Embed Size (px)
Citation preview

Treponemal Disease, Tuberculosis andSubsistence-settlement Pattern in the LateWoodland Period West-central IllinoisG. M. MOSHER,* M. O. SMITH, J. L. ALBRECHT AND V. P. SALAKADepartment of Anthropology, Illinois State University, Normal, IL, USA
ABSTRACT In later pre-Columbian prehistory (post AD 1000), the adaptation and intensification of maize agriculture andits correlate of aggregate village settlement (i.e. Mississippianization) is temporally and geographicallyvariable. In the Midwest, consequential to the florescence of the major ceremonial centre of Cahokia(AD 1050–1300), the Mississippi River Valley alluvial plain in Illinois, known as the American Bottom, becamea core area of this subsistence-settlement change. Much archaeological research has traced aspects of thistransition in the Lower and Middle Illinois River Valley, but little is known outside of these areas. A skeletalsample from the remote hinterland area of the Upper Mississippi River in west-central Illinois was examinedfor arguable paleopathological correlates of sedentism (treponemal disease) and Mississippianization(tuberculosis). The Schroeder Mounds (AD 900–1100) adult skeletal sample (N=53) exhibited a highfrequency of treponemal disease (13.2–15.1%). This result is consistent with paleopathological literature linkinga 9+% pre-Columbian North American prevalence with sedentism, challenging archaeologically basedinferences that the hinterland was occupied by mobile forager-horticulturalists. A hallmark of Mississippianizationis the presence of diagnostic cases of tuberculosis.No caseswere observed in the Schroeder sample, suggestinga pre-Mississippian subsistence-settlement pattern. Copyright © 2013 John Wiley & Sons, Ltd.
Key words: agriculture; forager; Illinois; Late Woodland; Mississippian; sedentism; treponemal; tuberculosis
The late LateWoodland period in Illinois (AD 650–1000)was a time of major subsistence, settlement, demographicand sociopolitical change. After AD 900, it involved theintensification of maize agriculture, settlement nucle-ation and political centralization characteristic of thesubsequent Mississippian period (AD 1050–1350)(Pauketat, 1998; Emerson and Lewis, 2000; McElrathet al., 2000). This transition in Illinois was apparentlytemporally and regionally variable (Esarey, 2000;Nansel and Green, 2000; Stoltman, 2000; Stoltmanand Christiansen, 2000; Theler and Boszhardt, 2000).It was earliest in Southern Illinois with the rapid riseof Cahokia (AD 900–1050), the eventual largestMississippian period settlement north of Mexico(Pauketat, 1998; Emerson and Lewis, 2000). Thetransition dynamics in Illinois varied considerably dueto evident cultural heterogeneity, ecological context(e.g. river bottom versus upland), and differentialCahokian influence (e.g. Benn and Green, 2000;Emerson and Lewis, 2000; Emerson and Titelbaum,
2000; O’Gorman and Hassen, 2000; Simon, 2000;Stoltman and Christiansen, 2000; Styles, 2000). Thisis particularly true of Woodland settlements in theupper Mississippi River valley of west-central Illinois,which are geographically remote relative to theMississippian culture core (Emerson and Lewis, 2000;Trader, 2011). Unfortunately, material culture is generallypoorly represented in this area and subsistence-settlementreconstruction vacillates between forager-horticulturalistsand sedentary agriculturalists (e.g. Benn and Lee, 2005;Hedman and Emerson, 2008; Trader, 2011).Nonvenereal treponemal disease (yaws and treponarid)
is a chronic disease transmitted by spirochetes of thegenus Treponema via breaks in the skin. It is a diseasecommonly contracted in childhood, is endemic whereit is found and is epidemiologically associated withcompromised hygiene (Hackett, 1976; Aufderheide andRodriguez-Martin, 1998; Ortner, 2003). The paleopatho-logical presence of the tertiary stage (i.e. bone dissemi-nated) of chronic treponemal disease has a considerableantiquity in North America in general (i.e. ArchaicPeriod, ca 6000 BC) (e.g. Hutchinson, 1993; Cook andPowell, 2005; Powell et al., 2005a; Powell et al., 2005b;Hutchinson and Richman, 2006; Smith, 2006) and Illinois
* Correspondence to: Germaine M. Mosher, Department of Anthropology,Illinois State University, Normal, IL 61761, USA.e-mail: [email protected]
Copyright © 2013 John Wiley & Sons, Ltd. Received 23 March 2013Revised 3 July 2013
Accepted 20 August 2013
International Journal of OsteoarchaeologyInt. J. Osteoarchaeol. 25: 776–787 (2015)Published online 20 September 2013 in Wiley Online Library(wileyonlinelibrary.com) DOI: 10.1002/oa.2344

in particular (ca 1000 BC) (Cook, 2005; Powell et al.,2005a). Generally speaking, the prevalence of pre-Columbian tertiary treponemal disease ‘rises sharply frompresedentary Archaic groups (5.8% overall) to the rise ofvillage life ca 1000 BC (9.0%) (Cook and Powell,2005:466). Indeed, despite archaeologically demon-strated changes in subsistence (i.e. agricultural intensifica-tion) and a dramatic increase in available osteologicalsamples that post-date AD 1000, Cook and Powell record(2005:466) that the generic prevalence of treponemaldisease in North America exhibits only a modest increase(10.8%). Although preservation, interobserver error,sampling bias and ecological variables may temper theveracity of this temporal comparison (Cook and Powell,2005), various other regional meta-analyses have affirmedthat sedentism is a valid paleoepidemiological variable(e.g. Cassidy, 1984; Powell, 2000; Hutchinson et al.,2005:107; Powell et al., 2005b:157; Hutchinson andRichman, 2006; Smith, 2006; Smith et al., 2010).Tuberculosis (TB), a paleoepidemiologically com-
plex pulmonary disease that disseminates to bone, isassociated with aggregate living and compromisedcommunity health (Roberts and Buikstra, 2003).Despite a great antiquity (Mackowiak et al., 2005), itis paleopathologically absent in the Americas beforeAD 300 (Wilbur et al., 2008). In the pre-ColumbianMidwest, the signature anterior vertebral kyphosis(i.e. vertebral body collapse) of the disease appearscircum AD 900, paralleling maize-intensification
(Stone et al., 2009). This implies that the diagnosticmacroscopic bone changes of TB is absent insubsistence-settlement patterns that do not mirrorMississippianization.The remote hinterland Late Woodland (AD 900–1100)
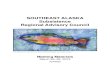
Schroeder Mounds site (11HE177) is a burialcontext in west-central Illinois (Figure 1). It has hadlittle bioarchaeological assessment (Hitzemann,1997; Langford, 1999), has little available comparativepaleopathological information (Hedman and Emerson,2008) and has no subsistence-settlement context(Riggle, 1981; Kolb, 1982; Benn and Lee, 2005). Anexamination of periosteal reaction on the bones ofthe adults for the diagnostic changes of treponemaldisease and TB may provide credible support forone or other hypothesis about the settlement patternor Mississippianization of the people interred inSchroeder Mounds.
