Embed Size (px)
Citation preview

ABSTRACT: The effects of electrical trigeminal stimulation on activatedfacial muscles were studied in 20 normal subjects in order to evaluatewhether excitatory or inhibitory responses are present and to investigatewhether the reflex organization is similar in all the facial muscles. No inhi-bition was observed in frontalis, orbicularis oculi, orbicularis oris, and men-talis muscles. By contrast, a clear suppression of electromyographic (EMG)activity (late silent period or SP2) was present in the levator labii superioris,depressor anguli oris, and depressor labii inferioris muscles, with a meanlatency ranging from 41.8 to 50.2 ms, and a mean duration ranging from 27.5to 40.9 ms. An early suppression of EMG activity (early silent period or SP1)was observed, with a latency of 16 to 20 ms and a duration of 10 ms, mainlyin inferior perioral muscles. Our findings show a selective trigeminal inhibi-tory influence upon some specific lower facial muscles.
© 2000 John Wiley & Sons, Inc. Muscle Nerve 23: 939–945, 2000
TRIGEMINO-FACIAL REFLEX INHIBITORY RESPONSESIN SOME LOWER FACIAL MUSCLES
GIOVANNI PAVESI, MD,1 GUIDO MARIA MACALUSO, MD, 2
PAOLA MARCHETTI, MD, 1 LUIGI CATTANEO, PhD, 1 STEFANO TINCHELLI, 1
ANTOON DE LAAT, DDS, PhD, 3 and DOMENICO MANCIA, MD 1
1 Istituto di Neurologia, University of Parma, Strada del Quartiere 4,I-43100 Parma, Italy2 Istituto di Clinica Odontoiatrica, University of Parma, Parma, Italy3 Department of Oral Physiology, School of Dentistry, Katholieke Universiteit,Leuven, Belgium
Accepted 18 February 2000
The abundant information that exists on the reflexmotor control of the upper facial muscles contrastswith the limited knowledge available for the lowerfacial muscles. The blink reflex is an excitatory tri-gemino-facial response, originally described by Over-end (1896)22 and investigated electrophysiologicallyfirst by Kugelberg (1952),18 that is limited to theorbicularis oculi muscle.15–17 In pathological condi-tions such as hemifacial spasm, both the R1 and R2responses can spread to the orbicularis oris muscle.Inhibitory responses have been extensively describedin the jaw-closing muscles, both after trigeminal andremote stimulation.20,21 Stimulation of the fifth cra-nial nerve has also been observed to elicit excitatoryand inhibitory responses in cervical muscles.9,10,12
More recently, inhibitory responses have been de-scribed in the levator palpebrae muscle.1 No clear
inhibitory responses have been shown in the lowerfacial muscles. Mechanical stimulation of the lipsand electrical stimulation of the infraorbital andmental nerves have been shown to elicit small andinconstant responses in the orbicularis oris muscleboth in normal subjects and in patients affected bybasal ganglia disorders.24
The aims of the present study were: (1) to evalu-ate whether excitatory or inhibitory responses arepresent in lower facial muscles after stimulation ofthe trigeminal nerve, and (2) to investigate whetherthe reflex organization is similar in all the lower fa-cial muscles. The results show a selective trigeminalinhibitory influence upon certain lower facialmuscles. The peculiar motor organization of thesemuscles may relate to their mainly mimic function.
MATERIALS AND METHODS
Subjects. Twenty healthy subjects (9 women and11 men; mean age 32 years; range 22–55 years), par-ticipated in the experiments and gave their in-formed consent. The experimental protocol was ap-proved by the local ethical committee.
Abbreviations: EMG, electromyographic; SP, silent period; SP1, earlysilent period; SP2, late silent period; Th, thresholdKey words: blink reflex; facial muscles; facial nerve; silent period; trigem-inal nerveCorrespondence to: G. Pavesi; e-mail: [email protected]
© 2000 John Wiley & Sons, Inc.
