Embed Size (px)
Citation preview

Treatments of chronic rhinitis in children
APAPARI Workshop ‐ Cambodia, September 12, 2015
Jiu‐Yao Wang, MD, DPhilDistinguished Professor of PediatricsDirector , Allergy and Clinical Immunology Research (ACIR) CenterNational Cheng Kung University Tainan, TAIWAN
Quality of Life
• Patients’ quality of life can be profoundly affected by Allergic Rhinitis.
• Typical Effects:
– Loss of QoL
– Fatigue
– Low energy
– Decrease in social functioning
– Learning impairment
– Anxiety
– Inability to integrate

Allergies in Asia‐Pacific: A Survey of Diagnosed Patients with Allergic Rhinitis
3
Population Sampling Frame Interview lengthAdults or children and adolescents diagnosed with nasal allergies or allergic rhinitis, symptomatic or being treated for nasal allergies in the past 12 months
Telephone* and in-person#
screening of national or major city sample of households
Range:10 - 90 min.Mean: 34.9 min.
CountryNumber of Households
Screened
Completed Sample
Philippines 1,285# 100
Australia
China
Korea
Hong Kong
Malaysia
Singapore
Taiwan
Vietnam
3,534*
19,580*
608&
2,118*
491#
2,002#
1,780*
2,588#
303
325
300
100
100
100
100
107
TOTAL: 33,986 1,535
&Korea used a different methodology – physician referral.
Comparison of three published allergic rhinitis control
questionnairesCARAT (33-35) RCAT (36,37) ARCT (38)
Administration mode Self-questionnaire Self-questionnaire Self-questionnaire
Diseases considered Allergic rhinitis and asthma Allergic rhinitis Allergic rhinitis
Period of evaluation The previous 4 weeks The previous week The previous 2 weeks
Number of final items/questions
17 in development, 10 in the final tool
26 in development 6 in the final tool
5 in the final tool
Response type 4-point frequency scale and some yes/no items
5-point Likert scale 5-point frequency scale
Validation status Tested in 141 non-treated adult patients (CARAT 1/)
and then 193 adults (CARAT 10). Internal consistency over 0.70. Longitudinal
validation in 51 patients at 4 outpatient clinics. Test-
retest reliability (intra-class correlation coefficient) =
0.82
Psychometric validation by 410 patients consulting allergy specialists. God psychometric properties
and reliable internal consistency (Cronbach alpha coefficient: 0.70)
Tested in 902 patients selected by 411 primary
care physicians and allergists. Internal consistency: 0.77
Other comments Tested in patients consulting an allergist
Significant correlations with physician-rated disease
severity, total nasal symptom score and
physician-recommended change in therapy
Based on the Asthma Control Questionnaire.
Significant correlations with the clinical picture and the
impact of allergic rhinitis on social and sports activities.
Demoly et al. Clinical & Translational Allergy 2013

Mean Work or School Productivity
Q26. Thinking about (your/your child’s) ability to do the things (you want/ he/she wants) to on a scale from 0 to 100, where 100 means 100% able, where would you rank (your/his/her) ability on days when (you don’t have/he/she doesn’t have) nasal allergy symptoms? N = 300
Q27. Where would you rank (your/your child’s) ability to the things (you want/he/she wants) to do on the same scale of 0 to 100, where 100 means 100% able, when (your/his/her nasal) allergies are at their worst? N = 100
Impact of Nasal Allergies on Daily Life
Q30. During the worst one month period, would you say the condition impacted (your/his/her) daily life a lot, a moderate amount, some, a little or did not really impact daily life? N = 99

Most Bothersome Symptom of Nasal Allergy: Allergies in Asia‐Pacific Survey
Q19. Which of these symptoms was the MOST bothersome to (you/your child)?Base: Had at least one extremely or moderately bothersome symptom, N = 89
How Bothersome are Symptoms:All AIAP Countries
Q18. When (you have/your child has) nasal allergy attacks, how bothersome are the following symptoms usually: extremely bothersome, moderately bothersome, slightly bothersome, or not bothersome?Base: Had symptom at least a few days a month

Worst Months for Nasal Allergies
Q15b. During what particular months of the year are (your/his/her) nasal allergies the worst? Base: Reported seasonal allergies N = 82



Allergic Rhinitis
Recurrent Rhinitis due to an IgE –mediated reaction of the nasal mucosa to allergens.
Characterize by sneezing,
itching,congestion, rhinorrhea
and ocular symptoms
Source: Bousquet et al. J Allergy Clin Immunol. 2001; 108 (5 suppl):S147; Bauchau and Durham. Eur Respir J.2004; 24:758; Linneberg. BMJ 2005:331.352; Wjst et al. PLoS Med. 2005; 2:e294; Jarvis et al. J Allergy Clin Immunol. 2005; 116:675.
Prevalence of Allergic Rhinitis (AR)
• AR is one of the most common chronic conditions, particularly in subjects under 18
– 500 million sufferers worldwide, 250 million in China
– Up to 40% of children
• Impact
– Impacts on quality of life, work/school
performance and productivity

Allergic Rhinitis
Provoked by exposure to allergens in the environment.
A. Pollens – birch grass, weed
B. House dust mites
C. Animal danders
D. Cockroaches and certain mold species


How does one develop Allergic Rhinitis

Diagnosis
1.History
a. Exposure to specific allergen
b. Nasal congestion, rhinorrhea, itching, and sneezing
c. Family history of allergy
2. Skin testing

