Embed Size (px)
Citation preview

TrombosisyCáncer:AspectosPrácticos
AndrésJ.Muñoz MartínMDPhDServicio deOncología Médica
Hospital GeneralUniversitario GregorioMarañónUniversidad Complutense,MadridSección Cáncer yTrombosis SEOM
Zaragoza,27junio 2018

My disclosures
• Consultantoradvisoryrole:Sanofi,LeoPharma,Pfizer-BMS, DaiichiSankyo
• Researchfunding:Sanofi,LeoPharma• Speakers’Bureau:Rovi,DaiichiSankyo

Guión
• Nuevosfactoresderiesgo• Nuevosmodelospredictivos– profilaxisenelpacientemédicoambulatorio
• TratamientodelaETV

NewVTErisk factors based on tumorgenomics
ORIGINAL ARTICLE
Tumor oncogene (KRAS) status and risk of venous thrombosisin patients with metastatic colorectal cancerS . ADES ,* S . KUMAR,* M. ALAM,† A. GOODWIN ,‡ D. WECKSTE IN ,§ M. DUGAN, ¶ T . ASH IKAGA,**M. EVANS ,† C. VERSCHRAEGEN* and C . E . HOLMES**Department of Medicine, Vermont Cancer Center, University of Vermont, Burlington, VT; †The James, Ohio State University Wexner
Medical Center, Columbus, OH; ‡Department of Pathology and Laboratory Medicine, University of Vermont, Burlington, VT; §New
Hampshire Oncology-Hematology PA, Hookset, NH; ¶New England Cancer Specialists, Scarborough, ME; and **Department of Math and
Statistics, University of Vermont, Burlington, VT, USA
To cite this article: Ades S, Kumar S, Alam M, Goodwin A, Weckstein D, Dugan M, Ashikaga T, Evans M, Verschraegen C, Holmes CE. Tumor
oncogene (KRAS) status and risk of venous thrombosis in patients with metastatic colorectal cancer. J Thromb Haemost 2015; DOI: 10.1111/
jth.12910.
Summary. Background: Patients with metastatic coloncancer (mCRC) are at increased risk of venous thrombo-embolism (VTE). Limited preclinical data suggest that theoncogene (KRAS) mutational status of the tumor repre-sents a plausible clinical link to systemic hypercoagulabili-ty in cancer patients. Objectives: To determine if a tumorgenetic characteristic, KRAS mutational status, is associ-ated with an increased risk of VTE in patients withmCRC. Patients/methods: A retrospective cohort study ofpatients with mCRC and KRAS test results was con-ducted at multiple practice sites across New England inthe United States. The primary outcome was a VTEevent, defined as deep venous thrombosis (DVT) and/orpulmonary embolism (PE), either 6 months before or atany time after the diagnosis of mCRC. KRAS status(mutated vs. wild type) and other relevant predictors ofthrombosis were collected. Results: Of 172 histologicallyconfirmed patients with mCRC, 40 developed a VTE(23.3%). Sixty-five patients (37.8%) had a mutant KRASstatus. The incidence of VTE and DVT among patientswith mutated KRAS was 32.3 and 23.1%, respectively.The corresponding incidence among patients with wild-type KRAS was 17.8 and 9.4%. Odd ratios for the associ-ation were 2.21 (95% CI, 1.08–4.53) for VTE and 2.62(95% CI, 1.12–6.12) for DVT, and remained significantdespite adjustment for Khorana score and bevacizumab
use. Conclusion: Tumor mutant KRAS status is associatedwith an increased risk of VTE in patients with mCRC.The tumor genetic profile may represent a novel andimportant risk factor for thrombosis in patients withcancer.
Keywords: cancer; colon cancer; pulmonary embolism;thromboembolism; venous thrombosis.
Introduction
Venous thromboembolism (VTE) is associated withincreased morbidity and mortality in cancer patients,especially in those with metastatic disease [1,2]. VTE con-fers a poor prognosis, which is associated with a combi-nation of fatal embolic complications and biologicallymore aggressive cancer [3,4]. Among the four most com-mon cancers, colorectal cancer (CRC) has the secondhighest incidence of VTE, with rates ranging from 16 to66 events/1000 person years [5]. The care of patients withmetastatic colorectal cancer (mCRC) is further compli-cated by the use of anti-angiogenic therapy, which isknown to increase the risk of bleeding and in some, butnot all, studies has been associated with an increase inthrombotic events [6,7]. As for all cancer patients treatedin the ambulatory setting, current guidelines do not rec-ommend routine pharmacologic VTE prophylaxis inpatients with CRC based on a small absolute decrease inVTE risk with thromboprophylaxis and the potential forincreased bleeding complications [3,8,9].
In an effort to improve VTE risk stratification and bet-ter tailor thromboprophylaxis, recent risk-scoring modelshave been developed to identify ambulatory cancerpatients receiving chemotherapy who are at high risk ofVTE. The Khorana model uses five readily available vari-ables, including site of cancer, pre-chemotherapy platelet
Correspondence: Chris E. Holmes, Department of Medicine, Hema-
tology and Oncology Division, 111 Colchester Avenue, Given Build-
ing Second Floor, University of Vermont, Burlington, VT 05401,
USA.
Tel.: +1 802 656 5487; fax: +1 802 847 4398.
E-mail: [email protected]
Received 7 October 2014
Manuscript handled by: J. Douketis
Final decision: F. R. Rosendaal, 11 March 2015
© 2015 International Society on Thrombosis and Haemostasis
Journal of Thrombosis and Haemostasis, 13: 1–6 DOI: 10.1111/jth.12910
sue or clinical data, respectively. Sixty-five specimens(37.8%) had a KRAS activating mutation and 107 werefound to be KRAS wild-type. Chemotherapy records wereavailable for 161 patients and 101 were treated with abevacizumab-containing chemotherapy regimen. The req-uisite data were available to calculate the Khorana scorefor 151 patients. Forty patients had at least one VTEevent (26 with DVT, 18 with PE) and four patients hadboth DVT and PE diagnosed after or within 6 monthsprior to the diagnosis of mCRC. Only one patient in ourstudy was diagnosed with VTE prior to the diagnosis ofmetastatic disease.
KRASmutation in mCRC specimens was equally distrib-uted amongst male and female patients and other demo-graphic variables (Table 1). Bevacizumab was administeredto 60.6% (n = 37) of patients with mutated KRAS and64.0% (n = 64) with WT KRAS. The majority of patients inthe overall 172-patient cohort (61.6%) were originally diag-nosed with metastatic disease. The majority of the 151-patient subset had a low Khorana score of 0 or 1 and only10.6% of patients had scores of 2 or above. Follow-up forall patients was similar: wild-type KRAS, 75th quan-tile = 15 months, 50th = 28 months and 25th = 47 months;mutant KRAS, 75th quantile = 15 months, 50th = 27months and 25th = 48 months.
KRAS status and VTE risk
KRAS mutated status was associated with an elevatedrisk of thrombosis, with an odds ratio (OR) of 2.21 for
the composite outcome of VTE and 2.62 for DVT(Table 2). No association was found between KRAS sta-tus and a diagnosis of PE. Table 3 shows the results oflogistic regression modeling with adjustment for knownpredictors of VTE. We found the association betweenKRAS mutated status and both DVT alone and compos-ite VTE remained significant despite adjustment for theKhorana score and bevacizumab use.
The association between Khorana score and DVT didnot reach significance (Cochran’s linear trend P = 0.072),in part due to the low number of patients with elevatedbaseline scores. The risk of DVT in patients with a scoreof 0, 1 or ≥ 2 was 13.0, 18.6 and 31.3%, respectively. Alogistic regression model with Khorana, KRAS and theirstatistical interaction increased the value of the adjustedKRAS odds ratio to 6.23 (95% CI, 1.56–24.96). In thesubset of patients (n = 92) with a score of 0, the risk ofDVT was 5.3% and 25.7% in patients with WT andmutant KRAS status, respectively (OR, 6.23; 95% CI,1.55–24.95). Corresponding risks for patients with a scoreof 1 were 18.5% and 18.8% (n = 43, NS) and for scoresof 2 or greater were 28.6% and 33.3% (n = 16, NS),respectively. Similar patterns were observed for the riskof VTE, with an increase in risk of events for the ‘Khor-ana score 0’ subset alone (12.3 vs. 34.3%; OR, 3.73; 95%CI, 1.30–10.70).
Table 4 lists the frequencies of all observed KRASmutation types in this population, and corresponding fre-quencies of VTE. There was no observed associationbetween mutation type and risk of VTE. Survival analysisindicated that better ECOG performance status at diag-
Table 1 Patient characteristics
All patients(n = 172) (%)
Patients withmutatedKRAS(n = 65) (%)
Patientswith WT*KRAS(n = 107) (%)
Age (! SD) 60 (! 12.4) 62 (! 11.4) 60 (! 13.0)Female 70 (40.1) 28 (43.1) 42 (39.2)History ofsmoking
80 (46.5) 33 (50.8) 47 (43.9)
Race: Caucasian 165 (95.9) 62 (95.3) 103 (96.2)ECOG† (n = 162)0–1 143 (88.3) 52 (86.7) 91 (89.2)≥ 2 19 (11.7) 8 (13.3) 11 (10.8)
Patientstreated withbevacizumab-containingregimen (n = 161)
101 (62.7) 37 (60.6) 64 (64.0)
Initial presentationas metastaticdisease
106 (61.6) 40 (61.5) 66 (61.7)
Khorana score 0.50 (n = 151) 0.58 (n = 60) 0.45 (n = 91)0 92 (60.9) 35 (58.3) 57 (62.6)1 43 (28.5) 16 (26.7) 27 (29.7)≥ 2 16 (10.6) 9 (15.0) 7 (7.7)
*Wild-type, †Eastern Cooperative Oncology Group performancestatus.
Table 2 Incidence of DVT and VTE among patients with mutatedand WT KRAS
All patients(n = 172)(%)
Patients withmutatedKRAS(n = 65) (%)
Patients withWT* KRAS(n = 107)(%)
Odds ratio†(95% CI)
DVT‡ 26 (15.1) 15 (23.1) 11 (9.4) 2.62 (1.12–6.12)PE§ 18 (10.5) 8 (12.3) 10 (9.3) 1.36 (0.51–3.65)VTE¶ 40 (23.3) 21 (32.3) 19 (17.8) 2.21 (1.08–4.53)
*Wild-type. †Logistic regression analysis. ‡Deep venous thrombosis.§Pulmonary embolism. ¶Venous thromboembolism.
Table 3 Association of KRAS status with DVT and VTE
Odds ratio* (95% CI)
CrudeAdjusted forKhorana score
Adjusted forbevacizumab use
DVT† 2.62 (1.12–6.12) 2.66 (1.10–6.45) 2.62 (1.11–6.19)VTE‡ 2.21 (1.08–4.53) 2.15 (1.01–4.58) 2.38 (1.14–4.96)
*Logistic regression analysis. †Deep venous thrombosis. ‡Venousthromboembolism.
© 2015 International Society on Thrombosis and Haemostasis
KRAS status is associated with VTE risk in mCRC 3
The tumorgenetic profile may represent anovelandimportant risk factorfor thrombosis inpatients with cancer(k-rasmutation andcolorectal cancer)
Adesetal.JThromb Haemost.2015;13(6):998-1003 4

NSCLCALK+andVTE
• Zugazagoitia,Muñoz&Manzano etal.EuropeanRespiratoryJournal2018– 241ALK-rearrangedNSCLCpatients– 73patients(30%)developedthromboembolicdisease– 74%inthe first 6months from cancer diagnosis– 16%recurrent VTE– Liver mets:significant risk factor– mOS VTE+20months vsVTE- 36months (p=0.036)– mOS atbaseline 15m– mOS recurrent VTE10m
5
Early View
Research letter
Incidence, predictors and prognostic significance of thromboembolic disease in patients with advanced ALK-rearranged non-small-cell lung cancer
Jon Zugazagoitia, Mercedes Biosca, Julio Olivera, María Eugenia Olmedo, Manuel Dómine, Ernest Nadal, José Carlos Ruffinelli, Nerea Muñoz, Ana María Luna, Berta Hernández, Maite Martínez, Iria Gallego, Eva Martínez de Castro, Carme Font, Virginia Calvo, Virginia Martínez-Marín, Jesús Corral, Esther Noguerón, Rebeca Mondéjar, Ignacio García Escobar, Carmen Salvador-Coloma, Óscar Juan, Manuel Sánchez Cánovas, Javier Valdivia, M. Pilar Ochoa, Rafael López Castro, Berta Obispo, Cristina Pangua, María Sereno, Lourdes Fernández Franco, Xabier Mielgo, Julia Calzas, Ana Blasco, Francisco Aparisi, Luis Chara, Juan Francisco Grau, Marta Soares, Ana Gómez, Victor Zenzola, Marcial García-Morillo, Diego Cacho, Asunción Díaz-Serrano, Carlos Aguado, Santiago Ponce-Aix, Jose Luis González-Larriba, Andrés J. Muñoz, David Lora, Luis Paz-Ares, Aránzazu Manzano
Please cite this article as: Zugazagoitia J, Biosca M, Olivera J, et al. Incidence, predictors and prognostic significance of thromboembolic disease in patients with advanced ALK-rearranged non-small-cell lung cancer. Eur Respir J 2018; in press (https://doi.org/10.1183/13993003.02431-2017).
This manuscript has recently been accepted for publication in the European Respiratory Journal. It is published here in its accepted form prior to copyediting and typesetting by our production team. After these production processes are complete and the authors have approved the resulting proofs, the article will move to the latest issue of the ERJ online.
Copyright ©ERS 2018
. Published on March 21, 2018 as doi: 10.1183/13993003.02431-2017ERJ Express
Copyright 2018 by the European Respiratory Society.

