Embed Size (px)
Citation preview

Treatments for cancer related fatigue: How can you help
your patients?
Debra Barton RN, PhD, AOCN, FAANMary Lou Willard French Endowed Professor of
Oncology NursingUniversity of Michigan School of Nursing
Ann Arbor, MI

Disclosures
Funding from the National Cancer Institute and the Breast Cancer Research Foundation
Wisconsin ginseng and placebo donated by the Ginseng Board of Wisconsin
©2011 MFMER | 3105994-2

The problem of fatigue
Fatigue can be a prevalent, distressing and persistent effect of cancer diagnosis and treatment (Lawrence, JNCI monographs, 2004)
Descriptive studies report up to 100% of patients experience fatigue at some point during treatment (Hofman M, The Oncologist, 2007; Fulton C, Eur J Cancer, 2000)

Fatigue exists before and after treatment
24% patients severely fatigued before curative intent treatment (GI,BC, PC)
(Goedendorp, BrJCa, 2008)
May not return to baseline and can persist several years after diagnosis (10 yrs)
(Bower, Cancer, 2006; Hjermstad, JCO, 2005; Adams, Current Hem Malig Report, 2007; Johansson, ONF, 2010)

Clinical GuidelinesOrganization-date Effective (highest
evidence)Likely effective (lower level evidence)
Not effective or no evidence
National Comprehensive Cancer Network,updated 2015
Physical activityMassage therapyCBTPsycho-educationalMindfulnessSupportiveexpressive
Does not distinguish other levels of evidence
Lists “considerpsychostimulantsafter ruling out other causes of fatigue” does not put level of evidence
Oncology Nursing Society, updated2014
Exercise-Physicalactivity
Psycho-educationalTreat comorbiditiesCBTRelaxation MeditationStress reductionStructured rehabYogaWisconsin ginseng
Lists erythro stimagents and dex as benefit balance harmOther pharm as “effect not established”

Clinical guidelines continued
©2011 MFMER | 3105994-6
Organization -date
Effective (highest evidence)
Likely effective (lower/some evidence)
Not effective or no evidence
American Society of Clinical Oncology, new, 2014
Physical activityPsycho-educationTreat comorbiditiesCognitive behavioral therapyPsychostimulants-advanced disease, during active treatment
Mindfulness based approaches Yogaacupuncture
Psychostimulantsfor post treatment fatigueMasageMusic therapyRelaxationReikiQigongginseng
Pan-Canadian Group, updated2015
Physical activityCBTGeneral education-energy conservation
Psycho-education Pharmacologicacupuncture

Pharmacologic Treatment
Role of pharmacologic treatment is primarily for managing diagnosed comorbidities:
painhypothyroidismanemiacardiac and pulmonary issues

Psychostimulants – just a word Psychostimulants MPH – Bulk of RCT’s negative (Moraska, JCO,
2010; Mar Fan, Supp Care Ca, 2008; Escalante, JCO, 2012)
Modafanil – 2 RCT negative (Morrow, Cancer, 2010; Fife, JCO, 2013)
Armodafanil – 1 RCT MM is negative (Berenson, Supp Care Cancer, 2015)
©2011 MFMER | 3105994-8

Steroids (Yennurajlingam, 2014)
Dexamethasone 8 mg/day orally and methylprednisolone 32 mg/day orally
Population of advanced cancer (N=132, 40) Over two weeks Improvement in fatigue Latest study (Yennu, 2013) demonstrates
improvement was not mediated by mood, but was a physical improvement
©2011 MFMER | 3105994-9

Fatigue Physiology – What is known Immune system: inflammation
pro-inflammatory cytokinesgenetic polymorphisms
(Bower, JCO, 2013; Bower, JCO, 2011)
Hypothalamic pituitary adrenal system:flattened cortisol slopeblunted cortisol response acute stressdecreased glucocorticoid response
(Bower, Br Beh Imm, 2007; Bower, Psychoneurodendo, 2005; Bower, Psychosomatic Med, 2005)

Mechanistic link Psychostimulants stimulate various
neurotransmitters in the brain to promote wakefulness: histamine (HA), norepinephrine (NE), serotonin (5-HT), dopamine (DA), and orexin systems are likely targets.
Not consistent with what is known about CRF
Steroids are potent anti-inflammatories which is consistent; more research is needed to understand inflammation as a mediator
©2011 MFMER | 3105994-11

Ginseng – Likely effective per ONS and mentioned in ASCO and NCCN
Genus: Panax, Araliaceae family, perennial plant
Used in Traditional Chinese Medicine
Requires 4+ years of growing
Active constituents: ginsenosides

Why Ginseng Inhibits MAPkinase - MCF-7 cells
(King & Murphy, Jrnl Exp Ther and Onc, 2007; Duda, Jrnl Surg Onc, 1999)
Decreased HPA activation and pro-inflammatory cytokines in mice with LPS induced depression
(Kang, Journal of Neuroinflamm, 2011)
Increased aerobic endurance while exercising at 70% Vo2 max
(Wang, Planta Medica, 1998)

