Embed Size (px)
Citation preview

RECONSTRUCTIVE
Triple Z Flap Technique for Reconstruction ofTriangular Defects in Problem Areas
Cenk Sen, M.D.Tonguc Isken, M.D.
Hakan Agir, M.D.Cigdem Unal, M.D.
Bahadır Ozkeskin, M.D.Deniz Iscen, M.D.
Kocaeli, Turkey
Background: Reconstruction of defects close to important structures wherestandard flaps cannot easily be used may sometimes challenge surgeons. Classicreconstructive options for such defects close to problem areas may not alwaysyield the best result.Methods: The authors used the triple Z flap technique for triangular defects closeto problem areas in 18 patients. The defects were triangular or close to triangularin shape, and three Z flaps were planned on each side of the defect. Flaps weretransposed and the defects were reconstructed without any complications.Results: The results were quite satisfying for both the patient and the surgeon.Neither retraction nor any distortion was observed.Conclusion: The triple Z flap technique can be used in selected cases where localflap choices are scarce and it is difficult to achieve good anatomical and aestheticresults. (Plast. Reconstr. Surg. 119: 880, 2007.)
Repair of defects for which standard flapscannot be planned or when alternative re-construction methods are limited because
of proximity to important structures presents achallenge for plastic surgeons. A good functionaland aesthetic result is hard to achieve using asingle large flap for reconstruction of defectswith critical locations.
For triangular defects where reconstruction isdifficult, we designed a triple Z flap technique.Although it exactly fits triangular defects, trian-gular shape is not a requirement and the flapcan be used for defects close to triangular inshape. The technique is easy to learn and exe-cute. It reduces the risk of donor-site morbiditybecause small flaps are elevated and trans-posed instead of a single larger flap. It reducesthe eventual scar because it breaks the inci-sions into several smaller components. It alsodistributes the tissue borrowing all around thedefect, which helps in preventing retractionsand distortions.
PATIENTS AND METHODSEighteen patients were operated on with the
triple Z flap technique between June of 2002and December of 2004 (Table 1). Thirteen ofthe cases were malignant skin lesions mostly lo-calized to the head and neck region. Four caseswere operated on for benign skin lesions andone for a traumatic defect. The ages of the pa-tients ranged between 41 and 92 years (average,58 years). Fourteen of the patients were menand four were women. Most of the lesions wereclose to important structures, where limited re-constructive options were present. The tech-nique was planned to achieve the best resultsboth functionally and cosmetically.
For triangular defects where reconstruction isdifficult, we used the triple Z flap technique. Afterexcision of the lesion triangular in shape or closeto triangular, we designed three standard Z flapson each side of the defect. The bases and the limbsof the Z flaps, the lengths of which change de-pending on the length of a side of the triangle, arehalf as long as the sides of the triangular defect.The bases of the Z flaps do not come into contactwith each other on each side of the triangulardefect (Fig. 1, above). After excising the lesion, thethree planned Z flaps were elevated onto the sub-cutaneous plane and rotated toward the center ofthe defect, and the other limbs of the Z flaps closethe donor areas (Fig. 1, below). To make the trans-position of the Z flaps easier, a minor undermin-ing is recommended, extending outside the limitsof the incisions. This undermining is not extensiveand depends on the size of the defect.
From the Department of Plastic and Reconstructive Surgery,Kocaeli University Medical Faculty.Received for publication May 3, 2005; accepted August 2,2005.Presented at the 24th Annual National Meeting of the Turk-ish Plastic, Reconstructive, and Aesthetic Surgery Society, inAnkara, Turkey, October 18 through 20, 2002; and the 10thCongress of the European Societies of Plastic, Reconstructive,and Aesthetic Surgery, in Vienna, Austria, August 30through September 3, 2005.Copyright ©2007 by the American Society of Plastic Surgeons
DOI: 10.1097/01.prs.0000252011.43748.e9
www.PRSJournal.com880
The size of the Z flaps changes according tothe size of the triangular defect, and one limb ofthe Z is half of the side of a triangle. The largestof the defects among these patients was a trian-gle with 4.5-cm sides located on the buccal areaclose to the zygoma, which was reconstructedsuccessfully. Dog-ears were seen in reconstruc-tions if the defect was not exactly triangular inshape. As the shape of the defect approachescircular, the dog-ears increase. However, be-cause this technique is planned for reconstruc-tion of triangular defects, the incidence of dog-ears is very low.
