Embed Size (px)
Citation preview

ORIGINAL PAPER
Trends in health-related quality of life and health serviceuse associated with comorbid diabetes and major depressionin South Australia, 1998–2008
Evan Atlantis • Robert D. Goldney •
Kerena A. Eckert • Anne W. Taylor •
Patrick Phillips
Received: 17 October 2010 / Accepted: 5 May 2011 / Published online: 18 May 2011
� Springer-Verlag 2011
Abstract
Purpose To investigate the trends in health-related qual-
ity of life and health service use associated with diabetes
and/or major depression in South Australia from 1998 to
2008.
Methods Data analyzed were from 9,059 persons aged
C15 years who participated in representative surveys of the
South Australian population in 1998, 2004 and 2008. Major
depression was determined using the mood module of the
Primary Care Evaluation of Mental Disorders (PRIME-
MD). Diagnosed diabetes and health service use were
determined by self-report. Health-related quality of life was
assessed using the 36-item Short-Form Health Survey (SF-
36) and the 15-item Assessment of Quality of Life (AQoL)
instruments. Socio-demographics (including mental health
literacy), arthritis, asthma, osteoporosis, and obesity
covariates were determined by self-report. Weighted age-
standardized and multiple covariate-adjusted means of
dependent measures were computed.
Results The prevalence of diabetes only, major depres-
sion only, and comorbid diabetes and major depression
increased by 3.0 (74%), 2.6 (36%), and 0.4 (53%) per-
centage points, respectively, from 1998 to 2008. Mean
health-related quality of life scores were 9 to 41% lower
(worse), and health service use was 49% higher for persons
with comorbid diabetes and major depression than for
those with diabetes only (all P values \0.05) independent
of all covariates, consistently over the 10-year period.
Conclusions If past trends continue, our results suggest
that the increased population health and economic burden
of comorbid diabetes and major depression could persist
over the next decade or so. These trends have important
implications for making health policy and resource allo-
cation decisions.
Keywords Depression � Diabetes � Trends � QOL �Service utilization
Introduction
Depression and diabetes mellitus are among the leading
causes of disability burden [1]. Depression is consistently
associated with diabetes mellitus prevalence [2–4] and
incidence [5, 6]. Comorbid depression significantly wors-
ens the health and economic burden of diabetes. Depres-
sion in persons with diabetes is associated with non
adherence to treatment and healthy lifestyle guidelines [7,
8], poor glycemic control [9, 10], low health-related quality
of life scores [11], increased medical complications [12],
and high health service utilization and costs [13, 14].
E. Atlantis (&)
Royal Adelaide Hospital/Institute of Medical and Veterinary
Science, SA Health, Government of South Australia, Adelaide,
SA 5000, Australia
e-mail: [email protected]
E. Atlantis � K. A. Eckert � A. W. Taylor � P. Phillips
School of Medicine, The University of Adelaide, Adelaide,
SA 5005, Australia
R. D. Goldney
Discipline of Psychiatry, The University of Adelaide, Adelaide,
SA 5005, Australia
R. D. Goldney
Hanson Institute, SA Pathology, Royal Adelaide Hospital,
Adelaide, SA 5000, Australia
P. Phillips
Department of Endocrinology, The Queen Elizabeth Hospital,
Woodville South, Adelaide, SA 5011, Australia
123
Soc Psychiatry Psychiatr Epidemiol (2012) 47:871–877
DOI 10.1007/s00127-011-0394-4

Population trends provide important epidemiologic
information for estimating changes in the burden of med-
ical conditions, including health-related quality of life
measures, for health resource allocation decisions [15]. We
recently showed that the prevalence of diabetes and major
depression in the Australian population increased signifi-
cantly over the recent decade [16, 17]. Similar trends have
been reported for the US population [18, 19]. Whether
changes in the burden of diabetes differed according to the
presence or absence of major depression during this period
is not yet determined. To address this knowledge gap, we
report 10-year trends in health-related quality of life and
health service use associated with diabetes and/or major
depression in the South Australian population aged
15 years or older from 1998 to 2008, independent of an
extensive range of potential covariates.