Facial Muscles Silent Periods MUSCLE & NERVE June 2000 939

Experimental Procedure. Our aim was to evaluatethe effects of trigeminal branch stimulation on theelectromyographic (EMG) activity of voluntarily ac-tivated individual facial muscles. Subjects wereseated comfortably in a reflex chair with eyesopened. The perceptive threshold (Th) for thestimulus was determined using the ascending anddescending method of limits in the peripheral terri-tory of each trigeminal branch. The blink reflex wasevoked at a stimulation intensity of 10 × Th as acontrol of the integrity of the trigemino-facial reflexarc. Depending on the type of experiment, a stimu-lation intensity multiple of Th was chosen. The sub-jects were instructed to perform a selective activationof the facial muscle under study and trained them-selves using a mirror to keep the voluntary contrac-tion as stable as possible.
Stimulation Procedure. The individual trigeminalbranches were stimulated with surface electrodes(Dantec 13L20; Dantec Medical, Copenhagen, Den-mark), at their respective sites of emergence fromthe skull, by means of a constant current stimulator.The active electrode was positioned at the foramen,and the reference electrode 2 cm away. The stimuliused were single square-waves of 0.2 ms duration andof an intensity determined according to threshold.Stimuli were randomly applied with an interstimulusinterval of at least 10 s. Stimuli were applied to thesupraorbital (13 cases), infraorbital (6 cases), andmental (6 cases) nerves, contralateral to the re-corded muscle. The ipsilateral supraorbital nervewas stimulated in 6 subjects; the second and thirdipsilateral branches were not extensively investigatedowing to stimulating artifacts on the nearby record-ing electrodes due to diffusion of current and to thedirect activation of the marginal branch of the facialnerve.
A recruitment curve was constructed in 3 sub-jects, recording from the levator labii superiorismuscle after stimulation of the contralateral supra-orbital nerve (intensities of stimulation: 1, 2, 4, 6, 8,10, 12 × Th).
Control Experiments. In 3 subjects, the ipsilateraland contralateral oral mucosa was stimulated at 5and 10 × Th by means of a surface bipolar stimulat-ing electrode mounted on a sponge (Dantec dispos-able sphincteric electrode, 13L81; Dantec Medical).Recordings were made from the activated levator la-bii superioris, depressor anguli oris, and massetermuscles.
In 3 subjects, the contralateral median nerve andthe C2–C4 cervical dermatomes were also electricallystimulated by surface electrodes in bipolar montage,at 10 × Th, while recording from the contracted le-
vator labii superioris muscle. In addition, the effectof an acoustic stimulus (a rarefaction click of 132 dBSPL) applied binaurally by means of a headphone,was investigated in the same muscle.
In all subjects, stimulation of the facial nerve atthe stylomastoid foramen was performed using ahand-held fork stimulating electrode (Dantec stimu-lating electrode: 13L36; handgrip: 13L34; DantecMedical), to evoke a direct motor response (M re-sponse) while recording from levator labii superiorisand orbicularis oris muscles, both at rest and duringvoluntary contraction.
Recording Conditions. The EMG activity was re-corded using disposable concentric needle elec-trodes (Meditec, Parma, Italy) from frontalis, orbi-cularis oculi, orbicularis oris, mentalis, levator labiisuperioris, depressor anguli oris, and depressor labiiinferioris muscles. The zygomaticus and the levatoranguli oris muscles were only examined in 2 subjects,due to difficulties in localizing these muscles withthe recording needle because of their deep locationand lack of reference points. Auditory feedback wasprovided to the subject, who was asked to maintain astable and sustained contraction. Different degreesof muscle activation were tested.
The EMG was recorded over a period of 400 ms(120 ms pre-stimulus, 280 ms post-stimulus). The sig-nal was amplified, filtered (band-pass 20 HZ–2 KHZ
for surface recordings and 20 HZ–10 KHZ for needlerecordings), digitized, and stored for off-line analy-sis. For each muscle, at least two blocks of foursweeps (eight traces) of nonrectified EMG activitywere recorded for each different experimental con-dition, using a Counterpoint MK2 electromyographsystem (Dantec Medical). Full wave rectified and av-eraged EMG activity were recorded in 3 subjects forstudy of the recruitment curve.
Data Analysis. A silent period of the EMG wasdefined as a decrease of at least 80% in the ongoingEMG activity. The latency and duration of the reflexresponses were calculated accordingly. The durationof the silent period (SP) was measured from thestimulus to the recovery of 80% of baseline EMGactivity. For statistical analysis, unpaired Student’st-test was used.
