Embed Size (px)
Citation preview

1
Juven-Wetzler, A., Fostick, L., Cwikel-Hamzany, S., Balaban, E., Zohar, J. (accepted,
2014). Treatment with Ziprasidone for Schizophrenia Patients with OCD. European
Neuropsychopharmacology.
***This is a self-archiving copy and does not fully replicate the published version***
Treatment with Ziprasidone for Schizophrenia Patients with OCD
Alzbeta Juven-Wetzler,1 Leah Fostick,
2 Shlomit Cwikel-Hamzany,
1 Evgenya
Balaban,1 and Joseph Zohar
1
1 Department of Psychiatry, Chaim Sheba Medical Center, Tel Hashomer, Israel
2 Department of Communication Disorders, Ariel University, Ariel, Israel
Corresponding author: Joseph Zohar, Department of Psychiatry, Chaim Sheba
Medical Center, Tel Hashomer, Israel 52621 [email protected]
Phone: +972 3 5303300 Fax: +972 3 5352788

2
Abstract
Comorbidity of obsessive-compulsive disorder (OCD) has been observed in about
15% of schizophrenic patients and has been associated with poor prognosis.
Therefore, there is a need for specific treatment options for these patients (schizo-
obsessive, ScOCD).
This is an open, prospective study, aiming to test the efficacy of Ziprasidone (80 to
200 mg/d) in ScOCD patients and comparing the response to the treatment between
stable schizophrenic (N=16) and stable ScOCD (N=29) patients.
Treatment effect with Ziprasidone was different in schizophrenic patients when
stratified based on OCD comorbidity. Overall, the effect on OCD symptoms (as
measured by the Yale Brown Obsessive Compulsive Scale, YBOCS) was found to be
bimodal—either no response or exacerbation (for 45% of the patients, n=13) or
significant improvement of symptoms (55%, n=16). Those who improved in OCD
symptoms, improved also in negative and general schizophrenia symptoms, wthe
ScOCD- unimproved group worsened in all symptoms. Whereas schizophrenic
patients without OCD responded in a modest Gausian distribution, they improved in
schizophrenia negative symptoms and in general anxiety.
This data suggests that schizo-obsessive disorder is a distinct and complex condition
with more than one underlying pathogenesis. Definition of these ScOCD subgroups
defined by their response to Ziprasidone might contribute to personalized medicine
within the OCD-schizophrenia spectrum. Moreover, this finding suggests that ScOCD
might be considered as a special schizophrenic subtype and their inclusion in

3
schizophrenia treatment studies need to be further explored due to their divergent
response.
Keywords: schizophrenia, OCD, Ziprasidone, personalized medicine.
4
Introduction
Schizophrenia and obsessive-compulsive disorder (OCD) are distinct diagnostic
entities with a high co-occurrence. Reports from epidemiological studies suggest
considerably higher-than-expected co-morbidity rates. The prevalence of clinically-
significant obsessive compulsive symptoms (OCS) in patients with schizophrenia
ranging between 10% and 59% (Fabisch et al., 2001; Bland, Newman, & Orn, 1987;
Berman, Kalinowski, Berman, Lengua, & Green, 1995; Lysaker et al., 2000; Porto et
al., 1997) and between 7.8% and 29% of the schizophrenia population who meet the
DSM-IV criteria for OCD (Porto et al., 1997; Eisen et al., 1997; Bermanzohn et al.,
2000; Tibbo et al., 2000; Poyurovsky et al., 2001). This high prevalence rate does not
appears to be the consequence result of neither chronic disease or treatment, as a
similar prevalence of OCD (14%) was found amongst untreated schizophrenic
patients during their first psychotic episode (Poyurovsky, Fuchs, & Weizman, 1999).
Moreover, OCD comorbidity also appears to be a predictor for a poor prognosis
(Berman et al., 1995; Lysaker et al., 2000; Fenton & McGlashan, 1986; Hwang,
Morgan, & Losconzcy, 2000; Ohta, Kokai, & Morita, 2003) and significant
neuropsychological impairments (Lysaker et al., 2000; Hwang, Morgan, &
Losconzcy, 2000; Berman et al., 1998; Lysaker et al., 2002; Whitney et al., 2004;
Patel et al., 2010).
Currently there are only few studies that address pharmacological options for the
treatment of patients with schizophrenia and OCD (schizo-obsessive, ScOCD)
(Poyurovsky et al., 2012). The commonly-accepted treatment approach is to use a
combination of neuroleptics with anti-obsessive medications (Zohar, Kaplan, &
Benjamin, 1993; Reznik & Sirota, 2000; Berman, Sapers, & Chang et al., 1995;