Methods
Survey design and sampling procedure
Data were obtained from the 1998, 2004 and 2008 South
Australian Health Omnibus Surveys (SAHOS) conducted
in the autumn of each year by the Population Research and
Outcome Studies Unit, Department of Health, South Aus-
tralia. Ethics approval for each of the three surveys was
received from the South Australian Department of Health
Human Research Ethics Committee.
The SAHOS is an annual user-pays population-based
survey administered to metropolitan and country South
Australian residents, aged 15 years or older, via a face-to-
face interview. Data collection included questions which
were of direct relevance to information requirements of
payee organizations. It uses a random stratified sampling
technique in metropolitan areas based on the census col-
lectors’ districts used by the Australian Bureau of Statis-
tics. Ten dwellings were chosen in each district by
selecting every fourth household from a random starting
point. The rural sample included country towns with a
population of 1,000 or more. Where more than one person,
aged 15 years or older, resided in the household, the person
with the last birthday was selected for interview. A mini-
mum of six visits were made to each household in an
attempt to interview the selected person and replacement
interviews were not conducted.
Measures
Socio-demographics
Age, sex, country of birth, relationship status, education
attainment, area of residence, living arrangement and
employment status information was collected using stan-
dard questions. Mental health literacy was assessed by
asking participants about their knowledge of and beliefs
about depression, as described previously [17, 20]. The
accuracy of responses was rated (scored from 0 to 200)
according to a previously validated algorithm [21], and
tertile cut-offs were used to group participants into ‘poor or
fair’ (0 to 149), ‘good’ (150 to 199) or ‘excellent’ (200)
mental health literacy categories.
Medical conditions
Lifetime diagnosis of arthritis, asthma, osteoporosis, and
diabetes was determined by self-report. Body mass index
(BMI) was derived from self-report height and weight
values, and computed as weight in kilograms divided by
height in meters squared. Obesity was defined by the BMI
cut-off of C30, according to international criteria. Major
depression was determined using the mood module of the
Primary Care Evaluation of Mental Disorders (PRIME-
MD) procedure, which has demonstrated reliability [22],
and diagnostic accuracy in primary health care settings
[23]. It consists of 16 questions relating to symptoms of
depression experienced nearly every day for the last
2 weeks (categorized as yes/no). Classification of major
depression was according to an algorithm based on the
Diagnostic and Statistical Manual of Mental Disorders, 4th
Edition, (DSM-IV) definition.
Health-related quality of life and health service use
outcomes
Health-related quality of life was assessed using the
36-item Short-Form Health Survey (SF-36) (available
from: http://www.qualitymetric.com) and the 15-item
Assessment of Quality of Life (AQoL) [24] instruments.
Physical and Mental Component Summary scores (PCS
and MCS) of the SF-36 were derived from the aggre-
gation of scores from 36 questions across eight dimen-
sions of health and wellbeing. Because the SF-36
Version 1 was used in the 1998 survey whereas the SF-
36 Version 2 was used in the subsequent cycles, T scores
for PCS and MCS were computed using appropriate
Australian population norms [25] for comparisons across
surveys.
AQoL scores are derived from 15 questions across five
dimensions of health-related quality of life (illness, inde-
pendent living, social relationships, physical senses, and
psychological wellbeing) [24]. Individual items are sum-
med to provide a score for each dimension ranging from
zero, worst AQoL (death) to one, full or normal health
(without handicap, impairment or disability) and an overall
score to compare AQoL profiles.
872 Soc Psychiatry Psychiatr Epidemiol (2012) 47:871–877
123

Health service use in the preceding month was deter-
mined by self-report. First, participants were asked ‘‘In the
last month, which of these health services have you used in
South Australia?’’ The list of health services was extensive
and included an ‘‘other (specify)’’ response option, but
dental health services was not listed in the 1998 survey.