RESULTS
The main finding of the present experiments wasthat stimulation of the contralateral and ipsilateralcutaneous trigeminal branches during a voluntarymuscular contraction induced a clear-cut suppres-sion of the EMG activity only in some of the studiedmuscles of the lower face, and specifically the levatorlabii superioris, depressor anguli oris, and depressor
940 Facial Muscles Silent Periods MUSCLE & NERVE June 2000
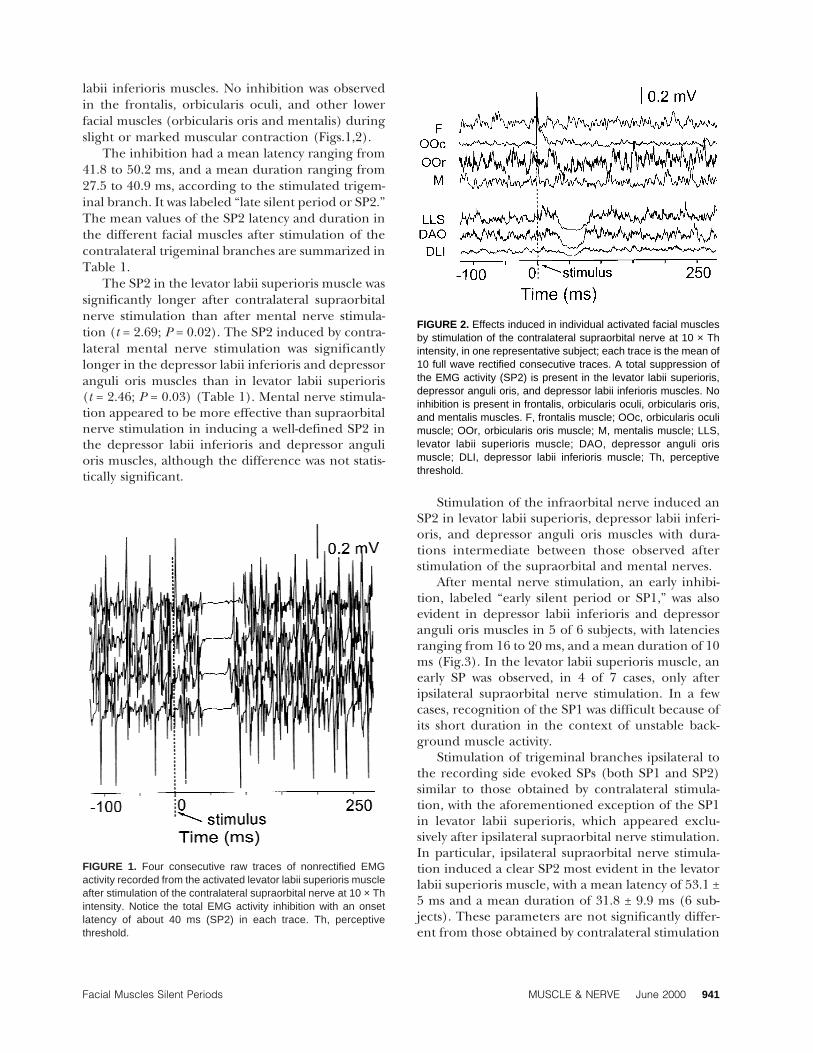
labii inferioris muscles. No inhibition was observedin the frontalis, orbicularis oculi, and other lowerfacial muscles (orbicularis oris and mentalis) duringslight or marked muscular contraction (Figs.1,2).
The inhibition had a mean latency ranging from41.8 to 50.2 ms, and a mean duration ranging from27.5 to 40.9 ms, according to the stimulated trigem-inal branch. It was labeled “late silent period or SP2.”The mean values of the SP2 latency and duration inthe different facial muscles after stimulation of thecontralateral trigeminal branches are summarized inTable 1.
The SP2 in the levator labii superioris muscle wassignificantly longer after contralateral supraorbitalnerve stimulation than after mental nerve stimula-tion (t = 2.69; P = 0.02). The SP2 induced by contra-lateral mental nerve stimulation was significantlylonger in the depressor labii inferioris and depressoranguli oris muscles than in levator labii superioris(t = 2.46; P = 0.03) (Table 1). Mental nerve stimula-tion appeared to be more effective than supraorbitalnerve stimulation in inducing a well-defined SP2 inthe depressor labii inferioris and depressor angulioris muscles, although the difference was not statis-tically significant.