RESULTSThe average follow-up period was 17 months,
ranging from 5 to 35 months. No flap loss was ob-served, but there was a slight congestion in one flap
of the three in the first case that resolved in 1 day,and no necrosis or suture detachment was seen.Because the length-to-width ratio is small, no dete-rioration of circulation was observed in any flap. Theonly early complication was minor infection in twocases and suture detachment in one case, all of whichhealed spontaneously. All malignant lesions wereexcised free of margin, and only one required re-excision because the tumor was very close to onemargin. None of the patients complained of scartissue. We did not observe any hypertrophic scar. Wealso did not encounter the dog-ear problem becauseall defects were close to triangular; in fact, if they everoccur, dog-ears regress spontaneously within a shorttime. In one patient, a minimal trap-door deformitywas seen that resolved in 2 months with massage andcompression. All patients were satisfied with the re-sult (Figs. 2 through 6).
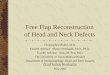
Table 1. Information Regarding Patients Undergoing the Triple Z Flap Technique
PatientAge(yr) Sex
Location of DefectLesion Complications Outcome
Follow-Up(mo)
1 52 M Right infraorbital area Basal cell carcinoma Early congestion inthe tip of one flap
No flap loss; tumorclose to one margin,no recurrence
35
2 49 F Tip of the nose Basal cell carcinoma — Free margin, norecurrence
34
3 57 M Chin Squamous cellcarcinoma
— Free margin, norecurrence
30
4 41 M Left buccal area Basal cell carcinoma — Free margin, norecurrence
27
5 67 F Left temporal area Basal cell carcinoma — Tumor close to onemargin, reexcision
27
6 45 M Right arm Hairy nevus — Minimal trap doordeformity, resolvedlater
21
7 71 M Dorsum of right hand Basal cell carcinoma — Free margin, norecurrence
19
8 60 M Forehead Seborrheic keratosis — Total excision 159 92 M Right zygomatic area Basosquamous cell
carcinoma— Free margin,
recurrence ofintraparotidmetastatic squamouscell carcinoma of earorigin
15
10 56 M Left preauricular area Squamous cellcarcinoma
— Free margin, norecurrence
13
11 47 M Left elbow Traumatic defect Minor infection Delayed healing 1312 79 F Left buccal area Squamous cell
carcinoma— Free margin, no
recurrence12
13 60 M Left zygomatic areaclose to eyelid
Squamous cellcarcinoma
— Free margin, norecurrence
11
14 55 M Right infraorbital area Basal cell carcinoma — Free margin, norecurrence
9
15 52 F Left ring finger Pyogenic granuloma — No recurrence 916 65 M Left infraorbital area,
close to eyelidBasal cell carcinoma — Free margin, no
recurrence8
17 48 M Left buccal area Basal cell carcinoma — Free margin, norecurrence
5
18 51 M Left index finger Pyogenic granuloma Infection and minorsuture detachment
Delayed healingwithout latecomplication
5