Second, participants were asked ‘‘How many times in the
last month have you visited any health services?’’ The total
number health services used (excluding dental) were
aggregated for analysis.
Statistical analyses
Statistical analyses were completed using SPSS version
17.0 (SPSS Inc. Chicago, US). All analyses accounted for
the complex sample design. Statistical tests were 2-sided
and a P value of \0.05 was considered indicative of sta-
tistical significance. All data were age within sex stan-
dardized to the South Australian population distributions
according to the 2001 Census of Population and Housing.
Trends in weighted age-standardized prevalence and mean
estimates of population characteristics were computed
using logistic regression for categorical data fitted with
survey year as a continuous variable, and general linear
models for continuous data with survey year for orthogonal
polynomial contrasts. Weighted age-standardized and
multiple-adjusted means (mean [95% CI]) of SF-36 PCS
T scores, SF-36 MCS T scores, AQoL scores, and health
service use were computed using general linear models that
included survey by diabetes and/or major depression group
interactions and survey year for orthogonal polynomial
contrasts, with adjustment for all socio-demographics and
medical conditions listed in the Table 1 (except for BMI
due to a large number of missing cases). All models were
subsequently repeated with BMI as a covariate, in a series
of sensitivity analyses.
Results
Response rates for the 1998, 2004, and 2008 surveys were
82, 76, and 73%, respectively; excluding persons who were
out of scope (households were vacant, not contactable after
six visits, or had occupants unable to speak English, or with
mental incapacity). Trends in the weighted age-standard-
ized prevalence and mean estimates of population charac-
teristics across the three surveys appear in the Table 1. The
prevalence of diabetes only, major depression only, and
comorbid diabetes and major depression (both) increased
by 3.0 (74%), 2.6 (36%), and 0.4 (53%) percentage points,
respectively, over the 10-year period. Mean SF-36 MCS
T scores and AQoL scores decreased by 2.9 (6%) and 0.02
(3%) points, SF-36 PCS T scores remained relatively
stable, and health service use increased by 0.2 (21%) units
over the 10-year period. The prevalence of male sex, higher
education attainment, full-time or part-time employment,
retirement, excellent mental health literacy, asthma, oste-
oporosis, and obesity increased across survey cycles. In
contrast, the prevalence of residing in metropolitan regions,
living alone, unemployment, and non workforce partici-
pation (other/homemaker/student status) decreased across
survey cycles. No significant changes were observed for
birth region, relationship status, or arthritis variables across
survey cycles.
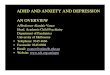
Results for health-related quality of life scores and
health service use by diabetes/major depression group
appear in the Fig. 1a–d. Weighted age-standardized and
multiple covariate-adjusted mean SF-36 PCS T scores, SF-
36 MCS T-scores, and AQoL scores were 3.63 (9%), 20.35
(41%), and 0.23 (35%) points lower, respectively; and
health service use was 0.75 (49%) units higher for persons
with comorbid diabetes and major depression than for
those with diabetes only (all P values \0.05). No signifi-
cant interactions for survey by diabetes and/or major
depression group were observed. Results remained
unchanged (all P values) when all models were addition-
ally adjusted for BMI.
Conclusions
These results indicate that the prevalence of diabetes only,
major depression only, and comorbid diabetes and major
depression increased by 74, 36 and 53%, respectively, in
the South Australian population from 1998 to 2008.
Health-related quality of life was worse and health service
use was higher for persons with comorbid diabetes and
major depression than for those with diabetes only inde-
pendent of all covariates, consistently over the 10-year
period. These effect sizes are consistent with those reported
in previous cross-sectional studies for health-related qual-
ity of life outcomes [11] and health service utilization in
the US [13].