Stimulation of the infraorbital nerve induced anSP2 in levator labii superioris, depressor labii inferi-oris, and depressor anguli oris muscles with dura-tions intermediate between those observed afterstimulation of the supraorbital and mental nerves.
After mental nerve stimulation, an early inhibi-tion, labeled “early silent period or SP1,” was alsoevident in depressor labii inferioris and depressoranguli oris muscles in 5 of 6 subjects, with latenciesranging from 16 to 20 ms, and a mean duration of 10ms (Fig.3). In the levator labii superioris muscle, anearly SP was observed, in 4 of 7 cases, only afteripsilateral supraorbital nerve stimulation. In a fewcases, recognition of the SP1 was difficult because ofits short duration in the context of unstable back-ground muscle activity.
Stimulation of trigeminal branches ipsilateral tothe recording side evoked SPs (both SP1 and SP2)similar to those obtained by contralateral stimula-tion, with the aforementioned exception of the SP1in levator labii superioris, which appeared exclu-sively after ipsilateral supraorbital nerve stimulation.In particular, ipsilateral supraorbital nerve stimula-tion induced a clear SP2 most evident in the levatorlabii superioris muscle, with a mean latency of 53.1 ±5 ms and a mean duration of 31.8 ± 9.9 ms (6 sub-jects). These parameters are not significantly differ-ent from those obtained by contralateral stimulation
FIGURE 1. Four consecutive raw traces of nonrectified EMGactivity recorded from the activated levator labii superioris muscleafter stimulation of the contralateral supraorbital nerve at 10 × Thintensity. Notice the total EMG activity inhibition with an onsetlatency of about 40 ms (SP2) in each trace. Th, perceptivethreshold.
FIGURE 2. Effects induced in individual activated facial musclesby stimulation of the contralateral supraorbital nerve at 10 × Thintensity, in one representative subject; each trace is the mean of10 full wave rectified consecutive traces. A total suppression ofthe EMG activity (SP2) is present in the levator labii superioris,depressor anguli oris, and depressor labii inferioris muscles. Noinhibition is present in frontalis, orbicularis oculi, orbicularis oris,and mentalis muscles. F, frontalis muscle; OOc, orbicularis oculimuscle; OOr, orbicularis oris muscle; M, mentalis muscle; LLS,levator labii superioris muscle; DAO, depressor anguli orismuscle; DLI, depressor labii inferioris muscle; Th, perceptivethreshold.
Facial Muscles Silent Periods MUSCLE & NERVE June 2000 941

(Table 1). Ipsilateral stimulation, like contralateral,was ineffective in evoking a SP in the tested musclesother than the levator labii superioris, depressor la-bii inferioris, and depressor anguli oris muscles.
Stimulation of the ipsilateral infraorbital andmental nerves induced artifacts due to currentspread when recording, respectively, from the leva-tor labii superioris muscle and from the depressorlabii inferioris and depressor anguli oris muscles, sowe could not measure the SP parameters systemati-cally. In addition, recordings from depressor angulioris and depressor labii inferioris muscles after ipsi-lateral mental nerve stimulation were contaminatedby the appearance of an M response due to directactivation of the marginal branch of the facial nerve.In spite of these technical limitations, both an earlyand a late SP could be recognized in these muscles.In the orbicularis oculi muscle, we occasionally ob-
served a reduction of EMG activity, which was partialand, when present, was always preceded by an in-crease in EMG activity, compatible in latency andduration with a R2 response of the blink reflex.
As previously stated (see Materials and Methods),we did not investigate systematically the zygomaticusand levator anguli oris muscles owing to difficultiesin localizing these muscles with the needle elec-trode; however, in the 2 subjects investigated, thesemuscles responded similarly to the levator labii su-perioris muscle.
Control Experiments. No EMG inhibition was evi-dent in the levator labii superioris or depressor an-guli oris muscles after electrical stimulation of theipsilateral and contralateral oral mucosa. The samestimuli applied extraorally to the cheek were effec-tive in evoking a clear inhibition of the EMG activity.Both the intra-oral and extra-oral stimulation evokednormal inhibitory reflexes in the masseter muscle(SP1 and SP2).
