Embed Size (px)
Citation preview
doi:10.1016/j.e
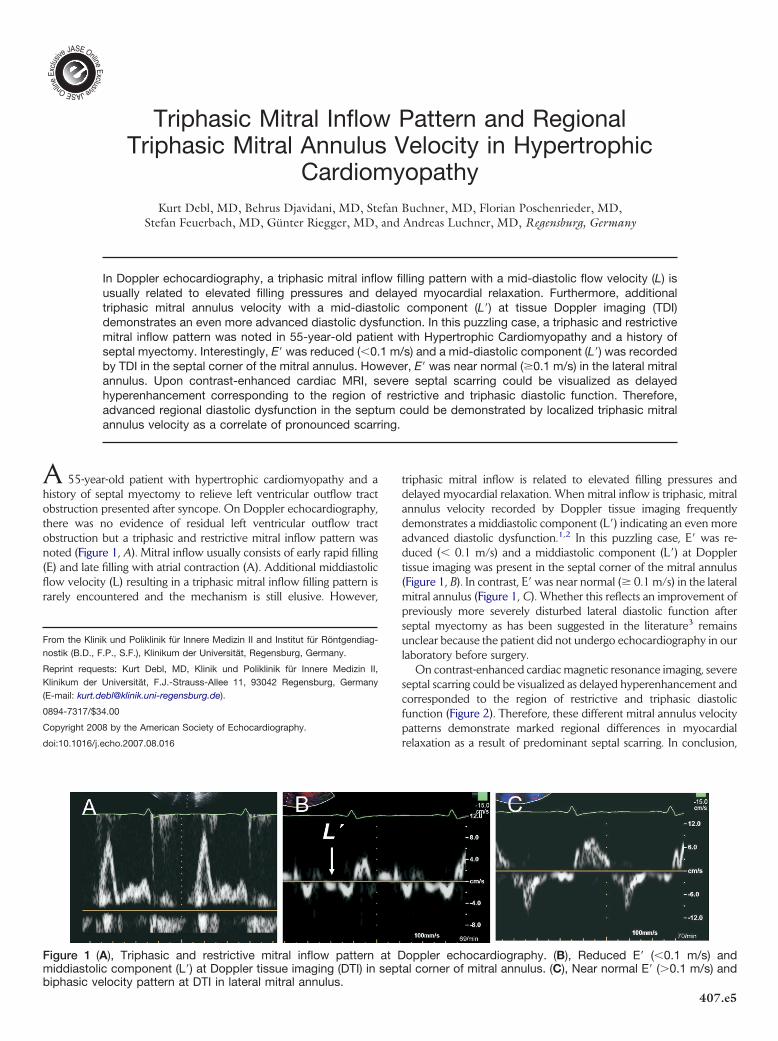
biphasic ve
Triphasic Mitral Inflow Pattern and RegionalTriphasic Mitral Annulus Velocity in Hypertrophic
Cardiomyopathy
cho.2
locit
Kurt Debl, MD, Behrus Djavidani, MD, Stefan Buchner, MD, Florian Poschenrieder, MD,
Stefan Feuerbach, MD, Günter Riegger, MD, and Andreas Luchner, MD, Regensburg, GermanyIn Doppler echocardiography, a triphasic mitral inflow filling pattern with a mid-diastolic flow velocity (L) isusually related to elevated filling pressures and delayed myocardial relaxation. Furthermore, additionaltriphasic mitral annulus velocity with a mid-diastolic component (L=) at tissue Doppler imaging (TDI)demonstrates an even more advanced diastolic dysfunction. In this puzzling case, a triphasic and restrictivemitral inflow pattern was noted in 55-year-old patient with Hypertrophic Cardiomyopathy and a history ofseptal myectomy. Interestingly, E= was reduced (�0.1 m/s) and a mid-diastolic component (L=) was recordedby TDI in the septal corner of the mitral annulus. However, E= was near normal (�0.1 m/s) in the lateral mitralannulus. Upon contrast-enhanced cardiac MRI, severe septal scarring could be visualized as delayedhyperenhancement corresponding to the region of restrictive and triphasic diastolic function. Therefore,advanced regional diastolic dysfunction in the septum could be demonstrated by localized triphasic mitralannulus velocity as a correlate of pronounced scarring.