5
Poyurovsky et al., 1999). However, the outcome is rather disappointing (Poyurovsky
& Koran, 2005). Indeed, a therapeutic lacuna for this subset of patients is
consensually acknowledged (Zohar, 1997). To the best of our knowledge, this is the
first study to compare the effects of a given medication (Ziprasidone in this case)
between schizophrenic patients with and without OCD.
The mixed dopaminergic-serotoninergic antipsychotics – known as second
generation, or atypical, antipsychotics (SGA) – are theoretically ideally suited to
ScOCD patients because of their affinity to both the dopaminergic and the
serotoninergic systems. (Hwank et al., 2009). However, several studies have reported
opposite results, namely, an exacerbation of OCS following treatment with Clozapine
(Baker et al., 1992; Reznik et al., 2004), Olanzapine (de Haan et al., 2002; Lykouras
et al., 2000), and Risperidone (Alevizos et al., 2002), while others report contradictory
findings ( Poyurovsky et al., 2000; Veznedaroglu et al., 2003; Baker et al., 1996).
Similarly, there are paradoxical results for Quetiapine as well (Tranulis et al., 2005).
The antipsychotic medication Ziprasidone is a potent antagonist at 5-HT2A and D2
receptors with a high 5-HT2A/D2 affinity ratio. It is also a 5HTT reuptakte inhibitor
that exhibits potent interaction with 5-HT1A, 5-HT1D, and 5-HT2C receptor subtypes
(Stahl et al., 2003). Clinical trials suggest that this drug is effective in treating both
positive and negative symptoms of schizophrenia and schizoaffective disorders, and
also proving efficacious in the treatment of affective symptoms in schizoaffective
patients (Weiden et al., 2003; Gunasekara et al., 2002; Simpson et al., 2004). Given
Ziprasidone's unique pharmacological properties in comparison with other SGAs with
respect to 5HT1D and the latter’s potential role in the treatment of obsessive
compulsive symptoms (Zohar et al., 2004), Ziprasidone appears to constitute a
6
promising treatment option for ScOCD patients. We therefor initiated a study of
Ziprasidone in this population subset.
The aim of the current study was to test the effect of Ziprasidone on ScOCD
patients, employing the Yale-Brown Obsessive Compulsive Scale (YBOCS) and
Positive and Negative Syndrome Scale (PANSS). In order to evaluate this effect, we
also compared treatment response between ScOCD and schizophrenic patients
without OC symptoms.

7
Methods
Participants
The study population consisted of 45 in- and out-patients receiving treatment at the
Psychiatry Department at Chaim Sheba Medical Center who met the DSM-IV criteria
for schizophrenia. Only adults (ages 18-65) who had been diagnosed at least 6 months
previously and who have been stable on their antipsychotic medication for at least two
months, scoring a minimum of 60 on the PANSS, were admitted to the study. Patients
already receiving Ziprasidone, those diagnosed as suffering from a schizophreniform
disorder, organic brain syndrome, mental retardation and/or pervasive developmental
disorder, who exhibited a recent history of substance abuse or dependence, or suffered
from any significant cardiovascular illness were excluded from the study. Of those
admitted, 29 had concurrent OCD with a minimal score of 14 on the YBOCS
(referred to herein as the “ScOCD group”) and 16 non-OCD schizophrenia (referred
to herein as the “Sc group”). Of the ScOCD group, 18 patients (62%) had OCD before
schizophrenia, and 11 (38%) had schizophrenia before OCD (see Table 1). The study
was approved by the Institutional Review Board of Sheba Medical Center. All the
subjects gave their written informed consent after being given a full explanation of the
study’s protocol.
Table 1 presents the demographic and clinical characteristics of the participants
during their baseline assessment.
Table 1

8
Study design
This study was open, prospective with a parallel group design, comparing response to
treatment with Ziprasidone in patients with schizophrenia (Sc) (N=16) to patients with
schizophrenia and OCD (ScOCD) (N=29). The participants underwent an initial
screening evaluation based upon a medical and psychiatric assessment and completion
of a demographic data questionnaire. The Structured Clinical Interview for DSM IV
(SCID) was used for the diagnosis of schizophrenia and OCD during the initial
baseline evaluation visit. Ratings included the Positive and Negative Syndrome Scale
(PANSS), the Yale-Brown Obsessive Compulsive Scale (YBOCS), the Clinical
Global Impressions—Severity of Illness (CGI-S) and Clinical Global Impressions—
Improvement (CGI-I) scales, and the Global Assessment of Functioning (GAF) scale.
Patients with YBOCS rates ≥ 14 at the baseline visit were classified as ScOCD.
After a full evaluation, the patients were down-titrated from their current
antipsychotic medication (Risperidone [N=18], Olanzapine [N=14], Quetiapine [N=
4], Zuclopenthixol [N=3], Perphenazine [N=2], Clozapine [N=2], Ridazine [N=1],
Penfluridol [N=1]), and Ziprasidone was increased gradually until reaching the dose
of 80-200 mg/day according to clinical considerations. Other concomitant
medications, like SRI (fluoxetine, citalopram, and paroxetine), benzodiazepines
(haloperidol), and non-benzodiazepines anxiolytics (risperidal), were continued. Each
patient was monitored using to the above ratings at baseline and at the end of weeks 2,
5, and 8.
Statistical analysis
Baseline characteristics were analyzed using chi-square test for categorical variables
and Multivariate analysis of variance (MANOVA) for continuous variables. In the

9
first analysis, we measured the effect of Ziprasidone on ScOCD using one-way
repeated-measures ANOVA, week of treatment serving as a within-subject variable.
This analysis was carried out separately on the PANSS, YBOCS, CGI, and GAF
scores. Due to bimodality in their YBOCS scores, the ScOCD participants were
divided into two subgroups—ScOCD-improved (change of 25% and above) and
ScOCD-unimproved. The YBOCS divergence between these subgroups was tested
using two-way repeated- measures ANOVA, week of treatment serving as a within-
subject variable and the ScOCD sub-group as a between-subjects variable.
The second analysis included comparison of the PANSS, YBOCS, CGI, and GAF
scores between the ScOCD and Sc groups, using two-way repeated measures
ANOVA with week of treatment as a within-subject variable and ScOCD sub-group
as a between-subjects variable. All PANSS analyses were carried out using
multivariate repeated measures ANOVA for including PANSS subscales.

