Embed Size (px)
Citation preview


Clinical Manualof
Trigeminal Neuralgia
CMTN 8023-Prelims.qxd 2/1/2007 8:48 PM Page i

CMTN 8023-Prelims.qxd 2/1/2007 8:48 PM Page ii

Clinical Manualof
Trigeminal Neuralgia
by
M Alan Stiles DMDThomas Jefferson University Hospital
Department of Oral and Maxillofacial SurgeryPhiladelphia, PA
USA
Somsak Mitrirattanakul DDS PhDInstructor, Faculty of Dentistry
Mahidol UniversityBangkokThailand
James J Evans MDThomas Jefferson University HospitalDepartment of Neurological Surgery
Philadelphia, PAUSA
CMTN 8023-Prelims.qxd 2/1/2007 8:48 PM Page iii

© 2007 Informa UK Ltd
First published in the United Kingdom in 2007 by Informa Healthcare, 4 Park Square, Milton Park, Abingdon, OxonOX14 4RN. Informa Healthcare is a trading division of Informa UK Ltd. Registered Office: 37/41 Mortimer Street,London W1T 3JH. Registered in England and Wales Number 1072954.
Tel.: +44 (0)20 7017 6000Fax.: +44 (0)20 7017 6336E-mail: [email protected]: www.informahealthcare.com
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in anyform or by any means, electronic, mechanical, photocopying, recording, or otherwise, without the prior permissionof the publisher or in accordance with the provisions of the Copyright, Designs and Patents Act 1988 or under theterms of any licence permitting limited copying issued by the Copyright Licensing Agency, 90 Tottenham CourtRoad, London W1P 0LP.
Although every effort has been made to ensure that all owners of copyright material have been acknowledged in thispublication, we would be glad to acknowledge in subsequent reprints or editions any omissions brought to our attention.
Although every effort has been made to ensure that drug doses and other information are presented accurately in thispublication, the ultimate responsibility rests with the prescribing physician. Neither the publishers nor the authorscan be held responsible for errors or for any consequences arising from the use of information contained herein. Fordetailed prescribing information or instructions on the use of any product or procedure discussed herein, pleaseconsult the prescribing information or instructional material issued by the manufacturer.
A CIP record for this book is available from the British Library.Library of Congress Cataloging-in-Publication Data
Data available on application
ISBN-10: 1 84214 253 4ISBN-13: 978 1 84214 253 0
Distributed in North and South America byTaylor & Francis6000 Broken Sound Parkway, NW (Suite 300)Boca Raton, FL 33487, USA
Within Continental USATel: 1 (800) 272 7737; Fax: 1 (800) 374 3401Outside Continental USATel: (561) 994 0555; Fax: (561)361 6018E-mail: [email protected]
Distributed in the rest of the world byThomson Publishing ServicesCheriton HouseNorth WayAndover, Hampshire SP10 5BE, UKTel.: +44 (0)1264 332424Email: [email protected]
Composition by C&M Digitals (P) Ltd, Chennai, IndiaPrinted and bound in India by Replika Press Pvt Ltd
CMTN 8023-Prelims.qxd 2/1/2007 8:48 PM Page iv

Contents
Preface vii
1 Evaluation of the facial pain patient 12 Differential diagnosis of trigeminal neuralgia 73 Pathogenesis and clinical approach to trigeminal
neuralgia treatment 354 Medical management of trigeminal neuralgia 615 Surgical management of (classic/typical/idiopathic) trigeminal
neuralgia 736 Treatment of refractory trigeminal neuralgia 87
Index 97
v
CMTN 8023-Prelims.qxd 2/1/2007 8:48 PM Page v

CMTN 8023-Prelims.qxd 2/1/2007 8:48 PM Page vi

vii
Preface
Trigeminal neuralgia is not the most common painful affliction of the face;however, it may be the most severe. Individuals who have experienced evenone of these cataclysmic episodes state that their lives are forever changed.They remember their first attack as if it were yesterday. Women say thattrigeminal neuralgia attacks eclipse even the pain of childbirth. The fear ofthe next attack haunts these unfortunate individuals, and some even considerdeath a viable alternative to life with these attacks.
The Clinical Manual of Trigeminal Neuralgia is written to enhance theknowledge of clinicians who treat patients with trigeminal neuralgia: to bettertheir working knowledge of the diagnosis, the disease, the medications nowbeing prescribed, and the neurosurgical techniques that are available, and tooffer ideas for the more refractory cases. It is written so that patients will beable to read these chapters and increase their knowledge of the treatmentoptions that are available to them.
Chapters 1 and 2 cover the evaluation and differential diagnosis of the patientwith facial pain. Chapter 3 reviews the pathophysiology of trigeminal neural-gia. Chapters 4 and 5 cover the medical management and surgical manage-ment, respectively, and chapter 6 presents additional ideas for refractory cases.
Our desire in writing this book was to enable clinicians to more easily recog-nize and diagnose trigeminal neuralgia. The disorder often goes unrecog-nized or is mistaken for other causes of facial pain, and this misdiagnosisleads to unsuccessful treatments and prolonged suffering. When cliniciansare familiar with the diagnosis of trigeminal neuralgia and the newest med-ications and advancements in surgical techniques, patients will be diagnosedearlier and have more treatment options than ever.
CMTN 8023-Prelims.qxd 2/1/2007 8:48 PM Page vii

It was our own patients’ persistent efforts to overcome the pain of trigeminalneuralgia that inspired us to write this book, and if it achieves its goals, thentrigeminal neuralgia patients everywhere shall benefit.
MAS, SM, JJE
viii
CMTN 8023-Prelims.qxd 2/1/2007 8:48 PM Page viii

IntroductionFacial pain is a symptom that has many possible origins; therefore, a thoroughhistory must be obtained to discern the nature of the facial pain, whether it beacute or chronic. Although a plethora of benign causes of facial pain exist,more ominous or secondary causes, such as infections, tumors, sinus disease,dental disease, brain tumors, strokes, and cardiac conditions, which all mayhave facial pain aspects in their symptomatology, need to be ruled out.
After taking a thorough history, a careful physical examination must becarried out. If any suspicious aspects arise during the history taking or physicalexamination, diagnostic studies are warranted. After excluding secondarycauses, the subjective symptoms are assigned a diagnostic category basedon accepted criteria (Figure 1.1). There may be more than one disorder causingthe patient’s pain in the head and face area.
1
Evaluation of the facial painpatient
HistoryClinical
examination
Diagnostictesting
DiagnosisDiagnosis
Figure 1.1 Pain diagnosis.
1
01-CMTN 8023.qxd 2/1/2007 7:37 PM Page 1

History taking Since there are very few diagnostic tests for the many primary causes offacial pain, a careful history is extremely important. The history takingallows the patient and the doctor to establish a rapport. Each element of thehistory should be systematically addressed when evaluating a patient (Figure1.2). The interview is specific and detailed and once completed allows thephysician to make further decisions about ordering diagnostic testing andwhat areas of the physical examination need to be emphasized. In trigeminalneuralgia the history is often the means by which the disease is diagnosed.
Chief complaintThe chief complaint uses the patient’s own words to state why he or she haspresented for an evaluation; in other words, the main reason for the consulta-tion. This is not all inclusive, but rather offers insight into the patient’s beliefof where the pain is originating.
History of present illnessOften confused with the current symptoms, this component is extremelyimportant in piecing together the puzzle of how the patient arrived at where
2
Figure 1.2 Pain history.
■ Chief complaint
■ History of present illness
■ Current symptons:
– Onset
– Location
– Quality
– Intensity
– Frequency
– Duration
– Aggravating and alleviating factors
– Concomitant or associated features
– Past treatments
01-CMTN 8023.qxd 2/1/2007 7:37 PM Page 2

he or she is today. The history of present illness represents the chronologicalsequence of events that led up to the pain onset and everything the patient hasundergone since the onset: when it was initiated, who was consulted, whatimaging and blood work has been carried out, what diagnosis was made, andwhat treatments were rendered. The results, positive or negative, of each ofthese events are extremely important. This is the patient’s story, and when thepain complaint is chronic the story can be very lengthy and confusing. Thisportion of the history must be guided by the physician to achieve as accurate atimeline as possible. It may require further investigation once the history hasbeen completed, and previous records and test results may need to be col-lected before a diagnosis can be made or therapy begun.
Current symptomsThe following subcategories need to be explored.
Onset
The onset of the pain (when it began) is very important in determiningwhether the chief complaint is chronic or acute. The onset identifies any ini-tiating events, such as trauma or infections, or it may be revealed that thepain was spontaneous in onset.
Since the pain may have changed location or pattern since the onset, thisinformation lays the foundation for the following components.
Location
The location of the pain helps identify potential sources. It may also be criti-cal in determining the diagnosis. Some pain syndromes have pain that islocation-specific and others have pain that varies in location. The exact loca-tion of the pain should be well documented and the structures in that regionmust be examined to rule out secondary local causes for the pain.
Quality
The quality of the pain that the patient is experiencing indicates its poten-tial cause. Neuropathic pain is usually burning or electrical in nature,whereas the pain of migraine is achy to throbbing. Descriptive terms,such as achy, burning, throbbing, sharp, shooting, etc., should be used todescribe the pain. The pain may have many components, and these maychange with time. It may start with one characteristic and change over time
3
01-CMTN 8023.qxd 2/1/2007 7:37 PM Page 3

or as it intensifies. The patient may need to be presented with a list ofdescriptions to choose from, and if the patient does not speak English, it isimportant that a person who is fluent in the patient’s native language isavailable to translate.
Intensity
Pain intensity is another descriptive term that works to quantify the amountof pain being experienced. Visual analog scales, number scales, or termssuch as mild, moderate, or severe may be used. These quantifications can beimportant in diagnosing the pain as well as evaluating the patient’s responseto treatments.
Frequency
The temporal behavior of the pain establishes a pain pattern. The pain isintermittent if the patient experiences pain-free intervals. The pain is contin-uous if the patient has no pain-free times. If the pain is intermittent, the fre-quency with which the patient experiences it helps to further quantify thepain and hone in on a diagnostic category. Frequency is so variable thatpatients may have multiple attacks of pain in 1 hour or 1 day; and somepatients may have just one episode per month.
Duration
The duration of the pain is dependent on the frequency. If the frequency iscontinuous, then the duration is truly non-stop. It may become evident thatthe patient has more than one type of pain, with a continuous baseline painand periods of exacerbation of a specific duration overlying the baseline. Ifthe pain frequency is intermittent, then the duration of the painful episodes isclearer. Some pain conditions may last for as short a time as 1 second andothers may last for days to months.
Alleviating and aggravating factors
Many pain syndromes have aggravating factors or triggers. These are oftenspecific for certain types of disorders and may help not only in diagnosingthe disorder but also in developing adequate treatment plans. Alleviating fac-tors are also important, for what helps some pains may have adverse effectson others, and again may help identify the diagnosis.
4
01-CMTN 8023.qxd 2/1/2007 7:37 PM Page 4

Concomitant or associated features
Many pain syndromes have associated features during an episode. Thesefeatures are too numerous to list, but may include nausea, vomiting, auto-nomic features, involuntary movements, visual changes or disturbances,sensitivity to lights or sounds, etc. Again, all of these symptoms that accom-pany the episodes of pain may not be recognized as part of the pain syndromeby the patient and are too numerous to be fully investigated by the history-taker, and it may be helpful to have the patient review a list of possibilities.
Past treatments
Past treatments and the results of these treatments can be very helpful indetermining the diagnosis and possible future therapies. Obtaining this infor-mation may require one to request past records and reports to determineexactly which medication, what dosage, dosage scheme, etc. was tried in thepast. One may discover that the patient has had a partial response or anadverse reaction to certain therapies, and this information would be helpfulin making future treatment choices.
Medical, family, psychosocial history, and review of systems
A thorough medical history should also be taken to help identify any othersystemic illnesses, either diagnosed or undiagnosed, and a psychosocialhistory may identify underlying psychological conditions that may need tobe addressed.
Physical examinationAfter completing a thorough history, a physical examination is performed.The examination should include a neurologic examination, a myofascialexamination of the head and neck, an intraoral examination, evaluation ofneck and jaw movements, and a fundoscopic evaluation. Any abnormalitiesmust be viewed in the context of the history, and then diagnostic testingshould be performed.
Diagnostic testingMany radiographic options exist, depending on the region or structures beinginvestigated. If systemic disease is suspected, laboratory testing or bloodwork may be needed. Before using certain therapies, some testing, such as
5
01-CMTN 8023.qxd 2/1/2007 7:37 PM Page 5

cardiac clearance or an electrocardiogram (EKG), may need to be done whenpatients are over 50 years of age or have a positive family history. The exacttests that should be done vary greatly depending on the patient’s presenta-tion. If abnormalities are found during the history taking or on examination,secondary causes must be ruled out, and this can be accomplished withdiagnostic testing (Figure 1.3).
6
Figure 1.3 Abnormalities in history or examination that require further diagnostic testing.
■ New onset of pain
■ Recent changes in cognition or personality with onset of pain
■ Rapid increase in pain
■ New onset of pain in patients with systemic illnesses such as cancer or HIV
infection
■ Pain onset in patients greater than 50 years old
■ Abnormalities on neurologic examination
■ Stiff neck or fever with pain
■ Pain exacerbated or brought on by exertion
■ An unexplainable change in pain pattern
■ A sudden, unrelenting increase in the pain
■ Abnormal range of motion of neck or jaw
■ Pain provoked specifically by jaw or neck movements
01-CMTN 8023.qxd 2/1/2007 7:37 PM Page 6

Diagnostic criteria for trigeminal neuralgiaThe clinical hallmark of trigeminal neuralgia is a sudden, excruciatingparoxysm of pain in the distribution of the trigeminal, or fifth cranial nerve.1
The paroxysmal pain of trigeminal neuralgia is initiated by innocuous stimu-lation of discrete areas, the so-called ‘trigger zones’, which concentrate nearthe lower central portion of the face (cheek, chin, lips, or tongue). Themedian age at diagnosis is 67 years.2 The diagnosis of trigeminal neuralgiadepends strictly on clinical criteria.3 There is no objective laboratory orpathological test for diagnosis.
DefinitionTrigeminal neuralgia is defined by the International Association for the Studyof Pain3 as ‘a sudden, usually unilateral, severe, brief, stabbing, recurrentpain in the distribution of one or more branches of the fifth cranial nerve.’ TheInternational Headache Society (IHS)4 classified trigeminal neuralgia intotwo types: classical and symptomatic. Classical trigeminal neuralgia is a uni-lateral disorder characterized by brief electric, shock-like pains. They areabrupt in onset and termination and limited to the distribution of one or moredivisions of the trigeminal nerve. Small areas in the nasolabial fold and/orchin (trigger zones) may be particularly susceptible to the precipitation ofpain. The pains may remit for variable periods of time. The pain of the symp-tomatic type is indistinguishable from the classical type that is caused bya demonstrable structural lesion other than vascular compression. The IHSsuggested criteria for the diagnosis of trigeminal neuralgia4 (Table 2.1).
Diagnosis of trigeminal neuralgiaDespite the availability of diagnostic criteria, problems exist in diagnosing andassessing trigeminal neuralgia. The rare incidence of trigeminal neuralgia, the
7
2Differential diagnosis oftrigeminal neuralgia
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 7

lack of objective tests, and the range of facial pain syndromes make diagnosisdifficult for health-care providers who are not familiar with this disorder.One study of referral patterns for facial pain of all types found that patientssought help from an average of 4.88 providers before being referred to a painclinic. During the referral process, about 70% saw a general dentist or adental specialist, and about 30% saw a physician.5 Currently, no study hasspecifically examined either referral patterns for trigeminal neuralgiapatients or the accuracy of diagnosis. Few studies have provided detailedassessment of the sensory features of trigeminal neuralgia and the nature oftriggering stimuli. Pioneering studies were conducted by Kugelberg and
8
Table 2.1 IHS diagnostic criteria for trigeminal neuralgia
Classic trigeminal neuralgia
A. Paroxysmal attacks of facial or frontal pain that last a few seconds to less than 2
minutes, affecting one or more divisions of the trigeminal nerve and fulfilling criteria
B and C.
B. Pain has at least one of the following characteristics:
1. Intense, sharp, superficial or stabbing
2. Precipitated from trigger areas or by trigger factors
3. The patient is entirely asymptomatic between paroxysms.
C.Attacks are stereotyped in the individual patient.
D.There is no clinically evident neurological deficit.
E. Not attributed to another disorder.
Symptomatic trigeminal neuralgia
A. Paroxysmal attacks of pain lasting from a fraction of a second to 2 minutes, with
or without persistence of aching between paroxysms, affecting one or more
divsions of the trigeminal nerve and fulfilling criteria B and C.
B. Pain has at least one of the following characteristics:
1. Intense, sharp, superficial or stabbing
2. Precipitated from trigger areas or by trigger factors
3. Attacks are stereotyped in the individual patient
4. A causative lesion, other than vascular compression, has been demonstrated
by special investigations and/or posterior fossa exploration.
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 8

Lindblom.6 Dubner et al7 identified the prominent clinical features asfollows: (1) triggering only by non-noxious, mechanical stimuli; (2) tempo-ral summation of trigger stimuli; (3) afterdischarge; (4) migration of triggerzone; (5) spatial radiation; and (6) trigger zone outside of affected trigeminalbranch. There is scant assessment of abnormalities in sensory thresholds.While sensory loss (hypoesthesia) is detected in 37% of patients referred toneurosurgeons,8 the degree is minimal enough to be overlooked during rou-tine neurologic examination.3,7 Provoking factors are strong predictors forthe presence of trigeminal neuralgia. The provoking factors most frequentlyreported are chewing and talking (76%), whereas in idiopathic facial pain thecorresponding figures are much lower at 24%. Trigger areas (zones) arereported in 50% of patients with trigeminal neuralgia and in only 9% ofpatients with idiopathic facial pain.9
Most patients have idiopathic trigeminal neuralgia; as many as 15% ofpatients may have an underlying cause or symptomatic trigeminal neuralgia.4
Secondary causes of trigeminal neuralgia include benign or malignanttumors of the posterior fossa10 or multiple sclerosis (MS).11 In their reviewof patients with facial pain who were seen at the Mayo clinic from 1976 to1990, Cheng et al.12 studied 2972 patients with trigeminal neuralgia, 296(10%) of whom had tumors. Of these 296 patients, only 58 (2% of totalpatients included in the study) had classic trigeminal neuralgia with noobjective motor or sensory deficit. However, their ages were youngerthan the average age of patients with idiopathic trigeminal neuralgia.Nevertheless, neurologic deficit later developed in 47% of patients withsymptomatic trigeminal neuralgia. The neurologic signs did not involve justthe trigeminal nerve, but also other cranial nerves or central effects.Although many of these patients responded initially to medical and surgicaltreatment, all experienced relapses. Most of the tumors were meningiomas ofthe posterior fossa. Puca et al.13 reviewed patients with middle and posteriorfossa tumors and found that 33% of patients presented with classic trigemi-nal neuralgia. MS has also been identified as a risk factor for trigeminal neu-ralgia.2 In a population of 1882 patients with MS, Hooge and Redekop14
identified 35 patients (1.9%) with trigeminal neuralgia. In this group of MSpatients with trigeminal neuralgia they found a younger age and a higherincidence of bilateral cases (14%). It is not unusual for patients to have twopossible secondary causes. Using magnetic resonance imaging (MRI) scan-ning, Meaney et al.15 demonstrated that seven patients with MS and trigemi-nal neuralgia had either tumors or vascular compression in addition to
9
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 9

plaques of MS. Familial history of trigeminal neuralgia has been reported,16
and there is a small cluster of patients who may have Charcot-Marie-Toothneuropathy.17
Differential diagnosisTrigeminal neuralgia commonly presents as a unilateral pain. Only 3% ofpatients presented with bilateral symptoms and in most cases the symptomsdid not occur at the same time. The differential diagnosis of trigeminal neu-ralgia should focus on those that presented as unilateral orofacial pain.18
However, many of the differential causes of orofacial pain may also havebilateral symptomatology, and uncommon unilateral presentation can bemisleading. The first attack of trigeminal neuralgia is often sudden in onsetand can mimic dental pain. Patients often assume that their pain is due todental causes and seek dental therapy as a first line of treatment.19 Sincedental pain is very common, this is a valid assumption. However, it is impor-tant that dentists should be open to non-dental causes of pain and notattempt irreversible procedures in the absence of clear dental pathology.Table 2.2 lists the conditions that should be considered for differential diag-nosis of trigeminal neuralgia.
Trigeminal neuralgia may also present exclusively intraorally, which can beconfusing for patients and clinicians. Zakrzewska18 lists some of the types oforofacial pain that need to be considered when there is no obvious immediatecause, such as an infection or trauma (Table 2.3).
An entity of pretrigeminal neuralgia has also been described20 that with timebecomes classic trigeminal neuralgia. This condition can present considerablediagnostic difficulties. The pain is very similar to the pain caused by dentaldisease. In some cases the diagnosis of pretrigeminal neuralgia has to awaitthe paroxysms of true trigeminal neuralgia.20
Secondary trigeminal neuralgia It is important to repeat neurologic examinations at intervals because theseabnormalities may become apparent with time, indicating that there is asecondary cause of trigeminal neuralgia.
Pain of dental originThe extreme variability of toothache is such that a good rule for any exam-iner is to consider all pains about the mouth and face to be of dental origin
10
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 10

until proven otherwise.21,22 Pains arise from the pulp and the periodontaltissues are inflammatory in nature.
Pulpal pain
Pulpal pain may be classified as reversible or irreversible, depending uponthe extent of inflammation. Reversible pulpitis may be treated by removingthe irritant and restoring the defect adequately. Irreversible pulpitis does not
11
Table 2.2 Differential diagnosis of classic trigeminal neuralgia
1. Secondary trigeminal neuralgia
2. Pain of dental origin
a. Pulpal pain
b. Periodontal pain
c. Parafunction-induced alveolitis
d. Crack tooth syndrome
3. Extracranial
a. Sinusitis
b. Temporomandibular disorders
4. Neuropathic
a. Pretrigeminal neuropathy
b. Trigeminal neuropathy
c. Glossopharyngeal neuralgia
d. Postherpetic neuralgia
e. Peripheral neuritis
f. Nerve compression
5. Neurovascular
a. Migraine
b. Cluster headache
c. Short-lasting unilateral neuralgiform headache with conjunctival injection and
tearing (SUNCT)
d. Chronic paroxysmal hemicrania
e. Giant cell arteritis
6. Psychogenic
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 11

12
Tabl
e 2.
3 Co
nditi
ons
that
sho
uld
be c
onsid
ered
whe
n th
ere
is no
obv
ious
imm
edia
te c
ause
for o
rofa
cial p
ain
Loca
tion
and
Freq
uenc
y/Se
veri
ty/
Agg
rava
ting
Ass
ocia
ted
Con
ditio
nre
ferr
al p
atte
rndu
ratio
nqu
ality
fact
ors
feat
ures
Den
tal
Pulp
alPo
orly
loca
lized
In
term
itten
t/M
ild-m
oder
ate/
Ther
mal
/mec
hani
cal/
Dee
p ca
ries,
intr
aora
llyho
urs
dull
achi
ngch
emic
alfr
actu
red
toot
h
Perio
dont
alLo
caliz
ed t
o on
eIn
term
itten
t/M
ild-m
oder
ate/
Perc
ussio
n,pu
lpat
ion
Peria
pica
l,les
ion
or m
ore
teet
hm
inut
es t
o ho
urs
dull
achi
ngof
the
are
ash
ows
on r
adio
grap
h,
late
ral g
ingi
val p
us
and
toot
h ex
trus
ion
Para
func
tion-
Loca
lized
to
one
Inte
rmitt
ent
to
Mild
-mod
erat
e/O
cclu
sal f
orce
Evid
ence
of
indu
ced
or m
ore
teet
hco
ntin
uous
dull
achi
ngpa
rafu
nctio
n,e.
g.
alve
oliti
soc
clus
al w
ear,
tong
ue
and
chee
k rid
ging
Cra
cked
Lo
caliz
ed t
o on
e be
Inte
rmitt
ent/
very
M
oder
ate/
shar
pBi
ting,
neve
r Fr
actu
re m
ay b
e
toot
hor
mor
e te
eth,
may
sh
ort-
last
ing,
spon
tane
ous
very
fine
synd
rom
ebe
poo
rly lo
caliz
edse
cond
s
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 12

13
Tabl
e 2.
3(C
ontin
ued) Loca
tion
and
Freq
uenc
y/Se
veri
ty/
Agg
rava
ting
Ass
ocia
ted
Con
ditio
nre
ferr
al p
atte
rndu
ratio
nqu
ality
fact
ors
feat
ures
Ext
racr
ania
l
Sinu
sitis
May
be
unila
tera
l C
ontin
uous
pai
nA
chin
g an
d Be
ndin
g do
wn
Nas
al d
ischa
rge/
stuf
fy
or b
ilate
ral/o
ften
thro
bbin
g/ca
n fe
elin
g
radi
ates
to
uppe
r be
sev
ere
teet
h
TMD
May
be
bila
tera
l,In
term
itten
t/m
ay
Mild
–mod
erat
e/Ja
w fu
nctio
ns
Join
t so
unds
pain
may
be
last
sev
eral
hou
rs
dull
achi
ng(c
hew
ing,
yaw
ning
)(c
licki
ng,p
oppi
ng),
refe
rred
to
one
with
occ
asio
nal
tinni
tus,
vert
igo,
or m
ore
teet
hse
vere
exa
cerb
atio
nsbi
te c
hang
es
Neu
ropa
thic
Pret
rigem
inal
Loca
lized
to
one
Inte
rmitt
ent/
shor
t-M
ild–m
oder
ate/
Som
etim
es c
an b
e –
neur
algi
asid
e,gi
ngiv
al/t
ooth
la
stin
gdu
ll ac
hing
trig
gere
d by
ligh
t
area
touc
h
(con
tinue
d)
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 13