Materials and methods
The multiple-mound interment complex of SchroederMounds (Henderson County, Illinois) was a salvagearchaeological excavation undertaken between 1975and 1978. On the basis of ceramic attributes, it wasoriginally assigned to the Late Woodland periodMaples Mills phase (AD 800–1100), the core area ofwhich is the CIRV (Riggle, 1981; Kolb, 1982)
Figure 1. Map of the Schroeder Mounds site (11He177) and location relative to the central Illinois River Valley (CIRV), lower Illinois River Valley(LIRV), American Bottom and Sly Bottom.
777Periosteal Reaction in Prehistoric Late Woodland Illinois
Copyright © 2013 John Wiley & Sons, Ltd. Int. J. Osteoarchaeol. 25: 776–787 (2015)

(Figure 1). But, Schroeder Mounds may more likely beassigned to a regional cultural analogue (Esarey, 2000)such as the Louisa phase (AD 800–1200) that straddlesthe Mississippi River Valley inclusive of HendersonCounty, Illinois (Benn and Lee, 2005).The Schroeder Mounds’ adult skeletal sample con-
sists of 75 adult individuals (third molar in occlusion),53 of which were complete enough (50+ % present)for tabular use. The exception to minimum complete-ness was the inclusion of the second individual in acomingled burial because duplicated bone elementsexhibited periosteal reaction. None of the other frag-mentary adult remains exhibited reactive bone change.The adults were aged and sexed using standard
nonmetric criteria (White and Folkens, 2005; Buikstraand Ubelaker, 1994). For those individuals missingsexable bone elements, sex-discriminating sectioningpoints for the highly dimorphic humeral and femoralhead diameters (Bass, 1995; Purkait, 2003; Frutos,2005) were calculated ( xmaleþ x female=2 ). Theadults were segregated into three skeletally agedcohorts: young adult (~18 to ~35 years old), middleaged adult (~35 plus to ~50 years old), and old adult(50 plus years old) (Table 1).The adult skeletons were examined for anymacroscopic
evidence of reactive change (i.e. proliferative or resorptive)to the bone (Ortner, 2003; Weston, 2012), includingosteomyelitis (identified by a cloaca, sequestration and/oran involucrum), porotic pitting, periostosis (apposition ofwoven or lamellar [e.g. compact, striated] bone to theexternal cortex), diaphyseal expansion and circumscribedareas of bone loss (i.e. focal resorptive lesions)(Aufderheide and Rodriguez-Martin, 1998; Buikstra andUbelaker, 2004; Ortner, 2003). Cases of treponemaldisease were differentially identified using three levels ofdiagnostic reliability (Smith et al., 2011): pathognomonic(i.e. ectocranial stellate scarring, contiguous serpiginouscavitation and caries sicca), indicative (i.e. true [curvedinterosseous line] or pseudo-bowed [anterior periostosis]sabre tibiae [Ortner:2003:296], cavitating nodal lesions)and consistent with (i.e. nodal lesions without cavitations,focal resorptive external rib lesions or naso-palatalperiostosis that are accompanied by reactive changes[e.g. periostosis, diaphyseal expansion] on at least one long
bone). Other reactive change (i.e. diaphyseal expansion orperiostosis on pathogenetically predilected long bones[i.e. clavicles and anterior tibia]) are not consideredsupportable cases of treponemal disease (Hackett, 1976;Ortner, 2003; Smith et al., 2011).Two levels of diagnostic reliability are applied to
identifying TB in the Schroeder Mounds sample:pathognomonic (gibbus formation [(Pott’s disease])and indicative (smooth-walled lytic lesions on anterior[primarily thoracic] vertebral bodies without neuralarch involvement and anterior wedging). Althoughreactive changes such as focal resorptive lesions onvisceral rib surfaces, destructive (e.g. abscessing,osteomyelitis and tuberculous arthritis) changes to themetaphyses and articular surface(s) of the large joints(knee, hip and elbow) or periostosis on long bonemetaphyses are consistent with TB, these conditionswill not be considered supportable indications of thedisease unless they present as a suite (Marcsik et al.,2006; Ortner, 2003; Stone et al., 2009).The reactive changes on all paired bones, vertebrae,
ribs, sterna/manubria and crania were recorded onstandard forms (Buikstra and Ubelaker, 1994) andphotographed. Fisher’s exact test was utilised to assessthe pathology prevalence differences between sexesand age cohorts.
Results
Eighteen individuals or 34% (18/53) of the adult sampleexhibited proliferative or destructive periostosis indica-tive of some infectious or inflammatory process (Table 2).Eleven of 18 cases (11/29, 37.9%) were females; fourwere male (4/17, 23.5%) with (barring sampling error)no sex bias (p=0.3525). There are no cases of osteomy-elitis (i.e. involucrae and sequestrae). The most com-monly affected bone was the tibia (13/18) followed bycases with either proliferative or resorptive focal lesionson one or more ribs (7/18). After these, the descendingorder of prevalence was the clavicle (6/18), fibula(6/18), cranium (4/18), radius (4/18), humerus (3/18)and femur (2/18). No reactive change was observed onany innominate, ulna, sacrum, sternum or manubrium.
Table 1. Age and sex distribution of the Schroeder Mounds adult sample
Age category Male Female Sex indeterminate Total
Young (18–35 years) 7/17 16/29 3/7 26/53Middle age (35–50 years) 7/17 9/29 1/7 17/53Old age (50+ years) 2/17 4/29 1/7 7/53Total 16/17 29/29 5/7 50/53
778 G. M. Mosher et al.
Copyright © 2013 John Wiley & Sons, Ltd. Int. J. Osteoarchaeol. 25: 776–787 (2015)

No vertebra displayed infectious or inflammatoryreactive change.One individual (burial 12) has reactive change
restricted to a single bone; four individuals (burials 2,25A, 69, 81A and 81B) solely display focal (resorptiveor proliferative) rib lesions (Table 2). The remainingeleven individuals (including the four with reactivechanges on the cranium) exhibit periostosis on multiplebones (Table 2). Seven individuals with multiple boneinvolvement (burials 10, 48, 37A, 51, 68, 70 and 96)have reactive changes consistent with trauma (i.e. diaph-yseal misalignment). Twenty one percent of all tibiaeexhibit some level of proliferative periostosis (18/86).Seven individuals (burials 11, 48, 103, 23A, 104, 110and 37A) (Table 2) who preserve both tibiae (7/42)exhibit this bilaterally. All affected clavicles (7/78),fibulae (7/81), radii (4/86), femora (3/88) and humeri(3/93) co-occur with tibial proliferative periostosis.