DIFFERENTIALGENEEXPRESSIONINLUNGCANCERPATIENTSWITHANDWITHOUTVTE
66
Genesunder-expressed inpatients with VTE
Genesover-expressed inpatients with VTE
Normalized counts
log2fo
ldchange
Sussman etal,ASH2017

BackupslidesDIFFERENTIALGENEEXPRESSIONINLUNGCANCERPATIENTSWITHAND
WITHOUTVTE:GSEA
77Sussman etal,ASH2017

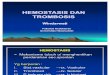
• Podoplanin was associated with ahigh risk ofVTE
• While mutant IDH-1-R12Hwas associated with avery low risk for VTE
• IDH-1-R132Hmutation is only detected intumors,which arepodoplanin negative– Subhazard ratio(SHR)for podoplanin positiveplusIDH-1-R132Hwt tumors,compared to
podoplanin negative plusIDH-1-R132Hmutant tumors:4.69,95%CI:1.28- 17.17;p=0.020).
1152 |
PB 2303 | Elevated Risk of Venous Thrombosis Post Allogeneic Transplantation for Leukemia: Patient Characteristics of a Single Centre Cohort
R. Ikesaka1, N. Cantor2, M. Carrier3, M. Sabloff4
1University of Ottawa and the Ottawa Hospital Research Institute, Hematology/Thrombosis, Ottawa, Canada, 2Ottawa Hospital Research Institute, Hematology, Ottawa, Canada, 3Ottawa Hospital Research Institute at the University of Ottawa, Hematology/Thrombosis, Ottawa, Canada, 4Ottawa Blood Disease Centre, Hematology, Ottawa, Canada
Background: Leukemia patients undergoing allogeneic hematopoietic
stem cell transplant are at increased risk of venous thromboembolism
(VTE) due to need for central venous catheter for supportive care,
chemotherapy and graft versus host disease(GVHD). This specific
post-transplant population is poorly described.
Aims: We sought to describe the rate of events and patient charac-
teristics of individuals who develop VTE in the post allogeneic hemat-
opoietic stem cell transplant period in a cohort of leukemia patients.
Methods: The study was approved by the Ottawa Health Science
Network Research Ethics Board. We retrospectively reviewed the
charts of all patients diagnosed with acute leukemia at the Ottawa
Hospital from January 2007 to September 2015. Patients‘ demo-
graphics, details of transplant and thrombosis characteristics were
added to a database of all leukemia patients diagnosed by our
centre.
Results: 166 leukemia patients underwent allogeneic bone marrow
transplantation. There were 46 venous thrombosis events (27.7%;
95% confidence intervals (CI): 21.1 to 35.2%). Of these events,
15/166 (9.0%; 95%CI: 5.1 to 14.5%) of the transplant population de-
veloped a VTE in the post-transplant period. Descriptive statistics are
depicted in Table 1.
T A B L E 1Պ Characteristics of patients developing post allogeneic hematopoietic stem cell transplant thrombosis. N=15
N % N %
Gender Leukemia Type
Male 11 73.0 AML 9 60.0
Female 4 27.0 ALL 5 33.3
Ambiguous Lineage
1 6.7
Mean Age (sd)
47.6 (16.2)
BMI (sd)
26.07 (3.17) Stem Cell Source
HLA Matched Unrelated Donor
10 66.7
HLA Matched Related Donor
4 26.7
HLA Mismatch 7/8 Unrelated Donor
1 6.7
11/15 (73%) of the patients with post allogeneic hematopoietic stem
cell transplant VTE had either acute or chronic GVHD. The median
time from transplant to diagnosis of VTE was 206 days(range 0-2498
days). There were 6 leukemia relapses post allogeneic hematopoietic
stem cell transplant in this population of 15 patients who developed
VTE. Thrombosis predated the diagnosis of relapse in 5/6 cases by a
mean of 3.35 months (standard deviation 2.20). The site of VTE and
first vs recurrent event is depicted in Table 2.
T A B L E 2ՊSite of VTE and First vs. Recurrente VTE event N=15
Site of Thrombosis N % Post Transplant VTE N %
PE 1 6.7 First VTE event 6 40.0
DVT 6 40.0 Recurrent VTE 9 60.0
PE+DVT 2 13.3
Upper Extremity DVT 2 13.3 On DVT prophylaxis at the time of VTE
1 6.7
Upper Extremity Superficial thrombosis
3 20.0
Portal Vein Thrombosis 1 6.7
Conclusions: There is a high rate of VTE in the post allogeneic hemat-
opoietic stem cell transplant leukemia population. GVHD is present
in a high number of those that develop VTE. Long term prophylaxis
strategies in this high risk population should be investigated.
PB 2304 | Combination of Podoplanin Expression and IDH-1 Mutation Status in Primary Malignant Brain Tumors Identifies Patients at Risk of Venous Thromboembolism
J. Riedl, P.M.S. Nazari, M. Preusser, F. Posch, C. Marosi, P. Birner, J. Thaler, G. Ricken, J.A. Hainfellner, I. Pabinger, C. AyMedical University of Vienna, Vienna, Austria
Background: Venous thromboembolism (VTE) is common in patients
with primary malignant brain tumors. Recently, independent stud-
ies have reported intratumoral podoplanin expression and IDH-1
mutation status as novel risk predictors for VTE in these patients.
However, the interrelation between podoplanin and IDH-1 muta-
tion and their combined effect on risk of VTE has so far not been
investigated.
Aims: We explored the association of podoplanin with IDH-1 muta-
tion status and their combined effect on VTE risk assessment in pa-
tients with primary malignant brain tumors.
Methods: Immunohistochemical staining against podoplanin and
IDH-1-R132H was performed in brain tumor specimens of 213 adult
patients (mostly high-grade gliomas [89%]) included in the Vienna
Cancer and Thrombosis Study (CATS), a prospective observational
| 1153
cohort study of patients with newly diagnosed cancer or progres-sive disease. Primary endpoint was symptomatic VTE within two years.Results: Eighty (37.6%) tumor specimens stained medium or highly positive for podoplanin. IDH-1 mutation was found in 42 (19.7%) tumors. IDH-1-R132H mutation was only found in podoplanin nega-tive tumors, while all podoplanin positive tumors were IDH-1-R132H wildtype (wt) (Figure 1A). During follow-up, 29 (13.6%) patients developed VTE. Expression of podoplanin was associated with a high risk of VTE, while mutant IDH-1-R12H was associated with a very low risk for VTE. In com-peting risk analysis, a combined variable of podoplanin and IDH-1 mutation predicted risk of VTE (Figure 1B). This association was independent of tumor type: subhazard ratio (SHR) for podoplanin positive plus IDH-1-R132H wt tumors, compared to podoplanin negative plus IDH-1-R132H mutant tumors: 4.69, 95%CI: 1.28-17.17; p=0.020).
Conclusions: IDH-1-R132H mutation is only detected in tumors, which are podoplanin negative. Determination of podoplanin and IDH-1-R132H mutation in primary malignant brain tumors identifies patients with both very high and very low risk of developing VTE.
PB 2305 | Podoplanin Promotes Oral Cancer Malignancy by Inducing Intravascular Coagulation in Orthotopic Xenograft Mice ModelH.-Y. Lee1, J.-C. Cheng2, C.-P. Tseng1,3
1Chang Gung University, Graduate Institute of Biomedical Sciences, Taoyuan, Taiwan, Republic of China, 2China Medical University, Taiwan, Department of Medical Laboratory Science and Biotechnology, Taichung, Taiwan, Republic of China, 3Chang Gung University, Department of Medical Biotechnology and Laboratory Science, Taoyuan, Taiwan, Republic of China
Background: Tumor-associated thrombosis is a lethal cause in patients with cancer. Podoplanin (PDPN), a small transmembrane glycoprotein, mediated tumor cell-induced platelets aggregation (TCIPA) has been studied in different cancer types. Emerging data also indicated that PDPN is a malignant indicator of human oral squamous cell carcinoma (OSCC).
Aims: To define whether and how PDPN promotes OSCC malignant progression.Methods: A luciferase-expressing PDPN positive (P+Luc+) OECM-1 cells was used as our study model. P+Luc+shLacZ and P+Luc+shPDPN sublines were established by introducing short-hairpin RNA target-ing on b-galactosidase or pdpn into P+Luc+ cells, respectively. The cell growth rate and the ability to induce platelet aggregation of these cell lines were analyzed in vitro. An orthotopic xenograft animal model was established for functional analysis of PDPN in OSCC. The tumor growth rate was analyzed by in vivo image system (IVIS). Indicators of tumor-associated thrombosis were analyzed by immunofluorescence staining for tumor sections and enzyme-linked immunosorbent assay (ELISA) for plasma samples.Results: In vitro analysis revealed no difference for the cell growth or the ability to induce TCIPA of shLacZ and shPDPN cells. In IVIS analysis, the tumor growth rate also had no difference between shLacZ and shPDPN tumor (p > 0.05). However, the survival time of the mice bearing shP-DPN tumors prolonged when compared to shLacZ tumors (p < 0.001). Notably, 29.4% (5/17) of mice bearing shLacZ tumor died suddenly, without any signs of deterioration. Comparing to mice bearing shPDPN tumor, mice with shLacZ tumor was associated with a 2.4-fold increase of platelet infiltration to tumor tissue (p < 0.05) and a 1.4-fold increase in the plasma levels of thrombin-anti-thrombin complex (p < 0.05).Conclusions: PDPN promotes disease progression by inducing tumor cells-platelet interactions and intravascular coagulation, which reduce lifespan of the mice with OSCC tumors.
PB 2306 | Thrombin Generation in Patients with Active Multiple Myeloma and Impact of Immunomodulators. The ROADMAP StudyL. Papageorgiou1, P. Van Dreden2, D. Fotiou3, M.S. Guye4, L. Garderet4, E. Terpos3, S. Salta5, T. Sergentanis3, M. Dimopoulos6, A. Larsen1, I. Elalamy1,7, G. Gerotziafas1,7
1Cancer Biology and Therapeutics, INSERM U 938, Institut Universitaire de Cancérologie (IUC), Université Pierre et Marie Curie (UPMC), Sorbonne Universities, Faculté de Médecine Pierre et Marie Curie, Paris, France, 2Clinical Research, Diagnostica Stago, Gennevilliers, France, 3National and Kapodistrian University of Athens, School of Medecine, Athens, Greece, 4Hôpital Saint Antoine, APHP, Hématologie et Thérapie Cellulaire, Paris, France, 5Service d‘Hématologie Biologique, Hôpital Tenon, Hôpitaux Universitaires Est Parisien, Assistance Publique Hôpitaux de Paris, Paris, France, 6National and Kapodistrian University of Athens, School of Medecine, Department of Clinical Therapeutics, Athens, Greece, 7Service d‘Hématologie Biologique Hôpital Tenon, Hôpitaux Universitaires Est Parisien, Assistance Publique Hôpitaux de Paris, Paris, France
Background: Multiple myeloma (MM) and the associated immunomodu-latory (IMiD) treatments are associated with an incresed risk of vascular complications. Thrombin generation (TG) assessment reflects the equi-librium between procoagulant and anticoagulant potenties in plasma.Aims: We conducted a multicenter study, to explore the relationship between stages of MM and alterations of TG profile.Methods: MM patients (n=129) were recruited from July 2014 to December 2016 and stratified to the following groups: 44 newly
F I G U R E 1Պ (A) IDH-1 R132H mutation according to podoplanin expression. (B) Incidence of VTE according to podoplanin expression and IDH-1 R132H mutation

NewVTErisk (or protective)factors based on tumorgenomicsIDHmutation andVTE
• Mutant IDH1haspotent antithrombotic activity within gliomasandthroughout the peripheral circulation– ActaNeuropathol.2016Dec;132(6):917930.

Khorana Predictive Model
Khoranaetal.Blood.2008;111(10):4902-7. 10Khoranaetal.Blood.2008;111(10):4902-7.
TheassociationofVTEwithmultiplevariableswascharacterizedinaderivationcohortof2701canceroutpatientsfromaprospectiveobservationalstudy.Ariskmodelwasderivedandvalidatedinanindependentcohortof1365patientsfromthesamestudy.

