Embed Size (px)
Citation preview
Triple negative breast cancer - are we making progress -
Aleksandra Filipovic MD PhD
UMOS Belgrade , Serbia May 16th, 2015

Contents
Introduction / definition
Current treatments for triple-negative
breast cancers
Other targets for treatment of triple-
negative breast cancers
Conclusions


Basal-Like Carcinoma not a complete overlap with TNBC
Sub-type from gene expression profiling
Cytokeratines 5/6/17 or 14 + (CK8/18-) : 0,8%
Combined (CK 8/18+ ) : 10 %
Particular morphotype and immunophenotype:Central
necrosis (74%)
Pushing margins (60%)
Grade III / high mitotic index
RO-/ RP-/ HER2-/ p53 + / EGFR + (41%) or c-KIT+ (31%)

Challenges in treating TNBC
Absence of biomarkers
Aggressive natural history
Propensity for early visceral metastasis
Paradoxical response to chemotherapy
BRCA-1 pathway activity (DNA repair, cell
cycle check point responses) may be
impaired
•

7 different molecular subtypes

How might we target each subtype?
Basal-like 1 and 2: DNA damaging agents,
growth factor inhibition (i.e. EGFR)
Immunomodulatory: ? Immune regulators
Mesenchymal and mesenchymal / stem cell:
PI3K/mTOR pathway
LAR: Androgen blockade


Targets for TNBC
Proliferation →anthracyclines
p-53 →taxanes
Genetic instability →DNA-damaging agents
(platinum compounds, . . . )
Angiogenesis
EGF-R
c-Kit
Targeted therapies
something old something new
•Neoadjuvant
•Adjuvant
•Metastatic
Chemotherapy: Adverse events
Activity Toxicity
Fever Nausea Infusional reactions Oral complications Diarrhea Anemia Neuropathy Alopecia Rash, Extravasation Emotional
Cardiac
Secondary Malignancies
Fatigue
Neuropathy
Arthropathy

Current Treatments for TNBC
Traditional Adjuvant Chemotherapy :
Anthracycline + alkylating agent, followed by taxane
doxorubicin + cyclophosphamide followed by paclitaxel
CMF – a comeback in TNBC CMF reduces locoregional recurrence rate and prolongs DFS in LN-ve
TNBC, tumours > 2 cm
N = 687
56 months (range 14-156 months)
decreased recurrence compared to anthracycline- or taxane- (RR = 0.66,
95%; CI 0.45-0.96; P = 0.030)
CMF regimens for TNBC patients may be more effective than anthracycline-
or taxane-based regimens

TNBC ‘Paradox’: Chemotherapy
N > 1000
pCR rates: TNBC ~20 – 30%; non-TNBC ~5 – 15%; (P = .034)
3-yr DFS and OS lower in TNBC vs non-TNBC; (P<.0001)