Paired comparisons of cases with any type ofperiostosis by age at death (Table 1) indicates thatthere is no significant difference between the young(9/26) and middle age at death (6/17) cohorts(p= 0.6079, one tailed), or either with the old agecohort (1/7 vs. 9/26, p= 0.2937, one tailed; 1/7 vs.6/17, p= 0.3065). If the affected sample is reducedto those ageable individuals exhibiting multiplebone involvement (N= 10), there is still no statisti-cally significant difference between the young andmiddle aged samples (5/26 vs. 4/17, p=0.5111). How-ever, the results are tentative given the incumbentsampling error.
Treponemal disease
Out of the 18 individuals with some form of reactiveremodelling of the bones, 7 (7/53, 13.2%) display the
Table 2. Pathological cases in the adult sample
Burial number Age (years) Sex Pathognomic/indicativea Non-specific
10 30–40 M Cranium: cavitating and stellate lesions,endocranial plaque of lamellar andfibre bone
L. tibia: healed nodeL. radius: diaphyseal expansion
R. humerus: cavitating node L. fibula: distal diaphyseal expansion (traumatic)3 ribs: 4 pseudarthroses (trauma), with active externalfocal lesions, one healed focal lesion
11 ? ? L. and r. tibia: sabre shins (pseudo-bowing) R. femur: anterior periostosis48 50+ F Cranium: cavitating lesions, stellate scars L. clavicle: healed trauma
L. humerus, mid diaphysis: nodal periostosis,L. and r. tibia, l & r. femur, l & r. distal fibula:diaphyseal expansion
96 35–50 F Cranium: healed cavitating lesions L. tibia, l. fibula: anterior periostosisL. rib: healed trauma (misalignment)
103 25–35 M L. and r. tibia: sabre shins (pseudo-bowing)23A 25–40 F Cranium, r. malar: stellate scar L. radius: diaphyseal expansion,
L. and r. tibia: sabre shins (pseudo-bowing) R. fibula: diaphyseal expansionCranium, frontal: nondiagnostic healed cavitation
104 25–35 F R. clavicle: diaphyseal expansionL. and r. tibia: bilateral healed node
110 30–40 F L. and r. nodular periostosisL. and r. clavicle: diaphyseal expansionL. fibula: diaphyseal expansion
2 25–35 F Single rib, visceral surface: focal lesion12 18–25 F L. tibia: periosteal plaque25A 25–40 M Single rib, external surface: focal lesion37A 45–55 F Cranium: healed traumatic lesion (1.5 cm diameter)
R. radius: healed traumaR. clavicle: healed traumaL. and r. tibia: diaphyseal expansion3+ rib fragments, external surface: focal lesions
51 25–35 ? R. tibia: distal diaphyseal expansionL. rib: healed trauma
68 25–35 F L. tibia: raised striated patchesR. clavicle: expansion at mid diaphysis
69 40–50 F Two ribs: external surface focal lesion on each70 45–55 F R. tibia: anterior periostosis81A/ 81B 40–50/? M/? 4 ribs: internal surface focal lesions
aTreponemal disease, tuberculosis.
779Periosteal Reaction in Prehistoric Late Woodland Illinois
Copyright © 2013 John Wiley & Sons, Ltd. Int. J. Osteoarchaeol. 25: 776–787 (2015)

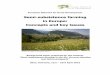
pathognomonic or indicative classification level oftreponemal disease (Table 2). Four individuals (burials10 [Figure 2a], 48, 96 and 23A) have pathognomoniccavitating, stellate and/or nodular ectocranial lesions.Burial 10 (male, aged 30–40 years) additionally hasectocranial perforation and discrete areas on theendocranial cortex of woven and lamellar plaque(Figure 2b, c), a cavitating node on the humerus(Figure 2d) and a healed node on the tibia. Burial 23Aadditionally has pseudo-bowed (anterior proliferativeperiostosis) sabre tibiae (Figure 3a) (Table 2). Threeof the pathognomonic treponemal cases exhibitreactive change indicative of traumatic injury: Burial10 has three rib pseudarthroses, burial 96 has a singlemisaligned rib and burial 48 (female, 50+ years) has atraumatic injury of the right clavicle (i.e. diaphysismisaligned and shortened). The co-association oftrauma with treponemal disease is not unusual, asectodermal injury is reportedly a common point ofentry for the spirochete (Ortner, 2003; Powell andCook, 2005).Three individuals exhibit reactive change at the
indicative level of diagnostic reliability. Burials 11(age/sex indeterminate) and 103 (male, 25–35years) havepseudo-bowed sabre tibiae (Figure 3b, c). Burial 104(female, aged 25–35years) has a cavitating node on theright tibia, a healed node on both tibia (Figure 4a, b, c),and diaphyseal expansion of the right clavicle.One additional individual has reactive bone changes
consistent with treponemal disease but is not a
supportable case. Burial 110 (female, aged 30–40 years)exhibits non-cavitating nodes on both tibiae (Figure 5a,b, c) and diaphyseal expansion of the clavicles (Table 2).If this possible case is included in the tally of treponemalcases, the Schroeder Mounds sample has a minimum of13.2% and a maximum of 15% (8/53, 15.1%). Consistentwith the literature (Cook and Powell, 2005), there isno sex difference in the maximum case sample (N=8,p=0.3657, one tailed).
Tuberculosis
No individuals exhibit reactive changes on anyvertebral body that suggest infection or inflammation(e.g., ventral destruction, ventral periostosis and fistulardefects). There are also no adult individuals whoexhibit reactive changes at the metaphyses or the largejoints. Therefore, there are no pathognomonic orindicative cases of TB.The only presenting pathology on three individuals
are resorptive or proliferative rib lesions on the pleuralsurface of one to three rib fragments (3/53, 5.3%).Burial 81A is comingled with ribs from a secondindividual (Burial 81B) and each display healed cavi-tated lesions and active perforating lesions (Figure 6a).Burial 2 has a single rib with a discrete striatedelevation (Figure 6b). TB cannot be excluded as thecausative agent (Kelley and Micozzi, 1984; Yao andSartoris, 1995; Lambert, 2002; Mays et al., 2002;Roberts and Buikstra, 2003; Raff et al., 2006; Nicklisch
Figure 2. Burial 10 (male, aged 30–40 years) exhibiting the following: (a) perforating lesions on the left frontal and stellate lesions on the posterior leftparietal, (b) frontal perforating lesions, (c) remodelled fiberbone on the endocranial surface of the frontal, and (d) a nodal lesion on the humerus.
