Embed Size (px)
Citation preview
8/9/2019 Triangular Stoma Suzuki
http://slidepdf.com/reader/full/triangular-stoma-suzuki 1/4
A novel permanent tracheostomy technique for prevention of stomalstenosis (triangular tracheostomy)
Masami Suzuki a, Atsunobu Tsunoda b,*, Satoshi Shirak ura b, Takuro Sumi b,Wataru Nishijima c, Seiji Kishimoto d
a Department of Head & Neck Surgery, Gunma Prefectural Cancer Center, Japanb Department of Otolaryngology, Tokyo Medical and Dental University, Japan
c Department of Head & Neck Surgery, Saitama Cancer Center, Japan
d Department of Head & Neck Surgery, Tokyo Medical and Dental University, Japan
Received 4 November 2009; accepted 18 November 2009
Available online 29 December 2009
Abstract
Objective: Stenosis of a permanent tracheostoma after total laryngectomy lowers postoperative quality of life (QOL), and its prevention is
clinically important.
Methods: From April 2003 to March 2009, the authors performed 87 permanent tracheostomies. For the purpose of prevention of
tracheostomal stenosis, we had applied new technique from October 2005.
Results: The incidence of the tracheostomal stenosis was retrospectively reviewed. Until September 2005, conventional permanent
tracheostomy was applied for 33 cases and tracheostomal stenosis developed in 6 cases (18.2%). On the other hand, stenosis did not
develop in any of the 54 cases in which the new technique was used. The triangular method was significantly superior to the conventional
method in preventing stenosis. Stomal recurrence did not develop in either technique.
Conclusion: The key point of the new technique is as follows: at the upper end of trachea, the posterior part of tracheal cartilage is preserved
and the anterior edge of the tracheostoma is made much lower. The shape of the tracheostoma approximates a triangle, and the area is greaterthan with other methods. From our experience, this technique is safe and effective for the prevention of tracheostomal stenosis.
# 2009 Elsevier Ireland Ltd. All rights reserved.
Keywords: Tracheostomal stenosis; Laryngectomy; Surgical technique
1. Introduction
Stenosis of the permanent tracheostoma after total
laryngectomy lowers postoperative QOL and requires
postoperative stenting and sometimes, reoperation [1–7].
Tracheostomal stenosis is relatively common, with a
reported incidence ranging from 4% to 55% [1–3]. Thefactors influencing this complication are as follows:
excessive scar formation after infection, gender, concomi-
tant neck dissection, stomal recurrence, and an inappropriate
operation. Wax et al. [3] classify permanent tracheostomy
into three techniques: circle, bevel, and plastic. Retro-
spective studies of tracheostomal stenosis in each technique
have reported incidences of 71%, 15%, and 8% [4] and 75%,
33%, and 0%, respectively [3].
As for the plastic technique, Hartwell and Dykes [8],
Trail et al. [9], and Myers and Gallia [10] added an incisionto the posterior wall of the trachea and inserted a skin flap to
widen the aperture of the tracheostoma. Wax et al. [3]
reported another plastic technique in which they incised the
anterior wall of trachea and also inserted a skin flap. Lam
et al. [7] recommended another technique; the skin incision
for the tracheostoma was made inferior to the main skin
incision for the laryngectomy. In these plastic techniques for
tracheostomy, stenosis is relatively uncommon (0–13%) [2–
4,7]. However, in cases in which previous tracheostomy with
www.elsevier.com/locate/anlAuris Nasus Larynx 37 (2010) 465–468
* Corresponding author at: Department of Otolaryngology and Head and
Neck Surgery, Tokyo Medical and Dental University, Bunkyo-ku, Yushima
1-5-45, Tokyo 113-8519, Japan. Tel.: +81 3 5803 5304;
fax: +81 3 3813 2134.
E-mail address: [email protected] (A. Tsunoda).
0385-8146/$ – see front matter # 2009 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.anl.2009.11.007
8/9/2019 Triangular Stoma Suzuki
http://slidepdf.com/reader/full/triangular-stoma-suzuki 2/4
longitudinal skin incision or presternal skin incision was
performed, these plastic techniques were difficult.
We have developed a new technique of permanent
tracheostomy that we call the triangular tracheostomy,
which prevents tracheal stenosis and is not influenced by a
previous tracheostomy or the type of skin incision. In this
study, we retrospectively investigate complications anddiscuss the advantages of our new technique.