14
Tabl
e 2.
3(C
ontin
ued)
Loca
tion
and
Freq
uenc
y/Se
veri
ty/
Agg
rava
ting
Ass
ocia
ted
Con
ditio
nre
ferr
al p
atte
rndu
ratio
nqu
ality
fact
ors
feat
ures
Trig
emin
alLo
caliz
ed t
oIn
term
itten
tM
ild–m
oder
ate/
Ligh
t to
uch,
–
neur
opat
hygi
ngiv
al/t
ooth
cont
inuo
ussh
arp,
shoo
ting,
(allo
dyni
a)
area
(co
mm
only
dull,
burn
ing
unila
tera
l)
Glo
ssop
hary
ngea
lIn
trao
ral i
nIn
term
itten
t,la
stSe
vere
,sha
rpSw
allo
win
g,–
neur
algi
adi
strib
utio
n of
seco
nds
tost
abbi
ngch
ewin
g,ta
lkin
g
glos
soph
aryn
geal
min
utes
nerv
e
Post
herp
etic
Mos
t co
mm
on:
Con
tinuo
usSe
verit
y va
ried/
Ligh
t to
uch
Sens
ory
defic
it
neur
algi
a1s
t di
visio
n of
tingl
ing,
burn
ing
(allo
dyni
a)
trig
emin
al n
erve
Perip
hera
lLo
caliz
ed t
oC
ontin
uous
Seve
rity
varie
d/–
Infla
mm
atio
n of
the
neur
itis
trau
mat
ized
area
achi
ng a
nd b
urni
ngne
rve
pain
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 14

15
Tabl
e 2.
3 (C
ontin
ued)
Loca
tion
and
Freq
uenc
y/Se
veri
ty/
Agg
rava
ting
Ass
ocia
ted
Con
ditio
nre
ferr
al p
atte
rndu
ratio
nqu
ality
fact
ors
feat
ures
Ner
ve
Loca
lized
to
area
In
term
itten
t,da
ilyA
chin
g,m
ay b
e Ea
ting
with
den
ture
Ofte
n re
dnes
s,
com
pres
sion
of c
ompr
essio
n,sh
arp
if ov
er
ulce
ratio
n in
the
e.g.
men
tal n
erve
men
tal n
erve
area
of p
ress
ure
Neu
rova
scul
ar
Mig
rain
eU
nila
tera
l,tem
pora
l In
term
itten
t–M
oder
ate–
seve
re/
Phys
ical
act
ivity
Phot
o/ph
onop
hobi
a
front
alco
ntin
uous
thro
bbin
g>
stea
dyN
ause
a/vo
miti
ng
ache
Osm
opho
bia,
scot
omat
a,
neur
olog
ical
def
icits
Clu
ster
O
rbita
l,sup
raor
bita
l,15
–180
min
utes
to
Seve
re/p
unct
ate,
Seas
onal
/alti
tude
C
onju
nctiv
al in
ject
ion,
tem
pora
lse
vera
l hou
rs/o
ne
stab
bing
chan
ges,
alco
hol
lacr
imat
ion,
nasa
l
ever
y ot
her
day
to
cong
estio
n,
eigh
t pe
r da
yrh
inor
rhea
,sw
eatin
g,
mio
sis,p
tosis
,eye
lid
edem
a
(con
tinue
d)
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 15

16
Tabl
e 2.
3 (C
ontin
ued)
Loca
tion
and
Freq
uenc
y/Se
veri
ty/
Agg
rava
ting
Ass
ocia
ted
Con
ditio
nre
ferr
al p
atte
rndu
ratio
nqu
ality
fact
ors
feat
ures
SUN
CT
Ocu
lar,
perio
cula
rIn
term
itten
t,ea
ch
Seve
re/b
urni
ng,
Nec
k m
ovem
ent
Con
junc
tival
inje
ctio
n,
may
rad
iate
to
episo
de la
sts
up
elec
tric
al,s
tabb
ing
lacr
imat
ion,
nasa
l
front
otem
pora
l to
2 m
inut
es s
ever
al
stuf
fines
s,rh
inor
rhea
,
area
,upp
er ja
w
atta
cks
per
day
and
pala
teth
en m
ay r
emit
CPH
Eye,
fore
head
5–10
att
acks
dai
ly/
Stab
bing
,thr
obbi
ng,
Hea
d m
ovem
ents
Con
junc
tival
inje
ctio
n,
last
2–4
5 m
inut
esbo
ring
lacr
imat
ion,
nasa
l
stuf
fines
s,rh
inor
rhea
,
Gia
nt c
ell
May
be
bila
tera
l,In
term
itten
t,th
en
Ach
ing,
thro
bbin
g,C
hew
ing
Tend
er s
calp
art
erie
s,
arte
ritis
Tend
erne
ss o
ver
cont
inuo
usbo
ring,
shar
pja
w c
laud
icat
ion,
neck
tem
pora
l art
ery
pain
,ano
rexi
a,vi
sual
sym
ptom
s,
poly
mya
lgia
rheu
mat
ica
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 16

have the reparative ability to heal on removal of the irritant, hence the needfor endodontic procedures.
Reversible pulpitis is characterized by a short-lasting pain sensation when anirritant, such as ice, is applied. This pain is present for the duration of thestimulus, and is not spontaneous in nature. Irreversible pulpitis, however,may be spontaneous or provoked and possesses tremendous variability in itsclinical presentation. It may be sharp or dull, continuous or episodic, local-ized or diffuse.23 Pulpal necrosis often ensues, and the tooth may be tender topercussion if the periapical region is involved. At this stage the tooth is usu-ally non-responsive to thermal stimuli. Pulpitis in multi-rooted teeth may beconfusing, as a variety of symptoms may be reported, due to the coexistenceof vital and non-vital tissue in the pulp.
Periodontal pain
Periodontal pain is usually readily identified through the action of the propri-oceptors in the periodontal ligament. The pain is related to biomechanical(masticatory) function and responds to provocation proportionately and ingraduated increments rather than as a threshold response like pulpal pain. Itdoes not pose as significant a problem as pulpal pain due to the ability ofperiodontal receptors to accurately localize the source of pain.
Parafunction-induced alveolitis
This condition usually involves several teeth, especially opposing teeth with-out any obvious gross disease. It commonly has the characteristics of peri-odontal pain. The common cause of this condition is overstressing fromparafunction such as clenching and bruxism.
Crack tooth syndrome
Some forms of pulpal pain are difficult to identify. Cracked teeth pose suchproblems. Teeth with cracks tend to have erratic pain on mastication.Generally, there is no pain to percussion, radiographs are inconclusive, andthere may or may not be pain to temperature extremes. Tooth cracks may bedifferentiated into craze lines, fractured cusps, cracked teeth, split teeth, andvertical root fractures. To diagnose a crack, one needs to take a careful dentalhistory and conduct subjective visual and tactile examinations, bite tests, peri-odontal probing, staining, transillumination, and radiographs. Unfortunately it issometimes necessary to remove restorations or surgically assess for the pres-ence of cracks to be confirmed.
17
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 17

Extracranial
Sinusitis
The apices of maxillary molar and premolar teeth are intimately related tothe maxillary sinus.24 This is patently clear on examination of periapicalradiographs of this region and when an oro-antral fistula is created, aftereven a benign extraction.
Maxillary sinusitis may be acute or chronic, and both varieties may mimicodontogenic pain. Acute sinusitis is usually secondary to a pyrogenic bacter-ial infection; chronic sinusitis is more prevalent and tends to be allergic innature. Sinusitis is caused by a blockage of drainage from the osteomeatalcomplex. The inflammation leads to ciliary dysfunction and retentionof mucous membrane secretions, which leads to bacterial invasion andovergrowth.
Typically a patient will complain of a constant, dull, aching or throbbing, pres-sure-like sensation in the maxillary posterior teeth. If the sinusitis is a conse-quence of a bacterial infection, the symptom tends to be more severe. Key signsand symptoms are those of sepsis: fever, chills, malaise and an elevated leuko-cyte count. An important diagnostic characteristic is that the pain is not locatedin one particular tooth, but tends to involve all molar and premolar teeth in thatquadrant. The teeth may exhibit percussion sensitivity and often patients willcomplain of chewing discomfort and cold sensitivity.25 Additionally, when thehead is lowered to a level below the knees (a maneuver that results in gravita-tional shifting of fluid in the sinus), the pain is exacerbated. Patients who com-plain of such pain tend to have a history of upper respiratory tract infections,nasal congestion, sinus problems, rhinitis, rhinorrhea, and post nasal dripping.This may worsen during pregnancy and the patients tend to have recurrentepisodes, especially in the spring and autumn.26 These patients may complainof exaggerated pain upon changes in barometric pressure; thus high altitudesand flying will exacerbate their pain. There is also infraorbital tenderness uponpalpation over the affected sinus.
Other diagnostic approaches include the use of transillumination. A fiberopticlight beam is placed against the palate, and in a darkened room a clear sinuswill transilluminate. Antra that are filled with exudates are clouded and will nottransilluminate. A Waters’ radiograph may show an air–fluid level or thickenedmucosa in the sinus. Treatment usually consists of antibiotic and topical decon-gestants. Okeson and Bell27 summarized the clinical characteristics of sinus ornasal mucosal toothache as follows:
18
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 18

1. Pressure below the eyes2. Increased pain with lowering the head3. Increased pain with pressure over the involved sinus4. Local anesthesia of the tooth does not eliminate the pain5. Diagnosis confirmed when air/fluid level seen on appropriate imaging studies.
Temporomandibular disorders
The most common form of referred toothache involves the muscles of mas-tication and their surrounding fascia. Myofascial pain is described as aregional pain referred from or emanating around myofascial trigger points.A myofascial trigger point is a hyperirritable spot, usually within a tautband of skeletal muscle or in the muscle fascia, that is painful on compres-sion and can give rise to characteristic and predictable referred pain, ten-derness, and autonomic phenomena.22 Diagnosis is made by digitallypalpating the trigger point deeply and assessing the patient’s response. Thediagnosis is confirmed with a vapocoolant spray, muscle stretch, and triggerpoint injections. The muscles most frequently implicated in the referral ofpain into teeth include the masseter, the temporalis, and the anterior digas-tric. This has been extensively described and diagrammed by Travell andSimons.22,28
Okeson and Bell27 summarized the clinical characteristics of toothache as areferred pain from masticatory muscle as follows:
1. Non-pulsatile, more constant aching2. Not responsive to local provocation of the tooth3. Pain increases with function of involved muscle (trigger points)4. Local anesthesia of the tooth does not affect the toothache.5. Local anesthesia of the involved muscle (trigger points) reduces the toothache.
Neuropathic
Pretrigeminal neuralgia
Even though this condition does not appear in any formal diagnosis classifi-cation, it is an important condition to recognize. It is a prodromal dull, achingpain preceding the onset of classical trigeminal neuralgia. This condition wasfirst described in 1949 by Symonds29 as a dull, continuous ache that laterbecomes classic trigeminal neuralgia. It was called pretrigeminal neuralgiaby Mitchell,30 and Fromm et al.20 have subsequently described more patientswith this condition. However, the diagnosis is commonly made in retrospectand being treated as odontogenic pain or trigeminal neuropathy.
19
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 19

From studies by Mitchell30 and Fromm et al.,20 the condition has beendescribed in 62 patients. The age of onset is in the mid 50s and there is a slightfemale predominance. Patients described the pain as dull, aching, gnawing, orburning, or compared it to toothache or sinusitis. The severity varied frommild to severe. The pain of pretrigeminal neuralgia is usually unilateral andconfined to one division, often a small, specific part of the tooth-bearing areaof the mouth. The pain is sometimes intermittent. Each episode can last aslong as 3 hours, and there may be one or two episodes a day. Sometimes painis continuous and lasts for weeks. There also can be an episode of completeremission. In some patients, the prodromal pain evolves directly into trigemi-nal neuralgia over a period of weeks or months. However, in others there willbe a period of no pain and then trigeminal neuralgia may present 1–11 monthslater. The longest documented time before trigeminal neuralgia occurred was12 years. In about one-third of pretrigeminal neuralgia, pain can be provokedby light touch, such as eating or brushing the teeth, or by temperature varia-tion. Dental treatment may give temporary relief, but the pain may return asclassic trigeminal neuralgia. Patients with pretrigeminal neuralgia have report-edly responded to anticonvulsants commonly prescribed for classic trigeminalneuralgia patients (Table 2.4).31
Trigeminal neuropathy
Neuropathy of the trigeminal nerve is frequently confused with classictrigeminal neuralgia.18 Trigeminal neuropathy usually follows some type oftraumatic event or injury that leads to changes in the peripheral as well asthe central nervous system (CNS). This condition can be divided intoperipheral and central neuropathic pain. Peripheral trigeminal neuropathic
20
Table 2.4 Diagnostic criteria for pretrigeminal neuralgia
1. Moderately severe, dull, toothache-like pain
2. Unilateral, often one division of fifth cranial nerve
3. Intermittent, short-lasting
4. Provoked by light touch
5. Relieved by anticonvulsant
6. No obvious local pathology
7. Progress to trigeminal neuralgia
Adapted from Zakrzewska.31
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 20

pain is characterized by aching and/or burning pain of moderate intensity inan area where there has been previous extra- or intraoral nerve trauma.Chronic neuropathic pain can develop from trivial injury and it may be diffi-cult, in the oral environment, to associate a causal event with the subsequentpain, especially when the healing is completed. Procedures as simple as adental prophylaxis have been associated with the development of trigeminalneuropathy. Peripheral neuropathies are characterized by their response totopical and/or local anesthetic blocking. This is because pain due to periph-eral neuropathies should be eliminated by peripheral blocking, whereas painfrom a central neuropathy will not be affected by a peripheral block, sincethe pain-generating mechanism is within the CNS and not due to peripheralneuronal activity.32,33
Central neuropathic pain is characterized by lack of response to topical orlocal anesthetic blockade. In addition to the lack of response to anestheticblocking, dynamic mechanical allodynia, or pain when a non-painful mov-ing stimulus (such as a wisp of cotton) is brushed across the area of pain, ispresent. There may also be an exaggerated painful response to pinprick inthe area supplied by the damaged pain fibers. This response is termedhyperalgesia.32,33
Glossopharyngeal neuralgia
Glossopharyngeal neuralgia is an uncommon facial pain syndrome firstdescribed by Weisenburg in 1910.34 Its incidence is between 0.2% and 1.3%of trigeminal neuralgia.35 Symptoms typically begin after the sixth decade.Because the pain is felt in the sensory distribution of the glossopharyngealand vagus nerves, some use the term ‘vagoglossopharyngeal neuralgia’ forthis disorder. Like trigeminal neuralgia, it may go into remission.36
Glossopharyngeal neuralgia is a severe, transient, stabbing pain experiencedin the ear, the base of the tongue, the tonsillar fossa, or beneath the angle ofthe jaw. The pain is therefore felt in the distributions of the auricular and pha-ryngeal branches of the vagus nerve as well as of the glossopharyngeal nerve.It is commonly provoked by swallowing, talking, or coughing and may remitand relapse in the fashion of trigeminal neuralgia4 (Table 2.5).
Postherpetic neuralgia
Herpes zoster infection must be considered in the elderly patient who pres-ents complaining of toothache when no objective findings can explain thepain.37–39 The varicella/zoster virus produces two distinct clinical syndromes.
21
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 21

Varicella (chickenpox) is a highly contagious, generalized skin eruption, andzoster (shingles) is a less common occurrence in older and/or immunocom-promised individuals.40
Acute herpes zoster infection is caused by activation of the varicella virus,which lies dormant in sensory ganglia subsequent to chickenpox infection.While the majority of infections affect the dermatomes of T3 to L2, somepatients present with infections limited to the trigeminal nerve. The majorityof such infections affect the ophthalmic branch, but the maxillary andmandibular branches may also be involved.41
When the prodromal symptoms of pain mimic pulpal or other dental disor-ders, the practicing dentist is presented with a significant diagnosticchallenge.42 It is common for pain to be the only presenting symptom.43
Other complaints in this early stage, which may aid the diagnosis, includeitching, tenderness along the involved sensory nerves, fever, and generalizedmalaise. The pain is often described as burning, itching, or tingling in theskin over the affected nerve distribution, which may be accompanied by adeeper stabbing or aching neuralgia type of pain.
Within a few days, unilateral vesicular eruptions, which follow the anatomic dis-tribution of the involved nerve(s), appear. These vesicles rarely cross the mid-line. The vesicles rupture, ulcerate, and eventually form a crust and heal. It is
22
Table 2.5 IHS diagnostic criteria for classical glossopharyngeal neuralgia
A. Paroxysmal attacks of facial pain lasting from a fraction of a second to 2 minutes
and fulfilling criteria B and C
B. Pain has all of the following characteristics:
1. Unilateral location
2. Distribution within the posterior part of the tongue, tonsillar fossa, pharynx
or beneath the angle of the lower jaw and/or in the ear
3. Sharp, stabbing, and severe
4. Precipitated by swallowing, chewing, talking, coughing, and/or yawning
C.Attacks are stereotyped in the individual patient
D.There is no clinically evident neurological deficit
E. Not attributed to another disorder
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 22

easy to make an accurate diagnosis at this stage, so it is advisable, when onesuspects zoster early in the prodromal stages, to defer any invasive interventionsuntil one is sure of the definitive diagnosis. Treatment of acute infection involvesantiviral therapy (e.g. acyclovir), adequate pain control, adequate fluid intake,and possible steroid therapy (Table 2.6).
Peripheral neuritis
Neuritis is defined by the IASP as ‘Inflammation of a nerve or nerves (not tobe used unless inflammation is thought to be present)’.3,27 As would beexpected, local inflammation of a nerve would respond to topical and localanesthetics and would be characterized by aching and burning pain. This formof neuropathy does not include conditions due to neuropraxis, neurotmesis, ordeafferentation.
Neuroma
When a peripheral nerve is injured, the damaged terminal sprouts and growsperipherally to the structure it innervated. This process always occurswhen the peripheral nerve is damaged. If the neural sheath is damaged and
23
Table 2.6 IHS diagnostic criteria for postherpetic neuralgia
Description:
Facial pain persisting or recurring ≥ 3 months after the onset of herpes zoster
infection.
Diagnostic criteria:
A. Head or facial pain in the distribution of a nerve or nerve division and fulfilling
criteria C and D.
B. Herpetic eruption in the territory of the same nerve.
C. Pain preceded herpetic eruption by <7 days.
D. Pain persists after 3 months.
Comment:
Postherpetic neuralgia is more often a sequel of herpes zoster as age advances,
afflicting 50% of patients contracting zoster over the age of 60 years. Hypoesthesia
or hyperalgesia and/or allodynia are usually present in the territory involved.
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 23

the sprout cannot enter, it continues to grow and produces a knotted masscalled a neuroma. The neuroma is sensitive to stimulus and usually accom-panied by spontaneous discharge activity. It is most sensitive within thefirst 2 weeks of development, but may continue at lesser levels for longerperiods of time. A neuroma can be identified by the response to tapping(Tinel’s sign).
Nerve compression (e.g. mental nerve compression by denture)
Pain may be due to structural lesions affecting the afferent fibers that supplysensory innervations to the head and neck. Sensory deficits are noted inthe distribution of the affected nerve. The causative lesion may be space-occupying, such as a tumor. Neuralgia due to pressure on the inferior alveolarnerve by an impacted third molar is not uncommon, but entrapment of thenerve within the substance of the tooth is rare.44
Nerve entrapments in the infratemporal fossa with a spastic condition of thelateral pterygoid muscle may be causally related to compression of anentrapped nerve that leads to numbness, pain, or both, in the respective areasof nerve distribution.3,27,45
NeurovascularMany primary headache disorders may camouflage what is initially diag-nosed as dental pain.46 The IHS has drawn up a classification system, whichshould be consulted.4 Headache disorders that replicate odontogenic paininclude migraine, cluster headache, indomethacin-sensitive headaches(chronic paroxysmal hemicrania and exertional headaches), and giant cellarteritis.
Migraine
Migraine headaches are erroneously considered to affect only the occipital,temporal, and frontal regions of the head. Raskin and Prusiner47 have describeda lower face migraine headache and labeled this entity carotidynia, or facialmigraine. Typically these headaches are episodic and have a duration of 4–72hours. The pain is often aggravated by exertion and relieved by rest and sleep.It is throbbing in nature and often quite severe in intensity. Patients may com-plain of photophobia and phonophobia and may feel nauseated or even vomitwhen the pain is most intense. There may also be ipsilateral carotid tender-ness (Table 2.7).
24
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 24

Cluster headache
Cluster headaches (migrainous neuralgia, sphenopalatine neuralgia, Sluder’sneuralgia) are characterized by severe, boring, orbital, supra-orbital, ortemporal pain. Occasionally the pain radiates to the maxilla, thus duplicatingodontogenic pain.48 Classically these patients are middle-aged men whosmoke. The pain is severe, strictly unilateral, and often wakes the patientfrom sleep. The pain comes in clusters of weeks to months. Each singleepisode lasts 15–180 minutes and there may be one to eight painful attacksin any one day. Autonomic signs, such as lacrimation, conjunctival injection,nasal congestion, forehead and facial perspiration, rhinorrhea, eyelid edema,miosis, and ptosis, are often present.
A retrospective study conducted by Bittar and Graff-Radford48 showed thatof 33 patients who were diagnosed with cluster headaches, 14 (42%) weretreated by a dentist and almost 50% received inappropriate dental treatments,such as orthotic fabrication, coronoplasty, root canal fillings, extractions, andapicoectomies.
Brooke studied 35 cases of cluster headache with pain referral to dental struc-tures.49 He described the condition as ‘periodic migrainous neuralgia’ and
25
Table 2.7 IHS diagnostic criteria for migraine without aura
Diagnostic criteria:
A.At least 5 attacks fulfilling criteria B–D
B. Headache attacks lasting 4–72 hours (untreated or unsuccessfully treated)
C. Headache has at least two of the following characteristics:
1. Unilateral location
2. Pulsating quality
3. Moderate or severe pain intensity
4. Aggravation by or causing avoidance of routine physical activity (e.g. walking
or climbing stairs)
D. During headache at least one of the following:
1. Nausea and/or vomiting
2. Photophobia and phonophobia
E. Not attributed to another disorder
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 25

showed that extractions, endodontic treatments, and other irreversible dentaltreatments were prevalent but unsuccessful (Table 2.8).
Short-lasting unilateral neuralgiform headache attacks withconjunctival injection and tearing (SUNCT)
SUNCT is a unilateral headache with frequently occurring (5 to 30 times perhour), short-lasting (15–60 seconds) attacks of pain.50,51 The pain occurs inand around one eye, and is accompanied by ipsilateral conjunctival injectionthat is often intense, lacrimation that may be impressive, and subclinical fore-head sweating. Attacks may be precipitated by cutaneous stimuli, chewing, oreating. The syndrome may be mistaken for trigeminal neuralgia involving thefirst division (V1) by the unwary, but it has a characteristic location, does notrespond to carbamazepine, and has autonomic concomitants52 (Table 2.9).
Chronic paroxysmal hemicrania
Paroxysmal hemicrania attacks can be characterized by pain and associatedsymptoms and signs similar to those of cluster headache, but they are shorter-lasting, more frequent, occur more commonly in women, and respond absolutelyto indomethacin. Chronic paroxysmal hemicrania is defined as attacks of
26
Table 2.8 IHS diagnostic criteria for cluster headache
Diagnostic criteria:
A.At least five attacks fulfilling criteria B–D
B. Severe or very severe unilateral orbital, supraorbital and/or temporal pain
lasting 15–180 minutes if untreated
C. Headache is accompanied by at least one of the following:
1. Ipsilateral conjunctival injection and/or lacrimation
2. Ipsilateral nasal congestion and/or rhinorrhea
3. Ipsilateral eyelid edema
4. Ipsilateral forehead and facial sweating
5. Ipsilateral miosis and/or ptosis
6. A sense of restlessness or agitation
D.Attacks have a frequency from one every other day to eight per day
E. Not attributed to another disorder
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 26