780 G. M. Mosher et al.
Copyright © 2013 John Wiley & Sons, Ltd. Int. J. Osteoarchaeol. 25: 776–787 (2015)

et al., 2012), but other conditions such as pneumococcalinfection (Aufderheide et al., 2008), inhalation of Nicotiana(Charlton, 2004), actinomycosis and blastomycosis(Buikstra andWilliams, 1991; Pfeiffer, 1991) also manifestas reactive responses on the visceral surface of ribs.Therefore, the pleural surface rib lesions are currently bestinterpreted as non-specific reactive change.
Non-specific pathology
Including the possible treponemal case (burial 110),and the 3 individuals with visceral rib surface lesions(i.e. burials 2, 81A and 81B), 11 individuals (11/18,61%) exhibit proliferative periostosis that is not diag-nostic of a specific disease process (Table 2). These
11 include 4 of the 7 individuals (Burials 37A, 51, 68and 70) who additionally display reactive change totraumatic injury.Resorptive external rib lesions are the only
presenting pathology on two individuals (burials 25Aand 69). Therefore, 5 of the 11 nondiagnostic caseshave reactive change limited to the ribs. Resorptivecavitating rib lesions (Figure 6c) are part of the suiteof reactive changes on Burial 37A (bilateral periostosisof the tibiae, and healed traumatic injury [angulationof the distal right radial diaphysis, right clavicle witha misaligned diaphysis]). Burial 37A and the five otherindividuals (6/11) all exhibit some form of reactivechange (diaphyseal expansion and periostosis), to atleast one tibia (Table 2).
Figure 4. Burial 104 (a) has multiple nodal lesions on both tibiae; (b) a healed and (c) a single cavitating one are illustrated.
Figure 3. Anterior periostosis on the tibiae resulting in sabre tibiae on the following: (a) burial 11, (b) burial 103, and (c) burial 23A.
781Periosteal Reaction in Prehistoric Late Woodland Illinois
Copyright © 2013 John Wiley & Sons, Ltd. Int. J. Osteoarchaeol. 25: 776–787 (2015)

Discussion
An implicit goal of bioarchaeological inquiry is archaeo-logical problem solving using patterns of morbidity,mortality, and disease prevalence (Larsen, 1997; Smith,2012). When judiciously applied, this inquiry can resultin new insights about societal, subsistence or settlementpatterning that is otherwise unobtainable or ambiguouslyreflected in the material culture. The Schroeder Moundsskeletal sample straddles the time of the pivotal socioeco-nomic (maize intensification) and demographic change(clustered permanent settlement) that characterisesMississippianization. Much of this process in Illinois has
been archaeologically framed in the American Bottom(e.g. Cahokia), the lower Illinois River Valley (LIRV)and the CIRV (McElrath et al., 2000). However, thepaleopathological correlates have not been unequivocallysecured. Late Woodland subsistence and settlement inwest-central Illinois is only generally understood (Collins,1997; Benn and Green, 2000; Emerson and Titelbaum,2000) and there is a lack of comparable paleopathologicaldata (Hedman and Emerson, 2008). However, thepaleopathological co-association of sedentism with ahigh skeletal sample prevalence (i.e., ~9+%) of tertiarytreponemal disease (Cook and Powell, 2005:466;Hutchinson and Richman, 2006; Powell et al., 2005b:157;
Figure 5. (a) Bilateral nodular periostosis of the tibiae of burial 110 with lateral views of a left (b) and right (c) boxed area of the left tibia highlightingthe reactive change.
Figure 6. External rib lesions on (a) burial 37A and visceral surface lesions on (b) burials 81A-B and (c) burial 2.
782 G. M. Mosher et al.
Copyright © 2013 John Wiley & Sons, Ltd. Int. J. Osteoarchaeol. 25: 776–787 (2015)

Smith, 2006) and the presence of the pathognomonic sig-nature of TB (i.e. ventral vertebral lytic lesions and Pott’sdisease) (Roberts and Buikstra, 2003) may be useful bench-marks to evaluate the Schroeder Mounds material.
Archaeological context: remote hinterland subsistence/settlement
The Schroeder Mounds site is physiographicallylocated on a bluff top overlooking the MississippiRiver floodplain, an environment that is amenableto forager farming or permanent homesteading(Kolb, 1982). However, the paucity of material cultureand the apparent heterogeneity of late Late Woodland(AD 900–1100) ceramics-defined cultures in Illinoisimpede modelling of the subsistence-settlement pattern(Benn et al., 1992; Schroeder, 1998; Alex, 2000;Benn and Green, 2000; Esarey, 2000; Green andNolan, 2000; Stoltman, 2000; Stoltman andChristiansen, 2000; Theler and Boszhardt, 2000; Bennand Lee, 2005; Hedman and Emerson, 2008; Hedmanand Emerson, 2008; Trader, 2011). Complicatingthe subsistence-settlement reconstruction, SchroederMounds is culturally located at the Mississippian frontierand at the interface of at least three contemporaryregional late Late Woodland phases that have consider-able synonymy of (primarily ceramic) material culture.Originally affiliated with the Maples Mills phase
(AD 750–1000) of the CIRV (Riggle, 1981; Kolb,1982), Schroeder Mounds is also located at the easternperimeter of the Minotts phase (AD 950–1100) ofeastern Iowa (Alex, 2000; Benn and Green, 2000),and may be temporally and spatially included in therecently defined Louisa phase (AD 800–1200) of south-eastern Iowa and the east bank of the Mississippi Rivertrench (Benn and Green, 2000; Benn and Lee, 2005).Significant for contextualising Schroeder Mounds,Louisa phase material culture has been recovered inriparian archaeological contexts in Henderson County,Illinois (Benn, 1987; Alex, 2000; Benn and Lee, 2005;Fishel, 2008). The settlement pattern of the Louisaphase is unknown, but it has tentatively been postulatedto be permanent base camps in conjunction with tempo-rary (‘bivouac’) resource extraction sites (Benn and Lee,2005; Fishel, 2008). Additionally, the ecological contextof Schroeder Mounds is similar to the Sny Bottomalluvial plain (Figure 1) of the Mississippi River that ishome to the coeval Poisson phase (AD 800–1100)(O’Gorman and Hassen, 2000). The archaeologicalmaterial culture from the Maples Mills core area, theMinotts phase of Iowa, and the Poisson phase isinterpretively vague and has been hypothesised to
suggest a semisedentary hunting-horticultural economy(Alex, 2000; Esarey, 2000; Green and Nolan, 2000;O’Gorman and Hassen, 2000).