2. Surgical technique
The laryngectomy from the trachea is usually made
between the cricoid cartilage and the first tracheal ring
(Fig. 1). If the margin of the tumor is not secured in this
separation, the incision is made much more inferiorly. The
thyroid gland is separated at the isthmus and the unaffected
hemilobe is left attached to the trachea as far as possible.
After pre- and paratracheal neck dissection is completed, the
permanent tracheostomy is then performed:
1. Subcutaneous fat around the tracheostomy is widely
removed.
2. The upper end of trachea is elevated upward with forceps.
The skin over the suprasternal notch is then elevated over
and placed in contact with the anterior surface of the
trachea. The lower margin of the tracheostomy is marked
on the tracheal wall (Fig. 2).
3. Preserving the posterior part of the tracheal cartilage, the
anterior part of the trachea is removed. The unaffected
side of the thyroid gland is left attached to the trachea
(Figs. 1 and 2).4. An inverted suture between the trachea and skin is made
at the lateral and inferior border (Fig. 3).
5. Skin is incised at the level of the inferior border of cricoid
cartilage and sutured with the upper border of the
membranous portion of trachea and posterior half of
the tracheal cartilage. This widens the upper border of the
tracheostomy and the aperture of the triangle shaped
tracheostomy (Fig. 3). The anterior part of the trachea is
incised obliquely and the final shape of the stoma
approximates a rounded triangle (Figs. 1 and 4)
3. Patients and methods
From April 2003 to March 2009, 87 patients who
underwent total laryngectomy at the Gunma Prefectural
Cancer Center and the Saitama Prefectural Cancer Center
were enrolled in this study. The first author performed all the
surgery as a surgeon or trainer. Until September 2005,
conventional permanent tracheostomy with bevel technique
(bevel) was applied in 33 cases (male:female = 29:4, mean
age 63.5 years, range 44–80 years; laryngeal cancer, n = 22;
hypopharyngeal cancer, n = 9; mesopharyngeal cancer,
n = 1; and tracheal cancer, n = 1). After this period, the
above-mentioned new technique (triangular) was applied in
54 cases (male:female = 48:6, mean age 67.1 years, range
49–84 years; laryngeal cancer, n = 25; hypopharyngeal
cancer, n = 25; and mesopharyngeal cancer, n = 4). Stomal
stenosis was defined as follows: (1) requirement for 24-h
stenting, or (2) requirement for surgery to widen the stenosis
within 6 months after the initial permanent tracheostomy.
The following factors were investigated for their influence
on the occurrence of stenosis: stomal recurrence, gender,
concurrent neck dissection, and surgical site infection.
M. Suzuki et al./ Auris Nasus Larynx 37 (2010) 465–468466
Fig. 1. Schematic drawing of the 3 techniques of permanent tracheostomy.
T, thyroid cartilage; C, cricoid cartilage; and I–VI, tracheal rings. Incision
lines through the trachea are red (circle), blue (bevel), and green (triangu-
lar). The point of the triangular technique is that the posterior part of the
tracheal cartilage is preserved. (For interpretation of the references to color
in this figure legend, the reader is referred to the web version of the article.)