Highest rates of pCR are seen in HER2 +ve and TNBC
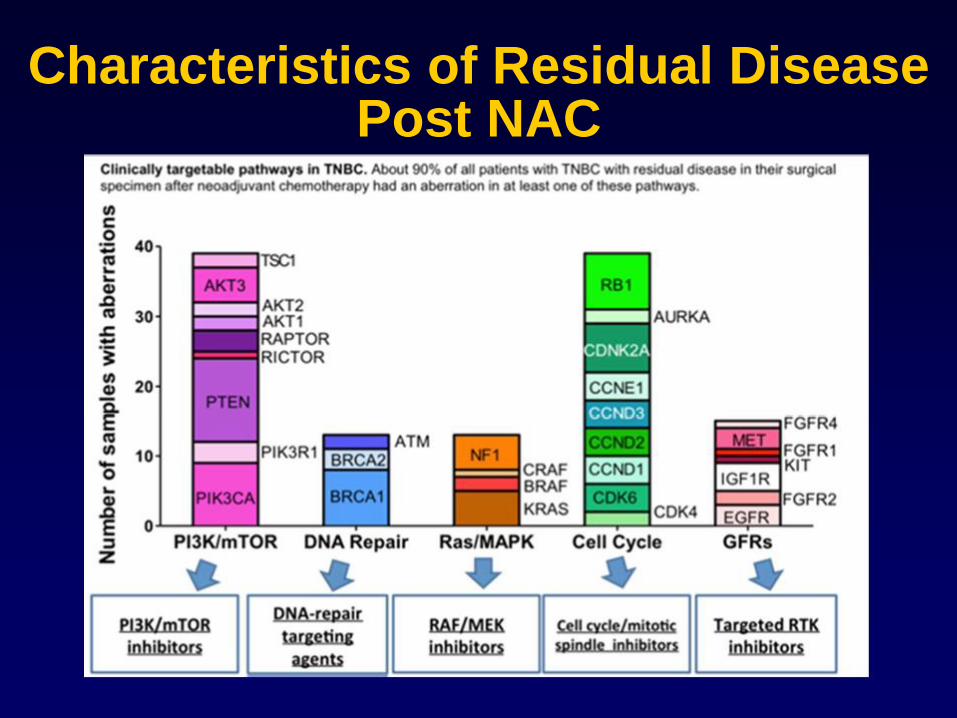
Characteristics of Residual Disease Post NAC
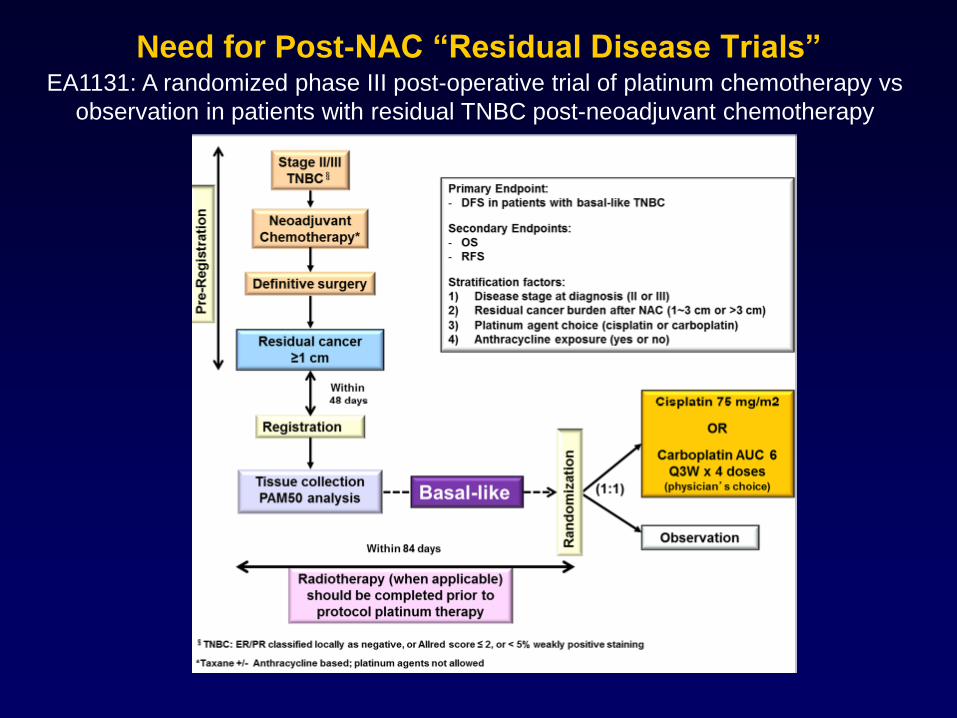
Need for Post-NAC “Residual Disease Trials”
EA1131: A randomized phase III post-operative trial of platinum chemotherapy vs
observation in patients with residual TNBC post-neoadjuvant chemotherapy
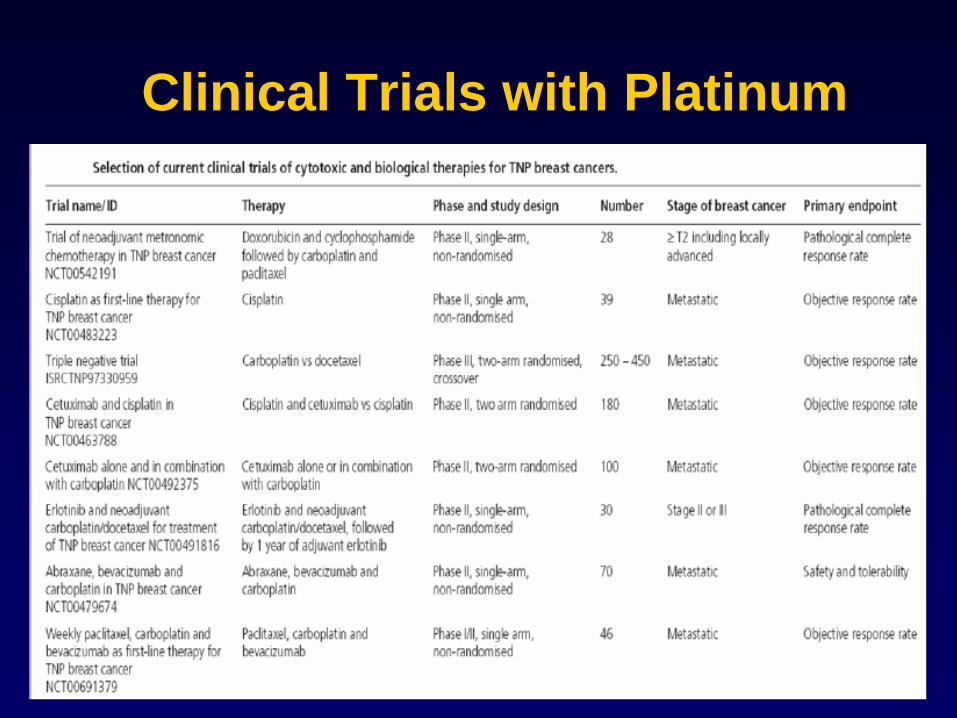
Clinical Trials with Platinum