Treponemal disease and sedentism
In Illinois, there are tertiary stage treponemal casesfrom Late Archaic (2500–500 BC) hunter-gatherercontexts (Pete Klunk and Carrier Mills sites) with a<1% recorded prevalence (Cook, 2005; Cook andPowell, 2005). Smith (2006) observed a steep increasein treponemal disease prevalence in Tennessee withthe transition to sedentism (<1% vs. 10.7%). Despitemethodological and sampling problems, the overarch-ing pattern of treponemal disease prevalence inpre-Columbian North America is a marked increase inchronic treponemal disease visibility with sedentism(Cook and Powell, 2005:466; Hutchinson andRichman, 2006; Powell et al., 2005b:157; Smith,2006). The prevalence of pathognomonic and indica-tive treponemal disease cases in the adult SchroederMounds sample (13.2%) is consistent with sedentism.This conforms to the general model for more sedentaryLate Woodland main river channel occupation (Greenand Nolan, 2000; Simon, 2000) and tentatively sug-gests that the Louisa phase main (i.e. Mississippi River)channel base camps in Henderson County were indeedlong-term residences.Few Late Woodland sites in Illinois have been
examined for the prevalence of treponemal disease(Cook, 2005). Three sites (Gibson, Joe Gay and Ledders)with published adult prevalence (9.3%) are LIRV andbelong to the Late Woodland Jersey Bluff phase(AD 800–1350) (Cook and Powell, 2005). Thehypothesised Jersey Bluff settlement pattern is the largelong-term residence base camp (Farnsworth et al., 2000;Studenmund, 2000) which supports the interpretationfor the Schroeder Mounds people. Although IllinoisMississippian period cases of treponemal disease arereported, there is no prevalence information (Cook, 2005).
Tuberculosis and the Late Woodland
Where TB is endemic, initial infection occurs in childhoodby inhalation of bacteria from the airborne respiratoryfluids of active pulmonary cases (Schluger, 2005). Mostinfected individuals remain asymptomatic (i.e. latent);however, compromised health (e.g. malnutrition andsecondary chronic ailment) and differential strain virulencecan result in progressive respiratory infection, which canbe fatal in acute phases or become a chronic waxing andwaning disease (Smith, 2003; Schluger, 2005; Phillipsand Ernst, 2012). It is a disease epidemiologically
783Periosteal Reaction in Prehistoric Late Woodland Illinois
Copyright © 2013 John Wiley & Sons, Ltd. Int. J. Osteoarchaeol. 25: 776–787 (2015)

associated with crowding and compromised communityhygiene (Lawn and Zumla, 2011). TB often disseminatesto extrapulmonary sites with predilections to the anteriorvertebrae, visceral rib surfaces, large joints and metaphyses(Kelley and Micozzi, 1984; Aufderheide and Rodriguez-Martin, 1998;Ortner, 2003). The pathognomonic skeletalsignature of TB is certainly gibbus formation (Pott’s dis-ease); however, rib lesions, although not unique to TB(Buikstra and Williams, 1991; Pfeiffer, 1991; Lambert,2002), can be diagnostically useful (Lambert, 2002; Mayset al., 2002; Raff et al., 2006).Schroeder Mounds is located in the centre of one of
two North American regional clusters where macro-scopic evidence of pre-Columbian TB has beenidentified (Roberts and Buikstra, 2003: Table 4.1).Generally, TB was assumed to be limited to contextsthat post-date AD 900 (Stone et al., 2009) and therebyco-associate with Mississippianization. However,suggestions of sampling bias (e.g. Roberts and Buikstra,2003), biomolecular evidence (Millward et al., 2012)and evidence from Point Hope, Alaska (100 BC–AD500) (Dabbs, 2009) challenge this assumption.Regardless of ultimate antiquity, Schroeder Moundsstraddles the temporal horizon (AD 800–1100) whenTB becomes unequivocally macroscopically evident.In the LIRV, TB is not diagnostically present but
biomolecularly demonstrated at the Jersey Bluff phaseSchild site (AD 800–1050) (Braun et al., 1998; Millwardet al., 2012). Approximately 15 km away, multiple casesof Pott’s disease were observed at the Jersey BluffHacker Mounds site (AD 1022–1185) (Mosher,2012). The apparently coeval Mississippian componentat Schild (AD 1000–1200) does have pathognomoniccases of TB (Raff et al., 2006). Perhaps epidemiologi-cally significant, in the Mississippi River Valley and atthe perimeter of the Jersey Bluff culture area, theYokem Mounds site (AD 1330–1530) does not exhibitany pathognomonic cases of TB, yet individuals havetested positive for the presence of some form of TB(Millward et al., 2012). If some strain of (perhapsdifferentially virulent) TB is indeed endemically present,subsistence-settlement strategy (i.e. Mississippianization)may be epidemiologically relevant as population density,settlement aggregation, diet (composition or malnutri-tion) and community hygiene may contribute to itsvisibility in the disseminated tertiary stage (Woods,2004; Wilbur et al., 2008; Stone et al., 2009). Socialisolation might be a barrier to disease transmission(McGrath, 1988). However, there apparently were nobarriers to Late Woodland interpopulational gene flow(Droessler, 1979; Steadman, 1997). It is certainly possi-ble that socioeconomic elements of Mississippianizationthat facilitated the ubiquity of tertiary TB were separable
factors (e.g. farmstead versus aggregate village).Schroeder Mounds may have epidemiological commondenominators with Yokem and the Late WoodlandSchild samples but not Hacker Mounds, which are asyet archaeologically indeterminable but potentiallybioarchaeologically discernable.
Conclusion and future directions
The paleopathological prevalence of tertiary stagetreponemal disease in the Late Woodland communitiesof the Mississippi River Valley, who buried their dead inSchroeder Mounds, is consistent with other archaeologi-cal sample frequencies identified as sedentary. Theabsence of cases of pathognomonic TB suggests particu-lar but not yet quantified, subsistence, community healthand population aggregation characteristics. In theabsence of baseline archaeological information, theseinterpretations provide points of departure for futurebioarchaeological evaluations of Schroeder Mounds aswell as underscore the need for comparative assessmentswith other terminal Late Woodland/Emergent Mississip-pian period samples from riverine west-central Illinois.