10
Results
1. Ziprasidone effect on ScOCD
A significant effect of Ziprasidone was found on the YBOCS scores (F(3,84)=4.42,
p<.01). However, no effect was found on any PANSS subscales (F(9,252)=.74, p>.05),
CGI-S (F(3,84)=.78, p>.05), CGI-I (F(2,56)=1.09, p>.05), or GAF (F(3,84)=.64, p>.05).
Close examination of the data revealed that the percentage of improvement from week
0 to week 8 in YBOCS was characterized by a bimodal distribution (Skewness = 0.05,
Kurtosis = -0.57) (Figure 1), whilst the other scales demonstrating Gaussian
distributions. Based on this analysis, ScOCD participants were subdivided into two
subgroups: ScOCD patients with 25% or more YBOCS improvement (referred to
herein as “ScOCD-improved”) and ScOCD patients with no response or symptom
exacerbation (referred to herein as “ScOCD-unimproved”). Table 1 presents the
demographic and clinical characteristics for these sub-groups during their baseline
assessment. At baseline, the ScOCD-improved had higher PANSS positive and total
scores and rated more severe on the CGI-severity.
Figure 1
Table 2 presents the results for the effect of week of treatment, ScOCD subgroups,
and week of treatment X ScOCD subgroups interaction for the study measures. While
the results indicate a significant effect for week of treatment and ScOCD subgroups
with respect to CGI-I, significant week of treatment X ScOCD subgroup was found
for all the measures (Table 2 and Figures 2-5).
Table 2

11
Figures 2-5
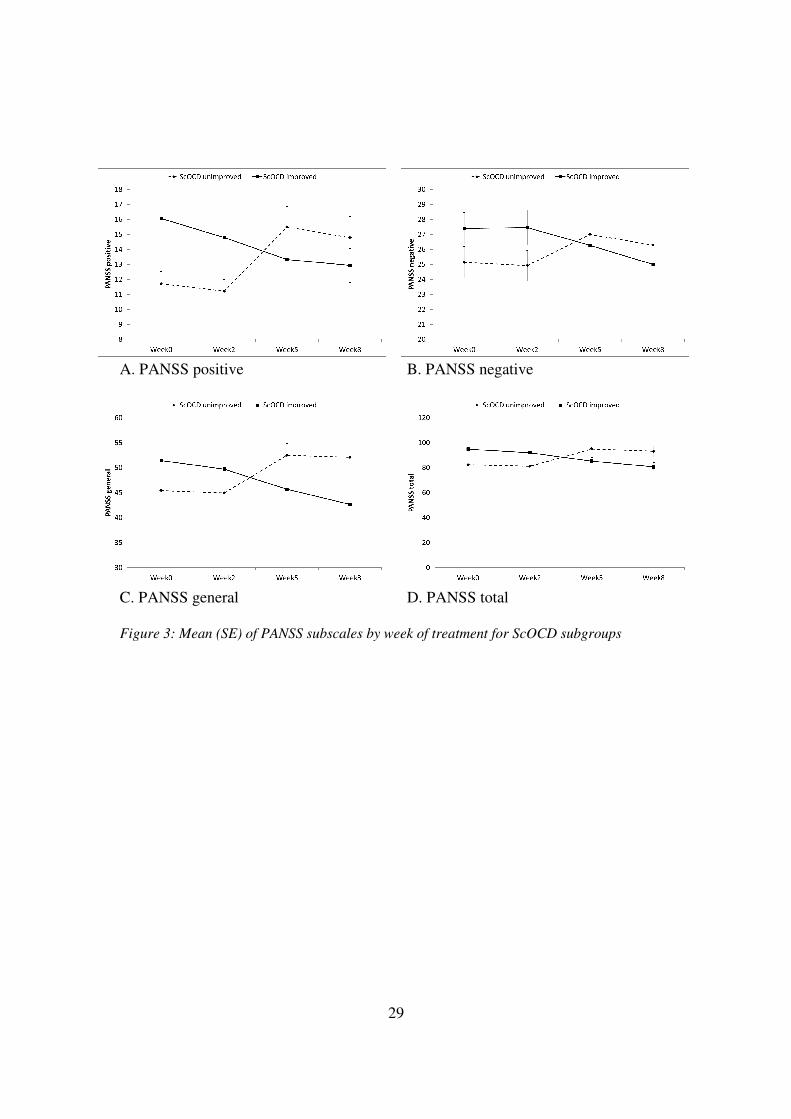
A separate post hoc repeated-measures ANOVA for each group demonstrated
significant improvement for the ScOCD-improved group in all the measures, with the
exception of PANSS positive (YBOCS: F[3,42] = 38.31, p<.001; PANSS positive:
F[3,42] = 1.93, p>.05; PANSS negative: F[3,42] = 6.05, p<.01; PANSS general: F[3,42] =
7.91, p<.01; PANSS total F[3,42] = 6.5, p<.05; CGI-S: F[3,42] = 3.82, p<.05; CGI-I :
F[2,26] = 4.12, p<.05; GAF: F[3,42] = 4.44, p<.05) and significant worsening in the
ScOCD-unimproved group on all the measures and a marginal decline on the PANSS
positive and GAF scores (YBOCS: F[3,39] = 4.71, p<.05; PANSS positive: F[3,39] =
4.00, p<.06; PANSS negative: F[3,39] = 4.28, p<.05; PANSS general: F[3,39] = 4.81,
p<.05; PANSS total: F[3,39] = 4.93, p<.05; CGI-S: F[3,39] = 6.45, p<.05; CGI-I:
F(2,28)=5.87, p<.01; GAF: F[3,39] = 3.83, p<.07).
2. Ziprasidone effect on ScOCD vs. schizophrenia patients
Table 3 presents the ScOCD and Sc scores on study measures by week of treatment.
Sc patients responded to Ziprasidone significantly better than ScOCD patients, as
measured by PANSS general and total scores (F[1,43] = 14.673, p<.001 and F[1,43] =
5.329, p<.05, respectively) and marginally better on the CGI-S scale (F[1,43] = 3.686,
p<.06). An overall decrease in the PANSS negative score occurred during the period
of the study (F[3,129] = 5.453, p<.01), with an interaction of week of treatment X group
(F[3,129] = 4.528, p<.01).
Discussion
Schizophrenic patients response to treatment with Ziprasidone was different when
stratified based on comorbidity to OCD. The effect of Ziprasidone upon schizo-
12
obsessive patients (as measured by Y-BOCS) was bimodal—approximately half
demonstrating a clinical improvement (at least 25%, Koran et al., 2002; Koran and
Simpson, 2013) and the other half no response or an exacerbation of their symptoms
in particular. This biomodel response is in line with previous work which suggest a
complex and at times opposite response to D2 activation (respond to both D2
antagonist and dopamine release) (Koran et al., 2002). It highlight the heterogeneous
response to Ziprasidone in Schizophrenic patients in general and for ScOCD patients
in particular, and emphasize the need for a personalized approach.
With respect to the ScOCD-unimproved group, the results are commensurate with
the lack of effect or even exacerbation of OCD in some ScOCD patients (Baker et al.,
1992; de Haan et al., 2002; Lykouras et al., 2000; Alevizos et al., 2002). Indeed other
studies also indicating the response to treatment—especially with “atypical”
antipsychotics (D2/5HT2 antagonists)—to be bi-directional (Hwank et al., 2009;
Reznik et al., 2004; Poyurovsky et al., 2000; Veznedaroglu et al., 2003; Baker et al.,
1996; Tranulis et al., 2005). These results suggest that schizo-obsessive disorder is a
complex condition with more than one underlying pathogenesis.
One of the limitations of this study is its small and unequal sample size—in
particular the schizophrenia without OCD group. The criteria for admission including
at least two months’ stability on medication and schizo-obsessive patients frequently
being treatment resistant and exhibiting severe residual symptoms (Berman et al.,
1995; Fenton & McGlashan, 1986; Hwang, Morgan, & Losconzcy, 2000), more of
these patients were referred than schizophrenia patients without OCD.
Another limitation is the relatively short follow up period, as late onset treatment
response in OCD patients is quite common (Bandelow et al., 2008). While eight
weeks might not be sufficient to achieve a maximal response in the OC component,