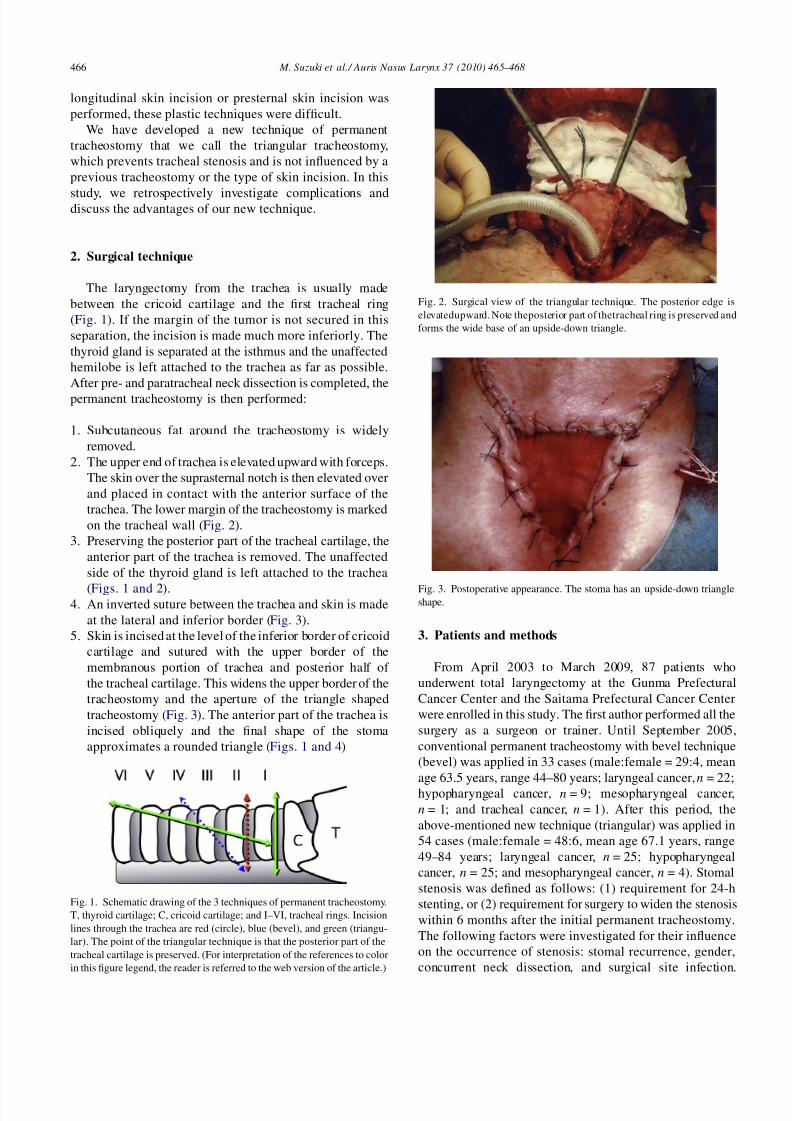
Fig. 2. Surgical view of the triangular technique. The posterior edge is
elevatedupward. Note theposterior part of thetracheal ring is preserved and
forms the wide base of an upside-down triangle.
Fig. 3. Postoperative appearance. The stoma has an upside-down triangleshape.
8/9/2019 Triangular Stoma Suzuki
http://slidepdf.com/reader/full/triangular-stoma-suzuki 3/4
Fisher’s exact probability test was used for statistical
analysis and p < 0.05 was defined as statistically significant.
4. Results
The results are summarized in the Tables 1 and 2. Stomal
recurrence was not observed. The bevel technique was
performed in 33 cases. Six of these showed stomal stenosis
(18.2%) and 2 of these required surgery. Surgical site
infection was seen in seven cases (21%) and concurrent neck
dissection was performed in 20 cases (61.6%), and these
relationships were not statistically significant ( p = 0.09 and
p = 0.21, respectively). One of the 4 female patients
developed stomal stenosis ( p = 0.57) (Table 1).
The triangular technique was applied in 54 patients, 6 of
whom were females 6 (11.1%) and47 (87.0%) hadconcurrent
neck dissection. Surgical site infection after the pharyngeal
fistula, necrosisof thefree-flap, or skin necrosis occurred in 10cases (18.5%). Although these factors are reported to increase
the risk of postoperative stomal stenosis, tracheostomal
stenosis was not encountered in any patients in whom the
triangular technique was used (Table 2). Hence in avoiding
tracheostomal stenosis, the triangular method is significantly
superior to the bevel method. No complaints concerning this
wide stoma were noted from the patients.
5. Discussion
Various factors relating to stomal stenosis are reported,
including stomal recurrence, surgical site infection, and skill
of the surgeon [1–11]. Since women have smaller tracheas
than men, gender is also reported as a factor influencing
stomal stenosis. In the present study, 6 patients showed
stomal stenosis; however, there were no statistically
significant relationships between stomal stenosis and the
above-mentioned factors. Whether or not these factors are
involved, for prevention of postoperative stomal stenosis, the
surgical technique must not only maintain a minimum width
of stenosis but also prevent stomal recurrence.