Applying Risk Assessment
11Angelini &Khorana.Sem Throm Hem2017
Emerging applications for risk assessment need tobeclinically integrated

Applying Risk AssessmentPrognosis
12
Kuderer etalOncologist2016Sohal etalCancer2015;Sohal etalASCOGI2016
PancreascancerN=334
GeneralcancerpopulationN=4,405

Applying Risk AssessmentEarly Detection
13
KhoranaAAetal.Throm Res2014KhoranaAAetal.Throm Res2016
Applying Risk Assessment Screening
Khorana AA et al. Throm Res 2014
Khorana et al. Thromb Res 2017;151:89-95.
Open design - Dalteparin 5000 IU od for 12 weeks versus no LMWH • cancer patients with a Khorana score ≥ 3• new chemotherapy (first or new regimen), CUS‡ / 4 weeks & CT scan at 12 weeks
PHACS (Prophylaxis of High-risk Ambulatory Cancer patients Study) study: KS ≥ 3
‡ Compression Ultrasonography
LMWH no LMWH
46 % 48 %pancreas, stoach
30 % 27 %lung, gynecologic,lymphoma
12 % 21 %all VTE HR = 0.69 [0.23 – 1.89] ns
2.0 % 2.1 %Major bleeding ns
12 % 2.1 %Major + CRNM bleeding
50 48
4 % 4 %symptomatic VTE
2 % 6 %incidental PE
4 % 10 %proximal DVT (CUS)
HR = 7.02 [1.24 – 131] p=0.025Singleinstitutionstudy
Screen-detected DVTEUS

Khorana scorelimitations
14Khorana A.ICTHICBérgamo2018

Development andExternal Validation ofaRisk Assessment Model(RAM)for Cancer-associated VTE
• Two prospective cohorts:CATS&MICAcohorts
• Development andexternal validation
• Model with 2variables:• Tumorsite• D-dimer
• The model discriminated well betweencancer patients with andwithout VTE
• C-Index=0.67,95%CI0.64-0.68• C-Index=0.66,95%CI:0.58-0.72
• Compared to KS:• Netreclassification improvement=0.44
Pabinger Ietal.Lancet Hematol 2018
2variables
15

Heritability of VTE
Family Twin
50-60% of the VTE events is attributed to genetic factors
Souto JC et al, Am J Hum Genet, 2000Larsen TB et al, Epidemiology, 2003Zöller B et al, Thromb Res, 2017

Anewclinico-genetic risk score(TiC score)GRS(12SNPS/7genes)
SNPs Gene Prevalence in DVT patients Relative risk
46C>T FXII 6% 5rs8176719
ABO Group (A1 carriers) nd
2-4
(+ FV Leiden: 4-23)
rs7853989rs8176743rs8176750Arg67Stop Serpin A10 (Pr Z) 4,4 % 3,3
Ala384Ser (Cambridge II) Serpin C1(Antitrombina) 1,7 % 10
Arg506Gln (FV Leiden)
Factor V (FV)
15-25% 5
Arg306Thr (FV Cambridge) nd nd
Arg306Gly (FV Hong Kong) nd nd
Val34Leu Factor XIII (FXIII) 2% Protective factor
G20210A ProthrombinFactor II (FII) 6-16% 2-3
MuñozAJ&SoriaJMetal.BJC2018

ARTICLEClinical Study
Multivariable clinical-genetic risk model for predicting venousthromboembolic events in patients with cancerAndrés J. Muñoz Martín1,2, Israel Ortega3, Carme Font2,4, Vanesa Pachón2,5, Victoria Castellón2,6, Virginia Martínez-Marín2,7,Mercedes Salgado2,8, Eva Martínez2,9, Julia Calzas2,10, Ana Rupérez2,11, Juan C. Souto12, Miguel Martín1,2, Eduardo Salas3 andJose M. Soria13
BACKGROUND: Venous thromboembolism (VTE) is a leading cause of death among patients with cancer. Outpatients with cancershould be periodically assessed for VTE risk, for which the Khorana score is commonly recommended. However, it has beenquestioned whether this tool is sufficiently accurate at identifying patients who should receive thromboprophylaxis. The presentwork proposes a new index, TiC-Onco risk score to be calculated at the time of diagnosis of cancer, that examines patients’ clinicaland genetic risk factors for thrombosis.METHODS: We included 391 outpatients with a recent diagnosis of cancer and candidates for systemic outpatient chemotherapy.All were treated according to standard guidelines. The study population was monitored for 6 months, and VTEs were recorded. TheKhorana and the TiC-Onco scores were calculated for each patient and their VTE predictive accuracy VTEs was compared.RESULTS:We recorded 71 VTEs. The TiC-Onco risk score was significantly better at predicting VTE than the Khorana score (AUC 0.73vs. 0.58, sensitivity 49 vs. 22%, specificity 81 vs. 82%, PPV 37 vs. 22%, and NPV 88 vs. 82%).CONCLUSIONS: TiC-Onco risk score performed significantly better than Khorana score at identifying cancer patients at high risk ofVTE who would benefit from personalised thromboprophylaxis.
British Journal of Cancer https://doi.org/10.1038/s41416-018-0027-8
INTRODUCTIONPatients with cancer (taking all types together) are at 7 times therisk of developing a venous thromboembolism (VTE); in somemalignancies the risk increases to 28 times.1 The incidence ofcancer-associated VTE is particularly high during the first fewmonths after diagnosis, when distant metastases are present, andafter initiating chemotherapy.1, 2 VTE is a leading cause of deathamong patients with cancer,3 and the survival of an episode mayhave clinical and economic implications, including hospitalisation,potential delays in cancer therapy, recurrent VTE, post-thromboticsyndrome, and chronic thromboembolic pulmonary hypertension.Indeed, these problems are common, costly, and have a profoundimpact on the patient's quality of life.3
Different guidelines cover the identification of patients withcancer at risk of VTE, VTE prevention strategies, and treatment.4–6
These documents indicate that most hospitalised patients withactive cancer require thromboprophylaxis throughout hospitalisa-tion. However, in the outpatient setting, it is indicated only for
high-risk patients. Outpatients with cancer should be periodicallyassessed for VTE risk, for which the validated risk assessment tooldeveloped by Khorana—the Khorana score7 is commonlyrecommended. However, in recent years, a number of studieshave questioned whether this tool is sufficiently accurate atidentifying patients who should receive thromboprophylaxis.8–10
In the present work, we hypothesised that a genetic componentis involved in the appearance of VTE, a factor that the Khoranascore does not take into account. Recently, the Vienna Group11
showed that the Leiden (rs6025) variant of the gene coding forfactor V in the coagulation pathway doubles the risk of a VTEevent occurring in patients with cancer. This variant might,therefore, provide a promising biomarker of venous thrombosis insuch patients, and could be used in individual risk prediction.12
Other genes are known to increase the risk of VTE in the generalpopulation, and a tool (the Thrombo inCode or TiC tool) involvingthem as markers has been developed to predict VTE—but only for
www.nature.com/bjc
Received: 25 September 2017 Revised: 17 January 2018 Accepted: 22 January 2018
1Medical Oncology Service, Hospital General Universitario Gregorio Marañón, C/ Doctor Esquerdo, 46, 28007 Madrid, Spain; 2Cancer & Thrombosis Working Group, SpanishSociety of Medical Oncology (SEOM), C/ de Velázquez, 7, 28001 Madrid, Spain; 3Scientific Department, Gendiag, Joan XXIII, 10, 08950 Esplugues de Llobregat, Spain; 4MedicalOncology, Hospital Clínic, c/ Villarroel, 170, 08036 Barcelona, Spain; 5Medical Oncology, Hospital Universitario Ramón y Cajal Madrid, Ctra. Colmenar Viejo, Km. 9,100, 28034Madrid, Spain; 6Medical Oncology, Complejo Hospitalario de Torrecárdenas, c/ Hermandad de Donantes de Sangre, 04009 Almería, Spain; 7Medical Oncology, HospitalUniversitario la Paz, Paseo de la Castellana, 261, 28046 Madrid, Spain; 8Medical Oncology, Complejo Hospitalario Universitario de Ourense, c/ Ramon Puga Noguerol, 54, 32005Ourense, Spain; 9Medical Oncology, Hospital Universitario Marqués de Valdecilla, Av. Valdecilla, 25, 39008 Santander, Spain; 10Medical Oncology, Hospital Universitario deFuenlabrada, Camino del Molino, 2, 28942 Madrid, Spain; 11Medical Oncology, Fundación Jiménez Díaz, Av. Reyes Católicos, 2, 28040 Madrid, Spain; 12Thrombosis andHaemostasia, Hospital de la Santa Creu i Sant Pau, Carrer de Sant Quintí, 89, 08041 Barcelona, Spain and 13Genomic of complex diseases, Institut d’Investigació Sant Pau (IIB-SantPau), Carrer de Sant Quintí, 89, 08041 Barcelona, SpainCorrespondence: Andrés J. Muñoz Martín ([email protected])
© The Author(s) 2018 Published by Springer Nature on behalf of Cancer Research UK
primary tumour site (low, high, and very high) was categorised aswhen determining the Khorana score.15 The risks associated withplatelet and leukocyte numbers were categorised using the samecut-offs as for the Khorana score.15
At 6 months, univariate analysis was performed to determinewhich of these variables were associated with the appearance of aVTE event. Those associated with an increased risk of VTE (p ≤0.25) were selected.3. Development of the clinical-genetic model.The genetic risk score and the clinical variables selected were
subjected to multivariate logistic regression analysis using an AIC-based backward selection process.16
Internal validationInternal validation to obtain the degree of optimism in the areaunder the receiver operating characteristic (ROC) curve (AUC)estimation was done using the bootstrap approach,17 considering100 resamples from the original data.
Comparing the Khorana and TiC-Onco risk scoresThe risk prediction capacity of the Khorana and TiC-Onco riskscores was evaluated using the area under the receiver operatingcharacteristic (ROC) curve (AUC, larger values indicate betterdiscrimination).18 Standard measures of sensitivity, specificity,positive, and negative predictive value (PPV and NPV), andpositive and negative likelihood ratios (PLR and NLR),19 weredetermined for specific cut-off points.For Khorana score the cut-off defining high risk was set at ≥3
(the normal cut-off value), and 0 for the low risk categorydefinition. We contemplate two scenarios when determining acut-off for the TiC-Onco score. In the first one (the main scenario),the cut-off is selected as the point on the ROC curve giving thesame specificity as provided by the Khorana score (around 80%). Itdefines those individuals who are in high risk. This will be thedefault cut-off for TiC-Onco when not specified in the text. In thisscenario, we also determine a second cut-off to classify the non-high risk individuals into either intermediate or low risk. Thus, weallow the TiC-Onco score to provide three risk categories—high,intermediate, and low risk. This second cut-off to discriminatebetween low and intermediate categories is selected as the pointgiving a sensitivity of 90%. The second scenario is presented justfor informative purposes. In this case, the cut-off is selected as thepoint which maximises the Youden’s index (defined as sensitivity+ specificity−1).20 In this scenario, we only consider a TiC-Oncowith two categories, high risk and non-high risk.
Statistical analysisContinuous variables were recorded as median [1st–3rd Quartiles],and categorical variables as proportions. Univariate associationbetween clinical/genetic variables and events was determinedusing either t-test or Wilcoxon rank sum tests for continuousvariables, and χ2 or Fisher tests for categorical variables. Allcalculations were performed using R statistical software (version3.1.3).21
Number of patients needed to treatTo assess the effect of the TiC-Onco risk score in terms ofpreventing VTE events, the number of patients needed to treat(NNT) was determined for both scores.22 It was assumed thatprophylactic medication would reduce cancer-associated VTE by46%.23
RESULTSPatient characteristicsTables 1 and 2 show the clinical and demographic characteristicsof the 391 patients at the start of the study. For each variable, the
Table 2. Population charactheristics per cancer type
Tumour type Colon Pancreas Lung Oesophagus Stomach Total
Total 163 72 87 14 55 391
Patients (%) 41.69 18.41 22.25 3.58 14.07 100
No-VTE 141 43 76 12 48 320
VTE 22 29 11 2 7 71
% VTE 13.50 40.28 12.64 14.29 12.73 18.16
Stage I+ II 29 18 9 3 12 71
Stage III 74 12 34 5 14 139
Stage IV 60 42 44 6 29 181
Death, n (%) 13 (7.98) 24 (33.33) 13 (14.94) 1 (7.14) 7 (12.73)
VTE death, n (%) 5 (38.46) 14 (58.33) 3 (23.08) 0 0
No-VTE deaths, n (%) 8 (61.54) 10 (41.67) 10 (76.92) 1 (100) 7 (100)
Table 3. Clinical-genetic risk score Thrombo inCode-Oncology (TiC-Onco)
Variable p-value
GRS 0.0049
BMI >25 0.0658
Family history 0.1076
Primary tumour site
HR 0.3483
VHR 0.0033
Tumourstage
0.0003
GRS
rs2232698 0.1460
rs6025 0.2064
rs5985 0.2003
rs4524 0.0396
GRS Genetic Risk Score, HR High Risk, VHR Very High Risk
Clinical-genetic model for predicting VTE in cancer patientAJ Muñoz Martín et al.
3
number and percentage of patients who experienced a VTE, ornot, at some point in the 6-month study period, are shown. Theoverall incidence of VTE was 18%. Patients suffering frompancreatic cancer experienced VTE at a significantly higherfrequency (40%) than patients with other type of cancers (p <0.001) (Table 2).
Development of the TiC-Onco risk modelTable 3 shows the genetic and clinical markers that weresignificantly associated by multivariate analysis with a VTE event,and thus selected for inclusion in the TiC-Onco risk score model.
Accuracy and validation of the risk modelThe TiC-Onco score showed an AUC of 0.73 (0.67–0.79), asensitivity of 49%, and a specificity of 81%. Its PPV was 37%,NPV 88%, PLR 2.6, and NLR 0.6% (Table 4). The Khorana scoreshowed a significantly lower capacity to distinguish betweenpatients who experienced/did not experience a VTE event (AUC0.73 vs. 0.58; p < 0·001). The sensitivity of the TiC-Onco score wassignificantly higher than that of the Khorana (49 vs. 22%; p <0.001), while the specificities of both scores were similar (81 vs.82%; p= 0.823). The PPV and NPV of the TiC-Onco score weresignificantly higher than those of the Khorana score (37 vs. 22%; p= 0.004 for PPV and 88 vs. 82%; p < 0.001 for NPV). The LRs of theTiC-Onco score were also significantly better (Table 4).Table 5 shows the distribution of patients with or without VTE
according to the Khorana score. The great majority of patientswho suffered a VTE event (77%) were identified by the Khoranascore as being at low or moderate risk (values 0, 1, and 2). Amongthese 55 patients, however, 17 (31%) were detected as high-risk
patients by the TiC-Onco score. When the cut-off for high risk wastaken as the best Youden Index, the TiC-Onco score returnedsignificantly better predictions of risk than the Khorana score,especially in terms of sensitivity (86 vs. 22%, p < 0.001) (Table 4). Inthis scenario, of the 55 patients who experienced a VTE event (butwho were classified as not being at high-risk by the Khoranascore), 40 (73%) were detected as high risk patients by the TiC-Onco score. Table 6 shows rates of VTE according to prespecifiedrisk categories for both TiC-Onco and Khorana.The NNT values for: (a) if all patients included in the study had
been treated (NNT= 12); (b) if only the patients with a Khoranascore of ≥3 had been treated (NNT= 10), or (c) if only patientswith a high risk TiC-Onco score (with the cut-off set at the samespecificity as the Khorana score) had been treated (NNT= 6).
DISCUSSIONWhen deciding whether to use primary antithrombotic prophy-laxis in outpatients with cancer who are candidates forchemotherapy, a clinician needs to determine the risk of VTEand weigh the likely benefit against the risk of bleeding. Despitethe awareness of scientific societies regarding cancer-associatedVTE, thromboprophylaxis is limited among outpatients, probablydue to the sub-optimal predictive capacity of the existing toolsused to predict the risk of experiencing a VTE event. The presentwork presents a new predictive score, the TiC-Onco score, whichshows significantly better predictive power in this regard than theKhorana score.The incidence of VTE in the present population at 6 months of
follow-up was 18% (occurring in 71/391 patients); this is within therange of figures cited in a previous publication24 for the samefollow-up period. It is also in agreement with the observation thatthe incidence of VTE is highest among patients with pancreaticcancer.25 However, no other clear differences between tumourtypes were seen with respect to the Khorana score, probablybecause a large proportion (46%) of the present patients hadstage IV tumours.The statistical analysis of the present data detected four genetic
variants that were independently associated with VTE in out-patients with cancer (Table 2). These were combined into thealgorithm for the Tic-Onco score, which initially allowed thepatients to be classified as either at high or low risk of VTE. Amongthe patients in the TiC-Onco high risk group, 37% eventuallysuffered a VTE event, while 12% of those in the low risk groupexperienced the same (Table 4). However, when the three-tier Tic-Onco risk category system was contemplated (explained inMethods), 37% of the high risk, 18% of the moderate risk, and6% of the low risk patients experienced a VTE event. Incomparison, 22, 20, and 13% of the patients in the equivalent
Table 4. Predictive capability of TiC-Onco and Khorana scores
TiC-Onco (1) TiC-Onco (2) Khorana p (TiC-Onco (1) vs Khorana) p (TiC-Onco (2) vs Khorana)
AUC (95% CI) 0.734 (0.67–0.79) 0.734 (0.67–0.79) 0.580 (0.51–0.65) <0.001 <0.001
Sensitivity, % (95% CI) 49.30 (37.7–60.9) 85.92 (77.8–94.0) 22.54 (12.8–32-3) <0.001 <0.001
Specificity, % (95%, CI) 81.25 (77.0–85.5) 49.06 (43.6–54.5) 81.76 (77.5–86.0) 0.823 <0.001
PPV, % (95% CI) 36.84 (27.1–46.5) 27.23 (21.4–33.1) 21.62 (12.2–31.0) 0.004 0.218
NPV, % (95% CI) 87.84 (84.1–91.6) 94.01 (90.4–97.6) 82.54 (78.3–86.7) <0.001 <0.001
PLR (95% CI) 2.63 (1.89 - 3.65) 1.69 (1.46 - 1.95) 1.24 (0.76 - 2.02) 0.005 0.244
NLR (95% CI) 0.62 (0.49 - 0.79) 0.29 (0.16 - 0.52) 0.95 (0.83 - 1.09) 0.001 <0.001
TiC-Onco (1) shows the predictive capabilities for the default cut-off (see Methods). TiC-Onco (2) shows the predictive capabilities for the cut-off providing thebest Youden’s Index. AUC Area Under the Roc Curve, PPV Positive Predictive Value, NPV Negative Predictive Value, PLR Positive Likelihood Ratio, NLR NegativeLikelihood Ratio
Table 5. Patient distribution according to Khorana score consideringpatients with and without VTE
Khorana VTE No-VTE Patients (n) Patients (%) % VTE
0 14 94 108 27.62 12.96
1 11 74 85 21.74 12.94
2 30 92 122 31.20 24.59
≥3 16 58 74 18.93 21.62
NA 0 2 2 0.51 0
Total 71 320 391
Patients (%) percentage of patients per Khorana score level. %VTE casespercentage of patients with VTE in relation to the number of patients perKhorana score level
Clinical-genetic model for predicting VTE in cancer patientAJ Muñoz Martín et al.
4
TiC Onco Khorana score pvalueTiC-onco vsKhorana
AUC 0.719 0.569 <0.001
AUC(95% CI) (0.656-0.781) (0.502-0.63)
MuñozAJ&SoriaJMetal.BJC2018

