5-point Likert scale,with response options ranging from strongly agree tostrongly disagree. We created a summary measure for eachof the subscales by taking the unweighted mean of theresponses to all the items in each subscale and transform-ing that value to a 0–10 scale, with lower values indicatingnegative perceptions of communication (lower participa-tion, centeredness, etc.) and higher values indicating pos-itive perceptions.
All questionnaires were translated to Spanish using aforward translation/backward translation methodology,followed by bilingual group evaluation and consensus(41). Seventy-seven percent of the interviews were con-ducted in English and 23% were in Spanish. Cronbach’s
alpha for the various Patient Perception of Communicationsubscales, the Patient Disclosure of Information Scale, andthe Trust in the US Health Care System Scale ranged from0.64– 0.86 (whole sample); 0.64– 0.87 (English); and 0.61–0.87 (Spanish).
Demographic characteristics included age, sex, ethnic-ity, education, marital status, and language preference (En-glish, Spanish, or both). Disease duration was defined astime elapsed from the onset of RA to the date the ques-tionnaire was completed. Patients’ self-assessments of global health, disease activity, and severity of side effectsfrom medications in the previous week were measured onscales of 0–10, where increasing values indicated increas-ing global health, increasing disease activity, or increasingside effects.
Statistical analysis. Descriptive statistics includemean Ϯ SD for continuous variables, and frequencies andpercentages for categorical variables. Pairwise correlationsamong communication subscales were evaluated withSpearman’s correlation tests. Analysis of variance wasused to assess associations between the various subscalesand categorical variables (e.g., ethnicity).
Our first objective was to determine which componentsof physicians’ communicative styles, as perceived by pa-tients, were related to trust. We conducted a multiplelinear regression analysis using Hall’s Trust in Physicians