27
Table 2.9 IHS diagnostic criteria for short-lasting unilateral neuralgiform headache attackswith conjunctival injection and tearing (SUNCT)
Diagnostic criteria:
A.At least 20 attacks fulfilling criteria B–D
B.Attacks of unilateral orbital, supraorbital or temporal, stabbing or pulsating
pain lasting 5–240 seconds
C. Pain is accompanied by ipsilateral conjunctival injection and lacrimation
D.Attacks occur with a frequency from 3 to 200 per day
E. Not attributed to another disorder
Table 2.10 IHS diagnostic criteria for paroxysmal hemicrania
Diagnostic criteria:
A.At least 20 attacks fulfilling criteria B–D
B.Attacks of severe unilateral orbital, supraorbital or temporal pain lasting 2–30
minutes
C. Headache is accompanied by at least one of the following:
1. Ipsilateral conjunctival injection and/or lacrimation
2. Ipsilateral nasal congestion and/or rhinorrhea
3. Ipsilateral eyelid edema
4. Ipsilateral forehead and facial sweating
5. Ipsilateral miosis and/or ptosis
D.Attacks have a frequency above five per day for more than half of the time,
although periods with lower frequency may occur
E.Attacks are prevented completely by therapeutic doses of indomethacin
F. Not attributed to another disorder
Chronic paroxysmal hemicrania
Description:
Attacks of paroxysmal hemicrania occurring for more than 1 year without
remission or with remissions lasting less than 1 month.
Diagnostic criteria:
A.Attacks fulfilling criteria A–F for Paroxysmal hemicrania
B.Attacks recur over > 1 year without remission periods or with remission periods
lasting < 1 month
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 27

paroxysmal hemicrania that occur for more than 1 year without remission orwith remissions lasting less than 1 month4 (Table 2.10).
Giant cell arteritis
Giant cell arteritis (temporal arteritis) is a new-onset headache that occurs inpatients older than 50 years of age. The pain is intermittent or continuous andis located primarily over the temples but may radiate to the maxilla or thetooth.53,54 Other symptoms include fever, myalgia, arthralgia, and jaw claudi-cation.55,56 Treatment with steroids is usually favorable; however, serioussequelae, including blindness, may occur if the condition is misdiagnosedand a delay in treatment occurs.
Unfortunately, because of the temporal pattern associated with neurovascularpain and its characteristic periods of remission, dental therapy that is per-formed is often believed to have been successful. Hence, when the painreturns at a later date additional futile therapy may be carried out again(Table 2.11).
PsychogenicOccasionally a patient’s symptomatology may completely confound the treat-ing doctor. In such a case, it is grossly unfair to decide that the patient is suf-fering from a psychogenic disorder unless positive inclusionary criteria aremet. Okeson and Bell27 list such criteria as follows:
28
Table 2.11 IHS diagnostic criteria for headache attributed to giant cell arteritis
Diagnostic criteria:
A.Any new persisting headache fulfilling criteria C and D
B.At least one of the following:
1. Swollen tender scalp artery with elevated erythrocyte sedimentation rate
and/or C-reactive protein
2. Temporal artery biopsy demonstrating giant cell arteritis
C. Headache develops in close temporal relation to other symptoms and signs of
giant cell arteritis
D. Headache resolves or greatly improves within 3 days of high-dose steroid
treatment
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 28

1. The patient reports that multiple teeth are often painful with frequent change incharacter and location.
2. There is a general departure from normal or physiologic patterns of pain.3. The patient presents with chronic pain behavior.4. There is a lack of response to reasonable dental treatment or there is an unusual
and unexpected response to therapy.5. There is no identifiable pathology that can explain the toothache.
Trigeminal autonomic cephalgia andtrigeminal neuralgiaTrigeminal autonomic cephalgias are a rare group of headache disordersassociated with ipsilateral cranial autonomic dysfunction. This group ofheadache disorders can occur coincidentally with trigeminal neuralgia.
Cluster-tic syndromeThe cluster-tic syndrome is characterized by the coexistence of two kinds ofpain. One is strictly unilateral, usually periocular, with evident autonomicfeatures, and daily attacks for weeks or months (cluster). The other is charac-terized by paroxysms similar to electric shocks (tics). As reported in the liter-ature, the mean age for the beginning of pain was 44.6 years, 60% of patientswere female, pain was always unilateral, and the left side of the face wasaffected in 60% of patients.57 Two groups of patients with this syndrome aredescribed: the first without concurrent clinical manifestations (28 patients, or65%) and the second with concurrent manifestations (11 patients, or 35%).The trigeminal neuralgia is probably caused by changes in the myelinatedsmall-caliber fibers, whereas the cluster headache is related to changes innon-myelinated trigeminal fibers of the trigeminal-vascular system at thelevel of the nervous plexus of the cavernous sinus.58
Paroxysmal hemicrania-tic syndromeThere are still too few cases to fully characterize this syndrome, but somegeneralizations can be made. Attacks can occur concurrently, non-concurrently,or both. The paroxysmal hemicrania (PH) component of the syndrome isoften episodic. Boes et al.59 published case reports of eight patients. In six ofeight patients, the PH was episodic at some time during the illness, and infour of eight it was episodic at the time of the case report. Thus the PHattacks may start and remain episodic throughout the illness. The tic componentcan always be triggered to some degree, and in some cases (five of eight) the
29
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 29

PH component is also triggerable. The relationship between PH and trigeminalneuralgia is not completely clear. The two conditions might occur coin-cidentally, or alternatively could be comorbid.60 It may be that the brain abnor-mality that causes PH allows a peripheral stimulus in trigeminal neuralgia to bemore readily expressed.60 Given the hypothalamic activation seen in clusterheadache61,62 and SUNCT attacks,63 and the phenotypic similarity between PH,cluster, and SUNCT, it seems likely that a CNS mechanism underlies the etiol-ogy of PH. Fromm et al. stated that trigeminal neuralgia has a peripheral causeand a central pathogenesis.64 Perhaps in PH-tic, the CNS abnormality includesimpaired inhibitory mechanisms that normally control afferent activity in thetrigeminal nucleus,65 as well as hypothalamic dysfunction.
References1. Zakrzewska JM. Trigeminal neuralgia. Prim Dent Care 1997; 4: 17–19.2. Katusic S, Beard CM, Bergstralh E et al. Incidence and clinical features of trigemi-
nal neuralgia, Rochester, Minnesota, 1945–1984. Ann Neurol 1990; 27: 89–95.3. Merskey H, Bogduk N. Classification of Chronic Pain. Seattle: IASP Press,
1994.4. Headache classification subcommittee of the International Headache Society.
The International Classification of Headache Disorders, 2nd edn. Cephalalgia2004; (Suppl 1): 24.
5. Turp JC, Kowalski CJ, Stohler CS. Treatment-seeking patterns of facial painpatients: many possibilities, limited satisfaction. J Orofac Pain 1998; 12: 61–6.
6. Kugelberg E, Linblom U. The mechanism of the pain in trigeminal neuralgia.J Neurochem 1959; 22: 36–43.
7. Dubner R, Sharav Y, Gracely RH et al. Idiopathic trigeminal neuralgia: sensoryfeatures and pain mechanisms. Pain 1987; 31: 23–33.
8. Barker FG, Jannetta PJ, Bissonette DJ et al. The long-term outcome ofmicrovascular decompression for trigeminal neuralgia. N Engl J Med 1996;334: 1077–83.
9. Rasmussen P. Facial pain. IV. A prospective study of 1052 patients with a viewof: precipitating factors, associated symptoms, objective psychiatric and neuro-logical symptoms. Acta Neurochir (Wien ) 1991; 108: 100–9.
10. Barker FG, Jannetta PJ, Babu RP et al. Long-term outcome after operation fortrigeminal neuralgia in patients with posterior fossa tumors. J Neurosurg 1996;84: 818–25.
11. Jensen TS, Rasmussen P, Reske-Nielsen E. Association of trigeminal neuralgiawith multiple sclerosis: clinical and pathological features. Acta Neurol Scand1982; 65: 182–9.
30
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 30

12. Cheng TM, Cascino TL, Onofrio BM. Comprehensive study of diagnosis andtreatment of trigeminal neuralgia secondary to tumors. Neurology 1993; 43:2298–302.
13. Puca A, Meglio M, Vari R et al. Evaluation of fifth nerve dysfunction in 136patients with middle and posterior cranial fossae tumors. Eur Neurol 1995; 35:33–7.
14. Hooge JP, Redekop WK. Trigeminal neuralgia in multiple sclerosis. Neurology1995; 45: 1294–6.
15. Meaney JF, Watt JW, Eldridge PR et al. Association between trigeminal neural-gia and multiple sclerosis: role of magnetic resonance imaging. J NeurolNeurosurg Psychiatry 1995; 59: 253–9.
16. Smyth P, Greenough G, Stommel E. Familial trigeminal neuralgia: case reportsand review of the literature. Headache 2003; 43: 910–15.
17. Coffey RJ, Fromm GH. Familial trigeminal neuralgia and Charcot-Marie-Toothneuropathy. Report of two families and review. Surg Neurol 1991; 35: 49–53.
18. Zakrzewska JM. Diagnosis and differential diagnosis of trigeminal neuralgia.Clin J Pain 2002; 18: 14–21.
19. Merrill RL, Graff-Radford SB. Trigeminal neuralgia: how to rule out the wrongtreatment. J Am Dent Assoc 1992; 123: 63–8.
20. Fromm GH, Graff-Radford SB, Terrence CF et al. Pre-trigeminal neuralgia.Neurology 1990; 40: 1493–5.
21. Bell WE. Toothaches of nonodontogenic origin. J Calif Dent Assoc 1976; 4:50–8.
22. Okeson JP, Falace DA. Nonodontogenic toothache. Dent Clin North Am 1997;41: 367–83.
23. Wright EF, Gullickson DC. Identifying acute pulpalgia as a factor in TMD pain.J Am Dent Assoc 1996; 127: 773–80.
24. Ingle JI, Bakland LK. Endodontics. Baltimore: Williams & Wilkins, 1994.25. Chen YH, Tseng CC, Chao WY et al. Toothache with a multifactorial etiology:
a case report. Endod Dent Traumatol 1997; 13: 245–7.26. Gallin DM, Rosenberg DB. Rhinitis mimicking odontalgia: a case report. N Y
State Dent J 1998; 64: 22.27. Okeson JP, Bell WE. Bell’s Orofacial Pains. Chicago: Quintessence Publishing
Co., 1995.28. Simons DG, Travell JG, Simons LS. Travell & Simons’ Myofascial Pain and
Dysfunction: the Trigger Point Manual. Baltimore: Williams & Wilkins, 1999.29. Symonds C. Facial pain. Ann R Coll Surg Engl 1949; 4: 206–12.30. Mitchell RG. Pre-trigeminal neuralgia. Br Dent J 1980; 149: 167–70.31. Zakrzewska JM. Trigeminal neuralgia. Clin Evid 2002; 1221–31.32. Merrill RL. Orofacial pain mechanisms and their clinical application. Dent Clin
North Am 1997; 41: 167–88.
31
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 31

33. Merrill RL. Orofacial pain mechanism. Tex Dent J 2000; 117: 26–9.34. Weisenburg TH. Cerebello-pontine tumor diagnosed for six years as tic
douloureux. JAMA 1910; 54: 1600–4.35. White JC, Sweet WH. Pain and the Neurosurgeon: a 40-year Experience.
Springfield, IL: Charles C Thomas, 1969.36. Rushton JG. Cranial nerve neuralgias. Med Clin North Am 1960; 44: 969–76.37. Sigurdsson A, Jacoway JR. Herpes zoster infection presenting as an acute pulpi-
tis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995; 80: 92–5.38. Lopes MA, de Souza Filho FJ, Jorge JJ et al. Herpes zoster infection as a differ-
ential diagnosis of acute pulpitis. J Endod 1998; 24: 143–4.39. Goon WW, Jacobsen PL. Prodromal odontalgia and multiple devitalized teeth
caused by a herpes zoster infection of the trigeminal nerve: report of case. J AmDent Assoc 1988; 116: 500–4.
40. Hager TS, Connor JP. Herpes zoster. Gen Dent 1987; 35: 464–5.41. Tidwell E, Hutson B, Burkhart N et al. Herpes zoster of the trigeminal nerve
third branch: a case report and review of the literature. Int Endod J 1999; 32:61–6.
42. Millar EP, Troulis MJ. Herpes zoster of the trigeminal nerve: the dentist’s role indiagnosis and management. J Can Dent Assoc 1994; 60: 450–3.
43. Gilden DH, Dueland AN, Cohrs R et al. Preherpetic neuralgia. Neurology 1991;41: 1215–18.
44. Mishra YC. Entrapment of the neurovascular bundle by the roots of an impactedmandibular third molar – a case report. Br J Oral Maxillofac Surg 1987; 25:261–4.
45. Loughner BA, Larkin LH, Mahan PE. Nerve entrapment in the lateral pterygoidmuscle. Oral Surg Oral Med Oral Pathol 1990; 69: 299–306.
46. Graff-Radford SB. Headache problems that can present as toothache. Dent ClinNorth Am 1991; 35: 155–70.
47. Raskin NH, Prusiner S. Carotidynia. Neurology 1977; 27: 43–6.48. Bittar GT, Graff-Radford SB. A retrospective study of patients with cluster
headaches. Oral Surg Oral Med Oral Pathol 1992; 73: 519–25.49. Brooke RI. Periodic migrainous neuralgia: a cause of dental pain. Oral Surg Oral
Med Oral Pathol 1978; 46: 511–16.50. Pareja JA, Sjaastad O. SUNCT syndrome. A clinical review. Headache 1997; 37:
195–202.51. Goadsby PJ, Matharu MS, Boes CJ. SUNCT syndrome or trigeminal neuralgia
with lacrimation. Cephalalgia 2001; 21: 82–3.52. Sjaastad O, Kruszewski P. Trigeminal neuralgia and ‘SUNCT’ syndrome: simi-
larities and differences in the clinical pictures. An overview. Funct Neurol 1992;7: 103–7.
53. Guttenberg SA, Emery RW, Milobsky SA et al. Cranial arteritis mimickingodontogenic pain: report of case. J Am Dent Assoc 1989; 119: 621–3.
32
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 32

54. Kleinegger CL, Lilly GE. Cranial arteritis: a medical emergency with orofacialmanifestations. J Am Dent Assoc 1999; 130: 1203–9.
55. Allen DT, Voytovich MC, Allen JC. Painful chewing and blindness: signs andsymptoms of temporal arteritis. J Am Dent Assoc 2000; 131: 1738–41.
56. Hayreh SS. Masticatory muscle pain: an important indicator of giant cell arteritis.Spec Care Dentist 1998; 18: 60–5.
57. Diamond S, Freitag FG, Cohen JS. Cluster headache with trigeminal neuralgia.An uncommon association that may be more than coincidental. Postgrad Med1984; 75: 165–72.
58. Monzillo PH, Sanvito WL, Da Costa AR. Cluster-tic syndrome: report of fivenew cases. Arq Neuropsiquiatr 2000; 58: 518–21.
59. Boes CJ, Matharu MS, Goadsby PJ. The paroxysmal hemicrania-tic syndrome.Cephalalgia 2003; 23: 24–8.
60. Goadsby PJ, Lipton RB. Paroxysmal hemicrania-tic syndrome. Headache 2001;41: 608–9.
61. May A, Bahra A, Buchel C et al. Hypothalamic activation in cluster headacheattacks. Lancet 1998; 352: 275–8.
62. May A, Goadsby PJ. Hypothalamic involvement and activation in clusterheadache. Curr Pain Headache Rep 2001; 5: 60–6.
63. May A, Bahra A, Buchel C et al. Functional magnetic resonance imaging inspontaneous attacks of SUNCT: short-lasting neuralgiform headache with con-junctival injection and tearing. Ann Neurol 1999; 46: 791–4.
64. Fromm GH, Terrence CF, Maroon JC. Trigeminal neuralgia. Current conceptsregarding etiology and pathogenesis. Arch Neurol 1984; 41: 1204–7.
65. Goadsby PJ. The pathophysiology of headache. In: Silberstein SD, Lipton RB,Solomon S, eds. Wolff’s Headache and Other Head Pain, 7th edn. Oxford:Oxford University Press, 2001: 57–72.
33
02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 33

02-CMTN 8023.qxd 2/1/2007 7:38 PM Page 34

IntroductionTreatment of trigeminal neuralgia as a chronic neuropathic pain disordershould be based on the underlying mechanism. Thus, understanding themechanism of trigeminal neuralgia will provide the insight for approaches tomanaging trigeminal neuralgia.
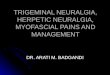
Review of trigeminal sensory pathwayThe trigeminal nerve or the fifth cranial nerve (CN V) is a general sensorynerve carrying touch, temperature, nociception, and proprioception fromsuperficial and deep structures of the face. The trigeminal nerve is composedof three major divisions: ophthalmic (V1), maxillary (V2), and mandibular(V3). The mandibular division is the largest among the three divisions.1 Eachdivision supplies a distinct dermatome on the head, face, and adjacentmucosal and meningeal tissues.2 Unlike spinal dermatomes, trigeminal nervedistributions show relatively little overlap. The cell bodies of trigeminal affer-ents are located in the trigeminal (semilunar/gasserian) ganglion. The trigem-inal nerve roots enter the brainstem at the midpontine level. The centralterminal of the trigeminal sensory neurons then synapse in the trigeminalspinal nucleus. This structure is very similar to the spinal cord dorsal horn. Itis commonly considered the extension of the dorsal horn and sometimesreferred to as the medullary dorsal horn. The trigeminal spinal tract nucleusalso receives input from nerves other than the trigeminal; cranial nerve IXand X as well as the upper cervical nerves supply input to the tract. Thetrigeminal spinal nucleus consists of subnucleus oralis, interpolaris, andcaudalis (Figure 3.1).
Once nociceptive input from orofacial structures is originated, the impulse isthen carried into central nervous system (CNS) by primary afferent fibers andsynapse with second-order neurons in the trigeminal nucleus caudalis, the
35
Pathogenesis and clinicalapproach to trigeminalneuralgia treatment
3
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 35

To associatedcortex
To reticular formation
Trigeminalganglia
Ophthalmic div.
Maxillary div.
Mandibular div. VIIIXX
C2–4
Principal sensory nucleus
N. oralis Spinaltrigeminalnucleus
N. interpolaris
N. caudalis
Somatosensorycortex
ThalamusTo PAG
Figure 3.1 Trigeminal pain pathway.The trigeminal primary afferent neuron (first-orderneuron); the cell body lying in the trigeminal ganglia enters the brainstem and synapseswith the second-order neuron in the spinal trigeminal nucleus.The spinal trigeminalnucleus is divided into subnucleus oralis (n. oralis), subnucleus interpolaris (n. interpolaris),and subnucleus caudalis (n. caudalis).The second-order neurons then project to the higherbrain structures including thalamus, periaqueductal gray (PAG), and reticular formation.From the thalamus the third-order neurons then terminate in the somatosensory cortexand associated area of the brain.
third part of the spinal trigeminal nucleus. Second-order trigeminal neuronsthen project to the thalamus as well as the periaqueductal gray, the para-brachial region, and the hypothalamus.3 These ascending non-thalamic pro-jections are likely to be responsible for the affective aspects of nociception asseen clinically. The axon of the third-order nerve cell body in the thalamusthen projects through the internal capsule and corona radiata to the appropriatearea in the somatosensory cortex.
36
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 36

Trigeminalganglia
VIIIX
X
C2–4
Hypothalamus
PAG
Thalamus
Somatosensorycortex
Trigeminal pain modulationNociceptive activity is also subjected to modulation by descending and afferentinhibitory mechanisms that are known to suppress pain. Projections from thenucleus raphe magnus, periaqueductal gray, sensorimotor cortex, pretectalarea, and parabrachial area are capable of influencing nociceptive responses.4
These afferent induced modulations appear to be an important mechanism intrigeminal nociception (Figure 3.2).
37
Figure 3.2 Trigeminal pain modulations.The descending inhibitory pain mechanism oftrigeminal pain originated from the higher center of the brain such as the hypothalamusand periaqueductal gray (PAG), which receives the input from the cortex and associatedarea of the brain. From periaqueductal gray cells give the descending inhibitory painprojection directly to the synapses between first and second-order neurons as well asindirectly through other nuclei of the brainstem such as the rostroventral medulla (RVM)and dorsolateral pontine tegmentum (DLPT).
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 37

Melzack and Wall’s original paper5 described how nociceptive impulsescould be altered in the dorsal horn of the spinal cord. Given that the trigemi-nal spinal nucleus is the brainstem continuation of the spinal cord dorsalhorn, it is assumed that the same discussion is true for trigeminal nerve input.The gate control theory (Figure 3.3) suggested that both myelinated andunmyelinated primary afferent neurons converge to synapse with both asecond-order neuron and an interneuron in the substantia gelatinosa (lamina II).Both myelinated and unmyelinated primary afferents were proposed to have adirect excitatory effect on the second-order neuron, which they called trans-mission cell (T cell). Since these T cells carry nociceptive impulses, we nowknow that they are either a nociceptive specific neuron or a wide dynamicrange neuron. The substantia gelatinosa interneurons were proposed to inhibittransmitter release from both primary afferent neurons, thus inhibiting the
38
Figure 3.3 Gate control theory. The gate control theory involves the interactions oftransmission neurons (T), inhibitory interneuron (I), large myelinated primary afferent (Aβ)amd small unmyelinated primary afferent (C).The inhibitory interneuron exerts an inhibitoryeffect on the transmission cells to reduce the perceived pain intensity at the same time asthis same I cell receives the excitatory input from the large primary afferent and inhibitoryinput from the small unmyelinated input. +, excitatory effect; − , inhibitory effect.
Aβ cell
C cell
T
+_
_
+
+
I
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 38

impulse carried by these neurons. The myelinated afferents were proposed toexcite the inhibitory interneurons, which in turn reduced the activity of thepain transmission neuron. This point is supported by clinical observation thatselective stimulation of large diameter myelinated fibers produced analgesia.In contrast, activity of unmyelinated nociceptive neurons was proposed toinhibit the inhibitory substantia gelatinosa interneurons, resulting in anenhancement of transmission from the primary afferents to the transmissioncell. This action would therefore increase nociceptive transmission to thehigher center.
Etiology of trigeminal neuralgiaAccording to Love and Coakham,6 the majority of trigeminal neuralgia casesare caused by compression of the trigeminal nerve root, usually within a fewmillimeters of entry into the pons, specifically the root entry zone (Table 3.1).Less commonly, trigeminal neuralgia is due to a primary demyelinatingdisorder. Other, rare causes include infiltration of the trigeminal nerve root,ganglion or nerve by a tumor or amyloid, and small infarcts or angioma in thepons or medulla. In a few cases the etiology is unknown.
Compression of the trigeminal nerve rootThe most common cause of trigeminal neuralgia is focal compression of thetrigeminal nerve root, close to its point of entry into the pons, by an abnormalloop of artery or vein. This was first recognized as a cause of trigeminal neural-gia by Jannetta7 and is now thought to account for 80–90% of cases.8–13 The partof the nerve root that is usually compressed is usually within CNS tissue whichextends several millimeters along the root, so that the junction between the cen-tral and peripheral nervous system is well away from the surface of the pons.Rarely, trigeminal neuralgia results from vascular compression of the nerve rootby saccular aneurysm,14 arteriovenous malformation,15,16 or pontine vein.17
39
Table 3.1 Etiology of trigeminal neuralgia proposed by Love and Coakham6
■ Compression of the trigeminal nerve root
■ Primary demyelination disorders
■ Infiltrative disorders of the trigeminal nerve root, ganglion and nerve
■ Non-demyelinating lesions of the pons or medulla
■ Familial trigeminal neuralgia
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 39

A wide range of other compressive lesions can cause trigeminal neuralgia.These include various posterior cranial fossa tumors,18–22 schwannomas,23
meningioma,24 and epidermoid cyst.25 Several case reports indicate that trigemi-nal neuralgia occurred contralateral to the side of the tumor or lesion.26–28
Compression of the trigeminal nerve root may be mediated by the tumor itself,by an interposed blood vessel or by distortion of the contents of the posteriorcranial fossa with displacement of nerve root against the blood vessel or theskull base. During a 20-year period, Barker et al.18,22 studied 26 patients withtypical symptoms of trigeminal neuralgia who were also found to have posteriorfossa tumors at operation. At operation, the root entry zone of the trigeminalnerve was examined for vascular cross-compression in 21 patients. Vessels com-pressing the nerve at the root entry zone were observed in all patients examined.Fujimaki et al.29 reported two cases of recurrent trigeminal neuralgia caused byan inserted prosthesis. Teflon material or polyurethane sponge inserted betweenthe trigeminal nerve and the superior cerebellar artery became hardened andcompressed the trigeminal nerve after the initial surgery. Rarely, trigeminal neu-ralgia results from bony compression of the nerve; for example, compressionfrom osteoma30 or deformity resulting from osteogenesis imperfecta.31
Primary demyelination disordersTrigeminal neuralgia is a well-recognized complication of multiple sclerosis(MS).32–37 Typically, a plaque of demyelination encompasses the root entryzone of the trigeminal nerve in the pons.38–41 Rarely, patients with peripheralnerve demyelination due to Charcot-Marie-Tooth disease develop trigeminalneuralgia.42 Vascular compression of the trigeminal nerve root by blood ves-sel has been demonstrated in a sizeable minority of patients with MS andtrigeminal neuralgia,43 and in an occasional patient with Charcot-Marie-Tooth disease.44 In many such cases, decompression of the nerve root leads torelief of symptoms.
Infiltrative disorders of the trigeminal nerve root,ganglion, and nerveThe principal infiltrative causes of trigeminal neuralgia are carcinomatousdeposits within the nerve root, trigeminal ganglion, and nerve.45 Perineuralspread of head and neck cancer is an uncommon cause of cranial neuropathy.Boerman et al.46 studied five patients with cranial neuropathy resulting fromperineural spread of head and neck carcinomas. Trigeminal neuropathy withfacial pain or paresthesias was the most common clinical manifestation.Magnetic resonance imaging (MRI) in the coronal plane under gadolinium
40
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 40

enhancement established the diagnosis by visualization of the lower divisionsof the trigeminal nerve. Perineural tumor spread can also cause headaches inpatients with head and neck cancer. Love et al.47 described a patient whodeveloped chronic bilateral trigeminal neuropathy that was found at autopsyto be due to lambda light chain amyloidosis involving the trigeminal nerves,ganglia, and roots bilaterally, as well as part of the intrapontine course of thetrigeminal nerve fibres. Love’s report indicates that the clinical features oftrigeminal amyloidosis are quite stereotyped, with initial trigeminal neuralgiaor dysesthesia, and subsequent development of facial anesthesia and weak-ness of muscles of mastication.
Non-demyelinating lesions of the pons or medullaSmall numbers of patients have been reported with the association of trigemi-nal neuralgia and either a small infarction or angioma in the brainstem.Golby et al.48 reported a case of trigeminal neuralgia resulting from infarc-tion of the root entry zone of the trigeminal nerve. The patient presented withsevere lancinating pain in the left V1 and V2 distributions. MRI of the braindemonstrated a small wedge-shaped infarct at the root entry zone of the lefttrigeminal nerve in the pons. Classic trigeminal neuralgia occurs in themiddle-aged to elderly and is usually a result of compression of the trigemi-nal nerve at its root entry zone by an ectatic, aging artery or, less commonly,a regional vein. However, when associated with a venous angioma at the rootentry zone, trigeminal neuralgia usually presents at a younger age.49
Familial trigeminal neuralgiaClinical observations suggesting a hereditary component to bilateral trigemi-nal pain were reported in 1936,50 and followed in 194051 with a series of 1433cases of trigeminal neuralgia and outcomes after alcohol injection of thetrigeminal ganglion to relieve pain. The earlier article described a family withever-earlier onset (anticipation), and the latter series found 30 (2%) of 1433index cases that had family members with similar facial pain. These reports byHarris, along with those of Allan,52 were consistent with autosomal dominantinheritance; the family studied by Allan also appeared to show anticipation.More recent case reports by Herzberg53 and Duff et al.54 are also consistentwith autosomal dominant transmission. Coffey and Fromm, reviewingan association between familial trigeminal neuralgia and Charcot-Marie-Tooth (CMT) neuropathy, also found evidence for autosomal dominant trans-mission.42 Charcot-Marie-Tooth disease (hereditary sensorimotor neuropathytype I) is autosomal dominant and results from peripheral demyelination.
41
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 41