13
an evident response difference was observed between the two schizo-obsessive
subgroups under identical conditions (same rating scales, rater [AJ-W], and time
framework).
Patients enrolling in the study having been stable on antipsychotic medication for
at least two months prior to entering the study, they lay largely at their baseline. This
partially explains the relatively low PANNS positive scores at the beginning of the
study and the relatively minor response to the Ziprasidone treatment.
Open studies are vulnerable to obvious limitations—including potentially biased
ratings and placebo effects. The bimodal and opposite response—clear responders vs.
clear exacerbators—in the schizo-obsessive group appears to suggest that no set bias
existed, the rated response not being unidirectional.
While the unequal number of ScOCD (N=29) vs. schizophrenia (N=16) patients
may have created a statistical imbalance, the study participants were in fact divided
into three (Sc, ScOCD-improved, and ScOCD-unimproved) rather than two groups
(Sc and ScOCD), each having roughly equal numbers. Thus, despite the small
number, the statistically-significant therapeutic differences between the groups
indicate the findings’ clinical significance.
The inequality in terms of gender between the ScOCD (15 females and 14 males)
and schizophrenia (15 females and 1 male) groups might hamper the interpretation of
those results (Table 1). When the analysis was repeated with females only, the same
results emerged. In future studies, close attention should be given to gender.
This study—in which one patient was helped by the drug and another was not—
further demonstrates the need for stratified medicine in psychiatry. While
characterizing subgroups and hence enhancing prediction of treatment response to
Ziprasidone in the schizo-obsessive population would be of great clinical importance,

