Embed Size (px)
Citation preview
TROPHOCARCINOMA (EMBRYONAL CARCINOMA) OF THE TESTIS
Factors Inf luencing Radiat ion and Surgical Treatment
MILTON FRIEDMAN, M.D., AND AXTONIO J. DT RIENZO, M.D.
ROPHOCARCINOMA, A PRIMITIVE PLACEN- T tal tumor generally designated as “em- bryonal carcinoma,” comprises 25% of all germ cell tumors of the testis. Prior to World War 11, not many cases were cured. There- after, the cure rate improved as a result of better understanding of histogenesis, radio- sensitivity classification, clinical staging, and improved surgical and radiation treat-
This paper will discuss the relationships among histogenesis, characteristic clinical fea- tures, treatment, and proposis.
The histological picture varies considerably because the tumor recapitulates successive stages in the development of the placenta (Fig. 1). Nevertheless the common denomina- tor of these lesions is the characteristic clinical behavior.
The term “trophocarcinoma” is more appro- priate than “embryonal carcinoma” because the tumor is derived from trophoblasts. All germ cell tumors of the testis are embryonal. Even the relatively innocent teratoma is more closely related to embryonal structures than is trophocarcinoma. Nevertheless the term “trophocarcinoma” has not been accepted since it was first proffered in 1943.6
mait.1-3, 5 , 9
-- From the Lila Motley Radiation Therapy Division,
Department of Radiology, New York University School of Medicine, 550 First Ave., New York, N.Y., and the Hospital for Joint Diseases, New York. N.Y.
The photomicrographs were made at the Armed Forces Institute of Pathology, Washington, D.C.
The opinions expressed herein are those of the au- thors and are not n d l y sponsored by the Armed Forces Institute of Pathology.
Figure 10 is reprinted by courtesy of Radiology, 1961.’0
Received for publication Nov. 26, 1962.
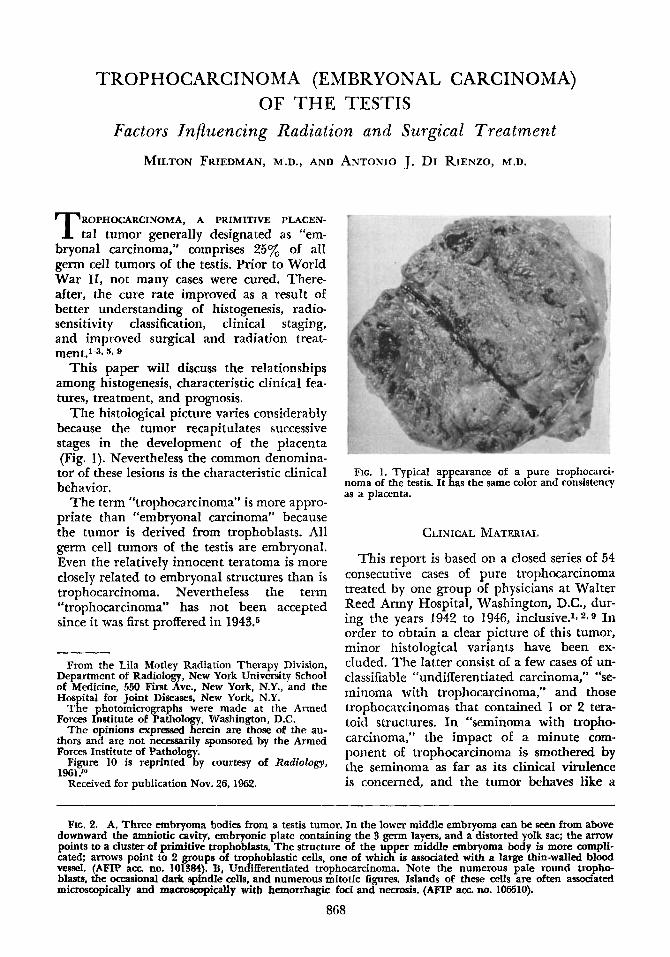
FIG. 1. Typical appearance of a pure trophocard- noma of the testis. I t has the same color and consistency as a placenta.
CLINICAL MATERIAL
This report is based on a closed series of 54 consecutive cases of pure trophocarcinoma treated by one group of physicians at Walter Reed Army Hospital, Washington, D.C., dur- ing the years 1942 to 1946, inclusive.1~2~9 In order to obtain a clear picture of this tumor, minor histological variants have been ex- cluded. The latter consist of a few cases of un- classifiable “undifferentiated carcinoma,” “se- minoma with trophocarcinoma,” and those trophocarcinomas that contained 1 or 2 tera- toid structures. In “seminoma with tropho- carcinoma,” the impact of a minute com- ponent of trophocarcinoma is smothered by the seminoma as far as its clinical virulence is concerned, and the tumor behaves like a
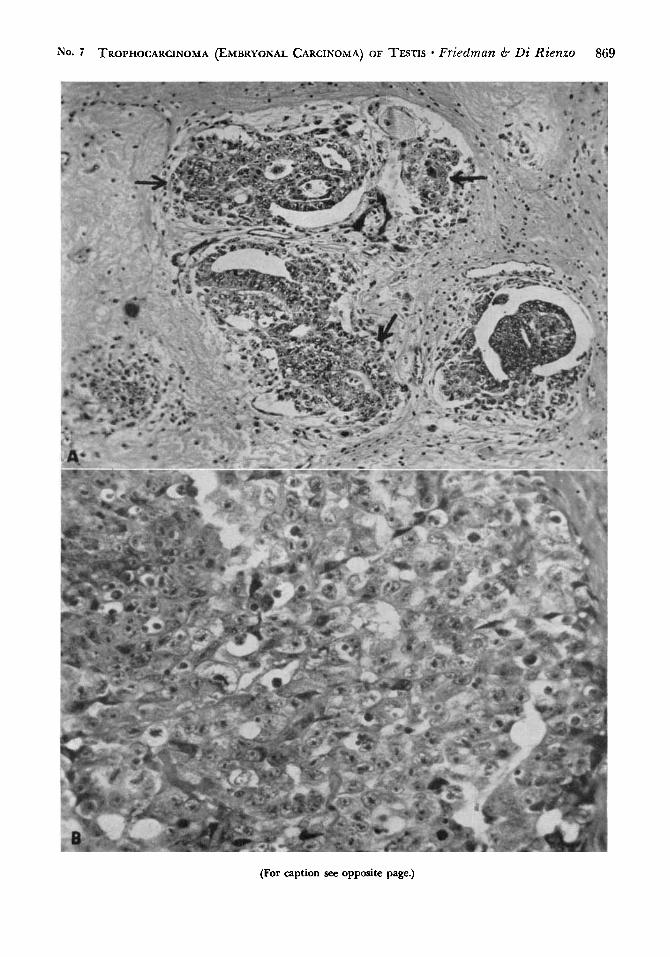
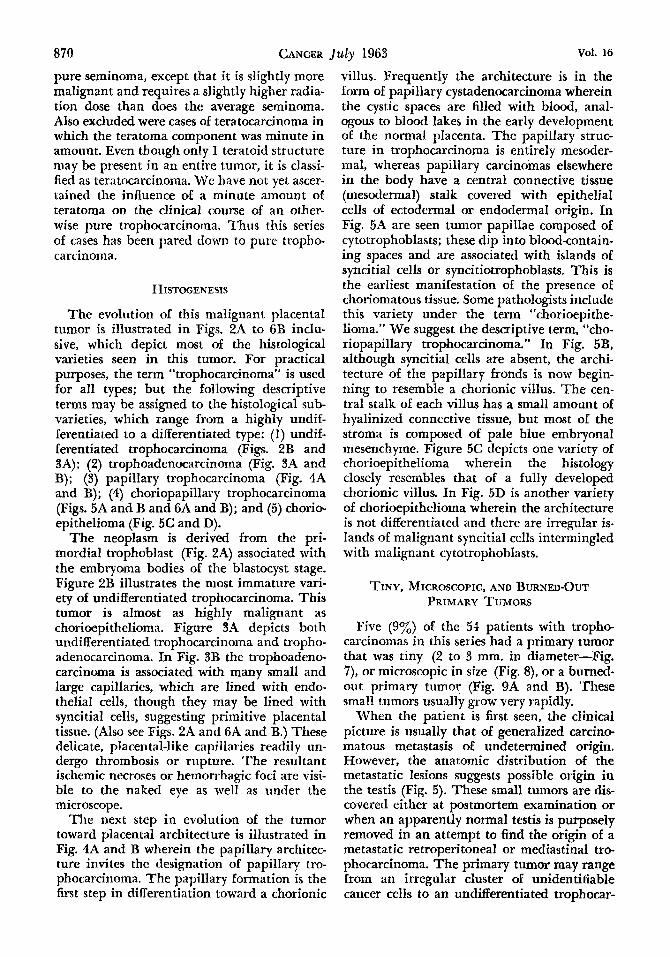
FIG. 2. A, Three embryoma bodies from a testis tumor. In the lower middle embryoma can be seen from above downward the amniotic cavity, embryonic plate containing the 3 germ layers, and a distorted yolk sac; the arrow points to a cluster of primitive trophoblasts. The structiire of the upper middle embryoma body is more compli- cated; arrows point to 2 groups of trophoblastic cells, one of which is associated with a large thin-walled blood vessel. (AFIP acc no. 101384). B, Undifferentiated trophocarcinoma. Note the numerous pale round tropho- blasts, the occasional dark spindle cells, and numerous mitotic figures. Islands of these cells are often associated microscopically and macroscopically with hemorrhagic foci and necrosis. (AFIP am. no. 106510).