Sporadic cases of trigeminal neuralgia-like pain have been associated with MSplaques as well. Including cases described by Coffey and Fromm, the numberof reported patients with both CMT and trigeminal neuralgia is 15. For famil-ial trigeminal neuralgia alone, Coffey and Fromm report a female to male ratioof 1.5 : 1, consistent with the 39-year survey of trigeminal neuralgia incidenceby Katusic and colleagues.55 In 1979, Knuckney and Gubbay55,56 proposed anassociation between trigeminal and glossopharyngeal neuralgia based on afamily in whom a grandfather had trigeminal neuralgia; his son developedboth trigeminal neuralgia and glossopharyngeal neuralgia and his grand-daughter had glossopharyngeal neuralgia. Twenty years later, Duffet al.54,55 presented a single case of a woman with contralateral hemifacialspasm, possibly due to a tumor, along with trigeminal neuralgia; her motherhad trigeminal neuralgia as did five of the patient’s siblings. Thus, the clinicalsyndrome of trigeminal neuralgia has been associated with several diseaseprocesses and rarely with concurrent cranial and noncranial neuropathies.
Pathophysiology of trigeminal neuralgia
Peripheral vs central mechanismThe pathophysiology of trigeminal neuralgia remains controversial. The con-troversial issue is whether the pathogenesis of trigeminal neuralgia involvesthe central or peripheral nervous system (Figure 3.4). A large proportion ofpatients with trigeminal neuralgia show evidence of external vascular com-pression, with focal demyelination near the compression site.57 However, thereis also evidence that minor compression of the trigeminal root is a commonincidence in individuals in the age group where trigeminal neuralgia normallyoccurs. Nevertheless, few individuals develop trigeminal neuralgia.58 Eventhough microvascular decompression usually provides prolonged pain relief intrigeminal neuralgia patients and is presumed to promote the remyelination,demyelination alone does not offer a complete explanation of trigeminal neu-ralgia symptomatology. For example, demyelination of myelinated sensoryfiber, which is normally responsible for light touch sensation, should result inthe interruption of signal propagation and focal sensory loss as a major conse-quence, not paroxysmal pain. In fact studies have indicated that trigeminalneuralgia patients demonstrate the abnormal sensory characteristic in theaffected distribution of trigeminal neuralgia.59,60
To correlate the clinical symptoms of trigeminal neuralgia with the underly-ing pathophysiology, Rappaport and Devor61 listed clinical symptoms of
42
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 42

trigeminal neuralgia that needed to be explained. For instance, what mecha-nisms prolong the trigeminal neuralgia pain sensation beyond the duration ofthe stimulus or mechanism underlying the spreading of painful sensationacross and beyond the trigger zone? Lastly what is a stop mechanism thatprevents an attack from going on for an indefinite period?62
The prolonged pain sensation of trigeminal neuralgia can be explained byhyperexcitability and afterdischarge of trigeminal ganglia neurons, as well asectopic discharge at the site of nerve injury. Several studies63–65 confirmedthat after nerve injury to the sensory nerve, neurons can become hyperex-citable and are able to generate spontaneous impulses due to the membraneremodeling of channels involving the impulse generation. The ectopic
43
Figure 3.4 Peripheral vs central mechanism of trigeminal neuralgia.This figure depicts asummary of peripheral and central mechanisms explaining the pain of trigeminal neuralgia.
Ectopic dischargeAfterdischarge
Cross-excitation
To thalamus
Trigeminal ganglion
Trigeminal n.caudalis
Centralsensitization
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 43

discharge site can fire spontaneously and can recruit the neighboring neuronsin the ganglia to fire in chain reaction manner. This will build up to theparoxysmal outburst. Devor and Rappaport called this process ‘ignition’ asthey proposed the ‘ignition hypothesis’ for trigeminal neuralgia.62
The explanation for intense and painful sensation of trigeminal neuralgiaevoked by light touch or non-noxious stimulus spreading to a large nearbyarea is probably due to the synchronizing activity of a large number oftrigeminal ganglion neurons including the nociceptive ones. Rappaport61 pro-posed that this phenomenon is the result of neuron-to-neuron cross-excitationwithin the trigeminal root and ganglion. In cross-talk or cross-excitationbetween sensory neurons within the ganglion, electrical currents in one neu-ron directly excite impulse activity in a neighboring neuron. This phenome-non does not commonly occur because nerve fiber and neurons themselvesare surrounded by insulating materials, e.g. myelin sheath or satellite cellsand their processes. In the circumstance where these insulators are inter-rupted or destroyed, nerve fibers have a direct contact. Then a nerveimpulse will be capable of jumping from one fiber to another one. As vascularcompression of the central axons of the trigeminal nerve, typically at the rootentry zone near the pons, has been inferred to be a possible cause of trigeminalneuralgia in most patients, the resulting demyelination is frequently sug-gested to be the cause of the electrical activity changes of trigeminal neurons.The ephaptic crosstalk and crossed afterdischarge that lead to the spreadingof electrical activity from Aβ fiber to nociceptive fiber can explain the uniquecharacteristic of trigeminal neuralgia wherein light touch can cause such anexcruciating pain.61
Finally, we consider the mechanisms that prevent either spontaneous or trig-ger trigeminal neuralgia pain from becoming continuous pain. Based on the‘ignition hypothesis’,61 the spontaneous and sustained firing activity is tran-sient. This activity only occurs when triggered or from the spreading adjacentneurons. The stop mechanism also involves the hyperpolarization of the neu-rons after the action potential firing. This also explains the ‘refractory period’commonly experienced following the trigeminal neuralgia attacks.
While previous paragraphs have focused on the peripheral hypothesis oftrigeminal neuralgia, there are also several studies indicating the involvementof not only peripheral but also central mechanisms. Within the spinal corddorsal horn or trigeminal nucleus where the majority of the pain modulationprocesses take place, the balance of excitatory and inhibitory inputs on thesesecond-order neurons plays a major role in determining information carried
44
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 44

through CNS circuits. Increases in excitation produced by increased inputssuch as from the ectopic activity in the periphery and increased responsive-ness or central sensitization of those trigeminal neurons in the brainstem byshifting the balance to increased excitability, can manifest as spontaneous orevoked pain. This can be the result of a reduction in inhibition (Figure 3.5).66
For example, partial nerve injury can reduce inhibition in the superficialdorsal horn by causing a selective loss of GABAergic inhibitory interneuronsthrough an induction of apoptosis.67 Undoubtedly, similar phenomena canhappen within the spinal trigeminal nucleus. As indicated by Fromm et al.,68
facilitation of inhibitory mechanisms appears to be at least as important asthe depression of excitatory mechanisms, suggesting that a failure ofinhibitory mechanisms may play a significant role in the pathogenesis of
45
Figure 3.5 Loss inhibition. Normal sensory inflow is actively controlled by inhibitoryinterneurons (I). Reduced synthesis of the inhibitory neurotransmitters GABA and glycine orloss of these inhibitory interneurons after excessive release of the excitotoxic amino acidglutamate following peripheral nerve injury increases the excitability of pain transmissionneurons such that they begin to respond to normally innocuous inputs.Adapted fromScholz and Woolf.66
Aβ cell
C cell
_
_
++ +
+
I T
Descendinginhibition
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 45

trigeminal neuralgia. Evidence from the latter study showed the remarkableeffects of carbamazepine, baclofen, and phenytoin in facilitating segmentalinhibition, as well as depressing the response to an unconditioned nervestimulus. On the other hand, phenobarbital usually depressed the segmentalinhibition. These results suggest that drugs that relieve trigeminal neuralgiaboth facilitate inhibitory mechanisms and depress excitatory mechanisms inthe spinal trigeminal nucleus.69,70
Increased response of the second-order neurons of the trigeminal nucleus hasbeen proposed to play a vital role in the trigeminal neuralgia central mecha-nism. Dubner et al.71 reported a patient with several unusual sensory featuresincluding multiple trigger zones that changed over time and involved allthree trigeminal divisions. Other clinical features were typical of trigeminalneuralgia. Sensory evaluation revealed that pain was evoked by repetitiveactivation of rapidly adapting, Aβ, low-threshold mechanoreceptive afferents.However, activation of such mechanoreceptive afferents alone never producespain in normal situations and often leads to a suppression of pain response, asindicated in the gate control theory. The findings support the idea that themechanism of trigeminal neuralgia pain involves pathophysiological mecha-nisms in the CNS, as the patient’s pain involved multiple trigger zones andwas not localized to one particular division. These authors proposed that struc-tural and functional changes in the trigeminal system result in an alteration inthe receptive field organization of wide dynamic range (WDR) neurons. Theyalso indicated that there may be an alteration in the inhibition mechanism ofthese neurons leading to an expansion of their touch receptive fields. Thisresults in touch stimuli producing activity in WDR neurons that mimics theactivity produced under normal conditions by noxious stimuli. Since WDRneurons participate in the encoding of the perceived intensity of noxious stim-uli, a series of punctate tactile stimuli are now perceived as localized, pinprickor electric shock-like sensations.
Neuropathic pain mechanism astrigeminal neuralgia mechanismConsidering that clinical characteristics of trigeminal neuralgia are strikinglysimilar to peripheral neuropathic pain in many aspects, together with the factthat currently there is no perfect animal model for trigeminal neuralgia, onecould assume that mechanisms responsible for peripheral neuropathic paincould possibly be applied in trigeminal neuralgia. As emphasized byWoolf,72,73 identification of the neurobiological mechanisms responsible for
46
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 46

neuropathic pain will lead to a mechanism-based approach, which offers thepossibility of greater diagnostic sensitivity and a more rational basis for ther-apy. This will move us from an empirical symptom control approach to thetreatment of pain to one targeting the specific mechanisms responsible.
The common feature of peripheral neuropathic pain includes the presence ofdisruption or damage to components of primary sensory neurons as a conse-quence of, for example, trauma, compression, or degenerative disorders. Thiswill lead to changes in the peripheral and central nervous system, and severalof these mechanisms have already been discussed in this chapter (ectopicexcitability of sensory neurons, central sensitization, and disinhibition in thespinal trigeminal nucleus). This section will discuss mechanisms of peripheralneuropathic pain which include the phenotype switch in the primary sensoryneuron and increased facilitation and structural reorganization in the CNS.
Phenotypic switch
To date, no study has specifically looked at changes in gene expression intrigeminal ganglia neurons of trigeminal neuralgia or peripheral trigeminalneuropathy. Most studies of altered gene expression of trigeminal neuronshave focused on another chronic trigeminal pain syndrome, ‘migraine’.74,75
Most data discussed in this section are based on findings in the neuropathicpain model of dorsal root ganglia, which are the equivalents of trigeminalganglia neurons. In differentiated neurons, expression of a great number ofspecific genes allows them to perform their particular functions. For primarysensory neurons, those genes enable transduction, conduction, and synaptictransmission of these sensory neurons, as well as many housekeeping func-tions. After peripheral nerve injury there is a large alteration in the levels of genetranscription – several hundred genes are either up- or down-regulated.76–81
These genes include regeneration-associated genes, survival factors, and manyother genes that determine the function or malfunction of the neurons. Thesignificance of these changes is a shift in the excitability of these neurons, aswell as their transduction, and transmitter properties (Figure 3.6).
Changes in gene expression could also result in a switch in the neuronalphenotype. For example, substance P (which is normally expressed only inC fibers) begins to be expressed in A fiber neurons after peripheral nerveinjury.82 This implies that these A fibers are now able to cause centralchanges such as central sensitization generally produced only by C fibers.83,84
Also, the α2δ calcium channel subunit is markedly up-regulated after nerveinjury.85–87 This subunit has been shown to be the target of gabapentin and
47
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 47

this finding may explain the analgesic action of gabapentin in neuropathicpain treatment.88,89
Neuroimmune interactions
One of the most common and obvious examples of neuroimmune interactionis peripheral sensitization during inflammation. Chemical mediators producedby local immune cells act on the peripheral nerve terminal and then eitherdirectly activate or indirectly sensitize the nerve terminals.
Recently, the emphasis has been on the central activation of spinal microgliaby interleukin-1 in neuropathic pain.89,90 These macrophage-like cells arequiescent in the normal spinal cord but are rapidly activated after nerve injuryand are probably a source of many cytokines and chemokines that act on neu-rons and their supporting glia to change their properties or patterns of geneexpressions. Changes in peripheral glia (Schwann cells) after nerve injury
48
Figure 3.6 Phenotypic switch.Transcriptional changes in the dorsal root ganglion.Activity,growth factors, and inflammatory mediators act on sensory neurons to activate intracellu-lar transduction cascades.These cascades control the transcription factors that modulategene expression, leading to changes in the levels of receptors, ion channels, and otherfunctional proteins. PKA, protein kinase A; MAP kinase, mitogen activated protein kinase;JNK, jun kinase.Adapted from Woolf.73
Voltage-gatedion channel
Nerve growthfactor
Inflammatorymediator
Cell body ofsensory neuron
ReceptorsIon channelsTransmitters
Structural proteinCentral terminal Peripheral terminal
mRNA
Protein
PKAMAP kinaseJNK, etc.
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 48

contribute to the direct activation of neighboring injured and non-injuredsensory neurons.
Increased pain facilitation
The powerful controls exerted by the brain on sensory processing in the spinalcord, and on its equivalent for the head and neck – the trigeminal nucleus ofthe medulla – are both inhibitory and facilitatory. The role of the periaqueduc-tal gray–rostral ventromedial medulla (RVM) system in descending inhibitionof nociception has been studied for over 30 years. The neural basis for thisantinociceptive action is reasonably well understood, with strong evidence thatactivation of a class of RVM neurons termed ‘off-cells’ exerts a net inhibitoryeffect on nociception. However, it has recently become clear that this systemcan facilitate, as well as inhibit pain.91 Although the mechanisms underlyingthe facilitation of nociception have not been conclusively identified, indirectevidence points to activation of a class of neurons termed ‘on-cells’ as mediat-ing descending facilitation. Neubert et al. have shown that selective activationof on-cells is sufficient to produce hyperalgesia, confirming the role of theseneurons in facilitating nociception. Activation of on-cells probably contributesto enhanced sensitivity to noxious stimulation or reduced sensitivity to anal-gesic drugs in a variety of conditions.
Since opioid analgesics are frequently used for the long-term management ofchronic pain states, prolonged use of opioids is associated with not only increas-ing doses to manage pain at a consistent level, or analgesic tolerance, but alsodevelopment of unexpected abnormal pain as shown in animals during theperiod of continuous opioid delivery. Several recent studies have demonstratedthat such pain may be secondary to neuroplastic changes that result, in part,from an activation of descending pain facilitation mechanisms. In addition,Burgess et al. pointed out that descending supraspinal influences are required forthe maintenance not the initiation of the neuropathic state.92 Prevention of suchfacilitation may help to reduce the maintenance of hypersensitivity to pain.
Structural reorganization
These changes have mostly been studied in the spinal cord. The details of themechanism for the trigeminal pain system may be different. The central ter-minals of nociceptor sensory neurons terminate in a distinct area of the spinalcord, the most superficial laminae of the dorsal horn. In contrast, lowerthreshold sensory fibers activated by touch, pressure, vibration, and normalranges of movement of joints terminate in the deep laminae of the dorsal
49
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 49

50
Figure 3.7 Structural reorganization.After peripheral nerve injury, the central terminals ofmyelinated non-nociceptive Aβ-afferents sprout in the dorsal horn and form new connectionswith nociceptive neurons in laminae I and II (for spinal cord).This rewiring of the circuitry ofthe spinal cord may contribute to persistent pain hypersensitivity. Adapted from Scholz andWoolf.66
C cell
Aβ cell
+
+
+
T
E
C cell
Aβ cell
+
++
+
T
E
a
b
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 50

horn. Experiments in rodents have shown that physical rearrangement of thiscircuitry occurs after peripheral nerve injury, and after several weeks, newgrowth or sprouting of the central terminals of the low-threshold afferentsinto the zone normally occupied exclusively by the nociceptor terminals isobserved.42 It has not been possible to determine whether a similar structuralrewiring of the connectivity of the spinal cord occurs in patients and under-lies their heightened sensitivity to pain. Such a phenomenon would explainthe intractability of many neuropathic pain conditions and raise the issues ofhow to prevent these changes and whether they are reversible (Figure 3.7). Itis known that the exquisite pain sensitivity to light touch in patients withneuropathic pain is due to an abnormal central response to low-threshold sen-sory fibers that usually elicit only touch sensations.43 This abnormal centralreaction to normal sensory input could be due to the combination of centralsensitization and structural reorganization, as well as to loss of inhibition(disinhibition).
Trigeminal neuralgia and genetics
Not much is known about the role of genes in the pathophysiology oftrigeminal neuralgia. Genetic contributions to complex pain traits are begin-ning to be studied through quantitative trait locus analysis and other formsof genetic analysis.93–95 More recently, there has been a growing bodyof evidence demonstrating differences in analgesic response to various phar-macotherapies,96 although the source of this variability largely remains to beexplained. Currently, basic science research is beginning to identify theallelic variants that underlie such antinociceptive variability using a multi-plicity of animal models, and powerful genetic approaches are beingexploited to accelerate this process. Although the vast majority of thesestudies have focused on the pharmacogenetics of opioids, owing to theirprominent status as analgesics, the number of pharmacotherapies demon-strating genetically based variability is rapidly expanding. In addition,analogous studies have been undertaken in humans, as a small but growingnumber of clinical trials have begun to evaluate prospectively the existence,although often not the origin, of interindividual differences in analgesic drugresponse. Importantly, with a few notable exceptions, such efforts haveprimarily identified differences in analgesic efficacy and/or potency betweenmale and female human subjects. Development of one or more widely uti-lized, pharmacogenetic screens would lead to modifications in treatmentplanning, at least with respect to the pharmacologic management of pain.
51
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 51

In recent years, gabapentin has been used off-label in the management of severalneuropathic pain conditions including trigeminal neuralgia.97 Gabapentin acts asligands at α2δ subunits of voltage-gated calcium channels. Recently, a studywith a genomic approach to this antiepileptic drug, gabapentin, and anotherstructurally related compound, pregabalin, revealed their potentially novelmechanisms. Chesler et al.98 examined the inheritability of sensitivity to analge-sia from gabapentin and pregabalin as a precursor to linkage mapping efforts.Accordingly, 11 inbred mouse strains were tested for inhibition of nociceptionby gabapentin or pregabalin in two different preclinical assays of inflammatorypain, the formalin test and zymosan thermal hyperalgesia, in the paw-with-drawal test. Significant strain dependence of drug action was noted in each case,indicating that sensitivity to these analgesics is inheritable. Furthermore, the pat-terns of strain sensitivities to gabapentin and pregabalin were mostly similar,supporting the notion that they act via similar genetic and physiological mecha-nisms. These findings empirically demonstrate the general principle that phar-macogenetic mechanisms underlying analgesic sensitivity are specific to thetype of pain being inhibited. This has considerable implications for ongoingpharmacogenetic investigations and, more generally, for the choices of preclini-cal models of pain used in drug development.
Even though it has been generally believed that the cause of trigeminal neu-ralgia is a result of an irritative lesion near the semilunar ganglion, it is worthmentioning the hypothesis proposed by Ecker and Smith,99 suggesting thatthe primary cause of trigeminal neuralgia is a single, active DNA sequence inthe persistent but non-integrated genome of latent herpes simplex virus type 1(HSV-1) commonly observed in a few infected Aδ nerve fibers of the cheek.Then pain occurs as a result of herpes virus reactivation and when supplies ofneurotrophins controlling normal transport functions of axonal ion channelsbecome depleted. Their hypothesis is based on the fact that nerve rootsinvolved in cranial neuralgias are exposed in the oropharynx to herpes sim-plex viruses, which are then maintained indefinitely as cryptic episomes inganglionic cell body nuclei, and the observation that various types of traumaapplied to the trigeminal root to relieve pain are frequently (up to 15%)followed by herpes labialis in the corresponding area.100
In detail, they propose that trigeminal neuralgia is basically an ion channelopa-thy and should be regarded as an epigenetic disease which arises in a few thinlymyelinated, nociceptive trigeminal neurons infected since childhood with latent(HSV-1). Their hypothesis offered an explanation for both the low incidence oftrigeminal neuralgia and the hyperexcitability in the affected neurons, resultingfrom a coincidental, dynamic interaction of the following three events. First,
52
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 52

the asymptomatic, latent, lifelong HSV-1 infection in the nuclei of some Aδneurons,101 especially in the maxillary and mandibular divisions. Second, amechanical disorder presents later in life at the axolemma of the central (oligo-dendroglia) portion of the sensory root near the brainstem. A variety of injurieshave been observed there, but commonly, neuralgia is associated with eitherstretching of the nerve by disturbance of a looping artery or localized demyeli-nation from MS plaque formation. Third, accumulated HSV-1 gene productscause an intermittent change in the critical level of one or more proteins thatmaintain normal ion channel transport and thus result in focal hyperexcitability.This system exhibits fast reversal when the infected cell is deliberately trauma-tized lightly and the channel controller substance(s) become modified orreduced. A slower, long-term reversal may also occur spontaneously, eventuallyproviding pain relief such as in a clinical remission.
The pathophysiology of trigeminal neuralgia warrants more research.Electrophysiological, morphological, biochemical, and genetic abnormalitiesin both the peripheral and central nervous systems should be exploredthrough human and animal tissue studies. Studies need to tease apart whichsensory fibers carry signals for pain triggering versus paroxysmal paindischarge. Studies need to examine variation in age, gender, and chronobiologyin relation to pathophysiology. Studies also should be conducted on thepotential contributions of non-neuronal cells, such as Schwann cells, vascularcells, and cells of the immune system. The development of model systemsis essential to confirm vascular compression in the etiology of trigeminalneuralgia and to probe related pathophysiology.102
References1. Pennisi E, Cruccu G, Manfredi M, Palladini G. Histometric study of myelinated
fibers in the human trigeminal nerve. J Neurol Sci 1991; 105: 22–8.2. Usunoff KG, Marani E, Schoen JH. The trigeminal system in man. Adv Anat
Embryol Cell Biol 1997; 136: I-126.3. Malick A, Burstein R. Cells of origin of the trigeminohypothalamic tract in the rat.
J Comp Neurol 1998; 400: 125–44.4. Sessle BJ. Acute and chronic craniofacial pain: brainstem mechanisms of
nociceptive transmission and neuroplasticity, and their clinical correlates. CritRev Oral Biol Med 2000; 11: 57–91.
5. Melzack R, Wall PD. Pain mechanisms: a new theory. Science 1965; 150:971–9.
6. Love S, Coakham HB. Trigeminal neuralgia: pathology and pathogenesis.Brain 2001; 124(Pt 12): 2347–60.
53
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 53

