Embed Size (px)
Citation preview

Trends in overdose deaths from drug misuse inEurope: what do the data tell us?
During the 1990s the number of drug-related deaths(acute poisonings) in the United Kingdom increasedrapidly. Between 1993 and 2000 the number of deathsdoubled from 864 to 1662 [1,2], precipitating the recog-nition that reducing drug misuse deaths was a publichealth priority [3]. The UK Advisory Council on theMisuse of Drugs recommended the creation of a new sur-veillance indicator to follow overdose trends, which wasincorporated into the government’s drugs strategy. Atarget was set to reduce deaths related to drug misuse by20% by 2004 compared to a 1999 baseline [4]. As morethan three-quarters of drug-related poisonings in theUnited Kingdom are opiate-related, expanding drug treat-ment options, especially methadone maintenance forproblem opiate users, was seen as a critical overdose pre-vention measure [5]. UK and European indicators ofdrug-related deaths include deaths certified as due to druguse or misuse and include acute poisonings (overdosedeaths) based on routine mortality statistics; the indica-tors exclude other deaths that may have been causeddirectly or indirectly by drug use but which cannot beattributed readily to drug use within routine statistics(such as infections, other injuries or chronic diseases) [1].
Early signs were very encouraging. Between 2001 and2004, the government investment in specialist drugtreatment doubled to over £250 million annually [6]. Thevolume of methadone prescriptions increased markedly,and there was a drop in the estimated number of deathsper 1000 patient-years treated with methadone [7]. Thenumber of drug misuse deaths fell from 2001, and by2003 the reduction in drug-related deaths had almostreached the target. However, in 2004 and 2005 therewere sharp increases in drug misuse deaths, due largelyto heroin overdose, meaning the government’s target wasnot met [8,9].
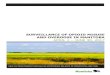
The European context is presented in Fig. 1, whichcompares trends in overdose deaths in selected Europeancountries with similar population sizes [10]. The figureshows drug misuse deaths per million population from1993 to 2005 for England and Wales, Italy, Germany andSpain (Madrid, Barcelona, Valencia, Bilbao, Seville andZaragoza only) based on routine mortality statistics. Thedrug-poisoning mortality rate in these six Spanish citiesprobably overestimates the rate for Spain overall, but islikely to provide an accurate representation of trends overtime.
By 2004/05 the drug misuse mortality rates inEngland and Wales was one of the highest in Europe.However, case definition and data extraction from mor-
tality statistics varies between countries despite therebeing a common European definition [11], which mayexplain, in part, the difference in the size of the mortalityrates between countries. There have been no changes inthe compilation of statistics over time. More illuminating,therefore, and a salutary reminder to policy makers inEngland and Wales, is the difference in trends over time.In none of the other selected European countries did theoverdose mortality rate double during the 1990s. Insteadthe evidence suggests that mortality rates declined inSpain and Italy and were stable in Germany. In addition,the other selected countries all achieved substantiallygreater reductions in drug-related deaths than Englandand Wales between 1999 and 2004/05, with Germanyand Italy exceeding a 20% reduction and Spain (six cities)reducing the drug-related mortality rate by 17%.
Surveillance of deaths related to drug misuse is impor-tant for measuring the impact of interventions and forplanning future harm minimization strategies, but itcannot answer more fundamental questions. What arethe main drivers of drug overdose trends? Is the risk ofoverdose changing? Clearly, the number of overdosedeaths is related to the interplay between changes in thesize of the drug-using population and to their overdosemortality risk, with the latter related to other factors suchas the proportion of IDU in treatment or changes in drugadministration. The increase in overdose deaths duringthe 1990s in England and Wales was driven largely byincreases in the prevalence of heroin use [2,8]. We havehypothesized that the reduction in overdose deaths from2001 may have been the result of the rate of increase intreatment superseding any increase in the prevalence ofdrug misuse, and reducing the overall risk of overdosedeath [6,12].
However, in the United Kingdom since 1993 there hasbeen no investment in large-scale longitudinal studiesthat could test this hypothesis and monitor whether theoverall risk of overdose is declining, or the emergence ordecrease of other forms of mortality among drug users.There have been a few, mainly city-based, studies inEurope [13], but the mortality patterns can be changingsubstantially and quickly [14–17] and large-scale cohortstudies are needed in different European countries thatcan provide comparable information about overdose risk.Interpreting mortality statistics and trends in drug use iscomplex, and unlikely to lead to any firm conclusionswithout information on overdose risk. The figure showsthat trends in overdose deaths vary between countries,implying differences in either the numbers of heroin
EDITORIAL doi:10.1111/j.1360-0443.2007.02102.x
© 2008 The Authors. Journal compilation © 2008 Society for the Study of Addiction Addiction, 103, 699–700

injectors or overdose mortality risk. What we need toknow, however, is whether (and why) the other Europeancountries experienced a reduction in overdose mortalityrisk and/or prevalence of injecting drug use. We believe itis important now that we seek a better understandingof the mechanisms that underlie overdose mortalitystatistics.
