Embed Size (px)
Citation preview

326 Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al
Undifferentiated TumorTrue Identity by Immunohistochemistry
Armita Bahrami, MD; Luan D. Truong, MD; Jae Y. Ro, MD, PhD
● Context.—‘‘Undifferentiated tumor’’ refers to a hetero-geneous group of neoplasms with little or no evidence ofdifferentiation on routine light microscopic morphology.
Objective.—To identify the true identity of undifferen-tiated tumors by immunohistochemical analysis.
Data Sources.—Review of the pertinent literature andthe authors’ experience.
Conclusions.—For treatment and prognostic evaluation,it is crucial to delineate whether an undifferentiated neo-plasm is epithelial, mesenchymal, melanocytic, or hema-topoietic in nature. Application of a screening panel todemonstrate the expression of markers of major lineages isfundamental for determination of the broad category ofneoplasia. Because poorly differentiated carcinomas and inparticular sarcomatoid carcinomas are known to be het-erogeneous in their antigen expression, several epithelialmarkers in combination may be required to establish the
carcinomatous nature of tumor. A diagnostic misinterpre-tation as a consequence of occasional aberrant or unex-pected antigen expression is best avoided by using a broadpanel that includes both antibodies that are anticipated tobe positive and those that are expected to be negative. Inthis treatise, the immunohistochemical dissection of undif-ferentiated tumors on the basis of their morphologic fea-tures is outlined, supplemented with algorithmic immu-nohistochemical analysis for each morphologic category ofsmall round cell tumors, carcinomatous tumors, sarcoma-tous (or sarcoma-like) tumors, and tumors with histologi-cally overlapping features, including hematolymphoid ma-lignancies, melanoma, and sarcomas with epithelioid ap-pearance. The utility of several organ- or tissue-specificmarkers in the context of undifferentiated tumors is re-viewed.
(Arch Pathol Lab Med. 2008;132:326–348)
The term undifferentiated tumor has been used in refer-ence to a heterogeneous group of tumors with little
or no evidence of differentiation. Some may link this ter-minology to morphologically undifferentiated neoplasmsthat cannot be otherwise classified, even with the appli-cation of immunohistochemistry. In our view, however,such tumors are extremely rare and in most instances fur-ther sampling or application of ancillary tests should helpto recognize them as a specific tumor type. For such rea-son, in this review we apply the term undifferentiated totumors lacking evidence of lineage differentiation on thebasis of routine light microscopic morphology alone.
An undifferentiated malignant tumor represents eithera metastasis of unknown origin or a primary neoplasiawithout obvious cell line of differentiation. It should benoted that undifferentiated tumor generally implies ahigh-grade malignancy, frequently associated with pleo-morphic to anaplastic appearance. Therefore, low-gradeneoplasms but without an obvious lineage of differentia-tion (eg, monomorphic spindled cell tumors) or low-gradetumors not infrequently encountered in the context of me-
Accepted for publication June 4, 2007.From the Departments of Pathology, Baylor College of Medicine (Drs
Bahrami and Truong) and Weill Medical College of Cornell University,The Methodist Hospital (Drs Truong and Ro), Houston, Tex.
The authors have no relevant financial interest in the products orcompanies described in this article.
Reprints: Jae Y. Ro, MD, PhD, Department of Pathology, Weill Med-ical College of Cornell University, The Methodist Hospital, 6565 FanninSt, Houston, TX 77030 (e-mail: [email protected]).
tastasis of unknown origin are not included in this dis-cussion.
For treatment purposes, it is crucial to determine wheth-er an undifferentiated neoplasm is epithelial, mesenchy-mal, or hematopoietic. In general, the diagnosis of lym-phoma for an undifferentiated tumor predicts a betterclinical outcome compared with that of carcinoma.1 Thevalue of immunohistochemical procedures for identifica-tion of the true identity of undifferentiated tumors hasbeen proved by studies in which approximately 90% oftumors posing diagnostic difficulties by morphologycould be accurately classified by exploiting immunohis-tochemistry.1–3
Even in undifferentiated tumors, subtle features of ep-ithelial versus mesenchymal differentiation can often beappreciated, which assist the immunohistochemical ap-proach to these tumors. Hints for epithelial differentiationinclude epithelioid cells (round to oval cells) with nestingarrangement and a desmoplastic stroma with feeding ves-sels separating tumor cell nests (Figure 1). In contrast,mesenchymal differentiation is suggested by a diffuse ar-rangement of spindled cells (Figure 2), without reactivestroma, but with feeding vessels in between tumor cells.Some tumors, however, may not fit into either of these 2categories because of their overlapping histologic features(Figure 3), for example, sarcomatoid carcinoma, melano-ma, lymphoma, neuroendocrine tumors, and sarcomawith epithelioid cells.
Immunohistochemical dissection of undifferentiated tu-mors is also helped by categorizing them into small round

Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al 327
Figure 1. Photomicrograph of undifferentiated carcinomatous tumorcomposed of epithelioid cells with nesting arrangement and a des-moplastic stroma separating tumor cell nests (hematoxylin-eosin, orig-inal magnification �10).
Figure 2. Photomicrograph of undifferentiated sarcomatous tumorcomposed of spindled cells with a diffuse arrangement with no reactivestroma in between tumor cells (hematoxylin-eosin, original magnifi-cation �20).
←Figure 3. Photomicrograph of undifferentiated tumor with overlap-ping histologic features, displaying epithelioid cells without nesting ar-rangement (hematoxylin-eosin, original magnification �20).
blue cell tumors (SRCTs) or large cell tumors. The lattergroup is further divided into (1) carcinomatous tumors,(2) sarcomatous or sarcoma-like tumors, and (3) tumorswith overlapping features. Each category entertains abroad list of entities from epithelial, mesenchymal, he-matopoietic, or melanocytic lineage in the differential di-agnosis.
In the following section, the immunohistochemical pro-cedure for a broad lineage determination of undifferenti-ated tumors is discussed, followed by immunohistochem-ical analysis of each individual category of SRCTs, carci-nomatous tumors, sarcomatous (or sarcoma-like) tumors,and tumors with overlapping features, supplementedwith diagnostic algorithms. It is emphasized that the out-lined algorithmic immunohistochemical approach is nei-ther meant to be comprehensive nor intended to be anabsolute method for immunohistochemical dissection ofthese tumors. In reality, each tumor requires an ‘‘individ-ually constructed panel’’ composed of carefully selectedantibodies that recognize all reasonable diagnostic possi-bilities in the context of the tumor’s morphology, anatomicsite, and clinical/radiologic findings.
BROAD LINEAGE DETERMINATIONThe immunohistochemical evaluation of undifferentiat-
ed tumors should first aim at determination of the broadcategory of neoplasia, that is, carcinoma, sarcoma, lym-phoma, or melanoma. A screening panel to demonstratethe expression of markers of major lineages (ie, epithelial,mesenchymal, lymphoid, and melanocytic) often providesthe first clue to the nature of an undifferentiated tumor.In certain circumstances, adjuvant immunostains are add-ed; thus, placental alkaline phosphatase (PLAP) andOCT3/4, markers for germ cell tumors (GCTs), may beincluded for tumors in younger men in view of the highincidence of GCTs in this age group. Based on the resultof the screening panel, a more detailed or specific panelis commonly followed to further subclassify the tumor orconfirm a particular diagnosis.
Screening Markers for Epithelial LineageCytokeratins. The low-molecular-weight cytokeratins
(LMW CKs), including CK8, CK18, and CK19, recognizedby the antibodies CAM 5.2 or 35BH11, and a cocktail ofkeratins (pankeratin), recognized by the antibody AE1/AE3, are useful screening markers for the recognition ofepithelial differentiation. Because poorly differentiatedcarcinomas are known to be heterogeneous in their ex-pression of antigens recognized by epithelial markers,when a negative result is obtained with a single antibodyand the diagnosis of carcinoma is still suspected, it is pru-dent to use additional antibodies in a backup panel. In astudy of 98 poorly differentiated carcinomas, CAM 5.2 andepithelial membrane antigen (EMA) each detected epithe-lial differentiation of 71% of the cases, whereas a com-bined CAM 5.2 and EMA elucidated the epithelial natureof 99%.4
Sarcomatoid carcinomas are in particular known to beunpredictable in regard to their CK expression; therefore,

328 Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al
Table 1. Malignant Neoplasms With Coexpression ofVimentin and Cytokeratin
CarcinomaRenal cell carcinomaEndometrial adenocarcinomaSerous ovarian carcinomaThyroid carcinoma, papillary and anaplasticMesothelioma (biphasic)Sarcomatoid carcinoma (spindle cell carcinoma)
SarcomaSynovial sarcomaDesmoplastic small round cell tumorMalignant rhabdoid tumorEpithelioid sarcomaEpithelioid angiosarcoma
Carcinosarcoma
it is sometimes required to use several markers in com-bination to detect the epithelial differentiation of these tu-mors (see ‘‘Sarcomatoid Carcinoma’’). In addition, CKmay not be detectable in certain carcinomas; for example,it is known that CK expression in adrenocortical carcino-mas is often diminished to levels too low to be recognizedfollowing the deleterious effects of fixation.5–7
Cytokeratin expression, most frequently with LMWCKs, has been occasionally described in a variety of sar-comas8,9 and rarely in hematopoietic malignancies10–14 andmelanocytic lesions.9,15,16 Aberrant CK staining in nonepi-thelial malignancies, however, has a weak, focal, andpatchy staining, which contrasts with the generally diffuseand strong staining seen in carcinomas or sarcomatoidcarcinomas. Conversely, a true strong CK expression,which is frequently associated with a morphologic ap-pearance of epithelial differentiation, is also seen in cer-tain sarcomas8 (see ‘‘Sarcomas With Epithelioid Appear-ance’’). Hence, caution should be taken to avoid overinter-pretation of CK expression as a specific feature of epithe-lial tumors.
Epithelial Membrane Antigen. As mentioned previ-ously, EMA may be used as a supplement to CKs for de-tection of epithelial differentiation, especially in sarco-matoid carcinoma or those undifferentiated carcinomasthat are negative or only focally positive for CKs. A num-ber of epithelial tumors, including GCTs and some endo-crine neoplasms such as medullary carcinoma of thyroidand adrenocortical carcinomas, lack immunoreactivity forEMA.17
Epithelial membrane antigen is not entirely specific forcarcinomas. Epithelial membrane antigen expression hasbeen seen in some normal and neoplastic hematopoieticcells, including reactive and neoplastic plasma cells,12 lym-phocytic and histiocytic (L&H) cells in nodular lympho-cyte predominant Hodgkin lymphoma,18,19 and neoplasticcells in some T-cell lymphomas17,19,20; thus, most anaplasticlymphoma kinase (ALK)–positive anaplastic large celllymphomas (�75%) are EMA positive.18,21
Screening Marker for Mesenchymal LineageVimentin. Vimentin is the sole intermediate filament
characteristic of mesenchymal cells and present in virtu-ally all sarcomas and melanomas and variably in lympho-mas.22 The antigenicity of vimentin is best preserved infrozen and alcohol-fixed tissues.22,23 Vimentin, however,suffers poor specificity for mesenchymal neoplasms be-cause it may be coexpressed with CK in a wide range ofcarcinomas (Table 1).22–24 Therefore, vimentin by itself can-not be used to differentiate mesenchymal from nonmesen-chymal neoplasms.
Vimentin/CK CoexpressionFrequent coexpression of vimentin with CK is seen in
some carcinomas, for example, renal cell, endometrial,papillary and anaplastic thyroid, and ovarian serous (var-iably) carcinomas.22,23 Consistent absence of vimentin, onthe other hand, is observed in colonic, small intestinal, andprostatic adenocarcinomas or in transitional cell carcino-mas.22 The finding of vimentin/CK coexpression helps fo-cus on certain types of epithelial tumors as possible pri-mary sites in the evaluation of metastatic tumors. On theother hand, a number of sarcomas, in particular thosewith epithelioid appearance, also express CK in additionto vimentin. A selected list of malignant neoplasms fre-
quently demonstrating vimentin/CK coexpression is pro-vided in Table 1.
Screening Markers for Malignant MelanomaS100 Protein. S100 protein is regarded as a screening
marker for melanoma with more than 95% sensitivity inprimary and metastatic sites. A valid positive S100 re-quires both nuclear and cytoplasmic staining. S100 pro-tein, however, is also expressed in various other lesions,including peripheral nerve sheath, granular cell, cartilag-inous and salivary gland tumors, chordomas, Langerhanscell histiocytosis, and occasional adenocarcinomas to vary-ing degrees.25 Thus, to confirm the melanocytic nature ofan S100-positive neoplasm, the tumor should be also pos-itive for one or more melanocyte-specific protein (eg,HMB-45 or MART-1/Melan-A).
HMB-45. HMB-45 is a quite specific marker for mel-anoma, labeling 90% to 100% of conventional primarymelanomas. The positivity rate declines to 80% in recur-rent or metastatic melanomas and spindle cell melano-mas.26 Desmoplastic melanomas are essentially negativefor HMB-45 or other specific melanoma markers.27 HMB-45 positivity is typically not observed in carcinomas, lym-phomas, or sarcomas.
Screening Marker for Hematopoietic MalignanciesCD45. Although CD45 (leukocyte common antigen
[LCA]) is known to have high sensitivity (97%) and spec-ificity (nearly 100%) for lymphoid tumors,28,29 exceptionshave been documented. For example, CD45 is undetect-able in most lymphoblastic lymphomas29–32 and is variablyexpressed in plasma cell neoplasms29,33–35 and anaplasticlarge T-cell lymphomas.36,37 CD45 immunoreactivity hasbeen considered exquisitely specific for hematopoieticcells28,29; yet, there are exceptional reports of CD45 ex-pression in undifferentiated or neuroendocrine carcino-mas.38
Aberrant or Unpredicted Antigen ExpressionAs stated in several previous examples, an aberrant or
unexpected antigen expression should be considered as asource of diagnostic pitfall in the surgical pathology eval-uation of undifferentiated tumors. A diagnostic misinter-pretation is best avoided by using a broad panel that in-cludes both antibodies that are anticipated to be positiveand those that are expected to be negative. The occasionalaberrant immunophenotyping must not undermine the
Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al 329
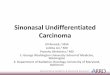
Table 2. The Immunoprofile of Small Round Cell Tumors*
CK CD45 S100 CD99 DesminMyogenin/
Myo-D1 CD56 WT1
Ewing sarcoma/primitive neuroectodermal tumor � � � � � � �† �Rhabdomyosarcoma � � � �† � � � �‡Desmoplastic small round cell tumor � � � � � � � �Poorly differentiated synovial sarcoma �§ � �† � � � � �Mesenchymal chondrosarcoma � � �� � � � � �Wilms tumor � � � �† � �¶ � �Neuroblastoma �† � �# � � � � �Small cell carcinoma � � � � � � � �Hematopoietic malignancies � �** � �†† � � � �Melanoma � � � � � � �† �‡
* CK indicates cytokeratin; �, variable; �, negative; and �, positive.† Often negative but occasionally positive.‡ Nonspecific cytoplasmic immunoreactivity.§ Cytokeratin positive in �50%, epithelial membrane antigen positive in �100%.� S100 positive in cartilaginous areas.¶ Positive only in rhabdomyomatous Wilms tumor.# Positive only in schwannian stroma.** Frequently negative in lymphoblastic lymphoma.†† Positive in most lymphoblastic lymphomas.
Figure 4. Algorithmic immunohistochemical analysis for small round blue cell tumors. NE mk indicates neuroendocrine markers; SmCC, smallcell carcinoma; PDSS, poorly differentiated synovial sarcoma; DSRCT, desmoplastic small round cell tumor; EWS/PNET, Ewing sarcoma/primitiveneuroectodermal tumor; MC, mesenchymal chondrosarcoma; NB, neuroblastoma; SCOS, small cell osteosarcoma; MyoG, myogenin; RMS, rhab-domyosarcoma; *, positive cytoplasmic but not nuclear staining in RMS; and WT, Wilms tumor.
recognized usefulness of screening markers in character-ization of undifferentiated malignant neoplasms.
SMALL ROUND CELL TUMORSSmall round cell tumors comprise heterogeneous neo-
plasms composed of relatively small, round to oval, close-ly packed undifferentiated cells with high nuclear-cyto-plasmic ratio, scant cytoplasm, and round nuclei withevenly distributed, slightly coarse chromatin and small orinconspicuous nucleoli. In spite of a similar light micro-scopic morphology, SRCTs include pathologic entitiesfrom vastly different lineages, including (1) epithelial tu-mors, for example, small cell carcinoma (SmCC) (poorlydifferentiated neuroendocrine carcinoma); (2) mesenchy-mal tumors encompassing malignant solid neoplasms ofchildhood and other small round cell sarcomas; and (3)tumors with overlapping features, such as lymphoma andmelanoma. Because of similar routine light microscopicfeatures of these tumors, immunohistochemistry is oftenmandated for a definitive diagnosis. The immunoprofileof SRCTs is provided in the following and in Table 2, andan algorithmic immunohistochemical analysis is outlinedin Figure 4.
Ewing Sarcoma/Primitive Neuroectodermal Tumor
CD99, the product of the MIC2 gene, is a cell surfaceglycoprotein that is expressed in more than 95% of Ewingsarcoma/primitive neuroectodermal tumors (EWS/PNETs)39–42 with a diffuse membranous staining pattern.CD99, however, is also expressed in several otherSRCTs42–44 including lymphoblastic lymphoma/leukemia(�90%),31,45 acute myelogenous leukemia (43%),46 granu-locytic sarcoma (55%),46 small cell variant of poorly dif-ferentiated synovial sarcoma (PDSS) (nearly all),47–49 mes-enchymal chondrosarcoma (80%–100%),50,51 desmoplasticsmall round cell tumor (DSRCT) (up to 50%),52 and rarelyin rhabdomyosarcoma (RMS).53 CD99, however, is not ex-pressed in neuroblastoma42 and is only exceptionally pres-ent in blastema-rich nephroblastoma.44,54 In contrast,CD56, a neural cell adhesion molecule (NCAM), which ispositive in most SRCTs, is expressed in only 10% to 25%of EWS/PNETs55–57 and rarely in lymphoblastic lymphoma(�10%).58,59 Therefore, a CD99�/CD56� profile supportsthe diagnosis of EWS/PNET or lymphoblastic lymphomaagainst other SRCTs.
The characteristic translocation in EWS/PNET, t(11;