Acknowledgements
The authors would like to thank Dr Michael Wiant(director, Dickson Mounds Museum) and the IllinoisState Museum (Springfield) for access to the SchroederMounds osteological sample, and Ms Shirley J.Schermer, burial programs director (retired), Office ofthe Iowa State Archaeologist.
References
Alex LM. 2000. Iowa’s Archaeological Past. University ofIowa Press: Iowa City.
Aufderheide AC, Rodriguez-Martin C. 1998. The CambridgeEncyclopedia of Human Paleopathology. CambridgeUniversity Press: Cambridge.
Aufderheide AC,Wittmers LE, Arriaza B. 2008. Pneumonia inantiquity: A comparison between Two Pre-antibiotic popu-lation samples from northern Chile and the United States.Chungara, Revista de Anthropología Chilena 40: 173–180.
Bass WM. 1995. Human Osteology: A Laboratory and FieldManual of theHuman Skeleton, 4th Edition. Special Publica-tion 2. Missouri Archaeological Society: Columbia Missouri.
Benn DW. 1987. Archaeology of the Mississippi RiverFloodplain at Sand Run Slough, Iowa. Report CAR-690.Center for Archaeological Research, Southwest MissouriState University, Springfield.
784 G. M. Mosher et al.
Copyright © 2013 John Wiley & Sons, Ltd. Int. J. Osteoarchaeol. 25: 776–787 (2015)

Benn DW, GreenW. 2000. Late Woodland cultures in Iowa. InLate Woodland Societies: Tradition and Transformationacross the Midcontinent, TE Emerson, DL McElrath, ACFortier (eds). University of Nebraska Press: Lincoln; 429–496.
Benn DW, Lee DV. 2005. A late Louisa phase household inthe upper Mississippi Valley, Henderson County, Illinois.Illinois Archaeology 14: 1–40.
Benn DW, Schermer S, Sellars J. 1992. Excavations of HumanRemains From The Sand Run West Site (13LA38) LouisaCounty, Iowa. BCA #150.U.S. Army Corps of EngineersRock Island District. Contract no.: DACW25-91–M-0982.
Braun M, Cook DC, Pfeiffer S. 1998. DNA from Mycobacte-rium tuberculosis complex identified in North America, pre-Columbian human skeletal remains. Journal of ArcheologicalScience 25: 271–277. DOI: 10.1006/jasc.1997.0240.
Buikstra JE, Ubelaker DH. 1994. Standards for DataCollection from Human Skeletal Remains. ArkansasArchaeological Survey Research Series, 44: Fayetteville.
Buikstra JE, Williams S. 1991. Tuberculosis in the Americas:Current perspectives. In Human Paleopathology, CurrentSyntheses and Future Options, D Ortner, A Aufderheide(eds.). Smithsonian Institution Press: Washington, DC.
Cassidy CM. 1984. Skeletal evidence for prehistoricsubsistence adaptation in the Central Ohio River Valley.In Paleopathology at the Origins of Agriculture, CohenMN, Armelagos GJ (eds). Academic Press: Orlando,Florida; 307–345.
Charlton A. 2004. Medicinal uses of tobacco in history.Journal of the Royal Society of Medicine 97: 292–296.
Collins JM. 1997. Prehistoric Archaeology of the MarriottSite: Archaeological Data Recovery at 13VB455 VanBuren County, Iowa. Research Papers Volume 22, Num-ber 2. Office of the State Archaeologist. The Universityof Iowa: Iowa City.
Cook DC. 2005. Syphilis? Not quite: Paleoepidemiology inan evolutionary context in the Midwest. In The Myth ofSyphilis: The Natural History of Treponematosis inNorth America, Powell ML, Cook DC (eds). UniversityPress of Florida: Gainesville; 177–199.
Cook DC, Powell ML. 2005. Piecing the puzzle together:North American treponematosis in overview. In TheMyth of Syphilis: The Natural History of Treponematosisin North America, ML Powell, DC Cook (eds). UniversityPress of Florida: Gainesville; 442–479.
Dabbs GR. 2009. Resuscitating the epidemiological model ofdifferential diagnosis: Tuberculosis at prehistoric PointHope, Alaska. Paleopathology Association Newsletter 148: 11–24.
Droessler J 1979. Change and Continuity: BioculturalInteraction at the Late Woodland–Mississippian Interface.Unpublished Ph.D. dissertation, Department of Anthro-pology, Indiana University, Bloomington.
Emerson TE, Lewis BR. 2000. Cahokia and the Hinterlands:Middle Mississippian Cultures of the Midwest. Universityof Illinois Press: Urbana-Champaign.
Emerson TE, Titelbaum AR. 2000. The Des Plaines complexand the Late Woodland stage of Northern Illinois. In LateWoodland Societies: Tradition and Transformation Across
the Midcontinent, TE Emerson, DL McElrath, AC Fortier(eds). University of Nebraska Press: Lincoln; 413–428.
Esarey D. 2000. The Late Woodland Maple Mills andMossville Phase Sequence in the Central Illinois RiverValley. In Late Woodland Societies: Tradition and Trans-formation Across the Midcontinent, TE Emerson, DLMcElrath, AC Fortier (eds). University of Nebraska Press:Lincoln; 387–410.
Farnsworth KB, Emerson TE, Glen RM. 2000. Patterns ofLate Woodland/Mississippian interaction in the Lower Il-linois Valley drainage: A view from Starr Village. InCahokia and the Hinterlands: Middle Mississippian Cul-tures of the Midwest, TE Emerson (ed.). University of Il-linois Press: Urbana-Champaign; 83–118.
Fishel RL. 2008. Archaeological Investigations at Site11HE551 (Shorten Site) for the TR 195A Bridge Replace-ment Over Dugout Creek Project. Archaeological TestingShort Report No. 263. Illinois Transportation Archaeo-logical Research Program. University of Illinois; Urbana-Champaign.
Frutos, LR. 2005. Metric determination of Sex from thehumerus in a Guatemalan forensic sample. Forensic ScienceInternational 147: 153–157. DOI:10.1016/j.forsciint.2004.09.077
Green W, Nolan DJ. 2000. Late woodland peoples in west-central Illinois. In Late Woodland Societies: Tradition andTransformation across the Midcontinent, TE Emerson, DLMcElrath, AC Fortier (eds). University of Nebraska Press:Lincoln; 345–386.
Hackett CJ. 1976. Diagnosis Criteria of Syphilis, Yaws andTreponarid (Treponematoses) and of Some Other Dis-eases in Dry Bones. Springer-Verlag: Berlin.
