Embed Size (px)
Citation preview

Trials of Antithrombotic Therapy Trials of Antithrombotic Therapy in AF – Where Do We Stand in AF – Where Do We Stand
Now?Now?
Daniel E. Singer, M.D.
Massachusetts General Hospital
Harvard Medical School

Speaker Disclosure Information
DISCLOSURE INFORMATION:The following relationships exist related to this presentation:
Daniel E. Singer, M.D. has served as a consultant to AstraZeneca, Bayer, GSK, Boehringer Ingelheim, ev3, Medtronic, Johnson and Johnson.

Trials of Antithrombotic Therapy in Trials of Antithrombotic Therapy in AFAF
Chronology:Chronology:1950s:1950s: LA thrombus in MS plus AFLA thrombus in MS plus AF1970s+:1970s+: NRAF raises risk of embolic NRAF raises risk of embolic
strokestroke1980s-1990s:1980s-1990s: Superiority trials of VKA and Superiority trials of VKA and
ASAASALate 1990sLate 1990s:: Non-inferiority trials of novel Non-inferiority trials of novel
agents vs VKAagents vs VKA

Stroke Prevention in AFStroke Prevention in AF
Core Efficacy/Superiority TrialsCore Efficacy/Superiority Trials

Stroke Prevention in AF: Core TrialsStroke Prevention in AF: Core Trials
AFASAKAFASAKBAATAFBAATAFCAFACAFA Primary PreventionPrimary PreventionSPAF I/IISPAF I/IISPINAFSPINAF
EAFTEAFT Secondary PreventionSecondary Prevention
SPAF IIISPAF III Very Low INR + ASA vs. Very Low INR + ASA vs. INR 2-3 in high-risk ptsINR 2-3 in high-risk pts

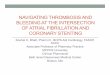
RCTs of VKA v. Control to Prevent Stroke in AF*RCTs of VKA v. Control to Prevent Stroke in AF*
5.5
3.0
7.4
5.24.3
12.3
1.60.4
2.3 2.5
0.9
3.9
0
2
4
6
8
10
12
14
AFASAK BAATAF SPAF-I CAFA SPINAF EAFT
An
nu
al
Str
ok
e R
ate
(%
)
ControlWarfarin
-71%* -86%* -69%* -52% -79%*
-66%*
*Go et al. Progr Cardiovasc Dis 2005
*P<0.05

Efficacy of Anticoagulation for AFEfficacy of Anticoagulation for AF
Trial Target Ranges: INR ~1.8-4.2Trial Target Ranges: INR ~1.8-4.2
RelativeRelative AbsoluteAbsolute
Risk ReductionRisk Reduction Risk ReductionRisk Reduction
Pooled 1° RCTs Pooled 1° RCTs 68%68% (50-79%) (50-79%) 3.1% 3.1% per yearper year
EAFTEAFT 66%66% (43-80%) (43-80%) 8.4% 8.4% per yearper year

Warfarin for AF: Secondary OutcomesWarfarin for AF: Secondary Outcomes
Primary prevention pooled analysis:Primary prevention pooled analysis:
1.1. Severe/fatal strokeSevere/fatal stroke RRR=68%RRR=68% (39-83%) (39-83%)
2.2. Death, all causeDeath, all cause RRR=33%RRR=33% (9-51%) (9-51%)

Safety of Anticoagulation for AFSafety of Anticoagulation for AF
Pooled 1° RCTsPooled 1° RCTs 0.3%0.3% per yr per yr 0.1%0.1% per yr per yr
Intracranial Hemorrhage:Intracranial Hemorrhage:
AnticoagulationAnticoagulation ControlControl
Absolute Rates ofAbsolute Rates of

Efficacy of Aspirin for AFEfficacy of Aspirin for AF
Pooled 3 trials versus placebo*:Pooled 3 trials versus placebo*:
AFASAKAFASAK 75 mg daily75 mg dailySPAF ISPAF I 325 mg daily325 mg dailyEAFTEAFT 300 mg daily300 mg daily
Relative Risk Reduction: Relative Risk Reduction: 21% (0-38%)21% (0-38%)No signif impact on severe/fatal strokeNo signif impact on severe/fatal stroke
*Arch Intern Med 1997; 157:1237-1240*Arch Intern Med 1997; 157:1237-1240