Scale as the dependent variable, and patient demograph-ics, self-assessed disease activity, and patients’ percep-tions of physicians’ communication subscales as inde-pendent variables. A second multiple linear regressionanalysis was conducted to identify variables that werepredictive of the dependent variable “patient willingnessto disclose information.” Independent variables in the sec-ond model included the same ones as identified for usewith the first regression model and, in addition, the Trustin Physicians Scale. We hypothesized that patients’ will-ingness to disclose information could be related to theirphysicians’ communication style and also to their level of
trust in their physicians. The interaction between sex andethnicity was examined in our regression models. Oursample size precluded us from examining other interac-tions. All statistical analyses were performed with SASsoftware, version 9.1 (SAS Institute, Cary, NC). Statisticalsignificance was set at 0.05, 2-tailed.
RESULTS
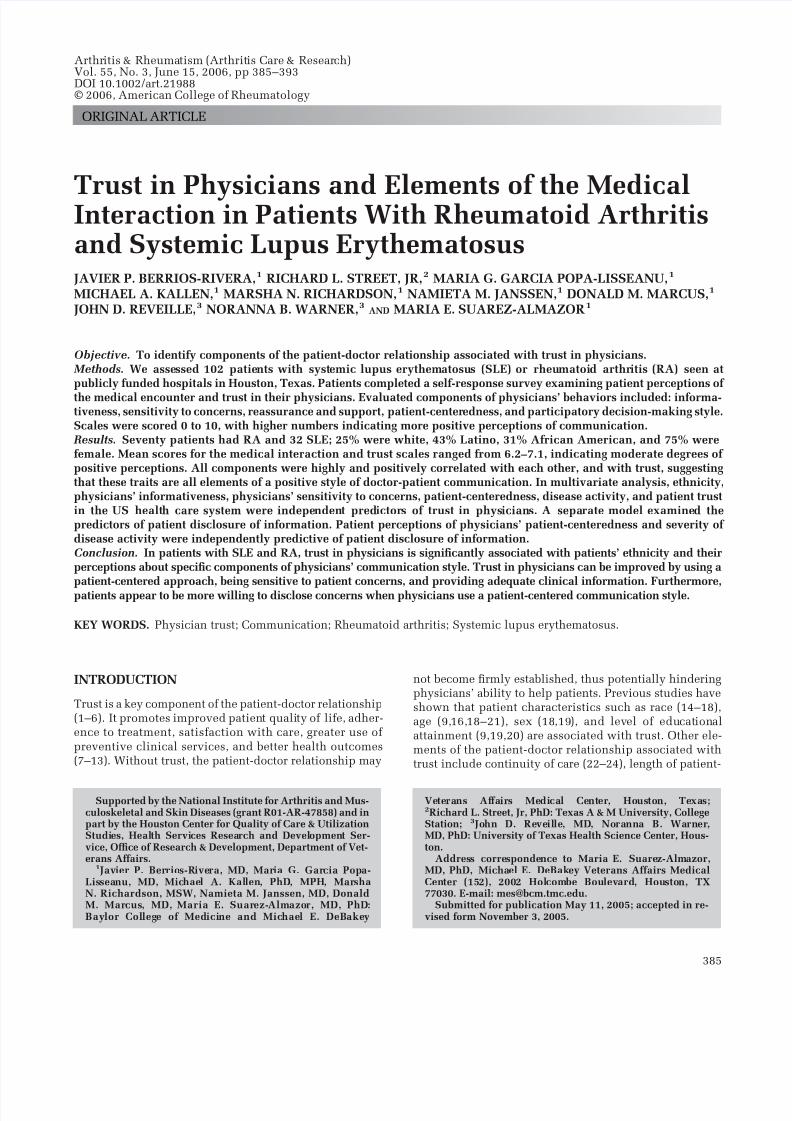
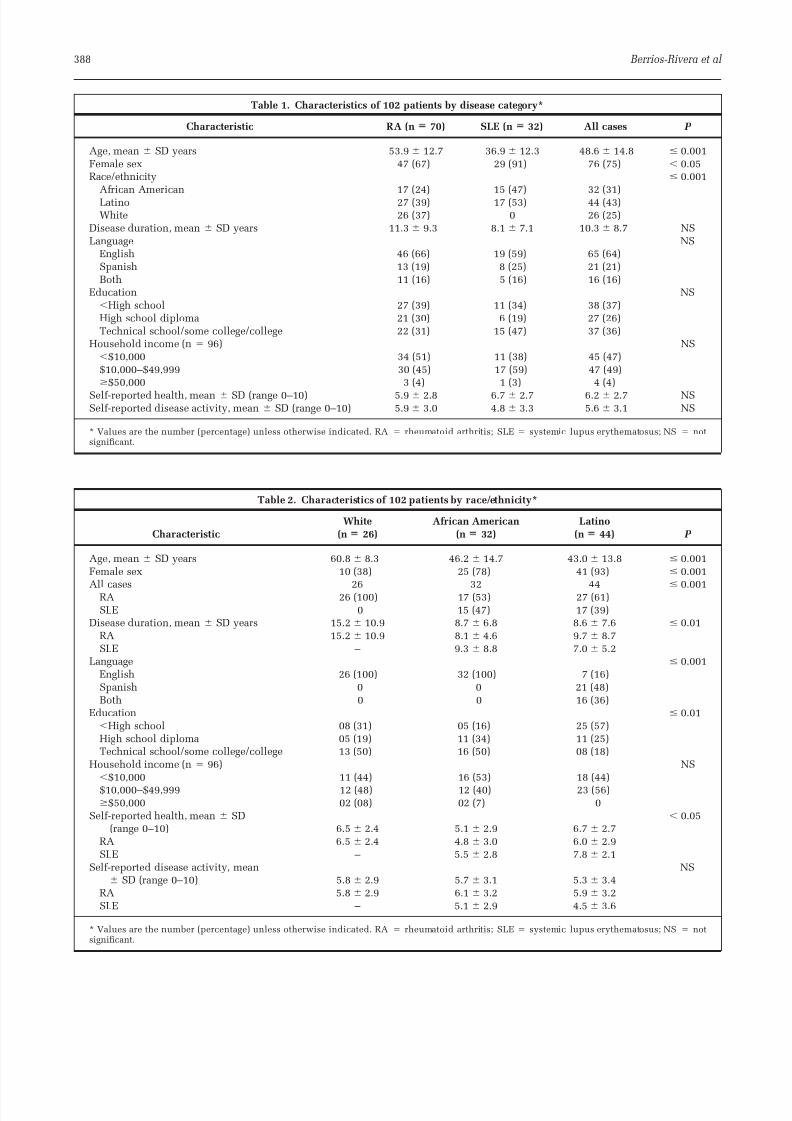
Patient characteristics by disease category are shown inTable 1. There were a total of 70 patients with RA and 32with SLE. The mean age of the subjects was 49 years.Thirty-one percent were African American, 43% wereLatino, and 25% were white. SLE patients were moreeducated, younger, and had shorter disease duration thanRA patients. SLE patients were also more likely to befemale, and more likely to be African American or Latino.
Table 2 lists the patient characteristics by race/ethnicity.White subjects were older with longer disease duration,while Latinos were less well-educated. A majority of sub-
jects rated their health and level of disease activity as being average to high. Table 3 presents the mean scores of the communication subscales by disease category and pa-tient characteristics. Mean scores ranged from 6.2 to 6.9,indicating moderate degrees of positive perceptions. Ap-proximately 25% of the patients scored Յ4 on the partic-ipatory decision-making subscale. The meanϮ SD score of the average Trust in Physician Scale was 7.1 Ϯ 1.6, reflect-ing fairly high levels of trust. English speakers rated theirphysicians as more patient-centered than either Spanishspeakers or bilingual speakers (P Ͻ 0.05). Ethnicity, lan-guage preference, and educational attainment were all sta-tistically associated with trust in the US health care system(with greater levels of trust being reported by Latinos,Spanish only speakers, and less educated subjects).