14
this study demonstrated no significant differences between these two subgroups with
respect to age, marital status, gender, age of onset, duration of OCD or schizophrenia,
family history, or type of symptom. Nevertheless, recognizing the differential
response to the same intervention (Ziprasidone in this study) might be a step towards
delineation of specific subgroups within the OCD-schizophrenia axis. If other
endophenotypic markers for these subgroups will be found, it might pave the way to
the hypothesis about specific subgroups within the ScOCD range (Hwank et al., 2009;
Baker et al., 1992; Reznik et al., 2004; de Haan et al., 2002; Lykouras et al., 2000;
Alevizos et al., 2002; Poyurovsky et al., 2000; Veznedaroglu et al., 2003; Baker et al.,
1996; Tranulis et al., 2005).
Recent clinical and biological findings have provided better insight into the schizo-
obsessive phenomenon (Patel et al., 2010, Pallanti et al., 2009, Hwang et al., 2000).
As schizo-obsessive patients continue to challenge clinicians, the currently-available
evidence calls for comprehensive clinical and neuropsychological assessment—as
well as personalized pharmacological interventions. The administration of
Ziprasidone was particularly helpful and leading to an improvement in all the clinical
measures amongst approximately half of the schizo-obsessive patients in our study.
Hence this study suggests that Ziprasidone is a therapeutic option to be considered in
those patients
While schizophrenia and obsessive-compulsive disorder are separate nosological
entities with discrete underlying brain mechanisms, clinical presentations, and
treatments, they appear to co-exist in a greater proportion of patients than might be
expected (Fabisch et al., 2001; Bland, Newman, & Orn, 1987; Berman, Kalinowski,
Berman, Lengua, & Green, 1995; Lysaker et al., 2000; Porto et al., 1997 Eisen et al.,
1997; Bermanzohn et al., 2000; Tibbo et al., 2000; Poyurovsky et al., 2001;

15
Poyurovsky, Fuchs, & Weizman, 1999). Schizo-obsessive patients exhibit distinct
clinical features and a different pattern of co-morbidity than schizophrenia patients
(Berman et al., 1995; Lysaker et al., 2000; Fenton & McGlashan, 1986; Hwang,
Morgan, & Losconzcy, 2000; Ohta, Kokai, & Morita, 2003; Berman et al., 1998;
Lysaker et al., 2002; Whitney et al., 2004; Patel et al., 2010; Patel et al., 2010).
Preliminary reports are also suggesting a distinct neuro-anatomical profile (Aoyama et
al., 2000). Several studies have found that schizo-obsessive patients exhibit more soft
neurological signs and neurocognitive deficits (Patel et al., 2010; Pallanti et al., 2009),
indicating that obsessive-compulsive symptoms represent a clinically meaningful
dimension of psychopathology in schizophrenia, with distinct clinical and
neurobiological characteristics. Growing evidence thus points towards the existence
of a schizo-obsessive subtype of schizophrenia (Poyurovsky et al., 2012).
The traditional methods employed by studies do not emphasize individual
variations in responses to treatment. This study suggests the need for stratified
medicine in psychiatry—specifically, the paying of particular attention to schizo-
obsessive patients in order to ensure better treatment targeting. In the light of
“individualized medicine” and in order to prevent any “blurring” of results, the
exclusion of this subset of schizophrenia patients (ScOCD) from studies on the effect
of “antipsychotic” drugs in schizophrenia should be reevaluated.
Conclusion
From the therapeutic perspective and in line with the promotion of personalized
medicine, this open prospective pilot study suggests that ScOCD patients respond
differently to Ziprasidone. As approximately half of them finding the intervention

16
particularly beneficial, it indicates that Ziprasidone trial constitutes a reasonable
therapeutic option for such patients.
Theoretically, the biphasic distribution of response to Ziprasidone—clear
responders versus exacerbators—together with earlier reports of exacerbation or de
novo surfacing of OC symptoms following the administration of Clozapine and/or
other D2/5HT2 antagonists suggests a divergent underlying pathology. Following up
this lead may uncover a hidden endophenotype door.
From a methodological point of view, the different response of ScOC (as compared
to Sc without OCD) suggests that including ScOC patients in treatment studies has a
potential to blur the signal as those patients respond differently to D2/5HT2
antagonist as compared to schizophrenic patients without OCD.
The conceptual framework of this study was to focus on symptoms (OCD) rather
than syndrome (schizophrenia) accordingly, tested the response along the domains of
compulsivity, negative symptoms etc. this approach is in line with the Research
Domain Criteria (RDoC), which suggest examining domain across different diagnosis
("horizontal" vs. "vertical" approach). Indeed, the main finding of this study is that
compulsivity as a domain should be taken into account both in the clinical level and
the drug design study as it affected the outcome of drug intervention.