Neoadjuvant Carboplatin for TNBC
von Minckwitz, Lancet Oncol 2014; 15: 747–56; Sikov, SABCS 2013; Rugo SABCS 2013; Alba, BCRT, 2012 (136)
Summary of recent randomized trials
Study Design N
pCR
Control Platinum
GeparSixto nplDox/Pac/Bev
+/- wCb (AUC1.5) X 18 wks
315 42.7% 53.2%
ALLIANCE 40603
2x2 design
wPac +/- Cb (AUC 6) +/- bev
AC X 4
433 41% 54%
ISPY2 wPac+/-Cb/veliparib ACx4 71 26%(est) 52%(est)
Both GeparSixto and CALGB 40603 included Bev along with Cb and I spy included PARPi

Slide 28
Presented By Melinda Telli at 2014 ASCO Annual Meeting

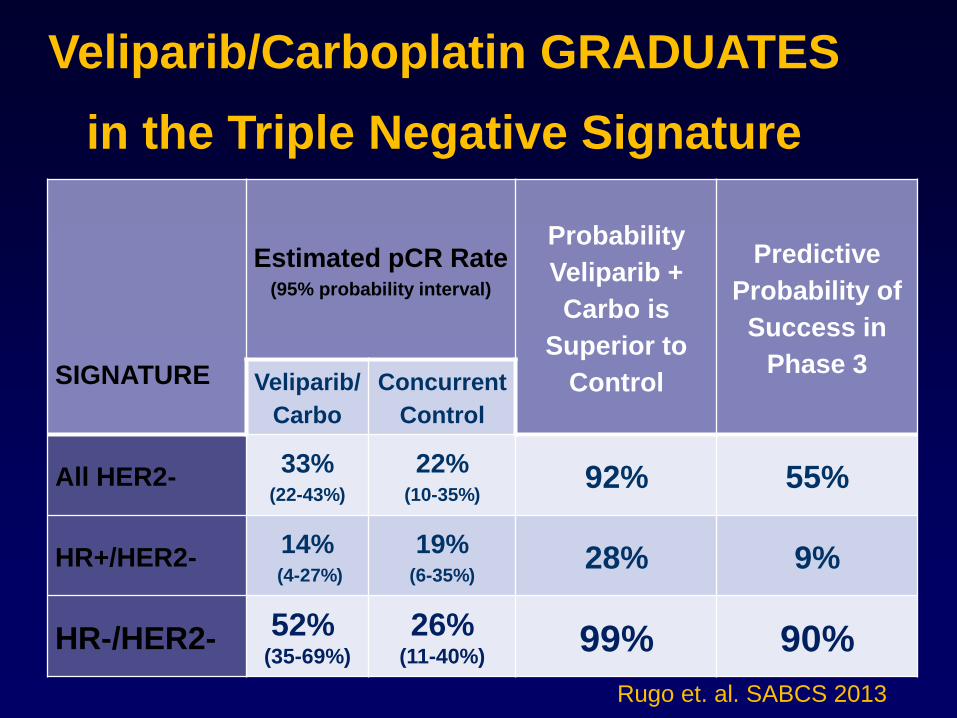
Veliparib/Carboplatin GRADUATES
in the Triple Negative Signature
SIGNATURE
Estimated pCR Rate (95% probability interval)
Probability
Veliparib +
Carbo is
Superior to
Control
Predictive
Probability of
Success in
Phase 3 Veliparib/
Carbo
Concurrent
Control
All HER2- 33%
(22-43%)
22%
(10-35%) 92% 55%
HR+/HER2- 14%
(4-27%)
19% (6-35%)
28% 9%
HR-/HER2- 52% (35-69%)
26% (11-40%)
99% 90%
Rugo et. al. SABCS 2013