Tables 4 and 5 show the Spearman’s correlation coeffi-cients between measures of patient-physician interactionand patient characteristics. All components of the medicalinteraction were highly and positively correlated witheach other and with Hall’s Trust in Physicians Scale.These scales have an evaluative component (e.g., higherscores indicating more favorable responses) and the factthat they are highly correlated suggests that all these traitsare positive styles of physicians’ interactions with theirpatients. No significant correlations were observed withage or disease duration. Educational attainment was posi-tively correlated with doctors’ informativeness and doc-tors’ patient-centered behavior, and negatively correlatedwith trust in the US health care system. No statisticallysignificant correlation was observed between level of ed-ucation and trust in physicians. Severity of side effectswas negatively correlated with various components of themedical interaction (informativeness, sensitivity to con-cerns, patient-centeredness, patient disclosure of informa-tion, and trust in physicians).
Table 6 shows the results of the multivariate analysiswith trust in physicians as a dependent variable. Indepen-dent variables that were independently and significantlypredictive of trust included ethnicity, doctors’ informa-tiveness, doctors’ sensitivity to concerns, patient-centered-
Trust in Physicians in RA and SLE Patients 387
7/28/2019 Trust in Physicians Published Paper
http://slidepdf.com/reader/full/trust-in-physicians-published-paper 4/9
Table 2. Characteristics of 102 patients by race/ethnicity*
Characteristic
White
(n 26)
African American
(n 32)
Latino
(n 44) P
Age, mean Ϯ SD years 60.8 Ϯ 8.3 46.2 Ϯ 14.7 43.0 Ϯ 13.8 Յ 0.001Female sex 10 (38) 25 (78) 41 (93) Յ 0.001
All cases 26 32 44Յ
0.001RA 26 (100) 17 (53) 27 (61)SLE 0 15 (47) 17 (39)
Disease duration, mean Ϯ SD years 15.2 Ϯ 10.9 8.7 Ϯ 6.8 8.6 Ϯ 7.6 Յ 0.01RA 15.2 Ϯ 10.9 8.1 Ϯ 4.6 9.7 Ϯ 8.7SLE – 9.3 Ϯ 8.8 7.0 Ϯ 5.2
Language Յ 0.001English 26 (100) 32 (100) 7 (16)Spanish 0 0 21 (48)Both 0 0 16 (36)
Education Յ 0.01ϽHigh school 08 (31) 05 (16) 25 (57)High school diploma 05 (19) 11 (34) 11 (25)Technical school/some college/college 13 (50) 16 (50) 08 (18)
Household income (n ϭ 96) NSϽ$10,000 11 (44) 16 (53) 18 (44)$10,000–$49,999 12 (48) 12 (40) 23 (56)Ն$50,000 02 (08) 02 (7) 0
Self-reported health, mean Ϯ SD Ͻ 0.05(range 0–10) 6.5 Ϯ 2.4 5.1 Ϯ 2.9 6.7 Ϯ 2.7
RA 6.5 Ϯ 2.4 4.8 Ϯ 3.0 6.0 Ϯ 2.9SLE – 5.5 Ϯ 2.8 7.8 Ϯ 2.1
Self-reported disease activity, mean NSϮ SD (range 0–10) 5.8 Ϯ 2.9 5.7 Ϯ 3.1 5.3 Ϯ 3.4
RA 5.8 Ϯ 2.9 6.1 Ϯ 3.2 5.9 Ϯ 3.2SLE – 5.1 Ϯ 2.9 4.5 Ϯ 3.6
* Values are the number (percentage) unless otherwise indicated. RA ϭ rheumatoid arthritis; SLE ϭ systemic lupus erythematosus; NS ϭ notsignificant.
Table 1. Characteristics of 102 patients by disease category*
Characteristic RA (n 70) SLE (n 32) All cases P
Age, mean Ϯ SD years 53.9 Ϯ 12.7 36.9 Ϯ 12.3 48.6 Ϯ 14.8 Յ 0.001Female sex 47 (67) 29 (91) 76 (75) Ͻ 0.05Race/ethnicity Յ 0.001
African American 17 (24) 15 (47) 32 (31)Latino 27 (39) 17 (53) 44 (43)White 26 (37) 0 26 (25)
Disease duration, mean Ϯ SD years 11.3 Ϯ 9.3 8.1 Ϯ 7.1 10.3 Ϯ 8.7 NSLanguage NS
English 46 (66) 19 (59) 65 (64)Spanish 13 (19) 8 (25) 21 (21)Both 11 (16) 5 (16) 16 (16)
Education NSϽHigh school 27 (39) 11 (34) 38 (37)High school diploma 21 (30) 6 (19) 27 (26)Technical school/some college/college 22 (31) 15 (47) 37 (36)
Household income (n ϭ 96) NSϽ$10,000 34 (51) 11 (38) 45 (47)$10,000–$49,999 30 (45) 17 (59) 47 (49)Ն$50,000 3 (4) 1 (3) 4 (4)
Self-reported health, mean Ϯ SD (range 0–10) 5.9 Ϯ 2.8 6.7 Ϯ 2.7 6.2 Ϯ 2.7 NSSelf-reported disease activity, mean Ϯ SD (range 0–10) 5.9 Ϯ 3.0 4.8 Ϯ 3.3 5.6 Ϯ 3.1 NS
* Values are the number (percentage) unless otherwise indicated. RA ϭ rheumatoid arthritis; SLE ϭ systemic lupus erythematosus; NS ϭ notsignificant.