Our results have implications for both clinical practice
and economic evaluation. Prospective findings of a ran-
domized trial conducted in patients with diabetes show
that a 10% higher health-related quality of life score is
associated with a 7% reduced risk of vascular events, a
13% reduced risk of diabetes complications, and a 14%
lower rate of all-cause mortality [26]. Of further clinical
importance, having problems with mobility was the only
dimension independently predictive of those events,
which suggests that physical rather than mental health
dimensions of health-related quality of life might provide
the most relevant prognostic information in patients with
diabetes.
Soc Psychiatry Psychiatr Epidemiol (2012) 47:871–877 873
123

Table 1 Trends in prevalence and mean estimates of population characteristics for South Australian Health Omnibus Surveys 1998, 2004, and
2008
Weighted no. of participantsa N = 3,010 (1998) N = 3,015 (2004) N = 3,034 (2008) P valueb
Factors % or mean (95% CI) % or mean (95% CI) % or mean (95% CI)
Socio-demographic
Age (Mean years) 45.2 (44.5–45.9) 45.2 (44.5–45.9) 45.2 (44.5–45.9) 0.973
Sex, male (%) 40.2 (38.4–42.0) 41.7 (39.9–43.5) 43.7 (41.9–45.5) 0.006
Birth region, Australia/UK/Ireland (vs. other) (%) 87.8 (86.6–88.9) 87.8 (86.5–88.9) 87.6 (86.4–88.7) 0.967
Relationship status, partnered (%) 53.2 (51.3–55.0) 53.0 (51.2–54.9) 55.3 (53.5–57.2) 0.097
Residential area, metropolitan (vs. rural) (%) 79.3 (77.8–80.7) 78.4 (76.9–79.9) 76.5 (74.9–78.0) 0.011
Living arrangement, alone (vs. with others) (%) 27.6 (26.1–29.3) 27.0 (25.4–28.6) 24.9 (23.4–26.5) 0.016
Education attainment
Primary/trade (%) 33.9 (32.2–35.6) 29.5 (27.8–31.1) 28.4 (26.8–30.1) \0.001
Secondary (%) 33.8 (32.1–35.5) 32.4 (30.7–34.2) 31.1 (29.4–32.8)
Tertiary (%) 32.3 (30.7–34.1) 38.1 (36.4–39.9) 40.5 (38.7–42.3)
Employment status
Working full-time/part-time (%) 50.4 (48.5–52.2) 53.7 (51.8–55.5) 55.4 (53.5–57.2) \0.001
Unemployed (%) 3.6 (2.9–4.3) 2.4 (1.9–3.1) 2.6 (2.1–3.3)
Retired (%) 16.4 (15.2–17.7) 18.6 (17.4–20.0) 19.1 (17.9–20.5)
Other/homemaker/student (%) 29.6 (28.0–31.3) 25.3 (23.7–27.0) 22.9 (21.3–24.5)
Mental health literacy
Poor/Fair (%) 50.1 (48.3–51.9) 33.0 (31.3–34.8) 31.7 (30.0–33.4) \0.001
Good (%) 19.5 (18.1–21.0) 21.9 (20.4–23.5) 20.0 (18.6–21.6)
Excellent (%) 30.4 (28.8–32.1) 45.1 (43.2–46.9) 48.3 (46.4–50.1)
Medical conditions
Arthritis (%) 24.1 (22.6–25.7) 25.1 (23.6–26.7) 24.6 (23.1–26.1) 0.665
Asthma (%) 19.0 (17.6–20.5) 23.3 (21.8–24.9) 25.4 (23.8–27.0) \0.001
Osteoporosis (%) 4.0 (3.4–4.8) 5.6 (4.9–6.4) 5.7 (5.0–6.6) 0.001
Obesityc (%) 17.4 (14.6–17.4) 20.0 (17.1–20.0) 22.4 (19.3–22.4) \0.001
Diabetes and/or major depression
None (%) 88.0 (86.8–89.1) 83.8 (82.4–85.1) 82.0 (80.5–83.3) \0.001
Diabetes only (%) 4.0 (3.4–4.8) 6.6 (5.8–7.5) 7.0 (6.2–8.0)
Major depression only (%) 7.2 (6.3–8.2) 8.5 (7.5–9.6) 9.8 (8.7–11.0)
Both (%) 0.8 (0.5–1.2) 1.1 (0.8–1.6) 1.2 (0.9–1.6)
Health-related quality of lifed
SF-36 PCS, mean T score 49.1 (48.8–49.5) 49.5 (49.1–49.9) 49.5 (49.1–49.9) 0.189
SF-36 MCS, mean T score 51.4 (51.0–51.8) 49.4 (49.0–49.8) 48.5 (48.1–48.9) \0.001
AQoL, mean score 0.81 (0.80–0.82) 0.80 (0.79–0.81) 0.79 (0.78–0.80) \0.001
Health service use in the preceding month
Mean no. 1.0 (0.9–1.0) 1.1 (1.0–1.1) 1.2 (1.1–1.2) \0.001
No. C2 (vs. 0–1) (%) 23.0 (21.5–24.5) 27.3 (25.7–28.9) 31.3 (29.6–33.0) \0.001