No consistent inhibitory responses were inducedin the activated levator labii superioris muscle aftermedian nerve or cervical dermatome stimulation,nor after binaural acoustic stimulation.
Supramaximal facial nerve stimulation at the sty-lomastoid foramen induced an M response in a con-tracting muscle, followed by a partial suppression ofthe EMG activity, lasting up to 25 ms from the stimu-lus onset. In the levator labii superioris, depressoranguli oris, and depressor labii inferioris muscles,stimulation at the stylomastoid foramen induced anadditional distinct suppression of EMG activity, withlatency and duration similar to the SP2 induced inthe same muscles by direct stimulation of the trigem-inal branches. Such a late and long-lasting SP wasnever observed in the orbicularis oris or orbicularisoculi muscles.
FIGURE 3. Four superimposed consecutive traces recorded fromthe activated depressor anguli oris muscle after stimulation of thecontralateral mental nerve at 10 × Th intensity. Notice the early(SP1) and late (SP2) silent periods in each trace. Th, perceptivethreshold.
Table 1. SP2 latency and duration in individual facial muscles.†
Stimulated nerve
Levator labii superiorisDepressor labii
inferioris/depressor anguli oris
Latency (ms) Duration (ms) Latency (ms) Duration (ms)
Supraorbital 46.1 ± 4.6 40.9 ± 10.5* 41.9 ± 9.2 34.8 ± 10.7Infraorbital 41.8 ± 7.8 38 ± 5.6 ND NDMentalis 50.2 ± 11.8 27.5 ± 8.7*,‡ 46.3 ± 4.4 40.2 ± 9.2‡
†SP2 latency and duration in LLS and DAO/DLI muscles after stimulation of the contralateral trigeminal branches at 10 × Th intensity. The data relativeto DAO and DLI muscles are pooled together because the individual values were not significantly different in the two muscles. The supraorbital nervewas stimulated in 13 subjects; the infraorbital and mental nerves were stimulated in 6 subjects. For each subject, latency and duration are the mean ofeight traces. SP2, late silent period; LLS, levator labii superioris muscle; DAO, depressor anguli oris muscle; DLI, depressor labii inferioris muscle; Th,perceptive threshold; ND, not done.* t = 2.69; P = 0.02.‡t = 2.46; P = 0.03.
942 Facial Muscles Silent Periods MUSCLE & NERVE June 2000
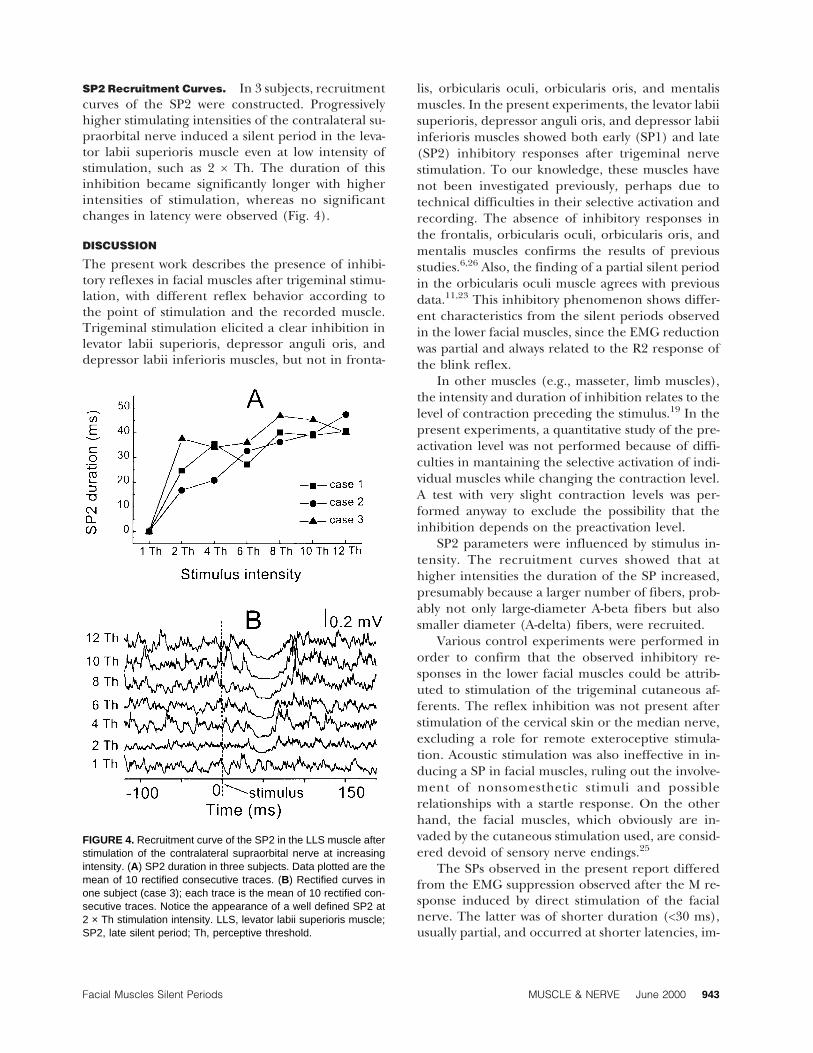
SP2 Recruitment Curves. In 3 subjects, recruitmentcurves of the SP2 were constructed. Progressivelyhigher stimulating intensities of the contralateral su-praorbital nerve induced a silent period in the leva-tor labii superioris muscle even at low intensity ofstimulation, such as 2 × Th. The duration of thisinhibition became significantly longer with higherintensities of stimulation, whereas no significantchanges in latency were observed (Fig. 4).
DISCUSSION
The present work describes the presence of inhibi-tory reflexes in facial muscles after trigeminal stimu-lation, with different reflex behavior according tothe point of stimulation and the recorded muscle.Trigeminal stimulation elicited a clear inhibition inlevator labii superioris, depressor anguli oris, anddepressor labii inferioris muscles, but not in fronta-