388 Berrios-Rivera et al

7/28/2019 Trust in Physicians Published Paper
http://slidepdf.com/reader/full/trust-in-physicians-published-paper 5/9
ness, disease activity, and trust in the US health system.
An interaction between sex and ethnicity was also ob-served with nonwhite males reporting lower trust in phy-sicians than nonwhite females. African American race andpatient-centered behavior explained the greatest variationin trust-in-physicians scores followed by the interaction of sex and ethnicity. In all, our model explained 76% of thevariation in trust-in-physicians scores. No appreciablecontributions were noted by the addition of the followingvariables: age, education, disease duration, participatory
decision-making style, global self-reported health, marital
status, and language preference.Table 7 shows the results of a stepwise regression ana-
lysis that aimed to identify the determinants of patientdisclosure of information. In addition to the other inde-pendent variables listed in Table 5, this model also in-cluded the trust-in-physicians scale as an independentvariable. Patient-centeredness was the only component of the medical care interaction associated with patient dis-closure of information.
Table 3. Measures of patient-physician interaction and trust by disease category and patient characteristics*
Inform Sensitive Reassurance P-centered PDM PDITrust
physician Trust US-HCS
All patients 6.7 6.8 6.9 6.9 6.2 6.6 7.1 6.5Disease
RA 6.6 6.7 6.9 7.0 6.1 6.5 7.0 6.6SLE 6.9 7.1 7.0 6.9 6.3 6.9 7.1 6.4P 0.49 0.28 0.79 0.75 0.70 0.43 0.89 0.71
SexMale 6.9 7.1 6.8 6.9 6.1 6.6 7.2 5.8Female 6.7 6.7 6.9 6.9 6.2 6.7 7.0 6.8P 0.54 0.36 0.83 0.95 0.78 0.87 0.63 0.09
Race/EthnicityWhite 7.2 7.1 7.1 7.2 6.0 6.7 7.6 5.5Latino 6.5 6.7 6.6 6.7 6.0 6.7 6.9 8.1African American 6.8 6.7 7.1 7.0 6.5 6.5 6.8 5.1P 0.25 0.69 0.44 0.47 0.55 0.86 0.09 Ͻ 0.01†
LanguageEnglish 7.0 6.9 7.1 7.3 6.5 6.6 7.3 5.6Spanish 6.2 6.5 6.5 6.3 5.6 6.5 6.7 8.2Both 6.3 6.5 6.4 6.5 5.8 7.0 6.4 7.8
P 0.08 0.53 0.11 Ͻ 0.05† 0.15 0.80 0.06 Ͻ 0.01†EducationϽHigh school 6.5 6.5 6.5 6.6 5.9 6.3 6.9 7.9HSD 6.8 6.7 7.0 6.8 6.2 6.3 6.9 6.2ՆTechnical 6.9 7.1 7.2 7.3 6.5 7.2 7.3 5.3P 0.45 0.31 0.25 0.21 0.46 0.14 0.45 Ͻ 0.01†
* Inform ϭ informativeness; Sensitive ϭ sensitivity to concerns; Reassurance ϭ reassurance and support; P-centered ϭ patient-centeredness; PDM ϭ
participatory decision-making; PDI ϭ patient disclosure of information; Trust physician ϭ trust in physician; Trust US-HCS ϭ trust in US health caresystem; RA ϭ rheumatoid arthritis; SLE ϭ systemic lupus erythematosus; HSD ϭ high school diploma; Technical ϭ technical school/somecollege/college.† P Յ 0.05.
Table 4. Spearman’s correlations between measures of patient-physician interaction and patient characteristics in 102
patients*
Inform Sensitive Reassurance P-centered PDM PDI
Trust
physician
Trust
US-HCS
Age Ϫ0.01 Ϫ0.09 0.01 0.02 Ϫ0.06 Ϫ0.09 0.04 Ϫ0.09Education 0.24† 0.11 0.16 0.22† 0.14 0.17 0.11 Ϫ0.44‡Disease duration 0.00 Ϫ0.19 Ϫ0.02 Ϫ0.03 Ϫ0.06 Ϫ0.07 Ϫ0.12 Ϫ0.12Global health (range 0–10) 0.14 0.13 0.13 0.13 Ϫ0.05 0.15 0.20† 0.14Disease activity (range 0–10) Ϫ0.13 Ϫ0.14 Ϫ0.04 Ϫ0.12 Ϫ0.01 Ϫ0.20† Ϫ0.03 Ϫ0.19Side effects (n ϭ 73; range 0–10) Ϫ0.30† Ϫ0.24† Ϫ0.16 Ϫ0.27† Ϫ0.16 Ϫ0.29† Ϫ0.28† Ϫ0.07
* Inform ϭ informativeness; Sensitive ϭ sensitivity to concerns; Reassurance ϭ reassurance and support; P-centered ϭ patient-centeredness; PDM ϭ
participatory decision-making; PDI ϭ patient disclosure of information; Trust physician ϭ trust in physician; Trust US-HCS ϭ trust in US health caresystem.† P Ͻ 0.05.‡ P Ͻ 0.0001.