In our new technique, the posterior part of the lateral wall
of the tracheal cartilage is preserved, so the stoma is not
M. Suzuki et al. / Auris Nasus Larynx 37 (2010) 465–468 467
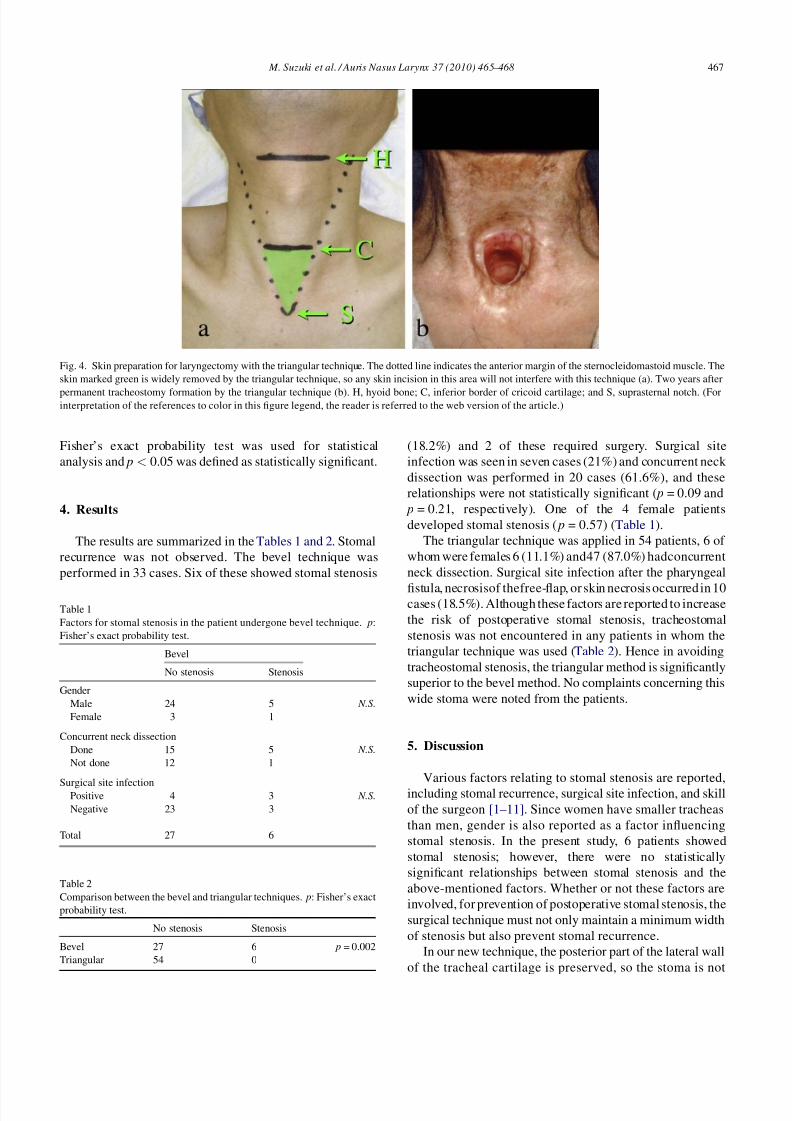
Fig. 4. Skin preparation for laryngectomy with the triangular technique. The dotted line indicates the anterior margin of the sternocleidomastoid muscle. The
skin marked green is widely removed by the triangular technique, so any skin incision in this area will not interfere with this technique (a). Two years after
permanent tracheostomy formation by the triangular technique (b). H, hyoid bone; C, inferior border of cricoid cartilage; and S, suprasternal notch. (Forinterpretation of the references to color in this figure legend, the reader is referred to the web version of the article.)
Table 1
Factors for stomal stenosis in the patient undergone bevel technique. p:
Fisher’s exact probability test.
Bevel
No stenosis Stenosis
Gender
Male 24 5 N.S.
Female 3 1
Concurrent neck dissection
Done 15 5 N.S.
Not done 12 1
Surgical site infectionPositive 4 3 N.S.
Negative 23 3
Total 27 6
Table 2
Comparison between the bevel and triangular techniques. p: Fisher’s exact
probability test.
No stenosis Stenosis
Bevel 27 6 p = 0.002
Triangular 54 0

8/9/2019 Triangular Stoma Suzuki
http://slidepdf.com/reader/full/triangular-stoma-suzuki 4/4
round or oval but instead an upside-down triangle (Fig. 3).