Keywords Drug misuse, mortality, overdose, surveil-lance monitoring.
OLIVER MORGAN
Imperial College, UKE-mail: [email protected]
JULIAN VICENTE & PAUL GRIFFITHS
European Monitoring Centre for Drugs and Drug Addiction,Portugal
MATTHEW HICKMAN
University of Bristol, UKReferences
1. Office for National Statistics. Report: deaths related to drugpoisoning: results for England and Wales, 1993–2000.Health Stat Q 2002; 13: 76–82.
2. De Angelis D., Hickman M., Yang S. Estimating long-termtrends in the incidence and prevalence of opiate use/injecting drug use and the number of former users: back-calculation methods and opiate overdose deaths. Am JEpidemiol 2004; 160: 994–1004.
3. Advisory Council of the Misuse of Drugs. Reducing DrugRelated Deaths. London: HMSO; 2000.
4. Drugs Strategy Directorate. Updated Drug Strategy. London:Home Office; 2002.
5. Ward J., Mattick R. P., Hall W. Methadone Maintenance Treat-ment and Other Opioid Replacement Therapies. Amsterdam:Harwood Academic Publishers; 1998.
6. Beynon C. M., Bellis M. A., McVeigh J. Trends in drop out,drug free discharge and rates of re-presentation: a retro-spective cohort study of drug treatment clients in the NorthWest of England. BMC Public Health 2006; 6: 205.
7. Morgan O., Griffiths C., Hickman M. Association betweenavailability of heroin and methadone and fatal poisoning inEngland and Wales 1993–2004. Int J Epidemiol 2006; 35:1579–85.
8. Morgan O., Griffiths C., Toson B., Rooney C., Majeed A.,Hickman M. Trends in deaths related to drug misuse inEngland and Wales, 1993–2004. Health Stat Q 2006; 31:23–7.
9. Office for National Statistics. Report: deaths related to drugpoisoning: England and Wales, 1999–2003. Health Stat Q2005; 33: 82–8.
10. European Monitoring Centre for Drugs and Drug Addiction.Statistical Bulletin, on-line publication. Available at: http://stats06.emcdda.europa.eu/en/elements/drdtab04-en.html.2006 (accessed 28 March 2007).
11. European Monitoring Centre for Drugs and Drug Addiction.The DRD Standard, version 3.0. Available at: http://www.emcdda.europa.eu/?nnodeid=14192002 (accessed28 March 2007).
12. Zador D., Mayet S., Strang J. Commentary: decline inmethadone-related deaths probably relates to increasedsupervision of methadone in UK. Int J Epidemiol 2006; 35:1586–7.
13. Bargagli A. M., Hickman M., Davoli M., Perucci C. A., Schi-fano P., Buster M. et al. Drug-related mortality and itsimpact on adult mortality in eight European countries. EurJ Public Health 2006; 16: 198–202.
14. Brugal M. T., Domingo-Salvany A., Puig R., Barrio G.,Garcia de Olalla P., de la Fuente L. Evaluating the impact ofmethadone maintenance programmes on mortality due tooverdose and aids in a cohort of heroin users in Spain.Addiction 2005; 100: 981–9.
15. Gossop M., Stewart D., Treacy S., Marsden J. A prospec-tive study of mortality among drug misusers during a4-year period after seeking treatment. Addiction 2002; 97:39–47.
16. Hickman M., Carnwath Z., Madden P., Farrell M., RooneyC., Ashcroft R. et al. Drug-related mortality and fatal over-dose risk: pilot cohort study of heroin users recruited fromspecialist drug treatment sites in London. J Urban Health2003; 80: 274–87.
17. Ghodse H., Oyefeso A., Kilpatrick B. Mortality of drugaddicts in the United Kingdom 1967–1993. Int J Epidemiol1998; 27: 473–8.
0
10
20
30
40
50
60
70
80
90
100
1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
Dru
g M
isus
e M
orta
lity
Rat
e
Germany Spain (selected cities) Italy England and Wales
Figure 1 Drug misuse mortality rates permillion population aged 15–64 in selectedEuropean countries, 1993 to 2005. For allcountries rates are calculated using the Euro-stat populations except for Spain, where dataare shown for six cities (Madrid, Barcelona,Valencia, Bilbao, Seville and Zaragoza) andpopulation data for these cities was providedby the 2001 Census
700 Editorial
© 2008 The Authors. Journal compilation © 2008 Society for the Study of Addiction Addiction, 103, 699–700