SchemaRandomization
Matching Placebo by mouth BID for 8
weeks
Panaxquinquefolius 2,000 mg by mouth BID
for 8 weeks
Ginseng was provided in capsules Both doses taken before noonStandardized to 3% ginsenoside content
(Barton et al, JNCI, 2013)

Eligibility Inclusion Adults with fatigue ≥ 4 for ≥ 1 month, curative
intent Other causes of fatigue ruled out (thyroid,
anemia (hgb >11), pain, insomnia)
Exclusion Chronic systemic steroids, opioids, infections Stop or start anti-cancer therapy Dietary supplements for fatigue

Primary Endpoint
Multidimensional Fatigue Symptom Inventory – Short Form (Stein, 2004)
General Subscale: pooped, worn out, fatigued, sluggish, run down, tired
0 “not at all” to 4 “extremely”

Secondary Endpoints
Side effects
MFSI-SF other subscales and total score
Profile of Mood States: fatigue-inertia

Analysis Change from baseline at 4 weeks, 8 weeks
Two sample, two sided, t-test
150 pts/arm = 90% power, 38% times SD
Stratified by: current treatment, baseline fatigue, days of prior treatment, tumor type

Consort Diagram364 Patients Enrolled
from 40 sites
Placebo 181 patientsGinseng 183 patients
12 cancelled
171 patients started study
133 Completed Treatment per protocol
11 cancelled
170 patients started study
147 available for primary endpoint
analysis
153 available for primary endpoint
analysis
128 Completed Treatment per protocol

Patient DemographicsGinseng N=170
Placebo(N=169)
p value
Age 0.76
Mean (SD) 55.2 (12.7) 55.9 (11.8)
Gender 0.18
Female 138 (81.2%) 127 (75.1%)
Race 0.35
White 154 (90.6%) 156 (92.3%)
Black or African American 10 (5.9%) 8 (4.7%)
Native Hawaiian or Other Pacific Islander 2 (1.2%) 0 (0%)
Asian 1 (0.6%) 3 (1.8%)
American Indian or Alaska Native 1 (0.6%) 2 (1.2%)
Menopausal Status 0.71
Pre 37 (21.8%) 31 (18.3%)
Post/natural-surgical 95 (56%) 89 (53%)
NA (Male) 32 (18.8%) 42 (24.9%)

Disease CharacteristicsGinseng N=170
Placebo(N=169)
p value
Time since current cancer diagnosis 0.84
< 180 days 62 (36.5%) 64 (37.9%)
180 – 360 days 47 (27.6%) 42 (24.9%)
> 360 days 61 (35.9%) 63 (37.3%)
Type of Cancer 0.46
Breast 110 (64.7%) 95 (56.2%)
Colon 20 (11.8%) 17 (10.1%)
Prostate 5 (2.9%) 8 (4.7%)
Hematologic 8 (4.7%) 9 (5.3%)
Gynecologic 5 (2.9%) 7 (4.1%)
Combination/Unknown/Other 22 (12.9%) 33 (19.5%)

Treatment CharacteristicsGinseng N=170
Placebo(N=169)
p value
Current Treatment 0.96
Yes 83 (48.8%) 82 (48.5%)
Duration of all prior cancer treatment 0.99
≥180 days 87 (51.2%) 86 (50.9%)
Current Endocrine Therapy 0.49
Tamoxifen 23 (13.5%) 22 (13.0%)
Aromatase Inhibitor 27 (15.9%) 32 (18.9%)
Anti-androgen 2 (1.2%) 5 (3.0%)
Other 7 (4.1%) 3 (1.8%)
None 111 (65.3%) 107 (63.3%)

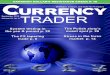
MFSI Mean Change from Baseline at 4 and 8 weeks0-100, higher is better
GinsengN=170
PlaceboN=169
MFSI-general 4 weeks 14.4 (27.1) 8.2 (24.8)8 weeks 20.0 (27.0) 10.3 (26.1)
0
10
20
30
40
50
4 wks 8 wks
GinsengPlacebo
p=.07 p=.003
MFS
I-SF
gene
ral s
ubsc
ale
(Barton, JNCI, 2013)

MFSI Mean Change from Baseline at 4 and 8 weeks0-100, higher is better Ginseng (S.D.)
N=170Placebo (S.D.)N=169
p-value
MFSI-physical 4 weeks 1.6 (15.9) -0.4 (14.7) 0.39
8 weeks 3.0 (17.9) -1.7 (18.2) 0.004
MFSI-Mental 4 weeks 2.0 (15.2) 0.6 (16.1) 0.41
8 weeks 2.8 (16.5) 3.4 (15.2) 0.80
MFSI-Emotional 4 weeks 0.5 (16.1) 0.5 (16.7) 0.99
8 weeks 3.0 (17.4) 2.3 (17.4) 0.68
MFSI-Vigor 4 weeks 1.8 (19.0) 0.4 (15.5) 0.70
8 weeks 4.6 (20.5) 2.5 (17.6) 0.71
MFSI-Total Score 4 weeks 4.1 (13.4) 2.1 (12.9) 0.21
8 weeks 6.7 (14.0) 3.7 (14.6) 0.02