BRIEF REPORT
Circulating tumor cell count and thrombosis in metastaticbreast cancerG. BE INSE ,* F . BERGER ,† P . COTTU,* M. -E . DUJAR IC ,† I . KR I EGEL ,‡ M.-N . GUILHAUME,*V . D I!ERAS ,* L . CABEL ,* J . -Y . P I ERGA*§ and F . -C . B IDARD**Department of Medical Oncology, Institut Curie, PSL Research University; †Institut Curie, Unit of Biometry, PSL Research University,
INSERM U900; ‡Department of Anesthesiology, Institut Curie, PSL Research University; and §Universit!e Paris Descartes, Paris, France
To cite this article: Beinse G, Berger F, Cottu P, Dujaric M-E, Kriegel I, Guilhaume M-N, Di!eras V, Cabel L, Pierga J-Y, Bidard F-C. Circulating
tumor cell count and thrombosis in metastatic breast cancer. J Thromb Haemost 2017; 15 : 1981–8.
Essentials
• Tumor cells circulating in blood (CTC) may favorthrombotic events in cancer patients.
• We assessed the impact of CTC on the risk of thrombo-sis in metastatic breast cancer.
• Baseline CTC detection was the only independent factorassociated with the risk of thrombosis.
• CTC detection under therapy may be the hidden linkbetween tumor progression & thrombosis.
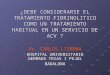
Summary. Background: Circulating tumor cell (CTC)count is a major prognostic factor in metastatic breastcancer (MBC) and has been reported to be associated withthrombosis in short-term studies on MBC patients. Objec-tive: To assess whether CTC detection (CellSearch!)before first-line chemotherapy impacts the risk of throm-bosis throughout the course of MBC. Patients/Methods:Among patients included before first-line chemotherapyfor MBC in the prospective IC2006-04 CTC detectionstudy (NCT00898014), the electronic medical files of thosepatients treated at Institut Curie (Paris, France) weresearched in silico and manually checked for incidentvenous or arterial thrombotic events (TE) in the course ofMBC. Univariate and multivariate analyses were per-formed using Cox and Fine-Gray models, adjusted for ageand Khorana score. Results/Conclusions: With a medianfollow-up of 64 months (25–81 months), among the 142patients included, 34 (24%) experienced a TE (incidencerate, 8 TE/100 patient-years). The TE incidence rate was13 TE/100 patient-years for the 80 patients with ≥ 1
CTC/7.5 mL of blood before initiating first-linechemotherapy, vs. only 4 TE/100 patient-years for the 62CTC-negative patients. Fine-Gray multivariate analysis(with death as competing event) included age, Khoranascore and baseline lactate dehydrogenase and CTC levels:detectable CTC was the only factor significantly associatedwith an increased risk of TE (sub-distribution hazardratio [SHR] for patients with [1–4] CTC = 3.1, 95% CI[1.1; 8.6], SHR for patients with ≥ 5 CTC = 1.4, 95% CI[0.5; 4.6]). This study shows that CTC detection beforestarting first-line chemotherapy is an independent riskfactor for TE in MBC patients.
Keywords: biomarkers; breast neoplasms; circulating;neoplasm metastasis; neoplastic cells; thrombosis.
Background
A cancer-related thrombotic event (TE) is a frequent andpossibly life-threatening condition. Known risk factorsfor TEs are age, cancer histology, presence of metastases,use of chemotherapy, presence of central venous cathe-ters, altered performance status (PS), anemia, thrombocy-tosis and high body mass index [1]. The Khorana score[2], based on type of cancer, body mass index, plateletcount, leukocyte count and hemoglobin level, has beenvalidated as a predictor of the risk of a venous TE in can-cer patients. In early breast cancer, a meta-analysisreported an overall low incidence of about 10 TE/1000patient-years [3], but the incidence of TEs in metastaticbreast cancer (MBC) patients remains uncertain becauseof the different methods used to detect TEs and heteroge-neous follow-up (11 to 176/1000 patients-years [3]).
The underlying mechanisms of cancer-related TEs havebeen reviewed elsewhere [3,4]. Among these various mech-anisms, tissue factor activity has been correlated withtumor burden and detection of tumor cells in blood [5,6].These cells, known as circulating tumor cells (CTCs),have been repeatedly reported to be a major prognostic
Correspondence: Francois-Clement Bidard, Department of Medical
Oncology, Institut Curie, Paris, France
Tel.: +33 144 324 000
E-mail: [email protected]
Received: 11 May 2016
Manuscript handled by: J.-B. Hansen
Final decision: F. R. Rosendaal, 1 August 2017
© 2017 International Society on Thrombosis and Haemostasis
Journal of Thrombosis and Haemostasis, 15: 1981–1988 DOI: 10.1111/jth.13792
CTCdetection before starting first-linechemotherapy is an independent risk factorfor TEinMBCpatients
Whether decreased CTCcount during therapy is significantly associated with decreased risk ofaTEremains tobeconfirmed
Baseline CTCcount,whenever available,should betaken into account when considering the need for primarythromboprophylaxis inMBCpatients
34 patients, 24 (71%) died thereafter. Only one of the 32patients alive without a TE was lost to follow-up (no dataavailable for > 6 months). TE subtypes were as follows:deep vein thrombosis in 11 patients (32% of TEs), vis-ceral vein thrombosis in 10 patients (29%), catheterthrombosis in five patients (15%), pulmonary embolismin five patients (15%) and arterial TEs in three patients(9%). These subgroups were too small to perform reliableassociation tests with CTC detection.
Higher TE incidences were observed in patients withelevated baseline LDH (15.6 TE/100 patient-years [8.5;26.1] vs. 5.9 TE/100 patient-years [3.4; 9.5]) and patientswith ≥ 1 CTC at baseline (12.8 TE/100 patient-years [8.2;19.0] vs. 4.4 TE/100 patient-years [2.1; 8.1]). In univariateanalysis using the Cox model, baseline characteristics sig-nificantly associated with higher risks of TEs were CTC
detection (patients with ≥ 1 CTC had an age- and Kho-rana score-adjusted CSHR = 2.9 [1.3; 6.6] compared withpatients with no CTC detected) and elevated LDH (ad-justed CSHR = 2.6 [1.2; 5.6]) (Table 2). When death wastaken into account as a competing event (Fine-Graymodel), univariate analyses confirmed that, at baseline,≥ 1 CTC (adjusted SHR = 2.3 [1.0; 5.4]) and elevatedLDH (adjusted SHR = 2.1 [1.0; 4.5]) were significantlyassociated with the risk of a TE (Table 2). Figure 1 dis-plays the cumulative incidence of TEs and death accord-ing to baseline CTC count. Multivariate analysesconfirmed that patients with CTC detected at baselinewere at higher risk of a TE (Table 2).
Finally, as the IC2006-04 study prospectively assessedearly CTC changes during first-line chemotherapy, weinvestigated whether CTC detection at 3–5 weeks was
0 12 24 36Months
48 60 72
Cumulative incidence of deathbased on Kaplan–Meier estimator (CSH)
CTC = 0CTC = [1-4]CTC ≥ 5
0.0
0.2
0.4
0.6
0.8
1.0C
umul
ativ
e in
cide
nce
0.00 12 24 36
Months48 60 72 0 12 24 36
Months48 60 72
0.2
0.4
0.6
0.8
1.0CTC = 0
Cumulative incidence of TEbased on Kaplan–Meier estimator (CSH)
Cumulative incidence of TEbased on cumulative incidence function (SH)
CTC = [1-4]CTC ≥ 5
CTC = 0
CTC = [1-4]CTC ≥ 5
Cum
ulat
ive
inci
denc
e
0.0
0.2
0.4
0.6
0.8
1.0
Cum
ulat
ive
inci
denc
e
Fig. 1. Cumulative incidence of thrombotic events and death according to baseline CTC count. CSH, cause-specific hazard; SH, sub-distribu-tion hazard; CTC, circulating tumor cells. Cause-specific hazards do not take into account competing events; sub-distribution hazard of throm-botic events takes into account death as a competing risk.
© 2017 International Society on Thrombosis and Haemostasis
1986 G. Beinse et al
34 patients, 24 (71%) died thereafter. Only one of the 32patients alive without a TE was lost to follow-up (no dataavailable for > 6 months). TE subtypes were as follows:deep vein thrombosis in 11 patients (32% of TEs), vis-ceral vein thrombosis in 10 patients (29%), catheterthrombosis in five patients (15%), pulmonary embolismin five patients (15%) and arterial TEs in three patients(9%). These subgroups were too small to perform reliableassociation tests with CTC detection.
Higher TE incidences were observed in patients withelevated baseline LDH (15.6 TE/100 patient-years [8.5;26.1] vs. 5.9 TE/100 patient-years [3.4; 9.5]) and patientswith ≥ 1 CTC at baseline (12.8 TE/100 patient-years [8.2;19.0] vs. 4.4 TE/100 patient-years [2.1; 8.1]). In univariateanalysis using the Cox model, baseline characteristics sig-nificantly associated with higher risks of TEs were CTC
detection (patients with ≥ 1 CTC had an age- and Kho-rana score-adjusted CSHR = 2.9 [1.3; 6.6] compared withpatients with no CTC detected) and elevated LDH (ad-justed CSHR = 2.6 [1.2; 5.6]) (Table 2). When death wastaken into account as a competing event (Fine-Graymodel), univariate analyses confirmed that, at baseline,≥ 1 CTC (adjusted SHR = 2.3 [1.0; 5.4]) and elevatedLDH (adjusted SHR = 2.1 [1.0; 4.5]) were significantlyassociated with the risk of a TE (Table 2). Figure 1 dis-plays the cumulative incidence of TEs and death accord-ing to baseline CTC count. Multivariate analysesconfirmed that patients with CTC detected at baselinewere at higher risk of a TE (Table 2).
Finally, as the IC2006-04 study prospectively assessedearly CTC changes during first-line chemotherapy, weinvestigated whether CTC detection at 3–5 weeks was
0 12 24 36Months
48 60 72
Cumulative incidence of deathbased on Kaplan–Meier estimator (CSH)
CTC = 0CTC = [1-4]CTC ≥ 5
0.0
0.2
0.4
0.6
0.8
1.0
Cum
ulat
ive
inci
denc
e
0.00 12 24 36
Months48 60 72 0 12 24 36
Months48 60 72
0.2
0.4
0.6
0.8
1.0CTC = 0
Cumulative incidence of TEbased on Kaplan–Meier estimator (CSH)
Cumulative incidence of TEbased on cumulative incidence function (SH)
CTC = [1-4]CTC ≥ 5
CTC = 0
CTC = [1-4]CTC ≥ 5
Cum
ulat
ive
inci
denc
e
0.0
0.2
0.4
0.6
0.8
1.0
Cum
ulat
ive
inci
denc
e
Fig. 1. Cumulative incidence of thrombotic events and death according to baseline CTC count. CSH, cause-specific hazard; SH, sub-distribu-tion hazard; CTC, circulating tumor cells. Cause-specific hazards do not take into account competing events; sub-distribution hazard of throm-botic events takes into account death as a competing risk.
© 2017 International Society on Thrombosis and Haemostasis
1986 G. Beinse et al
“Liquid biopsies”(circulating tumorDNA)andmiRNA profiling approaches arealso becoming moreinteresting inVTEprediction