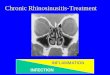
ARIA classification of allergic rhinitis
Moderate‐severe
one or more items
• abnormal sleep
• Impairment of daily
activities, sport, leisure
• abnormal work and school
• troublesome symptoms
Intermittent symptoms• 4 days per week• or 4 weeks
Persistent symptoms• 4 days per weeks• and 4 weeks
Mild all of the following• Normal sleep• No impairment of daily
activities, sport, leisure• Normal work and school• No troublesome symptoms
Scadding, G. Prim Care Respir J. 2010
MildIntermittent
Moderate/Severe
Intermittent
MildPersistent
Moderate/Severe
Persistent
Local Cromone (Mast Cell Stabilizer)
Oral or Local Non-Sedating Antihistamine
Intranasal Decongestant (<10 days) or Oral DecongestantAllergen and Irritant Avoidance
Immunotherapy
Intranasal Corticosteroid
Anti-leukotrienes
Treatment of Allergic Rhinitis

Pharmacologic Options for Allergic Rhinitis
Agent Sneezing Itching Congestion Rhinorrhea Ocular
Oral Antihistamine ++ ++ +/- ++ ++
Nasal Antihistamine + + +/- + –
IntranasalCorticosteroid ++ ++ ++ ++ +OralDecongestant – – + – –
IntranasalDecongestant – – ++ – –
Intranasal Mast Cell Stabilizer + + + + –
Topical Anticholinergic – – – ++ –
Adapted with permission from The AAAAI Allergy Report.
http:// www.aaaai.org/ar/working_vol2/001.asp. Accessed April 8, 2008.
– provides no benefit + provides modest benefit
+/‐ provides minimal benefit ++ provides substantial benefit
"The International Primary Care Respiratory Group, British Society for Allergy and Clinical Immunology, and American Academy of Allergy Asthma and Immunology
recommend initiating therapy with an intranasal corticosteroid alone for mild to moderate disease and using second‐line
therapies for moderate to severe disease”
Am Fam Physician. 2010;81:1440-1446.

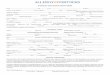
1. Shake bottle
2. Lock down
3. Using RIGHT hand for LEFT
nostril put nozzle just inside
nose aiming towards outside wall
4. Squirt once or twice (2 different directions
5. Change hands and repeat for other side
6. DO NOT SNIFF HARDAdapted scadding OK, Durham SR, Mirakian R. et al. BSACI
guidelines for the management of allergic and non‐allergic rhinitis. Clin Exp Allergy 2008; 38:19‐42
Correct procedure for using a nasal spray
Scadding, G. Prim Care Respir J 2012, 21;122
Allergic Rhinitis
Asthma
Asthma + AR
Approximately 80%of asthmatics have allergic rhinitis
Approximately 40%of allergic rhinitis patients have asthma
Epidemiologic studies have consistently shown that asthma and allergic rhinitis co‐exist in the same patient.
Allergic Rhinitis and Asthma


Summary of the features suggesting a bidirectional link between the upper
and lower airways
Expert Rev . Clin. Immunoll. 6(3), 413-423 (2010)

Physiopathological hypotheses explaining the concept of ‘one airway disease’
Expert Rev . Clin. Immunoll. 6(3), 413-423 (2010)
Reasons for continuing symptoms and poor asthma control
Category
Patient behavioural-related factors
Low/non adherence with therapyIncorrect use of inhaler leading to ineffective/reduceddrug deliverySmoking interfering with steroid treatmentLow patient expectations/aspirations/goals of therapyUnwillingness to use therapy and/or attend medicalconsultationsReliance on complimentary/alternative therapies
Scadding, G. Prim Care Respir J. 2010

Algorithm for the treatment of rhinitis
• Add intranasal corticosteroid (INS)
• Few side effects with good technique – see box
• Onset of action is 6‐8 hours after first dose but maximal effect may not be apparent until after 2 weeks
• Similar efficacy for all INS, systemic absorption negligible with
• mometasone and fluticasone, modest for remainder and high for betamethasone and dexamethasone
• Raised intra‐ocular pressure has been described and patients with
• glaucoma should be monitored more closely
• Fluticasone has UK license for >4 years of age for short term use
Diagnosis by history skin prick test/specific IgEAllergen/irritant avoidance nasal douching
Symptoms
1. Oral/topical non-sedating antihistamines
2. Regular use better than as required use
3. First generation e.g. chlorphenamine cause sedation which can reduce academic and/or non-academic performance and should be avoided.
4. Non-Sedating antihistamines licensed from age 1 year in UK
Treatment failure
Scadding, G. Prim Care Respir J 2010, 21;122
Treatment failure

Waterly rhinorrhoea-add topicalipratropium
1. Check use/compliance, increase dosage where appropriate2. Consider short course oral corticosteroids to gain control for severe nasal blockage or
important events e.g. exams. 3. Always use in conjunction with INS: suggested regime for adults is 0.5mg/kg orally in
the morning with food for 5-10days
Itch/sneeze – addnon-sedating antihistamine
Catarrh – addLeukotriene receptor
Antagonist if asthmatic
Blockage
? Infection/structural problem
Treatment failure
Surgical referralConsider immunotheraphy if symptoms
Predominantly due to one allergen
Add (briefly)• Decongestant• Or oral corticosteroids• Or longer term- long-acting
non-sedating antihistamines tropical azelastine/leukotriene receptor antagonist
Scadding, G. Prim Care Respir J 2010, 21;122
Algorithm for the treatment of rhinitis