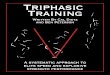
A 55-year-old patient with hypertrophic cardiomyopathy and ahistory of septal myectomy to relieve left ventricular outflow tractobstruction presented after syncope. On Doppler echocardiography,there was no evidence of residual left ventricular outflow tractobstruction but a triphasic and restrictive mitral inflow pattern wasnoted (Figure 1, A). Mitral inflow usually consists of early rapid filling(E) and late filling with atrial contraction (A). Additional middiastolicflow velocity (L) resulting in a triphasic mitral inflow filling pattern israrely encountered and the mechanism is still elusive. However,
From the Klinik und Poliklinik für Innere Medizin II and Institut für Röntgendiag-nostik (B.D., F.P., S.F.), Klinikum der Universität, Regensburg, Germany.
Reprint requests: Kurt Debl, MD, Klinik und Poliklinik für Innere Medizin II,Klinikum der Universität, F.J.-Strauss-Allee 11, 93042 Regensburg, Germany(E-mail: [email protected]).
0894-7317/$34.00
Copyright 2008 by the American Society of Echocardiography.
007.08.016
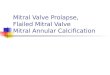
y pattern at DTI in lateral mitral annulus.
triphasic mitral inflow is related to elevated filling pressures anddelayed myocardial relaxation. When mitral inflow is triphasic, mitralannulus velocity recorded by Doppler tissue imaging frequentlydemonstrates a middiastolic component (L=) indicating an even moreadvanced diastolic dysfunction.1,2 In this puzzling case, E= was re-duced (� 0.1 m/s) and a middiastolic component (L=) at Dopplertissue imaging was present in the septal corner of the mitral annulus(Figure 1, B). In contrast, E= was near normal (� 0.1 m/s) in the lateralmitral annulus (Figure 1, C). Whether this reflects an improvement ofpreviously more severely disturbed lateral diastolic function afterseptal myectomy as has been suggested in the literature3 remainsunclear because the patient did not undergo echocardiography in ourlaboratory before surgery.
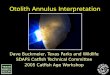
On contrast-enhanced cardiac magnetic resonance imaging, severeseptal scarring could be visualized as delayed hyperenhancement andcorresponded to the region of restrictive and triphasic diastolicfunction (Figure 2). Therefore, these different mitral annulus velocitypatterns demonstrate marked regional differences in myocardial
relaxation as a result of predominant septal scarring. In conclusion,Figure 1 (A), Triphasic and restrictive mitral inflow pattern at Doppler echocardiography. (B), Reduced E= (�0.1 m/s) andmiddiastolic component (L=) at Doppler tissue imaging (DTI) in septal corner of mitral annulus. (C), Near normal E= (�0.1 m/s) and
407.e5

(0.2 mmol/kg/bodyweight).
407.e6 Debl et al Journal of the American Society of EchocardiographyApril 2008
advanced regional diastolic dysfunction in the septum could bedemonstrated by localized triphasic mitral annulus velocity as acorrelate of pronounced scarring.
REFERENCES
1. Ha JW, Ahn JA, Moon JY, Suh HS, Kang SM, Rim SJ, et al. Triphasic mitralinflow velocity with mid-diastolic flow: the presence of mid-diastolic mitralannular velocity indicates advanced diastolic dysfunction. Eur J Echocar-diogr 2006;7:16-21.
2. Ha JW, Oh JK, Redfield MM, Ujino K, Seward JB, Tajik AJ. Triphasicmitral inflow velocity with middiastolic filling: clinical implications andassociated echocardiographic findings. J Am Soc Echocardiogr 2004;17:428-31.
3. Jassal DS, Neilan TG, Fifer MA, Palacios IF, Lowry PA, Vlahakes GJ, et al.Sustained improvement in left ventricular diastolic function after alcoholseptal ablation for hypertrophic obstructive cardiomyopathy. Eur Heart J2006;27:1805-10.
Figure 2 Short-axis slice showing scarring of septum and at junctionof right ventricle (arrows) visualized by contrast-enhanced magneticresonance imaging as delayed hyperenhancement 15 minutes afteradministration of gadolinium-diethylene-triamine-pentaacetic acid