17
References
Alevizos, B., Lykouras, L., Zarvas, I.M., Christodoulou, G.N., 2002. Risperidone-
induced obsessive-compulsive symptoms: a series of six cases. J Clin
Psychopharmacol 22 461-67.
Aoyama, F., Iida, J., Inoue, M., Iwasaka, H., Sakiyama, S., Hata, K., Kishimoto, T.,
2000. Brain imaging in childhood-and-adolescence-onset schizophrenia associated
with obsessive-compulsive symptoms. Acta Psychiatr Scand 102 32-7.
Baker, R.W., Ames, D., Umbricht, D.S., Chengappa, K.N., Schooler, N.R., 1996.
Obsessive-compulsive symptoms in schizophrenia: A comparison of olanzapine
and placebo. Psychopharmacol Bull 32 (1) 89-93.
Baker, R.W., Chengappa, K.N., Baird, J.W., Steingard, S., Christ, M.A., Schooler,
N.R., 1992. Emergence of obsessive compulsive symptoms during treatment with
clozapine. J Clin Psychiatry 53 439-42.
Bandelow, B., Zohar, J., Hollander, E., Kasper, S., Moller, H.J., 2008. World
Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for the
Pharmacological Treatment of Anxiety, Obsessive-Compulsive and Post-
Traumatic Stress Disorders-First Revision. World J Biol Psychiatry 9 (4) 248-312.
Berman, I., Kalinowski, A., Berman, S.M., Lengua, J., Green, A.I., 1995. Obsessive
and compulsive symptoms in chronic schizophrenia. Compr Psychiatry 36 6-10.
Berman, I., Merson, A., Viegner, B., Losonczy, M.F., Pappas, D., Green, A.I., 1998.
Obsessions and compulsions as a distinct cluster of symptoms in schizophrenia: A
neuropsychological study. J Nerv Ment Dis 186 150-156.
Berman, I., Sapers, B.L., Chang, H.H., Losonczy, M.F., Schmildler, J., Green, A.I.,
1995. Treatment of obsessive-compulsive symptoms in schizophrenic patients with
clomipramine. J Clin Psychopharmacol 15 206-10.

18
Bermanzohn, P.C., Porto, L., Arlow, B.P., Pollack, S., Stronger, R., Siris, S.G., 2000.
Hierarchical diagnosis in chronic schizophrenia: A clinical study of co-occurring
syndroms. Schizophr Bull 26 517-25.
Bland, R.C., Newman, S.C., Orn, H., 1987. Schizophrenia: Lifetime co-morbidity in a
community sample. Acta Psychiatr Scand 75 383-91.
Eisen, J.L., Beer, D.A., Pato, M.T., Venditto, T.A., Rasmussen, S.A., 1997. Obsessive
compulsive disorder in patients with schizophrenia or schizoaffective disorder. Am
J Psychiatry 154 271-273.
Fabisch, K., Fabisch, H., Langs, G., Huber, H.P., Zapotoczky, H.G., 2001. Incidence
of obsessive-compulsive phenomena in the course of acute schizophrenia and
schizoaffective disorder. Eur Psychiatry 16 336-341.
Fenton, W.S., McGlashan, T.H., 1986. The prognostic significance of obsessive-
compulsive symptoms in schizophrenia. Am J Psychiatry 143 437-41.
Gunasekara, N.S., Spencer, C.M., Keating, G.M., 2002. Ziprasidone: A review of its
use in schizophrenia and schizoaffective disorder. Drugs 62 1217-51.
Haan, L. de, Beuk, N., Hoogenboom, B., Dingemans, P., Linszen, D., 2002.
Obsessive-compulsive symptoms during treatment with olanzapine and risperidon:
A prospective study of 113 patients with recent-onset schizophrenia or related
disorders. J Clin Psychiatry 63 104-7.
Hwang, M.Y., Morgan, J.E., Losconzcy, M.F., 2000. Clinical and neuropsychological
profiles of obsessive-compulsive schizophrenia: A pilot study. J Neuropsychiatry
Clin Neurosci 12 91-4.
Hwank, M.Y., Kim, S.W., Yum, S.Y., Opler, L.A., 2009. Management of
schizophrenia with obsessive-compulsive features. Psychiatr Clin North Am 32 (4)
835-51.

19
Koran, L. M., Hackett, E., Rubin, A., Wolkow, R., Robinson, D., 2002. Efficacy of
Sertraline in the Long-Term Treatment of Obsessive-Compulsive Disorder. Am J
Psychiatry 159 88–95.
Koran, L. M., Simpson, H. B., 2013. Guideline Watch (March 2013): Practice
Guideline for the Treatment of Patients With Obsessive-Compulsive Disorder.
APA Practice Guidelines 1-22.
Lykouras, L., Zervas, I.M., Gournellis, R., Malliori, M., Rabavilas, A., 2000.
Olanzapine and obsessive-compulsive symptoms. Eur Neuropsychopharmacol 10
385-387.
Lysaker, P.H., Bryson, G.J., Marks, K.A., Greig, T.C., Bell, M.D., 2002. Association
of obsessions and compulsions in schizophrenia with neurocognition and negative
symptoms. J Neuropsychiatry Clin Neurosci 14 (4) 449-53.
Lysaker, P.H., Marks, K.A., Picone, J.B., Rollins, A.L., Fastenau, P.S., Bond, G.R.,
2000. Obsessive and compulsive symptoms in schizophrenia: Clinical and
neurocognitive correlates. J Nerv Ment Dis 188 78-83.
Ohta, M., Kokai, M., Morita, Y., 2003. Features of obsessive compulsive disorder in
patients primarily diagnosed with schizophrenia. Psychiatry Clin Neurosci 57 67-
74.
Pallanti, S., Castellini, G., Chamberlain, S.R., Quercioli, L., Zaccara, G., Fineberg,
N.A., 2009. Cognitive event-related potentials differentiate schizophrenia with
obsessive-compulsive disorder (schizo-OCD) from OCD and schizophrenia
without OC symptoms. Psychiatry Res 170 52-60.
Patel, D.D.,Whitney, K.A., Laws, K.R., Padhi, A., Farrow, J.M., Mukhopadhaya, K.,
Krishnaiah, R., Fineberg, N.A., 2010. The neuropsychology of the schizo-
obsessive subtype of schizophrenia: A new analysis. Psychol Med 40 921-33.