7. Jannetta PJ. Arterial compression of the trigeminal nerve at the pons in patientswith trigeminal neuralgia. J Neurosurg 1967; 26(1): Suppl-62.
8. McLaughlin MR, Jannetta PJ, Clyde BL et al. Microvascular decompression ofcranial nerves: lessons learned after 4400 operations. J Neurosurg 1999; 90: 1–8.
9. Jannetta PJ. Neurovascular compression in cranial nerve and systemic disease.Ann Surg 1980; 192: 518–25.
10. Hamlyn PJ. Neurovascular relationships in the posterior cranial fossa, withspecial reference to trigeminal neuralgia. 1. Review of the literature and devel-opment of a new method of vascular injection-filling in cadaveric controls. ClinAnat 1997; 10: 371–9.
11. Hamlyn PJ. Neurovascular relationships in the posterior cranial fossa, withspecial reference to trigeminal neuralgia. 2. Neurovascular compression of thetrigeminal nerve in cadaveric controls and patients with trigeminal neuralgia:quantification and influence of method. Clin Anat 1997; 10: 380–8.
12. Haines SJ, Jannetta PJ, Zorub DS. Microvascular relations of the trigeminal nerve.An anatomical study with clinical correlation. J Neurosurg 1980; 52: 381–6.
13. Bowsher D. Trigeminal neuralgia: an anatomically oriented review. Clin Anat1997; 10: 409–15.
14. Ildan F, Gocer AI, Bagdatoglu H et al. Isolated trigeminal neuralgia second-ary to distal anterior inferior cerebellar artery aneurysm. Neurosurg Rev1996; 19: 43–6.
15. Figueiredo PC, Brock M, De Oliveira AMJ, Prill A. Arteriovenous malforma-tion in the cerebellopontine angle presenting as trigeminal neuralgia. ArqNeuropsiquiatr 1989; 47: 61–71.
16. Edwards RJ, Clarke Y, Renowden SA, Coakham HB. Trigeminal neuralgiacaused by microarteriovenous malformations of the trigeminal nerve root entryzone: symptomatic relief following complete excision of the lesion with nerveroot preservation. J Neurosurg 2002; 97: 874–80.
17. Sato O, Kanazawa I, Kokunai T. Trigeminal neuralgia caused by compressionof trigeminal nerve by pontine vein. Surg Neurol 1979; 11: 285–6.
18. Barker FG, Jannetta PJ, Babu RP et al. Long-term outcome after operation fortrigeminal neuralgia in patients with posterior fossa tumors. J Neurosurg 1996;84: 818–25.
19. Cheng TM, Cascino TL, Onofrio BM. Comprehensive study of diagnosis andtreatment of trigeminal neuralgia secondary to tumors. Neurology 1993; 43:2298–302.
20. Puca A, Meglio M, Vari R, Tamburrini G, Tancredi A. Evaluation of fifth nervedysfunction in 136 patients with middle and posterior cranial fossae tumors.Eur Neurol 1995; 35: 33–7.
21. Weisenburg TH. Cerebello-pontine tumor diagnosed for six years as ticdouloureux. JAMA 1910; 54: 1600–4.
54
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 54

22. Matsuka Y, Fort ET, Merrill RL. Trigeminal neuralgia due to an acousticneuroma in the cerebellopontine angle. J Orofac Pain 2000; 14: 147–51.
23. Matthies C, Samii M. Management of 1000 vestibular schwannomas (acousticneuromas): clinical presentation. Neurosurgery 1997; 40: 1–9.
24. Samii M, Carvalho GA, Tatagiba M, Matthies C. Surgical management ofmeningiomas originating in Meckel’s cave. Neurosurgery 1997; 41: 767–74.
25. Kobata H, Kondo A, Iwasaki K. Cerebellopontine angle epidermoids present-ing with cranial nerve hyperactive dysfunction: pathogenesis and long-termsurgical results in 30 patients. Neurosurgery 2002; 50: 276–85.
26. Haddad FS, Taha JM. An unusual cause for trigeminal neuralgia: contralateralmeningioma of the posterior fossa. Neurosurgery 1990; 26: 1033–8.
27. Matsuura N, Kondo A. Trigeminal neuralgia and hemifacial spasm as falselocalizing signs in patients with a contralateral mass of the posterior cranialfossa. Report of three cases. J Neurosurg 1996; 84: 1067–71.
28. Revuelta R, Juambelz P, Balderrama J, Teixeira F. Contralateral trigeminalneuralgia: a new clinical manifestation of neurocysticercosis: case report.Neurosurgery 1995; 37: 138–9.
29. Fujimaki T, Hoya K, Sasaki T, Kirino T. Recurrent trigeminal neuralgiacaused by an inserted prosthesis: report of two cases. Acta Neurochir (Wien)1996; 138: 1307–9.
30. Ruelle A, Datti R, Andrioli G. Cerebellopontine angle osteoma causing trigemi-nal neuralgia: case report. Neurosurgery 1994; 35: 1135–7.
31. Reilly MM, Valentine AR, Ginsberg L. Trigeminal neuralgia associated withosteogenesis imperfecta. J Neurol Neurosurg Psychiatry 1995; 58: 665.
32. Eldridge PR, Sinha AK, Javadpour M, Littlechild P, Varma TR. Microvasculardecompression for trigeminal neuralgia in patients with multiple sclerosis.Stereotact Funct Neurosurg 2003; 81: 57–64.
33. Love S, Gradidge T, Coakham HB. Trigeminal neuralgia due to multiple sclero-sis: ultrastructural findings in trigeminal rhizotomy specimens. NeuropatholAppl Neurobiol 2001; 27: 238–44.
34. Resnick DK, Jannetta PJ, Lunsford LD, Bissonette DJ. Microvascular decom-pression for trigeminal neuralgia in patients with multiple sclerosis. SurgNeurol 1996; 46: 358–61.
35. Hooge JP, Redekop WK. Trigeminal neuralgia in multiple sclerosis. Neurology1995; 45: 1294–6.
36. Meaney JF, Watt JW, Eldridge PR et al. Association between trigeminal neuralgiaand multiple sclerosis: role of magnetic resonance imaging. J Neurol NeurosurgPsychiatry 1995; 59: 253–9.
37. Jensen TS, Rasmussen P, Reske-Nielsen E. Association of trigeminal neuralgiawith multiple sclerosis: clinical and pathological features. Acta Neurol Scand1982; 65: 182–9.
55
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 55

38. Lazar ML, Kirkpatrick JB. Trigeminal neuralgia and multiple sclerosis:demonstration of the plaque in an operative case. Neurosurgery 1979; 5:711–17.
39. Meaney JF, Watt JW, Eldridge PR et al. Association between trigeminal neural-gia and multiple sclerosis: role of magnetic resonance imaging. J NeurolNeurosurg Psychiatry 1995; 59: 253–9.
40. Golby AJ, Norbash A, Silverberg GD. Trigeminal neuralgia resultingfrom infarction of the root entry zone of the trigeminal nerve: case report.Neurosurgery 1998; 43: 620–2.
41. Love S, Gradidge T, Coakham HB. Trigeminal neuralgia due to multiple sclero-sis: ultrastructural findings in trigeminal rhizotomy specimens. NeuropatholAppl Neurobiol 2001; 27: 238–44.
42. Coffey RJ, Fromm GH. Familial trigeminal neuralgia and Charcot-Marie-Toothneuropathy. Report of two families and review. Surg Neurol 1991; 35: 49–53.
43. Broggi G, Ferroli P, Franzini A, Servello D, Dones I. Microvascular decompres-sion for trigeminal neuralgia: comments on a series of 250 cases, including10 patients with multiple sclerosis. J Neurol Neurosurg Psychiatry 2000; 68:59–64.
44. Meaney JF, Miles JB, Nixon TE et al. Vascular contact with the fifth cranialnerve at the pons in patients with trigeminal neuralgia: detection with 3D FISPimaging. AJR Am J Roentgenol 1994; 163: 1447–52.
45. Chong VF. Trigeminal neuralgia in nasopharyngeal carcinoma. J Laryngol Otol1996; 110: 394–6.
46. Boerman RH, Maassen EM, Joosten J et al. Trigeminal neuropathy secondary toperineural invasion of head and neck carcinomas. Neurology 1999; 53: 213–16.
47. Love S, Bateman DE, Hirschowitz L. Bilateral lambda light chain amyloidomasof the trigeminal ganglia, nerves and roots. Neuropathol Appl Neurobiol 1997;23: 512–15.
48. Golby AJ, Norbash A, Silverberg GD. Trigeminal neuralgia resulting frominfarction of the root entry zone of the trigeminal nerve: case report.Neurosurgery 1998; 43: 620–2.
49. Peterson AM, Williams RL, Fukui MB, Meltzer CC. Venous angioma adjacentto the root entry zone of the trigeminal nerve: implications for management oftrigeminal neuralgia. Neuroradiology 2002; 44: 342–6.
50. Harris W. Bilateral trigeminal tic: its association with hereditary and dissemi-nated sclerosis [letter]. Ann Surg 1936; 103: 161.
51. Harris W. An analysis of 1,433 cases of paroxysmal trigeminal neuralgia andthe end results of gasserian alcohol injection. Brain 1940; 43: 209–44.
52. Allan W. Familial occurrence of tic douloreaux. Arch Neurol Psychiatry 1938;40: 1019–20.
53. Herzberg L. Familial trigeminal neuralgia. Arch Neurol 1980; 37: 285–6.
56
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 56

54. Duff JM, Spinner RJ, Lindor NM, Dodick DW, Atkinson JL. Familial trigem-inal neuralgia and contralateral hemifacial spasm. Neurology 1999; 53:216–18.
55. Katusic S, Beard CM, Bergstralh E, Kurland LT. Incidence and clinical featuresof trigeminal neuralgia, Rochester, Minnesota, 1945–1984. Ann Neurol 1990;27: 89–95.
56. Knuckey NW, Gubbay SS. Familial trigeminal and glossopharyngeal neuralgia.Clin Exp Neurol 1979; 16: 315–19.
57. Devor M, Govrin-Lippmann R, Rappaport ZH. Mechanism of trigeminal neu-ralgia: an ultrastructural analysis of trigeminal root specimens obtained duringmicrovascular decompression surgery. J Neurosurg 2002; 96: 532–43.
58. Adams CB. Microvascular compression: an alternative view and hypothesis. JNeurosurg 1989; 70: 1–12.
59. Bowsher D, Miles JB, Haggett CE, Eldridge PR. Trigeminal neuralgia: a quan-titative sensory perception threshold study in patients who had not undergoneprevious invasive procedures. J Neurosurg 1997; 86: 190–2.
60. Sinay VJ, Bonamico LH, Dubrovsky A. Subclinical sensory abnormalities intrigeminal neuralgia. Cephalalgia 2003; 23: 541–4.
61. Rappaport ZH, Devor M. Trigeminal neuralgia: the role of self-sustaining dis-charge in the trigeminal ganglion. Pain 1994; 56: 127–38.
62. Devor M, Amir R, Rappaport ZH. Pathophysiology of trigeminal neuralgia: theignition hypothesis. Clin J Pain 2002; 18: 4–13.
63. Rappaport ZH, Devor M. Trigeminal neuralgia: the role of self-sustaining dis-charge in the trigeminal ganglion. Pain 1994; 56: 127–38.
64. Baumann TK, Martenson ME. Spontaneous action potential discharge in culturedorsal root ganglion neurons from patients with neuropathic pain. In: Devor M,Rowbotham MC, Wiesenfeld-Hallin Z, eds. Proceedings of the 9th WorldCongress on Pain, Seattle: IASP Press, 2000: 101–8.
65. Kocsis JD, Devor M. Altered excitability of large-diameter cutaneous afferentsfollowing nerve injury: consequences for chronic pain. In: Devor M,Rowbotham MC, Wiesenfeld-Hallin Z, eds. Proceedings of the 9th WorldCongress on Pain. Seattle: IASP Press, 2000: 119–35.
66. Scholz J.Woolf CJ. Can we conquer pain? Nat Neurosci 2002; 5(Suppl1):1062–7.
67. Moore KA, Kohno T, Karchewski LA, Scholz J, Baba H, Woolf CJ. Partialperipheral nerve injury promotes a selective loss of GABAergic inhibition inthe superficial dorsal horn of the spinal cord. J Neurosci 2002; 22: 6724–31.
68. Fromm GH, Chattha AS, Terrence CF, Glass JD. Role of inhibitory mecha-nisms in trigeminal neuralgia. Neurology 1981; 31: 683–7.
69. Fromm GH. Effects of different classes of antiepileptic drugs on brain-stempathways. Fed Proc 1985; 44: 2432–5.
57
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 57

70. Fromm GH, Terrence CF, Chattha AS. Differential effect of antiepileptic andnon-antiepileptic drugs on the reticular formation. Life Sci 1984; 35: 2665–73.
71. Dubner R, Sharav Y, Gracely RH, Price DD. Idiopathic trigeminal neuralgia:sensory features and pain mechanisms. Pain 1987; 31: 23–33.
72. Woolf CJ. Dissecting out mechanisms responsible for peripheral neuropathicpain: implications for diagnosis and therapy. Life Sci 2004; 74: 2605–10.
73. Woolf CJ. Pain: moving from symptom control toward mechanism-specificpharmacologic management. Ann Intern Med 2004; 140: 441–51.
74. Knyihar-Csillik E, Tajti J, Csillik AE et al. Effects of eletriptan on the peptider-gic innervation of the cerebral dura mater and trigeminal ganglion, and on theexpression of c-fos and c-jun in the trigeminal complex of the rat in an experi-mental migraine model. Eur J Neurosci 2000; 12: 3991–4002.
75. Wotherspoon G, Priestley JV. Expression of the 5-HT1B receptor by subtypesof rat trigeminal ganglion cells. Neuroscience 2000; 95: 465–71.
76. Costigan M, Befort K, Karchewski L et al. Replicate high-density rat genomeoligonucleotide microarrays reveal hundreds of regulated genes in the dorsalroot ganglion after peripheral nerve injury. BMC Neurosci 2002; 3: 16.
77. Xiao HS, Huang QH, Zhang FX et al. Identification of gene expression pro-file of dorsal root ganglion in the rat peripheral axotomy model of neuro-pathic pain. Proc Natl Acad Sci U S A 2002; 99: 8360–5.
78. Rabert D, Xiao Y, Yiangou Y et al. Plasticity of gene expression in injuredhuman dorsal root ganglia revealed by GeneChip oligonucleotide microarrays. JClin Neurosci 2004; 11: 289–99.
79. Wang H, Sun H, Della PK et al. Chronic neuropathic pain is accompanied byglobal changes in gene expression and shares pathobiology with neurodegener-ative diseases. Neuroscience 2002; 114: 529–46.
80. Kim DS, Lee SJ, Park SY et al. Differentially expressed genes in rat dorsal rootganglia following peripheral nerve injury. Neuroreport 2001; 12: 3401–5.
81. Newton RA, Bingham S, Davey PD et al. Identification of differentiallyexpressed genes in dorsal root ganglia following partial sciatic nerve injury.Neuroscience 2000; 95: 1111–20.
82. Noguchi K, Kawai Y, Fukuoka T, Senba E, Miki K. Substance P induced byperipheral nerve injury in primary afferent sensory neurons and its effect ondorsal column nucleus neurons. J Neurosci 1995; 15: 7633–43.
83. Yaksh TL, Hua XY, Kalcheva I, Nozaki-Taguchi N, Marsala M. The spinalbiology in humans and animals of pain states generated by persistent smallafferent input. Proc Natl Acad Sci U S A 1999; 96: 7680–6.
84. Li J, Simone DA, Larson AA. Windup leads to characteristics of central sensiti-zation. Pain 1999; 79: 75–82.
85. Luo ZD, Chaplan SR, Higuera ES et al. Upregulation of dorsal root ganglion(alpha)2(delta) calcium channel subunit and its correlation with allodynia inspinal nerve-injured rats. J Neurosci 2001; 21: 1868–75.
58
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 58

86. Newton RA, Bingham S, Case PC, Sanger GJ, Lawson SN. Dorsal root ganglionneurons show increased expression of the calcium channel alpha2delta-1 subunitfollowing partial sciatic nerve injury. Brain Res Mol Brain Res 2001; 95: 1–8.
87. Field MJ, Hughes J, Singh L. Further evidence for the role of the alpha(2)deltasubunit of voltage dependent calcium channels in models of neuropathic pain.Br J Pharmacol 2000; 131: 282–6.
88. Cho HS, Kim MH, Choi DH et al. The effect of intrathecal gabapentin onmechanical and thermal hyperalgesia in neuropathic rats induced by spinalnerve ligation. J Korean Med Sci 2002; 17: 225–9.
89. Wieseler-Frank J, Maier SF, Watkins LR. Glial activation and pathological pain.Neurochem Int 2004; 45: 389–95.
90. Sweitzer S, Martin D, DeLeo JA. Intrathecal interleukin-1 receptor antagonist incombination with soluble tumor necrosis factor receptor exhibits an anti-allodynicaction in a rat model of neuropathic pain. Neuroscience 2001; 103: 529–39.
91. Neubert MJ, Kincaid W, Heinricher MM. Nociceptive facilitating neurons inthe rostral ventromedial medulla. Pain 2004; 110: 158–65.
92. Burgess SE, Gardell LR, Ossipov MH et al. Time-dependent descending facili-tation from the rostral ventromedial medulla maintains, but does not initiate,neuropathic pain. J Neurosci 2002; 22: 5129–36.
93. Mogil JS. The genetic mediation of individual differences in sensitivity to painand its inhibition. Proc Natl Acad Sci U S A 1999; 96: 7744–51.
94. Mogil JS, Yu L, Basbaum AI. Pain genes?: natural variation and transgenicmutants. Annu Rev Neurosci 2000; 23: 777–811.
95. Mogil JS, McCarson KE. Identifying pain genes: bottom-up and top-downapproaches. J Pain 2000; 1(3 Suppl): 66–80.
96. Flores CM, Mogil JS. The pharmacogenetics of analgesia: toward a genetically-based approach to pain management. Pharmacogenomics 2001; 2: 177–94.
97. Stahl SM. Anticonvulsants and the relief of chronic pain: pregabalin andgabapentin as alpha(2)delta ligands at voltage-gated calcium channels. J ClinPsychiatry 2004; 65: 596–7.
98. Chesler EJ, Ritchie J, Kokayeff A et al. Genotype-dependence of gabapentinand pregabalin sensitivity: the pharmacogenetic mediation of analgesia is spe-cific to the type of pain being inhibited. Pain 2003; 106: 325–35.
99. Ecker AD, Smith JE. Are latent, immediate-early genes of herpes simplex virus-1 essential in causing trigeminal neuralgia? Med Hypotheses 2002; 59: 603–6.
100. Lunsford LD. Percutaneous retrogasserian glycerol rhizotomy. In: Rovit RL,Murali R, Jannetta PJ, eds. Trigeminal neuralgia. Baltimore: Williams &Wilkins, 1990: 145–64.
101. Behrman S, Knight G. Herpes simplex associated with trigeminal neuralgia.JAMA 1954; 246: 1564–7.
102. Kitt CA, Gruber K, Davis M, Woolf CJ, Levine JD. Trigeminal neuralgia:opportunities for research and treatment. Pain 2000; 85: 3–7.
59
03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 59

03-CMTN 8023.qxd 2/1/2007 7:42 PM Page 60

The main objective in treating trigeminal neuralgia is to relieve the patient ofpain. Clinicians should educate patients on all aspects of management andthis chapter we will present the general principles that govern the manage-ment of trigeminal neuralgia (Table 4.1). We will then review the medicationsthat are available (Table 4.2) and finally, we will discuss the clinical applica-tions of each medication and when it should be employed.
Medical versus surgical treatmentThe debate regarding surgical versus medical management continues withoutresolution. Some authors claim that early surgical intervention is best, butothers claim that patients who fail surgery are more refractory to medicalmanagement. These opinions stem from anecdotal evidence. This contro-versy will remain, but it is important to direct treatment to the individualpatient’s clinical presentation, pre-existing medical health, and personal pref-erences. With a multitude of medications and surgical options available thefinal approach to treatment will vary according to the clinician’s knowledgebase and experience and the patient’s preference.
Many consider that medication therapy should be the first line of treatmentfor trigeminal neuralgia.1 The treatment decision is not as simple as statingthat ‘all patients need to try medications first before any surgical options canbe considered’. The physician or physicians must customize the treatment ona case-by-case basis. Many factors play a role in developing a patient’s treat-ment plan: these include age, medication compliance history, concomitantmedical conditions, response to previous therapies, potential secondarycauses, the severity of the pain (which may inhibit proper caloric intake), andthe patient’s desires. Typically, surgical options have been reserved for thosepatients who have a clearly defined secondary cause for the trigeminalneuralgia, who are unresponsive, who have severe, unremitting pain that
61
4Medical management oftrigeminal neuralgia
04-CMTN 8023.qxd 2/1/2007 8:46 PM Page 61

limits their ability to eat, for whom multiple medications are intolerable orcontraindicated.
With multiple medications and surgical options available, it is important toestablish a plan of attack that makes the most of both medical and surgicaloptions. Patients need to be informed early on in the course of treatmentof multiple treatment modalities that are available. They should have bothmedical and surgical consultations, so that they understand all facets oftreatment. Medical management is often the initial attempt to control thepain, however the patient should consult with a neurosurgeon concurrently tolearn of the surgerical options that exist and are available for all patients.Consultation with a surgeon early in the treatment phase is necessary whenpatients have had multiple medication failures, severe pain escalation orare intolerant of medication side effects. Then, if medications fail to thor-oughly control the pain, then the patient has already been introduced to thesurgeon and has had time to assimilate the information regarding the variety
62
Table 4.1 Principles for treating trigeminal neuralgia
1. Both medical and surgical specialties need to be explored and it is imperative
that this occurs early in the course of treatment.
2. Antiepileptic medications remain the mainstay of pharmacotherapy for
trigeminal neuralgia. Some medications may be pushed to high doses to
control the pain but it is important to readjust the medication once the pain
is controlled and to use the smallest dose possible and not overtreat.
3. Watch for periods of remission and taper the medication when possible.This
allows for a medication vacation for those patients who experience periods
of remission.
4. Monotherapy is always the goal but is not always achievable. Starting at a low
dose and increasing gradually minimizes side effects. Proper dosing throughout
the day will also minimize breakthrough pain. Polypharmacy may be necessary
to achieve full relief.
5. Patient compliance with the medication titration and daily dosing is absolutely
essential to achieving success with medications.Alterations in dosing and
dosing schedules allow for recurrences of pain.
04-CMTN 8023.qxd 2/1/2007 8:46 PM Page 62

63
Tabl
e 4.
2Ph
arm
acol
ogic
choi
ces
for t
rigem
inal
neu
ralg
ia
Med
icat
ion
Trad
e na
mes
Dos
age
Side
effe
cts
Car
bam
azep
ine
Tegr
etol
,Teg
reto
l XL,
200–
1800
mg
in d
ivid
ed d
oses
2–3
N
ause
a,le
ukop
enia
,dro
wsin
ess,
Car
bitr
oltim
es d
aily,
perio
dic
bloo
d w
ork
fatig
ue,m
emor
y,di
plop
ia,li
ver
need
eddy
sfun
ctio
n,an
d he
pato
toxi
city
Oxc
arba
zepi
neTr
ilept
al30
0–18
00m
g in
2–3
div
ided
dos
es,
Diz
zine
ss,f
atig
ue,h
eada
che,
perio
dic
bloo
d w
ork
need
edtr
emor
s,co
ncen
trat
ion
prob
lem
s,
decr
ease
d so
dium
leve
ls
Gab
apen
tinN
euro
ntin
900–
3600
mg
daily
in 3
–4 d
ivid
ed
Ata
xia,
fatig
ue,n
ysta
gmus
,diz
zine
ss,
dose
sw
eigh
t ga
in
Lam
otrig
ine
Lam
icta
l10
0–60
0m
g da
ily in
2 d
ivid
ed d
oses
Diz
zine
ss,h
eada
che,
rash
,inso
mni
a,
arth
ralg
ia a
nd m
yalg
ia,
Stev
ens-
John
son
synd
rom
e
Bacl
ofen
Lior
esal
40–8
0m
g da
ily in
2–3
div
ided
dos
esEx
trem
e fa
tigue
,wea
knes
s,dr
owsin
ess
Topi
ram
ate
Topa
max
200–
400
mg
daily
in 2
div
ided
dos
esFa
tigue
,wor
d re
call
prob
lem
s,w
eigh
t
loss
,par
esth
esia
s,ta
ste
alte
ratio
ns,
rena
l sto
nes,
depr
esse
d m
ood
Sodi
um
Dep
akot
e50
0–20
00m
g da
ily in
2 d
ivid
ed d
oses
Nau
sea,
gast
roin
test
inal
ups
et,s
edat
ion,
valp
roat
e,pl
atel
et d
ysfu
nctio
n,ha
ir lo
ss,t
rem
or,
diva
lpro
exch
ange
in c
ogni
tion,
hepa
toto
xici
ty,
sodi
umw
eigh
t ga
in
(con
tinue
d)
04-CMTN 8023.qxd 2/1/2007 8:46 PM Page 63