Warfarin vs. AspirinWarfarin vs. Aspirin
Pooled Analysis*:Pooled Analysis*: All stroke All stroke RRR: 45%RRR: 45%
All CVD All CVD RRR: 29%RRR: 29%
MIMI RRR: 37%RRR: 37%
**JAMA 2002;288:2441-2448 (AFASAK I &II, EAFT, PATAF, SPAF I-III)JAMA 2002;288:2441-2448 (AFASAK I &II, EAFT, PATAF, SPAF I-III)

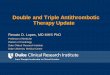
The Optimal INRThe Optimal INR

SPAF III: INR 1.2-1.5 plus ASA SPAF III: INR 1.2-1.5 plus ASA versus INR 2.0-3.0versus INR 2.0-3.0
TE rate: 7.9% vs 1.9% per yrTE rate: 7.9% vs 1.9% per yr
RRR favoring warfarin: 74% (50-87%)RRR favoring warfarin: 74% (50-87%)
No reduction in risk of ICHNo reduction in risk of ICH

Hylek, et al. N Engl J Med 1996;335:540-546.Hylek, et al. N Engl J Med 1996;335:540-546.
INRINR Odds RatioOdds Ratio2.02.0 1.01.01.71.7 2.02.01.51.5 3.33.31.31.3 6.06.0
1.0 1.5 3.0 4.0 7.0
135
10
15
2.0
Od
ds
Ra
tio
Od
ds
Ra
tio
INRINR
Lowest Effective Anticoagulation Lowest Effective Anticoagulation Intensity for Warfarin TherapyIntensity for Warfarin Therapy

Relative Odds of ICH by INR IntervalsRelative Odds of ICH by INR Intervals
Fang et al. Ann Intern Med 2004;141:745-52

Stroke Prevention in AFStroke Prevention in AF
More Recent Efficacy/Superiority More Recent Efficacy/Superiority TrialsTrials

Spanish NASPEAF TrialSpanish NASPEAF Trial
Triflusal vs triflusal + lower INR vs INR 2-3Triflusal vs triflusal + lower INR vs INR 2-3 Overall n=1209Overall n=1209 Complex design; includes mitral stenosis ptsComplex design; includes mitral stenosis pts 11oo outcome: vascular death + nonfatal stroke or outcome: vascular death + nonfatal stroke or
systemic embolismsystemic embolism Results at 2.76 yrs:Results at 2.76 yrs:
e.g., hi risk: median INR 2.08 vs INR 2-3e.g., hi risk: median INR 2.08 vs INR 2-3
Trifl + Warf:Trifl + Warf: 2.44%/yr2.44%/yr RRR=49% (!!)RRR=49% (!!)INR 2-3:INR 2-3: 4.76%/yr 4.76%/yr
Provocative, though many non-stroke outcome Provocative, though many non-stroke outcome eventsevents

Recent Superiority Trials for Recent Superiority Trials for Stroke Prevention in AFStroke Prevention in AF
1. Chinese RCT: INR 2-3 v ASA1. Chinese RCT: INR 2-3 v ASA
2. Japanese JAST RCT: ASA v PLBO2. Japanese JAST RCT: ASA v PLBO
3. Swedish RCT: warf 1.25 mg plus 75 3. Swedish RCT: warf 1.25 mg plus 75 mg ASA v Controlmg ASA v Control

Antithrombotic Trials in Antithrombotic Trials in AF: Core FindingsAF: Core Findings
Anticoag. at INR 2.0-3.0 Anticoag. at INR 2.0-3.0 veryvery effective effective- - Generally safeGenerally safe- Moderately burdensome- Moderately burdensome
Aspirin is Aspirin is muchmuch less effective less effective