868
No. 7 TROPHOCARCINOMA (EMBRYONAL CARCINOMA) OF TESTIS * Friedman 6 Di Rienzo 869
(For caption see opposite page.)
870 CANCER July 1963 Vol. 16
pure seminoma, except that it is slightly more malignant and requires a slightly higher radia- tion close than does the average seminoma. Also excluded were cases of teratocarcinoma in which the teratoma component was minute in amount. Even though only 1 teratoid structure may be present in an entire tumor, it is classi- fied as teratocarcinoma. We have not yet ascer- tained the influence of a minute amount of teratoma on the clinical course of an other- wise pure trophocarcinoma. Thus this series of cases has been pared down to pure tropho- carcinoma.
HISTOGENE~IS
The evolution of this malignant placental tumor is illustrated in Figs. 2A to 6B inclu- sive, which depict most of the histological varieties seen in this tumor. For practical purposes, the term “trophocarcinoma” is used for all types; but the following descriptive terms may be assigned to the histological sub- varieties, which range €rom a highly undif- ferentiated to a differentiated type: (1) undif- ferentiated trophocarcinoma (Figs. 2B and 3A); (2) trophoadenocarcinoma (Fig. 3A and B); (3) papillary trophocarcinoma (Fig. 4A and B); (4) choriopapillary trophocarcinoma (Figs. 5A and B and 6A and B); and (5) chorio- epithelioma (Fig. 5C and D).
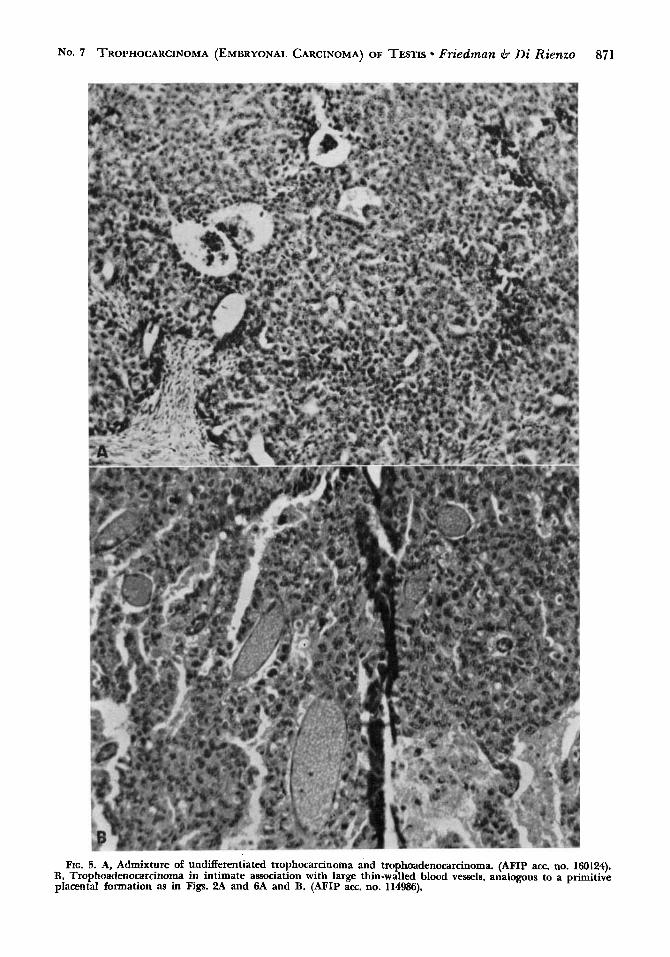
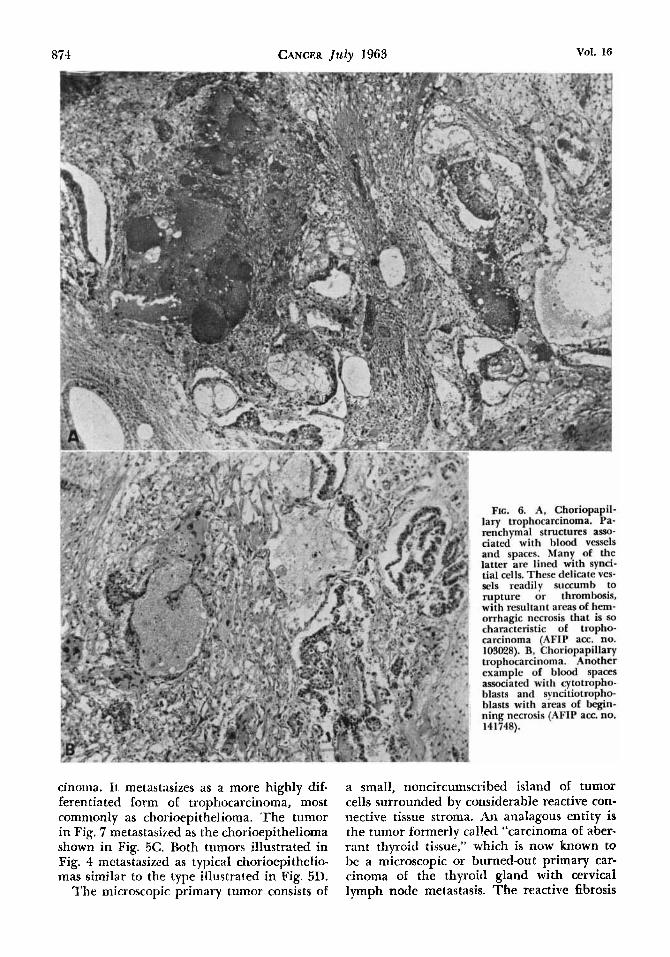
The neoplasm is derived from the pri- mordial trophoblast (Fig. 2A) associated with the embryoma bodies of the blastocyst stage. Figure 2B illustrates the most immature vari- ety of undifferentiated trophocarcinoma. This tumor is almost as highly malignant as chorioepithelioma. Figure 3A depicts both undifferentiated trophocarcinoma and tropho- adenocarcinoma. In Fig. 3B the trophoadeno- carcinoma is associated wiLh many small and large capillaries, which are lined with endo- thelial cells, though they may be lined with syncitial cells, suggesting primitive placental tissue. (Also see Figs. 2A and 6A and B.) These delicate, placental-like capillaries readily un- dergo thrombosis or rupture. The resultant ischemic necroses or hemorrhagic foci are visi- ble to the naked eye as well as under the microscope.