Hedman KM, Emerson TE. 2008. The luthy alps site:AMS dates, stable isotopes, and maize consumption inthe Central Illinois River Valley at the Late Woodland–Mississippian interface. Illinois Archaeology 20: 48–84.
Hitzemann NJ. 1997. Regional Osteoarthritis Patterns: AnExamination of Late Woodland Trends in West Central Il-linois. Unpublished Master’s thesis, Department of An-thropology, Illinois State University, Normal.
Hutchinson DL. 1993. Treponematosis in regional and chro-nological perspective from Central Gulf Coast Florida.American Journal of Physical Anthropology 92: 249–261.DOI: 10.1002/ajpa.1330920303
Hutchinson DL, Richman R. 2006. Regional, social, andevolutionary perspectives on treponemal infection in theSoutheastern United States. American Journal of Physical An-thropology 129: 544–558. DOI: 10.1002/ajpa.20301
Hutchinson D, Larsen CS, Williamson M, Green-Clow VD.2005. Temporal and spacial variation in the patterns oftreponematosis in Florida and Georgia. In The Myth ofSyphilis: The Natural History of Treponematosis inNorth America, Powell ML, Cook DC (eds). Universityof Florida Press: Gainesville; 92–116.
Kelley MA, Micozzi MS. 1984. Rib lesions in chronicpulmonary tuberculosis. American Journal of Physical Anthro-pology 65: 381–386. DOI: 10.1002/ajpa.1330650407
785Periosteal Reaction in Prehistoric Late Woodland Illinois
Copyright © 2013 John Wiley & Sons, Ltd. Int. J. Osteoarchaeol. 25: 776–787 (2015)

Kolb M. 1982. The Schroeder Mounds Site: A PreliminaryAnalysis from a Spatial Perspective. Unpublished Master’sthesis, Department of Anthropology, University ofWisconsin, Milwaukee.
Lambert PM. 2002. Rib lesions in a prehistoric puebloansample from Southwest Colorado. American Journal of Phys-ical Anthropology 117: 281–292. DOI: 10.1002/ajpa.10036
Langford DK. 1999. Indications of Health Status in TwoLate Woodland Sites in West-Central Illinois.Unpublished Master’s thesis, Department of Anthropol-ogy, Northern Illinois University, DeKalb.
Larsen CS. 1997. Bioarchaeology: Interpreting Behavior from theHuman Skeleton. Cambridge University Press: Cambridge.
Lawn SD, Zumla AL. 2011. Tuberculosis. Lancet 378 (9785):57–72. DOI: 10.1016/S0140-6736(10)62173-3
Mackowiak PA, Blos VT, Aguilar M, Buikstra JE. 2005. Onthe origin of American tuberculosis. Clinical Infectious Dis-eases 41(4): 515–518. DOI: 10.1086/432013
Marcsik A, Molnár E, Szathmáry L. 2006. The antiquity oftuberculosis in Hungary: the skeletal evidence. MemInst Oswaldo Cruz 101: 67–71. DOI: 10.1590/S0074-02762006001000012
Mays S, Fysh E, Taylor GM. 2002. Investigation of the linkbetween visceral surface Rib lesions and tuberculosis in amedieval skeletal series from England using ancientDNA. American Journal of Physical Anthropology 119: 27–36.DOI: 10.1002/ajpa.10099
McElrath DL, Emerson TE, Fortier AC. 2000. Social evolutionor social response? A fresh look at the “good grey cultures”after four decades of research in theMidwest. In LateWood-land Societies: Tradition and Transformation Across theMidcontinent, Emerson TE, McElrath DL, Fortier AC(eds.). University of Nebraska Press: Lincoln; 3–36.
McGrath JW. 1988. Social networks of disease spread in thelower Illinois river valley a simulation approach. AmericanJournal of Physical Anthropology 77: 483–496. DOI:10.1002/ajpa.1330770409
Millward GG, Harrison J, Cook DC, Kaestle FA. 2012.Genetic analysis of ancient Mycobacterium tuberculosiscomplex DNA from precolumbian late woodland andMississippian sites in the lower Illinois river valley.American Journal of Physical Anthropology 147(suppl 54):215. DOI: 10.1002/ajpa.22033
Mosher G. 2012. Dynamism in the Good Grey Cultures: AStudy of Communicable Disease Prevalence in the SkeletalAssemblage of Hacker South Mound 2. In Jersey County,Illinois. Program and Abstracts of the Midwestern Archae-ology Conference 2012, East Lansing, Michigan, 16.
Nansel BH, Green W. 2000. Time-trend analysis of LateWoodland pottery from western Illinois. In Mounds,Modoc, and Mesoamerica: Papers in Honor of Melvin L.Fowler, S Ahler, ED Benchley (eds). Scientific Papers,Vol XXVIII. Illinois State Museum: Springfield; 75–85.
Nicklisch N, Maixner F, Ganslmeier R, Friederich S, DreselyV, Meller H, Zink A, Alt KW. 2012. Rib lesions in skele-tons from early Neolithic sites in central Germany: Onthe trail of tuberculosis at the onset of agriculture. American
Journal of Physical Anthropology 149: 391–404. DOI:10.1002/ajpa.22137
O’Gorman J, Hassen H. 2000. Late woodland in the Missis-sippi valley of west-central Illinois: the Sny Bottom. In LateWoodland Societies: Tradition and Transformation Acrossthe Midcontinent, Emerson TE, McElrath DL, Fortier AC(eds). University of Nebraska Press: Lincoln; 277–300.
Ortner DJ. 2003. Identification of Pathological Conditionsin Human Skeletal Remains. Academic Press: Amsterdam.
Pauketat TR. 1998. Refiguring the archaeology of greaterCahokia. Journal of Archaeological Research 6: 45–89. DOI:10.1007/BF02443150
Pfeiffer S. 1991. Rib Lesions and New World Tuberculosis.International Journal of Osteoarchaeology 1: 191–198. DOI:10.1002/oa.1390010309
Phillips JA, Ernst JD. 2012. Tuberculosis pathogenesis andimmunity. Annual Review of Pathology 7: 353–384. DOI:10.1146/annurev-pathol-011811-132458
Powell, ML. 2000. Ancient diseases, modern perspectives:Treponematosis and tuberculosis in the age of agriculture.In Bioarchaeological Studies of Life in the Age of Agricul-ture: A View from the Southeast, Lambert PM (ed.). TheUniversity of Alabama Press: Tuscaloosa; 6–34.
Powell ML, Cook DC. 2005. Treponematosis: Inquiries intothe nature of a protean disease. In The Myth of Syphilis:The Natural History of Treponematosis in North America,Powell ML, Cook DC (eds). University of Florida Press:Gainesville; 9–62.
