Embed Size (px)
Citation preview

van de Putte LB. Effects of hydroxychloroquine and sulphasalazineon progression of joint damage in rheumatoid arthritis. Lancet1989;1:1036–8.
9. Huizinga TW, Amos CI, van der Helm-van Mil AH, Chen W, van
Gaalen FA, Jawaheer D, et al. Refining the complex rheumatoidarthritis phenotype based on specificity of the HLA–DRB1 sharedepitope for antibodies to citrullinated proteins. Arthritis Rheum2005;52:3433–8.
DOI 10.1002/art.21820
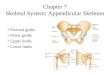
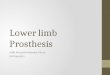
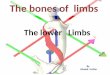
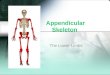
Clinical Images: Tropical pyomyositis of the lower limbs
The patient, a 45-year-old woman, presented with a 2-week history of fever associated with marked swelling, erythema, and painover the left lower limb. Ultrasound revealed a diffuse area of altered echotexture with thickening in the left upper thigh and glutealregion suggestive of myositis; however, no fluid collection was seen. Subsequent magnetic resonance imaging (MRI) (STIR coronalimage [A] and T2-weighted fat-saturated axial image [B]) confirmed the presence of pyomyositis, with extensive edema in thesubcutaneous fat and muscles of the thighs, glutei, and calves, along with foci of pus collections in the anterior, medial, and posteriorcompartments of the left thigh. Surgical incision yielded 350 ml of pus, which grew Escherichia coli. Tropical pyomyositis is a primaryinfection of skeletal muscle that often progresses to suppuration. Commonly affected muscles are the quadriceps, iliopsoas, andgastrocnemius; multiple muscle groups can be involved (1,2). Trauma, vigorous exercise, and immunocompromised states (e.g.,human immunodeficiency virus infection) predispose to this condition (3). Staphylococcus aureus is the most commonly culturedorganism (up to 90% of cases in tropical areas); other causative organisms include Streptococcus, Pneumococcus, Neisseria,Haemophilus, Aeromonas, Serratia, Yersinia, Pseudomonas, Klebsiella, and Escherichia (4). Computed tomography and MRI are thebest modalities for early diagnosis; with ultrasound, the diagnosis may be missed in the early stage, when suppuration has not yetoccurred (5).
1. Gambhir IS, Singh DS, Gupta SS, Gupta PR, Kumar M. Tropical pyomyositisin India: a clinico-histopathological study. J Trop Med Hyg 1992;95:42–6.
2. Malhotra P, Singh S, Sud A, Kumari S. Tropical pyomyositis: experience of atertiary care hospital in north-west India. J Assoc Physicians India 2000;48:1057–9.
3. Christin L, Sarosi GA. Pyomyositis in North America: case reports andreview. Clin Infect Dis 1992;15:668–77.
4. Chauhan S, Jain S, Varma S, Chauhan SS. Tropical pyomyositis (myositistropicans): current perspective. Postgrad Med J 2004;80:267–70.
5. Boniotti V, Carlone N, Perboni G, Caudana R. Contribution of imaging to theevaluation of pyomyositis. Radiol Med (Torino) 2005;109:404–13.
Rahul Grover, MDVarun Dhir, MDKannan Guruprasad, MDAtin Kumar, MDRohini Handa, MDAll India Institute of Medical SciencesNew Delhi, India
2030 CONCISE COMMUNICATIONS