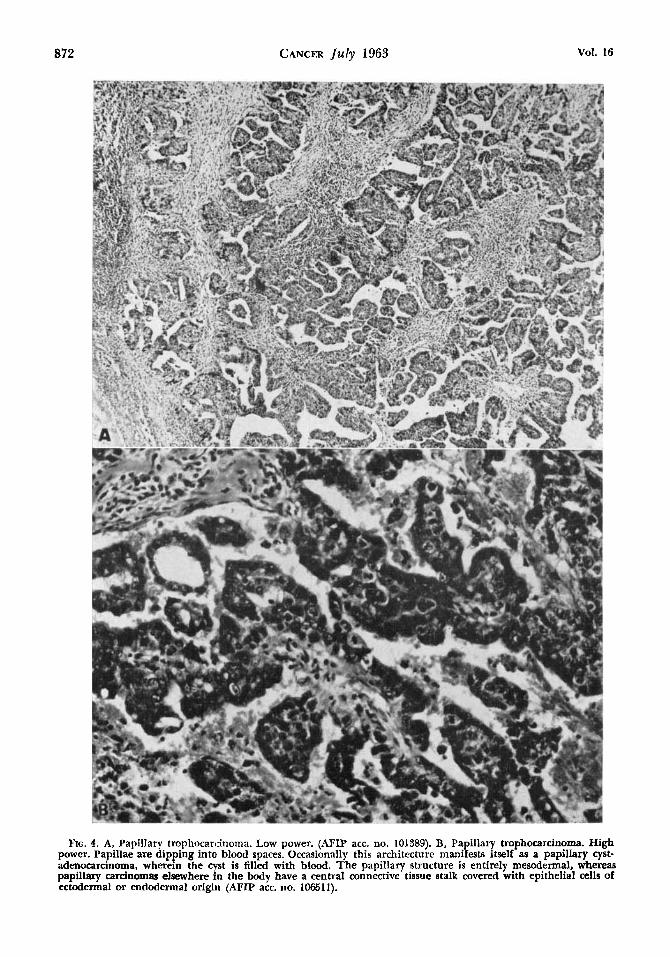
The next step in evolution of the tumor toward placental architecture is illustrated in Fig. 4A and B wherein the papillary architec- ture invites the designation of papillary tro- phocarcinoma. The papillary formation is the first step in differentiation toward a chorionic
villus. Frequently the architecture is in the form of papillary cystadenocarcinoma wherein the cystic spaces are filled with blood, anal- ogous to blood lakes in the early development of the normal placenta. The papillary struc- ture in trophocarcinoma is entirely mesoder- mal, whereas papillary carcinomas elsewhere in the body have a central connective tissue (mesodermal) stalk covered with epithelial cells of ectodermal or endodermal origin. In Fig. 5A are seen tumor papillae composed of cytotrophoblasts; these dip into blood-contain- ing spaces and are associated with islands of syncitial cells or syncitiotrophoblasts. This is the earliest manifestation of the presence of choriomatous tissue. Some pathologists include this variety under the term “chorioepithe- lioma.” We suggest the descriptive term, “cho- riopapillary trophocarcinoma.” In Fig. 5B, although syncitial cells are absent, the archi- tecture of the papillary fronds is now begin- ning to resemble a chorionic villus. The cen- tral stalk o€ each villus has a small amount of hyalinized connective tissue, but most of the stroma is composed of pale blue embryonal mesenchyme. Figure 5C depicts one variety of chorioepithelioma wherein the histology closely resembles that of a fully developed chorionic villus. In Fig. 5D is another variety of chorioepithelioma wherein the architecture is not differentiated and there are irregular is- lands of malignant syncitial cells intermingled with malignant cytotrophoblasts.
TINY, MICROSCOPIC, AND BURNED-OUT PRIMARY TUMORS
Five (9%) of the 54 patients with tropho. carcinomas in this series had a primary tumor that was tiny (2 to 3 mm. in diameter-Fig. 7), or microscopic in size (Fig. S), or a burned- out primary tumor (Fig. 9A and B). These small tumors usually grow very rapidly.
When the patient is first seen, the clinical picture is usually that of generalized carcino- matous metastasis of undetermined origin. However, the anatomic distribution of the metastatic lesions suggests possible origin in the testis (Fig. 5). These small tumors are dis- covered either at postmortem examination or when an apparently normal testis is purposely removed in an attempt to find the origin of a metastatic retroperitoneal or mediastinal tro. phocarcinoma. The primary tumor may range from an irregular cluster of unidentifiable cancer cells to an undifferentiated trophocar-
No. 7 TROPHOCARCINOMA (EMBRYONAL CARCINOMA) OF TESTIS Friedman e5 Di Rienzo 871
FIG. 3. A, Admixture of undifferentiated trophocarcinoma and tropbadenocarcinoma. (AFIP am. no. 160124). B, Trophoadenocarcinoma in intimate association with large thin-walled blood vessels, analogous to a primitive placental formation as in Figs. 2A and 6A and B. (AFIP acc. no. 114986).
872 CANCER July 1963 Vol. 16
FIG. 4. A, Papillary trophocarcinoma. Low power. (AFIP acc. no. 101389). B, Papillary trophocarcinoma. High power. Papillae are dipping into blood spaces. Occasionally this architecture manifests itself as a papillary cyst- adenocardnoma, wherein the cyst is filled with blood. The papillary structure is entirely mesodermal, whereas papillary cardnomas elsewhere i n the body have a central connective tissue stalk covered with epithelial cells of ectodermal or endodermal origin (AFIP acc. no. 106511).
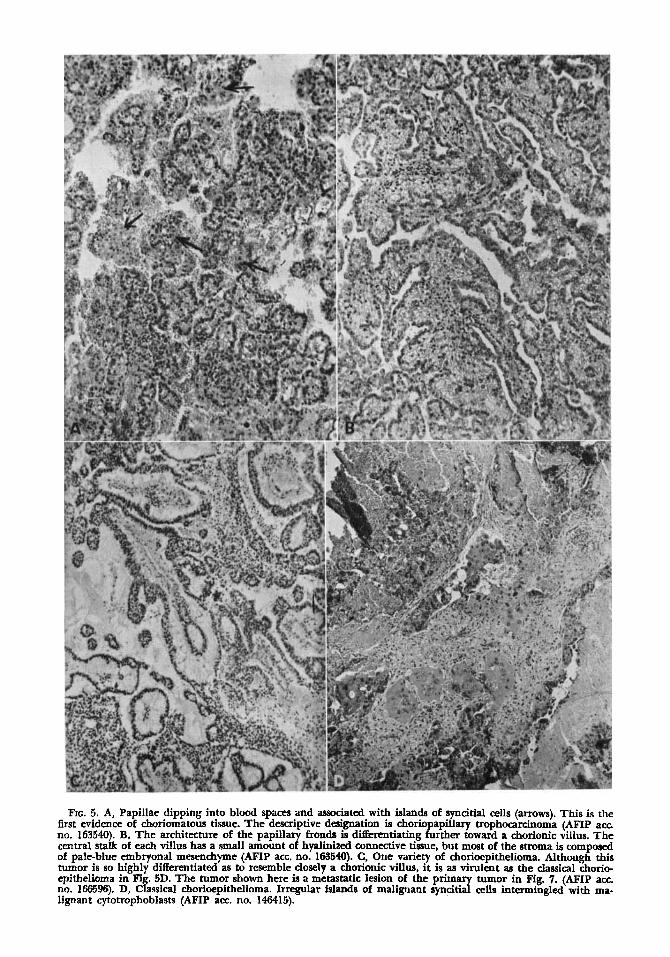
FIG. 5. A, Papillae dipping into blood spaces and associated with islands of syncitial cells (arrows). This is the first evidence of choriomatous tissue. The descriptive designation is choriopapillary trophocarcinoma (AFIP acc no. 163540). B, The architecture of the papillary fronds difEerentiating further toward a chorionic villus. The central stalk of each villus has a small amount of hyalinized connective tissue, but most of the stroma is composed of pale-blue embryonal mesenchyme (AFIP acc. no. 163540). C, One variety of chorioepithelioma. Although this tumor is so highly differentiated as to resemble closely a chorionic villus, it is as virulent as the classical chorio- epithelioma in Fig. 5D. The tumor shown here is a metastatic lesion of the primary tumor in Fig. 7. (AFIP acc. no. 166596). D, Classical chorioepithelioma. Irregular islands of malignant syncitial cells intermingled with ma- lignant cytotrophoblasts (AFIP a m no. 146415).
CANCER July 1963 Vol. 16
cinorna. It metastasizes as a more highly dif. ferentiated form of trophocarcinoma, most commonly as chorioepithel ioma. The tumor in Fig. 7 metastasized as the chorioepithelioma shown in Fig. 5C. Both tumors illustrated in Fig. 4 metastasized as typical chorioepithelio- mas similar to the type illustrated in Fig. 5D.