Impact of BRCA1/2 Mutation Status on Response to
Platinum-Based Chemotherapy in Triple-Negative
Breast Cancer in the TBCRC009 Trial
• The TBCRC009 phase II trial evaluated single-agent cisplatin or
carboplatin as first- or second-line therapy for metastatic TNBC
• 6 patients (7%) are long-term survivors who achieved durable
responses and remain off all therapy (22+ - 53+ months); all of
these patients are BRCA1/2 WT (5) or unknown (1), and
received platinum therapy as first-line treatment for MBC
All Patients
n=86
BRCA1/2
Positive
n=11
BRCA1/2 WT
n=65
Unknown
n=10
ORR 30.2% 54.6%* 26.2% 30%
Median PFS 88 days 96 days 86 days --
* P=.079 versus BRCA1/2 WT
Isakoff et al., SABCS 2012; abstract PD-09-03
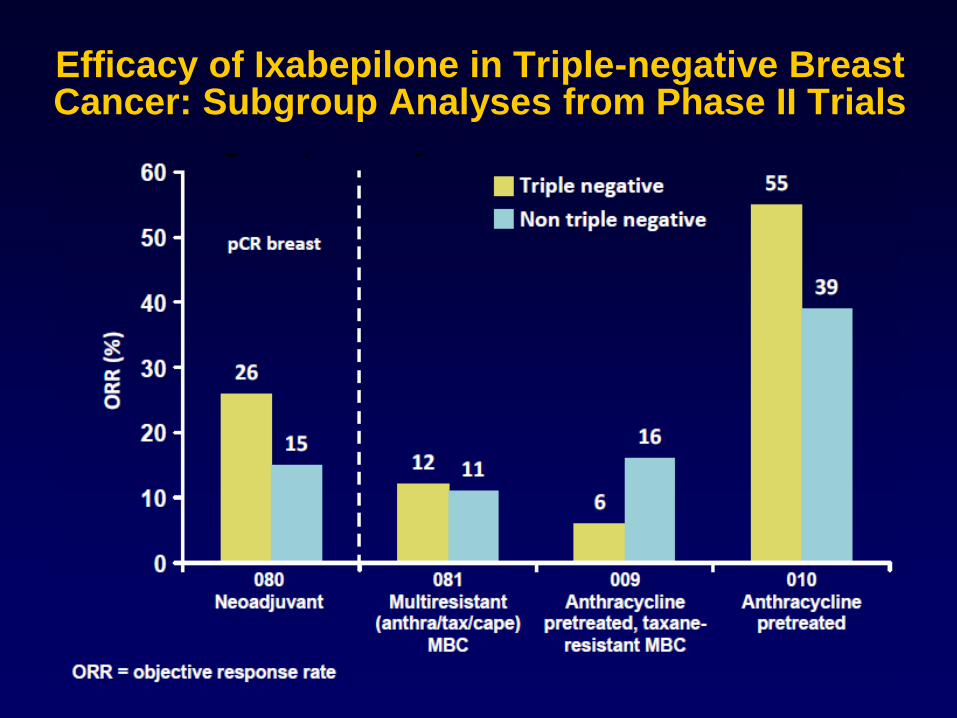
Efficacy of Ixabepilone in Triple-negative Breast Cancer: Subgroup Analyses from Phase II Trials