a Age within sex standardized to the South Australian population distribution according to the 2001 Census of Population and Housingb P value for linear trend analysis using logistic regression for categorical data fitted with survey year as a continuous variable, and general linear
model for continuous data with survey year for orthogonal polynomial contrastsc Sample sizes are N = 2,736, N = 2,737, and N = 2,749 for 1998, 2004, and 2008, respectively, due to missing data; obesity defined by body
mass index C30d PCS, physical component summary; MCS, mental component summary; AQoL, assessment of quality of life sample sizes are N = 2,933,
N = 3,015, and N = 3,026 for 1998, 2004, and 2008, respectively, due to missing data
874 Soc Psychiatry Psychiatr Epidemiol (2012) 47:871–877
123

Improving health-related quality of life for risk reduc-
tion in persons with comorbid diabetes and depression
might be achievable with appropriate intervention. Ran-
domized trials have shown that effects of lifestyle (exer-
cise-based) interventions on health-related quality of life
outcomes and clinically significant depressive symptoms
are sufficient in size to reduce the risk of adverse outcomes,
as detailed above [27]. But depression presents significant
barriers to effective and sustainable healthy lifestyle
changes [7, 8] that need to be addressed in order to benefit
persons with comorbid diabetes.
How to address the consistently higher health service
use among persons with major depression compared with
those with diabetes only is less clear. The prevalence of
major depression increased by 3.5 percentage points (from
6.8% to 10.3%) in South Australia over the 10-year period
[17] despite concerted efforts made at government, pro-
fessional, charitable and industry levels to enhance public
knowledge about major depression and the effectiveness
and availability of treatments, including the extension in
2006 of Medicare rebate services to general practitioners
and allied health professionals providing mental health
care, and increases in prescriptions for antidepressant
medications [28]. These initiatives might have even had
unintended consequences, as mental health literacy was
found to be significantly associated with higher prevalence
None Diabetes Major depression Both
None Diabetes Major depression Both None Diabetes Major depression Both
None Diabetes Major depression Both
SF
-36
PC
S T
-sco
re (
wei
gh
ted
mea
n, 9
5% U
CL
)
0
10
20
30
40
50
Ref
Ref
P < 0.001 for all
P = 0.002 P = 0.017
P = 0.158 for survey by diabetes and depression interactionP = 0.065 for orthogonal polynomial contrasts for trends across surveysWeighted N = 9,034; UCL, upper confidence limit
A
SF
-36
MC
S T
-sco
re (
wei
gh
ted
mea
n, 9
5% U
CL
)
0
10
20
30
40
50
60
Ref
Ref
P < 0.001 for both
P < 0.001 P = 0.647
P = 0.390 for survey by diabetes and depression interactionP < 0.001 for orthogonal polynomial contrasts for trends across surveys P < 0.001 for linear trend across survey (coefficient = -2.349)P = 0.363 for quadratic trend across surveys (coefficient = 0.504)Weighted N = 9,034
P = 0.210 B
AQ
oL
(w
eig
hte
d m
ean
, 95%
UC
L)
0.0
0.2
0.4
0.6
0.8
Ref
Ref
P < 0.001 for all
P < 0.001 P = 0.833
PP Weighted N = 8,963
CH
ealt
h s
ervi
ce u
se (
wei
gh
ted
mea
n, 9
5% U
CL
)
0.0
0.5
1.0
1.5
2.0
2.5
3.0
Ref
Ref
P < 0.001 for all
P < 0.001 P = 0.163
PPWeighted N = 9047
D
Fig. 1 Weighted age-standardized and multiple-adjusted mean SF-36 PCS T scores (a), SF-36 MCS T scores (b), AQoL scores (c), and health
service use (d) by diabetes and/or major depression group