DOACs inCancer Patients:Clinical Trials
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med nejm.org 1
From the University of Oklahoma Health Sciences Center, College of Public Health, Oklahoma City (G.E.R.); the Department of Vascular Medicine, Academic Medical Center, University of Amsterdam (N.E., H.R.B.), and ITREAS, Academic Research Organization (A.S.) — both in Amsterdam; the Department of Vascular Medicine and Hemostasis, University Hospitals Leuven, Leuven, Belgium (P.V.); Ottawa Hospital Research Institute, Ottawa (M.C.), London Health Sciences Centre–Victoria Hospital, London, ON (M.J.K.), University Health Network, University of Toronto, Toronto (E.Y.), and McMaster University and the Thrombosis and Atherosclerosis Research Institute, Hamilton, ON (J.I.W.) — all in Canada; the Department of Medicine and Aging Sciences, University G. D’Annunzio, Chieti, Italy (M.D.N.); the Department of Medicine, Division of Hematology, Uni-versity of Washington, Seattle (D.G.); Dai-ichi Sankyo Pharma Development, Bask-ing Ridge, NJ (M.A.G., M.F.M., M.S., G.Z.); Thrombosis Research Institute and Uni-versity College London, London (A.K.K.); the Department of Respiratory Disease, Hôpital Européen Georges-Pompidou, As-sistance Publique–Hôpitaux de Paris, Paris (G.M.); the Department of Internal Medi-cine, Division of Hematology, Ohio State University Wexner Medical Center, Colum-bus (T.-F.W.); and Beth Israel Deaconess Medical Center, Harvard Medical School, Boston (J.I.Z.). Address reprint requests to Dr. Raskob at the University of Okla-homa Health Sciences Center, College of Public Health, 801 NE 13th St., Oklaho-ma City, OK 73104, or at gary-raskob@ ouhsc . edu.
* A complete list of Hokusai VTE Cancer In-vestigators is provided in the Supplemen-tary Appendix, available at NEJM.org.
This article was published on December 12, 2017, at NEJM.org.
DOI: 10.1056/NEJMoa1711948Copyright © 2017 Massachusetts Medical Society.
BACKGROUNDLow-molecular-weight heparin is the standard treatment for cancer-associated ve-nous thromboembolism. The role of treatment with direct oral anticoagulant agents is unclear.
METHODSIn this open-label, noninferiority trial, we randomly assigned patients with cancer who had acute symptomatic or incidental venous thromboembolism to receive either low-molecular-weight heparin for at least 5 days followed by oral edoxaban at a dose of 60 mg once daily (edoxaban group) or subcutaneous dalteparin at a dose of 200 IU per kilogram of body weight once daily for 1 month followed by dalteparin at a dose of 150 IU per kilogram once daily (dalteparin group). Treatment was given for at least 6 months and up to 12 months. The primary outcome was a composite of re-current venous thromboembolism or major bleeding during the 12 months after randomization, regardless of treatment duration.
RESULTSOf the 1050 patients who underwent randomization, 1046 were included in the modi-fied intention-to-treat analysis. A primary-outcome event occurred in 67 of the 522 patients (12.8%) in the edoxaban group as compared with 71 of the 524 patients (13.5%) in the dalteparin group (hazard ratio, 0.97; 95% confidence interval [CI], 0.70 to 1.36; P = 0.006 for noninferiority; P = 0.87 for superiority). Recurrent venous thromboembolism occurred in 41 patients (7.9%) in the edoxaban group and in 59 patients (11.3%) in the dalteparin group (difference in risk, −3.4 percentage points; 95% CI, −7.0 to 0.2). Major bleeding occurred in 36 patients (6.9%) in the edoxaban group and in 21 patients (4.0%) in the dalteparin group (difference in risk, 2.9 per-centage points; 95% CI, 0.1 to 5.6).
CONCLUSIONSOral edoxaban was noninferior to subcutaneous dalteparin with respect to the com-posite outcome of recurrent venous thromboembolism or major bleeding. The rate of recurrent venous thromboembolism was lower but the rate of major bleeding was higher with edoxaban than with dalteparin. (Funded by Daiichi Sankyo; Hokusai VTE Cancer ClinicalTrials.gov number, NCT02073682.)
A BS TR AC T
Edoxaban for the Treatment of Cancer-Associated Venous Thromboembolism
Gary E. Raskob, Ph.D., Nick van Es, M.D., Peter Verhamme, M.D., Marc Carrier, M.D., Marcello Di Nisio, M.D., David Garcia, M.D.,
Michael A. Grosso, M.D., Ajay K. Kakkar, M.B., B.S., Michael J. Kovacs, M.D., Michele F. Mercuri, M.D., Guy Meyer, M.D., Annelise Segers, M.D.,
Minggao Shi, Ph.D., Tzu-Fei Wang, M.D., Erik Yeo, M.D., George Zhang, Ph.D., Jeffrey I. Zwicker, M.D., Jeffrey I. Weitz, M.D., and Harry R. Büller, M.D.,
for the Hokusai VTE Cancer Investigators*
Original Article
The New England Journal of Medicine Downloaded from nejm.org by HANS GELDERBLOM on December 12, 2017. For personal use only. No other uses without permission.
Copyright © 2017 Massachusetts Medical Society. All rights reserved.
Anticoagulation Therapy in SELECTeD Cancer Patients at Risk of Recurrence of Venous Thromboembolism
Annie Young PhD Professor of Nursing, University of Warwick, UK
on behalf of the select-d Collaborative Group 11 December 2017
L.ES.MA.01.2018.3810
JCO’2018
Raskob etal.NEJM2017

Hokusai VTE - Cancer Study Design
Treatment for up to 12 months (at least 6 months)
Efficacy and safety data collected during the entire 12 month study period
Independent blind adjudication of all suspected outcomes
Severity of major bleeding at presentation also adjudicated
N:~1000
Objectively Confirmed VTE• Stratified randomization for �Bleeding Risk �Dose Adjustment
• PROBE design•114 sites North America,
Europe, Australia, New Zealand
R
Dalteparin 200 IU/kg
Day 30Day 0
Dalteparin 150 IU/kg
Edoxaban 60 mg QD*
Day 5
LMWH
Month 12
N:~500
N:~500
Raskob etal.NEJM2017