The microscopic primary tumor consists of
a small, noncircurnscribed island of tumor cells surrounded by considerable reactive con- nective tissue stroma. An analagous entity is the tumor formerly called “carcinoma of aber- rant thyroid tissue,” which is now known to be a microscopic or burned-out primary car- cinoma of the thyroid gland with cervical lymph node metastasis. The reactive fibrosis
No. 7 TROPHOCARCINOMA (EMBRYONAL CARCINOMA) OF TESTIS Friedman 6. Di Rienzo 875
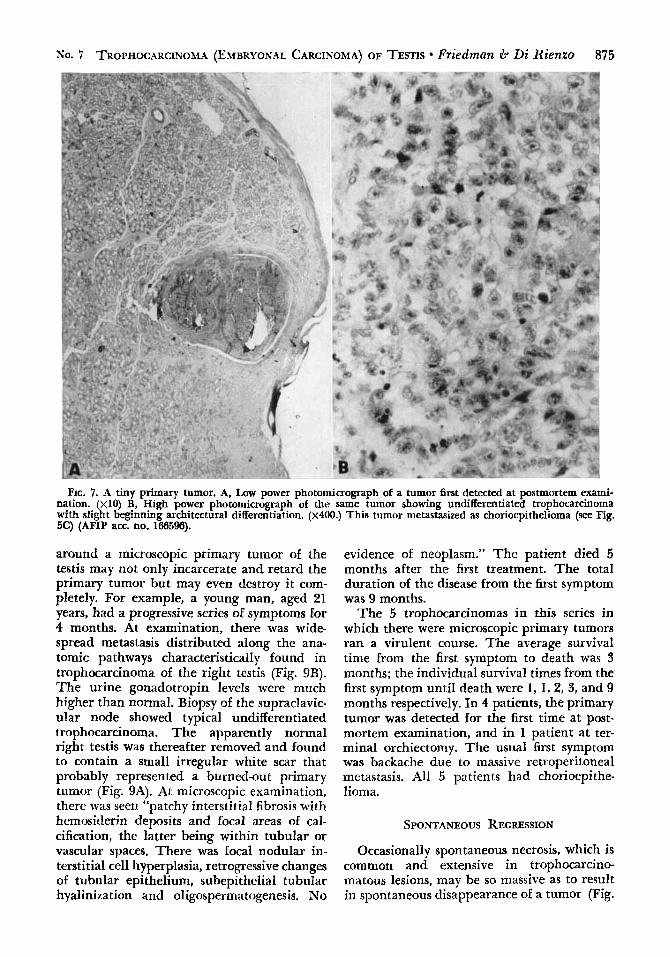
FIG. 7. A tiny primary tumor. A, Low power photomicrograph of a tumor first detected at postmortem exami- nation. ( ~ 1 0 ) B, High power photomicrograph of the same tumor showing undifferentiated trophocarcinoma with slight beginning architectural differentiation. ( ~ 4 0 0 . ) This tumor metastasized as chorioepithelioma (see Fig. 5C) (AFIP am. no. 166596).
around a microscopic primary tumor of the testis may not only incarcerate and retard the primary tumor but may even destroy it com- pletely. For example, a young man, aged 21 years, had a progressive series of symptoms for 4 months. At examination, there was wide- spread metastasis distributed along the ana- tomic pathways CharacteristicalIy found in trophocarcinoma of the right testis (Fig. 9B). The urine gonadotropin IeveIs were much higher than normal. Biopsy of the supraclavic- ular node showed typical undifferentiated trophocarcinoma. The apparently normal right testis was thereafter removed and found to contain a small irregular white scar that probably represented a burned-ou t primary tumor (Fig. 9A). At microscopic examination, there was seen “patchy interstitial fibrosis with hemosiderin deposits and focal areas of cal- cification, the latter being within tubular or vascular spaces. There w a s focal nodular in- terstitial cell hyperplasia, retrogressive changes of tubular epithelium, subepithelial tubular hyalinization and oligospermatogenesis. No
evidence of neoplasm.” The patient died 5 months after the first treatment. The total duration of the disease from the first symptom was 9 months.
The 5 trophocarcinomas in this series in which there were microscopic primary tumors ran a virulent course. The average survival time from the first symptom to death was 3 months; the individual survival times from the first symptom until death were 1, I , 2, 3, and 9 months respectively. I n 4 patients, the primary tumor was detected for the first time at post- mortem examination, and in 1 patient at ter- minal orchiectomy. The usual first symptom was backache due to massive retroperitoneal metastasis. All 5 patients had chorioepithe- lioma.
SPONTANEOUS REGRESSION
Occasionally spontaneous necrosis, which is common and extensive in trophocarcino- matous lesions, may be so massive as to result in spontaneous disappearance of a tumor (Fig.
876 CANCER July 1963 VOl. 16
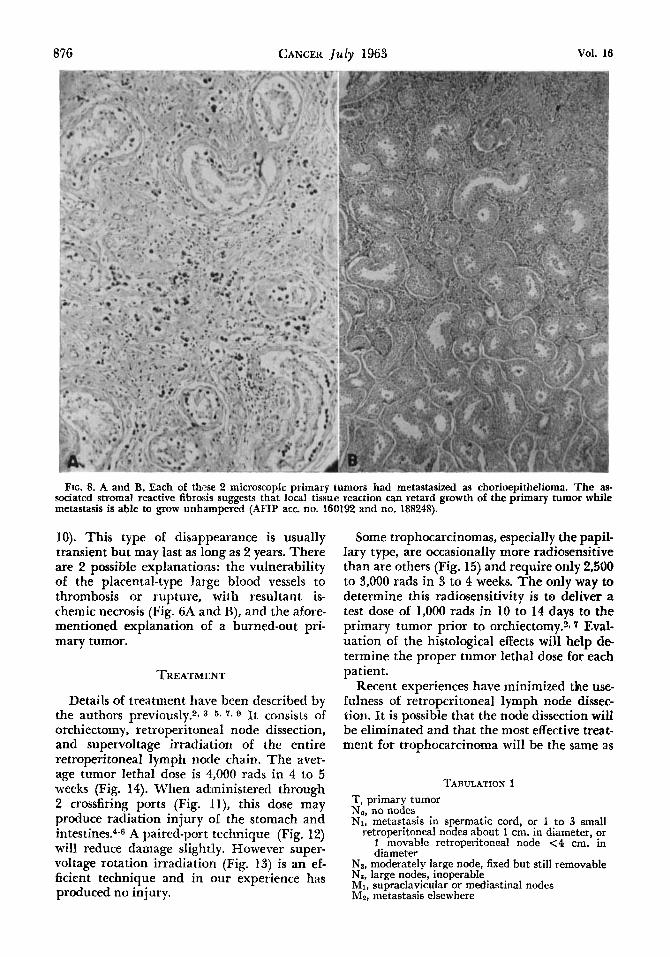
FIG. 8. A and B, Each of these 2 microscopic primary tumors had metastasized as chorioepithelioma. The as- sociated stromal reactive fibrosis suggcsts that local tissue reaction can retard growth of the primary tumor while metastasis is able to grow unhampered (AFIP acc no. 160192 and no. 188248).
10). This type of disappearance is usually transient but may last as long as 2 years. There are 2 possible explanations: the vulnerability of the placental-type large blood vessels to thrombosis or rupture, with resultant is- chemic necrosis (Fig. 6A and B), and the afore- mentioned explanation of a burned-out pri- mary tumor.
TREATMENT
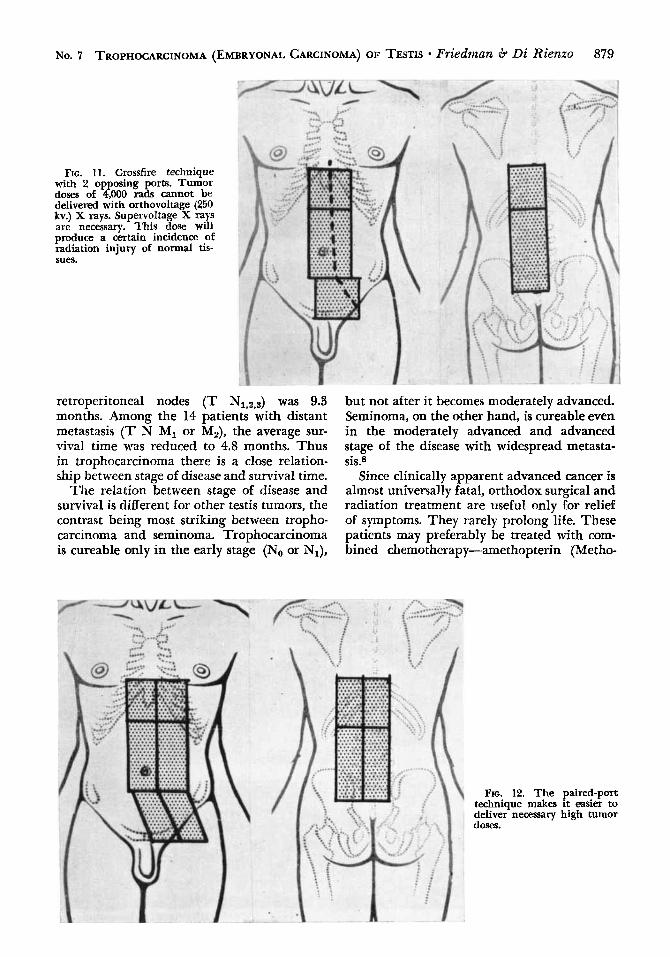
Details of treatment have been described by the authors previously.2* 3 ~ 7 , 9 It consists of orchiectomy, retroperitoneal node dissection, and supervoltage irradiation of the entire retroperitoneal lymph node chain. The aver- age tumor lethal dose is 4,000 rads in 4 to 5 weeks (Fig. 14). When administered through 2 crossfiring ports (Fig. ll), this dose may produce radiation injury of the stomach and
A paired-port technique (Fig. 12) will reduce damage slightly. However super- voltage rotation irradiation (Fig. 13) is an ef- ficient technique and in our experience has produced no injury.