330 Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al
Figure 5. Photomicrograph of rhabdomyosarcoma showing a diffusestrong nuclear staining for myogenin (original magnification �10).
22)(q24;q12), involving the Ewing sarcoma (EWS) gene onchromosome 22 and the FLI-1 gene on chromosome 11,results in overexpression of FLI-1 protein, which can bedetected immunohistochemically in more than 70% ofEWS/PNETs.40,60,61 Hence, a nuclear staining for FLI-1 pro-tein may help distinguish Ewing family of tumors fromother CD99-positive SRCTs, except for lymphoblastic lym-phomas, which also stain for FLI-1 protein in 88% of cas-es.60 Cytokeratin is expressed variably in EWS/PNETs (in20%–57%); in contrast, desmin expression is extremely un-common.40,54,62,63
Rhabdomyosarcoma
Myogenin and Myo-D1, the 2 myogenic transcriptionalregulatory proteins, are equally regarded as sensitive andspecific markers of skeletal muscle differentiation.64 Thesemarkers stain the overwhelming majority (�95%) ofRMSs53,64–66 including the primitive undifferentiated forms,regardless of morphologic evidence of skeletal muscle dif-ferentiation.65 Although a nuclear staining is deemed astrue positive (Figure 5), a cytoplasmic stain, which maybe observed in nonmyogenous tumors, should be consid-ered nonspecific. Because of the potential for cytoplasmicand high background staining with available antibodiesagainst Myo-D1, staining for myogenin is technically pref-erable.66,67
Desmin and muscle-specific actin, although highly sen-sitive markers for RMSs, are not specific for these tumorsbecause they also stain smooth muscle neoplasms andDSRCTs. A strong cytoplasmic staining for WT1, not thespecific nuclear staining, is observed in RMSs (in 100% ofcases in 1 report).68
Desmoplastic Small Round Cell Tumor
These tumors are characterized by a polyphenotypicdifferentiation, including frequent coexpression of vimen-tin, epithelial markers (CAM 5.2, AE1/AE3, EMA), WT1,neuron-specific enolase (NSE), and desmin,52,69,70 the latterwith a cytoplasmic or characteristic paranuclear dotlikepattern. Although most DSRCTs are positive for desmin,the absence of reactivity for Myo-D1 and myogenin52,70 dif-ferentiates them from RMSs. Because coexpression of CK
and desmin is rarely seen in other SRCTs, it is probablythe most specific immunohistochemical profile forDSRCT52 (Figure 6, a through d). The characteristic geneticfeature of DSRCT is a consistent association with t(11;22)(p13;q12) that results in the fusion of Wilms tumor(WT1) and EWS genes. The antibody directed against theWT1 part of the fusion protein is positive in 70% to 100%of cases.52,71,72 CD99 expression is variable and seen in onethird to one half of DSRCTs.52,70
Poorly Differentiated Synovial SarcomaAlthough the classic bimorphic form of synovial sarco-
ma is usually easily recognized based on the hematoxylin-eosin (H&E) morphology, its poorly differentiated variantsoften create diagnostic difficulty. Three types of PDSShave been recognized: a small cell variant, a large cellepithelioid variant, and a high-grade spindle cell variant.47
The small cell variant is often difficult to distinguishfrom other SRCTs, in particular EWS/PNET. The distinc-tion becomes even more complicated as both PDSS andEWS/PNET are reactive for CD99 in most cases.48,49,73
However, PDSS can be differentiated from EWS/PNETby positive staining for EMA (95%–100% of cases),CK (�50%), CD56 (100%), and collagen IV (100%).48,49,73
These markers are conversely negative in most EWS/PNETs.55–57,74 Because synovial sarcoma is nearly alwaysnegative for CD34, a positive stain for CD34 essentiallyexcludes the diagnosis of PDSS. Most synovial sarcomasregardless of histology have the specific translocation t(X;18)(SYT-SSX); hence, in questionable cases molecular test-ing may be required for definitive diagnosis.
Mesenchymal ChondrosarcomaMesenchymal chondrosarcoma is a biphasic tumor com-
posed of highly undifferentiated small round cells, ad-mixed with islands of hyaline-like cartilage. If the histo-logic tissue includes only the undifferentiated small cellcomponent, the distinction of mesenchymal chondrosar-coma from other SRCTs especially EWS/PNET will be dif-ficult or perhaps impossible.
Although the cartilaginous areas are reactive for S100protein, the small cell component is typically not.50 Theimmunoprofile of mesenchymal chondrosarcoma includesvariable expression for NSE and desmin but negativestaining for CKs and myogenin.50 CD99 is demonstratedin most cases (80%–100%) in the small cell component.50,51
Small Cell OsteosarcomaBecause of the lack of a specific immunoprofile for os-
teosarcoma,75 recognition of the small cell variant of os-teosarcoma from other SRCTs essentially relies on the ob-servation of osteoid production76 (Figure 7). Althoughmonoclonal antibodies for osteocalcin are specific for os-teoid-forming tumors,77,78 only a minority of small cell os-teosarcoma show osteocalcin reactivity.39 Osteosarcomasare immunophenotypically heterogeneous79 and may oc-casionally express desmin, smooth muscle actin, S100 pro-tein, and rarely CK,75,79,80 creating a potential diagnosticpitfall in their distinction from other SRCTs.
Wilms TumorWilms tumor is classically a triphasic tumor composed
of blastemal, epithelial, and stromal elements, but on oc-casions, particularly in small biopsy materials, it may pre-sent as a monophasic lesion with only blastemal compo-
Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al 331
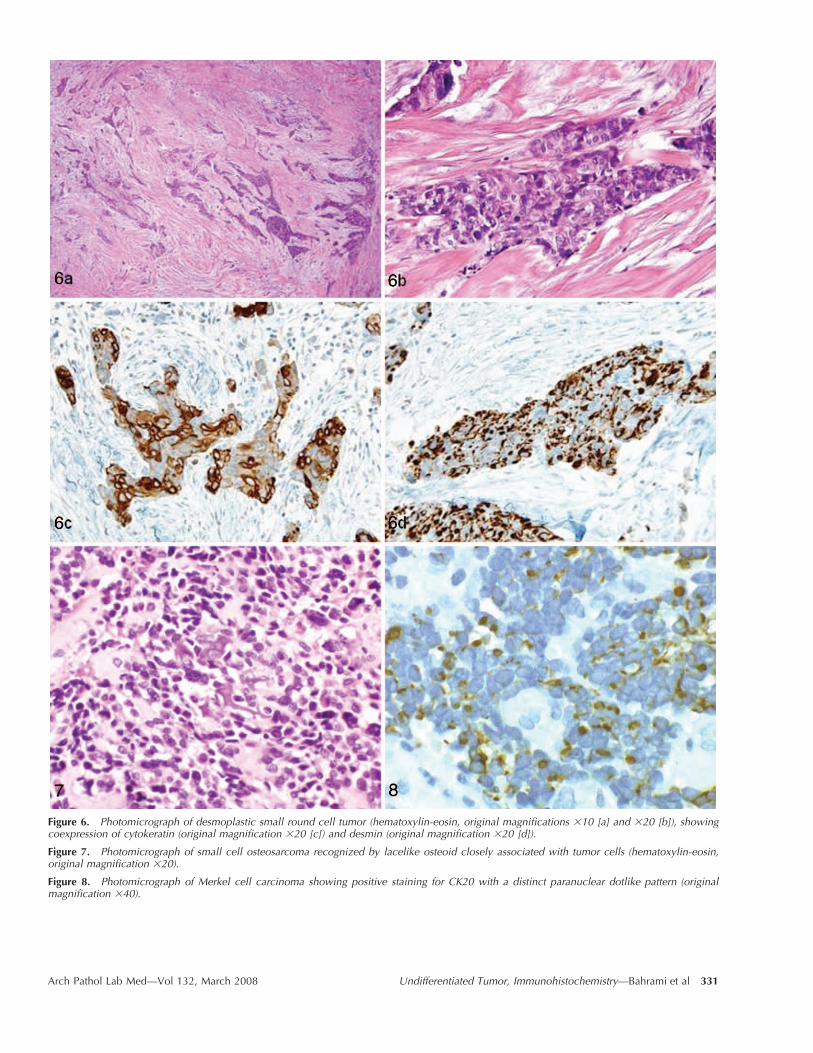
Figure 6. Photomicrograph of desmoplastic small round cell tumor (hematoxylin-eosin, original magnifications �10 [a] and �20 [b]), showingcoexpression of cytokeratin (original magnification �20 [c]) and desmin (original magnification �20 [d]).
Figure 7. Photomicrograph of small cell osteosarcoma recognized by lacelike osteoid closely associated with tumor cells (hematoxylin-eosin,original magnification �20).
Figure 8. Photomicrograph of Merkel cell carcinoma showing positive staining for CK20 with a distinct paranuclear dotlike pattern (originalmagnification �40).

332 Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al
nent. Blastema-rich Wilms tumor, mainly composed of un-differentiated blastemal cells, may be difficult to distin-guish from other SRCTs from a morphologic perspective,especially in the setting of metastatic disease.
WT1, the Wilms tumor suppressor gene, located onchromosome 11p13, encodes a putative transcription fac-tor implicated in tumorigenesis and in normal urogenitaldevelopment. WT1 nuclear staining in the blastemal areais seen in 70% to 100% of cases.54,68,81 Although the blas-temal component is reactive for vimentin and desmin(partially in up to 90%), the absence of staining for my-ogenin and Myo-D1 discriminates blastematous Wilms tu-mor from RMS.82,83 Blastemal foci are either negative oronly focally positive for CK. Although rare instances ofCD99 expression have been reported, staining for FLI-1has never been observed.54,60
NeuroblastomaNeuroblastoma is characterized by a neuronal pheno-
type, which is demonstrated by several markers includingNSE (positive in 38%–95%), neurofilament (63%), CD56(NCAM) (100%), synaptophysin (65%–88%), and chrom-ogranin (60%–88%).84–87 Expression of the more specificneuroendocrine markers, including chromogranin andsynaptophysin, may diminish in less differentiated tu-mors.87
The following markers, which are negative in neuro-blastoma, can help differentiate this tumor from EWS/PNET (CD99�), SmCC (CK�), lymphoma (CD45�), mela-noma (S100�), and RMS (positive myogenous mark-ers).42,84,85 Because up to 35% of olfactory neuroblastomasmay be CK positive,88,89 a concomitant negative EMA mayhelp differentiate them from SmCC. Although the tumorcells are negative for S100 protein, the presence of S100-positive dendritic cells around lobules of tumor cells is ahelpful immunohistochemical feature.
Small Cell CarcinomaSmall cell carcinomas (poorly differentiated neuroen-
docrine carcinomas) represent poorly differentiated neu-roendocrine neoplasms with an epithelial lineage. Theymay originate from a variety of locations, most commonlythe lung but also from extrapulmonary sites, includingnasal cavity and paranasal sinuses, breast, uterine cervix,bladder, prostate, gastrointestinal tract, pancreas, thyroid,adrenal gland, skin (Merkel cell carcinoma), and salivaryglands. The histopathologic features of these tumors, re-gardless of the site of origin, are nearly identical.
The immunodiagnosis of SmCCs rests on the immu-nohistochemical proof of a simultaneous epithelial andneuroendocrine differentiation. The former is reflected byreactivity for keratin, especially LMW CKs (CK8 andCK18),57,90 and the latter by a positive neuroendocrinepanel, which in order of increasing specificity includesNSE, CD56 (NCAM), synaptophysin, and chromogran-in.91,92 Against a common histologic and immunohisto-chemical background, SmCC from different organs maydisplay additional immunophenotypes that help deter-mine the primary site, because not infrequently these tu-mors present as metastases of unknown origin. For ex-ample, among SmCCs from different sites, including gas-trointestinal origin, CK20 is positive only in Merkel cellcarcinomas (�97%)93,94 and salivary gland SmCCs(�60%),93,95 often with a distinct paranuclear punctate pat-tern (Figure 8). Another example is positive reaction for
estrogen receptor (ER) and progesterone receptor (PR),which is seen in two thirds of mammary SmCCs accord-ing to 1 report.96 Although immunoreactivity for steroidhormone receptors, especially PR, has been occasionallyobserved in neuroendocrine tumors from various primarysites,97,98 unlike breast, simultaneous expression of ER andPR is unusual for them.
Thyroid transcription factor 1 (TTF-1) is a sensitivemarker for lung SmCC (positive in 80%–100%)99–102; how-ever, TTF-1 expression has been also observed in variousextrapulmonary SmCCs in several settings (11%–80%).99–101,103
TTF-1, therefore, should not be considered as a sole deter-minant in distinguishing extrapulmonary SmCC from itspulmonary counterpart. TTF-1 expression, however, isconsistently negative in Merkel cell carcinoma.100,103
One distinctive example of organ-specific SmCC is thatfrom the ovary. There are 2 distinct types of ovarianSmCC. One is the neuroendocrine type, which is morpho-logically and immunohistochemically indistinguishablefrom the pulmonary SmCC. The second is the hypercal-cemic type, which has a distinctive immunoprofile, dis-similar to that of traditional SmCC, characterized by pos-itive reactivity for CK, calretinin, CD10, N-terminal ofWT1, p53, and occasionally parathyroid hormone; nega-tive staining for chromogranin, CD99, desmin, inhibin,S100, and TTF-1; and variable reaction for other neuro-endocrine markers.104,105
One should be aware that extrapulmonary SmCCs donot consistently express the specific antigens of the organsof their origin. For instance, SmCCs of the prostate arenegative for prostate-specific antigen (PSA) and prostateacid phosphatase (PAP),106 and those of the urinary blad-der are negative for thrombomodulin, uroplakin III, high-molecular-weight cytokeratin (HMW CK), and CK20.107 Apositive CDX2, although specific to tumors of intestinalorigin, is seen in only 20% of SmCCs of the colon.108
Sinonasal undifferentiated carcinoma, a rare, highly ag-gressive tumor type arising in the nasal cavity and para-nasal sinuses, should be considered in the differential di-agnosis of both SRCTs and undifferentiated large carci-nomas in the head and neck region. These tumors are gen-erally positive for CKs but exclusively for CKs of simpleepithelia, such as CK8 (100%), CK19 (50%), and CK7(50%), and as such are negative for CK5/6.109 They stainvariably for EMA (18%), NSE (18%), and CD99 (14%) butare typically negative for chromogranin and synaptophy-sin.110
Hematopoietic MalignanciesA dense infiltrate of relatively small undifferentiated
cells of uncertain origin may be the first presentation of ahematolymphoid malignancy. As stated previously, be-cause lymphoblastic lymphomas may not expressCD45,30,32,111 a negative CD45 (LCA) does not totally ex-clude the possibility of hematopoietic malignancies. Nu-clear staining for terminal deoxyribonucleotide transferase(TdT), which is a sensitive marker for both T- and B-pre-cursor lymphoid cells, on the other hand, is consideredthe hallmark of lymphoblastic lymphoma. The majority(85%–90%) of lymphoblastic lymphomas derive from pre-cursor T cells, and the rest originate from immature Bcells.18 CD43 is a sensitive, although not a specific, T-cellmarker. Cytoplasmic CD3 (not surface CD3) is also fre-quently expressed by T-precursor lymphoblasts. CD79a isa more sensitive marker for detection of immature B cells

Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al 333
Table 3. Tumor-Specific Markers and Their Staining Pattern*
Marker Tumor Staining Pattern
TTF-1 Lung, thyroid NuclearThyroglobulin Thyroid CytoplasmicHepPar-1 Hepatocellular CytoplasmicCDX2 Colorectal/duodenal NuclearVillin Gastrointestinal (epithelia with brush border) ApicalER/PR Breast, ovary, endometrium NuclearGCDFP-15 Breast CytoplasmicMammaglobin Breast CytoplasmicRCC marker Renal MembranousPSA Prostate CytoplasmicPAP Prostate CytoplasmicUroplakin III Urothelial MembranousInhibin Sex cord–stromal, adrenocortical CytoplasmicMelan-A Adrenocortical, melanoma CytoplasmicCalretinin Mesothelioma, sex cord–stromal, adrenocortical Nuclear/cytoplasmicWT1 Ovarian serous, mesothelioma, Wilms, desmoplastic small round cell NuclearMesothelin Mesothelioma Cytoplasmic/membranousD2-40 Mesothelioma, lymphatic endothelial cell marker Membranous
* TTF-1 indicates thyroid transcription factor 1; HepPar-1, hepatocyte paraffin 1; ER/PR, estrogen receptor/progesterone receptor; GCDFP-15,gross cystic disease fluid protein 15; RCC, renal cell carcinoma; PSA, prostate-specific antigen; and PAP, prostate acid phosphatase.
compared with CD20. Thus, if lymphoblastic lymphomais suspected, the panel should include TdT, CD43, andCD79a, in addition to CD45.
Myeloid (granulocytic) sarcomas with little or no evi-dence of myeloid differentiation may manifest as undif-ferentiated tumors, sometimes with small round cell mor-phology. A high index of suspicion is often required toavoid diagnostic overlook of these malignancies. Myelo-blasts are usually positive for CD45 (in 75% of cases),CD43 (100%), myeloperoxidase (variably), and lysozyme(variably) but are generally negative for B- and T-lineagemarkers, including CD79a and CD3, respectively.112
As mentioned previously, most lymphoblastic lympho-mas45,111 and a large fraction of myeloid sarcomas46 expressCD99. However, application of lymphoid markers usuallyhelps to distinguish hematolymphoid malignancies fromEwing sarcomas, which are negative for these markers.
Malignant MelanomaIn keeping with various cytomorphologic and architec-
tural manifestations of malignant melanoma (MM), itssmall cell (neuroendocrine-like) variant, which occursmore commonly within the nasal cavity and paranasal si-nuses,26 is a differential diagnostic consideration forSRCTs. Because melanoma with small cell morphology of-ten lacks melanin pigment, immunohistochemistry playsan important role in its recognition.
The immunoprofile of MM is discussed in more detaillater in the section on tumors with overlapping histologicfeatures. Herein the potential for expression of aberrantmarkers in small cell melanoma as a source of diagnosticconfusion with other SRCTs is highlighted. These includeCD99 in rare to up to 60% of cases,113,114 WT1 (cytoplasmicbut not nuclear pattern) in as many as 70%,115 CD10 in40% to 50%,116,117 CD68 (a histiocytic marker) in 86%,118
NSE in approximately 50%,113 and neuroendocrine mark-ers (CD56, CD57, and synaptophysin) in up to 13%.113
Chromogranin, on the other hand, is consistently absentin melanocytic tumors.119
UNDIFFERENTIATED ‘‘CARCINOMATOUS’’ TUMORSUndifferentiated tumors with a carcinomatous appear-
ance are characterized by large round-oval to polygonal
cells with a nesting arrangement. These histologic attri-butes, however, are not specific to carcinomas and may bemimicked by other tumors, including sarcomas with epi-thelioid appearance, melanoma, and hematopoietic malig-nancies. Screening panel for major lineage determination(see previous discussion) is essential for clarification of thetrue identity of these tumors.
Tissue- or Organ-Specific DeterminationOnce the diagnosis of carcinoma by broad lineage
markers is established, immunohistochemistry may assistfurther by delineation of the cell line of differentiation.This is achieved by analysis of CK subtypes and othercomplementary or tissue- or organ-specific markers (Table3). Although some markers are expressed almost exclu-sively in a specific tissue, for example, PSA and PAP forprostate and uroplakin III for urothelial epithelium, othersare not strictly organ or tissue specific but may help focusthe diagnosis to a specific area.
It should be mentioned that because most reports onthe sensitivity and specificity of markers in the literatureare derived from studies that encompassed primary andmetastatic tumors of various grades, it is difficult to ex-trapolate those parameters exclusively in respect to un-differentiated or poorly differentiated forms of tumors.Nevertheless it can be concluded from the literature thatfor most entities, the sensitivity of tissue-specific markersdeclines as the tumor grade increases. Also, although theantigenic expression of some markers appears to be robustduring metastasis, for example, CDX2 for colorectal car-cinoma, others, such as the renal cell carcinoma (RCC)marker, tend to reduce their sensitivity in metastatic sites.
CK Profile. The CK phenotype often provides helpfulclues in determination of the cell line of differentiation inboth primary and metastatic carcinomas. This reflects theobservation that tumors tend to recapitulate the CK profileof the normal cells from which they are derived. Althoughmetastatic tumors may gain or lose antigens comparedwith primary tumors, their CK profiles usually remain thesame, as demonstrated by a number of studies, includinga comprehensive study of CK7 and CK20 for 384 primarytumors and their metastasis120 and other studies focusingon CK20 expression by primary and metastatic colorectal