n engl j med nejm.org 8
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
bolism or major bleeding. The rate of recurrent venous thromboembolism was numerically low-er with edoxaban than with dalteparin (7.9% and 11.3%, respectively; hazard ratio, 0.71; 95% CI, 0.48 to 1.06; P = 0.09) because of the lower rate of recurrent symptomatic deep-vein throm-bosis with edoxaban (Table 2). The 8.8% rate of recurrent venous thromboembolism at 6 months in the dalteparin group in this trial is consistent with rates reported with dalteparin in previous studies involving patients with cancer.4,16
The rate of major bleeding was significantly higher with edoxaban than with dalteparin (6.9% and 4.0%, respectively; hazard ratio, 1.77; 95% CI, 1.03 to 3.04; P = 0.04). This difference was mainly due to the higher rate of upper gas-trointestinal bleeding with edoxaban. This find-ing is consistent with results of previous studies of direct oral anticoagulants.11 The increase in upper gastrointestinal major bleeding occurred mainly in patients who had entered the trial with gastrointestinal cancer. However, the frequency of severe major bleeding (category 3 or 4; see Table 2) was similar with edoxaban and daltepa-rin. The 3.2% rate of major bleeding at 6 months in the dalteparin group in this trial is lower than previously reported rates with dalteparin.4,16
Our trial has some limitations. First, the use
of an open-label design is a potential weakness, but long-term administration of placebo injec-tions was not considered to be appropriate. To mitigate potential bias, all events were adjudi-cated by a committee whose members were un-aware of the treatment assignments. Second, the number of primary-outcome events was lower than expected; despite this limitation, noninfe-riority was established. Third, the median dura-tion of the assigned treatment was shorter with dalteparin than with edoxaban, which may have influenced the relative efficacy of the two treat-ments. However, this difference was primarily due to the inconvenience of the use of subcuta-neous dalteparin as compared with oral edoxa-ban, thus demonstrating the desirability of oral therapy in this context. In addition, the sensitiv-ity analysis of events that occurred during treat-ment in the per-protocol population confirmed the results of the primary analysis. Finally, the trial included a broad spectrum of patients with cancer who had received a wide array of cyto-toxic and biologic therapies, but the sample size limits our ability to make definitive conclusions about outcomes associated with individual tu-mor types.
In conclusion, in this trial involving patients with cancer-associated venous thromboembolism,
Figure 2. Kaplan–Meier Cumulative Event Rates for the Primary Outcome.
The primary outcome was a composite of recurrent venous thromboembolism or major bleeding. The inset shows the same data on an enlarged y axis.
Patie
nts
with
Rec
urre
nt V
enou
sTh
rom
boem
bolis
m o
r Maj
or B
leed
ing
(%)
100
80
90
70
60
40
30
10
50
20
00 30 60 90 120 150 180 210 240 270 300 330 360
Days
No. at RiskEdoxabanDalteparin
522524
472485
429449
388385
407420
360364
345352
161171
237241
270276
295313
310324
328340
Edoxaban
Dalteparin
20
15
5
10
00 30 60 90 120 150 180 210 240 270 300 330 360
The New England Journal of Medicine Downloaded from nejm.org by HANS GELDERBLOM on December 12, 2017. For personal use only. No other uses without permission.
Copyright © 2017 Massachusetts Medical Society. All rights reserved.
n engl j med nejm.org 7
Edoxaban for Cancer-Associated Venous Thromboembolism
with dalteparin (P = 0.02 for interaction in the safety population).
Adverse EventsThe adverse events reported in the trial are shown in Tables S9, S10, and S11 in the Supplementary Appendix. The most common adverse events were progression of neoplasm and pneumonia; for each of these events, the rate was similar in the two treatment groups.
Discussion
The Hokusai VTE Cancer trial, which involved patients with predominantly advanced cancer and acute symptomatic or incidental venous thrombo-embolism, showed that treatment with a fixed once-daily dose of oral edoxaban for up to 12 months was noninferior to treatment with sub-cutaneous dalteparin with respect to the com-posite outcome of recurrent venous thromboem-
OutcomeEdoxaban (N = 522)
Dalteparin (N = 524)
Hazard Ratio (95% CI) P Value
Primary outcome
Recurrent venous thromboembolism or major bleeding — no. (%) 67 (12.8) 71 (13.5) 0.97 (0.70–1.36) 0.006 for noninferiority;
0.87 for superiority
Secondary outcomes
Recurrent venous thromboembolism — no. (%) 41 (7.9) 59 (11.3) 0.71 (0.48–1.06) 0.09
Recurrent deep-vein thrombosis — no. (%) 19 (3.6) 35 (6.7) 0.56 (0.32–0.97)
Recurrent pulmonary embolism — no. (%)† 27 (5.2) 28 (5.3) 1.00 (0.59–1.69)
Major bleeding — no. (%) 36 (6.9) 21 (4.0) 1.77 (1.03–3.04) 0.04
Severity of major bleeding among those with major bleeding — no./total no. (%)‡
Category 1 0 0
Category 2 24/36 (66.7) 8/21 (38.1)
Category 3 12/36 (33.3) 12/21 (57.1)
Category 4 0 1/21 (4.8)
Clinically relevant nonmajor bleeding — no. (%)§ 76 (14.6) 58 (11.1) 1.38 (0.98–1.94)
Major or clinically relevant nonmajor bleeding — no. (%)§¶ 97 (18.6) 73 (13.9) 1.40 (1.03–1.89)
Death from any cause — no. (%) 206 (39.5) 192 (36.6) 1.12 (0.92–1.37)
Event-free survival — no. (%)∥ 287 (55.0) 296 (56.5) 0.93 (0.77–1.11)
* The overall trial period was the time from randomization through the end of 12 months or the end of the trial, regardless of the duration of treatment for each patient.
† No patient in either group had confirmed fatal pulmonary embolism. A total of six patients in the edoxaban group and four patients in the dalteparin group had unexplained death for which pulmonary embolism could not be ruled out as the cause.
‡ The severity of major bleeding at clinical presentation was adjudicated by an independent clinical events committee (whose members were unaware of the treatment assignments) according to the following prespecified categories: category 1 included bleeding events that were not considered to be a clinical emergency; category 2 included bleeding events that could not be classified in any of the other categories be-cause they led to some treatment but were not considered to be a clinical emergency; category 3 included bleeding events that were consid-ered to be a clinical emergency, such as bleeding with hemodynamic instability or intracranial bleeding with neurologic symptoms; and cate-gory 4 included bleeding events that led to death before or almost immediately after the patient entered the hospital.12
§ Clinically relevant nonmajor bleeding was defined as overt bleeding that did not meet the criteria for major bleeding but was associated with the use of medical intervention, contact with a physician, interruption of the assigned treatment, discomfort, or impairment of activities of daily living.
¶ For patients who had more than one event, only the first was counted.∥ Event-free survival was defined as the absence of recurrent venous thromboembolism, major bleeding, and death.
Table 2. Clinical Outcomes during the Overall Trial Period.*
The New England Journal of Medicine Downloaded from nejm.org by HANS GELDERBLOM on December 12, 2017. For personal use only. No other uses without permission.
Copyright © 2017 Massachusetts Medical Society. All rights reserved.
Raskob etal.NEJM2017

All Recurrent VTE Outcomes Edoxaban Dalteparin HR (95% CI)(N = 522) (N = 524)
Recurrent VTE 41(7.9%) 59 (11.3%) 0.71 (0.48, 1.06) P = 0.093
Recurrent DVT 19 (3.6%) 35 (6.7%) 0.56 (0.32, 0.97)
Recurrent PE 27 (5.2%) 28 (5.3%) 1.00 (0.59, 1.69)
Confirmed fatal 0 0
Unexplained death 6 (1.1%) 4 (0.8%) (PE not excluded)
Raskob etal.NEJM2017

Recurrent events
n engl j med nejm.org 9
Edoxaban for Cancer-Associated Venous Thromboembolism
edoxaban was noninferior to dalteparin with re-spect to the composite outcome of recurrent ve-nous thromboembolism or major bleeding.
Supported by Daiichi Sankyo.Disclosure forms provided by the authors are available with
the full text of this article at NEJM.org.
References1. Timp JF, Braekkan SK, Versteeg HH, Cannegieter SC. Epidemiology of cancer-associated venous thrombosis. Blood 2013; 122: 1712-23.2. Ay C, Pabinger I, Cohen AT. Cancer-
associated venous thromboembolism: burden, mechanisms, and management. Thromb Haemost 2017; 117: 219-30.3. Prandoni P, Lensing AWA, Piccioli A, et al. Recurrent venous thromboembo-
lism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood 2002; 100: 3484-8.4. Lee AY, Levine MN, Baker RI, et al.
Figure 3. Kaplan–Meier Cumulative Event Rates for Secondary Outcomes.
Shown are cumulative event rates for recurrent venous thromboembolism (Panel A) and major bleeding (Panel B). The insets show the same data on an enlarged y axis.
B
A
Patie
nts
with
Rec
urre
nt V
enou
sTh
rom
boem
bolis
m (%
)
100
80
90
70
60
40
30
10
50
20
00 30 60 90 120 150 180 210 240 270 300 330 360
Days
No. at RiskEdoxabanDalteparin
522524
480488
437452
395389
415423
370370
356358
168174
245246
281282
307321
320333
340348
Edoxaban
Dalteparin
20
15
5
10
00 30 60 90 120 150 180 210 240 270 300 330 360
Patie
nts
with
Maj
or B
leed
ing
(%)
100
80
90
70
60
40
30
10
50
20
00 30 60 90 120 150 180 210 240 270 300 330 360
Days
No. at RiskEdoxabanDalteparin
522524
484497
447466
404409
426436
375390
358378
168183
248262
282298
308335
323346
343356
Edoxaban
Dalteparin
20
15
5
10
00 30 60 90 120 150 180 210 240 270 300 330 360
The New England Journal of Medicine Downloaded from nejm.org by HANS GELDERBLOM on December 12, 2017. For personal use only. No other uses without permission.
Copyright © 2017 Massachusetts Medical Society. All rights reserved.
Raskob etal.NEJM2017

Bleeding Outcomes on Treatment
Edoxaban Dalteparin HR (95% CI)(N = 522) (N = 524)
Major 36 (6.9%) 21 (4.0%) 177 (1.03, 3.04) P = 0.04
CRNM 76 (14.6%) 58 (11.1%) 1.38 (0.98, 1.94)
Major or CRNM 97 (18.6%) 73 (13.9%) 1.40 (1.03, 1.89)
Death from any cause 206 (39.5%) 192 (36.6) 1.12 (0.92, 1.37)
Raskob etal.NEJM2017

Table S4. Types of Outcomes Contributing to the Primary Outcome
Clinical Outcomes Edoxaban (N=522)
Dalteparin (N=524)
Primary outcome: first recurrent VTE or major
bleeding – no. (%)
67 (12.8) 71 (13.5)
Recurrent VTE – no. (%) 34 (6.5) 54 (10.3)
Fatal PE 0 0
Death, with PE not ruled out 3 (0.6) 3 (0.6)
Nonfatal PE with or without DVT 18 (3.4) 21 (4.0)
DVT only 13 (2.5) 30 (5.7)
Symptomatic nonfatal VTE 22 (4.2) 40 (7.6)
Incidental nonfatal VTE 9 (1.7) 11 (2.1)
Major bleeding – no. (%) 33 (6.3) 17 (3.2)
Fatal† 0 2 (0.4)
Intracranial 2 (0.4) 4 (0.8)†
Gastrointestinal 20 (3.8) 6 (1.1)
Upper 17 (3.3) 3 (0.6)
Lower 3 (0.6) 3 (0.6)†
Urogenital 5 (1.0) 0
22
Raskob etal.NEJM2017

Bleeding events
n engl j med nejm.org 9
Edoxaban for Cancer-Associated Venous Thromboembolism
edoxaban was noninferior to dalteparin with re-spect to the composite outcome of recurrent ve-nous thromboembolism or major bleeding.
Supported by Daiichi Sankyo.Disclosure forms provided by the authors are available with
the full text of this article at NEJM.org.
References1. Timp JF, Braekkan SK, Versteeg HH, Cannegieter SC. Epidemiology of cancer-associated venous thrombosis. Blood 2013; 122: 1712-23.2. Ay C, Pabinger I, Cohen AT. Cancer-
associated venous thromboembolism: burden, mechanisms, and management. Thromb Haemost 2017; 117: 219-30.3. Prandoni P, Lensing AWA, Piccioli A, et al. Recurrent venous thromboembo-
lism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood 2002; 100: 3484-8.4. Lee AY, Levine MN, Baker RI, et al.
Figure 3. Kaplan–Meier Cumulative Event Rates for Secondary Outcomes.
Shown are cumulative event rates for recurrent venous thromboembolism (Panel A) and major bleeding (Panel B). The insets show the same data on an enlarged y axis.
B
A
Patie
nts
with
Rec
urre
nt V
enou
sTh
rom
boem
bolis
m (%
)
100
80
90
70
60
40
30
10
50
20
00 30 60 90 120 150 180 210 240 270 300 330 360
Days
No. at RiskEdoxabanDalteparin
522524
480488
437452
395389
415423
370370
356358
168174
245246
281282
307321
320333
340348
Edoxaban
Dalteparin
20
15
5
10
00 30 60 90 120 150 180 210 240 270 300 330 360
Patie
nts
with
Maj
or B
leed
ing
(%)
100
80
90
70
60
40
30
10
50
20
00 30 60 90 120 150 180 210 240 270 300 330 360
Days
No. at RiskEdoxabanDalteparin
522524
484497
447466
404409
426436
375390
358378
168183
248262
282298
308335
323346
343356
Edoxaban
Dalteparin
20
15
5
10
00 30 60 90 120 150 180 210 240 270 300 330 360
The New England Journal of Medicine Downloaded from nejm.org by HANS GELDERBLOM on December 12, 2017. For personal use only. No other uses without permission.
Copyright © 2017 Massachusetts Medical Society. All rights reserved.
Raskob etal.NEJM2017

Study design (1) Prospective, randomised, open-label, multicentre pilot phase III
Rivaroxaban
Study population: Active cancer with symptomatic DVT
and/or any PE ECOG PS < 2
Dalteparin
R
6 months
n=530
Stratification variables: Stage of disease Baseline platelet count Type of VTE Risk of clotting by tumour type
15 mg bid for 21 days followed by 20 mg od
200 IU/kg od for the first 30 days followed by 150 IU/kg od
Investigator-initiated academic trial
TMG Jaclyn Brown Oliver Chapman Janet Dunn Andrew Entwistle Karen French Danielle Hale Catherine Hill Richard Hobbs Mojid Khan Anand Lokare Mandy Maredza
Andrea Marshall Martin Scott-Brown Deb Smith Jenny Thirlwall Veronica Wilkie Annie Young Advisors Ajay Kakkar Peter Rose
TSC Jeremy Dale Charles Hutchinson Mark Levine (Chair) Gary Lyman Peter MacCallum Irene Singleton DMC Ganesh Radhakrishna Lisa Robinson Keith Wheatley (Chair)
Thank you to all the patients who participated in select-d
YoungAetal.Presented at:ASH2017;Abstract 625

Trial progress
• First patient randomised in October 2013 • Changes to protocol based on DMC recommendations in June 2016
� The second randomisation was closed to patients randomised into the trial after 31st August 2016 due to low recruitment (n=92)
� Sample size reduced from 530 to 400 patients (increased the width of the 95% CI for VTE recurrence rate from 8% to 9%)
� Patients with oesophageal and gastro-oesophageal cancer were excluded due to apparent imbalance in major bleeding rates compared to other tumour types
� Final bleeding adjudication committee, 24th November 2017
TMG Jaclyn Brown Oliver Chapman Janet Dunn Andrew Entwistle Karen French Danielle Hale Catherine Hill Richard Hobbs Mojid Khan Anand Lokare Mandy Maredza
Andrea Marshall Martin Scott-Brown Deb Smith Jenny Thirlwall Veronica Wilkie Annie Young Advisors Ajay Kakkar Peter Rose
TSC Jeremy Dale Charles Hutchinson Mark Levine (Chair) Gary Lyman Peter MacCallum Irene Singleton DMC Ganesh Radhakrishna Lisa Robinson Keith Wheatley (Chair)
Thank you to all the patients who participated in select-d