Soc Psychiatry Psychiatr Epidemiol (2012) 47:871–877 875
123

of major depression [17]. Collectively, this body of evi-
dence suggests that the benefits of enhancing public
knowledge about depression are questionable, and that new
and more efficient management systems for depression
need to be tested in Australia, such as collaborative care
[29] integrated within lifestyle programs.
The strength of our study is that the findings are based
on three large representative population-based surveys that
had used identical methodologies. Information was col-
lected via face-to-face interview, and major depression was
measured accurately and defined according to the DSM-IV
criteria. A principle limitation is that diabetes was mea-
sured by self-report, and thus some persons with unknown
diabetes would likely have been misclassified as not having
diabetes [30]; and specific diabetes (type 1/type 2) infor-
mation was not collected.
Changes in other dimensions of health services such
as integration of care for multiple conditions and inten-
sity of care (duration per consultation) were biases not
accounted for, and so the burden of health service use
assessed by frequency alone might have been under-
estimated. This potential limitation is attenuated some-
what because our main results were independent of a
changes in several medical conditions and obesity over
the 10-year period. Although commonly investigated in
previous studies [11], another limitation is that mental
health components of health-related quality of life mea-
sures overlap with symptoms of major depression.
Indeed, our results show that mean SF-36 MCS T-scores
and AQoL scores were very similar for persons with
major depression only and for those with both condi-
tions, and this raises doubts about the validity of
investigating mental health constructs of health-related
quality of life measures in persons with major depres-
sion. Other limitations include biases due to self-report
measures, respondent compliance, and to misclassifi-
cation errors for covariates.
In summary, health-related quality of life was worse and
health service use was higher in the South Australian
population for persons with comorbid diabetes and major
depression than for those with diabetes only, consistently
from 1998 to 2008. If past trends in the prevalence of
diabetes [16] and major depression [17] continue, in line
with the projected increases worldwide [31, 32], our results
suggest that the increased population health and economic
burden (from health service use) of comorbid diabetes and
major depression could persist over the next decade or so.
This is likely to lead to an increase in vascular events, risk
of diabetes complications and all-cause mortality [26].
Lifestyle interventions might reduce the health and eco-
nomic burden of comorbid diabetes and major depression,
but further research is needed to provide large-scale, long-
term randomized trial data. Furthermore, these trends have
important implications for making health policy and
resource allocation decisions.
Acknowledgments This research has been supported by grants
from Eli Lilly Australia, Janssen-Cilag, Lundbeck Australia, Organon
Australian, Sanofi-Synthelabo, Wyeth Australia, Ramsay Health Care
Australia, The Commonwealth Department of Health and Aging, The
Hanson Institute and Medvet Science, SA Pathology. None of these
organizations participated in the design of the study, analysis of data,
or the writing up of the results.