334 Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al
Figure 9. Algorithmic immunohistochemical analysis of undifferentiated carcinomas. CA indicates carcinoma; adenoCA, adenocarcinoma; SmCC,small cell carcinoma; SCC, squamous cell carcinoma; RCC, renal cell carcinoma; HCC, hepatocellular carcinoma; ¶, seminoma is keratin negative,OCT3/4 positive; *NE markers, neuroendocrine markers, including synaptophysin, chromogranin, and CD56; �, undifferentiated anaplastic thyroidcarcinoma is often negative for thyroid transcription factor 1 (TTF-1) and thyroglobulin; and , characteristic canalicular pattern.
carcinoma.94,121,122 Coordinate expression of CK7 and CK20defines subsets of carcinomas, as shown in Figure 9.
The CK7/CK20 phenotype can be especially useful incertain clinical situations, including the differentiation be-tween prostate (CK7�/CK20�) and urothelial (CK7�/CK20 variable) carcinoma123 (Figure 10); poorly differen-tiated squamous (CK7�) and poorly differentiated uro-thelial (CK7�) carcinoma of the urinary bladder; and met-
astatic colorectal carcinoma (CK7�/CK20�) from primarynonmucinous ovarian carcinoma or primary endometrial,pulmonary, or mammary adenocarcinoma (CK7�/CK20�).122,124
Other CK subtypes may also have a role in defining thelineage of tumor; for example, CK19 combined with CK7helps to differentiate between hepatocellular carcinoma(HCC) (CK7�/CK19�) and bile duct carcinoma (CK7�/

Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al 335
Figure 10. Photomicrograph of urothelial carcinoma with positive staining for cytokeratin (CK) 7 (a) and CK20 (b) (original magnifications �20).
Figure 11. Photomicrograph of lung adenocarcinoma with diffuse nuclear staining for thyroid transcription factor 1 (original magnification �10).
Figure 12. Photomicrograph of epithelioid mesothelioma with nuclear and cytoplasmic staining for calretinin (original magnification �20).
Figure 13. Photomicrograph of seminoma, showing a diffuse strong nuclear staining for OCT3/4 (original magnification �20).
Figure 14. Photomicrograph of sarcomatoid carcinoma with cytokeratin expression in both sarcomatous and carcinomatous areas (original mag-nification �20).

336 Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al
Table 4. Carcinoembryonic Antigen (CEA)Immunostaining in Carcinomas
CEA Positive CEA Negative
Colonic/rectal adenocarcinoma Endometrial adenocarcinomaGastric and esophageal adeno-
carcinomaRenal cell carcinomaProstate adenocarcinoma
Pancreatic adenocarcinoma Ovarian serous carcinomaBiliary tract adenocarcinoma Adrenal carcinomaEndocervical adenocarcinoma MesotheliomaLung adenocarcinoma
CK19�).125 CK5/6 serves as a sensitive marker for squa-mous cell carcinoma (SCC) (CK5/6�) and epithelioid me-sothelioma (CK5/6�) and helps differentiate them frompulmonary adenocarcinoma (CK5/6�).124,126–129 CK5/6 alsolabels urothelial carcinoma (in 50%–63% of cases)124,126 andthe large cell undifferentiated lung carcinoma (vari-ably).126,130
Figure 9 provides a selected list of specific tumors withtheir pertinent positive and negative markers, categorizedaccording to their CK7/CK20 profile. The choice of tissue-specific markers to be included in an investigative panelis largely determined by the clinical impression, site ofpresentation, and the CK7/CK20 expression of an undif-ferentiated carcinoma.
Carcinoembryonic Antigen. Carcinoembryonic anti-gen (CEA) is an oncofetal glycoprotein overexpressed bya variety of adenocarcinomas and consistently by gastro-intestinal adenocarcinomas.131,132 Table 4 summarizes re-activity for CEA in a variety of carcinomas. Use of CEAin a panel may especially assist in certain differential di-agnostic considerations, for example in the distinction ofendocervical (CEA positive) over endometrial (CEA neg-ative) adenocarcinoma133 or in the recognition of poorlydifferentiated colonic adenocarcinoma (CEA positive)from solid areas of ovarian serous adenocarcinoma (CEAnegative).132
Polyclonal CEA (pCEA) antibodies, in contrast to CEA-specific monoclonal antibody, have cross reactivity withCEA-related antigens, including biliary glycoprotein anti-gen. Hepatocellular carcinoma is negative for monoclonalCEA but expresses a characteristic bile canalicular stainingpattern with pCEA134 because of cross reactivity with bil-iary glycoprotein antigen. Carcinoembryonic antigen isalso frequently used as a negative marker in the mesothe-lioma panel.
MOC-31. MOC-31 is a cell surface glycoprotein large-ly found on the epithelial cells. MOC-31 helps differentiatebetween adenocarcinoma (MOC-31 positive) and meso-thelioma (MOC-31 negative).135,136 MOC-31 is also usefulin the recognition of cholangiocarcinoma and other met-astatic adenocarcinomas (MOC-31 positive) from HCC(MOC-31 negative).137
p63. p63, a p53 homologue, is a marker for basal cellsand helps maintain basal cells in squamous and other ep-ithelial linings.138 p63 stains the vast majority of SCCs(�97%) and, in addition to CK5/6, is recognized as agood marker for SCC, especially the poorly differentiatedforms.102,139–142 Thus, a combined p63�/CK5/6� immuno-profile in a poorly to undifferentiated carcinoma is highlypredictive of a squamous origin.139 Because urothelial car-cinoma also expresses p63 (in 70%–95% of cases) andCK5/6 (50%–63%),126,143 a p63�/CK5/6� immunoprofilecould also suggest a urothelial carcinoma. The 2 entities
are nevertheless distinguished based on their different co-ordinate CK7/CK20. p63 expression in the lung, however,is not specific to SCC; thus, a subset of adenocarcinomas(30%) and large cell carcinomas (37%), 50% of large cellneuroendocrine carcinomas (particularly higher-grade tu-mors), and a variable proportion of SmCCs (0%–77%)stain for p63.140,142 Because p63 is consistently negative inmesothelioma, it can assist in differentiating SCC of thelung from epithelioid mesothelioma.127,139
Neuroendocrine Markers. Neuroendocrine markersare tissue indicators of neuroendocrine neoplasms, includ-ing those with epithelial lineage (neuroendocrine carci-nomas) and those with neural derivation, such as para-ganglioma/pheochromocytoma and neuroblastoma.
The 2 most reliable markers of neuroendocrine neo-plasms, synaptophysin and chromogranin, have a com-parable sensitivity; thus, they are always used together ascomplementary reagents for neuroendocrine lineage de-termination. CD56 is generally regarded as a broad-spec-trum neuroendocrine marker and perhaps the most sen-sitive144,145 and is instrumental in confirming the diagnosisof neuroendocrine tumors in small biopsies.144–146 CD56,however, is not specific for neuroendocrine delineation be-cause it may label occasional nonneuroendocrine tissuesand their malignant counterpart (eg, follicular and pap-illary thyroid, renal cell, and hepatocellular carcinoma),natural killer cells, some T-cell lymphomas, and a largenumber of SRCTs.92,147 Neuron-specific enolase suffers apoor specificity for neuroendocrine tumors, and, as such,it is not used as a sole determinant of neuroendocrinedifferentiation.
An undifferentiated carcinoma may turn out to have anoccult neuroendocrine differentiation, disclosed by im-munostain. Although neuroendocrine markers are notusually included in the initial diagnostic panel for an un-differentiated tumor, detection of neuroendocrine differ-entiation is clinically significant, because this may implyprognosis and therapy similar to those for SmCC.148,149 Be-cause positive staining in a few tumor cells is frequent inany undifferentiated carcinoma, the diagnosis of neuro-endocrine carcinoma should only be made if the stain isunequivocal and, in our experience, present in at least 20%of the tumor cells.
In the lung, large cell neuroendocrine carcinoma mustbe differentiated from basaloid carcinoma. Because oftheir overlapping H&E morphology, the differential di-agnosis is often difficult but can be facilitated by theirspecific immunoprofiles. Basaloid carcinoma is negativefor neuroendocrine markers and TTF-1 and positive forHMW CK, whereas large cell neuroendocrine carcinomais consistently positive for neuroendocrine markers, posi-tive for TTF-1 in about 50% of cases, and often negativefor HMW CK.103,150,151
Thyroid Transcription Factor 1. TTF-1 is a nucleartranscription factor that promotes embryogenic pulmo-nary and thyroid differentiation and is expressed by most,but not all, lung or thyroid neoplasms. Although 80% to100% of SmCCs and 96% to 100% of adenocarcinomasfrom lung express TTF-1 (Figure 11), pulmonary SCCs arenegative in most cases.99–103,150,152,153
Furthermore, TTF-1 expression tends to decrease inpoorly differentiated (50% positive) compared with well-differentiated (100% positive) adenocarcinomas,153 dimin-ishing the sensitivity of this marker for identification ofthe pulmonary origin of a poorly differentiated adenocar-

Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al 337
cinoma. Among thyroid carcinomas, undifferentiated an-aplastic thyroid carcinomas are unfaithful in terms of TTF-1 expression (positive in �5%).154 TTF-1, as mentioned pre-viously, may also be expressed in SmCCs arising from avariety of locations other than the lung99,101,103,155 (see also‘‘Small Cell Carcinoma’’).
Thyroglobulin. Thyroglobulin is a very specific mark-er for thyroid follicular and papillary carcinomas but onlyrarely stains cells in undifferentiated anaplastic thyroidcarcinoma.154,156 Anaplastic thyroid carcinomas are gener-ally positive for vimentin and CK157,158 but are negative forCEA,157 TTF-1,154 and melanocytic, vascular, myogenous,and lymphoid markers.
Hepatocyte Paraffin 1. Hepatocyte paraffin 1 (HepPar-1) is a monoclonal antibody that stains a cellular antigenof unknown function of normal hepatocytes and is knownto be a highly sensitive (positive in �90% of cases) andrelatively specific marker for HCC.159–164 HepPar-1 expres-sion, however, decreases in HCC with higher nucleargrade.164 HepPar-1 is occasionally observed in nonhepaticcarcinomas, including those of gastrointestinal origin, inparticular gastric signet ring cell carcinoma (47%–83%),and rarely in other tumors.159,163–165
The distinction of HCC, especially its poorly differen-tiated forms, from metastatic adenocarcinoma and cholan-giocarcinoma is commonly a diagnostic challenge. A panelthat includes HepPar-1, MOC-31, pCEA, and CD10, in ad-dition to CK7 and CK20, is often helpful in making theaccurate diagnosis. The immunoprofile of HCC includesCK7�/CK20�, HepPar-1 positive, MOC-31 negative, sinu-soidal cell CD34�, and a canalicular pattern of positiveimmunostaining with both pCEA and CD10.134,160,161,166
Metastatic adenocarcinoma and cholangiocarcinoma, onthe other hand, are generally MOC-31 and CEA positive,the latter with a membrane/cytoplasmic staining pattern.The canalicular staining pattern with antibodies to CD10,positive in 68% of HCC, is distinct from the membrane orcytoplasmic staining seen in RCC.166
CDX2. CDX2, an intestine-specific transcription fac-tor, is a sensitive and specific marker for colorectal andduodenal adenocarcinomas in both primary and meta-static sites.167–169 However, CDX2 expression tends to de-cline in the higher grade and stage of colorectal tumors(positive in only 56% of poorly differentiated tumors)169
and is practically absent in an undifferentiated subset oflarge cell colonic carcinoma, usually associated with DNAmismatch repair defects.170 CDX2 is variably expressed inother adenocarcinomas of the digestive tract, includinggastric (55%–70%), esophageal (67%), pancreatic (32%–60%), and biliary (25%–60%).163,167
CDX2 is also observed in a few extraintestinal carcino-mas. For example, 47% to 100% of primary adenocarci-nomas of the bladder168,171 and 10.5% to 100% of ovariancarcinomas, particularly the mucinous type, are positivefor CDX2.167–169 Because bladder adenocarcinoma also dis-plays a ‘‘urothelial’’ profile (CK7, 65% positive; CK20, 53%positive; and thrombomodulin, 59% positive),172 it may bedifferentiated from metastatic colorectal carcinoma by im-munohistochemistry.
Villin. Villin is a cytoskeletal protein associated withbrush border microvilli of the intestine and proximal renaltubular epithelium. Villin is a sensitive marker of gastro-intestinal adenocarcinomas, staining 82% to 100% of pri-mary and metastatic colonic adenocarcinomas.168,173,174 Vil-lin expression does not seem to be associated with the
state of tumor differentiation.173 Villin, however, also stainsa number of extragastrointestinal adenocarcinomas, in-cluding some adenocarcinomas of ovary, endometrium,kidney, and bladder.171,173,175 Villin expression in lung ade-nocarcinoma correlates with the presence or absence ofmicrovilli (positive in 67% and 10% of cases, respective-ly).174
ER and PR. The role of ER and PR in determining theprimary site in undifferentiated tumors is hampered by awide spectrum of expression among a variety of tumors.Although ER and PR expression is expected to be associ-ated with hormone-responsive organs and their neo-plasms, such as breast, ovary, and endometrium,176 thereare frequent examples of unexpected ER or PR expressionreported in a variety of other tumors, including thosefrom lung,98,177–179 thyroid,180 stomach,181 and some neuro-endocrine tumors.97 Furthermore, given that many high-grade carcinomas arising from hormone-responsive or-gans such as breast lack ER expression, we discourage solereliance on ER and PR as determinants of the site of tumororigin, except in selected differential diagnoses and incombination with other immunomarkers. An example ofthe utility of ER in a diagnostic panel is its applicationcombined with CEA133 and vimentin in the distinction ofan endometrial (vimentin�/ER�/CEA�) from an endocer-vical (vimentin�/ER�/CEA�) adenocarcinoma.
Gross Cystic Disease Fluid Protein. Gross cystic dis-ease fluid protein 15 (GCDFP-15), a 15-kd secretory gly-coprotein of various body fluids, including saliva, milk,and seminal fluid, is considered a marker of apocrine dif-ferentiation182,183 with high specificity for breast carcino-mas.184–186 In a study of 328 metastatic adenocarcinomas,Kaufmann et al184 demonstrated that expression ofGCDFP-15 and/or ER or PR had a sensitivity of 83%, aspecificity of 93%, and a predictive accuracy of 92% forcarcinomas of the breast against all other carcinomas ex-cluding ovarian carcinomas. In another study, including105 breast cancers and 585 nonmammary malignancies,GCDFP-15 was able to identify breast carcinomas with asensitivity of 74% and a specificity of 95%.185 Other tumortypes with occasional GCDFP-15 expression include car-cinomas of the salivary glands, sweat glands, and pros-tate.185,187 Although a very specific marker, GCDFP-15 isnot a particularly sensitive marker of breast carcino-ma.188,189 It is uncertain whether GCDFP-15 expression de-clines in poorly differentiated forms of mammary carci-noma.
Mammaglobin. Mammaglobin, a mammary-specificmember of the uteroglobin family, is overexpressed in hu-man breast carcinoma. Mammaglobin expression has beenobserved in 48% to 84% of breast carcinoma and in 8% to15% of carcinomas not from breast, including salivarygland tumors (55%) and endometrial carcinoma (13%).188–190
Although mammaglobin appears to be a more sensitivemarker than GCDFP-15, it is not as specific as GCDFP-15for breast carcinoma.188 The predictive value of a com-bined mammaglobin and GCDFP-15 panel for mammarycarcinomas in tumors of unknown origin needs to be in-vestigated.
RCC Marker. Renal cell carcinoma marker, a mono-clonal antibody against a normal human proximal tubularbrush border glycoprotein known as gp200, decorates con-ventional and papillary RCCs with an approximate sen-sitivity of 85% and more than 95%, respectively.191,192
Among nonrenal carcinomas, a subset of breast (29%) and