Trust in Physicians in RA and SLE Patients 389

7/28/2019 Trust in Physicians Published Paper
http://slidepdf.com/reader/full/trust-in-physicians-published-paper 6/9
DISCUSSION
The objective of this study was to identify the patientcharacteristics and specific components of the patient-
physician relationship that are associated with trust inphysicians. The patients in the study had chronic diseases,had been under the care of different physicians, and had
been receiving care at publicly funded clinics staffed byresidents, fellows, and attending physicians. This lack of continuity of care with the same physician, as well as ourmodest sample size, prevented us from ascertaining as-pects regarding the multiple patient-physician dyads,which vary from consult to consult. As a result, we mea-sured trust in physicians in general, as opposed to trust inan individual physician. General trust in physicians, incontrast to individual trust, is by no means less important.A study by Hall et al demonstrated that general trust inphysicians is related to following doctors’ recommenda-
tions, satisfaction with care, trust in one’s physician, nothaving changed doctors, not having prior disputes withdoctors, and not having sought second opinions (7). Thisfinding and that of others showing an association betweentrust and use of preventive services (9,12) suggest that trustin physicians is an important construct in health care
(3,5,13). Few studies, however, have examined the con-struct of trust in patients with rheumatic diseases. A study
by Freburger et al that included mostly white subjects with
RA, osteoarthritis, or fibromyalgia demonstrated that trustwas associated with education, age, and health (20), butthe reported response rate was poor (42%). Our study hada different focus in that it included an ethnically diversepopulation of subjects with strictly inflammatory rheu-matic diseases receiving their care at public health facili-ties.
Mean scores for the various medical care interactionterms and trust ranged from 6.2 to 7.1, indicating moderatedegrees of satisfaction with patient-doctor communica-tion. All medical care interaction components were highlycorrelated with each other, suggesting that these traitsform an integral part of a positive style of doctor-patientcommunication. We found that various components of the
patient-physician interaction and patient characteristicswere independently predictive of trust in physicians. In
bivariate analysis, increased trust was significantly corre-lated with fewer side effects and better global health.These findings have also been corroborated by others(20,25,42). However, in our study, these effects were not
Table 5. Spearman’s correlations among measure of physician-patient interactions in 102 patients*
Inform Sensitive Reassurance P-centered PDM PDITrust
physicianTrust
US-HCS
Inform –Sensitive 0.59† –Reassurance 0.60† 0.51† –P-centered 0.68† 0.59† 0.82† –PDM 0.58† 0.50† 0.58† 0.72† –PDI 0.33‡ 0.35‡ 0.43† 0.43† 0.26§ –Trust in physicians 0.61† 0.59† 0.58† 0.75† 0.56† 0.36‡ –Trust US-HCS Ϫ0.08 0.06 Ϫ0.06 Ϫ0.04 0.04 Ϫ0.02 0.12 –
* See Table 4 for definitions.† P Ͻ 0.0001.‡ P Ͻ 0.001.§ P Ͻ 0.01.
Table 6. Determinants of trust in physicians by multiple regression analysis*
Parameters Beta P
Intercept 1.07 0 0.10Ethnicity (reference group white)
African American Ϫ2.17 Ϫ0.64 0.005†
LatinoϪ
0.92Ϫ
0.29 0.001†Informativeness 0.15 0.16 0.046†Sensitivity to concerns 0.23 0.26 0.001†Reassurance and support Ϫ0.13 Ϫ0.14 0.16Patient-centeredness 0.58 0.63 Ͻ 0.001†Disease activity 0.07 0.14 0.007†Trust in US health care system 0.10 0.16 0.010†Sex (reference group male) 1.01 0.28 0.020†Sex-ethnicity interaction Ϫ0.24 Ϫ0.46 0.03†
* Adjusted R2ϭ 0.76. Beta values are standardized coefficients. Age, education, marital status, language
preference, disease duration, participatory decision-making style, and global health status did not makeany appreciable contributions and were removed from the model.† Statistically significant.
390 Berrios-Rivera et al

7/28/2019 Trust in Physicians Published Paper
http://slidepdf.com/reader/full/trust-in-physicians-published-paper 7/9
significant once the multivariate analysis was conducted,suggesting that the associations with trust were mediatedthrough the other variables, in particular the doctor-pa-tient communication features.