Some trophocarcinomas, especially the papil- lary type, are occasionally more radiosensitive than are others (Fig. 15) and require only 2,500 to 3,000 rads in 3 to 4 weeks. The only way to determine this radiosensitivity is to deliver a test dose of 1,000 rads in 10 to 14 days to the primary tumor prior to orchiectomy.217 Eval- uation of the histological effects will help de- termine the proper tumor lethal dose for each patient.
Recent experiences have minimized the use- fulness of retroperitoneal lymph node dissec- tion. I t is possible that the node dissection will be eliminated and that the most effective treat- ment for trophocarcinoma will be the same as
TABULATION 1 T, primary tumor No, no nodes N1, metastasis in spermatic cord, or 1 to 3 small
retroperitoneal nodes about 1 cm. in diameter, or 1 movable retroperitoneal node <4 cm. in diameter
NZ, moderately large node, fixed but still removable Ns, large nodes, inoperable MI, supraclavicular or mediastinal nodes M:, metastasis elsewhere
No. 7 TROPHOCARCINOMA (EMBRYONAL CARCINOMA) OF TESTIS Friedman 6 Di Rienzo 877 TABLE 1
INCIDENCE OF POSITIVE NODES FOUND
TROPHOCARCINOMA IN 34 T No (CLINICAL) CASES OF
No. cases
No operation 4 Node dissection 30
No nodes found 13 Pos. nodes 17
NI 8 Nz 4 Ns 5 -
TOTAL 34
for seminoma, i.e., orchiectomy followed by supervoltage rotation irradiation of the entire retroperitoneal lymph node chain.
Advanced cancer, with clinically demon- strable metastasis is preferably treated with triple chemotherapy.10111
CLASSIFICATION OF TESTIS TUMORS
Using the principles of the system recom- mended by the International Union Against Cancer, we have arbitrarily constructed and employed the stage classification for testis tu- mors as shown in Tabulation 1.
The primary tumor is not subdivided into categories as there is no relation between its size and prognosis. However, the classification of retroperitoneal nodes has great prognostic significance.
The clinical classification is made prior to node dissection, the surgical classification, after node dissection.
The clinical classification is determined by physical examination, roentgenographic study of the chest, intravenous pyelogram, lymphan- giography, and evaluation of backache when present, Intravenous pyelogram is useless ex- cept to corroborate massive, easily palpable nodes. Lymphangiography 10 will improve the accuracy of diagnosis but had not been de- veloped when the patients in this series were treated. Lumbar backache is an important symptom in testis tumors and should always be carefully investigated and evaluated. Met- astatic tumor in retroperitoneal nodes may break through the capsule and infiltrate the adjacent structures, induding nerve roots. Backache results. Occasionally, myelography may disclose that backache is due to extension of disease through vertebral foramens into the spinal canal (Fig. 16). Response of the back-
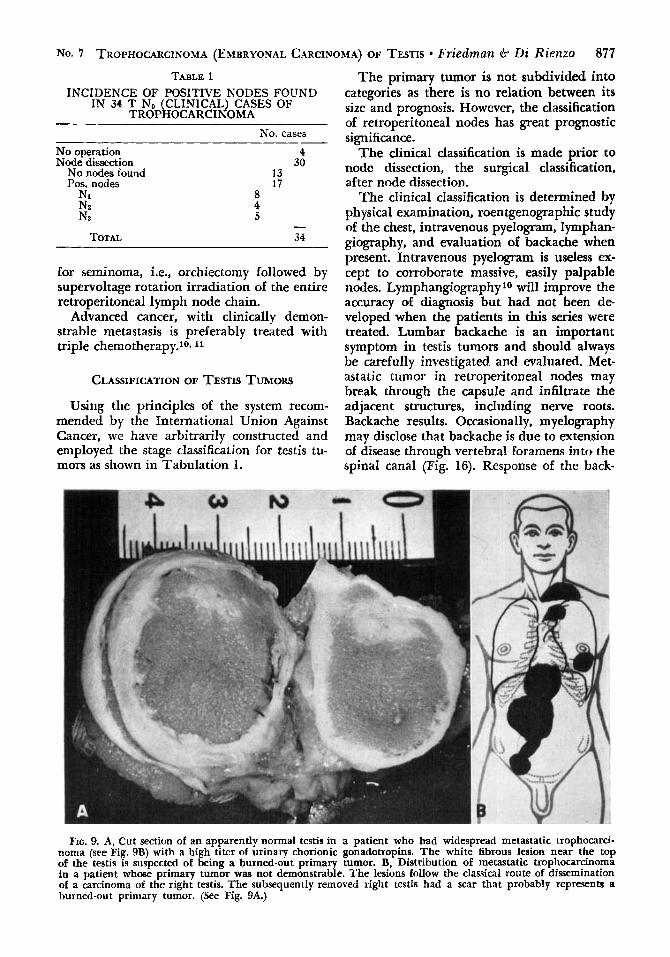
FIG. 9. A, Cut section of an apparently normal testis in a patient who had widespread metastatic trophocarci- noma (see Fig. 9B) with a high titer of urinary chorionic gonadotropins. The white fibrous lesion near the top of the testis is suspected of being a burned-out prima tumor. B, Distribution of metastatic trophocarcinoma in a patient whose primary tumor was not demonstraae. The lesions follow the classical route of dissemination of a carcinoma of the right testis. The subsequently removed right testis had a scar that probably represents a burned-ou t primary tumor. (See Fig. 9A.)
878 CANCER July 1963 Vol. 16
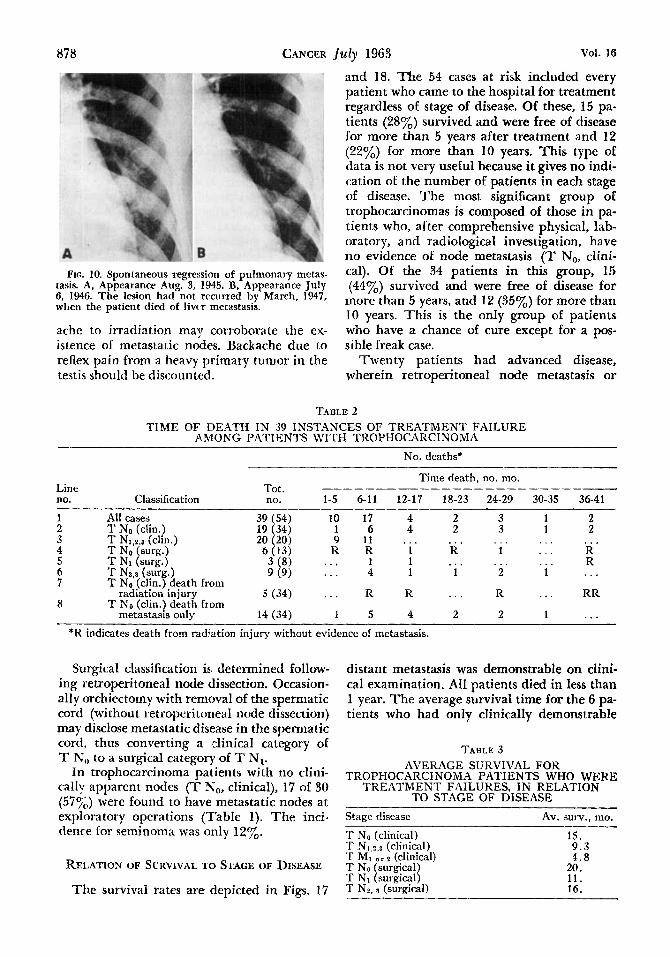
FIG. 10. Spontaneous regression of pulmonary metaa- task A, Appearance Aug. 3, 1945. B, Appearance July G, 1946. The lesion had not recurred by March, 1947, when the patient died of livrr metastasis.
ache to irradiation may corroborate the ex- istence of metastatic nodes. Backache due to reflex pain from a heavy primary tumor in the testis should be discounttd.
and 18. Tbe 54 cases at risk included every patient who came to the hospital for treatment regardless of stage of disease. Of these, 15 pa- tients (28%) survived and were free of disease for more than 5 years after treatment and 12 (22%) for more than 10 years. This type of data is not very useful because it gives no indi- cation of the number of patients in each stage of disease. The most significant group of trophocarcinomas is composed of those in pa- tients who, after comprehensive physical, lab- oratory, and radiological investigation, have no evidence 01 node metastasis (T No, clini- cal). Of the 34 patients in this group, 15 (44%) survived and were free of disease for more than 5 years, and 12 (35%) for more than 10 years. This is the only group of patients who have a chance of cure except for a pos- sible freak case.