338 Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al
embryonal carcinoma (28%) may stain with RCC mark-er.191 The sensitivity of RCC marker tends to decline fromlow-grade (92%) to high-grade (75%) conventionalRCCs.192 In addition, only 25% of sarcomatoid RCCs stainfor this marker.191
Although RCC marker remains highly specific (98%) formetastatic RCC, because of a rather low sensitivity in met-astatic sites (positive in 67%), a negative result does nottotally rule out metastatic RCC.191 Negative vimentin andCD10, however, enhances the negative predictive value forconventional RCCs in an investigative panel for metastatictumors. CD10, similar to vimentin, is a nonspecific markerfor RCCs. It is, however, a relatively sensitive indicator forRCCs and stains approximately 90% of these tumors witha diffuse cytoplasmic or membranous pattern.117 The dis-tribution of CD10 appears to be independent of the gradeor histologic type (conventional vs papillary) of theRCC.192
PSA and PAP. Immunostain for the prostate-specificmarkers PSA and PAP, 2 glycoproteins produced almostexclusively by the prostatic glandular epithelium, is wide-ly used for determination of the prostatic origin of meta-static tumors. Genega et al193 demonstrated a sensitivity of94% for intermediate- to high-grade prostate adenocarci-nomas (Gleason score �8) with both PSA and PAP. Pros-tate-specific antigen expression has been rarely reportedin some nonprostatic tissues and tumors, including sali-vary gland, breast, and gynecologic tumors.194–197
Prostate-specific antigen and PAP expression tends todecrease in higher grade prostate adenocarcinomas.198,199
In a study of 225 prostate adenocarcinomas by Gold-stein,200 all tumors with a Gleason score of 6 or 7 werereactive for PSA, whereas 13% of the adenocarcinomaswith a Gleason score of 10 were nonreactive. Althoughsome investigators found PAP slightly more sensitive thanPSA in diagnosing poorly differentiated prostatic adeno-carcinoma,200,201 others could not confirm these find-ings.199,202 Nevertheless, a combined immunostain for PAPand PSA would be expected to detect most prostatic ad-enocarcinomas in metastatic sites.199,203
Parenthetically, -methylacyl-CoA racemase (AMACR)encoded by the gene P504S, which is a highly specific andsensitive marker for prostatic carcinoma in prostatic spec-imens,204 has limited value in detecting metastatic prostatecancer because it is also expressed in various normal tis-sues and nonprostatic tumors.205
Thrombomodulin. Thrombomodulin, a cell surfaceglycoprotein involved in the regulation of intravascular co-agulation, is expressed in 70% to 90% of primary or met-astatic urothelial carcinomas.107,206,207 Thrombomodulin,however, is also expressed by a variety of nonurothelialtumors, including SCC (majority) and endothelial vasculartumors.207 Thrombomodulin is additionally known as apositive mesothelioma marker, although not as specific orsensitive as the other markers discussed later.128–130,208
Uroplakin III. Uroplakin III, expressed by terminallydifferentiated superficial urothelial cells, is a highly spe-cific marker for urothelial origin of tumors.107,209 Thismarker, however, is not quite sensitive for urothelial car-cinomas; thus, it is expressed in up to 60% of urothelialcarcinoma in primary sites and slightly less frequently inmetastases (�50%).107,209
The differential diagnosis between a poorly differenti-ated prostate adenocarcinoma involving the bladder anda high-grade urothelial carcinoma with prostatic extension
can be very challenging. This challenge, which is usuallysolved by careful cytomorphologic evaluations (monoto-nous tumor cells, prominent nucleolus, and less mitosesfor prostate cancers), may be facilitated by a panel thatincludes a number of discriminatory markers, in additionto CK profile, including PSA and PAP, markers of prostateadenocarcinoma, and HMW CK, p63, uroplakin III, andthrombomodulin, markers that are expected to be positivein urothelial carcinoma.210,211
Inhibin. Inhibin is a peptide hormone produced byovarian granulosa cells and testicular Sertoli cells. It servesas a sensitive and highly specific marker for ovarian andtesticular sex cord–stromal tumors.21–215 Inhibin is also asensitive marker for adrenal cortical neoplasms and reli-ably differentiates cortical from medullary adrenal tu-mors.216–218
Melan-A. Melan-A, a product of MART-1 gene, is anantigen on melanoma cells that is recognized by the an-tibody A103. Although Melan-A is essentially used as amelanoma marker,219 it is also a sensitive marker for ad-renal cortical neoplasms220 and, similar to inhibin and cal-retinin, a specific marker in differentiating cortical frommedullary adrenal tumors.216 Melan-A is additionally ex-pressed by perivascular epithelioid cell tumors (PECo-ma).219,221
Calretinin. Calretinin is a good marker for malignantmesothelioma with a sensitivity approaching 100%.127,128,208,222
It is also quite specific for mesothelioma against adeno-carcinomas, which are positive for it in only 8% to 11% ofcases.128,130,208,222 Calretinin decorates both mesothelial cellsand malignant mesothelioma with both nuclear and cy-toplasmic staining223 (Figure 12).
Calretinin additionally serves as a highly sensitivemarker for sex cord–stromal tumors. It is, however, not asspecific as inhibin in this respect because it also labels afraction of ovarian epithelial neoplasms (22%).215,224,225 Likeinhibin and Melan-A, calretinin also stains adrenal corti-cal neoplasms and discriminates them from adrenal med-ullary tumors.216
Mesothelin. Mesothelin is a cell surface antigen thatis strongly expressed in normal mesothelial cells, meso-theliomas, and a number of other carcinomas.226 Althougha highly sensitive marker for mesothelioma, mesothelinmay also be present in approximately half of the lung ad-enocarcinomas130,226; as such, it has limited value in dis-criminating between the 2 entities. Carcinomas with con-sistently strong exhibition for mesothelin include non-mucinous carcinomas of the ovary and adenocarcinomasof the pancreas and ampulla of Vater.226
WT1. WT1, in addition to its diagnostic utility forSRCTs (see ‘‘Small Round Cell Tumors’’), is a sensitivemarker for epithelioid mesothelioma, successfully discrim-inating it from adenocarcinoma.128,227 Another epithelialtumor strongly positive for WT1 is ovarian serous carci-noma, which is positive in nearly all cases including thehigh-grade forms.228 Because both peritoneal mesothelio-ma and ovarian serous carcinoma metastatic to the peri-toneum express WT1, additional markers are needed fortheir differential diagnosis: A panel including calretinin,Ber-EP4, ER, and PR is helpful in differentiating mesothe-lioma (calretinin�/Ber-EP4�/ER�/PR�) from primary ormetastatic serous ovarian carcinoma (calretinin�/Ber-EP4�/ER�/PR�).229
Other Mesothelioma Markers. Immunohistochemis-try has a crucial role in the differential diagnosis between

Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al 339
malignant epithelioid mesothelioma and adenocarcinomametastatic to the serous membranes. A number of discrim-inatory markers are available to facilitate this recognition.It is generally recommended to include at least 2 positiveand 2 negative markers in the differential panel for me-sothelioma.
Calretinin, WT1, and CK5/6 (discussed earlier) are es-tablished as highly reliable positive mesothelioma mark-ers.128 Other positive markers include mesothelin andthrombomodulin (discussed earlier). In addition, D2-40,230
a lymphatic endothelial marker, and h-caldesmon,231 a spe-cific marker for smooth muscle tumors, have recently beenshown to be valuable in discriminating mesotheliomafrom lung adenocarcinoma. On the other hand, CEA,MOC-31, Ber-EP4, BG-8, and B72.3128,129 are accepted asreliable negative markers for discriminating epithelioidmalignant mesothelioma from pulmonary adenocarcino-ma.
CD5. CD5 is a useful marker of primary thymic car-cinomas, expressed in neoplastic epithelial cells of the thy-mic carcinoma but typically not in thymoma or other car-cinomas involving the mediastinum.232–234 Of the 2 usedclones of anti-CD5 antibody, clone CD5/54/B4 identifies30% to 67% of thymic carcinomas.235,236 The other clone,NCL-CD5-4C7, although more sensitive for thymic carci-nomas (45%–100% positive), also labels other neoplasmsoccasionally.233–235
Markers of GCTs. Germ cell tumors sometimes pre-sent as undifferentiated metastatic carcinomas. Accuraterecognition of these tumors is of utmost importance be-cause of the available effective therapy. Placental alkalinephosphatase is consistently present in embryonal carci-noma and seminoma and variably in several other GCTs,including yolk sac tumor and choriocarcinoma.237,238 Pla-cental alkaline phosphatase immunoreactivity, however, isnot completely specific to GCTs, as it has been seen insome soft tissue tumors with known myogenic differen-tiation.239
OCT3/4, also known as POU5F1, is a transcription fac-tor and a robust diagnostic marker for seminoma (Figure13) and embryonal carcinoma in both primary and met-astatic sites.240–242 Seminoma also stains consistently withD2-40. Yolk sac tumor does not express OCT3/4 but ispositive for -fetoprotein, albeit with a patchy stainingpattern. Human chorionic gonadotropin is consistently ex-pressed by syncytiotrophoblasts of choriocarcinomas.
UNDIFFERENTIATED ‘‘SARCOMATOUS’’ OR‘‘SARCOMA-LIKE’’ TUMORS
In the approach to undifferentiated tumors with sarco-matous appearance, exclusion of nonmesenchymal neo-plasms such as sarcomatoid carcinoma and sarcomatoidmesothelioma and other mimickers, for example, spindlecell melanoma or hematopoietic malignancies with sar-comatous feature, is essential. The distinction is usuallyattained by using the screening panel previously dis-cussed in the introduction.
Undifferentiated High-Grade SarcomasOnce the true sarcomatous nature of an undifferentiated
tumor is established, investigation for a specific mode ofdifferentiation, that is, neural, myogenous, lipomatous, orvascular lineage, should be implemented.
Fletcher243 demonstrated that among 159 neoplastic le-sions initially diagnosed as pleomorphic sarcoma, 63%
could be reclassified as specific types of sarcoma after im-plementing further studies, including combined immu-nohistochemistry and electron microscopy. Coindre et al244
showed that among 25 tumors initially diagnosed as ret-roperitoneal malignant fibrous histiocytoma (MFH), 17could be reclassified as dedifferentiated liposarcoma byextensive sampling, combined with immunohistochemis-try and comparative genomic hybridization. These dis-tinctions are important above the academic interest inview of their variable prognostic implications.245
It is emphasized that ancillary tests do not replace prop-er tumor sampling, which often helps detect tumor fociwith features suggestive of or diagnostic for a specific lineof differentiation. According to the report of the Interna-tional Chromosomes and Morphology (CHAMP) studygroup on 46 pleomorphic soft tissue sarcomas, it is un-likely that cytogenetic analysis, mainly because of the kar-yotype complexity of these tumors, can further improvetheir differential diagnostic subclassification.246
With the help of immunohistochemistry in conjunctionwith generous tumor sampling, a high-grade undifferen-tiated sarcoma can often be classified into one specific cat-egory of pleomorphic sarcomas, including pleomorphicleiomyosarcoma, pleomorphic RMS, pleomorphic and de-differentiated liposarcoma, osteosarcoma, pleomorphicmalignant peripheral nerve sheath tumor (MPNST), andPDSS.
The diagnosis of pleomorphic leiomyosarcoma requiresdemonstration of a positive reaction for smooth musclemarkers, including smooth muscle actin, muscle-specificactin, desmin, calponin, and h-caldesmon,246,247 in the pres-ence of at least focal supporting morphologic characteris-tics (eosinophilic spindle cells with vesicular blunt-endednuclei arranged in a fascicular pattern). The expression ofmyoid markers in the pleomorphic areas, compared withthe leiomyosarcomatous foci, is usually significantly re-duced.247 Among myoid markers, h-caldesmon appears tobe a promising reagent for specific smooth muscle differ-entiation that allows distinction of leiomyosarcoma fromother tumors with smooth muscle–like differentiation, in-cluding myofibroblastic tumors.248,249 However, only 40%of pleomorphic leiomyosarcoma are labeled with this an-tibody.247
The immunoprofile of pleomorphic RMS includes ex-pression of muscle-related antigens, that is, desmin, myo-globin, and actin,250 along with a diffuse reaction with atleast one skeletal muscle–specific marker including my-ogenin and Myo-D1.251 The staining pattern for skeletalmuscle markers in pleomorphic RMS is typically diffuse,which should be distinguished from focal staining seen ina variety of sarcomas with limited areas of rhabdomy-omatous differentiation.
The diagnosis of liposarcomas, until a specific lipoblastmarker is discovered, continues to be made essentially onthe basis of the H&E light microscopy. Although normalfat cells are positive for S100, neoplastic adipocytes staininconsistently.252 S100 labels lipoblasts in up to half ofpleomorphic liposarcomas,253–255 but nonlipogenic areasonly rarely stain with S100.253,256 The aP2 gene product(aP2 protein) has been suggested as a relatively specificmarker for lipoblasts in all types of liposarcoma.257 Thismarker also stains brown fat cells but reportedly not be-nign adipocytes or cells of other mesenchymal or epithe-lial tumors.257 Because of the paucity of pertinent studies,the diagnostic value of this marker remains to be deter-

340 Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al
mined. Positive immunostainings for MDM2 and CDK4,which correlate with amplification of these genes in de-differentiated liposarcomas, may help differentiate dedif-ferentiated liposarcomas from poorly differentiated sar-comas.258
The diagnosis of osteosarcoma is essentially renderedat the H&E light microscopic level by demonstration ofbone or lacelike osteoid associated with malignant cells.Osteocalcin, which seems to specifically highlight the os-teoid and the cytoplasm of osteoblasts (90%–100% specif-ic),77,78 may be potentially helpful in the diagnosis of os-teosarcoma in small biopsy material in the absence of rec-ognizable osteoid. Notably, osteosarcomas can be immu-noreactive for actin and rarely for epithelial markers.
The diagnosis of pleomorphic MPNST is immunohis-tochemically supported by demonstration of nerve sheathdifferentiation by a number of neural markers includingS100, Leu-7 (CD57), myelin basic protein, and proteingene product 9.5.259,260 The coexpression of these antigensis more reassuring for the diagnosis because none of themin isolation is specific for nerve sheath tumors.259 A focalstaining for S100 is seen in most MPNSTs (50%–60%),259,261
yet many high-grade MPNSTs display a decreased or neg-ative reactivity for S100 and CD57.262
The diagnosis of high-grade spindle cell variant of PDSSis supported by demonstration of positive reaction forEMA, keratin and its subsets (CK7 and CK19), Bcl-2 an-tigen, and CD9947–49,261 and negative staining for S100 andCD34. In questionable cases, molecular testing may be re-quired for definitive diagnosis.
Pleomorphic MFH or undifferentiated high-grade pleo-morphic sarcoma is a group of pleomorphic sarcomas thatdo not demonstrate a definitive line of differentiation evenwith the application of immunohistochemistry. Malignantfibrous histiocytoma is therefore a diagnosis of exclusion,which is made in the absence of reaction with any lineage-selective markers in a high-grade pleomorphic sarcoma.With current advances in diagnostic techniques, it is ex-pected that the number of tumors diagnosed as MFH willbe progressively smaller. Because a number of nonmesen-chymal neoplasms may impart an MFH-like morphology,exclusion of these entities by immunohistochemistry is in-evitable. Although keratin may stain a minor portion (upto 25%) of pleomorphic MFHs, the staining is often weakand focal.55,263,264 The tumor cells may be focally positivefor smooth muscle actin or muscle-specific actin, but theyare generally negative for desmin and S100. Rare desmin-positive cells in tumors with MFH-like morphologyshould not be regarded as evidence of myogenic differ-entiation.
Sarcoma-like TumorsSarcomatoid Carcinoma. Sarcomatoid (spindle cell)
carcinomas are a group of poorly to undifferentiated car-cinomas that contain a component of spindle cell differ-entiation with or without differentiated heterologous ele-ments, such as malignant cartilage, bone, or skeletal mus-cle.265,266 Some tumors are histologically biphasic with ob-vious sarcomatous and carcinomatous areas, whereasothers may show no obvious epithelial areas despite gen-erous sampling.266,267 In such instances, the sarcomatoidfoci are hardly distinguishable from true sarcomas at thelight microscopic level; therefore, immunohistochemistryplays a pivotal role in delineation of epithelial differenti-ation.
The tumor cells often coexpress CK (Figure 14) and vi-mentin.266,268–270 However, because of the varied and un-predictable CK immunoreactivity in sarcomatoid carci-nomas, multiple epithelial markers, including EMA andvarious CK subtypes, such as pancytokeratin, HMW CK(CK34�E12 or CK5/6), and CK7, may be necessary todemonstrate epithelial differentiation.267,269,270 Evaluation ofa number of alternative immunostains beyond the tradi-tional epithelial markers (CKs and EMA) in the sarco-matoid carcinomas of the head and neck, lung, and uri-nary bladder showed some values in exposing the epithe-lial identity of tumors in that setting by adding p63 in thepanel.271
Sarcomatoid Mesothelioma. Immunohistochemistryhas a limited role in the diagnosis of sarcomatoid meso-thelioma and its distinction from sarcomatoid carcinomasand sarcomas. Sarcomatoid mesothelioma shows amarked decline in the expression of epithelial and meso-thelial markers and has a wide immunophenotypic over-lap with sarcomas and sarcomatoid carcinomas.272–274 Only57.8% of sarcomatoid mesotheliomas stain for calretinin,39% for thrombomodulin, 25% for WT1, 19.6% for CK5/6, and 75% for keratin.272 On the other hand, up to 60% ofthem may stain for actin.273,274 It has been recently reportedthat a combination of calretinin and D2-40 improves thesensitivity for detecting mesothelioma in sarcomatoid ar-eas to 66%.275 Nevertheless, because of the lack of a specificmarker, the diagnosis of sarcomatoid mesotheliomashould be made after exclusion of alternative diagnosticentities and only with an integration of clinical, radio-graphic, gross, microscopic, and immunohistochemicalfindings.
Spindle Cell MM. When dealing with a malignantspindle cell tumor at any site, the possibility of spindlecell melanoma should always be considered. The sensitiv-ity of S100 protein in spindle cell MM appears to be moreor less similar to conventional MM,27 but HMB-45 expres-sion is less frequent (positive in �80% compared with90%–100% in the conventional type).26
Of note, the immunohistologic features of desmoplasticMM, a morphologic subtype of spindle cell MM associ-ated with pronounced desmoplasia, is substantially dif-ferent from conventional melanoma and includes positivestaining for S100 (in 94%) but lack of reactivity for HMB-45 or other melanoma-specific markers.27,276
TUMORS WITH OVERLAPPING HISTOLOGIC FEATURESTumors with nondescript H&E histology that fail to fit
into either a sarcoma or a carcinoma category often posethe greatest diagnostic challenge. The differential diag-nosis is broad and includes melanoma, hematopoietic ma-lignancies, neuroendocrine tumors, poorly differentiatedcarcinomas, and mesenchymal neoplasms with epithelioidappearance. Ancillary tests, including immunohistochem-istry, play an essential role in the recognition of these tu-mors.
Sarcomas With Epithelioid AppearanceThe screening panel can often successfully disclose the
broad line of differentiation in tumors with overlappinghistology (see ‘‘Broad Lineage Determination’’). The epi-thelioid morphology of sarcomas, which commonly cor-relates with their potential CK expression, however, fur-ther complicates the distinction of these tumors from ep-ithelial malignancies. In a proper setting, a vimentin�/

Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al 341
Figure 15. Algorithmic approach to undifferentiated tumors with overlapping histologic features. CKs indicate cytokeratins; SMA, smooth muscleactin; PDSS, poorly differentiated synovial sarcoma; MPNST, malignant peripheral nerve sheath tumor; and PEComa, perivascular epithelioid celltumors.
CK� or a coordinate vimentin�/CK� in a tumor withoverlapping histology should raise the possibility of sar-comas with epithelioid features and prompt performanceof a battery of immunohistochemical stains for furthercharacterization of these tumors (Figure 15). Sarcomaswith epithelioid cells include epithelioid sarcoma, epithe-lioid angiosarcoma, clear cell sarcoma, epithelioidMPNST, and other rare sarcomas, such as sclerosing epi-thelioid fibrosarcoma, alveolar soft part sarcoma, and ep-ithelioid leiomyosarcoma.
The immunoprofile of epithelioid sarcoma includes pos-itive staining for vimentin (Figure 16, a), LMW CKs, andEMA and variable staining for CD34 (positive in 50%).277–280
The latter finding, if present (Figure 16, b), helps to dis-tinguish epithelioid sarcoma from carcinomas, which arerarely CD34 positive.
Most epithelioid angiosarcomas are positive for both vi-mentin and CKs.281–284 These tumors are recognized by ex-pression of at least one of the endothelial markers, includ-ing CD31, CD34, and factor VIII.281–283 FLI-1 protein hasbeen recently shown to have equal or superior sensitivityand specificity compared with the traditional markers forvascular tumors60,61 (Figure 17).
Clear cell sarcoma has a similar immunohistochemicalconstituent to melanoma that includes expression of S100,HMB-45, and microphthalmia transcription factor in themajority of cases.285,286 It is, however, genetically differentfrom melanoma by its specific t(12;22) translocation.287
Clear cell sarcomas are typically negative for CK andEMA.
Epithelioid MPNST, a rare variant of MPNST, may berecognized by positive staining for S100 (in 80%) andNSE.288 The epithelioid variant of pleomorphic liposarco-mas in up to half of the cases may show reaction withS100 or epithelial markers, an important finding to be con-sidered in the differential diagnosis of these tumors fromsolid carcinomas with clear cell feature.253,255 The diagnosisof a number of rare sarcomas with epithelioid appearance,for example, sclerosing epithelioid fibrosarcoma and al-veolar soft part sarcoma, is essentially made on the basisof their distinct light microscopic features.
Miscellaneous Mesenchymal Tumors WithEpithelioid Appearance
Some mesenchymal neoplasms of borderline or uncer-tain malignant behavior may impart epithelioid appear-ance and be considered in the differential diagnosis ofundifferentiated carcinomas; a few examples of which areherein given. Perivascular epithelioid cell tumors are mes-enchymal neoplasms of perivascular epithelioid cells,289
with a wide anatomic distribution, sometimes presentingas unusual clear cell tumors in various locations.290–292 Im-munohistochemically, these tumors are characterized bycoexpression of melanocytic, including HMB-45 and Me-lan-A, and smooth muscle markers.219,221,290 Sex cord–stro-mal tumors are a heterogeneous group of neoplasms ofthe ovary and testis with various histologic patterns, notuncommonly confused as an undifferentiated carcinoma.Epithelial membrane antigen, which is nearly always neg-ative, is a more reliable marker in distinction of these tu-mors from epithelial neoplasms because sex cord–stromaltumors, in particular granulosa cell tumor, may variablystain for CKs (0%–64%).214,225,293 Both inhibin and calretininare useful markers for confirming the diagno-sis.212,214,215,224,225 Gastrointestinal stromal tumor, includingthe epithelioid subtype, is immunohistochemically char-acterized by expression of CD117 (c-Kit) and CD34 inmost cases, rare expression of smooth muscle actin anddesmin, and negative staining for S100.294
Malignant Melanoma
S100 is a sensitive, albeit not a specific, melanoma mark-er, decorating more than 95% of MMs of primary and met-astatic sites. The diagnosis of MM requires confirmationwith a melanocytic-specific marker, including HMB-45,Melan-A, microphthalmia transcription factor, and tyros-inase.
HMB-45 is a specific monoclonal antibody against anantigen present in the cytoplasm of neoplastic melanocyticcells. It shows positive cytoplasmic staining in the major-ity of MMs (�95% in ethanol-fixed tissues and slightlyless in formalin-fixed tissues), with the exception of des-

342 Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al
Figure 16. Photomicrograph of epithelioid sarcoma showing positivestaining for vimentin (a) and CD34 (b) (original magnifications �20).
Figure 17. Photomicrograph of epithelioid angiosarcoma showingpositive nuclear staining for FLI-1 protein (original magnification �20).
moplastic MM, which rarely demonstrates HMB-45 ex-pression.27,295 Melan-A/MART-1 is a newer melanocyticmarker with sensitivity comparable to that of HMB-45 forconventional melanoma. Like HMB-45, it is negative inmost desmoplastic MMs.295 Although both Melan-A andHMB-45 are positive in more than 90% of conventionalforms, their sensitivity declines in recurrent, spindle cell,or metastatic melanomas to 80%.15,26 For metastatic mela-nomas, however, Melan-A seems to be more sensitive(positive in 82%) than HMB-45 (positive in 76%).219,221 BothHMB-45 and Melan-A stain the PEComa family of neo-plasms,219,221 yet Melan-A also stains adrenal cortical neo-plasms.220
Malignant melanomas stain intensely for vimentin butare typically negative for epithelial markers, glial fibrillaryacidic protein, CD45, and desmin. However, aberrant ex-pression for a number of immunostains, including CK,EMA, pCEA, or glial fibrillary acidic protein, has beenrarely reported (also see ‘‘Malignant Melanoma’’ under‘‘Small Round Cell Tumors’’).15,16,26,296
Hematopoietic MalignanciesThe spectrum of hematolymphoid malignancies pre-
senting as a mass of large atypical cells of uncertain originis broad and includes various types of lymphoma, myeloidsarcoma, and plasma cell neoplasm, each with a diverseimmunoprofile, the complexity of which is far beyond thescope of this manuscript. Some examples of the unex-pected immunohistochemical expression in selectedgroups of hematopoietic tumors are herein provided.
As mentioned previously, CD45 (LCA) is a valuable toolin the diagnostic separation of hematopoietic neoplasms,particularly of the lymphoid type, from poorly differen-tiated epithelial and mesenchymal neoplasms. Non-Hodg-kin lymphomas of the B- and T-cell types are immunore-active for LCA in 93% to 100% .28,29 A negative LCA, how-ever, does not absolutely preclude the diagnosis of lym-phoma in a large cell undifferentiated tumor because LCAis rarely absent in some lymphomas of the T-cell type andsome plasma cell neoplasms.
The immunoprofile of anaplastic large cell lymphomais highly variable and includes a positive reaction for LCA(60%–70% of cases), CD30 (nearly all), T-cell markers(54%–70%), ALK protein (60%–85%), and EMA(�75%).18,297–299 Hence, a potential CD45�/EMA� immu-noprofile in anaplastic large cell lymphoma may pose di-agnostic confusion with an undifferentiated carcinoma.On the other hand, the typical CK�/EMA� immunoprofilein anaplastic large cell lymphoma may help to differenti-ate it from embryonal carcinoma (CK�/EMA�), which isalso reactive for CD30.
Most but not all granulocytic sarcomas (�75%) expressLCA.112 CD43 is a more sensitive marker for myeloid sar-comas, staining up to 100% of cases with an intense wide-spread staining pattern.112 The diagnosis of myeloid tu-mor, however, requires demonstration of more specificmarkers, including myeloperoxidase and lysozyme.
The immunoprofile complexity of neoplastic plasmacells (plasmacytoma or plasma cell myeloma), includingvariable expression for CD45, EMA, and CK, combinedwith commonly negative reaction for B-cell markers(CD19, CD20), may pose potential diagnostic pitfalls intheir distinction from epithelial neoplasms.10,33,34 A highindex of suspicion should direct to a panel that includesCD38, CD138, and � and light chains. Of note, although

Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al 343
CD138 is an excellent marker of plasmacytic differentia-tion within the hematopoietic system (positive in nearlyall), it is also expressed in various nonhematopoietic neo-plasms; hence, it is not considered a definitive marker forplasmacytic derivation, unless the hematolymphoid originof tumor is established.300
In summary, classification of a tumor beyond its appar-ent undifferentiated morphology is possible in the major-ity of cases. This not only is important for prognosticationand therapy but should also provide further insights intothe pathobiology of these tumors. The diagnostic pathwayis started with recognizing a tumor as SRCT, carcinoma-tous tumor, sarcomatous (or sarcoma-like) tumor, or tu-mor with histologically overlapping features, followed byan immunohistochemical panel, which is judiciously con-structed for each tumor. Awareness of the diagnostic util-ity of several tissue- or organ-specific immunomarkers, assummarized in this review, should help meet one of themost significant challenges in diagnostic pathology.
References1. Coindre JM, Tanguy F, Merlio JP, De Mascarel I, De Mascarel A, Trojani M.
The value of immunohistological techniques in undifferentiated cancers. Tumori.1986;72:539–544.
2. Gatter KC, Alcock C, Heryet A, Mason DY. Clinical importance of analysingmalignant tumours of uncertain origin with immunohistological techniques. Lan-cet. 1985;1:1302–1305.
3. Vege DS, Soman CS, Joshi UA, Ganesh B, Yadav JN. Undifferentiated tu-mors: an immunohistochemical analysis on biopsies. J Surg Oncol. 1994;57:273–276.
4. Kamel OW, Rouse RV, Warnke RA. Heterogeneity of epithelial marker ex-pression in routinely processed, poorly differentiated carcinomas. Arch Pathol LabMed. 1991;115:566–570.
5. Gaffey MJ, Traweek ST, Mills SE, et al. Cytokeratin expression in adreno-cortical neoplasia: an immunohistochemical and biochemical study with impli-cations for the differential diagnosis of adrenocortical, hepatocellular, and renalcell carcinoma. Hum Pathol. 1992;23:144–153.
6. Wick MR, Cherwitz DL, McGlennen RC, Dehner LP. Adrenocortical carci-noma: an immunohistochemical comparison with renal cell carcinoma. Am JPathol. 1986;122:343–352.
7. Cote RJ, Cordon-Cardo C, Reuter VE, Rosen PP. Immunopathology of ad-renal and renal cortical tumors: coordinated change in antigen expression is as-sociated with neoplastic conversion in the adrenal cortex. Am J Pathol. 1990;136:1077–1084.
8. Miettinen M. Keratin subsets in spindle cell sarcomas: keratins are wide-spread but synovial sarcoma contains a distinctive keratin polypeptide patternand desmoplakins. Am J Pathol. 1991;138:505–513.
9. Banks ER, Jansen JF, Oberle E, Davey DD. Cytokeratin positivity in fine-needle aspirates of melanomas and sarcomas. Diagn Cytopathol. 1995;12:230–233.
10. Shin JS, Stopyra GA, Warhol MJ, Multhaupt HA. Plasmacytoma with ab-errant expression of myeloid markers, T-cell markers, and cytokeratin. J Histo-chem Cytochem. 2001;49:791–792.
11. Menestrina F, Lestani M, Scarpa A, et al. Common acute lymphoblasticleukaemia-lymphoma expressing cytokeratin: a case report. Virchows Arch. 1994;425:83–87.
12. Beschorner R, Horny HP, Petruch UR, Kaiserling E. Frequent expression ofhaemopoietic and non-haemopoietic antigens by reactive plasma cells: an im-munohistochemical study using formalin-fixed, paraffin-embedded tissue. HistolHistopathol. 1999;14:805–812.
13. Listrom MB, Dalton LW. Comparison of keratin monoclonal antibodiesMAK-6, AE1:AE3, and CAM-5.2. Am J Clin Pathol. 1987;88:297–301.
14. Gustmann C, Altmannsberger M, Osborn M, Griesser H, Feller AC. Cyto-keratin expression and vimentin content in large cell anaplastic lymphomas andother non-Hodgkin’s lymphomas. Am J Pathol. 1991;138:1413–1422.
15. Bishop PW, Menasce LP, Yates AJ, Win NA, Banerjee SS. An immunophe-notypic survey of malignant melanomas. Histopathology. 1993;23:159–166.
16. Selby WL, Nance KV, Park HK. CEA immunoreactivity in metastatic ma-lignant melanoma. Mod Pathol. 1992;5:415–419.
17. Pinkus GS, Kurtin PJ. Epithelial membrane antigen—a diagnostic discrim-inant in surgical pathology: immunohistochemical profile in epithelial, mesen-chymal, and hematopoietic neoplasms using paraffin sections and monoclonalantibodies. Hum Pathol. 1985;16:929–940.
18. Ioachim HL, Ratech H. Ioachim’s Lymph Node Pathology. 3rd ed. Phila-delphia, Pa: Lippincott Williams & Wilkins; 2002:341–476.
19. Delsol G, Gatter KC, Stein H, et al. Human lymphoid cells express epi-thelial membrane antigen. Implications for diagnosis of human neoplasms. Lan-cet. 1984;2:1124–1129.
20. Norton AJ, Isaacson PG. An immunocytochemical study of T-cell lympho-
mas using monoclonal and polyclonal antibodies effective in routinely fixed waxembedded tissues. Histopathology. 1986;10:1243–1260.
21. ten Berge RL, Snijdewint FG, Mensdorff-Pouilly S, et al. MUC1 (EMA) ispreferentially expressed by ALK positive anaplastic large cell lymphoma, in thenormally glycosylated or only partly hypoglycosylated form. J Clin Pathol. 2001;54:933–939.
22. Azumi N, Battifora H. The distribution of vimentin and keratin in epithelialand nonepithelial neoplasms. A comprehensive immunohistochemical study onform. Am J Clin Pathol. 1987;88:286–296.
23. McNutt MA, Bolen JW, Gown AM, Hammar SP, Vogel AM. Coexpressionof intermediate filaments in human epithelial neoplasms. Ultrastruct Pathol. 1985;9:31–43.
24. Dabbs DJ. Diagnostic Immunohistochemistry. 2nd ed. Philadelphia, Pa:Churchill Livingstone Elsevier; 2006:194.
25. Herrera GA, Turbat-Herrera EA, Lott RL. S-100 protein expression by pri-mary and metastatic adenocarcinomas. Am J Clin Pathol. 1988;89:168–176.
26. Banerjee SS, Harris M. Morphological and immunophenotypic variationsin malignant melanoma. Histopathology. 2000;36:387–402.
27. Longacre TA, Egbert BM, Rouse RV. Desmoplastic and spindle-cell malig-nant melanoma: an immunohistochemical study. Am J Surg Pathol. 1996;20:1489–1500.
28. Michels S, Swanson PE, Frizzera G, Wick MR. Immunostaining for leu-kocyte common antigen using an amplified avidin-biotin-peroxidase complexmethod and paraffin sections: a study of 735 hematopoietic and nonhemato-poietic human neoplasms. Arch Pathol Lab Med. 1987;111:1035–1039.
29. Kurtin PJ, Pinkus GS. Leukocyte common antigen—a diagnostic discrimi-nant between hematopoietic and nonhematopoietic neoplasms in paraffin sec-tions using monoclonal antibodies: correlation with immunologic studies andultrastructural localization. Hum Pathol. 1985;16:353–365.
30. Van Eyken P, Wolf-Peeters C, Van den OJ, Tricot G, Desmet V. Expressionof leukocyte common antigen in lymphoblastic lymphoma and small noncleavedundifferentiated non-Burkitt’s lymphoma: an immunohistochemical study. JPathol. 1987;151:257–261.
31. Ozdemirli M, Fanburg-Smith JC, Hartmann DP, et al. Precursor B-Lympho-blastic lymphoma presenting as a solitary bone tumor and mimicking Ewing’ssarcoma: a report of four cases and review of the literature. Am J Surg Pathol.1998;22:795–804.
32. Kahwash SB, Qualman SJ. Cutaneous lymphoblastic lymphoma in chil-dren: report of six cases with precursor B-cell lineage. Pediatr Dev Pathol. 2002;5:45–53.
33. Kumar S, Rajkumar SV, Kimlinger T, Greipp PR, Witzig TE. CD45 expres-sion by bone marrow plasma cells in multiple myeloma: clinical and biologicalcorrelations. Leukemia. 2005;19:1466–1470.
34. Wotherspoon AC, Norton AJ, Isaacson PG. Immunoreactive cytokeratinsin plasmacytomas. Histopathology. 1989;14:141–150.
35. Ferry JA, Young RH, Scully RE. Testicular and epididymal plasmacytoma:a report of 7 cases, including three that were the initial manifestation of plasmacell myeloma. Am J Surg Pathol. 1997;21:590–598.
36. Clavio M, Rossi E, Truini M, et al. Anaplastic large cell lymphoma: a clin-icopathologic study of 53 patients. Leuk Lymphoma. 1996;22:319–327.
37. Perkins PL, Ross CW, Schnitzer B. CD30-positive, anaplastic large-celllymphomas that express CD15 but lack CD45: a possible diagnostic pitfall. ArchPathol Lab Med. 1992;116:1192–1196.
38. Nandedkar MA, Palazzo J, Abbondanzo SL, Lasota J, Miettinen M. CD45(leukocyte common antigen) immunoreactivity in metastatic undifferentiated andneuroendocrine carcinoma: a potential diagnostic pitfall. Mod Pathol. 1998;11:1204–1210.
39. Devoe K, Weidner N. Immunohistochemistry of small round-cell tumors.Semin Diagn Pathol. 2000;17:216–224.
40. Folpe AL, Goldblum JR, Rubin BP, et al. Morphologic and immunophe-notypic diversity in Ewing family tumors: a study of 66 genetically confirmedcases. Am J Surg Pathol. 2005;29:1025–1033.
41. Weidner N, Tjoe J. Immunohistochemical profile of monoclonal antibodyO13: antibody that recognizes glycoprotein p30/32MIC2 and is useful in diag-nosing Ewing’s sarcoma and peripheral neuroepithelioma. Am J Surg Pathol.1994;18:486–494.
42. Hess E, Cohen C, DeRose PB, Yost BA, Costa MJ. Nonspecificity of p30/32MIC2 immunolocalization with the O13 monoclonal antibody in the diagnosisof Ewing’s sarcoma: application of an algorithmic immunohistochemical analysis.Appl Immunohistochem. 1997;5:94–103.
43. Scotlandi K, Serra M, Manara MC, et al. Immunostaining of the p30/32MIC2 antigen and molecular detection of EWS rearrangements for the diag-nosis of Ewing’s sarcoma and peripheral neuroectodermal tumor. Hum Pathol.1996;27:408–416.
44. Ramani P, Rampling D, Link M. Immunocytochemical study of 12E7 insmall round-cell tumours of childhood: an assessment of its sensitivity and spec-ificity. Histopathology. 1993;23:557–561.
45. Riopel M, Dickman PS, Link MP, Perlman EJ. MIC2 analysis in pediatriclymphomas and leukemias. Hum Pathol. 1994;25:396–399.
46. Zhang PJ, Barcos M, Stewart CC, Block AW, Sait S, Brooks JJ. Immunore-activity of MIC2 (CD99) in acute myelogenous leukemia and related diseases.Mod Pathol. 2000;13:452–458.
47. van de Rijn M, Barr FG, Xiong QB, Hedges M, Shipley J, Fisher C. Poorlydifferentiated synovial sarcoma: an analysis of clinical, pathologic, and moleculargenetic features. Am J Surg Pathol. 1999;23:106–112.