lis, orbicularis oculi, orbicularis oris, and mentalismuscles. In the present experiments, the levator labiisuperioris, depressor anguli oris, and depressor labiiinferioris muscles showed both early (SP1) and late(SP2) inhibitory responses after trigeminal nervestimulation. To our knowledge, these muscles havenot been investigated previously, perhaps due totechnical difficulties in their selective activation andrecording. The absence of inhibitory responses inthe frontalis, orbicularis oculi, orbicularis oris, andmentalis muscles confirms the results of previousstudies.6,26 Also, the finding of a partial silent periodin the orbicularis oculi muscle agrees with previousdata.11,23 This inhibitory phenomenon shows differ-ent characteristics from the silent periods observedin the lower facial muscles, since the EMG reductionwas partial and always related to the R2 response ofthe blink reflex.
In other muscles (e.g., masseter, limb muscles),the intensity and duration of inhibition relates to thelevel of contraction preceding the stimulus.19 In thepresent experiments, a quantitative study of the pre-activation level was not performed because of diffi-culties in mantaining the selective activation of indi-vidual muscles while changing the contraction level.A test with very slight contraction levels was per-formed anyway to exclude the possibility that theinhibition depends on the preactivation level.
SP2 parameters were influenced by stimulus in-tensity. The recruitment curves showed that athigher intensities the duration of the SP increased,presumably because a larger number of fibers, prob-ably not only large-diameter A-beta fibers but alsosmaller diameter (A-delta) fibers, were recruited.
Various control experiments were performed inorder to confirm that the observed inhibitory re-sponses in the lower facial muscles could be attrib-uted to stimulation of the trigeminal cutaneous af-ferents. The reflex inhibition was not present afterstimulation of the cervical skin or the median nerve,excluding a role for remote exteroceptive stimula-tion. Acoustic stimulation was also ineffective in in-ducing a SP in facial muscles, ruling out the involve-ment of nonsomesthetic stimuli and possiblerelationships with a startle response. On the otherhand, the facial muscles, which obviously are in-vaded by the cutaneous stimulation used, are consid-ered devoid of sensory nerve endings.25
The SPs observed in the present report differedfrom the EMG suppression observed after the M re-sponse induced by direct stimulation of the facialnerve. The latter was of shorter duration (<30 ms),usually partial, and occurred at shorter latencies, im-
FIGURE 4. Recruitment curve of the SP2 in the LLS muscle afterstimulation of the contralateral supraorbital nerve at increasingintensity. (A) SP2 duration in three subjects. Data plotted are themean of 10 rectified consecutive traces. (B) Rectified curves inone subject (case 3); each trace is the mean of 10 rectified con-secutive traces. Notice the appearance of a well defined SP2 at2 × Th stimulation intensity. LLS, levator labii superioris muscle;SP2, late silent period; Th, perceptive threshold.