'Twenty patients had advanced disease, wherein retroperitoneal node metastasis or
TABLE 2 TIME OF DEATH IN 39 INSTANCES OF TREATMENT FAILURE
AMONG PATIENTS \?IITH TROPHOCARCINOMA No. deaths*
Time death, no. mo. - -__--____ Line Tot.
no. Classification no. 1-5 6-11 12-17 18-23 24-29 30-35 36-41
1 2 3 4 5 6 7
8
All cases T No (clin.) T N1.2.8 (din.) T No (surg.) T N1 (surg.) T N2.3 (surg.1 T N, (clin.1 death from
radiation' injury
metastasis only T No (clin.) death from
39 (54) 19 (34) 20 (20)
5 (34)
14 (34)
10 17 4 1 6 4 9 11 . . .
I< R 1 ... 1 1 . . . 4 1
... R R
1 5 4
2 2
R . . . . . 1
. . . 2
3 1 3 1
1 . . .
2 1
. . . . . .
. . . . . .
R . . 2 1
2 2
R ' R
RR
... *I< indicates death from radiation injury without evidence of metastasis.
Surgical classification is determined follow- ing retroperitoneal node dissection. Occasion- ally orchiectomy with removal of the spermatic cord (without retroperitorieal node dissection) may disclose metastatic disease in the spermatic cord, thus converting a clinical category of T No to a surgical category of T N1.
In trophocarcinoma patients with no clini- cally apparent nodes (T No, clinical), 17 of 30 (5'i';.J were found LO have metastatic nodes at exploratory operations (Table 1). The inci- tlenre for seminoma was only 12%.
RELATION OF SURVIVAL TO STAGE OF DISEASE
The survival rates are depicted in Figs. 17
distant metastasis was demonstrable on clini- cal examination. All patients died in less than 1 year. The average survival time for the 6 pa- tients who had only clinically demonstrable
TABLE 3 AVERAGE SURVIVAL FOR
TROPHOCARCINOMA PATIENTS WHO WERE TREATMENT FAILURES. IN RELATION
TO STAGE OF DISEASE
Av. surv.. mo. Stage disease
T No (clinical) T N,,z,~ (clinical) T MI o r 2 (clinical) T NO (surgical) T N1 (surgical) T Ns. 3 (surgical)
~
15. 9 . 3 4 . 8
20. 11. 16.
No. 7 TROPHOCARCINOMA (EMBRYONAL CARCINOMA) OF TESTIS Friedman 6. Di Rienro 879
FIG. 11. Crossfire technique with 2 opposing ports. Tumor doses of 4,000 r a d s cannot be delivered with orthovoltage (250 kv.) X rays. Supervoltage X rays are necessary. This dose will produce a certain incidence of radiation injury of normal tis- sues.
retroperitoneal nodes (T N1,2,3) was 9.3 months. Among the 14 patients with distant metastasis (T N MI or M2)J the average sur- vival time was reduced to 4.8 months. Thus in trophocarcinoma there is a close relation- ship between stage of disease and survival time.
The relation between stage of disease and survival is different for other testis tumors, the contrast being most striking between tropho- carcinoma and seminoma. Trophocarcinoma is cureable only in the early stage (No or Nl)J
but not after it becomes moderately advanced. Seminoma, on the other hand, is cureable even in the moderately advanced and advanced stage of the disease with widespread metasta- sis.8
Since clinically apparent advanced cancer is almost universally fatal, orthodox surgical and radiation treatment are useful only for relief of symptoms. They rarely prolong life. These patients may preferably be treated with com- bined chemotherapy-amethopterin (Metho-
FIG. 12. The paired-port technique makes it easier to deliver necessary high tumor dom.
880 CANCER J u l y 1963 Vol. 16
trexate), chlorambucil, and actinomycin D. Whitmore111 12 has reported many survivals longer than those generally achieved with ir- radiation, including 3 patients who have sur- vived more than 3 years.
The surgical classification is based on the findings during retroperitoneal lymph node dissection, when the relation between stage of disease and prognosis is demonstrated more clearly. When the removed nodes had no metastasis (T No, surgical), the 5-year survival rate was 54%. When the removed nodes had metastasis in 1 or 2 small nodes (T N1, surgi- cal), the 5-year survival rate was 62%. This paradox can be explained either on the basis of statistical error due to the small sample, or to the fact that in the aforementioned group of 13 (T No, surgical) patients, 3 of the 6 deaths were caused by radiation injury with na evi- dence of metastasis at postmortem examina- tion (Table 2). They died 6, 15, and 36 months after orchiectomy. Assuming that there had been no radiation-induced deaths, 10 of 13 patients (7701,) might have survived. Thus the graded survival rates would be more consistent.
When the nodes were found at operation to large or fixed (T N2 or Na, su@al), no
patients survived. nus when the nodes are
operation, death seems inevitable with con-
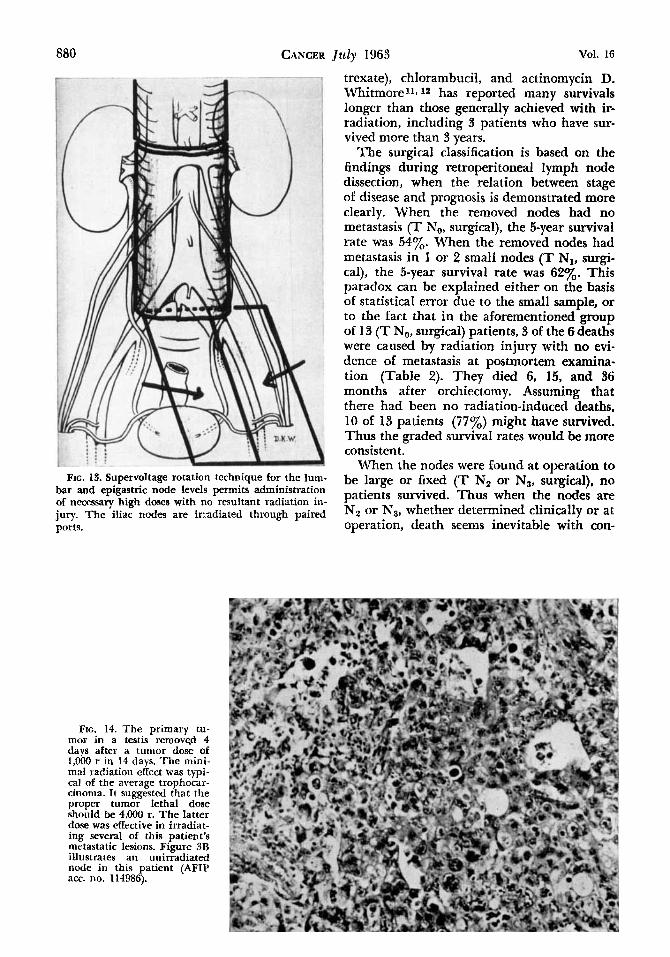
FIG. 13. Supervoltage rotation technique for the lum- bar and epigastric node levels permits administration of necessary high doses with no resultant radiation in-
ports. juqr. m e iliac nodm a x irradiated through paired NZ Or N3, whether determined clinically O r at
FIG. 14. The primary tu- mor in a testis removed 4 days after a tumor dose of 1,OOO r in I4 days. The mini- mal radiation effect was typi- cal of the average trophocar- cinorna. It suggested that the proper tumor lethal dose should be 4,000 r. The latter dose was effective in irradiat- ing several of this patient’s nietastatic lesions. Figure 3D illustrates an unirradiated node in this patient (AFIP acc. no. 114986).
No. 7 TROPHOCARCINOMA (EMBRYONAL CARCINOMA) OF TESTIS Friedman 6. Di Rienzo 881
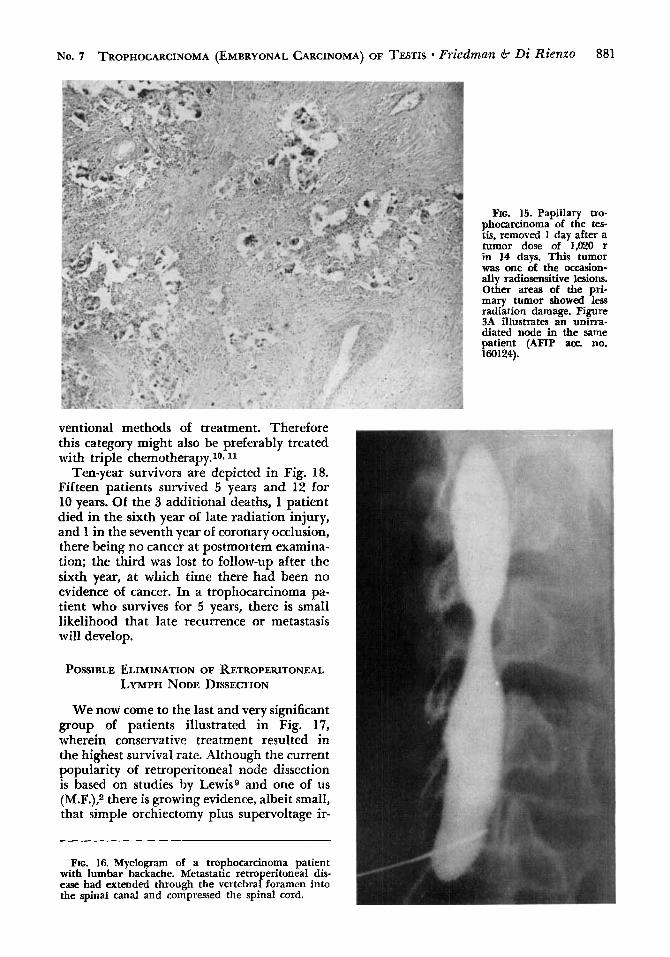
FIG. 15. Papillary tro- phocarcinoma of the tes- tis, removed 1 day after a tumor dose of 1,020 r in 14 days. This tumor was one of the occasion- ally radiosensitive lesions. Other areas of the pri- mary tumor showed less radiation damage. Figure 3A illustrates an unirra- diated node in the same patient (AFIP ace. no. 160124).