64
Tabl
e 4.
2(C
ontin
ued)
Med
icat
ion
Trad
e na
mes
Dos
age
Side
effe
cts
Phen
ytoi
nD
ilant
in20
0–40
0m
g da
ily in
a s
ingl
e do
se o
r D
izzi
ness
,dro
wsin
ess,
rash
,inso
mni
a,
in 2
div
ided
dos
esat
axia
,gin
givi
tis
Clo
naze
pam
Klon
opin
1.5–
8m
g da
ily in
3–4
div
ided
dos
esA
taxi
a,se
datio
n,de
velo
pmen
t of
tole
ranc
e,an
d w
ithdr
awal
syn
drom
e if
sudd
enly
disc
ontin
ued
Felb
amat
eFe
lbat
ol12
00–3
600
mg
daily
in 3
div
ided
dos
esA
nore
xia,
vom
iting
,inso
mni
a,na
usea
,
dizz
ines
s,so
mno
lenc
e,an
d he
adac
he,
mul
tiple
dru
g in
tera
ctio
ns
Pim
ozid
eO
rap
Base
d on
wei
ght
and
not
to e
xcee
d N
euro
mus
cula
r (e
xtra
pyra
mid
al)
10m
g pe
r da
yre
actio
ns,m
ultip
le d
rug
inte
ract
ions
Zon
isam
ide
Zon
egra
n20
0–40
0m
g da
ily in
2 d
ivid
ed d
oses
Som
nole
nce,
anor
exia
,diz
zine
ss,
head
ache
,nau
sea,
and
agita
tion/
irrita
bilit
y
Preg
abal
inLy
rica
100–
600
mg
daily
in 2
div
ided
dos
esSo
mno
lenc
e,di
zzin
ess,
atax
ia,c
onfu
sion,
asth
enia
,abn
orm
al t
hink
ing,
blur
red
visio
n,in
coor
dina
tion,
and
perip
hera
l ede
ma
04-CMTN 8023.qxd 2/1/2007 8:46 PM Page 64

of procedures available. Or if the patient’s trigeminal neuralgia pain wasoriginally controlled with medications, but he or she becomes less responsiveto the medications or the patient develops other medical conditions precludethe medication being continued, again it is advantageous for the patientto have already consulted the surgeon. The surgical options available arediscussed in Chapter 5.
Antiepileptic medications are the mainstayof medical management In general, pharmacological management of neuropathic pain ranges fromantidepressants and anticonvulsants, to topical medications such as capsaicin.Even though trigeminal neuralgia is a type of neuropathic pain and sharesseveral similar underlying mechanisms, not all pharmacologic therapies thatare available for neuropathic pain have been proven effective for trigeminalneuralgia. The pharmacological management of trigeminal neuralgia exploitscompounds with the capacity to decrease neuronal hyperexcitability eitherperipherally or centrally. Clinically, the goal of medication is to provide rapidand sustainable pain relief with the fewest side effects. Unfortunately, the clinicaltrials for trigeminal neuralgia are not robust enough to enable us to fully ana-lyze the usefulness of each medication; therefore, each patient is evaluatedindividually, taking into account age, other systemic illnesses, severity of thepain, and previous medications tried, following which medication choices aremade.
Remission periodsTrigeminal neuralgia may remit for periods that vary in length. Days, weeks,months, or even years may pass without an attack; however, in most casesthe pain eventually returns and the patient requires further medical treatment.Remission may occur during treatment; so if the patient has been withoutan attack for several months, it can be beneficial to slowly taper the cur-rent medication, and if the patient has truly entered a remission period, nomedication will be necessary until the remission period ends. If the patienthas experienced several weeks of no pain but is still experiencing some sideeffects, it is worth lowering the dose to eliminate the side effects. Routinefollow-up visits are essential to elicit side effect details. Many patients withtrigeminal neuralgia tend to under-report side effects, because the sideeffects are much less severe than the pain of trigeminal neuralgia.
65
04-CMTN 8023.qxd 2/1/2007 8:46 PM Page 65

Monotherapy versus polypharmacyIn general, medications are begun at a low dose and titrated up gradually,with close clinical monitoring, until either the maximum tolerated dose orpain-free dose is attained. The slow titration allows for fewer side effects andprevents over-treatment. Although monotherapy is a goal of therapy manypatients have severe side effects or limited benefit from one medication, andin this case, a second medication may be used. Often a combination ofantiepileptic medications is needed to achieve pain relief.
Patient compliance is necessary for successTo determine what benefit, if any, is being achieved it is essential that thepatient comply with his medication regime. Often, as pain relief is achievedor an unrecognized side effect becomes problematic, the patient may taperthe medication personally, only to report the pain starting again. It isimportant to counsel patients to be extremely compliant in order to fairlyassess and achieve maximum benefit from the medications. Close communi-cation between the treating clinician and the patient creates the best chancefor treatment success. It is also important to point out to the patient that ther-apeutic benefit may lag behind the medication’s titration schedule, soalthough the medication dosage is no longer being increased, the maximumbenefit of the medication may yet be realized over the coming weeks.
Available compounds (Table 4.2)For years, the gold standard of medication treatment has been carba-mazepine, 100 – 200 mg, two or three times daily, which provides benefit tomore than 75% of patients. Today there are multiple medications from whichto choose, but a response to carbamazepine has been described as beingalmost diagnostic.
If the initial medication is not tolerated due to side effects, then an alternativemedication is employed. For example, if carbamazepine is not tolerated, othermedications, including baclofen,2–8 sodium valproate,9 gabapentin,10–14
lamotrigine,11,12,15–19 oxcarbazepine,20–24 topiramate,20,25,26 felbamate,27
zonisamide, pregabalin, and clonazepam,28,29 are sometimes effective, butadequate formal studies of the therapeutic efficacy of most of these agentshave not been performed. There is a continuing need for new anti-neuralgicmedications because of the limited tolerance and limited efficacy of thoseagents already available.30
66
04-CMTN 8023.qxd 2/1/2007 8:46 PM Page 66

Carbamazepine For years carbamazepine (CBZ) has been taught as the gold standard intreating trigeminal neuralgia. Some authors have labeled a response to carba-mazepine as almost ‘diagnostic’. The initial study was done in 1962 and thisagent was effective in nearly 75% of the patients tested. The studies looking atcarbamazepine are not homogenous and are wrought with flaws. Long-termfollow-up data come mostly from open-label reports and show a severe declinein carbamazepine’s efficacy over time. Carbamazepine induces its own metabo-lism through autoinduction in the liver; therefore, the half-life drops drasticallywith time and the pain of trigeminal neuralgia returns. This return of the pain ismet with an increase in the dose, and if the pain is controlled again it becomesa matter of time until it returns. The cycle is repeated until the patient experi-ences too many side effects and pain becomes uncontrolled. Common sideeffects are severe fatigue, drowsiness, dizziness, ataxia, gastric pain, and con-stipation. Patients state that they feel ‘medicated’. Memory issues may inhibittolerance, and visual disturbances such as diplopia and nystagmus, are consid-ered signs of the patient reaching a toxic level.
The medication is sometimes better tolerated if it is taken at mealtimes, or ifthe extended-release formulations (Tegretol XR or Carbitrol) are used. Themedications are often dosed three to four times per day, which allows formissed doses and lack of full compliance by the patient. Long-term hepaticsuppression and hepatotoxicity are always a concern with this medication, androutine blood count and liver function tests need to be performed when apatient is on this medication.
In summary, carbamazepine may offer quick initial relief, but with neweragents available, its use is limited. Many physicians were taught to treat withcarbamazepine and as it fails and the patient becomes desperate to alleviatethe pain, he or she is referred to neurosurgery for evaluation and treatment.Many newer agents are nearly as effective and can sustain relief with fewerside effects.
OxcarbazepineOxcarbazepine (OBZ) is the 10-keto derivative of carbamazepine and can bevery effective and less susceptible to autoinduction. Oxcarbazepine is muchbetter tolerated than carbamazepine and is usually dosed two to three times perday, which aids in patient compliance. Oxcarbazepine can be increased morerapidly than the other antiepileptic drugs (AEDs), which helps in treatingpatients who are disabled due to extreme pain and/or are having very frequent
67
04-CMTN 8023.qxd 2/1/2007 8:46 PM Page 67

attacks. Blood count and liver function still need to be followed. Hyponatremiadoes occur in a subset of patients.
GabapentinGabapentin has only been studied in patients who have failed carbamazepine.Dosages vary greatly from 300 and 3600 mg in divided doses three to five timesdaily. Bioavailability of gabapentin at higher doses decreases drastically andtherefore less medication, dosed more times a day may be the best way ofachieving the highest blood levels. However, the compliance in taking the med-ication more times a day becomes problematic resulting in missed doses. Thiscreates variations in the blood levels allowing for intermittent breakthroughattacks, and sustained pain relief is often not achieved.
LamotrigineLamotrigine is a sodium channel blocker that has been shown to have beneficialresults in double-blind studies. Allergic reactions, including a higher incidence ofStephen-Johnson’s syndrome, have made many physicians wary of this medica-tion. With a slower titration, this medication is an excellent addition to othertherapies and anecdotally can work as monotherapy in dosages from 150 to600 mg in twice-daily dosing. The side effect profile is much better for Lamictal,and autoinduction does not seem to occur. If it is added to enzyme-inducing anti-epileptic drugs like carbamazepine the dosage may need to be pushed higher toachieve benefit. Once benefit is realized, the other anti-epileptic drug can bereduced and often eliminated. At this point, the patient may experience increasedside effects from the greater availability of the lamotrigine. Side effects includedizziness, headache, nausea, constipation, myalgia, and arthralgia.
BaclofenBaclofen was always known to potentiate the effects of work synergisticallywith carbamazepine, and therefore, many physicians were taught to addbaclofen as carbamazepine begins to fail to re-establish pain relief and extendthe usefulness of carbamazepine. Baclofen can also work as monotherapy andhas been shown to do so in two double-blind trials. However, clinically, fewpatients can tolerate the sedation it causes. With a short half-life, it requiresfrequent dosing, again allowing for missed doses.
Topiramate Topiramate has extremely limited evidence. In the one double-blind study thatwas performed, only three patients were tested. Topiramate has a long half-life
68
04-CMTN 8023.qxd 2/1/2007 8:46 PM Page 68

and can easily be dosed twice a day. The side effects include paresthesias,increased incidence of renal stones, taste alterations, and cognitive impairmentin the form of word recall issues. Weight loss is also reported as a side effect.
Sodium valproate Sodium valproate is a GABA agonist that is usually dosed two to three timesper day. The doses range from 500 to 2000 mg. Side effects are greatlyreduced by using enteric coated formulations or the newer extended-releaseformulation. The medication is metabolized by the liver and is contraindi-cated in hepatic disease. Hair loss, weight gain, and fatigue often limit itstolerability. Blood work must be performed to monitor liver functioning.Multiple interactions exist between this compound and many of the otheranti-epileptic drugs so caution must be used when using this in combinationwith other medications.
Clonazepam Clonazepam is a benzodiazepine that may be effective from 2 to 8 mg individed doses. Many patients experience extreme drowsiness, ataxia, and evenmood or personality changes. Withdrawal from this medication can be seriousand every effort must be made to avoid patients running out of medication.Again, compliance is extremely important.
Other agentsFelbamate and pimozide both have untoward side effects and are generallyreserved for extremely refractory cases that have failed all other medicationchoices.
Zonisamide and pregabalin have not been studied and have no reports of effi-cacy at this time.
Phenytoin is a much older anti-epileptic drug that has been shownto have some benefit but is very much limited by its side effects. The IVformulation can be very effective for patients hospitalized due to the painof trigeminal neuralgia. Drowsiness, ataxia, nystagmus, slurred speech,dizziness, gingivitis, and rash all can occur and limit its tolerability.Compliance with this medication is extremely important because increasesin the dosing by the patient to control the pain may result in the emergenceof side effects.
69
04-CMTN 8023.qxd 2/1/2007 8:46 PM Page 69

ConclusionsWith the lack of controlled trials, strong evidence for comparison ofcompounds is unavailable. Physicians must be aware that there are now sev-eral compounds on the market that all may be effective in a subset of patientswith trigeminal neuralgia. No single compound works in all patients. An inti-mate knowledge of pharmacodynamics, and physician persistence coupled withpatient compliance, yield benefit for many patients. Lamotrigine, gabapentin,topiramate, and oxcarbazepine may be more effective and better toleratedthan the older carbamazepine and phenytoin. Surgical consultation early inthe treatment planning should become the standard of care. A close relation-ship between medical and surgical providers helps to streamline treatmentand lessens needless patient suffering.
References1. Fields WS, Lemak NA. Trigeminal neuralgia: historical background, etiology,
and treatment. BNI Q 1987; 3: 47–56.2. Parmar BS, Shah KH, Gandhi IC. Baclofen in trigeminal neuralgia – a clinical
trial. Indian J Dent Res 1989; 1: 109–13.3. Fromm GH, Terrence CF. Comparison of L-baclofen and racemic baclofen in
trigeminal neuralgia. Neurology 1987; 37: 1725–8.4. Baker KA, Taylor JW, Lilly GE. Treatment of trigeminal neuralgia: use of
baclofen in combination with carbamazepine. Clin Pharm 1985; 4: 93–6.5. Hershey LA. Baclofen in the treatment of neuralgia. Ann Intern Med 1984; 100:
905–6.6. Fromm GH, Terrence CF, Chattha AS. Baclofen in the treatment of trigeminal
neuralgia: double-blind study and long-term follow-up. Ann Neurol 1984; 15:240–4.
7. Steardo L, Leo A, Marano E. Efficacy of baclofen in trigeminal neuralgia andsome other painful conditions. A clinical trial. Eur Neurol 1984; 23: 51–5.
8. Fromm GH, Terrence CF, Chattha AS, Glass JD. Baclofen in trigeminal neural-gia: its effect on the spinal trigeminal nucleus: a pilot study. Arch Neurol 1980;37: 768–71.
9. Peiris JB, Perera GL, Devendra SV, Lionel ND. Sodium valproate in trigeminalneuralgia. Med J Aust 1980; 2: 278.
10. Cheshire WP Jr. Defining the role for gabapentin in the treatment of trigeminalneuralgia: a retrospective study. J Pain 2002; 3: 137–42.
11. Solaro C, Messmer UM, Uccelli A, Leandri M, Mancardi GL. Low-dose gaba-pentin combined with either lamotrigine or carbamazepine can be useful thera-pies for trigeminal neuralgia in multiple sclerosis. Eur Neurol 2000; 44: 45–8.
70
04-CMTN 8023.qxd 2/1/2007 8:46 PM Page 70

12. Carrazana EJ, Schachter SC. Alternative uses of lamotrigine and gabapentin inthe treatment of trigeminal neuralgia. Neurology 1998; 50: 1192.
13. Sist T, Filadora V, Miner M, Lema M. Gabapentin for idiopathic trigeminalneuralgia: report of two cases. Neurology 1997; 48: 1467.
14. Khan OA. Gabapentin relieves trigeminal neuralgia in multiple sclerosispatients. Neurology 1998; 51: 611–14.
15. Leandri M, Lundardi G, Inglese M et al. Lamotrigine in trigeminal neuralgiasecondary to multiple sclerosis. J Neurol 2000; 247: 556–8.
16. Canavero S, Bonicalzi V. Lamotrigine control of trigeminal neuralgia: anexpanded study. J Neurol 1997; 244: 527.
17. Lunardi G, Leandri M, Albano C et al. Clinical effectiveness of lamotrigine andplasma levels in essential and symptomatic trigeminal neuralgia. Neurology1997; 48: 1714–17.
18. Canavero S, Bonicalzi V, Ferroli et al. Lamotrigine control of idiopathic trigemi-nal neuralgia. J Neurol Neurosurg Psychiatry 1995; 59: 646.
19. Zakrzewska JM, Chaudhry Z, Nurmikko TJ, Patton DW, Mullens EL.Lamotrigine (lamictal) in refractory trigeminal neuralgia: results from a double-blind placebo controlled crossover trial. Pain 1997; 73: 223–30.
20. Solaro C, Uccelli MM, Brichetto G, Gaspperini C, Mancardi G. Topiramaterelieves idiopathic and symptomatic trigeminal neuralgia. J Pain SymptomManage 2001; 21: 367–8.
21. Zakrzewska JM, Patsalos PN. Long-term cohort study comparing medical(oxcarbazepine) and surgical management of intractable trigeminal neuralgia.Pain 2002; 95: 259–66.
22. Grant SM, Faulds D. Oxcarbazepine. A review of its pharmacology and thera-peutic potential in epilepsy, trigeminal neuralgia and affective disorders. Drugs1992; 43: 873–88.
23. Patsalos PN, Elyas AA, Zakrzewska JM. Protein binding of oxcarbazepine andits primary active metabolite, 10-hydroxycarbazepine, in patients with trigemi-nal neuralgia. Eur J Clin Pharmacol 1990; 39: 413–15.
24. Zakrzewska JM, Patsalos PN. Oxcarbazepine: a new drug in the management ofintractable trigeminal neuralgia. J Neurol Neurosurg Psychiatry 1989; 52: 472–6.
25. Gilron I, Booher SL, Rowan JS, Max MB. Topiramate in trigeminal neuralgia:a randomized, placebo-controlled multiple crossover pilot study. Clin Neuro-pharmacol 2001; 24: 109–12.
26. Zvartau-Hind M, Din MU, Gilani A, Lisak RP, Khan OA. Topiramate relievesrefractory trigeminal neuralgia in MS patients. Neurology 2000; 55: 1587–8.
27. Cheshire WP. Felbamate relieved trigeminal neuralgia. Clin J Pain 1995; 11:139–42.
28. Caccia MR. Clonazepam in facial neuralgia and cluster headache. Clinical andelectrophysiological study. Eur Neurol 1975; 13: 560–3.
71
04-CMTN 8023.qxd 2/1/2007 8:46 PM Page 71

29. de Negrotto OV, Dalmas JF, Negrotto A. [Trigeminal neuralgia. Treatment withclonazepam.] Acta Neurol Latinoam 1974; 20: 139–45.
30. Fisher A, Zakrzewska JM, Patsalos PN. Trigeminal neuralgia: current treatmentsand future developments. Expert Opin Emerg Drugs 2003; 8: 123–43.
72
04-CMTN 8023.qxd 2/1/2007 8:46 PM Page 72

IntroductionSurgical intervention is most commonly considered when trigeminalneuralgia is refractory to medical management. Circumstances constitutingfailure of medical therapy should be determined by both doctor and patient.Certainly, persistence of pain despite rigorous trial of medications, eitherindividually or in combination, should lead to a consideration of surgicaloptions. Even a patient whose pain is initially well controlled medically mayeventually become a surgical candidate if the condition becomes refractoryto treatment. Furthermore, a significant number of patients whose pain isotherwise controlled become functionally incapacitated by the side effectsof medication. The most common side effects from medication are oftendescribed as cognitive slowness or dullness that is unacceptable to patients.Thus, doctors medically managing trigeminal neuralgia need to carefullyconsider patients’ complaints regarding the side effects and be open todiscuss the possibility of a surgical alternative.
The ideal surgical procedure for the treatment of trigeminal neuralgia wouldproduce long-lasting pain relief and minimal neurological deficit, and wouldbe simple and safe to administer.1 Many procedures are currently availablefor trigeminal neuralgia and some of the more commonly used include:microvascular decompression, glycerol rhizotomy, balloon decompression,radio frequency rhizotomy, and gamma knife radiosurgery. There are no ran-domized controlled trials to guide comparisons of their relative safety andefficacy of the various surgical procedures.2 In the absence of randomizedcomparisons, the relative advantages and disadvantages of these various sur-gical procedures have been debated.3,4 Surgical intervention may generate avery powerful placebo response that ethically cannot be controlled for. Othermajor questions surrounding surgery concern which patients are likely tobenefit most from which procedure and at what point over the course of their
73
Surgical management of(classic/typical/idiopathic)trigeminal neuralgia
5
05-CMTN 8023.qxd 2/1/2007 8:47 PM Page 73

disease. For example, the major predictors of recurrence in a large case seriesreceiving microvascular decompression included female sex, symptoms last-ing more than 8 years, and venous compression of the trigeminal root entryzone.5 What this suggests is the need for greater research on the mechanismsof trigeminal neuralgia, including gender-related mechanisms, research onmore advanced preoperative imaging technology, and research on matchingpatients with treatment, including the timing of the procedure relative to theduration of symptoms.
Surgical approach to managing trigeminal neuralgiaThe diagnosis of classic trigeminal neuralgia and initial medical managementhave been addressed in earlier chapters. This chapter addresses the morecommon surgical procedures used in the treatment of classic trigeminal neu-ralgia. Surgical treatment of trigeminal neuralgia is considered for thosepatients who have failed medical treatment or are unable to tolerate medicaltreatment due to side effects. Failure of medical therapy is a relative termwhich takes into account the number, duration, and maximal dosage or intol-erable side effects of medications used in attempts to control the trigeminalneuralgia. Occasionally, those who are so significantly impaired by pain thatthey are rendered unable to chew or drink may be offered surgery before fail-ing, or even beginning, medical treatment so as to avoid the prolonged timeoften associated with adding or escalating medications.
Type I and type II trigeminal neuralgia are believed to be caused by arterialand/or venous compression of the trigeminal nerve in the area of transitionfrom central to peripheral myelin (O-R zone) near the root entry zone of thenerve to the brainstem.6 Operations such as microvascular decompression(MVD) directly address the underlying pathology. This procedure requires ageneral anesthetic and retrosigmoid craniotomy/craniectomy; therefore, his-torically it has been reserved for young, healthy patients. All other surgicalinterventions for trigeminal neuralgia are directed at other areas along thecourse of the trigeminal pathway, such as the trigeminal tracts in the brain-stem, the retrogasserian nerve root, the trigeminal (gasserian) ganglion, or theperipheral trigeminal nerve distributions (V1–3).
In addition to MVD, other common surgical interventions for trigeminalneuralgia include percutaneous procedures directed at the gasserian ganglionor retrogasserian trigeminal nerve root and gamma knife radiosurgery (GKRS)treatment of the cisternal portion of the trigeminal nerve. The percuta-neous techniques include glycerol (retro)gasserian rhizotomy, radiofrequency
74
05-CMTN 8023.qxd 2/1/2007 8:47 PM Page 74

rhizotomy, and balloon compression of the trigeminal nerve. These percuta-neous procedures produce a chemical, thermal, or physical injury, respectively,to the trigeminal nerve or ganglion. GKRS produces a radiation-induced injuryof the trigeminal nerve. The percutaneous procedures, GKRS, and MVD areaddressed individually in the following sections. Less frequently used surgicaltechniques for refractory trigeminal neuralgia and other facial pain syndromesare addressed Chapter 6.
Percutaneous glycerol retrogasserian rhizotomyGlycerol rhizotomy is widely used for patients with type I, type II, or multi-ple sclerosis (MS)-related trigeminal neuralgia. Historically, this procedurewas done with absolute alcohol or phenol and subsequently with aphenol/glycerol mixture injected into the trigeminal cistern.6,7 Subsequently,Hakanson reported that glycerol alone (without phenol) could relieve facialpain with less facial sensory loss.6,8
At our institution the procedure is performed in the operating room with thepatient awake, but lightly sedated with intravenous versed and fentanyl. Thepatient is positioned supine and the ipsilateral corner of the mouth and cheekis prepared with betadyne; 1 g of intravenous Keflex is administered. A 20gauge 3.5 inch spinal needle is introduced into the cheek 2 cm lateral to thecommissure of the mouth through the buccal soft tissues. The needle isadvanced along the course of the mandibular division of the trigeminal nervebetween the pterygoid plate and the mandibular ramus to the foramen ovaleusing the Härtel technique.7 The first finger of the opposite hand is placedwithin the mouth to help avoid needle penetration of the buccal mucosa,which can lead to infection and meningitis if the procedure is continued andthe needle is then introduced into the cerebrospinal fluid (CSF). Lateraland oblique fluoroscopic views are used to confirm the appropriate trajectoryand needle depth. When the needle pierces the foramen ovale and enters thetrigeminal cistern there is usually a characteristic jaw twitch and CSF returnsthrough the needle. Lack of CSF return may be related to poor position ofthe needle or to scarring within the cistern due to prior surgery. Water solu-ble non-ionic contrast (Omnipaque) is then injected to confirm the appropri-ate position of the needle in the cistern and to estimate the volume of thecistern for glycerol injection (which can be approximately 0.2–0.5 ml).Saline is used to flush all of the contrast from the cistern. The contrast agenthas a greater density than the glycerol and if left in the cistern will causethe subsequently injected glycerol to ‘float’ on top of the contrast and
75
05-CMTN 8023.qxd 2/1/2007 8:47 PM Page 75

prevent sufficient treatment of the lower divisions of the trigeminal nerve.Alternatively, this technique can also be used intentionally to treat trigeminalneuralgia involving only the upper division(s) of the nerve (floating tech-nique) and reduce the risk of lower division numbness. Next, using care notto move the needle, the patient is brought up to a sitting position with thechin slightly flexed downward. This brings the cistern into a position that willhold the glycerol like a cup and prevent spillage of the glycerol out of the cis-tern into the posterior fossa. The predetermined volume of 99% anhydrousglycerol is injected into the trigeminal cistern and the needle is withdrawn.Proper location of the injection is often confirmed by a blush in the skinof the ipsilateral malar region. The patient may also report some tingling ormild numbness to touch in the trigeminal divisions treated. The sitting posi-tion is maintained for 2 hours in the recovery room and the patient is dis-charged home the same day. Relief from the facial pain will most often beexperienced immediately. Rarely, some patients will have trigeminal neural-gia pain following the injection and experience relief within a few hours to afew days.
Approximately 90% of patients achieved complete/immediate pain relief fol-lowing glycerol injection and 77% had good/excellent pain control overapproximately 10 years of follow-up.9,10 Facial sensory loss may occur fol-lowing glycerol rhizotomy as follows: 32–48% mild, 13% moderate, 6%dense.10,11 Facial dysesthesia has been reported in approximately 2–22%10
and anesthesia dolorosa in less than 1%.11 Transient perioral herpes outbreakis seen in up to 3.8–37% of patients up to 1 week postoperatively.10,11 Asepticmeningitis has been reported in 0.6–1.5% of patients.10,11 Intraoperativevasovagal response can occur in 15–20% of cases and does not usuallyrequire aborting of the procedure.10,11
Percutaneous balloon compressionof the trigeminal nerveThe initial concept of squeezing, manipulating, or compressing the trigeminalnerve was reported by surgeons in the 1950s and 1960s, who observed thatpatients who had the trigeminal nerve traumatized during surgery seemed tohave a better outcome with respect to pain relief. In 1983, Mullan and Lichtorreported a percutaneous technique for compression of the gasserian ganglionusing a Fogarty catheter.12 Currently, percutaneous balloon compression ismainly indicated for patients with type I or II (classic, idiopathic) trigeminalneuralgia and MS-related trigeminal neuralgia.
76
05-CMTN 8023.qxd 2/1/2007 8:47 PM Page 76