Ixabepilone + Capecitabine Active inIxabepilone + Capecitabine Active in Triple-Negative Anthracycline-
andTriple-Negative Anthracycline-and Taxane-Resistant MBCTaxane-Resistant MBC

PARP1 inhibition
DNA-repair defect characteristics of BRCA1-related cancers confer
sensitivity to bi-functional alkylating agents, mitomycinC and platinum
drugs
Defective BCRA1 function could be more specifically targeted
– Rationale in triple-negative population:
evidence of deficient BRCA1
in vitro data showing activity of PARP1 inhibitors in BRCA1 null cells
Phase I/II studies ongoing

Other targets for treatment of triple- negative breast cancers
Treatment Directed Against Angiogenesis
Bevacizumab, sunitinib
Rationale in triple-negative population:
highly angiogenic phenotype
responses for heavily pretreated patients during early
phase II trials
Phase II/III studies ongoing
Bevacizumab
Activity, 2 first line trialsPaclitaxel +/- Bevacizumab
(Miller NEJM 2007)
Docetaxel +/- Bevacizumab (AVADO ASCO 2008)
Completed trials, analysis pending
RIBBON I first line
- Docetaxel +/- Bevacizumab
- Anthracycline-based +/- Bevacizumab
- Capecitabine +/- Bevacizumab
RIBBON II second line
- Capecitabine +/- Bevacizumab

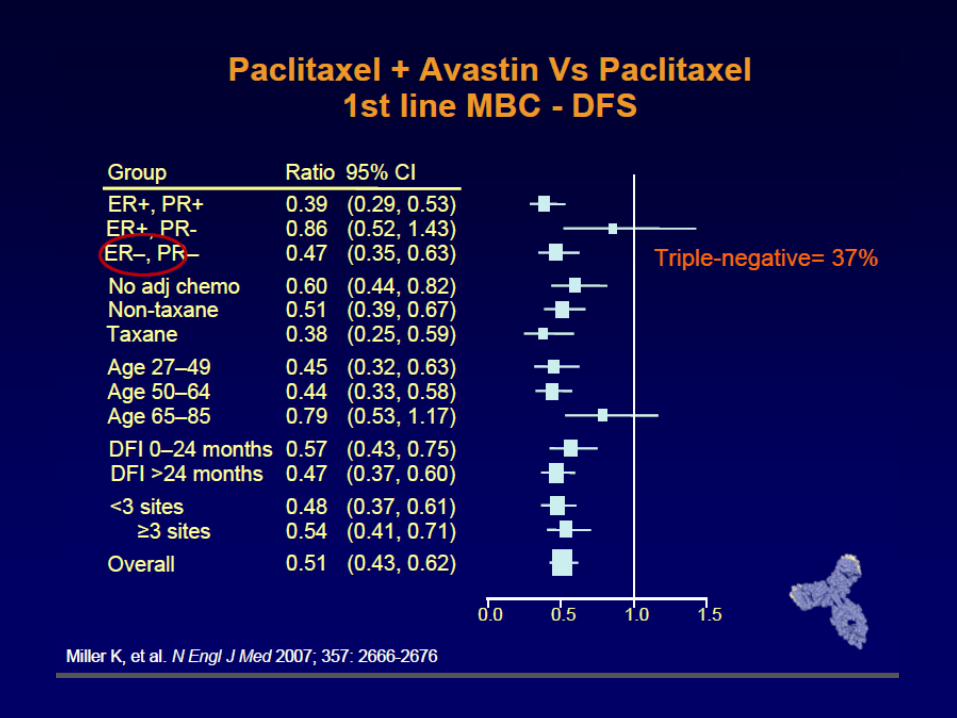
Metastatic Breast Cancer Phase III Paclitaxel versus Paclitaxel + Bevacizumab (ECOG 2100)


Treatment targeting EGFR
Cetuximab, gefitinib, erlotinib
Rationale in triple-negative population:
overexpression of EGFR
no evidence of activity to date
Phase II studies ongoing