ventional methods of treatment. Therefore this category might also be preferably treated with triple chemotherapy.10111
Ten-year survivors are depicted in Fig. 18. Fifteen patients survived 5 years and 12 for 10 years. Of the 3 additional deaths, 1 patient died in the sixth year of late radiation injury, and 1 in the seventh year of coronary occlusion, there being no cancer at postmortem examina- tion; the third was lost to follow-up after the sixth year, at which time there had been no evidence of cancer. In a trophocarcinoma pa- tient who survives for 5 years, there is small likelihood that late recurrence or metastasis will develop.
POSSIBLE ELIMINATION OF RETROPERITONEAL LYMPH NODE DISSECTION
We now come to the last and very significant group of patients illustrated in Fig. 17, wherein conservative treatment resulted in the highest survival rate. Although the current popularity of retroperitoneal node dissection is based on studies by Lewis0 and one of us (M.F.),2 there is growing evidence, albeit small, that simple orchiectomy plus supervoltage ir-
FIG. 16. Myelogram of a trophocarcinoma patient with lumbar backache. Metastatic retroperitoneal dis- ease had extended through the vertebral foramen into the spinal canal and compressed the spinal cord.
$82 CANCER July 1963 Vol. 16
A l l C a s e s 15/54 (28%) II
add 3 &at-war cases.
617 (86%)
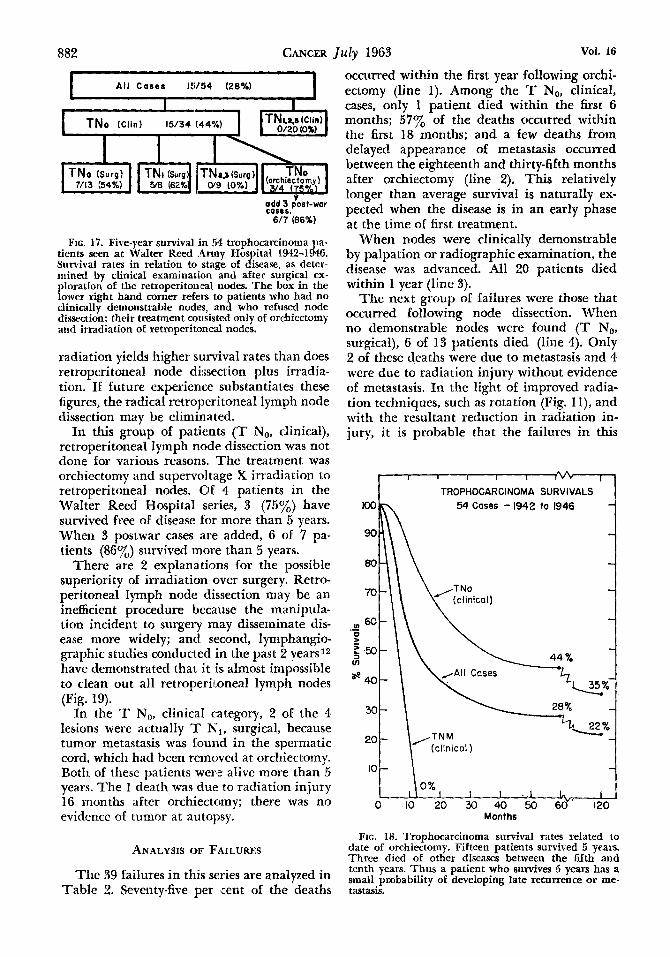
FIG. 17. Five-year survival in 54 trophocarcitionia tients seen at Walter Keed .Army Hospital 1942-1&: Survival rates in relation to stage of disease, as detcr- mined by clinical examination and after surgical ex- ploration of the remoperiton84 nodes. The box in the lower right hand corner refers to patients who had no clinically demonstrable nodes, and who refused node dissection: their treatment consisted only of orchicctomy and irradiation of retroperitoneal nodes.
radiation yields higher survival rates than does retroperitaneal node dissection plus irradia- tion. If iuture experience substantiates these figures, the radical retroperitoneal lymph node dissection may be eliminated.
I n this group of patients (T No, clinical), retroperitoneal lymph node dissection was not done for various reasons. The treatment was orchiectomy and supervol tage X irradiation to retroperitoneal nodes. Of 4 patients in the Walter Reed Hospital series, 3 (7501,) have survived free of disease for more than 5 years. When 3 postwar cases are added, 6 of 7 pa- tients (86y0) survived more than 5 years.
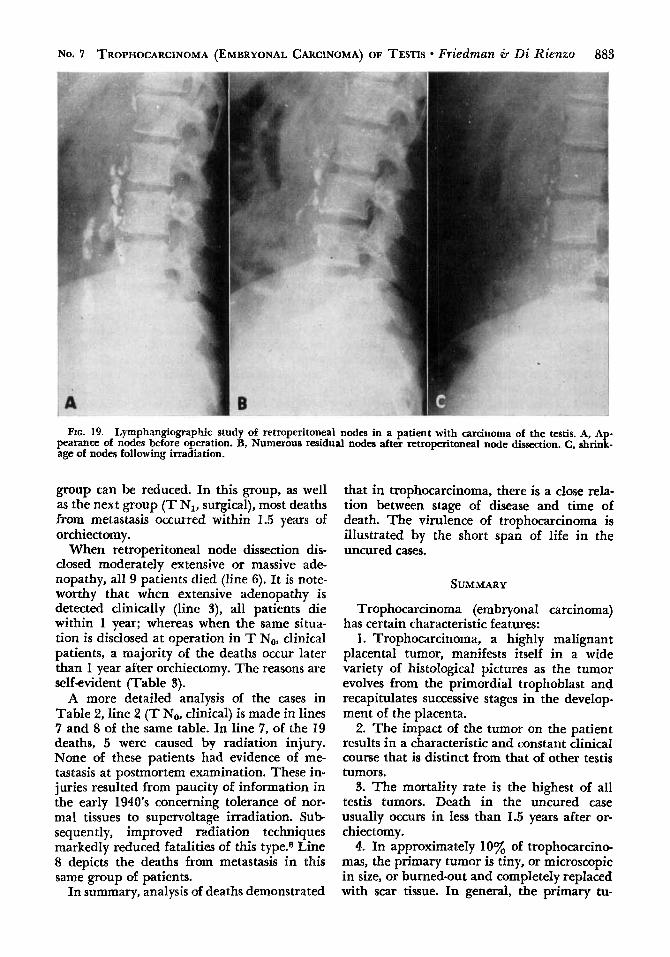
There are 2 explanations for the possible superiority of irradiation over surgery. Retro- peritoneal lymph node dissection may be an inefficient procedure because the manipula- tion incident ta surgery may disseminate dis- ease more widely; and second, lymphangio- graphic studies conducted in the past 2 years12 have demonstrated that it is almost impossible to clean out all retroperitoneal lymph nodes (Fig. 19).
In the ’I’ No, clinical category, 2 of the 4 lesions were actually T N,, surgical, because tumor metastasis was found in the spermatic cord, which had been remclved at orchiectomy. Both of these patients were alive more than 5 years. The 1 death was due to radiation injury 1 G months aEter orchiectomy; there was no evidence of tumor at autopsy.
ANALYSIS OF FAILURES
The 39 failures in this series are analyzed in TabIe 2. Seventy-five per cent of the deaths
occurred within the first year following orchi- ectomy (line 1). Among the T No, clinical, cases, only 1 patient died within the first 6 months; 577, of the deaths occurred within the first 18 months; and a few deaths from delayed appearance of metastasis occurred between the eighteenth and thirty-fifth months after orchiectomy (line 2). This relatively longer than average survival is naturally ex- pected when the disease is in an early phase at the time of first treatment.