The procedure is carried out under general anesthesia. It is prudent to havetranscutaneous cardiac pacer pads in place and atropine readily availablebecause of the transient depressor response from compression of the trigemi-nal nerve. The technique involves the same patient set-up and placement of a20 gauge spinal needle into the trigeminal cistern using the Härtel techniqueand fluoroscopy as described above for glycerol injection.7 Next, a 14 gaugeneedle is introduced along the trajectory defined by the 20 gauge spinal nee-dle to the foramen ovale and the spinal needle is withdrawn. Prior to penetra-tion of the foramen ovale, the sharp stylet of the 14 gauge needle is replacedwith a blunt stylet so as to avoid injury to the trigeminal nerve/ganglion.Once the needle has entered the foramen ovale, the blunt stylet is withdrawnand a no.# 4 Fogarty catheter is advanced into the Meckel’s cave/trigeminalcistern approximately 1.5–2.0 cm beyond the foramen. The balloon is theninflated with 0.75–1.0 ml of contrast (Omnipaque) with a tuberculin syringeor with an insufflating pump. The pump can allow precise titration of theintraluminal balloon pressure, which is typically 1200–1500 mmHg. Theideal position for the balloon is at the entrance to Meckel’s cave (poroustrigeminus), resulting in a pear-shaped configuration of the balloon with thelarger portion in the trigeminal cistern and the smaller portion in the sub-arachnoid space posterior to the petrous bone (prepontine cistern). This posi-tion allows adequate compression of the retrogasserian trigeminal nervefibers in the confines of the porous trigeminus, where the nerve is sur-rounded by the firm dura above and the petrous bone below. The balloon iskept inflated for 1 minute. There is often a cardiac depressor response whenthe balloon is inflated, followed by a compensatory hypertensive responseduring which the anesthesiologist will have to manage the heart rateand blood pressure with the cardiac pacer, atropine, or anesthetics. After 1minute, the balloon is deflated and the Fogarty catheter and needle are with-drawn together. If bleeding occurs from the cheek at the needle insertion site,local compression is usually sufficient. The betadyne is washed from thecheek and a spot Band-Aid is applied. The patient is then awakened, extu-bated, and observed in the recovery room for 2–4 hours before dischargehome.
Typically, pain relief is immediate (as for the other percutaneous techniques),but can occur in a delayed fashion up to 1 week after the procedure.Numbness in the V2 and V3 distribution is the norm (approximately 80% ofpatients), but is typically mild and often improves with time to the pointwhere it is not a major problem. Most patients will have some degree of jawor pterygoid weakness, which is usually mild and often resolves over weeks
77
05-CMTN 8023.qxd 2/1/2007 8:47 PM Page 77

to months. In rare cases the unilateral symptomatic jaw weakness may bepermanent. The possibility of permanent jaw weakness makes this procedurecontraindicated for any patient with pre-existing contralateral jaw weakness,as ‘drop jaw’ can result. Theoretically, this can also be a problem when per-forming this procedure bilaterally, such as for some MS patients. Other morerare complications could include diplopia from compression of the fourth orsixth cranial nerves.
Pain relief is immediate in 92–100% of patients and recurrence rates arereported from 19 to 32% over 5–20 years.13,14 Severe sensory loss or dyses-thesias occur in 3–20% of patients.13,14 Same 3–16% of patients may developmasseter or jaw weakness, although most improve or resolve after 1 year.13,14
Transient diplopia has been reported to occur in 1.6% of patients.14 Toour knowledge, corneal anesthesia and anesthesia dolorosa have not beenreported.
Radiofrequency trigeminal(retrogasserian) rhizotomyThe theory behind the use of radiofrequency (RF) to lesion the trigeminalnerve is that it may selectively injure/destroy the unmyelinated or poorlymyelinated nociceptive nerve fibers and spare the (heavily) myelinated fiberswhich serve touch, proprioception, and motor function. The procedure con-sists of a low-current stimulation to determine the proper position of the elec-trode at the offending trigeminal nerve fibers, followed by the creation of apermanent lesion using higher current to generate enough temperature todestroy the selected nerve fibers.
Patient set up and positioning are essentially similar to those for glycerol rhi-zotomy or balloon compression. The patient is lightly sedated initially andthe needle electrode is passed through the foramen ovale using fluoroscopyand the standard trajectory of Härtel.7 After penetration of the foramen ovale,the patient must be awake for low-current stimulation and positioning of theelectrode in the distribution of the facial pain. Settings for adequate stimula-tion are usually 0.1–0.5 V at 50 Hz with a pulse duration of 1 millisecond.The final position of the electrode depends on the patient’s response to stimu-lation. Stimulation should produce a mild tingling paresthesia and diminishedpain sensation to pinprick in the distribution of the patient’s trigeminal neural-gia. By advancing or rotating the electrode tip, an experienced surgeon canselect the ophthalmic, mandibular, or maxillary division(s) of the retrogasserian
78
05-CMTN 8023.qxd 2/1/2007 8:47 PM Page 78

trigeminal nerve. Once appropriate positioning of the needle is achieved,a permanent lesion in the retrogasserian trigeminal nerve is made by begin-ning at 10 V and approximately 60 mA for a duration of 30–40 seconds andincreasing to approximately 20 V and 100 mA. The radiofrequency lesion isa thermal injury and is both time and current dependent. A thermocouplesensor can be used to carefully titrate the temperature of the electrode tip tocreate a lesion by sequentially increasing the temperature by 5°C and theduration by 10–20 seconds.
A mild paresthesia in the distribution of the facial pain is the goal of radiofre-quency treatment of trigeminal neuralgia. Significant dysesthesia or sensory lossis reported in approximately 6–28% of patients and loss of the corneal reflexmay occur in 3–8% of patients, depending on the technique employed.15–17
Certainly, when treating ophthalmic distribution trigeminal neuralgia the risk ofcorneal anesthesia and keratitis is greater. Trigeminal nerve motor weaknesshas been reported following radiofrequency treatment in up to 14% of patients;however, it is most often mild and transient.15–17 The risk of anesthesia dolorosahas been reported in 0.5–1.6% of patients.15–17 Rare complications of carotidartery injury, stroke, diplopia, meningitis, seizures, and death have beenreported.
It has been reported that 88–99% of patients obtain immediate pain relief fol-lowing radiofrequency treatment, with 20–27% recurrence rates over 9–14-year follow-up.15,16 Patients with a more dense sensory loss from theradiofrequency lesion tend to have a lower rate of recurrence, but are subjectto greater complications from dysesthesias and analgesia. One author reportedthat following recurrence of pain, 81% of patients obtained ‘good or excellent’pain relief with a second radiofrequency treatment.15
Gamma knife radiosurgery treatmentof trigeminal neuralgiaGamma knife radiosurgery (GKRS) is the only noninvasive ‘surgical’ treat-ment of trigeminal neuralgia. It is a same-day procedure performed inthe outpatient radiosurgery center. Patients are admitted to the radiosurgerycenter on the morning of treatment and intravenous access is obtained. Mildintravenous sedation with versed and fentanyl is used only during the place-ment of the Leksell stereotactic headframe. Four pin sites, two frontal andtwo occipital, are prepared with betadyne and injected with bupivacaine/bicarbonate for local analgesia. After placement of the Leksell headframe,
79
05-CMTN 8023.qxd 2/1/2007 8:47 PM Page 79

standardized measurements of the patient’s head within the frame areobtained and stereotactic magnetic resonance imaging (MRI) of the brain isperformed. The MRI data are then loaded into the Gamma Knife planningcomputer and the cisternal portion of the trigeminal nerve is identified.Gamma Plan software is used to create a treatment plan. It must be noted thatthere is no uniformly accepted treatment plan and that many centers utilizeone or two shots (isocenters) and various prescription dates. At our center, weuse a single shot (isocenter) with a 4 mm collimator delivering 90 Gy to the100% isodose line with no more than the 20% isodose line touching the adja-cent brainstem. After the treatment plan is completed by the physicist, neuro-surgeon, and radiation-oncologist, the patient is positioned supine in theGamma Knife unit. Treatment delivery can take from 45 to 90 minutes,depending on the age of the cobalt sources in the Gamma Knife system beingused. After the treatment is completed, the headframe is removed and band-ages are placed over the pin sites. The patient is observed in the radiosurgerycenter to allow complete recovery from any residual intravenous sedation anddischarged home the same day.
Although GKRS can be done under general anesthesia, a particular advantageof this technique is that it can be done with minimal IV sedation. Drawbacksare the cost of purchasing and maintaining the radiosurgery device and thelatency period between treatment and facial pain improvement. Pain relieftypically will occur after a latency period of 4–12 weeks following treatment,with a range reported of 1 day to 13 months following treatment. The rates ofpain control and recurrence of trigeminal neuralgia have been rather variablebetween reports. The variability is probably due to different pain scales usedto report outcome, follow-up duration, number of patients lost to follow-up,prior surgical treatment, the size and placement of the radiation dosage, andthe maximal radiation dose. An excellent (complete pain relief without med-ication) and good response (50–90% improved pain with or without medica-tion) can be achieved in 57–86% of patients at 1 year following radiosurgerytreatment.18,19
As with most surgical treatments for trigeminal neuralgia, recurrence offacial pain following GKRS increases with time after treatment. Pain recur-rence rates of 23%, 33%, 39%, and 44% have been reported 1, 2, 3, and 5years following radiosurgery treatment, respectively.20,21 Mild or tolerablefacial numbness can occur in up to 25–29% of patients and significant numb-ness or dysesthesia can occur in 12–18% of patients.18,22 Other complicationsof facial weakness, trigeminal motor weakness, and anesthesia dolorosa haveessentially not been reported. Greater doses of radiation correlate with both
80
05-CMTN 8023.qxd 2/1/2007 8:47 PM Page 80

higher rates of pain control and higher rates of complications, mostly consistingof facial numbness and bothersome facial dysesthesias. Patients experiencingmore facial numbness seem to have a better chance of pain control.18 Repeatradiosurgery for patients with recurrent pain has also been reported, withapproximately 50% excellent or good pain relief and an increased rate offacial sensory loss within a limited follow-up period.23 Long-term follow-upstudies of more than 10–20 years are needed. The ideal Gamma Knife doseand treatment strategy as well as the role of other radiosurgery modalities,such as linear accelerator, remain to be determined.
Microvascular decompressionof the trigeminal nerve Unlike the percutaneous techniques and GKRS described above, microvascu-lar decompression (MVD) is the only medical or surgical intervention thatdirectly addresses the presumed underlying pathology of classic trigeminalneuralgia, which is focal vascular compression of the trigeminal nerve nearthe brainstem root entry zone. The procedure requires a general anesthetic.A lumbar subarachnoid catheter may be used to drain CSF and facilitatebrain relaxation to minimize retraction during the intradural portion of theprocedure. The patient is positioned either lateral or supine with the headfixed in a Mayfield head holder. The retroauricular region is shaved andprepared with betadyne. A slightly curved retroauricular incision is madeexposing the asterion and retrosigmoid suboccipital region. The high-speeddrill is used to create a retrosigmoid craniectomy. The dura is opened with adural leaflet toward the sigmoid and transverse sinuses. The cerebellar hemi-sphere is gently retracted, allowing exposure of the trigeminal nerve and sur-rounding arachnoid membrane. Using the intraoperative microscope, thearachnoid membrane surrounding the trigeminal nerve is opened and thenerve is explored from the brainstem to the entrance of the nerve to Meckel’scave where the trigeminal nerve ganglion (gasserian ganglion) is located.Microdissection is performed under microscopic and endoscopic visualiza-tion to mobilize any arteries or veins compressing the trigeminal nerve. Oneor more Teflon sponges are then placed between the dissected blood vesselsand the trigeminal nerve to prevent continued vascular compression of thetrigeminal nerve. Veins compressing the trigeminal nerve can occasionallybe cauterized and divided. It is important to note that the compression is usu-ally arterial, most commonly a branch of the superior cerebellar artery.24
However, venous compression alone or a combination of arterial and venous
81
05-CMTN 8023.qxd 2/1/2007 8:47 PM Page 81

compression may also occur.25,26 After adequate decompression of thetrigeminal nerve is completed, the dura is closed directly or with locallyharvested pericranium to patch the dura. Exposed mastoid air cells from thecraniectomy are sealed with small pieces of locally harvested muscle fromthe incision and bone wax. The incision is re-approximated in multiplemusculofascial layers.
When offending vessels are identified and decompressed, most patientsobtain immediate relief from their facial pain. Rates of immediate pain relieffollowing MVD have been reported to be as high as 90–98%. Barker et al.reported Dr Jannetta’s large series of MVD procedures with up to 10-yearfollow-up and defined outcome as ‘excellent’ if at least 98% pain relief wasachieved without the need for medications and ‘good’ if at least 75% painrelief was achieved with only intermittent need for pain medication.27 In thatseries, excellent or good early postoperative outcome was achieved in 98% ofpatients. This number decreased to approximately 84% and 67% after 1- and10-year follow-up, respectively. Tronnier et al. reported that 64% of theirpatients were pain-free 20 years after MVD.27 Whether or not there is contin-ued recurrence of facial pain with time is debated. Some authors havereported the majority of recurrences early (within 2 years following MVD),while others have reported a more constant rate of recurrence at 3.5% annu-ally in one series.28,29
Surgical complications associated with MVD have diminished since theintroduction of regular use of brainstem and cranial nerve intraoperative neu-rophysiological monitoring. Reported complications of MVD may includecerebellar injury (0.45%), transient facial numbness (15%), mild persistentfacial numbness (12%), significant facial numbness (1.6%), facial dysesthesia(0–3.5%), hearing loss (<1%), transient or permanent facial weakness (<1%),CSF leakage (1.5–2.5%), hematoma (0.5%), and mortality (0.3%).24,30,31 Also,lower morbidity rates have been reported from high-volume centers and fromhigh-volume surgeons.31
When no arterial or venous compression is identified, the trigeminal nerve maybe ‘traumatized’ by stroking or squeezing the nerve with micro-instruments, yetthe resulting pain relief is only temporary and such manipulation can be associ-ated with trigeminal dysesthesias. Some surgeons have advocated partial sec-tioning of the sensory portion of the trigeminal nerve for negative explorationsor during repeat surgical exploration of the nerve for recurrent pain followingMVD.28,32,33
82
05-CMTN 8023.qxd 2/1/2007 8:47 PM Page 82

ConclusionFor several decades, MVD has been the standard to which each of the othersurgical treatments for classic trigeminal neuralgia have been compared.However, in an experienced surgeon’s hands any of the techniques outlined inthis chapter may be used quite successfully to manage trigeminal neuralgia.Each procedure has its own attributes and limitations, and the procedureselected must be based on the individual patient’s situation. Therefore, from asurgical perspective trigeminal neuralgia patients are probably best managedat centers that are able to offer a variety of interventions, including one ormore percutaneous techniques, GKRS, and MVD.
References1. Burchiel KJ. Surgical treatment of trigeminal neuralgia: minor operative proce-
dures. In: Fromm GH, ed. The Medical and Surgical Management of TrigeminalNeuralgia. New York: Futura Publishing, 1987: 71–99.
2. Zakrzewska JM. Trigeminal neuralgia. Prim Dent Care 1997; 4: 17–19.3. Taha JM, Tew JM Jr. Comparison of surgical treatments for trigeminal neuralgia:
reevaluation of radiofrequency rhizotomy. Neurosurgery 1996; 38: 865–871.4. Apfelbaum RI. Neurovascular decompression – the procedure of choice. Congress
of Neurological Surgeons Annual Meeting Program Book, 1998 (abstract).5. Barker FG, Jannetta PJ, Bissonette DJ, Larkins MV, Jho HD. The long-term
outcome of microvascular decompression for trigeminal neuralgia. N EnglJ Med 1996; 334: 1077–83.
6. Burchiel KJ. A new classification for facial pain. Neurosurgery 2003; 53:1164–6.
7. Härtel F. Uber die intracranielle Injektionbehandlung der Trigeminusneuralgie.Med Klin 1914; 10: 582.
8. Hakanson S. Trigeminal neuralgia treated by the injection of glycerol into thetrigeminal cistern. Neurosurgery 1981; 9: 638–46.
9. Young RF. Glycerol rhizolysis for treatment of trigeminal neuralgia. J Neurosurg1988; 69: 39–45.
10. Jho HD, Lunsford LD. Percutaneous retrogasserian glycerol rhizotomy. Currenttechnique and results. Neurosurg Clin N Am 1997; 8: 63–74.
11. Blomstedt PC, Bergenheim AT. Technical difficulties and perioperative compli-cations of retrogasserian glycerol rhizotomy for trigeminal neuralgia. StereotactFunct Neurosurg 2002; 79: 168–81.
12. Mullan S, Lichtor T. Percutaneous microcompression of the trigeminal ganglionfor trigeminal neuralgia. J Neurosurg 1983; 59: 1007–12.
83
05-CMTN 8023.qxd 2/1/2007 8:47 PM Page 83

13. Brown JA, Gouda JJ. Percutaneous balloon compression of the trigeminal nerve.Neurosurg Clin N Am 1997; 8: 53–62.
14. Skirving DJ, Dan NG. A 20-year review of percutaneous balloon compression ofthe trigeminal ganglion. J Neurosurg 2001; 94: 913–17.
15. Nugent GR. Radiofrequency treatment of trigeminal neuralgia using acordotomy-type electrode. A method. Neurosurg Clin N Am 1997; 8: 41–52.
16. Taha JM, Tew JM Jr. Treatment of trigeminal neuralgia by percutaneousradiofrequency rhizotomy. Neurosurg Clin N Am 1997; 8: 31–9.
17. Kanpolat Y, Savas A, Bekar A, Berk C. Percutaneous controlled radiofrequencytrigeminal rhizotomy for the treatment of idiopathic trigeminal neuralgia: 25-year experience with 1,600 patients. Neurosurgery 2001; 48: 524–32.
18. Pollock BE, Phuong LK, Gorman DA, Foote RL, Stafford SL. Stereotacticradiosurgery for idiopathic trigeminal neuralgia. J Neurosurg 2002; 97: 347–53.
19. Kondziolka D, Lunsford LD, Flickinger JC. Stereotactic radiosurgery for thetreatment of trigeminal neuralgia. Clin J Pain 2002; 18: 42–7.
20. Petit JH, Herman JM, Nagda S, DiBiase SJ, Chin LS. Radiosurgical treatment oftrigeminal neuralgia: evaluating quality of life and treatment outcomes. Int JRadiat Oncol Biol Phys 2003; 56: 1147–53.
21. Maesawa S, Salame C, Flickinger JC et al. Clinical outcomes after stereotacticradiosurgery for idiopathic trigeminal neuralgia. J Neurosurg 2001; 94: 14–20.
22. McNatt SA, Yu C, Giannotta SL et al. Gamma knife radiosurgery for trigeminalneuralgia. Neurosurgery 2005; 56: 1295–301.
23. Hasegawa T, Kondziolka D, Spiro R, Flickinger JC, Lunsford LD. Repeat radio-surgery for refractory trigeminal neuralgia. Neurosurgery 2002; 50: 494–500.
24. Lovely TJ, Jannetta PJ. Microvascular decompression for trigeminal neuralgia.Surgical technique and long-term results. Neurosurg Clin N Am 1997; 8: 11–29.
25. Lee SH, Levy EI, Scarrow AM, Kassam A, Jannetta PJ. Recurrent trigeminalneuralgia attributable to veins after microvascular decompression. Neurosurgery2000; 46: 356–61.
26. Matsushima T, Huynh-Le P, Miyazono M. Trigeminal neuralgia caused byvenous compression. Neurosurgery 2004; 55: 334–7.
27. Tronnier VM, Rasche D, Hamer J, Kienle AL, Kunze S. Treatment of idiopathictrigeminal neuralgia: comparison of long-term outcome after radiofrequency rhi-zotomy and microvascular decompression. Neurosurgery 2001; 48: 1261–7.
28. Burchiel KJ, Clarke H, Haglund M, Loeser JD. Long-term efficacy of microvas-cular decompression in trigeminal neuralgia. J Neurosurg 1988; 69: 35–8.
29. Elias WJ, Burchiel KJ. Trigeminal neuralgia and other neuropathic pain syn-dromes of the head and face. Curr Pain Headache Rep 2002; 6: 115–24.
30. McLaughlin MR, Jannetta PJ, Clyde BL et al. Microvascular decompression ofcranial nerves: lessons learned after 4400 operations. J Neurosurg 1999; 90: 1–8.
31. Kalkanis SN, Eskandar EN, Carter BS, Barker FG. Microvascular decompres-sion surgery in the United States, 1996 to 2000: mortality rates, morbidity rates,
84
05-CMTN 8023.qxd 2/1/2007 8:47 PM Page 84

and the effects of hospital and surgeon volumes. Neurosurgery 2003; 52:1251–61.
32. Klun B. Microvascular decompression and partial sensory rhizotomy in thetreatment of trigeminal neuralgia: personal experience with 220 patients.Neurosurgery 1992; 30: 49–52.
33. Bederson JB, Wilson CB. Evaluation of microvascular decompression and par-tial sensory rhizotomy in 252 cases of trigeminal neuralgia. J Neurosurg 1989;71: 359–67.
85
05-CMTN 8023.qxd 2/1/2007 8:47 PM Page 85

05-CMTN 8023.qxd 2/1/2007 8:47 PM Page 86

IntroductionThe medical management and surgical procedures outlined in the precedingchapters are mainly used to treat typical (idiopathic, classic, type 1) trigemi-nal neuralgia, atypical (type 2) trigeminal neuralgia, or trigeminal neuralgiarelated to multiple sclerosis. Patients with persistent or recurrent facial paindespite the usual medical and surgical interventions outlined above mayrepresent refractory cases of trigeminal neuralgia or other forms of facialpain or trigeminal neuropathy. It is critical to recognize non-trigeminal neu-ralgia facial pain, as these patients are less likely to respond to the surgicalregimens outlined in the previous chapters, yet are susceptible to the sideeffects of these procedures, further complicating the patient’s condition. Forexample, cases of secondary trigeminal neuralgia, due to structural lesionssuch as tumor or vascular malformation, are best treated by directly addressingthe underlying pathology.
In the case of true refractory trigeminal neuralgia that has not been alleviatedby many of the treatments discussed, this chapter outlines the managementstrategies and surgical procedures that are available only after the other pro-cedures have been tried or are contraindicated. On this note, it is extremelyimportant that when a patient has tried multiple modalities and still experi-ences pain from trigeminal neuralgia, a careful medical history is taken.Many additional clinical pearls exist in fully determining a timeline of treat-ment, which include exact medication dates, dosages, surgeries, side effects,and benefits.
For example, Ms Smith may say that lamotrigine did not work in the past at400 mg in two divided doses. Taken alone, this statement may make manyclinicians avoid a second trial. On piecing together a history it is found thatshe was also on 1800 mg of oxcarbazepine in three divided doses at the sametime. With intimate knowledge of the medications one may notice that since
87
Treatment of refractorytrigeminal neuralgia 6
06-CMTN 8023.qxd 2/1/2007 7:39 PM Page 87

oxcarbazepine is an enzyme-inducing antiepileptic drug (AED), the correctdosage of lamotrigine would be 600 mg when used in conjunction. Now thatshe no longer is taking an enzyme-inducing AED a second trial of lamotrigineis warranted.
A thorough history-taking as discussed in the first chapter again becomes anexcellent starting point when determining what else to offer patients withrefractory trigeminal neuralgia in terms of therapeutic options. This chapterdiscusses the additional therapies available.
AcupunctureA recent trend in pain management is nonmedicinal alternatives to medicaltherapy. Acupuncture may have some benefit in trigeminal neuralgia. Beppuet al. evaluated the effect of meridian acupuncture treatment on trigeminalneuralgia1 in 10 patients aged 26–67 years (mean 55.4 years). Five of thepatients suffered from idiopathic and five from symptomatic trigeminal neu-ralgia. The patients underwent meridian treatment by acupuncture alone oracupuncture combined with moxibustion. The acupuncture method used wasprimarily basic treatment employing only needles without electrical stimula-tion. Meridian acupuncture treatments were repeated from two to four timesa month. Five patients were restored to a pain-free state. The other fivepatients noted a decrease in pain, but with some level of pain remaining (sig-nificant pain in one patient). They concluded that meridian acupuncturetreatment is useful and can be one therapeutic approach in the managementof trigeminal neuralgia.
Ge et al.2 studied the role of acupuncture in 1500 patients with trigeminal neu-ralgia. The treatment course was 10 days (daily or every other day) and wasrepeated in 3–5 days if unsuccessful. Most patients required an average of26 sessions to obtain relief ; 539 patients were followed from 1 to 6 years, and99.2% of them were helped. Approximately 44% had a recurrence of trigemi-nal neuralgia attacks but the attacks were less severe than before therapy.Patients who had a shorter past history of trigeminal neuralgia had the bestresponse. There was no correlation between success of acupuncture and paindistribution or the patient’s age or gender. This was not a controlled trial.
Botulinum toxinBotulinum neurotoxin is used to treat various neurological disorders associ-ated with pathologically increased muscle tone.3 Botulinum toxin inhibits the
88
06-CMTN 8023.qxd 2/1/2007 7:39 PM Page 88