20
Porto, I., Bermanzohn, P.C., Pollack, S., Morrissey, R., Siris, S.G., 1997. A profile of
obsessive compulsive symptoms in schizophrenia. CNS Spectrums 2 21-25.
Poyurovsky, M., Dorfman-Etrog, P., Hermesh, H., Munitz, H., Tollefson, G.D.,
Weizman, A., 2000. Beneficial effect of olanzapine in schizophrenic patients with
obsessive-compulsive symptoms. Int Clin Psychopharmacol 15 169-73.
Poyurovsky, M., Fuchs, K., Weizman, A., 1999. Obsessive-compulsive symptoms in
patients with first episode schizophrenia. Am J Psychiatry 156 1998-2000.
Poyurovsky, M., Hramenkov, S., Isakov, V., Rauchverger, B., Modai, I., Schneidman,
M., Fuchs, C., Weizman, A., 2001. Obsessive-compulsive disorder in hospitalized
patients with chronic schizophrenia. Psychiatry Res 102 49-57.
Poyurovsky, M., Isakov, V., Hromnikov, S., Modai, I., Rauchberger, B., Schneidman,
M., Weizman, A., 1999. Fluvoxamine treatment of obsessive-compulsive
symptoms in schizophrenic patients: An add-on open study. Int Clin
Psychopharmacol 14 95-100.
Poyurovsky, M., Koran, L.M., 2005. Obsessive-compulsive disorder with schizotypy
vs. schizophrenia with OCD: Diagnostic dilemmas and therapeutic implications. J
Psychiatr Res 39 399-408.
Poyurovsky, M., Zohar, J., Glick, I., Koran, L.M., Weizman, R., Tandon, R.,
Weizman, A., 2012. Obsessive-compulsive symptoms in schizophrenia:
Implications for future psychiatric classifications. Compr Psychiatry 53 (5) 480-3.
Reznik, I., Sirota, P., 2000. An open study of fluvoxamine augmentation of
neuroleptics in schizophrenia with obsessive and compulsive symptoms. Clin
Neuropharmacol 23 157-60.
Reznik, I., Yavin, I., Stryjer, R., Spivak, B., Gonen, N., Strous, N., Mester, R.,
Weizman, A., Kotler, M., 2004. Clozapine in the treatment of obsessive-

21
compulsive symptoms in schizophrenia patients: A case series study.
Pharmacopsychiatry 37 52-6.
Simpson, G.M., Glick, I.D., Weiden, P.J., Romano, S.J., Siu, C.O., 2004.
Randomized, controlled, double blind multicenter comparison of the efficacy and
tolerability of ziprasidone and olanzapine in acutely ill inpatients with
schizophrenia or schizoaffective disorder. Am J Psychiatry 161 1837-47.
Stahl, S.M., Shayegan, D.K., 2003. The psychopharmacology of ziprasidone:
receptor-binding properties and real-world psychiatric practice. J Clin Psychiatry
64 Suppl 19 6-12.
Tibbo, P., Kroetsch, M., Chue, P., Warneke, L., 2000. Obsessive-compulsive disorder
in schizophrenia. J Psychiatr Res 34 139-143.
Tranulis, C., Potvin, S., Gourgue, M., Leblanc, G., Mancini-Marie, A., Stip, E., 2005.
The paradox of quetiapine in obsessive-compulsive disorder. CNS Spectrums 10
(5) 356-61.
Veznedaroglu, B., Ercan, E.S., Kayahan, B., Varan, A., Bayraktar, E., 2003. Reduced
short-term obsessive-compulsive symptoms in schizophrenic patients treated with
risperidone: A single-blind prospective study. Hum Psychopharmacol 18 635-40.
Weiden, P.J., Simpson, G.M., Potkin, S.G., O’Sullivan, R.L., 2003. Effectiveness of
switching to ziprasidone for stable but symptomatic outpatients with
schizophrenia. J Clin Psychiatry 64 580-58.
Whitney, K.A., Fastenau, P.S., Evans, J.D., Lysaker, P.H., 2004. Comparative
neuropsychological function in obsessive-compulsive disorder and schizophrenia
with and without obsessive-compulsive symptoms. Schizophr Res. 69 (1) 75-83.
Zohar, J., 1997. Is there room for a new diagnostic subtype–the schizo-obsessive
subtype? CNS Spectrums 2 49-50.

22
Zohar, J., Kaplan, Z., Benjamin, J., 1993. Clomipramine treatment of obsessive
compulsive symptomatology in schizophrenic patients. J Clin Psychiatry 54 385-8.
Zohar, J., Kennedy, J.L., Hollander, E., Koran, L.M., 2004. Serotonin-1D hypothesis
of obsessive-compulsive disorder: An update. J Clin Psychiatry 65 Suppl 14 18-21.