P=.08
P=.008
0
10
20
30
40
50
Fatigue/Inertia 4 wks Fatigue/Inertia 8 wks
GinsengPlacebo
Other Fatigue EndpointsChange from baseline, 0-100, higher is better

Subgroups Fatigue Endpoints Change from Baseline 4 & 8 Weeks (0-100)
P=0.02
P=0.01
P=0.86
P=0.07
0
5
10
15
20
25
30
35
40
45
50
MFSISF General 4 weeks MFSISF General 8 weeks
Ginseng Ca TxPlacebo Ca TxGinseng Post TxPlacebo Post Tx
0
(Barton, JNCI, 2013)

Patient Reported Side Effects at 4 and 8 Weeks, 0-100
-50
-40
-30
-20
-10
0
10
20
30
40
50
Nau
sea
4 w
ks
Nau
sea
8 w
ks
Vom
iting
4 w
ks
Vom
ting
8 w
ks
Loos
e S
tool
4 w
ks
Loos
e S
tool
8 w
ks
Trou
ble
Sle
epin
g 4
wks
Trou
ble
Sle
epin
g 8
wks
Anx
ious
4 w
ks
Anx
ious
8 w
ks
Ner
vous
ness
4 w
ks
Ner
vous
ness
8 w
ks
GinsengPlacebo

What we learned Wisconsin ginseng has activity against cancer
related fatigue Demonstrated more consistently and earlier in
patients receiving treatment for cancer Wisconsin ginseng is not associated with
discernible toxicity Physical fatigue is improved No evidence of improvement in cognitive or
emotional elements Attention to potency

Physical Activity - Exercise Numerous meta-analyses over 4,000 patients
(60-ish studies) Effect size moderate at best .28-.45 Various types of cancer, aerobic and resistance,
during and after treatment Dose not evaluated but most studies over 12
weeks, 3 times per week, 45 minutes each session
(McMillan, Appl Physiol Nutr Metab, 2011; Tomlinson, American J Phys Med Rehab, 2014; Brown, Ca Epid Biomarkers Prev, 2011)
©2011 MFMER | 3105994-29

How can providers help? (Park, Cancer, 2015)
RCT to evaluate impact of oncologists’ recommendations for exercise over 4 wks1: Recommendation alone 2: Recommendation with exercise pkg3: Usual care control
162 early stage breast and colorectal pts. Outcome: AMOUNT of exercise Control -39 min/wk; REC 0.99 min/wk; REC +
PKG 48 min/wk
©2011 MFMER | 3105994-30

Physical Activity Prescription What is your patient doing regularly right now? Plan activity of choice and implementation plan
(when, where and motivators) Aim for 3 to 4 times per week 30 to 45 minutes
each Tailor for those already active versus those not
at all active BABY steps, overwhelming goals are not
achievable
©2011 MFMER | 3105994-31

Psycho-education Psycho-education: what is fatigue,
strategies to manage, usually included energy conservation (Barsevick, 2004)
What: Deliberate, planned management of personal energy to prevent depletion
How: priority setting, scheduling activities around energy peaks, scheduling rest periods, pacing
©2011 MFMER | 3105994-32

Energy Conservation Activity Management(Barsevick, Cancer, 2004)
N=396 Energy conservation and activity management (ECAM) vs healthy diet education
Various cancers, 28% stage ¾ receiving tx
3 phone calls, centrally administered with homework total of 75 minutes
Fatigue measures: POMS, Schwartz Cancer Fatigue Scale, General Fatigue Scale (investigator developed)

Findings ECAM group used more energy conservation
strategies (uptake) All three fatigue measures demonstrated
significantly lower fatigue in the ECAM group using intent to treat analyses
No difference in functional status but did find less disruption in usual activities
Replicated by Ream JPSM, 2006 – N=103 heterogeneous pop, 58% getting palliation, main difference usual care control and did not measure uptake

Cognitive Behavioral therapy Most studies have a kitchen sink approach Components include relaxation and stress and
sleep management, cognitive restructuring Many options: meditation, mindfulness, yoga,
progressive muscle relaxation, imagery Studies without PA or energy conservation
were not really positive
(Armes, Cancer, 2007; Brown, AJCO, 2006; Gaston-Johansson,Ca Nrsg, 2000; Kwekkeboom, JPSM, 2012)
©2011 MFMER | 3105994-35

Summary Lack of clear physiology hampers discovery of
effective interventions – For many strategies the “jury is still out”
For advanced patients, a short trial of a steroid is reasonable
Physical activity discussions and planning are needed
Principles of energy conservation are helpful
American ginseng may be a reasonable thing to try
©2011 MFMER | 3105994-36

Merci Beaucoup