Facial Muscles Silent Periods MUSCLE & NERVE June 2000 943

mediately after the M response; it may be due topostexcitatory and post-twitch inhibition.6,26
Facial nerve stimulation at the ear lobe evokedonly a post-M response silent period in the orbicu-laris oculi, orbicularis oris, and mentalis muscles. Inlevator labii superioris, depressor anguli oris, anddepressor labii inferioris, it induced an additional,late and long-lasting SP comparable to that obtainedafter stimulation of trigeminal branches. Spread ofthe stimulating current to cutaneous trigeminal af-ferents may be responsible. Further investigation ofthis point, e.g., by anesthetizing the infraorbital andmental nerves, has not been performed.
The latency and duration of the SP2 in the facialmuscles were similar to those in jaw-closing musclesafter stimulation of the second and third trigeminalbranches.3,4,5,14,21 Therefore, it might be speculatedthat similar afferents and synaptic organization un-derly both phenomena. In jaw-closing muscles, a bi-lateral early inhibition (SP1) with a latency of 10–15ms is evoked whereas, in the present experiments,SP1 with a longer latency (16–20 ms) and mainly inlower perioral muscles (i.e., depressor anguli orisand depressor labii inferioris) was observed. Similarto observations in jaw-closing muscles,7,8 the pres-ence of SP1 depended more on the stimulated tri-geminal branch than the presence of SP2. Neverthe-less, SP2 was preferentially induced in the depressoranguli oris and depressor labii inferioris muscles bymental nerve stimulation and in levator labii superi-oris by supraorbital nerve stimulation.
The inhibition of jaw-closing muscles is assumedto be protective of intraoral structures and to have arole in the fine control of mastication and speech,because it is evoked both by intra-oral and cutaneousstimulation. The SP in facial muscles was elicitedonly by exteroceptive stimuli; intra-oral stimulationwas totally ineffective. In this regard, recent work hasshown a role for cutaneous mechanoceptors as pu-tative proprioceptors of facial muscles during goal-oriented lip actions.2 The facial muscles in which wedescribe a silent period all produce lip movementscharacterized by retraction of the mouth.
The notion of nonhomogeneous reflex behaviorof facial muscles, suggested in the present work, issupported also by recent anatomical studies that in-vestigated the innervation pattern of human facialmuscles and compared it with that of skeletalmuscles.13 Numbers and locations of motor end-plates varied from muscle to muscle, but three mainpatterns were differentiated. In the orbicularis oculi,orbicularis oris, and buccinator muscles, the motorendplates were evenly spread over the muscles, ei-ther isolated or in a great number of small motor
zones. The levator labii superioris, levator angulioris, depressor labii inferioris, and depressor angulioris showed two to four motor zones distributed overthe muscle in eccentric positions. The zygomatic ma-jor and minor muscles showed a predominant motorzone located near the origin and two to three addi-tional small motor zones in an eccentric position.The mentalis muscle was not examined. This mor-phological heterogeneity of the facial muscles fol-lows closely the subgrouping that we observed on afunctional level. These subgroups could representindividual functional units.
REFERENCES
1. Aramideh M, Ongerboer de Visser B, VanderWerf F, Bour L,Brands J, Spielman J. The inhibitory response of the levatorpalpebrae muscle to evoked blink reflex. In: Valls-Sole J, To-losa E, editors. First European meeting on brainstem reflexesand functions. Barcelona: Litofinter S.A.; 1998. p 89–98.
2. Connor NP, Abbs JH. Movement-related skin strain associatedwith goal oriented lip actions. Exp Brain Res 1998;123:235–241.
3. Cruccu G, Agostino R, Lahuerta J, Manfredi M. Inhibition ofjaw-closing muscles by electrical stimulation of the ophthal-mic division in man. Brain Res 1986;371:298–304.
4. Cruccu G, Berardelli A, Inghilleri M, Manfredi M. Functionalorganization of the trigeminal motor system in man. Brain1989;112:1333–1350.