Other combinations
Gemcitabine + erlotinib Post A et T
ORR 25%
Paclitaxel + cetuximab
Skin relapse EGFR+

TCGA: Molecular Characteristics of TNBC -Provides Fuel for Future Therapeutics
P53 mut 84%
RB1 mut/loss 20%
PIK3CA mut 7%
MYC focal gain 40%
PTEN loss 35%
Global Hypomethylation
INPP4B loss 30%
Aneuploidy and genomic instability

Novel Trials: PI3K inhibition in TNBC

Novel Trials: Targeting the Androgen Receptor in TNBC
Immunotherapy - the breakthrough
KEYNOTE 012 : single agent pembrolizumab 10mg/kg
27 patients with measurable metastatic TNBC
overall response rate 18.5%,
one (3.7%) complete response
four (14.8%) partial responses.
seven patients (25.9%) stable disease
median duration of response ranging from 15 to 40 months
progression-free survival rate at 6 months 23.3% in heavily
pretreated patients
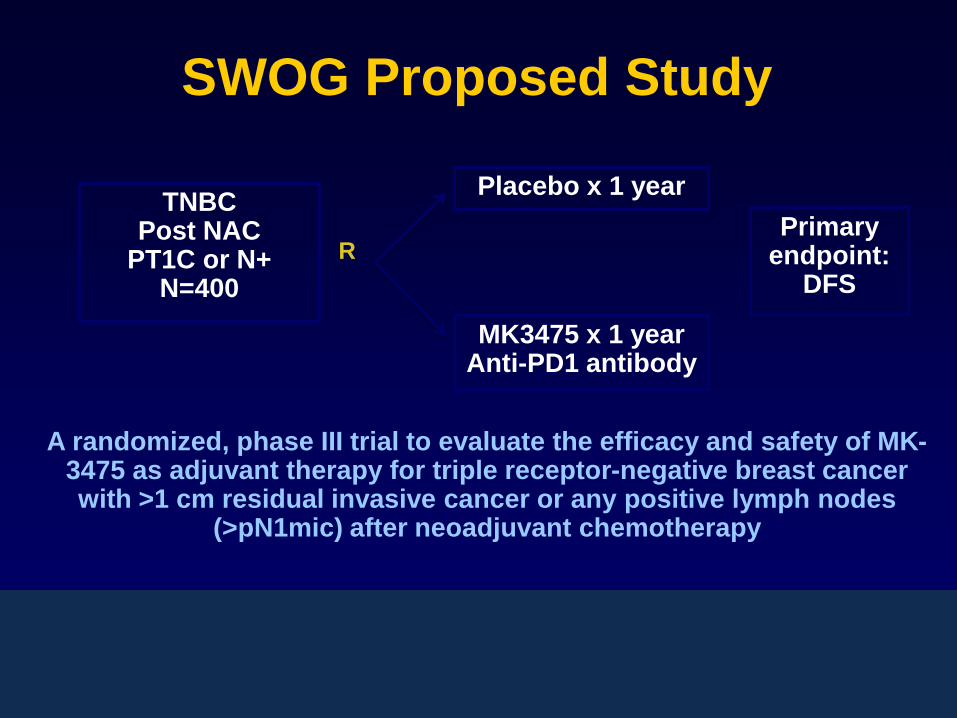
SWOG Proposed Study
R
TNBC Post NAC
PT1C or N+ N=400
Placebo x 1 year
MK3475 x 1 year Anti-PD1 antibody
Primary endpoint:
DFS
A randomized, phase III trial to evaluate the efficacy and safety of MK-3475 as adjuvant therapy for triple receptor-negative breast cancer with >1 cm residual invasive cancer or any positive lymph nodes
(>pN1mic) after neoadjuvant chemotherapy

Cancer cell
Cancer cell
Durable response
So, Are We Making Progress in TNBC?
YES
Continued dissection of
complex biology
Incorporation of genetic
Factors in therapeutic choices
(ie, BRCA mutations/PARPi)
Plethora of ongoing clinical trials
(Clinicaltrials.gov ~ 120)

THANK YOU
Hvala mojim uciteljima i
kolegama na svom znanju
koje sam upila od Vas
Aleksandra