Volume 119, Number 3 • Triple Z Flaps
881
DISCUSSIONMobility and elasticity are among the most im-
portant features of skin that provide a variety ofpossible reconstructive options for defect closure.1The planning of reconstruction carries significantimportance for the late result of the surgery. Theideal flap closure must redirect and minimize woundtension and enhance the cosmetic outcome in ad-dition to preventing the free margin distortion atproblem areas such as eyelid, lip, or nose.1 There-fore, reconstruction of defects located close to im-portant structures must alert the surgeon to choosea technique that will meet all requirements of re-construction. A variety of advancement, rotation,and transposition flaps or skin grafts may be selectedfor reconstruction of such defects. Many differenttechniques for reconstruction of geometric defectshave been defined, including the Limberg flap, therhomboid Z flap, the double-opposing semicircularflap, the multiple pinwheel flap, and the transposi-
tional flap, and all of these are used routinely.2–5
Some of them have been based on the principle ofmultiple flap reconstruction, which enables the useof smaller flaps, thus reducing the risk of distortion
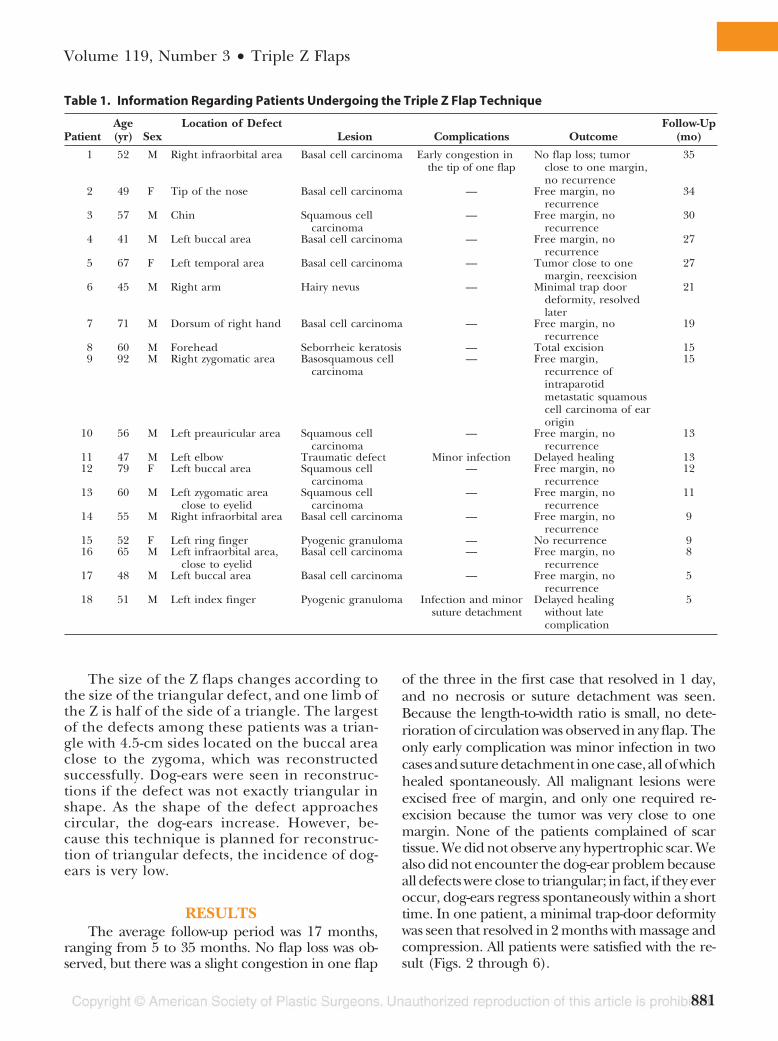
Fig. 3. A triangular lesion on the right infraorbital area beforereconstruction with triple Z flaps.
Fig. 1. (Above) Geometric planning of the triple Z flap for an op-timal triangular defect. (Below) The extent of tissue borrowingthat is distributed almost all around the defect after the flapswere transposed. Note that the tissue borrow is significantly lesson the sides where central limbs of the three Z flaps are directed.
Fig. 2. (Above) A triangular squamous cell carcinoma locatedclose to the eyelid was removed and triple Z flaps were planned.(Below) Appearance after the defect was reconstructed.
Plastic and Reconstructive Surgery • March 2007
882
and donor-site deformities. Actually, most of the lo-cal flaps for closure of defects are based on theZ-plasty principle, which is essentially a triangulartransposition flap based on independent randompattern vascular supplies.6,7
We used our technique of triple Z flaps for de-fects geometrically close to triangular. Although itexactly fits triangular defects, with very minimal dis-tortion and tissue borrowing, it is also applicable tonearly circular defects, with minimal dog-ears at thecorners. Actually, almost all flap reconstructions arebased on the principle of borrowing surroundingtissues to fill the defect. Therefore, a single flap al-most always causes distortion or donor-site sequelae