Here, we assume the shape of the trachea to be a
combination of semicircle and rectangle: 3 cm in width
and 3 cm in height. The cross-sectional area approximates
8 cm2 which approximates the area of a tracheostoma
formed by the circular technique (Fig. 5A). In the bevel
technique, the length of stoma increases by ffiffiffi
2p
times and the
area increases to 11. 4 cm2 (Fig. 5B). If the base is widened
to 5 cm and an anterior cut made at 6 cm below the upper
edge, the area of the triangle becomes 15 cm2 (Fig. 5C). In
the triangular technique, the anterior part of the trachea is cut
obliquely and the final shape of the stoma approximates a
rounded triangle. Even if the longitudinal length is restricted
to 5 cm, the area of the stoma is 19.6 cm2; 2.5 times as wide
as the original area (Fig. 5D). Although patients undergoing
this technique had various postoperative complications, no
stomal stenosis occurred. The likely reasons for this are the
wider stoma.
A wide tracheostoma is reported to be associated with
problems with postoperative phonation [12]. For patients
who undergo tracheo-esophageal (TE) shunt plasty, anextremely wide tracheostoma may make it difficult for the
patient to close the stoma with a finger. Since we have
never experienced TE shunt, we could not make a specific
comment on this kind of problem. On the other hand, the
TE shunt itself is reported to increase the risk of stomal
stenosis [2]. The triangular technique may therefore
prevent stomal stenosis even when patients undergo TE
shunt plasty.
6. Conclusion
The key points of the triangular technique are preserva-
tion of the posterior part of the tracheal cartilage at the upper
end and a lowered anterior edge of the tracheostoma. The
shape of the stoma approximates a triangle and is wide.
Neither stomal recurrence nor patient discomfort was notedwith this technique. Tracheostomal stenosis was not
encountered despite complications such as surgical site
infection. From our experience, this technique is straightfor-
ward, safe, and particularly effective for prevention of
tracheostomal stenosis.
References
[1] Iida S, Hosoi H, KimuraH, MurataK, Ohta F. A clinical observation of
tracheostomal stenosis. J Jpn Bronchoesophagol Soc 1990;41:47–56
(in Japanese).
[2] Kuo M, Ho CM, Wei WI, Lam KH. Tracheostomal stenosis after totallaryngectomy: an analysis of predisposing clinical factors. Laryngo-
scope 1994;104:59–63.
[3] Wax MK, Touma BJ, Ramadan HH. Tracheostomal stenosis after
laryngectomy: incidence and predisposing factors. Otolaryngol Head
Neck Surg 1995;133:242–7.
[4] Griffith GR, Luce EA. Tracheal stomal stenosis after laryngectomy.
Plast Reconstr Surg 1982;70:684–98.
[5] Loewy WR, Laker HI. Tracheal stoma problems. Arch Otolaryngol
1968;87:477–83.
[6] Balle VH, Bretlau P. Tracheal stoma following total laryngectomy. J
Laryngol Otol 1985;99:577–80.
[7] Lam KH, Wei WI, Wong J, Ong GB. Tracheostome construction
during laryngectomy—a method to prevent stenosis. Laryngoscope
1983;93:212–5.
[8] Hartwell SW, Dykes ER. Construction and care of the end tracheos-tomy. Am J Surg 1967;113:498–500.
[9] Trail M, Chambers R, Leonard J. Z-Plasty of trachealstoma at
laryngectomy. Arch Otolaryngol 1968;88:110–2.
[10] Myers EN, Gallia LJ. Tracheostomal stenosis following total laryn-
gectomy. Ann Otol Rhinol Laryngol 1982;91:450–3.
[11] Vlantis AC, Marres HAM. A surgical technique to prevent tracheos-
tomal stenosis after laryngectomy. Laryngoscope 1998;108:134–7.
[12] Verschuur HP, Gregor RT, HilgersFJM, Balm AJM.The tracheostomain
relation to prosthetic voice rehabilitation. Laryngoscope 1996;106:
111–5.
M. Suzuki et al./ Auris Nasus Larynx 37 (2010) 465–468468
Fig. 5. Difference of the cross-sectional area among tracheostomies: (A)
8.0 cm2 by circular technique; (B) 11.4 cm2 by bevel technique; (C) 15 cm2
by simple triangle; and (D) 19.6 cm2 by the triangular technique. (A)
3 Â 1.5 + 1.125p = 8.0; (B) ffiffiffi
2p
 A ¼ 11:4; (C) (5  6)/2 = 15; and (D)
(5/2)Â 5 Â p /2 = 19.6.