release of the neurotransmitter acetylcholine at the neuromuscular junction,thereby inhibiting striatal muscle contractions. Besides the reduction inmuscle tone botulinum toxin tends to reduce pain in pain syndromes associ-ated with muscle spasm. In addition, botulinum toxin has been proposed asan analgesic, suggesting alternative non-cholinergic mechanisms of action.4
Surprisingly, botulinum toxin was reported as a potential treatment fortension-type headache and migraine – both primary headache syndromeswithout an apparent muscular component. However, varying responses tobotulinum toxin have been found, overall without sufficient evidence for ageneral treatment.5,6 No randomized controlled trials (RCTs) for the use ofbotulinum toxin in trigeminal neuralgia were identified. Adverse effects werefound to be mild to moderate and dose-dependent.
Recently, botulinum toxin, specifically type A, has been reported to be effec-tive in case reports and open label studies.7–13 Placebo-controlled clinical trialsare needed to confirm these findings. The methodology in regards to the exactlocation injected and the units used as well as the duration of effect all need tobe better studied before treatment recommendations can be made.
Surgical therapies for refractory trigeminal neuralgia
Peripheral nerve blocksPeripheral nerve blocks have mostly been used diagnostically to localize painto a particular distribution of the trigeminal nerve or to provide immediatetemporary relief of facial pain. The injections are given in the region of theforamen where the trigeminal nerve division exits the skull to the face(V1/supraorbital foramen, V2/infraorbital foramen, and V3/mental foramen,inferior alveolar nerve block, long buccal, or lingual nerve block) correspon-ding to the distribution of the facial pain. Small volumes of local analgesicssuch as lidocaine or longer-lasting bupivacaine/bicarbonate may be injectedsubcutaneously in the office.
Subsequently, if a permanent block is desired absolute alcohol may beinjected in the same distribution(s). The advantage of these peripheral blocksis that they can be performed in the office without the need for any anesthesia.If the pain recurs or if a more definitive peripheral procedure is desired aperipheral trigeminal neurectomy or avulsion can be performed. Under localanalgesia and mild intravenous sedation, the supraorbital nerve and foramencan be exposed through a small eyebrow incision. The infraorbital or mentalforamen/nerve can be exposed through a small overlying skin incision or
89
06-CMTN 8023.qxd 2/1/2007 7:39 PM Page 89

through an intraoral approach through the mucosa. These procedures areusually performed in the operating room.
Electrical stimulation of the trigeminal ganglion The use of an implanted system for chronic electrical stimulation ofthe gasserian ganglion for relief of facial pain was described in 1980 byMeyerson and Hakansson.14 Young15 studied 23 patients with chronic intrac-table facial pain due to various forms of injury to the trigeminal nerve ornerve root who underwent implantation of an electrical stimulating system totreat their pain. All patients had failed previous extensive pain treatmentefforts. An electrode was implanted on the trigeminal nerve root via percuta-neous puncture of the foramen ovale. All patients experienced at least 50%reduction in pain intensity during a period of trial stimulation and underwentinternalization of the electrode and connection to a completely implantedpulse generator. Over a mean follow-up period of 24 months, six patientsreported nearly complete relief of pain and six others reported at least a 50%reduction in pain intensity using a visual analog scale. Thus, 12 (52%) of the23 patients achieved 50% or greater reduction in pain intensity. Althoughchanges in the patterns of analgesic medication usage were few, six patients(26%) now experience a normal lifestyle. Only one complication was seen –a dislocated electrode, which was easily replaced.
Holsheimer15 reviewed data from eight clinical trials involving patients whohad chronic, intractable trigeminal neuralgia. A small percutaneous stimula-tion electrode was placed through the foramen ovale to the gasserian cistern.If a percutaneous test stimulation was successful (at least 50% pain relief)the electrode was internalized and connected to a subcutaneous pulse genera-tor. Of 233 patients who had medication-resistant trigeminal neuralgia, 48%had at least a 50% long-term improvement in pain. In all, 83% of patientswho had a positive test stimulation had at least 50% long-term pain relief,and 70% had at least 75% long-term pain improvement. Patients who hadpostherpetic-induced trigeminal distribution pain did not do as well, withless than 10% of patients showing significant improvement. Van Zundertet al.17 presented five high-risk patients with idiopathic trigeminal neuralgiawho were treated with pulsed radiofrequency after multidisciplinary assess-ment, with a mean follow-up of 19.2 months (range 10–26). These patientswere at high risk due to age, co-morbidities or previous interventional andsurgical treatments. An excellent long-term effect was achieved in threeof the five patients, a partial effect in one patient, and a short-term effect in
90
06-CMTN 8023.qxd 2/1/2007 7:39 PM Page 90

one patient. No neurological side effects or complications were reported.Electrical stimulation of the trigeminal nerve root appears to be an easy andsafe technique for providing relief of trigeminal neuralgia and chronic facialpain related to injury to the trigeminal nerve in a significant number ofpatients, especially in the high-risk group.
Trigeminal nerve sectioningSectioning of the trigeminal nerve for the treatment of trigeminal neuralgiawas first reported in 1891 by Sir Victor Horsley and was performed via anextradural subtemporal middle fossa approach.18 Initially, complete section-ing of the nerve or ganglion was performed18,19 and later partial sectioningwas developed.20,21 Subsequently, Walter Dandy described a posterior fossaapproach for sectioning the cisternal segment of the trigeminal nerve.22 Thisposterior fossa open rhizotomy technique led to the recognition of the role ofvascular compression in trigeminal neuralgia, which culminated in the devel-opment of microvascular decompression.23–25 Today, some surgeons stilladvocate partial sectioning of the sensory portion of the trigeminal nervewhen no vascular compression is identified during an operation for microvas-cular decompression.26–28
Central destructive proceduresCentral destructive procedures for facial pain can involve the brainstem,thalamus/hypothalamus, and cerebral hemisphere. Primary pain and tem-perature nerve fibers from the trigeminal (gasserian) ganglion enter themid-lateral aspect of the pons and travel inferiorly within the brainstem tothe cervico-medullary region as the descending trigeminal tract and arejoined by similar fibers from cranial nerves VII, IX, and X (together calledthe descending bulbospinal tract). In the medulla, the descending bulbospinaltract synapses mainly with the caudal aspect of the trigeminal nucleus. Thisanatomy forms the basis for destructive procedures of the descending bul-bospinal tract (medullary trigeminal tractotomy) and the caudal aspect ofthe trigeminal nucleus (nucleus caudalis dorsal root entry zone – DREZ –radiofrequency lesioning). These procedures are usually performed via opensuboccipital craniectomy and C1–2 laminectomy. The main indications forthese procedures are postherpetic neuralgia, anesthesia dolorosa, andhead/neck cancer pain. Surgical complications can be significant due tobrainstem injury. Pain control rates of 50–80% have been reported, yet long-term recurrence of pain can occur.
91
06-CMTN 8023.qxd 2/1/2007 7:39 PM Page 91

The brainstem trigeminal nucleus subsequently sends secondary fibers to themidbrain periaqueductal gray area, the contralateral ventral posterior thala-mic nuclei (VPM and VPL), and to the fronto-parietal cortex of the brain.Destruction of the nuclei and tracts has been carried out with open surgicaltechniques, stereotactic surgical procedures using radiofrequency electrodes,and Gamma Knife radiosurgery. Thalamotomy (lesioning of the VPM and/orVPL thalamic nuclei) has been used for the treatment of postherpetic facialpain, anesthesia dolorosa, head/neck cancer pain, and chronic trunk/limbpain. Lesions of the frontal lobe white matter (frontal leukotomy) and thecingulated gyrus (cingulotomy) have been used to treat chronic pain. Frontalleucotomy and cingulotomy procedures may not necessarily directly reducepain, but may reduce the impact of chronic pain on patients by diminishingthe associated anxiety and depression, thereby possibly improving the qualityof life.
Peripheral nerve stimulatorsIn recent years, technology has advanced from making destructive lesions inthe brain to performing stimulation of nerves or brain nuclei allowing modu-lation of neural function. Neuromodulation provides a reversible stimulationor blockade of neural function. Transcutaneous and subcutaneous peripheraltrigeminal and occipital nerve stimulation has been employed to treatchronic face and head pain. Percutaneous placement of small electrodes ontothe trigeminal nerve or ganglion through the foramen ovale has also beenreported. Stereotactic micro-electrode placement in deep brain nuclei such asthe thalamus (VPM or VPL) or into the brainstem periaqueductal gray matterhas also been utilized to treat chronic, intractable facial pain. Anothermethod of neuromodulation for chronic facial pain is epidural electrode stim-ulation of the precentral (motor) cortex, yet the mechanism is not fully under-stood. Precentral stimulation may work by activation of non-nociceptiveneurons, which could have an inhibitory effect on associated nociceptiveneurons, whereas stimulation of postcentral (sensory) cortex seems to exac-erbate pain. Electronic and chemical neuromodulation procedures certainlyhold promise for the future treatment of facial pain as experience and tech-nology advance. However, currently many of these procedures/devices arenot approved by the US Food and Drug Administration (FDA), and thereforenot covered by most medical insurance schemes. Also, reports have hadmixed results, with often not more than 50% of patients achieving a 50%improvement in their pain.
92
06-CMTN 8023.qxd 2/1/2007 7:39 PM Page 92

ConclusionSeveral lines of research need to be pursued to improve drug and surgicaltreatments for trigeminal neuralgia. New molecular targets, carefully chosenfrom mechanism studies, need to be identified for drug development, andsimilarities or differences from other paroxysmal non-trigeminal neuropathicpain, such as the lancinating pain typically experienced by patients withbrachial plexus avulsion injuries, need to be explored. A potentiallyrich source of molecular targets are the new classes of voltage-gated ionchannels, including several sensory neuron-specific sodium channels. Pilotclinical trials are encouraged because they offer the best prospects for initialtesting of pharmacotherapies, especially for a rare condition with difficultyin patient accrual and diagnosis. Comparisons of drug and surgical treat-ments of different types are also critical to enable patients to make informeddecisions about treatment. Studies are needed to determine the best matchbetween patients (e.g. age, gender, clinical subtype, duration of symptoms)and treatments. The development and validation of outcome measures, aswell as their consistent use across studies, are especially important for theconduct of treatment research.
References1. Beppu S, Sato Y, Amemiya Y, Tode I. Practical application of meridian acupunc-
ture treatment for trigeminal neuralgia. Anesth Pain Control Dent 1992; 1: 103–8.2. Ge S, Xu B, Zhang Y. Treatment of primary trigeminal neuralgia with
acupuncture in 1500 cases. J Tradit Chin Med 1991; 11: 3–6.3. Lew MF. Review of the FDA-approved uses of botulinum toxins, including data
suggesting efficacy in pain reduction. Clin J Pain 2002; 18(6 Suppl): S142–S146.4. Aoki KR. Evidence for antinociceptive activity of botulinum toxin type A in
pain management. Headache 2003; 43 (Suppl 1): S9–S15.5. Schmitt WJ, Slowey E, Fravi N, Weber S, Burgunder JM. Effect of botulinum
toxin A injections in the treatment of chronic tension-type headache: a double-blind, placebo-controlled trial. Headache 2001; 41: 658–64.
6. Dodick DW. Botulinum neurotoxin for the treatment of migraine and other pri-mary headache disorders: from bench to bedside. Headache 2003; 43 (Suppl 1):S25–S33.
7. Zakrzewska JM, Cohen J, Brown J, et al. An open study of botulinum-A toxintreatment of trigeminal neuralgia. Neurology 2006; 66(9): 1458–9.
8. Voller B, Sycha T, Gustorff B, Kranz G, Auff E. An open study of botulinum-Atoxin treatment of trigeminal neuralgia. Neurology 2006; 66(9): 1458–9.
93
06-CMTN 8023.qxd 2/1/2007 7:39 PM Page 93

9. Brenner SR. An open study of botulinum-A toxin treatment of trigeminal neu-ralgia. Neurology 2006; 66(9): 1458–9.
10. Volcy M, Tepper SJ, Rapoport AM, Sheftell FD, Bigal ME. Botulinum toxin Afor the treatment of greater occipital neuralgia and trigeminal neuralgia: a casereport with pathophysiological considerations. Cephalalgia 2006; 26(3): 336–40.
11. Piovesan EJ, Teive HG, Kowacs PA, Della Coletta MV, Werneck LC, et al. Anopen study of botulinum-A toxin treatment of trigeminal neuralgia. Neurology2005; 65(8): 1306–8.
12. Turk U, Ilhan S, Alp R, Sur H. Botulinum toxin and intractable trigeminal neu-ralgia. Clin Neuropharmacol 2005; 28(4): 161–2.
13. Allam N, Brasil-Neto JP, Brown G, Tomaz C. Injections of botulinum toxin typea produce pain alleviation in intractable of trigeminal neuralgia. Clin J Pain2005; 21(2): 182–4.
14. Meyerson BA, Hakansson S. Alleviation of atypical trigeminal pain by stimula-tion of the Gasserian ganglion via an implanted electrode. Acta Neurochir Suppl(Wien) 1980; 30: 303–9.
15. Young RF. Electrical stimulation of the trigeminal nerve root for the treatmentof chronic facial pain. J Neurosurg 1995; 83: 72–8.
16. Holsheimer J. Electrical stimulation of the trigeminal tract in chronic,intractable facial neuralgia. Arch Physiol Biochem 2001; 109: 304–8.
17. Van ZJ, Brabant S, Van de KE, Vercruyssen A, Van Buyten JP. Pulsed radiofre-quency treatment of the Gasserian ganglion in patients with idiopathic trigemi-nal neuralgia. Pain 2003; 104: 449–52.
18. Horsley V TJCW. Remarks on the various surgical procedures devised for therelief or cure of trigeminal neuralgia (tic douloureux). Br Med J 1891; 1139-43,1191–3, 1249–52.
19. Cushing H. Landmark article April 28, 1900: A method of total extirpation ofthe Gasserian ganglion for trigeminal neuralgia. By a route through the temporalfossa and beneath the middle meningeal artery. By Harvey Cushing. JAMA1983; 250: 519–28.
20. Frazier CH. Subtotal resection of sensory root for relief of major trigeminal neu-ralgia. Arch Neurol Psychiatry 1925; 13: 378–84.
21. Spiller WG FC. The division of the sensory root of the trigeminus for relief oftic douloureux: an experimental, pathological, and clinical study with a prelimi-nary report of one surgically successful case. Phila Med J 1901; 8: 1039–49.
22. Dandy WE. An operation for the cure of tic douloureux: partial section of thesensory root at the pons. Arch Surg 1929; 18: 687–734.
23. Dandy WE. Concerning the cause of trigeminal neuralgia. Am J Surg 1934; 24:447–55.
24. Gardner WJ, MIklos MV. Response of trigeminal neuralgia to decompression ofsensory root; discussion of cause of trigeminal neuralgia. J Am Med Assoc1959; 170: 1773–6.
94
06-CMTN 8023.qxd 2/1/2007 7:39 PM Page 94

25. Jannetta PJ. Arterial compression of the trigeminal nerve at the pons in patientswith trigeminal neuralgia. J Neurosurg 1967; 26(Supp l): 62.
26. Hussein M, Wilson LA, Illingworth R. Patterns of sensory loss following frac-tional posterior fossa Vth nerve section for trigeminal neuralgia. J NeurolNeurosurg Psychiatry 1982; 45: 786–90.
27. Klun B. Microvascular decompression and partial sensory rhizotomy in thetreatment of trigeminal neuralgia: personal experience with 220 patients.Neurosurgery 1992; 30: 49–52.
28. van Loveren H, Tew JM Jr, Keller JT, Nurre MA. A 10-year experience inthe treatment of trigeminal neuralgia. Comparison of percutaneous stereotaxicrhizotomy and posterior fossa exploration. J Neurosurg 1982; 57: 757–64.
95
06-CMTN 8023.qxd 2/1/2007 7:39 PM Page 95

06-CMTN 8023.qxd 2/1/2007 7:39 PM Page 96

acupuncture 88aggravating factors 4alcohol injections 89alleviating factors 4alveolitis, parafunction-induced 12, 17amyloidosis, trigeminal 41anticipation, genetic 41anticonvulsants 65, 67–9
pretrigeminal neuralgia 20unresponsiveness of SUNCT 26see also specific agents
antiepileptic drugs see anticonvulsantsantiviral therapy 23arterial compression, trigeminal nerve
39, 74, 81–2associated features 5
baclofen 63, 66, 68mechanism of action 46
balloon compression of trigeminalnerve, percutaneous 76–8
bony compression, trigeminal nerveroot 40
botulinum toxin 88–9brainstem, non-demyelinating
lesions 40–1bulbospinal tract, descending,
destructive procedures 91
carbamazepine 63, 66, 67mechanism of action 46unresponsiveness of SUNCT 26
carcinoma, infiltrative lesions 40–1carotidynia 24central destructive procedures 91–2central nervous system (CNS)
role in trigeminal neuralgia 42–6, 43, 45
trigeminal pain modulation 37, 37–8trigeminal sensory pathway 35–6, 36
central neuropathic pain 21central sensitization 45Charcot-Marie-Tooth (CMT) disease
10, 40, 41–2chickenpox 22chronic paroxysmal hemicrania (CPH)
16, 26–8, 27cingulotomy 92classic (idiopathic) trigeminal
neuralgia 7diagnosis 8, 9surgical management see surgical
managementclassification of trigeminal
neuralgia 7clinical features, trigeminal
neuralgia 9clonazepam 64, 66, 69cluster headache 15, 25–6, 26cluster-tic syndrome 29compliance, patient 66concomitant features 5continuous pain 4cracked tooth syndrome 12, 17
97
Index
Page numbers in italics indicate figures or tables.
CMTN 8023-Index.qxd 2/1/2007 8:31 PM Page 97

definition, trigeminal neuralgia 7demyelination
disorders, primary 40pathogenic role 42, 44
dental pain 10–17, 12descending bulbospinal tract,
destructive procedures 91diagnosis
facial pain 1, 1–6trigeminal neuralgia 7–10
diagnostic criteria, trigeminalneuralgia 7, 8
diagnostic testing 5–6, 6differential diagnosis 10–33, 11divalproex sodium see
sodium valproatedrug therapy see medical managementduration, pain 4
electrical stimulation, trigeminalganglion 90–1
etiology of trigeminal neuralgia39, 39–42
evaluation, facial pain 1–6examination, physical 5extracranial pain 13, 18–19
facial paindiagnostic testing 5–6, 6evaluation 1–6history taking 2, 2–5non-trigeminal neuralgia 87physical examination 5
familial trigeminal neuralgia 10, 41–2family history 5felbamate 64, 66, 69frequency, pain 4frontal leukotomy 92
gabapentin 63, 66, 68inheritance of sensitivity 52mechanism of action 47–8
gamma knife radiosurgery (GKRS)74–5, 79–81
gasserian ganglion see trigeminalganglion
gate control theory 38, 38–9gene expression, changes in
47–9, 48genetics, trigeminal neuralgia
and 51–3giant cell arteritis 16, 28, 28glossopharyngeal neuralgia 14, 21
diagnostic criteria 22familial association 42
glycerol retrogasserian rhizotomy,percutaneous 75–6
headache disorders 24–8head and neck cancer, perineural
spread 40–1hereditary sensorimotor neuropathy
type I see Charcot-Marie-Toothdisease
herpes simplex virus type 1 (HSV-1),latent 52–3
herpes zoster 21–3history taking 2, 2–5
refractory trigeminal neuralgia 87–8hyperalgesia 21, 49hypoesthesia 9
idiopathic trigeminal neuralgia seeclassic trigeminal neuralgia
ignition hypothesis 44indomethacin 26inhibition, loss of 45, 45–6intensity, pain 4interleukin-1 48intermittent pain 4International Association for the Study
of Pain (IASP) 7, 23International Headache Society (IHS)
neuropathic disorders 22, 23
98
CMTN 8023-Index.qxd 2/1/2007 8:31 PM Page 98

99
neurovascular headaches 24, 26,27, 28
trigeminal neuralgia 7, 8intraoral trigeminal neuralgia 10
lamotrigine 63, 66, 68location, pain 3
magnetic resonance imaging(MRI) 40–1, 80
maxillary sinusitis 18–19medical history 5medical management 61–72, 62
failure 73mainstay 65medications available 66–9monotherapy vs polypharmacy 66patient compliance 66remission periods 65vs surgical 61–5
medullanon-demyelinating lesions 41rostral ventromedial (RVM) 49
medullary trigeminal tractotomy 91meningiomas 9mental nerve compression 24microglia 48–9microvascular decompression (MVD)
74, 81–2migraine 15, 24
diagnostic criteria 25facial 24history taking 3
migrainous neuralgia see clusterheadache
moxibustion 88multiple sclerosis (MS) 9–10, 40myofascial pain 19
nerve compression 15, 24neuroimmune interactions 48–9neuroma 23–4
neuromodulation 92neuropathic pain
differential diagnosis 13–15, 19–24history 3increased pain facilitation 49mechanisms 46–51phenotypic switch 47–9, 48structural reorganization 49–51, 50
neurovascular pain syndromes15–16, 24–8
nucleus caudalis dorsal root entryzone, radiofrequency lesioning 91
onset, pain 3opioid analgesics 49orofacial pain, differential
diagnosis 10–30oxcarbazepine 63, 66, 67–8
painincreased facilitation 49mechanisms see pathophysiology
of trigeminal neuralgiamodulation 37, 37–9
parafunction-induced alveolitis 12, 17paroxysmal hemicrania (PH)
chronic (CPH) 16, 26–8, 27diagnostic criteria 27trigeminal neuralgia and 29–30
paroxysmal hemicrania-ticsyndrome 29–30
pathophysiology of trigeminalneuralgia 42–53
neuropathic pain mechanism 46–51peripheral vs central mechanisms
42–6, 43, 45role of genetics 51–3
percutaneous procedures 74–9periaqueductal gray (PAG)
36, 37facilitation of nociception 49
periodontal pain 12, 17
CMTN 8023-Index.qxd 2/1/2007 8:31 PM Page 99

peripheral hypothesis of trigeminalneuralgia 42–6, 43
peripheral nerve blocks 89–90peripheral nerve stimulators 92peripheral neuritis 14, 23peripheral sensitization 48–9peripheral trigeminal
neurectomy 89–90peripheral trigeminal neuropathy 20–1pharmacogenetics 51–2pharmacological management see
medical managementphenobarbital 46phenotypic switch, trigeminal ganglia
neurons 47–9, 48phenytoin 46, 64, 69physical examination 5pimozide 64, 69polypharmacy 66pons, non-demyelinating lesions 41posterior fossa tumors 9, 40postherpetic neuralgia 14, 21–3, 23pregabalin 64, 66, 69
inheritance of sensitivity 52pretrigeminal neuralgia 10, 13, 19–20
diagnostic criteria 20provoking factors 9psychogenic disorders 28–9psychosocial history 5pulpal pain 11–17, 12
quality, pain 3–4
radiofrequency lesioning, nucleuscaudalis dorsal root entry zone 91
radiofrequency trigeminal(retrogasserian) rhizotomy 78–9
referral patterns 8refractory trigeminal neuralgia 87–95remission periods 65rostral ventromedial medulla
(RVM) 49
secondary trigeminal neuralgia seesymptomatic trigeminal neuralgia
semilunar ganglion see trigeminalganglion
sensory loss 9shingles (herpes zoster) 21–3short-lasting unilateral neuralgiform
headache attacks withconjunctival injection and tearingsee SUNCT
sinusitis 13, 18–19Sluder’s neuralgia see cluster headachesodium valproate 63, 66, 69sphenopalatine neuralgia see cluster
headachespinal cord, structural reorganization
49–51, 50spinal trigeminal nucleus 35–6, 36, 38
pathophysiologic role 44–6structural reorganization 49–51, 50substance P 47SUNCT 16, 26, 27, 30surgical management 73–85
indications 73, 74refractory trigeminal neuralgia
89–92techniques 74–82vs medical 61–5
symptomatic (secondary)trigeminal neuralgia 7
causes 9–10diagnosis 8, 10treatment 87
symptomshistory taking 2–5pathophysiologic correlates 42–4
temporal arteritis see giant cell arteritistemporomandibular disorders (TMD)
13, 19thalamotomy 92Tinel’s sign 24
100
CMTN 8023-Index.qxd 2/1/2007 8:31 PM Page 100

topiramate 63, 66, 68–9traumatization of trigeminal nerve,
surgical 76, 82treatment
past 5principles 61–5, 62refractory trigeminal neuralgia
87–95see also medical management;
surgical managementtrigeminal autonomic
cephalgias 29–30trigeminal ganglion 35
electrical stimulation 90–1infiltrative disorders 40–1neurons see trigeminal sensory
neuronspathophysiologic mechanisms 43–4
trigeminal nerve 35infiltrative disorders 40–1pain modulation 37, 37–9percutaneous balloon
compression 76–8sectioning 82, 91sensory pathway 35–9, 36surgical traumatization 76, 82
trigeminal nerve roots 35compression 39–40infiltrative disorders 40–1
percutaneous glycerol injection 75–6radiofrequency lesioning 78–9
trigeminal neurectomy,peripheral 89–90
trigeminal neuropathy 14, 20–1trigeminal sensory neurons
cross-excitation 44ectopic discharge/afterdischarge
43–4phenotypic switch 47–9, 48
trigger points, myofascial 19trigger zones (areas) 7, 9tumors 9, 40
unilateral facial pain 10
vagoglossopharyngeal neuralgia seeglossopharyngeal neuralgia
valproate see sodium valproatevaricella 22varicella-zoster virus 21–2vascular compression, trigeminal nerve
39, 40, 74, 81–2venous compression, trigeminal nerve
39, 74, 81–2
wide dynamic range (WDR) neurons 46
zonisamide 64, 66, 69
101
CMTN 8023-Index.qxd 2/1/2007 8:31 PM Page 101

CMTN 8023-Index.qxd 2/1/2007 8:31 PM Page 102