in problem areas and should be limited only ifenough tissue at that site is present. Especially if thedefect is close to important structures, we prefer theuse of the triple Z technique. This technique, withthree Z flaps planned on each side of the defect,causes minimal distortion because the tissues areborrowed from all around the defect (Fig. 1, below).The total length of the incisions of this technique iscomparable to the incisions of a single large flap;therefore, the triple Z flap technique also minimizesthe late-term scars because it breaks the incisionsinto several small components. As a basic principle,Z-plasty elongates the scar on its central axis, andtherefore this technique of the triple Z flap also
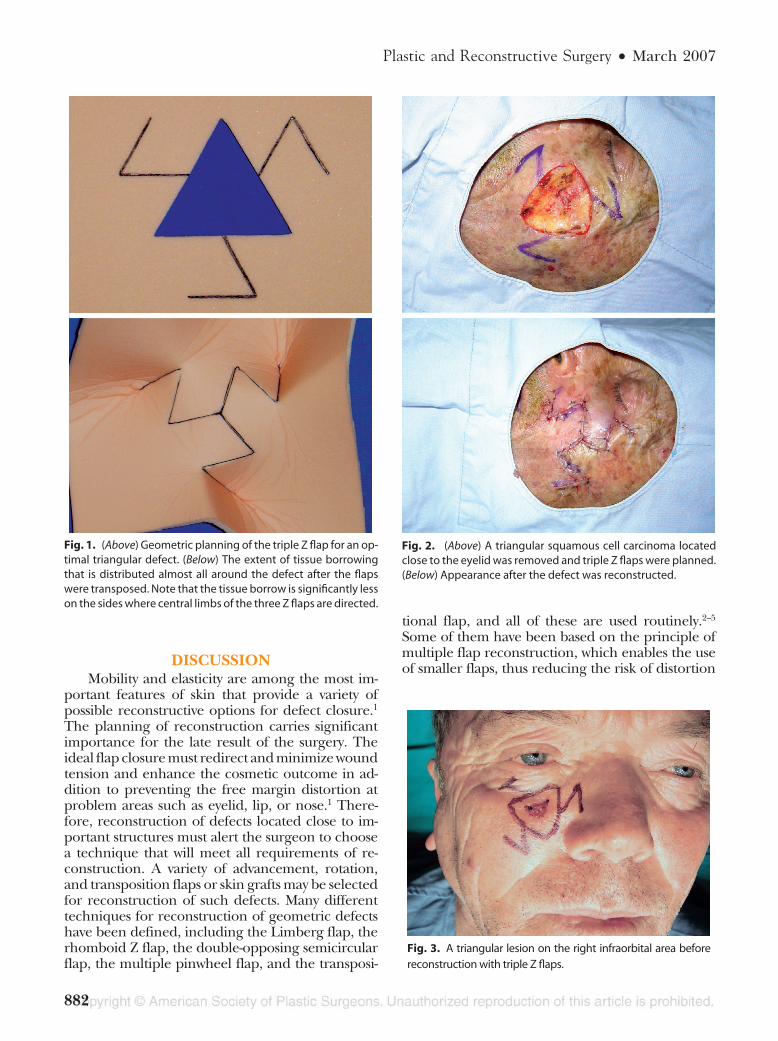
Fig. 4. Postoperative views of a patient with his eyes closed (left) and (right) open, without any retraction.
Fig. 5. Postoperative views of a patient with his eyes closed (left) and (right) open, without any retraction.
Volume 119, Number 3 • Triple Z Flaps
883
enables the surgeon to place and design the Z flapon the specific side of the defect that is close toimportant structures so that it results in less tissuebeing borrowed from that side.6,8 Significantly less
tissue is borrowed on the axis where the central limbsof the three Z flaps are directed. This helps thesurgeon to place the central limbs toward the sidewhere distortion should be minimal. There are nomajor contraindications besides the general contra-indications for random flaps.
CONCLUSIONSThis multiple flap application of the triple Z flap
technique has the advantage of almost full mobili-zation of surrounding tissues compared with a classicsingle-flap reconstruction with limited mobilization.The most important advantage of this technique isthat three small Z flaps can be elevated from adja-cent tissue of the defect instead of a single large flapthat may cause donor-site morbidity. The techniqueis easy to learn and execute. We believe that thetriple Z flap technique can be used in selected caseswith triangular defects where local flap choices arescarce and it is difficult to achieve good anatomicaland aesthetic results.
Cenk Sen, M.D.Department of Plastic and Reconstructive Surgery
Kocaeli University Faculty of Medicine41900 Derince
Kocaeli, [email protected]
DISCLOSURESWe hereby certify that, to the best of our knowledge, no
financial support or benefits have been received by any of theauthors, by any member of our immediate family, or by anyindividual or entity with whom or with which we have asignificant relationship from any commercial source whichis related directly or indirectly to the scientific work reportedon in the article.
REFERENCES1. Darrell, J. F., Wang, T. S., and Johnson, T. M. The Z-plasty
transposition flap for reconstruction of the middle cheek.J. Am. Acad. Dermatol. 46: 738, 2002.
2. Keser, A., Sensoz, O., and Mengi, A. S. Double opposingsemicircular flap: A modification of opposing Z-plasty for clos-ing circular defects. Plast. Reconstr. Surg. 102: 1001, 1998.