Multivariate linear regression analyses revealed statisti-
cally significant independent associations between trust inphysicians and ethnicity, quality of the patient-doctor re-lationship, disease activity, and trust in the US health caresystem. In general, these findings are consistent with thoseof other studies showing similar associations (15,16,21,24,27). We cannot explain, however, why increasingdisease activity was associated with higher levels of trust,
but we cannot exclude the possibility of a spurious asso-ciation. We also found an interaction between sex andethnicity with African American and Latino men reportinglower trust in their physicians than African American andLatino women. This is consistent with the work of Doe-scher et al in which significant interactions between raceand sex and trust in physicians were found (24).
The lower trust in physicians observed in Latino andAfrican American patients, when compared with whites,is consistent with previous studies and suggests that trustmay be an impediment to a better patient-doctor relation-ship and to better outcomes (5,14,15,17,18,24,43). Interest-ingly, the relationship between ethnicity and trust re-mained significant after controlling for the characteristicsof the doctor-patient communication, suggesting that otherfactors are at play. Perhaps physicians (and/or patients)have subconscious biases, stereotypes, perceptions, ormisconceptions (44–46) that interfere with open commu-nication, empathy, and the development of trust. Onestudy involving patients with coronary artery diseaseshowed that physicians’ perceptions of patients were in-fluenced by patients’ sociodemographic characteristics, in-cluding race (47). Another explanation may be that there isa mismatch between patient and physician expectations(48). It may also be the case that cultural and ethnic dif-ferences between patients’ and physicians’ communica-tion style and behavior, including nonverbal communica-tion, lead to exchanges that are not as conducive to thedevelopment of trust (6).
We found that physicians’ patient-centered communica-tion was the only medical interaction variable that wassignificantly and independently associated with patientdisclosure of information. Disease activity, on the other
hand, was negatively associated with patient disclosure of information. Interestingly, we found no independent asso-ciation between ethnicity and patient willingness todisclose information. Nor did we find an independentassociation between trust and patient disclosure of infor-mation. This finding suggests that physician interactionstyles that are centered on patients’ concerns result inmore effective communication on the part of the patient,clearly reinforcing the importance of the doctor-patientdynamic. Emphasis on these components of the patient-doctor relationship can lead to increased information shar-ing by patients.
Two of the goals of Healthy People 2010 are to increasethe quality and years of healthy lives and eliminate healthdisparities (49). Surely trust in physicians is just one of many complex and interrelated factors potentially associ-ated with health disparities, for trust has been seen to beassociated with satisfaction with care, adherence to treat-ment, improved patient quality of life, greater use of pre-ventive services, and better health outcomes (7–12). Addi-
tional studies in other patient populations are needed togain a better understanding of these relationships. Never-theless, our study suggests that interventions to improvedoctor-patient communication would result in increasedtrust in physicians, with consequent positive health be-haviors.
This study has several strengths. First, it evaluated theimpact of patient characteristics and specific componentsof the patient-doctor encounter on trust in physicians in anethnically diverse and indigent patient population diag-nosed with 2 of the most common inflammatory rheumaticdiseases. Second, we had nearly complete data for most of the reported variables, thereby minimizing misclassifica-tion bias. Third, our model explained 76% of the variationin the trust-in-physicians variable. Finally, despite ourmodest sample size, we found a number of significantmoderate-to-large associations; therefore, we are confidentthat any other associations not shown to be statisticallysignificant in our models are likely to be of small magni-tude.
Our study, however, is not without limitations. It ispossible that responses elicited from patients only repre-sent the most recent experiences (recall bias). Anotherpossibility is social desirability bias whereby patients giveresponses that they deem to be socially acceptable. More-over, our sample size was modest. Finally, due to its cross-sectional design, we cannot make valid conclusions re-
garding the temporal association of specific elements of the medical interaction and trust in physicians.
In conclusion, our data suggest that trust in physicians issignificantly and independently associated with patient’sethnicity and specific components of physicians’ commu-nicative style, including informativeness, sensitivity toconcerns, and patient-centeredness. Whereas patient dis-closure of information can be improved by using a patient-centered approach, trust in physicians can be improved byusing a patient-centered approach as well as by beingsensitive to patients’ concerns and providing adequatemedical information.
Table 7. Determinants of patient willingness to disclose
information by multiple regression analysis*
Parameters Beta P
Intercept 4.23 0 Ͻ 0.001Patient-centeredness 0.45 0.38 Ͻ 0.001†Disease activity Ϫ0.13 Ϫ0.20 0.03†
* Adjusted R2ϭ 0.18. Beta values are standardized coefficients.
Race/ethnicity, age, sex, education, disease duration, doctors’ infor-mativeness, sensitivity to concerns, reassurance and support, par-ticipatory decision-making style, trust in physicians, and trust inUS health care system did not make any appreciable contributionsand were removed from the model.† Statistically significant.