‘When nodes were clinically demonstrable by palpation or radiographic examination, the disease was advanced. All 20 patients died within 1 year (line 3).
The next group o€ failures were those that occurred following node dissection. When no demonstrable nodes were found (T No, surgical), 6 of 13 patients died (line 4). Only 2 of these deaths were due to metastasis and 4 were due to radiation injury without evidence of metastasis. In the light of improved radia- tion techniques, such as rotation (Fig. l l), and with the resultant reduction in radiation in- jury, it is probable that the failures in this
I. 1 I I I I V V * A
I I TROPHOCARCINOMA SURVIVALS 54 Cases - 1942 to 1946
I 0%
I I . I L. I 0 10 20 30 40 50 So*‘ I20
Months
FIG. 18. ‘I‘rophocarcinoma survival rates related to date of orchiectomy. Fifteen patients survived 5 years. Thrce died of other diseases between the fifth and tcnth years. Thus a patient who survives 5 years has a small probability of developing late recnrrence or me- tastasis.
No. 7 TROPHOCARCINOMA (EMBRYONAL CARCINOMA) OF TESTIS Friedman 6. Di Rienzo 883
FIG. 19. Lymphangiographic study of retroperitoneal nodes in a patient with carcinoma of the testis. A, Ap- pearance of nodes before operation. B, Numerous residual nodes after retroperitoneal node dissection. C, shrink- age of nodes following irradiation.
group can be reduced. In this group, as well as the next group (T N1, surgical), most deaths from metastasis occurred within 1.5 years of orchiectomy.
When retroperitoneal node dissection dis- closed moderately extensive or massive ade- nopathy, all 9 patients died (line 6). It is note- worthy that when extensive adenopathy is detected clinically (line S), all patients die within 1 year; whereas when the same situa- tion is disclosed at operation in T No, clinical patients, a majority of the deaths occur later than 1 year after orchiectomy. The reasons are self-evident (Table 3).
A more detailed analysis of the cases in Table 2, line 2 (T No, clinical) is made in lines 7 and 8 of the same table. In line 7, of the 19 deaths, 5 were caused by radiation injury. None of these patients had evidence of me- tastasis at postmortem examination. These in- juries resulted from paucity of information in the early 1940’s concerning tolerance of nor- mal tissues to supervoltage irradiation. Sub sequently, improved radiation techniques markedly reduced fatalities of this type.8 Line 8 depicts the deaths from metastasis in this same group of patients.
In summary, analysis of deaths demonstrated
that in trophocarcinoma, there is a close rela- tion between stage of disease and time of death. The virulence of trophocarcinoma is illustrated by the short span of life in the uncured cases.
SUMMARY
Trophocarcinoma (embryonal carcinoma) has certain characteristic features:
1. Trophocarcinoma, a highly malignant placental tumor, manifests itself in a wide variety of histdogical pictures as the tumor evolves from the primordial trophoblast and recapitulates successive stages in the develop- ment of the placenta. 2. The impact of the tumor on the patient
results in a characteristic and constant clinical course that is distinct from that of other testis tumors.
3. The mortality rate is the highest of all testis tumors. Death in the uncured case usually occurs in less than 1.5 years after or- chiectomy.
4. In approximately 10% of trophocarcino- mas, the primary tumor is tiny, or microscopic in size, or burned-out and completely replaced with scar tissue. In general, the primary tu-
884 CANCER
mor is smaller in size th.an other types of testis tumors.
5. Focal or massive necrosis occurs fre- quently due to the propensity of trophoblasts to destroy or thrombose the blood vessels and blood spaces that these trophoblasts had orig- inally helped to construct.
6. Occasionally spontaneous necrosis may be so massive as to cause spontaneous regres- sion of a primary tumor or spontaneous re- gression of pulmonary metastasis. In our ex- perience, this has never resulted in a cure, as death occurs from metakstasis elsewhere.
7. The tumor commonly produces excessive amounts of pituitary and chorionic gonado- tropins and 17-ketosteroids.
8. The clinical behav:ior of the various his- tological types tends to be constant. The inci- dence of node metastasis in T No, clinical, cases is 57% for trophocarcinoma as compared with 12% for seminoma. In the uncured case, metastasis proceeds quickly from the retroperi- toneal nodes through he blood stream to lungs and liver, causing early death. Tropho- carcinoma often skips the mediastinal or Virchow’s node, whereas seminoma rarely misses them. Sometimes trophocarcinoma metastasizes from the testis directly into the general circulation. The pure chorioepithe- liomas (Fig. 5C and D) tend to be more viru- lent than average; the same is only slightly less true for the most undifferentiated type of trophocarcinoma (Fig. 213).
9. There is little relation between histologi- cal type and prognosis, except for occasional atypical instances.
10. There is a direct and close relation be- tween stage of disease and prognosis.
J u l y 1963 Vol. 16
11. The tumor lethal radiation dose for typical trophocarcinoma is approximately 4,000 rads in 4 to 5 weeks. This dose range may injure the stomach or intestines unless supervoltage rotation techniques are employed. A small percentage of trophocarcinomas may be arrested with smaller doses.
CONCLUSIONS
1. Trophocarcinoma of the testis, the SG-
called embryonal carcinoma, is a malignant placental tumor derived from the primordial trophoblast. I t is the most highly malignant germ cell tumor of the testis. Unless cured, it runs a rapid course.
2. There is a direct relation between stage of disease and prognosis, but almost none be- tween histological type and prognosis. Pa- tients in this series with clinically detectable retroperitoneal node metastasis were not cured.
3. Current treatment entails orchiectomy, retroperitoneal node dissection, and postopera- tive irradiation, preferably with supervoltage rotation techniques. However, there is grow- ing evidence that omission of the retroperi- toneal node dissection and employment of orchiectomy and irradiation yields higher survival rates. 4. In a series of 54 consecutive cases of
pure trophocarcinoma treated at Walter Reed Army Hospital, Washington, D. C., from 1942 to 1946, the 5- and 10-year survival rates were 28% and 22% respectively. Among 34 patients who had no clinical or radiographic evidence of metastasis prior to surgery, the 5- and 10- year survival rates were 44% and 35% re- spectively.
REFERENCES 1. FRIEDMAN, M.: Supervoltage ( l , ~ , O O O volt) roent-
gen therapy at Walter Reed General Hospital. S. Clin. North America 24: 1424-1432, 1944.
2. FRIEDMAN, M.: Tumors of testis and their treat- ment. In PORTMANN, U. V., Etl.: Clinical Therapeutic Radiology. New York, N.Y. Thomas Nelson & Sons.
3. FRIEDMAN, M.: Tumors of testis; relation of his- togenic classification to radiosensitivity and prognosis. Proc. New Yofk Path. SOC. [1950-1951]: 33-41, 19.50.
4. FRIEDMAN, M.: Calculated .risks of radiation injury of normal tissue in treatment of cancer of testis. In Proceedings of the Second National Cancer Conference. New York, N.Y. American Ca:ncer Society, Inc. 1952;
5. FRIEDMAN, M.: Superior value of supervoltage irra- diation in special situations; carcinoma of mouth and carcinoma of testis. Radiology 67: 484-497, 1956.
6. FRIEDMAN, M.: Normal tisue tolerance. In FRIED- MAN, M.; BRUCER, M., and ANDERSON, E., Eds.: Roent- gens, Rads and Riddles. Washington, D.C. US. Govern-
1950; pp. 276-308.
pp. 390-400.
ment Printing Office. 1959; pp. 217-238. 7. FRIEDMAN, M.: Radiation treatment of tumors of
testis. In PACK, G. T., and ARIEL, I. M., Eds.: Treatment of Cancer and Allied Diseases, 2d ed.. vol. 8. New York, N.Y. Harper & Row, Publishers. 1962; pp. 32-50.
8. FRIEDMAN, M., and PURKAYASTHA, M. C.: Recur- rent seminoma; management of late metastasis, recur- rence, or second primary tumor. Am. J. Roentgenol.
9. LEWIS, L. G.: Testis tumors; report on 250 cases. 83: 25-42, 1960.
J . Urol. 59: 763-772, 1948. 10. WALLACE, S.; JACKSON, L.; SCHAFFER, B.; COULD,
T.; GREENING, R. R.: WEISS. A.. and KRAMER. S.: Lvmoh- bgiograms; their diagnostic and therapeutic poieniial. Radiology 76: 179-1W, 1 9 6 1 .
11. WHITMORX, W. F., JR.: Treatment of testis neo- plasms. In Proceedings of the Fourth National Cancer Conference. Philadelphia, Pa. J. B. Lippincott Com- pany. 1961; pp. 503-518.
12. WHITMORE, W. F., JR.: Personal communication.