344 Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al
48. Folpe AL, Schmidt RA, Chapman D, Gown AM. Poorly differentiated sy-novial sarcoma: immunohistochemical distinction from primitive neuroectoder-mal tumors and high-grade malignant peripheral nerve sheath tumors. Am J SurgPathol. 1998;22:673–682.
49. Pelmus M, Guillou L, Hostein I, Sierankowski G, Lussan C, Coindre JM.Monophasic fibrous and poorly differentiated synovial sarcoma: immunohisto-chemical reassessment of 60 t(X;18)(SYT-SSX)-positive cases. Am J Surg Pathol.2002;26:1434–1440.
50. Hoang MP, Suarez PA, Donner LR, et al. Mesenchymal chondrosarcoma:a small cell neoplasm with polyphenotypic differentiation. Int J Surg Pathol. 2000;8:291–301.
51. Granter SR, Renshaw AA, Fletcher CD, Bhan AK, Rosenberg AE. CD99reactivity in mesenchymal chondrosarcoma. Hum Pathol. 1996;27:1273–1276.
52. Zhang PJ, Goldblum JR, Pawel BR, Fisher C, Pasha TL, Barr FG. Immu-nophenotype of desmoplastic small round cell tumors as detected in cases withEWS-WT1 gene fusion product. Mod Pathol. 2003;16:229–235.
53. Hicks J, Flaitz C. Rhabdomyosarcoma of the head and neck in children.Oral Oncol. 2002;38:450–459.
54. Jimenez RE, Folpe AL, Lapham RL, et al. Primary Ewing’s sarcoma/primitiveneuroectodermal tumor of the kidney: a clinicopathologic and immunohisto-chemical analysis of 11 cases. Am J Surg Pathol. 2002;26:320–327.
55. Weiss SW, Goldblum JR. Enzinger and Weiss’s Soft Tissue Tumors. 4th ed.St Louis, Mo: Mosby; 2001:235, 549.
56. Garin-Chesa P, Fellinger EJ, Huvos AG, et al. Immunohistochemical anal-ysis of neural cell adhesion molecules: differential expression in small round celltumors of childhood and adolescence. Am J Pathol. 1991;139:275–286.
57. Miettinen M, Cupo W. Neural cell adhesion molecule distribution in softtissue tumors. Hum Pathol. 1993;24:62–66.
58. Ravandi F, Cortes J, Estrov Z, et al. CD56 expression predicts occurrenceof CNS disease in acute lymphoblastic leukemia. Leuk Res. 2002;26:643–649.
59. Khanlari B, Buser A, Lugli A, Tichelli A, Dirnhofer S. The expression patternof CD56 (N-CAM) in human bone marrow biopsies infiltrated by acute leukemia.Leuk Lymphoma. 2003;44:2055–2059.
60. Folpe AL, Hill CE, Parham DM, O’Shea PA, Weiss SW. Immunohistochem-ical detection of FLI-1 protein expression: a study of 132 round cell tumors withemphasis on CD99-positive mimics of Ewing’s sarcoma/primitive neuroectoder-mal tumor. Am J Surg Pathol. 2000;24:1657–1662.
61. Rossi S, Orvieto E, Furlanetto A, Laurino L, Ninfo V, Dei Tos AP. Utility ofthe immunohistochemical detection of FLI-1 expression in round cell and vas-cular neoplasm using a monoclonal antibody. Mod Pathol. 2004;17:547–552.
62. Collini P, Sampietro G, Bertulli R, et al. Cytokeratin immunoreactivity in41 cases of ES/PNET confirmed by molecular diagnostic studies. Am J Surg Pathol.2001;25:273–274.
63. Gu M, Antonescu CR, Guiter G, Huvos AG, Ladanyi M, Zakowski MF.Cytokeratin immunoreactivity in Ewing’s sarcoma: prevalence in 50 cases con-firmed by molecular diagnostic studies. Am J Surg Pathol. 2000;24:410–416.
64. Kumar S, Perlman E, Harris CA, Raffeld M, Tsokos M. Myogenin is a spe-cific marker for rhabdomyosarcoma: an immunohistochemical study in paraffin-embedded tissues. Mod Pathol. 2000;13:988–993.
65. Sebire NJ, Malone M. Myogenin and MyoD1 expression in paediatricrhabdomyosarcomas. J Clin Pathol. 2003;56:412–416.
66. Wang NP, Marx J, McNutt MA, Rutledge JC, Gown AM. Expression ofmyogenic regulatory proteins (myogenin and MyoD1) in small blue round celltumors of childhood. Am J Pathol. 1995;147:1799–1810.
67. Cessna MH, Zhou H, Perkins SL, et al. Are myogenin and myoD1 expres-sion specific for rhabdomyosarcoma? A study of 150 cases, with emphasis onspindle cell mimics. Am J Surg Pathol. 2001;25:1150–1157.
68. Carpentieri DF, Nichols K, Chou PM, Matthews M, Pawel B, Huff D. Theexpression of WT1 in the differentiation of rhabdomyosarcoma from other pedi-atric small round blue cell tumors. Mod Pathol. 2002;15:1080–1086.
69. Gerald WL, Ladanyi M, de Alava E, et al. Clinical, pathologic, and molec-ular spectrum of tumors associated with t(11;22)(p13;q12): desmoplastic smallround-cell tumor and its variants. J Clin Oncol. 1998;16:3028–3036.
70. Ordonez NG. Desmoplastic small round cell tumor, II: an ultrastructuraland immunohistochemical study with emphasis on new immunohistochemicalmarkers. Am J Surg Pathol. 1998;22:1314–1327.
71. Barnoud R, Sabourin JC, Pasquier D, et al. Immunohistochemical expres-sion of WT1 by desmoplastic small round cell tumor: a comparative study withother small round cell tumors. Am J Surg Pathol. 2000;24:830–836.
72. Hill DA, Pfeifer JD, Marley EF, et al. WT1 staining reliably differentiatesdesmoplastic small round cell tumor from Ewing sarcoma/primitive neuroecto-dermal tumor: an immunohistochemical and molecular diagnostic study. Am JClin Pathol. 2000;114:345–353.
73. Dei Tos AP, Wadden C, Calonje E, et al. Immunohistochemical demon-stration of glycoprotein p30/32 MIC2 (CD99) in synovial sarcoma: a potentialcause of diagnostic confusion. Appl Immunohistochem. 1995;31:68–73.
74. Mechtersheimer G, Staudter M, Moller P. Expression of the natural killercell-associated antigens CD56 and CD57 in human neural and striated musclecells and in their tumors. Cancer Res. 1991;51:1300–1307.
75. Devaney K, Vinh TN, Sweet DE. Small cell osteosarcoma of bone: an im-munohistochemical study with differential diagnostic considerations. Hum Pathol.1993;24:1211–1225.
76. Nakajima H, Sim FH, Bond JR, Unni KK. Small cell osteosarcoma of bone:review of 72 cases. Cancer. 1997;79:2095–2106.
77. Fanburg-Smith JC, Bratthauer GL, Miettinen M. Osteocalcin and osteonec-
tin immunoreactivity in extraskeletal osteosarcoma: a study of 28 cases. HumPathol. 1999;30:32–38.
78. Fanburg JC, Rosenberg AE, Weaver DL, et al. Osteocalcin and osteonectinimmunoreactivity in the diagnosis of osteosarcoma. Am J Clin Pathol. 1997;108:464–473.
79. Hasegawa T, Hirose T, Kudo E, Hizawa K, Usui M, Ishii S. Immunophe-notypic heterogeneity in osteosarcomas. Hum Pathol. 1991;22:583–590.
80. Okada K, Hasegawa T, Yokoyama R, Beppu Y, Itoi E. Osteosarcoma withcytokeratin expression: a clinicopathological study of six cases with an emphasison differential diagnosis from metastatic cancer. J Clin Pathol. 2003;56:742–746.
81. Muir TE, Cheville JC, Lager DJ. Metanephric adenoma, nephrogenic rests,and Wilms’ tumor: a histologic and immunophenotypic comparison. Am J SurgPathol. 2001;25:1290–1296.
82. Domagala W, Chosia M, Bedner E, Kubicka C, Weber K, Osborn M. Im-munocytochemistry in fine needle aspirates of small cell-, round-, blue-cell ma-lignant tumors of childhood (neuroblastoma, nephroblastoma, lymphoma, Ew-ing’s sarcoma, rhabdomyosarcoma). Patol Pol. 1991;42:79–82.
83. Folpe AL, Patterson K, Gown AM. Antibodies to desmin identify the blas-temal component of nephroblastoma. Mod Pathol. 1997;10:895–900.
84. Hasegawa T, Hirose T, Ayala AG, et al. Adult neuroblastoma of the retro-peritoneum and abdomen: clinicopathologic distinction from primitive neuroec-todermal tumor. Am J Surg Pathol. 2001;25:918–924.
85. Franquemont DW, Mills SE, Lack EE. Immunohistochemical detection ofneuroblastomatous foci in composite adrenal pheochromocytoma-neuroblasto-ma. Am J Clin Pathol. 1994;102:163–170.
86. Wirnsberger GH, Becker H, Ziervogel K, Hofler H. Diagnostic immuno-histochemistry of neuroblastic tumors. Am J Surg Pathol. 1992;16:49–57.
87. Hachitanda Y, Tsuneyoshi M, Enjoji M. An ultrastructural and immunohis-tochemical evaluation of cytodifferentiation in neuroblastic tumors. Mod Pathol.1989;2:13–19.
88. Frierson HF Jr, Ross GW, Mills SE, Frankfurter A. Olfactory neuroblastoma:additional immunohistochemical characterization. Am J Clin Pathol. 1990;94:547–553.
89. Banerjee AK, Sharma BS, Vashista RK, Kak VK. Intracranial olfactory neu-roblastoma: evidence for olfactory epithelial origin. J Clin Pathol. 1992;45:299–302.
90. Moll R, Franke WW. Cytoskeletal differences between human neuroen-docrine tumors: a cytoskeletal protein of molecular weight 46,000 distinguishescutaneous from pulmonary neuroendocrine neoplasms. Differentiation. 1985;30:165–175.
91. Mertz H, Vyberg M, Paulsen, SM, Teglbjærg, PS. Immunohistochemicaldetection of neuroendocrine markers in tumors of the lungs and gastrointestinaltract. Appl Immunohistochem. 1998;6:175–180.
92. Shipley WR, Hammer RD, Lennington WJ, Macon WR. Paraffin immuno-histochemical detection of CD56, a useful marker for neural cell adhesion mol-ecule (NCAM), in normal and neoplastic fixed tissues. Appl Immunohistochem.1997;5:87–93.
93. Chan JK, Suster S, Wenig BM, Tsang WY, Chan JB, Lau AL. Cytokeratin 20immunoreactivity distinguishes Merkel cell (primary cutaneous neuroendocrine)carcinomas and salivary gland small cell carcinomas from small cell carcinomasof various sites. Am J Surg Pathol. 1997;21:226–234.
94. Miettinen M. Keratin 20: immunohistochemical marker for gastrointestinal,urothelial, and Merkel cell carcinomas. Mod Pathol. 1995;8:384–388.
95. Nagao T, Gaffey TA, Olsen KD, Serizawa H, Lewis JE. Small cell carcinomaof the major salivary glands: clinicopathologic study with emphasis on cytokeratin20 immunoreactivity and clinical outcome. Am J Surg Pathol. 2004;28:762–770.
96. Shin SJ, DeLellis RA, Ying L, Rosen PP. Small cell carcinoma of the breast:a clinicopathologic and immunohistochemical study of nine patients. Am J SurgPathol. 2000;24:1231–1238.
97. Bacchi CE, Garcia RL, Gown AM. Immunolocalization of estrogen andprogesterone receptors in neuroendocrine tumors of the lung, skin, gastrointes-tinal and female genital tracts. Appl Immunohistochem. 1997;5:17–22.
98. Viale G, Doglioni C, Gambacorta M, Zamboni G, Coggi G, Bordi C. Pro-gesterone receptor immunoreactivity in pancreatic endocrine tumors: an immu-nocytochemical study of 156 neuroendocrine tumors of the pancreas, gastroin-testinal and respiratory tracts, and skin. Cancer. 1992;70:2268–2277.
99. Johansson L. Histopathologic classification of lung cancer: relevance ofcytokeratin and TTF-1 immunophenotyping. Ann Diagn Pathol. 2004;8:259–267.
100. Cheuk W, Kwan MY, Suster S, Chan JK. Immunostaining for thyroid tran-scription factor 1 and cytokeratin 20 aids the distinction of small cell carcinomafrom Merkel cell carcinoma, but not pulmonary from extrapulmonary small cellcarcinomas. Arch Pathol Lab Med. 2001;125:228–231.
101. Ordonez NG. Value of thyroid transcription factor-1 immunostaining indistinguishing small cell lung carcinomas from other small cell carcinomas. AmJ Surg Pathol. 2000;24:1217–1223.
102. Zhang H, Liu J, Cagle PT, Allen TC, Laga AC, Zander DS. Distinction ofpulmonary small cell carcinoma from poorly differentiated squamous cell carci-noma: an immunohistochemical approach. Mod Pathol. 2005;18:111–118.
103. Kaufmann O, Dietel M. Expression of thyroid transcription factor-1 inpulmonary and extrapulmonary small cell carcinomas and other neuroendocrinecarcinomas of various primary sites. Histopathology. 2000;36:415–420.
104. McCluggage WG, Oliva E, Connolly LE, McBride HA, Young RH. Animmunohistochemical analysis of ovarian small cell carcinoma of hypercalcemictype. Int J Gynecol Pathol. 2004;23:330–336.

Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al 345
105. McCluggage WG. Ovarian neoplasms composed of small round cells: areview. Adv Anat Pathol. 2004;11:288–296.
106. Oesterling JE, Hauzeur CG, Farrow GM. Small cell anaplastic carcinomaof the prostate: a clinical, pathological and immunohistological study of 27 pa-tients. J Urol. 1992;147:804–807.
107. Parker DC, Folpe AL, Bell J, et al. Potential utility of uroplakin III, throm-bomodulin, high molecular weight cytokeratin, and cytokeratin 20 in noninva-sive, invasive, and metastatic urothelial (transitional cell) carcinomas. Am J SurgPathol. 2003;27:1–10.
108. Erickson LA, Papouchado B, Dimashkieh H, Zhang S, Nakamura N, LloydRV. Cdx2 as a marker for neuroendocrine tumors of unknown primary sites. En-docr Pathol. 2004;15:247–252.
109. Franchi A, Pasquinelli G, Cenacchi G, et al. Immunohistochemical andultrastructural investigation of neural differentiation in Ewing sarcoma/PNET ofbone and soft tissues. Ultrastruct Pathol. 2001;25:219–225.
110. Cerilli LA, Holst VA, Brandwein MS, Stoler MH, Mills SE. Sinonasal un-differentiated carcinoma: immunohistochemical profile and lack of EBV associ-ation. Am J Surg Pathol. 2001;25:156–163.
111. Ozdemirli M, Fanburg-Smith JC, Hartmann DP, Azumi N, Miettinen M.Differentiating lymphoblastic lymphoma and Ewing’s sarcoma: lymphocyte mark-ers and gene rearrangement. Mod Pathol. 2001;14:1175–1182.
112. Traweek ST, Arber DA, Rappaport H, Brynes RK. Extramedullary myeloidcell tumors: an immunohistochemical and morphologic study of 28 cases. Am JSurg Pathol. 1993;17:1011–1019.
113. Thompson LD, Wieneke JA, Miettinen M. Sinonasal tract and nasopha-ryngeal melanomas: a clinicopathologic study of 115 cases with a proposed stag-ing system. Am J Surg Pathol. 2003;27:594–611.
114. Wilkerson AE, Glasgow MA, Hiatt KM. Immunoreactivity of CD99 ininvasive malignant melanoma. J Cutan Pathol. 2006;33:663–666.
115. Nakatsuka S, Oji Y, Horiuchi T, et al. Immunohistochemical detection ofWT1 protein in a variety of cancer cells. Mod Pathol. 2006;19:804–814.
116. Bilalovic N, Sandstad B, Golouh R, Nesland JM, Selak I, Torlakovic EE.CD10 protein expression in tumor and stromal cells of malignant melanoma isassociated with tumor progression. Mod Pathol. 2004;17:1251–1258.
117. Chu P, Arber DA. Paraffin-section detection of CD10 in 505 nonhema-topoietic neoplasms: frequent expression in renal cell carcinoma and endometrialstromal sarcoma. Am J Clin Pathol. 2000;113:374–382.
118. Pernick NL, DaSilva M, Gangi MD, Crissman J, Adsay V. ‘‘Histiocyticmarkers’’ in melanoma. Mod Pathol. 1999;12:1072–1077.
119. Wick MR, Stanley SJ, Swanson PE. Immunohistochemical diagnosis ofsinonasal melanoma, carcinoma, and neuroblastoma with monoclonal antibodiesHMB-45 and anti-synaptophysin. Arch Pathol Lab Med. 1988;112:616–620.
120. Wang NP, Zee S, Zarbo RJ. Coordinate expression of cytokeratins 7 and20 defines unique subsets of carcinomas. Appl Immunohistochem. 1995;3:99–107.
121. Shah KD, Tabibzadeh SS, Gerber MA. Comparison of cytokeratin expres-sion in primary and metastatic carcinomas: diagnostic application in surgicalpathology. Am J Clin Pathol. 1987;87:708–715.
122. Loy TS, Calaluce RD, Keeney GL. Cytokeratin immunostaining in differ-entiating primary ovarian carcinoma from metastatic colonic adenocarcinoma.Mod Pathol. 1996;9:1040–1044.
123. Bassily NH, Vallorosi CJ, Akdas G, Montie JE, Rubin MA. Coordinateexpression of cytokeratins 7 and 20 in prostate adenocarcinoma and bladderurothelial carcinoma. Am J Clin Pathol. 2000;113:383–388.
124. Chu P, Wu E, Weiss LM. Cytokeratin 7 and cytokeratin 20 expression inepithelial neoplasms: a survey of 435 cases. Mod Pathol. 2000;13:962–972.
125. Maeda T, Kajiyama K, Adachi E, Takenaka K, Sugimachi K, TsuneyoshiM. The expression of cytokeratins 7, 19, and 20 in primary and metastatic car-cinomas of the liver. Mod Pathol. 1996;9:901–909.
126. Ordonez NG. Value of cytokeratin 5/6 immunostaining in distinguishingepithelial mesothelioma of the pleura from lung adenocarcinoma. Am J SurgPathol. 1998;22:1215–1221.
127. Ordonez NG. The diagnostic utility of immunohistochemistry in distin-guishing between epithelioid mesotheliomas and squamous carcinomas of thelung: a comparative study. Mod Pathol. 2006;19:417–428.
128. Ordonez NG. The immunohistochemical diagnosis of mesothelioma: acomparative study of epithelioid mesothelioma and lung adenocarcinoma. Am JSurg Pathol. 2003;27:1031–1051.
129. Carella R, Deleonardi G, D’Errico A, et al. Immunohistochemical panelsfor differentiating epithelial malignant mesothelioma from lung adenocarcinoma:a study with logistic regression analysis. Am J Surg Pathol. 2001;25:43–50.
130. Miettinen M, Sarlomo-Rikala M. Expression of calretinin, thrombomo-dulin, keratin 5, and mesothelin in lung carcinomas of different types: an im-munohistochemical analysis of 596 tumors in comparison with epithelioid me-sotheliomas of the pleura. Am J Surg Pathol. 2003;27:150–158.
131. Sheahan K, O’Brien MJ, Burke B, et al. Differential reactivities of carci-noembryonic antigen (CEA) and CEA-related monoclonal and polyclonal anti-bodies in common epithelial malignancies. Am J Clin Pathol. 1990;94:157–164.
132. Berezowski K, Stastny JF, Kornstein MJ. Cytokeratins 7 and 20 and car-cinoembryonic antigen in ovarian and colonic carcinoma. Mod Pathol. 1996;9:426–429.
133. Alkushi A, Irving J, Hsu F, et al. Immunoprofile of cervical and endo-metrial adenocarcinomas using a tissue microarray. Virchows Arch. 2003;442:271–277.
134. Ma CK, Zarbo RJ, Frierson HF Jr, Lee MW. Comparative immunohisto-
chemical study of primary and metastatic carcinomas of the liver. Am J ClinPathol. 1993;99:551–557.
135. Oates J, Edwards C. HBME-1, MOC-31, WT1 and calretinin: an assess-ment of recently described markers for mesothelioma and adenocarcinoma. His-topathology. 2000;36:341–347.
136. Sosolik RC, McGaughy VR, De Young BR. Anti-MOC-31: a potential ad-dition to the pulmonary adenocarcinoma versus mesothelioma immunohisto-chemistry panel. Mod Pathol. 1997;10:716–719.
137. Proca DM, Niemann TH, Porcell AI, DeYoung BR. MOC31 immunore-activity in primary and metastatic carcinoma of the liver: report of findings andreview of other utilized markers. Appl Immunohistochem Mol Morphol. 2000;8:120–125.
138. Yang A, McKeon F. P63 and P73: P53 mimics, menaces and more. NatRev Mol Cell Biol. 2000;1:199–207.
139. Kaufmann O, Fietze E, Mengs J, Dietel M. Value of p63 and cytokeratin5/6 as immunohistochemical markers for the differential diagnosis of poorly dif-ferentiated and undifferentiated carcinomas. Am J Clin Pathol. 2001;116:823–830.
140. Wang BY, Gil J, Kaufman D, Gan L, Kohtz DS, Burstein DE. P63 in pul-monary epithelium, pulmonary squamous neoplasms, and other pulmonary tu-mors. Hum Pathol. 2002;33:921–926.
141. Wu M, Wang B, Gil J, et al. p63 and TTF-1 immunostaining: a usefulmarker panel for distinguishing small cell carcinoma of lung from poorly differ-entiated squamous cell carcinoma of lung. Am J Clin Pathol. 2003;119:696–702.
142. Au NH, Gown AM, Cheang M, et al. P63 expression in lung carcinoma:a tissue microarray study of 408 cases. Appl Immunohistochem Mol Morphol.2004;12:240–247.
143. Chu PG, Weiss LM. Expression of cytokeratin 5/6 in epithelial neoplasms:an immunohistochemical study of 509 cases. Mod Pathol. 2002;15:6–10.
144. Kaufmann O, Georgi T, Dietel M. Utility of 123C3 monoclonal antibodyagainst CD56 (NCAM) for the diagnosis of small cell carcinomas on paraffinsections. Hum Pathol. 1997;28:1373–1378.
145. Lantuejoul S, Moro D, Michalides RJ, Brambilla C, Brambilla E. Neuralcell adhesion molecules (NCAM) and NCAM-PSA expression in neuroendocrinelung tumors. Am J Surg Pathol. 1998;22:1267–1276.
146. Rossi G, Marchioni A, Milani M, et al. TTF-1, cytokeratin 7, 34�E12, andCD56/NCAM immunostaining in the subclassification of large cell carcinomas ofthe lung. Am J Clin Pathol. 2004;122:884–893.
147. Wong KF, Chan JK, Ng CS. CD56 (NCAM)-positive malignant lymphoma.Leuk Lymphoma. 1994;14:29–36.
148. Wick MR. Immunohistology of neuroendocrine and neuroectodermal tu-mors. Semin Diagn Pathol. 2000;17:194–203.
149. Wick MR, Berg LC, Hertz MI. Large cell carcinoma of the lung withneuroendocrine differentiation: a comparison with large cell ‘‘undifferentiated’’pulmonary tumors. Am J Clin Pathol. 1992;97:796–805.
150. Sturm N, Lantuejoul S, Laverriere MH, et al. Thyroid transcription factor1 and cytokeratins 1, 5, 10, 14 (34betaE12) expression in basaloid and large-cellneuroendocrine carcinomas of the lung. Hum Pathol. 2001;32:918–925.
151. Lyda MH, Weiss LM. Immunoreactivity for epithelial and neuroendocrineantibodies are useful in the differential diagnosis of lung carcinomas. Hum Pathol.2000;31:980–987.
152. Folpe AL, Gown AM, Lamps LW, et al. Thyroid transcription factor-1:immunohistochemical evaluation in pulmonary neuroendocrine tumors. ModPathol. 1999;12:5–8.
153. Nakamura N, Miyagi E, Murata S, Kawaoi A, Katoh R. Expression ofthyroid transcription factor-1 in normal and neoplastic lung tissues. Mod Pathol.2002;15:1058–1067.
154. Miettinen M, Franssila KO. Variable expression of keratins and nearlyuniform lack of thyroid transcription factor 1 in thyroid anaplastic carcinoma.Hum Pathol. 2000;31:1139–1145.
155. Agoff SN, Lamps LW, Philip AT, et al. Thyroid transcription factor-1 isexpressed in extrapulmonary small cell carcinomas but not in other extrapul-monary neuroendocrine tumors. Mod Pathol. 2000;13:238–242.
156. Carcangiu ML, Steeper T, Zampi G, Rosai J. Anaplastic thyroid carcinoma:a study of 70 cases. Am J Clin Pathol. 1985;83:135–158.
157. Ordonez NG, El Naggar AK, Hickey RC, Samaan NA. Anaplastic thyroidcarcinoma: immunocytochemical study of 32 cases. Am J Clin Pathol. 1991;96:15–24.
158. Venkatesh YS, Ordonez NG, Schultz PN, Hickey RC, Goepfert H, SamaanNA. Anaplastic carcinoma of the thyroid: a clinicopathologic study of 121 cases.Cancer. 1990;66:321–330.
159. Wennerberg AE, Nalesnik MA, Coleman WB. Hepatocyte paraffin 1: amonoclonal antibody that reacts with hepatocytes and can be used for differentialdiagnosis of hepatic tumors. Am J Pathol. 1993;143:1050–1054.
160. Lau SK, Prakash S, Geller SA, Alsabeh R. Comparative immunohisto-chemical profile of hepatocellular carcinoma, cholangiocarcinoma, and meta-static adenocarcinoma. Hum Pathol. 2002;33:1175–1181.
161. Morrison C, Marsh W Jr, Frankel WL. A comparison of CD10 to pCEA,MOC-31, and hepatocyte for the distinction of malignant tumors in the liver. ModPathol. 2002;15:1279–1287.
162. Siddiqui MT, Saboorian MH, Gokaslan ST, Ashfaq R. Diagnostic utility ofthe HepPar1 antibody to differentiate hepatocellular carcinoma from metastaticcarcinoma in fine-needle aspiration samples. Cancer. 2002;96:49–52.
163. Chu PG, Ishizawa S, Wu E, Weiss LM. Hepatocyte antigen as a markerof hepatocellular carcinoma: an immunohistochemical comparison to carci-