Conflict of interest None of the authors have any relevant conflict
of interest to disclose.
References
1. Vos T, Mathers C, Herrman H, Harvey C, Gureje O, Bui D,
Watson N, Begg S (2001) The burden of mental disorders in
Victoria, 1996. Soc Psychiatry Psychiatr Epidemiol 36:53–62
2. Goldney RD, Phillips PJ, Fisher LJ, Wilson DH (2004) Diabetes,
depression, and quality of life: a population study. Diabetes Care
27:1066–1070
3. Ali S, Stone MA, Peters JL, Davies MJ, Khunti K (2006) The
prevalence of co-morbid depression in adults with type 2 diabe-
tes: a systematic review and meta-analysis. Diabet Med 23:
1165–1173
4. Rajala U, Keinanen-Kiukaanniemi S, Kivela SL (1997) Non-
insulin-dependent diabetes mellitus and depression in a middle-
aged Finnish population. Soc Psychiatry Psychiatr Epidemiol
32:363–367
5. Atlantis E, Browning C, Sims J, Kendig H (2010) Diabetes
incidence associated with depression and antidepressants in the
Melbourne Longitudinal Studies on Healthy Ageing (MELSHA).
Int J Geriatr Psychiatry 25:688–696
6. Mezuk B, Eaton WW, Albrecht S, Golden SH (2008) Depression
and type 2 diabetes over the lifespan: a meta-analysis. Diabetes
Care 31:2383–2390
7. Gonzalez JS, Peyrot M, McCarl LA, Collins EM, Serpa L,
Mimiaga MJ, Safren SA (2008) Depression and diabetes treat-
ment nonadherence: a meta-analysis. Diabetes Care 31:
2398–2403
8. Lin EH, Katon W, Von Korff M, Rutter C, Simon GE, Oliver M,
Ciechanowski P, Ludman EJ, Bush T, Young B (2004) Rela-
tionship of depression and diabetes self-care, medication adher-
ence, and preventive care. Diabetes Care 27:2154–2160
9. Lustman PJ, Anderson RJ, Freedland KE, de Groot M, Carney
RM, Clouse RE (2000) Depression and poor glycemic control: a
meta-analytic review of the literature. Diabetes Care 23:934–942
10. Chiu C-J, Wray L, Beverly E, Dominic O (2010) The role of
health behaviors in mediating the relationship between depressive
symptoms and glycemic control in type 2 diabetes: a structural
equation modeling approach. Soc Psychiatry Psychiatr Epidemiol
45:67–76
11. Schram MT, Baan CA, Pouwer F (2009) Depression and quality
of life in patients with diabetes: a systematic review from the
European depression in diabetes (EDID) research consortium.