Stroke Prevention in AFStroke Prevention in AF
Novel Agents/Non-Inferiority Novel Agents/Non-Inferiority TrialsTrials

XimelagatranXimelagatranOral Direct Thrombin InhibitorOral Direct Thrombin Inhibitor
• Prompt onset and offset of Prompt onset and offset of anticoagulationanticoagulation
• Predictable pharmacokinetics: bid Predictable pharmacokinetics: bid dosedose• Low potential for food and drug Low potential for food and drug
interactionsinteractions • ~No dose adjustment~No dose adjustment• No coagulation monitoringNo coagulation monitoring
Sarich TC, et al. Sarich TC, et al. J Am Coll CardiolJ Am Coll Cardiol 2003;41:557. 2003;41:557.Eriksson H, et al. Eriksson H, et al. Drug Metab DispDrug Metab Disp 2003;31:294. 2003;31:294.

SPORTIF III and V: SPORTIF III and V: Trial DesignTrial Design
• Ximelagatran, 36 mg bid vs. Warfarin, INR 2-3Ximelagatran, 36 mg bid vs. Warfarin, INR 2-3
• Outcome: all stroke and systemic embolismOutcome: all stroke and systemic embolism
• Non-inferiority (Risk Difference Non-inferiority (Risk Difference <<2.0%)2.0%)
• Patients with AF and Patients with AF and 1 additional stroke risk factor1 additional stroke risk factor
• Minimum exposureMinimum exposure– 12 months/patient12 months/patient– 4000 patient-yrs4000 patient-yrs80 events80 events

SPORTIF III & V: Quality of SPORTIF III & V: Quality of Warfarin RxWarfarin Rx
SPORTIF IIISPORTIF III SPORTIF VSPORTIF V
INR 2.0-3.0INR 2.0-3.0 66% 66% 68% 68%
INR 1.8-3.2INR 1.8-3.2 81% 81% 83% 83%

Pooled SPORTIF III and V: Stroke and Systemic Pooled SPORTIF III and V: Stroke and Systemic
EmbolismEmbolism
Cerebrovasc Dis 2006;21:279-293

SPORTIF V: SPORTIF V: BleedingBleeding
XimelagatranXimelagatran WarfarinWarfarin
Major extracerebral Major extracerebral Bleeding, nsBleeding, ns
Fatal, nsFatal, ns
63 cases63 cases 84 cases 84 cases(2.4% per year) (2.4% per year) (3.1% per year) (3.1% per year)
2 cases2 cases 1 case 1 case

SPORTIF V: SPORTIF V: Liver ToxicityLiver Toxicity
ALT ALT >> 3 x ULN 3 x ULN
ALT ALT >> 3 x ULN + 3 x ULN + Bili > 2 x ULN Bili > 2 x ULN
(“Hy’s Law”)(“Hy’s Law”)
Liver FatalityLiver Fatality
All Cause MortalityAll Cause Mortality
117 (6.0%) 15 (0.8%)
9 (0.46%) 1 (0.05%)
1 case (?3) 0 cases
116 (6.0%) 123 (6.3%)
XimelagatranXimelagatran WarfarinWarfarin

FDA CardioRenal, 9 Sept, 2005 FDA CardioRenal, 9 Sept, 2005 Ximelagatran Ximelagatran Not ApprovedNot Approved
AZeneca, Jan 2006, withdraws AZeneca, Jan 2006, withdraws XimelagatranXimelagatran

ACTIVE-W TrialACTIVE-W Trial
Non-inferiority; open; clopidogrel 75mg + Non-inferiority; open; clopidogrel 75mg + 150-200mg ASA vs. adjusted dose OAC; 150-200mg ASA vs. adjusted dose OAC; n=6706 n=6706
Patients with AF and at least a moderate risk Patients with AF and at least a moderate risk for strokefor stroke
Primary outcome: combined stroke, Primary outcome: combined stroke, peripheral embolism, myocardial infarction, peripheral embolism, myocardial infarction, vascular deathvascular death