Powell ML, Bogdan G, Cook DC, Sanford MK, Smith MO,Weaver DS. 2005a. Treponematosis before 1000 BC? Theskeletal evidence. In TheMyth of Syphilis: The Natural His-tory of Treponematosis in North America, Powell ML, CookDC (eds). University of Florida Press: Gainesville; 418–441.
Powell ML, Jacobi K, Danforth ME, Eisenberg LE. 2005b.“Syphilis in mound builders’ bones”: Treponematosis inthe Central Southern United States. In The Myth ofSyphilis: The Natural History of Treponematosis inNorth America, Powell ML, Cook DC (eds). Universityof Florida Press: Gainesville; 117–161.
Purkait R. 2003. Sex determination from femoral headmeasure-ments: A new approach. Legal Medicine (Tokyo) 5(Suppl 1):S347–50. DOI: 10.1016/S1344-6223(02)00169-4
Raff J, Cook DC, Kaestle F. 2006. Tuberculosis in the NewWorld: A study of ribs from the Schild Mississippianpopulation, west-central Illinois. Memórias do InstitutoOswaldo Cruz 101(Suppl II): 25–27. DOI: 10.1590/S0074-02762006001000005
Riggle S. 1981. LateWoodland transition in the central Missis-sippi Valley: AD 700–1100. South Dakota Archaeology 5: 5–18.
Roberts CA, Buikstra JE. 2003. The Bioarchaeology ofTuberculosis. University of Florida Press: Gainesville.
Schluger NW. 2005. The pathogenesis of tuberculosis.American Journal of Respiratory Cell and Molecular Biology 32:251–256. DOI: 10.1165/rcmb.F293
Schroeder MB. 1998. Archaeobotanical sampling. In TheLiverpool Lake Site: A Late Woodland Village on theChautauqua Unit of the Illinois River National Wildlife
786 G. M. Mosher et al.
Copyright © 2013 John Wiley & Sons, Ltd. Int. J. Osteoarchaeol. 25: 776–787 (2015)

Refuges, Mason County, Illinois. Quarternary StudiesProgram, Illinois State Museum: Springfield; 108–121.
Simon ML. 2000. Regional variation in plant use strategies. InLate Woodland Societies: Tradition and Transformationacross the Midcontinent, TE Emerson, DL McElrath, ACFortier (eds). University of Nebraska Press: Lincoln; 37–76.
Smith I. 2003. Mycobacterium tuberculosis pathogenesis andmolecular determinants of virulence. Clinical Microbiology Re-views 16: 463–496. DOI: 10.1128/CMR.16.3.463-496.2003
Smith MO. 2006. Treponemal disease in the Middle Archaicto Early Woodland Periods of the western TennesseeRiver Valley. American Journal of Physical Anthropology 131:205–217. DOI: 10.1002/ajpa.20427
Smith MO. 2012. Paleopathology. In Research Methods inHuman Skeletal Biology. DiGangi EA, Moore MK (eds).Academic Press: New York; 181–218.
Smith MO, Betsinger TK, Williams LL, Robbins, AM. 2010.Canary in the coal mine: treponemal disease across subsis-tence, settlement patterning, and sociopolitical change inSouthern Appalachia. American Journal of Physical Anthropol-ogy 141(Suppl 50): 219–220. DOI: 10.1002/ajpa.21276
Smith MO, Betsinger TK, Williams LL. 2011. Differentialvisibility of treponemal disease in pre-Colombian strati-fied societies: Does rank matter? American Journal of PhysicalAnthropology 144: 185–195. DOI 10.1002/ajpa.21381
Steadman DW. 1997. Population Genetic Analysis of Regionaland Interregional Prehistoric Gene Flow in West-CentralIllinois. Unpublished Ph.D. dissertation, Department ofAnthropology, University of Chicago, Chicago.
Stoltman JB. 2000. A reconsideration of the culturalprocesses linking to its Northern Hinterlands during theperiod A.D. 1000–1200. In Mounds, Modoc, andMesoamerica: Papers in Honor of Melvin Fowler. IllinoisState Museum: Springfield; 439–467.
Stoltman JB, Christiansen GW. 2000. The Late Woodlandstage in the driftless area of the upper Mississippi Valley.In Late Woodland Societies: Tradition and Transforma-tion across the Midcontinent, TE Emerson, DL McElrath,
AC Fortier (eds). University of Nebraska Press: Lincoln;497–528.
Stone AC, Wilbur AK, Buikstra JE, Roberts CA. 2009.Tuberculosis and leprosy in perspective. American Journal ofPhysical Anthropology 52: 66–94. DOI: 10.1002/ajpa.21185
Studenmund S. 2000. Late Woodland occupations in thelower Illinois Valley: research questions and data sets. InLate Woodland Societies: Tradition and TransformationAcross the Midcontinent, Emerson TE, McElrath DL,Fortier AC (eds). University of Nebraska Press: Lincoln;301–343.
Styles BW. 2000. Late Woodland faunal exploitation in theMidwestern United States. In Late Woodland Societies:Tradition and Transformation across the Midcontinent,TE Emerson, DL McElrath, AC Fortier (eds). Universityof Nebraska Press: Lincoln; 77–96.
Theler JL, Boszhardt RF. 2000. The end of the effigy moundculture: The Late Woodland to Oneota transition inSouthwestern Wisconsin. Midcontinental Journal of Archaeol-ogy 25: 289–312.
Trader PD. 2011. Fragmented frontier: Examining a LateWoodland settlement in West-Central Illinois. IllinoisArchaeology 23: 124–157.
Weston DA. 2012. Nonspecific infection in palaeopathology:interpreting periosteal reactions. In A Companion toPaleopathology. Grauer AL (ed). Blackwell Publishing:Chichester, UK; 492–512.
White TD, Folkens PA. 2005. The Human Bone Manual.Academic Press: New York.
Wilbur AK, Farnbach AW, Knudson KJ, Buikstra JE. 2008.Diet, tuberculosis, and the paleopathological record.Current Anthropology 49: 963–991. DOI: 10.1086/592434
Woods WI. 2004. Population nucleation, intensive agricul-ture, and environmental degradation: The Cahokiaexample. Agriculture and Human Values 21: 151–157. DOI:10.1023/B:AHUM.0000029398.01906.5e
Yao DC, Sartoris DJ. 1995. Musculoskeletal tuberculosis.Radiologic Clinics of North America 33: 679–689.
787Periosteal Reaction in Prehistoric Late Woodland Illinois
Copyright © 2013 John Wiley & Sons, Ltd. Int. J. Osteoarchaeol. 25: 776–787 (2015)