Curr Diabetes Rev 5:112–119
12. Lin EH, Rutter CM, Katon W, Heckbert SR, Ciechanowski P,
Oliver MM, Ludman EJ, Young BA, Williams LH, McCulloch
DK, Von Korff M (2010) Depression and advanced complica-
tions of diabetes: a prospective cohort study. Diabetes Care
33:264–269
876 Soc Psychiatry Psychiatr Epidemiol (2012) 47:871–877
123

13. Egede LE, Zheng D, Simpson K (2002) Comorbid depression is
associated with increased health care use and expenditures in
individuals with diabetes. Diabetes Care 25:464–470
14. Le T, Able S, Lage M (2006) Resource use among patients with
diabetes, diabetic neuropathy, or diabetes with depression. Cost
Eff Resour Alloc 4:18
15. Torrance GW (1986) Measurement of health state utilities for
economic appraisal: a review. J Health Econ 5:1–30
16. Atlantis E, Lange K, Wittert GA (2009) Chronic disease trends
due to excess body weight in Australia. Obes Rev 10:543–553
17. Goldney RD, Eckert KA, Hawthorne G, Taylor AW (2010)
Changes in the prevalence of major depression in an Australian
community sample between 1998 and 2008. Aust N Z J Psy-
chiatry 44:901–910
18. Sclar DA, Robison LM, Skaer TL (2008) Ethnicity/race and the
diagnosis of depression and use of antidepressants by adults in the
United States. Int Clin Psychopharmacol 23:106–109
19. Cowie CC, Rust KF, Ford ES, Eberhardt MS, Byrd-Holt DD, Li
C, Williams DE, Gregg EW, Bainbridge KE, Saydah SH, Geiss
LS, Cowie CC, Rust KF, Ford ES, Eberhardt MS, Byrd-Holt DD,
Li C, Williams DE, Gregg EW, Bainbridge KE, Saydah SH,
Geiss LS (2009) Full accounting of diabetes and pre-diabetes in
the US population in 1988–1994 and 2005–2006. Diabetes Care
32:287–294
20. Jorm AF, Korten AE, Jacomb PA, Christensen H, Rodgers B,
Pollitt P (1997) ‘‘Mental health literacy’’: a survey of the public’s
ability to recognise mental disorders and their beliefs about the
effectiveness of treatment. Med J Aust 166:182–186
21. Dunn KI, Goldney RD, Grande ED, Taylor A (2009) Quantifi-
cation and examination of depression-related mental health lit-
eracy. J Eval Clin Pract 15:650–653
22. Bakker IM, Terluin B, van Marwijk HWJ, van Mechelen W,
Stalman WAB (2009) Test-retest reliability of the PRIME-MD:
limitations in diagnosing mental disorders in primary care. Eur J
Public Health 19:303–307
23. Spitzer RL, Williams JB, Kroenke K, Linzer M, deGruy FV 3rd,
Hahn SR, Brody D, Johnson JG (1994) Utility of a new procedure
for diagnosing mental disorders in primary care. The PRIME-MD
1000 study. JAMA 272:1749–1756
24. Hawthorne G, Richardson J, Osborne R (1999) The Assessment
of Quality of Life (AQoL) instrument: a psychometric measure of
Health-Related Quality of Life. Qual Life Res 8:209–224
25. Hawthorne G, Osborne R, Taylor A, Sansoni J (2007) The SF36
Version 2: critical analyses of population weights, scoring algo-
rithms and population norms. Qual Life Res 16:661–673
26. Clarke PM, Hayes AJ, Glasziou PG, Scott R, Simes J, Keech AC
(2009) Using the EQ-5D index score as a predictor of outcomes
in patients with type 2 diabetes. Med Care 47:61–68
27. Atlantis E, Chow C-M, Kirby A, Fiatarone Singh M (2004) An
effective exercise-based intervention for improving mental health
and quality of life measures: a randomized controlled trial. Prev
Med 39:424–434
28. Mant A, Rendle VA, Hall WD, Mitchell PB, Montgomery WS,
McManus PR, Hickie IB (2004) Making new choices about
antidepressants in Australia: the long view 1975–2002. Med J
Aust 181:S21–S24
29. Gilbody S, Bower P, Fletcher J, Richards D, Sutton AJ (2006)
Collaborative care for depression: a cumulative meta-analysis
and review of longer-term outcomes. Arch Intern Med 166:
2314–2321
30. Dunstan DW, Zimmet PZ, Welborn TA, Sicree RA, Armstrong T,
Atkins R, Cameron AJ, Shaw JE, CSobotAS Committee (2001)
Diabesity & associated disorders in australia—2000. The accel-
erating epidemic. International Diabetes Institute, Melbourne
31. World Health Organization (2008) The global burden of disease:
2004 update WHO Press
32. International Diabetes Federation (2009) IDF Diabetes Atlas 4th
edition. International Diabetes Federation
Soc Psychiatry Psychiatr Epidemiol (2012) 47:871–877 877
123