Trust in Physicians in RA and SLE Patients 391

7/28/2019 Trust in Physicians Published Paper
http://slidepdf.com/reader/full/trust-in-physicians-published-paper 8/9
ACKNOWLEDGMENTS
The authors would like to thank Vanessa Cox (Michael E.DeBakey VA Medical Center) for her assistance with theanalysis of the data, and the research assistants who as-sisted with patient recruitment and data collection.
REFERENCES
1. Kao AC, Green DC, Davis NA, Koplan JP, Cleary PD. Patients’trust in their physicians: effects of choice, continuity, andpayment method. J Gen Intern Med 1998;13:681–6.
2. Pearson SD, Raeke LH. Patients’ trust in physicians: manytheories, few measures, and little data. J Gen Intern Med2000;15:509–13.
3. Thom DH, Campbell B. Patient-physician trust: an explor-atory study. J Fam Pract 1997;44:169–76.
4. Hall MA, Dugan E, Zheng B, Mishra AK. Trust in physiciansand medical institutions: what is it, can it be measured, anddoes it matter? Milbank Q 2001;79:613–39.
5. Sheppard VB, Zambrana RE, O’Malley AS. Providing healthcare to low-income women: a matter of trust. Fam Pract 2004;21:484–91.
6. Mainous AG 3rd, Kerse N, Brock CD, Hughes K, Pruitt C.Doctors developing patient trust: perspectives from theUnited States and New Zealand. NZFP 2003;30:336–40.
7. Hall MA, Camacho F, Dugan E, Balkrishnan R. Trust in themedical profession: conceptual and measurement issues.Health Serv Res 2002;37:1419–39.
8. Thom DH, Kravitz RL, Bell RA, Krupat E, Azari R. Patienttrust in the physician: relationship to patient requests. FamPract 2002;19:476 – 83.
9. O’Malley AS, Sheppard VB, Schwartz M, Mandelblatt J. Therole of trust in use of preventive services among low-incomeAfrican-American women. Prev Med 2004;38:777–85.
10. Safran DG, Taira DA, Rogers WH, Kosinski M, Ware JE, TarlovAR. Linking primary care performance to outcomes of care. JFam Pract 1998;47:213–20.
11. Bonds DE, Camacho F, Bell RA, Duren-Winfield VT, Ander-son RT, Goff DC. The association of patient trust and self-care
among patients with diabetes mellitus. BMC Fam Pract 2004;5:26.
12. Parchman ML, Burge SK. The patient-physician relationship,primary care attributes, and preventive services. Fam Med2004;36:22–7.
13. Schneider J, Kaplan SH, Greenfield S, Li W, Wilson IB. Betterphysician-patient relationships are associated with higher re-ported adherence to antiretroviral therapy in patients withHIV infection. J Gen Intern Med 2004;19:1096–103.
14. Boulware LE, Cooper LA, Ratner LE, LaVeist TA, Powe NR.Race and trust in the health care system. Public Health Rep2003;118:358–65.
15. Keating NL, Gandhi TK, Orav EJ, Bates DW, Ayanian JZ.Patient characteristics and experiences associated with trustin specialist physicians. Arch Intern Med 2004;164:1015–20.
16. Tarrant C, Stokes T, Baker R. Factors associated with patients’trust in their general practitioner: a cross-sectional survey.
Br J Gen Pract 2003;53:798–800.17. Kao AC, Green DC, Zaslavsky AM, Koplan JP, Cleary PD. The
relationship between method of physician payment and pa-tient trust. JAMA 1998;280:1708–14.
18. Ahern MM, Hendryx MS. Social capital and trust in provid-ers. Soc Sci Med 2003;57:1195–203.
19. Bonds DE, Foley KL, Dugan E, Hall MA, Extrom P. An explo-ration of patients’ trust in physicians in training. J Health CarePoor Underserved 2004;15:294–306.
20. Freburger JK, Callahan LF, Currey SS, Anderson LA. Use of the Trust in Physician Scale in patients with rheumaticdisease: psychometric properties and correlates of trust in therheumatologist. Arthritis Rheum 2003;49:51–8.
21. Fiscella K, Meldrum S, Franks P, Shields CG, Duberstein P,McDaniel SH, et al. Patient trust: is it related to patient-
centered behavior of primary care physicians? Med Care2004;42:1049–55.
22. Thom DH, Ribisl KM, Stewart AL, Luke DA, and the StanfordTrust Study Physicians. Further validation and reliabilitytesting of the Trust in Physician Scale. Med Care 1999;37:510–7.
23. Mainous AG 3rd, Baker R, Love MM, Gray DP, Gill JM. Con-tinuity of care and trust in one’s physician: evidence from
primary care in the United States and the United Kingdom.Fam Med 2001;33:22–7.24. Doescher MP, Saver BG, Franks P, Fiscella K. Racial and
ethnic disparities in perceptions of physician style and trust.Arch Fam Med 2000;9:1156 –63.
25. Shenolikar RA, Balkrishnan R, Hall MA. How patient-physi-cian encounters in critical medical situations affect trust:results of a national survey. BMC Health Serv Res 2004;4:24.