ACTIVE-W ResultsACTIVE-W Results
Annual Event Rate, %Annual Event Rate, %
ASA+Clopido.ASA+Clopido. OACOAC RRRRRR pp
Primary Primary OutcomeOutcome 5.65.6 3.93.9 30%30% <0.01<0.01
Isch. StrokeIsch. Stroke 2.152.15 1.0(!)1.0(!) 53%53% <0.01<0.01
MIMI 0.860.86 0.550.55 36%36% 0.090.09
Major bleedMajor bleed 2.42.4 2.22.2 8.6%8.6% 0.50.5
Stopped early because OAC clearly superiorStopped early because OAC clearly superior
OAC less dominant among pts newly starting OACOAC less dominant among pts newly starting OAC

RCTs of Other Novel RCTs of Other Novel AntithromboticsAntithrombotics
AMADEUS: idraparinux vs warfarin (INR 2-3) in AMADEUS: idraparinux vs warfarin (INR 2-3) in “hi-risk” AF: stopped early in favor of warfarin“hi-risk” AF: stopped early in favor of warfarin
Multiple other agents near or in phase 3 trialsMultiple other agents near or in phase 3 trials

PROGRESS Trial: Anti-hypertensives as PROGRESS Trial: Anti-hypertensives as AntithromboticsAntithrombotics
Perindopril+/-indapamide vs placebo in all patients Perindopril+/-indapamide vs placebo in all patients with a prior stroke, all types, with/without hx of with a prior stroke, all types, with/without hx of HTN?HTN?
Outcome: all strokeOutcome: all stroke N=6105; #AF=476, 51% on anticoag; f/u=3.9 yrsN=6105; #AF=476, 51% on anticoag; f/u=3.9 yrs RRR=38% (-13 to 61%)RRR=38% (-13 to 61%)

Stroke Prevention in AF: The FutureStroke Prevention in AF: The Future
1.1. More new antithrombotics: More new antithrombotics: • oral direct thrombin and Xa inhibitors, oral direct thrombin and Xa inhibitors,
othersothers• Irbesartan (ACTIVE-I)Irbesartan (ACTIVE-I)
2. “Rx” of LAA: surgery, catheter approach2. “Rx” of LAA: surgery, catheter approach
3. True cure of AF:3. True cure of AF:• initiator: ablation/isolation of PVinitiator: ablation/isolation of PV• substrate:substrate: “maze” procedure“maze” procedure
4. Preventing AF4. Preventing AF

Trials of Antithrombotic Therapy Trials of Antithrombotic Therapy in AFin AF
Lessons learned:Lessons learned: Warfarin, INR 2-3, is extremely effective and Warfarin, INR 2-3, is extremely effective and
can be safecan be safe
ASA has little efficacy in AFASA has little efficacy in AF
Warfarin is tough to beat or even tie in RCTsWarfarin is tough to beat or even tie in RCTs

Trials of Antithrombotic Therapy Trials of Antithrombotic Therapy in AFin AF
Concerns:Concerns: Warfarin’s performance in the real worldWarfarin’s performance in the real world
1. Patient selection in RCTs1. Patient selection in RCTs2. INR control in RCTs2. INR control in RCTs3. Initiation phase3. Initiation phase
Secular decrease in absolute stroke risk for Secular decrease in absolute stroke risk for AF patientsAF patients
Bleeds: adding ASA, or ASA + clopidogrel Bleeds: adding ASA, or ASA + clopidogrel to warfarinto warfarin

Trials of Antithrombotic Therapy Trials of Antithrombotic Therapy in AF – Where Do We Stand in AF – Where Do We Stand
Now?Now?
Warfarin, INR 2-3, remains the Warfarin, INR 2-3, remains the treatment of choice for patients with treatment of choice for patients with AF and risk factors for stroke, but the AF and risk factors for stroke, but the field is “alive” with novel research, field is “alive” with novel research, and we can anticipate additional and we can anticipate additional management and treatment options management and treatment options soon.soon.

ENDEND