5. Cruccu G, Bowsher D. Intracranial stimulation of the trigem-inal nerve in man. II.Reflex responses. J Neurol NeurosurgPsychiatry 1986;49:419–427.
6. Cruccu G, Inghilleri M, Berardelli A, Romaniello A, ManfrediM. Cortical mechanisms mediating the inhibitory period aftermagnetic stimulation of the facial motor area. Muscle Nerve1997;20:418–424.
7. Cruccu G, Romaniello A. Jaw opening reflex after CO2 laserstimulation of the perioral region in man. Exp Brain Res1998;118:564–568.
8. Cruccu G, Romaniello A. Nociceptive and non-nociceptiveafferents for the two inhibitory periods in the human jaw-closing muscles. In: Valls-Sole J, Tolosa E, editors. First Euro-pean meeting on brainstem reflexes and functions. Barce-lona: Litofinter S.A.; 1998. p 215–225.
9. Di Lazzaro V, Quartarone A, Higuchi K, Rothwell JC. Shortlatency trigemino-cervical reflexes in man. Exp Brain Res1995;102:474–482.
10. Di Lazzaro V, Restuccia D, Nardone R, Quartarone A, TonaliP, Rothwell JC. Preliminary clinical observations on a newtrigeminal reflex: the trigeimino-cervical reflex. Neurology1996;46:479–485.
11. Elek JM, Dengler R, Hermans R, Struppler A. Silent perods insingle orbicularis oculi motoneurones. ElectroencephalogrClin Neurophysiol 1988;70:370–373.
12. Ertekin C, Celebisoyand N, Uludag B. Trigemino-cervical re-flexes in normal subjects. J Neurol Sci 1996;143:84–90.
13. Happak W, Liu J, Burggasser G, Flowers A, Gruber H,Freilinger G. Human facial muscles: dimensions, motor end-plate distribution, and presence of muscle fibers with mul-tiple motor endplates. Anat Rec 1997;249:276–284.
14. Hoffman P, Tonnies J. Nachweis des vollig konstantenvorkommens des zungen-Kiefer-reflexes beim menschen.Pfluger Arch 1948;250:103–108.
15. Hopf H. Clinical implications of testing brainstem reflexesand corticobulbar connections in man. In: Kimura J, Shi-
944 Facial Muscles Silent Periods MUSCLE & NERVE June 2000

basaki H, editors. Recent advances in clinical neurophysiol-ogy. Amsterdam: Elsevier; 1996 p 39–47.
16. Hopf H. Topodiagnostic value of brainstem reflexes. MuscleNerve 1994;14:326–330.
17. Kimura J. Electrodiagnosis in diseases of nerve and muscle:principles and practice. Philadelphia: Davis; 1983. p 323–351.
18. Kugelberg E. Facial reflexes. Brain 1952;75:385–396.19. Lavigne G, Frysinger R, Lund J. Human factors in the mea-
surement of the masseter silent period. J Dent Res 1983;62:985–988.
20. Ongerboer de Visser BW, Cruccu G, Manfredi M, KoelmanJH. Effects of brainstem lesions on the masseter inhibitoryreflex. Functional mechanisms of reflex pathways. Brain 1990;113:781–792.
21. Ongerboer de Visser BW, Goor C. Cutaneous silent period in
masseter muscles: electrophysiological and anatomical data. JNeurol Neurosurg Psychiatry 1976;39:674–679.
22. Overend W. Preliminary note on a new cranial reflex. Lancet1896;1:619.
23. Sanes JN, Ison J. A silent period in orbicularis oculi muscles ofhumans. J Neurol Neurosurg Psychiatry 1980;43:504–509.
24. Topka H, Hallett M. Perioral reflexes in orofacial dyskinesiaand spasmodic dysphonia. Muscle Nerve 1992;15:1016–1022.
25. Vander Werf F. Autonomic and sensory innervation of someorbital structures in the primate. Amsterdam: University ofAmsterdam, The Netherlands; 1993.
26. Werhahn KJ, Classen J, Benecke R. The silent period inducedby transcranial magnetic stimulation in muscles supplied bycranial nerves: normal data and changes in patients. J NeurolNeurosurg Psychiatry 1995;59:586–596.
Facial Muscles Silent Periods MUSCLE & NERVE June 2000 945