346 Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al
noembryonic antigen, CD10, and alpha-fetoprotein. Am J Surg Pathol. 2002;26:978–988.
164. Fan Z, van de RM, Montgomery K, Rouse RV. Hep par 1 antibody stainfor the differential diagnosis of hepatocellular carcinoma: 676 tumors tested usingtissue microarrays and conventional tissue sections. Mod Pathol. 2003;16:137–144.
165. Lugli A, Tornillo L, Mirlacher M, Bundi M, Sauter G, Terracciano LM.Hepatocyte paraffin 1 expression in human normal and neoplastic tissues: tissuemicroarray analysis on 3,940 tissue samples. Am J Clin Pathol. 2004;122:721–727.
166. Borscheri N, Roessner A, Rocken C. Canalicular immunostaining of ne-prilysin (CD10) as a diagnostic marker for hepatocellular carcinomas. Am J SurgPathol. 2001;251297–1303.
167. Barbareschi M, Murer B, Colby TV, et al. CDX-2 homeobox gene ex-pression is a reliable marker of colorectal adenocarcinoma metastases to thelungs. Am J Surg Pathol. 2003;27:141–149.
168. Werling RW, Yaziji H, Bacchi CE, Gown AM. CDX2, a highly sensitiveand specific marker of adenocarcinomas of intestinal origin: an immunohisto-chemical survey of 476 primary and metastatic carcinomas. Am J Surg Pathol.2003;27:303–310.
169. Kaimaktchiev V, Terracciano L, Tornillo L, et al. The homeobox intestinaldifferentiation factor CDX2 is selectively expressed in gastrointestinal adenocar-cinomas. Mod Pathol. 2004;17:1392–1399.
170. Hinoi T, Tani M, Lucas PC, et al. Loss of CDX2 expression and micro-satellite instability are prominent features of large cell minimally differentiatedcarcinomas of the colon. Am J Pathol. 2001;159:2239–2248.
171. Suh N, Yang XJ, Tretiakova MS, Humphrey PA, Wang HL. Value of CDX2,villin, and alpha-methylacyl coenzyme A racemase immunostains in the distinc-tion between primary adenocarcinoma of the bladder and secondary colorectaladenocarcinoma. Mod Pathol. 2005;18:1217–1222.
172. Wang HL, Lu DW, Yerian LM, et al. Immunohistochemical distinctionbetween primary adenocarcinoma of the bladder and secondary colorectal ad-enocarcinoma. Am J Surg Pathol. 2001;25:1380–1387.
173. Bacchi CE, Gown AM. Distribution and pattern of expression of villin, agastrointestinal-associated cytoskeletal protein, in human carcinomas: a studyemploying paraffin-embedded tissue. Lab Invest. 1991;64:418–424.
174. Tan J, Sidhu G, Greco MA, Ballard H, Wieczorek R. Villin, cytokeratin 7,and cytokeratin 20 expression in pulmonary adenocarcinoma with ultrastructuralevidence of microvilli with rootlets. Hum Pathol. 1998;29:390–396.
175. Tamboli P, Mohsin SK, Hailemariam S, Amin MB. Colonic adenocarci-noma metastatic to the urinary tract versus primary tumors of the urinary tractwith glandular differentiation: a report of 7 cases and investigation using a limitedimmunohistochemical panel. Arch Pathol Lab Med. 2002;126:1057–1063.
176. Carcangiu ML, Chambers JT. Sex steroid receptors in gynecologic neo-plasms. Pathol Annu. 1992;27(pt 2):121–151.
177. Cagle PT, Mody DR, Schwartz MR. Estrogen and progesterone receptorsin bronchogenic carcinoma. Cancer Res. 1990;50:6632–6635.
178. Ollayos CW, Riordan GP, Rushin JM. Estrogen receptor detection in par-affin sections of adenocarcinoma of the colon, pancreas, and lung. Arch PatholLab Med. 1994;118:630–632.
179. Vargas SO, Leslie KO, Vacek PM, Socinski MA, Weaver DL. Estrogen-receptor-related protein p29 in primary nonsmall cell lung carcinoma: pathologicand prognostic correlations. Cancer. 1998;82:1495–1500.
180. Diaz NM, Mazoujian G, Wick MR. Estrogen-receptor protein in thyroidneoplasms: an immunohistochemical analysis of papillary carcinoma, follicularcarcinoma, and follicular adenoma. Arch Pathol Lab Med. 1991;115:1203–1207.
181. Wu CW, Chi CW, Chang TJ, Lui WY, P’eng FK. Sex hormone receptorsin gastric cancer. Cancer. 1990;65:1396–1400.
182. Mazoujian G, Pinkus GS, Davis S, Haagensen DE Jr. Immunohistochem-istry of a gross cystic disease fluid protein (GCDFP-15) of the breast: a marker ofapocrine epithelium and breast carcinomas with apocrine features. Am J Pathol.1983;110:105–112.
183. Viacava P, Naccarato AG, Bevilacqua G. Spectrum of GCDFP-15 ex-pression in human fetal and adult normal tissues. Virchows Arch. 1998;432:255–260.
184. Kaufmann O, Deidesheimer T, Muehlenberg M, Deicke P, Dietel M. Im-munohistochemical differentiation of metastatic breast carcinomas from meta-static adenocarcinomas of other common primary sites. Histopathology. 1996;29:233–240.
185. Wick MR, Lillemoe TJ, Copland GT, Swanson PE, Manivel JC, Kiang DT.Gross cystic disease fluid protein-15 as a marker for breast cancer: immunohis-tochemical analysis of 690 human neoplasms and comparison with alpha-lact-albumin. Hum Pathol. 1989;20:281–287.
186. Raab SS, Berg LC, Swanson PE, Wick MR. Adenocarcinoma in the lungin patients with breast cancer: a prospective analysis of the discriminatory valueof immunohistology. Am J Clin Pathol. 1993;100:27–35.
187. Tian W, Osawa M, Horiuchi H, Tomita Y. Expression of the prolactin-inducible protein (PIP/GCDFP15) gene in benign epithelium and adenocarcinomaof the prostate. Cancer Sci. 2004;95:491–495.
188. Bhargava R, Beriwal S, Dabbs DJ. Mammaglobin vs GCDFP-15: an im-munohistologic validation survey for sensitivity and specificity. Am J Clin Pathol.2007;127:1–11.
189. Han JH, Kang Y, Shin HC, et al. Mammaglobin expression in lymph nodesis an important marker of metastatic breast carcinoma. Arch Pathol Lab Med.2003;127:1330–1334.
190. Sasaki E, Tsunoda N, Hatanaka Y, Mori N, Iwata H, Yatabe Y. Breast-specific expression of MGB1/mammaglobin: an examination of 480 tumors fromvarious organs and clinicopathological analysis of MGB1-positive breast cancers.Mod Pathol. 2007;20:208–214.
191. McGregor DK, Khurana KK, Cao C, et al. Diagnosing primary and met-astatic renal cell carcinoma: the use of the monoclonal antibody ‘renal cell car-cinoma marker.’ Am J Surg Pathol. 2001;25:1485–1492.
192. Avery AK, Beckstead J, Renshaw AA, Corless CL. Use of antibodies toRCC and CD10 in the differential diagnosis of renal neoplasms. Am J Surg Pathol.2000;24:203–210.
193. Genega EM, Hutchinson B, Reuter VE, Gaudin PB. Immunophenotype ofhigh-grade prostatic adenocarcinoma and urothelial carcinoma. Mod Pathol.2000;13:1186–1191.
194. Levesque M, Hu H, D’Costa M, Diamandis EP. Prostate-specific antigenexpression by various tumors. J Clin Lab Anal. 1995;9:123–128.
195. Bostwick DG. Prostate-specific antigen: current role in diagnostic pa-thology of prostate cancer. Am J Clin Pathol. 1994;102:S31–S37.
196. Alanen KA, Kuopio T, Collan YU, Kronqvist P, Juntti L, Nevalainen TJ.Immunohistochemical labelling for prostate-specific antigen in breast carcino-mas. Breast Cancer Res Treat. 1999;56:169–176.
197. Dennis JL, Hvidsten TR, Wit EC, et al. Markers of adenocarcinoma char-acteristic of the site of origin: development of a diagnostic algorithm. Clin CancerRes. 2005;11:3766–3772.
198. Varma M, Berney DM, Jasani B, Rhodes A. Technical variations in pros-tatic immunohistochemistry: need for standardisation and stringent quality assur-ance in PSA and PSAP immunostaining. J Clin Pathol. 2004;57:687–690.
199. Steffens J, Friedmann W, Lobeck H. Immunohistochemical diagnosis ofthe metastasizing prostatic carcinoma. Eur Urol. 1985;11:91–94.
200. Goldstein NS. Immunophenotypic characterization of 225 prostate ade-nocarcinomas with intermediate or high Gleason scores. Am J Clin Pathol. 2002;117:471–477.
201. Keillor JS, Aterman K. The response of poorly differentiated prostatic tu-mors to staining for prostate specific antigen and prostatic acid phosphatase: acomparative study. J Urol. 1987;137:894–896.
202. Abrahamsson PA, Lilja H. Three predominant prostatic proteins. Andro-logia. 1990;22(suppl 1):122–131.
203. Stein BS, Vangore S, Petersen RO. Immunoperoxidase localization ofprostatic antigens: comparison of primary and metastatic sites. Urology. 1984;24:146–152.
204. Jiang Z, Wu CL, Woda BA, et al. Alpha-methylacyl-CoA racemase: a mul-ti-institutional study of a new prostate cancer marker. Histopathology. 2004;45:218–225.
205. Jiang Z, Fanger GR, Woda BA, et al. Expression of alpha-methylacyl-CoAracemase (P504s) in various malignant neoplasms and normal tissues: a study of761 cases. Hum Pathol. 2003;34:792–796.
206. Ordonez NG. Value of thrombomodulin immunostaining in the diagnosisof transitional cell carcinoma: a comparative study with carcinoembryonic anti-gen. Histopathology. 1997;31:517–524.
207. Ordonez NG. Thrombomodulin expression in transitional cell carcinoma.Am J Clin Pathol. 1998;110:385–390.
208. Comin CE, Novelli L, Boddi V, Paglierani M, Dini S. Calretinin, throm-bomodulin, CEA, and CD15: a useful combination of immunohistochemicalmarkers for differentiating pleural epithelial mesothelioma from peripheral pul-monary adenocarcinoma. Hum Pathol. 2001;32:529–536.
209. Kaufmann O, Volmerig J, Dietel M. Uroplakin III is a highly specific andmoderately sensitive immunohistochemical marker for primary and metastaticurothelial carcinomas. Am J Clin Pathol. 2000;113:683–687.
210. Kunju LP, Mehra R, Snyder M, Shah RB. Prostate-specific antigen, high-molecular-weight cytokeratin (clone 34�E12), and/or p63: an optimal immuno-histochemical panel to distinguish poorly differentiated prostate adenocarcinomafrom urothelial carcinoma. Am J Clin Pathol. 2006;125:675–681.
211. Mhawech P, Uchida T, Pelte MF. Immunohistochemical profile of high-grade urothelial bladder carcinoma and prostate adenocarcinoma. Hum Pathol.2002;33:1136–1140.
212. Stewart CJ, Jeffers MD, Kennedy A. Diagnostic value of inhibin immu-noreactivity in ovarian gonadal stromal tumours and their histological mimics.Histopathology. 1997;31:67–74.
213. McCluggage WG, Shanks JH, Whiteside C, Maxwell P, Banerjee SS, Big-gart JD. Immunohistochemical study of testicular sex cord-stromal tumors, in-cluding staining with anti-inhibin antibody. Am J Surg Pathol. 1998;22:615–619.
214. Iczkowski KA, Bostwick DG, Roche PC, Cheville JC. Inhibin A is a sen-sitive and specific marker for testicular sex cord-stromal tumors. Mod Pathol.1998;11:774–779.
215. Movahedi-Lankarani S, Kurman RJ. Calretinin, a more sensitive but lessspecific marker than alpha-inhibin for ovarian sex cord-stromal neoplasms: animmunohistochemical study of 215 cases. Am J Surg Pathol. 2002;26:1477–1483.
216. Zhang PJ, Genega EM, Tomaszewski JE, Pasha TL, Livolsi VA. The role ofcalretinin, inhibin, melan-A, BCL-2, and C-kit in differentiating adrenal corticaland medullary tumors: an immunohistochemical study. Mod Pathol. 2003;16:591–597.
217. Pelkey TJ, Frierson HF Jr, Mills SE, Stoler MH. The alpha subunit of inhibinin adrenal cortical neoplasia. Mod Pathol. 1998;11:516–524.
218. Renshaw AA, Granter SR. A comparison of A103 and inhibin reactivityin adrenal cortical tumors: distinction from hepatocellular carcinoma and renaltumors. Mod Pathol. 1998;11:1160–1164.

Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al 347
219. Busam KJ, Jungbluth AA. Melan-A, a new melanocytic differentiationmarker. Adv Anat Pathol. 1999;6:12–18.
220. Ghorab Z, Jorda M, Ganjei P, Nadji M. Melan A (A103) is expressed inadrenocortical neoplasms but not in renal cell and hepatocellular carcinomas.Appl Immunohistochem Mol Morphol. 2003;11:330–333.
221. Jungbluth AA, Busam KJ, Gerald WL, et al. A103: an anti-melan-a mono-clonal antibody for the detection of malignant melanoma in paraffin-embeddedtissues. Am J Surg Pathol. 1998;22:595–602.
222. Doglioni C, Tos AP, Laurino L, et al. Calretinin: a novel immunocyto-chemical marker for mesothelioma. Am J Surg Pathol. 1996;20:1037–1046.
223. Chhieng DC, Yee H, Schaefer D, et al. Calretinin staining pattern aids inthe differentiation of mesothelioma from adenocarcinoma in serous effusions.Cancer. 2000;90:194–200.
224. McCluggage WG, Maxwell P. Immunohistochemical staining for calretin-in is useful in the diagnosis of ovarian sex cord-stromal tumours. Histopathology.2001;38:403–408.
225. Deavers MT, Malpica A, Liu J, Broaddus R, Silva EG. Ovarian sex cord-stromal tumors: an immunohistochemical study including a comparison of cal-retinin and inhibin. Mod Pathol. 2003;16:584–590.
226. Ordonez NG. Application of mesothelin immunostaining in tumor diag-nosis. Am J Surg Pathol. 2003;27:1418–1428.
227. Foster MR, Johnson JE, Olson SJ, Allred DC. Immunohistochemical anal-ysis of nuclear versus cytoplasmic staining of WT1 in malignant mesotheliomasand primary pulmonary adenocarcinomas. Arch Pathol Lab Med. 2001;125:1316–1320.
228. O’Neill CJ, Deavers MT, Malpica A, Foster H, McCluggage WG. An im-munohistochemical comparison between low-grade and high-grade ovarian se-rous carcinomas: significantly higher expression of p53, MIB1, BCL2, HER-2/neu,and C-KIT in high-grade neoplasms. Am J Surg Pathol. 2005;29:1034–1041.
229. Barnetson RJ, Burnett RA, Downie I, Harper CM, Roberts F. Immunohis-tochemical analysis of peritoneal mesothelioma and primary and secondary se-rous carcinoma of the peritoneum: antibodies to estrogen and progesterone re-ceptors are useful. Am J Clin Pathol. 2006;125:67–76.
230. Chu AY, Litzky LA, Pasha TL, Acs G, Zhang PJ. Utility of D2-40, a novelmesothelial marker, in the diagnosis of malignant mesothelioma. Mod Pathol.2005;18:105–110.
231. Comin CE, Dini S, Novelli L, Santi R, Asirelli G, Messerini L. h-Caldes-mon, a useful positive marker in the diagnosis of pleural malignant mesothelioma,epithelioid type. Am J Surg Pathol. 2006;30:463–469.
232. Hishima T, Fukayama M, Fujisawa M, et al. CD5 expression in thymiccarcinoma. Am J Pathol. 1994;145:268–275.
233. Berezowski K, Grimes MM, Gal A, Kornstein MJ. CD5 immunoreactivityof epithelial cells in thymic carcinoma and CASTLE using paraffin-embeddedtissue. Am J Clin Pathol. 1996;106:483–486.
234. Tateyama H, Eimoto T, Tada T, Hattori H, Murase T, Takino H. Immuno-reactivity of a new CD5 antibody with normal epithelium and malignant tumorsincluding thymic carcinoma. Am J Clin Pathol. 1999;111:235–240.
235. Kornstein MJ, Rosai J. CD5 labeling of thymic carcinomas and other non-lymphoid neoplasms. Am J Clin Pathol. 1998;109:722–726.
236. Dorfman DM, Shahsafaei A, Chan JK. Thymic carcinomas, but not thy-momas and carcinomas of other sites, show CD5 immunoreactivity. Am J SurgPathol. 1997;21:936–940.
237. Bailey D, Marks A, Stratis M, Baumal R. Immunohistochemical stainingof germ cell tumors and intratubular malignant germ cells of the testis usingantibody to placental alkaline phosphatase and a monoclonal anti-seminoma an-tibody. Mod Pathol. 1991;4:167–171.
238. Burke AP, Mostofi FK. Placental alkaline phosphatase immunohistochem-istry of intratubular malignant germ cells and associated testicular germ cell tu-mors. Hum Pathol. 1988;19:663–670.
239. Goldsmith JD, Pawel B, Goldblum JR, et al. Detection and diagnosticutilization of placental alkaline phosphatase in muscular tissue and tumors withmyogenic differentiation. Am J Surg Pathol. 2002;26:1627–1633.
240. Looijenga LH, Stoop H, de Leeuw HP, et al. POU5F1 (OCT3/4) identifiescells with pluripotent potential in human germ cell tumors. Cancer Res. 2003;63:2244–2250.
241. Jones TD, Ulbright TM, Eble JN, Baldridge LA, Cheng L. OCT4 stainingin testicular tumors: a sensitive and specific marker for seminoma and embryonalcarcinoma. Am J Surg Pathol. 2004;28:935–940.
242. Cheng L. Establishing a germ cell origin for metastatic tumors using OCT4immunohistochemistry. Cancer. 2004;101:2006–2010.
243. Fletcher CD. Pleomorphic malignant fibrous histiocytoma: fact or fiction?A critical reappraisal based on 159 tumors diagnosed as pleomorphic sarcoma.Am J Surg Pathol. 1992;16:213–228.
244. Coindre JM, Mariani O, Chibon F, et al. Most malignant fibrous histio-cytomas developed in the retroperitoneum are dedifferentiated liposarcomas: areview of 25 cases initially diagnosed as malignant fibrous histiocytoma. ModPathol. 2003;16:256–262.
245. Fletcher CD, Gustafson P, Rydholm A, Willen H, Akerman M. Clinico-pathologic re-evaluation of 100 malignant fibrous histiocytomas: prognostic rel-evance of subclassification. J Clin Oncol. 2001;19:3045–3050.
246. Mertens F, Fletcher CD, Dal Cin P, et al. Cytogenetic analysis of 46 pleo-morphic soft tissue sarcomas and correlation with morphologic and clinical fea-tures: a report of the CHAMP Study Group. Chromosomes and MorPhology.Genes Chromosomes Cancer. 1998;22:16–25.
247. Oda Y, Miyajima K, Kawaguchi K, et al. Pleomorphic leiomyosarcoma:
clinicopathologic and immunohistochemical study with special emphasis on itsdistinction from ordinary leiomyosarcoma and malignant fibrous histiocytoma.Am J Surg Pathol. 2001;25:1030–1038.
248. Ceballos KM, Nielsen GP, Selig MK, O’Connell JX. Is anti-h-caldesmonuseful for distinguishing smooth muscle and myofibroblastic tumors? An immu-nohistochemical study. Am J Clin Pathol. 2000;114:746–753.
249. Watanabe K, Kusakabe T, Hoshi N, Saito A, Suzuki T. h-Caldesmon inleiomyosarcoma and tumors with smooth muscle cell-like differentiation: its spe-cific expression in the smooth muscle cell tumor. Hum Pathol. 1999;30:392–396.
250. Gaffney EF, Dervan PA, Fletcher CD. Pleomorphic rhabdomyosarcoma inadulthood: analysis of 11 cases with definition of diagnostic criteria. Am J SurgPathol. 1993;17:601–609.
251. Furlong MA, Mentzel T, Fanburg-Smith JC. Pleomorphic rhabdomyosar-coma in adults: a clinicopathologic study of 38 cases with emphasis on morpho-logic variants and recent skeletal muscle-specific markers. Mod Pathol. 2001;14:595–603.
252. Dei Tos AP, Wadden C, Fletcher CDM. S-100 protein staining in liposar-coma: its diagnostic utility in the high-grade myxoid (round cell) variant. ApplImmunohistochem. 1996;4:95–101.
253. Gebhard S, Coindre JM, Michels JJ, et al. Pleomorphic liposarcoma: clin-icopathologic, immunohistochemical, and follow-up analysis of 63 cases: a studyfrom the French Federation of Cancer Centers Sarcoma Group. Am J Surg Pathol.2002;26:601–616.
254. Hornick JL, Bosenberg MW, Mentzel T, McMenamin ME, Oliveira AM,Fletcher CD. Pleomorphic liposarcoma: clinicopathologic analysis of 57 cases.Am J Surg Pathol. 2004;28:1257–1267.
255. Miettinen M, Enzinger FM. Epithelioid variant of pleomorphic liposar-coma: a study of 12 cases of a distinctive variant of high-grade liposarcoma. ModPathol. 1999;12:722–728.
256. Hasegawa T, Seki K, Hasegawa F, et al. Dedifferentiated liposarcoma ofretroperitoneum and mesentery: varied growth patterns and histological grades—a clinicopathologic study of 32 cases. Hum Pathol. 2000;31:717–727.
257. Joyner CJ, Triffitt J, Puddle B, Athanasou NA. Development of a mono-clonal antibody to the aP2 protein to identify adipocyte precursors in tumours ofadipose differentiation. Pathol Res Pract. 1999;195:461–466.
258. Binh MB, Sastre-Garau X, Guillou L, et al. MDM2 and CDK4 immuno-stainings are useful adjuncts in diagnosing well-differentiated and dedifferentiatedliposarcoma subtypes: a comparative analysis of 559 soft tissue neoplasms withgenetic data. Am J Surg Pathol. 2005;29:1340–1347.
259. Meis JM, Enzinger FM, Martz KL, Neal JA. Malignant peripheral nervesheath tumors (malignant schwannomas) in children. Am J Surg Pathol. 1992;16:694–707.
260. Hoang MP, Sinkre P, Albores-Saavedra J. Expression of protein gene prod-uct 9.5 in epithelioid and conventional malignant peripheral nerve sheath tumors.Arch Pathol Lab Med. 2001;125:1321–1325.
261. Smith TA, Machen SK, Fisher C, Goldblum JR. Usefulness of cytokeratinsubsets for distinguishing monophasic synovial sarcoma from malignant periph-eral nerve sheath tumor. Am J Clin Pathol. 1999;112:641–648.
262. Zhou H, Coffin CM, Perkins SL, Tripp SR, Liew M, Viskochil DH. Malig-nant peripheral nerve sheath tumor: a comparison of grade, immunophenotype,and cell cycle/growth activation marker expression in sporadic and neurofibro-matosis 1-related lesions. Am J Surg Pathol. 2003;27:1337–1345.
263. Litzky LA, Brooks JJ. Cytokeratin immunoreactivity in malignant fibroushistiocytoma and spindle cell tumors: comparison between frozen and paraffin-embedded tissues. Mod Pathol. 1992;5:30–34.
264. Rosenberg AE, O’Connell JX, Dickersin GR, Bhan AK. Expression of ep-ithelial markers in malignant fibrous histiocytoma of the musculoskeletal system:an immunohistochemical and electron microscopic study. Hum Pathol. 1993;24:284–293.
265. Wick MR, Swanson PE. Carcinosarcomas: current perspectives and anhistorical review of nosological concepts. Semin Diagn Pathol. 1993;10:118–127.
266. Nappi O, Glasner SD, Swanson PE, Wick MR. Biphasic and monophasicsarcomatoid carcinomas of the lung: a reappraisal of ‘carcinosarcomas’ and ‘spin-dle-cell carcinomas.’ Am J Clin Pathol. 1994;102:331–340.
267. Carter MR, Hornick JL, Lester S, Fletcher CD. Spindle cell (sarcomatoid)carcinoma of the breast: a clinicopathologic and immunohistochemical analysisof 29 cases. Am J Surg Pathol. 2006;30:300–309.
268. Ikegami H, Iwasaki H, Ohjimi Y, Takeuchi T, Ariyoshi A, Kikuchi M. Sar-comatoid carcinoma of the urinary bladder: a clinicopathologic and immunohis-tochemical analysis of 14 patients. Hum Pathol. 2000;31:332–340.
269. Lewis JE, Olsen KD, Sebo TJ. Spindle cell carcinoma of the larynx: reviewof 26 cases including DNA content and immunohistochemistry. Hum Pathol.1997;28:664–673.
270. Thompson LD, Wieneke JA, Miettinen M, Heffner DK. Spindle cell (sar-comatoid) carcinomas of the larynx: a clinicopathologic study of 187 cases. AmJ Surg Pathol. 2002;26:153–170.
271. Lewis JS, Ritter JH, El Mofty S. Alternative epithelial markers in sarco-matoid carcinomas of the head and neck, lung, and bladder-p63, MOC-31, andTTF-1. Mod Pathol. 2005;18:1471–1481.
272. Suster S, Moran CA. Applications and limitations of immunohistochem-istry in the diagnosis of malignant mesothelioma. Adv Anat Pathol. 2006;13:316–329.
273. Kung IT, Thallas V, Spencer EJ, Wilson SM. Expression of muscle actinsin diffuse mesotheliomas. Hum Pathol. 1995;26:565–570.
274. Lucas DR, Pass HI, Madan SK, et al. Sarcomatoid mesothelioma and its

348 Arch Pathol Lab Med—Vol 132, March 2008 Undifferentiated Tumor, Immunohistochemistry—Bahrami et al
histological mimics: a comparative immunohistochemical study. Histopathology.2003;42:270–279.
275. Hinterberger M, Reineke T, Storz M, Weder W, Vogt P, Holger M. D2-40and calretinin-a tissue microarray analysis of 341 malignant mesotheliomas withemphasis on sarcomatoid differentiation. Mod Pathol. 2007;20:248–255.
276. Skelton HG, Smith KJ, Laskin WB, et al. Desmoplastic malignant mela-noma. J Am Acad Dermatol. 1995;32:717–725.
277. Miettinen M, Fanburg-Smith JC, Virolainen M, Shmookler BM, Fetsch JF.Epithelioid sarcoma: an immunohistochemical analysis of 112 classical and var-iant cases and a discussion of the differential diagnosis. Hum Pathol. 1999;30:934–942.
278. Manivel JC, Wick MR, Dehner LP, Sibley RK. Epithelioid sarcoma: animmunohistochemical study. Am J Clin Pathol. 1987;87:319–326.
279. Hasegawa T, Matsuno Y, Shimoda T, Umeda T, Yokoyama R, Hirohashi S.Proximal-type epithelioid sarcoma: a clinicopathologic study of 20 cases. ModPathol. 2001;14:655–663.
280. Arber DA, Kandalaft PL, Mehta P, Battifora H. Vimentin-negative epithe-lioid sarcoma: the value of an immunohistochemical panel that includes CD34.Am J Surg Pathol. 1993;17:302–307.
281. Fletcher CD, Beham A, Bekir S, Clarke AM, Marley NJ. Epithelioid an-giosarcoma of deep soft tissue: a distinctive tumor readily mistaken for an epi-thelial neoplasm. Am J Surg Pathol. 1991;15:915–924.
282. Deshpande V, Rosenberg AE, O’Connell JX, Nielsen GP. Epithelioid an-giosarcoma of the bone: a series of 10 cases. Am J Surg Pathol. 2003;27:709–716.
283. Zhang PJ, Livolsi VA, Brooks JJ. Malignant epithelioid vascular tumors ofthe pleura: report of a series and literature review. Hum Pathol. 2000;31:29–34.
284. Meis-Kindblom JM, Kindblom LG. Angiosarcoma of soft tissue: a studyof 80 cases. Am J Surg Pathol. 1998;22:683–697.
285. Granter SR, Weilbaecher KN, Quigley C, Fletcher CD, Fisher DE. Clearcell sarcoma shows immunoreactivity for microphthalmia transcription factor: fur-ther evidence for melanocytic differentiation. Mod Pathol. 2001;14:6–9.
286. Swanson PE, Wick MR. Clear cell sarcoma: an immunohistochemicalanalysis of six cases and comparison with other epithelioid neoplasms of softtissue. Arch Pathol Lab Med. 1989;113:55–60.
287. Fujimura Y, Ohno T, Siddique H, Lee L, Rao VN, Reddy ES. The EWS-ATF-1 gene involved in malignant melanoma of soft parts with t(12;22) chro-
mosome translocation, encodes a constitutive transcriptional activator. Onco-gene. 1996;12:159–167.
288. Laskin WB, Weiss SW, Bratthauer GL. Epithelioid variant of malignantperipheral nerve sheath tumor (malignant epithelioid schwannoma). Am J SurgPathol. 1991;15:1136–1145.
289. Bonetti F, Pea M, Martignoni G, et al. Clear cell (‘‘sugar’’) tumor of thelung is a lesion strictly related to angiomyolipoma—the concept of a family oflesions characterized by the presence of the perivascular epithelioid cells (PEC).Pathology. 1994;26:230–236.
290. Folpe AL, Mentzel T, Lehr HA, Fisher C, Balzer BL, Weiss SW. Perivascularepithelioid cell neoplasms of soft tissue and gynecologic origin: a clinicopatho-logic study of 26 cases and review of the literature. Am J Surg Pathol. 2005;29:1558–1575.
291. Zamboni G, Pea M, Martignoni G, et al. Clear cell ‘‘sugar’’ tumor of thepancreas: a novel member of the family of lesions characterized by the presenceof perivascular epithelioid cells. Am J Surg Pathol. 1996;20:722–730.
292. Martignoni G, Pea M, Reghellin D, Zamboni G, Bonetti F. Perivascularepithelioid cell tumor (PEComa) in the genitourinary tract. Adv Anat Pathol. 2007;14:36–41.
293. Costa MJ, DeRose PB, Roth LM, Brescia RJ, Zaloudek CJ, Cohen C. Im-munohistochemical phenotype of ovarian granulosa cell tumors: absence of ep-ithelial membrane antigen has diagnostic value. Hum Pathol. 1994;25:60–66.
294. Miettinen M, Sobin LH, Lasota J. Gastrointestinal stromal tumors of thestomach: a clinicopathologic, immunohistochemical, and molecular geneticstudy of 1765 cases with long-term follow-up. Am J Surg Pathol. 2005;29:52–68.
295. Bacchi CE, Bonetti F, Pea M, Martignoni G, Gown AM. HMB-45: a re-view. Appl Immunohistochem. 1996;4:73–85.
296. Ben Izhak O, Stark P, Levy R, Bergman R, Lichtig C. Epithelial markersin malignant melanoma: a study of primary lesions and their metastases. Am JDermatopathol. 1994;16:241–246.
297. Jaffe ES, Harris NL, Stein H, Vardiman JW. Pathology and Genetics ofTumours of Haematopoietic and Lymphoid Tissues. Lyon, France: IARC Press;2001:230–235. World Health Organization Classification of Tumours.
298. Chott A, Kaserer K, Augustin I, et al. Ki-1-positive large cell lymphoma:a clinicopathologic study of 41 cases. Am J Surg Pathol. 1990;14:439–448.
299. Agnarsson BA, Kadin ME. Ki-1 positive large cell lymphoma: a morpho-logic and immunologic study of 19 cases. Am J Surg Pathol. 1988;12:264–274.
300. O’Connell FP, Pinkus JL, Pinkus GS. CD138 (syndecan-1), a plasma cellmarker immunohistochemical profile in hematopoietic and nonhematopoieticneoplasms. Am J Clin Pathol. 2004;121:254–263.