26. Keating NL, Green DC, Kao AC, Gazmararian JA, Wu VY,Cleary PD. How are patients’ specific ambulatory care expe-riences related to trust, satisfaction, and considering changingphysicians? J Gen Intern Med 2002;17:29–39.
27. Thom DH, and the Stanford Trust Study Physicians. Physi-cian behaviors that predict patient trust. J Fam Pract 2001;50:323–8.
28. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF,Cooper NS, et al. The American Rheumatism Association
1987 revised criteria for the classification of rheumatoid ar-thritis. Arthritis Rheum 1988;31:315–24.
29. Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ, RothfieldNF, et al. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum 1982;25:1271–7.
30. Kaplan SH, Greenfield S, Gandek B, Rogers WH, Ware JE Jr.Characteristics of physicians with participatory decision-making styles. Ann Intern Med 1996;124:497–504.
31. Hall MA, Zheng B, Dugan E, Camacho F, Kidd KE, Mishra A,et al. Measuring patients’ trust in their primary care providers[published erratum appears in Med Care Res Rev 2003;60:118]. Med Care Res Rev 2002;59:293–318.
32. Galassi JP, Schanberg R, Ware WB. The patient reactionsassessment: a brief measure of the quality of the patient-provider medical relationship. Psychol Assess 1992;4:346–51.
33. Ludman EJ, Simon GE, Rutter CM, Bauer MS, Unutzer J. Ameasure for assessing patient perception of provider supportfor self-management of bipolar disorder. Bipolar Disord 2002;4:249–53.
34. Anderson LA, Dedrick RF. Development of the Trust in Phy-sician scale: a measure to assess interpersonal trust in patient-physician relationships. Psychol Rep 1990;67:1091–100.
35. Little P, Everitt H, Williamson I, Warner G, Moore M, GouldC, et al. Observational study of effect of patient centerednessand positive approach on outcomes of general practice con-sultations. BMJ 2001;323:908–11.
36. Self-determination theory: an approach to human motivation& personality. The Health Care Climate Questionnaire (HCCQ).URL: http://www.psych.rochester.edu/SDT/measures/auton_hlth.html.
37. Schwartz CE, Brotman S, LaRocca N, Lee H. Patient percep-
tion of quality of care provided by specialists and generalists.Mult Scler 1998;4:426–32.38. Agency for Healthcare Research and Quality and the NIH
Office of Research on Minority Health through the EXCEEDprogram (PO1HS10876). URL: http://www.bcm.edu/medicine/exceed/.
39. Ashton CM, Haidet P, Paterniti DA, Collins TC, Gordon HS,O’Malley K, et al. Racial and ethnic disparities in the use of health services: bias, preferences, or poor communication? J Gen Intern Med 2003;18:146 –52.
40. Garcia Popa-Lisseanu MG, Greisinger A, Richardson M,O’Malley KJ, Janssen NM, Marcus DM, et al. Determinants of treatment adherence in ethnically diverse, economically dis-advantaged patients with rheumatic disease. J Rheumatol2005;32:913–9.
392 Berrios-Rivera et al

7/28/2019 Trust in Physicians Published Paper
http://slidepdf.com/reader/full/trust-in-physicians-published-paper 9/9
41. Guillemin F, Bombardier C, Beaton D. Cross-cultural adapta-tion of health-related quality of life measures: literature re-view and proposed guidelines. J Clin Epidemiol 1993;46:1417–32.
42. Balkrishnan R, Dugan E, Camacho FT, Hall MA. Trust andsatisfaction with physicians, insurers, and the medical pro-fession. Med Care 2003;41:1058–64.
43. Cooper-Patrick L, Gallo JJ, Gonzales JJ, Vu HT, Powe NR,
Nelson C, et al. Race, gender, and partnership in the patient-physician relationship. JAMA 1999;282:583–9.44. Rathore SS, Lenert LA, Weinfurt KP, Tinoco A, Taleghani CK,
Harless W, et al. The effects of patient sex and race onmedical students’ ratings of quality of life. Am J Med 2000;108:561–6.
45. Shavers VL, Lynch CF, Burmeister LF. Racial differences infactors that influence the willingness to participate in medicalresearch studies. Ann Epidemiol 2002;12:248–56.
46. Freimuth VS, Quinn SC, Thomas SB, Cole G, Zook E, DuncanT. African Americans’ views on research and the TuskegeeSyphilis Study. Soc Sci Med 2001;52:797–808.
47. Van Ryn M, Burke J. The effect of patient race and socio-economic status on physicians’ perceptions of patients. Soc
Sci Med 2000;50:813–28.48. Kravitz RL. Measuring patients’ expectations and requests.Ann Intern Med 2001;134:881–8.
49. Healthy People 2010. A systematic approach to health im-provement. URL: http://www.healthypeople.gov/Document/html/uih/uih_2.htm#goals.
Trust in Physicians in RA and SLE Patients 393





