23
Schizophrenia
(without
OCD) (N=16)
ScOCD
(N=29)
ScOCD-
improved
ScOCD-
unimproved
Age 39.25 (15.17) 38.59
(11.77)
F(1,45)=.027 34.6 (11.6) 35.6 (14.3) F(1,29)=.903**
Sex (m/f) 1/15 14/15 χ2
(1)=8.195** 8/7 6/8 χ2
(1)=.037
Mean age at
onset of
schizophrenia
28.93 (12.0)
23.21
(5.33)
F(1,45)=5.404*
21.6 (5.4) 23.6 (6.1) F(1,29)=.333
Mean age at
onset of
OCD
— 18.32
(10.68)
— 15.6 (2.7) 24.6 (13.5) F(1,29)=2.079
Mean
duration of
schizophrenia
(years)
9.29 (9.79)
15.38
(10.35)
F(1,45)=3.386����
13 (11.9) 12 (10.1) F(1,29)=.025
Mean
duration of
OCD (years)
—
15.23
(10.47)
—
18.8 (9.0) 10.6 (9.6) F(1,29)=2.243
Baseline
PANSS
positive
14.38 (5.4) 13.97
(6.0)
F(1,45)=.051 16.1 (6.7) 11.7 (4.4) F(1,29)=4.248*
Baseline
PANSS
negative
26.88 (6.38) 26.31
(5.73)
F(1,45)=.093 27.4 (5.7) 25.1 (5.7) F(1,29)=1.130

24
Baseline
PANSS
general
39.5 (8.68) 48.52
(9.60)
F(1,45)=9/719** 51.4 (9.5) 45.4 (9.0) F(1,29)=3.004
Baseline
PANSS total
80.75 (15.12) 88.79
(17.72)
F(1,45)=2.347 94.9 (16.5) 82.3 (17.1) F(1,29)=4.048*
Baseline
CGI-S
4.44 (.89) 4.76
(.87)
F(1,45)=1.375 5.1 (.8) 4.4 (.7) F(1,29)=6.950*
Baseline
GAF
38.75 (12.5) 37.48
(8.92)
F(1,45)=.156 35.1 (8.3) 40 (9.2) F(1,29)=2.250
Baseline
YBOCS
— 23.97
(6.81)
— 25.5 (6.1) 22.4 (7.3) F(1,29)=1.541
Treated with
SRIs
3 23 χ2
(1)=15.502*** 12 11 χ2
(1)=.009
�p=.07, *p<.05, **p<.01, ***p<.001
ScOCD=Scizophrenia with OCD
Table 1: Mean (SD) and group differences of background and baseline variables for
Schizophrenia patients with and without OCD

25
Week of treatment ScOCD subgroups Week of treatment
X ScOCD
subgroups
YBOCS 8.49** 2.32 34.47***
PANSS positive .61 .28 5.41*
PANSS negative 1.5 .11 8.81***
PANSS general .54 .17 11.53***
PANSS total .66 .003 10.56**
CGI-S 1.08 .67 9.13**
CGI-I 1.46 18.8*** 8.71**
GAF .89 .07 7.35**
*p<.05; **p<.01; ***p<.001
Table 2: Repeated measures ANOVA results (F) for the effect of week of treatment /
ScOCD subgroups and week of treatment X ScOCD subgroups interaction
Week 0 Week 2 Week 5 Week 8 pa
PANSS positive .925
ScOCD 13.97 (6.0) 13.07 (5.8) 14.38 (6.1) 13.83 (6.8) .545
Sc 14.38 (5.4) 14.94 (5.8) 14.00 (5.4) 14.19 (5.8) .646
PANSS negative .007
ScOCD 26.31 (5.7) 26.24 (5.8) 26.62 (5.6) 25.62 (5.6) .297
Sc 26.88 (6.4) 25.19 (5.2) 24.00 (3.9) 24.19 (3.9) .005
PANSS general .549
ScOCD 48.52 (9.6) 47.41 (9.5) 48.97 (11.1) 47.21 (12.72) .602

26
Sc 39.50 (8.7) 38.75 (8.2) 37.19 (7.1) 37.38 (8.0) .292
PANSS total .442
ScOCD 88.79 (17.71) 86.72 (17.6) 89.97 (18.5) 86.66 (21.5) .548
Sc 80.75 (15.1) 78.88 (14.6) 75.19 (12.6) 75.75 (13.6) .133
GAF .377
ScOCD 37.48 (8.9) 38.97 (10.0) 36.48 (10.1) 37.66 (10.9) .454
Sc 38.75(12.5) 39.25 (11.9) 41.94 (10.7) 42.88 (10.2) .031
CGI-S .642
ScOCD 4.76 (.9) 4.72 (.8) 4.93 (.9) 4.76 1.0) .432
Sc 4.44 (.9) 4.44 (.8) 4.31 (.7) 4.25 (.9) .491
CGI-I .680
ScOCD 3.90 (.7) 4.24 (1.3) 3.93 (1.6) .326
Sc 3.94 (.9) 3.50 (1.0) 3.63 (1.1) .110
a Effect for week of treatment
Table 3: Mean (SD) scores for all the study measures and the effect of week of treatment for
ScOCD and Sc patients by week of treatment

27
Figure 1: Distribution of the percentage of improvement in YBOCS from week 0 to
week 8 for ScOCD group

28
Figure 2: Mean (SE) of YBOCS score by week of treatment for ScOCD subgroups
29
A. PANSS positive B. PANSS negative
C. PANSS general D. PANSS total
Figure 3: Mean (SE) of PANSS subscales by week of treatment for ScOCD subgroups

30
A. CGI-S B. CGI-I
Figure 4: Mean (SE) CGI severity and improvement by week of treatment for ScOCD
subgroups

31
Figure 5: Mean (SE) GAF by week of treatment for ScOCD subgroups