VTE recurrence Dalteparin
(n=203) Rivaroxaban
(n=203) VTE recurrences within 6 months, n
DVT or PE Other location
18 16 2
8 6 2
6-month VTE recurrence rate, % (95% CI) 6-month lower limb DVT or PE recurrence rate
11% (7–16%) 9% (6-15%)
4% (2–9%) 3% (1-7%)
0
5
10
15
20
25
30
35
40
0 1 2 3 4 5 6
Perc
enta
ge o
f VTE
recu
rren
ces
Months from trial entry
Dalteparin
Rivaroxaban
Numbers at Risk:Dalteparin 203 169 129 106Rivaroxaban 203 170 143 123
0
5
10
15
20
25
30
35
40
0 1 2 3 4 5 6
Perc
enta
ge o
f VTE
recu
rren
ces
Months from trial entryNumbers at Risk:Dalteparin 203 171 139 115Rivaroxaban 203 174 149 134

Bleeding - number of patients (%)
Category Dalteparin (n=203)
Rivaroxaban (n=203)
Major* 6 (3%) 11 (5%) Clinically relevant non-major 6 (3%) 25 (12%) Total 12 (6%) 36 (17%)
*1 fatal bleeding event in each arm Most major bleeding events were gastrointestinal bleeding; no CNS bleeds Most CRNMBs were gastrointestinal or urological

Combined analysis:Hokusai &Select-D
| 5WANG et Al.
and the CANVAS study, (NCT02744092) comparing DOAC class
with LMWH class. Additional information (such as risk factors for
bleeding) will undoubtedly emerge from these trials, along with
those already published, that will help clinicians further optimize
the risk–benefit tradeoffs of DOACs for cancer patients. For ex-
ample, risk–benefit trade- off discussion is particularly needed in
patients with gastrointestinal malignancies, given the increased
risk of bleeding seen in this subgroup.
F IGURE 1 (A) Risk of recurrent venous thromboembolism in 6 months in randomized controlled trials of LMWH vs VKA (random effect
model). (B) Risk of major bleeding in 6 months in randomized controlled trials of LMWH vs VKA (random effect model). CI, confidence
interval; LMWH, low- molecular- weight heparin; M-H, Mantel-Haenszel; VKA, vitamin K antagonists
Study or subgroup
CANTHANOXCLOTMAIN-LITEONCENOXCATCH
Total (95% CI)Total events
CANTHANOXCLOTMAIN-LITEONCENOXCATCH
Total (95% CI)Total events
70
49
114
3146
272
449
1017
61100336
71
45
43
31053
3
451
992
30100336
75
42.4%
100.0%
4.0%8.6%
42.4%2.6%
0.69 [0.45, 1.07] 2015
0.60 [0.45, 0.80]
1025 995 100.0% 1.07 [0.65, 1.75]
0.66 [0.16, 2.74] 20060.60 [0.23, 1.59] 20060.51 [0.33, 0.79] 20030.70 [0.12, 4.09] 2002
1267
195
44967
100338
71
1117
1212
45134
100335
75
25.9%5.3%
18.6%31.0%19.2%
1.10 [0.49, 2.46] 20153.04 [0.38, 24.28] 2006
1.00 [0.36, 2.75] 20061.57 [0.77, 3.18] 20030.44 [0.16, 1.19] 2002
Heterogeneity: τ2 = 0.00; χ2 = 0.99, df = 4 (P = .91); I2 = 0%Test for overall effect: Z = 3.52 (P = .000)
Heterogeneity: τ2 = 0.07; χ2 = 5.20, df = 4 (P = .27); I2 = 23%Test for overall effect: Z = 0.26 (P = .80)
LMWHEvents Total Events Total Weight M-H, Random, 95% CI Year M-H, Random, 95% CI
0.01 0.1 1 10Favours LMWH Favours VKA
100
0.01 0.1 1 10Favours LMWH Favours VKA
100
VKA Risk ratio
Study or subgroupLMWH
Events Total Events Total Weight M-H, Random, 95% CI YearVKA Risk Ratio
Risk ratio
M-H, Random, 95% CIRisk Ratio
(A)
(B)
F IGURE 2 (A) Risk of recurrent VTE in 6 months in randomized controlled trials of DOAC vs LMWH (random effect model).48
(B) Risk
of major bleeding in 6 months in randomized controlled trials of DOAC vs LMWH (random effect model).48
CI, confidence interval; DOAC,
direct oral anticoagulants; LMWH, low- molecular- weight heparin; M-H, Mantel-Haenszel; VTE, venous thromboembolism
Study or subgroupDOAC
Events Total Events Total Weight M-H, Random, 95% CI M-H, Random, 95% CILMWH Risk ratio Risk ratio
Study or subgroupDOAC
Events Total Events Total Weight M-H, Random, 95% CI Year M-H, Random, 95% CILMWH Risk ratio Risk ratio
0.01 0.1 1 10Favours DOAC Favours LMWH
100
0.01 0.1 1 10Favours DOAC Favours LMWH
100
Heterogeneity: τ2 = 0.02; χ2 = 1.21, df = 1 (P = .27); I2 = 17%Test for overall effect: Z = 1.92 (P = .06)
Total (95% CI)
Select-D 2017Hokusai VTE cancer 2017
Total events
Heterogeneity: τ2 = 0.00; χ2 = 0.01, df = 1 (P = .91); I2 = 0%Test for overall effect: Z = 2.17 (P = .03)
Total (95% CI)
Select-D 2017Hokusai VTE cancer 2017
Total events
34 522 46 524 73.4% 0.74 [0.48, 1.14]8 203
725
18
42 64
40 23
203
727
26.6%
100.0%
0.44 [0.20, 1.00]
29 522 17 524 73.5% 1.71 [0.95, 3.08] 201711 203 6 203 26.5% 1.83 [0.69, 4.86] 2017
0.65 [0.42, 1.01]
725 727 100.0% 1.74 [1.05, 2.88]
(A)
(B)
WanT etal.Res Pract Thromb Haemost.2018

DOACs:InteractionsDrug interactions may beclinically relevant?
short course of low-dose LMWH is effective and safe in treatingcatheter-related thrombosis in patients with severe thrombocytopenia.75
To date, published data and clinical experience suggest thatcatheter-related thrombosis is associated with a low risk forthrombosis recurrence and postthrombotic syndrome.76,77 There-fore, conservative treatment is recommended. A sensible approachis to remove the catheter only if (1) central venous access is nolonger required; (2) the device is nonfunctional or defective; or (3)line-related sepsis is suspected or documented. Unless contraindicated,therapeutic anticoagulation should be given using either LMWHalone or LMWH followed by warfarin therapy. A short period ofanticoagulation (3-5 days of LMWH) may even salvage somethrombosed catheters and obviate the need to remove and replacethe line. Anticoagulation is recommended for a minimum of 3 monthsand while the catheter remains in place.
Treatment of splanchnic vein thrombosis inpatients with cancer
Splanchnic vein thromboses, involving the portal, splenic, mesen-teric, or hepatic veins, are uncommon in the general population, butsignificant rates have been reported in patients with intraabdominalmalignancies.78 In a retrospective single-institution study of 135consecutive patients with pancreatic adenocarcinoma, incidentalsplanchnic vein thrombosis was present in 23%.60
Management of splanchnic vein thrombosis has not been wellstudied. Limited experience is available from studies that includedboth patients with and without cancer. In a retrospective cohort of832 patients with splanchnic vein thrombosis, of which 27% hadunderlying cancer, warfarin therapy and gastrointestinal tract variceswere independent predictors of bleeding.79 Furthermore, VTErecurrence was not reduced after anticoagulant therapy. An inter-national registry of 613 patients with splanchnic vein thrombosisreported that most patients are treated with anticoagulation and thatthe risk of major bleeding is low.80 Whether such results apply tocancer-related splanchnic vein thrombosis is not known.
In patients with acute, symptomatic splanchnic vein thrombosiswithout contraindications to anticoagulation, guidelines recommend
the use of anticoagulant therapy.21 For patients with incidentallydetected splanchnic vein thrombosis, there is no specific guidanceon treatment. It is reasonable to withhold anticoagulation if the patientis truly asymptomatic, especially if radiologic evidence indicates thatthe thrombus is chronic in nature. Repeated imaging is prudent todetect thrombus progression if anticoagulation is not given.
Use of NOACs in cancer-associatedthrombosis
The development of NOACs that directly inhibit factor Xa orthrombin is a milestone achievement in the prevention and treatmentof VTE. These agents are more attractive to patients and cliniciansbecause they are taken by mouth in fixed doses once or twice daily,have few drug and food interactions, and do not require laboratorymonitoring. Dabigatran, a direct thrombin inhibitor, and rivarox-aban and apixaban, 2 direct factor Xa inhibitors, are the forerunnersin this class of agents. These drugs have been shown to be effectivein VTE prophylaxis after major hip and knee arthroplasty and instroke prevention in patients with nonvalvular atrial fibrillation.81
They are also noninferior to warfarin for the prevention of recurrentVTE without an increased risk of bleeding, and rivaroxaban hasreceived regulatory approval as monotherapy in the treatment ofDVT.82-87 All 3 agents are effective and safe for long-termsecondary VTE prophylaxis in patients who have already received6 to 12 months of anticoagulation.82,85,87 Unfortunately, very smallnumbers of patients with cancer were included in these trials, andthe results of this patient subgroup have not been published. A smallphase 2 study evaluating the safety and tolerability of apixabanfound a low risk of major bleeding (2.2%) during 12 weeks oftherapy in 125 patients with metastatic or advanced cancer withoutthrombosis.88 No studies have specifically addressed the treatmentof cancer-associated VTE using these direct inhibitors.
Despite the undeniable practical advantages of these agents vsVKA and LMWH therapy for the prevention and treatment of cancer-associated thrombosis, important and clinically relevant concernsprevail regarding the extrapolation of published results to the cancerpopulation. These include the small number of highly selectedpatients with cancer (approximately 5%) enrolled in each studyand the use of warfarin or placebo rather than LMWH in the controlgroup. In addition, although these anticoagulants have fewer druginteractions than VKAs, interactions do exist with some chemo-therapeutic agents (Table 2). Whether these interactions are clinicallysignificant is not known. Finally, gastrointestinal tract problems inpatients with cancer can potentially alter drug delivery and absorption,and higher rates of gastrointestinal tract bleeding have been reportedwith dabigatran compared with warfarin.81 These shortcomings arecompounded by the lack of reversal agents to rapidly normalizehemostasis and the lack of widely available laboratory assays tomeasure the anticoagulant activity. Clinicians need to discuss theselimitations to fully inform their patients with cancer and know thatthe current ASCO Guideline does not recommend the use of thesenew agents.14 Clinical trials are strongly encouraged to address thisand the many other unmet clinical needs in patients with cancer-associated thrombosis.
Authorship
Contribution: A.Y.Y.L. and E.A.P. wrote the manuscript.
Table 2. Interactions between chemotherapeutic agents andimmunosuppressants with NOACs based on known metabolicpathway activity
Dabigatran Rivaroxaban Apixaban
Interactioneffect* P-glycoprotein
P-glycoproteinCYP3A4
P-glycoproteinCYP3A4
Increases NOAC
plasma levels†
Cyclosporine Cyclosporine Cyclosporine
Tacrolimus Tacrolimus Tacrolimus
Tamoxifen Tamoxifen Tamoxifen
Lapatinib Lapatinib Lapatinib
Nilotinib Nilotinib Nilotinib
Sunitinib Sunitinib Sunitinib
Imatinib Imatinib
Reduces NOAC
plasma levels‡
Dexamethasone Dexamethasone Dexamethasone
Doxorubicin Doxorubicin Doxorubicin
Vinblastine Vinblastine Vinblastine
CYP3A4, cytochrome P450 3A4.*Clinicians should consult with the pharmacist to determine if these and other
drug interactions exist when NOACs are being considered.
†Drugs that inhibit P-glycoprotein transport or CYP3A4 pathway can increaseNOAC levels.
‡Drugs that induce P-glycoprotein transport or CYP3A4 pathway can lowerNOAC levels.
BLOOD, 3 OCTOBER 2013 x VOLUME 122, NUMBER 14 TREATMENT OF CANCER-ASSOCIATED THROMBOSIS 2315
LeeetalBlood.2013;122(14):2310- 2317 33

My thoughts:DOACs aregood news for cancer patients…
However maybe not the right drug for all cancer patients…
• High-riskbleeding– Thrombocytopenia– Mucosainvolvementorprimarytumor inplace(GIorGUnotresected)– Concomitanttreatmentwithantiangiogenics(antiangiogenictherapyincreasetheriskofbleeding:bevacizumab,aflibercept,etc.)
– Tumor invadinggreatvessels(lungcancerandvenacava/aorta/pulmonaryartery…)• Concomitanttreatmentwithotherdrugs(interactions)• Impairedoralintake:obstructivetumors,nauseas&vomiting,etc.• Malabsorption:extensiveGIresection(cytoreductive surgery),etc.• Liverimpairment:extensivelivermets,etc.