3. Gurunluoglu, R., Dogan, T., Bayramicli, M., and Numanoglu,A. Closure of infratip nasal defect by two triangular flaps. Plast.Reconstr. Surg. 108: 148, 2001.
4. Cruz, N. I., Ariyan, S., Duncan, C. C., and Cuono, C. B. Repairof lumbosacral myelomeningoceles with double Z-rhomboidflaps: Technical note. J. Neurosurg. 59: 714, 1983.
5. Vecchione, T. R. Multiple pinwheel scalp flaps. In B. Strauch,L. O. Vasconez, and E. J. Hall-Findlay (Eds.), Grabb’s Encyclo-pedia of Flaps, Vol. 1, 1st Ed. Boston: Little, Brown, 1990. Pp.10–12.
6. Hudson, D. A. Some thoughts on choosing a Z-plasty: The Zmade simple. Plast. Reconstr. Surg. 106: 665, 2004.
7. Da-Yuan, C. Mathematical principle of planar Z-plasty. Plast.Reconstr. Surg. 105: 105, 2000.
8. Hyakousoku, H., and Fumiiri, M. The square flap method. Br.J. Plast. Surg. 40: 40, 1987.
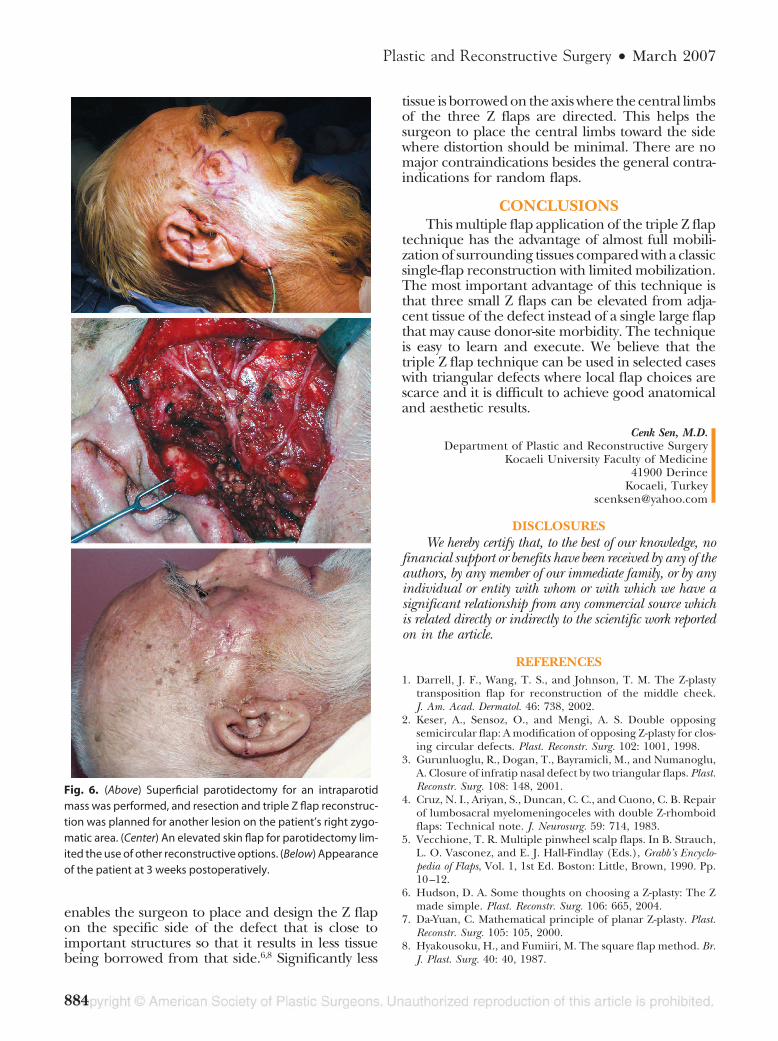
Fig. 6. (Above) Superficial parotidectomy for an intraparotidmass was performed, and resection and triple Z flap reconstruc-tion was planned for another lesion on the patient’s right zygo-matic area. (Center) An elevated skin flap for parotidectomy lim-ited the use of other reconstructive options. (Below) Appearanceof the patient at 3 weeks postoperatively.
Plastic and Reconstructive Surgery • March 2007
884