Conclusions
• NewRAMandnewmolecularriskfactorusedinclinicalpracticemaychangethelandscapeofprimarythromboprophylaxis
• LMWHisthestandardofcareforinitialandlong-termanticoagulationincancerpatients
• Directoralanticoagulants(DOACs)areanotheroptionforthetreatmentofcancer-associatedthrombosis

TESEORegistry
• VTE&CancerRegistry
• Cancer&ThrombosisWorkingGroup,SpanishSocietyofMedicalOncology(SEOM)
• Start:May2018,Spain43startingcenters
• Internationalregistry

CancerPatients-Thromboprophylaxis2018Recommendations?
Surgery forcancer(Grade1A)
CancerPatientsClinical setting
Hospitalization forAcutemedical illness
Chemotherapy inhighrisk ambulatory
cancerpatientsandlow bleeding risk
37

CONKO-004
CI=confidenceinterval;HR=hazardratio;PFS=progression-freesurvival;OS=overallsurvival. Pelzer U,etal.JClinOncol 2015;33:2028–2034.
To compensate for the inflation of the error level caused by an interme-diate evaluation of the primary aim, the approximated alpha and/or betaspending functions according to Pocock30 were used. Because of the presenceof competing risks, analyses of the symptomatic VTEs and major hemorrhagerates were performed using the Gray test.31,32 The Gray test compares theweighted averages of the hazards of the cumulative incidence rate (CIR).Comparisons between cumulative incidence curves at fixed points were con-structed, along with the SEs of these estimates.33
The formal !2 test was used to compare nominal counts; the Fisher’sexact test was used as appropriate. Median PFS and median OS were estimatedaccording to Kaplan-Meier methods, providing medians with 95% CIs. Com-parisons between the groups were performed using the two-sided log-ranktest, with a significance level of .05. HRs with 95% CIs were estimated with theCox regression model. Statistical analyses were performed using R (version3.01) with software package CMPRSK (http://www.r-project.org) and SPSSsoftware (version 19.0; SPSS, Chicago, IL).
RESULTS
A total of 312 patients were enrolled between April 2004 and January2009. The planned interim analysis (12 patients with symptomaticVTEs; 115 recruited patients) was conducted in May 2006. Consistentwith the protocol, the null hypothesis was maintained, and randomassignment continued (!2 P ! .235; standardized test statistic,"1.183). With respect to safety aspects, no difference was observed inmajor bleeding events between the two groups (!2 P ! .975).
One of the statistical end points (24 cases of symptomatic VTEsconfirmed by ERB) was reached in January 2009, when 312 patientsfrom 33 centers had been enrolled. An additional eight symptom-atic VTEs were identified during follow-up. All patients could beincluded in the intention-to-treat analysis (Fig 2). Quality-of-lifedata were not analyzed. There was no interaction between antico-agulation (based on random assignment) and chemotherapy as-signment (based on performance status and renal function; P !.884). Random assignment was satisfactory, and patient character-istics were well balanced (Table 1).
A total of 32 symptomatic VTEs were finally assessed by the ERB.The symptomatic VTE occurrences within the first 3 months were asfollows: 15 of 152 patients in the observation group and two of 160patients in the enoxaparin group (HR, 0.12; 95% CI, 0.03 to 0.52; !2 P! .001). The numbers of major bleeding events were as follows: five of152 patients in the observation arm and seven of 160 patients in theenoxaparin arm (HR, 1.4; 95% CI, 0.35 to 3.72; !2 P ! 1.0).
The estimated CIR of symptomatic VTEs within the first 3months was 10.2% in the observation arm and 1.3% in the enoxaparinarm (P ! .001); 12 patients required treatment to prevent a symptom-atic VTE (95% CI, 7 to 28). The estimated CIR of major bleeds withinthe first 3 months was 3.4% in the observation arm and 4.5% in theenoxaparin arm (P ! .641).
The overall CIR of symptomatic VTEs was 15.1% in the observa-tion arm and 6.4% in the enoxaparin arm (HR, 0.40; 95% CI, 0.19 to0.83; P ! .01). The overall CIR of major bleeds was 6.9% in theobservation arm and 8.3% in the enoxaparin arm (HR, 1.23; 95% CI,0.54 to 2.79; P ! .63; Fig 3). The nominal counts and origins of thesymptomatic VTEs and major bleeds are listed in Table 2. Patientswith major bleeds ceased enoxaparin treatment, whereas patients withsymptomatic VTEs were further treated with a therapeutic dose. Threelethal bleeding events occurred. Two (observation arm) were caused byconfirmed fulminant cancer ulceration of the duodenum; one (enoxa-parinarm)wastheresultof fatalesophagealvaricosebleeding.Twomajorbleeding events (enoxaparin arm) occurred after LMWH treatment hadalready been ceased for at least 7 days: in one patient because ofchemotherapy-induced thrombocytopenia, and in the other patient be-cause of local cutaneous irritations after subcutaneous injection of enoxa-parin. The incidence of all other adverse events and hospitalizations wassimilar in both groups. No patient experienced heparin-induced throm-bocytopenia. The therapeutics used produced no novel adverse effectsother than those described in the Summary of Product Characteristics.
Median PFS was 5.42 months (95% CI, 4.21 to 5.78 months) inthe observation arm and 4.99 months (95% CI, 3.71 to 5.52 months)
BA
0
Cum
ulat
ive
Inci
denc
eRa
te (%
)
Time (months)
20
15
10
5
3 6 9 12 18
Gray P = .01
HR, 0.40; 95% CI, 0.19 to 0.83Competing risk regression
EnoxaparinObservation
0
Cum
ulat
ive
Inci
denc
eRa
te (%
)
Time (months)
20
15
10
5
3 6 9 12 18
Gray P = .63
HR, 1.23; 95% CI, 0.54 to 2.79Competing risk regression
EnoxaparinObservation
No. at riskEnoxaparin 160 102 55 26 12 4Observation 152 87 47 27 14 5
Incidence rate, %Enoxaparin 0 1.3 3.8 5.1 5.7 6.4Observation 0 10.2 14.4 14.4 15.1 15.1
No. at riskEnoxaparin 160 99 52 26 14 5Observation 152 94 52 26 13 4
Incidence rate, %Enoxaparin 0 4.5 7.6 7.6 8.3 8.3Observation 0 3.4 5.5 5.5 6.9 6.9
Fig 3. Cumulative incidence curve and rates of (A) symptomatic venous thromboembolic events and (B) bleeding events. HR, hazard ratio.
Pelzer et al
4 © 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Information downloaded from jco.ascopubs.org and provided by at sanofi-aventis on May 21, 2015 from 193.202.91.11Copyright © 2015 American Society of Clinical Oncology. All rights reserved.
PFS: HR 1.06; 95% CI, 0.84 to 1.32; p=0.64OS: HR 1.01; 95% CI, 0.87 to 1.38; p=0.44
To compensate for the inflation of the error level caused by an interme-diate evaluation of the primary aim, the approximated alpha and/or betaspending functions according to Pocock30 were used. Because of the presenceof competing risks, analyses of the symptomatic VTEs and major hemorrhagerates were performed using the Gray test.31,32 The Gray test compares theweighted averages of the hazards of the cumulative incidence rate (CIR).Comparisons between cumulative incidence curves at fixed points were con-structed, along with the SEs of these estimates.33
The formal !2 test was used to compare nominal counts; the Fisher’sexact test was used as appropriate. Median PFS and median OS were estimatedaccording to Kaplan-Meier methods, providing medians with 95% CIs. Com-parisons between the groups were performed using the two-sided log-ranktest, with a significance level of .05. HRs with 95% CIs were estimated with theCox regression model. Statistical analyses were performed using R (version3.01) with software package CMPRSK (http://www.r-project.org) and SPSSsoftware (version 19.0; SPSS, Chicago, IL).
RESULTS
A total of 312 patients were enrolled between April 2004 and January2009. The planned interim analysis (12 patients with symptomaticVTEs; 115 recruited patients) was conducted in May 2006. Consistentwith the protocol, the null hypothesis was maintained, and randomassignment continued (!2 P ! .235; standardized test statistic,"1.183). With respect to safety aspects, no difference was observed inmajor bleeding events between the two groups (!2 P ! .975).
One of the statistical end points (24 cases of symptomatic VTEsconfirmed by ERB) was reached in January 2009, when 312 patientsfrom 33 centers had been enrolled. An additional eight symptom-atic VTEs were identified during follow-up. All patients could beincluded in the intention-to-treat analysis (Fig 2). Quality-of-lifedata were not analyzed. There was no interaction between antico-agulation (based on random assignment) and chemotherapy as-signment (based on performance status and renal function; P !.884). Random assignment was satisfactory, and patient character-istics were well balanced (Table 1).
A total of 32 symptomatic VTEs were finally assessed by the ERB.The symptomatic VTE occurrences within the first 3 months were asfollows: 15 of 152 patients in the observation group and two of 160patients in the enoxaparin group (HR, 0.12; 95% CI, 0.03 to 0.52; !2 P! .001). The numbers of major bleeding events were as follows: five of152 patients in the observation arm and seven of 160 patients in theenoxaparin arm (HR, 1.4; 95% CI, 0.35 to 3.72; !2 P ! 1.0).
The estimated CIR of symptomatic VTEs within the first 3months was 10.2% in the observation arm and 1.3% in the enoxaparinarm (P ! .001); 12 patients required treatment to prevent a symptom-atic VTE (95% CI, 7 to 28). The estimated CIR of major bleeds withinthe first 3 months was 3.4% in the observation arm and 4.5% in theenoxaparin arm (P ! .641).
The overall CIR of symptomatic VTEs was 15.1% in the observa-tion arm and 6.4% in the enoxaparin arm (HR, 0.40; 95% CI, 0.19 to0.83; P ! .01). The overall CIR of major bleeds was 6.9% in theobservation arm and 8.3% in the enoxaparin arm (HR, 1.23; 95% CI,0.54 to 2.79; P ! .63; Fig 3). The nominal counts and origins of thesymptomatic VTEs and major bleeds are listed in Table 2. Patientswith major bleeds ceased enoxaparin treatment, whereas patients withsymptomatic VTEs were further treated with a therapeutic dose. Threelethal bleeding events occurred. Two (observation arm) were caused byconfirmed fulminant cancer ulceration of the duodenum; one (enoxa-parinarm)wastheresultof fatalesophagealvaricosebleeding.Twomajorbleeding events (enoxaparin arm) occurred after LMWH treatment hadalready been ceased for at least 7 days: in one patient because ofchemotherapy-induced thrombocytopenia, and in the other patient be-cause of local cutaneous irritations after subcutaneous injection of enoxa-parin. The incidence of all other adverse events and hospitalizations wassimilar in both groups. No patient experienced heparin-induced throm-bocytopenia. The therapeutics used produced no novel adverse effectsother than those described in the Summary of Product Characteristics.
Median PFS was 5.42 months (95% CI, 4.21 to 5.78 months) inthe observation arm and 4.99 months (95% CI, 3.71 to 5.52 months)
BA
0
Cum
ulat
ive
Inci
denc
eRa
te (%
)
Time (months)
20
15
10
5
3 6 9 12 18
Gray P = .01
HR, 0.40; 95% CI, 0.19 to 0.83Competing risk regression
EnoxaparinObservation
0
Cum
ulat
ive
Inci
denc
eRa
te (%
)
Time (months)
20
15
10
5
3 6 9 12 18
Gray P = .63
HR, 1.23; 95% CI, 0.54 to 2.79Competing risk regression
EnoxaparinObservation
No. at riskEnoxaparin 160 102 55 26 12 4Observation 152 87 47 27 14 5
Incidence rate, %Enoxaparin 0 1.3 3.8 5.1 5.7 6.4Observation 0 10.2 14.4 14.4 15.1 15.1
No. at riskEnoxaparin 160 99 52 26 14 5Observation 152 94 52 26 13 4
Incidence rate, %Enoxaparin 0 4.5 7.6 7.6 8.3 8.3Observation 0 3.4 5.5 5.5 6.9 6.9
Fig 3. Cumulative incidence curve and rates of (A) symptomatic venous thromboembolic events and (B) bleeding events. HR, hazard ratio.
Pelzer et al
4 © 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Information downloaded from jco.ascopubs.org and provided by at sanofi-aventis on May 21, 2015 from 193.202.91.11Copyright © 2015 American Society of Clinical Oncology. All rights reserved.
Symptomatic VTE events Bleeding events
38
Patients with histologically proven APC were randomly assigned to ambulant first-line chemotherapy and prophylactic use of enoxaparin or chemotherapy alone to investigate the probable reduction in symptomatic VTEs and the impact on survival.

Meta-Analysis(IndividualParticipantData)
• 13(of18identified)randomizedtrialswereanalyzedtoevaluatetheimpactofprophylacticuseofheparinincancerpatients
• GreatestbenefitfromLMWHthromboprophylaxis:– lungcancer:OR=0.52(95%CI:0.39,0.68;P<0.001)and– pancreaticcancer:OR=0.55(95%CI:0.35,0.88;P=0.01)
• Doesa50%reductioninsymptomaticVTEisrelevantforcancerpatientswithoutasignificantincreaseinbleeding?
CI,confidenceinterval;LMWH,lowmolecularweightheparin;OR,oddsratioSchünemann Hetal.Blood.2017;130:626.

NICE2018:Cancer-AssociatedThrombosisUpdate
ICPguidance(2013)andnowNICE(2018)recommendconsiderationofLMWHthromboprophylaxis inaPDAC asadiscreetclinicalentity

CancerPatients-Thromboprophylaxis2018Recommendations?
Surgery forcancer(Grade1A)
CancerPatientsClinical setting
Hospitalization forAcutemedical illness
Chemotherapy inhighrisk ambulatory
cancerpatientsandlow bleeding risk
PROTECHTCONKO-004FRAGEM
SAVEONCOAkl 2012
DiNisio 2014Ben-Aharon 2014
Risk Assessment Models
41